chsli.org/st-francis-hospital
A note from Catholic Health’s President & Chief Executive Officer
We’re all part of the solution.
Dear Colleagues,
Catholic Health has a comprehensive plan for enhancing Health Equity across our service area. The pages you’re about to read through will show you just how and where you play an indispensable role.
The sad truth is that many people, both nationally and regionally, suffer a vastly disproportionate amount of preventable disease. These are largely driven by the social determinants of health (SDOH): dietary habits, neglect and lack of access to quality health care.
We can do something about this, and Catholic Health is committed to doing so. Under the leadership of Dr. Lawrence Eisenstein, we have a comprehensive program to address the economic and social obstacles to good health.
Rooted in mission, Catholic Health believes health care is a right, not a privilege. That’s why we treat all patients in need of our services, regardless of their ability to pay. It’s also why we have proactive programs designed to bring exceptional health care to our underserved communities.
By working together, we can bend the disease curve. As you ramp up access to quality care, you address those SDOH. As you screen for and detect disease at its earliest stages, you make it possible to preempt serious, long-term debilitating diseases.
And that computes to longer, healthier lives as well as sharp reductions in health care costs. I thank you for being part of this all-important effort.
Patrick O’Shaughnessy, DO, MBA President & CEO
A note from St. Francis Hospital & Heart Center’s President
Dear Colleagues,
At St. Francis Hospital & Heart Center we are guided by our mission, vision and values to achieve excellence in all that we do. The Health Equity Plan is developed with the goal of improving the health and well-being of all. We believe health care is a right, not a privilege.
Unfortunately, some Long Islanders face barriers to good health and as a result are more likely to suffer from preventable disease. Disparities in health outcomes are closely linked to social, economic and environmental factors.
Our Health Equity Plan aims to reduce health disparities by providing access to quality care to under-resourced communities and by addressing the social drivers of health. It is intended to identify actual or potential health care disparities among population groups, and in the way demographic groups access, experience and receive health care. The plan considers both individual and community needs.
Some of our Health Equity initiatives include the Student Athlete Program, providing cardiac screening for high school students free of charge; the Gift of Life Program, providing corrective cardiac procedures for children who cannot access this care in their own countries; a Community Outreach Program, providing a multitude of educational classes, screenings and vaccinations; and the Food is Medicine Program, providing a ready bag of food and referrals to nutrition resources for patients who are in need.
Together, we are making great strides towards improving health outcomes for all. Thank you for your ongoing care for our patients and our communities. I am proud of the work we’re doing and look forward to continuing to improve access to the exceptional health care at St. Francis Hospital & Heart Center.
Peace and all good,
Charles Lucore, MD, MBA President, St. Francis Hospital & Heart Center
Catholic Health is a faith-based health care delivery organization, predominantly serving the residents of Nassau and Suffolk counties on Long Island. Comprised of 6 hospitals, 3 skilled nursing facilities, vibrant home care service delivery, home hospice and thousands of providers across Long Island, Catholic Health is proud of our mission of mercy, and considers mission and health equity as part of everything that is done at Catholic Health facilities and by its providers.
St.
St. Joseph Hospital
Catholic Health Ambulatory Care hubs – Commack – East Hills – Flushing – Lake Success – Merrick – Patchogue – Riverhead – West Babylon – Westbury – Woodbury
Executive Summary
Urgent Care – Ronkonkoma
Catholic Health Ambulatory & Urgent Care – Centereach – Melville
In 2022, Catholic Health set out to establish and incorporate a strategy and path forward for a newly formed Community and Public Health Program, of which health equity would be at the core. The inaugural Health Equity Written Strategic Plan 2023–2024 was released in the Fall of 2023. Guided by data, and following a model of defined goals and objectives, we present the third annual edition of Catholic Health’s written Health Equity Strategic Plan, 2025–2026. This year’s plan looks back on the second full year of efforts, and provides an update on objectives and direction. Further, this plan adds new objectives based on the incredible growth of Catholic Health’s equity initiative.
In line with Catholic Health’s Mission and Vision, and for compliance with regulatory requirements, Catholic Health continues to advance work towards health equity. Led by our Director of Epidemiology and Public Health Analytics, this year’s data is presented with a higher degree of stratification and analysis. Data collection is done with purpose and intent, and measures have been evaluated to assess the specific needs of the communities we serve, and to guide strategic operations going forward. With an emphasis on identifying and impacting health disparities, all of this work is done with the goal of achieving maximal health outcomes for our patients.
Catholic Health Physician Partners Practices – Babylon – Bay Shore
Bethpage
Deer Park – East Islip
East Setauket
Fresh Meadows
Garden City
Great Neck – Greenvale
Hampton Bays – Hicksville
Huntington
Islip
Levittown
Lynbrook
Massapequa
Medford
New Hyde Park
Oakdale
Plainview
Port Jefferson
Port Jefferson Station – Rockville Centre – Ronkonkoma – Roslyn – Smithtown – St. James – Valley Stream – Wantagh – West Babylon – West Islip – West Sayville
Catholic Health has committed to improving the health and wellness of all people within the communities we serve. With the support of Catholic Health leadership and the Board of Directors, the pillars of the Community Health Roadmap (see Figure 1.0) have not changed. This Health Equity Strategic Plan describes efforts to achieve objectives within the pillars. This report evaluates opportunities for improvement, and identifies deliverables and objectives, along with associated timeframes. Much of the design and implementation of this work is carried out by the volunteer members of Catholic Health’s health equity taskforce, referred to as the Health Equity Leadership Council (HELC). With representation from all campuses and major departments, the HELC and its four subcommittees continued to make great strides during their second year. These efforts are summarized in the Plan and the HELC is a vital source of objectives moving forward.
Much has changed since last year’s plan was released. One thing that has not changed is Catholic Health’s commitment to serving all of our patients, to help them live a life of wellness including successful preventive care and to assist in overcoming obstacles. Guided by our Ethical and Religious Directives we provide care for everyone, and as health equity is defined as the opportunity for everyone to achieve their highest level of health outcomes, our efforts continue and grow. This report summarizes the health equity efforts undertaken by Catholic Health and provides a strategic plan going forward.
Good Samaritan University Hospital Mercy Hospital
St. Catherine of Siena Hospital
St. Charles Hospital
Francis Hospital & Heart Center
Catholic Health’s Mission and Health Equity
As described in the definitions section which follows, health equity is defined as “the state in which everyone has a fair and just opportunity to attain their highest level of health. As a Catholic health care provider organization, Catholic Health is bound to follow the Ethical and Religious Directives for Catholic Health Care Services, 6th Ed. (ERDs), a book published by the United States Conference of Catholic Bishops. The ERDs guide us and not only support health equity work, but also require it. Catholic Health’s Mission aligns with the ERDs. As such, health equity is not seen as a political topic for debate. Rather, health equity simply refers to the care we provide, with an emphasis on ensuring that we care for the most vulnerable, with the goal that all patients have their best potential health outcome.
The most relevant ERD connecting with our mission is ERD#3: In accord with its mission, Catholic Health should distinguish itself by service to and advocacy for those people whose social condition puts them at the margins of our society and makes them particularly vulnerable to discrimination: the poor; the uninsured and the underinsured; children and the unborn; single parents; the elderly; those with incurable diseases and chemical dependencies; racial minorities; immigrants and refugees. In particular, the person with mental or physical disabilities, regardless of the cause or severity, must be treated as a unique person of incomparable worth, with the same right to life and to adequate health care as all other persons.
Further, following these directives are mandatory for Catholic health care providers as expressed in ERD #5: Catholic Health care services must adopt these directives as policy, require adherence to them within the institution as a condition for medical privileges and employment, and provide appropriate instruction regarding the directives for administration, medical and nursing staff and other personnel.
Caring for our patients and helping them achieve their highest health outcomes remains our objective. This Health Equity Strategic Plan is based on the tenets of our mission and follows the requirements of being a Catholic health care provider. Deliverables described within this plan are reported and discussed at Mission and Ministry Committee meetings. This written Strategic Plan is presented to the Board of Directors for approval via the Quality Management Committee meeting (QMC).
Key definitions
Health equity
Catholic Health defines health equity using the Centers for Disease Control and Prevention’s (CDC) definition: “Health equity is the state in which everyone has a fair and just opportunity to attain their highest level of health.” Catholic Health also ascribes to the CMS advancement of health equity actions including:
• Identify health disparities.
• Define specific and actionable goals for addressing any disparities identified.
• Prioritize populations and communities that are historically underserved.
• Establish and implement their organization’s health equity strategy.
• Determine what tools and resources their organization needs to implement its strategy.
• Monitor and evaluate progress in addressing health disparities.
Priority populations
Catholic Health serves a diverse population across Long Island. Our patients, who represent nationalities from all across the world, speak more than a dozen primary languages. In evaluating population health and demographics on Long Island, including race, ethnicity and language data, along with geography (see figures 1.1.1–1.3.1), Catholic Health’s equity strategy defines the system-wide priority population as those living in zip codes with the highest quartile of social vulnerability, as defined by the Social Vulnerability Index (SVI). The highest SVI quartile represents approximately 15% of our patient population and significant health disparities can be found when comparing the highest quartile to the rest of our patients (see figure 2.0).
Social Determinants of Health (SDOH)
Social Determinants of Health (SDOH) are the non-medical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, worship and age. This includes but is not limited to factors including economic, environmental, built environment, literacy and access to healthy food.
Social Vulnerability Index (SVI)
The SVI is a database of the CDC and Agency for Toxic Substances and Disease Registry (ASTDR), which refers to “the resilience of communities (the ability to survive and thrive) when confronted by external stresses on human health.” There are 16 factors that are formulated into a geographic map of social vulnerability, including demographics (e.g., race and ethnicity, socioeconomics) and numerous SDOH (e.g., housing situation and transportation access).
REaL
The term REaL refers to data collected on race, ethnicity and preferred language. Appropriate collection of demographic data plays a key role in understanding health equity. Both CMS and the American Hospital Association (AHA) have published numerous points of information emphasizing the need to collect REaL data. As explained by the AHA, “collecting and stratifying patient REaL data are crucial for hospitals and health systems to understand the populations they serve and to implement the appropriate interventions for improving quality of care.”
New York State 1115 Medicaid Waiver
New York State approved the 1115 Medicaid Waiver and the waiver period began on April 1, 2024. The Waiver period runs through March 31, 2027. New York State has chosen nine Social Care Networks (SCN) to administrate the Waiver over nine regions. The Health and Welfare Council of Long Island (HWCLI), longtime partners of Catholic Health, have been chosen as the SCN of Long Island. The main goal of the Waiver will be to address SDOH in Medicaid patients, and connect them to ongoing social services through community based partners. The resulting improvement in health outcomes, and decrease in preventable downstream health care utilization, are the long term justifications for the project. Catholic Health is actively participating as screeners for SDOH.
Equity as the central theme of the Community Health Roadmap
In 2022, Catholic Health established a Community Health Roadmap, which incorporates health equity into every aspect. This roadmap describes specific objectives and action steps that will guide Catholic Health along the health equity journey. The specific pillars, objectives and system action steps to improve health equity are presented.
Pillars of community health on the equity journey
Organizational culture, systemic integration & education
Catholic Health is working to incorporate an improved organizational culture of health equity system-wide. Educating more than 17,000 employees at Catholic Health on the tenets and practices of health equity was achieved through numerous in-service and educational objectives. Since the launch of our health equity initiative in early 2023, we have successfully trained over 4,300 new employees during the system-wide orientation on the fundamentals of health equity. This foundational training is part of our commitment to create an inclusive health care environment that recognizes and addresses disparities in care. The goal is to ensure that all employees receive comprehensive education on essential topics, including unconscious bias, SDOH and health equity principles. The Education subcommittee of the HELC has developed a robust educational framework. This includes mandatory learning modules and resources that employees must complete. This prioritizes ongoing professional development aimed at fostering a culture of continuous learning and improvement in health equity practices.
Organizational culture, systemic integration and education
Social determinants of health
and Equity
Data analytics and strategic planning
Equity programs must be based on appropriate collection, stratification and analysis of demographic and epidemiologic outcome data. It is imperative to improve the collection of REaL data to identify health disparities. The most appropriate geographic data (i.e. census tract, zip code, or SVI data) will be used to identify community needs and vital stakeholders, resources and strategic initiatives to decrease health disparities. Led by our Director of Epidemiology and Public Health Analytics, and with the incredible support of the Digital Transformation Systems (DTS) team, a new SDOH Dashboard has been launched to help ensure that all Catholic Health practitioners have access to the actual data within the communities they serve, so they can appropriately gear efforts at preventive health.
Screening for SDOH using the New York State Accountable Health Communities (NYSAHC) tool became the standard of care at Catholic Health, and a subsequent resource Database in Epic is expected to be activated soon to ensure there are resources for providers to offer to those who screen positive. Continual improvement in collection, stratification and analysis of data is paramount for any health equity program.
Community engagement/participation
Community member participation in their own health care will ultimately lead to improved outcomes. Access to care is a key component of achieving participation in care and outcome measures will be used to assess internal efforts at community engagement. Targeted community engagement based on statistical needs, health disparities and outcome measures, ensures the tenet that we provide tailored services to individuals and communities, with emphasis on serving the most at-risk. This aligns with our definition of health equity.
Figure 1.0
To help meet our goal of gaining community member participation in their own health care, we have numerous active initiatives in progress. This includes but is not limited to our speakers’ bureau (can present in 26 different languages), our telehealth access initiative at St. Brigid’s Parish, the growth of community health workers screening for SDOH, alignment and re-routing of our two Community Outreach buses to meet the needs of specific communities (with addition of bilingual social workers on the buses to help with insurance enrollment for those eligible), and hundreds of community health screening, education and resource-oriented events across Long Island.
Social Determinants of Health (SDOH)
Catholic Health supports a strategy of “well care” over the more traditional “sick care” often offered by hospitals and hospital systems. In our model of well care, addressing the SDOH as a means of helping people stay healthy and out of the hospital is a guiding principal. More than 80% of a person’s health outcomes are not clinical, but rather, are based on the social drivers and influences in their lives, along with their genetics. While we cannot alter genetics, Catholic Health endeavors to improve the controllable social drivers that lead positively to health, and negatively to illness and diseases, often chronic in nature. To launch Catholic Health’s work in this realm, in 2022, we launched a Food Insecurity Screening Program in all six of our Emergency Departments (ED). The initiative consists of screening all patients coming into the ED with the “Hunger Vital Signs,” published by the CDC. What differs this award-winning program from many others is that anybody who screens positive is provided with a “foodto-go bag” to ensure they do not go home to an empty kitchen. While that bag is only meant to cover food needs over the first couple of days post-discharge, social work teams spend those days addressing the social service need and ensuring ongoing food and nutrition services are implemented.
Food insecurity is not the only important SDOH and over the past year, Catholic Health has taken the major step of incorporating the New York State Accountable Health Communities (NYSAHC) social determinant screening tool as standard of care for all patients admitted to our hospitals. Further, we began the difficult task of preparing and providing a community resource data base which will be available in our Electronic Health Record (Epic) for all of our providers to use as a resource when patients screen positive. Practicing “well-care” will not be successful if we do not acknowledge the role of non-clinical and social factors. This brings us into realms outside of our book of business, so community collaboration is vital. Partnering with Community-Based
Organizations (CBOs) is a vital component of achieving health equity and meeting the SDOH needs of our patients. Catholic Health has established strong relations with the Health and Welfare Council of Long Island (HWCLI), including representation on the SCN governing body for the New York State 115 Medicaid Waiver, which is hosted by HWCLI. This helps us connect with many of the CBOs they represent. All of this leads to helping patients proactively stay healthy and well, avoiding unnecessary hospitalization.
Quality and Patient Experience
Catholic Health values quality to the point that “there is no quality without equity.” As such, equity is to be treated with quality metrics and measures, and performance is to be evaluated in an ongoing fashion. The HELC is establishing quality metrics and measures, staff is being trained and there will be a culture of accountability for the results. Ensuring that we meet our patients’ needs, including their cultural and religious needs, is paramount in our patient experience strategy. Factors such as communicating with patients in their preferred language, is an example of the intersection of equity, patient experience and quality. Outcomes are impacted by a patient’s comprehension of medical discussions.
The intersection of health equity and quality is so important that the formal reporting of the minutes of the HELC is part of the system-wide QMC (a Board of Directors level meeting), and the HELC Chairman presents a report on equity activities at the meetings. This year’s Health Equity Strategic Plan represents increased collection, stratification, and analysis of data metrics as it relates to quality and patient experience. As an example, ensuring that we communicate with patients in a way they understand will surely lead to improved outcomes and decreased negative quality indicators.
Regulatory requirements
Catholic Health diligently monitors and updates new procedures and reporting regulations from major oversight, regulatory and evaluative bodies, including but not limited to CMS, the Joint Commission and Leapfrog. Training staff in new rules and reporting requirements is embedded in equity metrics and training.
Catholic Health strives to achieve the highest scores on reviews, meet all emerging measures and reporting requirements, and comply with new imperatives as it relates to health equity, health disparities, evaluation and any identified necessary corrective measures.
Health Equity Leadership Council (HELC)
Catholic Health has established a multidisciplinary system-wide HELC to further the mission of Catholic Health and its affiliated entities. The Council shall champion and steward the system’s continued advancements in health equity for its patients, its employees and the Long Island community in a manner consistent with the system’s responsibilities under state and federal law, and the ERDs for Catholic health care services as interpreted and applied by the Bishop of the Diocese of Rockville Centre.
Catholic Health defines “health equity” as being achieved when every person has a fair and just opportunity to attain his or her highest level of health. Specifically, Catholic Health is dedicated to ensuring, insofar as it depends on the system, that excellent health outcomes are available to every person who presents at one of the system’s facilities or physician practice locations, notwithstanding social, political, economic or other conditions that commonly result in and perpetuate injustice or inequity among individuals.
The six-pronged mission of the Council is as follows:
• Establish Catholic Health as the most trusted health care system on Long Island by its dedication to justice in the system’s delivery of health services.
• Align the system with its Catholic Mission to reach and serve all communities, especially the most vulnerable, through the stewardship and deployment of its resources for the advancement of health equity.
• Increase, improve and leverage community relationships and partnerships to inspire, empower and sustain individuals to augment their health.
• Integrate consideration of health equity into all aspects of the system’s operations.
• Address and ameliorate SDOH to improve overall health outcomes and decrease unnecessary hospital admissions and readmissions.
• Meet emerging regulatory and industry requirements relative to health equity.
Subcommittees of the Council
Scope by Subcommittee
• Catholic Health First: Address health equity related needs, objectives and deliverables within the workforce and walls of Catholic Health.
• Education: Address education and training, disseminate information and raise awareness of equity activities, system initiatives and regulatory.
• Long Live Long Island: Address community partnerships, patient engagement and social drivers.
• Quality and Data Analytics: Address screening tools, epidemiology and digital optimization for information collection and messaging.
Catholic Health First Education
Long Live Long Island
& Data Analytics
Summary of year’s results by subcommittee
Catholic Health First (Paul Stuart, Chair)
Completed objectives:
• Evaluated and selected the eCornell equity-related certificate program as the foundational training for building our Health Equity Champion network.
• Graduated first cohort from the eCornell certificate program and secured funding for the second cohort in 2026.
• Identified four questions on the annual employee engagement survey to track as a measure of how our employees are feeling about belonging at Catholic Health as it relates to health equity.
• Compiled childcare resources available to our employees in one convenient location on the Catholic Health intranet.
• Increased employee awareness of the Employee Crisis Fund through incorporating it into the New Employee Orientation.
Ongoing objectives:
• Leverage the eCornell certificate program to establish and grow our campus equity champion network.
• Track engagement survey results related to health equity.
• Ensure our employees are aware of existing public and private childcare resources available to them.
• Increase visibility, accessibility and utilization of existing Catholic Health programs and offerings that support the health and welfare of our workforce.
Future objectives:
• Establish a formalized internal pathway for employees in crisis to follow in order to access assistance and resources.
– Leverage our internal Care Management expertise to support our employees in crisis through providing intake and referrals services.
• Leverage our Health Equity Champion network to gather deeper insight from our employees regarding our engagement survey results.
• Collaborate with the Long Live Long Island subcommittee to foster community relationships that support our recruitment strategy.
• Partner with our Center for Performance Excellence to increase awareness and utilization of existing Catholic Health programs and offerings that support career development and advancement.
Education subcommittee (Annmarie Smith and Dilys White, MD, Co-Chairs)
Completed objectives:
• Develop education programs that cover SDOH, implicit bias, cultural appropriateness and health equity frameworks.
– Inclusive Leadership Behavior workshop.
– Managing Difficult Conversation workshop.
• Require employee participation in continuing education sessions focused on health equity.
– Unconscious Bias online module, launched April 2024, refreshed April 2025.
– Health Equity education for new employees, implemented in 2023.
– SDOH education, launched 2024 and expanded January 2025.
• Expand GME curriculum.
– Education on health equity, and SDOH has been integrated into the physician resident program at Good Samaritan University Hospital and throughout the system.
• Activate Internal Speakers Bureau (equity education, system orientation speakers).
• Create an educational library on topics related to Health Equity (Catholic Health Academy).
Future objectives:
• Regularly evaluate the effectiveness of health equity education programs and make adjustments based on feedback and outcomes.
– Create tailored learning modules for different roles within the health care system.
• Support the Catholic Health first subcommittee with the Health Equity Champions Program. Equity Champions completed Cornell’s certificate program.
• Incorporate topics of health equity, SDOH and inclusive behaviors into the GME Series.
• Collaborate with educational institutions to improve learning resources.
Long Live Long Island (Lisa Santeramo, Chair)
Completed objectives:
• Established a Speakers Bureau: Currently 26 languages able to be presented by Catholic Health staff: Arabic, Bengali, Chinese, Creole, English, Filipino, French, German, Greek, Hindi, Italian, Korean, Malayalam, Mandarin, Polish, Portuguese, Punjabi, Romanian, Russian, Spanish, Tagalog, Tamil, Telugu, Turkish, Ukrainian and Urdu.
Ongoing objectives:
• Curate equity-specific community events based on data and mission.
• Expand collaboration with CBOs.
• Seek community grants in alignment with key equity priorities.
Future objectives:
• Volunteer Recruitment: Collaborate with the Human Resources Committee to create a system-wide program to better recruit employees for volunteer community outreach and speaking opportunities. This will enable Catholic Health to expand our reach within vulnerable communities.
• CBO Partnerships:
– Utilizing the listening session data: Identify and engage potential community partners that will support our mission goals.
– Bandwidth analysis: Establish internal mechanisms and processes to manage external partner relationships and address potential bandwidth challenges.
• Physician Partners and IPA synergy:
– Map practices with Health Equity focus
Develop and maintain an inventory of Catholic Health employed practices, facilities, and associated voluntary practices that either (a) operate a health equity initiative or (b) serve a patient panel with at least [20]% Medicaid or uninsured patients.
– Engage in listening sessions
Conduct structured listening sessions with leaders and frontline staff from the identified practices/facilities from item (i) to document their experiences and strategies in addressing social drivers of health outcomes.
– Align with Community Outreach
Identify actionable opportunities to align practice-level health equity and SDOH efforts with Catholic Health’s existing community outreach programs, with recommendations for cooperation and integration.
Data and Quality subcommittee
(Monique Ford and Jason Tagliarino, Co-Chairs)
Completed objectives:
• Establish and deploy system-wide SDOH screening tool.
• Expand SDOH mandatory education to Catholic Health employees.
• Develop an SDOH dashboard with stratification by unit and demographic information.
• Stratify patient experience data by demographic information with key improvement targets.
Ongoing objectives:
• Expand SDOH to all hospital outpatient departments and patient self-service during e-Check in.
• Implement action plans related to enhanced health equity data reporting to site to develop tailored action plans to address these gaps.
• Ensure equitable access to age-friendly care by systematically identifying and addressing the unique social, cultural, and clinical needs of diverse older adult populations, with the aim of reducing disparities in health outcomes and improving quality of life across all demographic groups.
• Implement the Epic Community Resource dashboard to track the most common resources recommended.
• Enable community resource directory in MyChart.
Future objectives:
• Implement new Epic encounter level dashboard to assess encounter-level instead of patient-level screening rates for SDOH. Compare screening and positivity rates across encounter types and combinations of departments and providers, and use metrics related to the specific questionnaires and modes of screenings to find factors contributing to success.
• Extract SDOH from notes using generative AI: Keep patients from falling through the cracks. Use generative AI to process visit notes and identify potential SDOH concerns. When the AI detects a risk, inline reminders prompt clinicians to complete a formal screening, which helps them ensure that patients can receive assistance and helps make your population-level reports more accurate.
• SDOH interventions shown front and center so that clinicians, care managers, community health workers, and others can see a full picture of how a patient’s social needs are being addressed. Social drivers include more information about interventions, such as whether an intervention might be needed, is in progress, or is not requested. They also show orders, procedures, and referrals that address a domain in addition to the Compass Rose Programs and community resource recommendations that already appear.
Demographics of Catholic Health’s patients
The following data are based on patient encounters from January 1, 2024 to December 31, 2024.
CHS System All Pts
Catholic Health’s Patient Population Overview
Patient race Figure 1.1.1: Patient race for all patients 18 years and older who had an encounter in 2024 (N=576,412). Source: Epic
Preferred language Figure 1.3.1: Preferred language for all patients 18 years and older who had an encounter in 2024 (N=576,412). Source: Epic
Non-Hispanic or Latino Hispanic or Latino No answer/ unknown
Ethnicity Figure 1.2.1: Patient ethnicity for all patients 18 years and older who had an encounter in 2024 (N=576,412). Source: Epic
CHS System Hosp Admiss
Catholic Health’s Hospital Admissions Patient Population Overview
Patient race Figure 1.1.2: Patient race for all patients 18 years and older who had a hospital admission in 2024 (N=75,278). Source: Epic
Preferred language Figure 1.3.2: Preferred language for all patients 18 years and older who had a hospital admission in 2024 (N=75,278). Source: Epic
Ethnicity Figure 1.2.2: Patient ethnicity for all patients 18 years and older who had a hospital admission in 2024 (N=75,278). Source: Epic
CHS System ED Admiss
Catholic Health’s Emergency Department Patient
Population Overview
Patient race Figure 1.1.3: Patient race for all patients 18 years and older who had an emergency department encounter in 2024 (N=139,409). Source: Epic
Preferred language Figure 1.3.3: Preferred language for all patients 18 years and older who had an encounter in 2024 (N=139,409). Source: Epic
answer/ unknown
Ethnicity Figure 1.2.3: Patient ethnicity for all patients 18 years and older who had an encounter in 2024 (N=139,409). Source: Epic
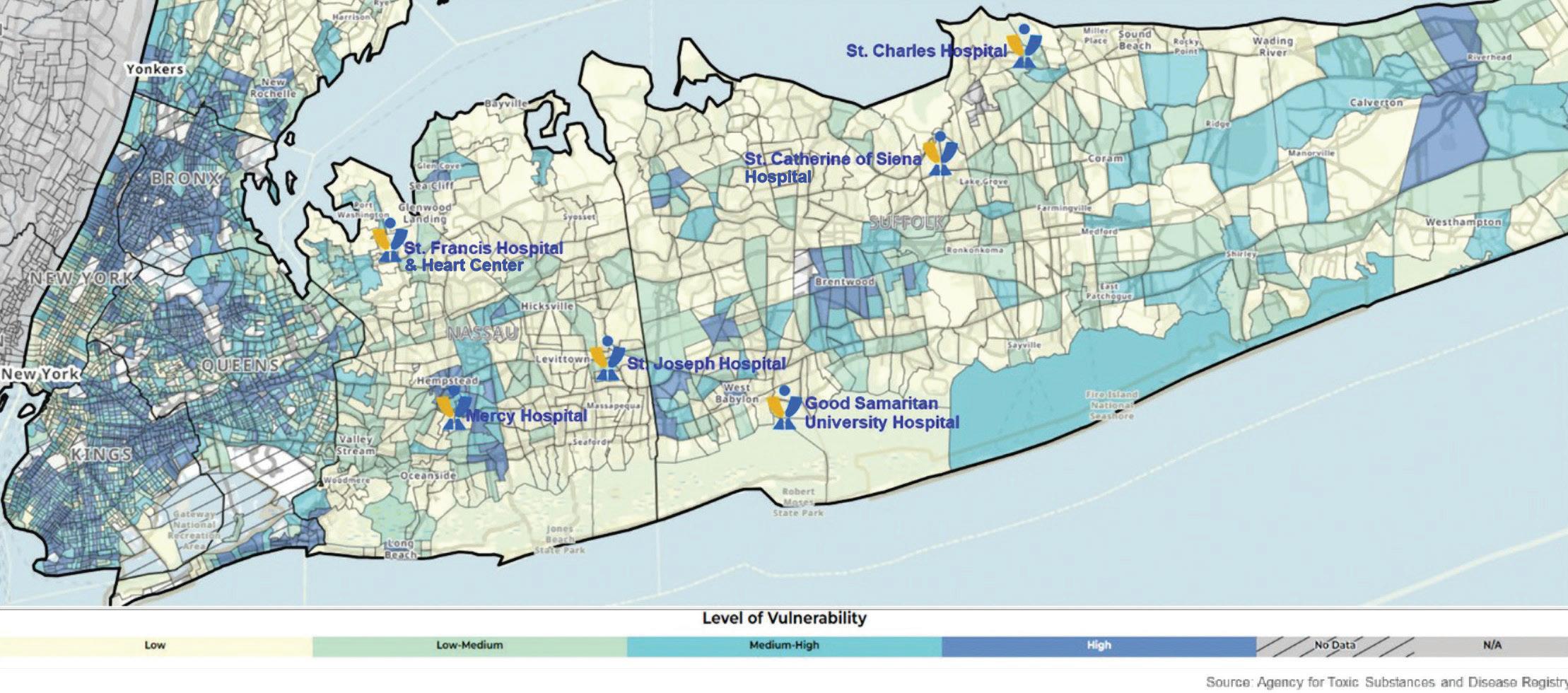
2020 Social Vulnerability Index by Census Tract for Queens, Nassau and Suffolk
Figure 2.0: SVI by Census Tract for Catholic Health service areas. Source: Epic
Identified System-wide Health Disparities
All disparities have been measured using Chi-square tests for statistical significance. Statistical significance was considered to be a p-value of less than 0.05. If no statistically significant differences were found it is denoted by an asterisk (*).
All data were obtained through Epic and include all patients with any encounter in the Catholic Health System from January 1 to December 31, 2024. Patients who died during or prior to 2024 were excluded from the sample. Age was calculated based upon each patients’ date of birth. For the influenza vaccination measure, the time period followed the ’24 – ’25 flu season (August 1, 2024 –July 31, 2025).
Race and ethnicity follow the Office of Management and Budget (OMB) federal race and ethnicity standard classifications. These are standard definitions provided by OMB to promote uniformity and comparability for race and ethnicity data. These categories are used in the decennial census, household surveys, administrative forms and medical/public health research.
Preferred language was categorized as English, Spanish or other languages from the patient’s last stored value during 2024.
Language data were disaggregated by our top two languages to facilitate visualization and statistical analyses. Stratification by preferred language does not include changes in self-reported preferred language.
Body Mass Index (BMI)
Table 1.1: Percent of patients 18 years and older with a BMI >25 by SVI
Source: Epic SVI 2020 overall
(zip
Table 1.2: Percent of patients 18 years and older with a BMI≥25 by race
Source: Epic
Table 1.3: Percent of patients 18 years and older with a BMI ≥25 by ethnicity Source: Epic
Table 1.4: Percent of patients 18 years and older with a BMI ≥25 by preferred language Source: Epic
Breast Cancer screening
Breast cancer screening was defined as a patient having a breast cancer screening or mammography marked as completed from January 1, 2023 to December 31, 2024 for all women that had an encounter with Catholic Health in 2024.
Table 2.1: Percent of patients 40– 75 years with a Breast Cancer screening by SVI Source: Epic
Table 2.2: Percent of patients 40 – 75 years with a Breast Cancer screening by race Source: Epic
Table 2.3: Percent of patients 40 – 75 years with a Breast Cancer screening by ethnicity Source: Epic
Table 2.4: Percent of patients 40 – 75 years with a Breast Cancer screening by preferred language Source: Epic
Primary Care Physician (PCP)
Having a PCP was defined as having a health care provider documented in the electronic health record during 2024.
Table 3.1: Percent of patients 18 years and older with a PCP by SVI Source: Epic
Table 3.2: Percent of patients 18 years and older with a PCP by race Source: Epic
Table 3.3: Percent of patients 18 years and older with a PCP by ethnicity Source: Epic
Table 3.4: Percent of patients 18 years and older with a PCP by preferred language Source: Epic
Flu vaccine
Influenza vaccination was defined as all patients who received an influenza vaccination from August 1, 2024 to July 31, 2025. Influenza vaccination was defined through self-reported vaccination outside of Catholic Health and documentation of influenza vaccination administered in the electronic health record. Patients who were contraindicated for the flu vaccine were excluded. Contraindication was defined as hypersensitivity to eggs/thimerosal, had a prior negative reaction to a vaccination, had a bone marrow transplant within the last six months and had a history of Guillain-Barre syndrome. Patients who refused to receive a flu vaccination and did not receive a vaccination at another encounter were excluded.
Table 4.1: Percent of patients 60 years and older with an influenza vaccination by SVI Source: Epic
Table 4.2: Percent of patients 60 years and older with an influenza
Table 4.3: Percent of patients 60 years and older with an influenza vaccination by ethnicity Source: Epic
Table 4.4: Percent of patients 60 years and older with an influenza vaccination by preferred language Source: Epic
Annual Wellness Visit (AWV) or Physical Examination
Annual Wellness Visit or physical examination was measured by ICD codes related to an AWV or physical examination documented as visit diagnosis, billing diagnosis or on the patient’s problem list during 2024. If a patient had an ICD code documented during 2024, they were marked as “yes” having an AWV or physical exam during the 2024 year.
Table 5.1: Percent of patients 18 years and older with an annual wellness visit or physical exam by SVI Source: Epic SVI
(zip code) Low
St.
Table 5.2: Percent of patients 18 years and older with an annual wellness visit or physical exam by race Source: Epic OMB Race White Black or African American Asian
Table 5.3: Percent of patients 18 years and older with an annual wellness visit or physical exam by ethnicity Source: Epic
5.4:
St. Francis Hospital & Heart Center Health Equity Strategic Plan
The following data were obtained from Epic and includes all patients who had an encounter with St. Francis Hospital & Heart Center from January 1 to December 31, 2024. Patients are only included in the sample once, even if they had more than one encounter with Catholic Health. Patients who died during or prior to 2024 were excluded from the sample.
SFH System All Pts
St. Francis Hospital and Heart Center’s Patient Population Overview
Patient race Figure 3.1.1: Patient race for all patients 18 years and older who had an encounter in 2024 (N=142,834). Source: Epic
Preferred language Figure 3.3.1: Preferred language for all patients 18 years and older who had an encounter in 2024 (N=142,834). Source: Epic
Ethnicity Figure 3.2.1: Patient ethnicity for all patients 18 years and older who had an encounter in 2024 (N=142,834). Source: Epic
SFH System Hosp Admiss
St. Francis Hospital & Heart Center’s Hospital Admissions Patient
Patient race Figure 3.1.2: Patient race for all patients 18 years and older who had a hospital admission in 2024 (N=20,757). Source: Epic
Population Overview
Ethnicity Figure 3.2.2: Patient ethnicity for all patients 18 years and older who had a hospital admission in 2024 (N=20,757). Source: Epic
Preferred language Figure 3.3.2: Preferred language for all patients 18 years and older who had a hospital admission in 2024 (N=20,757). Source: Epic
SFH System ED
St. Francis Hospital & Heart Center’s Emergency Department Patient Population Overview
Patient race Figure 3.1.3: Patient race for all patients 18 years and older who had an emergency department encounter in 2024 (N=35,122). Source: Epic
Ethnicity Figure 3.2.3: Patient ethnicity for all patients 18 years and older who had an emergency department encounter in 2024 (N=35,122). Source: Epic
Some
Preferred language Figure 3.3.3: Preferred language for all patients 18 years and older who had an emergency department encounter in 2024 (N=35,122). Source: Epic
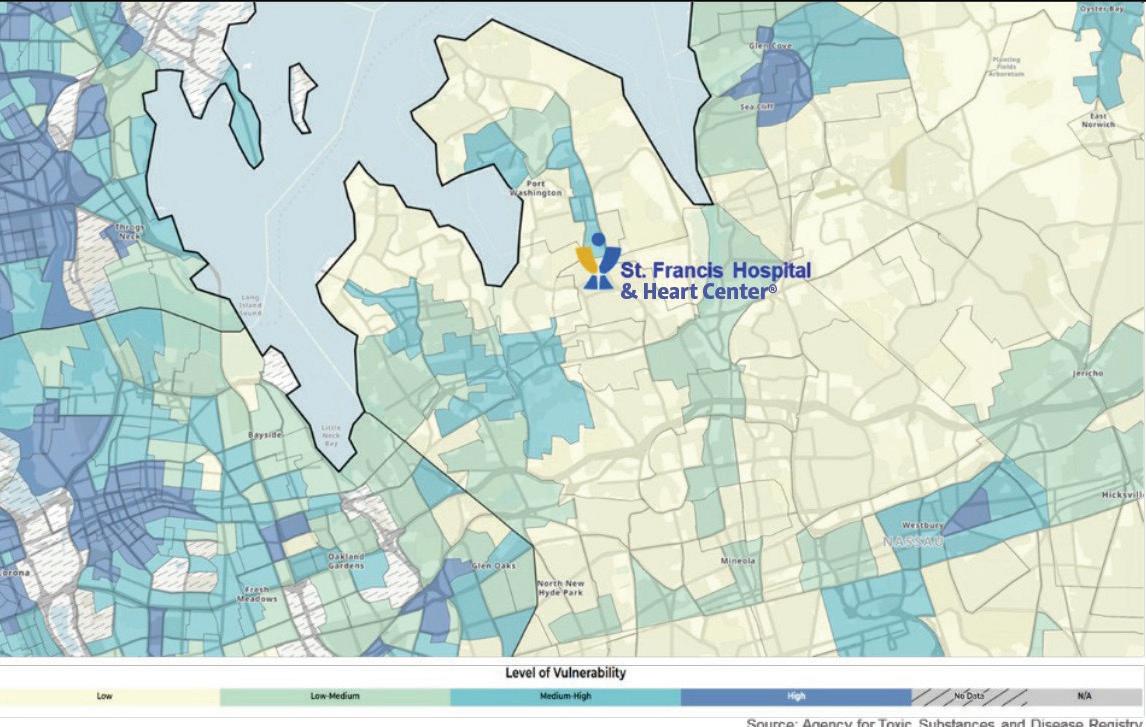
Social Vulnerability Index by Census Tract for St. Francis Hospital & Heart Center Service Areas
Figure 4.0: SVI by Census Tract for St. Francis Hospital & Heart Center service areas.
Source: Epic
St. Francis Hospital & Heart Center Identified Health Disparities
All disparities have been measured using Chi-square tests for statistical significance. All analyses were statistically significant. All data were obtained through Epic and include all patients with any encounter at St. Francis Hospital & Heart Center from January 1 to December 31, 2024. Patients who died during or prior to 2024 were excluded from the sample. Age was calculated based upon each patients’ date of birth. For the influenza vaccination measure, the time period followed the ’24 – ’24 flu season (August 1, 2024 –July 31, 2025).
Race and ethnicity follow the Office of Management and Budget (OMB) federal race and ethnicity standard classifications.
Body Mass Index (BMI)
These are standard definitions provided by OMB to promote uniformity and comparability for race and ethnicity data. These categories are used in the decennial census, household surveys, administrative forms and medical/public health research. Preferred language was categorized as English, Spanish or other languages from the patient’s last stored value during 2024. Language data were disaggregated by our top two languages to facilitate visualization and statistical analyses. Stratification by preferred language does not include changes in self-reported preferred language.
Table 6.1.1: Percent of patients 18 years and older with an annual wellness visit or physical exam by SVI Source: Epic SVI 2020 overall
Table 6.1.2: Percent of patients 18 years and older with a BMI ≥25 by race Source: Epic
Table 6.1.3: Percent of patients 18 years and older with a BMI ≥25 by ethnicity Source: Epic
Table 6.1.4: Percent of patients 18 years and older with a BMI ≥25 by preferred language
Source: Epic
Breast Cancer screening
Breast cancer screening was defined as a patient having a breast cancer screening or mammography marked as completed from January 1, 2023 to December 31, 2024 for all women for all encounters in 2024.
Table 6.2.1: Percent of patients 40 – 75 years with a Breast Cancer screening by SVI Source: Epic SVI
Table 6.2.2: Percent of patients 40 – 75 years with a Breast Cancer screening by race Source: Epic
Table 6.2.3: Percent of patients 40 – 75 years with a Breast Cancer screening by ethnicity Source: Epic OMB Ethnicity Not
Table 6.2.4: Percent of patients 40 – 75 years with a Breast Cancer screening by language Source: Epic Language English
Primary Care Physician (PCP)
Having a PCP was defined as having a health care provided documented in the electronic health record during 2024.
Table 6.3.1: Percent of patients 18 years and older with a PCP by SVI Source: Epic
SVI overall percentile (zip code) Low vulnerability
Table 6.3.2: Percent of patients 18 years and older with a PCP by race Source: Epic
Table 6.3.3: Percent of patients 18 years and older with a PCP by ethnicity Source: Epic
Table 6.3.4: Percent of patients 18 years and older with a PCP by preferred language Source: Epic
Flu vaccine
Influenza vaccination was defined as all patients who received an influenza vaccination from August 1, 2024 to July 31, 2025. Influenza vaccination was defined through self-reported vaccination outside of Catholic Health and documentation of influenza vaccination administered in the electronic health record. Patients who were contraindicated for the flu vaccine were excluded. Contraindication was defined as hypersensitivity to eggs/thimerosal, had a prior negative reaction to a vaccination, had a bone marrow transplant within the last six months and had a history of Guillain-Barre syndrome. Patients who refused to receive a flu vaccination and did not receive a vaccination at another encounter were excluded.
Table 6.4.1: Percent of patients 60 years and older with an influenza vaccination by SVI Source: Epic
Table 6.4.2: Percent of patients 60 years and older with an influenza vaccination by race Source: Epic
Table 6.4.3: Percent of patients 60 years and older with an influenza vaccination by ethnicity Source: Epic
Table 6.4.4: Percent of patients 60 years and older with an influenza vaccination by preferred language Source: Epic
Language English
Annual Wellness Visit (AWV) or Physical Examination
Annual Wellness Visit or physical examination was measured by ICD codes related to an AWV or physical examination documented as visit diagnosis, billing diagnosis or on the patient’s problem list during 2024. If a patient had an ICD code documented during 2024, they were marked as “yes” having an AWV or physical exam during the 2024 year.
Table 6.5.1: Percent of patients 18 years and older with an annual wellness visit or physical exam by SVI Source: Epic SVI overall percentile (zip code) Low vulnerability
Table 6.5.2: Percent of patients 18 years and older with an annual wellness visit or physical exam by race Source: Epic
with AWV/ physical exam with AWV/ physical exam
Table 6.5.3: Percent of patients 18 years and older with an annual wellness visit or physical exam by ethnicity Source: Epic
OMB Ethnicity Not Hispanic/Latino Hispanic/Latino No answer/unknown
Measures % patients with AWV/ physical exam # patients with AWV/ physical exam
Table 6.5.4: Percent of patients 18 years and older with an annual wellness visit or physical exam by preferred language Source: Epic
Language English Spanish Other languages
Measures % patients with AWV/ physical exam # patients with AWV/ physical exam
# patients
patients with AWV/ physical exam # patients with AWV/ physical exam
patients with AWV/ physical exam # patients with AWV/ physical exam
Market-specific Priority Population Equity Action Plan for St. Francis Hospital & Heart Center
Below, please find the health disparities the hospital will focus on improving, including the discreet action steps that will be tracked to close the identified gap.
Health disparity: Flu vaccine
Identified Intervention
• Increase influenza vaccination pods in communities with high SVI.
Owner
• Quality and Performance Improvement
Key stakeholders
• Executive Leadership
• Community Health and Outreach Program
• Community Partners
• Pharmacy Department
• Community Advisory Board
• Patient Family Advisory Council
• Employee Health
Key milestones
• Identify communities with high SVI.
• Strategize with community partners to establish influenza vaccination calendar of events.
• MyChart reminders of vaccination status.
Timeline to completion
• End of NYS Flu Season
Resources
• Epic reporting
• Marketing
• Pharmacy
• Education
• Outreach Bus
Measures of success
• Additional influenza vaccination pods scheduled in communities identified with high SVI.
Health disparity: Primary Care Physician (PCP)
Identified Intervention
• Identify a PCP for all patients.
Owner
• Quality and Performance Improvement
Key stakeholders
• Executive Leadership
• Patient Access
• Care Management/Social Work
• Nursing
• Transitions of Care Program
• Catholic Health Physician Partners
• Community Outreach Program
• Community Advisory Board
• Patient Family Advisory Council
Key milestones
• Staff education on PCP referral process and electronic health record documentation.
• Community Health and Outreach events.
• MyChart reminders of upcoming appointments.
Timeline to completion
• Rolling
Resources
• Epic reporting
• Compass Rose
• Find-a-Doctor referral
• Catholic Health Physician Partners
• Catholic Health Central Referral
Measures of success
• Increase in number of patients assigned to a PCP.
Health disparity: Annual Wellness Visit (AWV) or physical examination
Identified Intervention
• Increase in number of patients with annual physical exam.
Owner
• Quality and Performance Improvement
Key stakeholders
• Executive Leadership
• Patient Access
• Care Management/Social Work
• Nursing
• Transitions of Care Program
• Catholic Health Physician Partners
• Community Outreach Program
• Community Advisory Board
• Patient Family Advisory Council
Key milestones
• Staff education on PCP referral process and electronic health record documentation.
• Community Health and Outreach events.
• MyChart reminders of upcoming appointments.
Timeline to completion
• Rolling
Resources
• Epic reporting
• Compass Rose
• Find-a-Doctor referral
• Catholic Health Physician Partners
• Catholic Health Central Referral
Measures of success
• Increase in number of patients with documented annual physical exam.
Acknowledgments
A special thanks to co-authors
• Lawrence Eisenstein, MD, MPH, FACP VP, Community and Public Health
• Gabriella Pandolfelli, PhD, MPH Director, Epidemiology and Public Health Analytics
Thank you to key contributors
• John Abalajon, RN, MS Systems Analyst, Population Health
• Monique Ford, MBA, CPXP VP, Human Experience
• Christine Hendriks, MA, MFA VP, Community Outreach
• Donna Mari Director, Brand & Advertising
• Emily Heath Marketing Manager, System Initiatives & Service Lines
• Randi Mednick, MHA VP, Strategic Planning
• Lisa Santeramo VP, Government Relations and Regulatory Affairs
• Annmarie Smith, EdD Director, Organizational Learning and Innovation
• Dilys Whyte, MD Pediatric Nephrology, Good Samaritan University Hospital
• Paul Stuart, MBA VP, Human Resources
• Jason Tagliarino, RN, MBA AVP, Population Health Systems
St. Franics Hospital & Heart Center Equity Leads
• Ingrid Collymore, MSN, RN, CCM Manager, Quality & Performance Improvement, St. Francis Hospital & Heart Center
• Laurie Nolan-Kelley, DNP, RN VP, Quality and Performance Improvement, St. Francis Hospital & Heart Center
Health Equity Leadership Council Committee Chairs
• Catholic Health First: Paul Stuart, MBA VP, Human Resources
• Long Live Long Island: Lisa Santeramo VP, Government Relations and Regulatory Affairs
• Education: Annmarie Smith, EdD Director, Organizational Learning and Innovation Dilys Whyte, MD
Pediatric Nephrology, Good Samaritan University Hospital
• Quality and Data: Monique Ford, MBA, CPXP VP, Human Experience
Jason Tagliarino, RN, MBA AVP, Population Health and Enterprise Analytics
Catholic Health Quality and Regulatory team leaders
• Monique Ford, MBA, CPXP VP, Human Experience
• Chhavi Katyal, MD, MBA, MS SVP, System Chief Quality Officer
• Anna ten Napel, PhD, RN, NP VP, Regulatory Affairs and Performance Improvement
100 Port Washington Boulevard Roslyn, NY 11576
Follow Catholic Health!