
Maturitas
journalhomepage: www.elsevier.com/locate/maturitas

Therapeuticapplicationsofpolarizedlight:Tissuehealingand immunomodulatoryeffects
JackFeehana,b,SorayaPatriciaBurrowsa,LeonardoCorneliusa,AlyseMalietzisCooka, KathleenMikkelsenc,VassoApostolopoulos c,⁎,1,MajaHusarica,c,d,⁎,1,DimitriosKiatosa,c,⁎,1
a OsteopathyGroup,CollegeofHealthandBiomedicine,VictoriaUniversity,VIC,Australia
b AustralianInstituteforMusculoskeletalScience(AIMSS),UniversityofMelbourneandWesternHealth,St.Albans,VIC,Australia
c InstituteforHealthandSport,VictoriaUniversity,VIC,Australia
d FirstYearCollege,CollegeofHealthandBiomedicine,VictoriaUniversity,VIC,Australia
ARTICLEINFO
Keywords: Polarizedlighttherapy(PLT) Polarizedlight Photodynamictherapy(PDT) Phototherapies Low-levellasertherapy(LLLT) Woundhealing
ABSTRACT
Asthepopulationgrowsandages,non-pharmaceuticaloptionsforthetreatmentandmanagementofwounds, diseaseandinjuryarerequiredtoensureadequatecare.Polarizedlighttherapy(PLT)utilizesvisible-spectrum polarizedlightforanumberofclinicalapplications.Theadvantageofpolarizedlightisthatitisabletopenetratetheskintoadepthofupto5cm,reachingdeepertissuesinvolvedinwoundhealing.PLThasbeenshown toacceleratethehealingprocessforulcers,surgicalwoundsanddermalburnsaswellasasmallnumberof musculoskeletalinjuries.AsresearchintothehistologicalandphysiologicaleffectsofPLTislargelyabsent, studiesrelatedtootherlighttherapymodalities,largelylow-levellasertherapy,maypavethewaytoidentify putativemechanismsbywhichPLTmightexertitseffects.Changestocellsignallingandsecretionofsubstances requiredforwoundhealinghavebeenidentifiedinresponsetophototherapies.Thereviewedliteraturesuggests thatPLTmaybeefficaciousinsomewoundandinjuryhealingcontexts,thoughagapintheliteratureexists regardingitsmechanismsofaction.FuturestudiesshouldfullyexplainthetherapeuticeffectsofPLTandthe physiologicalmechanismsunderpinningthem.
1.Introduction
Healingisacomplexprocesscomprisingawidevarietyofcelltypes, secretedfactorsandotherphysiologicalparameters.Inanormal, healthypatient,thehumanbodyiscapableofhealingcompletelyfrom awiderangeofwoundsandinjuries.Howeverwhenthesystemis compromizedbyexternalfactorssuchasageing,chronicdiseaseor malnourishment,thehealingresponsecanbedelayed,orincomplete, placingthepatientatrisk[1].Despitethiscommonproblem,thereare alimitednumberofinterventionsavailable,mostofwhicharesupportiveinnature.Thetherapeuticuseoflightcanbetracedbackto ancientEgypt.ThesungodRawasworshippedastheirhighestdeity, andtheEgyptianswouldbaskinthesuntoincreasetheirenergylevels [2].TheancientGreeks,whoweremedicallyadvancedfortheirtime, alsousedsunlighttohelptreatillness[3],andinmoderntimes,seasonalaffectivedisorderistreatedwithbrightartificiallights[4].
AccordingtotheInternationalCommissiononIllumination,lightis “anyradiationcapableofcausingavisualsensationdirectly” [5].Its
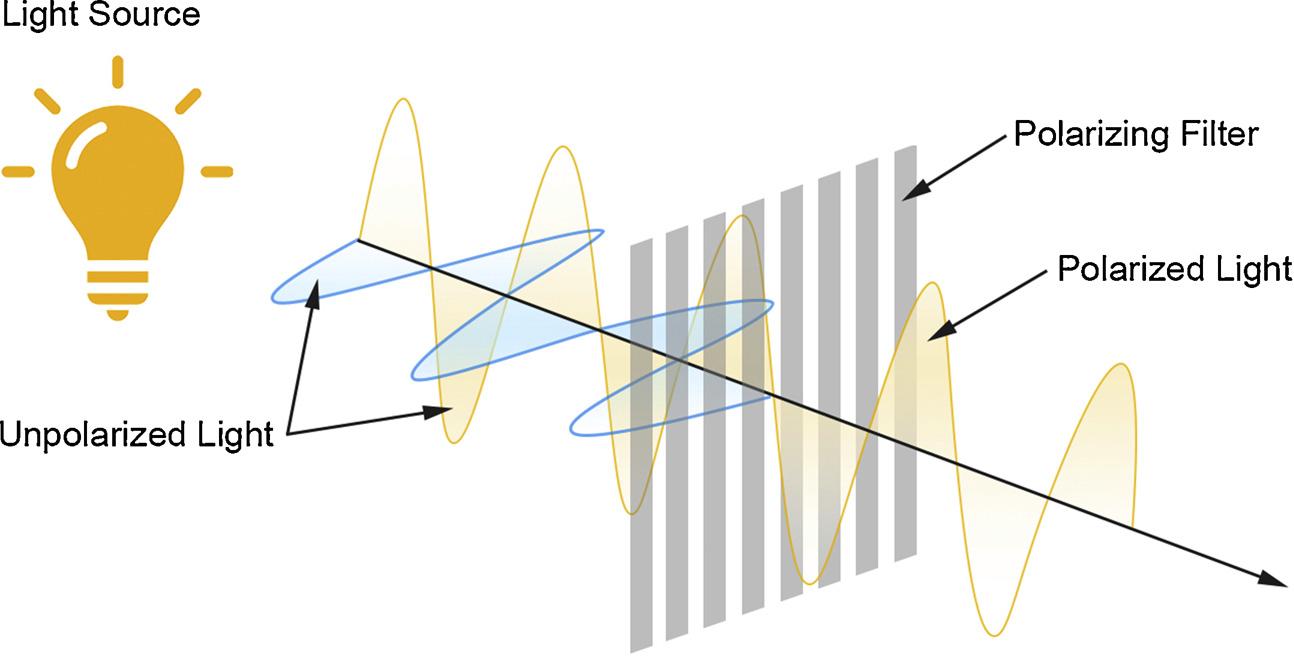
physicalpropertiesaredescribedbyitswavelength(i.e.thedistance betweenthetwonearestpeaksinthewave),withvisiblelightspanning from390to700nminhumans.Specificwavelengthscorrelatewiththe visualphenomenonofcolorwhenprocessedbythebrain.Lightwavelengthsbelowthisareknownasultraviolet(UV)light,andaboveas infrared(IR),bothofwhicharenotdetectablebythehumanretina.In itstypicalsettinglightisincoherentorunpolarized,withindividual wavestravellinginallplanesanddirections.Polarizationisachievedby passingincoherentlightthroughspeciallydesigned filters,whichallow wavestravellinginthedesiredplanetopassandblockingthoseoutside thedesiredparameter(Fig.1).Polarizedlightcanbeofasinglewavelengthorpolychromatic,aslongasallwavestravelinthesame plane.
Thereexistarangeofphototherapeuticmodalities,exploitingdifferentpartsofthevisiblespectrum(Fig.2).Themajormodalitiesare: UV-AandUV-Btherapies,lowlevellasertherapy(LLLT),lightemitting diode(LED)therapyandIRtherapies.UVtherapiesareoftenusedto reducetheseverityofsomechronicskinconditionssuchaspsoriasis
⁎ Correspondingauthorsat:InstituteforHealthandSport,VictoriaUniversity,VIC,Australia.
E-mailaddresses: Vasso.Apostolopoulos@vu.edu.au (V.Apostolopoulos), Maja.Husaric@vu.edu.au (M.Husaric), Jim.Kiatos@vu.edu.au (D.Kiatos).
1 Theseauthorscontributedequally.
https://doi.org/10.1016/j.maturitas.2018.07.009
Received8June2018;Receivedinrevisedform7July2018;Accepted18July2018
0378-5122/©2018PublishedbyElsevierB.V.
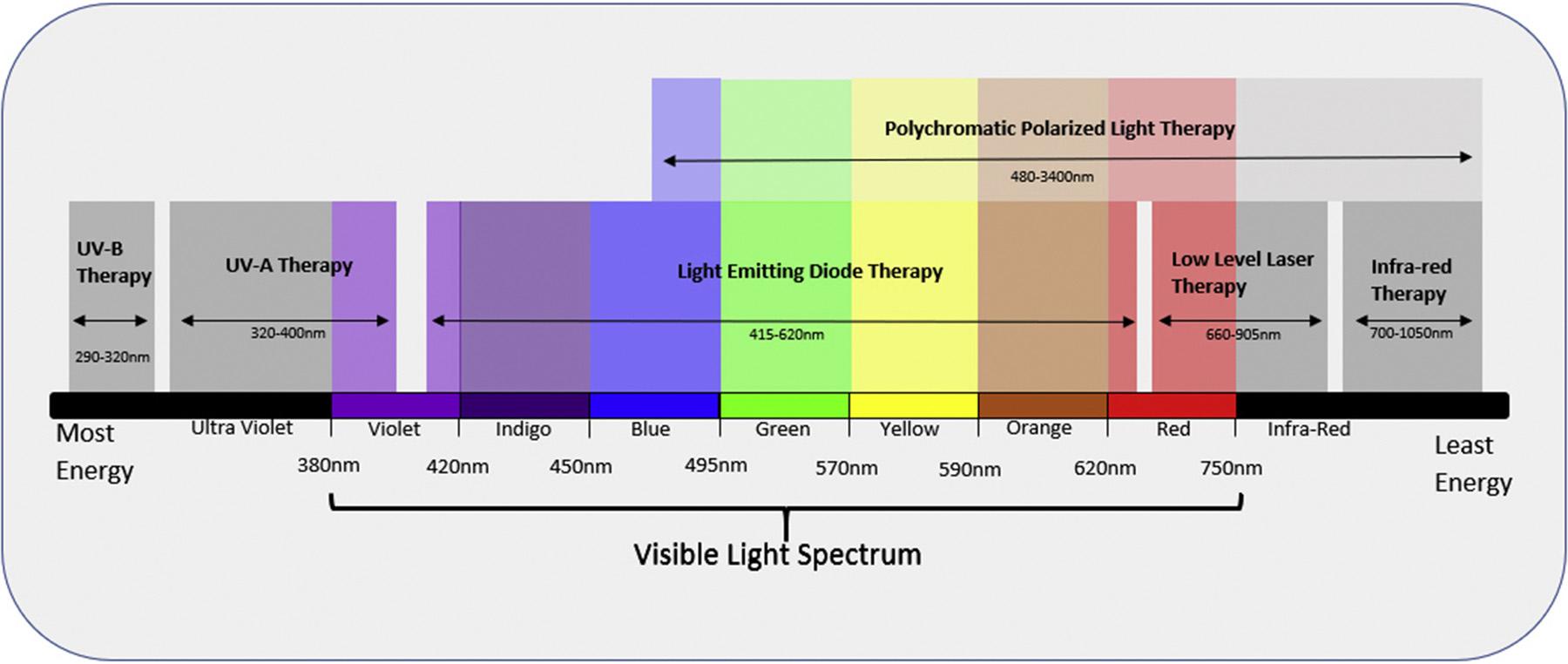
[6],andthereissomeevidencetosupportitsuseinatopicdermatitis [7].UV-Atherapiestypicallyutilizelightinthe320–400nmrange,and aregenerallyconsideredsafeforuse,thoughduetothehighenergyof lightinthisrange,burnscanoccur[8].NarrowbandUV-Btherapy utilizeslightinthe290–320nmrange.Thoughcorrectapplicationis generallyconsideredsafe,UV-Bradiationisstronglyassociatedwith developmentofawiderangeofskincancersandsoit’susemustbe tightlycontrolled[9].Followingitsinventioninthe1960s,laserlight hasbeensuccessfullyusedtherapeuticallywithmuchoftherelevant researchfocusedonlowlevellasertherapyforitslowriskofburnsand otheradverseeffects.LLLTisusedinarangeofconditions,suchas musculoskeletalinjuries,painreliefandwoundhealing[10],andhas thestrongestevidencetoinformitsusecomparedtootherformsof phototherapy.IRtherapiesutilizeeither “near” or “far” wavelengthsin theIRlightspectrum(700nm–1050nm),andtraditionallyhasbeen usedtowarmprematureinfantsinhospitalduetoitslowenergylevels. TheselowenergylevelsmakeIRlightverysafe,howeverithasquestionablecapacityforpenetration,limitingitsusetodermatological application.LEDtherapiesareanewerentity,whichutilizelightofa singlespecificwavelength,typicallycharacterizedbycolor.Themost commonmodalitiesareblueandredLEDtherapies,howeveryellow andgreendevicesarealsoavailable.Asthereislittleevidencesurroundingitsclinicaluse,thesedevicesarelargelylimitedtocosmetic applications,forconditionssuchasacnevulgaris.ThelowmanufacturingcostofLEDsystemshaspromptedanumberofcommercial entitiestobeginthedevelopmentandsaleofthesedevicesdespite lackingevidencesupportingtheiruse.
Lighttherapyusingbroad,visiblespectrumpolarizedlight(PLT) hasalsogainedinpopularityoverthepast30years.Personalized ‘at home’ devicesexistformanyofthesetherapies,allowingpatientstouse laserorPLTdevicestoself-administertheirowntreatment.Thesedevicesaremarketedasaidsforthetreatmentofvariousskinconditions suchaspsoriasis,atopicdermatitis,acnevulgarisandvitiligo.Despite theseassertionsbydevicemanufacturers,thereisadearthofevidence supportingtheefficacyofPLTinmanyofthesescenarios.
Over3decadesago,itwasproposedthatwhenthecellmembrane phospholipidbilayerisexposedtoalaserorpolarizedlight,therandom distributionofpolar-headedphospholipidsisreplacedbyamore structuredconfiguration,possiblyredistributingthebiologicallyactive proteinsandenablingmoreefficientfunction[11].Additionally,ithas beensuggestedthatPLTcouldalsoimprovecellularprocessessuchas activeandpassivetransport,recognitionofantibodiesandhormones, releaseandreceptionofneurotransmittersorenergytransmissionand conversion[12,13],allofwhichmaycontributetoimprovingthe healingprocess.Morerecently,itwasproposedthatdifferentwavelengthscausedifferentratesofcellularapoptosis,howeverthephysiologicalmechanismsarestillunclear[14].
Inmorerecentyears,theuseofPLThasbeenproposedinthe treatmentofvariousconditionsandisreportedtoacceleratethehealing process.PLTutilizesbroadspectrum,polarizedlight,typicallywithin the visible,andinfra-redranges(400nm – 3400nm).Thepolarization reducestheamountofenergyemittedbythelight,makingitsaferto use,whilststillallowingittopenetrateintodeepertissues.PLThas beenassociatedwithimprovedoutcomesin in-vivo modelsaswellasin
theclinicaltreatmentofdeepdermalburns,pressureanddiabeticulcers.Expectedtissuehealingtimesaresignificantlydecreasedincomparisontostandardwoundcareprotocols.Surgicalinterventionsare avoidedandbothcliniciansandpatientsfrequentlyexpresstheirdisbeliefinthepositiveoutcomes[12,15,16].Despitethispositiveevidence,qualitativemeasuresarescarce,relyinginsteadonexpertopinion,subjectiveoutcomemeasuresandlackingrobustcontrolled measures.
VerylittledocumentedresearchhasbeencarriedoutonpolychromaticspectrumPLTunderexperimentalconditions.Mostpublished studiesinvolvelasertreatmentssuchasPDT,ortheuseofsinglewavelengthphototherapy.Itisnotclearwhatchangesoccuratthemolecular,cellularandphysiologicallevelswhenPLTisusedtotreatskin lesionsandwounds.Herewepresentthelimitedresearchthatexists regardingPLTwithanemphasisondermalwoundhealingandmusculoskeletalinjuries.ThisreviewfocusesonpossiblePLTeffectsoccurringatthecellularlevel.Inaddition,wedescribehowotherformsof lighttherapyhavebeenshowntoaffectcellsatthecellularlevel,to identifypossiblelinksbetweenthemandPLT.
2.Methodology
SearcheswereconductedusingPUBMED,CINAHL(Cumulative IndextoNursingandAlliedHealthLiterature),TheCochraneLibrary, andMEDLINEusingthefollowingsearchterms:lighttherapy,phototherapy,polarization,biostimulation,polarizedlight,polychromatic non-coherentlight.Inadditionthefollowingsearchtermswereincludedinthecontextoflighttherapy – woundhealing,skinwound, biostimulation,ulcer,diabeticulcer,pressureulcer,burnsandmusculoskeletalinjuries.EnglishandAmericanEnglishspellingsofpolarized anditderivativeswereincluded.Studiesfromallyearswereincluded. Referencelistsofreviewedarticleswerealsoassessedforotherrelevant articles.Inclusioncriteriawerepeerreviewedpapersandtherapeutic useofpolychromaticpolarizedlight.StudiesthatusedUVspectrum lightfortreatmentandnon-Englisharticleswhichwerenotabletobe translatedwereexcluded.Titleandabstractanalysiswasperformedto identifyappropriatestudies,andfulltextsofincludedstudieswere assessed.Intotal17studieswerefoundonpolarizedlight,coveringa rangeoftopicsincluding:ulcers,burns,woundsandmusculoskeletal injuries.
3.Non-healingwounds
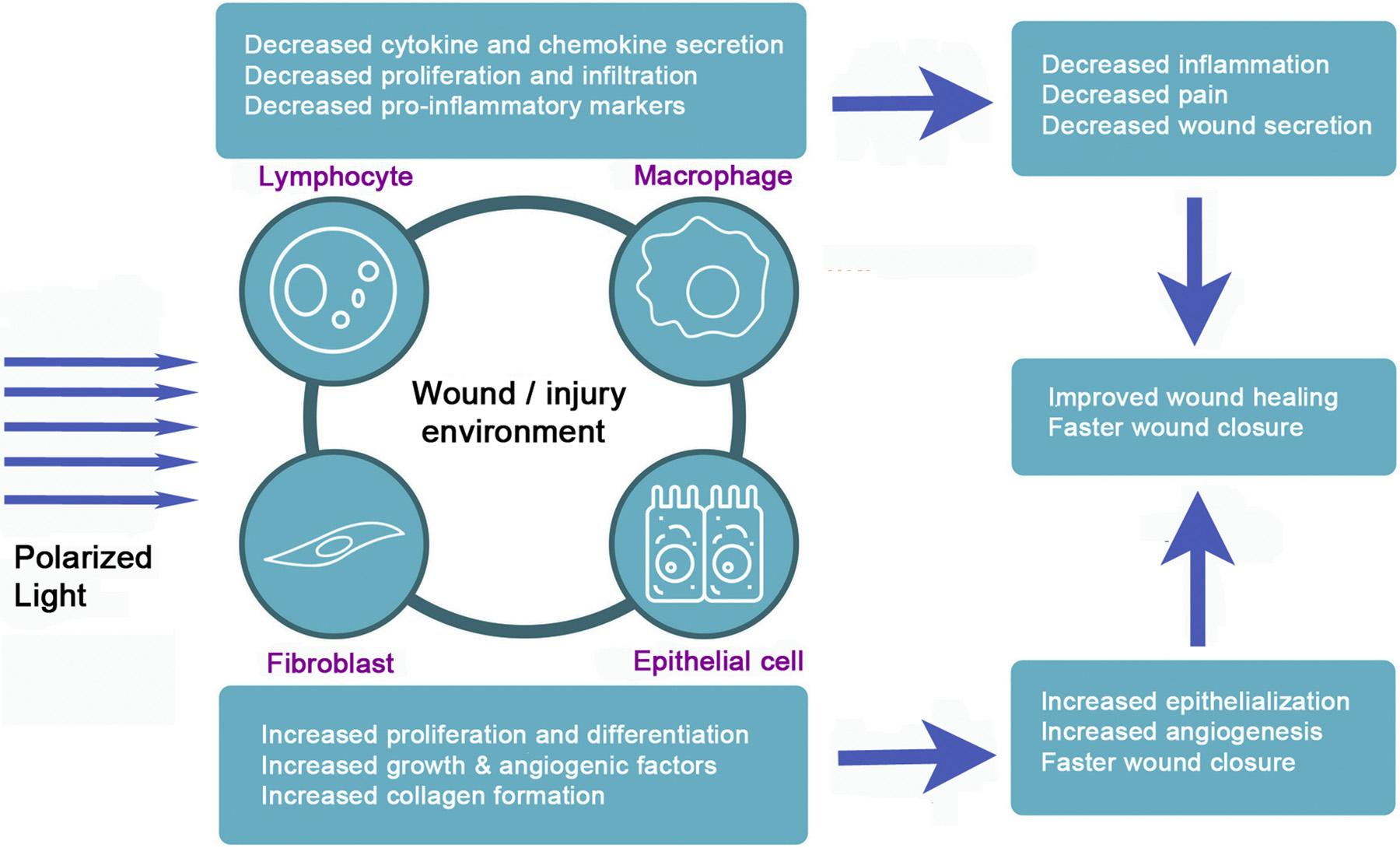
OnestudyinvestigatedtheeffectsofbroadspectrumPLTtopatients withwoundswhichwereresistanttonormaltreatmentmethods.PLTof 400nm–3000nmwasappliedto30patients,withnon-healingwounds includingdiabeticfootulcers,atherosclerosisobliterans,varicositiesor postthrombicsyndromes,decubitusulcerandosteomyelitis.Following PLTexposureresultedindecreasedwoundsecretionsandincreased epithelializationandwoundclosure.Inaddition,thisledtoanincreasedimmunecellinfiltrationandsecretionofcytokinesandchemokineswhichwasproportionaltotherateofhealing[12].However, muchofthisresearchwasnotappropriatelyblinded,controlled,randomized,orstatisticallyanalysedweakeningitsconclusion.Nevertheless,thestudydemonstratedacompellingcaseforthepossibilitiesof PLTapplicationfordelayedwoundhealing.
4.Dermalburns
Dermalburns,whichareknowntohavesignificantlyreducedpotentialforhealing,havebeenstudiedasatargetforPLT.Inonestudy, 22patientswithburnsweretreatedwithpolarizedlightwhichsubjectivelyacceleratedthehealingrateandrequiredlessfrequenttreatments[16].Whilstpromising,thestudyoutcomewasbasedonsubjectiveexpertopinion,andlackedacontrolorshamtreatmentgroupby whichtomakecomparisons,decreasingtheapplicabilityofthestudy.
Inratburnmodelshowever,PLThasbeenshowntohaveapositive effectonwoundhealing.Infact,seconddegreeburnscreatedonthe backsofratswereanalysedandscoredweeklyfor3weeks,comparing theirmacroscopicandhistopathologicalproperties.Macroscopically, woundclosurewasimprovedinthePLTgroup,aswellashistopathologicallysignificantimprovementinvascularizationandepithelialization.ThisdataaddstothetheorythatPLTaccelerateshealingbyaffectingboththeimmediateandlaterstagesofthehealingprocess[17]. Inanotherstudy,theeffectsof400nm–2000 nmPLTonthehealing effectsofthirddegreeburnsinratswithorwithoutdiabeteswas evaluated.Diabetesisknowntocausesignificantdiminishmentofa patientshealingcapacity.Hence,theeffectsofPLTover3weeks,was assessedinregardstoinflammation,re-epithelialization,neovascularization, fibroblastproliferationandcollagen fibredeposition.PLTwas showntoincreasecollagendeposition,enhancetheinflammatoryresponseandimprovevascularizationofwounds.Notably,itwasshown that10.2J/cm2 tobethemosteffectivedose,withincreaseddoses causingeffect[18].
5.Artificialwounds
Somestudieshaveusedartificialorsurgicalwoundstodetermine theeffectsofPLTonhealing.Onesuchstudyusedacohortof20patientsundergoingskingraftsasamodeltoexaminethis.Thedonor areasforskingraftswereconsidered ‘standardwounds’.Aseachpatient wastohavegraftstakenfromskinonboththighs,theybecametheir owncontrol.Thewoundsweretendedanddressedviastandardhospitalprocedures,butonethighwasirradiatedwithPLTwhichshowed vastimprovementinhealing[19].Thecreationofstandardwounds, althoughcontrolled,alsointroducespossiblesourcesoferror.Forexample,controlledsurgicalproceduresareunlikelytogeneralizewellto therealisticsettingofpathologicalwounding.However,thisstudydoes provideagoodbaselineforfuturestudiesofrealwoundsbylimitingthe numberofconfoundingvariablesthatcanbeencounteredinmore realisticsettings,suchasinfection,woundlocationanddebris.The modelofusingthepatientastheirowncontrolhaslikewisebenefits andrisks.Itensuresevenbaselinevariablesbetweenexperimentaland controlsubjects,meaningspecificparticipantfactorsthatmayinfluence healing(e.g.individualpathology),areaccountedforbutdoesnot accountforasystemicmodeofeffectsuchasimmunomodulation, whichwouldhaveeffectsonbilateralwounds.Animalmodelscango somewaytoremedyingthis,asvariablescanbemoretightlycontrolled betweenexperimentalanimals.InWistarratstheeffectsofLLLTand PLTonwoundhealingwasevaluated;eachratreceivedasingle,dorsal, surgicalcut,followedby20J/cm2 and40J/cm2 of685nmLLLTand 400nm–2000nm,andcomparedagainstuntreatedcontrolgroup.It wasnotedthat20J/cm2 ofPLTorLLLTcausedimprovementsincollagendepositionandorganization,andPLTadditionallyincreasedthe numberofmyofibroblastspresent[20].Asimilarstudyused 480nm–3400nmPLTonfullthicknessskinwoundsandnotedstatisticallysignificantimprovementsinepithelializationandsuggesteda qualitative(butnon-significant)improvementinwoundhealing[21]. Inaddition,differentlightparameterswereassessed,suchas,polarized, linearlypolarized,rightcircularlypolarizedandleftcircularlypolarized,toa20mmdiameterwound.Thewoundsshowedsignificant decreaseinsizeafterexposuretorightcircularlyandlinearlypolarized light,andtype1procollagenmRNAexpressionwasupregulatedinthe rightcircularlypolarizedlightgroup[22].Further,rightcircularlyand linearlypolarizedlightgroupsshowedincreasedproliferationof fibroblasts.Thisstudyprovidesimportantinformationregardingthe physiologicaleffectscausedbyrightcircularlypolarizedtreatmentand thatanopticalactivematerialpossessingacirculardichroicspectrum facilitatedabiochemicalreaction[22].Thisstudyhadastrongmethodology,withappropriatecontrolsandquantitativemeasuresgiving morereliableevidenceinfavourofPLT(Table1).
Table1
EffectsofLowlevellasertherapy(LLLT)oncellsurfacemarkers,chemokines,cytokines.
Celltype/Model
MaturedendriticCells[34]
MaturedendriticCells[35]
RatModel[36]
Aorticsmoothmusclecells(in-vitro)[37] IL-1beta
Mice[41] MCP-1
Arthritisinducedrats[40] CCL2 CCL4
Humanmonocytes[39] CCL2 CXCL10 TNF-alpha
6.Ulcers
Ulcers,regardlessoftheircause,oftenhavepoorcapacityfor healing,andseveralstudieshavedeterminedwhetherPLTcanplaya roleinreversingthis.Inastudycomprising55patientswithpaired controlandexperimentalulcers,demonstratedsignificantimprovement inhealingwith50%ofthewoundscompletelyresolvedwithinone week[15].Likewise,pressureulcerswerealsosignificantlyimprovedin 40patientsinarandomizedsingle-blindedcontroltrialwhichused woundsurfaceareaandthepressureulcerscaleasoutcomemeasures [23].However,thecontrolandexperimentalgroupswerepoorly matchedatbaselineandwoundscoringwasinconsistent.Despitethe promisingoutcomes,thedifferencesatbaselinemayhaveskewedthe resultstowardsfavourablehealingwithPLT.Inaddition,in25patients withvenouslegulcersweresignificantlyreduced(woundsurfacearea andnumberofulcers)followingphototherapyonceadayforfour weeks[24].PLThasalsobeenshowntobeeffectiveinulcerprevention inanacutecaresetting.Infact,10minofPLT/dayinadditionto standardulcerpreventionprotocolsresultedinlesssacralandheelulcersofgradeIIandaboveoverthetwomonthsin23patientscompared tocontrols.ThissuggeststhatPLTcouldbeaneffectiveadjunctto normalulcerpreventiontechniquesinbedriddenpatients.Thisevidence,whilstpreliminary,indicatesthatPLThaspotentialasanoninvasivenon-pharmacologicalinterventioninulcercontrolandprevention,howeverrobust,controlledtrialsarerequiredtofullyexpand these findings.
7.Musculoskeletalinjuries
AnotherareainwhichPLThasbeenappliedclinicallyisthetreatmentofmusculoskeletalinjuries.Threestudieshaveassessedtheuseof PLTintendinousinjuriesofthelateralelbow,generally findingpositive results.Tendinopathiesareknowntobedifficultinjurieswhichoften havelimitedimprovementstostandardtherapies.Onestudycompared theeffectsofsupervisedexerciserehabilitation,Cyriaxphysiotherapy (astructured,unsupervisedrehabilitationregimen)andPLTtopatients reportedpainandpain-freegripstrengthinthesepatients.Itwasnoted thatsupervisedphysiotherapytobethesuperiorintervention,however, PLTdidshowsignificantimprovementsinallparameters[25].PLThas alsobeencomparedtoLLLTinthetreatmentofthesepatients.Fifty patientsweredividedintotwogroupsandreceivedfourweeksofeither LLLTorPLTinconjunctionwithastandardexerciseprogram, finding nosignificantdifferencesamongstthetwoinpainandfunctionalimprovement,thoughbothgroupsshowedimprovementfrombaseline [26].Inasimilarvein,PLThasbeenshowntobeeffectiveintreating lateralelbowepicondylalgia,decreasingpatientpainandincreasing functionandpain-freegripstrength[27].Whilethesestudiesprovide
positiveevidencefortheplaceofPLTintreatingtheseconditions,all threesufferfromthelackofanuntreated,orstandardpracticecontrol andlackofblindingofpatientsandpractitioners.Thisweakenstheir conclusionsasitisunclearwhethertheeffectsdemonstratedweredue tothePLTintervention,oranotherfactorsuchaspatienthealing, placeboorchance.Nonetheless,theyprovideaninterestingoutlookof PLT’sefficacyinthetreatmentofthesestubborninjuries.Anotherstudy investigatedtheeffectofPLTonacuteanklesprains,acommon,painful injury encounteredinphysicaltherapy.Theyenrolled50participants anddividedthemevenlyintocontrolandexperimentalgroups.Both groupsreceivedstandardcryotherapyandtheexperimentalgroupadditional5treatmentsofPLT(10min.daily,for5days),andpatient reportedpainscores,oedemaandanklerangeofmotion(ROM)were assessedafter5days.PLTwasfoundtocausestatisticallysignificant improvementacrossallparameterswhencomparedtocontrol,providingstrongevidenceofitspotentialfortreatment.Thisstudyhad robustmethodology,thoughwasonlysingleblinded,leavingitunable toaccountforplaceboeffectoftreatment,orthepsychologicaleffects ofregularcontactwithhealthcarepersonnel[28].Likewise,inpatients withidiopathiccarpaltunnelsyndrome,apainfulconditioninthehand PLT3times/weekfor6minover4weeks,showedimprovementsin nocturnalpainandparaesthesiabutdidnotreportanystatisticalanalysisoreffectsizesanddidnotuseacontrolgroup,limitingtheinformationthatcanbegainedfromthestudy[29].Overall,thereis evidencethatsuggeststhatPLTcanimprovepatientsymptomsand functionintendinousandligamentousinjuries,howevermethodologicalissueswithmostofthestudiesinthearealimittheapplicabilityof thisresearch,andmorecarefullycontrolledtrialsarerequiredtofully confirmPLTsefficacy,aswellastocreatedoseresponsecurvesand protocols.Additionally,therearenoreportsonthephysiologicalmechanismfortheeffectsofPLTintheseinjuries,and invitro studiesare requiredtoexpandonthistoenableitstranslationintoclinicalpractice.
8.Limitations
Whilethereisagrowingbodyofevidencedemonstratingthe healingpotentialofPLT,thebodyofliteratureremainssmall,and generallyoflowquality.Mostoftheidentifiedstudieshadsmallsample sizesandgenerallylackedrobustmethodologies,includingblinding andcontrolpopulations.Additionally,manyofthestudiesrelied heavilyonqualitativeoutcomesandhadmixedresultsregardingstatisticallysignificantchanges.TherewasalsovariancewithintheprotocolsofPLTapplication.Ingeneral,theapplicationofPLTwassimilar: treatmentwasappliedforshorttimeframes(1–3weeks),withsome shorttermfollowup.However,anumberofdifferingprotocolswere usedregardingtheamount,timeandfrequencyofapplication,making acomparisonofresultsdifficult.Additionally,nolong-termfollowup
studieshavebeenreported,leavinginformationastothelong-term effectsofPLTscarce.Despitethese flaws,theoverallconsensuswasthat PLTprovidedsmalltomodestimprovements,particularlyattheearly timepoints[12,15–17,19]onwoundswithagreaterpreservationof tissuestructuralintegrity[23,30].However,therearestillmany questionsremainingthatneedtobeansweredformorewidespreaduse ofPLTtoberecommended.Firstly,thesafetyofPLTisyettobefully evaluated.ThereisacasestudyreportingthedevelopmentofametastasizedmyxoidmelanomainapatientusingPLT[31]however,the applicationofthisislimitedduetomethodologicalissues.Someforms oflight,mostnotablyUV,havebeenassociatedwithanincreasedrisk ofmalignancy[32],andassuchitisimportanttoevaluatethese,and anyother,patientrisks.Itisimportanttonotehowever,thatUV therapyhasbeenfoundtobeasafeintervention[33],andbasedonthe lowerenergylevelsinvolvedinPLT,thisislikelytoholdtrue.However, ifPLTistobecomeamorewidelyusedinterventionfullriskevaluation mustbeperformed.ThereisalsolittleevidenceregardingthemechanismsbywhichPLTmayexertitseffect.Thereissomeindication thatPLThaseffectsonbothlocalconnectivetissuecells[12,22],and hascapacitytoinfluencetheimmunesystem[12],thoughlittleinformationexistsregardingspecific,biologicalchangesdrivingthis.One studyidentifiedachangeintheexpressionofprocollagenmRNA[22], providingarationaleforfurtherstudiestodeterminechangesatthe molecularandcellularlevel(Fig.3).Whilethereisacompleteabsence ofevidencesupportingabiochemicalorphysicalmechanismforthe effectsofPLToncellfunction.However,somesuggestedmechanisms havebeentheorizedabout,theseareyettobesubstantiated(Fig.4). Thesemechanismsincludechangestothepolarizationorstructureof thephospholipidmembrane,increasedATPproductionviamitochondrialstimulationoractivationofphotosensitivereceptorsineitherthe cellornuclearmembranes,withresultingchangestocellphysiologyor geneexpression.Finally,furthercontrolled,robuststudiesarerequired todemonstratePLTseffectiveness,aswellastoestablishbestpractice dosageprotocolsanddoseresponsecurves.Overall,theliteratureseems toindicateagenerallypositiveeffect,howeversignificantmethodologicalissuesmakedefinitivestatementsofefficacyimpossible.Itdoes howeverprovideadirectionforfutureresearch,asitholdsthepotential toprovideasafe,cheapandeffectiveadjuncttothestandardcareofa
numberofconditions.
9.Immunomodulation:alow-levellaserperspective
Astheimmunesystemismostactiveintheacutestagesofwound healing,andPLThasbeenshowntobemosteffectiveatthistime,itis inferred thatPLTmayexhibitimmunomodulatoryeffects.ThesequestionsmaybeansweredbyselectivelyexaminingtheeffectsofPLTon immunecells.ThelackofPLTresearchmakesthesequestionsdifficult toanswer,however,researchpublishedusingLLLT,inwhichasingle wavelengthisusedmaypavethewaytopossiblemechanismsofaction forPLT.
Phototherapies,particularlyLLLT,havebeendemonstratedtohave immunomodulatoryeffectsonmammaliancells.Chenetal.,examined theeffectsofan810nmlaseronmurinebone-marrowderiveddendritic cells(DCs), in-vitro.ImmatureDCswerematuredwitheitherlipopolysaccharideorCpGoligodeoxynucleotide,andexposedtolaserlight therapy,resultinginthedownregulationofMHCclassIIandupregulationofCD86cellsurfacemarkers.ImmatureDCsexposedtothesame LLLThadnochange.TheauthorsconcludedthatLLLThasananti-inflammatoryeffectonactivatedDCs,andsuggesteditwaspossibly mediatedbycAMPandreducedNF-κBsignalling[34].Inanother study,maturesplenicDCs,whichhadbeentreatedwithaphotosensitizer,weretreatedwitha690nmlaseratadoseof5J/cm2,and showeddownregulationofcellsurfacemarkers(MHCclassI,MHCclass II,CD80andCD86)andaresultingsuppressionofTcellactivation [35].Inrats,2groupsreceivedwoundsbyscalpel(groupsAandC) whilsttheother2groupshadtheirwoundsinducedbylaser(groupsB andD).Twoofthefourgroups(AandB)weresubjectto2boutsoflow levellaserirradiation24hapartfollowingtheirwounds(wavelength 870nm,totalirradiationtime120sand9.6Jcm2).Whencomparing GroupA(scalpelinducedwoundwithLLLT)withgroupC(laserinducedwoundwithnoLLLT)itwasclearthattherewasamarkeddecreaseintheexpressionofIL-1β forgroupA.Additionally,therewere slight,non-significantdecreasesinmRNAlevelsofIL-1β inGroupB (laser-inducedwoundswithLLLT)whencomparedtoGroupD(laser inducedwoundswithnoLLLT)[36].GeneexpressionofIL-1β inGroup B(laserinducedwoundandLLLT)wasslightlylowerthanthatofGroup
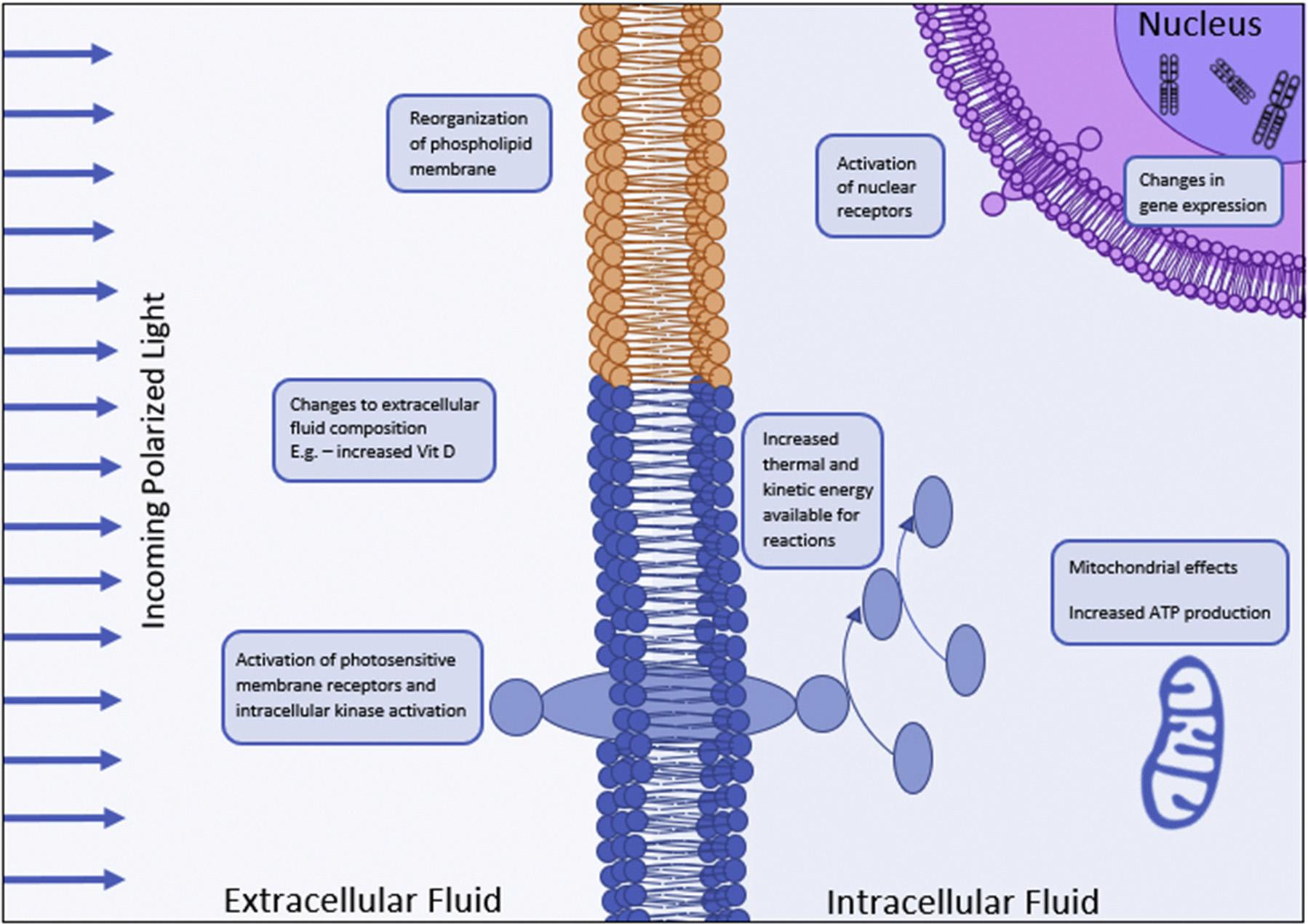
Summaryofthepossiblephysiologicalmechanismsofpolarizedlighttherapy.
C(scalpelinducedwoundandnoLLLT)butnotsignificantlydifferent. Likewise,inporcineaorticsmoothmusclecells,IL-1β geneexpression wasalsoreducedwithinthe firsthalfhourfollowingLLLTtreatment (780nmwith1–2J/cm2)[37].Moreover,theeffectsoflight-emitting diodetherapy(LEDT)showedthatLEDTinducedpro-inflammatory cytokines(TNF-α andIL-1β)inanacutetimeframebutswitchedto anti-inflammatory(IL-10)post5daysLEDTexposure[38].
TheeffectsofasingleboutofLLLT(660nmat1–2J/cm2)tohuman monocytecellline(THP-1)showedthatCCL2mRNAexpressionwas enhanced24h’ postirradiation,althoughexposureat3J/cm2 LLLT suppressedCCL2expressioninTHP-1cells[39].Thisresultsuggests thatatdifferingdoses,LLLTcanbeapotentenhancerorsuppressorof pro-inflammatorycytokinesandchemokinesinhumanmonocytes.This studyalsoshowedthat1J/cm2 LLLTinducedCCL2andCXCL10proteinexpressionwhereashigherdosesof2J/cm2 and3J/cm2 didnot.In ratswithcollagen-inducedarthritis,LLLTupregulatedtheexpressionof CCL2andCCL4inthesynovialtissues,resultingintheenhancementof healing[40].Additionally,inanotherstudyitwasnotedthatinfrared LLLTof780nmat10J/cm2 administeredacrossthreesessionsmarkedlyreducedMCP-1levels,andmayhaveabeneficialeffectonsurgical wounds[41].Althoughitisnotpossibletoautomaticallyextrapolate theresultsofthis invitro experimenttointactlivingorganisms,thedata issuggestivethattheimmunomodulatoryeffectofLLLTonmonocyte polarizationcouldbeapotentialtreatmentforallergicorauto-immune diseasesandatadifferentdosecouldalsobeusedtopromoteinflammationandimmuneresponsetopathogenicstimuli.
10.Conclusionandfutureprospects
Manyofthestudiesincludedinthisreviewsufferedfrom flawed methodology,weakeningtherecommendationsthatcanbemadefrom thisreview.Overallhowever,theevidenceislargelyfavourableofPLT asatherapyinarangeofconditions,withastrongsafetyprofile,and unanimouslybeneficialeffectsreported.However,beforePLTcanbe
confidentlyrecommendedforregularmedicaluse,researchwithrobust methodologiesmustbedoneinbothhealthyandpathologicalsettings tofullyunderstanditseffects.Doseresponsetrailsmustalsobeperformedto findthemosteffectiveprotocolsfortreatmentofthevarious conditionsidentified.Additionally,studieswithlongtermfollowup shouldbeemployedtofullyvalidatethelong-termefficacyandsafety profileofPLT.Asanadjuncttothis, invitro studiesontheeffectsofPLT onthevariouscelltypesinvolvedinthehealingprocessshouldbe performedtoprovideplausibletherapeuticmechanismsandtargets. Overall,PLTisanexcitingtherapywithlargepotentialforutilizationin arangeofconditions,howeveradeeperunderstandingofitsbiological mechanismsandphysiologicaleffectsisessentialforitstranslationinto commonplacemedicaluse.
Contributors
JackFeehancontributedtothedraftingofthearticle,andedited andreviewedthedraft.
SorayaPatriciaBurrowscontributedtothedraftingofthearticle. LeonardoCorneliuscontributedtothedraftingofthearticle.
AlyseMalietzisCookcontributedtothedraftingofthearticle.
KathleenMikkelsencontributedtothedraftingofthearticle,and editedandreviewedthedraft.
VassoApostolopouloscontributedtothedraftingofthearticle,and editedandreviewedthedraft.
MajaHusariccontributedtothedraftingofthearticle,andedited andreviewedthedraft.
DimitriosKiatoscontributedtothedraftingofthearticle,andedited andreviewedthedraft.
Conflictofinterest
Theauthorshavenoconflictofinteresttodeclare.
Funding
Nofundingwasreceivedspecificallyforthepreparationofthisreview.
Ethicalapproval
Noethicswasrequiredforthisreviewarticle.
Provenanceandpeerreview
Thisarticlehasundergonepeerreview.
Acknowledgements
TheauthorswouldliketothanktheImmunologyprograminthe CentreforChronicDiseaseandtheCollegeofHealthandBiomedicine forsupportanddiscussions.VAwouldliketothanktheVictoria UniversityCollegeofHealthandBiomedicinestart-upfundsandthe CentreforChronicDisease,VictoriaUniversityfor financialsupport. KMwassupportedbytheViceChancellorsVictoriaUniversity ScholarshipandJFbytheUniversityofMelbournePostgraduate Scholarship.Finally,theauthorsthankMyfanwyThewlisfortheproductionofthe figures.
References
[1] S.Guo,L.A.DiPietro,Factorsaffectingwoundhealing,J.Dent.Res.89(2010) 219–229
[2] D.T.McCoy,EgyptianMythologyforSmartPeople,(2017)
[3] A.H.Coulter,AlternativeandComplementerayTherapies92003,(2018)
[4] J.W.Stewart,F.M.Quitkin,M.Terman,J.S.Terman,Isseasonalaffectivedisordera variantofatypicaldepression?Differentialresponsetolighttherapy,Psychiatry Res.33(1990)121–128
[5]CIES.017/E:20112011ILV:InternationalLightingVocabulary.Commission InternationaledelÉclairage.
[6] R.K.Singh,K.M.Lee,M.V.Jose,M.Nakamura,D.Ucmak,B.Farahnik,etal.,The patient’sguidetopsoriasistreatment.Part1:UVBphototherapy,Dermatol.Ther. (Heidelb)6(2016)307–313
[7] M.Hannuksela,J.Karvonen,M.Husa,R.Jokela,L.Katajamäki,M.Leppisaari, Ultravioletlighttherapyinatopicdermatitis,ActaDerm.-Venereol.Suppl.114 (1985)137–139
[8] E.C.Siegfried,M.S.Stone,K.C.Madison,Ultravioletlightburn:acutaneouscomplicationofvisiblelightphototherapyofneonataljaundice,Pediatr.Dermatol.9 (1992)278–282
[9] H.Slaper,A.Schothorst,RiskevaluationofUVBtherapyforpsoriasis:comparison ofcalculatedriskforUVBtherapyandobservedriskinPUVA-treatedpatients, Photo-dermatology3(1986)271–283
[10] L.J.Walsh,Thecurrentstatusoflowlevellasertherapyindentistry,part1.Soft tissueapplications,Aust.Dent.J.42(1997)247–254
[11] I.Kertesz,M.Fenyö,E.Mester,G.Bathory,Hypotheticalphysicalmodelforlaser biostimulation,Opt.LaserTechnol.14(1982)31–32.
[12] M.Fenyo,Theoreticalandexperimentalbasisofbiostimulation,Opt.Laser (1984)4
[13] T.Kubasova,M.Horváth,K.Kocsis,M.Fenyö,Effectofvisiblelightonsomecellularandimmuneparameters,Immunol.CellBiol.73(1995)239
[14] L.Helander,H.E.Krokan,A.Johnsson,O.A.Gederaas,K.Plaetzer,Redversusblue lightilluminationinhexyl5-aminolevulinatephotodynamictherapy:theinfluence oflightcolorandirradianceonthetreatmentoutcomeinvitro,J.Biomed.Opt.19 (2014)088002
[15] P.Iordanou,G.Baltopoulos,M.Giannakopoulou,P.Bellou,E.Ktenas,Effectof polarizedlightinthehealingprocessofpressureulcers,Int.J.Nurs.Pract.8(2002) 49–55
[16] S.Monstrey,H.Hoeksema,H.Saelens,K.Depuydt,M.Hamdi,K.VanLanduyt, etal.,Aconservativeapproachfordeepdermalburnwoundsusingpolarised-light therapy,Br.J.Plast.Surg.55(2002)420–426
[17] C.A. Karadag,M.Birtane,A.C.Aygit,K.Uzunca,L.Doganay,Theefficacyoflinear
polarizedpolychromaticlightonburnwoundhealing:anexperimentalstudyon rats,J.BurnCareRes.28(2007)291–298
[18] P.C.Oliveira,A.L.B.Pinheiro,I.C.deCastro,J.A.ReisJunior,M.P.Noia,C.Gurgel, etal.,Evaluationoftheeffectsofpolarizedlight(λ400–200nm)onthehealingof third-degreeburnsininduceddiabeticandnondiabeticrats,Photomed.LaserSurg. 29(2011)619–625
[19] S.Monstrey,H.Hoeksema,K.Depuydt,VanMaele,K.VanLanduyt,P.Blondeel, Theeffectofpolarizedlightonwouldhealing,Eur.J.Plast.Surg.24(2002) 377–382
[20] A.L.B.Pinheiro,D.H.Pozza,M.G.D.Oliveira,R.Weissmann,L.M.P.Ramalho, Polarizedlight(400–2000nm)andnon-ablativelaser(685nm):adescriptionofthe woundhealingprocessusingimmunohistochemicalanalysis,Photomed.LaserTher. 23(2005)485–492
[21] P.Iordanou,E.G.Lykoudis,A.Athanasiou,E.Koniaris,M.Papaevangelou, T.Fatsea,etal.,Effectofvisibleandinfraredpolarizedlightonthehealingprocess offull-thicknessskinwounds:anexperimentalstudy,Photomed.LaserSurg.27 (2009)261–267
[22] K.Tada,K.Ikeda,K.Tomita,Effectofpolarizedlightemittingdiodeirradiationon woundhealing,J.Trauma67(2009)1073–1079
[23] A.Durovic,D.Maric,Z.Brdareski,M.Jevtic,S.Durdevic,Theeffectsofpolarized lighttherapyinpressureulcerhealing,Vojnosanit.Pregl.65(2008)906–912.
[24] L.Medenica,M.Lens,Theuseofpolarisedpolychromaticnon-coherentlightalone asatherapyforvenouslegulceration,J.WoundCare12(2003)37–40
[25] D.Stasinopoulos,I.Stasinopoulos,Comparisonofeffectsofcyriaxphysiotherapy,a supervisedexerciseprogrammeandpolarizedpolychromaticnon-coherentlight (bioptronlight)forthetreatmentoflateralepicondylitis,Clin.Rehabil.20(2006) 12–23
[26] D.Stasinopoulos,I.Stasinopoulos,M.Pantelis,K.Stasinopoulou,Comparingthe effectsofexerciseprogramandlow-levellasertherapywithexerciseprogramand polarizedpolychromaticnon-coherentlight(bioptronlight)onthetreatmentof lateralelbowtendinopathy,Photomed.LaserSurg.27(2009)513–520
[27] D.Stasinopoulos,Theuseofpolarizedpolychromaticnon-coherentlightastherapy foracutetenniselbow/lateralepicondylalgia:apilotstudy,Photomed.LaserTher. 23(2005)66–69
[28] D.Stasinopoulos,C.Papadopoulos,D.Lamnisos,I.Stasinopoulos,Theuseof bioptron light(polarized,polychromatic,non-coherent)therapyforthetreatment ofacuteanklesprains,Disabil.Rehabil.39(2017)450–457
[29] D.Stasinopoulos,I.Stasinopoulos,M.Johnson,Treatmentofcarpaltunnelsyndromewithpolarizedpolychromaticnoncoherentlight(bioptronlight):apreliminary,prospective,openclinicaltrial,Photomed.LaserTher.23(2005) 225–228
[30] J.Verbelen,Useofpolarisedlightasamethodofpressureulcerpreventioninan adultintensivecareunit,J.WoundCare16(2007)145–150
[31] M.Ulamec,A.Soldo-Belic,M.Vucic,M.Buljan,B.Kruslin,D.Tomas,Melanoma withsecondmyxoidstromalchangesafterpersonallyappliedprolongedphototherapy,Am.J.Dermatopathol.30(2008)185–187
[32] J.D’Orazio,S.Jarrett,A.Amaro-Ortiz,T.Scott,UVradiationandtheskin,Int.J. Mol.Sci.14(2013)12222–12248
[33] E.Lee,J.Koo,T.Berger,UVBphototherapyandskincancerrisk:areviewofthe literature,Int.J.Dermatol.44(2005)355–360
[34] A.C.Chen,Y.Y.Huang,S.K.Sharma,M.R.Hamblin,Effectsof810-nmlaseron murinebone-marrow-deriveddendriticcells,Photomed.LaserSurg.29(2011) 383–389
[35] D.E.King,H.Jiang,G.O.Simkin,M.O.Obochi,J.G.Levy,D.W.Hunt,Photodynamic alterationofthesurfacereceptorexpressionpatternofmurinesplenicdendritic cells,Scand.J.Immunol.49(1999)184–192
[36] I.S.Sayed,A.Saafan,F.K.Abdel-Gawad,T.A.Harhash,M.A.Abdel-Rahman,Effect oflow-levellasertherapyongeneexpressionofvascularendothelialgrowthfactor andinterleukin-1ßinscalpel-inducedandlaser-inducedoralwoundsinrats,J. Dent.Lasers(2015)1
[37] L.Gavish,L.Perez,S.D.Gertz,Low-levellaserirradiationmodulatesmatrixmetalloproteinaseactivityandgeneexpressioninporcineaorticsmoothmusclecells, LasersSurg.Med.38(2006)779–786
[38] D.F.Martins,B.L.Turnes,F.J.Cidral-Filho,F.Bobinski,R.F.Rosas,L.G.Danielski, etal.,Light-emittingdiodetherapyreducespersistentinflammatorypain:roleof interleukin10andantioxidantenzymes,Neuroscience324(2016)485–495
[39] C.H.Chen,C.Z.Wang,Y.H.Wang,W.T.Liao,Y.J.Chen,C.H.Kuo,etal.,Effectsof low-levellasertherapyonM1-relatedcytokineexpressioninmonocytesviahistone modification,Mediat.Inflamm.(2014)2014625048.
[40] L.Zhang,J.Zhao,N.Kuboyama,Y.Abiko,Low-levellaserirradiationtreatment reducesCCL2expressioninratrheumatoidsynoviaviaachemokinesignaling pathway,LasersMed.Sci.26(2011)707–717
[41] T.Y.Fukuda,M.M.Tanji,J.F.deJesus,S.R.daSilva,M.N.Sato,H.Plapler,Infrared low-leveldiodelaseronserumchemokineMCP-1modulationinmice,LasersMed. Sci.28(2013)451–456