There is no completed, up-to-date business plan in place that sets out the case for delivering the Shaping a Healthier Future (SaHF) programme, demonstrating that the programme is affordable and deliverable.
There was limited and inadequate public consultation on the SaHF proposals and those proposals themselves did not provide an accurate view of the costs and risks to the people affected.
The escalating cost of the programme does not represent value for money and is a waste of precious public resources.
NHS facilities, delivering important public healthcare services, have been closed without adequate alternative provision being put in place.
The original business case seriously underestimated the increasing size of the population in North West London and fails to address the increasing need for services.
Main Recommendations:
The SaHF programme needs to be halted.
Local authorities should consider seeking a judicial review of the decision to implement the programme if it is not halted.
Executive Summary
Section 1: Current and future healthcare needs
It is clear to the Commission, from the evidence received, that there have been significant increases in actual population and in future population projections across the North West London region since the SaHF programme’s Pre-consultation and Decision Making Business Cases were laid down in 2012 and early 2013. What is not clear, because we have not been given access to the documentation, is whether these changes have been accounted for in the current Business Case and what impact this has had on plans for the future of healthcare services in the region, especially where major new housing developments are being planned. Crucially, the SaHF proposals are not based on any robust needs assessment of the population that would give confidence in the proposed reduction in services.
Recommendation
1. The Commission recommends that the current Business Case is immediately made available for proper public scrutiny. This is the only way to ensure that the SaHF programme has taken full account of the current and projected population changes in North West London since 2012 and is soundly based on an up-to-date assessment of needs. The need for this is reinforced by the observations in the next section.
Section 2: Finance and economics
The SaHF programme is to cost the NHS £1billion to implement and the likely return on this investment is insufficient, based on the strength of the existing evidence. Although it is understood that the NHS must plan to ensure resources are used most economically, the expensive reconfiguration proposed is not the best way to make savings or to improve quality. The planned centralisation of hospital services does not appear to have been formulated on the basis of patient need. The evidence points to financial factors playing a significant, if not decisive, role in the SaHF programme’s selection of major and local hospitals, to the detriment of the more deprived communities in North West London, which are also the communities with the most acute healthcare needs. Contrary to the tacit assurances of the SaHF consultation document (e.g. pages 8, 14, 18 and elsewhere), which profess a concern to address inequalities, cutbacks are being targeted on the most deprived communities as part of a plan for additional investment in central London.
If the information collated by the consultants acting for the Commission is borne out, it reveals that the much vaunted plans to create a sustainable health economy will actually cost far more than will be saved and reduce the quality of access and the delivery of services to local people.
The Commission is most disappointed and deeply concerned at the failure of the NHS witnesses to produce the Business Case. The lack of this document leaves a gaping hole in
the evidence. Without a published Business Case there can be no meaningful external scrutiny of the SaHF programme plans. The exclusion of local government from the development of this document is also of concern.
Recommendation
2. The Commission recommends that the National Audit Office undertakes a review of the value for money of the SaHF programme.
Section 3: Public consultation
There is clearly widespread concern and continuing criticism as to the public consultation exercise conducted in 2012. Witnesses representing a range of different interests and from a variety of backgrounds – clinicians, politicians, patients and residents – have all raised similar criticisms about the process and structure of the exercise, as well as how the results have been analysed and interpreted. We have heard from a Healthwatch body how the Independent Reconfiguration Panel’s call for closer engagement with the public does not appear to be happening and yet the key NHS witness describes an extensive consultation process having occurred, with an outcome demonstrating resounding support for the programme. There is clearly a mismatch between the perception of the NHS as to how consultation has been managed and that of the many witnesses that have presented to the Commission on this issue over the four days of public hearings.
On a more fundamental point, the consultation that did take place in 2012 was on the basis of a Business Case that has now been very substantially changed, not least in the huge increase in the costs of implementing the scheme. With the plan not yet finalised, our consultants have been advised that the eventual cost is likely to be more than five times the original projection, questioning its affordability and viability. It seems from this that the case for a fresh, genuine consultation on what’s now planned as part of SaHF is essential to secure public confidence.
Recommendation
3. The Commission calls for a fresh consultation on the latest version of the Business Case (referred to as the Investment Business Case in official guidance but as the Implementation Business Case by SaHF programme leads) as the programme has changed significantly since the Pre-consultation and Decision Making Business Cases were published. There should be extensive and uniform publicity across the region and a clear consultation document with appropriate translations of the full text as well as summaries made available in areas of high concentrations of BME communities.
Section 4: A&E closures and other reconfiguration plans
The evidence presented to the Commission, regarding A&E performance on waiting times over the course of the past year and more, clearly indicates the impact that the early closures of Hammersmith and Central Middlesex A&E departments have had on waiting times at other A&E departments across the region and, in particular, on Northwick Park Hospital. The fact that performance was poor elsewhere does not escape the fact that it was worst in North West London, particularly after September 2014 when the closures took place.
The NHS witnesses’ denials, in the face of this evidence, that this is the case, is of concern to the Commission as it suggests a reluctance to accept that the modelling on expected patient movements, that was employed to inform the closure plans, was inaccurate. From the evidence heard, it is the Commission’s view that this modelling failed to take account of service failures across the various levels of healthcare provision in the region, especially GP services, that has resulted in an increasing reliance on A&E services and an inability of those services to cope with the increased demand.
The selection of hospitals on which SaHF service closure plans are focussed, i.e. Hammersmith, Central Middlesex, Ealing and Charing Cross, whether by accident or design, are in areas of comparative deprivation when looked at next to the selected major hospitals, i.e. St. Marys, Chelsea and Westminster, West Middlesex, Northwick
Park and Hillingdon. The residents that will be having to travel further for acute healthcare services are those who are most vulnerable and least able to afford travel costs. Invariably they are also the communities that exhibit the most acute healthcare needs.
The evidence heard by the Commission reveals widespread confusion among GPs, consultants and patients as to what an urgent care centre (UCC) can deliver in the way of services and who should be referred there. As a result of this confusion there is no consistency in referrals to UCCs, either self-referrals or clinical referrals. This confusion can lead to fatal consequences. The Commission concurs with the view of many expert witnesses that A&Es and UCCs, especially in London, should be colocated. In areas where this is no longer the case, i.e. the catchment for Hammersmith and Central Middlesex hospitals at present, there should be a co-ordinated and intensive education campaign to raise both public and professional awareness of which services can be provided at these UCCs, and which cannot safely be dealt with, so as to clarify what injuries or symptoms are appropriate for people to be referred or self refer to these centres. The guidance on A&E and UCCs due to be published by the Chief Medical Officer, Sir Bruce Keogh, remains outstanding amid continuing evidence of the breakdown of the existing system. This is not a stable environment for planning major change.
The Commission has been impressed by the evidence of the exemplary services provided at Ealing maternity unit. The specialist care that the unit clearly offered to a vulnerable and deprived client group has, from the
evidence of service users, immeasurable community benefits. In the view of the Commission, the costs on this community of the loss of the unit has not been adequately considered by the SaHF programme medical directors nor Ealing CCG.
Recommendations
4. In the light of these factors, and recommendations 1-3, it is imperative that there be no further implementation of SaHF in the following two principal respects:
i) The Commission demands that there must be no further closures of any A&E departments in North West London. Ealing and Charing Cross hospitals must retain full ‘blue light’ A&E services for the foreseeable future;
ii) The Commission calls for an equalities impact assessment to be carried out into the whole SaHF programme, with a particular focus on the communities that will be deprived of services at Ealing and Charing Cross hospitals, as it is clear to the Commission that the selection of these hospitals for service closures will adversely affect the more deprived BME communities in the region.
5. The Commission recommends that all UCCs in North West London should be co-located with A&E departments. Where this is no longer the case there should be an immediate and extensive
publicity campaign mounted to raise awareness as to what such centres can provide and who should refer there.
6. The Commission recommends that the decision to close Ealing maternity unit should be reversed with immediate effect.
7. The Commission recommends that the A&E department at Central Middlesex Hospital should be re-opened to alleviate the burden on other A&Es, especially Northwick Park.
Section 5: Out-of-hospital provision
The evidence suggests that out-of-hospital provision is developing in a piecemeal fashion and at a very slow pace, largely due to the lack of any fixed or detailed plans, together with the complex procurement processes that GP commissioners are having to deal with. It is not yet clear how performance will be monitored and, therefore, how decisions about closing acute services will be made. The lack of any published outline business cases or any update on progress towards the promised new provision of services makes scrutiny of the out-of-hospital strategies impossible at this point in time.
The continuing absence of any business cases is particularly worrying in this case. Without this information it has been impossible to scrutinise plans across North West London. The Commission would like to see performance monitoring both at a local and North West London level. At present it
is not clear how success will be measured and, therefore, at what point it would be considered safe to close acute provision and rely on out-of-hospital provision.
As part of evidence gathering, each CCG provided the Commission with their Out-ofHospital Strategy but these are CCG specific and there seems to be little in the way of a sub-regional strategy. There is also concern that there is little understanding of how performance of out-of-hospital services will be measured, either locally or sub-regionally, and, therefore, how they will be judged effective enough to support patients in the absence of services that are being closed as part of the SaHF reconfiguration. The success of hospital reconfiguration is dependent on a safe and reliable out-of-hospital strategy.
The evidence also reveals a developing crisis in the delivery of GP services, that are clearly failing to meet demand across the region, contributing to the crisis in A&E performance. Without adequate GP services, none of the SaHF proposals are capable of implementation.
The cuts in social care provision, imposed as a result of central government spending cuts since 2010, have compounded the problems of excess demand on the acute services, with patient discharge being affected by a lack of bedspaces in care homes and/or a lack of domiciliary care. Various witnesses have referred to significant reductions in social workers in post over recent years. This reduction in social care creates bed-blocking and a resulting logjam in patient intake.
Recommendations
8. The Commission calls for a substantial investment in GP and out-ofhospital services, which are clearly overwhelmed and inconsistent, to meet the additional demands of more vulnerable patients, and a recruitment drive for additional GPs and primary care staff.
9. The Commission calls for a sub-regional out-of-hospital strategy to be produced with clear metrics and targets setting out at what level such services will be considered sufficiently successful to allow for further reconfiguration.
10. The Commission notes that levels of spending on social care in North West London and elsewhere have been hit by ill-conceived central government policies, but recommends that social care budgets are increased and protected to maintain patient flows from hospital to domiciliary and residential care.
Section 6: Governance and scrutiny
There is a lack of transparency in the governance arrangements for the SaHF programme. There needs to be clearer accountability for decision-making across the whole programme. There has been no direct engagement of local authorities in their wider community leadership role, nor sufficient engagement with adult social care departments about the sub-regional agenda,
beyond the borough level mechanisms, despite the impact of these changes on adult social care practices.
The scrutiny role of Healthwatch bodies needs to be clarified as the organisations are, themselves, unclear as to exactly what their role is in challenging the programme.
The role of Patient Participation Groups (PPGs) might also be clarified as there appears to be some uncertainty around confidentiality issues, especially when patient representatives are involved in procurement processes.
Recommendations
11. The Commission recommends that elected local authority representatives be invited to attend SaHF Programme Board meetings to give greater public accountability and transparency.
12. The Commission recommends that NHS England issues up to date guidance to CCGs and Healthwatch England as to the exact scrutiny role of Healthwatch bodies and Patient Participation Groups in all matters of commissioning and service reconfiguration.
Postscript:
The Commission delayed publication of this report, on the promise of additional information from NHS England’s London office, but were disappointed to find that the documentation provided did not answer any of the outstanding questions raised in this report. The Commission has still not been given sight of a completed final Business Plan for a project which, according to current NHS estimates, has now ballooned in cost to £1.3 billion.
In 2012 the NHS consulted on proposals to make significant changes to the healthcare economy of North West London, set out under the heading “Shaping a Healthier Future”. This involved the downgrading of several hospitals across North West London to “local” hospitals without A&E provision, closure of acute provision and reduction or downgrading of specific services. It also promised commitments to investment in capacity of out-of-hospital, GP and community services in order to offset reductions in acute provision.
Two years into the implementation of “Shaping a Healthier Future”, Brent, Ealing, Hammersmith & Fulham and Hounslow Councils (later joined by Harrow Council) set up an independent commission of inquiry to review the programme, in particular: the impact of reductions to acute provision on the North West London population; the extent of progress with investment in capacity and capability of community and out-of-hospital services to meet local needs, and; the extent to which demand for acute services has changed as a result of those investments. The Independent Healthcare Commission for North West London was launched on 1st December 2014.
The Commission’s brief
The Commission’s terms of reference were agreed at its first meeting on 10 January 2015. It was recognised that, given the speed with which widespread far reaching Government proposals were being implemented, there was a clear and urgent requirement to focus and identify basic principles. Within these
it was imperative to prioritise those areas of significance where change was either underway or imminent.
First principles of analysis entail the identification of the constituents of healthcare which are then developed on a firm evidence base.
The specific terms of reference set for the Commission were to identify:
1. The nature of each of the boroughs with particular regard to the citizens who form the contemporary patient constituency;
2. The current principal medical needs of this community;
3. The means by which these needs are presently being met;
4. Whether these are the best attainable means;
5. What resources are required to sustain the best attainable means;
6. The extent to which the government’s 2012 plan,
(a) in inception,
(b) subsequent implementation, and (c) intended development in 2015,satisfies the ‘best attainable means’ test.
Drinkell assured us that those clinicians had been made well aware of the Commission’s existence and SOH had tried to get them to submit evidence but that “there is a real culture of nervousness about getting involved.”
We are told, by the CCGs, that the SaHF programme is clinically-led and has the support and backing of health professionals but the evidence for that is in very short supply. What we would like to see is an open but anonymous survey of all health professionals across the region to gauge the true perceptions of those who work most closely with patients.
National context: impact of the Health and Social Care Act 2012
Professor Allyson Pollock, from Queen Mary University of London, in her evidence to the Commission, defined two key aspects of the Health and Social Care Act 2012 that she believes are integral to the changes that are taking place in the NHS today: firstly, the abolition of the duty on the Secretary of State to provide listed services throughout England and, secondly, the entrenching of contracting.
CCGs have been left with a duty to promote health services but there is no longer a duty to provide those services, as there had been a duty incumbent on the Secretary of State and area based health services since 1948. That duty has now been totally abolished by the 2012 Act. As Professor Pollock stated in her evidence:
“There is no duty to provide. They (CCGs) have a duty to arrange, which is contracting those services, and an overarching framework duty of a duty to promote.”
Further evidence, provided by the Commission’s consultants, identified dysfunctional relationships between the intermediate bodies newly created and ineffective tendering arrangements. Our conclusion is that the system newly created is wrong in principle and not working in practice, yet somehow it is no one’s responsibility to put the problems right.
Consultants’ interim report
At the beginning of the process we commissioned consultants to review the existing evidence, including all available documents pertaining to SaHF, and to interview key decision-makers and members of the SaHF Programme Board and then to report to us on their findings. This they did in March 2015 and both the summary and full report are published online at www. lbhf.gov.uk/healthcarecommission. This report provided a basis of evidence for us in constructing questions for the witness sessions.
Oral evidence hearings
We conducted four full day hearings, held in public, at four town halls across the region. Invited to give oral evidence at those hearings were local politicians, the Royal Colleges and other national bodies, the clinical commissioning groups, NHS trusts, independent experts, clinicians, other health professionals, patients, service users and local residents.
In March we heard from 16 witnesses at Hammersmith Town Hall, 14 witnesses at Ealing and 10 witnesses at Hounslow Civic Centre and, at the final hearing in May, we heard from another 16 witnesses in Brent. Those 56 witnesses included two MPs, 12 local councillors, three Royal Colleges, 10 clinicians, 20 patients/service users but only three CCG representatives and only one NHS trust representative. The lack of NHS engagement with the Commission has been a grave disappointment.
The chairs of the eight CCGs, the chief executives of the four NHS trusts and the chief officer of the SaHF programme were all invited to give oral evidence to the Commission at any of the four hearings but only four of those 13 key witnesses attended a hearing. The Commission got the distinct impression that there is a siege mentality developing across the North West London CCGs.
The proximity of the public hearings to the general election may explain the refusal of the NHS representatives to give evidence at any of the three March hearings and it may also explain the recruitment of a media consultant to act as an intermediary in all communications between the Commission and all NHS bodies from February onwards. What it does not explain, however, is why only a third of the NHS representatives, invited to give evidence at the hearings, were able to attend the final hearing on 9 May, which was post-election.
Full trancripts of the four evidence hearings, along with video recordings of the witnesses giving their evidence, can be found via the following link: www.lbhf.gov.uk/ healthcarecommission. Also published there is correspondence between the Commission and the NHS.
Section
1.1 The SaHF programme was drawn up using retrospective figures on population and demographic changes, three years ago, at a time of considerable population growth in London and England as a whole. Subsequently a number of decisions have been taken on new housing developments, changing the reality substantially – yet with no sight of the draft Business Case we have no evidence that these changes have been taken on board and service provision tailored to population needs. Concerns that the SaHF programme is out of touch with demographics are underlined by the haste to close the maternity services at Ealing Hospital.
“The evidence behind assumed reductions in demand for acute capacity that would allow the closure of sites and replacement by less capacity on the remaining sites is deeply flawed, failing as it does to take proper account of population growth, increased acuity of illness within that population, and being dependent on ill-founded assumptions about the impact out-ofhospital services would have on acute demand…”
Consultants’ interim report
Population estimates and future projections
1.2 London generally and West London in particular has increased its population since the mid eighties (London from 6.5 million to 8.5 million) and this increase is projected to continue. What has not happened is a commensurate increase in resources to match this increase in demand.
1.3 Evidence from Brent, Ealing and Hammersmith and Fulham Councils reveal a number of planned housing developments that will substantially increase local population figures in those boroughs. The largest known development is planned for Old Oak Common, which both Brent and Hammersmith and Fulham Council have confirmed in written and oral evidence as estimated at 24,000 additional homes, a likely population increase of at least 70,000 people. The Hammersmith and Fulham Council Leader, Cllr Stephen Cowan, also highlighted a planned development in Earls Court that is likely to add a further 10,000 to the population of the area and further developments that may arise from the sinking of the A4 flyover in Hammersmith. Both Brent and H&F council leaders are clear that these developments have not been taken into account by the SaHF plans, as they were not known about in 2012.
1.4 Professor Ursula Gallagher, Director of Quality and Patient Safety for Brent, Harrow and Hillingdon CCGs,
in her evidence to the Commission, accepted that 24,000 new homes at Old Oak Common would have a major impact on the SaHF programme plans. Professor Gallagher stated that the SaHF programme is “quite a long term programme and, therefore, it needs to be constantly refreshed as new information, both about clinical evidence and population, comes on stream which could include population growth linked to developments”. She was unsure, however, whether the current draft Business Case has taken account of the latest data on new developments and population projections.
1.5 The Leader of Ealing Council, Cllr Julian Bell, highlighted the apparent existence of a ‘shadow’ population in Ealing, where the Office for National Statistics (ONS) estimates the population at 350,000 but 405,000 people are registered with GPs. The Chair of Ealing CCG, Dr Mohini Parmar, in her evidence to the Commission, acknowledged the discrepancy between the ONS population data and the numbers appearing on the GP registered list in Ealing.
1.6 Cllr Bell noted that the population projection to 2031 in Ealing is an increase of 9% in total population but an increase of 30% in over 65s. He also alerted the Commission to the plans for 4000 new homes in the Southall Gasworks development alone over the next 15 years. The Leader of Hounslow
Council, Cllr Steve Curran, also made reference to “a huge population increase” in Hounslow.
1.7 Tomas Rosenbaum, a consultant urologist at Ealing Hospital, gave further evidence of an apparent underestimation of the population size that is receiving services from Ealing Hospital. Mr Rosenbaum gave evidence of a large peripatetic population in the Southall area that does not appear to have been counted in official population figures.
1.8 Dr Onkar Sahota, Chair of the GLA Health Committee, London Assembly Member for Ealing and Hillingdon and an Ealing GP, with practices in Hanwell and Southall, came to the Commission with a valuable range of both regional and local experience and expertise. On the issue of population projections and healthcare provision in London, Dr Sahota stated:
“I think that the premise that these calculations are based upon may be inaccurate. We were all surprised at how rapidly the population of London is increasing. By 2025 the population of London will be nine million. By 2035 the population of London will be ten million. London is a city growing very rapidly. We are being stretched in terms of our education system, public transport and hospitals.”
Section
Changing health needs and deprived communities
1.9 Jonathan Ramsey, of the Royal College of Surgeons, highlighted the “increased demand for level 2 and level 3 care… also known as high dependency HDU and intensive care”. His explanation for this was the combination of an ageing population and improved surgical techniques meaning more operations are being performed.
1.10 Dr Onkar Sahota stated:
“I think that patients are getting much more ill, they have more specific needs, and what we need to do is a huge investment in primary care in community services if you ever want to think about closing your hospitals down. On the current model it does not operate at all and you would not be delivering care to the patients.”
1.11 Tomas Rosenbaum highlighted the “much higher than average level of cardio-vascular disease and of certain infectious diseases and of metabolic syndrome” of Southall residents using Ealing Hospital.
1.12 The Leader of Brent Council, Cllr Muhammed Butt, referred to Stonebridge, Harlesden and Kensall Green as some of the most economically deprived areas of the borough with, also, some of the most acute healthcare needs. Both Cllr Butt and Cllr Krupesh Hirani, Brent Council’s
Cabinet Member for Adults, Health and Wellbeing, criticised the closures of Central Middlesex and Hammersmith Hospital A&E departments as having forced deprived communities with greater healthcare needs to travel longer distances to access A&E services at Northwick Park Hospital.
Conclusion
1.13 It is clear to the Commission, from the evidence received, that there have been significant increases in actual population and in future population projections across the North West London region since the SaHF programme’s Pre-consultation and Decision Making Business Cases were laid down in 2012 and early 2013. What is not clear, because we have not been given access to the documentation, is whether these changes have been accounted for in the Business Case and what impact this has had on plans for the future of healthcare services in the region, especially where major new housing developments are being planned. Crucially, the SaHF proposals are not based on any robust needs assessment of the population that would give confidence in the proposed reduction in services.
Recommendation 1:
The Commission recommends that the current Business Case is immediately made available for proper public scrutiny. This is the only way to ensure
that the SaHF programme has taken full account of the current and projected population changes in North West London since 2012 and is soundly based on an up-to-date assessment of needs. The need for this is reinforced by the observations in the next section.
2.1 SaHF originated in plans led by NHS London, drawn up by McKinsey. Primary Care Trusts (PCTs) in London were grouped into five “clusters” (North West, North Central, North East, South East and South West) with orders to find ways to meet the expected financial pressures on health economies of the 2008-9 banking crash and the likely freeze on spending from 2010, after the ten years of above inflation increases in NHS budgets had come to an end. NHS London declared that the capital’s PCTs were expected to deliver savings of £5 billion – and North West London represents 24% of London’s health budget. The projections of the “cash gap” these savings were designed to bridge, now appear to have been inaccurate as budgets have been more or less balanced up to 2015.
2.2 The SaHF programme was always intended to be a cost-saving plan. However, it has now gone from a plan aiming to generate £1 billion of savings to one requiring £1 billion of capital investment – only a small proportion of which could be generated from sales of land assets from the closure of services at Ealing and Charing Cross hospitals. This questions the extent to which the proposals have ever been genuinely “clinically-led,” rather than attempts by a minority of clinicians, engaged in PCTs and later CCGs (along with McKinsey and other management consultants), to cope with financial problems.
2.3 Various documents from NHS North West London (the cluster of PCTs prior to the creation of CCGs) confirm that the North West London target for “efficiency savings”, to meet rising pressures on health services with near zero real terms increases in NHS budgets, was £1 billion over five years (compared with a budget of £3.4bn)1. The savings were to come from reductions in staff, closed beds and in hospital care (tacitly assuming that any alternative services would be cheaper and require fewer clinical staff). But the 2012-15 NHS North West London Commissioning Strategy Plan (Part B: page 163) also carried a table setting out the planned reduction in North West London’s NHS workforce needed to generate the required savings, with an overall planned reduction of 13.8% of staff (5,630 posts), more than 70% of these posts to be clinical.
2.4 The following table summarises the projected costs, as set out in the Preconsultation Business Case (PCBC), the Decision Making Business Case (DMBC) and the latest estimates, as reported by the Commission’s consultants.
Influence of PFI hospitals on the reconfiguration plans
2.8 Cllr Julian Bell, in his evidence to the Commission, highlighted the impact on the SaHF programme of the existence of hospitals that have been built or redeveloped with investment from a private finance initiative (PFI) arrangement. Both Central Middlesex and West Middlesex hospitals are PFI-funded hospitals but Cllr Bell’s evidence pointed to the latter as having had the greatest impact on decisions affecting Ealing Hospital. He stated that once “Ealing was twinned with West Middlesex, that…because the financial problem that West Middlesex had with its PFI was driving the whole process… it was inconceivable for West Middlesex not to be the major hospital and for Ealing to lose out and just be a local hospital.”
2.9 Mrs Judy Breens, an Ealing resident, also raised the question of what impact PFI hospitals have had on the selection of major hospitals under the reconfiguration plans. She suggested, in her oral evidence to the Ealing hearing, that Ealing and Charing Cross hospitals, being wholly owned by the hospital trusts, offer better scope and better return on land sales than those hospitals which have private investors involved.
2.10 Our consultants drew attention to the fact that Ealing Hospital is the most efficient hospital site in London (Consultants’ Interim Report, p75). Charing Cross is acknowledged to hold the leading specialist stroke unit in the country. It is paradoxical that the most efficient site and most successful service are both to be more or less closed so that new PFI hospitals can be constructed in central London.
Costs of reorganisation and devolved commissioning
2.11 Dr Onkar Sahota, in his evidence to the Commission, was highly critical of the financial aspects of the NHS reorganisation programme arising from the coalition government’s Health & Social Care Act. He stated that:
“We certainly do not think that spending £3 billion for a top-down reorganisation that no one wanted and no one needed has helped the NHS at all.”
2.12 In a criticism of devolved commissioning arrangements he stated:
“We have got GPs now, and I speak as a GP, sitting across the various CCGs looking at contractual arrangements, they have been taken out of consulting rooms, they are sitting now in CCGs and do you know these poor doctors are so busy with their day job looking after patient care.”
2.13 Dr Sahota referred to a query raised by Stephen Dorrell, Chair of the Parliamentary Select Committee on Health, as to the transactional costs of the NHS, i.e. monitoring and setting up contracts, and stated:
“The answer is about 10-11% of the NHS budget is spent on negotiating contracts, monitoring contracts, seeing whether the contracts are being put out. Local GPs in Ealing had to set up a federation because the local CCG is required to tender out contracts…they waste their time.”
2.14 As well as GP commissioning taking up a lot of time that might otherwise be spent in clinical practice, the Commission also heard evidence with regard to the experience and expertise of CCG commissioning boards. Phillip Brownley Eldridge is a resident of Isleworth and was a patient representative on the Hounslow CCG. In this role he was invited to participate in a number of procurement panels, including co-commissioning panels with other CCGs. In his evidence to the Commission he was highly critical of the expertise and experience of the CCG panel members in procurement and tendering, giving examples of panels being unfamiliar with TUPE regulations and of failing to examine the past performance of bidding organisations.
2.15 Peter Latham, Chair of Willesden Patient Participation Group, gave evidence to the Commission of a recent failed procurement exercise
for out-of-hospital musculoskeletal and gynaecology services in Brent. Mr Latham’s evidence, reciting information provided to him by the senior responsible officer, revealed two main reasons why Brent CCG discontinued the Wave 2 musculoskeletal and gynaecology procurement halfway through the bidding process:
“The Mott MacDonald impact assessment was that, of the £9 million for those groups of outpatient consultants, about £4 million was still going to have to go to the secondary hospitals because the draft specifications for both gynaecology and musculoskeletal had a whole list of expected conditions which were going to have to go to the secondary hospital in any event”, and;
“On examining the Bedfordshire musculoskeletal project, that has been put in place contracted to Circle Healthcare, they ran into serious difficulties…because of competition with the local hospital (leading to) GPs continuing to refer to the secondary hospital (meaning that) in Bedfordshire the CCG is paying twice over”.
2.16 Robin Sharp CB, Chair of Kilburn Patient Participation Group added:
“On the whole we think it is right that the CCG has now abandoned this procurement but it is after huge expenditure of time, money and involvement of outside experts and the patient volunteers.”
2.17 These criticisms confirm the findings of our consultants (Consultants Interim Report, p84) of the difficulties the CCGs and various NHS and public bodies have had in managing this process which is now proceeding without a formal approved plan, an agreed budget or confidence that the changes designed to reduce acute demand are deliverable: a recipe for disaster.
Centralisation of hospital services
2.18 We heard a range of views on the pros and cons of centralisation of hospital services. One doctor, Dr K, who had formerly worked at Ealing Hospital and has since been studying health economics, referred to evidence from the US and elsewhere that suggests that the best number of beds that hospitals should run on is 300. She stated that:
“When you merge hospitals that is a bad idea because then you get inefficiency and it is inequitable so you have both problems running side by side.”
2.19 An alternative view was expressed by Dr Julian Redhead, Chair of the London Board of the Royal College of Emergency Medicine (RCEM) and an A&E consultant who stated that for a small proportion of the emergency hospital caseload, patients benefit from referral to more specialist hospitals, even at further distance:
“We have a very good evidence base now around services of trauma, hyperacute stroke and cardiac that you improve outcomes and save patients’ lives by ensuring that the patient gets to the correct hospital with the right backup services in the fastest possible time. The previous system of taking patients to the local or the closest hospital did not have the same benefits to patients as taking them to a hospital which has the set-up and ability to deal with the care that they require.”
2.20 However, the SAHF team has shown no evidence to prove that similar benefit can be found for the remaining 95% of emergency patients by transporting them further for care.
2.21 Professor Clara Lowy, a retired consultant physician from St Thomas’s Hospital, was clear in her evidence to the Commission that consultants’ private practice is highly influential in where hospital services are centralised, with a focus on central London and wealthier areas.
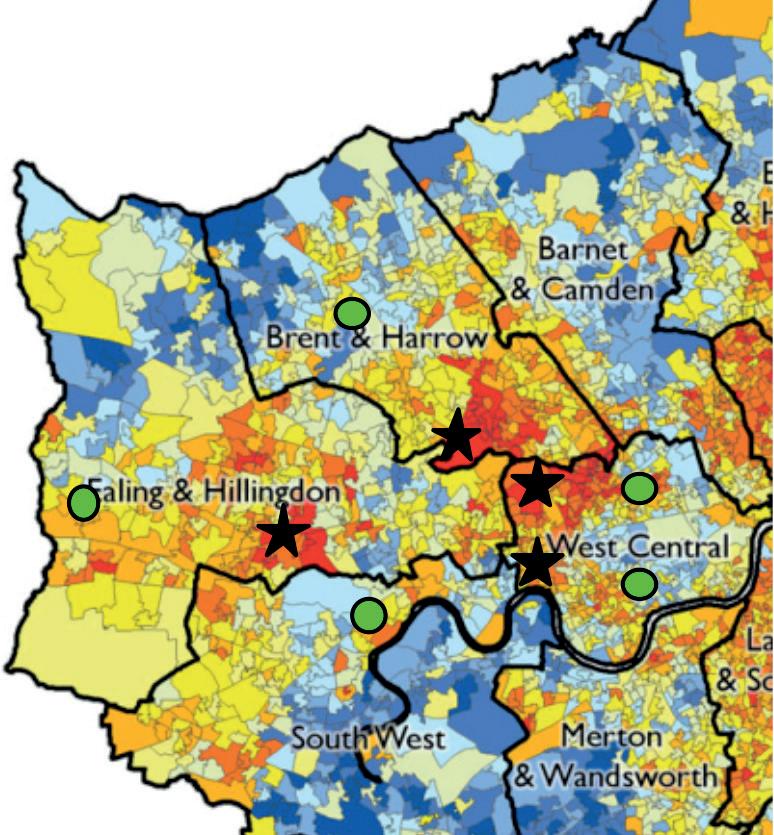
2.22 Dr Gurjinder Singh Sandhu, a consultant in infectious diseases and acute medicine at Ealing Hospital, provided the Commission with a map, previously submitted to the Independent Reconfiguration Panel, that superimposed SaHF emergency department closure plans over areas of deprivation (see over page). This clearly shows that the hospitals where service closures have occurred or are planned are located in areas of high deprivation.
2.23 Dr Sandhu stated in his oral evidence:
“The emergency departments in Southall, Harlesden and Acton are set to close whilst the emergency departments in Chelsea, Paddington and Harrow are set to stay open. As Dr K has also said earlier on, there is evidence from the US that emergency departments were closed primarily in Medicaid areas, black minority ethnic areas and areas where you needed a safety net for a core of patients.”
Level of deprivation
Hospital with A&E (prior to September 2014) Hospital without A&E
Impact of land asset sales
2.24 A number of witnesses alluded to NHS trust proposals to sell off land for development purposes where hospitals are to be downgraded, most specifically at Charing Cross and Ealing Hospitals. Cllr Mel Collins, Chair of the Joint Health Overview and Scrutiny Committee for North West London (JHOSC), in his evidence to the Commission, stated:
“The JHOSC is particularly concerned about the loss of estate to the private sector…if the estate is lost to the private sector, it will never, ever come back and we believe that the case for selling off some of the estate on the various sites across the piece has not been properly thought out and whether it is possible to work in conjunction with our social care teams to make greater use of a linking up between health and social care on the same site.”
Financing of emergency medicine
2.25 Dr Julian Redhead, Chair of the London Board of the Royal College of Emergency Medicine (RCEM), called for reform of the way in which emergency medicine is financed, arguing that the tariff system is not working:
“The way that the NHS within secondary care is funded is through a tariff system so…, in a general sense, each patient that comes to your hospital carries a sum of money with them to pay for their care which comes from the CCG. The trouble is that these tariffs were set several years ago…(and) have not changed to reflect (changes to) those services so, therefore, it is very difficult for a trust to invest money in a department which is losing money for them in terms of the tariff that they receive for it.”
2.26 Dr Redhead went on to say:
“There is also the fact that, across the whole board of acute medicine the government set a target that said you should not increase your number of admissions over a threshold that was set about four or five years ago and they basically took a 70% tax away from the hospitals and you are only paid 30% of the tariff when you go over and above those thresholds of admissions. So the whole funding is very, very tricky in order to invest in your systems of emergency medicine.”
2.27 This 30% of tariff is known as the marginal cap rate, with the 70% retained by the CCG for investment in out-of-hospital services. Tina Benson, Director of Operations at London North West Healthcare NHS Trust, suggested that this creates a “healthy tension” between hospital trusts and CCGs. Peter Latham, representing the Brent PPGs, however, suggested that this loss of revenue to hospital trusts, without a subsequent drop in attendance, must affect hospital staff morale as performance targets are missed. He also offered up evidence of possible conflicts of interest for GPs in commissioning services through CCGs and GP networks.
Cost of the SaHF programme
2.28 Colin Standfield, an Ealing resident, revealed to the Commission that, over a 10 month period in 2014, the SaHF programme had cost £13 million in consultancy fees alone. A subsequent Freedom of Information request revealed that the consultancy spend in just the past two years, from April 2013 to March 2015, has amounted to over £33 million. This is not the full picture as many millions more was spent on consultants, such as McKinsey, prior to 2013.
2.29 Dr Mark Spencer, Medical Director and clinical lead for the SaHF programme, was asked to explain some of the financial costs but declined to do so on the basis that he was not responsible for the financing of the programme. He stated that we could have invited the Finance Director to answer such questions. For the record, the Commission wishes it to be known that we invited Clare Parker, the SaHF Chief Officer and former Finance Director, to give evidence but the witnesses who attended the May hearing were selected by the NHS and Clare Parker was not put forward.
The Business Case
2.30 The Commission has expressed its concern, throughout the course of the public hearings, that the implementation of the SaHF programme has begun before the Business Case has been completed and made public. In his evidence to the Commission, Dr Mark Spencer stated that the Business Case is “in draft formation being informally discussed with the Department of Health and the Trust Development Agency”. He explained the delay in completing this as:
“Because part of the recommendations from the Secretary of State was that further discussions should happen with the local population around Hammersmith and Ealing to help define what a local hospital would be on those sites. … There have been other delays around the merger with Ealing and
Northwick Park Hospital as part of a separate process.”
2.31 Dr Spencer stated that he has seen an early draft of the Business Case. In response to counsel’s questioning, as to why the document can not be shared with the Commission, he stated that:
“It is an implementation plan designed by the CCGs but it is being shared with the Trust Development Agency and the Department of Health and they have given advice at this stage in its early development that it should not be shared.”
2.32 Dr Spencer was unable to advise the Commission as to when the overall Business Case, or the outline business cases for the out-of-hospital provision within each CCG area, would be ready and available for scrutiny.
Conclusions
2.38 The SaHF programme is to cost the NHS £1 billion to implement and the likely return on this investment is insufficient, based on the strength of the existing evidence. Although it is understood that the NHS must plan to ensure resources are used most economically, the expensive reconfiguration proposed is not the best way to make savings or to improve quality. The planned centralisation of hospital services does not appear to have been formulated on the basis of patient need. The evidence points to financial factors playing a significant, if not decisive, role in the SaHF programme’s selection of major and local hospitals, to the detriment of the more deprived communities in North West London, which are also the communities with the most acute healthcare needs. Contrary to the tacit assurances of the SaHF consultation document (e.g. pages 8, 14, 18 and elsewhere), which profess a concern to address inequalities, cutbacks are impacting on the most deprived communities as part of a plan for additional investment in central London.
2.39 The SaHF process has been driven by a misguided belief that substantial reductions in the demand for acute services are achievable and this would justify closures of hospital premises and enable large net decreases in costs. The claims for large reductions in demand for acute services are unproven at best, lack support or a clear strategy and do not justify pre-emptive closures
in the meantime. The economics of this approach are based on unreliable projections and on, what have turned out to be, massive errors in costing.
2.40 If the information collated by the consultants acting for the Commission is borne out, it reveals that the much vaunted plans to create a sustainable health economy will actually cost far more than will be saved and reduce the quality of access and the delivery of services to local people.
2.41 The Commission is most disappointed and deeply concerned at the failure of the NHS witnesses to produce the Business Case. The lack of this document leaves a gaping hole in the evidence. Without a published Business Case there can be no meaningful external scrutiny of the SaHF programme plans, a point that the Joint Health Overview and Scrutiny Committee (JHOSC) has also made repeatedly to the SaHF programme team. The exclusion of local government from the development of this document is also of concern.
Recommendation 2:
The Commission recommends that the National Audit Office undertakes a review of the value for money of the SaHF programme.
3.6 She also went on to criticise the lack of ongoing engagement with the public since the initial consultation phase:
“When the proposals went to the Independent Reconfiguration Panel they said that there needed to be a shift in emphasis from telling people what was going to happen to an active engagement with the community in order to co-design the services, and that is a shift that we would like to see happening because a lot of what has been happening has really been about telling people who are already very confused.”
3.7 The Joint Health Overview and Scrutiny Committee (JHOSC), in its written evidence to the Commission, is also critical of the level of public engagement, concluding that the numbers of people directly engaged was very low in relation to the population that would be affected by the changes. On the other hand, Dr Mark Spencer, in his evidence to the Commission, pointed to JHOSC approval of the planned consultation timetable. In response, the JHOSC submitted further evidence to the Commission which highlights its concerns with the consultation, at the time of the consultation taking place, which contradicts Dr Mark Spencer. This adds to concerns about how the SaHF programme has responded to outside comment, and the inaccuracies in information coming from the programme. Dr Spencer also referred
to public information being made available in all local GP surgeries, in libraries and town halls and he pointed to the deployment of a full-time worker seeking to engage with hard-to-reach groups “like the small Somali groups working throughout Southall and other areas.”
3.8 In his oral evidence to the Commission, Dr Spencer’s explanation as to why there is a strong and widespread perception that the consultation failed to engage people enough, focussed on the timing of the exercise:
“The timing of this whole programme has been difficult because it coincided with wider changes in the NHS that were being imposed by Government which were unpopular amongst a wide range of people. There has been a lot of campaigning to save the NHS and to stop privatisation within the NHS and people have become confused about the various processes in here. I would argue very strongly that what we are doing in North West London is exactly those two things and I would sign up to many of the petitions that have been around to save the NHS because we are exactly having a programme that does that.”
evidence to the Commission, pointed to the fact that 54.2% of respondents also wanted Ealing Hospital to be the major hospital.
3.15 Robin Sharp, Chair of Kilburn PPG, was critical of the official interpretation of the outcome of the consultation:
“The heading was just over three-fifths support option A, but when you look at the numbers that is 3,770 in support and 1,780 opposing so that is only 5,000 responses out of a population of two million. Since there was no stratified sampling, this is not a reliable way of gauging true opinion.”
Geographical variations
3.16 Fulham resident, Dede Wilson, highlighted the discrepancies in the way in which the consultation was promoted across different areas. She was very clear as to the lack of promotion in Hammersmith and Fulham, in comparison to the extensive promotion in Chelsea:
“There was no leafletting in Hammersmith and Fulham, whatsoever. The only way that people knew about it was through newspaper reports and advertising in the Fulham Chronicle. Otherwise it was not available unless you went online to Hammersmith and Fulham Council to find out there was something there and that there were going to be meetings.”
3.17 Ms Wilson provided the Commission with examples of consultation leaflets that were circulated in Chelsea and Westminster Hospital but not at Charing Cross Hospital, the inference being that the views of staff and patients at proposed major hospitals were sought far more readily than those at hospitals which were targeted for downgrading. She stated that:
“There was open electioneering in all of the favoured hospitals and this was most evident in Chelsea and Westminster. In Chelsea and Westminster, when I went in, it was not just the Trust newspapers that were there, there were actually instructions as to how to vote for Chelsea and Westminster. Not only were there instructions as to how to vote, and I went through the whole hospital into every single department, on every counter in every reception department there were these purply blue cards where people could tick a box and they could submit this.”
Conclusion
3.18 There is clearly widespread concern and continuing criticism as to the public consultation exercise conducted in 2012. Witnesses representing a range of different interests and from a variety of backgrounds – clinicians, politicians, patients and residents – have all raised similar criticisms about the process and structure of the exercise, as well as how the results have been analysed and interpreted. We have heard from Healthwatch how the Independent Reconfiguration Panel’s call for closer engagement with the public does not appear to be happening and yet the key NHS witness describes an extensive consultation process having occurred with an outcome demonstrating resounding support for the programme. There is clearly a mismatch between the perception of the NHS as to how consultation has been managed and that of the many witnesses that have presented to the Commission on this issue over the four days of public hearings.
Recommendation 4:
The Commission calls for a fresh consultation on the Business Case (referred to as the Investment Business Case in official guidance but as the Implementation Business Case by SaHF programme leads) as the programme has changed significantly since the Pre-consultation and Decision Making Business Cases were published. There should be extensive and uniform publicity across the region and a clear consultation document with appropriate translations made available in areas of high concentrations of BME communities.