No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
ISBN: 978-0-323-89839-3
For Information on all Elsevier publications visit our website at https://www.elsevier.com/books-and-journals
Publisher: Andre Gerhard Wolff
Acquisitions Editor: Michelle Fisher
Editorial Project Manager: Susan E. Ikeda
Production Project Manager: Omer Mukthar
Cover Designer: Miles Hitchen
Typeset by Aptara, New Delhi, India
2. Phototherapy for skin diseases
1. Phototherapy: A critical review
Nilesh Rarokar, Shailendra Gurav, Dadasaheb M. Kokare, Vijay Kale, Nishikant A. Raut
1.1
1.2.1
1.2.2
1.3
1.5
1.4.1
1.4.2
1.4.3
1.4.4
1.5.1
1.5.3
3. Phototherapy: The novel emerging treatment for cancer
21.7 Magnetic resonance imaging for monitoring release of drug 437
21.8 Photo-triggered theranostics nanomaterials: Principle and applications 438
21.8.1 Applications of photo-triggered theranostics nanomaterials in cancer treatments 438
21.8.2 Therapeutic applications of photobased theranostic nanoparticles 438
21.9 Opportunities and limitations of nanomaterials 439
21.10 Preclinical challenges 439
21.11 Future aspects of nanomaterials in the therapeutics 439
References 440
22. Nanocrystals in the drug delivery system
Raju Ramesh Thenge, Amar Patel, Gautam Mehetre
22.1 Introduction to nanocrystals and nanosuspension 443
22.1.1 Properties of nanocrystals 443
22.1.2 Nanocrystals and bioavailability 444
22.1.3 Various methods of characterization of nanocrystals formulations 444
22.2 Production methods and technology of nanocrystals 445
22.2.1 Top down technology 445
22.2.2 Bottom up technology 446
22.2.3 Top down and bottom up technology 446
22.2.4 Spray drying 447
22.3 Advantages and Disadvantages of nanocrystals 448
22.3.1 Potential advantages and disadvantages of nanocrystals 448
22.3.2 Disadvantages of nanocrystals 448
22.4 Pharmaceutical Nanocrystals of API 448
22.4.1 Case studies of drug loaded in the nanocrystals 448
22.4.2 Application of nanocrystalsloaded carrier 449
22.5 Conclusion 452
Contributors
Nishant Awandekar Smt. Kishoritai Bhoyar College of Pharmacy, Kamptee, Nagpur, India
Panchali Barman Institute of Forensic Science and Criminology (UIEAST), Panjab University, Chandigarh, India
Veena Belgamwar Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Mangesh Bhalekar Department of Pharmaceutics, AISSMS College of Pharmacy, Pune, India
Vidyadevi Bhoyar University Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Alap Chaudhari Formulation R&D, Teva Pharmaceuticals, Weston, FL, USA
Vibha Chopra P.G. Department of Physics & Electronics, DAV College, Amritsar, Punjab, India
Vivek S. Dave Department of Pharmaceutical Sciences, St. John Fisher College, Wegmans School of Pharmacy, Rochester, NY, USA
Nirupama S. Dhoble Deaprtment of Chemistry, Sevadal Mahila Mahavidhyalaya, Nagpur, Maharashtra, India
Sanjay J. Dhoble Department of Physics, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Sachin Dubey Drug Product and Analytical Development, Ichnos Sciences SA, La Chaux-de-Fonds, Switzerland
Shraddha Dubey Inselpital University of Bern, Bern, Switzerland
Purushottam Gangane Dept of Pharmaceutics, Dadasaheb Balpande College of Pharmacy, Besa, Nagpur, MS, India
Anjali Ganjare Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Shailendra Gurav Department of Pharmacognosy, Goa College of Pharmacy, Goa University, Panaji, Goa, India
Nilesh Haran Department of Radiology HCG-NCHRI Cancer Centre, Near Automotive Square, Nagpur, Maharashtra, India
Prakash R. Itankar Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Sheeba Jacob Virginia Commonwealth University, Richmond, VA, USA
Shubhi Joshi Energy Research Centre, Panjab University, Chandigarh, India
Vijay Kale College of Pharmacy, Roseman University of Health Sciences, South Jordan, UT, United States
Vinita Kale Pharmaceutics Deptt., Gurunanak College of Pharmacy, Nagpur, Maharashtra, India
Shagufta Khan Department of Pharmaceutics, Institute of Pharmaceutical Education and Research, Borgaon (Meghe) Wardha, Maharashtra, India
Rohini Kharwade Dadasaheb Balpande College of Pharmacy, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Pramod B. Khedekar Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Vaishali Kilor Department of Pharmaceutics, Gurunanak College of Pharmacy, Nagpur, Maharashtra, India
Dadasaheb M. Kokare Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Mallesh Kurakula Product Development, CURE Pharmaceutical, Oxnard, CA, USA
Anurag Luharia Department of Radiology, Datta Meghe Institute of Medical Science (Deemed to be University), Sawangi, Wardha, Maharashtra, India
Renuka K. Mahajan Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
Nilesh M. Mahajan Dadasaheb Balpande College of Pharmacy, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
S ection 1
Phototherapeutics
1. Phototherapy: A critical review 3
2. Phototherapy for skin diseases 15
3. Phototherapy: The novel emerging treatment for cancer 31
4. Fundamentals of photodynamic therapy 51
5. Photodynamic therapy for cancer treatment 89
6. Photodiagnostic techniques 115
7. The role of physics in modern radiotherapy: Current advances and developments 139
8. Physics in treatment of cancer radiotherapy 163
9. Role of carbon ion beam radiotherapy for cancer treatment 193
Chapter 1
Phototherapy: A critical review
Nilesh Rarokara, Shailendra Guravb, Dadasaheb M. Kokarea, Vijay Kalec, Nishikant A. Rauta
aDepartment of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
bDepartment of Pharmacognosy, Goa College of Pharmacy, Goa University, Panaji, Goa, India
cCollege of Pharmacy, Roseman University of Health Sciences, South Jordan, UT, United States
1.1 Introduction
Phototherapy can be broadly defined as the use of photons for the treatment of diseases without the addition of an exogenous photosensitizer. Ultraviolet B (UVB) radiations (280–320 nm) are the most biologically active radiation in sunlight and are mainly responsible for erythema. The term “phototherapy” was used as a synonym for UVB radiation in the management of psoriasis. Phototherapy has wide clinical applications like pityriasis lichenoides, vitiligo, atopic eczema, polymorphous light eruption, pruritus, etc. ( Morison, 1993 ). Recent work in phototherapy explores the selective use of UV with a narrow wavelength centered on 311 ± 1 nm. It has been proven more effective and less erythemogenic than conventional broadband phototherapy (Larkö, 1989 ). Treatments are usually given three to five times a week. The most widely used initial dose is 70% of the predetermined minimal erythema dose (MED) ( Green et al., 1988 ). Treatment is continued until the condition is resolved ( Wainwright et al., 1998 ). Selective UV phototherapy is the treatment of choice in children, which was used in the various study. The short-term side effects of phototherapy are usually mild and consist of xerosis and erythema, partly due to occasional overexposure. Another risk can be the photoactivation of herpes-virus. Long-term side effects of UVB phototherapy include premature photoaging and carcinogenesis with an increased incidence of wrinkling, actinic keratoses, lentigines, telangiectasia, and basal, and squamous cell carcinomas ( De Gruijl, 1986 ). Radiation received from UVB phototherapy is cumulative with chronic sunlight exposure. UVB in combination with UVA phototherapy (UVAB) has been shown to produce better therapeutic success than UVB per se in treating mild to moderate atopic dermatitis ( Falk, 1985 ; Hannuksela et al., 1985 ; Paši ć et al., 2003 ). Phototherapy uses UV radiation or visible light for the treatment of different diseases by the exposure of small, well-defined anatomical areas to non-ionizing radiations using dichromic lamps, fluorescent lamps, light-emitting diodes, lasers, polychromatic polarized light, or very bright, full-spectrum light for therapeutic advantages. The origin of phototherapy can be traced back to 1500 BC, when Hindus treated vitiligo, an autoimmune skin disorder, with photosensitizing plant extracts and subsequent sunlight exposure. For many centuries only natural sunlight (heliotherapy) was used to treat different skin conditions. Interestingly, it is still highly popular for psoriasis and atopic dermatitis in many geographic areas in the world, especially in the Dead Sea region ( Matos et al., 2016 ). As heliotherapy is only feasible in certain periods of the year with additional dosing variables depending on the geographic locations, artificial light sources are developed to emit selective wavelengths of electromagnetic radiation. Furthermore, identifying photosensitizers from plant extracts with unique photochemical properties resulted in the development of the photochemotherapeutic approach. It was found to be most effective in the treatment of inflammatory skin diseases. Lasers and intense pulse light (IPL) are well-established therapeutic tools to treat congenital and acquired vascular lesions. The erythema, skin inflammation can be treated by targeting blood vessels with lasers or IPLs, and it has proven a good alternative for the treatment of various skin diseases. Decades of research have been shown to improve inflammatory skin conditions with variable success by using vascular lasers. In recent years, low-level light/laser treatments (LLLT) emitting low-intensity visible light were tried for psoriasis and atopic dermatitis. Still, their efficacy and the mechanism of action need further clarification. When selecting the appropriate treatment for patients, many different conditions, such as comorbidities, age, and disease severity, must be considered ( Kaushik and Lebwohl, 2019a , 2019b ). Although there are several traditional and biologically active agents for psoriasis and atopic dermatitis, phototherapy approaches are still widely utilized ( Kemény et al., 2019 ).
Goethe’s idea on the impact of light on emotional states was resurrected when phototherapy was employed to treat depression. In 1946, in Scandinavia, the first descriptions of depression treatment using light were published (Marx, 1946); however, the fundamental development of phototherapy in the treatment of depression did not occur for four more decades (Rosenthal et al., 1984).
Phototherapy was also explored in ophthalmology. Gerhard Meyer-Schwickerath (1920–1992) investigated the use of natural sunlight for treating retinal disorders. Gerhard Meyer-Schwickerath performed a successful surgical operation with a photocoagulator in 1949 (Meyer-Schwickerath, 1960). It was a device designed and placed on the clinic’s roof to aggregate light onto a mirror in the operating room, paving the way for the application of laser therapy in retinal diseases (Grzybowski et al., 2016).
1.2.2 Overview on various types of phototherapies
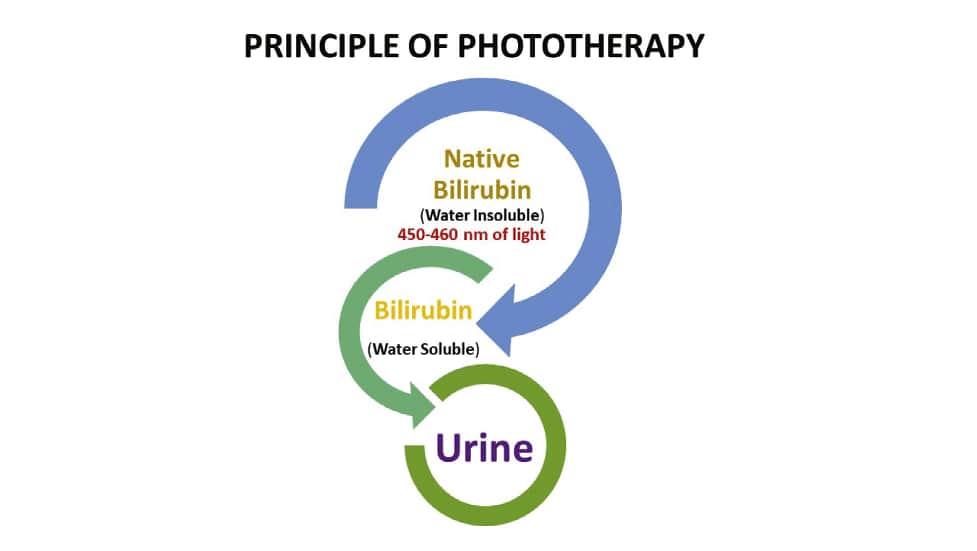
The traditional phototherapy units using fluorescent tubes contain standard blue (Westinghouse F20T 12B), daylight (F20 T12D), and cool white (F20 T12CW) lamps. The most effective lights are those with a high energy output near the maximum absorption peak of bilirubin (450 to 460 nm) as shown in Fig. 1.1 (Weiss and Zimmerman, 2013). Special blue lamps (Phillips TL 52/20W, Westinghouse 20 watt F20 T12BB) are the most efficient for neonatal phototherapy because it has more than twice the energy output at 450 nm than the standard blue bulb (Ennever et al., 1983). Investigators reported the significance of blue light in phototherapy with rapid reduction of serum bilirubin than with daylight or standard blue bulbs. On the other hand, these special blue bulbs cause nausea and dizziness among the neonatal care staff. A combination of four special blue lamps placed in the center of the phototherapy unit with two days’ light lamps on either side has been found to provide excellent irradiance without producing significant discomfort to staff. Non-fluorescent halogen lamps make a more intense light over a smaller surface. If lamps are placed closer than 50 cm, halogen lamps, unlike fluorescent bulbs, incur a risk of burns to an infant.
Light-Emitting Diode (LED) lights are now commercially available for use in the United States (Maisels and McDonagh, 2008). The Neo Blue LED systems incorporate optimal blue LED technology and are manufactured by Natus Medical Inc., San Carlos, CA, USA. Neo Blue LED’s emit blue light in the 450–470 nm spectrum. It is one of the safest phototherapy devices available as they do not emit light in the harmful ultraviolet and infrared radiation range. Further, the absence of heat when delivering overhead neo blue phototherapy is less likely to cause physiological water loss (Seidman et al., 2000). Fiber-optic phototherapy systems first appeared in the market around 1989. They are widely considered to be equally effective and more convenient than overhead lights. Light is delivered from a halogen bulb through a fiber optic cable and is
FIG. 1.1 Principle of phototherapy showing conversion of water-insoluble bilirubin to the soluble form upon exposer to a light wavelength of 450–460 nm.
emitted from the sides and ends of fibers inside a plastic blanket protected by a disposable cover. Infants lie on the blanket or are held with the blanket wrapped around them, and the need for eye patches, otherwise required in neonatal phototherapy, is eliminated.
Technology currently provides the clinician with three different modes of phototherapy delivery: fiber optic, low intensity, and high-intensity phototherapy. For low-intensity phototherapy, overhead lamps are typically set at a distance of 50 cm from the patient. The American Academy of Pediatrics has defined High-intensity phototherapy as a spectral irradiance of at least 30 MW per square meter per nanometer. High-intensity phototherapy is achieved by using a unit with eight special blue lamps, or Neo Blue LED systems 25 cm above the unclothed infant on a fiber optic phototherapy blanket in a bassinet while wearing a tie-on surgeon’s mask as a diaper. This method allows maximum skin exposure and achieves irradiance as high as 50 uw/cm2/nm.
However, as overhead lamps to infant distance are decreased, there is an increase in the heterogeneity of irradiation, with a much greater expansion at the center than at the periphery. Lining the bassinet with a white cloth produces greater homogeneity or irradiance and an increase in indirectly reflected irradiance (Maisels et al., 2007; Zauk, 2015).
1.2.2.1 UVB therapy
The UVB therapy includes NB-UVB and BB-UVB. The UVB therapy exerts effect by damaging nuclear DNA within epidermal-dermal junctional cells leading to apoptosis and cellular death of keratinocytes, immune cells, and fibroblasts (Bulat et al., 2011; Bolognia and Schaffer, 2012; Vangipuram and Feldman, 2016). NB-UVB (wavelength 311–312 nm) has largely replaced the use of BB-UVB (290–320 nm) due to its greater efficacy and emission duration at lower cumulative doses resulting in a reduction of associated long-term complications. NB-UVB is indicated as a first-line treatment of moderate-to-severe psoriasis and is also efficacious in treating numerous other dermatologic conditions (Ighani et al., 2018). The excimer laser is a targeted form of UVB treatment. It uses an active medium composed of excited dimers (noble gas argon/krypton/xenon) and reactive halogen gas (fluoride or chloride), delivering 308 nm light and facilitating the delivery of high doses of UVB to localized areas of skin (Mehraban and Feily, 2014). This focal treatment is beneficial in areas, which are difficult to treat such as the scalp, palms, and soles. It allows for a higher initial dose, less treatments, and thus, low long-term side effects. The excimer laser is currently approved in the USA for the treatment of conditions including psoriasis, and vitiligo, in addition to other localized inflammatory dermatoses (Alshiyab et al., 2015).
1.2.2.2 UVA therapy
The UVA is absorbed in the dermis and exerts its apoptotic effect on dermal blood vessel components, dendritic cells, fibroblasts, endothelial cells, and mast cells. UVA is further categorized into UVA1 (340–400 nm) and UVA2 (320–340 nm). UVA1 utilizes non-erythemogenic wavelengths and is indicated in the treatment of atopic dermatitis, localized scleroderma (morphea), systemic sclerosis, urticaria pigmentosa, cutaneous T cell lymphoma, dyshidrotic eczema, as well as other dermatoses (York and Jacobe, 2010).
1.2.2.3 PUVA therapy
PUVA involves administering either oral, topical, or bath psoralen followed by subsequent exposure to UVA, either via phototherapy or direct sunlight (PUVAsol). Psoralens (commonly methoxsalen or 8-methoxypsoralen) intercalate between DNA base pairs and, upon photon absorption, chemically activate to crosslink DNA. It results in several antiproliferative, antiangiogenic, apoptotic, and immunosuppressive effects. Melanogenesis is also stimulated via unknown mechanism. PUVA is effective in the treatment of several dermatologic conditions. PUVA treatments can result in severe blistering photoreactions/burns. PUVA is associated with a higher risk of skin cancer compared to other forms of phototherapy (Youssef et al., 2016).
1.2.2.4
Home phototherapy
Home phototherapy is another type that is limited to otherwise healthy term infants older than 48 hours with bilirubin levels 15-20 mg/dl with no hemolysis. Parents are required to be able to monitor the temperature and hydration status of infant. Home visits by a skilled nurse in evaluating newborns are performed, and bilirubin levels are assessed periodically. UVB therapy is equally effective when performed at home versus in the outpatient office setting and could be cost effective and more convenient to patients. Home phototherapy was associated with higher rates of dose reduction and/or discontinuation of biologics and apremilast, especially in patients with multiple comorbidities. There are several advantages assessing the efficacy of home phototherapy in treating other dermatologic conditions (Click et al., 2017; Howell et al., 2018). Tanning beds are an efficacious method of UV exposure and are recommended for patients who benefit from a more accessible,
less costly alternative to office and/or home phototherapy. The effect of tanning beds may be from UVA exposure, though common tanning bulbs emit varying degrees of UVB light. Of concern, use of tanning bed require limited supervision of control settings and duration of treatments, leading to the potential for increased adverse events (AEs) (Radack et al., 2015), however the amount of UV radiation received is likely to be better controlled with tanning beds than with sun exposure (Krenitsky et al., 2020).
1.3 Various light sources and methods of phototherapy
There is a considerable selection of several custom-made and commercial phototherapy devices, which have been produced for investigative and clinical applications. The phototherapy devices are categorized by their light source as follows: (1) fluorescent tube (TL12, 60 cm, 20W) devices with different colors of light (cool white [CW], blue, special blue [BB, 52, and 03], turquoise, or green) of straight or U-shaped (18 cm, 18W tubes), (2) metal halide bulbs used in spotlights and incubator lights, (3) metal halide bulb and fiberoptic light guide combinations as used in pads, blankets or spotlights, and (4) high-intensity LEDs used presently as canopies.
1.3.1 Fluorescent tubes
The most commonly used light source in the U.S. is the special blue tube, such as F20 T12/BB or TL52/20W (Philips, The Netherlands). CW light has also been used together with special blue tubes to ameliorate caregivers’ complaints regarding the blue hue of the light (Sisson and Kendall, 1973). Still, this combination of tubes dramatically decreases efficacy by 50% depending on the proportion of CW to special blue tubes. At a standard distance of 40 cm, the devices with a 1:1 ratio of tubes can deliver up to 11 W/cm2/nm, while a unit containing only special blue tubes can deliver up to 24 W/cm2/nm. However, the use of CW light typically provides only homeopathic doses of phototherapy. In addition, it may be inadequate in sufficiently decreasing total bilirubin levels in a jaundiced infant unless the lights are positioned in close proximity, such as directly above the infant (De Carvalho et al., 1999).
1.3.2 Halogen spotlights
Halogen spotlight systems utilize single or multiple metal halide lamps as the light source and provide fairly high irradiance, often exceeding 20 W/cm2/nm. However, these units can generate considerable heat, which can, in turn, cause thermal injury to the infant and staff if applied too closely and can emit ultraviolet (UV) radiation if not appropriately shielded. The use of spotlights is sometimes preferred in the neonatal intensive care unit because with premature or critically ill neonates on radiant warmers, its design allows for ad hoc positioning of these devices for the convenience of caregivers. However, their variable positioning with respect to the distance from the infant and angle of application and their irradiance heterogeneity can lead to unreliable dosing and unpredictable clinical response (Vreman et al., 2004).
1.3.3 Fiberoptic blankets
Fiberoptic devices contain a tungsten-halogen bulb that delivers light via a cable into a plastic pad containing fiberoptic fibers. The pad remains cool and can be placed directly under an infant to increase the skin surface area that is exposed. The pad can also be wrapped around the infant’s midsection to provide phototherapy (Vreman et al., 2004). The spectral power of the pad alone is low, therefore it is commonly used in conjunction with overhead lights to provide double phototherapy.
1.3.4
Light-emitting diodes
The gallium nitride LED is one of the most recent innovations in phototherapy. These devices provide high irradiance in the blue to blue-green spectrum without excessive heat generation (Maisels, 2005) Light-emitting-diode units are efficient, long-lasting, and cost-effective. The latest models incorporate amber LEDs to counteract the “blue hue” effect that can irritate caregivers (Stokowski, 2006).
1.3.5
Filtered sunlight
The lack of devices and/or reliable electric power limits the use of phototherapy in underdeveloped countries. Further, modern phototherapy devices are not affordable, often break down because of electrical power surges, and are difficult to maintain due to the unavailability of replacement parts. Even where phototherapy devices are available, most hospitals lack
targeted approach that enhances specificity towards cancer cells. However, success of PDT depends on the selection of PS, as the administered PS must be deep entered into the tumor cells and then activated by irradiation of light. The cell death that occurs during PDT is the apoptotic response of the sub-cellular localization of PS. There are two approaches generally used in PDT: electron transfer (eT) happens due to the generation of radical species at the excited state. Another is energy transfer (ET) created by electronic excitation and energy transfer from an excited triplet of PS to a triplet oxygen molecule. Hence, the clinical use of PDT in combination with chemotherapy would be the better option as it works at the electronic level inside the cell.
Phototherapy involves the irradiation of tissues with light and is commonly implemented in PDT and photothermal therapy (PTT). Photosensitizers (PSs) are often needed to improve the efficacy and selectivity of phototherapy via enhanced singlet oxygen generation in PDT and photothermal responses in PTT. In both cases, efficient and selective delivery of PSs to the diseased tissue is of paramount importance. PTT monotherapy typically cannot completely eradicate tumors due to non-homogeneous heat distribution in tumor tissues. Several strategies have been adopted to increase the anticancer efficacy of PTT and PTT-based combination therapies. First, better PTT agents with high light absorptivity in the near-infrared spectrum, high photothermal conversion efficiency, long blood circulation times, and enhanced tumor uptake are being sought to improve photothermal therapy. Second, synergistic effects of PTT and other therapeutic modalities are being explored to enhance anticancer efficacy. The combination of PTT with reactive oxygen species, small interference RNAs, or chemotherapeutics can drastically increase treatment efficacy. Third, image-guided PTT with theranostic agents (which are used for treatment and diagnosis both) based on multifunctional nanomaterials can also increase treatment efficacy of PTT via selective delivery of PTT agents to tumors ( Morton et al., 2002 ).
1.4.4 Limitations of home phototherapy and sunlight
The irradiance and surface area exposure produced by the home phototherapy unit is lower than typical units used in the hospital, making them less efficient at lowering the serum bilirubin level. Although phototherapy is indicated as treatment, current guidelines state that clinically high bilirubin warrants treatment should be managed in the hospital. Lack of control treatment guidelines, duration of therapy, and variable sunlight prevented its use to treat hyperbilirubinemia and/or poor treatment, leading to adverse outcomes. Although in the past, parents had been told to expose jaundiced infants to the sunlight at courtyard of an English hospital, this practice is not considered a safe or reliable way to treat jaundice. There are reports in the literature of infants developing kernicterus after their parents were instructed to treat their jaundice at home by exposing them to sunlight, in some cases for 15 min per day. Sunlight is ineffective and contributes to delays in recognizing the severity of the hyperbilirubinemia (Stokowski, 2006; Lan et al., 2019).
1.5 Recent developments and future scopes
1.5.1 The immunoregulatory effects of phototherapy: Possible pathways
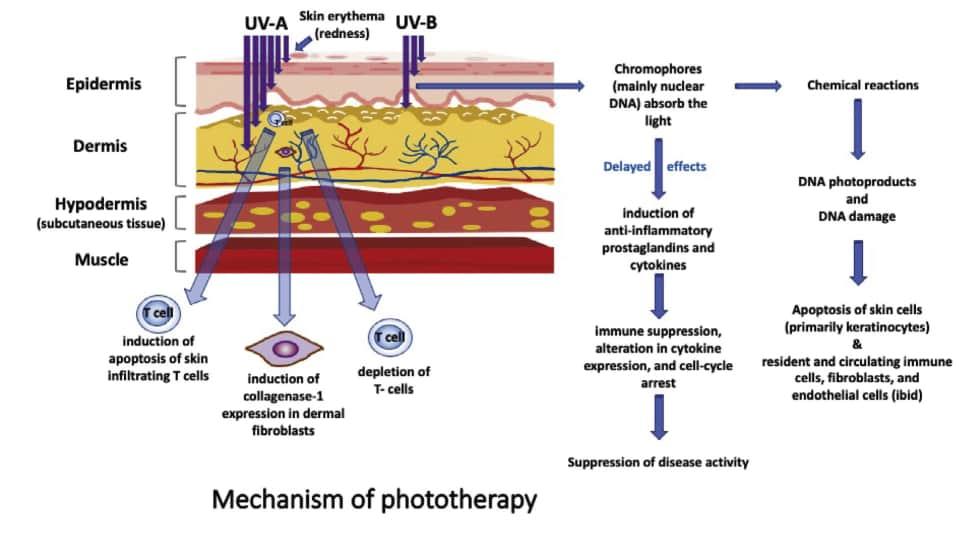
Psoriasis is caused by abnormal interactions among innate immune cells, T cells, and keratinocytes, leading to activation of the T helper cell type 1/T helper cell type 17 (Th1/Th17) immune axes and related cytokines. It contributes to the hyperproliferation, and inflammation seen in psoriasis. There are various mechanisms by which phototherapy may be effective for psoriasis. First, UV light induces apoptosis of keratinocytes and T cells in the epidermis and dermis. Second, UV light promotes immunosuppression by promoting migration of Langerhans cells of the epidermis and decreasing mast cell degranulation and histamine release. Lastly, UV light induces alteration in the cytokine profile of psoriasis ( Bulat et al., 2011 ). The schematic representation for mechanism of phototherapy has been depicted in Fig. 1.2
Research carried out recently has led to a better understanding of the specific pathways and alteration of cytokines by phototherapy. This therapy shifts the immune response away from the Th1/Th17 pathway toward the counter regulatory Th2 axis. The Th1/Th17 pathway is suppressed by NB-UVB, leading to decreased interleukin-12 (IL-12), IL-17, IL-20, IL-22, and IL-23. These effects on cytokines appear to be systemic and not just localized to psoriatic lesions. PUVA and NB-UVB lower plasma levels of tumor necrosis factor-alpha, IL-17, IL-22, and IL-23 at the end of 6 weeks of treatment. Furthermore, regulatory T (Treg) cells in patients with severe psoriasis display an enhanced propensity to convert into IL-17A-producing cells, linked to the loss of forkhead box P3 (Foxp3). UVB increases Foxp3-positive Treg cells in psoriatic skin lesions. This increase in Foxp3 expression improves Treg cell stability and reduces pro-inflammatory Th1/Th17 cytokines in psoriatic skin lesions (Wong et al., 2013).
1.2
explanation depicting how phototherapy works.
1.5.2 Handheld phototherapy: Targeting difficult-to-treat psoriasis in the office and at home
Whole-body phototherapy is limited as needless exposure of uninvolved skin and no benefit to unexposed skin (such as the hair-covered scalp). In the last decade, various portable and lightweight handheld phototherapy units have become available to treat localized psoriasis in the clinic and at home. These handheld devices, as compared to full-body irradiance in a booth or by a panel, have the added benefit of limiting skin exposure to UV light. The handheld devices are useful for the treatment of scalp psoriasis as well as recalcitrant localized psoriasis plaques. For example, the Dermalight 90 by National Biological Corporation, USA has a comb attachment that permits the direct application of light to scalp lesions (https://www.natbiocorp.com/our-units/dermalight-90/). Although large-scale clinical trials are lacking, such light combs appear to be productive with longer remission than other phototherapy treatments. The handheld devices typically deliver NB-UVB, but some devices use BB-UVB or UVA. The Dua Light by Theralight, Inc. and Psoria-Light by Psoria-Shield can provide UVB and UVA, but these devices are used only in the clinic setting ( National Biological Corporation, 2021).
1.5.3
The excimer laser: A potential new indication and a novel dosimetry protocol
In addition to targeted therapy in the form of handheld devices, the 308 nm excimer laser was developed in 1997 as a targeted NB-UVB source to treat psoriasis. The advantage of using the excimer laser is that because psoriasis plaques can take higher doses of light than normal skin, targeted treatment of psoriasis lesions using higher doses permits quicker time to clearance. In a multicenter open-label trial, 72% of patients with mild to moderate psoriasis achieved at least 75% improvement of the target plaque in an average of 6.2 treatments. In addition, compared with traditional whole-body phototherapy, the excimer laser required fewer visits.
In another study, 13 out of 26 patients with plaque-type psoriasis had continued clearance or long-term improvement after 1 year. These initial studies tested the excimer laser in patients with localized psoriasis. Although the excimer laser is currently indicated by the US Food and Drug Administration for treating mild to moderate psoriasis; however, the excimer laser may also be safe and effective for use in generalized, moderate to severe psoriasis. In a single-center pilot study, patients with greater than 10% but less than 30% body surface area involvement (moderate to severe psoriasis) were treated with excimer laser twice weekly for 12 weeks for a total of 24 treatment sessions. Fifty-four percent achieved PASI-75, and 83% achieved PASI-50, maintained without further treatment for six months. However, the downside to treating moderate to severe psoriasis is the long duration required per session to treat a large body surface area, which may not be feasible in many dermatology office settings (Abrouk et al., 2016).
FIG.
Schematic
1.5.4 Phototherapy and biologic agents: Combination therapy for recalcitrant psoriasis
Although several biologic agents showing excellent efficacy in treating moderate to severe psoriasis have been developed in the last decade, phototherapy appears to play an important role in a subset of patients with severe, recalcitrant psoriasis despite treatment with biologic agents. Several studies have demonstrated the efficacy of using etanercept and NB-UVB in combination. These studies evaluated this combination therapy in patients who had not previously received treatment, patients who had an inadequate response with etanercept alone (50 mg once-weekly or 50 mg twice-weekly dosing), or patients who had an inadequate response to NB-UVB alone. Overall, combination therapy was superior, and time to clearance was reduced. A study by Lynde et al. also demonstrated the importance of high adherence to the NB-UVB regimen to achieve significant clinical improvement. High adherence to the NB-UVB regimen was defined as missing two treatments in any four weeks (Nakamura et al., 2016; Choi et al., 2021).
1.5.5 Future scope
Future research areas for the excimer laser include large-scale, long-term studies evaluating its use for the treatment of moderate to severe psoriasis as a potential new indication. In addition, assessing the safety, efficacy, and practicality of the “plaque-based sub-blistering dosimetry” in a large-scale, long-term study is also of interest. Over many decades, phototherapy evolved and will continue to grow further in due course. None the less besides its usefulness in hyperbilirubinemia, it’s a valuable treatment option for many other skin disorders.
References
Abrouk, M., et al., 2016. Excimer laser for the treatment of psoriasis: safety, efficacy, and patient acceptability. Psoriasis (Auckl) 6, 165–173. doi:10.2147/ PTT.S105047.
Adauwiyah, J., Suraiya, H., 2010 Dec. A retrospective study of narrowband-UVB phototherapy for treatment of vitiligo in Malaysian patients. Med J Malaysia 65 (4), 297–299.
Alshiyab, D., et al., 2015. Targeted ultraviolet B phototherapy: definition, clinical indications and limitations. Clin. Exp. Dermatol. 40 (1), 1–5. doi:10.1111/ CED.12441.
Bulat, V., et al., 2011. The mechanisms of action of phototherapy in the treatment of the most common dermatoses. Coll Antropol. 35 (Suppl 2), 147–151.
De Carvalho, M., et al., 1999. Intensified phototherapy using daylight fluorescent lamps. Acta Paediatr. 88 (7), 768–771. doi:10.1080/08035259950169071. Chevreul, M., 1839. De la loi du contraste simultané des couleurs (eBook, 1839) [WorldCat.org] [Internet]. [cited 2015 Aug 10]. Pitois-Levrault, Paris. Available from: https://www.worldcat.org/title/de-la-loi-du-contraste-simultane-des-couleurs/oclc/797011105 (Accessed 1 November 2021).
Choi, G., et al., 2021. Inorganic–inorganic nanohybrids for drug delivery, imaging and photo-therapy: recent developments and future scope. Chem. Sci. 12 (14), 5044–5063. doi:10.1039/D0SC06724E.
Click, J., et al., 2017. Effect of availability of at-home phototherapy on the use of systemic medications for psoriasis. Photodermatol. Photoimmunol. Photomed. 33 (6), 345–346. doi:10.1111/PHPP.12349.
Cremer, R., Perryman, P., Richards, D., 1958. Influence of light on the hyperbilirubinaemia of infants. Lancet 1 (7030), 1094–1097. doi:10.1016/S01406736(58)91849-X.
Diffey, B.L., 1980. Ultraviolet radiation physics and the skin. Phys. Med. Biol. 25 (3), 405. doi:10.1088/0031-9155/25/3/001.
Downes, A., et al., 1877. Researches on the effect of light upon bacteria and other organism. RSPS 26, 488–500. Available from: https://ui.adsabs.harvard. edu/abs/1877RSPS…26.488D/abstract (Accessed 1 November 2021).
Ennever, J.F., McDonagh, A.F., Speck, W.T., 1983. Phototherapy for neonatal jaundice: optimal wavelengths of light. J. Pediatr. 103 (2), 295–299. doi:10.1016/S0022-3476(83)80370-9.
Falk, E., 1985. UV-light therapies in atopic dermatitis – PubMed. Photodermatology 2, 241–246. Available from:. https://pubmed.ncbi.nlm.nih. gov/3903678/ (Accessed 1 November 2021).
Finsen, N., 1896. Om Anvendelse I Medicinen af koncentrerede kemiske Lysstraaler. [On the application in medicine of concentrated chemical rays of light]. Gyldendalske Boghandels Forlag, Kjøbenhavn. Available from: https://www.jameslindlibrary.org/finsen-nr-1896/ (Accessed 1 November 2021). Finsen, N., Forchhammer, H., 1904. Resultate der Lichtbehandlung bei unseren ersten 800 Fallen von Lupus vulgaris [results of light therapy in our first 800 cases of lupus vulgaris]. Mitt Fins Med Lichtinst 5 (6), 1–48.
Goethe, J.W., 1810. In: Cotta, J. (Ed.), Zur Farbenlehre (Goethe’s Theory of Colours: Translated from the German; with Notes by Charles Lock Eastlake, R.A., F.R.S. 1840. Archived from the original on 12 December 2016. Retrieved 18 October 2017 – via Internet Archive.). John Murray, London. Available from: https://www.christies.com/en/lot/lot-6246603 (Accessed 1 November 2021). Green, C., et al., 1988. 311 nm UVB phototherapy–an effective treatment for psoriasis. Br. J. Dermatol. 119 (6), 691–696. doi:10.1111/J.1365-2133.1988. TB03489.X.
De Gruijl, F., 1986. Long-term side effects and carcinogenesis risk in UVB therapy. In: Hönigsmann, H., Jori, G., Young, A. (Eds.), The Fundamental Bases of Phototherapy. OEMF Spa, Milan, Italy, pp. 153–170.
Grzybowski, A., Pietrzak, K., 2012. From patient to discoverer–Niels Ryberg Finsen (1860–1904) – the founder of phototherapy in dermatology. Clin. Dermatol 30 (4), 451–455. doi:10.1016/J.CLINDERMATOL.2011.11.019.
Grzybowski, A., Sak, J., Pawlikowski, J., 2016. A brief report on the history of phototherapy. Clin. Dermatol. 34 (5), 532–537. doi:10.1016/J.CLINDERMATOL.2016.05.002.
Hannuksela, M., et al., 1985. Ultraviolet light therapy in atopic dermatitis. Acta Derm. Venereol. Suppl. (Stockh) 114 (SUPPL. 114), 137–139. doi:10.2340/00015555114137139.
Hession, M., Markova, A., Graber, E., 2015. A review of hand-held, home-use cosmetic laser and light devices. Dermatol Surg 41 (3), 307–320. doi:10.1097/DSS.0000000000000283.
Howell, S.T., Cardwell, L.A., Feldman, S.R., 2018. A review and update of phototherapy treatment options for psoriasis. Curr. Dermatol. Rep 7 (1), 43–51. doi:10.1007/S13671-018-0211-3.
Ighani, A., et al., 2018. Comparison of management guidelines for moderate-to-severe plaque psoriasis: a review of phototherapy, systemic therapies, and biologic agents. J. Cutan. Med. Surg. 23, 204–221. doi:10.1177/1203475418814234.
Kaushik, S., Lebwohl, M., 2019a. Psoriasis: Which therapy for which patient: focus on special populations and chronic infections. J. Am. Acad. Dermatol. 80 (1), 43–53. doi:10.1016/J.JAAD.2018.06.056.
Kaushik, S., Lebwohl, M., 2019b. Psoriasis: Which therapy for which patient: Psoriasis comorbidities and preferred systemic agents. J. Am. Acad. Dermatol. 80 (1), 27–40. doi:10.1016/J.JAAD.2018.06.057.
Kemény, L., Varga, E., Novak, Z., 2019. Advances in phototherapy for psoriasis and atopic dermatitis. Expert. Rev. Clin. Immunol. 15 (11), 1205–1214. doi:10.1080/1744666X.2020.1672537.
Krenitsky, A., Ghamrawi, R.I., Feldman, S.R., 2020. Phototherapy: a review and update of treatment options in dermatology. Cur. Dermatol. Rep. 9 (1), 10–21. doi:10.1007/S13671-020-00290-6.
Lan, G., Ni, K., Lin, W., 2019. Nanoscale metal-organic frameworks for phototherapy of cancer. Coord. Chem. Rev. 379, 65–81. doi:10.1016/J. CCR.2017.09.007.
Larkö, O., 1989. Treatment of psoriasis with a new UVB-lamp – PubMed. Acta Derm. Venereol. 69 (4), 357–359. Available from: https://pubmed.ncbi. nlm.nih.gov/2568064/ (Accessed 1 November 2021).
Levental, Z., 1977. Der ‘Sonnendoktor’ Arnold Rikli (1823–1906). Gesnerus 34, 394–403.
Lucey, J., Ferreiro, M., Hewitt, J., 1968. Prevention of hyperbilirubinemia of prematurity by phototherapy. Pediatrics 41 (6) 1047–1054.
Maisels, M., 2005. Jaundice. In: MacDonald, M., Mullett, M., Seshia, M. (Eds.), Avery’s Neonatology. 6th ed. Lippincott Williams & Wilkins, Philadelphia, PA, pp. 768–846.
Maisels, M., Kring, E., DeRidder, J., 2007. Randomized controlled trial of light-emitting diode phototherapy. J. Perinatol. 27 (9), 565–567. doi:10.1038/ SJ.JP.7211789.
Maisels, M., McDonagh, A., 2008. Phototherapy for neonatal jaundice. N. Engl. J. Med. 358 (9), 920–928. doi:10.1056/NEJMCT0708376. Marx, H., 1946. Zur Klinik des Hypophysenzwischenhirnsystems. Klin. Wochenschr. 24 (1), 18–21. doi:10.1007/BF01635615.
Matos, T., Ling, T., Sheth, V., 2016. Ultraviolet B radiation therapy for psoriasis: pursuing the optimal regime. Clin. Dermatol. 34 (5), 587–593. doi:10.1016/J.CLINDERMATOL.2016.05.008.
Mehraban, S., Feily, A., 2014. 308 nm excimer laser in dermatology. J. Lasers Med. Sci 5 (1), 8. Available from: /pmc/articles/PMC4290518/ (Accessed 2 November 2021).
Meyer-Schwickerath, G., 1960. Light Coagulation. CV Mosby, St. Louis. Morison, W., 1993. Photochemotherapy. In: Lim, H., Soter, N. (Eds.), Clinical Photomedicine. Marcel Dekker, New York, pp. 327–343. Morton, C., et al., 2002. Guidelines for topical photodynamic therapy: report of a workshop of the British Photodermatology Group. Br. J. Dermatol. 146 (4), 552–567. doi:10.1046/J.1365-2133.2002.04719.X.
Nakamura, M., Farahnik, B., Bhutani, T., 2016. Recent advances in phototherapy for psoriasis. F1000Res. 13 (5), 1684. doi:10.12688/F1000RESEARCH.8846.1.
National Biological Corporation, 2021. Dermalight® 90 https://www.natbiocorp.com/our-units/dermalight-90/ (accessed 07-08-2021).
Palm, T., 1890. The geographical distribution and aetiology of rickets. Practitioner, 10–11.
Pašić, A., et al., 2003. Phototherapy in pediatric patients. Pediatr. Dermatol. 20 (1), 71–77.
Patrizi, A., Raone, B., Ravaioli, G., 2015. Management of atopic dermatitis: safety and efficacy of phototherapy. Clin. Cosmet. Investig. Dermatol. 8, 511–520. doi:10.2147/CCID.S87987.
Pei, 2021. Light-based therapies in acne treatment. Indian Dermatol. Online J 6 (3), 145. doi:10.4103/2229-5178.156379.
Radack, K.P., et al., 2015. A review of the use of tanning beds as a dermatological treatment. Dermatol. Ther. 5 (1), 37–51. doi:10.1007/S13555-0150071-8.
Roelandts, R., 2002. Bicentenary of the discovery of the ultraviolet rays. Photodermatol. Photoimmunol. Photomed. 18, 208.
Roelandts, R., 2002. The history of phototherapy: something new under the sun? J. Am. Acad. Dermatol. 46 (6), 926–930. doi:10.1067/MJD.2002.121354.
Rollier, A., Rosselet, A., 1923. Heliotherapy. London, H. Frowde; Hodder & Stoughton, London. Available from: https://www.worldcat.org/title/heliotherapy/oclc/14777476 (Accessed 1 November 2021).
Rosenthal, N., et al., 1984. Seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. Arch. Gen. Psychiatry 41 (1), 72–80. doi:10.1001/ARCHPSYC.1984.01790120076010.
Seidman, D.S., et al., 2000. A new blue light-emitting phototherapy device: a prospective randomized controlled study. J. Pediatr. 136 (6), 771–774. doi:10.1016/S0022-3476(00)75202-4.
Sisson, T., Kendall, N., 1973. Avoidance of undesirable effects of blue light in phototherapy. J. Pediatr. 82 (1), 163–164. doi:10.1016/S00223476(73)80040-X.
Slusher, T., et al., 2014. Safety and efficacy of filtered sunlight in treatment of jaundice in African neonates. Pediatrics 133 (6), 1568–1574. doi:10.1542/ PEDS.2013-3500.
Stokowski, L., 2006. Fundamentals of phototherapy for neonatal jaundice. Adv. Neonatal Care 6 (6), 303–312. doi:10.1016/J.ADNC.2006.08.004.
Vangipuram, R., Feldman, S., 2016. Ultraviolet phototherapy for cutaneous diseases: a concise review. Oral Dis. 22 (4), 253–259. doi:10.1111/ODI.12366.
Vreman, H., et al., 2013. Evaluation of window-tinting films for sunlight phototherapy. J. Trop. Pediatr. 59 (6), 496–501. doi:10.1093/TROPEJ/FMT062.
Vreman, H., Wong, R., Stevenson, D., 2004. Phototherapy: current methods and future directions. Semin. Perinatol. 28 (5), 326–333. doi:10.1053/J. SEMPERI.2004.09.003.
Wainwright, D., Ferguson, 1998. Narrowband ultraviolet B (TL-01) phototherapy for psoriasis: which incremental regimen? Br. J. Dermatol. 139 (3), 410–414. doi:10.1046/J.1365-2133.1998.02403.X.
Weiss, E.M., Zimmerman, S.S., 2013. A tale of two hospitals: the evolution of phototherapy treatment for neonatal jaundice. Pediatrics 131 (6), 1032–1034. doi:10.1542/PEDS.2012-3651.
Wong, B.T., Hsu, B.L., Liao, M., 2013. Phototherapy in psoriasis: a review of mechanisms of action. J. Cutan. Med. Surg. 17 (1), 6. doi:10.2310/7750. 2012.11124.
York, N., Jacobe, H., 2010. UVA1 phototherapy: a review of mechanism and therapeutic application. Int. J. Dermatol. 49 (6), 623–630. doi:10.1111/ J.1365-4632.2009.04427.X.
Youssef, R., et al., 2016. Phototherapeutic modalities pose no significantly increased risk of oxidative damage to DNA in dark skinned individuals. Indian J. Dermatol. Venereol. Leprol 82 (6), 666–672. doi:10.4103/0378-6323.186485.
Yurdakök, M., 2015. Phototherapy in the newborn: what’s new? J. Pediatric Neonatal Individ. Med. 4 (2), e040255.
Zauk, A.M., 2015. Phototherapy: a simple and safe treatment for neonatal jaundice. J. Pediatr. Neonatal Care 2 (3). doi:10.15406/JPNC.2015.02.00070.
Zupanic-Slavec, Z., Toplak, C., 1998. Water, air and light: Arnold Rikli (1823–1906). Gesnerus 55, 58–69.
Chapter 2
Phototherapy for skin diseases
Renuka K. Mahajan, Dadasaheb M. Kokare, Nishikant A. Raut, Prakash R. Itankar Department of Pharmaceutical Sciences, Rashtrasant Tukadoji Maharaj Nagpur University, Nagpur, Maharashtra, India
2.1 Introduction
The organs, such as hair, glands, and nails together with the skin make up the integumentary system. Moreover, the skin is the outlying of the integumentary system (Lawton, 2019; Abdo et al., 2020). The skin, is a sizeable organ of the body, covering 16% of total body weight and 1.5–2.0 m2 of total surface area in an average adult. This multifunctional organ, besides providing protection from pathogens, physical abrasions and radiation from the sun, plays a vital role in synthesis of vitamin D, protection of vitamin B folates, and also makes us aware of external stimuli. Maintaining a constant body temperature with the help of sweating or shivering is another major role performed by skin. Integument is made up of epithelial and connective tissue. Fig. 2.1 illuminates the layers of skin namely, the epidermis, the dermis, and the underlying hypodermis.
2.1.1
The epidermis
The outer most protective wrap of the skin, composed of stratified squamous epithelium and dendritic cells is known as epidermis. It consists specific constellation of four types of cells. Keratinocytes: Keratinocytes produces keratin, a protein that hardens the skin. They also contain a special type of fat cells which makes the skin waterproof. The cells from basal layer (column-shaped keratinocytes) emigrate to the surface, resulting in keratinization. In this process keratinocytes pass from synthetic to degenerative phase. The mature keratinocytes at the surface are dead and filled entirely with keratin (Piotrowska et al., 2016). Melanocytes: They are dendritic, melanin synthesizing cells. Melanin is a pigment produced in membrane bound organelle called melanosome. This pigment allots color to skin and safeguard one from ultraviolet radiation. Melanocytes are responsible for transfer of melanin from melanosomes to the keratinocytes. This layer exuviates continuously and renews every 15–30 days giving rise to derivative structures, such as sweat glands and nails. Langerhans cells: These are phagocytic macrophages, derived from bone marrow. They interact with white blood cells (WBCs) during an immune response and are involved in T cells response. They are distributed over squamous, granular and basal cell layer. Merkel cells: These are oval shaped, discs-forming cells appearing deep into the epidermis at the boundary of epidermis and dermis. Merkel cells produce chemical signal in adjoining neuron and perform sensory functions.
The epidermis is further sub divided into five layers as shown in Fig. 2.2. Stratum corneum is at the periphery containing innumerable layers of dead, anucleate keratinocytes filled with keratin. This layer has tightly packed cells, which empowers the skin to be tough and impermeable. Its function is prevention from external things like bugs and bacteria. Stratum lucidum is generally found on the palms and soles of feet; it contains two to three layers of anucleate cells. The stratum granulosum, second layer in epidermis, contains 2–4 sheets of cells held in conjunction by desmosomes (a cell structure specialized for adhesion of cells). These cells hold keratohyaline granules, which give contribution in the development of keratin for skin strengthening. The layer, stratum spinosum contains 8–10 sheets of cells, which changes shape and are quite active in mitosis. Stratum basale is the bottomless layer of the epidermis containing one sheet of columnar cells actively splitting up by mitosis to construct cells that trek into the upper epidermal layers and eventually to the exterior of the skin. The stratum basale is segregated from the succeeding layer by a basement membrane, made up of proteins and collagen (Bergfelt, 2009; Abdo et al., 2020; Theoret and Stashak, 2014).
2.1.1.1 Dermis
The dermis is the supporting core layer of the integumentary system, made up of elastin, fibrillar structured protein called collagen, capillaries, and nerves. The collagen is responsible for strengthening, while elastin maintains elasticity of skin.