Parking: Onsite parking in the South Lot is complimentary
We greatly appreciate your time and feedback!
Heather Cooper Ortner Incoming President & CEO International Myeloma Foundation
“I am humbled to serve alongside so many who are making a different every day for patients and families affected by myeloma, and I look forward to building on the IMF’s legacy of impact”
Scientific Advisory Board
S. Vincent Rajkumar, MD IMF Board Chair
Thomas Martin, MD
UCSF, Helen Diller Family Comprehensive Cancer Center
Wee Joo Chng, MD
National University of Singapore
María-Victoria Mateos, MD, PhD University of Salamanca
Vania Hungria, MD, PhD Santa Casa de São Paulo
Joseph Mikhael, MD, MEd, FRCPC, FACP IMF Chief Medical Officer
Sigurður Yngvi Kristinsson, MD, PhD University of Iceland
Philippe Moreau, MD University Hospital of Nantes
Shaji Kumar, MD Mayo Clinic
NIkhil Munshi, MD Dana-Farber Cancer Institute
Jesús San Miguel, MD, PhD University of Navarra
Sagar Lonial, MD, FACP
Winship Cancer Institute, Emory University
Saad Zafar Usmani, MD, MBA, FACP, FASCO
Memorial Sloan Kettering Cancer Center
The IMF Support Group Team is Here
For You!
Shared Experiences Help to Better Understand the Myeloma Journey
• Support Groups empower patients & care partners with information, insight & hope
• The IMF provides educational support to a network of over 150 myeloma specific groups
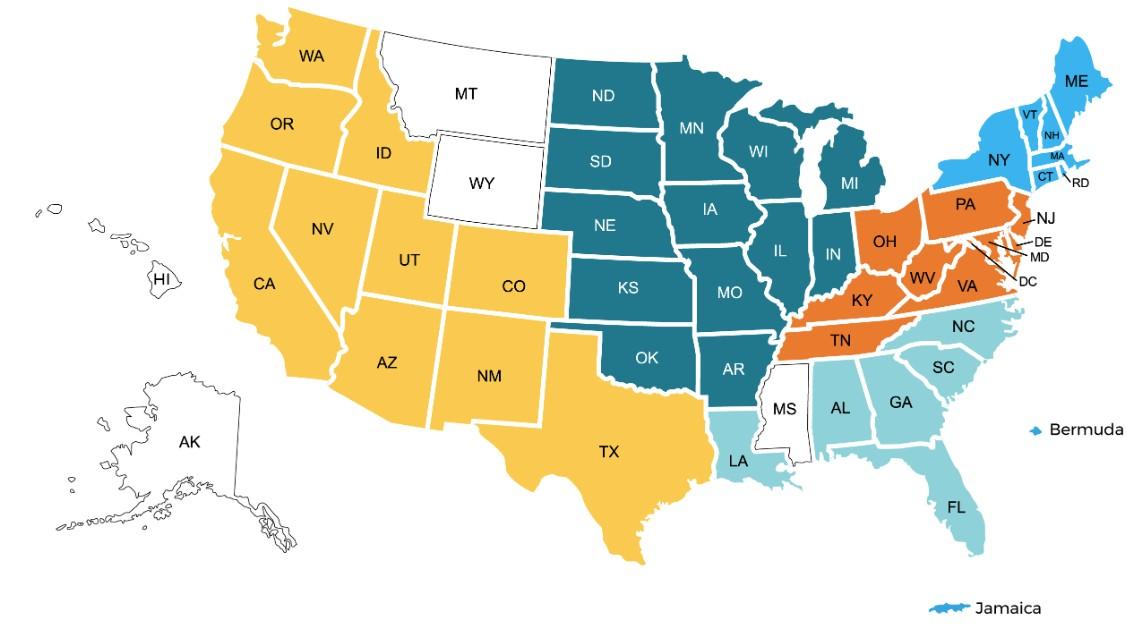
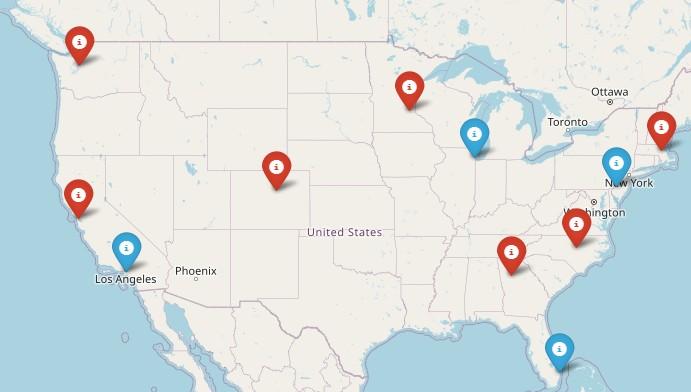
150+ US Support Groups
Over 200 Support Group Visits/year
Univ. of IL at Chicago
Meets virtually on the 2 Tuesday of each month at 6:30 PM Central Time
Aurora
Meets hybrid on the 1st Wednesday of each month at 6:00 PM Central Time
University of Chicago
Meets virtually on the 2nd Wednesday of each month at 10:30 AM Central Time
Mokena
Meets virtually on the last Thursday of each month at 4:00 PM Central Time
Northbrook
Meets virtually on the 1st Wednesday of each month at 7:00 PM Central Time
Fort Wayne
Meets hybrid on the 1st Tuesday of each month at 6:00 PM Central Time
Bloomington
Meets hybrid on the 2nd Tuesday of each month at 5:30 PM
Central Time
Indianapolis
Meets in-person on the 1st Monday of each month at 6:00 PM Central Time
Special Interest Groups
Special interest groups are designed as a supplemental support for specific populations of patients, in addition to their local Support Groups
MM Families
Founded in 2021
For patients & care partners with young children
Las Voces de Mieloma
Founded in 2022
For Spanish speaking patients & care partners
Living Solo & Strong
Founded in 2022
For patients without a care partner
Click here for more inf
Smolder Bolder
Founded in 2023
For smoldering myeloma patients & care partners
Veterans SIG
Founded in 2025
For those who served our country
High Risk Multiple Myeloma
Founded in 2023
For high-risk myeloma patients & care partners
Care Partners Only
Founded in 2024
For myeloma care partners only
WRITTEN EDUCATION
Live Patient Education
2025 Live Patient Education
Patient & Family Seminars
• Boca Raton, FL – March 14 – 15
• Philadelphia, PA – May 2 – 3
• Los Angeles, CA – August 15 – 16
• Chicago, IL – October 3 – 4
Myeloma Community Workshops
• Virtual - March 4
• San Mateo, CA - March 29
• Atlanta, GA - April 5
• Edina, MN - April 26
• Denver, CO - June 21
• Virtual – July 29
• Seattle, WA - August 9
• Waltham, MA - September 27
• Raleigh-Durham, NC - November 15
• Virtual – November 17
1. Ensure Access to Care: We advocate to ensure all myeloma patients have equitable, comprehensive, patient-centered care without insurance barriers that limit options or delay treatment initiation.
2. Eliminate Financial Barriers: We advocate for policies that allow myeloma patients access to treatments and supportive care interventions without facing financial hardships.
3. Advance Myeloma Research: We advocate for annual appropriations funding for myeloma research and the advancement of clinical trial eligibility and research protocols that ensure representation from diverse populations.
The IMF Grassroots Advocacy Program is multi-faceted and growing
• Advocacy Training & Leadership Development
• Policy and Legislative Education
• Grassroots Campaign Planning
• Health Policy Forums & Roundtables
• Advocacy Resource Development
• Storytelling and Personal Narratives
Scan for Upcoming Programs and Events!
Understanding Clinical Trials
Joseph Mikhael MD, MEd, FRCPC, FACP, FASCO Chief Medical Officer, International Myeloma Foundation
Professor, Translational Genomics Research Institute, City of Hope Cancer Center
Provide The Rationale For Clinical Trials
Objectives
Outline The Phases Of Clinical Trials
Discuss The Risks And Benefits Of Clinical Trials
Clinical Trials - Overview
Some Of The Important Principles Of Clinical Trials:
The drive of research has brought us to where we are
No one is expected to be a “guinea pig” with no potential benefit to them
Research is under very tight supervision and standards
Open, clear communication between the physician and the patient is fundamental Driving research forward!
MYTH: If I participate in a clinical trial, I might get a placebo, not active treatment
MYTH: If I participate in a clinical trial, I can’t change my mind
Clinical Trials: Myths
• Phase 1 and 2, everyone gets active treatment
• Phase 3 standard of care vs new regimen: often standard regimen with/without additional agent in MM trials
• Patients can withdraw their consent for clinical trial participation at any time
MYTH: Clinical trials are dangerous because they have new medicines and practices
• Some risk is involved with every treatment, but medicines are used in clinical trials with people only after they have gone through testing to indicate that the drug is likely to be safe and effective for human use
MYTH: Clinical trials are expensive and not covered by insurance
• Research costs are typically covered by the sponsoring company
• Standard patient care costs are typically covered by insurance
• Check with clinical trial team/insurers; costs such as transportation, hotel, etc may not be reimbursed and are paid by patient
PhRMA website. Accessed March 25, 2024. https://phrma.org/-/media/Project/PhRMA/PhRMA-Org/PhRMA-Org/PDF/A-C/CLINICAL-TRIALS-MYTH-FACT-PRINT.pdf?hsCtaTracking=f6689b95-1626-40d9-8c87-c6b 8d31600a4%7C35221aa8-d487-4db3-9416-b9c3c35e3bac
.
Clinical Trials – Why Me??
Every patient is unique and must be viewed that way
Benefits of trials are numerous and include:
Early access to “new” therapy
Delay use of standard therapy
Contribution to myeloma world – present and future
Financial access to certain agents
Must be balanced with potential risks
“Toxicity” of side effects
Possibility of lack of efficacy
Overview of New Drug Development
Identify a target for therapy in the laboratory
Confirm the anticancer activity in laboratory and animal studies
Clinical trials (human studies) to determine safety, dosing and effectiveness
The whole process costs millions of dollars and years of effort!
Even Before Phase I
Most agents are tested in lab models
Various “myeloma cell lines”, also known as “in vitro”
Next step is animal model
We are more like mice than you think!!
Earliest study in Phase I is called “First in Human”
Often uses extremely low dose of drug to ensure safety
Phase 1 Clinical Trials
All patients receive the experimental therapy
Phase 1 trials find the optimal dose of a new drug or drug combination
Patients get higher doses as the study continues
Determine side effects of new drugs or combinations
Explore how the drug is metabolized by the body
Important for all stages of myeloma
Phase 2 Clinical Trials
Determine if a new drug or combination is effective against the cancer
May be added to a Phase 1 study once the ideal dose is found
Patients usually receive the experimental therapy
In some cases, the study may include two “arms” comparing either two different doses or a different treatment (another combination of drugs)
Phase 3 Clinical Trials
Highest form of clinical evidence. Typically, a large number of patients are required…usually required for full FDA approval
Patients receive either an experimental therapy (one or more drugs) or the current standard treatment
o The patient is randomly assigned to a treatment—a process called “randomization”
o Neither the physician or the patient can determine which treatment is given
May be placebo controlled, if no standard treatments are available
Very closely monitored for effectiveness and side effects
Preclinical
Clinical Trial Phases
ANIMAL STUDIES: Examine safety and potential for efficacy
PHASE 1
PHASE 2
FIRST INTRODUCTION OF AN INVESTIGATIONAL DRUG INTO HUMANS
• Determine metabolism and PK/PD actions, MTD, and DLT
• Identify AEs
• Gain early evidence of efficacy, studied in many conditions; typically, 20 to 80 patients; everyone gets agent
EVALUATION OF EFFECTIVENESS IN A CERTAIN TUMOR TYPE
• Determine short-term AEs and risks; closely monitored
• Includes up to 100 patients, typically
PHASE 3
GATHER ADDITIONAL EFFECTIVENESS AND SAFETY
PHASE 4
INFORMATION COMPARED TO STANDARD OF CARE
• Placebo may be involved if no standard of care exists; hundreds to several thousand patients
• Often multiple institutions; single or double blind; sometimes open label
APPROVED AGENTS IN NEW POPULATIONS OR NEW DOSE
Clinical Trials: Benefits of Participation
Possible Benefits:
• Patients will receive, at a minimum, the best standard treatment
• If the new treatment or intervention is proven to work, patients may be among the first to benefit
• Patients have a chance to help others and improve cancer care
Risks of Participation
Possible risks:
• New treatments or interventions under study are not always better than, or even as good as, standard care
• Even if a new treatment has benefits, it may not work for every patient
• Health insurance and managed care providers do not always cover clinical trials
Why Do So Few Cancer Patients Participate in Trials?
Patients may:
• Be unaware of clinical trials
• Lack access to trials
• Fear, distrust, or be suspicious of research
• Have practical or personal obstacles
• Face insurance or cost problems
• Be unwilling to go against their physicians’ wishes
• Not have physicians who offer them trials
• Have a disconnect with their healthcare team
Diversity in Clinical Trials
There has been a lack of diverse representation in clinical trials in myeloma.
In the U.S., approximately 20% of all myeloma patients are of African descent, but only 5%–8% of patients in myeloma clinical trials are of African descent.
This is significant for the following reasons:
All patients of all races and ethnicities should be able to benefit from clinical trials.
Diverse patient representation in clinical trials is required to ensure that the outcomes are applicable to all patients.
Reasons for underrepresentation in clinical trials are complex and include:
Systemic racism, accessibility of clinical trials, sensitivity to diversity by medical professionals
Misconduct in medicine in the past, the lack of trust in the system, and more.
Importance of Clinical Trial Participation by Diverse Populations
[P]eople from racial and ethnic minorities and other diverse groups are underrepresented in clinical research. This is a concern because people of different ages, races, and ethnicities may react differently to certain medical products.
– FDA
Leadership and commitment
Community engagement practices
Investigator hiring, training, and mentoring practices
Patient engagement practices
US Cancer Centers of Excellence: Strategies for Increased Inclusion of Racial and Ethnic Minorities in Clinical Trials
Commonly Asked Questions
How does the study work? How often will I need to see my doctor or visit the cancer center?
Will I need to undergo additional tests?
What is currently known about the new drug or combination?
What benefits can I expect?
What side effects should I expect? Who should I notify if I have side effects?
Can I take my vitamins or other medications?
Can I get the treatment with my local doctor?
Will my insurance pay for my participation in the clinical trial?
Is A Clinical Trial Right For Me?
Discuss with your physician if you are eligible for a clinical trial
Work with your physician to determine the best trial for you
Meet with the clinical research nurse or trials coordinator to discuss the trial
Carefully review the provided “Informed Consent” Describes the study and any potential safety concerns related to the experimental medication
Clinicaltrials.gov https://clinicaltrials.gov/
ncreasing-diversity-in-cancer-clinical-research
Fireside Chat: What is the Future of Myeloma? With Q&A
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO, Chief Medical Officer, International Myeloma Foundation
Benjamin Derman, MD University of Chicago, Chicago, IL
BREAK
WHEN YOU RETURN FROM BREAK PLEASE HEAD TO YOUR SELECTED BREAKOUT SESSION:
BREAKOUT A: NEWLY DIAGNOSED: FRONTLINE THERAPY
Please move to the Salon G-J
BREAKOUT B: MANAGING RELAPSED MYELOMA
Please remain in this room
Housekeeping Items
Presentation Slides: Are available by scanning the QR code, Instructions are on the QR code handout on each table.
Program Evaluations: evaluations at the end of the program or on your way out.
Restrooms: Turn left exiting the meeting room and bathrooms are on your left before the lobby
Badge Holders: Please return your badge holders and we can recycle them
Intravenous (IV) or subcutaneous injection (under the skin) Kyprolis (carfilzomib)
(ixazomib)
Chemotherapy Cytoxan (cyclophosphamide)
or intravenous Alkeran or Evomela (melphalan) M or Mel
Decadron (dexamethasone) Dex or D or d
Monoclonal Antibodies
Darzalex (daratumumab) Sarclisa (isatuximab)
or intravenous
Intravenous (IV) or subcutaneous injection (under the skin)
Bi-Specific Antibodies
Talquetamab CAR-T
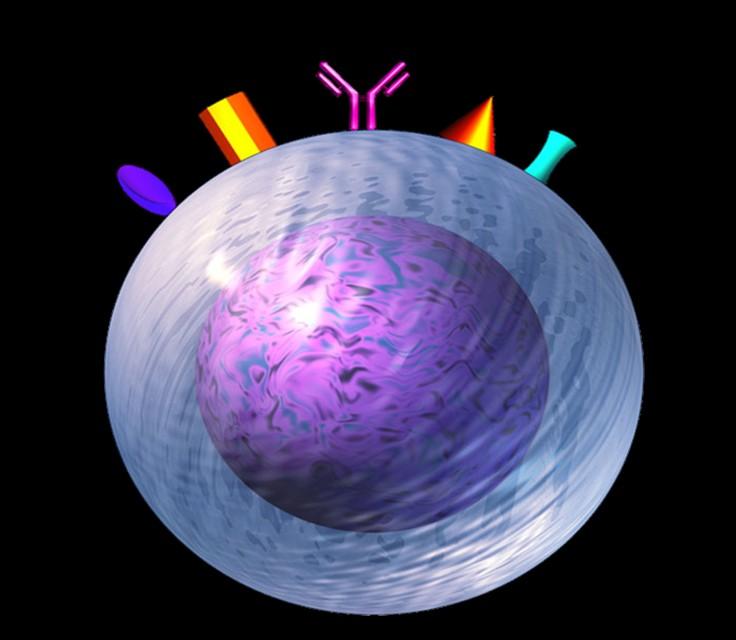
Targets on the Myeloma Cell Surface and Therapeutic Antibodies
Antibody Drug
Elotuzumab
Bi-Specific Antibodies
Bi-Specific Antibodies
Cevostamab CAR-T
Immune Therapies
Ide-cel CAR-T
Cilta-cel CAR-T
Teclistamab
Elranatamab
Linvoseltamab
Etentamig
Antibody Drug Conjugates
Belantamab
Treatment of Newly Diagnosed Myeloma
Transplant Eligible
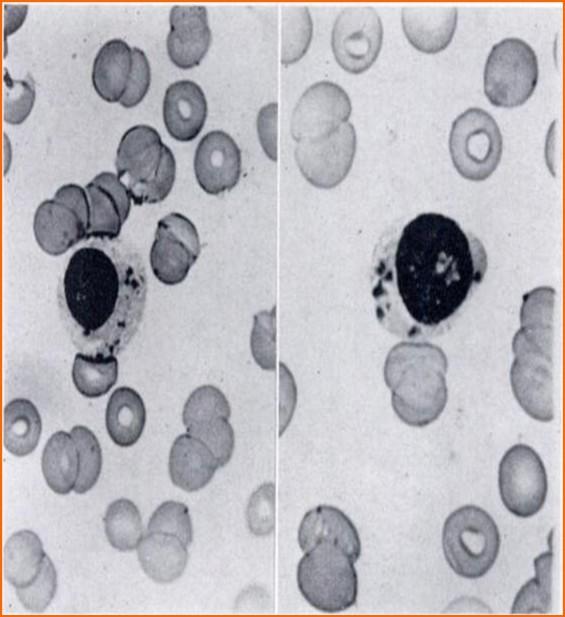
JH Wright. Trans Assoc of Am Phys,1900 Vol15, 137-147
mSMART Guidelines
Transplant Eligible
STANDARD RISK MYELOMA
Dara-VRd or Isa-VRd x ~4 cycles
Collect Stem Cellsa
Autologous stem cell transplant (preferred)
Dar-VRd or IsaVRd x 4 cycles
Len maintenanceb
Len until progression; Delayed ASCTb
HIGH RISK MYELOMA
Double or Triple Hit
Dara-VRd or Isa-VRd x ~4 cycles
Dara-VRd or Isa-VRd x ~4 cycles
Autologous Stem Cell Transplant (ASCT)
Autologous Stem Cell Transplant (ASCT)
Bortezomib plus lenalidomide maintenance till progressionb, c
Bortezomib plus lenalidomide maintenance till progressionb, c
a If age >65 or > 4 cycles of induction therapy, consider mobilization with G-CSF plus cytoxan or plerixafor; b Duration usually until progression based on tolerance; c In patients with grade 2 or higher neuropathy at baseline, and for patients in whom bortezomib needs to be dose reduced or discontinued due to neuropathy, consider carfilzomib instead.
Dispenzieri et al. Mayo Clin Proc 2007;82:323-341; Kumar et al. Mayo Clin Proc 2009 84:1095-1110; Mikhael et al. Mayo Clin Proc 2013;88:360376. v22 //last reviewed Oct 2024
Stem Cell Transplant: Fighting Myeloma with the Left Hook!
Transplant
Myeloma
General
Eligibility Criteria for Autologous Stem Cell Transplant
Performance Status
‒ Ambulatory and capable of self-care
Organ Function
‒ Heart: left ventricular ejection fraction (LVEF) ≥40 percent, and no uncontrolled coronary artery disease or uncontrolled arrhythmias
‒ Lungs: optimal threshold for pulmonary function is not well-defined, but the level of ≥50 percent DLCO (diffusing capacity of the lungs)
‒ Kidneys- All kidney function taken
‒ Liver: Cirrhosis is a contraindication
Patient choice is key!
‒ Infections — There should be no uncontrolled active infections. Biol Blood Marrow Transplant. 2016;22(9):1582. Epub 2016 Jun 14. .
RVD +Stem Cell Transplant vs. RVD without Transplant
DETERMINATION Trial of Newly Diagnosed MM
-Patients aged 18-65 yrs with symptomatic newly diagnosed MM following 1 cycle of RVD -56 sites within the United States from 2010 to 2018
End Points of Study and Follow-up
• Primary end point: progression-free survival (time to next relapse)
• Secondary end points included:
• Response rates, overall survival, quality of life, and adverse events
• Follow-up on participant status : median of 6 years
RVD +Stem Cell Transplant vs. RVD without Transplant DETERMINATION Trial of Newly Diagnosed MM RESULTS
Parameter
No Transplant (n = 357)
with Up Front Transplantation
• At a median follow-up of 76.0 months, the risk of disease progression or death was 53% higher in the RVD-alone group than in the transplantation group (P<0.001)
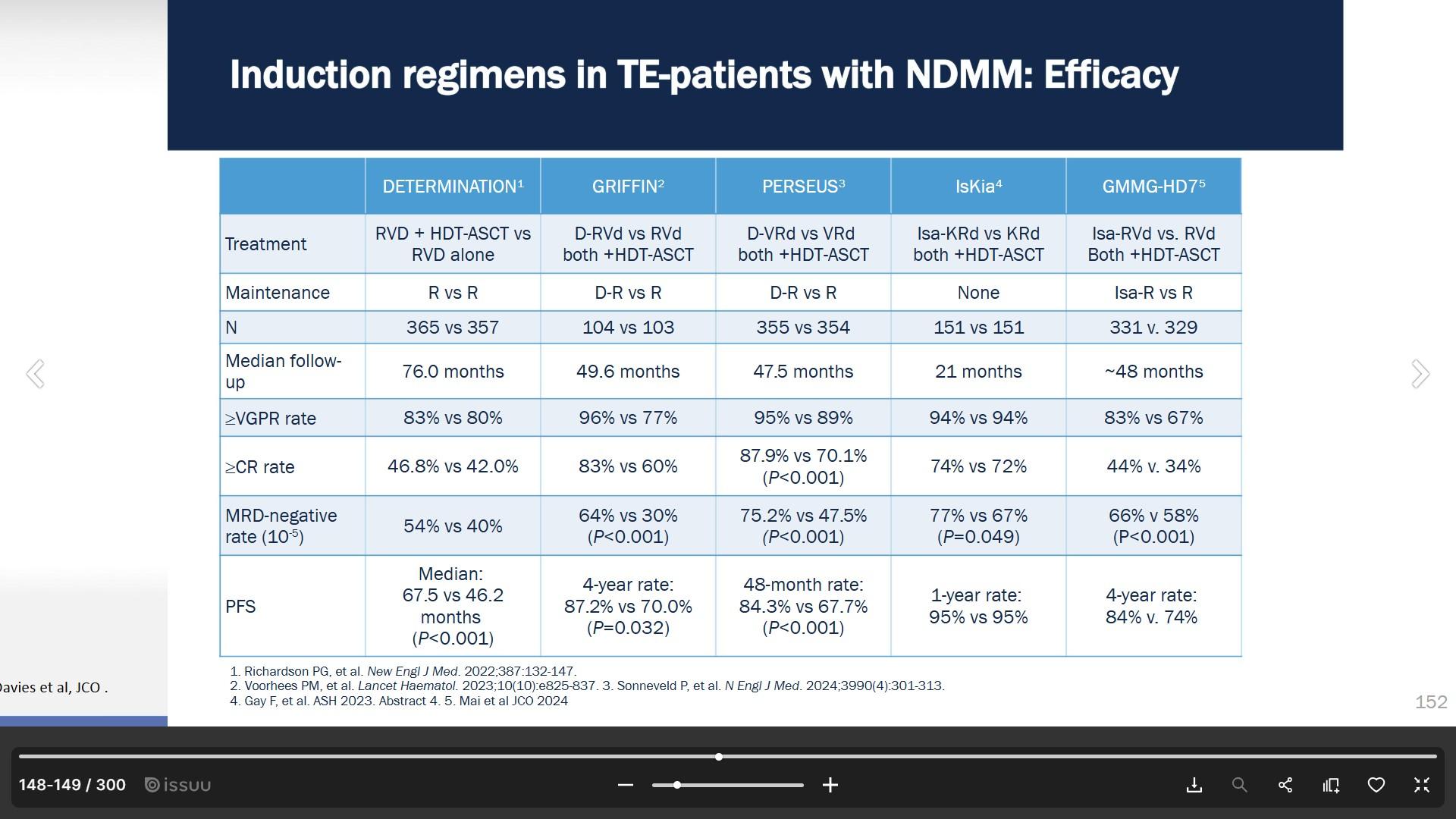
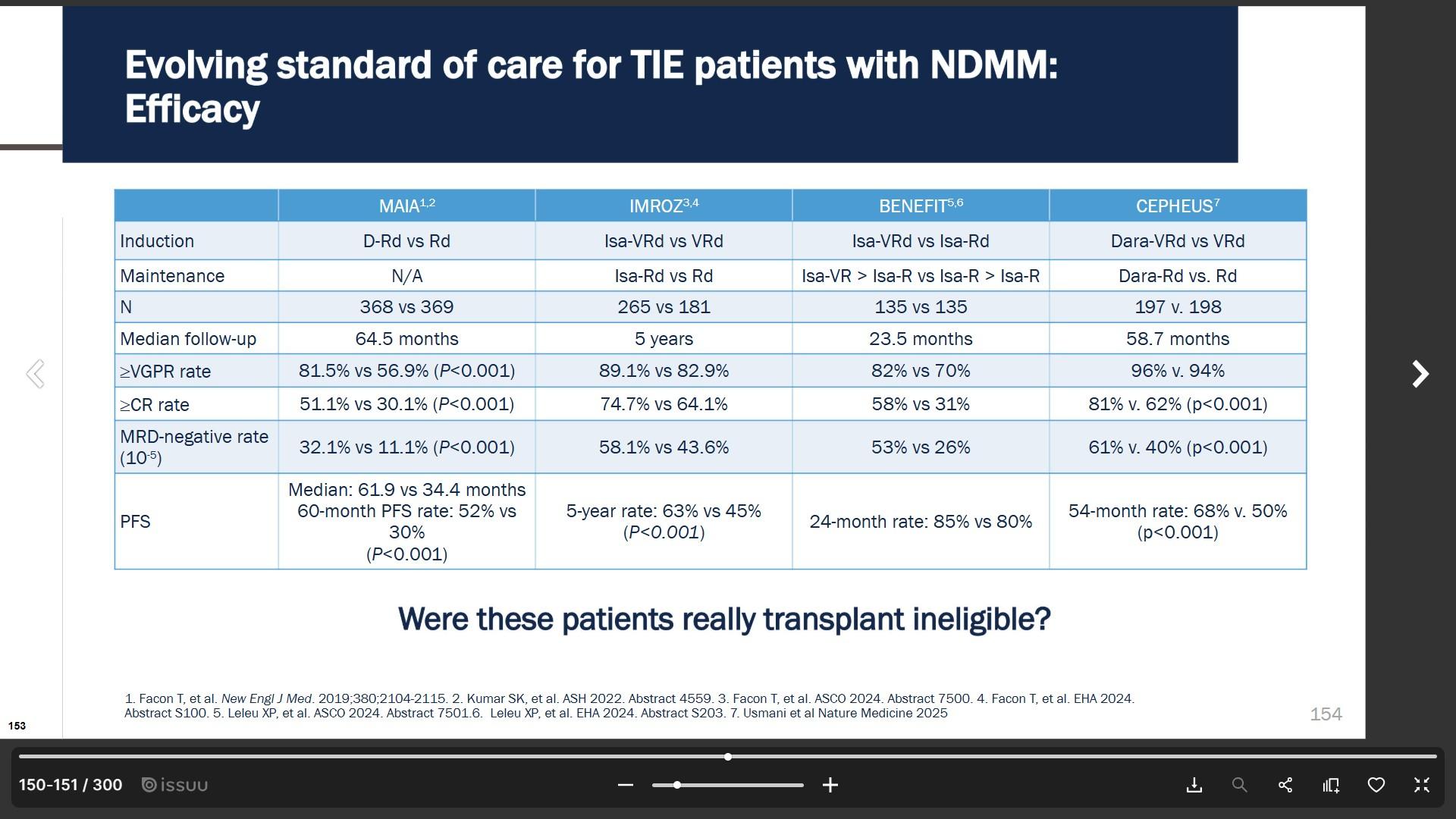
Efficacy of Induction Regimens for Transplant Eligible
Newly Diagnosied Multiple Myeloma
Treatment of Newly Diagnosed Myeloma
Transplant Ineligible
1945 -the first “chemotherapy” used for myeloma was the antibiotic combination of Stilbamidine and Pentamidine. Blood.1946 Nov;1(6):534-6.
mSMART Guidelines
Transplant Ineligible
STANDARD RISK MYELOMA
HIGH RISK MYELOMA
Dara-VRd or Isa-VRd for ~9 cycles followed by Len maintenance
For frail patients: DRda
Dara-VRd or Isa-VRd for ~9 cycles followed by bortezomib plus lenalidomide maintenance
Or
For frail patients: DRd or VRd for ~9 cycles followed by doublet DR or VR maintenance
aDuration is usually until progression, based on tolerance
Dispenzieri et al. Mayo Clin Proc 2007;82:323-341; Kumar et al. Mayo Clin Proc 2009 84:1095-1110; Mikhael et al. Mayo Clin Proc 2013;88:360376. v22 //last reviewed Oct 2024
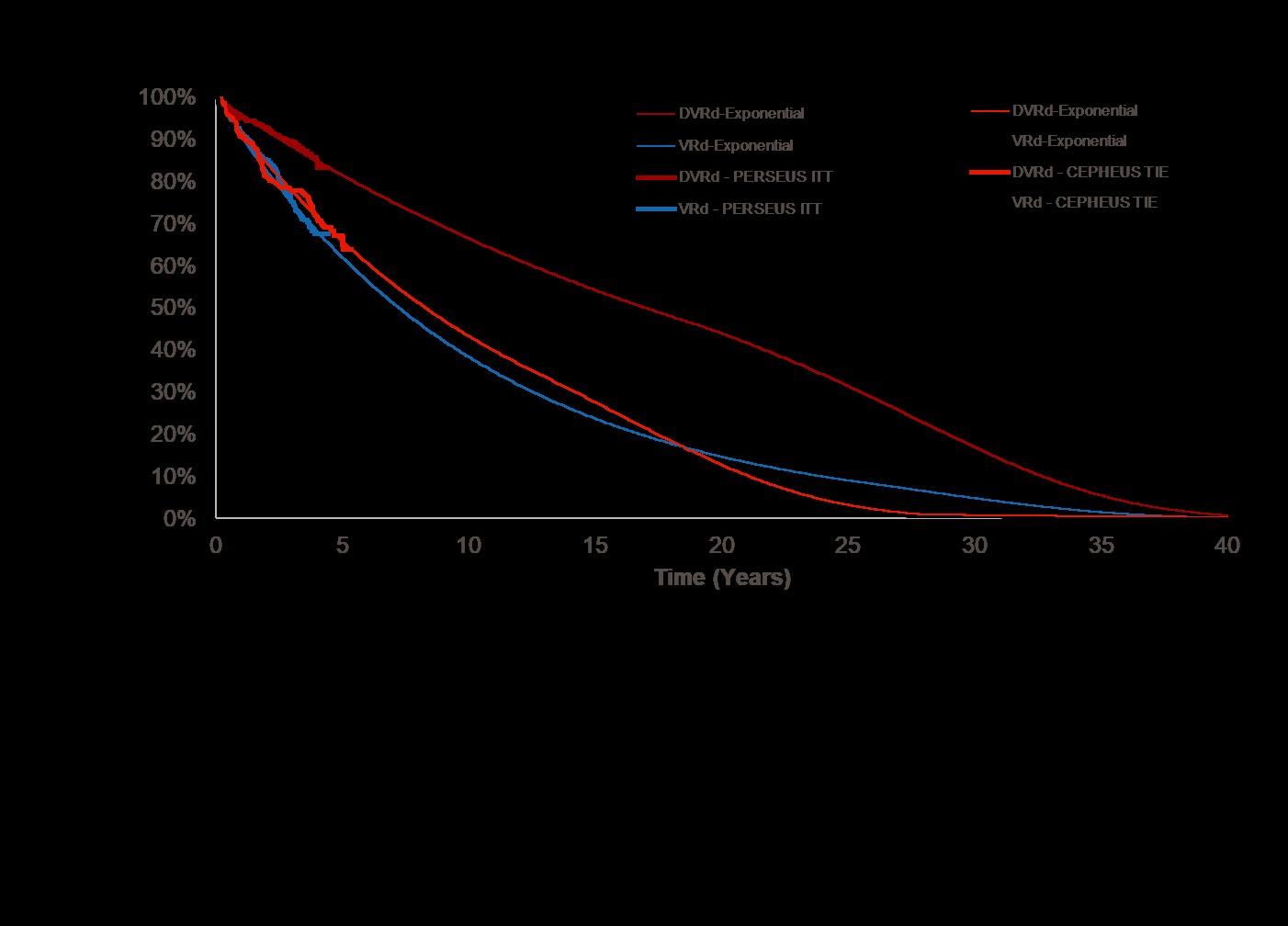
Significantly
Longer Estimated Progression
Survival (PFS) Projections With DVRd vs VRd
VRd-Exponential PERSEUS ITT
DVRd – PERSEUS ITT
VRd – PERSEUS ITT
DVRd-Exponential CEPHEUS TIE
VRd-Exponential CEPHEUS TIE
DVRd – CEPHEUS TIE
VRd – CEPHEUS TIE
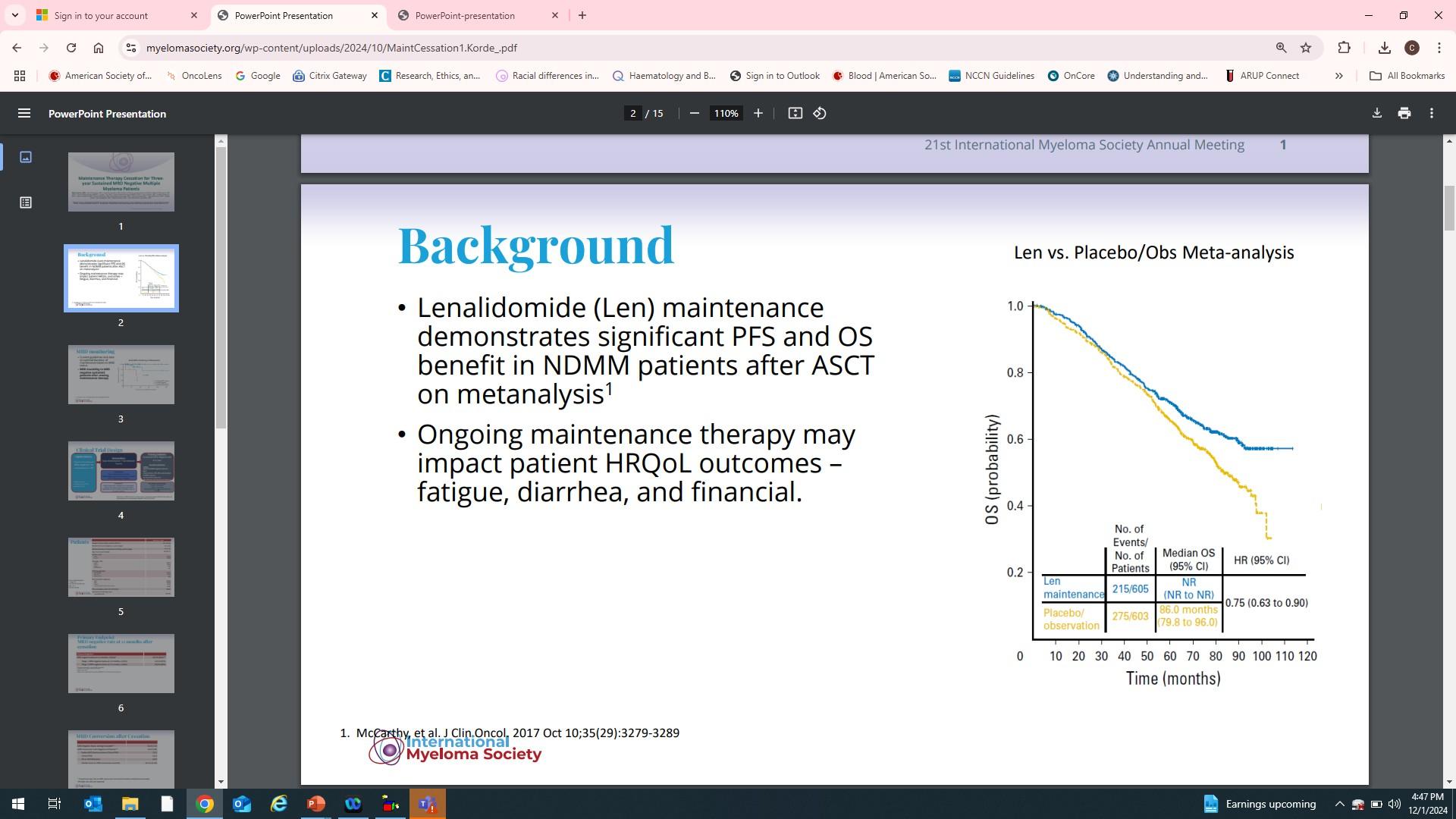
Maintenance Therapy in Myeloma
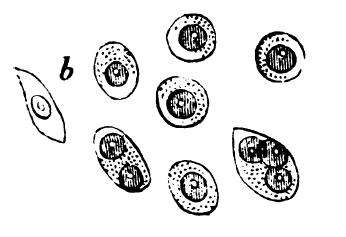
1846- The plasma cells of the second patient described with Mollities Ossium (Multiple Myeloma Mr.
Made from drawings by Mr Dalrymple.
Dublin Quarterly Journal of Medical Science.1846 2, 85-95.
McBean
• Maintenance is to prevent disease progression for as long as possible while maintaining favorable quality of life
• Data from 4 randomized trials of Revlimid
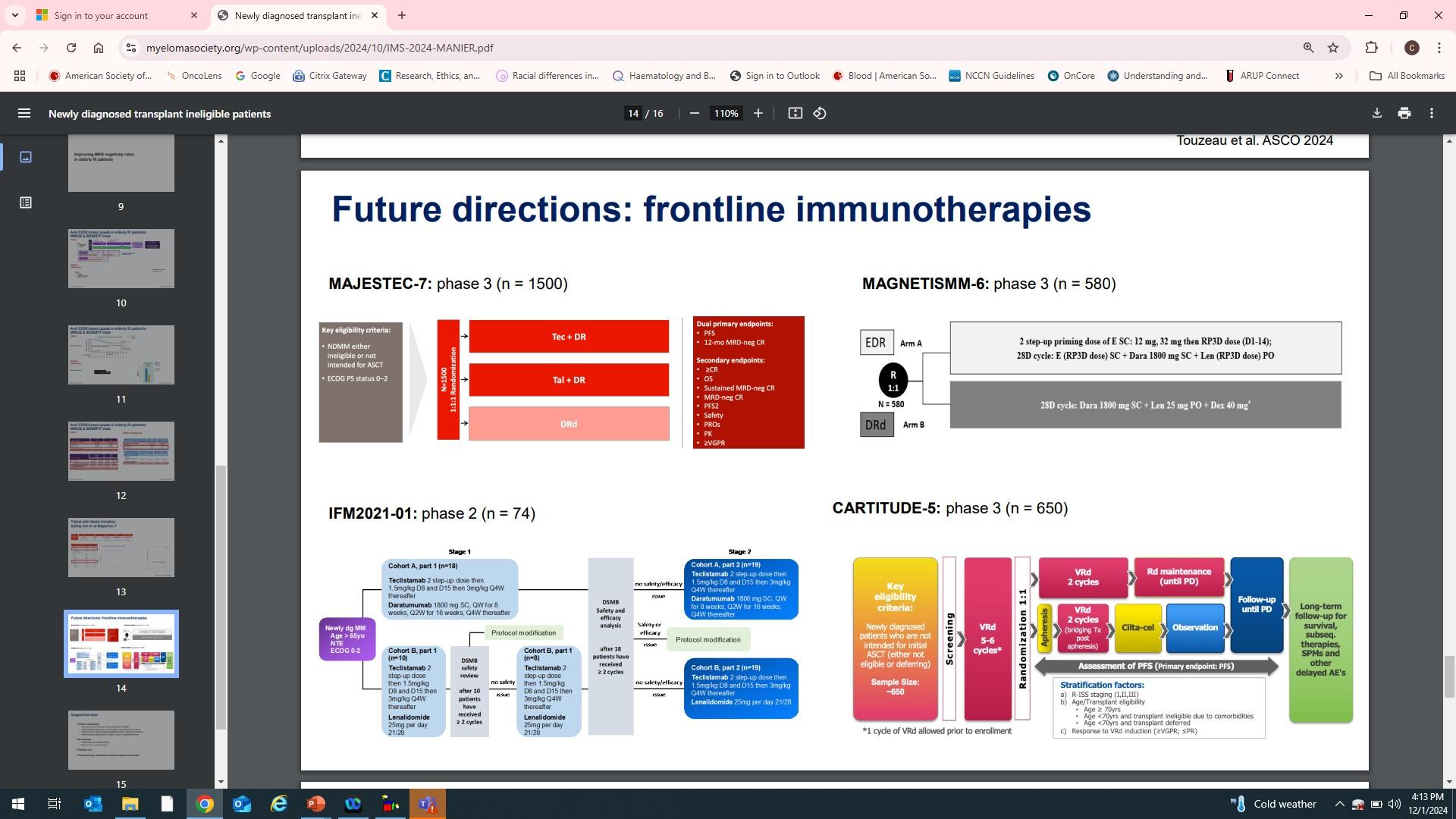
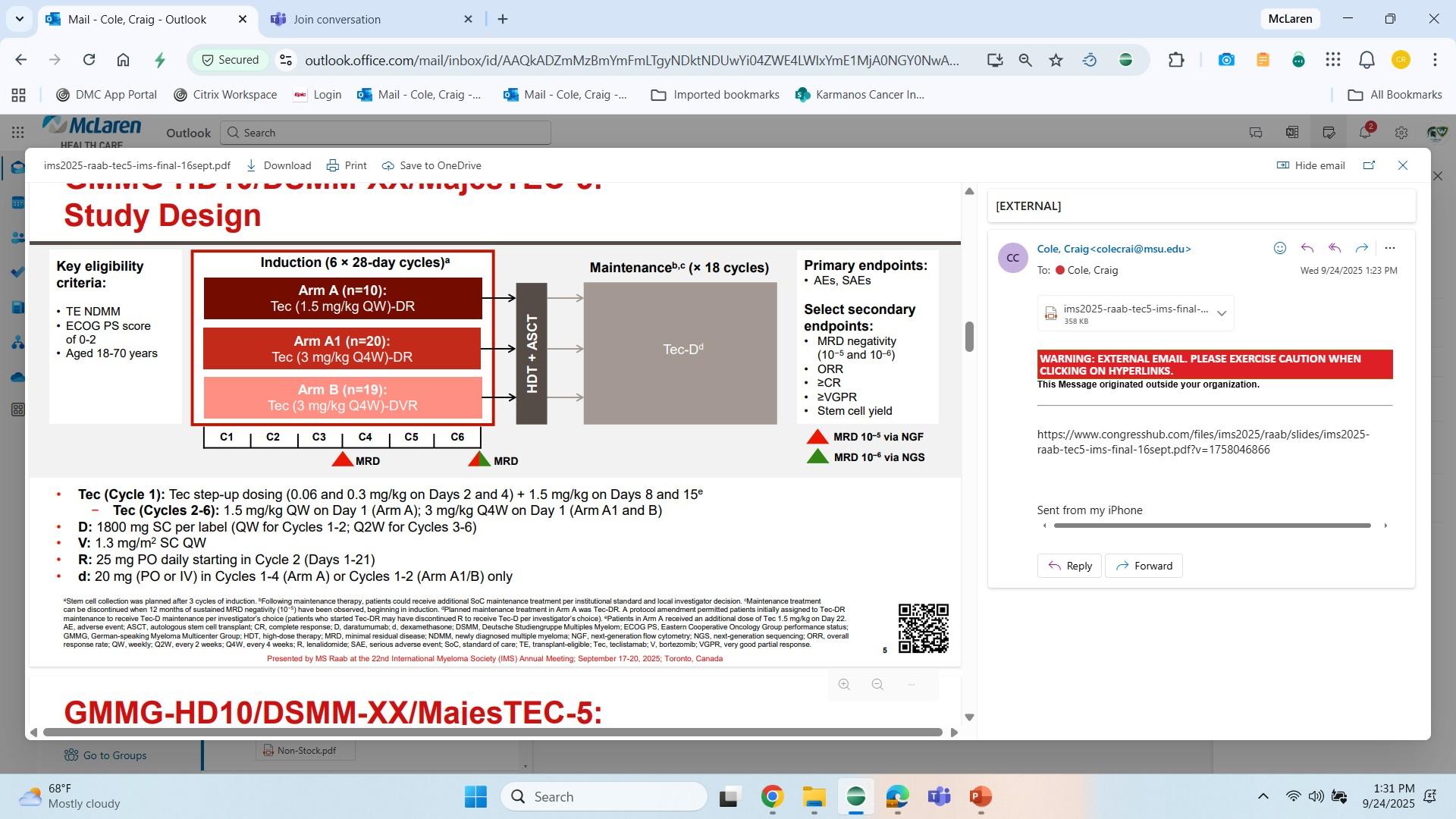
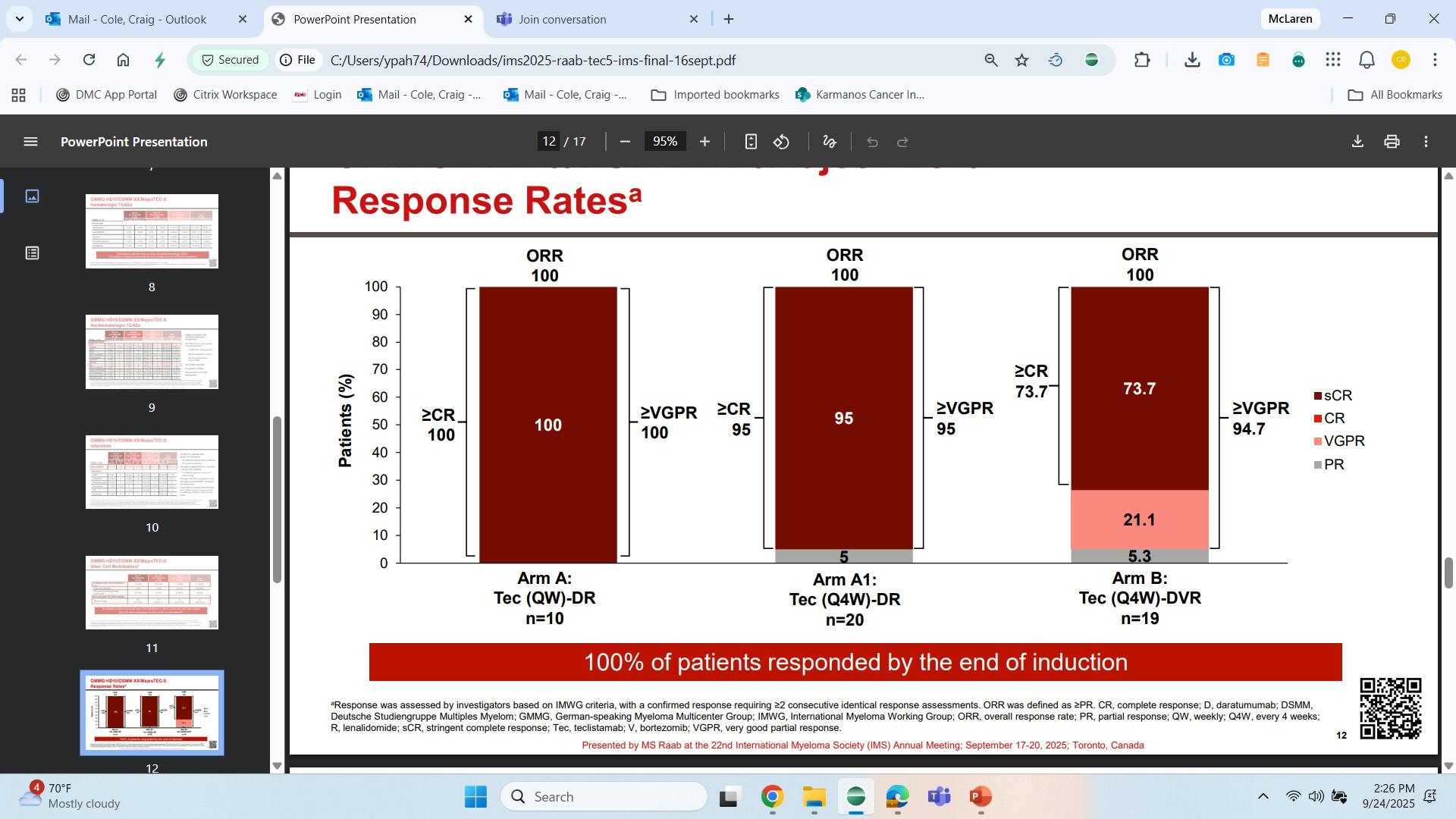
MajesTEC-5 trial evaluating teclistamab (Tec) +
Standard daratumumab (D)-based regimens in patients with transplant-eligible NDMM: Design
Breakout B: Managing Relapsed Myeloma
Rahma Warsame, MD
Mayo Clinic, Rochester, MN
RELAPSED MULTIPLE MYELOMA
Rahma Warsame, M.D. Associate Professor of Medicine & Oncology
International Myeloma Foundation, Patient and Family Seminar
October 4, 2025
DISCLOSURES:
• Consulting:
• Third bridge
• Sanofi
• Off label discussion
• Belantamab mafadotin
• Venetoclax
• Anitocel
LEARNING OBJECTIVES
Identify important definitions for response & relapse
Understand the considerations for treatment of relapsed myeloma
Timing and optimal candidate for different immune based therapy
Learn about Unique toxicities
IMPORTANT DEFINITIONS
•Depth of Response (DOR):
•Minimal residual disease negative (MRD –ve), sCR and no evidence of disease by NGS or flow cytometry
•Stringent CR: no disease in bone marrow or blood/urine
•CR: <5% in bone marrow, no disease in blood/urine
•VGPR: 90% reduction in free light chains (FLC), M spike, urine proteins
•PR: 50% reduction in FLC, M spike, Urine protein
•NR
IMPORTANT DEFINITIONS - CONT
•Objective response rate: Percentage of patients in a study or treatment group who experience a partial or complete response
•Progression free survival: Length of time during and after a treatment that a patient lives with disease without it worsening
•Includes disease progression AND death
•Overall survival: Length of time from diagnosis or start of treatment until death from any cause
IMPORTANT DEFINITIONS - CONTINUED
•Progression: worsening of disease that was never eradicated
•Worsening M spike, FLC, worsening or new bone lesions, worsening urine proteins
•Relapse: reappearance of disease (bone, blood, bone marrow, or urine)
•Refractory: relapse while receiving a particular therapy (i.e. Lenalidomide)
•Lines of Therapy (LOT) : Number of treatment regimens you have had
•Class exposed: Types of drug families you've already received exposed
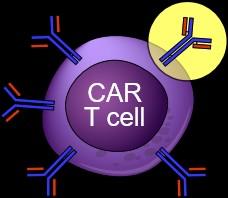
• MM cells use these proteins for cellular communication, survival, and potential target for drugs
• T cells
• Type of white blood cells
• Usual function to fight infections and cancer
• Stimulated by other immune cells to identify target proteins
• Identify cancer through T-cell receptor
• Antibodies
• Proteins produced by plasma cells to fight infections
• Attach to specific protein pathogens and cancer cells
• Very specific (1 antibody has only 1 target protein)
WHAT TO CONSIDER FOR RELAPSED DISEASE
BIOCHEMICAL RELAPSE MAINTENANCE RESIDUAL TOXICITY PERFORMANCE STATUS PRIOR LINES OF TREATMENT
DURATION OF RESPONSE NEW MUTATIONS
WHEN TO TREAT MYELOMA RELAPSE
• When there is any new organ compromise: start treatment immediately
• Restage with bone marrow if possible, to look for any new genetic mutations
• Biochemical relapse only:
THERE IS NO SPECIFIC NUMBER TO START TREATMENT
• Depends on the situation
• 1) Slow uptitration of FLC or M protein, may watch and wait
• 2) Trajectory of change, i.e. increases suddenly, changes swiftly
• 3) Limited treatment options available, may still watch for potential clinical trial options, or risk threshold
WHAT TO DO?
MYELOMA TREATMENT PARADIGM
Induction
Induction followed by continuous therapy Consolidation Maintenance S C T E l i g i b l e S C T I
Tumor Burden
TREATMENT LANDSCAPE
Alkylators/Cytotoxics
Pillars of Myeloma therapy
Steroids (Dexamethasone, Prednisone)
MM cells can:
• Decrease surface protein expression No more BCMA or GPRC5
STRATEGIES TO ESCAPE IMMUNE SYSTEM
• Mask as normal cell
• Decrease proteins requires to stimulate immune cells
• Express surface proteins to suppress normal immune cell activation
B CELL MATURATION AGENT
(BCMA) IS A FREQUENT TARGET FOR IMMUNOTHERAPY TRIALS IN MYELOMA
• BCMA is member of the TNF receptor superfamily
• Expressed nearly universally on myeloma cells
• Expression largely restricted to plasma cells and some mature B cells
• Play important role in plasma cell survival
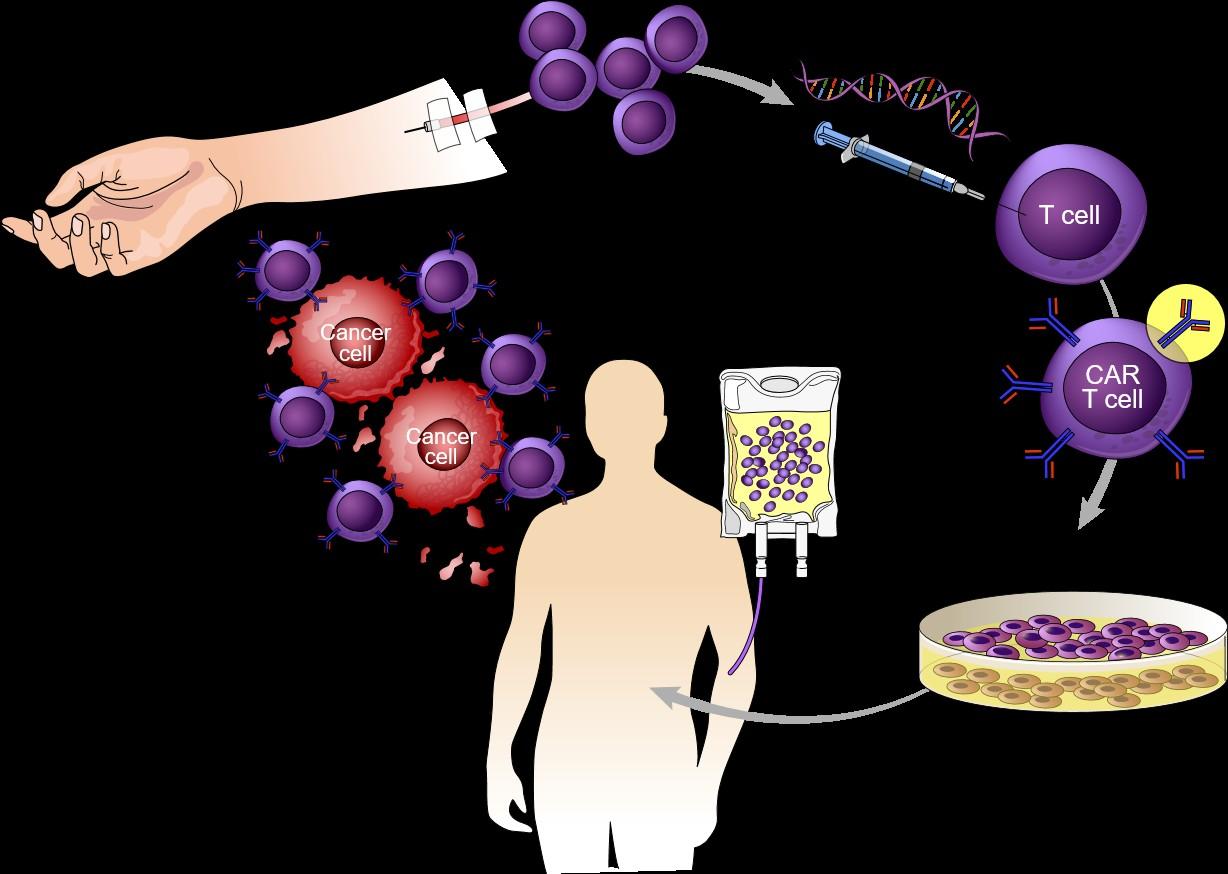
CHIMERIC ANTIGEN RECEPTOR T-CELL THERAPY
ELIGIBILITY FOR CAR T THERAPY
Disease not likely to progress too quickly
Meets trial guidelines or product labeling
Attempted at least 1 or 2 other lines of therapy that have failed (as per product label)
Is at least 3 months post-SCT risk for graft-versus-host disease
In generally good health (ECOG 0-2)
Adequate organ function and labs
Has a support system for patient and Caregiver
Locate hospital or CAR T treatment center and send all relevant patient files
Patient and caregiver should review logistical considerations
*In general, more patients would be eligible for CAR T-cell therapy compared to stem cell transplantation
**Fewer patients would be eligible for CAR T cell therapy compared to Bispecific Ab
Dave H, et al. Curr Hematol Malig Rep. 2019. doi.org/10.1007/s11899-019-00544-6, Beaupierre A, et al. Clin J Oncol Nursing. 2019;23(2):27-34, Perica K, et al. Biol Blood Marrow Transplant. 2018;24:1135-1141, Cohen AD. American Society of Clinical Oncology Educational Book 38 (May 23, 2018) e6-e15. doi: 10.1200/EDBK_200889
INTAKE
• Non-CAR MDs
• Administrative staff
• Financial coordinator Consultation
• CAR-certified MD
• Nurse coordinator
• Social worker
• Apheresis staff
IT TAKES A VILLAGE
Bridging Chemotherapy
• Non-CAR MDs
• CAR MDs
• Nursing
• Pharmacy
Infusion
• CAR MDs
• Cell therapy
• Nursing
• Pharmacy
• FACT
Acute care
• CAR MDs
• ICU, Neurology
• Nursing
• Pharmacy
• FDA
Late care
• Non-CAR MDs
• CAR MDs
• Nursing
• Pharmacy Regulation
• Financial Services
• Billing
• Data Management
• FACT, CIBMTR, FDA
Adapted from Perica K et al. Biol Blood Marrow Transplant. 2018;24(6):1135-1141.
CAR T-CELL THERAPY PROCESS
Remove blood from patient to get T cells
Make CAR T cells in the lab
Chimeric antigen receptor (CAR)
Antigens
Grow millions of CAR T cells
CAR T cells bind to cancer cells and kill them
Lymphodepleting chemotherapy
BCMA-DIRECTED CAR T CELLS: CURRENT STATE
RWE, real-world evidence.
Munshi NC et al. N Engl J Med. 2021;384(8):705-716; Berdeja JG et al. Lancet. 2021;398(10297):314-324; Martin T et al. J Clin Oncol. 2023;41(6):1265-1274; Hansen D et al. J Clin Oncol. 2023;41(11):2087-2120.
(KarRMa)
94.8%, G3-4: 4% Median onset, days Onset: 1 (1-12), duration: 5 (1-63) Onset: 7 (5-8), duration: 4 (3-6) Neurotoxicity All grade: 18%, G3: 3% All grade: 21%, G3-4: 9%
Median onset, days Onset: 2 (1-10), duration: 3 (1-26) Onset: 8 (6-8), duration: 4 (3-6.5)
RWE has demonstrated similar outcomes in commercially treated patients (idecel/cilta-cel) relative to the KarMMa/CARTITUDE-1 trial despite >50% being ineligible for trial inclusion.
CILTACABTAGENE
AUTOLEUCEL (CARVYKTI)
• Approved after 1 or more Line of therapy including PI and IMID AND lenalidomide refractory (4/4/24)
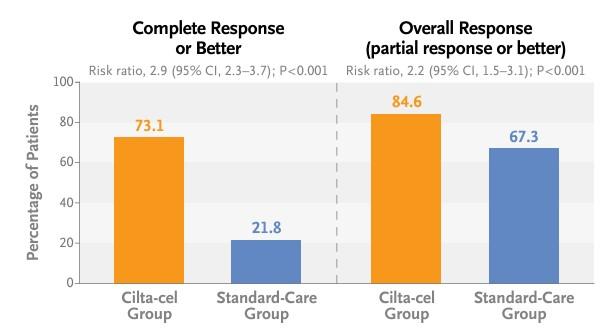
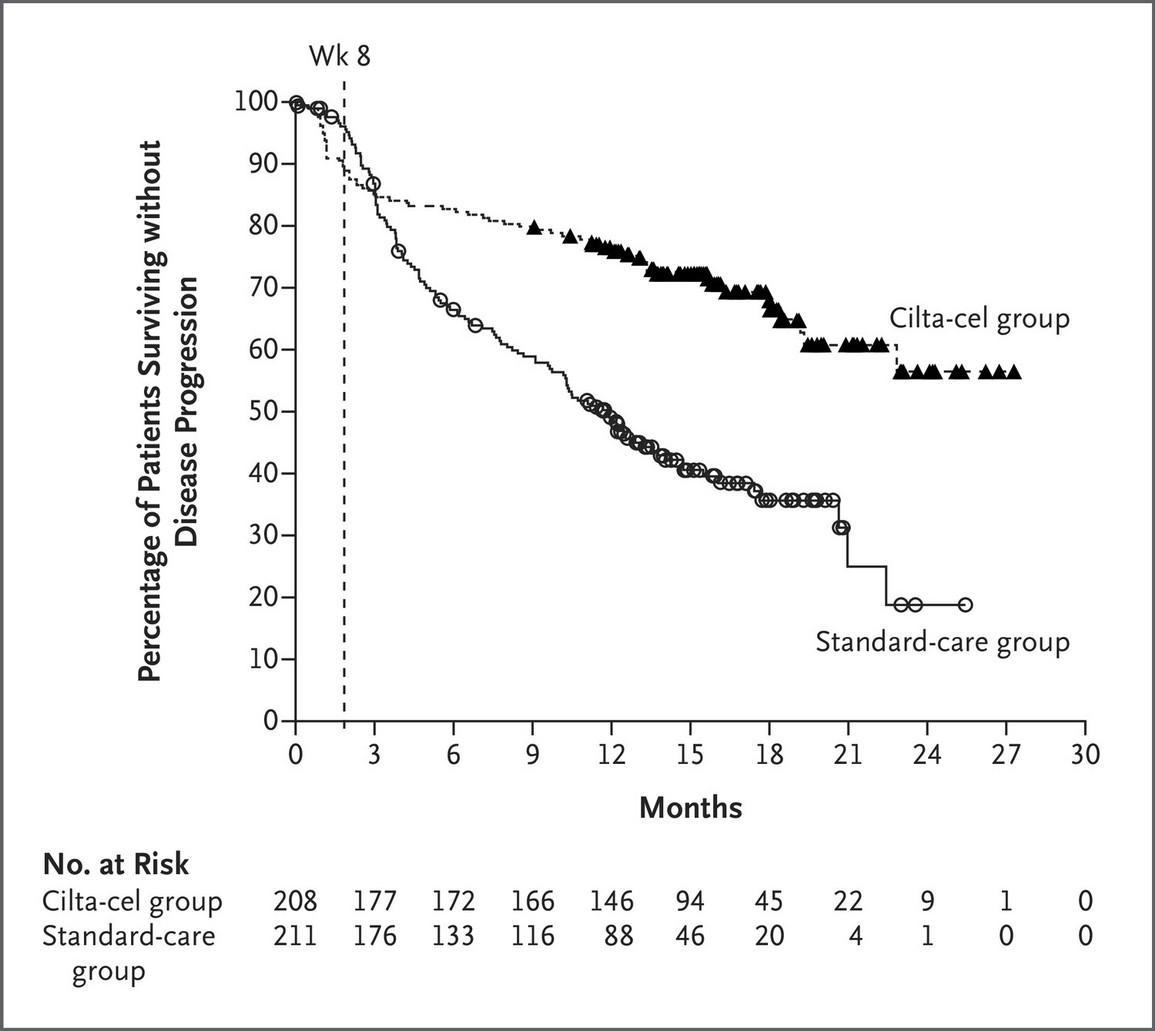
• Based on CARTITUDE 4 Ciltacel vs PVD or DPD
• Received PI/IMID, len refractory and after 1 to 3 LOT
• Triple class refractory 14% vs 16%
Ciltacel had retained significant PFS benefit in Triple class refractory patients
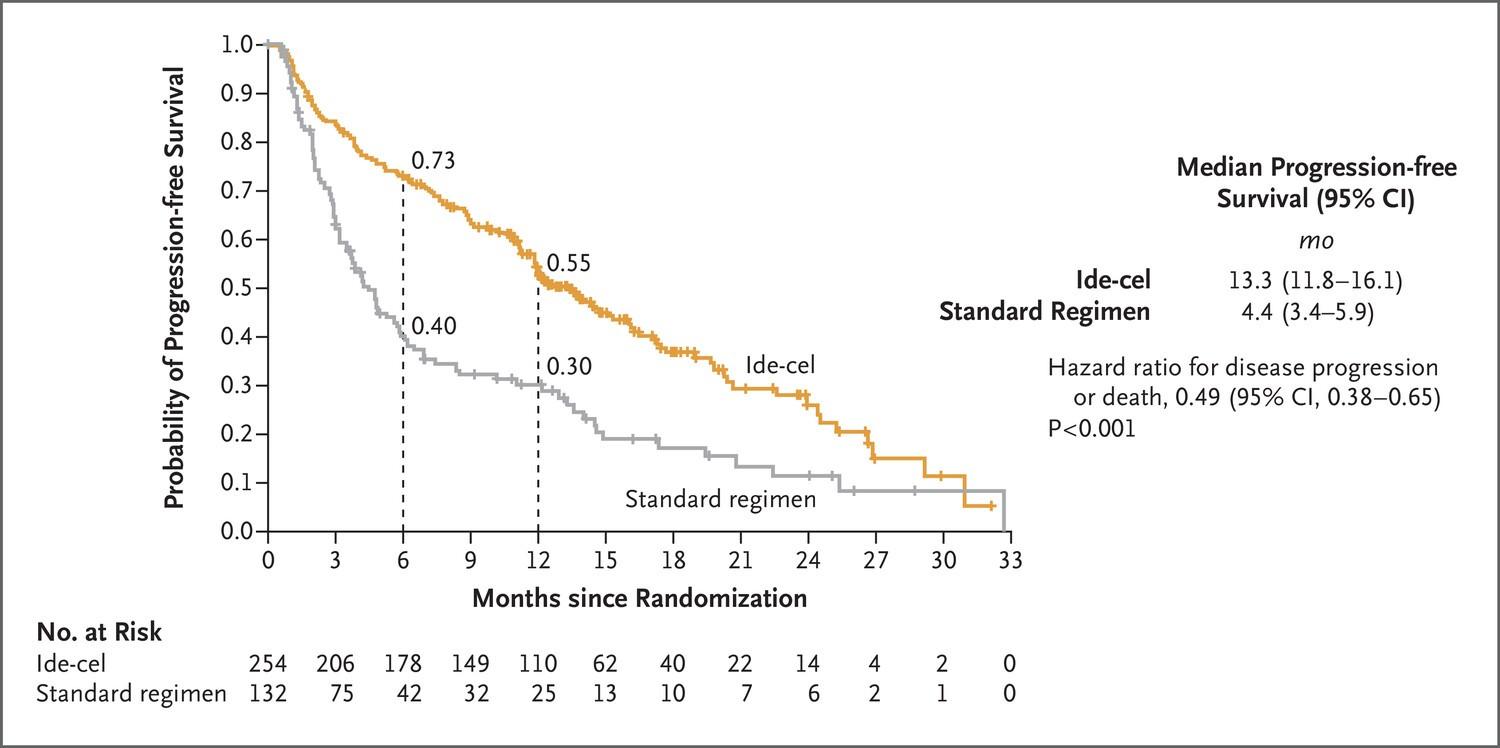
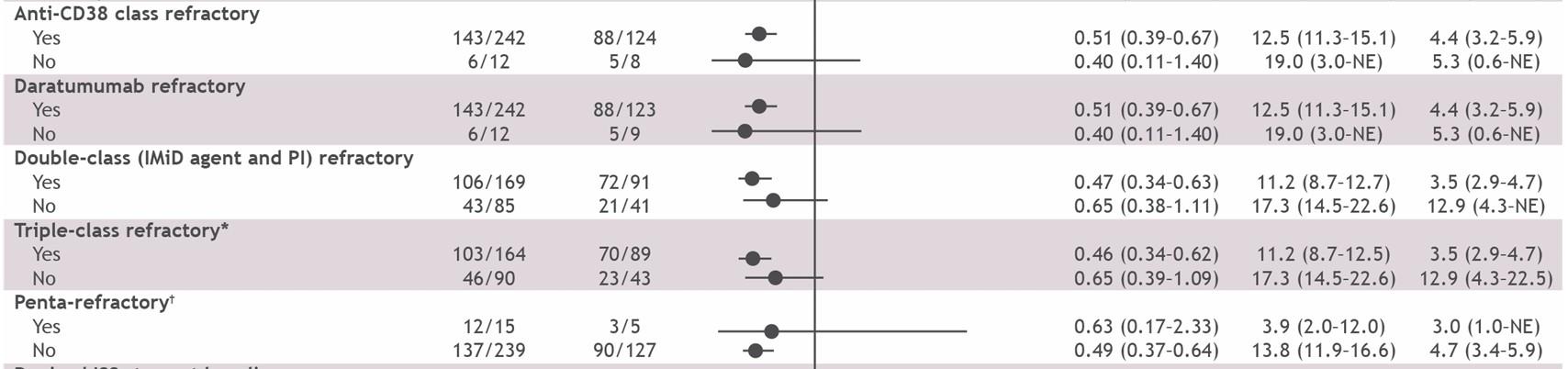
IDECABTAGENE VICLEUCEL
(ABECMA)
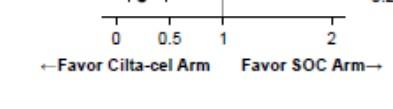
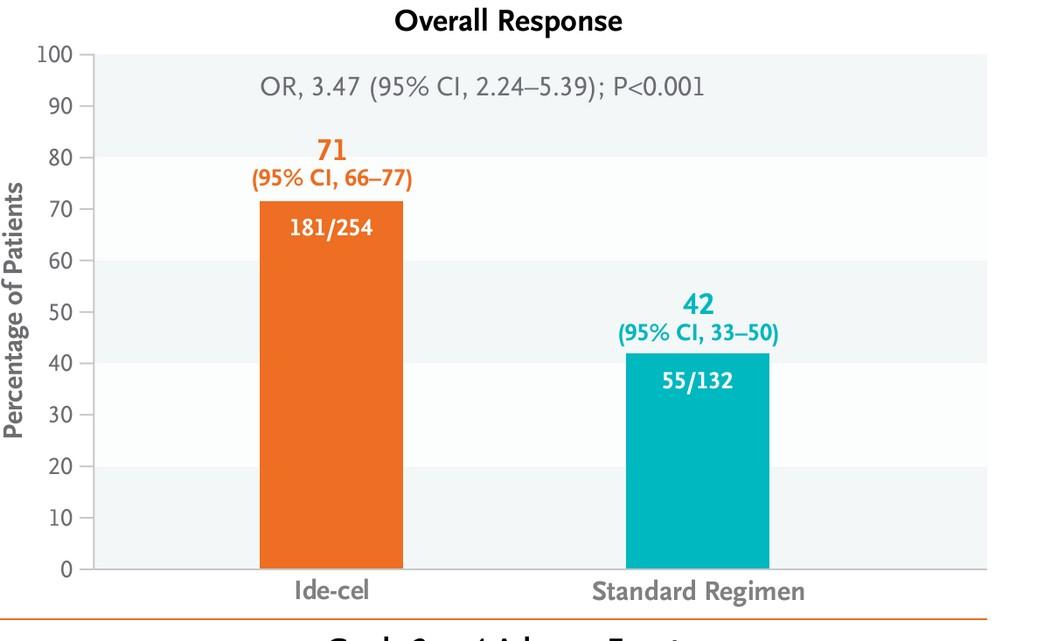
• Approved for patients with RRMM after two or more prior lines of therapy including an iMID, PI and CD38 antibody (4/4/24)
• Based on KarMMA-3: Idecel vs Standard Regimen after 2 to 4 LOT
• SOC: PVD, DVD, IxaPD, KD, EPD
• 1° end pt PFS
• Characteristics
• TCR 65% vs 67%
• HR 42% vs 46%
Forest Plot Subgroup Analysis shows Idecel PFS benefit maintained in Triple class refractory and Penta-refractory disease
CAR T-RELATED TOXICITY ONSET AND DURATION
Neelapu S et al. Nat Rev Clin Oncol. 2018;15:47-62; Brudno JN et al. Blood. 2016;127(26):3321-3330; National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. Management of immunotherapy-related toxicities, v1.2024.
NCCN Clinical Practice Guidelines in Oncology. Management of immunotherapy-related toxicities, v1.2024. NCCN Clinical Practice Guidelines in Oncology. Prevention and treatment of cancer-related infections, v2.2023.
IDE-CEL VS CILTA-CEL
• Single binding domain
• ORR ↑
• Median CRS onset ↓
• Outpatient administration ↓
• Cost ↑
• Availability • ADE incidence
• Patient population
Double binding domain
ORR ↑↑
Median CRS onset ↑
Outpatient administration ↑
Cost ↑↑
Summary: Access to timely treatment will often outweigh the safety and efficacy differences
ADE, adverse drug event. Davis J et al. Expert Rev Hematol. 2022;15(6):473-475.
ANITOCABTAGENE AUTOLEUCEL (ANITO-CEL)
• iMMagine-1 R/R MM
• >4 LOT
• 12-month f/u results
• (ORR) of 97%,
• 68% CR
• 12-month PFS 79% and OS 95%
• NO INCIDENTS OF DELAYED NEUROTOXICITY
WHY DOES CAR T NOT ALWAYS WORK ?
MM is too aggressive (progresses before infusion)
Patient T cells are less effective (manufacturing failure, or weakened T cell)
Do not persist long enough
Loss of target by MM cell
BISPECIFIC ANTIBODY
Bispecific antibody
T-cell
IMMUNE SYNAPSE BETWEEN T-CELLS AND TUMOR
CELLS ESSENTIAL FOR BISPECIFIC MEDIATED TUMOR LYSIS
Tian, Z et al. Bispecific T cell engagers: an emerging therapy for management of hematologic malignancies. J Hematol Oncol 14, 75 (2021)
WHO IS ELIGIBLE FOR IMMUNOTHERAPY
BISPECIFIC AB SUMMARY
Route SC SC SC
Step-up: 0.06 mg/kg > 0.3
mg/kg > 1.5 mg/kg
Dosing
Treatment: 1.5 mg/kg
weekly; transition to biweekly if in CR after 6 months
Step-up: 12 mg > 32 mg > 76 mg
Treatment: 76 mg weekly;
transition to biweekly if PR or better after 6 cycles
Tecvayli. Prescribing information. Janssen Biotech; February 2024; Moreau P et al. N Engl J Med. 2022;387:495-505; Elrexfio. Prescribing information. Pfizer; August 2023; Lesokhin AM et al. Nat Med. 2023;20(9):2259-2267; Talvey. Prescribing information. Janssen Biotech; August 2023; Chari A et al. N Engl J Med. 2022;387(24):2232-2244.
UNIQUE TOXICITY FOR TALQUETAMAB
Skin Related Events
• Asteatotic eczema
• Dry skin
• Eczema
• Pruritus
• Skin exfoliation
• Skin fissures
• Hyperpigmentation
• Lesions or ulcers
Rash Related
Events
• Contact dermatitis
• Dermatitis
• Erythematous rash
• Generalized exfoliative dermatitis
• Maculopapular rash
• Rash
Chari A et al. N Engl J Med. 2022;387(24):2232-2244.
Nail Related
Events
• Nail bed disorder
• Discoloration
• Dystrophy
• Hypertrophy
• Ridging
• Onycholysis
• Onychomadesis
Oral Toxicity
• Dysgeusia
• Dry mouth
• Dysphagia
• Poor appetite
• Weight loss
PRACTICAL TIPS FOR TALQUETAMAB
• Use ammonium lactate lotion on hands and feet twice daily. Recommend SPF 30 or greater for daily use.
• Nail changes: Recommend maintaining oral hydration with at least 8 glasses of water daily.
• Oral toxicity: Maintain good oral hygiene by brushing and flossing twice daily. Avoid alcohol based mouthwashes which can worsen dry mouth. If having difficulty swallowing or eating, contact your hematology team immediately.
• Other side effects: low blood counts, increased infection risk, and injection site reactions
BISPECIFIC ANTIBODY THERAPY UNDER STUDY
Not Exhaustive list
Bispecific Antibody Targets
Route of Administration ABBV-383 (TNB-383B)
Forimtamig (RO7425781)
Cevostamab (BFCR4350A)
FcRL5, fragment crystallizable receptor-like 5.
Lee H et al. Hematology Am Soc Hematol Educ Program. 2023(1):332-339.
•Who should get CAR T cell early?
•What order do you sequence immunotherapy?
•How do you manage toxicity, especially delayed toxicities?
•Where can these treatments be conducted?
BISPECIFIC AB VS CART CONSIDERATIONS?
Bispecific T cell Ab CART
Off-the-shelf option
Manufacturing limitations, limited slots, manufacturing failure up to 10% *
Production times for CAR-T vary from 4 to 6 weeks
No Bridging Likely need interim bridging treatment until CART infusion No Lymphodepletion required LD chemo with fludarabine and cyclophosphamide Lower grade CRS/ICANS Higher grade and frequency of CRS/ICANS Can be used in
Kegyes, D., Constantinescu, C., Vrancken, L. et al. Patient selection for CAR T or BiTE therapy in multiple myeloma: Which treatment for each patient?. J Hematol Oncol 15, 78 (2022)*Majzner RG, Mackall CL. Clinical lessons learned from the first leg of the CAR T cell journey. Nat Med. 2019;25(9):1341–55
ANTIBODY
DRUG CONJUGATE
BELANTAMAB (ADC)
Benefits
• Targeted release of chemotherapy/immunotox in/immunotherapy
• Attracts immune cells that clear cancer even if the treatment does not
• Dead cancer cells attract even more immune effector cells enhancing its potential response Risk
• Ocular toxicity is common and significant
DREAMM-7: BVd led to a significant increase in PFS vs DVd
Danielle Doheny, Director of Public Policy and Advocacy
International Myeloma Foundation
2025 Myeloma Advocacy Priorities & How You Can Get Involved
Danielle Doheny IMF, Director of U.S. Policy & Advocacy
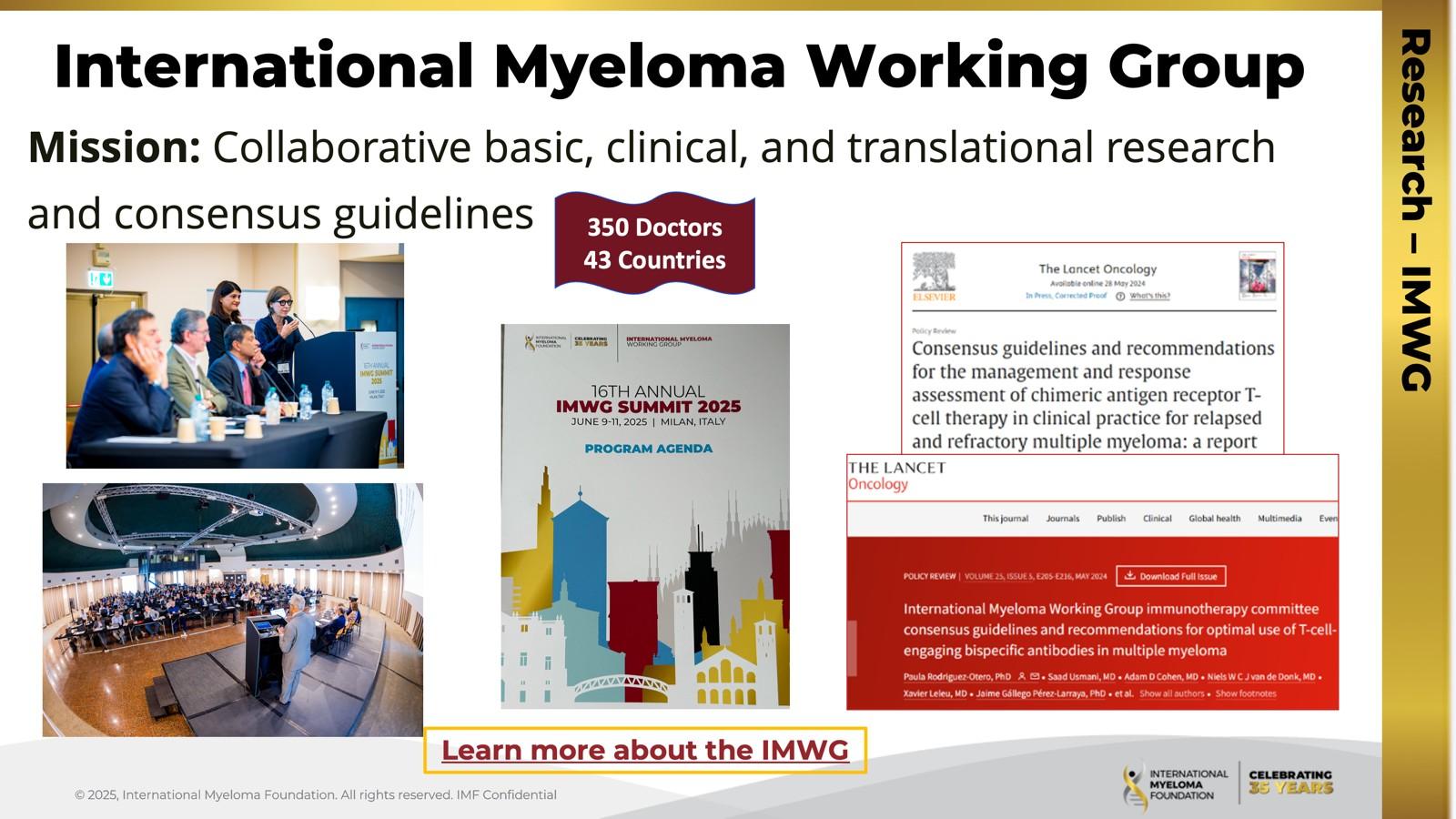
Introduction | Advocacy at the IMF
The Global Advocacy Team collaborates with multiple stakeholders to inform and influence decision-making on the critical healthcare issues that directly impact myeloma patients.
The U.S. Advocacy Team advocates for equitable access to timely diagnosis, innovative treatments and research on Capitol Hill and with key regulatory
The team advocates both alongside of and on behalf of the patient community that we serve.
Advocacy play a critical role to educate policymakers about the issues important to our community and motivate them to act.
What Do We Advocate For?
The following policy principles are the foundation on which we prioritize our advocacy work.
1. Ensure Access to Care: We advocate for policies that ensure all myeloma patients have equitable, comprehensive, patientcentered care without insurance barriers that limit options or delay treatment initiation.
2. Eliminate Financial Barriers: We advocate for policies that allow myeloma patients access to treatments and supportive care interventions without facing financial hardships.
3. Advance Myeloma Research: We advocate for annual appropriations funding for myeloma research and the advancement of clinical trial eligibility and research protocols that ensure representation from diverse populations.
2025 U.S. Advocacy Priorities Snapshot
1. ENSURE ACCESS TO CARE
2. ELIMINATE FINANCIAL BARRIERS
3. ADVANCE MYELOMA RESEARCH
INSURANC E REFORM: DRUG ACCESS
Step Therapy Protocols Safe Step Act
INSURANC E REFORM: COINSURANCE
Oral Parity Cancer Drug Parity Act
INSURANC E REFORM: DRUG ACCESS PBM Reform PBM Reform Act
INSURANC
E REFORM: COPAYS Copay Accumulators HELP Copays Act
FEDERAL FUNDING
ANNUAL APPROPS
Annual Appropriations
NIH: National Cancer Institute, National Institute on Minority Health, ARPA-H
CDC: Comprehensive Cancer Control Initiative
DoD: Congressionally Directed Medical Research Program (CDMRP) for Myeloma.
MEDICARE REFORM:
PHYSICIAN ACCESS
Tele-Health/Medicine
Telehealth Modern. Act
MEDICARE REFORM: ANNUAL COST LIMITS
Inflation Reduction Act implementation Cap & Smoothing (MPPP), Drug Pricing, Drug Formularies
CLINICAL
TRIAL ACCESS
Primary care education, Focus on underserved, POC, rural settings and socioeconomically disadvantaged groups
Inflation Reduction Act (IRA) & Highlight of Changes to Medicare
Inflation Reduction Act (IRA) of 2022 is a federal law which aims to curb inflation by working to reduce the federal government budget deficit, lowering Medicare prescription drug prices and investing in domestic energy production.
3.
• Inpatient hospital stays • Care in a Skilled Nursing Facility
• Hospice Care
• *Does not cover regular MD visits or Rx drugs
What is Going on in DC/Why This is Important to Us
• Cancer and Public Health Funding:
Proposed cuts to NCI, NIH, CDC, and CDMRP threaten cancer research, treatment advances, and public health programs. The Senate has rejected these cuts in a bipartisan, but continued advocacy is essential to maintain progress.
• Reconciliation and Medicaid Cuts:
Proposed Medicaid cuts could reduce healthcare access for vulnerable patients. We’re actively advocating to protect Medicaid’s role in ensuring timely, affordable treatment.
• Cancer Drug Parity Act & Access Issues:
The Cancer Drug Parity Act, recently introduced in the House, aims to ensure insurance covers oral cancer drugs equally to IV treatments by lowering out-of-pocket costs and improving access. We continue working with congressional champions to advance this bill despite broader legislative challenges
How You Can Get Involved
Blood Cancer Awareness Month Capitol Hill
Visit
Your Voice Matters in Washington, D.C.
•Together, we’ll share stories and advocate for better treatment access and research funding.
•No policy expertise needed: Just a willingness to share your experience.
•We provide guidance every step of the way.
•Note: This session is full; patients for September are already trained and ready.
•You can’t join this time, but you can get trained now!
•This September, IMF will bring myeloma patients and caregivers to Capitol Hill to meet with lawmakers.
•Email us to take our Master Class and prepare for the next Hill Day.
Addressing healthcare barriers for multiple myeloma patients depends on winning over the hearts and minds of policymakers. It is not enough to just identify an issue and have data-driven evidence/research to back it up. It is not even enough to work with coalition partners that agree with our point of view. We must convince policymakers to prioritize our issues, draft legislation and vote it into law. Email
Thank You
Symptom Management and Living Well with Myeloma
Tiffany Richards, PhD, ANP-BC, AOCNP®
University of Texas MD Anderson Cancer Center, Houston, TX
Myeloma: Putting the Pieces of the Puzzle Together
Tiffany
Richards, PhD, ANP-BC, AOCNP®
MD Anderson Cancer Center
A presentation from the IMF’s Nurse Leadership Board
Myeloma: Putting The Pieces of the Puzzle
Focus on Managin g Sympto ms
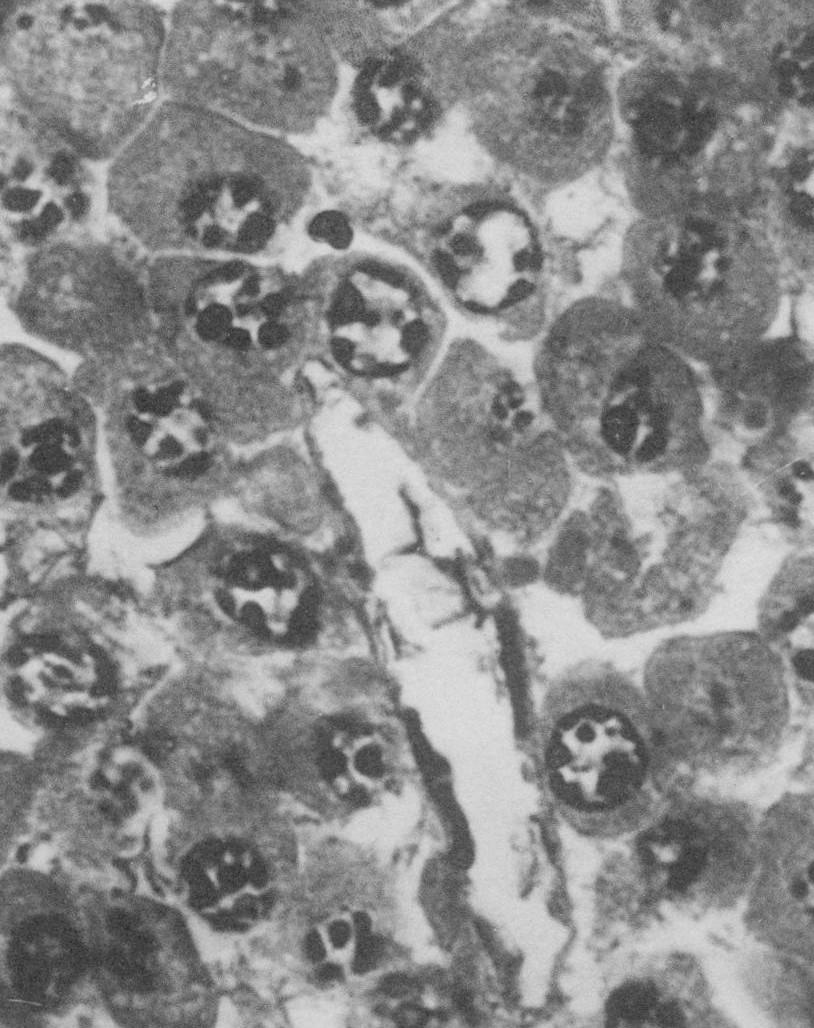
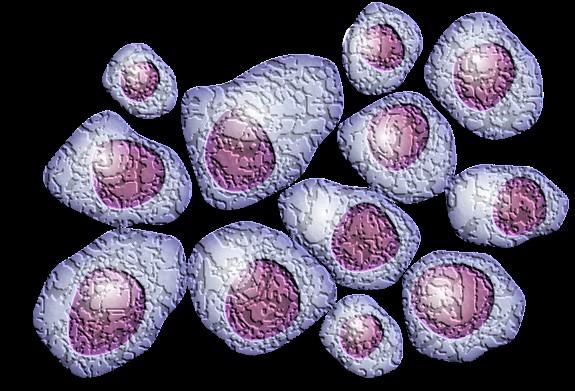
Myeloma Is a Cancer of the Plasma Cells
Plasma Cells come from white blood cells produced in the bone marrow and make many different antibodies to help fight infection (polyclonal).
In Multiple Myeloma, one plasma cell mutates, making many identical plasma cells (monoclonal).
Bone marrow
Bone marrow
Myeloma Causes Cell Dysfunction &
Anxiety
Stress
Depression
Decreased red blood cells
Anemia & Fatigue
Decreased white blood cells
Myeloma protein in blood and urine
Changes in bone remodeling
Clonal myeloma plasma cells can cause many symptoms
– Crowd out normal bone marrow cells
– Produce myeloma protein
– Can cause kidney dysfunction
– Affect bone cells (balance of osteoclasts & osteoblasts)
Immune Dysfunction & Infection
Renal Dysfunction
Infections Are Serious for People with Myeloma
Preventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
Treatment of Newly Diagnosed Multiple Myeloma (NDMM)
Induction
Consolidation
Initial treatments aimed at reducing the amount of myeloma cells
Intensification of treatment to deepen response. Either additional cycles of induction or autologous stem cell transplant (in eligible patients)
Prolonged lower-intensity treatment designed to sustain remission
Induction Standard of Care
Induction
Quadruplet therapy is preferred for nearly all patients with newly diagnosed myeloma
Anti-CD38 monoclonal antibody (mAb)
• Darzalex (daratumumab)
• Sarclisa (isatuximab)
Proteosome
Inhibitor (PI)
• Velcade (bortezomib)
• Kyprolis (carfilzomib)
At infusion clinic: subcutaneous injection or infusion
Supportive medication:
Immunomodulator
y drug (IMiD)
• Revlimid (lenalidomide)
• Pomalyst (pomalidomide)
Steroid
• Decadron (dexamethasone)
• Prednisone
Oral medication taken at home
• Antiviral prophylaxis (i.e., acyclovir or valacyclovir) to prevent viral infections particularly shingles.
• Antibacterial agents (i.e., Bactrim, levofloxacin) to prevent bacterial infections.
• Aspirin or other anticoagulant therapy to reduce the risk of blood clots from IMiDs.
• Bone-strengthening agents (i.e., zoledronic acid, denosumab) to strengthen bones and protect against fractures.
Steroids: An Important Piece Of The Treatment Plan
Steroids enhance the effectiveness of other myeloma therapies
Your provider may decrease or discontinue the dose as myeloma responds to therapy.
Do not stop or alter your dose of steroids without discussing it with your provider
Steroid Side Effects
• Irritability, mood swings, depression
• Blurred vision, cataracts
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Difficulty sleeping (insomnia), fatigue
Managing Steroid Side Effects
• Flushing/sweating
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
Consistent schedule (AM vs. PM)
Take with food
Stomach discomfort: Over-thecounter or prescription medications
Medications to prevent shingles, thrush, or other infections
Rajkumar SV, et al. Lancet Oncol 11(1):29–37. King T, Faiman B. Clin J Oncol Nurs. 2017;21(2):240-249. Banerjee,R. et al. Blood 9.25.24
Peripheral Neuropathy
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e., diabetes).
Early reporting of symptoms may prevent worsening symptoms.
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Tariman, et al. CJON.2008;12(3)suppl:29-36. Zhao T, et al. Molecules. 2022;27(12):3909.
Blood Clots: Managing DVT and PE Risk
Blood clots can cause swelling, pain, discoloration (DVT), shortness of breath, chest pain, sense of doom (PE). Blood clots
► HCPs may manage DVT/PE risk by
• Adjusting medications and schedules
• Prescribing blood-thinning medications according to assessed risk (DOAC, aspirin, warfarin, heparin)
• Balancing the risk of DVT and PE with that of bleeding with low platelets
► Additional strategies to reduce risk of clots:
• Anti-embolism stockings (elastic stockings)
• Exercise regimen
• Moving frequently when sitting long periods
• Travel precautions (foot/leg exercises, walking, aspirin if not already on blood thinner)
DVT=Deep Vein Thrombosis; PE=Pulmonary
Embolism
are serious and can be life threatening.
Family History
Obesity
Immobility
Smoking
Surgery
Rome, S, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105. De Stefano, et al. Hematologica, 2022
Stem Cell Transplant
ELIGIBILITY
P H A S E 1
Measuring treatment response
Testing for Eligibility
Insurance authorization
Collecting stem cells
Duration: Approximately 2 weeks
Location: Transplant Center
A S E 2 TRANSPLANT
P H
HD-Melphalan
Stem cell infusion
Supportive Care
• GI Management
• Transfusions
• Antibiotics
Hair Loss
Engraftment
Duration:
Approx. 3-4 weeks
Location: Transplant Center
P H A S E 3
POSTTRANSPLA NT
Restrengthening
Appetite recovery “Day 100” assessment
Begin maintenance therapy
Duration: Approximatel y 10-12 weeks
Location: HOME
stem cell transplant remains the standard of care for eligible patients
Miceli T and Steinbach, M. Multiple Myeloma:
Multiple Myeloma. V1.2025.
GI Symptoms: Prevention & Management
Fluid intake can help with both diarrhea and constipation and helps kidney function
Constipation is more common in the induction phase
Opioid pain relievers, antidepressants, heart or blood pressure medications (check with provider, pharmacist)
Supplements: Calcium, Iron, vitamin D (rarely), vitamin B-12 deficiency
Anorexia, the inability to eat, is common during transplant and resolves with time.
• Hydration is most important
• Small, frequent meals with a focus on protein intake
• You will work closely with a dietician to help monitor your calorie intake
Diarrhea is common during transplant and long-term maintenance therapy.
Other medications and supplements can cause GI issues.
Hydration is very important
Electrolyte replacement is common
Good skin care will help prevent irritation
Stool exam may be needed to rule-out infection
Increase fiber
Stay well hydrated
Fruits, vegetables, high fiber whole grain foods
Fiber binding agents – Metamucil® ,
Citrucel®, Benefiber®
If no infection, anti-diarrheal medication may be prescribed
Discuss GI issues with healthcare providers to identify causes and adjust medications and supplements
Smith LC, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105.
Myeloma: Putting The Pieces of the Puzzle
Relapsing Nature of Myeloma
=
Adapted from Durie B. Keats JJ, et al. Blood. 2012;120(5):1067-1076.
Many Treatment Options at Relapse
Myeloma Therapies
Belantamab mafodotinb
Bispecific Antibodies
Bortezomib (SQ admin)
Common Combinations
Bela, BVd, BPd, BKRd
Elrexfio®, Lynozyfic™, Talvey® , Tecvayli®
VRd, Vd, VCd
Carfilzomib KRd, Kd, Dara-Kd, Isa-Kd
Car T-cell therapies
Daratumumab
Elotuzumab
Cilta-Cel® or Ide-Cel®
Dara-Rd, Dara-Vd, Dara-Pd, Dara-VMp, Dara-Kd
ERd, EPda
Isatuximab Isa-Pda, Isa-Kd
Ixazomib IRd
Lenalidomide
VRd, Rd, KRd, Dara-Rd, ERd, IRd
Pomalidomidea Pda, Dara-Pd, EPda, PCdb
Selinexor
Xd, XVd, XKdb, Dara-Xdb
New agents or regimens in clinical trials are always an option
a2 or more prior therapies. bOff-label; not currently FDA-approved.
Many treatment options are available.
More therapies are being studied
Clinical trials may be an option
C = cyclophosphamide; d = dexamethasone; Dara = daratumumab; FDA = US Food and Drug Administration; E = elotuzumab; Isa = isatuximab; I = ixazomib; K = carfilzomib; M = melphalan; p = prednisone; P = pomalidomide; R = lenalidomide; SQ = subcutaneous; V = bortezomib; X = selinexor.
Rajkumar SV. 2024 Myeloma Algorithm. https://clinicaloptions.com/CE-CME/oncology/2024-mm-algorithm/18440-26989. Accessed 12.14.24. NCCN Guidelines®. Multiple Myeloma. V3.2024. Accessed March 15, 2024. Noonan K, et al. J Adv Pract Oncol. 2022;13(suppl 4):15-21. Steinbach M, et al. J Adv Pract Oncol. 2022;13(suppl 4):23-30. Moreau P, et al. Lancet Oncol. 2021;22(3):e105-e118. O’Donnell EK, et al. Br J Haematol. 2018;182(2):222-230. Mo CC, et al. EJHaem. 2023;4(3):792-810. Chang D. et al., Blood 2024, Abstract 2287.
CAR T Cell Therapy
BCMA target
• Abecma (Ide-Cel)
• Carvykti (Cilta-Cel)
1
Relapsed MM with 1-2 prior LOT Bridging therapy, if needed; Lymphodepleting therapy when CAR T cells are ready T Cell Infusion Close monitoring and Management of side effects
T-Cell Engager (TCE) Therapies
Relapsed MM after 4 prior LOT (or clinical trials)
TCE are innovative immunotherapies used in the treatment of relapsed multiple myeloma. These therapies work by redirecting the patient's own T-cells to recognize and attack myeloma cells.
3
2 a 2 b 4 5 HOME ! Apheresis to Collect T Cells T Cell Manufacturi ng
Bispecific antibodies
• About 7 in 10 patients respond
• Off-the-shelf treatment; no waiting for engineering cells
BCMA target: greater potential for infection
• Tecvayli® (teclistamab)
• Elrexfio ® (elranatamab)
Cytotoxic cytokines
Bispecific antibody T cell MM cell
• Lynozyfic™ (linvoseltamab)
GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
CAR T= Chimeric Antigen Receptor T Cell; LOT = Lines of
• Talvey ® (talquetamab)
BISPECIFIC ANTIBODIES
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; GPRC5D = G protein–coupled receptor, class C, group 5, member D; MM = multiple myeloma; scFV = single chain fragment variable.
Hucks G, Rheingold SR. Blood Cancer J. 2019;doi:10.1038/s41408-018-0164-6.
Shah N, et al. Leukemia. 2020;34(4):985-1005. Yu B, et al. J Hematol Oncol. 2020;13:125.
CAR T and Bispecific Antibodies: Known Side Effects
CYTOKINE RELEASE
SYNDROME
• Fever
• Fatigue & Weakness
• Headache
• Nausea/Vomiting/Diarrhea
• Chills
• Low blood pressure
• Rapid heart rate
CRS is a common but often mild & managea ble side effect
Neurotoxicity is a rare but a serious side effect
• Difficulty breathing PREVENTION AND MANAGEMENT
• Disease management to reduce tumor burden
• Bispecific Step-Up Dosing (SUD)
• Tocilizumab
• Steroids
• Anti-Seizure medications
• Intravenous Immunoglobulin (IVIG)
• Close monitoring
ICANS AND NEUROTOXICITY
• Headache
• Difficulty concentrating
• Lethargy
• Agitation
• Hallucinations
• Tremors
• Aphasia (difficulty with speech, reading, writing, or understanding language)
• Confusion
• Memory loss
• Personality change
• Delayed Neurotoxicity can include Parkinsonism, Cranial Nerve Palsies and Peripheral Neuropathy/Guillan Barré syndrome (GBS)
CAR = chimeric antigen receptor. ICANS = Immune Effector Cell-Associated Neurotoxicity Syndrome Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638. Kumar, et al. Blood (2024) 144 (Supplement 1): 4758.
Infection: Medications Can Mitigate Risk
Type of Infection Risk
Medication Recommendation(s) for Healthcare Team Consideration
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL and maintain treatment dose intensity
Weight, GI Symptoms & The Drugs That Affect Them: Prevention
& Management
Anorexia (difficulty eating) Weight loss
• ASCT
• GPRC5D therapy
Steroids Weight gain, fluid retention
Excess hunger ASCT
GPRC5Ddirected therapy Opioids
Weight Loss
Weight Gain
Weight Management
• Monitor weight for significant loss or gain
• Adjust diet (reduce calories or add supplements )
• Work with a dietician
Smith LC, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105.
Management of Oral Side Effects
Xerostom
ia
OTC dry mouth rinse, gel, spray are recommended. Avoid hot beverages. Anti-fungal therapy for oral thrush.
Dysgeusi a
Dysphagi a
=Dry Mouth =Difficulty Swallowing =Taste Change
Dexamethasone oral solutions “swish and spit” may provide benefit. Sour citrus or candies before meals are also recommended.
Dental
Care
Attention to oral hygiene.
Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms
Weight Monitorin g
Some medications lead to weight gain, others to weight loss. Meet with a Nutritionist
Consider diet changes, supplements
Work closely with your entire health care team to manage oral side effects.
Skin and Nail Side Effects
Possible side effect to some treatments and supportive care medications
Skin Rash:
Prevent dry skin; apply lotion
Report changes to your care team
Medication interruption or alternative, as needed
Steroids:
• Topical for grades 1-2,
• Systemic and topical for Grade 3
Antihistamines, as needed
Nail Changes:
Keep your nails short and clean.
Watch for “catching and tearing”
Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
A nail hardener may help with thinning
Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Myeloma: Putting The Pieces of the Puzzle
Fatigue, Anxiety and Depression
Fatigue Depression Anxiety
Fatigue is the most reported symptom. Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression. Symptoms can improve with continued physical activity.
Symptoms are under-reported:
“I mentioned it before. Nothing can be done.” “I don’t want to be put on another medication.”
>35% of patients ≈25% of patients
More Pieces to the Big Picture
Adopt Healthy Behaviors
• Mental health / social engagement
• Stress reduction; relaxation
• Sufficient Sleep
• Maintain a healthy weight; eat nutritiously
• Activity / exercise / prevent falls, injury
• Stop smoking Sexual health / intimacy
• Have a PCP for general check ups, preventative care, health screenings, vaccinations
Complementary or alternative therapy
• Have specialists for dental care, eye exams/screening, skin cancer screening
Recommended Health Screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Colonoscopy
• Dental checkups & cleaning
• Dermatologic evaluation
• Diabetes
• Hepatitis
• Hearing
• Vision
• Women specific: mammography, pap smear
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56.
• Men specific: prostate
Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.
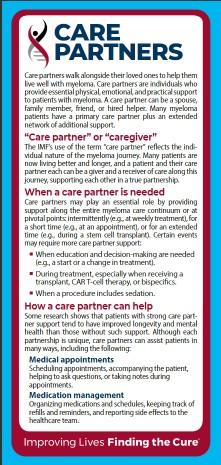
Care Partners: Essential Pieces of the Puzzle
Multiple studies demonstrate that strong social ties are associated with
• Increased longevity including people with cancer
• Improved adherence to medical treatment leading to improved health outcomes
• Lower risk of cardiovascular diseases
• Increased sense of purpose & life satisfaction
• Improved mood and happiness
• Reduced stress and anxiety
• Enhanced resilience
Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)
Caring for the Care Partner
• Recognize that caregiving is difficult/stressful
• Encourage care partners to maintain their health, interests, and friendships
• The IMF has information and resources to help care partners
“Thank You!”
From the NLB and the IMF
Closing the Gap: Health Disparities in Myeloma
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO, Chief Medical Officer, International Myeloma Foundation
Patient and Family Seminars
HEALTH DISPARITIES IN MYELOMA
Joseph Mikhael MD, MEd, FRCPC
Chief Medical Officer, International Myeloma Foundation
Professor, Translational Genomics Research Institute, City of Hope Cancer Center
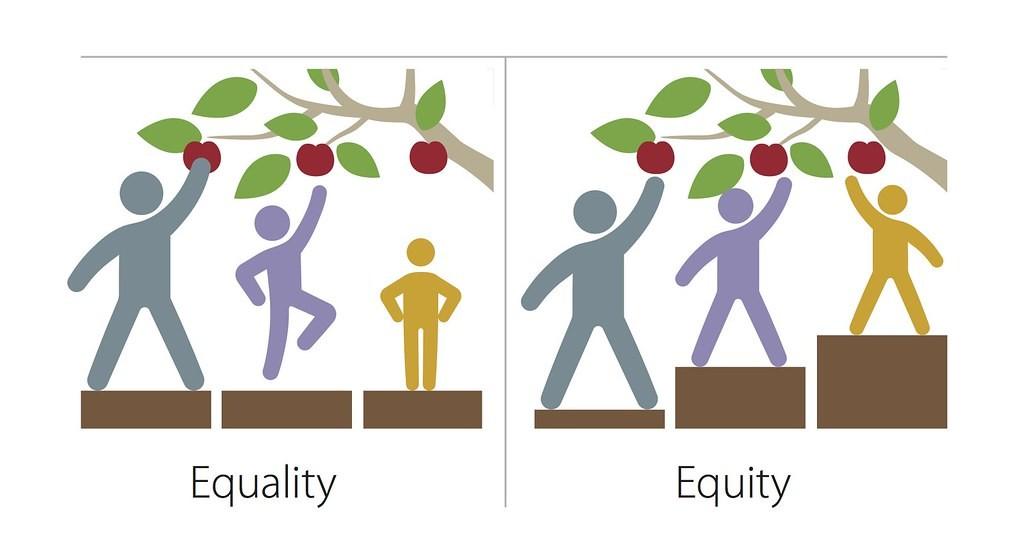
What are Health Disparities?
•Health disparities are preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations
- Centers for Disease Control (CDC)
•Health equity generally refers to individuals achieving their highest level of health through the elimination of disparities in health and health care
This Photo by Unknown Author is licensed under CC BY-NC
What
A Call to Action Facts About Disparities in Myeloma
M-Power = Myeloma Power
The core vision of this initiative is to improve the short- and long-term outcomes for African American patients with myeloma.
We want to empower patients and communities to change the course of myeloma…
Enhance access to optimal care by educating myeloma providers about the disparity and how to reduce it
Engage the community to increase awareness and provide support
Shorten the time to diagnosis by educating primary care providers to recognize the disease and order the right tests
M-Power Is Both a National and Local Movement
2024 M-Power Community Workshops
April 2024
Multiple cities in Indiana
Annual Indiana Black Barbershop Health Initiative
• Health screenings for Black men on the 1st and 2nd Saturdays in April
• Shared materials on myeloma and M-Power for distribution in 18 barbershops in Evansville, Elkhart, and South Bend
June 20, 2024
New York, New York
50+ attended
76% African American
• 86% planned to share something they learned with their family, friend or healthcare provider
• 100% of attendees rated the program as excellent to very good
September 5, 2024
Charlotte, North Carolina
October 10, 2024
Richmond, Virginia
Primary Care Physician Dinner Meeting
• Presenting on multiple myeloma to the diverse community of healthcare professionals during the quarterly meeting of the Charlotte Medical Dental Pharmaceutical Society
40+ Attended
81% African American
• 88% plan to share something they learned with their family, friend, or healthcare provider
• 100% of attendees rated the program as excellent to very good
Juneteenth 2024: Abyssinian Church, Harlem, NYC
June21st , 2025
CelebratingJuneteenthinBrooklyn,NewYork!
M-Power Community Workshop: Richmond, VA
Facebook Live
Education of Primary Care Providers
Our goal is to reduce DELAYS in diagnosis among African Americans by educating the primary care community with a focus on:
• Recognizing the signs and symptoms of myeloma
• Discriminating myeloma from other diagnoses such as diabetes
• Capturing an accurate diagnosis through proper use of testing
• Providing referral guidelines for Hematology and Oncology
• Grand Rounds
8,000
• Postcards mailed to 6,000+ PCPs in target cities
• Free PCP CME course “Don’t Miss Myeloma”
• Cobb Institute talk
• Talk at NMA Annual Meeting Dinner Meetings Articles and pending publications
Learners
Annual Meeting of the National Medical Association
• 12 1st – 3rd year medical students from all over the country met on August 5th in NYC at the NMA Annual Convention and Scientific Assembly
• Presented their posters, they worked on with a multiple myeloma experts immediately following the Jane Cooke Wright Symposium; which was dedicated to Dr. Edith Mitchell
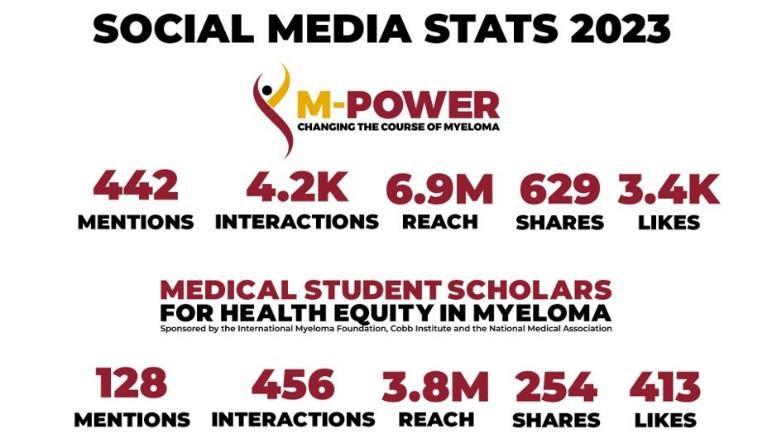
Over 400,000 visits to M-Power site!
M-Power Website
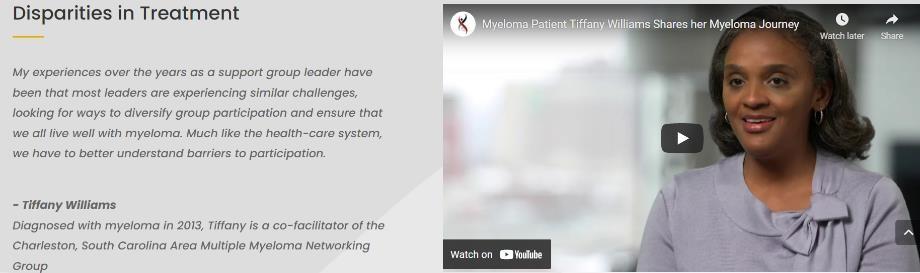
Patient Interview On Local News
M-Power Connections
M-Power Website:
•Web Stats: Over 40k Page views across main, city sites & myeloma.org
•Google PPC targeted web traffic
Email Stats:
•Total Sent: 18 emails
•Total Audience: 38k*
•Open Rate Avg: 31%*
*Note: We have continued to refine lists, contributing to a more engaged audience as evidenced in the Open Rates (The industry standard high-mark is 21%).
M-Minute Promotion Stats:
•Total Sent: 19 emails
•Total Audience: 323k
•Open Rate Avg: 38.91%
M-Power Related Video Stats:
• Total Views: Over 50k
…And Growing!
2025 and Beyond
Engage
• 2025 Juneteenth Workshop, NYC
• M-Power Community Workshop in Miami and Philly
• Expand online and social media strategy
Educate
• Primary care program in Charlotte
• Lab based education
• Electronic Medical Record Initiative
Enhance
• Diversity in Clinical Trial Academy as part of the Diversity in Clinical Trials initiative
• Nurse equity decision tool
What Can I Do??
•Be more conscious of the topics of health equity
•Evaluate the opportunities in your experience to reduce disparities
•Support the M-Power movement!
BREAKOUT SESSION 2
PLEASE HEAD TO YOUR SELECTED BREAKOUT SESSION:
BREAKOUT A: PATIENTS ONLY – LESSONS LEARNED
Please remain in this room
BREAKOUT B: CARE PARTNERS ONLY
Please move to Salon G - J
Breakout Session A: Patients Only –Lessons Learned
Michael Tuohy, 25-year Myeloma Patient, Support Group Leader
Breakout Session B: Care Partners Only
Robin Tuohy, Vice President - Patient Support
International Myeloma Foundation & 25-year care partner
Controversies in Myeloma: Moderated by Dr. Joseph Mikhael
Craig Emmitt Cole, MD
Associate Professor, Karmanos Cancer Institute
Wayne State University/Michigan State University, Detroit/ Lansing, MI
Benjamin Derman, MD University of Chicago, Chicago, IL
Rahma Warsame, MD
Mayo Clinic, Rochester, MN
Ask
– the – Experts w/ Guest Faculty
Closing Remarks & Evaluation
Upcoming IMF Events
October 15, 2025: Living Well With Myeloma – Webinar: Infection Prevention & Management
November 17, 2025: Myeloma Community Workshop What’s the ‘Right’ Answer? – Controversies in Myeloma
March 13-14, 2026: Patient and Family Seminars Boca Raton PFS – Marriott Boca Raton at Boca Center
IMF Program Evaluations
Please return your program evaluations on your way out – whether you stay for the full program, or only one session, your feedback is invaluable to our team. Thank you for taking the time completing this.
Thank you to our sponsors!
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.