Photobiomodulation,Photomedicine,andLaserSurgery
Volume37,Number4,2019
ª MaryAnnLiebert,Inc. Pp.227–232
DOI:10.1089/photob.2018.4576

Photobiomodulation,Photomedicine,andLaserSurgery
Volume37,Number4,2019
ª MaryAnnLiebert,Inc. Pp.227–232
DOI:10.1089/photob.2018.4576
MassimoPetruzzi,DDS,PhD,1 GiannaMariaNardi,BSDH,2 FabioCocco,DCS,PhD,3 FedoradellaVella,DDS,1 RobertaGrassi,DDS,3 andFeliceRobertoGrassi,MD,DMD,PhD1
Abstract
Objective: Aimofthisstudywastoassesstheefficacyofpolarizedpolychromaticnoncoherentlight(Bioptron light)inthetreatmentofchronicoralmucosalpain(COMP).
Patientsandmethods: Twenty-twopatientsaffectedbyCOMPweretreatedwithstandardizedpharmacological protocolsinassociationwithBioptronlight(90W;lightwavelength = 480–3400nm;degreeofpolarization = 95%;specificpowerdensity = 40mW/cm2;energydensity = 2.4J/cm).Theoutcomemeasureswereintensityofpain[measuredbyvisualanalogscale(VAS)score]andsignsreduction(measuredbyEisenscore) recordedatbaseline(t0),after4weeks(t1),andafter8weeks(t2).Signsandsymptomsscoreswerecompared withthoseofacohortofcomparablepatientsselectedfrominstitutionalmedicalrecordfiles.
Results: PatientsinpharmacologicaltreatmentassociatedwithBioptronshowedasignificantVASscore decreaseat t1 and t2 (t0 = 6.9, t1 = 3.9, t2 = 1.8, p < 0.05),whereasthepatientsinexclusivepharmacological treatmentshowedasignificantVASscoreimprovementonlyat t2.ComparingtheVASscoreat t1 and t2 inthe twogroups,asignificantimprovementwasrecordedinpatientsundergoingBioptronadjunctivetreatment (t1 = 3.9vs.5.9; p < 0.05and t2 = 1.8vs.3.6; p < 0.05).InbothgroupsEisenscoreimprovedat t1 and t2,butin theBioptron-treatedpatientstheimprovementwasstatisticallybetterat t1 (1.9vs.0.8; p < 0.05)andat t2 (2.7vs. 1.4; p < 0.05).
Conclusions: InCOMPpatients,Bioptronuseassociatedwithpharmacologicaltreatmentallowsabetterand fastersignsandsymptomsreductionwhencomparedwiththeexclusivepharmacologicaltreatment.Further controlledstudiesareneededtoestablishtherelativeandabsoluteeffectivenessofBioptroninCOMPmanagement.
Keywords: Bioptron,oralmucosalpain,photobiomodulation
Introduction
Chronicoralmucosalpain (COMP)isdefinedasa painlasting >3monthsandoutlastingtheinflammatory stimulus.1 Differentpathologieswithdifferentetiologyand pathogenesis,inducedbylocalorsystemicfactors,cancause COMP.AlthoughZakrzewskareportsthatchronicorofacial paininitsbroadestdefinitioncanaffectupto7%ofthe population,therearenoepidemiologicaldataabouttheexact incidenceandprevalenceofCOMP,consideredasubsetof patientssufferingfromchronicorofacialpain.2 Themain causesofthislackofepidemiologicaldataareprobablydue
totheextremevarietyofclinicalconditionsthatcangenerate chronicpainaffectingtheoralmucosaandthelackofa consensusandguidelinesthatdefinethecriteriatodiagnose theCOMP.ThemostcommoncausesofCOMPareburning mouthsyndrome(BMS),oralerosivelichenplanus,recurrent aphthousstomatitis,vesiculobullousdiseasesandchronic ulcerations.3 Thechronicpainisoftencharacterizedbya burning,stinging,orsoresensationthatimpairsthepatients’ qualityoflifeandincreasestheriskofpsychologicalmorbiditiessuchasanxietyanddepression.2–4
Pharmacologicaltreatmentincludessystemicand/ortopicalcorticosteroids,bioadhesiveandmucoprotectiveagents,
1InterdisciplinaryDepartmentofMedicine–SectionofDentistry,DentalSchool,University‘‘AldoMoro’’ofBari,Bari,Italy. 2DepartmentofOralandMaxilloFacialSciences,DentalSchool,University‘‘LaSapienza’’ofRome,Rome,Italy. 3DepartmentofSurgical,MicrosurgicalandMedicalSciences,DentalSchool,UniversityofSassari,Sassari,Italy.
polyvitaminiccomplexes,benzodiazepines,andanesthetic ointments.5,6 However,thechronicuseofdrugsinCOMP patientscancausesideand/orundesiredeffectsorbeineffective;alsoforthesereasons,newtherapeuticstrategies havebeenemployedtolimitpainandtheconsequentpatients’frustration.7,8
Inrecentyears,theuseofphototherapyisincreasingand alsoappliedtothemanagementofCOMP.Infact,alarge numberofauthorsreportabouttheeffectivenessofthe photobiomodulationinducedbylow-levellasertherapy (LLLT),photodynamictherapy,andpolarizedpolychromaticnoncoherentlightinCOMPpatients.9–11
Therationaleistheinteractionbetweenphotonsanda widerangeofmoleculesthankstoscatteringandabsorption processes.Thephotonicenergyinteractswiththemolecules inducingphotochemicalandphotobiologicaleffects,suchas thegenerationofreactiveradicals(reactiveoxygenspecies) andsingletoxygen,destructionofenzymesincellularsignalingpathways,theopeningofionchannels,andthepromotionofspecificgeneexpression.12–14
Theaimofthisstudywastoevaluatetheeffectivenessof photobiomodulationwithpolarizedlightinthecoadjuvant treatmentofCOMP.
Samplesizedefinition
Poweranalysis,usingone-sidedconfidenceinterval,was performedtoidentifyapropersamplesize.
Thestandardizedeffectwassetat0.40,withasample sizeof18subjectsandanupper80%one-sidedconfidence limitof0.3967.15
Patients’data
Twenty-twopatientsaged18yearsorolder,suffering fromCOMPwereenrolled.InCOMPpatientswereincludedthoseaffectedbyatrophic-erosivelichenplanus, mucousmembranepemphigoid,pemphigusvulgaris, chronicoralulcerations,BMS,andoralsystemiclupuserythematosus(SLE).Thediagnosiswasconfirmedbyhistopathologicalexaminationanddirectimmunofluorescencein caseoforallichen,pemphigus,pemphigoid,andoralSLE. Patientswithhistopathologicalevidenceofdysplasia(mild, moderate,andsevere),inchemo-radiotreatmentorassuminganalgesic,anti-inflammatoryorpsychoactivedrugs,or withapreviousmedicalhistoryofmelanoma,actiniccheilitis,actinicreticulosis,andxerodermapigmentosumwere excluded.
ThestudywasconductedaccordingtotheDeclarationof HelsinkiandapprovedbytheInstitution’sEthicalCommittee.Awritteninformedconsentwasobtainedfromevery patientbeforeparticipationinthestudy.
Enrolledpatients’datawerecomparedwiththoseofa cohortofpatientscomparableforgender,age,comorbidities,diagnosisoforaldisease,andtreatmentregimen,selectedfromthemedicalrecordfilesoftheDentalClinicof University‘‘AldoMoro’’ofBari.
Oralmucosalsignsandsymptomsassessment
Twoblindedindependentclinicianscalibratedinpair evaluatedthesignsevolutionoftheorallesions.Presenceof
erosions,ulcerations,andatrophywasrecordedandphotographedforeachpatient.Signsimprovementwasscored accordingtoEisen16:0 = nochangeorworsening;1 = light improvement(20–50%);2 = markedimprovement(50–80%);and3 = healing(80–100%).The10pointsscoreof visualanalogscale(VAS)wasusedforpainrecording. Symptomswererecordedatthebeginningbeforestaring thetreatment(t0),attheendofthefourthweek(t1),andat theendoftheeighthweek(t2),whereasEisenscorewas evaluatedat t1 and t2.
Photobiomodulationtreatmentintervention
ABioptron-2phototherapeuticdevice(BioptronAG, Wollerau,Switzerland)wasusedfortheirradiationofthe oralmucosawiththefollowingoutputcharacteristics:rated powerofhalogen = 90W;lightwavelength = 480–3400nm; degreeofpolarization = 95%;specificpowerdensity = 40mW/cm2;andenergydensity = 2.4J/cm.Thedurationofeachtreatmentsessionwas15min.Bioptronlight waspositioned10cmfromtheoralmucosaandaC-shaped mouthopenerwaspositionedfortheentiredurationofthe session(Fig.1).Twoweeklysessionsfor8weekswere planned.
Patientsaffectedbyatrophic-erosivelichenplanus,mucousmembranepemphigoid,andoralSLEweretreatedwith clobetasolpropionatecream0.05%inOrabase,twiceaday for8weeks.Oralpemphigusvulgarispatientsweretreated withprednisone peros [0.5mg/(kg die)].Prednisonewas taperedaccordingtolesionsremission.Chronicoral
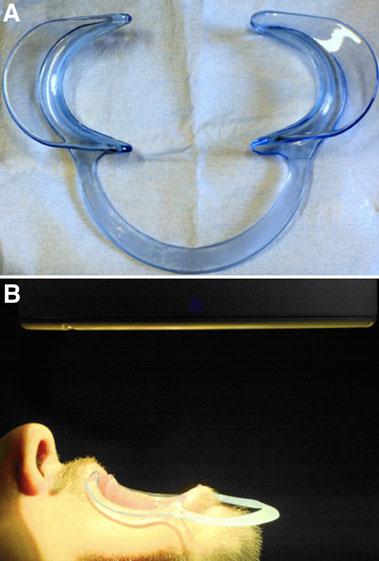
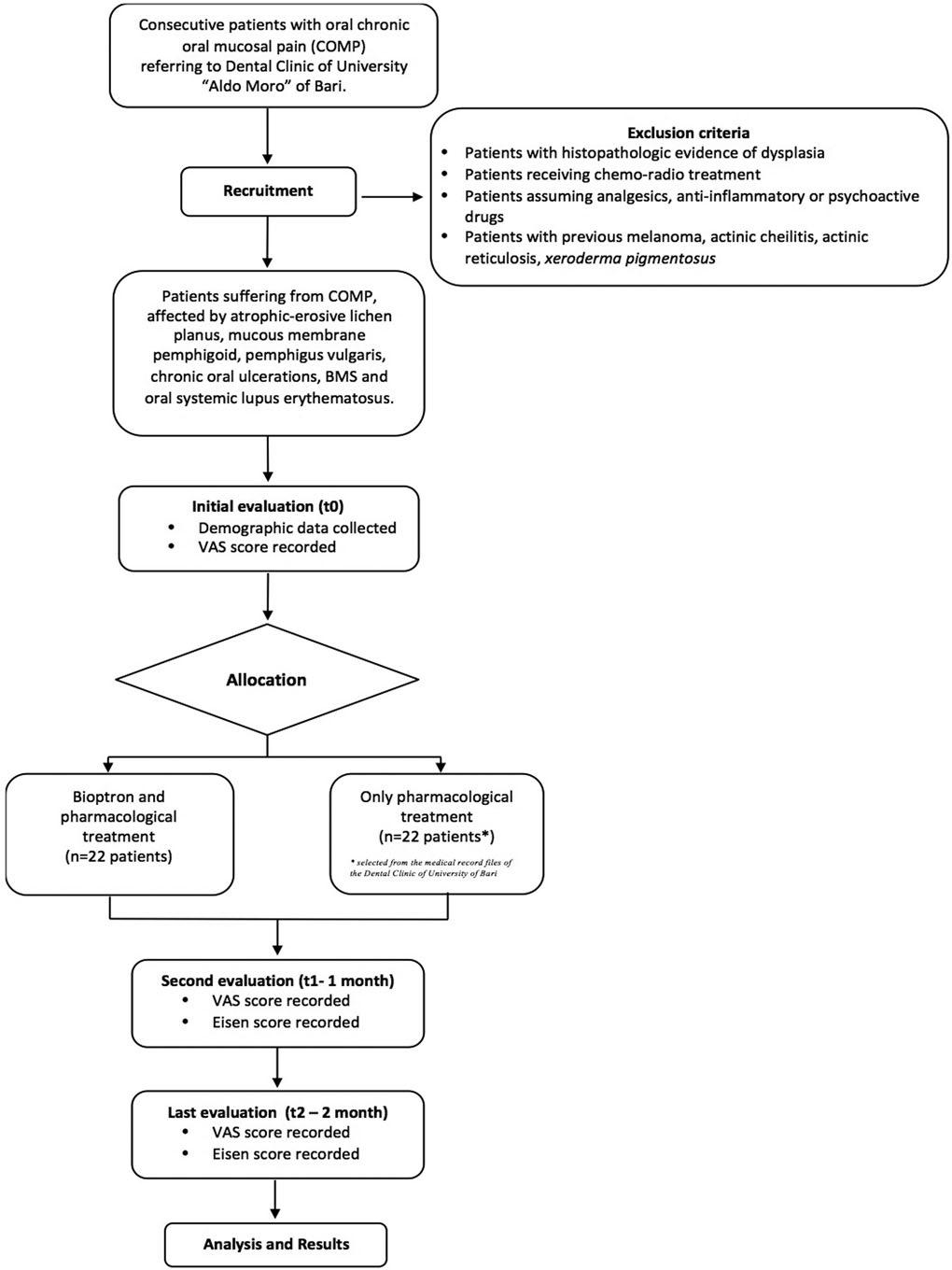
FIG.2. Flowchartresumingpatients’enrollmentcriteria.
Table 1. DemographicCharacteristicsandCauseofChronicOralMucosalPainintheTwoGroups
No.ofpatientsAge(years)Male/female
CauseofCOMP
EnrolledControla EnrolledControla EnrolledControla
Orallichenplanus6666.0 – 4.965.5 – 7.74/24/2
Mucousmembranepemphigoid2256.0 – 2.058.3 – 1.50/20/2
Pemphigusvulgaris1161.060.01/01/0
Chronicoralulcerations4443.7 – 8.342.0 – 11.22/22/2
OralSLE1156.053.00/10/1
Burningmouthsyndrome8860.4 – 8.859.4 – 7.91/71/7
Total222258.2 – 10.357.7 – 11.28/148/14
aSelectedfromthemedicalrecordfilesoftheDentalClinicofUniversityofBari. COMP,chronicoralmucosalpain;SLE,systemiclupuserythematosus.
ulcerationsweretreatedwithachlorhexidine0.12%gel alternatedtoahyaluronicacidgel.Alpha-lipoicacidcapsules400mgtwiceadaywereprescribedtopatientsaffectedbyBMS.
Dataanalysisandstatistics
StatisticalanalyseswereperformedusingaSTATA13 (www.stata.com).
VASandEisenscorevariationsineachgroupbeforeand aftereachtreatmentwerecomparedusingone-wayanalysis ofvariance(ANOVA),whereasintergroupdifferenceswere analyzedusingrepeated0.05.ceANOVA.Differencesbetweenmeanswereconsideredsignificantfor p £ 0.05.The studyprotocolisresumedinFig.2.
Results
Twenty-twopatientsaffectedbyCOMPwereenrolledin thisstudy.Theoralmucosalpainwascausedbyorallichen planus(sixpatients),mucousmembranepemphigoid(two patients),pemphigusvulgaris(onepatient),chronicoralulcerations(fourpatients),oralSLE(onepatient),andBMS (eightpatients).Thepatients’characteristicsatstudyentry(t0) arereportedinTable1.NeitherdemographicnorVASscore differenceswerefoundbetweenthetwogroupsatbaseline. Patientswhoreceivedphotobiomodulationinadditionto pharmacologicaltreatmentshowedasignificantVASscore decreasealreadyafter4weeks(t0 = 6.9to t1 = 3.9; p < 0.05); VAShadafurthersignificantreductionafter8weeks (t1 = 3.9to t2 = 1.8; p < 0.05).Patientswhoreceivedonly pharmacologicaltreatmentshowednosignificantVASscore improvementafter4weeks(t0 = 6.5to t1 = 5.9; p = 0.10), whereasasignificantimprovementwasobservedonlyafter
8weeksofpharmacologicaltreatment(t1 = 5.9to t2 = 3.6; p < 0.05).
Comparingthetwogroups’VASscoreat t0 and t1,a significantimprovementwasrecordedinpatientswhounderwentphotobiomodulationadjunctivetreatment(t1 = 3.9 vs.5.9; p < 0.05and t2 = 1.8vs.3.6; p < 0.05).TheEisen scoreinthephotobiomodulation-treatedgroupstatistically improved(t1 = 1.9to t2 = 2.7; p < 0.05)aswellasinthe controlgroup(t1 = 0.8to t2 = 1.4; p < 0.05).However,the groupofpatientsreceivingadjunctivetreatmentwith Bioptronshowedastatisticallysignificantimprovementof Eisenscoreat t1 (1.9vs.0.8; p < 0.05)andat t2 (2.7vs.1.4; p < 0.05)comparedwiththecontrolgroup.Table2summarizestheaforementioneddata.
Nosideeffectsoradversereactionswererecorded.
Inthisstudy,painseveritybasedonVASscoreaswellas oralsignsevaluatedbyEisenscoreshowedasignificantimprovementin8weeksafterthe beginningofthetreatmentin boththegroups.However,patientsreceivingadditionaltreatmentwithphotobiomodulationshowedafasterandmoreeffectiveimprovementofsymptomsandoralsigns,compared withpatientsundergoingexclusivelypharmacologicaltherapy.
Wealsodescribedforthefirsttime,theopportunitytouse aC-shapedmouthopenertofacilitateirradiationofintraoral mucosalsitesbytheBioptronlight.
Atthebestofourknowledge,nostudiesevaluatedthe effectofBioptronlighttherapyonpatientswithCOMP: onlyapreviousstudy,11 limitedtoasubgroupofpatients sufferingfromgenericoralulcerations,reportedamarked exudationandpainreductionafter1and3months,other
Table 2. SignsandSymptomsintheTwoGroupsofChronicOralMucosalPainPatients
Eisenscore(mean – SD)
VAS,visualanalogscale.
thaninfectionimprovement.Thepositiveeffectsofphotobiomodulationontheoralmucosafrequentlyconcernthe useofthelasertechnology.deCarvalhoetal.17 demonstratedthelaserandlightemittingdiodephotobiomodulationefficacyonananimalmodelinacceleratingthehealing offormocresol-inducedoralulcersinbothclinicaland histologicalaspects.Also,inBMSpatients,thephotobiomodulationinducedbyLLLTsignificantlyreducesthe symptomsandrepresentsanalternativetotheconventional treatmentregimens.18 Onlysixcasesoforalpemphigoid treatedwithlaserphototherapyarereportedinliterature,and alltheauthorsagreetoconsiderlaserphototherapyavaluabletreatment.19 LLLTisalsoemployedinOLP:arecent metanalysisconcludedthatLLLTseemstobeareliable alternativetocorticosteroidsforOLPtreatment,lackingthe adversepharmacologicaleffects.10
However,thephotobiomodulationinducedbyBioptron differsinseveralaspectsfromthatinducedbyLLLT.In particular,thelightusedbytheBioptrontechnologyis polychromaticandnoncoherentalthoughitispolarizedsuch asthelaserlight.Thesecharacteristicsallowtotreatalarger areawithawiderwave-widthspectrum.Further,Bioptron userequiresasimplerandquickerlearningcurve.20
Woundhealingandtissuerepair,painrelief,andreduction oninflammationarethemainclinicaloutcomesobservedin severalstudieswhenphotobiomodulationwasused.21 Thebiologicalmechanismsthatsupporttheclinicaleffectsarerelated totheupregulationofbasicfibroblastgrowthfactor[hepatocyte growthfactor(HGF)andstemcellfactor(SCF)],enhancementofcellularmetabolismandvascularization(vascular endothelialgrowthfactorincreasedproduction),cellular migrationanddifferentiation,andanincreasedsynthesisof variousproteinsinvolvedinoxidativestressreduction,nociceptivepaintransmission,andinfectioncontrol.22–24
Thestudydoeshavelimitations.Wetreatedpatientsaffectedbyheterogeneouspathologies(insomeinstances singlecases,aspemphigusvulgarisororalSLE)characterizedbydifferentetiopathogenesisandkindofpain; consequently,differentphotobiomodulation-relatedactions wereinvolvedinthepainandsignsreduction.Inparticular, inflammationreductionobtainedintheautoimmunediseaseswasprobablyduetoNF-jBexpressionandmodulation,reductionoftheproinflammatorycytokineslevelsin activatedinflammatorycells,andphenotypicalchangesof theactivatedmonocytesormacrophages.25
Thesymptomsimprovementachievedinpatientsaffected byBMSismainlyduetotheeffectsonthepainneuralpathwaysandtransmission.Photobiomodulation,infact,seemsto inducereversiblemorphologicalchangesinneuronalcells. Specifically,itcausesadecreaseofmitochondrialmembrane potentials,withasignificantreductionofadenosinetriphosphate(ATP)level.Thisaffectsthereleaseofglutamateandits excitatoryactivity,attenuatingneuronalhypersensitivity. Thesemorphologicalchangesonlyoccurincellswithdisruptedmicrotubule b-tubulin,indicatorofanalteredneural conduction.Inaddition,photobiomodulationinhibitsthebradykininstimulatoryeffectonAd andCnociceptors.26,27
However,ratherthananalyzingseparatelythephotobiomodulationeffectsoneverysingleoralpathological condition,itwouldbeappropriatetosupposethatallthe differentbiologicalmechanismsactivatedbytheirradiation withBioptronlightactsynergicallyintheclinicalimprovementoftheanalyzedpatients.
Thetremendouspotentialoflow-dosebiophotontherapiessuggestsfurtherusesinoralandfacialpainconditions, suchastemporomandibulardisorders,chronicperiodontitis, andtrigeminalneuralgia.29 Initialpositiveresultsonthe efficacyofphotobiomodulationarealsoreportedinthe treatmentofosteonecrosisofthejawsinducedbybisphosphonates.30
Theuseofphotobiomodulationasadjunctivesupportto thepharmacologicalprotocolsisavalidchoiceinthe managementofsignsandsymptomsincourseofCOMP. Furtherstudiesonlargercohortsofpatientsareneededto confirmthedataobtainedinthispilotstudyandtoexplore thefuturepotentialapplicationsinoralsciences.
AuthorDisclosureStatement Nocompetingfinancialinterestsexist.
References
1.WolfE.Chronicorofacialpain.Understandingpatients fromtwoperspectives:theclinicalviewandthepatient’s experience.SwedDentJ2006;181Suppl:9–69.
2.ZakrzewskaJM.Multi-dimensionalityofchronicpainof theoralcavityandface.JHeadachePain2013;14:37.
3.HegartyAM,ZakrzewskaJM.Differentialdiagnosisfor orofacialpain,includingsinusitis,TMD,trigeminalneuralgia.DentUpdate2011;38:396.
4.RajanB,AhmedJ,ShenoyN,DennyC,OngoleR,Binnal A.Assessmentofqualityoflifeinpatientswithchronic oralmucosaldiseases:aquestionnaire-basedstudy.PermJ 2014;18:e123–e127.
5.StooplerET,SollecitoTP.Oralmucosaldiseases:evaluationandmanagement.MedClinNorthAm2014;98:1323–1352.
6.SheikhS,GuptaD,PallagattiS,SinglaI,GuptaR,GoelV. Roleoftopicaldrugsintreatmentoforalmucosaldiseases. Aliteraturereview.NYStateDentJ2013;79:58–64.
7.PetersS,GoldthorpeJ,McElroyC,etal.Managingchronic orofacialpain:aqualitativestudyofpatients’,doctors’,and dentists’experiences.BrJHealthPsychol2015;20:777–791.
8.AlrashdanMS,AlkhaderM.Psychologicalfactorsinoral mucosalandorofacialpainconditions.EurJDent2017;11: 548–552.
9.KathuriaV,DhillonJK,KalraG.Lowlevellasertherapy:apanaceafororalmaladies.LaserTher2015;24:215–223.
10.HoseinpourJajarmH,AsadiR,BardidehE,ShafaeeH, KhazaeiY,EmadzadehM.Theeffectsofphotodynamic andlow-levellasertherapyfortreatmentoforallichen planus-Asystematicreviewandmeta-analysis.PhotodiagnosisPhotodynTher2018;S23:254–260.
11.AragonaSE,GrassiFR,NardiG,etal.Photobiomodulation withpolarizedlightinthetreatmentofcutaneousand mucosalulcerativelesions.JBiolRegulHomeostAgents 2017;31(2Suppl.2):213–218.
Lighttherapycanhelpchronicoralulcershealingprocess bystimulatingtheepithelialcellsproliferationandmigration,aswellasimprovingbloodflowintotheaffectedsite. Theseprocessesaremediatedbytheincreaseofsome cytokines,especiallyIF-1b,TNFa,andMVP,whichactivateendothelial,fibroblastic,andepithelialgrowthfactors themselves.17,28
12.YunSH,KwokSJJ.Lightindiagnosis,therapyandsurgery.NatBiomedEng2017;1:0008.
13.HuangYY,ChenAC,CarrollJD,HamblinMR.Biphasic doseresponseinlowlevellighttherapy.DoseResponse 2009;7:358–383.
14.HuangYY,SharmaSK,CarrollJ,HamblinMR.Biphasic doseresponseinlowlevellighttherapy-anupdate.Dose Response2011;9:602–618.
15.CocksK,TorgersonDJ.Samplesizecalculationsforpilot randomizedtrials:aconfidenceintervalapproach.JClin Epidemiol2013;66:197–201.
16.EisenD,EllisCN,DuellEA,GriffithsCEM,VoorheesJJ. Effectoftopicalcyclosporinerinseonorallichenplanus. Adouble-blindanalysis.NEnglJMed1990;323:290–294.
17.deCarvalhoFB,AndradeAS,RasquinLC,etal.Effectof laser(k 660nm)andLED(k 630nm)photobiomodulation onformocresol-inducedoralulcers:aclinicalandhistologicalstudyonrodents.LasersMedSci2015;30:389–396.
18.dosSantosLdeF,deAndradeSC,NogueiraGE,LeaoJC, deFreitasPM.Phototherapyonthetreatmentofburning mouthsyndrome:aprospectiveanalysisof20cases.PhotochemPhotobiol2015;91:1231–1236.
19.CafaroA,BroccolettiR,ArduinoPG.Low-levellaser therapyfororalmucousmembranepemphigoid.Lasers MedSci2012;27:1247–1250.
20.HeiskanenV,HamblinMR.Photobiomodulation:lasersvs. lightemittingdiodes?PhotochemPhotobiolSci2018;17: 1003–1017.
21.AranyPR.Craniofacialwoundhealingwithphotobiomodulationtherapy:newinsightsandcurrentchallenges.JDentRes2016;95:977–984.
22.FeehanJ,BurrowsSP,CorneliusL,etal.Therapeuticapplicationsofpolarizedlight:tissuehealingandimmunomodulatoryeffects.Maturitas2018;116:11–17.
23.HamblinMR.Mechanismsandmitochondrialredoxsignalinginphotobiomodulation.PhotochemPhotobiol2018; 94:199–212.
24.IordanouP,LykoudisEG,AthanasiouA,etal.Effectof visibleandinfraredpolarizedlightonthehealingprocess
offull-thicknessskinwounds:anexperimentalstudy. PhotomedLaserSurg2009;27:261–267.
25.HamblinMR.Mechanismsandapplicationsoftheantiinflammatoryeffectsofphotobiomodulation.AIMSBiophys2017;4:337–361.
26.ChowRT,ArmatiPJ.Photobiomodulation:implicationsfor anesthesiaandpainrelief.PhotomedLaserSurg2016;34: 599–609.
27.JanzadehA,NasirinezhadF,MasoumipoorM,JameieSB, HayatP.Photobiomodulationtherapyreducesapoptotic factorsandincreasesglutathionelevelsinaneuropathic painmodel.LasersMedSci2016;31:1863–1869.
28.WagnerVP,CurraM,WebberLP,etal.Photobiomodulationregulatescytokinereleaseandnewblood vesselformationduringoralwoundhealing.LasersMed Sci2016;31:665–671.
29.RahmanSU,MoscaRC,GovindoolReddyS,etal. Learningfromclinicalphenotypes:low-dosebiophotonics therapiesinoraldiseases.OralDis2018;24:261–276.
30.daGuardaMG,Paraguassu ´ GM,CerqueiraNS,CuryPR, FariasJG,RamalhoLM.LaserGaAlAs(k860nm)photobiomodulationforthetreatmentofbisphosphonate-induced osteonecrosisofthejaw.PhotomedLaserSurg2012;30: 293–297.
Addresscorrespondenceto: MassimoPetruzzi,DDS,PhD UniversityofBari‘‘AldoMoro’’ DepartmentofInterdisciplinaryMedicine PoliclinicodiBari–ClinicaOdontoiatrica PiazzaG.Cesare11 Bari70124
Italy
E-mail: massimo.petruzzi@uniba.it
Received:October6,2018. Acceptedafterrevision:December20,2018. Publishedonline:March20,2019.