
A case of oral spindle sarcoma with intracytoplasmic inclusion bodies in a dog



N.M. Meertens1, T. Veenendaal2, K. van Dam3 1Royal GD, Deventer, The Netherlands, 2Center for Molecular Medicine, University Medical Center Utrecht, The Netherlands, 3Evidensia Dierenziekenhuis Arnhem, Arnhem, The Netherlands
Background
Oral spindle cell sarcomas are relatively common in dogs, including low-grade sarcomas which can be a challenge for diagnosis and successful treatment. This case report describes a novel type of low-grade soft tissue sarcoma with intracytoplasmic inclusion bodies in the gingiva of a 9-year old dog, further investigated by immunohistochemistry and transmission electron microscopy. The histopathology and immunohistochemical findings are similar to (subsets of) human cases of inclusion body fibromatosis (Reye’s tumor) in children and myofibroblastic sarcoma with intracytoplasmic inclusion bodies in adults. In this case myofibroblastic differentiation could not be shown by electron microscopy.
Materials and Methods
A 9-year old female sterilized labradoodle dog was presented with an oral gingival mass on the lingual surface of tooth elements 408 and 409 (Figure 1). On CT scan, the lesion showed strong homogenous contrast enhancement and measured 14 mm long and 6.5 mm in height; no evidence of bone involvement. The mass was removed by partial mandibulectomy. Histopathology, immunohistochemistry for vimentin, desmin, smooth muscle actin, and muscle-specific actin were performed, as well as transmission electron microscopy.
Results and Discussion
On histopathology the well-circumscribed mass consisted of spindle-shaped cells in loose to moderately cellular bundles and rarely storiform patterns. In-between the cells whispy delicate fibers and abundant extracellular pale material was present. The cells had an oval to wavy, sometimes tapered or cigar-shaped nucleus with finely stippled chromatin and a small nucleolus (Figure 2). The cells had poorly circumscribed cell borders, pale cytoplasm with often a single round hyaline eosinophilic inclusion body measuring 2-5 µm, sometimes adjacent to the nucleus (Figure 3). The cells showed mild anisocytosis and anisokaryosis, 2 mitotic figures in 10 HPF (corresponding to 2,37 mm²). At the periphery of the mass, mild perivascular lymphoplasmacellular inflammation was present. The mass was completely excised, the dog uneventfully recovered and is doing well 1 year after surgery.
The neoplastic cells stained strongly positive for vimentin (Figure 4) and alpha-smooth muscle actin (SMA) (Figure 5). Most cells were negative for muscle-specific actin (MSA), except in the center of the mass, in which some cells were positive (Figure 6). The cells were mostly negative for desmin, with only rare perivascular tumour cells staining weakly (not shown). The inclusion bodies did not react to any of the antibodies used.
Transmission electron microscopy showed abundant rough endoplasmatic reticulum, thin filaments, and micropinocytotic vesicles within the neoplastic cells. The inclusion bodies consisted of large cytoplasmic globular non-membrane bound clusters of thin filaments (Figure 7 and 8). No focal electron-dense patches and subplasmalemmal plaques were present, which should be present in the case of myofibroblastic differentiation.
Conclusion
This case report is to our knowledge the first case of a spindle cell sarcoma with intracytoplasmic inclusion bodies described in a dog. The histopathological findings and immunohistochemical findings are similar to (subsets of) inclusion body fibromatosis (Reye’s tumor) in children and low-grade human myofibroblastic sarcomas with intracytoplasmic hyaline (fibroma-like) inclusion bodies in adults. Myofibroblastic differentiation could not be shown by electron microscopy in this case, more consistent with fibroblastic differentiation.
The report highlights the importance of diagnostics of oral masses and the role of histopathology. As the mass was unusually well-circumscribed for a sarcoma, the clinical behaviour of this new entity might be different from other low-grade oral sarcomas like the histopathologically benign, biologically malignant fibrosarcoma (“high-low fibrosarcoma”) which is usually very aggressive and shows infiltrative and destructive growth, with rapid progression. However further research and more cases are necessary before conclusions can be drawn.
Acknowledgements
The authors thank the laboratory technicians of Royal GD and the Pathology department of the Veterinary faculty of the University of Utrecht for performing the immunohistochemical stains.
Literature
1. Oral and maxillofacial pathology, 3rd ed., ed. by Neville/Damm/Allen/Boucquot, Saunders, 2009. Myofibroma/myofibromatosis, Chapter 12, Soft tissue tumors, pp. 515-516.
2. Shenjere, P. et al., Ultrastructurally confirmed myofibrosarcoma: a series of 10 new cases, with a discussion on diagnostic criteria, Intern. Journal of Surgical Pathology, Vol. 21, Issue 1, 2013.
3. Mentzel, T. et al., Low-grade myofibroblastic sarcoma; an analysis of 18 cases in the spectrum of myofibroblastic tumors, Am J Surg Pathol. 1998; 22:1228-1238.
4. Godse R. et al., Infantile digital fibromatosis/inclusion body fibromatosis: a comprehensive literature review, Skin Appendage Disord 2023; 9:1-7.

Presenting author: N.M. Meertens n.meertens@gdanimalhealth.com www.gdanimalhealth.com

1 Oral gingival mass on the lingual surface of
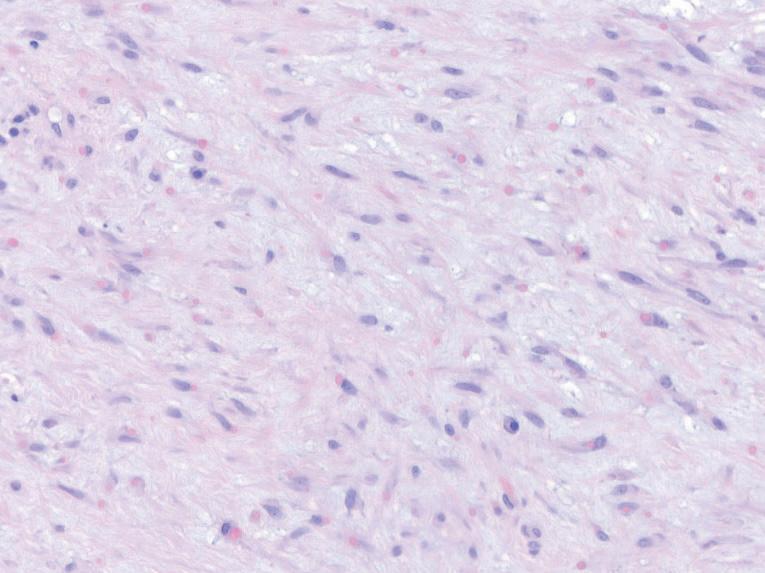
Fig. 3 HE, 400x. The cells have an oval to wavy, sometimes tapered or cigar-shaped nucleus with finely stippled chromatin and a small nucleolus. Frequently a single round hyaline eosinophilic inclusion body sometimes adjacent to the nucleus.
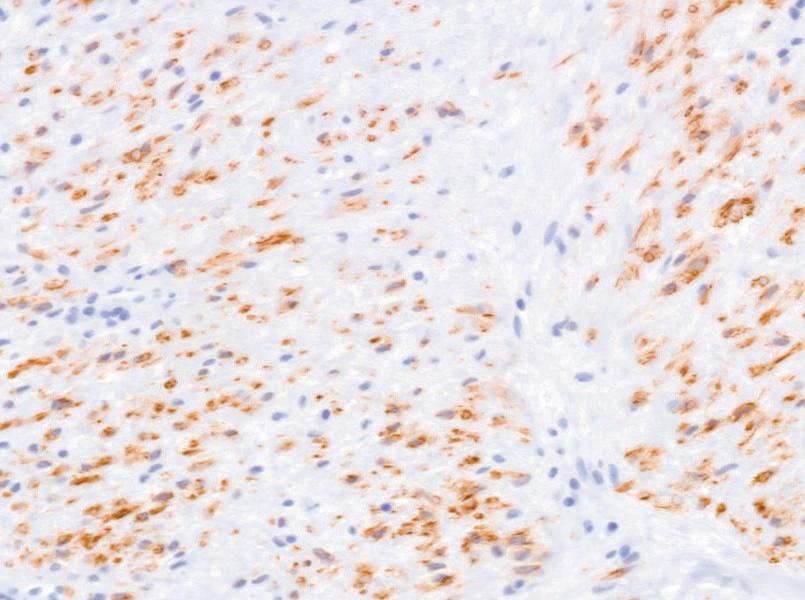
Fig. 5 Alpha-smooth muscle actin (SMA) IHC, 400x. The cells are strongly positive.
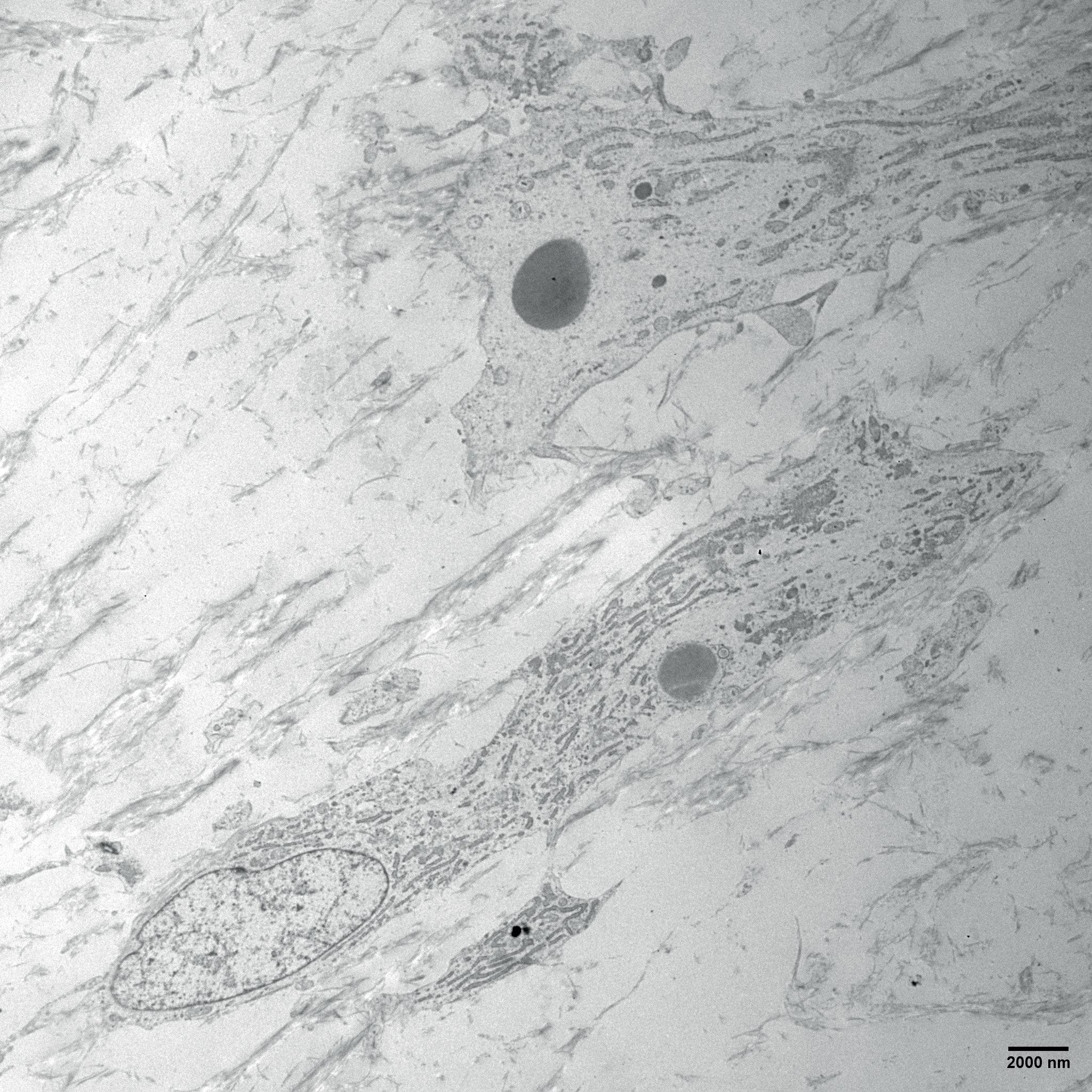
Fig. 7 Transmission electron microscopy. Two neoplastic cells with intracytoplasmic inclusion body and abundant rough endoplasmatic reticulum, an oval nucleus.
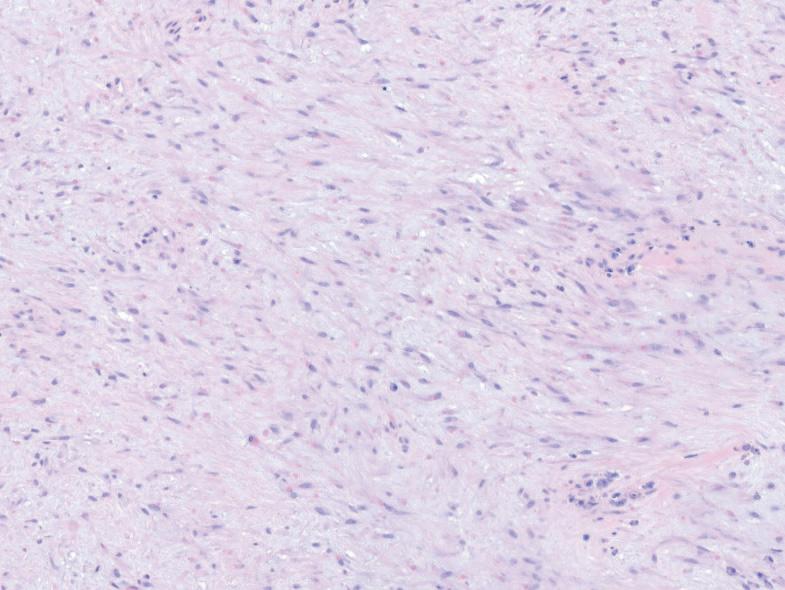
Fig. 2 HE, 200x. Spindle-shaped cells neoplastic cells in loose to moderately cellular bundles and less storiform patterns.
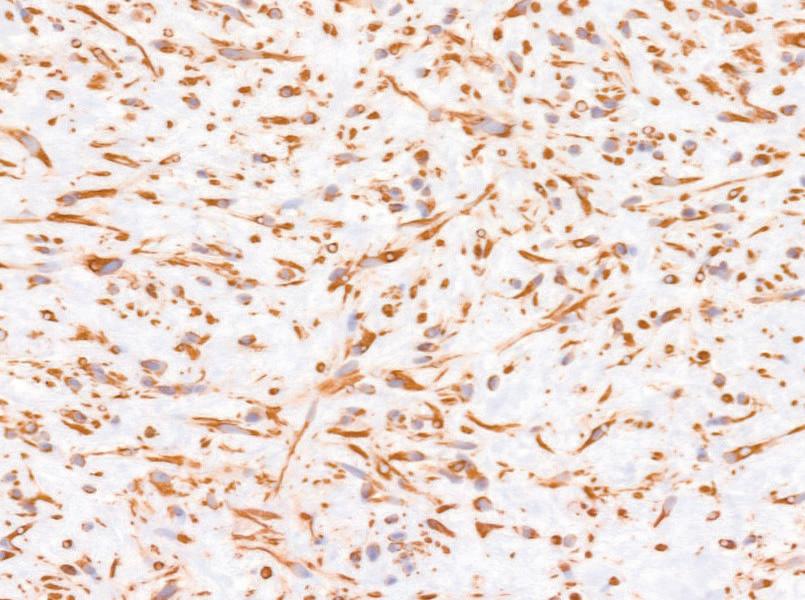
Fig. 4 Vimentin IHC, 400x. The cells are strongly positive.
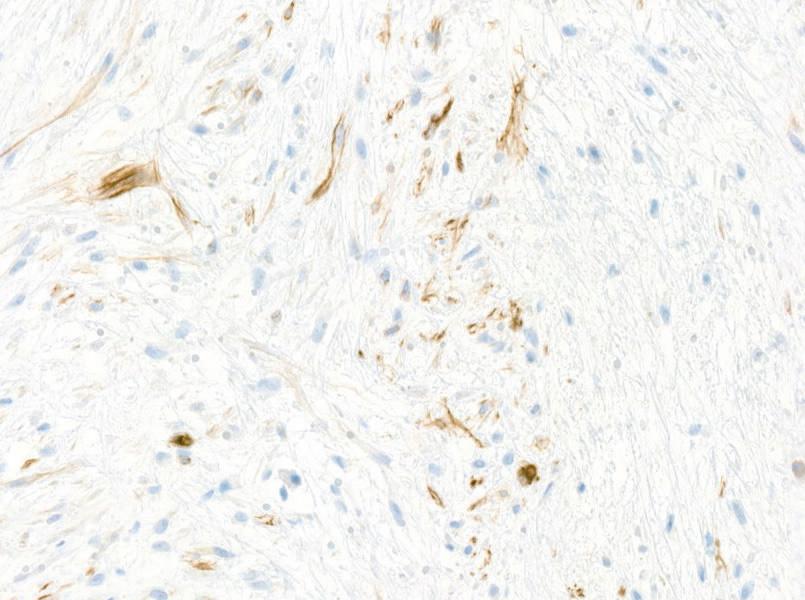
Fig. 6 Muscle-specific actin (MSA) IHC, 400x. Locally cells are positive in the center of the lesion.
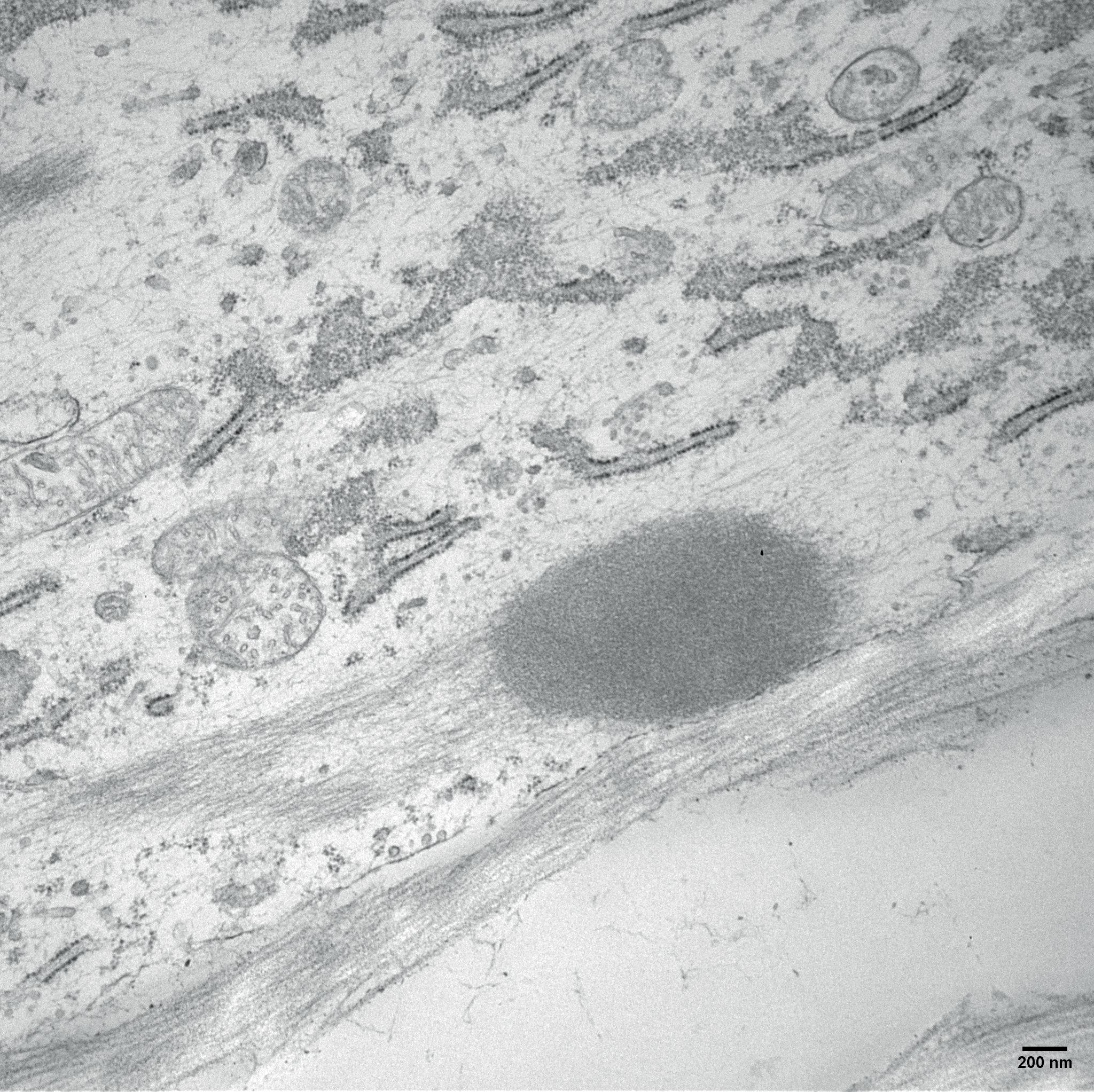
Fig. 8 Transmission electron microscopy. The inclusion bodies consist of large cytoplasmic globular non-membrane bound clusters of thin filaments.