
Photobiomodulation,Phototherapy,andLaserSurgery
VolumeXX,NumberXX,2018
ª MaryAnnLiebert,Inc.
Pp.1–7
DOI:10.1089/photob.2018.4544
ComplexRegionalPainSyndrome(SudeckAtrophy)
PreventionPossibilityandAcceleratedRecoveryinPatients withDistalRadiusattheTypicalSiteFractureUsing
Polarized,PolychromaticLightTherapy
MirjanaI.Zlatkovic-Svenda,MD,PhD,1,2 ClaudiaLeitner,PhD,3
BiljanaLazovic,MD,PhD,4 andDejanaM.Petrovic,MD5
Abstract
Objective: Distalradiusfracture(DRF)isoneofthemostfrequentpopulationfracturemostlyaffectingwomen, andfrequentlyleadingtocomplexregionalpainsyndrome(CRPS).ManagementofDRFandCRPSingerontologyiscomplex.Theaimwastoevaluatetheuseofpolarized,polychromatic,low-energylighttherapy combinedwithconventionaltreatmentafterDRFingerontologyandtofollowuppatientsforCRPSemergence.
Materialsandmethods: Afterplasterremoval,femalepatients(n = 52)weredividedintotwogroups.Group1 (n = 26)wastreatedwithexercisesandcryotherapyonthewristanddorsalhand(control).Group2(n = 26)was additionallytreatedwithlighttherapy(Bioptron).
Results: Whilepaindecreasedandsupinationandpronationimprovedinallpatientsafter15daysoftherapy, painreductionwasacceleratedandsupinationenhancedinthelighttherapy-treatedgroup( p < 0.05).Noneof thepatientsinthelighttherapy-treatedgroupdevelopedCRPSduringthe6-monthfollow-up,comparedwith fourpatients(15.4%)inthecontrolgroup( p < 0.05).Completehandfist-formingcapacitywasachievedin19 patients(73.1%)inthelighttherapy-treatedgroupcomparedwith16patients(61.5%)inthecontrolgroup ( p > 0.05).
Conclusions: BioptronlighttherapycombinedwithconventionaltherapyimprovespatientoutcomeafterDRF ingerontology,comparedwithconventionaltreatmentalone.
Keywords: complexregionalpainsyndrome,Sudeck,fracturaradiilocotypico,radialfracture,prevention, Bioptron,laserotherapy,kriotherapy,lighttherapy,gerontology
Introduction
Distalradiusat thetypicalsitefracture(fracturaradii locotypico)—distalradiusfracture(DRF),largely knownasabrokenwrist(afractureoftheradiusverycloseto thewrist)—isoneofthemostfrequentpopulationfractures, accountingfor10–18%ofallfracturesinadults.1 Overthe past40years,DRFhasshownaconstantprogressionin prevalence,whichcouldpartiallybeexplainedbyanextensionoftheaveragelifespaninhumanity.1
Becauseoftheunbalancedboneturnoverthatcauses osteoporosisinclimactericandpostmenopausalwomen,
evenaminortrauma(accidentalslipandfallathomeoron thestreet)cancauseDRF.Around79%ofcasesarewomen, andincidencesincreasewithagefollowingtheonsetof menopause,withthepeakinthe60-to65-yearperiod.2 AccordingtoOmslandetal.3 womenfromtheurbanarea havea30%higherriskofdevelopingDRFthanthosefrom ruralareas,whichmightbeconnectedwithinsufficientsun exposureandlackofvitaminDproduction,whichiscrucial forthemaintenanceofproperbonedensity.
ConventionalDRFtreatmentcomprises3–4weeksofimmobilizationfollowedbyphysiotherapyafterremovingthe plaster.Theaimofphysiotherapyistoreachadequaterange
1InternalMedicineSpecialist-Rheumatologist,InstituteofRheumatology,UniversityofBelgradeSchoolofMedicine,Belgrade,Serbia. 2UniversityofEastSarajevoMedicalFaculty,RepublikaSrpska,Lukavica,BosniaandHerzegovina. 3BioptronAG,Wollerau,Switzerland.
4InternalMedicineSpecialist,UniversityClinicalHospitalCenterZemun,UniversityofBelgradeSchoolofMedicine,Belgrade,Serbia.
5PhysicalMedicineandRehabilitationSpecialist,TheBelgradeCityInstituteofGerontology,Belgrade,Serbia.
ofwristjointmovementandtoempowerpatientsfortheir everydaylives.Diadynamiccurrentorelectromagneticfield therapyismostlyusedforthatpurpose,addedwithcryotherapyandexercise.Cryotherapyandexercisesareroutinely usedafterDRF,incombinationwithdiadynamiccurrents,but thelatteroneismostlycontraindicatedintheelderly.Dueto poorskinqualityandskinatrophyinoldpeopleaccompanied withsensitivitydamage,aswellasduetoanumberofcomorbiditiesduetoaging,theapplicationofphysicalagents (diadynamiccurrentsspecifically)islimitedinmostcases. Thishighlightstheneedforadequatetreatmentoptionsforthe elderly.
Complexregionalpainsyndrome(CRPS)isoneofthe mostcommonDRFcomplications,mostlyoccurringwithin thefirst4monthsafterthefracture.Itsprevalenceisestimatedat39%4 andoccursin4–7%ofpatientsafterthe fracturesurgeryoftheextremity.5
CRPSisoneofthemostambiguousandobscuredchronic painconditionsaffectingthelimb,named,accordingtointernationallyagreedtaxonomy,astheCRPSsince1994.6 CRPSdiagnosisisusuallymadebasedonsymptomsand clinicalfindings.ThemainCRPSsignsaretheautonomic nervoussystemdysfunctionandtropicalchangesoftheskin. Initiallychangesinvasomotoractivityandsensationare presentedintheaffectedextremity,suchasalteredsensitivitytotouch(i.e.,allodyniaandhyperalgesiatomechanicalorthermalstimuli).Therefore,itisalsoknownas causalgia,theshoulder-handsyndrome,algodystrophy,algoneurodystrophy, Sudeckatrophy, reflexsympatheticdystrophy, reflexneurovasculardystrophy, post-traumatic dystrophy,andfracturedisease.7
Therearethreetypicalstagesinthediseasecourseof CRPS:stageI:sympatheticdysfunctionwithdermatomal distributionofthepain;stageII:progressiontodystrophy shownasedema,hyperhidrosis,neurovascularinstability, hairloss,ridging,dystrophic,brittleanddiscolorednails, skinrash,subcutaneousbleeding,neurodermatitisorulcerativelesions,changesintemperatureorcoloringoftheskin; stageIII:transitionfromsympatheticpaintosympatheticallyindependentpainpresentingwithdifferentdegreesof atrophy,frequentlyovershadowedbysubcutaneousedema,5 andirreversiblecontracturesandlossoflimbfunctionatthe finalstage,evidentthroughreducedstrength,decreased rangeofmotion,tremor,anddystonia.
StagesIandIImaybespreadtootherextremitiesin approximatelyone-thirdoftheCRPSpatients,andmayalso becomegeneralized,whichisaninfrequentcomplication duringthelatestage,8 leadingtoalteredbodyperceptionand proprioception.9,10
AllthreeCRPSstagesarecharacterizedbyveryintensive,sometimesunbearablepain,whichsignificantlyinfluencesthepatient’severydaylife.CRPSisthemostcommon complicationafterdistalupperextremityfracture,causedby DRF,resultinginadelayinreturningtowork,diminished health-relatedqualityoflife,andincreasedlikelihoodof pooroutcomeand/orlitigation.11 CRPSisoneofthemostdisablingconditionsinagedwomen,presentingarealtherapeutic challengehighlightingtheneedforitsadequateprevention. Accordingtorandomizedcontrolledtrials,physio-and occupationaltherapyareeffectiveforCRPStreatment.The majorityofpatientsarecuredwithinthefirstyear,whereas forafewindividualsthediseaseprogressestoachronic
stage,characterizedby‘‘warmCRPS’’to‘‘coldCRPS’’ transition12 involvingautonomousdysfunction.InstageIII, bisphosphonates,calcitonin,intravenousadministrationof ketamine,bindersoffreeradicals,oralcorticosteroids,and spinalcordstimulationarebeingused,5 althoughwithout majorsuccess.
Low-levellasertherapy(LLLT)hasalsoshowngood improvementofthechronicpainsymptoms13 onceCRPS hasbeendeveloped.Somestudiessuggestthatlight,whetherintheformofLLLTradiationorfromothercoldlight sources,benefitsavarietyofpainfulmusculoskeletaland neurologicalconditions.14,15
Lighttherapy(BioptronAG)hasbeenshowntoprovide analgesiceffects,improvedmicrocirculation,andvasomotor function16–18 foravarietyofillnessesanddiseasesdueto itsbiostimulatoryeffects.19,20 Thepropertiesofthislight therapydeviceincludespolarized,polychromatic,incoherent, andlow-energylight,whichsetsthisdeviceapartfromother lighttherapydevicesinthemarket.Thedifferentwavelengths (480–3400nm)ofBioptronlighttherapydevicespenetratethe skinatdifferentdepths,triggeringandenhancingavarietyof cellularprocesseswithbeneficialphysiologicaleffects21,22 (includingresolutionofinflammationandactivationof theimmunesystem,23–26 mitochondriaactivation,27 reductionofpainintensity, 28–30 tissuerepair, 31 vasodilatation, andincreasedlocalandsystemiccirculation).18,32
WeselectedBioptronlighttherapy,becauseithasarelativelylargetreatmentareacomparedwithLLLTandbecauseitcanbeusedbynonmedicalstaffatthepatients’ home.Incontrast,LLLTshouldbeusedbymedicalstaff onanalreadymanifestedsyndrome,directlyonhandpain pointsandstrictlydosed.
Therefore,theaimofthisstudywastoevaluatelight therapy(polarized,polychromatic,noncoherent,low-energy radiation)applicationcombinedwithcryotherapyandoptimalexercisesinpatientsafterDRFandtoinvestigate whethertheriskofCRPScouldbeminimized.
MaterialsandMethods
Patients
FromJanuary2014toDecember2017,theprospective studyconsequentlyincludedpatientswithDRFfromthe BelgradeCityInstituteofGerontologytobetreatedwith physiotherapy.Atotalof55femalepatientswithDRFatthe typicalsitewerescreenedforthestudy.Treatmentstarted immediatelyafterremovaloftheplaster.Twopatientswere notincluded,becausetheyhadalreadydevelopedCRPS undertheplaster,andweretreatedaccordingly.Follow-up ofanotherpatientcouldnotbecollectedbecausethepatient diedfromcomplicationsassociatedwithheartfailure,resultinginafulldatasetof52femalepatientswhowere includedinthestudy.
Twoage-matchedgroupswererandomlyassignedatthe beginning:group1(meanage64.0 – 6.9years)consistedof femalepatients(n = 26)withDRFwhoweretreatedwith nonsteroidanti-inflammatorydrugs,exercises,andcryotherapyonthewristanddorsalsideofthehand(control). Group2(meanage62.0 – 7.2years)consistedof26female patientswhoweretreatedwiththesameprotocolasgroup1, butreceivedBioptron(polarized,polychromatic,noncoherent,low-energyradiation)lightinaddition(intervention
group).Allpatientsweretreatedattheirownhomeand evaluatedatdays0(D0),7(D7),and15(D15)forpain [VisualAnalogueScale(VAS)],andatD7andD15fora rangeofwristsupinationandpronation,andatD15forhand fist-formingcapacityandfollowedupforCRPS-induced complicationsfor6monthsaftercompletionoftherapy.
Cryotherapy
Icecubes(frozenat -20 C)of *2cm3 wereappliedtwo timesaday(12hapart)for5minatthewristanddorsal regionofthehandwithcircularmassage.Thehandwas driedafterwardandwrappedincottonfabricfor20minafter eachicemassage.
Exercise
Kinesiotherapyexerciseswereperformedtoenhancethe rangeofwristmotion,withparticularfocusonsupinationand pronation.Activeexercisewascarriedoutwithphysiotherapistassistancefor30mindaily.Assistedexercisebeganfrom theneutralpositiontoamaximumofsupinationandpronation,limitedbypain.Exerciseforfist-formingcapacitywas performedwithasmallrubberball,squeezed20timesaday bythepatient,limitedbypainaswell.
Bioptronlighttherapy
ABioptronphototherapeuticdevice(BioptronAG,Wollerau,Switzerland)with5cmtreatmentdiameter(Bioptron MedAll;480–3400nm;polarizationlevel95%;powerdensity40mW/cm2;energydensity2.4J/cm2/min)wasusedfor irradiationofthedorsalhandregion,accordingtomanufacturer’srecommendations(Table1).Group2receivedBioptronlighttherapyforatotalof10minperdayonfivepoints ofthedorsalhandregion(2mineach)atadistanceof10cm foraperiodof15days(Fig.1).Bioptronlighttherapy,unlike laserlight,containspolychromaticlightinthevisibleandpart oftheinfraredrange(withoutultravioletradiation).Bioptron lighttherapyhasseveralbenefits,butforthecurrentpurpose, improvedmicrocirculation,vasomotorfunction,andanalgesiceffectsareofclinicalimportance(Fig.2).16–18
Outcomemeasures
PainwasassessedatD0,D7,andD15;supinationand pronationweremeasuredatD7andD15.Painwasassessed
CriteriaSpecification
Wavelength480–3400nm
Degreeofpolarization >95%,590–1550nm
Treatmentdiameter5cm
Ratedpowerofhalogen20W
Powerdensity40mW/cm2
Lightintensity10,000lux
Lightenergyperminute2.4J/cm2
Durationofeachsession10min
Lightenergypersession24J/cm2
Numberofdailysessions15
Cumulativedose360J/cm2
Model:BioptronMedAll,BioptronAG,Wollerau,Switzerland.
Patientset-upbeforeBioptronlighttherapy (simulatedpatient).
usingtheVAS,whichisaunidimensionalmeasureforpain intensity,performedona100-mmline.Patientswereasked todrawaverticalmarkontheline,expressingthelevelof theirpain,onascalefrom0to100.
Rangeofwristmotionwasassessedforpronationand supinationmovementcapacity,expressedindegrees.Ninety degreesforsupinationandpronationareconsideredthefull rangeofmotion.Supinationisdefinedasrotationfromthe neutralpositionofthehandandforearmsothatthepalm facesupwards.Pronationisdefinedasrotationofthehand andforearmfromtheneutralpositionsothatthepalmfaces downwards.Thesemeasurementswerenottakenatbaseline (D0)becauseoftheinabilityofthewristtoperformsuch movementsrightafterremovingtheplaster.
Patientswereevaluatedforthehandfist-formingcapacity atthefollow-up,becauseoftheinabilityofthewristtoform afistwithinthefirstweeksafterinjury.
Allpatientswerefollowedupfor6monthsforCRPS occurrenceandhandfist-formingcapacity.Themaincriteria forCRPSwerechronic,intensivepainofthehand,limited rangeofmovement,withorwithoutdiffuseswellingofthe hand,andchangesinskintemperature.
Ethics
ThestudywasapprovedbytheGerontologyInstitute EthicalCommittee.Allsubjectsgavesignedinformed consenttoparticipate.Patientswereabletodropoutfrom thestudyatanystageandwithoutreason.
Statisticalanalysis
Resultswereanalyzedbydescriptivemethodsofstatistics,aswellaswithnonparametricMann-Whitney U-testfor
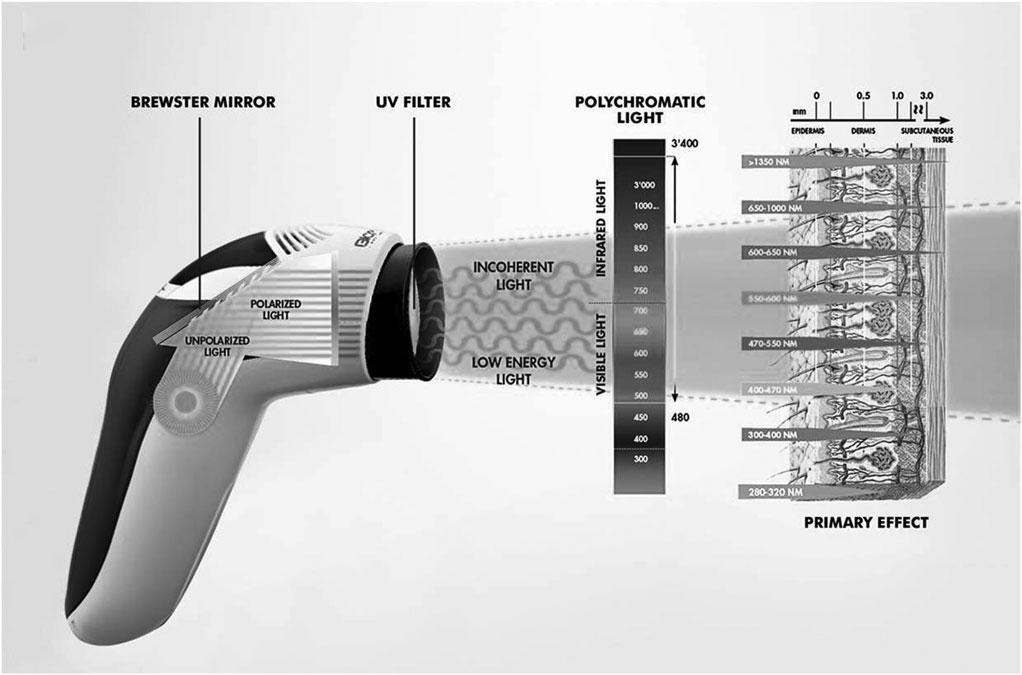
FIG.2. Schematicrepresentationofthelighttherapydevice(BioptronMedAll,BioptronAG,Wollerau,Switzerland). ThedeviceusedaBrewstermirrortocreatepolarizedlightoflow-energylevels.Thepolychromatic,incoherentwavelengths,excludingultravioletradiation,induceprimary,biostimulatoryeffectsontheskin.
independentsamplesandWilcoxonsignedranktestusing SPSS20.
Results
TheaverageVASvaluesandrangeofmotion,measured intheformofsupinationandpronation,aregivenin Table2.Baseline(D0)VASscoresdidnotdifferbetween
groupsbeforetreatment.Allvalues(VASscores,supination,andpronation)improvedduringthecourseoftreatment,independentofthetreatmentgroup,butlighttherapy (group2)acceleratedpainrelief( p < 0.05)andsupination improvement( p < 0.05)atD15,comparedwithcryotherapy andexercisetreatmentalone(group1).Therangeofmotion forsupinationwasalreadysignificantlyimprovedatD7and D15forthelighttherapy-treatedgroupcomparedwiththe
Table 2. VisualAnalogueScaleValues,RangeofMotion(SupinationandPronation) inGroup 1 (CryotherapyandExercises)andGroup 2 (Cryotherapy,Exercises,andLightTherapy) atBaseline,7, and 15 DaysofTherapy
Group1Group2Gr1:Gr2Group1Group2Gr1:Gr2Group1Group2Gr1:Gr2
Day037.7(1.7)33.1(1.6)0.251—————— Day719.2(1.2)16.2(0.9)0.28137.7(5.7)42.3(7.4)0.019*49.7(16.9)52.1(17.9)0.167
Day157.5(9.8)2.1(2.6)0.046*47.3(6.7)56.1(9.3)0.001**60.0(13.1)63.8(14.0)0.284 Day7/day15b 0.000**0.000**0.000**0.000**0.000**0.000**
*p < 0.05,**p < 0.01. aIndependentsamplesMann-Whitney U-test. bRelatedsamplesWilcoxonsignedranktest. VAS,VisualAnalogueScale.
controlgroup(group1; p < 0.05).Althoughpronationimprovedovertime,nodifferencewasfoundforpronation betweentreatmentgroups( p > 0.05).
Atthe6-monthfollow-upperiodaftercompletionof therapy,CRPSoccurrencewassignificantlyreducedinthe lighttherapy-treatedgroupcomparedwiththecontrolgroup ( p < 0.05),0%and15.4%,respectively.Furthermore,atthe follow-up,completehandfist-formingcapacitywasachieved in16controlgrouppatients(group1;61.5%)andin19light therapy-treatedgroup(group2;73.1%),althoughthisdidnot reachstatisticalsignificance( p = 0.375).
Discussion
TheaimofthisstudywastoevaluateBioptronlight therapy(polarized,polychromatic,noncoherent,low-energy radiation)applicationcombinedwithcryotherapyandoptimalexercisesinpatientsafterDRFandtoinvestigatethe preventionofCRPS.Wefoundthatlighttherapysignificantlyacceleratedpainreliefandimprovedsupinationin elderlypatients,comparedwithconventionaltreatment (cryotherapyandoptimalexercises)alone.Inaddition,we foundthattheriskofCRPScouldbeminimizedwithlight therapy,providingevidencethatlighttherapyhassignificant benefitswhenusedincombinationwithalreadyexisting therapyoptionsforelderlypatientswithDRF.
Thecombinationoflighttherapy,cryotherapy,andexerciseshowedgoodpaincontrolandsignificantimprovementofthewristmotionrange.Aftertherapycompletion, noneofthelighttherapy-treatedpatientsdevelopedthe CRPSwithinthe6-monthfollow-upperiod,whereas15.4% ofpatientstreatedwithonlycryotherapyandexercisedid.
Whilethisstudyhasspecificallyselectedthetargetgroup ofelderlywomenwithDRF,thehigherageofparticipants andthespecificminortraumafracturearethecurrentstudy limitations,sothattheresultscannotbedirectlyextrapolatedtoallpatientsandpatientswithmajororaccidental trauma.Becauseofthelimitednumberofsubjectsincluded inthestudy,itisalsonotclearwhetherlighttherapynot onlyreducestheincidencebutalsocompletelyprevents CRPSdevelopmentinelderlypatients.
Accordingtotheliterature,CRPSmostlyoccurswithin thefirst4monthsafterwristfracture,withvariationsin incidencerates.ThomsonMcBrideetal.33 reportedincidencesof20%withinthefirst10weeks;Atkinsetal.34 reported37.2%withinthefirst4months,whereasDemir etal.35 reportedincidencesashighas58%forthefirst3 months.Thishighlightstheeffectivereductionintherisk andpreventionoptionoflighttherapywithpolarized, polychromatic,andlow-energyproperties.
Moreimportantly,intheabsenceofefficientCRPS treatmentfortheelderly,findingpatient-friendlytherapy thataidsitspreventionisextremelyvital.9 CRPStreatment iscomplexandlimited,asthereisnoconsistentinformation aboutefficiencyofpharmaceuticalagents,oreffectiveness ofothermethods.36 Infact,researchsynthesisofrandomizedcontrolledclinicaltrialsfoundnosignificantanalgesic effectforinhibitingsympatheticactivity,includingagents suchasganethidine,regionalsympatheticblockers,calcitonin,codeine,magnesiumchloride,propranolol,lorazepam, intravenousphentolamine,epiduralclonidine,andintravenousregionalblocks.35
Sofar,onlyonepreventionmechanismwasexploredby severalrandomizedcontrolledtrials,whichincludedvitaminCusageafterlimbsurgerywithlimitedsuccess.37 Thus far,laserandothercoldlightsourceshavenotbeenevaluatedinDRFtreatmentandCRPSpreventiontherapy.FurtherstudiesonCRPSlasertherapyandothercoldlight sourcetreatmentwouldbebeneficial,especiallyinthelight ofpossibilitiesforCRPSprevention.Inline,exactprotocols ondosageregimensshouldbeevaluated.
OurresultssuggestthatBioptronlighttherapystrongly reducestheincidencerateofCRPSwithinthe6-month periodaftertherapy,suggestingalong-lastingeffectoflowenergylighttherapy.Polarizedlightpenetratesdeeperinto theskinthanotherlightsources,andthepolychromatic wavelengthpropertiesensureeffectivebiostimulationofa varietyofprocessesfromdifferentwavelengths.38–43
Changesthatoccurandthatmaycontributetothetherapeuticbenefitsobservedinthisstudymayincludechanges inmembranepermeabilityofcells,44,45 stimulationofmitochondriaforincreasedavailabilityofadenosinetriphosphate,27 increasedmicrocirculationthroughthestimulation ofthesynthesisofnitricoxide,18,32 stimulationofimmune parametersandthehumandefensesystem(systemiceffect),22–24 increasedcollagensynthesisfromfibroblasts46–48 throughthestimulationofmacrophage-stimulatinggrowth factors,49 andalterationsinpainperception.28–30 Dueto polychromaticstimulation,andthereforethewide-ranging effects,theapplicationsofthisdevicearenotonlylimitedto woundhealingandpainrelief.
Evidenceforthepracticalandclinicalapplicationof polarized,polychromaticlightanditsbiostimulatoryeffects insportsmedicinehavealsobeeninvestigated.50–54 Furthermore,polarizedlighttherapyhasalsobeenassociated withnormalizationofautonomicimbalance,andashiftin thebalancefromthesympathetictoparasympatheticautonomichomeostasis.55 Inpatientswithchronicglomerulonephritis,asingle10-minapplicationofBioptronlight therapyledtoimprovementsinthecardiacrhythmanda dropinthesystolicanddiastolicarterialpressure.55
Recently,theuseofpolarizedlightinsympathetically mediatedneuropathicpain,56,57 includingCRPS,58 revealed normalizationofsympatheticfunctions,includingdecreased sympathetichyperactivityandtheintegrationofsympathovagalbalance.59 Thisformoftreatmenthasbeenusedasa noninvasiveclinicalapplicationformanagingasympathetic blockadewithoutanyreportedcomplicationsorsideeffects inthepastforotherindications.60 Therefore,itisfeasible thattheobservedanalgesiceffectsandreductionsinthe occurrenceofCRPSinourpresentstudyinpatientsaftera distalradialfractureareassociatedalsowithasympathetic blockadeachievedbypolarizedpolychromaticlighttherapy.
Thelowenergyandincoherentpropertiesofthelight therapydeviceusedinourstudyalsoensuressafetreatment ofpatientswithoutsideeffects.Mostimportantly,thistype oflighttherapydoesnotinterferewithothertreatment choicesandisidealforcombiningtreatmentregimes.
Insummary,low-energy,polarized,andpolychromatic lighttherapycombinedwithconventionaltherapy(cryotherapyandkinesiotherapy)inpatientswithDRFappearsabetter choiceandtreatmentoptionforpaincontrolimprovement andarangeofmotionachievement;italsosignificantly reducesCRPSoccurrenceafterDRFingerontology.
Acknowledgments
Theauthorswouldliketothankthepatientsfortheirtrust inthetherapists,aswellasthemultidisciplinaryteamforthe careoftheirpatients.
AuthorDisclosureStatement
M.I.Z.-S.,D.M.P.,andB.L.declaretheyhavenoconflict ofinterestsandthattheywerenotfundedforthiswork.Dr C.L.,MedicalDirectorofBioptron,wasconsultedafterdata collectionandsupportedthewrite-uponly.
References
1.NellansKW,KowalskiE,ChungKC.Theepidemiologyof distalradiusfractures.HandClin2012;28:113–125.
2.HoveLM,FjeldsgaardK,ReitanR,etal.Fracturesofthe distalradiusinaNorwegiancity.ScandJPlastReconstr SurgHandSurg1995;29:263–267.
3.OmslandTK,AhmedLA,GronskagA,etal.Moreforearm fracturesamongurbanthanruralwomen:theNOREPOS studybasedontheTromsostudyandtheHUNTstudy. JBoneMinRes2011;26:850–856.
4.LiZ,SmithBP,TuohyC,SmithTL,AndrewKomanL. Complexregionalpainsyndromeafterhandsurgery.Hand Clin2010;26:281–289.
5.BruehlS.Complexregionalpainsyndrome.BMJ2015;29: 351.
6.MerskeyH,BogdukN.Classificationsofchronicpain: descriptionofchronicpainsyndromesanddefinitionof painterms.In:ReportbytheInternationalAssociationfor theStudyofPainTaskForceonTaxonomy.HMerskey,N Bogduk(eds.).Seattle:IASPPress,1994.
7.SchottG.Complex.Regional?Pain?Syndrome?Pain2007; 7:145–157.
8.ChelimskyT,LowPA,NaessensJM,WilsonPR,Amadio PC,O’BrienPC.Valueofautonomictestinginreflex sympatheticdystrophy.MayoClinProc1995;70:1029–1040.
9.LewisJS,KerstenP,McPhersonKM,etal.Whereverismy arm?Impairedupperlimbpositionaccuracyincomplex regionalpainsyndrome.Pain2010;149:463–469.
10.CohenH,McCabeC,HarrisN,HallJ,LewisJ,BlakeDR. ClinicalevidenceofparietalcortexdysfunctionandcorrelationwithextentofallodyniainCRPStype1.EurJPain 2013;17:527–538.
11.ForderreutherS,SailerU,StraubeA.Impairedselfperceptionofthehandincomplexregionalpainsyndrome (CRPS).Pain2004;110:756–761.
12.BruehlS,MaihofnerC,Stanton-HicksM,etal.Complex regionalpainsyndrome:evidenceforwarmandcoldsubtypesinalargeprospectiveclinicalsample.Pain2016;157: 1674–1681.
13.TurchinC.Lasertherapy:newtreatmentforCRPS.RSDSA Review:2010;23:4–5.
14.BjordalJM,Couppe ´ C,LjunggrenAE.Low-levellaser therapyfortendinopathy:evidenceofadoseresponsepattern.PhysTherRev2001;6:91–99.
15.KocicM,LazovicM,DimitrijevicI,MancicD,Stankovic A.Evaluationoflowlevellaserandinterferentialcurrentin thetherapyofcomplexregionalpainsyndromebyinfrared thermographiccamera.VojnosanitPregl2010;67:755–760.
16.GulyarSA,StrelchenkoII,JelskiiVN.Influenceofpolychromaticpolarizedlightcombinedwithnear-infraredra-
diationonneurohumoral,immuneandtissuechangesat burninjury.MedInformEng2016;2:15–20.
17.GulyarSA,LimanskyYuP,TamarovaZA,BidkovEG. AnalgesiceffectsofBIOPTRONPILERLight.GenPractJ 1999;4:21–23.
18.SamoilovaKA,ObolenskayaKD,VologdinaAV,Snopov SA,ShevchenkoEV.Singleskinexposuretovisiblepolarizedlightinducesrapidmodificationofentirecirculating blood.1.Improvementofrheologicandimmuneparameters.ProgressinBiomedicalOptics/ProceedingsofLowPowerLightonBiologicalSystems1998;3569:90–103.
19.FenyoM.Theoreticalandexperimentalbasisofbiostimulation.OpticsLaserTechnol1984;16:209–215.
20.SutherlandJC.Biologicaleffectsofpolychromaticlight. PhotochemPhotobiol2002;76:164–170.
21.KubasovaT,FenyoM,SomosyZ,GazsoL,KerteszI. Investigationsonbiologicaleffectofpolarizedlight.PhotochemPhotobiol1988;48:505–509.
22.ZhevagoNA,SamoilovaKA,ObolenskayaKD.Theregulatoryeffectofpolychromatic(visibleandinfrared)light onhumanhumoralimmunity.PhotochemPhotobiolSci 2004;3:102–108.
23.ZhevagoN,SamoilovaKA.Modulationofproliferationof peripheralbloodlymphocytesafterirradiationofvolunteers withpolychromaticvisibleandinfraredlight.Cytology 2004;46:567–577.
24.ZhevagoNA,ZiminAA,GlazanovaTV,etal.Polychromaticlight(480–3400nm)similartotheterrestrialsolar spectrumwithoutitsUVcomponentinpost-surgicalimmunerehabilitationofbreastcancerpatients.JPhotochem PhotobiolB2017;166:44–51.
25.FenyoM,MandlJ,FalusA.Oppositeeffectoflinearly polarizedlightonbiosynthesisofinterleukin-6inahuman Blymphoidcelllineandperipheralhumanmonocytes.Cell BiolInt2002;26:265–269.
26.FulgaC.Antiinflammatoryeffectoflasertherapyin rheumatoidarthritis.RomJInternMed1998;36:273–279.
27.KaruTI,PyatibratLV,AfanasyevaNI.Anovelmitochondrialsignalingpathwayactivatedbyvisible-to-near infraredradiation.PhotochemPhotobiol2004;80:366–372.
28.GulyarSA,TamarovaZA.Physiologicalmechanismsof polarizedlightinfluenceonpain.MedInformEng2016;1: 41–46.
29.GulyarSA,TamarovaZA.AnalgesiceffectsofthepolarizedRed+InfraredLEDLight.JUS-ChinaMedSci2017; 14:47–57.
30.LimanskyY,TamarovaZA,GulyarSA.Suppressionof painbyexposureofacupuncturepointstopolarizedlight. PainResManag2006;11:49–57.
31.BogachevaON,SamoilovaKA,ZhevagoNA,etal.Enhancementoffibroblastgrowthpromotingactivityofhumanbloodafteritsirradiationinvivo(transcutaneously) andinvitrowithvisibleandinfraredpolarizedlight.Tsitologiia2004;46:159–171.
32.SamoilovaKA,BogachevaON,ObolenskayaKD,Blinova MI,KalmykovaNV,KuzminikhEV.Enhancementofthe bloodgrowthpromotingactivityafterexposureofvolunteerstovisibleandinfraredpolarizedlight.I.Stimulation ofhumankeratinocyteproliferationinvitro.Photochem PhotobiolSci2004;3:96–101.
33.ThomsonMcBrideAR,BarnettAJ,LivingstoneJA,Atkins RM.Complexregionalpainsyndrome(type1):acomparisonof2diagnosticcriteriamethods.ClinJPain2008; 24:637–640.
34.AtkinsRM,DuckworthT,KanisJA.FeaturesofalgodystrophyafterColles’fracture.JBoneJointSurgBr1990; 72:105–110.
35.DemirSE,OzarasN,KaramehmetogluSS,KaracanI, AytekinE.Riskfactorsforcomplexregionalpainsyndromeinpatientswithtraumaticextremityinjury.Ulusal TravmaVeAcilCerrahiDerg2010;16:144–148.
36.PerezRS,KwakkelG,ZuurmondWW,deLangeJJ. Treatmentofreflexsympatheticdystrophy(CRPStype1): aresearchsynthesisof21randomizedclinicaltrials.JPain SymptomManage2001;21:511–526.
37.EkrolI,DuckworthAD,RalstonSH,etal.Theinfluenceof vitaminContheoutcomeofdistalradialfractures:a double-blind,randomizedcontrolledtrial.JBoneJoint SurgAm2014;96:1451–1459.
38.KaruT.Primaryandsecondarymechanismsofactionof visibletonear-IRradiationoncells.JPhotochemPhotobiol 1999;49:1–17.
39.StochelG,StasickaZ,BrindellM,MacykW,Szacilowski K.BioinorganicPhoto-Chemistry.Chichester:JohnWiley &Sons,2009;p.298.
40.KerteszI,Fenyo M,MesterE,BathoryG.Hypothetical physicalmodelforlaserbiostimulation.OpticsLaser Technol1982;14:31–32.
41.FriedmannH,LubartR.Nonlinearphotobiostimulation:the mechanismofvisibleandinfraredlaser-inducedstimulationandreductionofneuralexcitabilityandgrowth.Laser Ther1993;5:39–41.
42.LubartR,SlnyakovM,FriedmanH,etal.Photobiostimulationbyvisiblelight:involvementofhydrogen peroxide.Photo-chemPhotobiol1999;6:169–174.
43.LubartR,FriedmannH,LavieR.Photobiostimulationas afunctionofdifferentwave-lengths.LaserTher2000;12: 38–41.
44.LiuTCY,DuanR,YinPJ,LiY,LiSL.Membrane mechanismoflow-intensitylaserbiostimulationonacell. Membranemechanismoflowintensitylaserbiostimulation onacell.ProcSPIE2000;4224:186–192.
45.BraddomRL.PhysicalMedicineandRehabilitationEBook.Philadelphia:ElsevierHealthSciences2010;p.1472.
46.GulyarSA.BIOPTRON-lighttherapyandresourcesof itsapplicationinsurgery.PhotobiolPhotomed2012;9: 16–30.
47.IordanouP,BaltopoulosG,GiannakopoulouM,BellouP, KtenasE.Effectofpolarizedlightinthehealingprocessof pressureulcers.IntJNursPract2002;8:49–55.
48.MonstreyS,HoeksemaH,DepuydtK,VanMaeleG,Van LanduytK,BlondeelP.Theeffectofpolarizedlighton woundhealing.EurJPlasticSurg2002;24:377–382.
49.BoltonP,DysonM,YoungS.Theeffectofpolarizedlight onthereleaseofgrowthfactorsfromtheU-937 macrophage-likecellline.LaserTher1992;4:33–37.
50.RaeissadatSA,RayeganiSM,RezaeiS,etal.Theeffectof polarizedpolychromaticnoncoherentlight(BIOPTRON) therapyonpatientswithcarpaltunnelsyndrome.JLasers MedSci2014;5:39–46.
51.SimunovicZ,IvankovichAD,DepoloA.Woundhealingof animalandhumanbodysportandtrafficaccidentinjuries usinglow-levellasertherapytreatment:arandomized clinicalstudyofseventy-fourpatientswithcontrolgroup. JClinLaserMedSurg2000;18:67–73.
52.StasinopoulosD,PapadopoulosC,LamnisosD,StasinopoulosI.TheuseofBIOPTRONlight(polarized,polychromatic,non-coherent)therapyforthetreatmentofacute anklesprains.DisabilRehabil2017;39:450–457.
53.StasinopoulosD,StasinopoulosI,JohnsonMI.Treatment ofcarpaltunnelsyndromewithpolarizedpolychromatic noncoherentlight(BIOPTRONlight):apreliminary,prospective,openclinicaltrial.PhotomedLaserSurg2005;23: 225–228.
54.StasinopoulosD.Theuseofpolarizedpolychromaticnoncoherentlightastherapyforacutetenniselbow/lateralepicondylalgia:apilotstudy.PhotomedLaserSurg2005;23:66–69.
55.GulyarSA,NikulaTD,KirilenkoEE,KirilenkoEK.AnthologyofLightTherapy.MedicalBIOPTRONTechnology.Kyiv:BogomoletzInstituteofPhysiologyatthe NationalAcademyofSciencesofUkraine,Kiev.2009; pp.421–429.
56.WilseyB,TeicheiraD,CanerisOA,FishmanSM.Areview ofsympatheticallymaintainedpainsyndromesinthecancerpainpopulation:thespectrumofambiguousentitiesof RSD,CRPS,SMPandotherpainstatesrelatedtothe sympatheticnervoussystem.PainPract2001;1:307–323.
57.SchlerethT,DrummondPD,BirkleinF.Inflammationin CRPS:roleofthesympatheticsupply.AutonNeurosci 2014;182:102–107.
58.BasfordJ,SandroniP,LowP,HinesSM,GehrkingJA, GehrkingTL.Effectsoflinearlypolarized0.6–1.6 lMirradiationonstellateganglionfunctioninnormalsubjects andpeoplewithcomplexregionalpain(CRPSI).Lasers SurgMed2003;32:417–423.
59.LiaoCD,RauCL,LiouTH,TsauoJY,LinLF.Effectsof linearlypolarizednear-infraredirradiationnearthestellate ganglionregiononpainandheartratevariabilityinpatients withneuropathicpain.PainMed2017;18:488–503.
60.HuangD,GuY-H,LiaoQ,YanXB,ZhuSH,GaoCQ. Effectsoflinear-polarizednear-infraredlightirradiationon chronicpain.SciWorldJ2012;2012:1–4.
Addresscorrespondenceto: ClaudiaLeitner,PhD ZepterInternational BIOPTRONAG Sihleggstrasse23 WollerauCH-8832 Switzerland
E-mail: leitner@bioptron.com
Received:August8,2018
Acceptedafterrevision:October31,2018
Publishedonline:February20,2019.