Vaginal atrophy is more than a physical condition — it’s a silent disruptor of intimacy and emotional connection for many South African women and their partners (CLOSER Study, n=400)1
Restoring feminine confidence
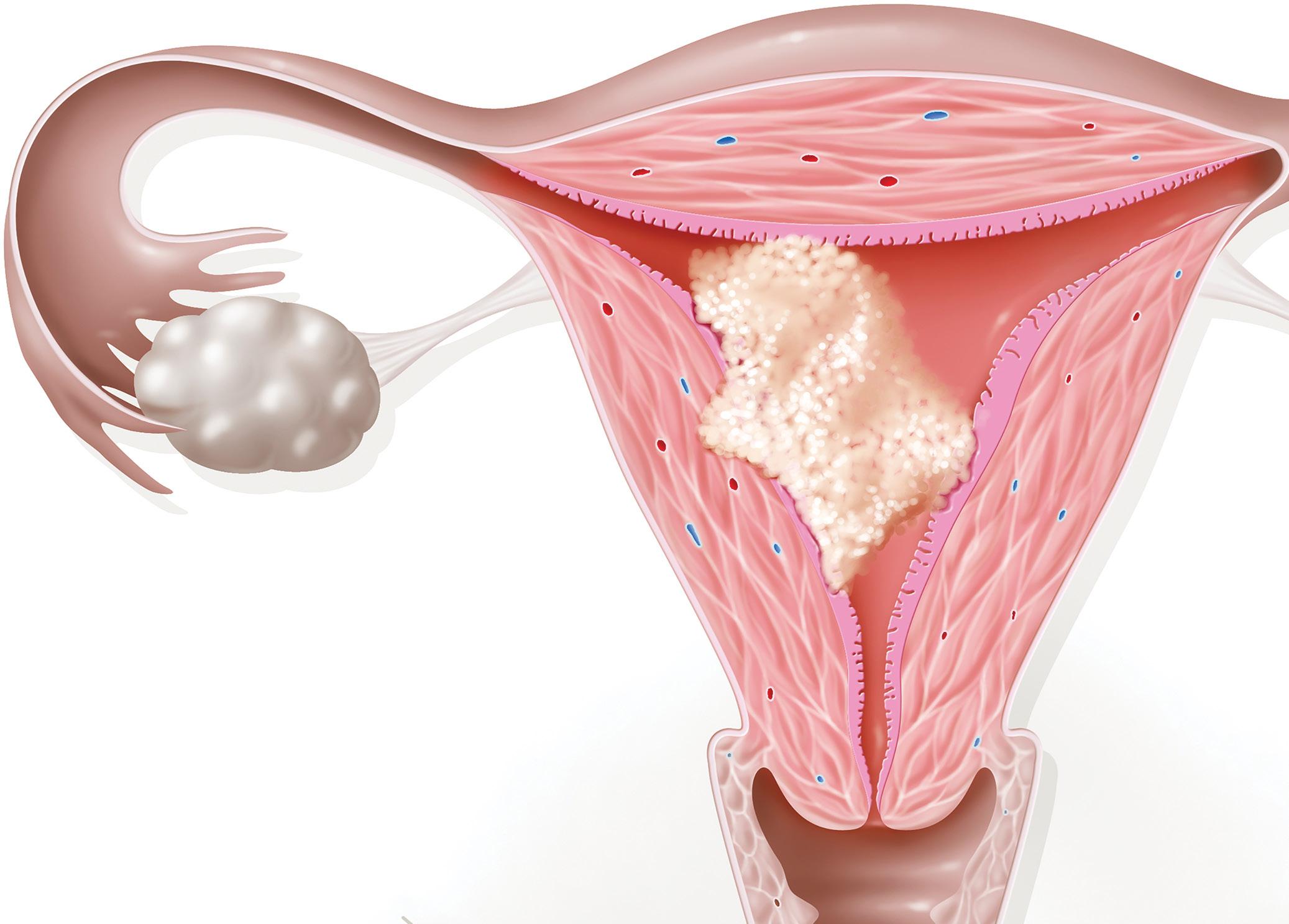
Local estrogen therapy is the first-line treatment for symptomatic vaginal atrophy, offering effective relief of symptoms such as dryness, irritation, and dyspareunia, with minimal systemic absorption and a favourable safety profile2
Restores vaginal health and relieves symptoms associated with a thin dry vaginal lining such as burning, itching and vaginal irritation3,4
Women using Vagifem® reported greater comfort, improved hygiene, and less inconvenience compared with those using estriol vaginal suppositories.5
Patients reported greater ease, comfort, and overall satisfaction with Vagifem® compared to vaginal cream formulations.6 Scan for API. For full prescribing information, refer to the professional information approved by the Medicines Regulatory Authority. References: 1.Guidozzi F, et al. Climateric. 2017. 2. Portman DJ, Gass ML. Menopause. 2014. 3. Vagifem® 10 μg vaginal tablets approved professional information, 2024. 4. Simon J, et al. Obs & Gynecol. 2008. 5. Dugal R, et. al. Acta Obstet Gynecol Scand. 2000. 6. Rioux JE, et al. Menopause. 2000.
Scheduling status: S2 Name of the medicine: Vagifem® 10 μg vaginal tablets. Qualitative and quantitative composition: One film-coated vaginal tablet contains: Estradiol hemihydrate equivalent to estradiol 10 micrograms. Reg No.: 47/21.8.1/0166. Applicant Address: Novo Nordisk (Pty) Ltd, 90 Grayston Drive, Sandown, Sandton, 2031, Gauteng, South Africa. Tel: 011 202 0500. Novo Nordisk (Pty) Ltd, 1959/000833/07. ZA25VG00019. 2025_10.
CPDs that work for real-world practice
Gynaecology Beyond hot flushes
EDITORIAL
EDITOR: René Bosman
René.Bosman@media24.com
SUB EDITOR: Gill Abrahams
LAYOUT & DESIGN: Allison McCallum
ADVERTISING
ADVERTISING EXECUTIVE
Angi Latimer | 083 999 3123
Angela.Latimer@media24.com
DISTRIBUTION & SUBSCRIPTIONS
Felicity Garbers
Felicity.Garbers@media24.com
PUBLISHING TEAM
General Manager: Dev Naidoo
Head of Content & Digital Strategy: Varushka Padayachi
Production Manager: Angela Silver
Group Art Director: David Kyslinger
MEDIA24 MEDIA
CEO: Minette Ferreira
CFO: Lana Goliath
MEDIA24 CORPORATE
CEO MEDIA24: Raj Lalbahadur
CFO MEDIA24: Nelmarie Beyers
B2B JOHANNESBURG OFFICE
Building 13, The Woodlands Office Park, 20 Woodlands Drive, Woodmead, Sandton PO Box 784698, Sandton 2146 Tel: +27 11 867 6111
Published by Media24 B2B www.medicalacademic.co.za PRINTING
Printed by Novus Print, Cape Town COVER PRICE
Specialist Forum per issue R80,00 VAT Incl. ISSN: 2218-8282
Cover photograph: Getty Images/ erhui1979
Disclaimer: Please take note that the products featured in this journal are available in South Africa. Products may be marketed under a different name or might not be registered in your country. For more information, contact your local representative. All content in Specialist Forum is sourced independently and under no circumstances should articles be considered promotional unless specified with a postscript.
Articles are created with the assistance of artificial intelligence (AI) tools to aid in research and drafting. The content has been reviewed and edited by a human expert for quality and reliability.
Please note that all advertising is intended for healthcare professionals only.
CPD season is here
Staying compliant without the panic
It is that time of year again when continuing professional development (CPD) moves firmly into the spotlight. While the Health Professions Council of South Africa (HPCSA) conducts CPD audits on an ongoing and often random basis, the early months of the year are traditionally when many practitioners pause to assess their compliance and address any gaps. With key compliance milestones such as March and June approaching, this is an opportune moment to ensure that your CPD portfolio is complete, current, and defensible.
Practitioners are individually notified if selected for a detailed portfolio audit and are required to submit their documentation within 21 days. Failure to do so may result in suspension. Increasingly, the system is moving towards continuous compliance, supported by uploads to the HPCSA online portal, reinforcing the need for year-round attention rather than lastminute catch-up.
At its core, CPD is not merely an administrative requirement. Implemented under Section 26 of the Health Professions Act, 1974 (Act No. 56 of 1974), the CPD programme is a professional obligation for every registered health practitioner. It is intended to document and track the skills, knowledge, and experiences gained both formally and informally as practitioners grow beyond their initial training. Many CPD activities are embedded in everyday professional practice, but for these to count towards continuing education units (CEUs), most must be approved prior to delivery or participation.
Following revisions to the CPD guidelines, practitioners must now meet minimum CEU requirements as stipulated by their relevant professional board, over a rolling 12-month cycle. Crucially, this includes both clinical CEUs and ethics, human rights, and health law CEUs. Even if the overall CEU total exceeds the minimum threshold, a shortfall in either component will result in non-compliance. This dual requirement has caught out many otherwise diligent practitioners.
To support you during this audit season, we have compiled a practical guide featuring our most popular CPD activities of 2025. All activities have been reaccredited for 2026, and completion of the full programme allows you to earn up to 30 general CEUs. Consider this an opportunity not only to remain compliant, but to meaningfully invest in your professional development.
Good luck
René and team
RRR IN STROKE/SE 6 HR 0.80 (95% CI, 0.73-0.89)
434 ,046 PATIENTS 6
Favourable safety with uncompromised efficacy
For ELIQUIS®(apixaban) prescribing information, scan the QR code
References:
To access the ELIQUIS® (apixaban) website, scan the QR code
The reference standard here refers to the innovator molecule. (Watson J, et al. Drugs. 2011;71(15):2079-2089). SE: Systemic embolism. RRR: Risk rate reduction. HR: Hazard ratio. CI: Confidence interval.
2. Granger CB, et al. N Engl J Med. 2011;365(11):981-92. 3. Ruff CT, et al. Lancet. 2014;383(9921):955-62.
4. Cohen AT, et al. Adv Ther. 2014;31:473-93. 5. Agnelli G, et al. N Engl J Med. 2013;369(9):799-808. 6. Lip GYH, Et al. Stroke. 2018(12):2933-2944. Erratum in: Stroke. 2020;51(2):e44. Erratum in: Stroke. 2020;51(4):e71.
This image is for representation purpose only. For the use only of a Registered Medical Practitioners or a Hospital or a Laboratory.
S4 ELIQUIS® 2,5 MG AND 5 MG FILM-COATED TABLETS (REG. NO’S: 47/8.2/0463, 0464). EACH FILM-COATED TABLET CONTAINS EITHER 2,5 MG OR 5 MG APIXABAN.
To report an adverse event, please contact ZAF.AEReporting@pfizer.com If you wish to contact Pfizer for any other purpose, please use contact details below. +2711 320 6000 or 0860 734 937 (SA). Monday-Friday 09h00-17h00.
Is twice-daily dosing
the key to unlocking optimal anticoagulation benefits?
The advent of non-vitamin K antagonist oral anticoagulants (NOACs) such as apixaban represented a pivotal advancement in stroke management among patients living with atrial fibrillation (AFib). NOACs have also been shown to be effective in the prevention and treatment of venous thromboembolism (VTE). These agents offer benefits such as no routine coagulation monitoring, minimal food interactions, and fewer drug interactions compared to vitamin K antagonists (VKAs) such as warfarin.1,2
Several landmark phase 3 trials have demonstrated the efficacy and safety of NOACs reducing the risk of stroke and mortality in patients living with AFib, as well as VTE.3,4,5,6
Granger et al conducted a randomised, double-blind study comparing apixaban (5mg twice daily) with warfarin (target international normalised ratio [INR] 2.0 to 3.0) in patients (n= 18 201) with one additional stroke risk factor.3
Over a median follow-up of 1.8 years, apixaban significantly reduced the primary outcome (ischaemic or haemorrhagic stroke or systemic embolism) compared to warfarin (1.27% vs 1.60% per
year). Apixaban also lowered major bleeding (2.13% vs 3.09% per year), and all-cause mortality (3.52% vs 3.94%) rates.3
Haemorrhagic stroke incidence was significantly lower with apixaban (0.24% vs 0.47% per year). The study authors concluded that in patients living with AFib, apixaban was superior to warfarin in preventing stroke or systemic embolism, with lower bleeding and mortality.
3
In a trial comparing rivaroxaban (20mg daily) to warfarin in patients (n= with 14 264) at risk of stroke, rivaroxaban showed noninferiority to warfarin for stroke or systemic embolism prevention, with fewer intracranial and fatal bleedings. In the per-protocol
Photo
analysis, stroke or systemic embolism rates were 1.7% with rivaroxaban versus 2.2% with warfarin, while major bleeding rates were similar.4
In another trial, dabigatran (110mg or 150mg twice daily) was compared to warfarin in patients (n=18 113) at risk of stroke. Dabigatran 110mg showed non-inferiority for stroke or systemic embolism (1.53% vs 1.69% per year for warfarin) and lower major bleeding rates (2.71% vs 3.36% per year). Dabigatran 150mg demonstrated superiority for stroke prevention (1.11% per year) and similar major bleeding rates (3.11% per year) compared to warfarin. Haemorrhagic stroke rates were significantly lower with both doses of dabigatran.5
Cohen et al conducted a study comparing the effectiveness and safety of apixaban versus warfarin in patients with VTE who were at increased risk of bleeding or recurrent VTE. Results showed that apixaban patients had a lower risk of recurrent VTE, major bleeding, and clinically relevant non-major bleeding compared to warfarin patients.6
Subgroup analyses revealed consistent findings across various patient groups at increased risk of bleeding or recurrences. Importantly, there were no significant interactions between treatment and subgroup strata on VTE, major bleeding, and clinically relevant non-major bleeding.6
Conversely, taking extra doses was linked to an increased risk of excessively high INR levels. Adhering to appropriate dosing regimens can protect patients from unfavourable outcomes, stresses Beyer-Westendorf et al 8,9
Which dosing regimen can improve patient adherence: Once- or twice-daily?
Traditionally, it was believed that reducing the frequency of dosing (eg once-daily dosing) could enhance adherence. According to Vrijens and Hedibuchel, this idea originated from concentrating solely on the number of doses taken, without considering when the doses were actually taken.9
Comparisons between once-daily and twice-daily dosing regimens reveal that despite a higher percentage of prescribed doses being taken with once-daily dosing, twice-daily dosing ensures a greater degree of continuity in drug action.9
Apixaban is superior to warfarin in terms of reduced VTE recurrence and bleeding risk
The study concluded that apixaban demonstrated superior outcomes in terms of reduced VTE recurrence and bleeding risk compared to warfarin, with consistent effects observed across different patient subgroups.6
Importance of appropriate NOAC dosing NOACs vary in pharmacokinetics and dosing regimens, depending on the indication. For instance, rivaroxaban is administered once daily for stroke prophylaxis, twice daily for acute VTE treatment, and once daily for VTE secondary prevention. In contrast, dabigatran and apixaban are consistently given twice daily, irrespective of the indication.7
Despite the effectiveness and safety of NOACs in decreasing the risk of stroke among patients living with AFib and VTE, realworld studies show that the prescribing of anticoagulant therapy frequently deviates from the dosing regimen as recommended by medical regulatory bodies, potentially diminishing the protective benefits of NOACs.6,8
Another challenge is suboptimal patient adherence to anticoagulation therapy. Patient adherence involves three key components: Initiation, implementation, and discontinuation. Initiation marks the beginning of treatment, implementation refers to following the dosing regimen as prescribed, and discontinuation signifies the end of therapy.9
A study evaluating patient adherence to warfarin revealed widespread non-adherence, with ~92% of patients having at least one missed or extra dose over a mean period of 32 weeks. Additionally, 36% missed >20% of their prescribed doses, and 4% took more than 10% extra doses.9
This poor adherence significantly impacted anticoagulation control, with missing one to two doses per week associated with up to a two-fold increased likelihood of sub-therapeutic INR values.
Furthermore, stress Vrijens and Hedibuchel, while once-daily dosing may appear to simplify dosing regimens and improve patient adherence, it requires near-perfect adherence to achieve intended pharmacodynamic and clinical outcomes. In contrast, twice-daily dosing, depending on the agent’s pharmacokinetics, is more forgiving of variations in dose timing or occasional missed doses 9
A crucial aspect to consider when prescribing an agent is that patients undergoing once-daily NOAC treatment face a greater risk of gastrointestinal (GI) bleeding compared to those on warfarin regimens. This increased risk is believed to be linked to the peak level of drug concentration, which is anticipated to be higher in once-daily regimens than in twice-daily regimens.10
According to Ido et al, opting for twice-daily dosing over oncedaily dosing could theoretically reduce the peak level of drug concentration in both the gut lumen and blood plasma. This adjustment may lead to a narrower range of drug concentration within the twice-daily regimen compared to the once-daily regimen, potentially contributing to an improved safety profile.10
To test this theory, Ido et al assessed the effect of oncedaily versus twice-daily regimens on GI bleeding in a real-world setting. This study was conducted as a single-center prospective observational registry. It enrolled adult patients (aged ≥18 years) living with AFib who were prescribed apixaban, dabigatran, rivaroxaban, and a fourth NOAC not yet approved in South Africa.10
Patients (n=2216) were categorised into two groups based on their regimen: The twice-daily regimen group (comprising dabigatran and apixaban users) and the once-daily regimen group (consisting of rivaroxaban and the as yet unapproved NOAC).10
The primary endpoint was GI bleeding, defined as any bleeding within the GI tract identified through medical records, irrespective of site or severity. Secondary endpoints included all-cause mortality, stroke, major bleeding, and any bleeding.10
Stroke was characterised by a neurological deficit persisting for at least 24 hours, attributed to acute focal injury of the central nervous system by a vascular cause. Major bleeding was defined per the International Society on Thrombosis and Haemostasis (ISTH) criteria, involving clinically evident bleeding accompanied by a decrease in haemoglobin level of at least 2g/dL, transfusion of at
least two units of packed red cells, occurrence at a critical site, or resulting in death.10
Any bleeding constituted a composite of major bleeding and clinically relevant non-major bleeding, following ISTH criteria. Clinical events were monitored through questioning, physical examination, and laboratory tests at outpatient visits conducted every two to four months. Follow-up was about two years.10
Ido et al showed that the incidence of GI bleeding was notably lower in the twice-daily regimen group compared to the once-daily regimen (3.5 per 100 person-years vs 6.2 per 100 person-years.10
Furthermore, the occurrence of major bleeding was significantly reduced in patients receiving the twice-daily regimen. However, no significant differences were observed in all-cause mortality, stroke, or any bleeding between the two regimens groups.10
In the overall study population, the risk of GI bleeding was lower in the twice-daily regimen. Importantly, the superiority of the twice-daily regimen was consistently observed across various subgroups.10
Conclusion
It seems that the conventional wisdom favouring once-daily dosing regimens for enhanced adherence may not apply to patients living with AFib undergoing treatment with NOACs.
Studies comparing NOACs suggest that twice-daily dosing offers better drug action continuity, and a more balanced risk-benefit profile with the latter, especially regarding stroke prevention, intracranial haemorrhage and GI bleeding.
Conventional wisdom favouring once-daily dosing regimens for enhanced adherence may not apply to patients living with AFib treated with NOACs
Clemens et al compared the risk-benefit balance between twiceand once-daily dosing regimens of NOACs. They conducted a rigorous, stepwise meta-analysis with predefined quality criteria for heterogeneity to derive common estimates for twice- and oncedaily dosing regimens.11
Comparing twice- and once-daily versus regimens, the hazard ratios (HR) for stroke and systemic embolism were 0.75 for dabigatran 150mg twice-daily and 0.91 for apixaban twice daily.11
For ischaemic stroke, the HR of twice- versus once-daily versus was 0.85. In terms of intracranial haemorrhage, the HR for twicedaily versus rivaroxaban once-daily was 0.57.11
The authors concluded that twice-daily dosing regimen appears to offer a more balanced risk-benefit profile concerning stroke prevention and intracranial haemorrhage.11
Once-daily dosing does not improve adherence
The key question remains: Does once-daily dosing improve patient adherence? A recent study by Hwang et al assessed the impact of once- or twice-daily dosing on adherence and clinical outcomes in patients living with AFib. The study compared adherence levels and clinical outcomes among patients (n=33 515) prescribed different NOACs with varying dosing regimens.12
High adherence was defined as a proportion of days covered of the index NOAC of 80% or higher. Clinical outcomes included stroke, acute myocardial infarction, death, and a composite outcome measure.12
The study found that 95% of patients achieved high adherence to NOAC therapy, with no significant differences observed based on dosing regimen. Across all dosing regimens, the mean proportion of days covered for NOACs was ~96%.12
Notably, adherence was highest among apixaban users, followed by rivaroxaban users, and lowest among dabigatran users, irrespective of dosing frequency. Adverse outcomes were more prevalent among patients with low adherence to NOAC therapy, regardless of the dosing regimen.12
In conclusion, while NOAC therapy has significantly advanced stroke management in AFib patients and VTE treatment, optimising dosing regimens and ensuring patient adherence remain pivotal for favorable outcomes.
The selection between once- and twicedaily dosing should carefully weigh factors like drug continuity, safety, and patient preferences, aiming to maximise therapeutic benefits while minimising risks.
References
1. Ho THQ, Ton MT, Nguyen VL, et al. Selection of Non-vitamin K Antagonist Oral. Ant icoagulant for Stroke Prevention in Atrial Fibrillation Based on Patient Profile: Perspectives from Vietnamese Experts. Part 1. European Cardiology Review, 2023.
2. Renta G, de Caterina R. The new oral anticoagulants in atrial fibrillation: Once daily or twice daily? Vascular Pharmacology, 2013.
3. Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation, NEJM, 2011.
4. Patel MR, Mahaffey KW, Garg J, et al Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. NEJM, 2011.
5. Connolly SJ, Ezekowitz MD, Yusuf S, et al Dabigatran versus warfarin in patients with atrial fibrillation. NEJM, 2019.
6. Cohen AT, Sah J, Dhamane AD, et al. Effectiveness and Safety of Apixaban vs Warfarin in Patients with Venous Thromboembolism with Risk Factors for Bleeding or for Recurrences. Adv Ther, 2023.
7. Patti G, Haas S. Non-Vitamin K Antagonist Oral Anticoagulants and Factors Influencing the Ischemic and Bleeding Risk in Elderly Patients with Atrial Fibrillation: A Review of Current Evidence. J Cardiovasc Pharmacol, 2020.
8. Beyer-Westendorf J, Fay M, Amara W. The Importance of Appropriate Dosing of Nonvitamin K Antagonist Oral Anticoagulants for Stroke Prevention in Patients with Atrial Fibrillation. TH Open, 2021.
9. Vrijens B, Heidbuchel H. Non-vitamin K antagonist oral anticoagulants: considerations on once- vs. twice-daily regimens and their potential impact on medication adherence. Europace, 2015.
10. Ido T, Sasaki S, Sotomi Y, Hirata A, et al Twice- or once-daily dosing of direct oral anticoagulants and gastrointestinal bleeding in patients with atrial fibrillation. Am Heart J Plus, 2022.
11. Clemens A, Noack H, Brueckmann M, Lip GY. Twiceor once-daily dosing of novel oral anticoagulants for stroke prevention: a fixed-effects meta-analysis with predefined heterogeneity quality criteria. PLoS One. 2014.
12. Hwang H-J, Sohn S, Jin E-S, Bae Y-J. Adherence and clinical outcomes for twice-daily versus once-daily dosing of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: Is dosing frequency important? PLoS ONE, 2023. SF
RRR IN STROKE/SE 6 HR 0.80 (95% CI, 0.73-0.89)
434 ,046 PATIENTS 6
Favourable safety with uncompromised efficacy
For ELIQUIS®(apixaban) prescribing information, scan the QR code
References:
To access the ELIQUIS® (apixaban) website, scan the QR code
The reference standard here refers to the innovator molecule. (Watson J, et al. Drugs. 2011;71(15):2079-2089). SE: Systemic embolism. RRR: Risk rate reduction. HR: Hazard ratio. CI: Confidence interval.
2. Granger CB, et al. N Engl J Med. 2011;365(11):981-92. 3. Ruff CT, et al. Lancet. 2014;383(9921):955-62.
4. Cohen AT, et al. Adv Ther. 2014;31:473-93. 5. Agnelli G, et al. N Engl J Med. 2013;369(9):799-808. 6. Lip GYH, Et al. Stroke. 2018(12):2933-2944. Erratum in: Stroke. 2020;51(2):e44. Erratum in: Stroke. 2020;51(4):e71.
This image is for representation purpose only. For the use only of a Registered Medical Practitioners or a Hospital or a Laboratory.
S4 ELIQUIS® 2,5 MG AND 5 MG FILM-COATED TABLETS (REG. NO’S: 47/8.2/0463, 0464). EACH FILM-COATED TABLET CONTAINS EITHER 2,5 MG OR 5 MG APIXABAN.
To report an adverse event, please contact ZAF.AEReporting@pfizer.com If you wish to contact Pfizer for any other purpose, please use contact details below. +2711 320 6000 or 0860 734 937 (SA). Monday-Friday 09h00-17h00.
Clots, cuts, and caution
Orthopaedic VTE
The incidence of venous thromboembolism (VTE) is ~1 per 1000 persons annually, increasing to ~5 per 1000 in individuals >80-years. VTE, which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a significant cause of morbidity and mortality in surgical patients. In the broader surgical population, DVT occurs in 15%-40% of general surgery patients, and VTE incidence can reach up to 60%. Orthopaedic surgeries, particularly total hip arthroplasty (THA) and total knee arthroplasty (TKA), are associated with a markedly increased risk of postoperative VTE due to tissue trauma, venous stasis, and hypercoagulability. Without effective prophylaxis, the risk of DVT post-THA may reach 54%, and up to 64% post-TKA. PE may occur if thrombi embolise, with potentially fatal outcomes.1,2,3,4,5
The primary goal of anticoagulant treatment is to prevent thrombus extension, embolisation, and the formation of new clots. If anticoagulant therapy is discontinued in patients with unprovoked VTE, the risk of recurrence is at least 10% within the first year and increases to 30% over five years. Recurrent DVT can result in post-thrombotic syndrome, a chronic condition marked by leg swelling, pain, and, in severe cases, venous ulcers. Alarmingly, up to 70% of hospital-acquired DVT cases are preventable.1,6
When clots conspire: Orthopaedic surgery and the perfect thrombotic storm
The pathogenesis of VTE is classically explained by Virchow’s triad, which encompasses three key factors: Vascular injury, venous stasis, and hypercoagulability. VTE risk is determined by patient demographics, comorbidities, and thromboprophylaxis strategy.2,5
Patients undergoing THA or TKA often have multiple risk factors for VTE. Key contributors include a history of prior VTE, hereditary thrombophilia, undergoing TKA rather than THA, and male sex. Inadequate prophylaxis is a concern: Only ~50% of hospitalised patients receive guideline-recommended VTE prevention.3,6
Clinical guidelines recommend primary prophylaxis – a combination of pharmacologic and mechanical interventions –as the standard approach to VTE prevention. Low-risk patients typically need no prophylaxis. Moderate-risk patients, with at
least one risk factor, benefit from pharmacologic agents such as low-molecular-weight heparin (LMWH), optionally paired with mechanical methods. High-risk patients, particularly those undergoing THA or TKA, should receive combined mechanical and pharmacologic prophylaxis.4,6
Evolution of pharmacologic DVT prophylaxis in orthopaedic surgery
Current clinical guidelines in orthopaedic surgery recommend a combination of mechanical and pharmacological strategies for VTE prophylaxis. As patients typically present to general physicians or cardiovascular specialists rather than orthopaedic surgeons, VTE may go unrecognised in the surgical context. This underscores the need for effective anticoagulation that balances thrombotic risk reduction with minimised bleeding complications.4
Traditionally, LMWH and vitamin K antagonists (VKAs) were widely used for thromboprophylaxis after THA and TKA. However, both classes have notable limitations. LMWH and fondaparinux are challenging in outpatient care due to their parenteral administration and high cost.4
LMWHs also carry the risk of heparin-induced thrombocytopenia, while fondaparinux is not recommended in patients weighing <50kg, those >75 years, or individuals with moderate-to-severe renal impairment. VKAs pose additional challenges with their
slow onset and offset, narrow therapeutic window (INR 2–3), and complex pharmacodynamics, requiring frequent coagulation monitoring and dose adjustments. They also interact with various foods and drugs and are affected by genetic polymorphisms.4
Aspirin: A controversial option
Aspirin (acetylsalicylic acid) is inexpensive, oral, and widely available, and has historically been used for postsurgical VTE prophylaxis in THA and TKA due to its perceived low bleeding risk. This preference arose after bleeding concerns emerged with fractionated heparins.
However, most data supporting aspirin use are observational. Higher-risk patients were often prescribed warfarin or other anticoagulants, while aspirin was used more broadly. Importantly, these studies did not focus on PE, a key surrogate marker of VTE.4
NOACs: A new era in VTE prophylaxis
Non-vitamin K oral anticoagulants (NOACs) address several shortcomings of traditional agents. Apixaban and rivaroxaban function as direct factor Xa inhibitors, while dabigatran inhibits thrombin directly. These agents have been evaluated in multiple phase III trials for VTE prevention following joint replacement.4
In South Africa, apixaban is indicated for the prevention of VTE in adult patients following elective hip or knee replacement surgery, for reducing the risk of stroke, systemic embolism, and death in patients with non-valvular atrial fibrillation (SPAFib) with one or more risk factors, and for the treatment of DVT and PE, as well as the prevention of recurrent DVT and PE.7
Dabigatran is indicated for the prevention of VTE in patients undergoing hip or knee replacement surgery, the reduction of stroke and systemic embolism risk in AFib, and for the treatment and secondary prevention of DVT and/or PE.8
Rivaroxaban 10mg is indicated for the prevention of VTE in patients undergoing major orthopaedic surgery of the lower limbs. Rivaroxaban 15mg and 20mg are indicated for the prevention of stroke and systemic embolism in SPAFib, for the treatment of DVT, and for the prevention of recurrent DVT and PE.9
The Randomized Double-Blind Comparison of Apixaban with Enoxaparin for Thromboprophylaxis after Knee Replacement:
The ADVANCE-1 Trial, a phase III randomised, double-blind, multicentre study (2009), compared apixaban 2.5mg orally twice daily with enoxaparin 30mg subcutaneously every 12-hours for VTE prevention after TKA. Treatment started 12- to 24-hours postoperatively and continued for around 12 days.10
Among 3195 patients, the primary efficacy outcome (composite of DVT, PE, or all-cause mortality) occurred in 8.99% of apixaban patients versus 8.85% on enoxaparin, not meeting non-inferiority criteria. Symptomatic PE was more frequent in the apixaban group (1.0% vs 0.44%). However, apixaban resulted in less bleeding: major or clinically relevant non-major bleeding occurred in 2.88% of apixaban users versus 4.28% with enoxaparin. Major bleeding alone was also lower with apixaban (0.69% vs 1.39%). While efficacy was similar, apixaban showed a favourable bleeding profile, suggesting potential benefit with future dosing optimisation.10
Agnelli et al (2013) evaluated apixaban, a fixed-dose oral factor Xa inhibitor, as a potential simplified treatment for VTE. In this study, 5395 patients with acute VTE were randomised to receive either apixaban (10mg twice daily for seven days, then 5mg
twice daily for six months) or conventional therapy (subcutaneous enoxaparin followed by warfarin). The primary efficacy outcome –recurrent symptomatic VTE or VTE-related death – occurred in 2.3% of patients on apixaban and 2.7% in the conventional therapy group, confirming noninferiority of apixaban.11
Major bleeding was significantly lower with apixaban (0.6% vs 1.8%). The combined rate of major and clinically relevant nonmajor bleeding was also significantly reduced with apixaban (4.3% vs 9.7%), while other adverse event rates were comparable. In summary, apixaban was noninferior to conventional therapy for acute VTE treatment and demonstrated a superior safety profile with significantly less bleeding.11
Venker et al (2017) conducted a review of randomised trials comparing several anticoagulants for safety and efficacy in THA and TKA. Edoxaban, fondaparinux, and rivaroxaban had the lowest relative risk for VTE compared to enoxaparin 40mg once daily, while dabigatran had the highest VTE risk. Apixaban showed the lowest bleeding risk, whereas rivaroxaban and fondaparinux were associated with higher bleeding. Fondaparinux was the only agent superior to enoxaparin 30mg twice daily. Overall, most newer anticoagulants reduced VTE risk but increased bleeding, with apixaban offering the most favourable balance of safety and efficacy.12
A network meta-analysis by Hur et al (2017) showed that apixaban, fondaparinux, and rivaroxaban significantly reduced the risk of VTE compared with enoxaparin. Dabigatran did not show superior VTE prevention. While fondaparinux and rivaroxaban increased bleeding compared with enoxaparin 40mg once daily, apixaban did not and was associated with less bleeding than both enoxaparin 30mg twice daily and 40mg once daily. When edoxaban
Photo
was included, it also reduced VTE risk without increasing bleeding. Overall, apixaban emerged as the most favourable agent in terms of both efficacy and safety. These findings suggest apixaban may offer the best risk–benefit profile, although results were derived from indirect comparisons and influenced by variation in bleeding definitions, dosing schedules, and surgical procedures.13
In this study by Mayer et al, 400 patients undergoing elective THA or TKA received either dabigatran or apixaban. Both anticoagulants were evaluated for effects on bleeding and thromboembolic outcomes. The key finding was that dabigatran significantly prolonged wound secretion duration compared to apixaban – averaging 4.1 ± 2.1 days versus 2.9 ± 1.8 days, a difference of 1.2 days. No significant differences were found between the two groups in terms of pre- and post-operative haemoglobin levels, postoperative blood loss, transfusion requirements, thromboembolic events, or other bleeding complications. These results suggest that while both drugs offer similar safety and efficacy regarding bleeding and thromboembolic risks, dabigatran may lead to delayed wound healing, making apixaban potentially more favourable in this surgical setting.14 Feng et al (2021) conducted a network meta-analysis including 53 studies (45 067 patients) to compare 19 anticoagulants for preventing VTE after total THA and TKA. Using enoxaparin as the comparator, rivaroxaban, edoxaban, and apixaban showed the highest efficacy in VTE prevention. However, bleeding rates were notably higher with rivaroxaban. In contrast, apixaban, edoxaban,
and darexaban demonstrated the best balance of efficacy and safety, with the lowest and most consistent bleeding risks.15
Conclusion
Apixaban demonstrates a favourable balance of efficacy and safety in the prevention and treatment of VTE, particularly in high-risk orthopaedic settings such as THA and TKA. Across multiple studies, including phase III trials and meta-analyses, apixaban was non-inferior to conventional therapies like enoxaparin and warfarin in preventing VTE, while consistently showing lower rates of major and clinically relevant bleeding. Unlike other agents such as rivaroxaban and fondaparinux, apixaban effectively reduces thrombotic risk without significantly increasing bleeding complications. Its oral administration, predictable pharmacokinetics, and reduced need for monitoring further enhance its clinical utility. Taken together, the evidence supports apixaban as a highly effective and well-tolerated option for perioperative VTE prophylaxis in orthopaedic patients.
References
1. Cox C, Roberts LN. Basics of diagnosis and treatment of venous thromboembolism. J Thromb Haemost, 2025.
2. Basli AA, et al Deep vein thrombosis risk and preventive nursing practices in surgical patients: A descriptive cross-sectional study. Journal of Vascular Nursing, 2025.
3. Simon SJ, et al Venous Thromboembolism in Total Hip and Total Knee Arthroplasty. JAMA Netw Open, 2023.
4. Mody BS, et al Current Evidence and Expert Opinion on Thromboprophylaxis After Total Knee and Hip Replacement. Cureus, 2023.
5. Wegner N, et al Pulmonary embolism and deep vein thrombosis: Similar but different. Thrombosis Research, 2021.
6. Badireddy M, Mudipalli VR. Deep Venous Thrombosis Prophylaxis. [Updated 2023 May 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534865/
7. PI Eliquis. 2022 [Internet]. Available at: https://pi-pil-repository.sahpra.org.za/wpcontent/uploads/2022/07/Eliquis-Approved-PI_11-Jul-2022.pdf
8. PI Pradaxa. 2025 [Internet]. Available at: https://pi-pil-repository.sahpra.org.za/wpcontent/uploads/2025/03/pi-pradaxa-28feb2025.pdf
9. PI Rivoxa. 2025 [Internet]. Available at: https://pi-pil-repository.sahpra.org.za/wpcontent/uploads/2025/05/Final_PI_Rivoxa-10-15-20.pdf.pdf
10. Lassen RM, et al. Randomized Double-Blind Comparison of Apixaban with Enoxaparin for Thromboprophylaxis after Knee Replacement: TheADVANCE-1 Trial. Blood, 2008.
11. Agnelli G, et al. Oral Apixaban for the Treatment of Acute Venous Thromboembolism. NEJM, 2013.
12. Venker BT, et al. Safety and efficacy of new anticoagulants for the prevention of venous thromboembolism after hip and knee arthroplasty: a meta-analysis. J Arthroplasty, 2017.
13. Hur M, et al Comparative efficacy and safety of anticoagulants for prevention of venous thromboembolism after hip and knee arthroplasty. Acta Orthop, 2017.
14. Mayer A, et al. A comparison of apixaban and dabigatran etexilate for thromboprophylaxis following hip and knee replacement surgery. Arch Orthop Trauma Surg, 2017.
15. Feng W, et al Ranking the efficacy of anticoagulants for the prevention of venous thromboembolism after total hip or knee arthroplasty: a systematic review and a network meta-analysis. Pharmacol Res, 2021. SF
RRR IN STROKE/SE 6 HR 0.80 (95% CI, 0.73-0.89)
434 ,046 PATIENTS 6
Favourable safety with uncompromised efficacy
For ELIQUIS®(apixaban) prescribing information, scan the QR code
References:
To access the ELIQUIS® (apixaban) website, scan the QR code
The reference standard here refers to the innovator molecule. (Watson J, et al. Drugs. 2011;71(15):2079-2089). SE: Systemic embolism. RRR: Risk rate reduction. HR: Hazard ratio. CI: Confidence interval.
2. Granger CB, et al. N Engl J Med. 2011;365(11):981-92. 3. Ruff CT, et al. Lancet. 2014;383(9921):955-62.
4. Cohen AT, et al. Adv Ther. 2014;31:473-93. 5. Agnelli G, et al. N Engl J Med. 2013;369(9):799-808. 6. Lip GYH, Et al. Stroke. 2018(12):2933-2944. Erratum in: Stroke. 2020;51(2):e44. Erratum in: Stroke. 2020;51(4):e71.
This image is for representation purpose only. For the use only of a Registered Medical Practitioners or a Hospital or a Laboratory.
S4 ELIQUIS® 2,5 MG AND 5 MG FILM-COATED TABLETS (REG. NO’S: 47/8.2/0463, 0464). EACH FILM-COATED TABLET CONTAINS EITHER 2,5 MG OR 5 MG APIXABAN.
To report an adverse event, please contact ZAF.AEReporting@pfizer.com If you wish to contact Pfizer for any other purpose, please use contact details below. +2711 320 6000 or 0860 734 937 (SA). Monday-Friday 09h00-17h00.
Balancing bleeds
and beats: AFib anticoagulation
Atrial fibrillation (AFib) is the most common cardiac arrhythmia, increasing the risk of cardiovascular (CV) events like stroke, systemic embolism (SE), and heart failure (HF), while also exacerbating cardiac and noncardiac conditions. It is marked by chaotic and irregular electrical activity. For stroke prevention in AFib patients, both vitamin K antagonists (VKAs), such as warfarin, and non-VKA oral anticoagulants (NOACs), including apixaban, dabigatran, and rivaroxaban, are recommended. However, NOACs are now preferred over VKAs due to their superior efficacy and safety.1,2
All OACs carry a risk of gastrointestinal (GI) bleeding. Major GI bleeding after OAC initiation is linked to significant 30-day mortality, hospitalisation, and increased healthcare resource use, contributing to morbidity and mortality rates of 5%-15%.1,2
The International Society on Thrombosis and Hemostasis defines major bleeding as symptomatic bleeding in a critical organ or area, a ≥20g/l drop in haemoglobin, or the need for a transfusion of ≥2 units of whole blood or red cells. The American College of Cardiology expands this definition to include hemodynamic instability, characterised by increased heart rate, systolic blood pressure (SBP) <90mmHg, a SBP decrease >40mmHg, or orthostatic BP changes (SBP drop ≥20mmHg or diastolic blood pressure [DBP] drop ≥10 mmHg upon standing).1
A study by Deitelzweig et al found that GI bleeding sites vary by OAC. Warfarin is associated primarily with upper GI bleeding, while dabigatran users with major GI bleeding experience 53% lower GI involvement. In contrast, upper GI bleeding is more common than lower GI bleeding with apixaban (63% vs 37%) and rivaroxaban (76% vs 24%).2
Deitelzweig et al reported a major GI bleeding incidence rate of 2.50 per 100 person-years among OAC-treated patients. Unadjusted rates per 100 person-years were 1.8 (apixaban), 2.2 (dabigatran), 2.8 (rivaroxaban), and 3.0 (warfarin). The average time from OAC initiation to major GI bleeding was 78.3 days. Hospitalisation for these events lasted a mean of 4.4 days, with 40% of patients admitted to the ICU, 66% requiring blood transfusions, and many undergoing esophagogastroduodenoscopy (41%) or colonoscopy.2
Risk factors for major GI bleeding
NOAC-related GI bleeding risk depends on dosage, patient factors (age >75-years, comorbid chronic kidney disease [CKD], cirrhosis),
and medication use (eg proton pump inhibitors, histamine 2-receptor antagonists). Acute coronary syndrome (5.21 times greater) and renal impairment further increase the bleeding risk in individuals living with CKD and treated with a NOAC.1
Other risk factors include a higher Charlson Comorbidity Index, CHA₂DS₂-VASc, and HAS-BLED scores, a history of bleeding, coronary artery disease, and HF. Hypertension (SBP >160mmHg), stroke, anaemia, hepatic or renal disease, and antiplatelet therapy worsen outcomes.1,2
Mechanisms of GI bleeding with OACs
The mechanisms of GI bleeding associated with NOACs can be attributed to several factors, including systemic anticoagulant effects, focal anticoagulant effects, inhibition of mucosal healing, and direct caustic effects. While warfarin’s systemic anticoagulant activity is a general concern, NOACs like apixaban, dabigatran, and rivaroxaban have focal anticoagulant effects due to their partial absorption, leading to localised bleeding in the GI tract.3
Dabigatran, which contains tartaric acid, may also cause direct caustic injury to the gut lining. In contrast, edoxaban does not target digestive enzymes like trypsin and chymotrypsin yet still shows higher GI bleeding risk than warfarin.3
According to Martin et al, variability in bleeding risk may stem from differences in drug dosage, reporting methods, or study populations. For example, patients in the Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET-AF) trial were older with more comorbidities than those in the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE), Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY).1
However, in the ARISTOTLE trial, apixaban had a similar risk of GI bleeding compared to warfarin. In the RE-LY trial, twice-daily dabigatran 150mg showed a higher risk of GI bleeding (50%), while the twice-daily 110mg dose showed a non-significant increase in risk (10%) compared with warfarin. In the ROCKET-AF trial, major GI bleeding was more common in the rivaroxaban group (3.2%) than in the warfarin group (2.2%).2
The European Society of Cardiology (ESC) guidelines for managing AFib recommend choosing a VKA or another NOAC over twice-daily dabigatran 150mg or once-daily rivaroxaban 20mg in individuals at high risk of GI bleeding.2
A recent study by Al-Hussainy et al investigated the risk of GI bleeding and stroke among NOACs in individuals diagnosed with AFib and moderate or severe anaemia. Compared with apixaban, dabigatran and rivaroxaban were associated with significantly higher risks of GI bleeding, with a 73% and 56% increase in risk, respectively, at 12-months. No significant differences in stroke risk were observed among the NOACs.4
significant difference was found for dabigatran or rivaroxaban compared to warfarin.5
Impact of dosing frequency on GI bleeding
Research shows that the twice-daily dosing regimen may be safer than once-daily regimens as it stabilises drug concentrations, reducing the likelihood of peak concentrations that could increase bleeding risk. Studies support that twice-daily regimens, such as apixaban, show lower bleeding risks compared to once-daily regimens.3
The risk of NOACrelated GI bleeding depends on dosage, patient factors –including age >75, CKD, or cirrhosis – and concurrent medications such as PPIs or H2-receptor antagonists
Kohasa et al compared the risk of GI bleeding in participants treated with warfarin and apixaban, warfarin and dabigatran, and warfarin and rivaroxaban, respectively. Compared to warfarin, apixaban showed a 41.4%, dabigatran 38.3%, and rivaroxaban a 30.7% decrease in the risk of major bleeding. The risk of any bleeding was significantly lower for apixaban (21.8%), but no
As shown in the above studies, rates of GI bleeding were higher in several NOAC regimens compared to warfarin, especially in once-daily regimens. This may be due to the fact that peak concentration is higher in once-daily regimens than in twice-daily regimens. Twice-daily dosing may suppress the peak drug concentration in the gut lumen and blood plasma, which may result in a better safety profile.3
Ido et al conducted a real-world investigation of GI bleeding in individuals treated with NOACs (n=2216, follow-up duration 650 days). Patients were divided into two groups: The twice-daily regimen group (dabigatran and apixaban) and the once-daily regimen group (rivaroxaban). After matching 904 patients in each group using propensity scores, the primary endpoint of GI bleeding was evaluated.6
The study found that the event rate of GI bleeding was significantly lower in the twice-daily regimen group than in the once-daily regimen group (3.5/100 person-years vs 6.2/100
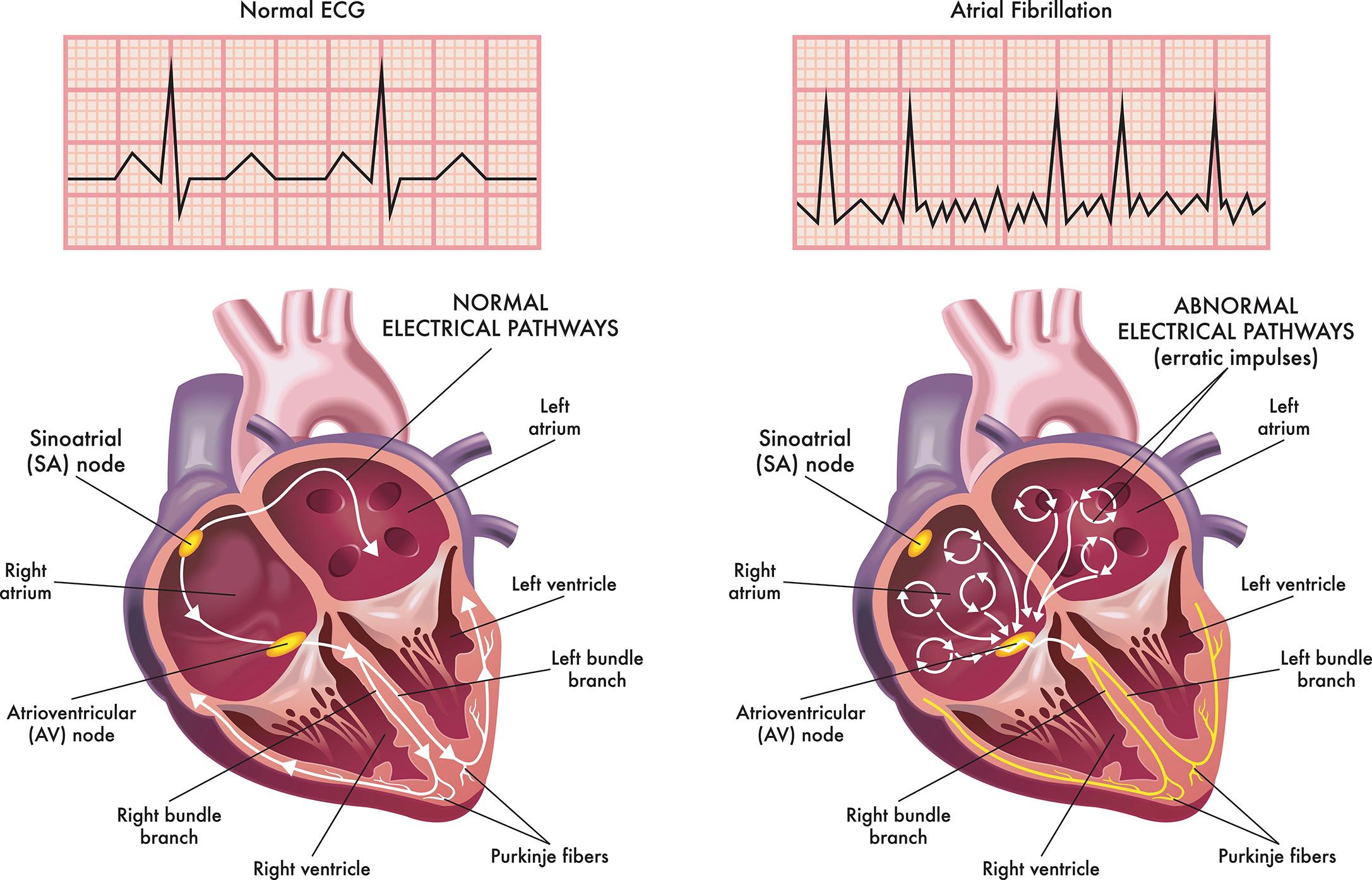
The yellow lines demonstrate the electrical (conduction) system of the heart. The heart at right shows an irregular heartbeat (arrhythmia) and atrial fibrillation.
person-years). Moreover, the rate of major bleeding was also significantly lower in the twice-daily regimen group. However, there were no significant differences between the twice-daily and oncedaily regimen groups for all-cause death, stroke, or any bleeding. In the overall population, the risk of GI bleeding was lower (44.4%) in the twice-daily group. The superiority of the twice-daily regimen was consistent across various subgroups, concluded Ido et al 6
Triage for GI bleeding in the emergency department
Upon admission to hospital with GI bleeding, anticoagulants and antiplatelets should be discontinued. For most cases, the pharmacokinetic profile of NOACs suggests that time is the best antidote.1
When an individual presents in the emergency department with a suspected GI bleed, a thorough evaluation is essential. Key factors include medical history, OAC dosage and timing, concomitant medications, bleeding severity, and possible sources. Vital signs, haemorrhagic shock status, and prior digestive bleeding should be assessed.1
Haemodynamic and respiratory stabilisation follows the ABCDE (airway, breathing, circulation, disability, and exposure) approach, with oxygen supplementation or intubation if needed, though excessive oxygen may harm cardiac function.1
Immediate intravenous access is crucial for volume resuscitation. The European Society of GI Endoscopy recommends restrictive red blood cells transfusion, targeting haemoglobin levels between 7g/dl–9g/dl, with higher targets for individuals with significant comorbidities like myocardial infarction (MI). Several scales, including Thrombolysis in MI, Global Use of Strategies to Open Occluded Arteries, and Bleeding Academic Research Consortium, can help to assess bleeding severity.1
However, reversal should be considered in lifethreatening bleeding or if initial resuscitation fails. For VKAs, prothrombin complex concentrate (PCC) at 25IU/kg is recommended. NOAC reversal is needed for concentrations >50ng/ml. Below this threshold, bleeding is unlikely to be related to NOACs.1
Specific reversal agents for NOACs include idarucizumab for dabigatran, and andexanet alfa for
factor Xa inhibitors (apixaban, rivaroxaban). When these antidotes are unavailable, PCC (50IU/kg) or activated PCC (30–50IU/kg) can be administered. Recent studies suggest activated PCC may be effective for life-threatening GI bleeding.1
Should OACs be resumed after major GI bleeding?
According to the ESC guidelines resuming OACs after a major bleeding event when the risk of thromboembolism outweighs the risk of further bleeding. Studies show resuming OAC treatment after a major GI bleed has a positive impact, reducing the risk of thromboembolism (70%) and mortality (49%) despite a higher risk of recurrent GI bleeding (91%).1,2
Conclusion
AFib poses a significant risk for CV events, including stroke, SE, and HF, which necessitates effective anticoagulation therapy for stroke prevention. While VKAs like warfarin have been used historically, NOACs such as apixaban, dabigatran, and rivaroxaban are now preferred due to their superior safety and efficacy profiles. All OACs carry a risk of GI bleeding, which is a serious concern as it contributes to morbidity and mortality. Studies have shown that the frequency of GI bleeding with NOACs can vary based on the specific regimen and dosing schedule, with twice-daily dosing regimens like apixaban showing a lower risk of GI bleeding compared to once-daily regimens. Additionally, patient factors such as age, comorbidities, and concomitant medications further influence bleeding risks. While the management of GI bleeding in patients on OACs requires careful triage and reversal strategies, resuming anticoagulation after a major bleeding event remains crucial for reducing thromboembolic risks. Ultimately, the choice of anticoagulant and dosing regimen must be individualised, balancing the need for stroke prevention with the potential risk of bleeding complications.
References
1. Martin AC, et al. Management of Gastrointestinal Bleeding and Resumption of Oral Anticoagulant Therapy in Patients with Atrial Fibrillation: A Multidisciplinary Discussion. American Journal of Cardiovascular Drugs, 2023.
2. Deitelzweig S, et al Burden of major gastrointestinal bleeding among oral anticoagulant-treated non-valvular atrial fibrillation patients. Therapeutic Advances in Gastroenterology. 2021.
3. Ido T, et al Twice- or once-daily dosing of direct oral anticoagulants and gastrointestinal bleeding in patient with atrial fibrillation. Am Heart J Plus, 2022.
4. Al-Hussainy N, et al Gastrointestinal bleeding with direct oral anticoagulants in patients with atrial fibrillation and anaemia. Thrombosis Research, 2023.
5. Kohsaka S, et al. Bleeding risk of apixaban, dabigatran, and low-dose rivaroxaban compared with warfarin in Japanese patients with non-valvular atrial fibrillation: a propensity matched analysis of administrative claims data Curr Med Res Opin 2017.
6. Ageno W, et al Once- versus twice-daily direct oral anticoagulants in non-valvular atrial fibrillation. Expert Opinion on Pharmacotherapy, 2017. SF
EVOREL®: Hormone Replacement Therapy (HRT) patch with a complete range:
EVOREL® range gives you the option to meet the needs for pre and postmenopausal women choosing HRT and adopt an individualised approach1-5
• International and local guidelines recommend transdermal HRT as first-line treatment5,8,9,10
• The EVOREL® range displays many additional benefits over and above the relief of VMS symptoms1-4,11,17-21
• Transdermal HRT should be considered in all suitable women4-6,18,21
• Transdermal patches ensure consistent release of the hormone component and control of VMS7,19,20
Effects of Oral vs Transdermal Estrogen Therapy on Sexual Function in Early Postmenopause: Ancillary Study of the Kronos Early Estrogen Prevention Study (KEEPS). JAMA Intern Med. 2017;177(10):1471-1479. doi: 10.1001/jamainternmed.2017.3877.12. Gleason CE, Dowling NM, Wharton W, Manson JE, Miller VM, Atwood CS, et al Effects of Hormone Therapy on Cognition and Mood in Recently Postmenopausal Women: Findings from the Randomized, Controlled KEEPS-Cognitive and Affective Study. PLoS Med. 2015;12(6):e1001833; discussion e1001833. doi: 10.1371/journal.pmed.1001833.13. Stepan JJ, Hruskova H, Kverka M. Update on Menopausal Hormone Therapy for Fracture Prevention. Curr Osteoporos Rep. 2019;17(6):465-473. doi: 10.1007/s11914-019-00549-3. 14. Abdi F, Mobedi H, Bayat F, et al. The Effects of Transdermal Estrogen Delivery on Bone Mineral Density in Postmenopausal Women: A Meta-analysis. Iran J Pharm Res. 2017;16(1):380-389.15. Palmisano BT, Zhu L, Stafford JM. Estrogens in the Regulation of Liver Lipid Metabolism. Adv Exp Med Biol. 2017;1043:227-256. doi: 10.1007/978-3-319-70178-3_12. 16. Lundström E, Wilczek B, von Palffy Z, et al. Mammographic breast
TWomen’s health: Priorities through
every life-stage
Women’s health evolves across distinct stages of life, each characterised by unique physiological changes, health priorities, and preventive care needs. The journey from reproductive years through menopause involves significant hormonal transitions that impact every body system.1-70
hese changes occur against a backdrop of individual genetics, lifestyle factors, and socioeconomic determinants that collectively shape health outcomes.1-70
Twenties in full swing: Fertile ground, fragile balance
Womb for improvement: Fertility
in the twenties
Though the twenties represent peak reproductive potential, fertility actually begins a gradual decline during this decade. Women <30-years have about a 71% chance of conceiving within three months of trying, with egg quality and menstrual regularity as key determinants. By age 30, subtle changes in ovarian reserve and oocyte quality begin to impact conception rates, though these changes often go unnoticed until later decades.¹
Nutrition significantly impacts fertility, with plant-based proteins and full-fat dairy associated with improved ovulation rates. Research indicates that replacing animal protein with plant protein sources (beans, nuts, seeds) may reduce ovulatory infertility by ~50%. Similarly, women consuming at least one serving of full-fat dairy daily show 27% lower risk of infertility compared to those consuming primarily low-fat options.¹
Conversely, extreme body mass indexes (BMI) – both underand overweight – disrupt hormonal balance and menstrual cyclicity. Women with BMI <18.5 often experience hypothalamic amenorrhoea due to energy deficit, while those with BMI >30 frequently develop insulin resistance and hyperandrogenism, both detrimental to ovulation. Moderate exercise (≤5 hours weekly) optimises reproductive function, while excessive training can suppress ovulation through alterations in leptin and other metabolic signals.¹
Environmental factors including stress, alcohol consumption, and exposure to endocrine-disrupting chemicals further influence fertility outcomes. Chronic stress elevates cortisol levels, potentially interfering with gonadotropin-releasing hormone pulsatility and subsequent ovulation.
Regular alcohol consumption (>8 drinks weekly) correlates with longer time to conception and increased risk of ovulatory dysfunction.¹
For women delaying childbearing, early fertility awareness and preservation options provide important safeguards. Education regarding age-related fertility decline allows for informed family planning decisions, while options such as oocyte cryopreservation offer possibilities for preserving reproductive potential for those deferring pregnancy.¹
Plan ahead, not just a plan B: The role of contraception
Modern contraceptive methods, including long-acting reversible contraceptives and hormonal options, enable women to align family planning with educational and career goals. With ~44% of pregnancies worldwide being unintended, reliable contraception remains essential for reproductive autonomy. Effective contraception not only prevents unplanned pregnancy but also reduces maternal mortality, with an estimated 30% of maternal deaths preventable through adequate contraceptive access.2,3
The contraceptive landscape for women in their twenties has evolved significantly, with increased emphasis on long-acting methods offering >99% effectiveness with minimal user dependence. Intrauterine devices (hormonal and non-hormonal) and subdermal implants provide three- to 10-years of protection with failure rates <1%,
compared to 7%-9% for typical use of pills, patches, and rings.⁴
Beyond pregnancy prevention, many contraceptive methods offer non-contraceptive benefits including menstrual regulation, reduction in heavy bleeding, improvement in acne, and decreased risk of certain cancers. Combined hormonal contraceptives reduce risk of ovarian and endometrial cancers by ~50% and ~30% respectively with long-term use.⁴
Contraceptive counselling should address both immediate needs and future fertility plans. Women in their twenties benefit from personalised guidance on method selection based on efficacy, side effect profiles, and compatibility with lifestyle factors. The ability to control reproductive timing contributes significantly to educational attainment, economic stability, and maternal health outcomes.⁴
The silent spreaders: STI prevention in the prime of life
Young women face disproportionate vulnerability to sexually transmitted infections (STIs), including human papillomavirus (HPV), which affects ~291 million women globally. HPV acquisition typically occurs within the first few years of sexual activity, with high-risk strains potentially leading to cervical, anal, and oropharyngeal cancers. Current estimates suggest that ~80% of sexually active women will contract HPV by age 50, with peak incidence in the late teens and early twenties.⁵
Women experience higher rates of complications from STIs compared to men, including pelvic inflammatory disease, chronic pelvic pain, and infertility. Chlamydia trachomatis and Neisseria gonorrhoeae infections remain asymptomatic in up to 70% of female cases, facilitating transmission and delaying treatment. When untreated, these infections ascend to the upper reproductive tract in 10%-15% of cases, potentially causing tubal scarring and subsequent infertility.⁵
Risk factors including inconsistent condom use, multiple partners, and delayed testing contribute to STI prevalence. Prevention strategies must combine education, access to protection, regular screening, and vaccination programmes.
Consistent condom use reduces transmission risk of most STIs by 80%-90%, though HPV may still spread through uncovered genital contact.⁶
HPV vaccination significantly reduces infection rates and cervical cancer risk by ~70% when administered before sexual debut, highlighting the importance of early intervention. Population-level data from countries with high vaccination coverage demonstrate dramatic decreases in high-grade cervical lesions and genital warts.6,7
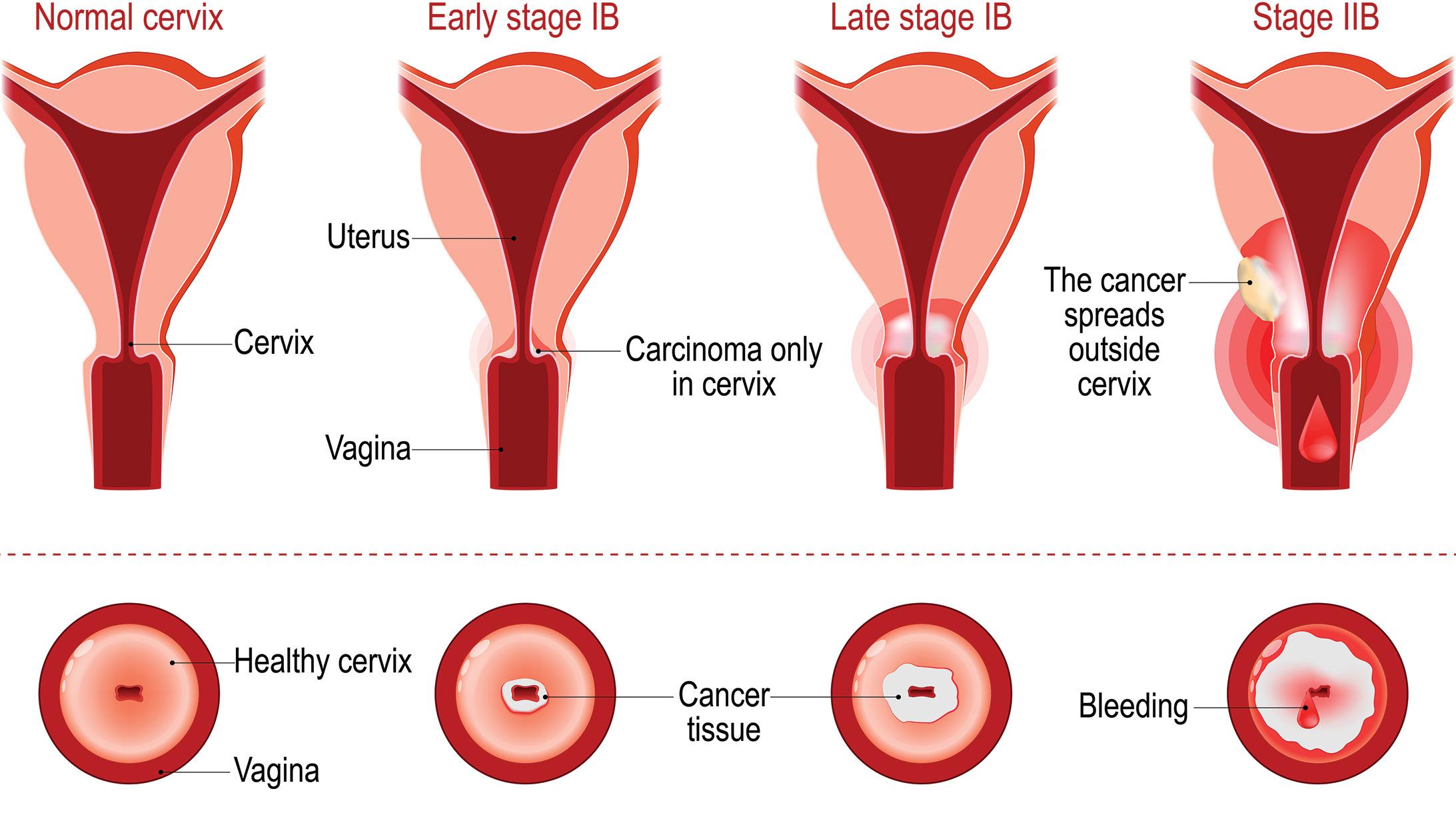
Cervical checkpoint: Why screening cannot wait
In South Africa, cervical cancer (CCa) is the leading cause of cancer-related mortality among women, with >10 000 new cases and 5000 deaths annually. While national guidelines recommend screening from age 30, the high prevalence of early HPV exposure supports earlier initiation of screening protocols. Studies indicate that up to 25% of precancerous lesions develop <30-years, particularly in settings with high HIV prevalence.7,8
Screening options include traditional Pap smears and HPV DNA testing, with self-sampling strategies showing promise for increasing accessibility. Pap smears have historically reduced CCa incidence by 50%-70% in well-screened populations, while HPV testing offers increased sensitivity for high-risk strain detection.⁸
School-based HPV vaccination programmes represent a critical prevention strategy, though implementation faces challenges including education gaps and vaccine hesitancy. Current vaccines protect against HPV types responsible for ~90% of CCa, potentially preventing ~50 000 new cases annually with optimal coverage.⁹
Early detection through appropriate screening significantly improves outcomes, making cervical health a priority from the twenties onward. Five-year survival rates >90% for early-stage CCa but drop <20% for advanced disease, underscoring the critical importance of timely screening and intervention.⁹
Offbeat rhythms: Menstrual irregularities and what they reveal
Photo
Menstrual disorders affect 14%-25% of women aged 20- to 29-years, often signalling underlying health issues. Conditions such as polycystic ovary syndrome (PCOS), hypothalamic amenorrhoea, and thyroid dysfunction manifest through irregular cycles and require prompt investigation. PCOS alone affects 8%-13% of reproductive-age women, with manifestations including oligomenorrhoea, hyperandrogenism, and metabolic disturbances.¹⁰
Cycle irregularities in the twenties often indicate hypothalamicpituitary-ovarian axis disruption, with potential causes ranging from stress and extreme exercise to structural abnormalities and endocrine disorders. Evaluation should include detailed history, physical examination, and targeted laboratory assessment based on clinical presentation.¹⁰
Beyond reproductive implications, menstrual irregularities can indicate increased risk for metabolic syndrome, type 2 diabetes (T2DM), and cardiovascular (CV) disease. Women with PCOS show two- to four-fold increased risk of glucose intolerance by age 40, with ~40% developing prediabetes or diabetes. Similarly, CV risk markers including dyslipidaemia, hypertension, and endothelial dysfunction appear earlier in women with menstrual disorders.¹¹
Low oestrogen states resulting from irregular cycles also impact bone health, potentially accelerating osteoporosis risk. Women with hypothalamic amenorrhoea demonstrate 10%-15% lower bone mineral density (BMD) compared to age-matched controls, with fracture risk increased by ~30% if amenorrhoea persists >6-months.¹¹
Management focuses on addressing underlying causes through nutritional optimisation, stress management, and appropriate hormonal therapy when indicated. For PCOS, combination approaches targeting both symptoms and metabolic risks show greatest efficacy, with metformin reducing insulin resistance and combination contraceptives regulating cycles and reducing androgen effects.¹¹
Mirror, mirror: Adult acne and emotional well-being
Adult female acne affects a considerable proportion of women in their twenties, with hormonal fluctuations, stress, and genetic factors as primary contributors. Unlike adolescent acne, adult female acne typically manifests in the lower face and jawline, with flares often corresponding to menstrual cycles. Prevalence ranges from 12%-22% in this age group, with persistence or new-onset cases increasingly common.¹²
Beyond physical manifestations, acne significantly impacts emotional health, often leading to depression, social avoidance, and reduced quality of life (QoL). Studies demonstrate that women with moderate to severe acne score 30%-50% higher on depression and anxiety scales compared to unaffected peers.¹²
Treatment approaches include topical retinoids, oral contraceptives for hormonal regulation, and anti-androgen therapies such as spironolactone. Topical options constitute first-line therapy for mild to moderate cases, with combination regimens showing superior efficacy. For moderate to severe cases, hormonal therapy addresses underlying endocrine drivers, with combination oral contraceptives reducing serum androgens and increasing sex hormone binding globulin.¹²
Isotretinoin remains the most effective option for severe, recalcitrant cases, offering remission rates of 70%-80% with
appropriate dosing. However, strict pregnancy prevention measures are essential due to teratogenicity risks. Addressing both dermatological and psychological aspects through integrated care optimises outcomes and prevents lasting emotional consequences.¹²
Mind matters: Mental health in the era of comparison
The prevalence of anxiety and depression among young women has increased, exacerbated by social media exposure and societal pressures. Women aged 18- to 29-years demonstrate 1.5-2 times higher rates of depression and anxiety disorders compared to male counterparts, with ~25% meeting diagnostic criteria for at least one mental health condition annually.¹³
Body image dissatisfaction, perfectionism, and digital comparison culture contribute to psychological distress during this formative decade. Social media use correlates with increased depression risk, with each hour of daily use associated with 13% higher likelihood of depressive symptoms.¹³
Biological factors including hormonal fluctuations also influence mood regulation, with oestrogen and progesterone affecting neurotransmitter systems including serotonin, dopamine, and gamma-aminobutyric acid (GABA). These hormonal effects may partially explain gender disparities in depression prevalence.¹³
Evidence-based interventions include cognitive behavioural therapy (CBT), mindfulness practices, and media literacy training. CBT demonstrates 50%-70% response rates for depression and anxiety disorders, with effects comparable to medication for mild to moderate symptoms. Digital mental health interventions show particular promise for younger women, with online platforms and mobile applications increasing accessibility while reducing stigma barriers.¹³
Thriving thirties: Balancing pregnancy, prevention, and health
Hypertensive disorders of pregnancy
Hypertensive disorders complicate 2%-8% of pregnancies globally, with increased prevalence among women of advanced maternal age (≥35-years). These disorders encompass a spectrum including chronic hypertension, gestational hypertension, pre-eclampsia, and eclampsia. Pre-eclampsia, characterised by hypertension and proteinuria after 20 weeks’ gestation, carries significant risks for maternal and neonatal morbidity.¹⁴
Women with pre-eclampsia face three- to four-fold higher risk of severe outcomes including placental abruption, acute kidney injury, pulmonary oedema, and maternal death. Foetal complications include intrauterine growth restriction, preterm birth, and perinatal mortality, with risks proportional to disease severity and gestational age at onset.¹⁴
Risk factors include nulliparity, previous pre-eclampsia, chronic hypertension, obesity, and autoimmune conditions. Women with prior pre-eclampsia face seven-fold increased recurrence risk, while those with pre-pregnancy BMI >30 demonstrate twoto three-times higher incidence compared to normal-weight counterparts.¹⁵
Prevention strategies focus on optimising modifiable risk factors and implementing aspirin prophylaxis for high-risk women. Lowdose aspirin (81mg-150mg daily) initiated between 12-16 weeks’ gestation may reduce pre-eclampsia risk by 24%-62% in high-risk
populations. Calcium supplementation (1.5g-2g daily) provides additional benefit in women with low dietary intake.¹⁵
Early detection through regular prenatal monitoring improves outcomes, while severe cases require prompt intervention to prevent complications including eclampsia and haemolysis, elevated liver enzymes, low platelets, or HELLP syndrome. Hypertensive disorders during pregnancy also increase long-term CV risk, necessitating ongoing monitoring and preventive care in subsequent decades.¹⁵
Sugar trouble: Gestational diabetes
Gestational diabetes mellitus (GDM) affects ~14% of pregnancies worldwide, with rates continuing to increase alongside obesity prevalence. Defined as glucose intolerance first recognised during pregnancy, GDM results from inadequate insulin secretion relative to pregnancyinduced insulin resistance. Beyond immediate pregnancy complications, GDM significantly increases lifetime risk for T2DM and CV disease.16,17
Pregnancy naturally induces progressive insulin resistance, with insulin sensitivity decreasing by 50%-60% by the third trimester. Placental hormones including human placental lactogen, progesterone, and corticotropin-releasing hormone contribute to this physiologic insulin resistance.¹⁶
and dopamine, potentially triggering depressive episodes in susceptible individuals.²⁰
Beyond maternal suffering, PPD significantly impacts infant development and family functioning. Infants of depressed mothers show altered stress responses, with cortisol patterns reflecting heightened hypothalamic-pituitary-adrenal axis activation. Behavioural effects include reduced positive affect, increased negative emotionality, and potential developmental delays.²¹
Despite its prevalence, PPD remains underdiagnosed, with significant implications for maternal functioning, infant attachment, and family dynamics. Screening tools such as the Edinburgh Postnatal Depression Scale facilitate early identification, with sensitivity of between 80%-90% using appropriate cutoff scores.²¹
Current MHT approaches emphasise individualised riskbenefit assessment, with cardiovascular effects influenced by timing of initiation relative to menopause onset, per the timing hypothesis
Foetal consequences include macrosomia (birthweight >4000g), which affects 15%-45% of GDM pregnancies compared to 8%14% of normoglycemic pregnancies. Macrosomia increases the risk of shoulder dystocia, birth trauma, and caesarean delivery. Additionally, neonatal hypoglycemia affects 15%-25% of infants born to mothers with GDM.¹⁸
Screening between 24- to 28-weeks’ gestation is standard practice, though earlier testing is recommended for high-risk women. Management through dietary modification, physical activity, and insulin therapy, when necessary, reduces adverse outcomes. Nutritional therapy constitutes the cornerstone of management, with carbohydrate distribution improving postprandial glucose excursions.¹⁸
Postpartum follow-up is essential, with ~50% of women with GDM developing T2DM within five-to 10-years. Lifestyle interventions during this critical window can reduce progression risk by up to 58%.¹⁹
Mind the gap: Postpartum depression
Postpartum depression (PPD) affects ~15% of mothers globally, with prevalence reaching 29% in African settings. Risk factors include previous depression, limited social support, traumatic birth experiences, and hormonal fluctuations. Prevalence may be higher than reported due to screening challenges and stigma surrounding mental health conditions.²⁰
Physiologically, the dramatic postpartum drop in oestrogen and progesterone contributes to mood vulnerability, particularly in hormonally sensitive women. These hormonal shifts affect neurotransmitter systems including serotonin
Treatment options include psychotherapy, support groups, and selective serotonin reuptake inhibitors (SSRIs) when appropriate. CBT and interpersonal therapy demonstrate particular efficacy, with 60%-70% of women showing significant improvement following eight- to 12- sessions.²²
Preventive approaches focusing on psychoeducation and supportive care during pregnancy and the early postpartum period show promise for reducing incidence and severity. Targeted interventions for high-risk women reduce PPD incidence by 20%-30%.²²
The ticking clock and the chronic load: A perfect storm of comorbidities
Women in their thirties increasingly face the emergence of chronic health conditions, often coinciding with family planning decisions and career demands. Conditions including hypertension, autoimmune disorders, and mood disorders may first manifest during this decade, requiring proactive management approaches. National survey data indicate that ~30% of women between 30- to 39-years have at least one chronic health condition.²³
Pregnancy complications often serve as early warning signs for future chronic disease, with conditions such as pre-eclampsia and GDM associated with increased CV risk. Women with hypertensive disorders of pregnancy demonstrate two- to three-fold higher risk of hypertension and CV events within 10- to 15-years of delivery.²³
The concept of metabolic memory highlights how reproductive health events influence long-term health trajectories. Vascular changes, inflammatory activation, and epigenetic modifications occurring during complicated pregnancies may persist postpartum, accelerating subsequent disease processes.²⁴
Autoimmune conditions demonstrate particular female predominance, with peak onset during reproductive years. Conditions including rheumatoid arthritis, systemic lupus erythematosus, and autoimmune thyroiditis affect women twoto nine-times more frequently than men, suggesting hormonal influences on immune regulation.²⁴
Preventive strategies should address modifiable risk factors including weight management, physical activity, and stress reduction. Postpartum weight retention averages 3kg-5kg after first pregnancy, with 14%-20% of women retaining ≥5kg. Structured interventions combining dietary modification and physical activity
demonstrate 60%-70% success in returning to pre-pregnancy weight when initiated within the first year postpartum.²⁴
Fabulous forties:
Hot flashes, heart risks, moods, and moves
Perimenopause: When the calendar gets irregular and so does everything else
Perimenopause typically begins in the early to mid-forties, characterised by fluctuating hormone levels and declining ovarian function. This transitional phase precedes menopause by four- to eight-years on average, though duration varies widely among individuals. Hormonal fluctuations during this period often exceed those seen during reproductive years, with oestrogen levels occasionally rising higher than previously experienced before ultimately declining.²⁵
Common symptoms include menstrual irregularity, vasomotor symptoms of menopause (VSM, hot flashes and night sweats), sleep disturbances, and mood changes. Around 80% of women experience VSM during perimenopause, with 25%-30% reporting symptoms severe enough to seek medical attention.²⁵
Sleep architecture changes significantly during perimenopause, with reduced sleep efficiency, increased nocturnal awakenings, and decreased slow-wave sleep. These disturbances stem from both primary hormonal effects on sleep regulation and secondary disruption from night sweats. Sleep disruption contributes to daytime fatigue, mood disturbances, and cognitive complaints commonly reported during this transition.²⁶
Diagnostic criteria focus on menstrual pattern changes and symptom presentation, with hormonal testing having limited utility due to significant fluctuations. Increased cycle variability (>7 days different from normal) typically marks early perimenopause, while skipped periods (≥60 days of amenorrhoea) indicate late perimenopause.²⁶
Management approaches range from lifestyle modifications to hormone replacement therapy (HRT), with treatment decisions based on symptom severity, QoL impact, and individual risk profiles. Non-hormonal options for vasomotor symptoms include SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), gabapentinoids, and clonidine, though efficacy remains below that of HRT.²⁶
HRT, when initiated during peri- or early postmenopause, offers the most effective symptom relief with favourable risk-benefit ratio for most women. Low-dose systemic oestrogen (with progestogen in women with intact uterus) reduces VSM by 75%-80% compared to placebo, while also improving sleep quality, mood stability, and genitourinary symptoms.²⁶
Breast cancer at 40: Timing, risk, and the screening balancing act
Breast cancer (BCa) incidence starts increasing significantly in the forties, with women aged 40-to 49-years accounting for ~20% of all BCa diagnoses. Mortality rates have declined over recent decades due to improved screening and treatment modalities, though optimal screening approaches for this age group remain controversial due to considerations regarding benefit-to-harm ratios.²⁷
For women with average risk, individualised decision-making regarding screening initiation between ages 40- to 49-years is
recommended, with biennial mammography becoming standard from age 50. This approach balances potential benefits of early detection with concerns regarding false positives, recall anxiety, and overdiagnosis.²⁷
Risk assessment should incorporate factors including family history, genetic predisposition, breast density, and reproductive history. Women with first-degree relatives diagnosed with BCa face double the average risk, while those with genetic mutations such as BCa gene 1 and gene 2 (demonstrate five- to 10-fold increased lifetime risk.²⁷
Breast density, which affects 40%-50% of women in their forties, both increases BCa risk and reduces mammographic sensitivity. Dense breast tissue appears white on mammography, potentially obscuring masses that also appear white. Supplemental screening with ultrasound or magnetic resonance imaging may be appropriate for women with dense breast tissue or elevated risk profiles.²⁷
The balance between early detection benefits and potential harm (including false positives and overdiagnosis) requires careful consideration and shared decision-making with patients. False positive results affect ~10% of women in their forties undergoing annual mammography, potentially leading to unnecessary biopsies, anxiety, and healthcare costs.²⁷
Midlife metabolism mayhem: The perimenopausal domino effect
Hormonal shifts during perimenopause contribute to metabolic changes including increased visceral adiposity, insulin resistance, and lipid profile alterations. These changes collectively increase the risk for metabolic syndrome, with prevalence increase from ~20% in the early forties to 30%-40% by the early fifties. This metabolic transition extends beyond simple weight gain, involving fundamental changes in body composition and energy regulation.²⁸
Oestrogen plays significant roles in glucose homeostasis, lipid metabolism, and body fat distribution. Declining oestrogen levels during perimenopause reduce insulin sensitivity by 15%-25% and alter lipoprotein patterns, with increases in low-density lipoprotein cholesterol and decreases in high-density lipoprotein cholesterol. Simultaneously, visceral fat accumulation accelerates, with women gaining an average of 0.5kg of fat mass annually during this transition despite stable or even reduced caloric intake.²⁸
Central adiposity during perimenopause results primarily from redistribution rather than simply increased total fat. This shift from gynoid (lower body) to android (central) distribution carries significant metabolic consequences, as visceral fat demonstrates greater metabolic activity than subcutaneous deposits.²⁸
Muscle mass preservation becomes increasingly important during this transition, as sarcopenia accelerates with diminishing estrogen levels. Lean mass typically declines 0.5%-1% annually >40-years, increasing to 1%-2% annually during perimenopause. This loss reduces basal metabolic rate by ~50-100 calories daily per decade, contributing to weight gain even with stable dietary intake.²⁸
Prevention strategies should emphasise maintaining muscle mass through resistance training, optimising nutrition with emphasis on protein adequacy and anti-inflammatory food patterns, and regular cardiometabolic screening. Resistance training twice weekly
preserves lean mass and resting metabolic rate while improving insulin sensitivity independent of weight change.²⁸
Nutritional approaches should also address bone health, with emphasis on nutrient-dense whole foods rather than caloric restriction alone. Mediterranean dietary patterns demonstrate particular benefit during perimenopause, reducing metabolic syndrome risk by 30%-40% while supporting bone density and CV health.²⁸
The midlife bone shake-up: How perimenopause chips away at skeletal strength
Accelerated bone loss begins around two- to three-years before the final menstrual period, with annual losses of 1.8%-2.3% in the spine and 1%-1.4% in the hip during the perimenopausal transition. This acceleration results from declining oestrogen levels, which increase bone resorption relative to formation. Over the menopause transition, women lose 10%-12% of bone mineral density (BMD), increasing fracture vulnerability.²⁹
Oestrogen’s protective effects on bone operate through multiple mechanisms, including inhibition of osteoclast activity, regulation of inflammatory cytokines that influence bone turnover, and modulation of calcium handling in the intestines and kidneys. As oestrogen levels decline, osteoclast activity increases by 50%90%, while osteoblast function remains unchanged, creating an imbalance that favours net bone loss.²⁹
Trabecular bone, which predominates in vertebrae and the femoral neck, demonstrates particular vulnerability during perimenopause due to its higher surface area and metabolic activity. This pattern explains the increased prevalence of vertebral and hip fractures in postmenopausal women.²⁹
Risk factors for accelerated bone loss include low peak bone mass, family history of osteoporosis, low body weight (BMI <20), smoking, excessive alcohol consumption, and medical conditions affecting bone metabolism. Women with premature ovarian insufficiency or extended periods of amenorrhoea demonstrate particularly high risk.²⁹
Prevention strategies include adequate calcium and vitamin D intake, weight-bearing and resistance exercises, and consideration of pharmacologic therapy for women with significant risk factors. Calcium requirements increase to 1200mg daily during perimenopause, with emphasis on dietary sources supplemented as needed to reach targets. Vitamin D (800-1000 IU daily) optimises calcium absorption and directly supports bone mineralisation.²⁹
Exercise interventions combining impact activities with progressive resistance training demonstrate the greatest efficacy for bone preservation. Impact forces stimulate osteoblast activity through mechanotransduction, while resistance training provides both direct skeletal loading and indirect benefits through musclebone interactions.²⁹
Fifty plus flair: Balancing bones, beats, and brainwaves
Hot flushes and hard facts: Untangling the menopause maze
Menopause, defined as 12 consecutive months of amenorrhoea resulting from permanent cessation of ovarian function, typically occurs between ages 45- to 55-years. VSM affect up to 80% of women, with duration averaging seven- to 10-years but
extending >10-years for ~10% of women. Contrary to previous assumptions, recent studies demonstrate that VSM often begin during perimenopause and may persist well into the postmenopausal period.³⁰
The pathophysiology of VSM involves hypothalamic thermoregulatory dysfunction resulting from estrogen withdrawal. Norepinephrine and serotonin serve as key neurotransmitters in this process, explaining the efficacy of certain antidepressants in symptom management.³¹
Genitourinary syndrome of menopause (GSM), characterised by vaginal dryness, dyspareunia, and urinary symptoms, affects up to 50% of postmenopausal women and, unlike VSM, tends to worsen progressively without treatment. The urogenital tissues are particularly sensitive to oestrogen deprivation, with changes including epithelial thinning, decreased vascularisation, altered pH, and reduced elasticity.³²
Sleep disturbances affect 40%-60% of women during menopause, resulting from both primary effects of oestrogen withdrawal on sleep architecture and secondary disruption from VSM. Decreased oestrogen alters circadian rhythm regulation and reduces production of melatonin, while progesterone decline diminishes its sedative and anxiolytic effects.³²
Management options include menopausal hormone therapy (MHT), which remains the most effective treatment for VSM and provides additional benefits for bone health and cognitive function when initiated within 10-years of menopause. Oestrogen therapy reduces VSM by 75%-80% compared to placebo, with most women experiencing significant relief within four- to 12-weeks of initiation.33,34
Current approaches to MHT emphasise individualized riskbenefit assessment and the timing hypothesis, which suggests that CV effects depend on timing of initiation relative to menopause onset. Women starting MHT within 10-years of menopause demonstrate neutral or favourable CV profiles, while delayed initiation may increase risk.³⁵
Non-hormonal options including SSRIs/SNRIs, gabapentinoids, and CBT provide alternatives for women with contraindications to MHT. Selected SSRIs/SNRIs reduce hot flash frequency by 30%60% compared to placebo, with paroxetine, escitalopram, and venlafaxine showing greatest efficacy.³⁶⁻³⁸
Localised oestrogen therapy effectively addresses GSM with minimal systemic absorption, while moisturisers and lubricants provide symptomatic relief. Vaginal oestrogen preparations (creams, tablets, rings) restore epithelial thickness, normalize pH, and improve blood flow to urogenital tissues, resulting in symptom improvement in 80%-90% of women within 12-weeks.³⁹
A personalised approach considering symptom burden, QoL impact, and individual risk factors optimises outcomes during this transition. Regular reassessment of treatment efficacy and safety profile ensures appropriate management throughout the postmenopausal years.³⁹
Matters of the heart: When menopause upsets the CV balance
CV disease risk accelerates following menopause, with oestrogen loss impacting vascular function, lipid metabolism, and glucose homeostasis. The protective effect of oestrogen on the CV system diminishes, revealing underlying risk factors that may have
been partially masked during reproductive years. This transition contributes to women’s lifetime CV risk equaling that of men by age 55- to 60-years, despite earlier advantages.⁴⁰
Oestrogen exerts cardioprotective effects through multiple mechanisms, including improved endothelial function, reduced vascular inflammation, favourable lipid profiles, and enhanced insulin sensitivity. The loss of these benefits during menopause results in increased vascular stiffness, endothelial dysfunction, and accelerated atherosclerosis.⁴⁰
Women experience unique CV presentations, with higher prevalence of microvascular disease and non-obstructive coronary artery disease compared to men. These sexspecific patterns contribute to diagnostic challenges, as traditional stress testing may yield false negative results despite significant microvascular pathology.⁴¹
Symptoms often include atypical chest pain, dyspnoea, and fatigue rather than classic angina, contributing to diagnostic delays. Women experience an average delay of 37 minutes longer than men from symptom onset to hospital presentation for acute coronary syndromes, with subsequent delays in diagnosis and treatment.⁴¹
loss, kyphosis, reduced pulmonary function, and chronic pain with cumulative impact on quality of life.⁴³
Fracture risk assessment tools such as FRAX® incorporate clinical risk factors to guide intervention decisions. These tools consider factors including age, BMI, previous fracture, parental hip fracture, current smoking, glucocorticoid use, rheumatoid arthritis, secondary osteoporosis causes, and alcohol consumption, generating 10-year probability estimates for major osteoporotic fractures and hip fractures specifically.⁴⁴
Prevention strategies include ensuring adequate calcium (10001200mg daily) and vitamin D (800-1000 IU daily) intake, regular weight-bearing and resistance exercise, smoking cessation, and moderation of alcohol consumption. Nutritional approaches should emphasise food sources of calcium where possible, including dairy products, fortified plant milks, leafy greens, and small fish consumed with bones.45,46
Menopausal weight gain of 2-5kg stems from hormonal changes, lower energy use, and visceral fat increase – increasing cardiometabolic risk independent of overall weight
Preventive strategies should address sexspecific risk factors including autoimmune conditions, and premature menopause. A history of pre-eclampsia confers similar CV risks to smoking, doubling lifetime risk for heart disease and stroke. Similarly, premature menopause increases CV risk by 50%, with earlier onset correlating with greater risk.⁴¹
Depression and psychosocial stress demonstrate stronger associations with CV outcomes in women compared to men, with depression conferring 1.7-fold increased risk for coronary events in women versus 1.3-fold in men. These mental health conditions not only serve as independent risk factors but also influence adherence to preventive measures and medical therapy.⁴¹
Regular screening for traditional risk factors with sex-specific interpretation of results optimises risk stratification and intervention timing. Blood pressure targets during menopause may require adjustment, as women demonstrate steeper increases in systolic pressure during this transition.⁴¹
Osteoporosis: The silent saboteur behind every fragile fall
Osteoporosis affects ~23% of women >50-years, with prevalence increasing to 44% among those ≥80-years. Accelerated bone loss continues for around five- to seven-years following menopause, resulting in average losses of 10%-12% of bone mass during this period. The clinical significance of these losses manifests in fragility fractures, which occur in ~50% of women over their remaining lifetime if preventive measures are not implemented.42,43
Fracture consequences extend far beyond acute pain and temporary disability, significantly impacting long-term function, independence, and survival. Hip fractures carry particular severity, with 20% mortality within the first year and only 40% of survivors regaining pre-fracture functional status. Vertebral fractures, though often clinically silent initially, lead to progressive height
Exercise interventions combining impact activities with progressive resistance training provide greatest benefit for bone preservation and fall prevention. Weight-bearing aerobic activities stimulate bone formation through gravitational loading, while resistance training applies direct mechanical stress to the skeleton while simultaneously strengthening muscles that support and protect vulnerable sites.⁴⁶
Pharmacologic options include antiresorptive agents (bisphosphonates, denosumab) and anabolic therapies (teriparatide) for those at high fracture risk. Bisphosphonates remain first-line therapy for most postmenopausal women with osteoporosis, reducing vertebral fracture risk by 40%-70% and non-vertebral fracture risk by 20%-40% over three- to five-years of treatment.47,48
Treatment decisions should balance fracture reduction benefits against potential adverse effects, with periodic reassessment of risk-benefit ratio. Long-term bisphosphonate therapy raises concerns regarding rare complications including atypical femoral fractures and osteonecrosis of the jaw, leading to consideration of drug holidays after three- to five-years in moderate-risk patients with stable BMD.⁴⁸
Screening after 50:
Balancing the cancer catch with the complications
Cancer screening recommendations evolve with advancing age, requiring recalibration of risk-benefit assessments. BCa screening through biennial mammography is recommended for women aged 50- to 74-years with average risk, while CCa screening intervals lengthen >30-years and may be discontinued >65-years with adequate prior negative screening. These adjustments reflect changing incidence patterns and competing mortality risks with advancing age.⁴⁹
CCa screening transitions from cytology alone to cytology with HPV co-testing or primary HPV testing at age 30, with extended intervals (three- to five-years) for women with normal results. After age 65-years, screening may be discontinued following adequate negative prior screening (three consecutive negative cytology
results or two consecutive negative co-tests within the previous 10-years, with the most recent test within five-years).⁴⁹
Colorectal cancer screening should continue through age 75 for most women, with options including colonoscopy, sigmoidoscopy, and stool-based tests. Colonoscopy every 10-years and annual faecal immunochemical testing represent the most common approaches, with comparable mortality reduction when performed according to recommended intervals.⁴⁹
Lung cancer screening with low-dose computed tomography is recommended for long-term smokers aged 50- to 80-years with significant pack-year history (≥20 pack-years for current smokers or those who quit within the past 15-years). This recent addition to screening guidelines reduces lung cancer mortality by 20%-25% in high-risk populations, with greatest benefit for current smokers.⁴⁹
The midlife weight trap:
When hormones, muscles, and metabolism join forces
Weight gain during the menopausal transition averages 2kg-5kg, primarily attributed to hormonal changes, decreased energy expenditure, and redistribution of fat toward visceral deposits. This central adiposity increases cardiometabolic risk independent of total weight gain. The timing of weight changes often aligns with hormonal transitions rather than chronological age, with accelerated fat accumulation beginning during perimenopause and continuing into early postmenopause.⁵⁰
Metabolic rate declines ~2% per decade >50-years, with both age-related and menopause-specific factors contributing to this reduction. Declining oestrogen levels decrease energy expenditure through direct effects on hypothalamic regulation and indirect effects on body composition.⁵¹
Sarcopenia accelerates during this period, with muscle mass declining ~0.5%-1% annually >50-years. This loss contributes to decreased resting metabolic rate and functional capacity, creating
a cycle of declining physical activity and increasing adiposity. By age 80, women typically lose 20%-40% of peak muscle mass, with strength declining even more precipitously at 1%-3% annually.⁵²
Physical activity levels often decline during this transition, further exacerbating metabolic challenges. Objective measurement studies demonstrate that total daily energy expenditure decreases 20%-30% between ages 50-70, primarily due to reduced activity rather than lower resting metabolism.⁵²
Intervention strategies should emphasise preservation of muscle mass through adequate protein intake (1g-1.2g/kg daily) and progressive resistance training. Protein requirements increase with age due to anabolic resistance, requiring higher intake to stimulate muscle protein synthesis.53,54
Resistance training twice weekly maintains muscle mass and metabolic rate while improving insulin sensitivity and functional capacity. Programmes emphasising major muscle groups with progressive overload demonstrate greatest efficacy for preserving lean mass. Combined aerobic and resistance training provides optimal body composition and metabolic outcomes.⁵⁵
Dietary approaches focusing on nutrient density rather than caloric restriction alone optimize body composition outcomes and address the micronutrient needs of ageing women. Mediterranean dietary patterns demonstrate particular benefit, with studies showing 20%-30% lower weight gain during menopause compared to typical Western diets.⁵⁵
The midlife mood shift: When hormones and depression collide
The menopausal transition represents a period of vulnerability for mood disorders, with women having no previous psychiatric history experiencing a two- to four-fold increased risk of depression during perimenopause compared to premenopausal years. Around 16%-23% of women experience clinically significant depressive symptoms during this transition, with risk particularly elevated during late perimenopause when hormonal fluctuations reach maximum amplitude.56,57
Hormonal mechanisms include effects of estrogen fluctuation on serotonergic function, with declining levels reducing serotonin synthesis, transmission, and receptor binding. Oestrogen additionally modulates dopamine, norepinephrine, and GABA systems, collectively influencing mood regulation.⁵⁸
Risk factors include VSM severity, sleep disruption, prior depression, stressful life events, and genetic vulnerability. VSM correlate with depression risk in multiple studies, with women reporting frequent or severe hot flashes demonstrating two- to three-times higher depression prevalence.⁵⁹
Psychosocial factors during midlife, including role transitions, relationship changes, and caregiving responsibilities, contribute additional stress during an already vulnerable period. Women simultaneously navigating parental caregiving and adolescent/young adult children (sandwich generation) demonstrate particularly elevated depression risk.⁶⁰
Treatment approaches include traditional antidepressants, CBT, and MHT, which show particular efficacy for perimenopausal depression with concurrent
VSM. SSRIs and SNRIs demonstrate response rates of 50%-70% in perimenopausal depression, comparable to those seen in premenopausal women.⁶¹⁻⁶³
CBT, mindfulness-based stress reduction, and interpersonal therapy provide non-pharmacologic options with efficacy comparable to medication for mild to moderate depression. These approaches address both mood symptoms and adjustment to midlife transitions, potentially providing more sustainable improvements than medication alone.⁶⁴
Screening for mood disturbances should be integrated into routine care during the menopausal transition, with particular attention to differentiating clinical depression from expected adjustment reactions to this life stage. Tools such as the Patient Health Questionnaire-9 facilitate identification of clinically significant symptoms requiring intervention.⁶⁴
The double trouble of incontinence: A heavy burden on women’s lives
Urinary incontinence affects 25%-45% of women >50-years, with prevalence increasing with age. Stress incontinence predominates in younger postmenopausal women, while urge and mixed incontinence become more common with advancing age. Despite high prevalence, only 25%-30% of affected women seek treatment, often due to embarrassment, normalisation of symptoms as inevitable, or pessimism regarding treatment efficacy.65,66
Postmenopausal status contributes to incontinence through multiple mechanisms, including urogenital atrophy, decreased tissue elasticity, and altered collagen composition in pelvic support structures. Oestrogen receptors exist throughout the lower urinary tract, with receptors in the urethra, trigone, pelvic floor muscles, and connective tissues all responding to menopausal oestrogen decline.⁶⁶
Risk factors include vaginal delivery, obesity, chronic cough, and oestrogen deficiency. Women with BMI >30 demonstrate two- to three-fold increased incontinence risk, with each five-unit BMI increase raising risk by 30%-60%. Mechanical effects of increased abdominal pressure combine with metabolic factors including chronic inflammation and insulin resistance to impact bladder and urethral function.⁶⁷
First-line management includes pelvic floor muscle training, which demonstrates efficacy for both stress and urge components. Supervised programmes produce superior outcomes compared to self-directed exercises, with 60%-70% improvement rates for stress incontinence and 40%-50% for urge incontinence following 12-week structured programmes.⁶⁸
Bladder training, weight loss when appropriate, and treatment of contributing factors such as constipation provide additional benefit. Bladder training protocols gradually extend intervals between voids, improving functional bladder capacity and reducing urgency. Combined approaches addressing multiple risk factors demonstrate additive benefits.⁶⁸
Pharmacologic options for urge incontinence include antimuscarinic agents and β3-adrenergic agonists, while surgical approaches may be considered for stress incontinence refractory to conservative measures. Antimuscarinic drugs reduce detrusor overactivity through blockade of
muscarinic receptors, improving capacity and reducing urgency episodes by 60%-70%.⁶⁹
Midurethral slings represent the most common surgical intervention for stress incontinence, with 85%-90% objective success rates and 75%-85% patient satisfaction at five-years. Minimally invasive approaches including single-incision techniques and outpatient procedures have expanded options while reducing recovery time.⁶⁹
Vaginal oestrogen therapy addresses the component related to urogenital atrophy, improving tissue integrity and urethral function. Local therapy increases urethral vascularity, improves epithelial thickness, and enhances connective tissue elasticity without significant systemic absorption.⁶⁹
Brain health: Reproductive milestones and dementia
Emerging research highlights significant connections between reproductive history, hormonal transitions, and cognitive health in women. Premature or early menopause increases dementia risk by ~50% compared to women experiencing menopause at typical ages (50- to 52-years). With each year of earlier menopause onset, risk increases by about 3%, highlighting the neuroprotective effects of oestrogen.⁷⁰
Oestrogen’s beneficial effects on brain health operate through multiple mechanisms, including promotion of neuronal growth and synapse formation, enhancement of cerebral blood flow, reduction of oxidative stress, and modulation of neurotransmitter systems. These effects collectively support cognitive resilience throughout the ageing process.⁷⁰
Women’s longer lifespan paradoxically contributes to their higher lifetime dementia risk, with >60% of Alzheimer’s disease cases occurring in women. This disparity reflects both increased longevity and biological vulnerabilities related to hormonal transitions and genetic factors, including the apolipoprotein E allele which confers greater Alzheimer’s risk in women than men.⁷⁰
Preventive strategies include maintenance of CV health, as cerebrovascular disease contributes significantly to cognitive decline. Regular physical activity, Mediterranean-style dietary patterns, cognitive stimulation, and social engagement demonstrate protective effects against cognitive deterioration. Additionally, management of metabolic risk factors including diabetes, hypertension, and dyslipidemia supports both CV and brain health.⁷⁰
MHT may offer cognitive benefits when initiated during the perimenopausal transition or early postmenopause (within 10-years of final menstrual period), though evidence remains mixed regarding long-term cognitive outcomes. For women with premature or early menopause, MHT until the typical age of menopause may mitigate increased dementia risk associated with extended oestrogen deprivation.⁷⁰
Conclusion
Women’s health evolves across the lifespan, requiring age-specific care while ensuring continuity. Early decades focus on reproductive health, later shifting to metabolic and age-related concerns after menopause. Preventive care remains central, as early intervention influences long-term outcomes.
References available on request. SF
RRR IN STROKE/SE 6 HR 0.80 (95% CI, 0.73-0.89)
434 ,046 PATIENTS 6
Favourable safety with uncompromised efficacy
For ELIQUIS®(apixaban) prescribing information, scan the QR code
References:
To access the ELIQUIS® (apixaban) website, scan the QR code
The reference standard here refers to the innovator molecule. (Watson J, et al. Drugs. 2011;71(15):2079-2089). SE: Systemic embolism. RRR: Risk rate reduction. HR: Hazard ratio. CI: Confidence interval.
2. Granger CB, et al. N Engl J Med. 2011;365(11):981-92. 3. Ruff CT, et al. Lancet. 2014;383(9921):955-62.
4. Cohen AT, et al. Adv Ther. 2014;31:473-93. 5. Agnelli G, et al. N Engl J Med. 2013;369(9):799-808. 6. Lip GYH, Et al. Stroke. 2018(12):2933-2944. Erratum in: Stroke. 2020;51(2):e44. Erratum in: Stroke. 2020;51(4):e71.
This image is for representation purpose only. For the use only of a Registered Medical Practitioners or a Hospital or a Laboratory.
S4 ELIQUIS® 2,5 MG AND 5 MG FILM-COATED TABLETS (REG. NO’S: 47/8.2/0463, 0464). EACH FILM-COATED TABLET CONTAINS EITHER 2,5 MG OR 5 MG APIXABAN.
To report an adverse event, please contact ZAF.AEReporting@pfizer.com If you wish to contact Pfizer for any other purpose, please use contact details below. +2711 320 6000 or 0860 734 937 (SA). Monday-Friday 09h00-17h00.
Clot control in cancer
Venous thromboembolism (VTE) is a frequent complication in cancer, affecting up to 15% of patients during the course of their disease – irrespective of cancer type. VTE, which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is the secondleading cause of death after the malignancy itself. The incidence of VTE is five- to seven-times higher than in non-cancer populations, with 12.3 per 1000 cancer patients developing VTE within the first six months after diagnosis.1,2
The risk of VTE in cancer is linked to a hypercoagulable state, which is further aggravated by repeated chemotherapy (ChT) via central or peripheral venous catheters, vascular endothelial injury, tumour-induced blood flow obstruction, release of procoagulant microparticles, comorbidities, advanced age, and reduced mobility.2
Breast, lung, colon, and prostate cancers account for the greatest burden of active cancer-associated VTE. Compared with VTE in non-cancer patients, cancer-associated VTE is linked to a significantly higher risk of both recurrence and major bleeding.3 According to Cohen et al, because of the high risk of recurrent VTE beyond the initial three months of anticoagulant therapy,
Photo
patients with VTE and active cancer generally require at least six months of anticoagulation. Extended treatment should be considered until the cancer is cured or in remission, provided the patient does not have a high bleeding risk.3
Historically, low molecular weight heparins (LMWH) have served as the cornerstone of treatment for cancer-associated VTE. However, the introduction of non-vitamin K oral anticoagulants (NOACs) has provided new therapeutic options with potential advantages including oral administration, predictable pharmacokinetics, and reduced monitoring requirements.2,4,5
Apixaban: Predictable, powerful, and patient-friendly
Apixaban, a selective factor Xa inhibitor, has garnered significant attention for its favourable efficacy and safety profile. Apixaban has an absolute oral bioavailability of ~50%, which is not meaningfully affected by food. Drug exposure increases proportionally with doses up to 10mg. It is rapidly absorbed, reaching peak plasma concentrations within three- to four-hours, and has a half-life of about 12-hours.6,7
Elimination occurs through multiple pathways, including metabolism, biliary excretion, and direct intestinal excretion, with renal clearance accounting for ~27% of total elimination. Its pharmacokinetics are consistent across diverse patient populations, and clinically relevant drug–drug interactions are limited, enabling the use of fixed dosing without therapeutic monitoring.7
Tackling clots head-on: Strategies for treating established VTE
Active Malignancy-Associated Venous Thromboembolism (ADAM) study. The study reported no major bleeding events in participants treated with apixaban, compared with 1.4% of those receiving dalteparin. Recurrent VTE occurred in 0.7% of participants in the apixaban group versus 6.3% in the dalteparin group, demonstrating a significantly lower risk with apixaban. For the composite bleeding outcome of major or clinically relevant non-major bleeding, events occurred in 6% of participants in both groups, with no significant difference observed.8
Real-world evidence from a comprehensive analysis of 14 086 cancer patients across four American commercial health insurance databases further substantiated these findings. Compared with LMWH, apixaban was associated with a lower risk of recurrent VTE (hazard ratio [HR] 0.61), major bleeding (HR 0.63), and clinically relevant non-major bleeding (HR 0.81).3
Apixaban combines favourable efficacy and safety with predictable pharmacokinetics, rapid absorption, food-independent bioavailability, proportional dosing, and a convenient 12-hour half-life
Recent evidence from large-scale population-based studies has demonstrated apixaban’s effectiveness in primary VTE prevention among cancer patients. An analysis of national health insurance data involving 47 216 cancer patients revealed that NOACsparticularly apixaban - significantly reduced VTE risk with an overall odds ratio (OR) of 0.40 compared to no anticoagulation. This protective effect was particularly pronounced for DVT (OR = 0.38), while PE reduction showed less consistent results.2
The efficacy of apixaban extended across various patient subgroups, including both male and female patients and those with increased VTE risk scores according to the Khorana index (≥1, see Table 1) . Importantly, patients undergoing high-risk ChT regimens demonstrated particularly robust responses to apixaban therapy, with the drug showing superior efficacy compared to warfarin in this high-risk population (OR = 0.19).2
In the therapeutic setting, apixaban has demonstrated noninferiority to standard anticoagulation regimens. The landmark Apixaban for the Treatment of Venous Thromboembolism in Patients with Cancer (CARAVAGGIO) trial, examining NOACs in cancerassociated thrombosis, showed that apixaban achieved a recurrent VTE rate of 5.6% compared to 7.9% for dalteparin, establishing noninferiority while maintaining comparable safety profiles.6
This finding was corroborated by the Apixaban and Dalteparin in
Participants receiving warfarin had risks of recurrent VTE, major bleeding, and clinically relevant non-major bleeding similar to LMWH. Compared with warfarin, apixaban reduced the risk of recurrent VTE (HR 0.68), while risks of major bleeding (HR 0.73) and clinically relevant non-major bleeding (HR 0.89) were similar. Over the entire follow-up (mean 3.5–5.5 months, maximum ~3–3.3 years), findings were consistent, with apixaban showing a significantly lower risk of major bleeding compared with warfarin (HR 0.72).
3
Carrier et al conducted a randomised, double-blind, placebo-controlled trial evaluating apixaban (2.5mg twice daily) for thromboprophylaxis in ambulatory cancer patients at intermediate-to-high risk for VTE (Khorana score ≥2) initiating ChT. The primary efficacy outcome was objectively confirmed VTE over 180 days, and the main safety outcome was major bleeding.9
VTE occurred in 4.2% of participants receiving apixaban versus 10.2% receiving placebo. Major bleeding occurred in 3.5% of participants on apixaban and 1.8% on placebo. During the treatment period, major bleeding was 2.1% with apixaban versus 1.1% with placebo. The authors concluded that apixaban significantly reduced the risk of VTE compared with placebo in this high-risk ambulatory cancer population, though the incidence of major bleeding was increased.9
Clotting the dots: What ESMO recommends
According to the 2023 European Society of Medical Oncology (ESMO) guideline, oral factor Xa inhibitors may be considered a viable alternative to LMWH for the treatment of cancer-associated VTE10p9. For the acute phase of cancer-associated VTE, LMWH, unfractionated heparin (UFH), fondaparinux, apixaban, or rivaroxaban are recommended. LMWH is preferred over UFH or fondaparinux. UFH may be considered in patients with severe renal impairment (creatinine clearance [CrCl] <30 mL/min).10
Long-term anticoagulation for at least six months should preferably be with LMWH, apixaban, or rivaroxaban rather than vitamin K antagonists (VKAs), which may be used only if LMWH or direct factor Xa inhibitors are unavailable.10
In patients with luminal gastrointestinal (GI) or urothelial cancers, LMWH is preferred, particularly in those at high risk of GI bleeding or receiving drugs affecting P-glycoprotein or cytochrome P450 3A4 (CYP3A4), a key enzyme in the liver and intestines responsible for metabolising many drugs, while oral factor Xa inhibitors can be considered according to patient preference.10
Extended anticoagulation beyond six months is recommended for patients with active cancer who remain at high risk of recurrent VTE, with regular reassessment of the risk–benefit balance. Incidentally detected VTE should be treated the same as symptomatic VTE, and anticoagulation is suggested for most subsegmental pulmonary emboli, although a watchful approach or shorter course may be appropriate in selected patients with high bleeding risk.10
Vena cava filters may be inserted in cases of acute, life-threatening VTE when anticoagulation is absolutely contraindicated or as an adjunct in recurrent or progressive VTE despite optimal therapy. For catheter-related thrombosis, routine prophylaxis is not recommended.10
Symptomatic cases should receive anticoagulation for a minimum of three months, preferably with LMWH, while VKAs or direct oral anticoagulants may be considered if alternatives are unsuitable. Catheter removal is recommended if it is unnecessary, infected, anticoagulation is contraindicated, or thrombus progresses despite therapy, and extended anticoagulation until catheter removal may be considered for patients with low bleeding risk.10
Clotting with care: Practical consideration for thromboprophylaxis in cancer
When considering pharmacological thromboprophylaxis in cancer patients, shared decision-making is essential, considering the convenience of oral administration, renal and hepatic function, potential drug–drug interactions, and bleeding risk. Special caution is warranted in patients with GI malignancies, particularly if the primary lesion is luminal and unresected.10
The optimal duration of thromboprophylaxis in ambulatory cancer patients is not firmly established. The first three months following cancer diagnosis and initiation of anticancer therapy represent a higher-risk period, during which >50% of VTE venous episodes occur - all major studies have included at least this period.10
Two direct oral anticoagulant studies implemented a six-month thromboprophylaxis period, while studies in pancreatic ductal adenocarcinoma explored up to three months with higher-dose low-molecular-weight heparin.10
Given that these patients often have a Khorana Risk Score of ≥2 and frequently progressive disease, extending thromboprophylaxis with a direct oral anticoagulant up to six months remains evidence-based. Beyond six months, the decision should be individualised based on ongoing risk factors and patientspecific considerations, in line with ESMO guidelines.10
Risk stratification based on total score:
S 0 points → Low risk of VTE
S 1–2 points → Intermediate risk of VTE
S ≥3 points → High risk of VTE.
Risk factor Points assigned Criteria
Primary tumour site +1 or +2 Specific tumour types associated with higher VTE risk
Platelet count +1 ≥350 × 109/L
Haemoglobin/ Erythropoiesis-stimulating agent (ESA) use +1
Haemoglobin ≤100g/l or use of ESA agents
Leukocyte count +1 ≥ 11 × 109/L
Body Mass Index +1 ≥ 35kg/m²
Conclusion
Apixaban represents a compelling alternative to LMWH for both the prevention and treatment of cancer-associated VTE. Evidence from randomised trials, including the Caravaggio and ADAM studies, demonstrates that apixaban effectively reduces the risk of recurrent VTE while maintaining comparable safety profiles, with no significant increase in major bleeding. Real-world data further support its efficacy across diverse patient populations, including those at high thrombotic risk. Oral administration, predictable pharmacokinetics, limited drug–drug interactions, and avoidance of routine monitoring enhance patient convenience and adherence. Current guidelines, including ESMO, recognise apixaban as a viable option for both acute and long-term anticoagulation, with individualised consideration of cancer type, bleeding risk, and patient preference ensuring optimal clinical outcomes.
References
1. van der Hulle T, et al Effectiveness and safety of novel oral anticoagulants compared to vitamin K antagonists in cancer patients with acute venous thromboembolism: A systematic review and meta-analysis. J Thromb Haemost, 2014.
2. Choi YJ, et al Effectiveness and safety of novel oral anticoagulants versus conventional anticoagulation in cancer patients: A population-based analysis. Risk Management and Healthcare Policy, 2021.
3. Cohen AT, et al Real-world effectiveness and safety of apixaban, low-molecularweight heparin, and warfarin in cancer patients with venous thromboembolism: A comparative analysis of commercial health insurance databases. Thromb Haemost, 2021.
4. Lee SH, et al. Cancer-associated thrombosis: Treatment challenges and emerging therapeutic approaches in oncology patients. Blood First, 2013.
5. Wumaier A, et al Novel oral anticoagulants in cancer-associated thrombosis: A comprehensive review of efficacy, safety, and clinical outcomes. Drug Design, Development and Therapy, 2022.
6. Agnelli G, et al Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. NEJM, 2020.
7. Byon W, et al. Apixaban: A Clinical Pharmacokinetic and Pharmacodynamic Review. Clinical Pharmacokinetics, 2019.
8. McBane RD, et al. Apixaban and dalteparin in active malignancyassociated venous thromboembolism: The ADAM VTE trial. JTH, 2019.
9. Carrier M, et al Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. NEJM, 2019.
10. Falanga A, et al Venous thromboembolism in cancer patients: ESMO Clinical Practice Guideline. Annals of Oncology, 2023.
11. Mulder FI, et al. CAT-prediction collaborators. The Khorana score for prediction of venous thromboembolism in cancer patients: a systematic review and meta-analysis. Haematologica, 2019. SF
Table 1: Khorana Risk Score
Mastering the switch
between anticoagulants with precision and safety
Atrial fibrillation (AFib), characterised by chaotic and irregular electrical activity in the upper chambers of the heart, is the most common heart dysrhythmia worldwide. The prevalence of AFib is increasing due to the growing ageing population. Between 2010 and 2019, the global prevalence of AFib increased from 33.5 million to 59 million. This trend is expected to continue in the coming decades.1,2
Non-valvular AFib (NVAF) - AFib without rheumatic valvular disease - is the most common type and is a strong independent predictor of stroke. Apart from stroke (5-fold), individuals living with AFib are at increased risk of myocardial infraction (MI, 2-fold), heart failure, as well as dementia and cognitive decline.1,2
NOACs compared to warfarin
The main goal in managing AFib is stroke prevention. Oral anticoagulants (OACs) are recommended to mitigate the risk of stroke and reduce overall mortality. Before the development of direct OACs or non-vitamin K antagonists (NOACs) such as apixaban, dabigatran, and rivaroxaban, vitamin K antagonists (VKAs) such as warfarin, was the standard of care for stroke prevention in individuals living with NVAF. However, since the launch of NOACs more than a decade ago, numerous studies have shown that these agents are not only more convenient for patients, but also have similar or better efficacy and safety profiles than warfarin.1,3
The largest observational study to date comparing NOACs (apixaban, dabigatran, rivaroxaban) and warfarin titled A nticoagulants for Reduction in Stroke: Observational Pooled Analysis on Health Outcomes and Experience of Patients), included 434 046 participants living with NVAF. The study compared the safety and efficacy of NOACs compared to warfarin in reducing the risk of stroke/systemic embolism (SE) and major bleeding (MB).3
The study matched six cohorts: 100 977 patient pairs for apixaban-warfarin, 36 990 for dabigatran-warfarin, 125 068 for rivaroxaban-warfarin, 37 314 for apixaban-dabigatran, 107 236 for apixaban-rivaroxaban, and 37 693 for dabigatran-rivaroxaban. Results showed that compared to warfarin, apixaban (hazard ratio [HR] 0.64), dabigatran (HR 0.82), and rivaroxaban (HR 0.79) were associated with lower rates of stroke/SE. Apixaban (HR 0.60) and dabigatran (HR 0.71) had lower rates of MB compared to warfarin, while rivaroxaban (HR 1.06) had a higher rate compared to warfarin.3
Apart from the lower rates of stroke/SE, and MB shown with
apixaban and dabigatran, NOACs are associated with fewer monitoring requirements, less frequent follow-up, more immediate drug onset and offset effects (important for peri-procedural and acute bleeding management), as well as fewer drug and food interactions.4
Patterns of OAC switching
As mentioned, prior to the launch of NOACs, VKAs were the only options for OACs in patients living with AFib. Since the launch of NOACs, these agents are increasingly being used. However, caution Kefale et al (2021), switching from one OAC to another, can negatively affect clinical outcomes and healthcare costs.5
The team conducted a comprehensive review on the patterns of OAC switching in patients living with NVAF patients, possible rationales for switching, associated clinical outcomes, and predictors of switching.5
They found that switching rates differed notably between specific OACs: Dabigatran users had the highest rates, while apixaban users had lower rates.
Switching was highest within the first three months of OAC initiation but continued to increase with longer follow-up. For VKAs, switching rates ranged from 2.7% to 33.8% within a year, while NOAC rates were 4.9%-14.9% combined. The highest recorded switching rate for DOACs was 19.6% within 24 months. Notably, patients on VKAs frequently switched to apixaban, rivaroxaban or dabigatran.5
The team found that the decision to switch is influenced by various clinical or patient-related factors. A 2021 Danish study involving 50 623 participants found that clinical events contributing to switches from VKAs to NOACs included thrombotic complications, bleeding, anaemia, new contraindications, and procedures to restore sinus rhythm.5
Another study investigating switching from warfarin to a NOAC, found that among patients initially treated with warfarin, 3.7% switched due to ease of use. Ease-of-use issues included unstable international normalised ratio (INR), frequent monitoring, poor adherence, dietary restrictions, and side effects.5
In terms of clinical outcomes, Kefale et al found that switching from warfarin to dabigatran resulted in a reduced rate of gastrointestinal (GI) bleeding with a hazard ratio (HR) of 0.69 and intracranial haemorrhage (ICH) with an HR of 0.53. It was also associated with a 43% reduction in all-cause mortality. However, there was no significant difference in the rate of ischaemic stroke (IS, HR 1.19).5
An Italian study examined the effectiveness and safety of switching from a VKA to a NOAC in patients with a CHA2DS2VASc score ≥2. These patients had been on a VKA for at least six months before switching and were followed for at least six months post-switching. Switchers experienced a 50% lower risk of CV events (HR 0.5) and a 50% lower risk of bleeding (HR 0.5).5
Another study focused on switching from apixaban to warfarin found that a higher proportion of switchers experienced major bleeding (8.2% vs 2.2%) and stroke/SE (3.2% vs 1.4%) compared to those who continue apixaban.5
A large retrospective cohort study with 55 749 patients assessed the clinical outcomes of switching from warfarin to rivaroxaban. Patients who switched to rivaroxaban (n=11 845) were matched with warfarin-only users (n=43 904) using propensity scoring. Switchers had an increased risk of GI bleeding compared to non-switchers (HR 1.55), which was notably higher in the first 90-days following switching (HR 2.33). There were no significant differences in the rates of IS (HR 1.06), ICH (HR 1.04), or MI (HR 1.08).5
Strategy for switching from warfarin to DOACs
According to Abdelnabi et al, it is safe to promptly initiate NOACs once the INR is ≤2. If the INR is between 2 and 2.5, NOACs can also be started immediately or the following day. However, if the INR is >2.5, it is recommended to consider both the actual INR level and the half-life of warfarin (36–48 hours) to determine the appropriate starting time.6
For apixaban, indicated in South Africa for the prevention of stroke/SE in adult patients living with NVAF who have one or more risk factors such as prior stroke or transient ischaemic attack, age ≥75 years, hypertension, diabetes, or symptomatic HF (New York Heart Association Class ≥II), the following is recommended:7 S Switching treatment from parenteral OACs to apixaban (and
CARDIOLOGY
vice versa) can be done at the next scheduled dose, avoiding simultaneous administration
S When switching from a VKA to apixaban, discontinue VKA therapy and start apixaban when the INR is <2
S When switching from apixaban to VKA therapy, continue apixaban for at least two days after starting VKA therapy. Coadministration should continue until the INR is ≥2, with an INR check prior to the next apixaban dose.
Is it safe to switch from one NOAC to another?
According to Deitelzweig et al, switching between NOACs happens frequently in clinical practice. Patients may switch from one NOAC to another for various reasons as mentioned above. In addition, they may also switch NOACs due to restrictions such as formulary exclusion or increased out-of-pocket costs associated with formulary tier increase.1
risk of stroke/SE and a lower risk of MB vs continuous rivaroxaban treatment. These findings may aid physicians and patients in making informed decisions when considering a switch between apixaban or rivaroxaban.1
Switching between NOACs is common in AFib care, driven by clinical factors and formulary costs, influencing stroke and bleeding risks
To answer the question posed above, the team evaluated stroke/ SE and MB risks among patients living with NVAF continuing or switching to a different NOAC (apixaban and rivaroxaban). The study included data from 264 026 privately insured individuals.1
The study outcomes were stroke/SE and MB events during the follow-up period (10.5 months for apixaban-to-rivaroxaban switchers and 11.5 months for apixaban continuers1p4). Stroke/SE events included IS, haemorrhagic stroke (HS), and SE. MB events included GI bleeding, ICH, and MB at other key sites.1
Among apixaban initiators, the incidence rate of stroke/SE and MB was 1.53 and 4.59, respectively, for those who switched from apixaban to rivaroxaban, compared to 0.75 and 2.44 for those who continued on apixaban. Patients switching from apixaban to rivaroxaban had a higher risk of stroke/SE (HR 1.99) and MB (HR 1.80) compared to apixaban continuers. Specifically, these switchers were at higher risk of IS, HS (HR 2.12), GI bleeding (HR 2.15), and other bleeding (HR 1.50).1
Among rivaroxaban initiators, the incidence rate of stroke/SE and MB was 0.61 and 2.01, respectively, for those who switched to apixaban, compared to 0.78 and 3.89 for those who continued on rivaroxaban. Patients switching from rivaroxaban to apixaban had a similar risk of stroke/SE (HR 0.74) but a lower risk of MB (HR 0.49), GI bleeding (HR 0.44), and other bleeding (HR 0.59.1
The findings of the sensitivity analysis were consistent with those of the main analysis. Among patients who initiated the standard dose of apixaban, those who switched to rivaroxaban had a higher risk of stroke/SE (HR 1.69) and MB (HR 1.76) compared to apixaban continuers. Conversely, among patients who initiated the standard dose of rivaroxaban, those who switched to apixaban had a similar risk of stroke/ SE (HR 0.76), but a lower risk of MB (HR 0.82) compared to rivaroxaban continuers.1
The authors concluded that switching from apixaban to rivaroxaban was associated with a higher risk of stroke/SE and MB vs continuous apixaban treatment, while switching from rivaroxaban to apixaban was associated with a similar
Key messages
Efficacy and safety profiles: NOACs (apixaban, dabigatran, rivaroxaban) have shown comparable or better efficacy in reducing stroke/SE and MB compared to warfarin.3
Reasons for switching : Common reasons for switching include adverse effects, poor anticoagulation control with warfarin, and specific patient preferences. Patients may also switch due to formulary restrictions or changes in drug coverage, impacting both clinical outcomes and healthcare costs.1,5
Switching patterns and timing : Switching rates vary significantly depending on the OAC used initially, with higher rates observed within the first three months and continuing over time.5
Safety of switching : It is generally safe to switch from one NOAC to another, however, clinical outcomes such as stroke/SE and MB risks should be carefully monitored during the transition.1
Timing of switching : When switching from warfarin to NOACs, it is recommended to start NOACs promptly once the INR is ≤2 to minimise the risk of bleeding or thrombotic events.6
Specific considerations for apixaban : When switching from VKAs to apixaban, ensuring the INR is <2 before starting apixaban is recommended to avoid overlapping anticoagulation effects.7
Risk of adverse events: Switching from apixaban to rivaroxaban has been associated with a higher risk of stroke/SE and MB compared to continuous apixaban treatment, whereas switching from rivaroxaban to apixaban showed a lower risk of MB.1
Shared decision-making : Informed decision-making involving both physicians and patients is crucial when considering a switch between OACs to balance risks, benefits, and patient preferences.1
References
1. Deitelzweig S, Kang A, Jiang J, et al Clinical Impact of Switching or Continuation of Apixaban or Rivaroxaban among Patients with Non-Valvular Atrial Fibrillation. J Clin Med, 2024.
2. Linz L Gawalko M, Betz K, et al Atrial fibrillation: epidemiology, screening and digital health. The Lancet, 2024.
3. Lip GYH, Keshishian A, Li X, et al. Effectiveness and Safety of Oral Anticoagulants Among Nonvalvular Atrial Fibrillation Patients. The ARISTOPHANES Study. Stroke, 2018.
4. Chen A, Stecker E, Warden BA. Direct Oral Anticoagulant Use: A Practical Guide to Common Clinical Challenges. Jour Amer Heart Assoc, 2020.
5. Kefale AT, Peterson GM, Bezabhe WM, Bereznicki LR. Switching of oral anticoagulants in patients with nonvalvular Atrial fibrillation: A narrative review. Br J Clin Pharmacol, 2022.
6. Abdelnabi M, Benjanuwattra J, Okasha O, et al. Switching from Warfarin to Direct-Acting Oral Anticoagulants: It is time to move forward! Egypt Heart J, 2022.
7. Professional information. Eliquis. 2023. [Internet]. Available at: https://labeling.pfizer.com/ShowLabeling.aspx?id=12118 SF
RRR IN STROKE/SE 6 HR 0.80 (95% CI, 0.73-0.89)
434 ,046 PATIENTS 6
Favourable safety with uncompromised efficacy
For ELIQUIS®(apixaban) prescribing information, scan the QR code
References:
To access the ELIQUIS® (apixaban) website, scan the QR code
The reference standard here refers to the innovator molecule. (Watson J, et al. Drugs. 2011;71(15):2079-2089). SE: Systemic embolism. RRR: Risk rate reduction. HR: Hazard ratio. CI: Confidence interval.
2. Granger CB, et al. N Engl J Med. 2011;365(11):981-92. 3. Ruff CT, et al. Lancet. 2014;383(9921):955-62.
4. Cohen AT, et al. Adv Ther. 2014;31:473-93. 5. Agnelli G, et al. N Engl J Med. 2013;369(9):799-808. 6. Lip GYH, Et al. Stroke. 2018(12):2933-2944. Erratum in: Stroke. 2020;51(2):e44. Erratum in: Stroke. 2020;51(4):e71.
This image is for representation purpose only. For the use only of a Registered Medical Practitioners or a Hospital or a Laboratory.
S4 ELIQUIS® 2,5 MG AND 5 MG FILM-COATED TABLETS (REG. NO’S: 47/8.2/0463, 0464). EACH FILM-COATED TABLET CONTAINS EITHER 2,5 MG OR 5 MG APIXABAN.
To report an adverse event, please contact ZAF.AEReporting@pfizer.com If you wish to contact Pfizer for any other purpose, please use contact details below. +2711 320 6000 or 0860 734 937 (SA). Monday-Friday 09h00-17h00.
Injection 100 mg
CERVICAL CANCER
KEYTRUDA, in combination with chemoradiotherapy (CRT), is indicated for the treatment of patients with high-risk, locally advanced cervical cancer 1
KEYTRUDA, in combination with chemotherapy with or without bevacizumab, is indicated for the treatment of patients with persistent, recurrent, or metastatic cervical cancer 1
KEYTRUDA, as monotherapy, is indicated for the treatment of patients with recurrent or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥1) as determined by a validated test, with disease progression on or after chemotherapy.1
REFERENCE: 1. KEYTRUDA Approved Professional Information, August 2025.
Learn more about the KNA18 trial (cervical cancer)
See page 208 to 213
SELECTED SAFETY INFORMATION: CONTRAINDICATIONS: KEYTRUDA is contraindicated in patients with hypersensitivity to pembrolizumab or any inactive ingredients, and should not be used during pregnancy and lactation. SPECIAL WARNINGS AND PRECAUTIONS FOR USE: Safety and efficacy not established in children <18 years except for paediatric patients with melanoma or classical Hodgkin Lymphoma (cHL). No dose adjustments needed for elderly patients (≥65 years) or mild-to-moderate renal/hepatic impairment. Use caution in severe renal/hepatic impairment (not studied). No formal pharmacokinetic drug interaction studies exist/ have been conducted. Avoid corticosteroids/immunosuppressants before treatment. Poses fetal risks – use contraception during and 4 months post-treatment. Avoid breastfeeding. SIDE EFFECTS (UNDESIRABLE EFFECTS): Pembrolizumab commonly triggers immune-mediated adverse reactions, most resolving with appropriate treatment or discontinuation. The adverse events were assessed across tumour types. Monotherapy (7,631 patients, 8.5 months median observation): Very common adverse reactions included Blood and lymphatic system disorders: anaemia; Endocrine disorders: hypothyroidism; Metabolism and nutrition disorders: decreased appetite; Nervous system disorders: headache; Respiratory, thoracic and mediastinal disorders: dyspnoea, cough; Gastrointestinal disorders: diarrhoea, abdominal pain, nausea, vomiting, constipation; Skin and subcutaneous tissue disorders: pruritus, rash; Musculoskeletal and connective tissue disorders: musculoskeletal pain, arthralgia; General disorders and administration site conditions: fatigue, asthenia, oedema, pyrexia. Mostly Grades 1 or 2 in severity. Severe adverse reactions included immune- mediated and severe infusion-related reactions. Combination with Chemotherapy or chemoradiotherapy (CRT) (6,093 patients): Very common adverse reactions included: Blood and lymphatic system disorders: anaemia, neutropenia, thrombocytopenia; Endocrine disorders: hypothyroidism; Metabolism and nutrition disorders: hypokalaemia, decreased appetite; Psychiatric disorders: insomnia; Nervous system disorders: neuropathy peripheral, headache, dizziness; Respiratory, thoracic and mediastinal disorders: dyspnoea, cough; Gastrointestinal disorders: diarrhoea, nausea, vomiting abdominal pain, constipation; Skin and subcutaneous tissue disorders: alopecia, pruritus, rash; Musculoskeletal and connective tissue disorders: musculoskeletal pain, arthralgia; General disorders and administration site conditions: fatigue, asthenia, pyrexia, oedema; Investigations: alanine aminotransferase increased, aspartate aminotransferase increased, blood creatinine increased. Combination with tyrosine kinase inhibitor (TKI) (1,456 patients): Very common adverse reactions include: Infections and Infestations: urinary tract infection; Blood and lymphatic system disorders: anaemia; Endocrine disorders: hypothyroidism; Metabolism and nutrition disorders: decreased appetite; Nervous system disorders: headache, dysgeusia; Vascular disorders: hypertension; Respiratory, thoracic and mediastinal disorders: dyspnoea, cough; Gastrointestinal disorders: diarrhoea, vomiting abdominal pain, nausea, constipation; Skin and subcutaneous tissue disorders: rash, pruritus; Musculoskeletal and connective tissue disorders: arthralgia, musculoskeletal pain, myositis, pain in extremity; General disorders and administration site conditions: fatigue, asthenia, oedema, pyrexia; Investigations: lipase increased, alanine aminotransferase increased, aspartate aminotransferase increased, blood creatinine increased. Immune-mediated adverse reactions across various doses reported included pneumonitis, colitis, hepatitis, nephritis, endocrinopathies and Severe skin reactions. Other immune-mediated adverse reactions reported in less than 1 % of patients treated included uveitis, myositis, Guillain-Barré syndrome, pancreatitis, encephalitis, sarcoidosis, myasthenic syndrome/myasthenia gravis (including exacerbation), myelitis vasculitis, hypoparathyroidism, gastritis, haemolytic aneamia and pericarditis. Immune-mediated adverse reactions reported in post-marketing use included myocarditis, sclerosing cholangitis, optic neuritis and exocrine pancreatic insufficiency.
Pembrolizumab’s
new role in high-risk
locally advanced CCa
Globally, in 2022, an estimated 662 044 new cervical cancer cases were diagnosed, with an age-standardised incidence of 14.12 per 100 000 population, and 348 709 deaths occurred, corresponding to an age-standardised mortality of 7.08 per 100 000.2 According to the 2025 GLOBOCAN Report, Southern Africa has the second-highest CCa incidence globally at 34.89 per 100 000 population.2
Over 85% of new cases and 90% of deaths occurred in women aged ≥40, with late-onset CCa showing incidence and mortality rates 10-fold and 20-fold higher, respectively, than early-onset cases.
2
When detected early, CCa has a 5-year relative survival rate of ~92%, yet only around 44% of patients are diagnosed at this stage. Inconsistent screening contributes to delayed diagnosis.3 Survival declines with advancing stage: five-year survival is 60% for local or regional spread and drops to 19% for cases presenting with distant metastases.
3
Persistent infection with high-risk human papillomavirus (HPV), particularly types 16 and 18, is responsible for 71% of CCa cases.2 Other contributing risk factors include smoking, HIV infection, early sexual activity, multiple sexual partners, and use of oral hormonal contraceptives.2 Fortunately, CCa is largely preventable through HPV vaccination and regular screening, which remain the most effective prevention strategies.3
From precursor lesions to advanced disease: The progression of cervical cancer
Squamous cell carcinoma (SCC) and adenocarcinoma (AC) are the most common CCa histologies, with SCC predominating. AC accounts for ~5% of invasive cases globally, though its incidence is rising in some regions. Both subtypes develop from precursor lesions – cervical intraepithelial neoplasia or carcinoma in situ (CIS) – with squamous CIS and AC in situ representing the immediate precursors to invasive disease.3
Most malignancies originate at the squamocolumnar junction and, microscopically, show irregular nests or single tumour cells with stromal inflammation or desmoplasia. Lymphovascular space invasion may also occur. Tumour grading, based on nuclear pleomorphism, nucleoli size, mitotic activity, and necrosis, does not reliably predict prognosis. AC should be distinguished from endometrial AC using immunohistochemistry and HPV in situ hybridisation.3
In stage I disease, the tumour is confined to the cervix, with subclassification determined by depth of invasion. Stage II indicates spread beyond the uterus without extension into the lower vagina, while stage III involves the lower vaginal third, pelvic sidewall, or hydronephrosis. Recognition of nodal involvement as a key prognostic factor has led to the addition of stages IIIC1 and IIIC2, reflecting pelvic and para-aortic nodal disease respectively. Stage IVA represents local invasion into adjacent organs such as the bladder or rectum, whereas stage IVB denotes distant metastases, including nonregional nodal spread.3
Updated guidelines and trial evidence supporting pembrolizumab use in advanced and metastatic CCa
The 2023 guidelines by the European Society of Gynaecological Oncology (ESGO)/the European Society for Radiotherapy and Oncology (ESRO)/European Society of Pathology (ESP) recommend that patients with distant recurrent or metastatic CCa should undergo a comprehensive clinical and diagnostic evaluation to determine the full extent of disease and guide the choice of the most appropriate treatment strategy, including best supportive care where relevant.4
For chemo-naïve, medically fit patients, platinum-based ChT with or without bevacizumab remains the recommended firstline treatment, with carboplatin/paclitaxel or cisplatin/paclitaxel as preferred regimens. The addition of bevacizumab should be considered following thorough assessment and discussion of potential GI and genitourinary toxicities.4
Pembrolizumab may be added to platinum-based ChT, with or without bevacizumab, in patients with PD-L1-positive tumours, defined by a CPS ≥1. For patients who progress after receiving platinum-based ChT, treatment with the anti-PD-1 agent cemiplimab is recommended, regardless of PD-L1 expression, provided they have not received prior immunotherapy.4
Development
Patients presenting with metastatic disease at diagnosis who respond to systemic ChT may be considered for additional radical pelvic radiotherapy (RT), including image-guided brachytherapy in selected cases. Similarly, those with residual oligometastatic disease following systemic therapy may be candidates for sitespecific interventions such as surgery, thermal ablation, or RT. Inclusion of patients with recurrent or metastatic disease in clinical trials is strongly recommended to improve access to novel therapies and optimise outcomes.4
Raising the bar in locally advanced CCa: Pembrolizumab Plus ChT delivers improved survival without compromising QoL
The American Food and Drug Administration granted accelerated approval of pembrolizumab in combination with CrTr for the treatment of patients with FIGO stage III-IVA (locally advanced) CCa in 2024 based on the results of the Pembrolizumab or Placebo With Chemoradiotherapy Followed By Pembrolizumab or Placebo for Newly Diagnosed, High-Risk, Locally Advanced Cervical Cancer (ENGOT-Cx11/GOG-3047/KEYNOTE-A18): A Randomised, DoubleBlind, Phase 3 Clinical Trial.5
According to Lorusso et al (2024) despite treatment with curative intent in patients with persistent, recurrent, or metastatic CCa, prognosis can be poor, five-year rates of progression-free survival (PFS) and overall survival (OS) ranging from 47% to 80% have been reported, with worse disease control rates and survival in patients with an advanced stage of disease or nodal involvement.6
The team evaluate whether pembrolizumab, when administered in combination with and after CrTr, improves efficacy compared with CrTr alone in newly diagnosed, high-risk, locally advanced CCa.
6
This was a randomised, doubleblind, placebocontrolled, phase 3 trial conducted across 176 medical centres in 30 countries,
stages in cervical cancer or cervix carcinoma
enrolling 1060 adults (aged ≥18) with newly diagnosed, high-risk locally advanced CCa – specifically FIGO stage IB2-IIB with nodepositive disease or stage III-IVA, across histologies such as SCC, AC, or adenosquamous carcinoma, with no prior systemic therapy, surgery, or radiation.6
Participants were assigned in a 1:1 ratio to receive either pembrolizumab with CrT followed by pembrolizumab, or placebo with CrT followed by placebo, using central randomisation stratified by type of external beam RT, FIGO stage, and planned total RT dose.6
Treatment involved cisplatin-based CrT, with five cycles concurrent with RT, followed by 15 cycles of pembrolizumab (400mg every six weeks) or placebo after an initial five cycles at 200mg every three weeks. RT quality was centrally monitored. Treatment continued until progression, toxicity, pregnancy, investigator decision, or consent withdrawal, with flexibility for interruptions for toxicity management.6
Treatment-related grade ≥3 AEs occurred in 67% versus 61%, most commonly cytopenias. Serious treatment-related AEs occurred in 17% versus 12%.6
Health-related quality of life (QoL) and physical functioning scores were similarly maintained, with 76% of pembrolizumab patients and 75% of placebo patients reporting stable or improved global health status, and equal 76% reporting stable or improved physical functioning.6
Comprehensive clinical and diagnostic assessment is essential in recurrent or metastatic CCa to define disease extent and guide optimal, individualised treatment decision
The primary endpoints were PFS and OS. Key secondary endpoints included blind centralreview PFS, 24month PFS status, PFS and OS by PDL1 status, PFS2 (time from randomisation to the second disease progression [after the initiation of subsequent therapy] or death from any cause, whichever occurs first), overall response rate (ORR), complete response at 12-weeks, patientreported outcomes, safety, and 36month survival.6
In the pembrolizumab-CrTr group, 22% of participants experienced a PFS event compared to 29% in the placebo-CrTr group, resulting in a hazard ratio (HR) of 0.70. The estimated 24month PFS rate was 68% for the pembrolizumab arm versus 57% for the placebo arm. Within the PDL1-positive subgroup (CPS ≥1), the HR for progression or death was 0.72, whereas in PDL1negative cases, it was 0.61.6 A total of 8% of participants in the pembrolizumab group and 11% in the placebo group died. The HR for OS was 0.73. Estimated 24month OS rates were 87% versus 81%, respectively.8
Regarding ORR, 79% of participants in the pembrolizumab group and 76% in the placebo group responded per investigator review, with fewer progressing in the pembrolizumab arm. Median duration of response was not reached, with 12month response durations observed in 81% versus 77% participants, respectively.8
Median treatment duration was 11.8-months versus 10.9-months, with both groups receiving a median of 11 pembrolizumab/placebo cycles and five cisplatin cycles. RT exposure was consistent: Median treatment time was 52-days, with 75% treated within the 56-day threshold, total cervix dose was 76 Gy (physical) and 87 Gy in both groups.8
Adverse events (AEs) occurred in 99% of participants in both arms. Grade ≥3 events were seen in 75% (pembrolizumab) vs 69% (placebo). Pembrolizumab increased the risk of hypothyroidism (19% versus 5%), hyperthyroidism (11% versus 2%), leukopaenia (24% versus 18%), hypokalaemia (22% versus 16%), and elevated aspartate aminotransferase (18% versus 12%).
Conclusion
Pembrolizumab, a PD-1 monoclonal antibody, represents a significant advancement in the management of high-risk, locally advanced CCa. When added to standard CrTr, pembrolizumab improves PFS and OS, with 24-month PFS rates of 68% versus 57% and OS rates of 87% versus 81% compared with CrTr alone.6 The benefit extends across PD-L1 subgroups (CPS ≥1), and ORR are slightly higher with pembrolizumab (79% vs 76%), reflecting enhanced tumour control.6 Safety profiles remain manageable, with expected immune-related adverse events, and health-related QoL is preserved.6 Regulatory approval in 2024 now allows pembrolizumab as first-line therapy in combination with CrTr for FIGO stage III-IVA CCa5, marking an important option for patients with locally advanced disease. Additionally, pembrolizumab is indicated as monotherapy for recurrent or metastatic PD-L1-positive CCa1
References
1. Professional Information. Keytruda. Updated August 2025.
2. Wu J, Jin Q, Zhang Y, et al Global burden of cervical cancer: current estimates, temporal trend and future projections based on the GLOBOCAN 2022. Journal of the National Cancer Center, Volume 5, Issue 3, 2025, Pages 322-329, ISSN 2667-0054. https://doi.org/10.1016/j. jncc.2024.11.006
3. Fowler JR, Maani EV, Dunton CJ, et al Cervical Cancer. [Updated 2023 Nov 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/ books/NBK431093/
4. Cibula D, Raspollini MR, Planchamp F, et al ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer – Update 2023. Int J Gynecol Cancer. 2023 May 1;33(5):649-666. doi: 10.1136/ijgc2023-004429. PMID: 37127326; PMCID: PMC10176411.
5. Food and Drug Administration. FDA approves pembrolizumab with chemoradiotherapy for FIGO 2014 Stage III-IVA cervical cancer. 2024 [Internet]. Available at: https://www.fda.gov/drugs/resources-informationapproved-drugs/fda-approves-pembrolizumab-chemoradiotherapy-figo-2014stage-iii-iva-cervical-cancer. Accessed 5 September 2025.
6. Lorusso D, Xiang Y, Hasegawa K, et al ENGOT-cx11/ GOG-3047/KEYNOTE-A18 investigators. Pembrolizumab or placebo with chemoradiotherapy followed by pembrolizumab or placebo for newly diagnosed, high-risk, locally advanced cervical cancer (ENGOT-cx11/GOG3047/KEYNOTE-A18): a randomised, double-blind, phase 3 clinical trial. Lancet, 2024 Apr 6;403(10434):1341-1350. doi: 10.1016/S0140-6736(24)00317-9. Epub 2024 Mar 20. PMID: 38521086. SF
Beyond hot flushes
Addressing the silent struggles of genitourinary syndrome of menopause
While hot flashes and night sweats are the most noticeable symptoms, menopause represents a complex health transition with far-reaching implications. It affects cardiovascular (CV), bone, metabolic, and cognitive health, shaping women’s wellbeing well beyond the immediate symptoms. Around 50% of post-menopausal women develop genitourinary syndrome of menopause (GSM)-related vaginal atrophy, causing genital, sexual and urinary symptoms from declining sex hormones. Remarkably, emerging research indicates that the menopause transition can span up to 20-years, highlighting the need for proactive, comprehensive care throughout this extended life stage.1,2,3
The 2024 National Institute for Health and Care Excellence (NICE) guidelines define menopause in healthy individuals assigned female at birth aged ≥45-years as the absence of menstruation for at least 12 months in the absence of hormonal contraception.4
The South African Menopause Society (SAMS) describes menopause as a normal, age-related transition during which the ovaries cease releasing eggs and menstruation stops, marking the end of reproductive capacity. It may occur naturally >40-years or earlier (premature menopause) due to factors such as surgery (eg hysterectomy), ovarian damage from chemotherapy, genetic factors, autoimmune disease, or premature ovarian insufficiency.5
Menopause unboxed: Symptoms, sexual health, and systemic changes
The international Study of Women’s Health Across the Nation (SWAN), one of the largest and longest investigations of the menopausal transition (MT) (1996), confirms the wide variability and chronicity of menopause-related symptoms across multiple body systems. Core features include vasomotor symptoms (VMS), mood disorders, sleep disruption, cognitive changes, and genitourinary and sexual health concerns, alongside notable effects on cardiovascular (CV), bone and overall physical health.1
Around 80% of women reported VMS, such as hot flashes and night sweats, peaking in early to late peri-menopause. Rather than
resolving quickly, frequent VMS persisted for a median of 7.4-years, often much longer.1
SWAN identified distinct trajectories namely early onset, late onset, minimal/no symptoms, and a ‘super flasher’ group where symptoms began before the final menstrual period and extended into post-menopause. Depressed mood and anxiety increased perceived symptom burden independent of frequency. Adiposity increased VMS risk early in MT, but post-menopause this association reversed, mirroring similar transitions in adipokines and inflammatory markers.1
Sleep disturbance was more common in late peri- and postmenopause versus pre-menopause, regardless of VMS, while hormone therapy users reported pre-menopausal sleep patterns. Waking several times nightly showed the strongest association with MT stage. Mental health risk rises, with women being two- to four-times more likely to experience major depressive episodes during MT or early post-menopause, though MT was not predictive of first-onset depression. Anxiety remains under-studied.1
As mentioned, around 50% of post-menopausal women have vaginal atrophy, central to GSM. Oestrogen falls by 95%, with ~75% reporting vaginal dryness, 40% dyspareunia and 30%-40% urinary urgency. Symptoms impaired intimacy in South African women with 55% of women and 61% of men attributing intimacy avoidance to painful sex).2,6
Cardiometabolic and bone health decline, with adverse lipid shifts and bone mineral density loss beginning pre-final menstrual period, contributing to reduced overall physical functioning.1
GSM: A lasting burden – but are we talking about it enough?
vaginal oestrogen therapy offers a highly effective option for the treatment of GSM without requiring systemic hormone therapy. Early diagnosis and broader access to appropriate treatments could significantly improve post-menopausal quality of life (QoL).3
Local and international guidelines recommend hormone replacement therapy (HRT) for menopause-associated symptoms. NICE recommends considering HRT in individuals aged ≥40 years, weighing potential benefits and risks. The North American Menopause Society (NAMS) notes that HRT is the most effective treatment for VSM and GSM and can also prevent bone loss and fractures.4,7
NAMS cautions that the risks of HRT vary by type, dose, duration, route of administration, timing of initiation, and use of progestogen. Treatment should be individualised based on the best available evidence to maximise benefits and minimise risks, with periodic reassessment of ongoing therapy.7
For women with bothersome GSM symptoms not relieved by over-the-counter treatments and without indications for systemic hormone therapy, low-dose vaginal oestrogen or alternative therapies, are recommended by NAMS.7
Up to 50% of postmenopausal women experience vaginal atrophy, with dryness, dyspareunia and urinary urgency profoundly affecting intimacy and quality of life
No, the majority (~70%) of women do not discuss symptoms with healthcare professionals, often due to embarrassment, cultural or societal beliefs, or the misconception that symptoms are a normal part of ageing. While VMS tend to improve over time, GSM symptoms worsen with age and persist for years beyond the MT. Despite the substantial burden of GSM, >50% of affected women remain untreated. Many women are also unaware of available treatments, and clinicians frequently do not screen for GSM, contributing to underdiagnosis and undertreatment.3,6
The Society for Women’s Health Research advocates for ‘menopause preparedness’ beginning as early as 35-years, with a focus on patient awareness, education, and empowerment before the transition. By increasing public knowledge, stigma around ageing and menopause can be reduced, and individuals will be better equipped to recognise symptoms and seek help.3
Drawing parallels with pregnancy care where structured education, routine medical engagement, and support networks improve outcomes, the group highlights the value of a similarly multifaceted approach for menopause. Such preparation could ensure a smoother transition for women and their families during this critical stage of life.3
Vaginal oestrogen: A key tool to managing GSM
If left untreated, GSM can progressively worsen. Very low-dose
Regulatory guidance meets clinical practice
According to regulatory agencies and women’s health societies, the development of ultralow-dose 10 µ g oestradiol vaginal tablets aligns with regulatory and women’s health recommendations to use the lowest effective hormonal dose. Due to its efficacy, safety, and minimal systemic absorption, the oestradiol tablet provides reassurance for healthcare providers and postmenopausal women.8
According to Davis et al, oestradiol vaginal tablets (0.01mg) administered nightly for two- weeks, followed by two to three times per week, and oestriol (0.5mg) nightly for three weeks, then twice weekly is a viable option for vaginal symptoms. In South Africa, oestradiol vaginal tablets (0.01mg) are available, which can be administered intravaginally using an applicator.9,10
It is indicated for the treatment of vaginal atrophy due to oestrogen deficiency. The recommended regimen is one tablet daily for two weeks (initial dose), followed by one tablet twice weekly (maintenance dose). Oestradiol tablets should be used with caution in women ≥65-years.10
Numerous studies support the use of oestradiol vaginal tablets. Weissmann-Brenner et al investigated adherence to local oestrogen therapy for GSM in women aged between 40- and 89-years. Among 2269 participants using continuous monotherapy, 1782 received vaginal creams/gels and 487 received vaginal tablets. Adherence was significantly higher with vaginal tablets: 64% treated ≥4 months versus 39% with vaginal cream/gel, and 83% requested another prescription at six-months versus 54% for vaginal cream/gel. Mean treatment duration was longer with vaginal tablets (1002 vs 787 days), demonstrating superior adherence with oestrogen tablets (P <0.000006).11
Mattsson et al investigated the preferences of 423 women over 50 years regarding local oestrogen therapy for postmenopausal vaginal atrophy. However, as the study was conducted in Sweden,
its applicability to the local population may be limited. Participants completed an online questionnaire. While timing of local oestrogen therapy application did not show a significant preference, women expressed a willingness to pay an additional R1349.10 (€66.58) per month for disposable applicators with small tablets over dosing syringes with vaginal cream, and R1228.74 (€60.32) more for this format over vaginal suppositories, mainly to avoid smudges and leakage. These findings suggest that offering local oestrogen therapy in preferred formats may improve adherence and management of vaginal atrophy.12
Dugal et al compared oestradiol vaginal tablets and oestriol vagitories in 96 post-menopausal women with vaginal atrophy over 24-weeks. Both treatments improved vaginal symptoms, including itching, irritation, dryness, and dyspareunia. Oestradiol vaginal tablets was associated with less leakage (6% vs 65%) and lower need for sanitary protection (0% vs 29%) than oestriol vagitories. More oestradiol vaginal tablets users found the treatment hygienic (90% vs 79%) and easy to use (49% vs 28%). Endometrial thickness increased slightly in both groups initially but returned to baseline with twice-weekly dosing. Oestradiol vaginal tablets offers an effective and user-friendly alternative to traditional local oestrogen therapy.13
Portman et al assessed one-year persistence with local oestrogen therapy in post-menopausal women with vaginal atrophy using pharmacy refill data. Treatment-naive women ≥45 years were included. Of 30 197 women, 40.4% started conjugated oestrogen cream, 38.3% oestradiol cream, and 21.3% 0.01mg oestradiol tablets. Discontinuation after the first prescription was 86.2%-89.4% for creams versus 57.8% for tablets. Mean treatment duration was 103.4 days for tablets versus 44.6-48.1 days for creams. Low-dose tablets showed greater persistence and lower discontinuation risk.14
Ulrich et al evaluated the endometrial safety of a 0.01mg oestradiol vaginal tablet in post-menopausal women with vaginal atrophy. A total of 336 healthy, non-hysterectomised women (mean age 59.5-years) were treated for 12-months – daily for two-weeks, then twice weekly for 50-weeks – with endometrial biopsies at baseline and week 52. Of 283 evaluable biopsies at 52-weeks, 258 were atrophic or inactive, with no cases of hyperplasia or cancer. Mean endometrial thickness decreased slightly from 2.04mm to 1.94mm, and oestradiol levels remained post-menopausal. The study confirms endometrial safety over 12-months.15
Conclusion
Low-dose 0.01mg oestradiol vaginal tablets offer a highly effective and patient-friendly option for managing GSM across diverse populations. They improve symptoms of vaginal atrophy –including dryness, dyspareunia, itching, and irritation – while minimising systemic hormone exposure. Adherence and persistence are superior compared with creams or gels, with longer treatment duration and higher rates of repeat prescription requests. Women value the hygienic, convenient tablet format and disposable applicators, enhancing satisfaction and ongoing use. Safety is demonstrated by stable endometrial thickness and absence of hyperplasia or malignancy over 12-months. By combining efficacy, safety, and user preference,
low-dose vaginal oestradiol tablets provide a tailored, sustainable therapy that addresses the multifaceted impact of menopause on sexual, urinary, and overall QoL.
References
1. El Khoudary SR, Greendale G, Crawford SL, et al. The menopause transition and women’s health at midlife: a progress report from the Study of Women’s Health Across the Nation (SWAN). Menopause. 2019 Oct;26(10):1213-1227. doi: 10.1097/ GME.0000000000001424. PMID: 31568098; PMCID: PMC6784846.
2. Guidozzi F, Thomas C, Smith T, Nappi RE. CLarifying vaginal atrophy’s impact On SEx and Relationships (CLOSER) survey in South Africa. CLIMACTERIC, 2017 Vol 20, NO. 1, 49-54. http://dx.doi.org/10.1080/13697137.2016.1262838
3. Aninye IO, Laitner MH, Chinnappan S , on behalf of the Society for Women’s Health Research Menopause Working Group. Menopause preparedness: perspectives for patient, provider, and policymaker consideration. Menopause. 2021 Jun 28;28(10):1186-1191. doi: 10.1097/GME.0000000000001819. PMID: 34183564; PMCID: PMC8462440.
4. NICE. Menopause: identification and management. 2024 [cited 22 September 2025]. Available from: https://www.nice.org.uk/guidance/ng23/resources/ menopause-identification-and-management-pdf-1837330217413
5. South African Menopause Society. Menopause Facts. [Internet]. Available at https://www.menopause.co.za/menopause-facts/. Accessed 24 October 2025.
6. Carlson K, Nguyen H . Genitourinary Syndrome of Menopause. [Updated 2024 Oct 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559297/
7. Faubion SS, Crandall CJ, Davis L, et al. NAMS Position Statement. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause 29(7):p 767-794, July 2022. | DOI: 10.1097/GME.0000000000002028
8. Panay N, Maamari R. Treatment of postmenopausal vaginal atrophy with 10μg estradiol vaginal tablets. Menopause Int, 2012 Mar;18(1):15-9. doi: 10.1258/ mi.2012.011120. PMID: 22393176.
9. Davis SR, Taylor S, Hemachandra C, et al The 2023 Practitioner’s Toolkit for Managing Menopause. Climacteric, 2023 Dec;26(6):517-536. doi: 10.1080/13697137.2023.2258783. Epub 2023 Dec 1. PMID: 37902335.
10. Professional Information. Vagifem ® 10μg vaginal tablets. 2024 [SAPHRA]. Available from: https://pi-pil-repository.sahpra.org.za/wp-content/uploads/2025/02/PIVagifem-3-December-2024.pdf
11. Weissmann-Brenner A, Bayevsky T, Yoles I. Compliance to vaginal treatmenttablets versus cream: a retrospective 9 years study. Menopause, 2017. Jan;24(1):7376. doi: 10.1097/GME.0000000000000729. PMID: 27648663.
12. Mattsson LÅ, Ericsson Å, Bøgelund M, Maamari R. Women’s preferences toward attributes of local estrogen therapy for the treatment of vaginal atrophy. Maturitas, 2013 Mar;74(3):259-63. doi: 10.1016/j.maturitas.2012.12.004. Epub 2013 Jan 9. PMID: 23312488.
13. Dugal R, Hesla K, Sordal T, et al Comparison of usefulness of estradiol vaginal tablets and estriol vagitories for the treatment of vaginal atrophy. Acta Obstet Gynecol Scand, 2000;79(4):293-297.
14. Portman D, Shulman L, Yeaw J, et al One-year treatment persistence with local estrogen therapy in postmenopausal women diagnosed as having vaginal atrophy. Menopause, 2015;22(11): DOI: 10.1097/ gme.0000000000000465.
15. Ulrich TSG, Naessen T, Elia D et al, on behalf of the VAG-1748 trial investigators. Endometrial safety of ultra-low-dose Vagifem 10 μg in postmenopausal women with vaginal atrophy. Climacteric, 2010; 13(3), 228-237. https://doi.org/10.3109/13697137.2010.481058
16. Simon J, Nachtigall L, Gut R, et al Effective treatment of vaginal atrophy with an ultra-low-dose estradiol vaginal tablet. Obs & Gynecol, 2008;112(5):1053-1060. SF
Vaginal atrophy is more than a physical condition — it’s a silent disruptor of intimacy and emotional connection for many South African women and their partners (CLOSER Study, n=400)1
Restoring feminine confidence
Local estrogen therapy is the first-line treatment for symptomatic vaginal atrophy, offering effective relief of symptoms such as dryness, irritation, and dyspareunia, with minimal systemic absorption and a favourable safety profile2. Effective
Restores vaginal health and relieves symptoms associated with a thin dry vaginal lining such as burning, itching and vaginal irritation3,4
Women using Vagifem® reported greater comfort, improved hygiene, and less inconvenience compared with those using estriol vaginal suppositories.5
Patients reported greater ease, comfort, and overall satisfaction with Vagifem® compared to vaginal cream formulations.6
Scan for API. For full prescribing information, refer to the professional information approved by the Medicines Regulatory Authority.
References: 1.Guidozzi F, et al. Climateric. 2017. 2. Portman DJ, Gass ML. Menopause. 2014. 3. Vagifem® 10 μg vaginal tablets approved professional information, 2024. 4. Simon J, et al. Obs & Gynecol. 2008. 5. Dugal R, et. al. Acta Obstet Gynecol Scand. 2000. 6. Rioux JE, et al. Menopause. 2000.
Scheduling status: S2 Name of the medicine: Vagifem® 10 μg vaginal tablets. Qualitative and quantitative composition: One film-coated vaginal tablet contains: Estradiol hemihydrate equivalent to estradiol 10 micrograms. Reg No.: 47/21.8.1/0166. Applicant
Address: Novo Nordisk (Pty) Ltd, 90 Grayston Drive, Sandown, Sandton, 2031, Gauteng, South Africa. Tel: 011 202 0500. Novo Nordisk (Pty) Ltd, 1959/000833/07. ZA25VG00019. 2025_10.
Optimising UC management
High-dose once-daily mesalazine
Ulcerative colitis (UC) is a chronic inflammatory bowel disease affecting the colon, with inflammation ranging from the rectum to longer segments of the large intestine.1 Typically presenting between the ages of 30- and 50-years, UC can negatively impact quality of life (QoL), cause disability, and increase the lifetime risk of colorectal cancer.2 The disease course is unpredictable, with alternating flare-ups and remission1, and severity can range from mild-to-moderate to moderate-to-severe.1 Bloody diarrhoea, often with mucus, is the hallmark symptom, accompanied by urgency, tenesmus, abdominal pain, malaise, weight loss, and fever depending on disease extent and severity.3
Extraintestinal manifestations (EIMs) occur in 10%-30% of patients diagnosed with UC.3 EIMs linked to disease activity include episcleritis, scleritis, uveitis, peripheral arthritis, erythema nodosum, and pyoderma gangrenosum.3 While EIMs independent of colitis activity include axial arthropathies, sacroiliitis, and ankylosing spondylitis.3 Longstanding inflammation also increases the risk of colorectal cancer, with risks reported at 0.5%-1% per year.4
Seeing UC clearly: From colonoscopy to calprotectin
Diagnosis of UC relies on clinical evaluation supported by endoscopic findings, histology, and exclusion of infectious causes.3 Initial assessment should include stool testing for bacterial and parasitic infections, as colonic infections can mimic UC.3 While radiologic studies are not essential, they may be helpful as longstanding disease can show a ‘stove-pipe’ appearance on double-contrast barium enema.3
Colonoscopy or proctosigmoidoscopy can sometimes reveal loss of vascular pattern, granularity, friability, and ulceration, often beginning in the distal rectum and progressing proximally in a continuous, circumferential manner.3
Disease extent is classified as affecting the rectum only (proctitis), disease distal to the splenic flexure (left-sided UC), or extending beyond the splenic flexure (extensive UC ).1 Populationbased studies have shown proctitis to occur in 30%-60% of patients, left-sided colitis occurring in 16%-45%, and pancolitis (a subset of extensive UC where the entire colon, from rectum to cecum, is inflamed) in 14%-35% of patients.3
Laboratory evaluation often shows elevated inflammatory markers
(erythrocyte sedimentation rate, C-reactive protein, leukocytosis) in an acute flare, with 60%-70% of patients positive for perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) regardless of disease stage.3 In addition to testing P-ANCA, anti-saccharomyces cerevisiae antibodies can also be useful in distinguishing UC from Crohn’s disease as they are more prevalent in Chron’s disease.3
Fecal calprotectin correlates with intestinal neutrophil activity and can aid in ruling out IBD, though it is nonspecific.3 Multiple biopsies are recommended to confirm diagnosis, revealing fragile, granular mucosa, erosions, and the presence of pseudopolyps.3
Targeting the colon: Tailoring UC therapy for maximum impact
Management typically follows a step-up approach, starting with topical or oral therapies and escalating to more complex agents if first-line treatments fail. As UC has no cure aside from colectomy, most patients require long-term maintenance therapy to prevent relapse.4
Considering the extent of disease is crucial when planning UC treatment.4 The aim of treatment is to preserve patients’ QoL and prevent disability.1 This requires rapid relief of symptoms and endoscopic healing, which is now associated with improved longterm outcomes.1
For active distal UC, the American College of Gastroenterology guidelines recommend topical therapy with mesalazine, hydrocortisone, or budesonide.4 For disease extending beyond the sigmoid colon, oral 5-aminosalicylic acid (5-ASAs) such as mesalazine or sulfasalazine are indicated, with doses of up to 4.8g/ day recommended for patients with mild-to-moderate extensive UC.4
The 2022 European Crohn’s and Colitis Organisation (ECCO) guideline recommends oral mesalazine at ≥2g/day to induce remission in mild-to-moderate UC.1 ECCO also recommends mesalazine for the maintenance of remission in patients with UC.1
Mesalazine exerts its therapeutic effect locally, directly on the inflamed colonic mucosa.5 Mesalazine’s anti-inflammatory effects are thought to involve upregulation of peroxisome proliferatoractivated receptors in gastrointestinal epithelial cells and inhibition of cyclooxygenase enzymes, reducing prostaglandin-mediated colonic inflammation.6 Symptom improvement is generally observed within two- to four-weeks of starting therapy. Mesalazine is the most commonly prescribed treatment; used in >88% of UC patients.6
Endoscopic healing and remission:
Defining UC step-by-step
The definition of endoscopic healing is widely regarded as the complete resolution of inflammatory mucosal lesions.7 Sood et al note that defining remission in UC is more challenging, with clinical remission variably interpreted across settings, leading to inconsistency in practice.8
They propose defining remission based on individual components such as: The absence of symptoms (symptomatic remission), normalisation of inflammatory biomarkers (biomarker remission), mucosal healing on endoscopy (endoscopic remission), and histological remission.8 Collectively, these elements would constitute composite remission, promoting greater clarity and uniformity in both clinical and research contexts.8
MMX mesalazine unleashed: Smart delivery for targeted colonic relief
A variety of oral mesalazine formulations have been developed to minimise systemic absorption and optimise delivery to inflamed colonic tissue.5 One such formulation is once-daily mesalazine using a multi-matrix (MMX) system.5
The MMX system combines hydrophilic and lipophilic matrices within a pH-sensitive Eudragit-S coating, which dissolves in the terminal ileum at pH ≥ 7.5 The matrices allow slow, controlled diffusion of mesalazine through the colon5 , enabling once-daily dosing of high-concentration tablets.4
Pharmacokinetic studies show high interindividual variability in plasma and mucosal concentrations of delayed-release 5-ASA in both healthy volunteers and UC patients.4 Following a single dose of either a delayed-release or an azo-bonded formulation, roughly 20% of the 5-ASA is systemically absorbed, with mesalazine and its metabolite (N-acetyl-5-aminosalicylic acid-5-ASA) also secreted back into the colonic lumen, further limiting systemic exposure.4
Administration of food was shown to delay the appearance of mesalazine in plasma by two hours compared to a fasted state.4 Variations between individuals in colonic transit time and pH may influence drug release and mucosal uptake.4 Plasma concentrations of mesalamine were detectable after four-hours and were maximal by eight-hours after the single dose, and a steady state was achieved generally within two-days after dosing.4
Studies show MMX mesalazine disintegrates earlier (4.8-hours vs 6.2-hours) but complete disintegration occurs more slowly (17.4-hours vs 7.3-hours) than other pH-dependent formulations.5 This allows for controlled and extended drug delivery across the colon.5 MMX mesalazine as maintenance therapy in patients with
left-sided UC also showed greater patient-reported outcomes (62.2% vs 51.5%) compared to other formulations.5 In addition, MMX mesalazine shows the potential to be more cost-effective with up to a 76% probability of cost savings, while gaining 0.011 quality-adjusted life years.5
In South Africa, MMX mesalazine is approved for both induction and maintenance of remission in UC.9 For induction, adults (including those >65-years) should take 2.4-4.8g once daily. Patients who are unresponsive to lower doses may use the maximum 4.8g/day, with treatment response assessed at eightweeks.9 For maintenance, 2.4g once daily is recommended.9
In summary, MMX mesalazine enables once-daily dosing with targeted, delayed-release of 5-ASA throughout the colon, minimising systemic absorption, improving symptom control, and demonstrating potential cost-effectiveness compared with pHdependent formulations.4,5
Staying power: MMX mesalazine for long-term clinical remission
Numerous studies show MMX mesalazine effectively induces clinical and endoscopic remission in mild-to-moderate UC.10 In a trial of 517 patients, remission rates at eight-weeks were 37.2% (2.4g/day) and 35.1% (4.8g/day) versus 17.5% for placebo, with complete mucosal healing in 32% versus 16%. Safety profiles in all studies were comparable across groups, with only mild-tomoderate adverse events (AEs) reported.10
Lichtenstein et al conducted an eight-week trial of 280 patients with mild-to-moderate UC, showing MMX mesalazine 2.4g twice daily or 4.8g once daily induced clinical and endoscopic remission in 34.1% and 29.2% of patients, respectively, versus 12.9% for placebo.11
In another eight-week study by Kamm et al, once-daily MMX mesalazine at 2.4g/per day or 4.8g/day given once daily induced clinical and endoscopic remission in 40.5% and 41.2% of patients with active mild-to-moderate UC, versus 22.1% for placebo.12 Treatments were well tolerated, offering effective, convenient therapy to improve adherence.12
Two phase III trials involving 517 patients with active, mild-tomoderate UC evaluated MMX mesalazine (2.4g/day or 4.8g/day) versus placebo over eight-weeks.13 Both doses of MMX mesalazine significantly increased clinical and endoscopic remission across subgroups defined by disease extent, severity, gender, and prior 5-ASA use.13
Among patients switching from low-dose 5-ASA, MMX mesalazine 4.8g/day was significantly more effective than placebo (P = 0.018).13 Overall, MMX mesalazine is effective for inducing remission regardless of baseline patient characteristics.13
A 12-month multicentre trial evaluated MMX mesalazine 2.4g/ day, given once or twice daily, for maintenance in UC patients in remission.14 Clinical and endoscopic remission at 12- months was achieved in 64.4% (once-daily group) and 68.5% (twice-daily group), with maintained clinical remission rates of 88.9% and 93.2% respectively.14 This supports the ability of once-daily dosing of MMX Mesalazine to achieve and maintain high clinical and endoscopic remission rates.14
In an eight-week study, 304 patients with active, mild-tomoderate UC who had not achieved remission in prior phase III trials received high-dose MMX mesalazine 4.8g/day.15 Overall, 59.5% attained clinical and endoscopic remission, regardless of
prior treatment.15 The study shows that extended high-dose MMX mesalazine can induce remission and potentially prevent the need for step-up therapy.15
In a 12-month randomised comparator study of 331 patients with left-sided UC in remission, once-daily 5-ASA-MMX 2.4g demonstrated similar efficacy and safety to a delayed-release mesalazine 2.4g twice daily.16 Clinical remission was achieved in 68.0% versus 65.9%, and clinical plus endoscopic remission in 60.9% versus 61.7%, supporting convenient once-daily dosing.16
In a 12- to 14-month phase IV study, 208 patients diagnosed with UC received MMX mesalazine 2.4g/day once daily for maintenance.17 Following six- and 12-months of treatment, 76.5% and 64.4% of evaluable patients respectfully, were re-occurrence free.17 Adherence ≥80% was associated with lower recurrence at both time points, highlighting MMX mesalazine’s effectiveness and the importance of consistent dosing.17
A multicentre, six-month, double-blind trial compared once-daily MMX mesalazine 2.4g with twice-daily delayed-release mesalazine 1.6g.18 Among 826 patients, 83.7% and 77.8% of patients in the PP and intend-to-treat (ITT) populations respectively, maintained endoscopic and clinical remission.18
Comparative to remission rates of 81.5% (PP) and 76.9% (ITT) of patients receiving delayed-release mesalazine.18 AEs were similar (37.1% vs 36.0%), supporting MMX mesalazine as a well-tolerated, convenient once-daily maintenance option.18
In a more recent multicenter, eight-week randomised study, 280 patients diagnosed with mild-to-moderate UC received once-daily high-dose MMX mesalazine at 4.8g/day or pH-dependent release mesalazine at 3.6g/day three times daily.19 MMX mesalazine demonstrated greater reduction in UC-Disease Activity Index scores (−2.6 vs −1.8), with consistent efficacy across subgroups. AEs were similar, supporting MMX 4.8g/day as a more effective, well-tolerated treatment option.19
Conclusion
High-dose once-daily MMX mesalazine provides effective, targeted therapy for patients with mild-to-moderate UC, inducing both clinical and endoscopic remission while maintaining a favourable safety profile.10,12 Its once-daily dosing improves adherence, a key factor in sustaining remission and reducing relapse risk.17 MMX mesalazine combines convenience, tolerability, superior mucosal healing, and cost effectiveness, making it a cornerstone in optimised UC management.5,12,17,19
References
1. Raine T, Bonovas S, Burisch J, et al ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. Journal of Crohn’s and Colitis, 2022;16(1):2-17.
2. Fanizzi F, Allocca M, Fiorino G , et al. Raising the bar in ulcerative colitis management. Therap Adv Gastroenterol, 2024;17:1-34.
3. Lynch D, Hsu R. Ulcerative Colitis. [Online]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459282/ [Accessed September 2025].
4. Nanda K, Moss C. Update on the management of ulcerative colitis: treatment and maintenance approaches focused on MMX® mesalazine. Clinical Pharmacology: Advances and Applications, 2012;4:41-50.
5. Ye B, van Langenberg D. Mesalazine preparations for the treatment of ulcerative colitis: Are all created equal? World J Gastrointest Pharmacol Ther, 2015;6(4):137-144.
6. Sehgal P, Colombel F, Aboubakr A, Narula N. Systematic review: safety of mesalazine in ulcerative colitis. Aliment Pharmacol Ther, 2018; 47:1597-1609.
7. Buda A, Pessarelli T, Aldinio G, et al Endoscopic healing in IBD: Still the target to achieve? Digestive and Liver Disease, 2025;57:969-967.
8. Sood A, Singh A, Mahajan R, et al (Re)Appraising Remission in Ulcerative Colitis. Inflammatory Bowel Diseases, 2023;29: 1317-1326.
9. Mezavant professional information, May 2025.
10. Sandborn W, Kamm M, Lichtenstein G, et al MMX Multi Matrix System® mesalazine for the induction of remission in patients with mild-to-moderate ulcerative colitis: a combined analysis of two randomized, double-blind, placebo-controlled trials. Aliment Pharmacol Ther, 2007;26(2):205-215.
11. Lichtenstein G, Kamm M, Boddu P, et al Effect of once-or twice-daily MMX mesalazine (SPD476) for the induction of remission of mild to moderately active ulcerative colitis. Clin Gastroenterol Hepatol, 2007;5:95-102.
12. Kamm A, Sandborn W, Gassull M, et al. Once-daily, high-concentration MMX mesalazine in active ulcerative colitis. Gastroenterology, 2007;132:66-75.
13. Lichtenstein G, Kamm M, Sandborn W, et al. MMX mesalazine for the induction of remission of mild-to-moderately active ulcerative colitis: efficacy and tolerability in specific patient subpopulations. Aliment Pharmacol Ther, 2008;27(11):1094-1102.
14. Kamm M, Lichtenstein G, Sandborn W, et al. Randomised trial of once-or twice-daily MMX mesalazine for maintenance of remission in ulcerative colitis. Gut, 2008;57:893-902.
15. Kamm M, Lichtenstein G, Sandborn W, et al Effect of extended MMX mesalazine therapy for acute, mild-to-moderate ulcerative colitis. Inflamm Bowel Dis, 2009;15(1):1-8.
16. Prantera C, Kohn A, Campieri M, et al Clinical trial: ulcerative colitis maintenance treatment with 5-ASA: a 1-year, randomized multicentre study comparing MMX® with Asacol®. Aliment Pharmacol Ther, 2009;30(9):908-918.
17. Kane S, Katz S, Jamal M, et al Strategies in maintenance for patients receiving long-term therapy (SIMPLE): A study of MMX mesalazine for the long-term maintenance of quiescent ulcerative colitis. Inflamm Bowel Dis, 2012;18(6):1026-1033.
18. D’Haens G, Sandborn WJ Barrett K, et al. Once-daily MMX(®) mesalamine for endoscopic maintenance of remission of ulcerative colitis. Am J Gastroenterol, 2012.
19. Ogata H, Aoyama N, Mizushima S, et al Comparison of efficacy of multimatrix mesalazine 4.8 g/day once-daily with other high-dose mesalazine in active ulcerative colitis: a randomized, double-blind study. Intest Res, 2017, 107(7):1064-1077. SF
[S3] Mezavant® (enteric coated, prolonged release tablet.) Each tablet contains mesalazine 1200 mg. Reg. No. 45/11/0463. For full prescribing information, refer to the MEZAVANT® Professional Information as approved by SAHPRA. Takeda (Pty) Ltd, Reg. No.: 1982/011215/07, Building A, Monte Circle, 64 Montecasino Boulevard, Fourways 2191. Tel: +27115143000. Marketed and distributed by Adcock Ingram Limited. Reg. No.: 1949/034385/06. Private Bag X69, Bryanston, 2021, South Africa. Customer Care: 0860 ADCOCK/232625. www.adcock.com C-APROM/ZA/ MEZ/0059. October 2025.
FROM START TO FINISH, MEZAVANT ® HAS ULCERATIVE COLITIS (UC) COVERED
1,2,3
MEZAVANT ® TREATS-TO-TARGET 4-7
• Utilises MMX® technology for delivery of 5-ASA throughout the entire colon1,2,3
• Achieves clinical & endoscopic remission and restores QoL4-7
• Always once-daily with a low pill burden1,8
• Well tolerated with a good safety profile7
• Reduces the need for enemas and suppositories8
MEZAVANT® is indicated for the treatment and maintenance of remission in ulcerative colitis1
5-ASA: 5-aminosalicylate; MMX: Multi Matrix System®; QoL: quality of life
REFERENCES: 1. MEZAVANT® professional information, May 2022. 2. Tenjarla S, Romasanta V, Zeijdner E, Villa R, Moro L. Release of 5-Aminosalicylate From an MMX Mesalamine Tablet During Transit Through a Simulated Gastrointestinal Tract System. Adv Ther 2007;24(4):826-840. 3. Tenjarla S, Abinusawa A. In-Vitro Characterization of 5-Aminosalicylic Acid Release from MMX Mesalamine Tablets and Determination of Tablet Coating Thickness. Adv Ther 2011;28(1):62-72. 4. Turner D, Ricciuto A, Lewis A, D’Amico F, Dhaliwal J, Griffiths AM, et al STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterol 2021;160:1570 -1583. 5. Kamm MA, Sandborn WJ, Gassull M, Schreiber S, Jackowski L, Butler T, et al. Once-Daily, High-Concentration MMX Mesalamine in Active Ulcerative Colitis. Gastroenterol 2007;132:66-75. 6. Willian MK, D’Haens G, Yarlas A, Joshi AV. Changes in health-related quality of life and work-related outcomes for patients with mild-to-moderate ulcerative colitis receiving short-term and long-term treatment with multimatrix mesalamine: a prospective, open-label study. J Patient Rep Outcomes 2018;2:22. https://doi.org/10.1186/s41687-018-0046-5. 7. Kamm MA, Lichtenstein GR, Sandborn WJ, Schreiber S, Lees K, Barrett K et al. Randomised trial of once- or twice-daily MMX mesalazine for maintenance of remission in ulcerative colitis. Gut 2008;57:893–902. 8. Hu MY, Peppercorn MA. MMX mesalamine: a novel high-dose, oncedaily 5-aminosalicylate formulation for the treatment of ulcerative colitis. Expert Opin Pharmacother 2008;9(6):1049-1058.
S3 Mezavant® (enteric coated, prolonged release tablet.) Each tablet contains mesalazine 1200 mg. Reg. No. 45/11/0463. For full prescribing information, refer to the MEZAVANT® Professional Information as approved by SAHPRA. Takeda (Pty) Ltd, Reg. No.: 1982/011215/07, Building A, Monte Circle, 64 Montecasino Boulevard, Fourways 2191. Tel: +27115143000. Marketed and distributed by Adcock Ingram Limited. Reg. No.: 1949/034385/06. Private Bag X69, Bryanston, 2021, South Africa. Customer Care: 0860 ADCOCK/232625. www.adcock.com C-APROM/ZA/MEZ/0053. October 2024.
Pembrolizumab
expands its horizons in ECa
Pembrolizumab, a programmed death-1 (PD-1) monoclonal antibody,1 has received regulatory approval as firstline treatment for patients with recurrent or advanced endometrial cancer (ECa) in combination with chemotherapy (ChT), followed by pembrolizumab monotherapy.1
ECa is the sixth most common cancer among women worldwide, and its incidence has increased markedly over the past twenty years2 – likely driven by the growing prevalence of risk factors such as advanced age and obesity.3
ECa cancer is predominantly a postmenopausal disease, with 14%-20% of cases occurring in premenopausal women and only around 5% diagnosed in those younger than 40-years.4 Most younger women with ECa present with favourable histology, better prognosis, early-stage disease, limited myometrial involvement, and absence of lymphatic vascular invasion.2
The majority of patients present with symptoms such as postmenopausal bleeding or abnormal uterine bleeding. In advanced disease, symptoms may include pelvic pain, abdominal bloating, bowel and bladder dysfunction, premature satiety, dyspnoea, and dyspareunia.2
Fortunately, ~70% of patients are diagnosed at an early stage, contributing to the relatively high five-year 2 overall survival (OS) of 81%.2 However, despite this generally favourable prognosis, some patients do experience poor OS outcomes.2 For example, the five-year OS for stage IVA and IVB ECa is only 17% and 15%, respectively.2
The International Federation of Gynecology and Obstetrics (FIGO) Committee on Women’s Cancer defines stage IVA as invasion of the bladder mucosa and/or the intestinal (bowel) mucosa.5 Stage IVB is defined as abdominal peritoneal metastasis beyond the pelvis.5
Stepwise progression of endometrial cancer: Histology, invasion, and staging
Histological tumour type is an important prognostic predictor in ECa.5 Eight histological types have been identified: Endometrioid carcinoma (EEC) of low grade (grades 1 and 2) or high grade (grade 3), serous carcinoma (SC), clear cell carcinoma (CCC), mixed carcinoma, undifferentiated carcinoma, carcinosarcoma, and other unusual types such as mesonephric-like or
gastrointestinal (GI) mucinous carcinomas.5
These subtypes differ in molecular features, microscopic appearance, precursor lesions, and natural history.5 Histological typing may be essential in staging, particularly for distinguishing non-aggressive low-grade EECs from aggressive high-grade EECs and other high-risk histologies.5 The extent of myometrial invasion is a key prognostic factor. Invasion is expressed as the percentage of myometrial thickness infiltrated by carcinoma: None, <50%, or ≥50%.5
Lymphovascular space invasion (LVSI) should be assessed at the invasive front, with substantial or extensive LVSI distinguished from focal or absent LVSI.5 Cervical stromal invasion is defined as any invasion at or deeper than a benign endocervical crypt, whereas glandular extension alone does not contribute to staging.5 Adnexal involvement influences OS. In high-grade tumours, ovarian involvement is usually considered metastatic.5 Studies confirm a clonal relationship between endometrial and ovarian tumours in most cases.5
Fallopian tube involvement should be recorded and staged as IIIA1, though its prognostic significance remains uncertain.5 Uterine serosal involvement occurs when the tumour reaches submesothelial fibroconnective tissue or the mesothelial layer.5 Lymph node metastases are classified by size: Macrometastases >2mm, micrometastases 0.2-2mm, and isolated tumour cells ≤0.2mm.5
Molecular classification stratifies recurrence risk and survival.5
The Cancer Genome Atlas classifies endometrial carcinomas as polymerase epsilon/ultramutated (excellent prognosis), microsatellite instability-high (MSI-H)/hypermutated (intermediate prognosis), somatic copy number alterations (SCNA)-high/serouslike (poor prognosis), and SCNA-low (intermediate prognosis influenced by grade and oestrogen receptor expression).5
FIGO staging reflects tumour spread: Stage IA1 includes tumours limited to an endometrial polyp or confined endometrium of lowgrade EECs.5 Stage IA2 involves ≤50% myometrial invasion with no or focal LVSI.5 Stage IB involves ≥50% myometrial invasion of
low-grade EECs5 and stage IC are aggressive tumour types within a polyp or confined to the endometrium without myometrial invasion.5
Stage IIA tumours involve non-aggressive histological types with cervical stromal invasion.5 Stage IIB refers to non-aggressive tumours with substantial LVSI.5 Stage IIC includes aggressive histologies with myometrial invasion, while Stage IC lacks invasion. Types include high-grade EEC, SC, CCC, and others.5
Stage III encompasses local or regional spread,5 differentiating adnexal (IIIA1) from serosal (IIIA2), IIIB1 vaginal/parametrial involvement,5 IIIB2 pelvic peritoneal involvement,5 and IIIC lymph node metastases subdivided by micro- and macrometastases.5
As mentioned, stage IVA involves bladder or bowel mucosa, stage IVB is defined by extrapelvic visceral or peritoneal metastases, distinguishing it from stage IIIB2, which involves peritoneal spread confined to the pelvis, while stage IVC denotes distant metastases, including extra-abdominal nodes and organs.5
Emerging role of pembrolizumabbased immunotherapy in recurrent and advanced ECa: Insights from KEYNOTE-775 and subsequent trials
The European Society of Medical Oncology notes that ~30% of primary ECas are MSI-H/ deficient mismatch repair (dMMR), reflecting immune dysregulation. Immune checkpoint inhibitors (ICIs), including pembrolizumab, has been explored as monotherapy or combined with ChT, other immunotherapies, or targeted agents in numerous studies. Pembrolizumab received American Food and Drug Administration (FDA) accelerated approval for advanced MSI-H/dMMR solid ECa tumours, marking the first tumour-agnostic, biomarkerdriven therapy.6
every three-weeks (30-minute infusion), for up to 35 doses. In the ChT group, patients received either 60mg/m² of IV doxorubicin every three weeks or 80mg/m² of IV paclitaxel weekly (three weeks on, one week off). Treatments were administered based on prior dosing studies and physician discretion for ChT selection and scheduling.8 The primary endpoints were PFS and OS, secondary endpoints included objective response rates (ORR), safety and sideeffect profile, and health-related quality of life (HrQoL).8
In the pMMR population, lenvatinib plus pembrolizumab significantly improved PFS compared to ChT (median 6.6 versus 3.8 months). Similar benefits were observed in the overall population (median 7.2 versus 3.8 months).8
In the pMMR population, OS was significantly longer with lenvatinib plus pembrolizumab (median 17.4-months) compared to ChT (median, 12-months), with a hazard ratio (HR) for death of 0.68.8 Similar results were observed in the overall trial population, where median OS was 18.3-months with lenvatinib plus pembrolizumab, as compared with 11.4-months with ChT (HR 0.62). The proportional-hazards assumptions for PFS and OS were met among all patients.8
Pembrolizumab has received regulatory approval as firstline treatment for recurrent or advanced ECa, in combination with ChT, followed by monotherapy
In 2021, the FDA granted accelerated approval of pembrolizumab for advanced ECa based on the results of the Lenvatinib in Combination with Pembrolizumab Versus Treatment of Physician’s Choice in Participants with Advanced Endometrial Cancer (Study 309-Keynote 775) by Makker et al 7
Makker et al (2022) compared the efficacy and safety of lenvatinib plus pembrolizumab with the physician’s choice of doxorubicin or paclitaxel ChT in patients with advanced ECa who had disease progression after the receipt of at least one platinumbased therapy.8
Women aged ≥18-years with advanced, recurrent, or metastatic ECa (excluding carcinosarcoma and sarcoma) were enrolled after progressing on platinum-based ChT, without prior vascular endothelial growth factor or PD-1-targeted therapy. Up to two platinum regimens were allowed if one was neoadjuvant/adjuvant, and prior hormonal therapy was permitted.8
Eligible patients were randomly assigned (1:1) to receive either lenvatinib plus pembrolizumab or ChT (doxorubicin or paclitaxel, selected before randomisation).8 Randomisation was stratified according to MMR status (dMMR or proficient mismatch repair [pMMR]).8 A total of 827 patients were enrolled across 167 sites in 21 countries, comprising 697 in the pMMR population and 130 in the dMMR population.8
In the lenvatinib-pembrolizumab group, patients received 20mg of oral lenvatinib daily and 200mg of intravenous (IV) pembrolizumab
The analyses of PFS and OS consistently favoured lenvatinib plus pembrolizumab over ChT across all evaluated subgroups –regardless of age, histologic subtype, or prior therapy lines – with similar trends observed in both the pMMR population and the overall trial population.8
In the pMMR population, confirmed ORR were higher with lenvatinib plus pembrolizumab (30.3%) than ChT (15.1%). In the overall population, response rates were 31.9% versus 14.7%, respectively. Complete responses occurred in 5.2% (lenvatinib-pembrolizumab) versus 2.6% (ChT) in the pMMR group, and 6.6% versus 2.6% in the overall population.8
More patients – about twice as many – in the ChT group had progressive disease as their best response compared to the lenvatinib-pembrolizumab group.8 Among responders in the pMMR population, median duration of response was longer with lenvatinib plus pembrolizumab (9.2-months) than with ChT (5.7-months). In the overall population, durations were 14.4-months and 5.7-months, respectively. More patients in the lenvatinibpembrolizumab group also experienced tumour shrinkage. Although the trial was not powered for comparison in the dMMR group, clinically meaningful efficacy benefits were still observed across endpoints.8
In the safety population, median treatment duration was longer with lenvatinib plus pembrolizumab (231-days) compared to ChT (104.5-days). Median lenvatinib dose intensity was 13.8mg/day, and patients received a median of 10 pembrolizumab cycles.8 ChT patients received a median of five cycles (doxorubicin) or six (paclitaxel). More patients in the lenvatinib-pembrolizumab group had treatment durations of ≥6-, ≥12-, and ≥18-months. Median time to first lenvatinib dose reduction was 1.9-months, 45.6% had two or more reductions.8
More than 99% of patients in both groups experienced AEs. The most common were hypertension (64%) with lenvatinibpembrolizumab and anaemia (48.7%) with ChT. Grade ≥3 events
occurred in 88.9% versus 72.7%, respectively. Serious AEs included hypertension (4.2%) and febrile neutropaenia (4.1%), while grade 5 events occurred in 5.7% and 4.9% of patients, respectively.8 No substantial differences in HrQoL were observed between the groups.8
In the intention-to-treat population, 28% of patients treated with lenvatinib plus pembrolizumab and 48.1% of those treated with ChT received subsequent systemic anticancer therapies. Among the ChT group, 9.1% of patients with pMMR tumours received lenvatinib plus pembrolizumab as subsequent treatment, while 16.9% of patients with dMMR tumours received PD-1 pathway-targeting monotherapy or combination regimens as later therapies.8
Updated efficacy and safety results from the randomised phase 3 Study 309/KEYNOTE-775 confirmed the sustained clinical benefit of lenvatinib plus pembrolizumab in previously treated advanced, recurrent, or metastatic ECa. 9 In this open-label trial, participants were randomised to lenvatinib 20mg daily plus pembrolizumab 200mg or ChT 9 (doxorubicin or paclitaxel) every three weeks.8
The final prespecified analysis demonstrated continued improvement in OS (pMMR HR 0.70, all-comers HR 0.65), PFS (pMMR HR 0.60, all-comers HR 0.56), and ORR (pMMR: 32.4% vs 15.1%, all-comers: 33.8% vs 14.7%) versus ChT. Benefits were consistent across all key subgroups, including histology, prior therapy, and mismatch-repair status.9
Safety findings remained in line with the known profile of the regimen, with no new safety signals observed. Overall, lenvatinib plus pembrolizumab continues to demonstrate superior efficacy and manageable safety compared with chemotherapy in patients with previously treated advanced ECa.9
Building on these findings, Eskander et al (2023) conducted a trial evaluating the addition of pembrolizumab to first-line paclitaxel plus carboplatin in patients with advanced, metastatic, or recurrent ECa.10 This study compared standard ChT (paclitaxel plus carboplatin) combined with either pembrolizumab or placebo in this patient population.11
The trial was conducted at 395 sites in four countries (the United States, Canada, Japan, and South Korea).11 The median follow-up was 12-months in the dMMR cohort and 7.9 months in the pMMR cohort. Follow-up times were similar according to randomised group in each cohort.11
Adult women (≥18-years of age) with confirmed advanced-stage, metastatic, or recurrent ECa except those with carcinosarcoma were eligible for enrollment.11 A total of 816 patients were enrolled, with 225 in the dMMR cohort and 591 in the pMMR cohort. Of these, 588 were available for efficacy analysis.11 Patients were randomly assigned to receive paclitaxel plus carboplatin with either pembrolizumab or placebo for six cycles, followed by maintenance therapy up to 14 additional cycles.11 The primary outcome was PFS, with secondary endpoints including safety, OS, and HrQoL.11
In the 12-month analysis in the dMMR cohort, the risk of progression or death was 70% lower with pembrolizumab.11 In the pMMR cohort, median PFS was 13.1 months versus 8.7 months with placebo,11 though results varied by location and subgroup size.11 HrQoL at six-weeks was similar across groups.11
AEs (≥15% of patients in either group) occurred frequently.11 In the dMMR cohort, any-cause AEs were
reported in 98.2% (pembrolizumab) and 99.1% (placebo).11 Grade ≥3 AEs occurred in 63.3% versus 47.2%, respectively.11 In the pMMR cohort, any-cause AEs were 93.5% versus 93.4%,11 and grade ≥3 AEs in 55.1% versus 45.3%.11 Grade 5 AEs occurred in 1.4% (dMMR) and 1.5% (pMMR).11 Deaths were due to sepsis, cardiac arrest, or GI events.11 One grade 5 cardiac arrest in the pMMR cohort was possibly related to pembrolizumab.11
Conclusion
Recent clinical investigations have positioned pembrolizumab as a pivotal therapy in advanced and recurrent ECa. Data from KEYNOTE-775 demonstrated superior OS and PFS compared with standard ChT, with clinically meaningful ORR sustained across subgroups.6 Importantly, benefits extended to patients with pMMR tumours, historically associated with poor outcomes.6 Earlier findings from KEYNOTE-158 further established durable responses in dMMR cohorts, providing biological rationale for broader use.9
References
1. KEYTRUDA® 100 mg approved professional information, 11 August 2025.
2. Mazidimoradi A, Momenimovahed Z, Khalajinia Z, et al. The global incidence, mortality, and burden of uterine cancer in 2019 and correlation with SDI, tobacco, dietary risks, and metabolic risk factors: An ecological study. Health Sci Rep. 2024;7(1):e1835.
3. Mirza MR, Lorusso D, Shen Q, et al. First-line treatments for advanced or recurrent endometrial cancer: Systematic literature review of clinical evidence. Crit Rev Oncol Hematol. 2025; 206:104555.
4. Abdol Manap N, Ng BK, Phon SE, Abdul Karim AK, Lim PS, Fadhil M. Endometrial cancer in pre‐menopausal women and younger: risk factors and outcome. Int J Environ Res Public Health, 2022.
5. Berek JS, Matias-Guiu X, Creutzberg C, et al. FIGO staging of endometrial cancer: 2023. Int J Gynecol Obstet. 2023;162:383-394.
6. Oaknin A, Bosse TJ, Creutzberg CL, et al Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Annals of Oncology, 2022;33:9:860-877.
7. Food and Drug Administration. FDA grants regular approval to pembrolizumab and lenvatinib for advanced endometrial carcinoma. 2021 [Internet]. Available at: https://www.fda.gov/drugs/resourcesinformation-approved-drugs/fda-grants-regular-approvalpembrolizumab-and-lenvatinib-advanced-endometrial-carcinoma Last edited 02/01/2022. Accessed 24 November 2025.
8. Makker V, Colombo N, Casado Herráez A, et al. Lenvatinib plus Pembrolizumab for Advanced Endometrial Cancer. N Engl J Med, 2022;386(5):437-448.
9. Makker V, Colombo N, Casado Herráez A, et al. Lenvatinib Plus Pembrolizumab in Previously Treated Advanced Endometrial Cancer: Updated Efficacy and Safety From the Randomized Phase III Study 309/ KEYNOTE-775. J Clin Oncol, 2023.
10. Eskander RN, Sill MW, Beffa L, et al. Pembrolizumab plus chemotherapy in advanced or recurrent endometrial cancer: overall survival and exploratory analyses of the NRG GY018 phase 3 randomized trial. Nat Med, 2025;31(5):1539-1546.
11. Eskander RN, Sill MW, Beffa L, et al. Pembrolizumab plus Chemotherapy in Advanced Endometrial Cancer. N Engl J Med, 2023;388(23):2159 -2170. SF
A Key to Rewriting Her Tomorrows with New Treatment Possibilities for certain Gynaecological Cancers 1
ENDOMETRIAL CANCER
KEYTRUDA, in combination with chemotherapy, followed by KEYTRUDA as monotherapy, is indicated for the treatment of patients with primary advanced or recurrent endometrial carcinoma 1
KEYTRUDA, in combination with lenvatinib, is indicated for the treatment of patients with advanced endometrial carcinoma who have disease progression following prior systemic therapy in any setting and are not candidates for curative surgery or radiation.1
CERVICAL CANCER
KEYTRUDA, in combination with chemoradiotherapy (CRT), is indicated for the treatment of patients with high-risk, locally advanced cervical cancer 1
KEYTRUDA, in combination with chemotherapy with or without bevacizumab, is indicated for the treatment of patients with persistent, recurrent, or metastatic cervical cancer 1
KEYTRUDA, as monotherapy, is indicated for the treatment of patients with recurrent or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥1) as determined by a validated test, with disease progression on or after chemotherapy.1
REFERENCE: 1. KEYTRUDA Approved Professional Information, August 2025.
Learn more about the KN868/NRG GY018 trial (endometrial cancer)
Learn more about the KNA18 trial (cervical cancer)
See page 208 to 213
SELECTED SAFETY INFORMATION: CONTRAINDICATIONS: KEYTRUDA is contraindicated in patients with hypersensitivity to pembrolizumab or any inactive ingredients, and should not be used during pregnancy and lactation. SPECIAL WARNINGS AND PRECAUTIONS FOR USE: Safety and efficacy not established in children <18 years except for paediatric patients with melanoma or classical Hodgkin Lymphoma (cHL). No dose adjustments needed for elderly patients (≥65 years) or mild-to-moderate renal/hepatic impairment. Use caution in severe renal/hepatic impairment (not studied). No formal pharmacokinetic drug interaction studies exist/ have been conducted. Avoid corticosteroids/immunosuppressants before treatment. Poses fetal risks – use contraception during and 4 months post-treatment. Avoid breastfeeding. SIDE EFFECTS (UNDESIRABLE EFFECTS): Pembrolizumab commonly triggers immune-mediated adverse reactions, most resolving with appropriate treatment or discontinuation. The adverse events were assessed across tumour types. Monotherapy (7,631 patients, 8.5 months median observation): Very common adverse reactions included Blood and lymphatic system disorders: anaemia; Endocrine disorders: hypothyroidism; Metabolism and nutrition disorders: decreased appetite; Nervous system disorders: headache; Respiratory, thoracic and mediastinal disorders: dyspnoea, cough; Gastrointestinal disorders: diarrhoea, abdominal pain, nausea, vomiting, constipation; Skin and subcutaneous tissue disorders: pruritus, rash; Musculoskeletal and connective tissue disorders: musculoskeletal pain, arthralgia; General disorders and administration site conditions: fatigue, asthenia, oedema, pyrexia. Mostly Grades 1 or 2 in severity. Severe adverse reactions included immune- mediated and severe infusion-related reactions. Combination with Chemotherapy or chemoradiotherapy (CRT) (6,093 patients): Very common adverse reactions included: Blood and lymphatic system disorders: anaemia, neutropenia, thrombocytopenia; Endocrine disorders: hypothyroidism; Metabolism and nutrition disorders: hypokalaemia, decreased appetite; Psychiatric disorders: insomnia; Nervous system disorders: neuropathy peripheral, headache, dizziness; Respiratory, thoracic and mediastinal disorders: dyspnoea, cough; Gastrointestinal disorders: diarrhoea, nausea, vomiting abdominal pain, constipation; Skin and subcutaneous tissue disorders: alopecia, pruritus, rash; Musculoskeletal and connective tissue disorders: musculoskeletal pain, arthralgia; General disorders and administration site conditions: fatigue, asthenia, pyrexia, oedema; Investigations: alanine aminotransferase increased, aspartate aminotransferase increased, blood creatinine increased. Combination with tyrosine kinase inhibitor (TKI) (1,456 patients): Very common adverse reactions include: Infections and Infestations: urinary tract infection; Blood and lymphatic system disorders: anaemia; Endocrine disorders: hypothyroidism; Metabolism and nutrition disorders: decreased appetite; Nervous system disorders: headache, dysgeusia; Vascular disorders: hypertension; Respiratory, thoracic and mediastinal disorders: dyspnoea, cough; Gastrointestinal disorders: diarrhoea, vomiting abdominal pain, nausea, constipation; Skin and subcutaneous tissue disorders: rash, pruritus; Musculoskeletal and connective tissue disorders: arthralgia, musculoskeletal pain, myositis, pain in extremity; General disorders and administration site conditions: fatigue, asthenia, oedema, pyrexia; Investigations: lipase increased, alanine aminotransferase increased, aspartate aminotransferase increased, blood creatinine increased. Immune-mediated adverse reactions across various doses reported included pneumonitis, colitis, hepatitis, nephritis, endocrinopathies and Severe skin reactions. Other immune-mediated adverse reactions reported in less than 1 % of patients treated included uveitis, myositis, Guillain-Barré syndrome, pancreatitis, encephalitis, sarcoidosis, myasthenic syndrome/myasthenia gravis (including exacerbation), myelitis vasculitis, hypoparathyroidism, gastritis, haemolytic aneamia and pericarditis. Immune-mediated adverse reactions reported in post-marketing use included myocarditis, sclerosing cholangitis, optic neuritis and exocrine pancreatic insufficiency.
S4 KEYTRUDA® Solution for Infusion. Reg. No.: 50/30.1/0957. Each vial contains 100 mg Pembrolizumab in 4 ml solution (25 mg/ml). Contains 280 mg sucrose.
Ulcerative colitis
What the GP needs to know (part 1)
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) primarily affecting the colon and rectum. The disease is characterised by symptoms such as frequent diarrhoea mixed with blood and mucus, abdominal pain, and weight loss. The goal of diagnosis is to differentiate UC from other conditions that present similarly, such as Crohn’s disease, infectious colitis, or malignancy.
Diagnosis begins with a thorough history and physical examination. Key factors include the duration, frequency, and characteristics of diarrhea, as well as associated symptoms like weight loss or fever.
A history of recent antibiotic use could indicate a Clostridium difficile infection, which might mimic UC symptoms. An evaluation of stool characteristics, including presence of blood or mucus, and any nocturnal diarrhea is crucial.
A family history of IBD or colorectal cancer, alongside other systemic symptoms like joint pain or skin lesions, can provide additional diagnostic clues.
The physical examination might reveal anaemia, abdominal tenderness, or perianal abnormalities. Digital rectal examination, while not always pleasant, can sometimes uncover hidden pathologies. Extra-intestinal manifestations such as eye inflammation, skin lesions, or joint pain can also suggest underlying IBD.
Diagnosing UC involves ruling out other conditions with similar presentations. Tests such as faecal calprotectin are useful to differentiate IBD from irritable bowel syndrome, as elevated levels indicate intestinal inflammation.
Endoscopy, including colonoscopy, is essential for visualising the colon and rectum, assessing the extent of inflammation, and identifying mucosal changes characteristic of UC. The Mayo score is used to classify disease severity from mild to severe based on endoscopic findings.
The goals of treatment are to control inflammation, induce and maintain remission, and improve the patient’s quality of life while minimising side effects. Long-term management often requires a multidisciplinary approach involving gastroenterologists, dietitians, and other specialists to address the various aspects of the disease and its impact on daily life.
The treatment of UC aims to induce and maintain remission while preventing complications.
The management approach is tailored to the disease severity and the patient’s response to previous treatments.
Initial treatment often involves 5-aminosalicylic acid compounds, which are effective for inducing and maintaining remission in mild to moderate cases. These can be administered orally or rectally depending on the extent of the disease.
For moderate to severe cases, corticosteroids (CS) such as prednisone or budesonide are used to quickly induce remission. However, due to potential side effects like weight gain, hypertension, and osteoporosis, CS are not suitable for long-term use. Their use is typically limited to short-term management and bridging to other therapies.
Immunomodulators, including azathioprine and 6-mercaptopurine, are effective for maintaining remission and reducing steroid dependency, but they take several weeks to become effective and require regular monitoring due to potential side effects. Methotrexate may be used in some cases, though its application is less common. Biologics such as anti-TNF agents (eg infliximab, adalimumab) offer targeted therapy by addressing specific immune responses involved in UC. These are particularly useful in severe cases or when patients are unresponsive to conventional therapies. Newer options like integrin inhibitors and small molecules are emerging, offering additional choices for managing UC.
In summary, managing UC effectively involves accurate diagnosis, targeted therapy, and regular monitoring to adjust treatment as needed and address potential complications.
The webinar is accredited for one (1) CPD point. Once you have watched the replays, send an e-mail to john.woodford@newmedia.co.za and request to have your CPD point allocated to your profile on the HPCSA database. Include the webinar name and your HPCSA number in your e-mail. SF
Dr Nazeer Ahmed Ismail Chopdat
FROM START TO FINISH, MEZAVANT ® HAS ULCERATIVE COLITIS (UC) COVERED
1,2,3
MEZAVANT ® TREATS-TO-TARGET 4-7
• Utilises MMX® technology for delivery of 5-ASA throughout the entire colon1,2,3
• Achieves clinical & endoscopic remission and restores QoL4-7
• Always once-daily with a low pill burden1,8
• Well tolerated with a good safety profile7
• Reduces the need for enemas and suppositories8
MEZAVANT® is indicated for the treatment and maintenance of remission in ulcerative colitis1
5-ASA: 5-aminosalicylate; MMX: Multi Matrix System®; QoL: quality of life
REFERENCES: 1. MEZAVANT® professional information, May 2022. 2. Tenjarla S, Romasanta V, Zeijdner E, Villa R, Moro L. Release of 5-Aminosalicylate From an MMX Mesalamine Tablet During Transit Through a Simulated Gastrointestinal Tract System. Adv Ther 2007;24(4):826-840. 3. Tenjarla S, Abinusawa A. In-Vitro Characterization of 5-Aminosalicylic Acid Release from MMX Mesalamine Tablets and Determination of Tablet Coating Thickness. Adv Ther 2011;28(1):62-72. 4. Turner D, Ricciuto A, Lewis A, D’Amico F, Dhaliwal J, Griffiths AM, et al STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterol 2021;160:1570 -1583. 5. Kamm MA, Sandborn WJ, Gassull M, Schreiber S, Jackowski L, Butler T, et al. Once-Daily, High-Concentration MMX Mesalamine in Active Ulcerative Colitis. Gastroenterol 2007;132:66-75. 6. Willian MK, D’Haens G, Yarlas A, Joshi AV. Changes in health-related quality of life and work-related outcomes for patients with mild-to-moderate ulcerative colitis receiving short-term and long-term treatment with multimatrix mesalamine: a prospective, open-label study. J Patient Rep Outcomes 2018;2:22. https://doi.org/10.1186/s41687-018-0046-5. 7. Kamm MA, Lichtenstein GR, Sandborn WJ, Schreiber S, Lees K, Barrett K et al. Randomised trial of once- or twice-daily MMX mesalazine for maintenance of remission in ulcerative colitis. Gut 2008;57:893–902. 8. Hu MY, Peppercorn MA. MMX mesalamine: a novel high-dose, oncedaily 5-aminosalicylate formulation for the treatment of ulcerative colitis. Expert Opin Pharmacother 2008;9(6):1049-1058.
S3 Mezavant® (enteric coated, prolonged release tablet.) Each tablet contains mesalazine 1200 mg. Reg. No. 45/11/0463. For full prescribing information, refer to the MEZAVANT® Professional Information as approved by SAHPRA. Takeda (Pty) Ltd, Reg. No.: 1982/011215/07, Building A, Monte Circle, 64 Montecasino Boulevard, Fourways 2191. Tel: +27115143000. Marketed and distributed by Adcock Ingram Limited. Reg. No.: 1949/034385/06. Private Bag X69, Bryanston, 2021, South Africa. Customer Care: 0860 ADCOCK/232625. www.adcock.com C-APROM/ZA/MEZ/0053. October 2024.
What the GP needs to know (part 2)
The global incidence of inflammatory bowel disease (IBD), which includes Crohn’s disease and ulcerative colitis (UC), is increasing – especially in newly industrialised and westernised countries. This increase is linked to lifestyle and dietary changes associated with modernisation. As countries adopt more urban, industrial, and sedentary lifestyles, the prevalence of IBD continues to grow, highlighting the urgent need for greater awareness and management of this condition worldwide. Primary healthcare practitioners play an essential role in IBD management, particularly in early identification and ongoing monitoring of the disease.
IBD is not simply a disease but a lifelong journey for those diagnosed. From the moment of diagnosis, both patients and healthcare providers often lack sufficient knowledge about the disease, as it is less familiar compared to chronic conditions like hypertension or diabetes.
Over time, patients face various challenges such as relapses, potential pregnancy complications, surgeries, and other disease-related issues. Managing IBD requires ongoing support, guidance, and medical intervention to control symptoms, prevent complications, and ensure the best possible outcomes.
As a chronic condition, IBD’s onset and progression are influenced by a variety of factors that begin before adulthood. Genetics plays a significant role, but factors like the mode of delivery (C-section versus natural birth), early antibiotic exposure, the composition of the gut microbiome, and even the removal of the appendix can contribute to its development. Apart from urbanisation and industrialisation, other environmental risk factors such as smoking, and lack of physical activity, also exacerbate the progression of IBD.
The impact of IBD extends beyond the digestive system, affecting nearly every aspect of a patient’s life, including healthcare, psychological well-being, and daily activities like eating, traveling, and working. The psychological burden of IBD, particularly for young patients such as teenagers with UC, can be profound and life-altering.
Effective management requires a comprehensive approach that not only addresses the physical symptoms but also the emotional, social, and psychological challenges faced by patients.
In recent years, significant advancements have been made in understanding IBD’s pathophysiology, resulting in the development of advanced therapies such as biologics, small molecules, and personalised treatment strategies. These innovations have improved patient outcomes, reduced complications, and enhanced overall quality of life. However, challenges persist, particularly with
the rising global incidence of IBD, the high costs of treatments, and the financial burden these medications place on patients and healthcare systems.
The need for new treatment approaches is critical. Advances in AI, early diagnostics, and improved monitoring will enable more personalised and patient-specific therapies. However, the high cost of newer therapies remains a major barrier, especially in regions like Asia Pacific, the Middle East, and Africa.
In these areas, cost-effective such as aminosalicylates (5ASA) are recommended for managing moderate UC. Despite the availability of more advanced therapies, 5-ASA remains one of the most affordable options with fewer side effects and effective disease management when used correctly.
Ensuring patient adherence to prescribed treatments like 5-ASA is crucial for successfully inducing remission. Patient education is essential to ensure they understand the importance of following their prescribed regimen. As the disease progresses, treatment escalation is necessary for more aggressive forms of the disease, but premature use of advanced therapies can have significant long-term health and financial consequences. Optimising the use of current treatments and focusing on patient adherence can help patients achieve and maintain remission for longer periods, improving their quality of life. SF
This webinar was sponsored by Adcock and is accredited for one (1) CPD point. Once you have watched the replays, send an e-mail to john.woodford@ newmedia.co.za and request to have your CPD point allocated to your profile on the HPCSA database. Include the webinar names and your HPCSA number in your e-mail. Please note, it may take up to four weeks for your point to be reflected on your portfolio.
Dr Nazeer Ahmed Ismail Chopdat
DEXILANT ONE-OF-A-KIND PPI1#
THE ONLY PPI WITH A 2ND RELEASE FOR MAINTAINED RELIEF2,3
DEXILANT DDR:
• the MOST POWERFUL inhibitory effect on the proton pump of ALL available PPIs.4
• TRUE once-daily dosing.5
References: 1. South African Medicine Price Registry. Database of Medicine Prices, 01 November 2023 [online]. [cited November 2023]; Available from URL: http://www.mpr.gov.za/. 2. Monthly Index of Medical Specialities. September 2023;63(No. 8):185-191. 3. Metz DC, Howden CW, Perez MC, et al. Clinical trial: dexlansoprazole MR, a proton pump inhibitor with dual delayed-release technology, effectively controls symptoms and prevents relapse in patients with healed erosive oesophagitis. Aliment Pharmacol Ther. 2009;29(7):742-54. doi: 10.1111/j.1365-2036.2009.03954.x. 4. Gąsiorowska A. The role of pH in symptomatic relief and effective treatment of gastroesophageal reflux disease. Prz Gastroenterol. 2017;12(4):244249. doi: 10.5114/pg.2017.72097. 5. Frye JW, Peura DA. Managing gastroesophageal reflux disease - comparative efficacy and outcomes of dexlansoprazole MR. Ther Clin Risk Manag 2015;11:1649-56. doi: 10.2147/TCRM.S66680. 6. Dexilant Professional Information. Takeda (Pty) Ltd, South Africa; August 2021. 7. Sharma P, Shaheen NJ, Perez MC, et al Clinical trials: healing of erosive oesophagitis with dexlansoprazole MR, a proton pump inhibitor with a novel dual delayed-release formulation--results from two randomized controlled studies. Aliment Pharmacol Ther 2009;29(7):731-41. doi: 10.1111/j.1365-2036.2009.03933.x. 8. Fass R, Chey WD, Zakko SF, et al. Clinical trial: the effects of the proton pump inhibitor dexlansoprazole MR on daytime and nighttime heartburn in patients with non-erosive reflux disease. Aliment Pharmacol Ther. 2009;29(12):1261-72. doi: 10.1111/j.1365-2036.2009.04013.x.