OCTOBER 21, 2025
PARTICIPATORY
ARCHITECTURE OF
MEDIUM COMPLEXITY

OCTOBER 21, 2025
PARTICIPATORY
ARCHITECTURE OF
MEDIUM COMPLEXITY
PARTICIPATORY ARCHITECTURE OF MEDIUM COMPLEXITY
AD2025
INSTITUTO TECNOLÓGICO DE ESTUDIOS SUPERIORES DE MONTERREY, CAMPUS QUERÉTARO.
TEACHING TEAM
RODRIGO PANTOJA CALDERÓN | ARCHITECT AND
LANDSCAPE ARCHITECT
DIANA GARCÍA CEJUDO | MSC IN ARCHITECTURE
PEDRO MENDOZA | ARCHITECT
YETZI VERÓNICA TAFOYA TORRES | URBAN PLANNER
ANDREA MARÍA PARGA VAZQUEZ | EDITORIAL
VIVIANA MARGARITA BARQUERO DÍAZ BARRIGA | ARCHITECT
DANIELA CRUZ NARANJO | ARCHITECT
SANTIAGO LUJÁN CÓRDOVA | ARCHITECT
CARLOS GONZÁLEZ | ARCHITECT
UDO PAUL MUCHOW | ARCHITECT
ALLIANCES
IIT - ILLINOIS INSTITUTE OF TECHNOLOGY
ROGELIO CADENA, JUSTIN DEGROFF, DIRK DENINSON
STUDENT
ALFONSINA ESPINOSA AZUARA

In Chicago, Latino adults face uninsured rates nearly three times higher than those of nonHispanic white residents. For thousands of families, this means living on the edge: a chronic illness or accident could immediately trigger financial hardship, limiting their access to even the most basic healthcare services.

Socioeconomic inequality
Immigrant population
Unequal access to services
1 in every 5 adults is uninsured
→ Postponement of medical care
Dental Care Medical Care
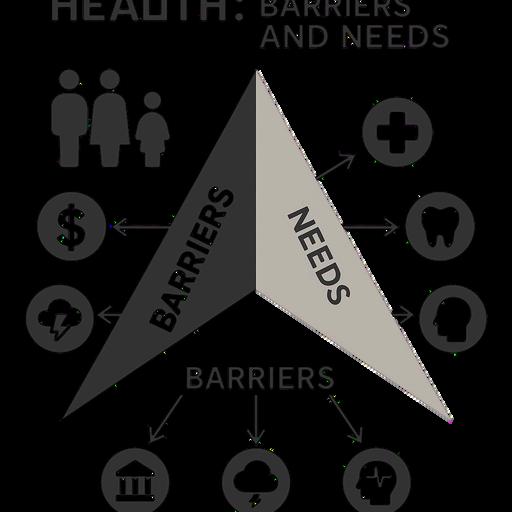
Health
Integrated Well-Being
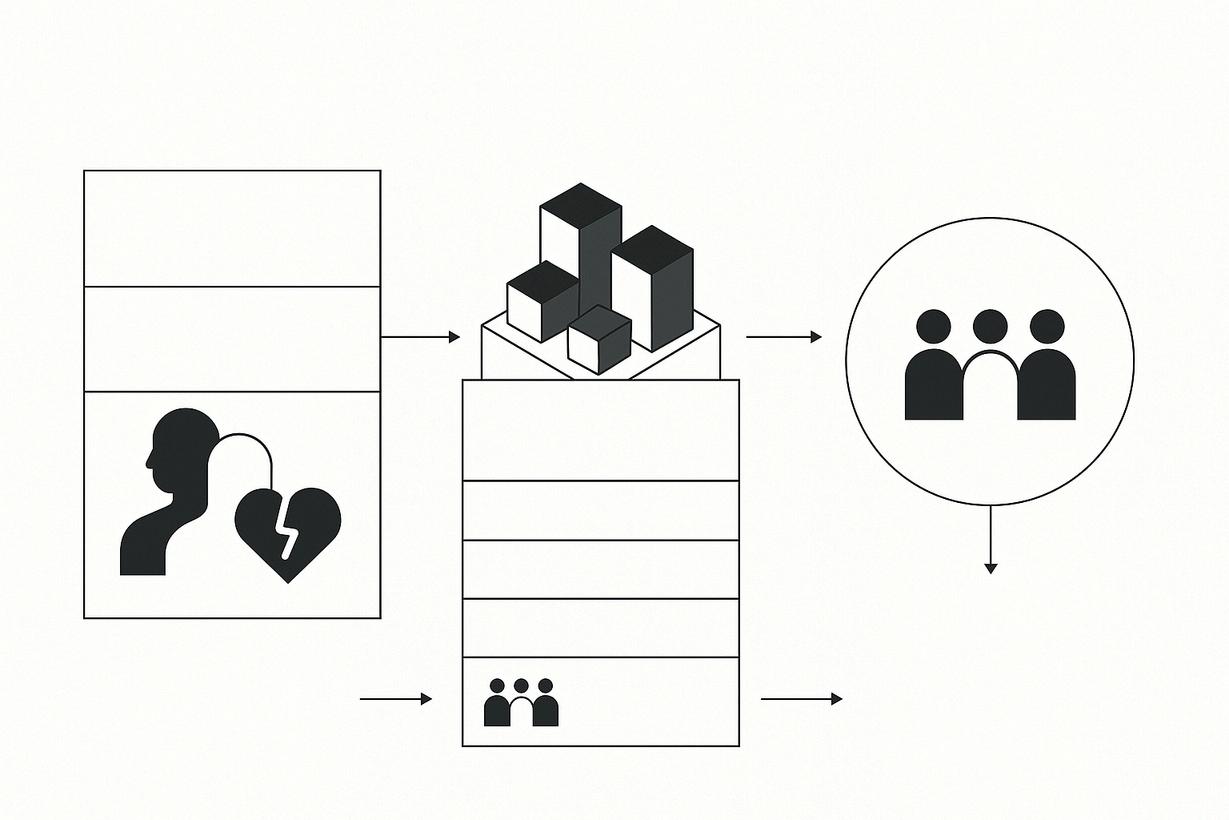
The diagram shows how socioeconomic inequality, a large immigrant population, and unequal access to services in Chicago contribute to a major healthcare coverage gap In some groups, 1 in 5 adults is uninsured, causing delays in medical, dental, and mental health care
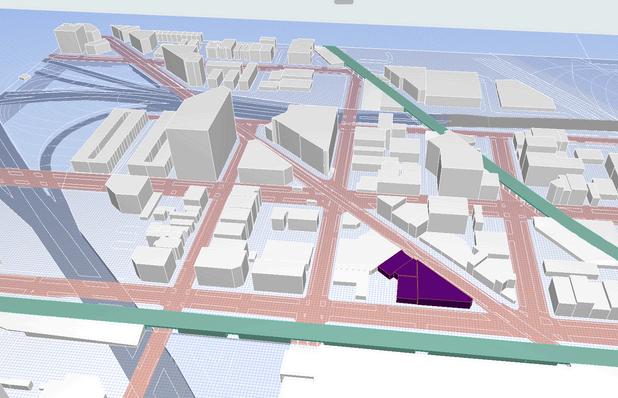
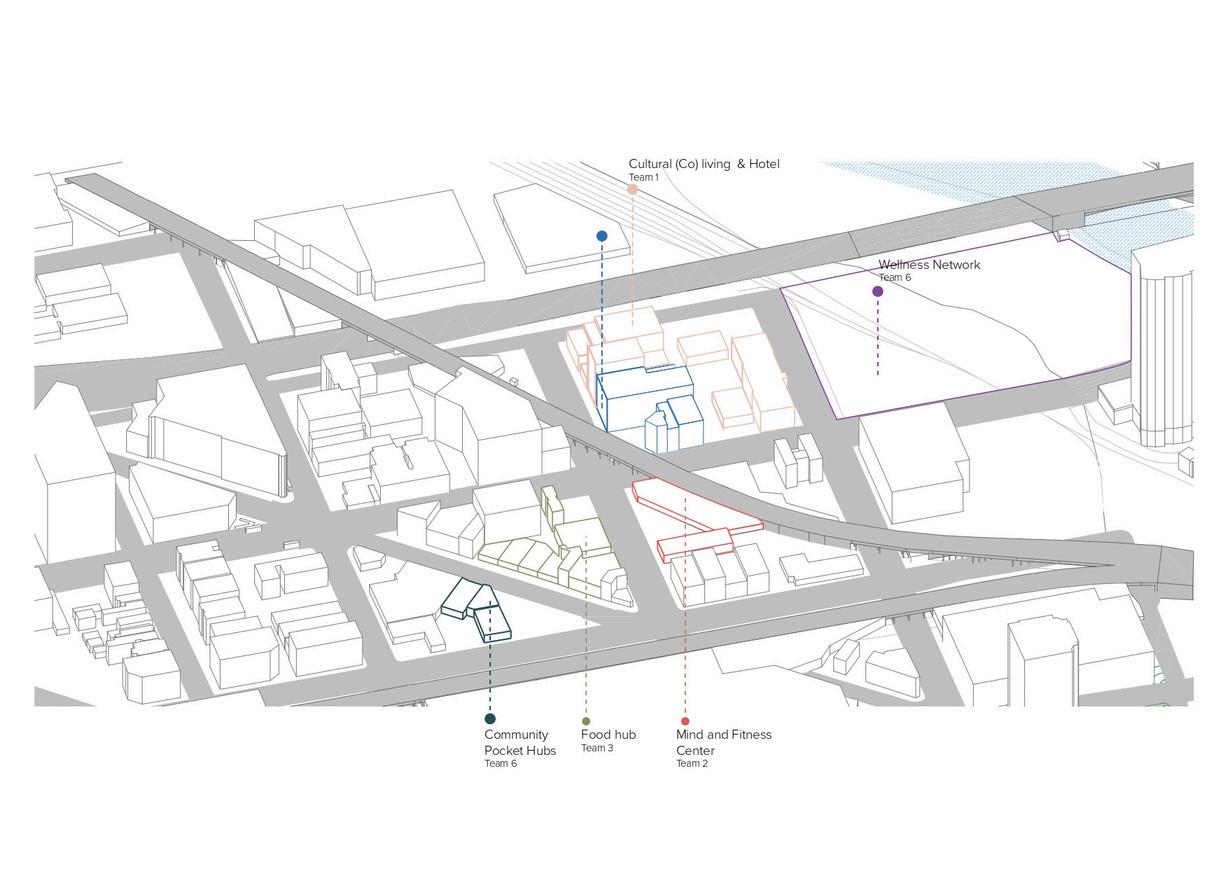
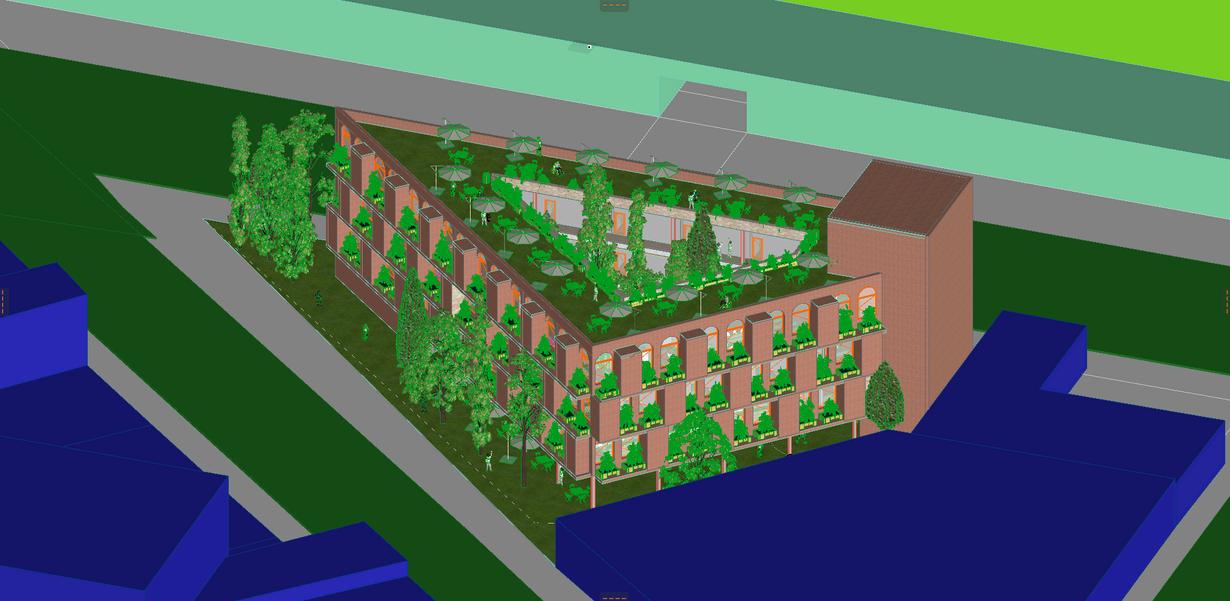
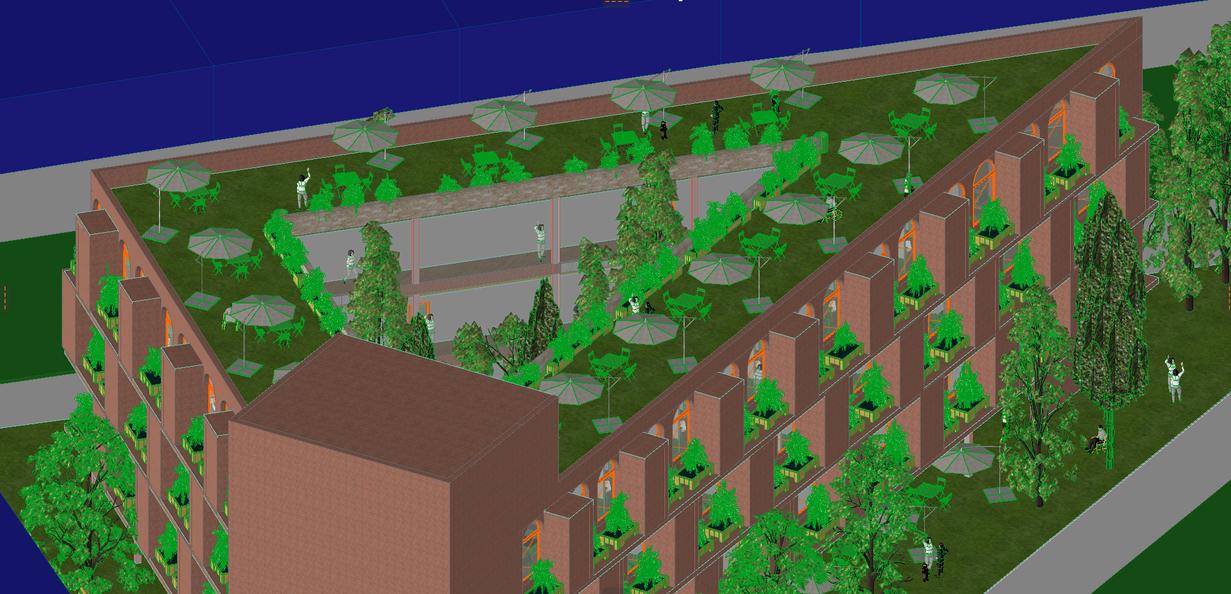
To address this issue, the proposal introduces the Community Pocket Hubs neighborhood-scale centers that integrate essential healthcare services with community activation and social programs. Their purpose is to support accessible preventive care while strengthening social cohesion.
The final outcome illustrated is integrated well-being, achieved through improved access, prevention, and community connection.
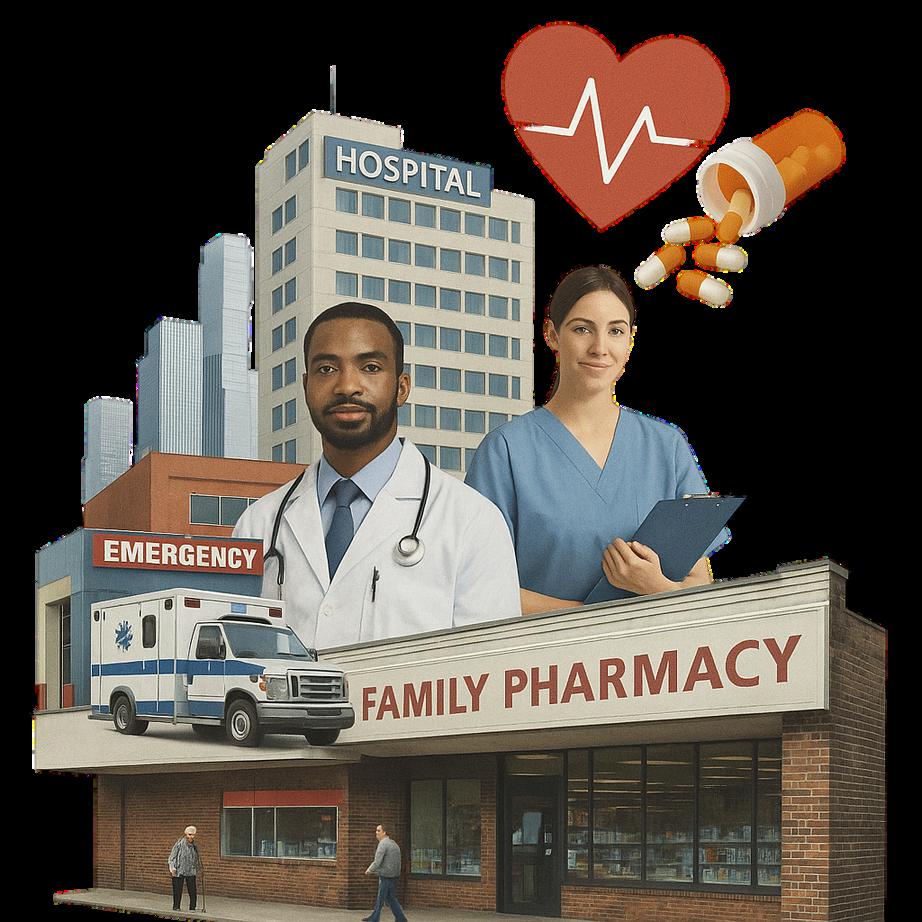
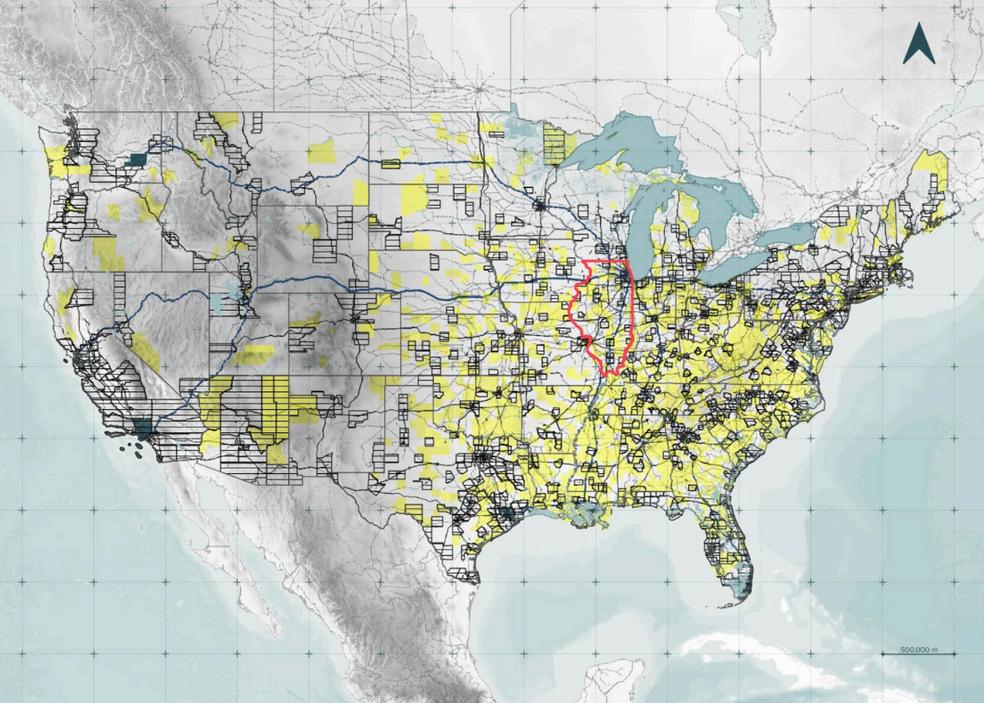
The U.S. healthcare system reflects a market-based model in which access to medical services is not universally guaranteed. The combination of unregulated pricing and complex administrative structures has produced one of the most expensive systems in the world, generating significant inequities in who can obtain timely and adequate care.
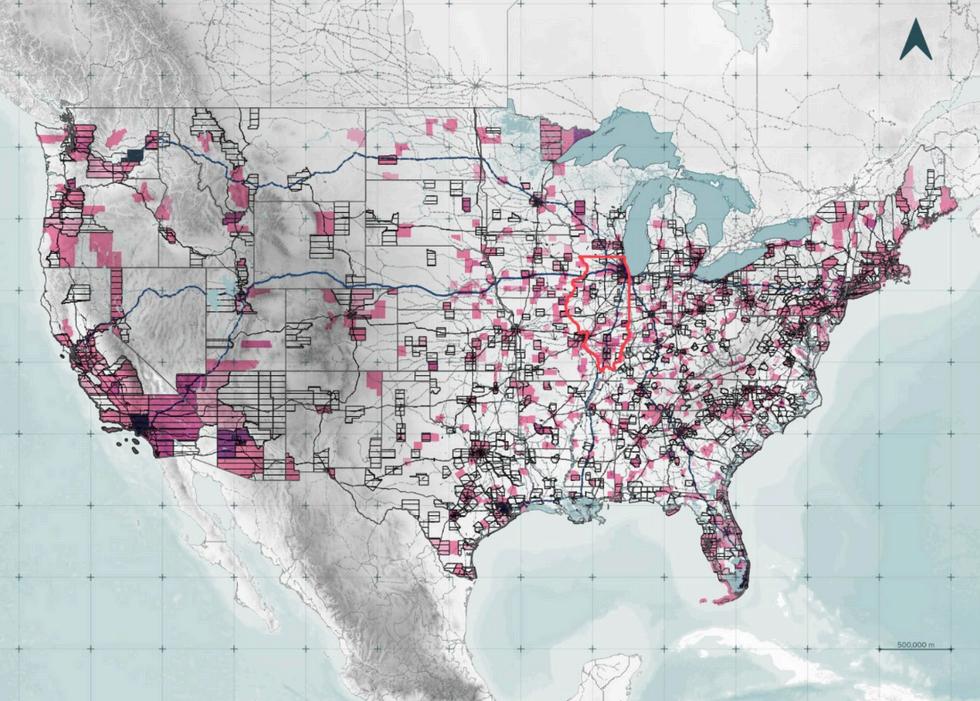
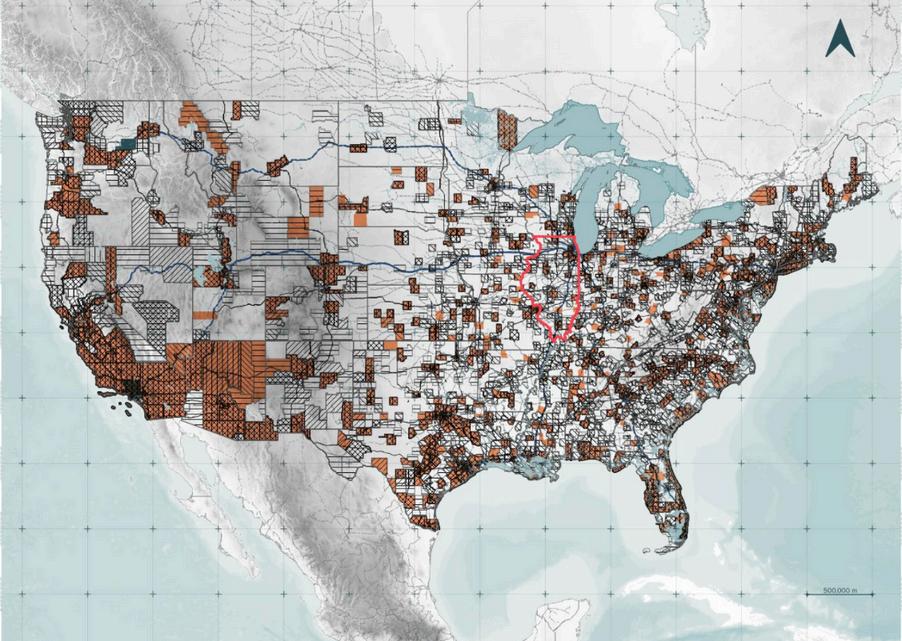
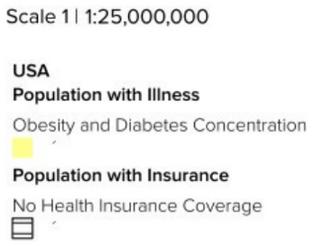
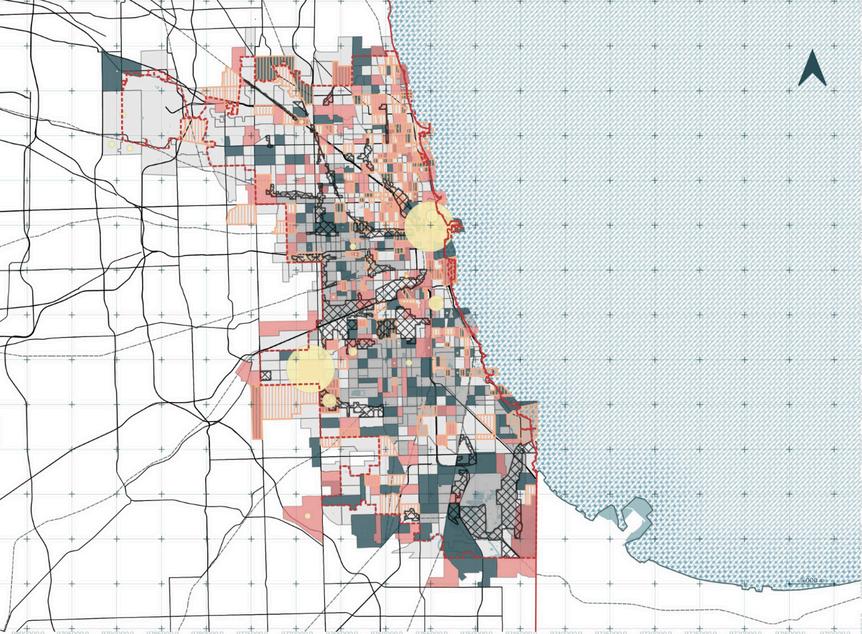
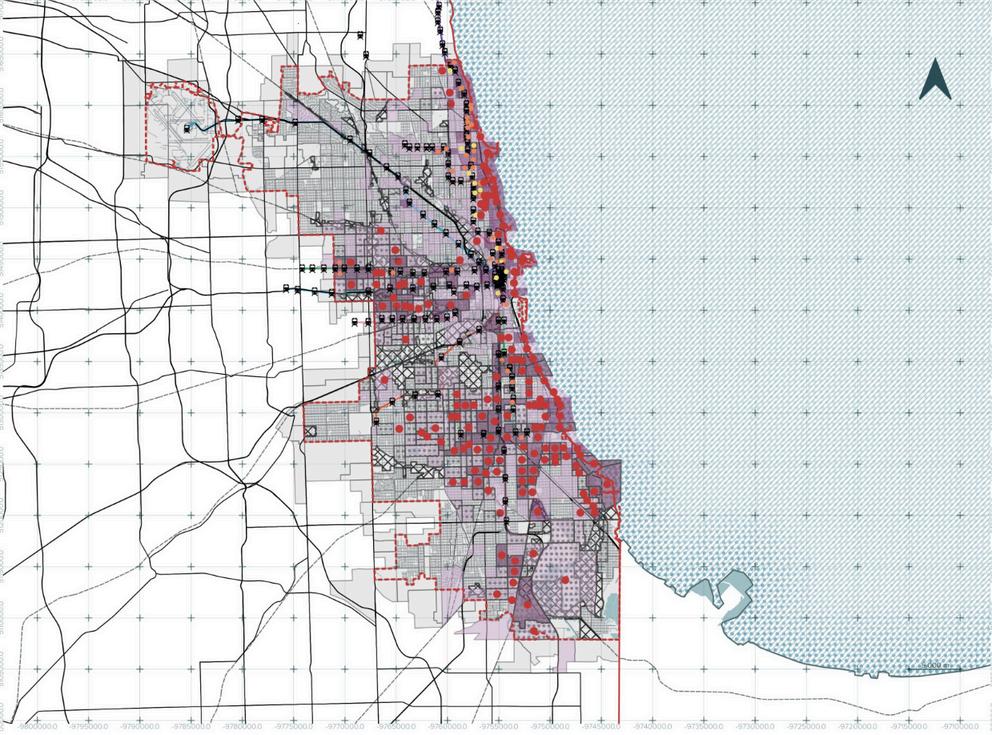
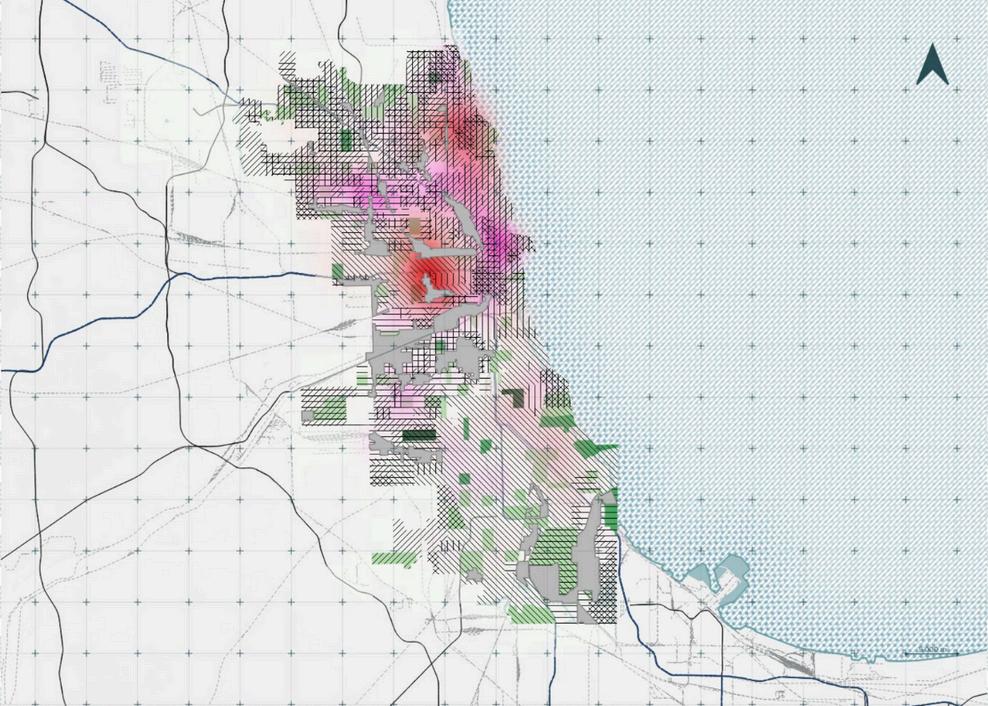
In major U.S. cities and especially in Chicago healthcare access has splintered into a pattern of urban medical segregation. High costs, insurance disparities, and uneven city planning have created neighborhoods where clinics, specialists, and mental-health services are almostabsent.
On Chicago’s South and West Sides, uninsured rates reach up to three times those of wealthier, majority-white districts. This forces residents to postpone care, endure silent deterioration, and face emergencies that generate crushing medicaldebt.
The issue is not simply about cost it is a structural urban failure that consistently leaves the same communities without the basic healthcare infrastructure required to preventavoidablesuffering.


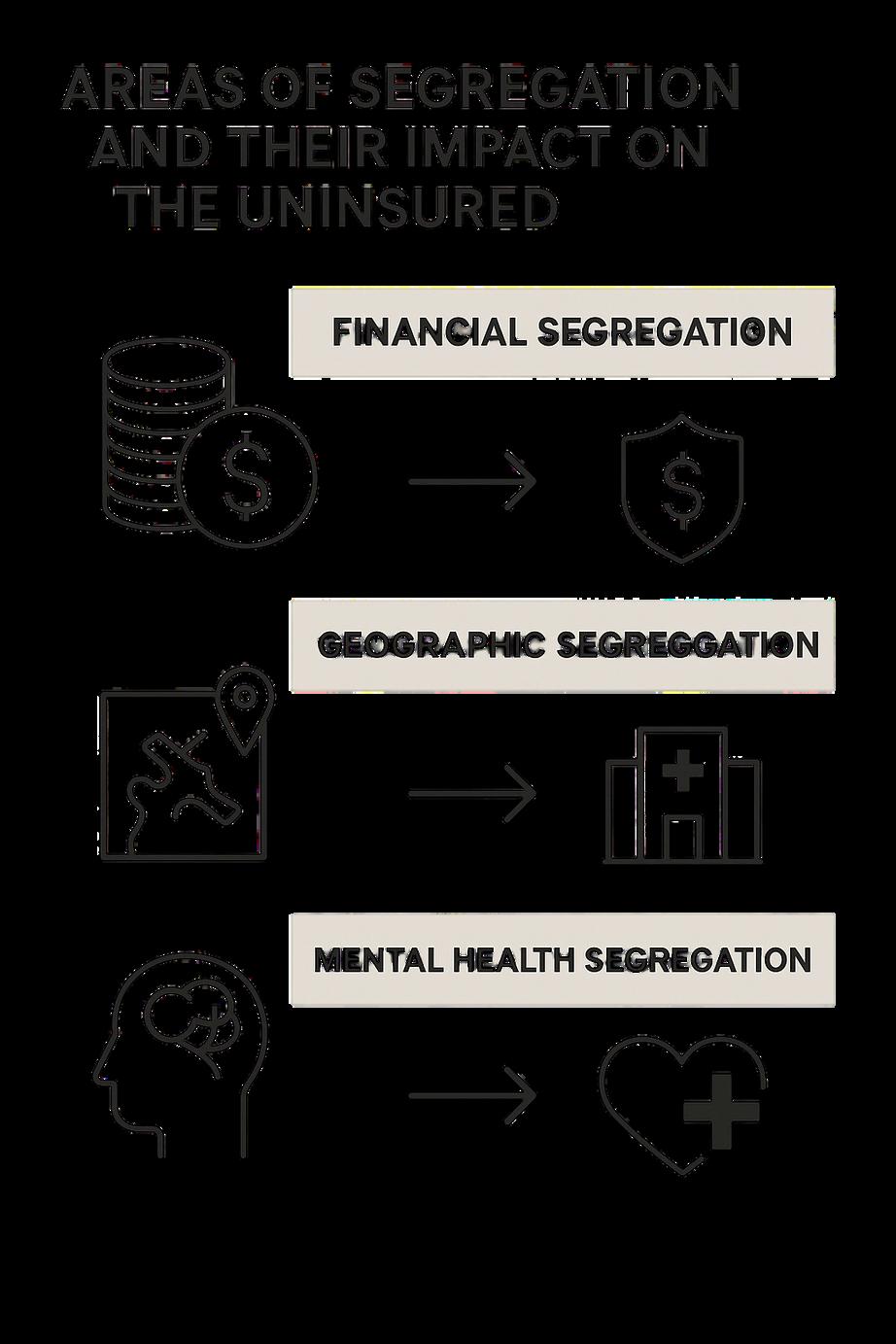
Medical segregation is the systemic, unequal distribution of healthcare resources and quality based on race, socioeconomic status, and ability to pay.
This diagram illustrates three structural forms of segregation that shape the lived reality of uninsured communities.
Financial segregation highlights how the cost-driven healthcare system restricts access to those who can afford high-tier coverage.
Geographic segregation shows how low-income neighborhoods often designated as “health deserts” lack essential medical and mental health facilities, forcing residents to rely on distant or overcrowded services
Mental health segregation underscores how psychological and psychiatric care remain inaccessible luxuries, leaving vulnerable populations without the support needed to maintain emotional and social wellbeing.
Together, these layers reveal how systemic barriers intersect, reinforcing inequality and limiting access to even the most fundamental forms of care.
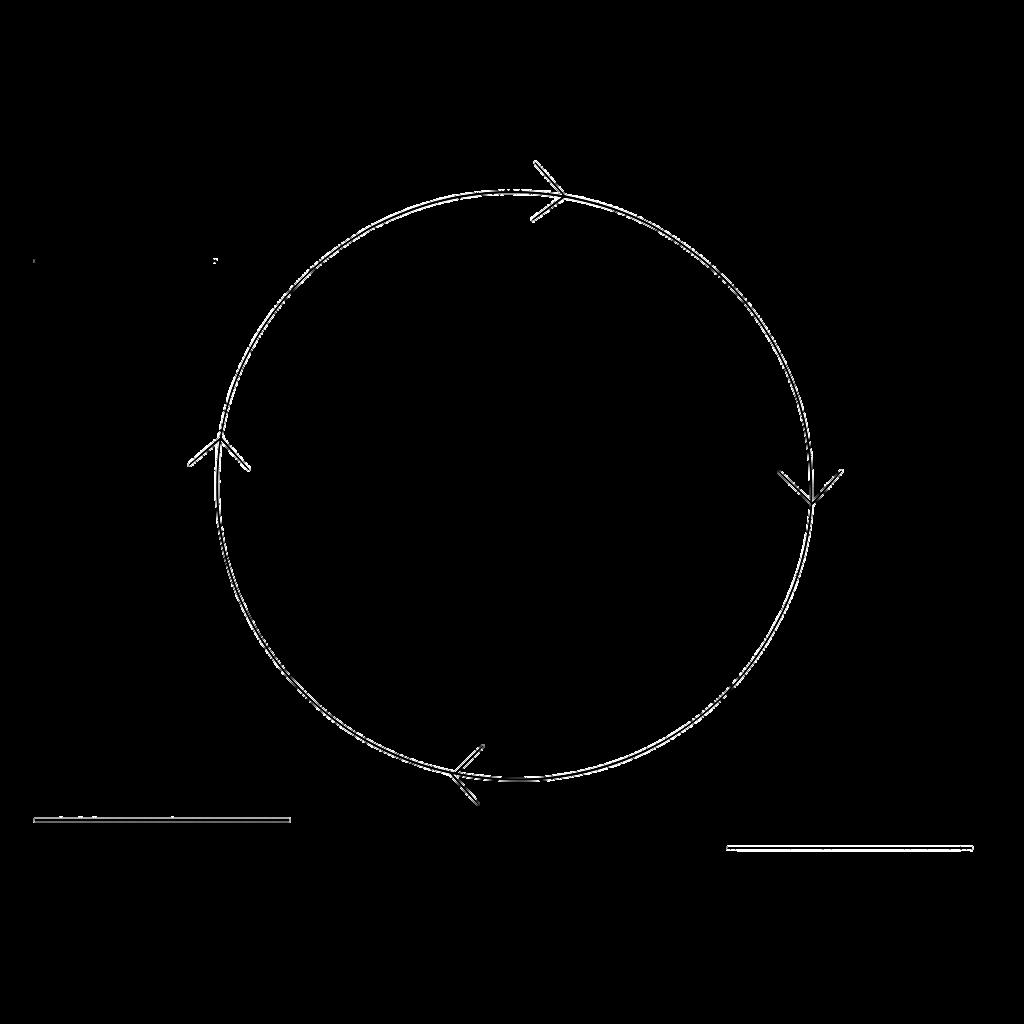
This diagram illustrates how vulnerable populations become trapped in a repeating loop of health exclusion. In the United States, 11% of adults remain uninsured, but the burden is far greater in marginalized groups: among Hispanic adults, the rate rises to 24.6%, and in several Chicago neighborhoods such as Little Village or Brighton Park it reaches 26–27%
Without insurance, people avoid seeking care due to cost, leading to silent deterioration until conditions become emergencies. Emergency visits then generate overwhelming medical debt, deepening financial instability. This debt pushes individuals further away from the healthcare system, causing relapse and renewed exclusion, which restarts the cycle.
The circular nature of the diagram emphasizes how each stage reinforces the next, creating a structural trap that disproportionately affects low-income and minority communities.
RUIN AND MASSIVE DEBT
MASSIVE
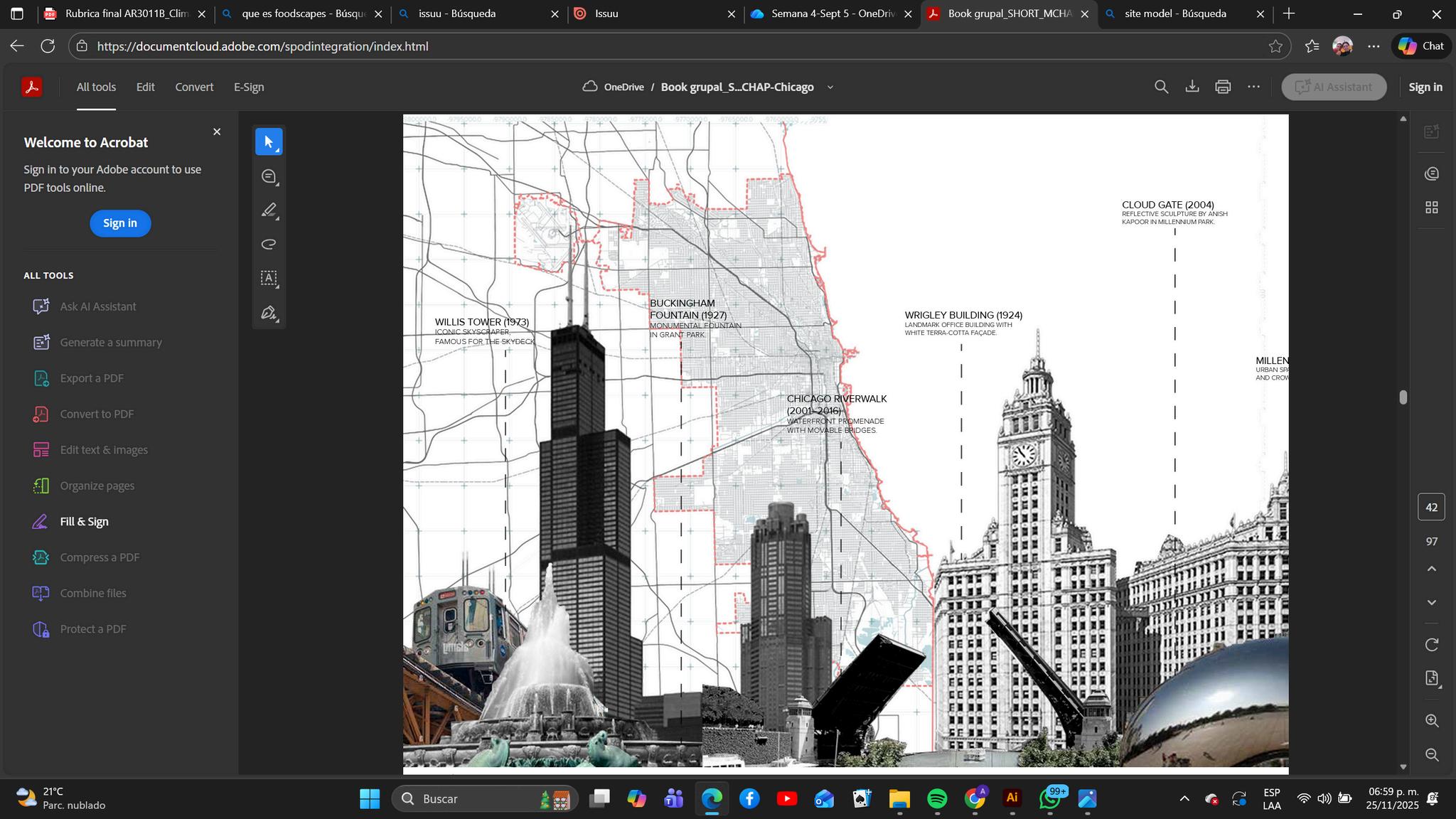
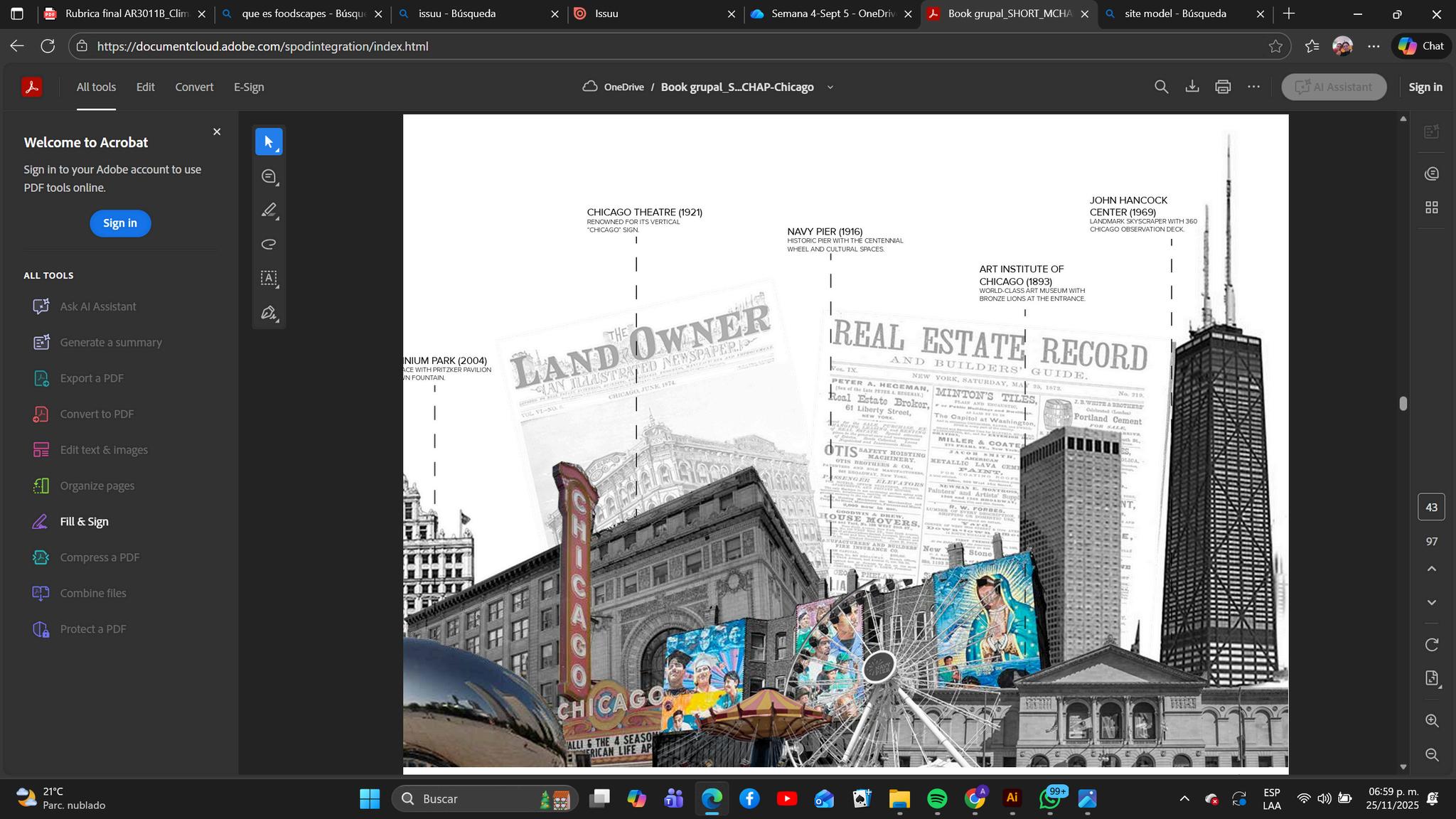
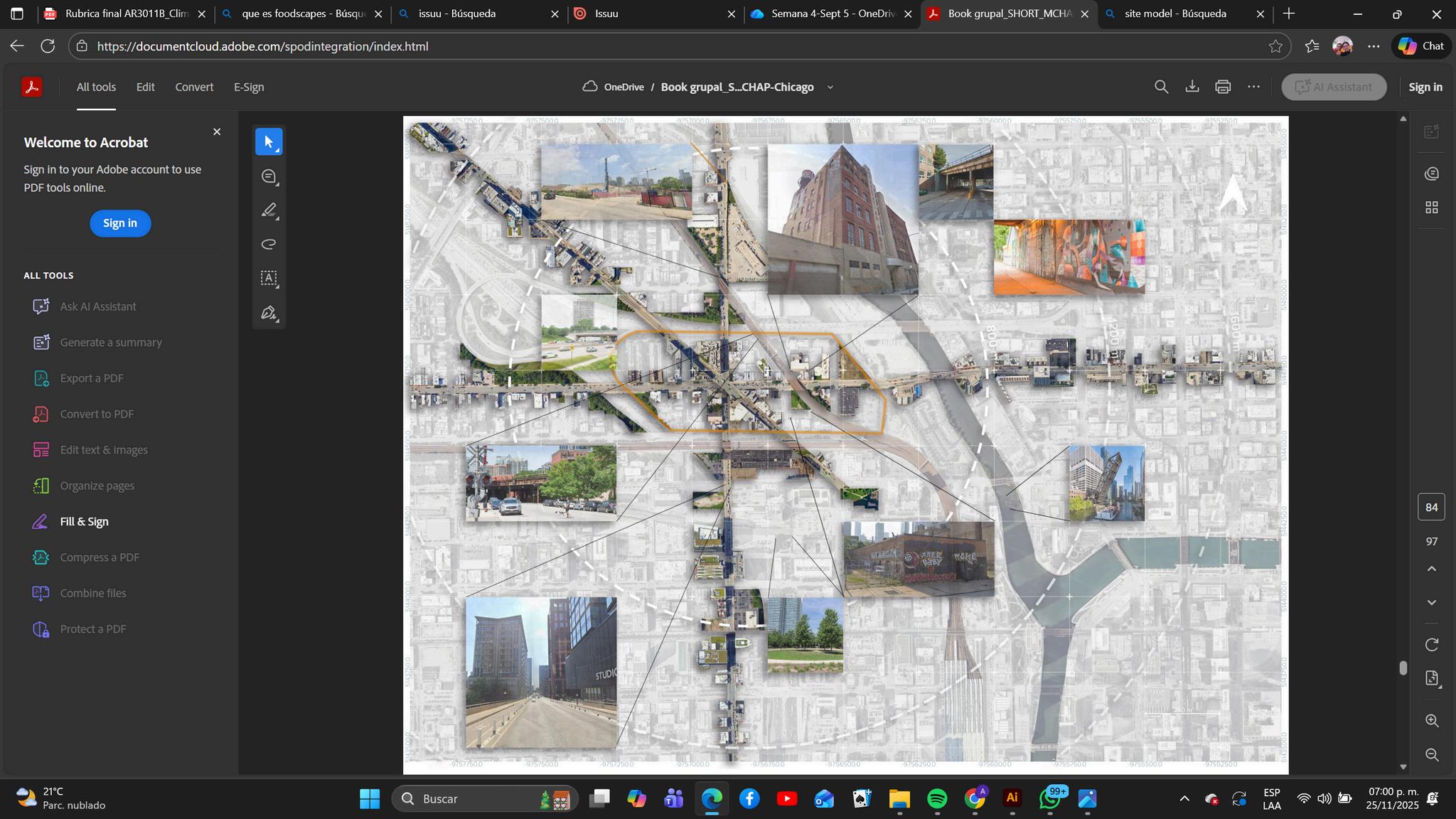
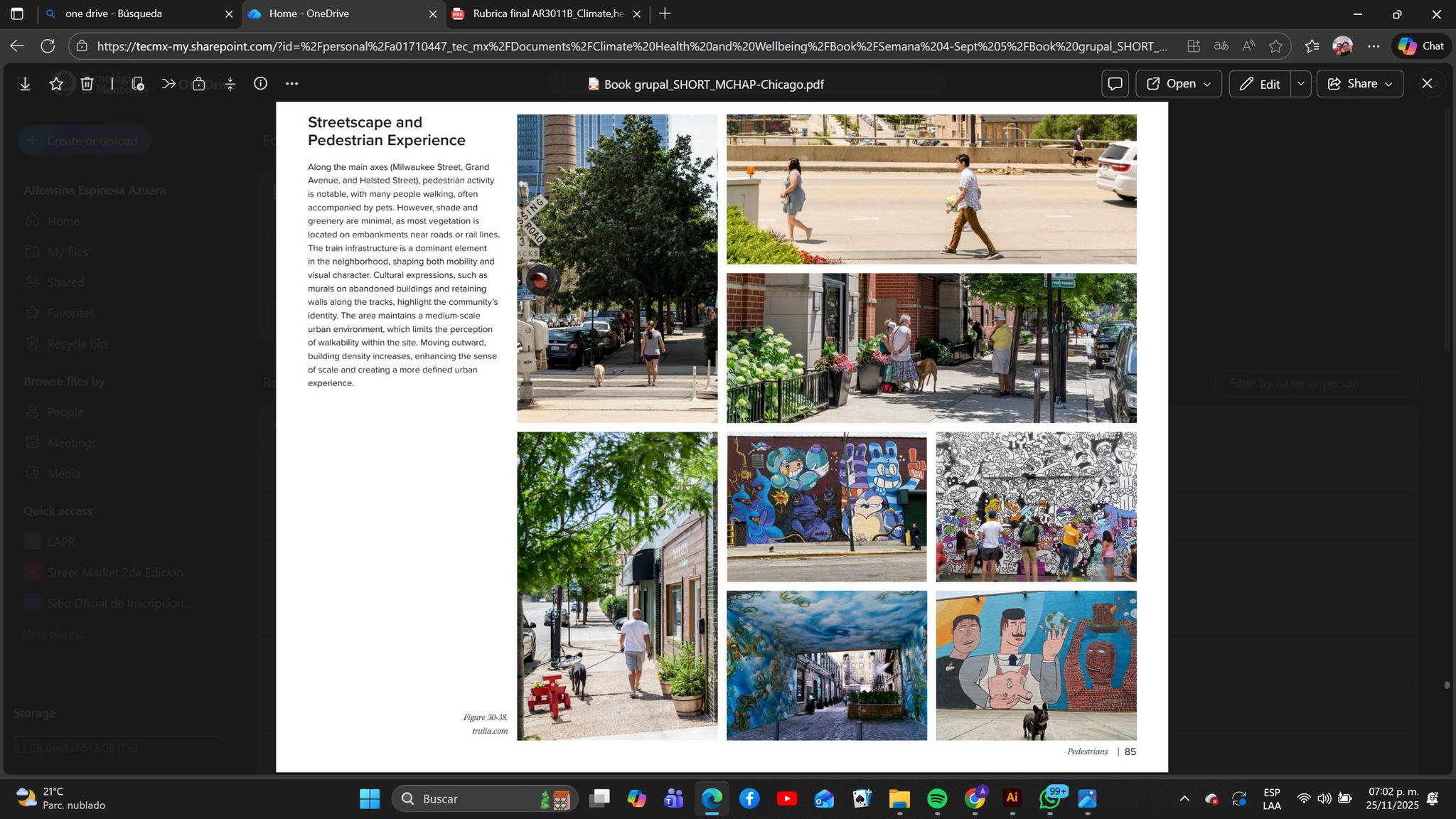
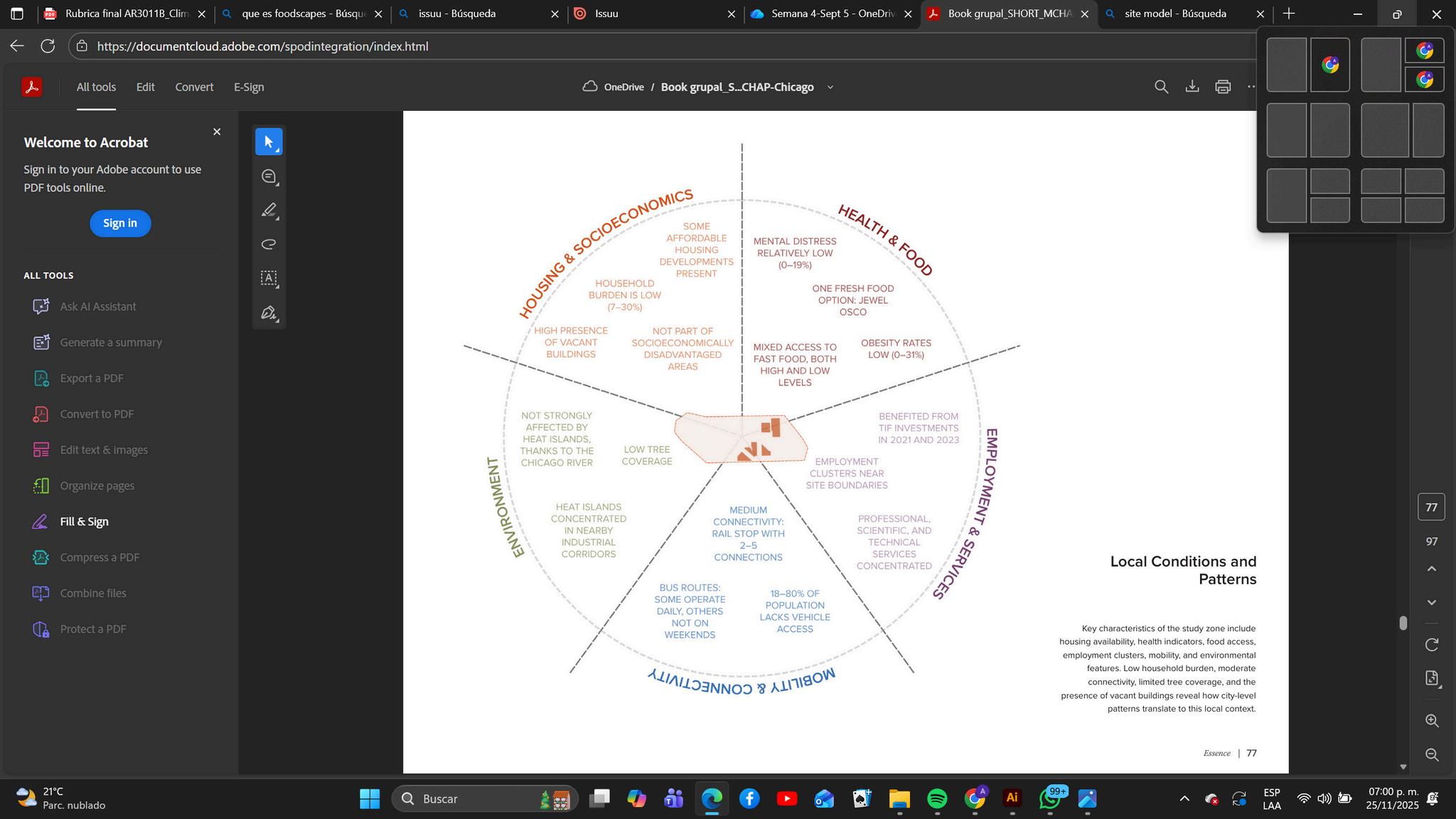



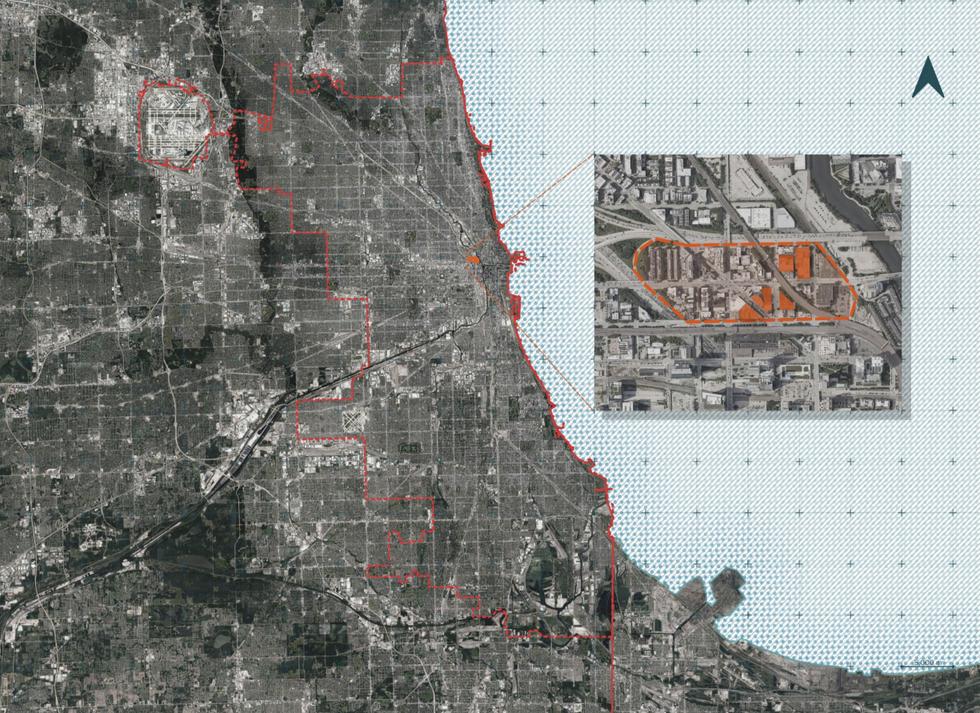

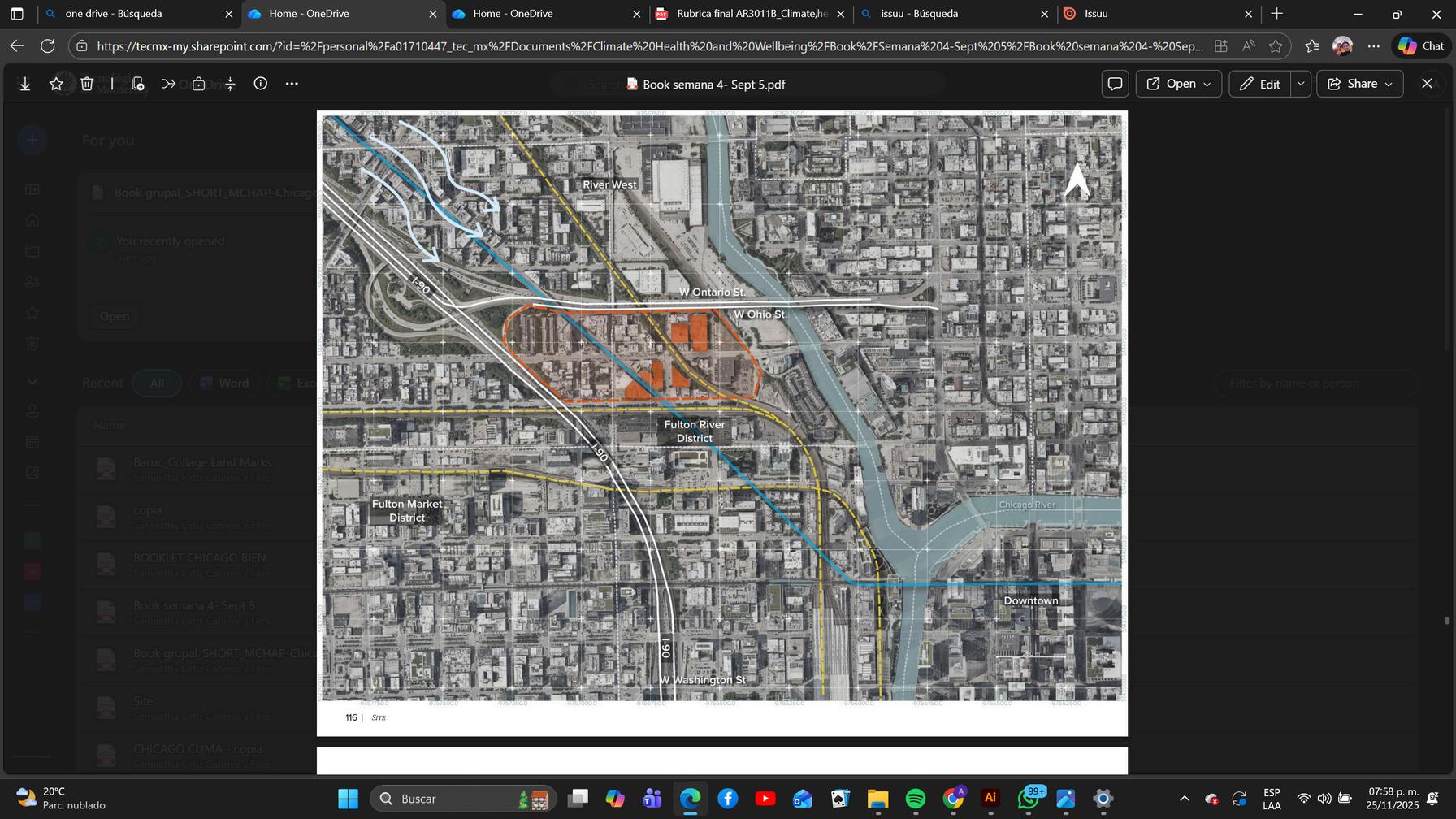
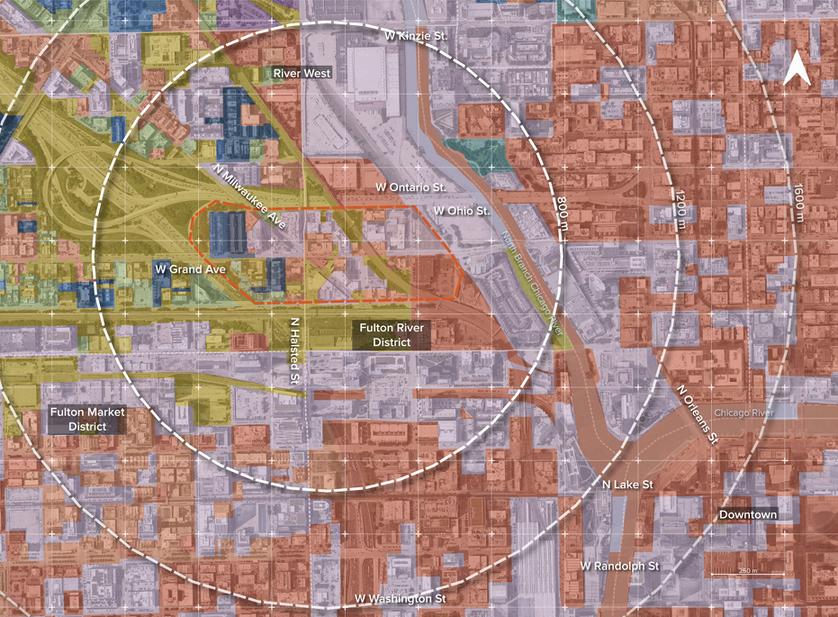
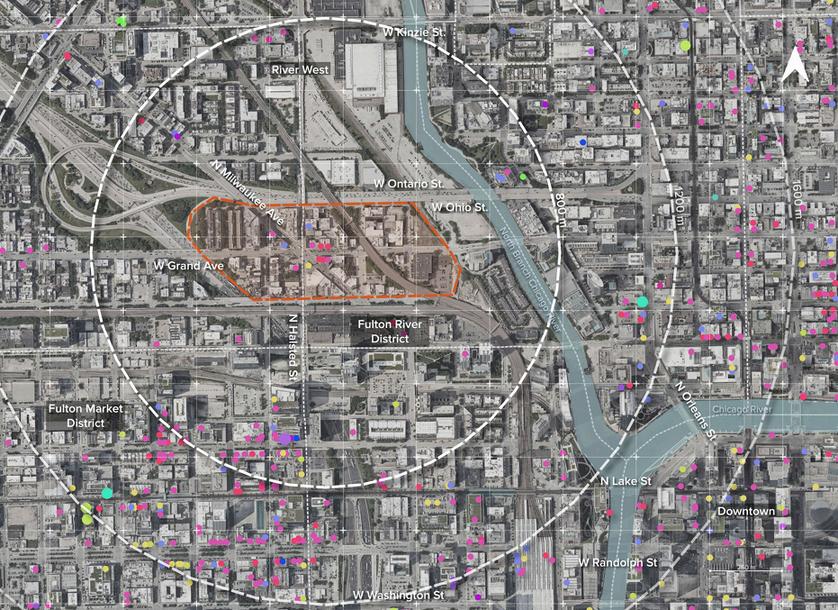
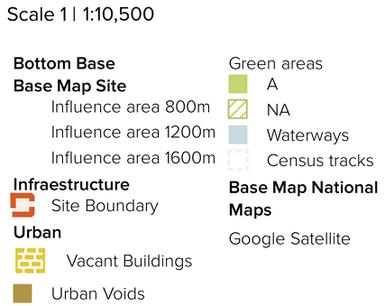
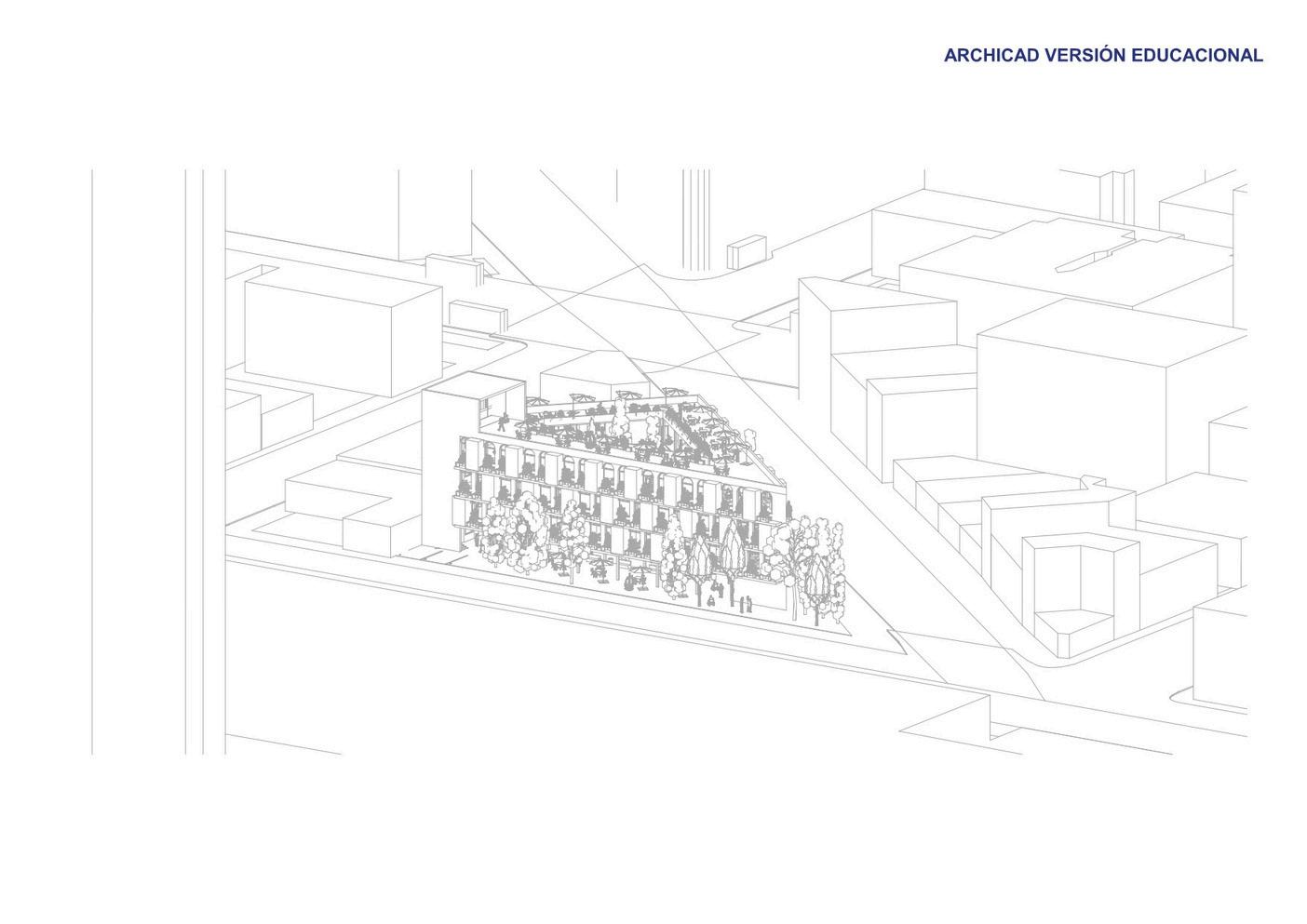
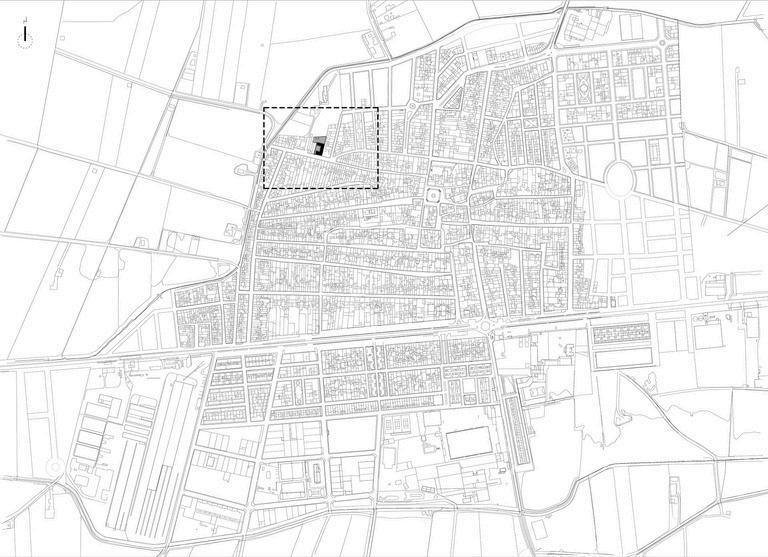
The study area, located in Chicago’s northwestern edge near Downtown, has evolved into a high-income, predominantly white enclave. Over the past two decades, massive reinvestment has reshaped the district, replacing industrial infrastructure and working-class immigrant communities with high-density housing, retail clusters, and tech-oriented office spaces. This wave of adaptive reuse marks a shift in Chicago’s economic priorities: historic industrial shells have been converted into creative workplaces and lifestyle developments, while the area’s original cultural and economic identity has been systematically displaced.






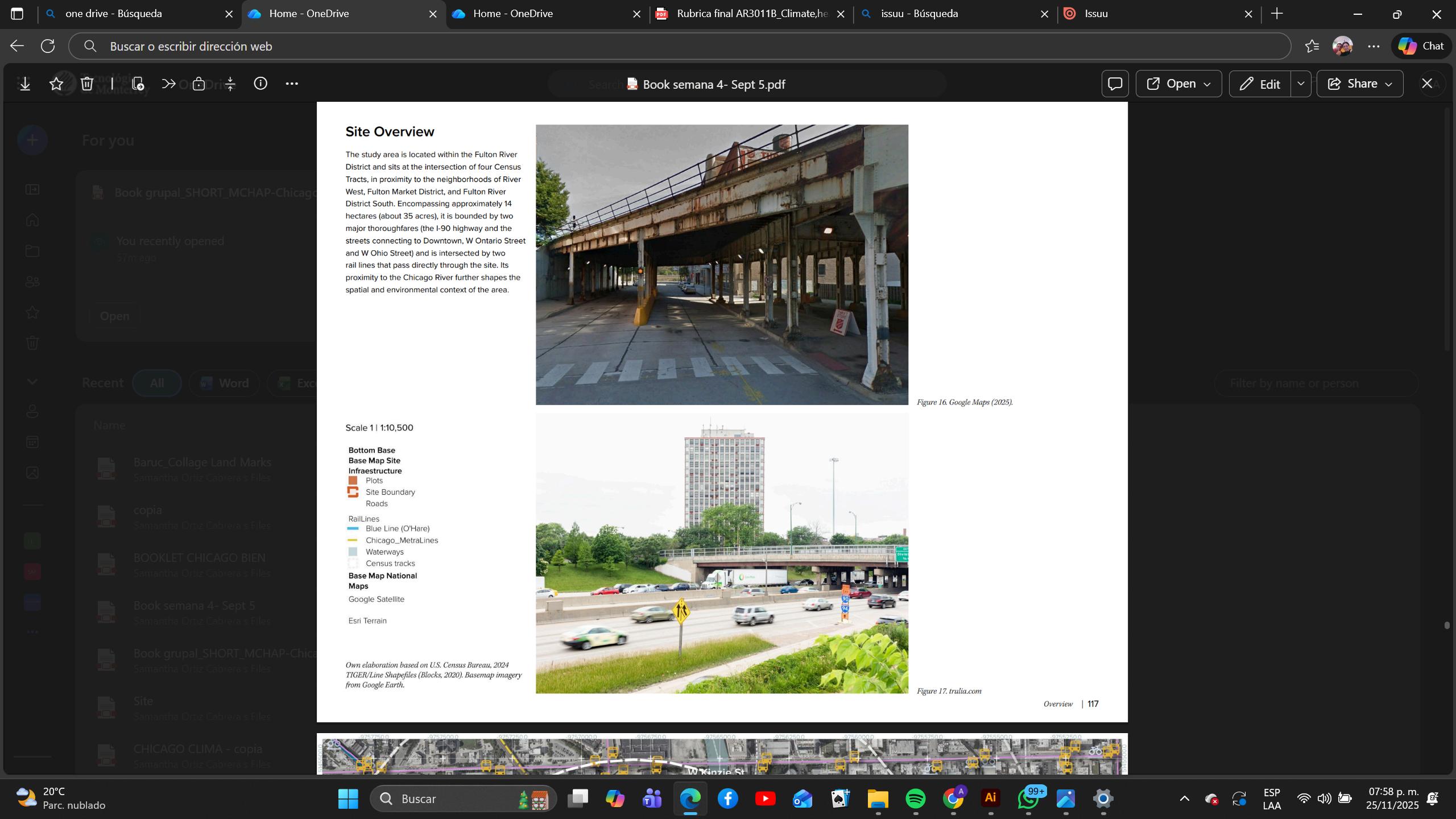

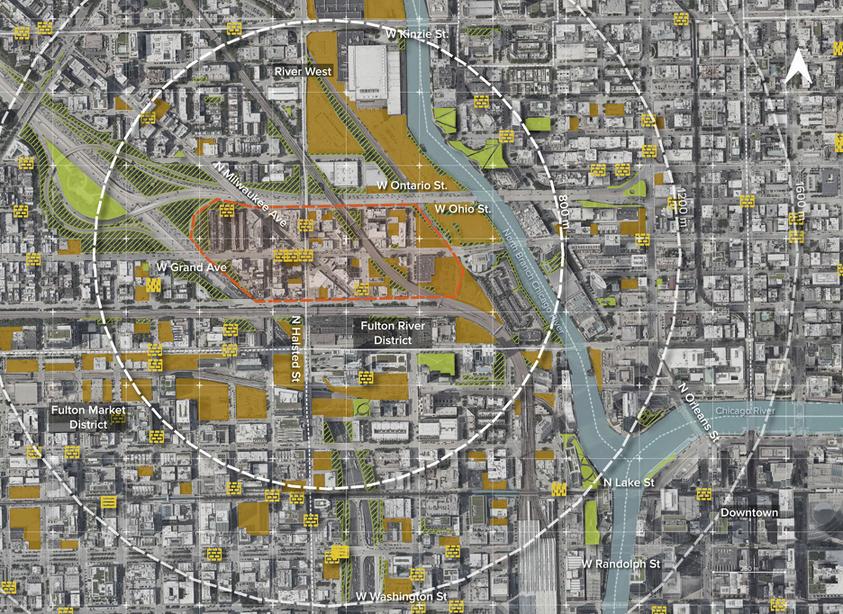

Primary
Railway
Housing


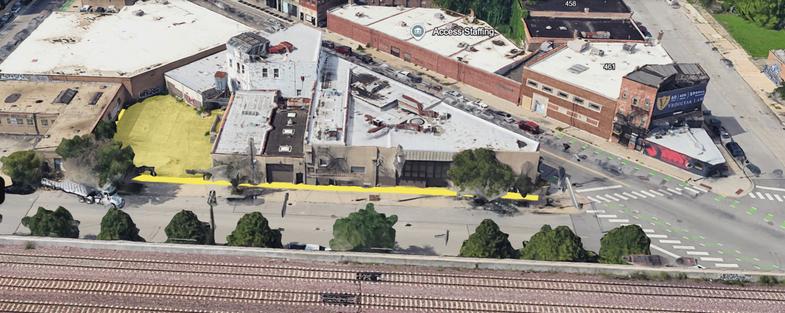




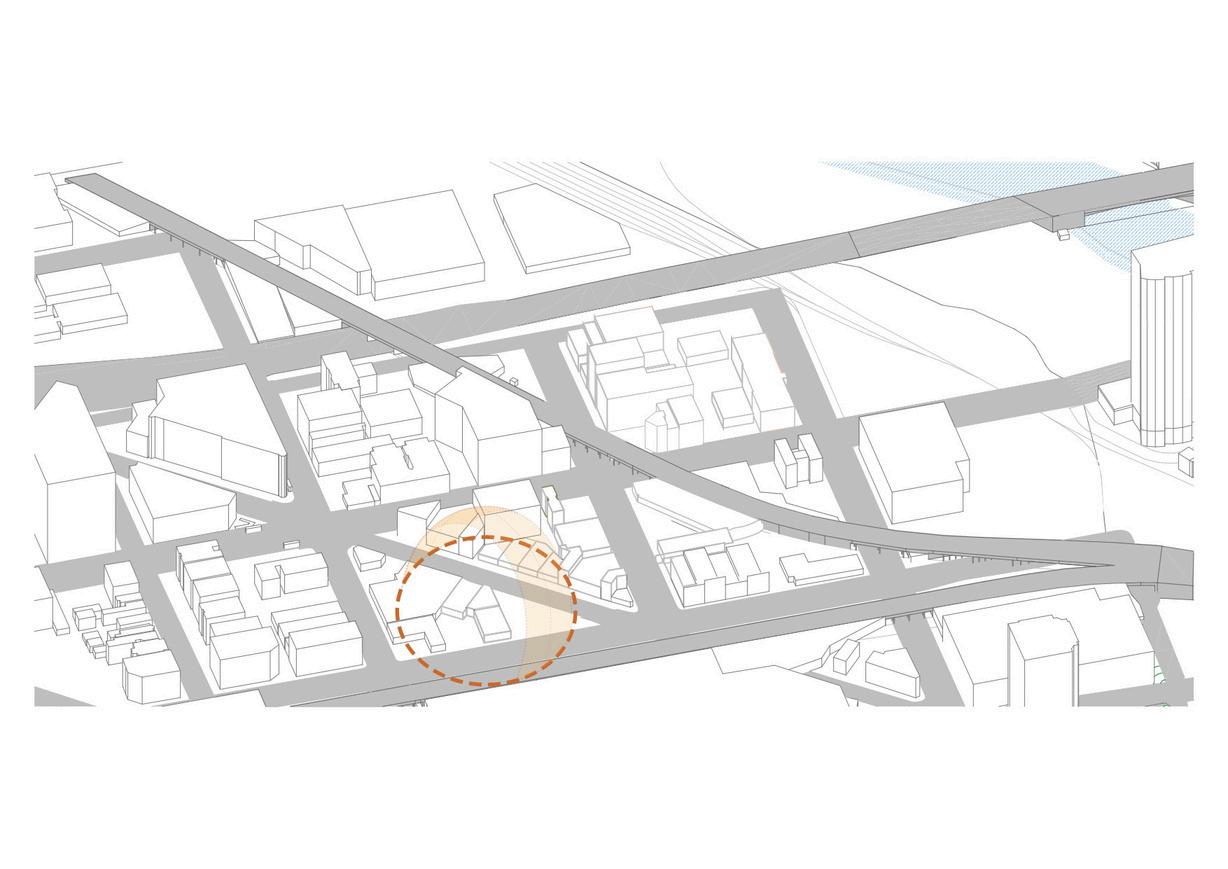
Roads Site
Prevailing winds from the west Buildings

36 YEARS OLD LATINO
UNINSURED CHICAGO ESSENTIAL WORKER
ECONOMIC BARRIERS
LOW INCOME
HIGH COSTS PRIORITIZING
RENT & FOOD
SOCIAL & LEGAL BARRIERS
FEAR LANGUAGE
LIMITED INFORMATION
NEEDS
MEDICAL CARE
DENTAL CARE
COMMUNITY
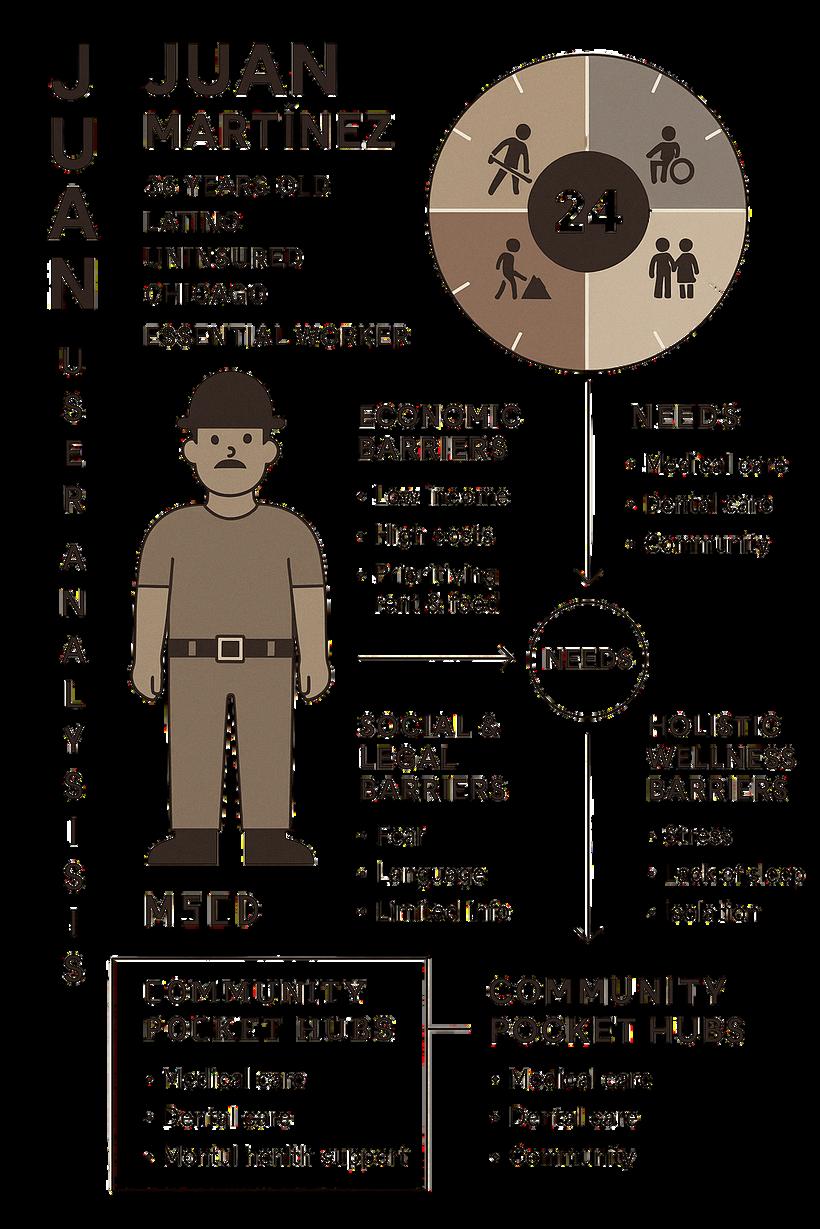
HOLISTIC
WELLNESS
BARRIERS
STRESS
LACK OF SLEEP ISOLATION


BRIDGINGTHEHEALTHEQUITYGAP
DESCENTALIZED COMMUNITYHEALTH MODEL
BRIDGINGTHEHEALTHEQUITYGAP
BARRIERS HUB ACCESS
INTEGRATED,BARRIER-FREECARE
ESSENTIALMEDICALCARE
DENTALSERVICES
MENTALHEALTHPRIORITYCARE
SOCIALCOHESION
Workshops and community spaces fostering well-being and community support.

The core objective of the Community Pocket Hubs is the eradication of health access barriers.
The project is established under the fundamental mandate of ensuring that all individuals, regardless of their socioeconomic status, immigration condition, or mental health history, can access comprehensive and high-quality care.
Additional Purpose: The architectural and social infrastructure of the Hub actively seeks to narrow the social inequality gap in Chicago by neutralizing cost as a factor of exclusion and fostering community cohesion through shared wellbeing.
In a city where health is treated as a commodity, what is the true cost of being uninsured? The Community Pocket Hubs project is defined as the design of a zerocost, integrated community health center, a direct architectural and social intervention confronting the systemic inaccessibility of healthcare in Chicago. Conceived to break the vicious cycle of sickness and debt, the Hub critically merges essential access to medical, dental, and psychological care, eliminating the economic barrier that forces vulnerable populations to postpone care until illness becomes a crisis. Beyond clinical provision, the design intentionally integrates workshops and socialization spaces to act as an anchor of resilience, addressing the mental health crisis and social isolation. By being strategically situated in an area of rapid gentrification, the Hub establishes itself as a beacon of equity, asserting the right to health above economic profit.
INACCESSIBLEHEALTHCARE
CHOICEBETWEENHEALTH&
FINANCIALRUIN

CYCLEOFSICKNESSANDDEBT
POSTPONEDCARE
WORSENINGILLNESSES
MENTALHEALTHCRISES
SOCIALISOLATION
COMMUNITYPOCKETHUBS
ZERO-COST,INTEGRATEDWELLNESSCENTER
ARTWORKSHOPS
SOCIALIZATIONSPACES
FOSTERINGBELONGINGANDEMOTIONALWELL-BEING
ANCHORFORCOMMUNITYRESILIENCE
ARTWORKSHOPS
SOCIALIZATIONSPACES
FOSTERINGBELONGINGANDEMOTIONALWELL-BEING
STRATEGICALLYLOCATEDINAREAS
RESTRUCTUREDBYGENTRIFICATION
THERIGHTTOHEALTHABOVEECONOMICPROFIT.
HOLISTICWELLNESSBARRIER
CHRONICSTRESS
ISOLATION
UNADDRESSED
PHYSICAL CONDITIONS
SOCIAL&LEGALBARRIER
LACKOF RESOURCES
UNDER-SERVED COMMUNITIES IMMIGRANT CHALLENGES
ECONOMICBARRIER
LOW-INCOME STATUS UNINSURED POPULATION HIGH HEALTHCARE COSTS
The Community Pocket Hubs model transcends Chicago's borders, establishing itself as a deeply replicable and urgently needed architectural and social prototype on a global scale. Within the United States, it offers a proven solution to mitigate financial, geographical, and mental health segregation in countless cities and healthcare deserts where access to health remains a privilege. Internationally, the design can be adapted by developed nations with fragmented systems or by communities facing migration crises, serving as critical urban survival infrastructure for refugees, immigrants, and any vulnerable population. Essentially, the Hub demonstrates that a comprehensive, zero-cost, human-centered health model is universally applicable and vital for transforming health into a fundamental right in any global context.
A public place for people to meet, socialize, learn, and access recreational or support services.
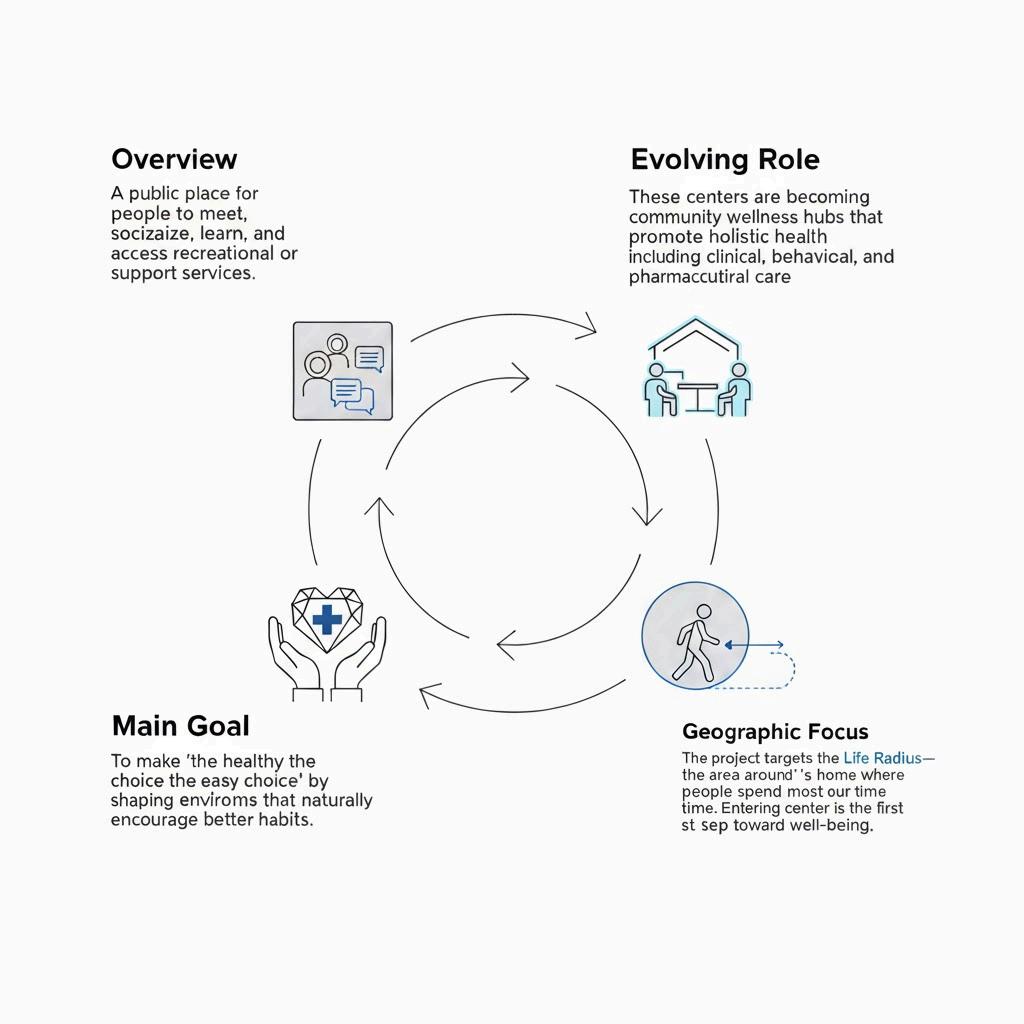
To make “the healthy choice the easy choice” by shaping environments that naturally encourage better habits.
These center are becoming community wellness hubs that promote holistic health including clinical, behavioral, and pharmaceutical care.
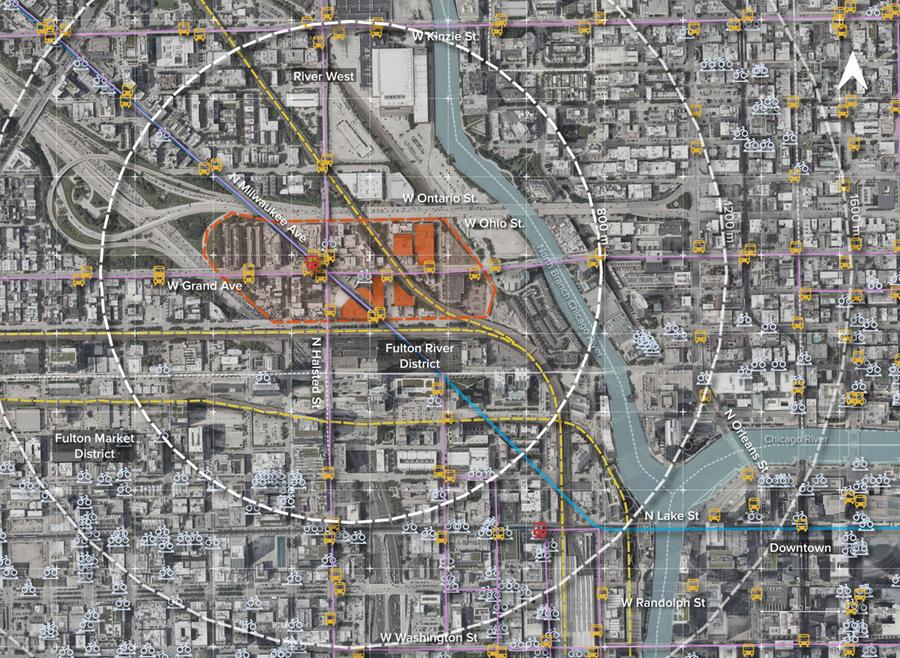
The project targets the Life Radius the area around one’s home where people spend most of their time.
Entering the center is the first step toward well-being.
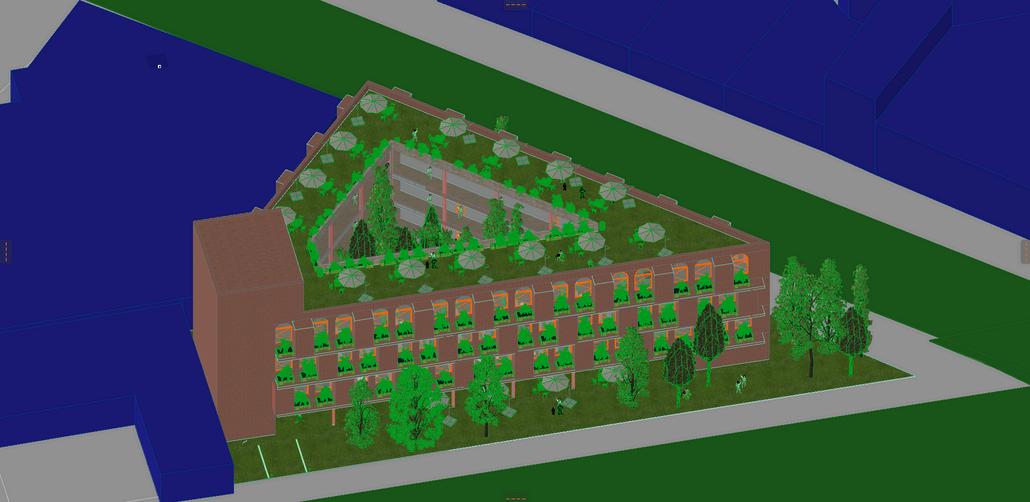
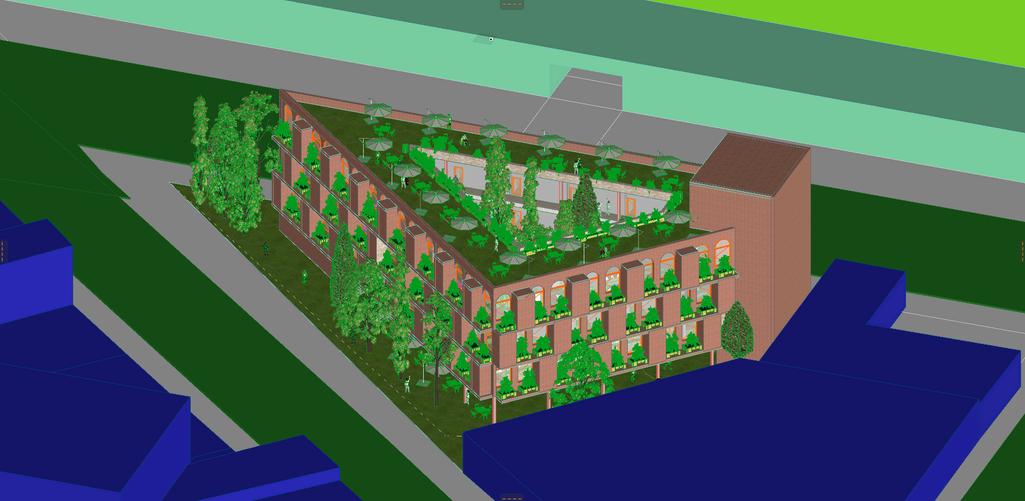
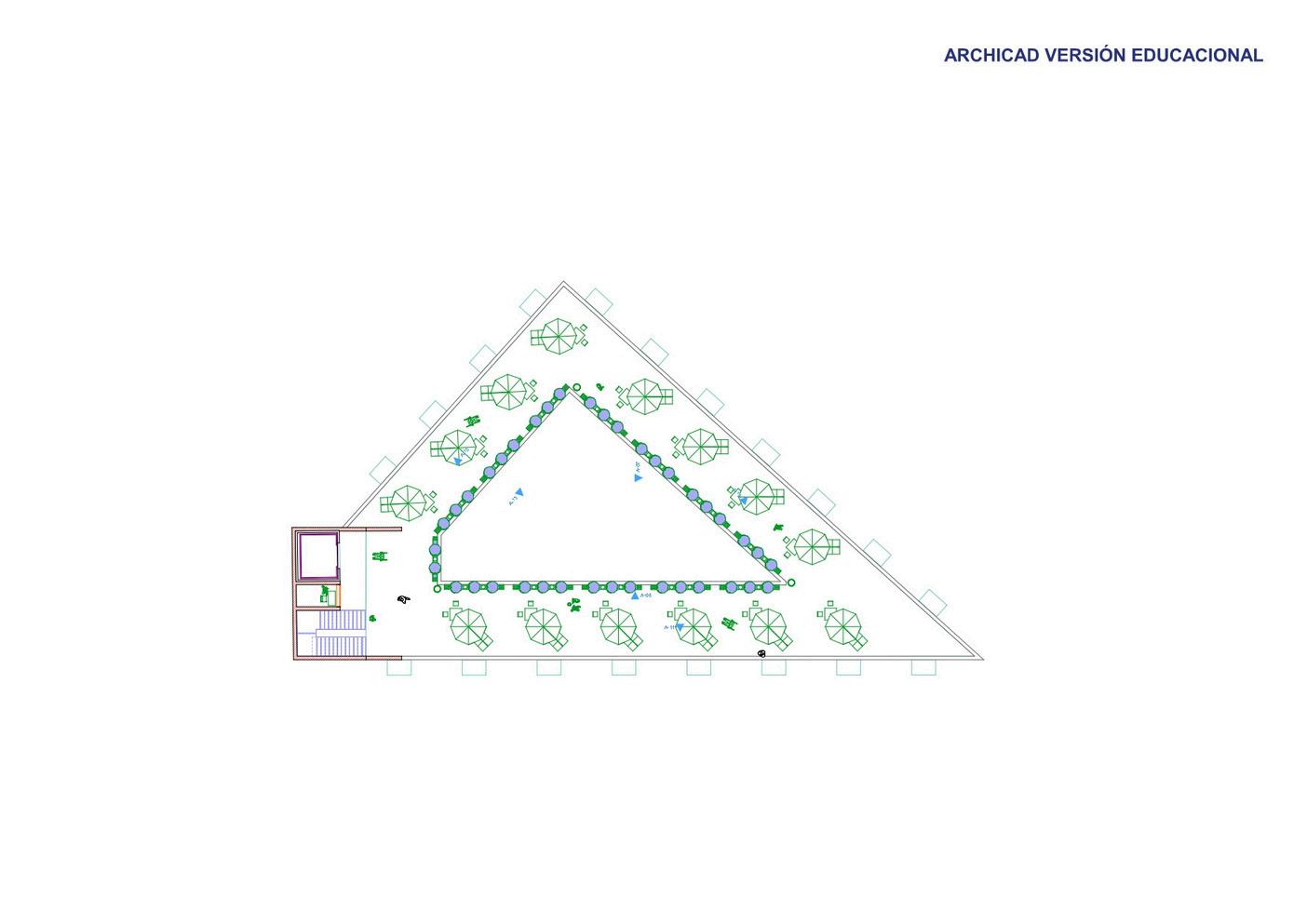
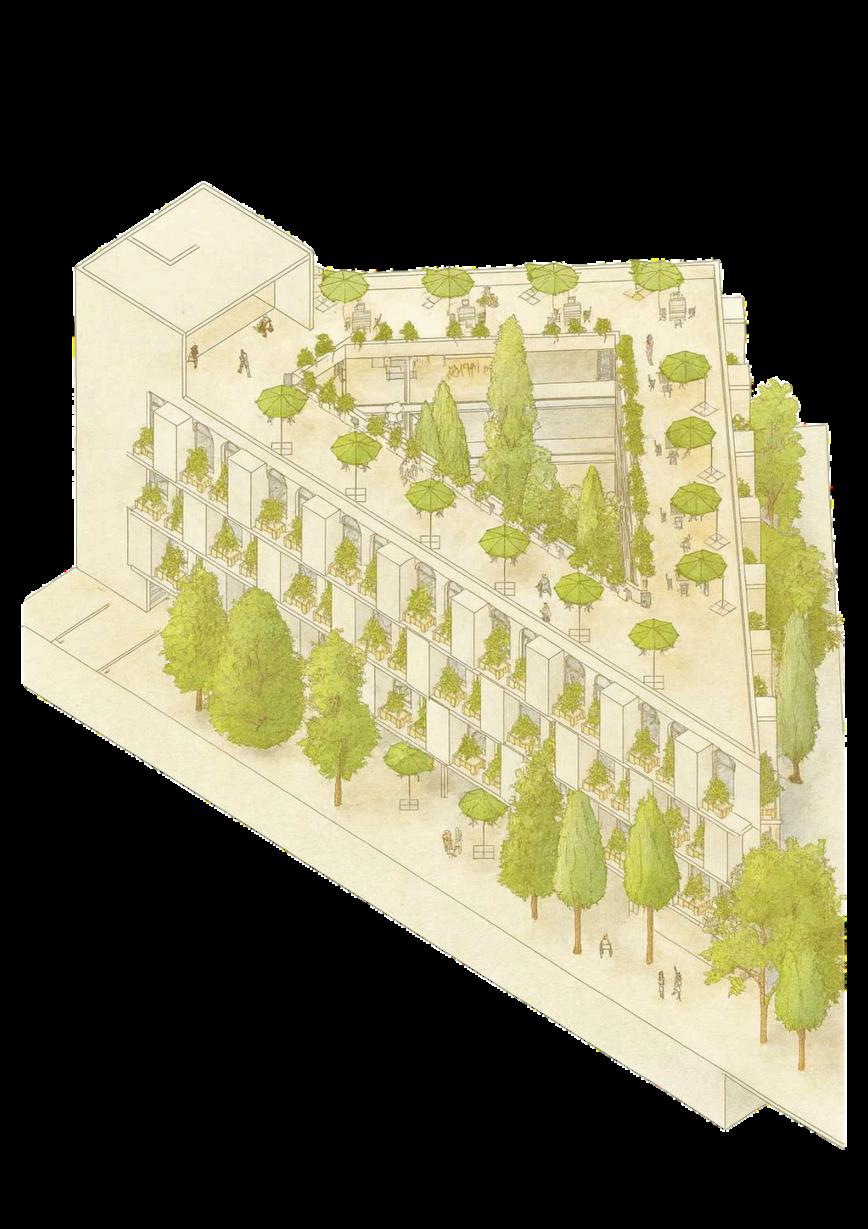
LANDSCAPESTRATEGIES
NATIVE, DROUGHTTOLERANTSPECIES
LOW-MAINTENANCE
PLANTING SUPPORTING LOCALBIODIVERSITY
POLLINATOR-FRIENDLY
VEGETATIONCORRIDORS
SHADED STRUCTURES: GREEN PERGOLAS, TRELLISES, OR VINE SYSTEMS
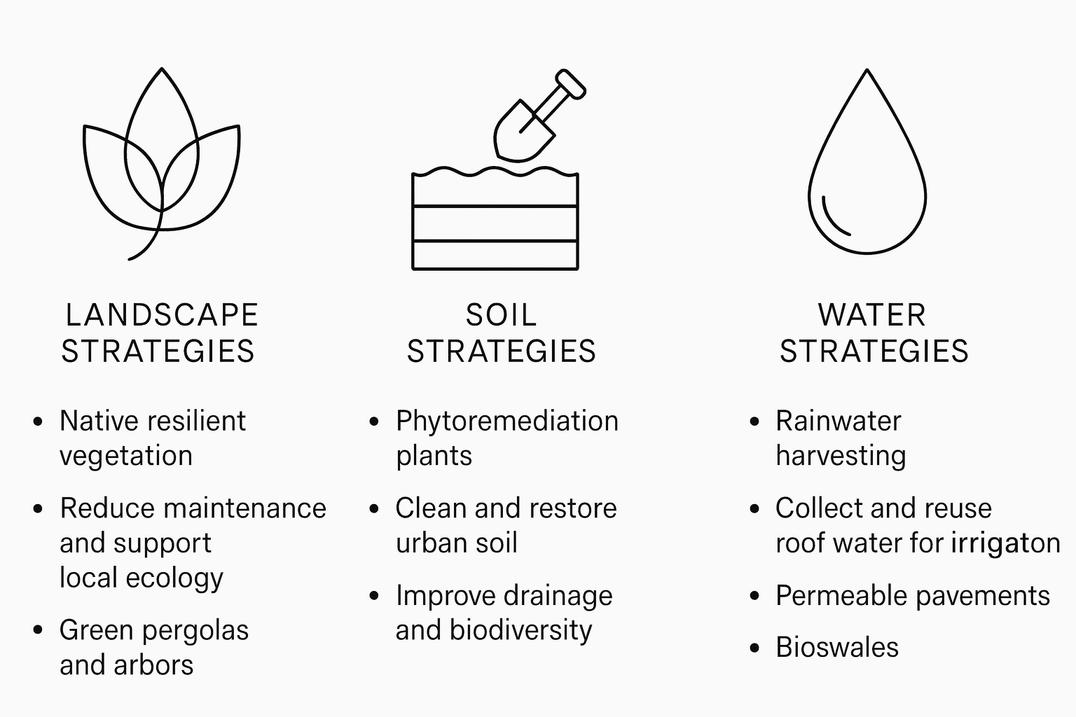
PHYTOREMEDIATION USING
HYPERACCUMULATOR SPECIES
SOIL DETOXIFICATION + ORGANIC MATTER
RESTORATION
MICRO-TOPOGRAPHYAND
POROUS SUBSTRATES TO IMPROVEDRAINAGE
ON-SITE COMPOSTING TO STRENGTHEN SOIL HEALTH
RAINWATER HARVESTING INTEGRATED WITH BUILDINGROOFS
ROOF RUN-OFF COLLECTION + GREYWATER REUSE FOR IRRIGATION
PERMEABLE SURFACES (PAVERS, GRAVEL BEDS, POROUSCONCRETE)
BIOSWALES + LINEAR WETLAND STRIPS FOR STORMWATER MANAGEMENT
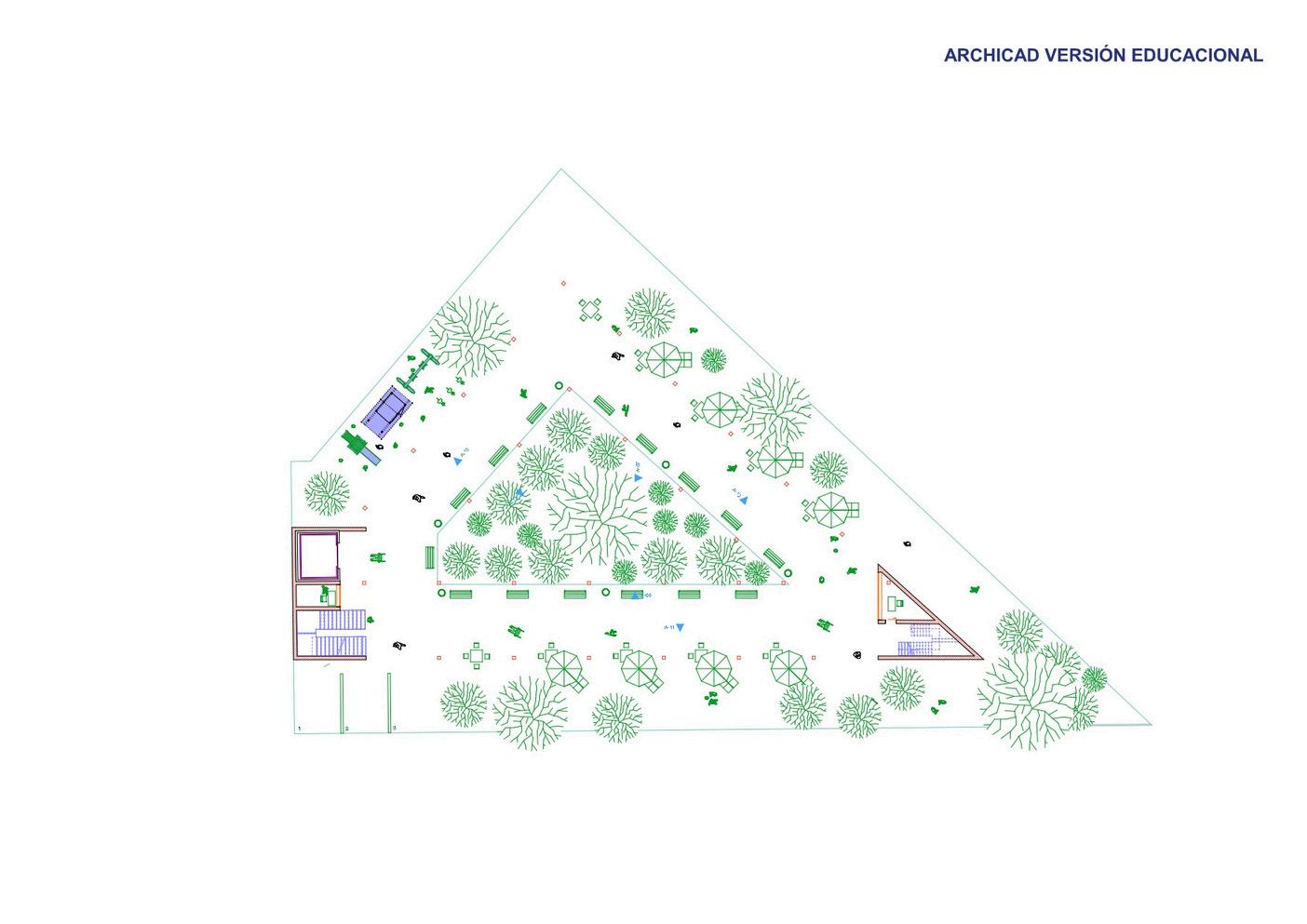
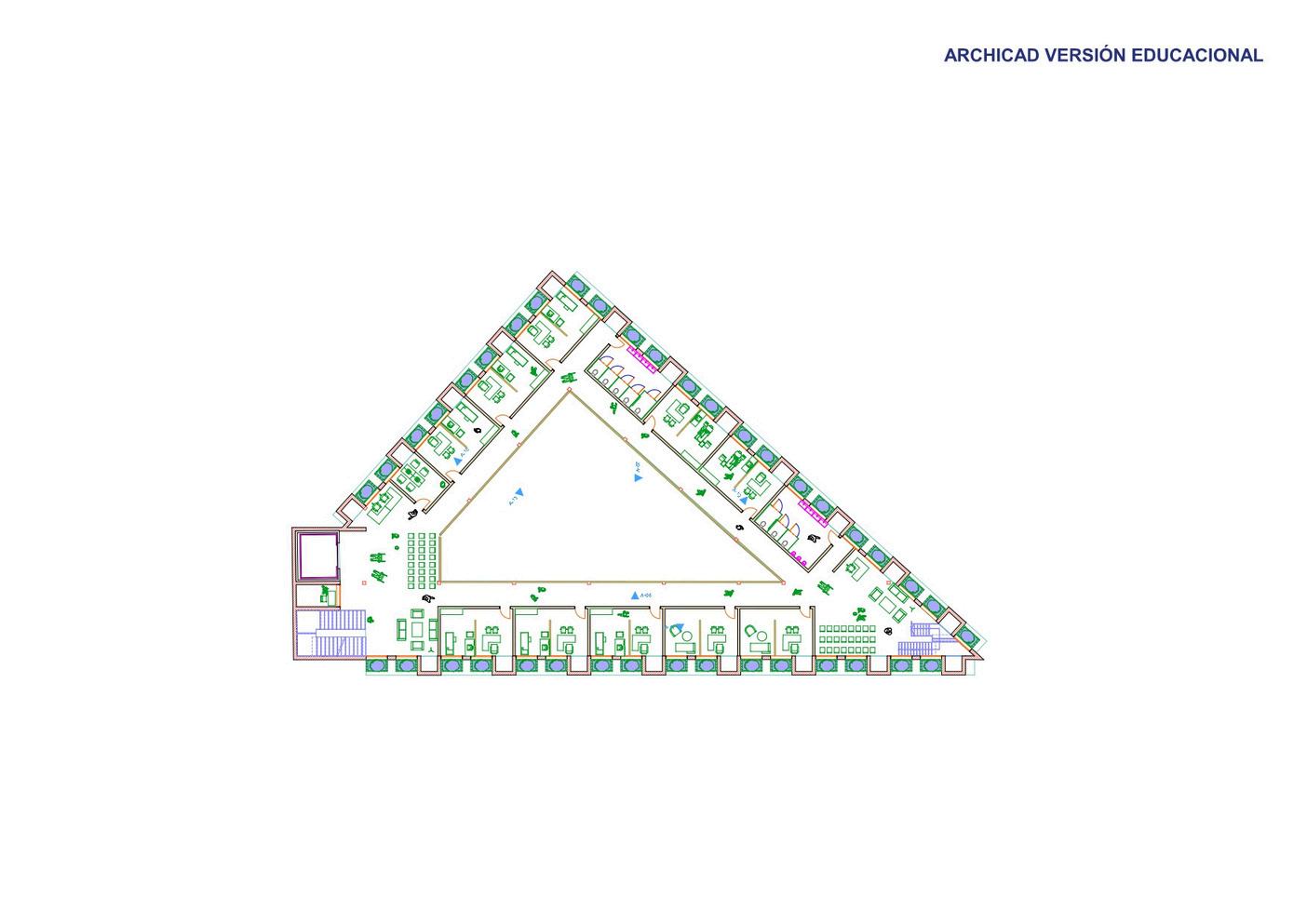
Public

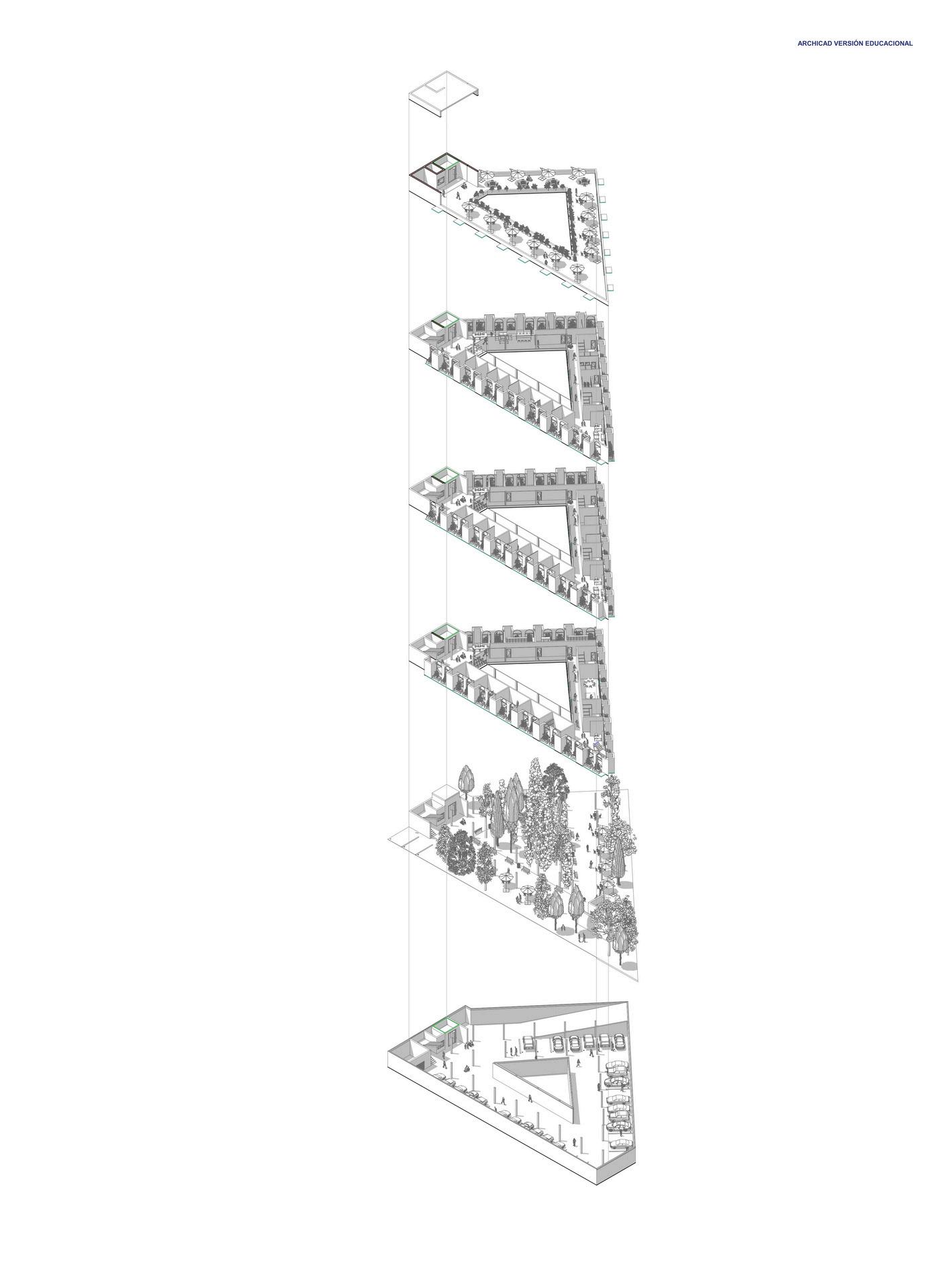
FIRST FLOOR FIRST FLOOR
GARDEN
INFORMATION POINT
WAITING AREA
DRAWING
PAINTING
COMPUTING / COMPUTER ROOM
DANCE ROOM
MULTIPURPOSE ROOM
VISUAL ARTS ROOM
LIBRARY
COMMUNITY KITCHEN
OFFICES
CO-WORKING
WOMEN’S RESTROOMS
MEN’S RESTROOMSSTAIRS
ELEVATOR
ACCESS CONTROL
STAIRS
PARK / JARDEN
PLAYGROUND EQUIPMENT
STAIRS
ELEVATOR
ACCESS CONTROL
EMERGENCY PARKING
RAMP (DOWNWARD ACCESS TO THE PARKING)
UNDERGROUND PARKING AREAS
INDOOR PLANTER
STAIRS
ELEVATOR
ACCESS CONTROL
MECHANICAL ROOM
RAMP (DOWNWARD ACCESS TO THE PARKING)
FIFTH FLOOR FIFTH FLOOR
ROOF
FOURTH FLOOR FOURTH FLOOR
GARDEN ROOFTP GARDEN
ELEVATOR
ACCESS CONTROL STAIRS
GARDEN INFORMATION POINT HOUSING / DWELLING SHOWERS
CHANGING ROOM CO-WORKING
LIVING ROOM
WOMEN’S RESTROOMS MEN’S RESTROOMSSTAIRS
ELEVATOR
ACCESS CONTROL STAIRS
GARDEN
INFORMATION POINT
WAITING AREA
MEDICAL OFFICE
PSYCHOLOGY OFFICE DENTAL OFFICE OFFICES
WOMEN’S RESTROOMS MEN’S RESTROOMSSTAIRS ELEVATOR
ACCESS CONTROL STAIRS










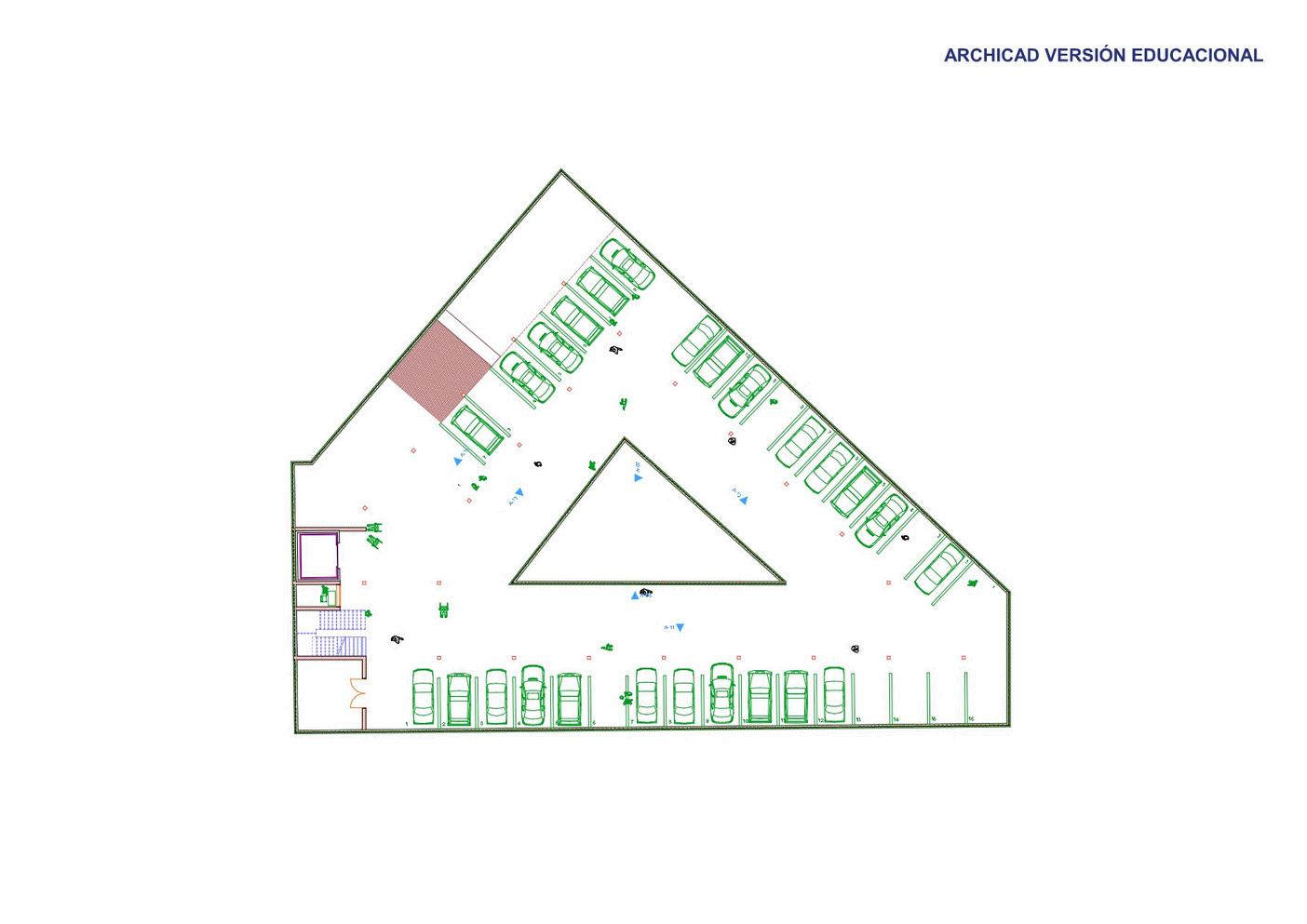
1.UNDERGROUND PARKING AREAS
2.INDOOR PLANTER
3.STAIRS
4.ELEVATOR
5.ACCESS CONTROL
6.MECHANICAL ROOM
7.RAMP (DOWNWARD ACCESS TO THE PARKING)
1.PARK / JARDEN
2.PLAYGROUND EQUIPMENT
3.STAIRS
4.ELEVATOR
5.ACCESS CONTROL
6.EMERGENCY PARKING
7.RAMP (DOWNWARD ACCESS TO THE PARKING)

1.GARDEN
2.INFORMATION POINT
3.WAITING AREA
4.DRAWING
5.PAINTING
6.COMPUTING / COMPUTER ROOM
7.DANCE ROOM
8.MULTIPURPOSE ROOM
9.VISUAL ARTS ROOM
10.LIBRARY
11.COMMUNITY KITCHEN
12.OFFICES
13.CO-WORKING
14.WOMEN’S RESTROOMS
15.MEN’S RESTROOMSSTAIRS
16.ELEVATOR
17.ACCESS CONTROL
18.STAIRS
1.GARDEN
2.INFORMATION POINT
3.WAITING AREA
4.MEDICAL OFFICE
5.PSYCHOLOGY OFFICE
6.DENTAL OFFICE
7.OFFICES
8.WOMEN’S RESTROOMS
9.MEN’S RESTROOMSSTAIRS
10.ELEVATOR
11.ACCESS CONTROL
12.STAIRS

1.GARDEN
2.INFORMATION POINT
3.HOUSING / DWELLING
4.SHOWERS
5.CHANGING ROOM
6.CO-WORKING
7.LIVING ROOM
8.WOMEN’S RESTROOMS
9.MEN’S RESTROOMSSTAIRS
10.ELEVATOR
11.ACCESS CONTROL
12.STAIRS
1.GARDEN
2.ROOFTP GARDEN
3.ELEVATOR
4.ACCESS CONTROL
5.STAIRS






















Brick
Wood
Lattices
Steel
Glass
Home Automation
Formwork + Installations
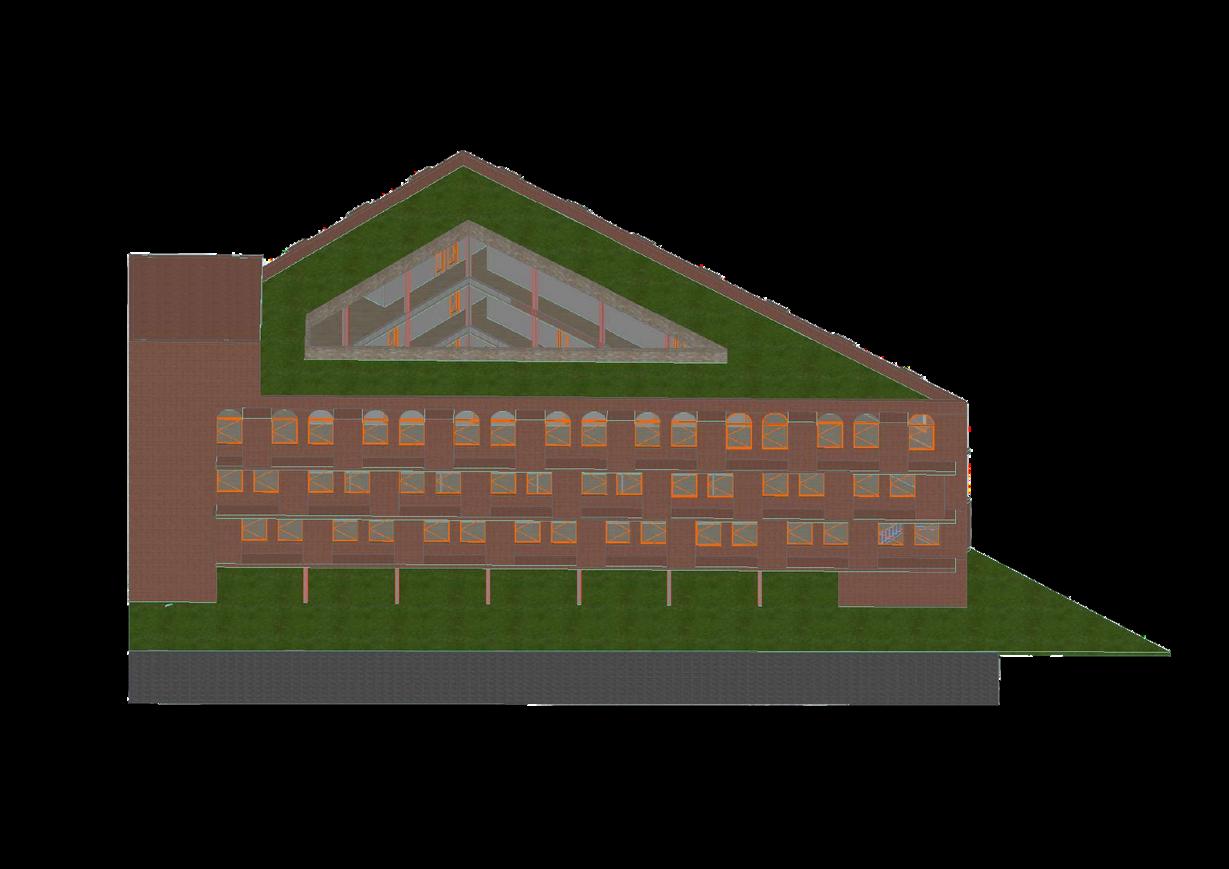
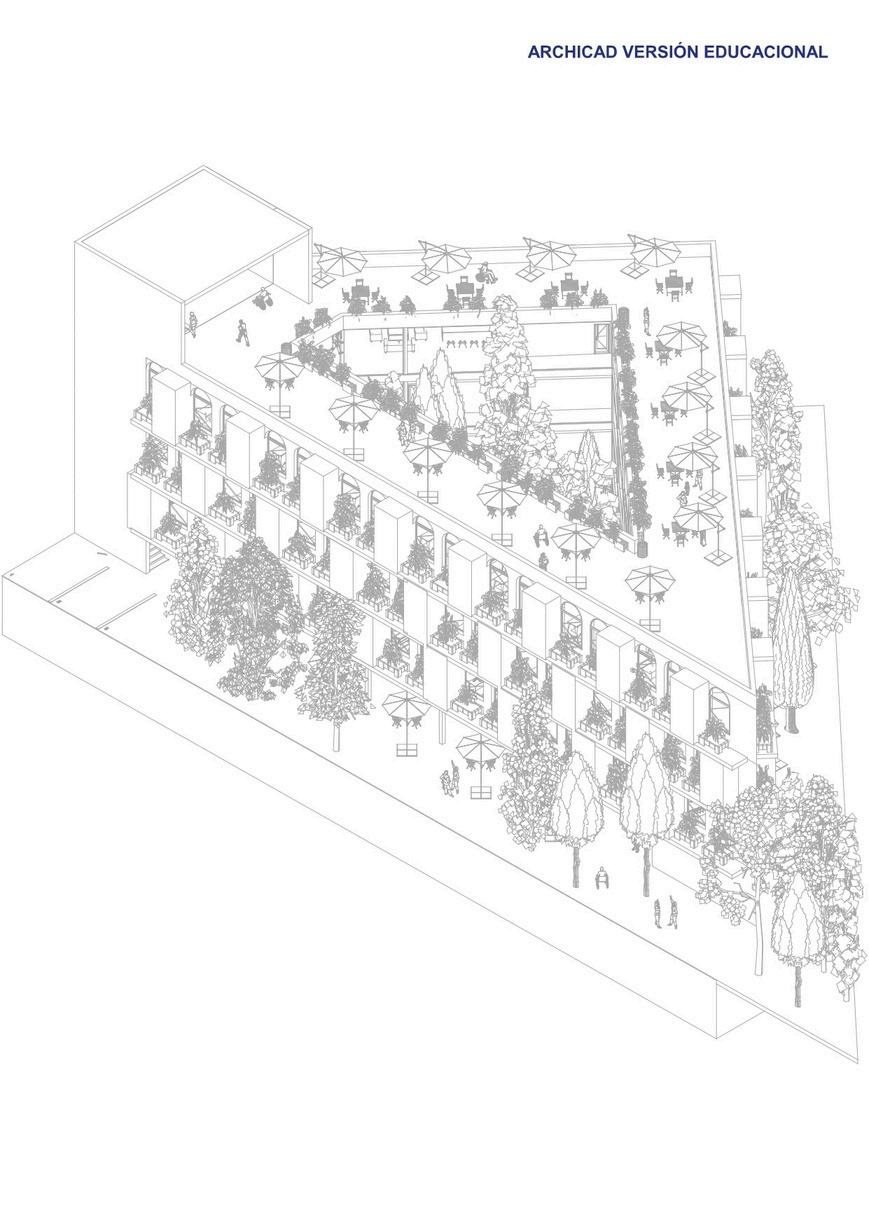
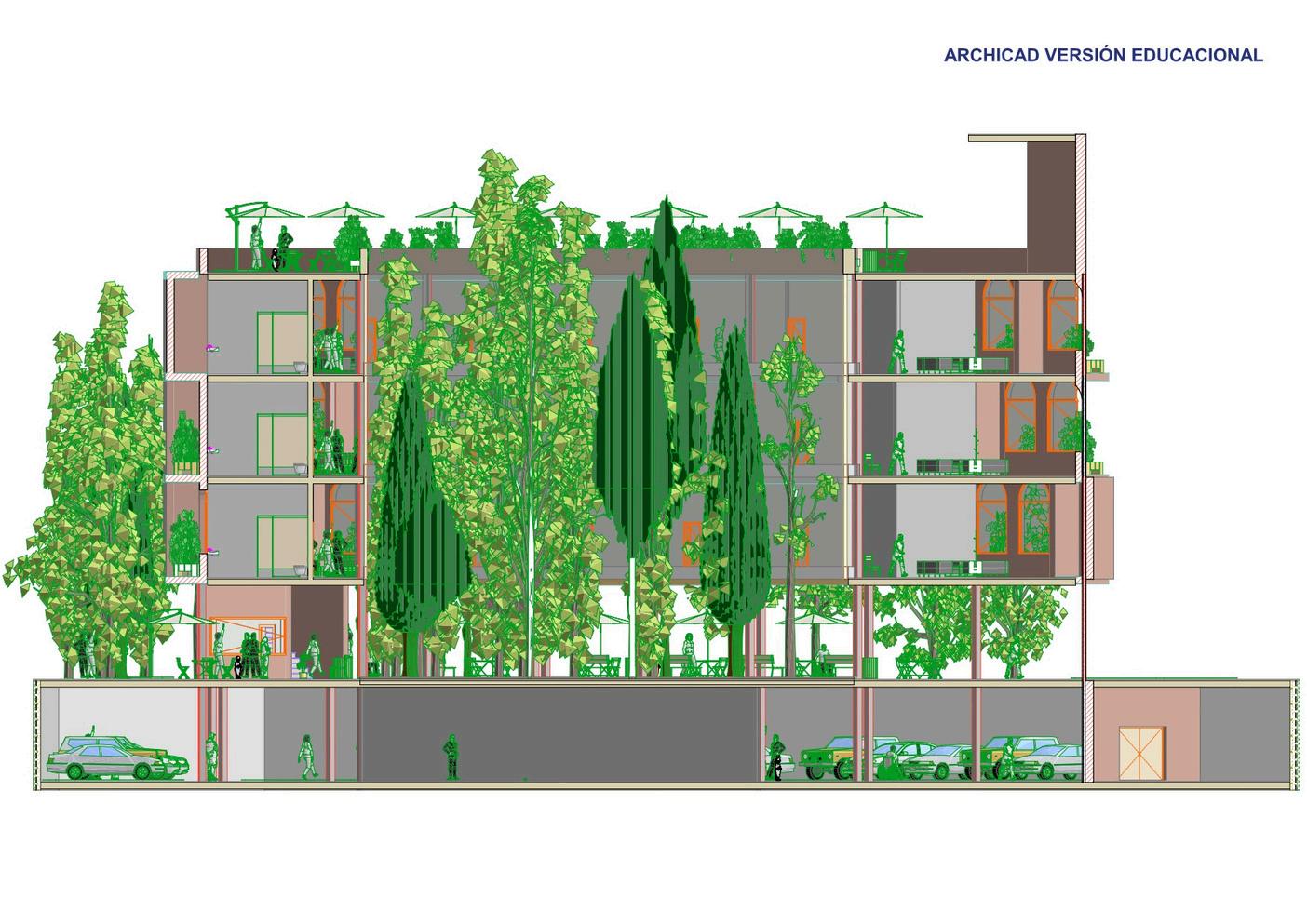
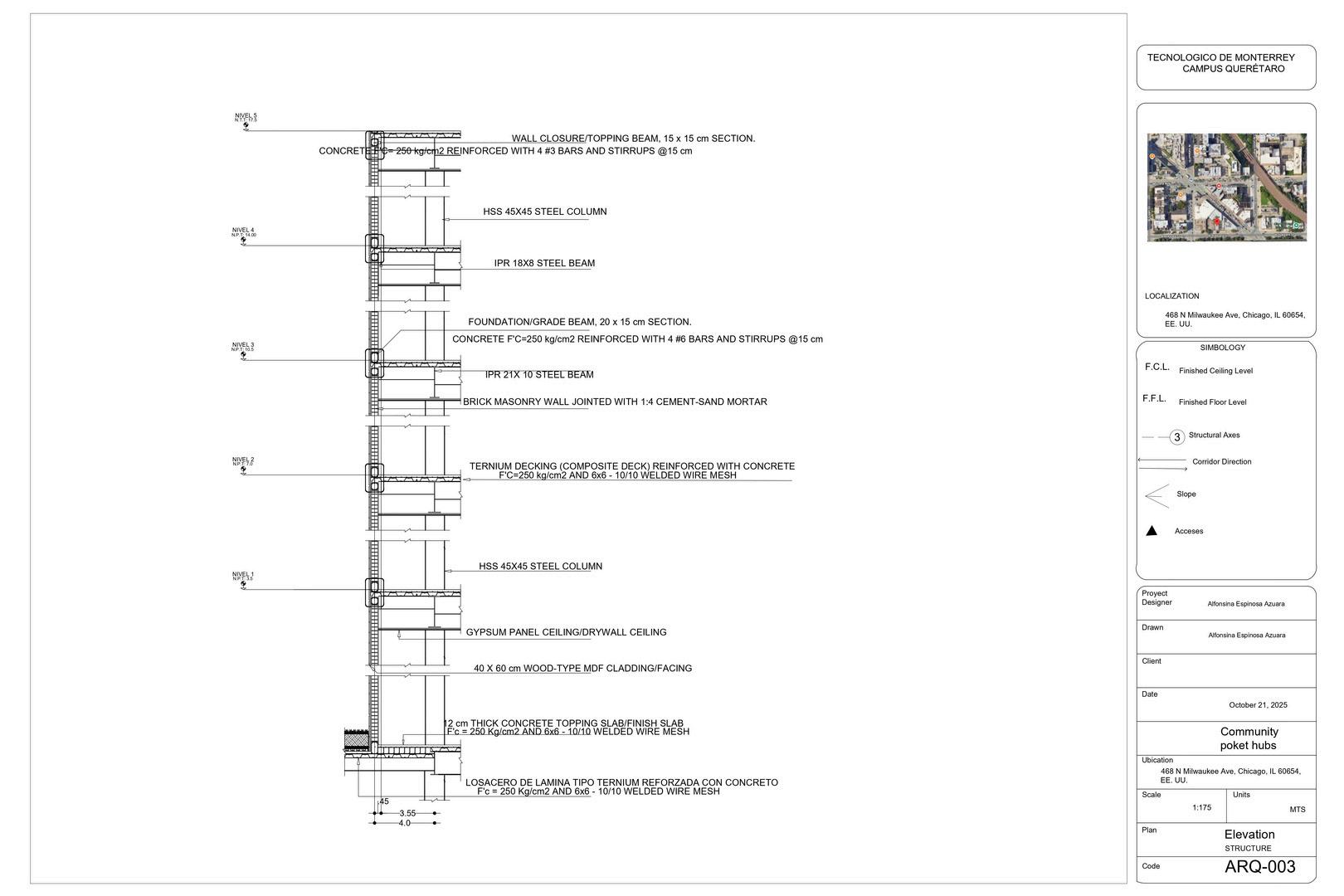
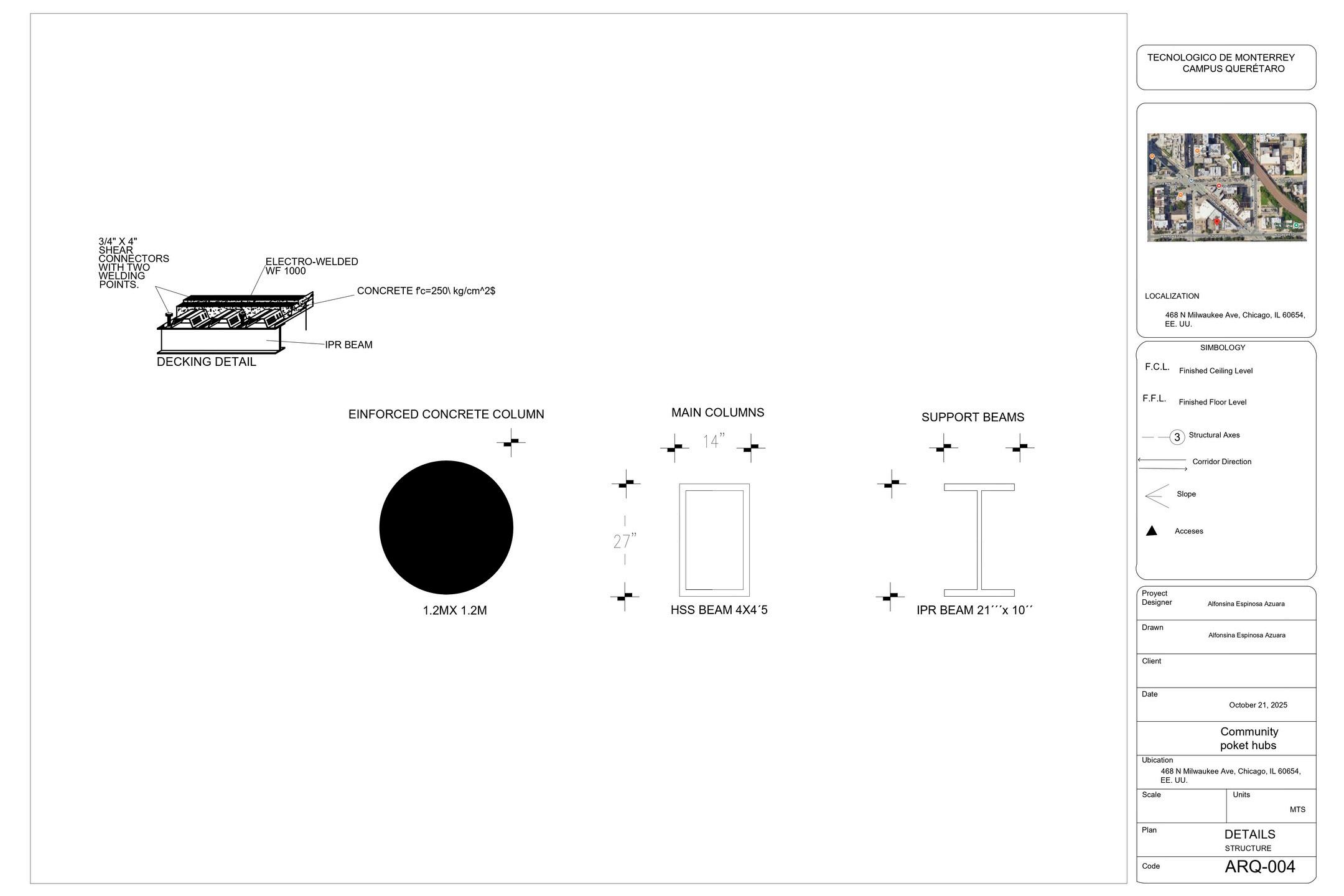
THEBUILDINGEMPLOYSAPRIMARYSTRUCTURALSYSTEMCOMPOSEDOFSTEELCOLUMNSANDANETWORKOF STEELBEAMSTHATEFFICIENTLYDISTRIBUTELOADSTOTHEFOUNDATION.THISSTRUCTURALSTEELSYSTEM ALLOWSFORGREATERSPANS,REDUCESTHEOVERALLWEIGHTOFTHEBUILDING,ANDACCELERATES CONSTRUCTIONPROCESSES.
FURTHERMORE,THEMETALSTRUCTUREENABLESMODULARITY,PREFABRICATION,ANDTHECAPACITYFOR FUTUREEXPANSIONORRECONFIGURATION.ITSRIGIDITY,DUCTILITY,ANDSTRONGPERFORMANCEUNDER DYNAMICLOADSMAKEITANOPTIMALSOLUTIONFORAHIGH-INTENSITYCOMMUNITYBUILDING.

Location: Puebla de la Calzada, Badajoz, Spain
Architect: APT Arquitectos
Year: 2023
Area: 410 m2
The program integrates primary healthcare with spaces dedicated to health promotion and wellbeing. It includes medical and nursing consultations, multipurpose rooms for prevention activities, and support areas. Its key feature is a Community Focus, designed as a social meeting and activation point to encourage healthy habits and community cohesion. Spaces are flexible to adapt to different uses.





The material selection emphasizes sustainability and contextual integration. Ceramic Brick is used on the façades, providing a warm, traditional texture related to vernacular architecture. Exposed Concrete offers structural solidity. The design prioritizes systems that maximize natural light and cross-ventilation, reducing the need for artificial climate control.
The structure is simple and modular to allow for programmatic flexibility. It uses a Portico Structure (columns and beams) that frees the internal walls, making future modifications easier. The construction is optimized for sustainability and reduced environmental impact.
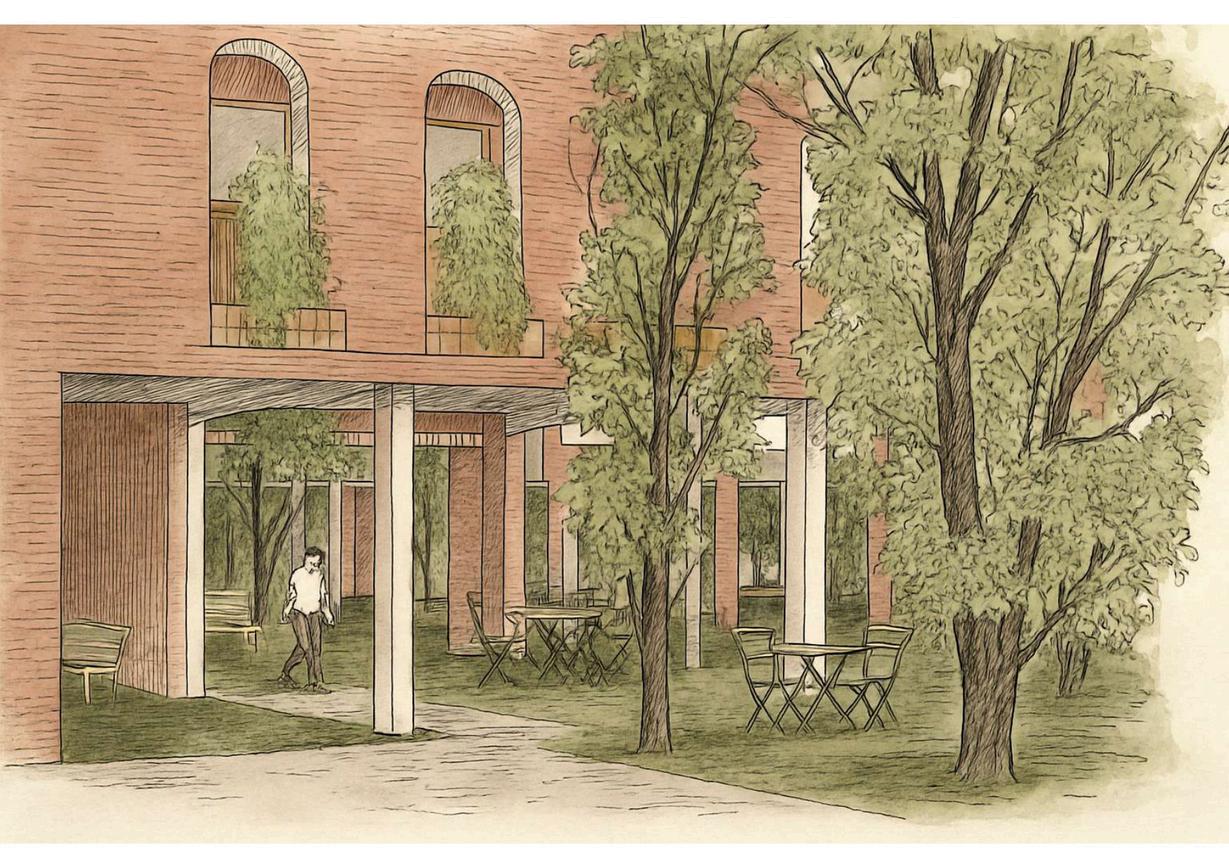
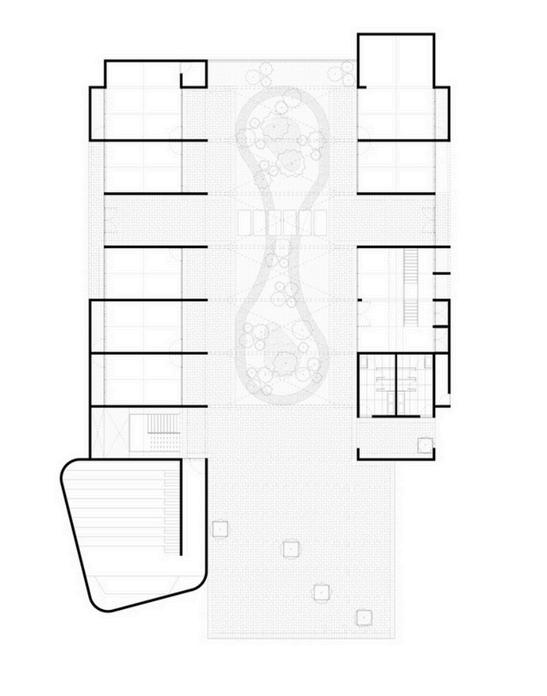
The design is based on the duality of privacy and openness. The building is organized around interior courtyards (patios), which function as "lungs" for light and ventilation, and as transitional spaces. Circulation is clear, and the Indoor-Outdoor Connection is achieved through courtyards and large windows, creating an welcoming and therapeutic environment (Biophilic Architecture).
The project responds to the social and urban needs of its location. It seeks Urban Insertion with a respectful scale, avoiding a cold institutional image. By creating an attractive public space, it contributes to the social and physical betterment of the site, acting as a driver for comprehensive community development.
Location: Jalpa de Méndez, Tabasco, México
Architect: CCA
Focus Community Mental Health and Inclusion
Year: 2022 (not finished)
Area: 1240 m2
The CDC focuses on cultural and educational development to foster social integration and inclusive development, forming part of a larger public space revitalization project (El Campestre Recreational Park).
Core Focus: Cultural and educational development as a driver for social wellbeing.
Key Spaces: Multifunctional classrooms, workshops, meeting areas, and an outdoor auditorium.
Social Wellbeing: It promotes wellbeing by offering training opportunities and a safe space for community life, strengthening the social fabric and local economy.


The material selection emphasizes sustainability and contextual integration. Ceramic Brick is used on the façades, providing a warm, traditional texture related to vernacular architecture. Exposed Concrete offers structural solidity. The design prioritizes systems that maximize natural light and cross-ventilation, reducing the need for artificial climate control.
The structure is simple and modular to allow for programmatic flexibility. It uses a Portico Structure (columns and beams) that frees the internal walls, making future modifications easier. The construction is optimized for sustainability and reduced environmental impact.
The design is based on the duality of privacy and openness. The building is organized around interior courtyards (patios), which function as "lungs" for light and ventilation, and as transitional spaces. Circulation is clear, and the Indoor-Outdoor Connection is achieved through courtyards and large windows, creating an welcoming and therapeutic environment (Biophilic Architecture).
The project responds to the social and urban needs of its location. It seeks Urban Insertion with a respectful scale, avoiding a cold institutional image. By creating an attractive public space, it contributes to the social and physical betterment of the site, acting as a driver for comprehensive community development.
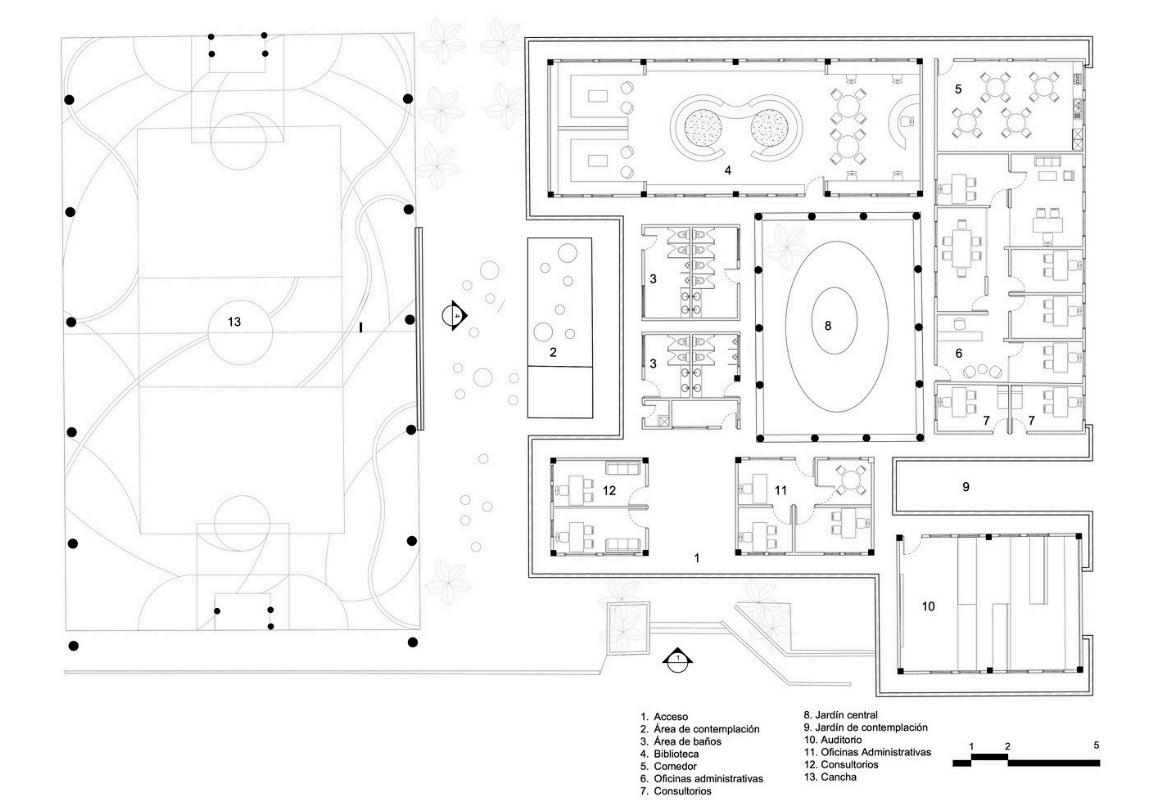
Location: Monterrey, Nuevo León, Mexico
Architect: Proyecto Reacciona
Year: 2022
Area: 840 m2
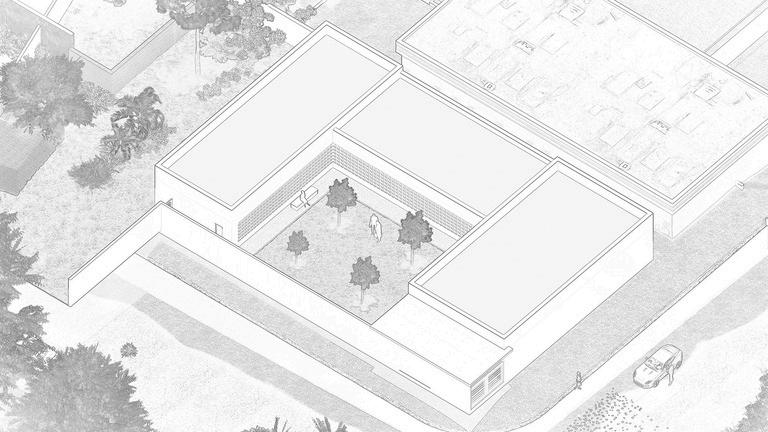
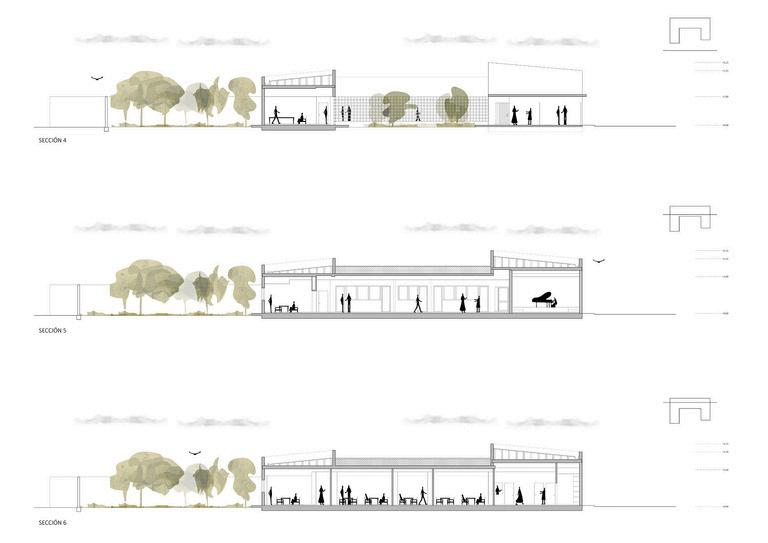
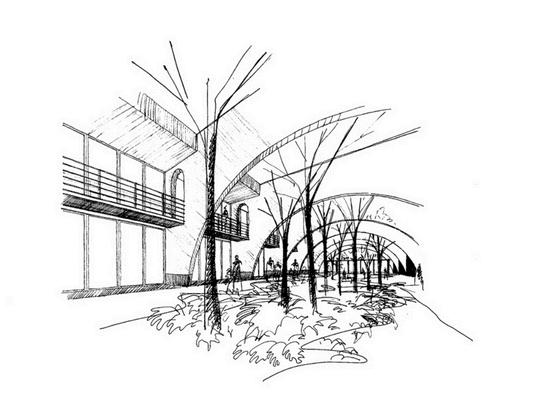
The center was rehabilitated from an old school to serve as a comprehensive community center focused on safety, mental health, and social development. The Secretary of Crime Prevention requested administrative areas, consultation rooms for psychological counseling, and a film/documentary viewing space. The design sought to create dynamic, multifaceted spaces that incentivize the development of multiple activities according to the community's needs.






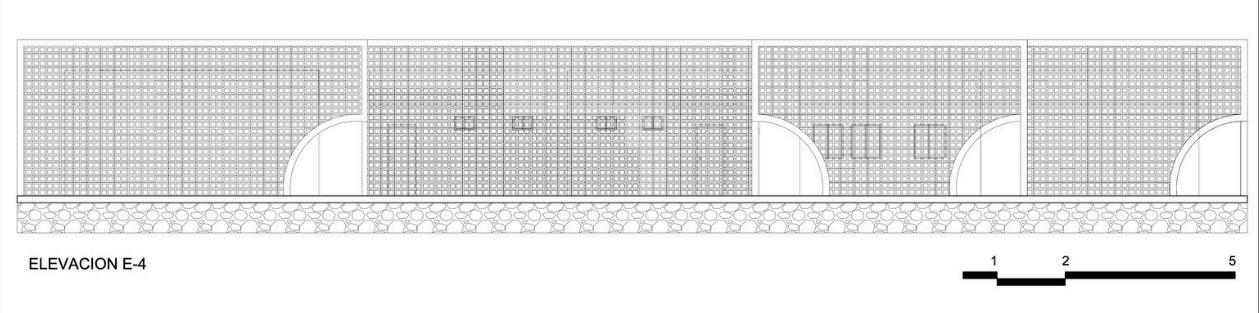
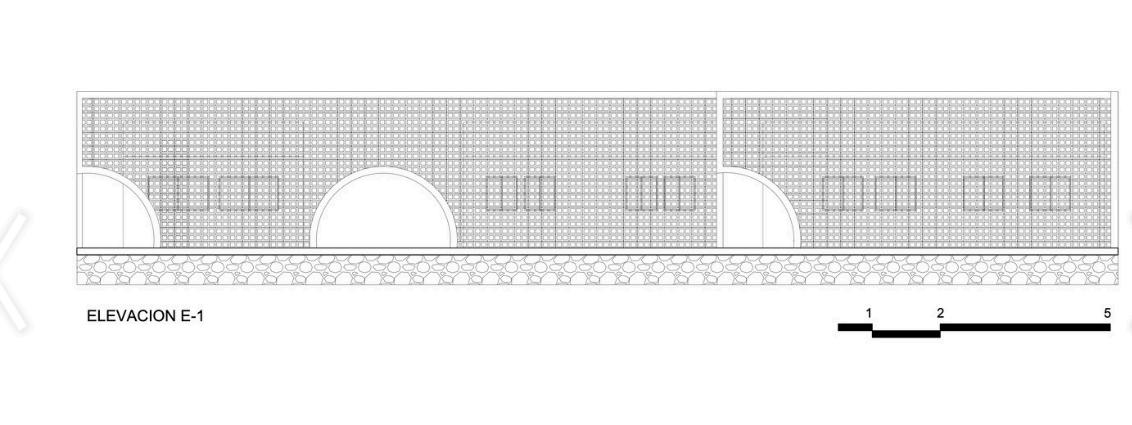
The materiality strategy focused on unifying the old structure with the new intervention using color and a key architectural element: the latticework. The existing building was painted a solid yellow tone, which is visible through the perforations of the new ceramic latticework applied to the façade. The latticework functions as a dynamic veil that protects the interior from the intense sun of Monterrey and offers a sense of privacy while maintaining visual connection with the outside. The use of different forms and colors was key to generating dynamic and stimulating spaces.
The structural intervention involved reusing and adapting the existing masonry structure of the school. The main structural addition is the use of a large lattice wall that acts as a second skin, giving the building a new identity without modifying the original volumes excessively. This strategic use of the structural envelope maximizes natural light while protecting from solar heat gain.
The spatial logic revolves around creating a connection between the exterior and the interior to facilitate contemplation and community gathering. The vastness of the perimeter wall is interrupted by strategic extractions, creating openings that connect the inside and outside. A central landscaped area was created in the center of the project, allowing users to have a relaxation space at the door of each interior area. The entire perimeter features cylindrical benches designed to create spaces for contemplation and gathering.
The project is located in a highly dense urban area of Monterrey and is a direct response to the need for safe spaces and access to mental health services and community integration programs. The center is a resource for the local community, promoting a safer environment and offering psychological support and film/documentary viewing areas to foster social cohesion. The renovation sought to generate a differentiated and attractive image to stimulate attendance and community ownership.

APT ARQUITECTOS (2024, 18 DE JULIO) PROYECTO | CENTRO DE LA SALUD Y EL BIENESTAR, PUEBLA DE LA CALZADA, BADAJOZ PROARQUITECTURA
HTTPS://WWW WASHINGTONPOST COM/ES/POST-OPINION/
CCA | BERNARDO QUINZAÑOS. (2023, 22 DE NOVIEMBRE). CENTRO DE DESARROLLO COMUNITARIO / CCA | BERNARDO QUINZAÑOS. ARCHDAILY MÉXICO.
HTTPS://WWW ARCHDAILY MX/MX/1010044/CENTRO-DE-DESARROLLO-COMUNITARIO-CCA-CENTRO-DE-COLABORACION-ARQUITECTONICA
PROYECTO REACCIONA (2022, 31 DE OCTUBRE) CENTRO COMUNITARIO CASA NUEVA ESPERANZA / PROYECTO REACCIONA ARCHDAILY MÉXICO
HTTPS://WWW ARCHDAILY MX/MX/991354/CENTRO-COMUNITARIO-CASA-NUEVA-ESPERANZA-PROYECTO-REACCIONA
SERVICIO DE SALUD METROPOLITANO SUR ORIENTE (SSMSO) (S F ) MODELO DE SALUD MENTAL Y PSIQUIATRÍA COMUNITARIA COSAM LA PLATINA [DOCUMENTO DE PLANIFICACIÓN INSTITUCIONAL O REPOSITORIO ACADÉMICO].
WILLIAMS, D R , & COLLINS, C (2001) RACIAL RESIDENTIAL SEGREGATION: A FUNDAMENTAL CAUSE OF RACIAL DISPARITIES IN HEALTH PUBLIC HEALTH REPORTS, 116(5), 404–416
BETANCUR, J J (2011) GENTRIFICATION AND SOCIAL INJUSTICE IN YOUTH-ORIENTED AREAS: THE CASE OF PILSEN, CHICAGO URBAN STUDIES, 48(4), 785–802
KELLERT, S R , HEERWAGEN, J , & MADOR, M (EDS ) (2008) BIOPHILIC DESIGN: THE THEORY, SCIENCE AND PRACTICE OF BRINGING LIFE TO BUILDING SPACE JOHN WILEY & SONS.
MINDELL, J S (2020) HEALTH, WELL-BEING AND THE BUILT ENVIRONMENT SPRINGER
CHICAGO METROPOLITAN AGENCY FOR PLANNING (CMAP) (2024) COMMUNITY DATA SNAPSHOT: LOGAN SQUARE (O EL INFORME ESPECÍFICO DE LA COMUNIDAD QUE ELIJAS).
RHODES, K. V., SANTIN, O., BREYER, M., & VARELA, M. V. (2020). UNINSURED IMMIGRANTS IN CHICAGO: CHARACTERISTICS AND HEALTH CARE ACCESS. ILLINOIS COALITION FOR IMMIGRANT AND REFUGEE RIGHTS (ICIRR)
COMMUNITYHEALTH (N D ) OUR IMPACT AND MISSION (O LA MISIÓN/PUBLICACIONES DE UNA ORGANIZACIÓN SIMILAR EN EL ÁREA)