Business Development Manager: Andrew Jackson Ph: 0400 604 646 ajackson@wfmedia.com.au
PUBLISHED BY Westwick-Farrow Media
A.B.N. 22 152 305 336
Welcome to the October/November 2025 Infection Control Issue
www.wfmedia.com.au
Head Office
Unit 5, 6-8 Byfield Street, North Ryde Locked Bag 2226 North Ryde BC NSW 1670 AUSTRALIA ph: +61 2 9168 2500
If you have any queries regarding our privacy policy please email privacy@wfmedia.com.au
Subscriptions for unregistered readersprice on application
Printed and bound by Ive Group Print Post Approved PP100022780 ISSN 2204-3438 PRINT ISSN 2204-3446 DIGITAL
Westwick-Farrow Media is committed to using environmentally responsible print services to produce our publications. This edition is made with a mixture of materials from FSC-certified forests, recycled materials, and/or FSC-controlled wood. While controlled wood doesn't come from FSC-certified forests, it mitigates the risk of the material originating from unacceptable sources . It is delivered in a totally degradable plastic wrapper.
Hospital-acquired infections (HAIs) are a central, but mostly preventable, concern in health care — in the first feature of this issue, some key HAI prevention and control developments are set out. Also in line with this issue’s theme, we delve into some recent infection prevention and control research and case studies. This includes, in the context of antibiotic-resistant infections, asking whether home washing is contributing to spread and also considering a call from European researchers for a reassessment of healthcare guidelines in the wake of research suggesting an ICU disinfectant procedure used in certain countries may increase risk.
In our regular series, we are In Conversation with Australian College of Nursing CEO Dr Kathryn Zeitz — approaching one year in the role, we learn where we’re at, and where we need to go, with nurses’ scope of practice. For Design in Health, we tour the $180 million St Vincent’s Private Hospital Fitzroy expansion — completed this year, it includes a boutique hotel aesthetic and adaptive reuse of heritage buildings. And we spend A Day in the Life of Linda Nguyen — owner and founder of mobile optometrist practice Care Optometry, Linda was a finalist in the 2025 HESTA Excellence Awards.
WANT TO CONTRIBUTE?
Also in this issue: for our CEO Column, Mark Brooke of Lung Foundation Australia shares data from the Lived Experience Survey, showing the debilitating effect stigma has on patients; with hospitals all around the world integrating digital displays to create a more seamless, efficient and reassuring environment for everyone, Steven Baxter explores some key patient and staff benefits; and, concerning IVF, Professor David Gardner AM — co-author of research published this year in Biomolecules — explains how metabolism of the embryo could be a major component determining the success of implantation.
Plus more — happy reading.
Dr Joseph Brennan, PhD
Editor, H+H
hh@wfmedia.com.au
We welcome articles and research reports from health professionals across Australia for review for the bimonthly print publication and our daily web page. If you have a story you think would be of interest, please send an email to hh@wfmedia.com.au
CASE STUDY
NHS hospital pilots AI in discharge summaries
In the UK, Chelsea and Westminster Hospital NHS Foundation Trust has been involved in a pilot of the use of AI in discharge summaries — part of the UK Government’s AI Exemplars programme, announced in August. The AI-assisted tool is designed to help doctors draft discharge documents faster by extracting key details from medical records, such as diagnoses and test results, using a large language model. After a full review from a medical expert responsible for the patient, these documents are then used to discharge a patient from a ward and refer them to other care services that may be needed.
“It would radically improve an outdated system that can leave patients
go home,” the government said in a statement. “In some cases, the current system for writing discharge summaries can also inaccurately record basic patient details — like what treatment they’ve had, or changes to medication — and put them in harms way.”
The idea behind the program is that ‘exemplars’ — such as the program at Chelsea and Westminster Hospital NHS Foundation Trust; an AI diagnostics program to identify conditions such as lung cancer from scans; and a Ministry of Justice probation casework program, announced at the same time as the discharge documents program — will be developed and trialled, with those showing the most promise potentially rolled out more widely.
Speaking on a 13 August visit to Chelsea and Westminster Hospital, Technology Secretary Peter Kyle said: “This is exactly the kind of change we need: AI being used to give doctors, probation officers and other key workers more time to focus on delivering better outcomes and speeding up vital services.”
On 13 August, Peter Kyle and the Department of Science, Innovation and Technology team were welcomed by Roger Chinn, Chief Medical Officer, Marcella Vizcaychipi, Chief Clinical Information Officer, Gary Davies, Hospital Medical Director for Chelsea, and many of the Chelsea and Westminster Hospital NHS Foundation Trust staff demonstrating the innovative ways the Trust is currently harnessing the use of AI in both clinical care and administrative work flows. Source: Chelsea and Westminster Hospital NHS Foundation Trust
Hospital-acquired infections (HAIs) are a central, but mostly preventable, concern in health care — here’s some key HAI prevention and control developments.
In 2008, a 58-year-old man presented to his local ED with neurological symptoms, including confusion, dizziness and impaired memory — the symptoms of what was later discovered to be transient ischaemic attack.1
While he was undergoing investigations at the hospital, the man contracted an infection and, five days after admission, became febrile, dyspnoeic and tachycardic.
A blood test later confirmed he had acquired methicillin-susceptible staphylococcus aureus (MSSA) during the diagnostic process — a condition that prevented him from working in the four months thereafter.
Not an unusual case
While mainly associated with surgery, hospital-acquired infections (HAIs), including MSSA, often occur without an invasive procedure or device — and when they do occur, they prolong hospital stays by an average of 10 days.1
In Australia, serious complications from MSSA are not particularly common, but they are from other HAIs like pneumonia, surgical site and urinary tract infections.
In fact, every year, there are an estimated 170,574 cases of the top five most common HAIs across the country and these result in around 7583 deaths.2
A HAI can occur in any healthcare setting, including a hospital, healthcare office, general practice or dental clinic, or community health facility. They can also be transmitted in any site attended by a paramedic.
While often caused by multidrug resistant organisms (MDROs), a HAI can result from exposure to any bacteria, fungus, virus, parasite or prion.
HAIs also come with a hefty price tag, with one study estimating their annual cost to be US$200 billion.3
Most are preventable
What’s more, more than half of HAI cases are believed to be preventable, with the use of evidence-based strategies.4
For this reason, the Australian Commission on Safety and Quality in Health Care continually refreshes its infection prevention and control (IPC) guidelines, with the latest update released last year.
The 2024 revisions emphasise risk-based approaches, antimicrobial stewardship and strong leadership to foster safety culture in healthcare settings.
Proactive, multimodal approach
Hospitals are now also required to proactively monitor and continuously improve their IPC practice, not just comply with specified mandates.
Multimodal approaches have proven particularly efficacious. These include education and training, standardised processes and maximal use of sterile barrier precautions; along with adequate skin preparation, hand hygiene and catheter care.
A study in 2006 found that such approaches could reduce rates of catheter-related bloodstream infection by 66%, and that these reductions were maintained over an 18-month period.6
This trumps more passive strategies, which are mainly centred on surveillance and
feedback. A classic study in 1985 found that surveillance-based strategies reduced nosocomial infections by just 32%.7
The role of technology
In recent years technology has proved to be an important prong in a multimodal approach.
Globally, the IPC technology market is valued at USD 2.16 billion and is expected to reach USD 3.50 Billion by 2032.8
One option is an AI-powered electronic infection tracking system, which can identify outbreaks early and ensure staff are compliant with protocols.
Tools like hand hygiene compliance systems (HHCS) are also proving valuable. These are typically based on sound and light signals that activate when an opportunity to improve hand hygiene is detected, reminding staff, patients and visitors to sanitise their hands.
One study compared the use of HHCSs with human observation in intensive care units (ICUs) and found the technology was much more proficient at spotting these hand hygiene opportunities.9
Even though they recorded more opportunities than a human would, they wound up with a significantly lower rate of hand hygiene issues.
When they pilot tested the technology in the broader hospital, they recorded a reduction in catheter-associated urinary
tract infections and central line-associated bloodstream infections.9
In high-risk settings, like ICUs and operating theatres, robotics and automation provide an added layer of protection.
These tools include ultra-violet radiationbased devices, highly dynamic robotic grippers and sensing systems and autonomous heavy-duty cleaning robots. Many also rely on dry vacuum and mopping to remove germs and pesticides.
Robots can significantly improve IPC and showed great efficacy during the COVID-19 pandemic.10
Research indicates that many hospitals avoid IPC technology due to cost, but there is mounting evidence that the healthcare burden from HAIs may significantly outweigh the cost of implementation.11
Safety in numbers
Aside from technology, healthcare providers are encouraged to lean on partnerships and collaborations to ensure best practice in their IPC efforts.
During the COVID-19 pandemic, a collaboration between regional hospitals and referring nursing homes in a public health network led to a significant reduction in nursing home infections, such as urine cultures.12
The collaboration fostered knowledge exchange, allowing best practice IPC strategies to be shared with speed and ease.
Hospitals are now also required to proactively monitor and continuously improve their IPC practice, not just comply with specified mandates.
Cross sectoral collaboration can also help providers stay privy and prepared for emerging threats.
As the world learned during COVID-19, IPC is often a moving target and one which is best tackled together.
1. Infection Prevention and Control Practice Handbook. Section one — Healthcare Associated Infections. Clinical Excellence Commission; 2020. Accessed 23 September, 2025. https://www.cec.health.nsw.gov.au/__data/assets/ pdf_file/0009/706536/Section-1-Healthcare-AssociatedInfections.pdf
2. Lydeamore MJ, Mitchell BG, Bucknall T, et al. Burden of five healthcare associated infections in Australia. Antimicrob Resist Infect Control. 2022;11(69). doi: 10.1186/s13756-022-01109-8
3. Scott RD 2nd, Culler SD, Rask KJ. Understanding the economic impact of health care-associated infections: a cost perspective analysis. J Infus Nurs. 2019;42(2):61–69. doi: 10.1097/NAN.0000000000000313
4. Bearman G, Doll M, Cooper K, Stevens MP. Hospital infection prevention: how much can we prevent and how hard should we try? Curr Infect Dis Rep. 2019;21(1):2. doi: 10.1007/s11908019-0660-2
5. Australian Guidelines for the Prevention and Control of Infection in Healthcare. Australian Commission on Safety and Quality in Health Care; 2019 (updated 2024). Accessed 23 September, 2025 https://www.safetyandquality.gov.au/ publications-and-resources/resource-library/australianguidelines-prevention-and-control-infection-healthcare
6. Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–2732. doi: 10.1056/ NEJMoa061115
7. Haley RW, Culver DH, White JW, et al. The efficacy of infection surveillance and control programs in preventing nosocomial infections in US hospitals. Am J Epidemiol. 1985;121(2):182–205. doi: 10.1093/oxfordjournals.aje.a113990
8. Pawar, S. Global infection prevention devices market size, share, and trends analysis report — industry overview and forecast to 2032. Data Bridge Market Research; 2024. Accessed 23 September, 2025. https://www.
9. McCalla S, Reilly M, Thomas R, et al. An automated hand hygiene compliance system is associated with decreased rates of health care-associated infections. Am J Infect Control. 2018;46(12):1381–1386. doi: 10.1016/j.ajic.2018.05.017
10. Khan ZH, Siddique A, Lee CW. Robotics utilization for healthcare digitization in global COVID-19 management. Int J Environ Res Public Health. 2020;17(11):3819. doi: 10.3390/ ijerph17113819
11. Piaggio D, Zarro M, Pagliara S, et al. The use of smart environments and robots for infection prevention control: a systematic literature review. Am J Infect Control 2023;51(10):1175–1181. doi: 10.1016/j.ajic.2023.03.005
12. Jones KM, Greene MT, Meddings J, et al. Impact of a collaboration-focused intervention to prevent healthcareassociated infections before and during the COVID-19 pandemic. Clin Infect Dis. 2025;81(2):358–368. doi: 10.1093/ cid/ciaf122
*Amy Sarcevic is a freelance science and technical writer who regularly writes for Hospital + Healthcare. She has an academic background in psychology.
iStock.com/photoman
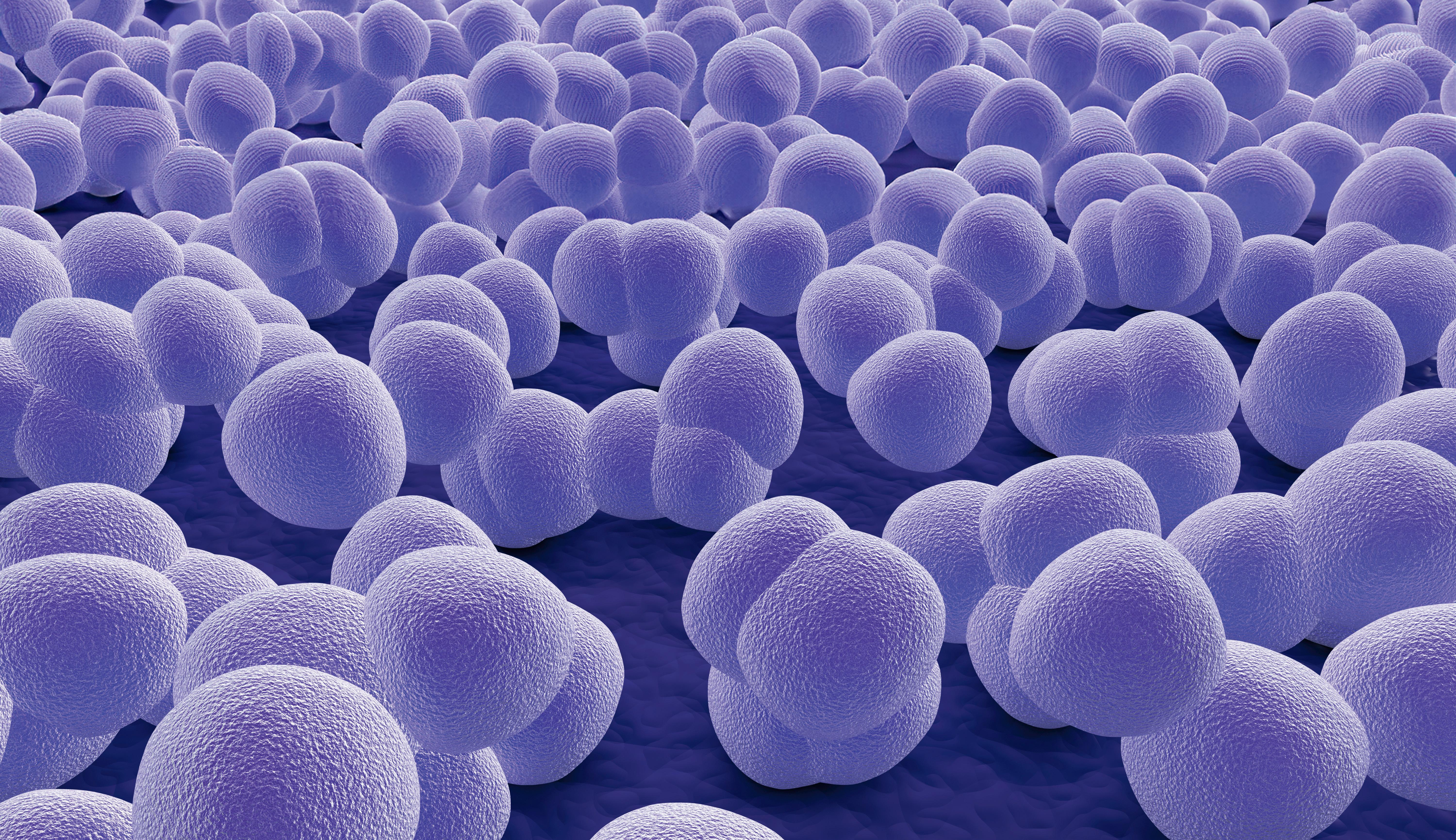
The Challenge of Biofilms in Healthcare
Biofilms represent a formidable challenge in the ongoing battle against healthcare-associated infections (HAIs), as they render pathogens more tolerant to conventional cleaning and disinfection methods. Tristel chlorine dioxide products have been specifically tested for their effectiveness against both wet and dry biofilms.
The Challenge of Biofilms in Healthcare
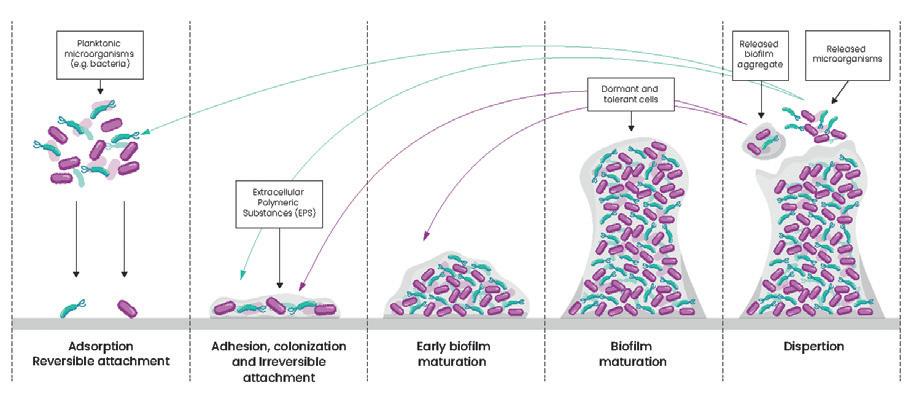
Biofilms are structured microbial communities encased in a selfproduced matrix, often found clinging to surfaces in healthcare environments. Once formed, they become difficult to eradicate. This is not just a cleaning issue, it’s a patient safety issue. Biofilms act as a reservoir for multi-drug resistant organisms (MDROs), shielding them from antimicrobials whilst also increasing the potential for horizontal gene transfer, accelerating the spread of resistance.
Bacteria living in a biofilm exhibit a 10 to 1000-fold increase in resistance to antibiotics compared to their planktonic counterparts.
Studies suggest that up to 65% of all microbial infections, and 80% of chronic infections involve biofilms. Biofilms can lead to persistent infections, increased resistance to treatments, and a heightened risk of cross-contamination. Their presence on medical equipment, environmental surfaces, and within environments such as water systems can also contribute to hospital-acquired infections (HAIs), posing a serious risk to patient safety.1,2
Are All Biofilms the Same?
While all biofilms represent a community of microorganisms encased in a protective matrix, their composition and characteristics can vary. They can consist of bacteria, yeasts and fungi, and even viruses. They typically consist of one or more different species of organisms and can persist on a surface for many hours.
Wet bio�ilm is a type of biofilm that forms in moist environments, where microorganisms thrive due to the presence of water and available nutrients. These microorganisms secrete a slimy layer of extracellular polymeric substance (EPS) containing polysaccharides, proteins, and lipids, embedding themselves in a protective matrix. Typically, they will consist of gram-negative bacteria such as Pseudomonas aeruginosa. In healthcare, wet biofilms can develop on and within the channels of reusable medical devices, in water lines, and on sinks, showers, and toilets and their surrounding surfaces.
Dry bio�ilm comprises microorganisms that form in dry or lowmoisture and nutrient-deficient environments. Due to these harsh conditions, microorganisms within a developed dry biofilm tend to be more resilient. Unlike wet biofilms, dry biofilms are found on surfaces with minimal moisture, such as on medical equipment or dry environmental surfaces. These biofilms can be challenging to detect and remove, as they are often more resistant to cleaning and disinfection efforts due to their dry state.3
Chlorine dioxide: Targeting Biofilms
There are methods available to assess the effectiveness of a disinfectant against a biofilm.
For wet bio�ilms , the MBEC assay (ASTM E2799) and the CDC model (ASTM E2871-22) can be used to assess disinfectant performance against biofilms of Staphylococcus aureus and Pseudomonas aeruginosa
Tristel chlorine dioxide solutions have been assessed using these methods against biofilms grown over a 72-hour period. All chlorine dioxide solutions tested achieved ≥4 log reduction in the MBEC assay and ≥5 log reduction in the CDC model at their respective contact times, as short as 30 seconds. This rapid and robust activity is critical in real-world IPC workflows where time and efficacy must align.
For dry bio�ilms, chlorine dioxide’s performance was evaluated using the CDC model (ASTM E2871-22) modified using a 12-day dehydration/ rehydration cycle. This approach is increasingly recognised for replicating real-world decontamination challenges posed by biofilms. All chlorine dioxide solutions tested achieved ≥5 log reductions at their respective contact times.
Implications for Infection Prevention
With chlorine dioxide proving effective against both surface contaminants and entrenched biofilms, its integration into routine IPC protocols could help tackle the challenge presented by biofilms and bridge the gap between compliance and real-world effectiveness.
1. Ledwoch, K., Dancer, S.J., Otter, J.A., Kerr, K., Roposte, D., Rushton, L., Weiser, R., Mahenthiralingam, E., Muir, D.D. and Maillard, J.-Y. . (2018). Beware biofilm! Dry biofilms containing bacterial pathogens on multiple healthcare surfaces; a multi-centre study. Journal of Hospital Infection, 100(3), pp.e47–e56. https://doi.org/10.1016/j.jhin.2018.06.028.
2. Maillard, J.-Y. and Centeleghe, I. (2023). How biofilm changes our understanding of cleaning and disinfection. Antimicrobial Resistance and Infection Control, [online] 12(1), p.95. https:// doi.org/10.1186/s13756-023-01290-4.
3. K Ledwoch, Vickery, K. and Maillard, J-Y. (2022). Dry surface biofilms: what you need to know. British journal of hospital medicine, 83(8), pp.1–3. https://doi.org/10.12968/hmed.2022.0274.
For more information, visit www.tristel.com/au-en/
High-end heritage
St Vincent’s Private Hospital, Fitzroy’s $180 million expansion of its Victoria Parade site was completed this year. With a new building designed to be energy efficient, flexible, functional, and fit seamlessly and sympathetically into its external surroundings, the expansion brought more than 100 new beds, new operating rooms and suites, a new medical imaging department, and a new pharmaceutical and retail space.
An adaptive reuse of the heritage buildings on the site, the expansion’s new 13-level building replaced two administration buildings and adjoins the existing hospital building; the new build’s decorative façade, with a neutral tone and colour, is sensitive to the heritage façades at street level, while newly refurbished arrival forecourts maximise the amenity of the available external spaces within the site’s urban context.
Designed by Billard Leece Partnership for St Vincent’s Health Australia, by ‘deinstitutionalising’ the interior design of the hospital environment and maternity suites, the design team have created a boutique hotel aesthetic; an environment that closely resembles a ‘home away from home’, here, family life was a guiding concept for the building and user experience.
Such an aesthetic is clear in the newly renovated maternity suites, which encourage wellness, recovery and smooth transition into motherhood. Generous room layouts create a more family-focussed environment, including larger beds and bathrooms that are
Courtesy Billard Leece Partnership
Courtesy Billard Leece Partnership
Courtesy Billard Leece Partnership
‘normalised’ but still compliant. Using neutral and natural tones, fixtures and finishes within the rooms and ensuites resemble those found in a high-end hotel.
City and cathedral views are a centrepiece of each suite, beds and nursing seats positioned to take advantage of natural light and the views, evoking feelings of contentment and wellbeing — designed to contribute to a sense of luxury and a de-stressing environment. While in the day-of-surgery patient amenity, personalised seating areas increase comfort and privacy and access to outlook and views.
Connection with an existing older, heritage site came with numerous challenges that needed to be overcome. These included limited open spaces between buildings, alignment with current ceiling height and room regulations, as well as fire risks. But while bridging between the old and new was structurally complex, the project navigated these while the hospital — including operating theatres — remained fully operational.
Using neutral and natural tones, fixtures and finishes within the rooms and ensuites resemble those found in a high-end hotel.
Revolutionising healthcare on-premise laundry
In order to keep linen, towels and uniforms washed to consistently high standards, onpremise laundries (OPLs) within healthcare facilities such as hospitals and care homes rely on automatic detergent dosing systems capable of handling heavy load demand.
Leading the market is global chemical dosing expert SEKO, which has been active in the sector for decades with a comprehensive portfolio of cutting-edge OPL systems ranging from single-pump units to multimachine solutions.
Alongside peristaltic, solenoid and pneumatic pump-driven equipment, SEKO has revolutionised laundry detergent dosing with its LS100 venturi-powered system.
A venturi is a device that uses water pressure to control flow and therefore contains no moving parts. For LS100 users, this means less wear compared to mechanical systems and hundreds of thousands of doses before they even need to consider venturi cartridge replacement.
Meanwhile, LS100 injects up to 10 chemicals — from detergent and fabric softener to
additives — in as many as four washers, making it perfect for on-premise laundries of every size. It’s modular, too, so operators can easily add additional units to their original system as demand increases and their laundry grows.
LS100 can be operated via the SekoBlue app, which uses Wi-Fi and Bluetooth connectivity for local and remote dosing management and data on demand. SekoBlue offers operators a portal from which they can access live and historical data on wash cycle status, chemical consumption and equipment performance at any time through their smart device, PC or laptop.
With vital information such as chemical consumption per kilo of laundry at their fingertips, managers can gain a detailed understanding of the true cost of their operation and identify and reduce detergent and water wastage as part of a sustainable operation.
Meanwhile, SekoBlue provides access to downloadable manuals, intelligent autotuning sensors and online step-by-step technical support which can facilitate
installation, setup and commissioning and reduce associated time and costs.
Having documents available in digital form is not only convenient but also ensures that engineers and end users always have access to the latest versions which can prevent errors and save time during installation and operation.
LS100’s user-focused design includes an intuitive 4.5″ touchscreen display plus a handheld colour-coded formula selector, making the system accessible for every user — essential when staff turnover is high and new recruits must learn on the job.
As intelligent pump equipment is increasingly specified for on-premise laundry machines within hospitals, care homes and other healthcare sites, SEKO’s dedicated systems such as LS100 provide discerning operators with the ability to save time, reduce spending and take command of their processes.
A day in the life of Linda Nguyen a mobile optometrist
06:45 As a busy mobile optometrist also juggling motherhood, wake-up hour means juggling the kids’ breakfasts, uniforms, hair and lunch boxes. Thankfully super-dad is also on call to move the kids along and help get them to school.
09:00 On this particular day, I am visiting the local Aboriginal health service. I first check in and assess the patient list for the day and have a quick catch-up with the healthcare workers with any issues that need my attention. Then a busy clinic usually involves juggling eye tests, dilated eye exams and selecting of glasses, and then reports to various providers including GPs, ophthalmologists and the Brien Holden Foundation, which are all part of this chronic healthcare team.
07:30 Running a portable clinic means you need to pre-plan your day to the tee and this includes using pre-filled forms so I know what is in store for the day and having equipment charged the day before. The first hour involves loading the car up with all the relevant kits for the day and also mental preparation for any difficult cases. Mobile clinics can range from a class of young children to seeing elderly patients in their homes. It may also involve visiting a satellite clinic location or seeing non-verbal individuals living with disability. Or it may be a combination of the above! From fun toys to disabilityfriendly portable equipment and a variety of frames for different tastes, you would be surprised how much you can fit in a couple of suitcases. Once the boot is packed it’s time to hit the road.
12:30 Time for a quick lunch and at this point I may try and squeeze in a little admin time, including answering patient enquiries. Then it’s time to hit the road again.
13:30 The afternoon is spent seeing patients in homes and we try to schedule them in the same localities where possible to make time on the road more efficient. Having the privilege to see patients in their homes allows me to better understand their situation and better manage their individual needs. I gain information such as their occupational set-up, lighting and the home care supports available to help form my treatment plan. Some home visits require thinking outside of the box and adapting the tests for the patient’s comfort and safety. If you asked me: can I test patients whose only position is lying down? Yes, absolutely.
However, a mobile optometry visit extends beyond an eye exam alone. Yes, it is a great feeling to be able to allow the patient to see ‘20/20’ for TV or reading, or help a patient resolve their doubled vision. It is even more rewarding knowing that improving vision means providing access to communication and a sense of belonging to the outside world. Good vision can mean maintaining mobility and independence. To my home-bound patients, this is everything. And seeing them get as excited as I do, is really nice.
17:00 Getting back to my home office means unpacking the car, getting new spectacle orders ready to be sent the next day and setting electronic equipment to charge.
Linda Nguyen is the owner and founder of Sydney-based Care Optometry — a family-run mobile optometrists’ practice started in early 2020 with a vision to make eye care more accessible and inclusive for everyone. Graduating with a Bachelor of Optometry from UNSW in 2006 and subsequently obtaining additional qualifications to become an endorsed Ophthalmic Medicines Prescriber, Linda’s practice includes disability and aged care, assisting children in schools and daycares, and those recovering from traumatic brain injuries in rehabilitation hospitals. A finalist in the Allied health — Individual Leadership category of the 2025 HESTA Excellence Awards, here’s a day in her life.
17:30 Time to get back to the family headspace and get dinner sorted. This is a great time for everyone to unpack their day. Some nights I am very fortunate that hubby has cooked a warm dinner ready and waiting for me in the oven, thanks again super-dad. The kids have hopefully finished their homework by now!
19:30 Time to squeeze in a little more family time including board games, helping with any homework or some television (if they are lucky!). Another extension of the ‘night shift’ is trying to get the kids in bed on time!
18:30 I call this the ‘night shift’ and every tired parent out there knows this hour. It’s kitchen pack-up time, lunch box and bag clean-outs, it’s the picking up of random toys from the floor and a night vacuum.
22:00 Then the quietest part of the night is where I can get into my creative headspace when I am conjuring up my next great idea, quietly cleaning or maybe both!
21:00 Unwinding time finally means my husband and I can catch up again and get up to speed with the news of the day.
A Day in the Life is a regular column opening the door into the life of a person working in their field of health care. If you would like to share a day in your working life, please write to: hh@wfmedia.com.au
Melanoma & Cancer Centre
The Paula Fox Melanoma and Cancer Centre at The Alfred in Melbourne was developed to bring cancer research, clinical trials, and patient treatment together in one facility. It provides patients with access to leading specialists and offers staff a wellplanned environment to deliver care.
In a healthcare setting, even small details can make a big difference to safety. That is why the project team chose products that support infection control and long-term reliability. GENTEC worked closely with the contractors to supply solutions for clinical areas where hygiene is essential.
Two key products were installed in the facility. The STERISAN® Clinical Basin with Rear Offset Waste was designed to help reduce splash and make cleaning easier, which supports daily hygiene practices. The GPURE® SMARTEC PLUS Electronic Tapware offers a hands-free operation and a durable stainless steel build, helping patients and staff maintain good handwashing routines while lowering the chance of cross-contamination. By combining practical design with infection control features, these products contribute to a safer and more efficient environment for both patients and healthcare staff.
The Paula Fox Melanoma and Cancer Centre shows how thoughtful choices in fixtures and fittings can support better healthcare outcomes. On the following page, you can learn more about the GENTEC solutions that continue to help hospitals and healthcare facilities provide safer spaces for care.
STEVEN BAXTER*
In hospitals, digital displays have the potential to create a more seamless, efficient and reassuring environment. Here are some potential patient and staff benefits.
Walking into a busy medical facility can be overwhelming. Whether it’s a GP waiting room, an ED or a specialist’s office, long queues, confusing layouts and unclear communication can add stress to an already challenging experience. And it’s not just patients who are affected; as any healthcare professional knows, poor patient experiences can lead to operational inefficiencies and a greater burden on staff.
Patient benefits
In
waiting spaces
Waiting in healthcare settings can be stressful and anxiety-inducing. Patients often feel frustrated by delays, particularly in EDs or specialist clinics, where wait times can be unpredictable. Digital signage helps mitigate this stress by serving as an effective distraction. Displays showing calming visuals, real-time queue updates, wellness content and entertainment can significantly enhance patient experience.
While healthcare facilities may not be able to control unforeseen delays or busy periods, digital signage can effectively improve the patient waiting experience. Research shows that integrating scenes of nature can reduce the perception of pain1 and reduce feelings of stress2. By incorporating videos and sounds of nature onto digital signage, healthcare settings can ensure they are creating a more peaceful and enjoyable waiting experience for patients.
In addition to entertainment and relaxation, digital signage can be used to display mental health tips, preventive care information and hospital policies, ensuring patients are engaged with valuable content while they wait. This helps create a more informative and reassuring environment before they even meet their healthcare provider.
In wayfinding
Navigating large hospitals or medical centres can be overwhelming for patients and visitors. Confusing layouts, a lack of clear signage and multiple departments can make wayfinding a significant challenge. Digital signage provides an effective solution by offering detailed wayfinding maps, directional signage and real-time updates on clinic locations and appointment schedules.
Internationally, facilities such as Boston’s Brigham and Women’s Hospital (BWH) have successfully begun using this technology.3 In
its use at BWH, the ability to provide up-todate, easily accessible information on digital displays was found to reduce missed or late appointments due to navigational issues and to improve the patient experience overall.
Wayfinding signage can be particularly beneficial for ageing patients and those with dementia by externalising spatial knowledge, decision-making and spatial planning, which can compensate for declining cognitive abilities.4 Digital signage, with its ability to be easily customised, streamlines this process of providing accessible information to patients with a variety of needs.
For retention of critical health information
When most patients picture doctors’ offices and hospitals, they likely think of walls adorned with posters and pamphlets containing important health information. If asked to recall what this information was about, however, there would be difficulty; the ‘picture superiority effect’5 suggests that people recall only 10% of the information they read but 65% of the visual content they see.
In one study, participants who were shown 500 words were able to recall 88% of the information, while participants who were shown images were able to recall 97% of what they saw.6 These findings suggest that digital signage, with its ability to seamlessly incorporate pictures and videos, would be a more effective communication method than traditional print options.
Clear communication of medical information is important for many reasons, from early diagnosis to encouraging healthy lifestyle habits or informing patients about their treatment options. While posters and pamphlets often fail to catch the eye, digital signage can be customised, personalised and adapted to capture patients’ attention.
In particular, research shows that animation helps to guide viewers’ attention, ensuring they focus on important details or instructions.7 This is attributed to animations requiring less cognitive load to understand than other visuals, such as static images. This research shows that by leveraging high-definition animations as part of your messaging, healthcare organisations can ensure that important health guidelines, medication instructions and public health alerts are more effective for patients.
How this could work in practice:
A pharmacy could use digital signage to educate customers on medication side effects or proper dosages.
A hospital waiting area could display reminders about the importance of flu vaccines during peak seasons.
A general practice could showcase lifestyle tips to prevent chronic illnesses such as diabetes and heart disease.
Unlike static posters, digital screens can be updated instantly, ensuring that information remains relevant and up to date. This is particularly beneficial in emergencies, where real-time alerts and crisis communication can be broadcast instantly across multiple screens.
For time-sensitive messages
One of the biggest advantages of digital signage is its flexibility. Healthcare organisations can schedule content based on the time of day, patient demographics or facility needs.
How this could work in practice:
Morning displays could show appointment reminders, medication adherence tips and general health awareness messages.
Afternoon displays could show lighthearted entertainment, wellness programming and service promotions.
Evening displays could show ED updates, overnight service information and staff shift changes for internal staff communication.
The ability to dynamically update and automate content delivery ensures that patients and staff always receive the right information at the right time. This can significantly improve patient engagement and provide a more seamless experience across different touchpoints within a medical facility.
Staff benefits
For internal communication
Beyond patient-facing benefits, digital signage is an invaluable tool for internal staff communication. Hospitals and medical centres are fast-paced environments where clear, timely communication is critical. Digital displays can be used to relay important updates, staff scheduling changes, emergency alerts and training reminders in real time.
How this could work in practice:
Staff break rooms could feature rotating content on hospital policies and wellness programs.
Nurses’ stations could display live updates on bed availability and patient flow.
Surgical departments could utilise digital boards to manage operating room schedules efficiently.
Internal operational inefficiencies can quickly lead to miscommunication, frustration and a lack of engagement among staff — three issues that no business, especially not a healthcare organisation, can afford to have. Digital signage helps bridge this gap by ensuring instantaneous and consistent messaging across teams.
The
message
The integration of digital signage in healthcare settings offers tangible benefits for patients, staff and entire organisations. As hospitals and clinics continue to embrace digital transformation, adopting intelligent, data-driven signage solutions will be key to creating more efficient and patient-friendly medical environments. In an industry where clear communication is essential, digital signage is a potential game changer.
1. Malenbaum S, Keefe FJ, Williams ACC, Ulrich R, Somers TJ. Pain in its environmental context: implications for
designing environments to enhance pain control. Pain 2008;134(3):241–244. doi: 10.1016/j.pain.2007.12.002
2. Kjellgren A, Buhrkall H. A comparison of the restorative effect of a natural environment with that of a simulated natural environment. J. Environ. Psychol 2010;30(4):464–472. doi: 10.1016/j.jenvp.2010.01.011
3. Center for Connected Medicine. Digital wayfinding becomes popular way to boost patient experience at health systems. UPMC Enterprises. July 14, 2020. Accessed 20 May, 2025. https://enterprises.upmc.com/ resources/insights/digital-wayfinding-becomes-popularway-to-boost-patient-experience-at-health-systems
4. Passini R, Pigot H, Rainville C, Tétreault MH. Wayfinding in a nursing home for advanced dementia of the Alzheimer’s type. Environ. Behav. 2000;32(5): 684–710. doi: 10.1177/00139160021972748
5. Pamplona F. The power of visuals. MedTech Intelligence February 8, 2023. Accessed 20 May, 2025. https:// medtechintelligence.com/column/the-power-of-visuals
6. Shepard RN. Recognition memory for words, sentences, and pictures. J. Verb. Learning Verb. Behav 1967;6(1):156–163. doi: 10.1016/S0022-5371(67)80067-7
7. Praveen CK, Srinivasan K. Psychological impact and influence of animation on viewer’s visual attention and cognition: a systematic literature review, open challenges, and future research directions. Comput. Math. Methods Med. 2022:1–29. doi: 10.1155/2022/8802542
*Steven Baxter is CEO and founder of Mandoe Media.
Is home washing contributing to antibiotic-resistant infection spread in hospitals?
Hospital-acquired infections are a major public health concern. This is in part because they frequently involve antibiotic-resistant bacteria. Many nurses and healthcare workers clean their uniforms at home in standard washing machines; however, according to a 2025 study out of the UK, washing machine biofilms may harbour potential pathogens and antibiotic resistance genes, meaning home washing of healthcare worker uniforms may be unknowingly contributing to the spread of antibiotic-resistant infections in hospitals.
With some studies having found that bacteria can be transmitted through clothing, the question that follows is whether these machines can sufficiently prevent the spread of dangerous microbes. To tackle this question, a research team — led by Katie Laird of the UK’s De Montfort University — examined six models of home washing machine to evaluate whether they were successfully decontaminating healthcare worker uniforms.
This evaluation involved washing contaminated fabric swatches in hot water, using a rapid or normal cycle. What was found is that half of the machines did not disinfect the clothing during a rapid cycle, while one-third failed to clean sufficiently during the standard cycle. Biofilms from inside 12 washing machines were also sampled, with DNA sequencing revealing the presence of potentially pathogenic bacteria and antibiotic resistance genes.
Pre- and post-domestic laundering of bacteria contaminated textiles. Image credit: Dr Caroline Cayrou, CC-BY 4.0 (https://creativecommons.org/licenses/by/4.0/)
Also shown through investigation was that bacteria can develop resistance to domestic detergent, something that increases bacterial resistance to certain antibiotics. What is suggested by these findings is that many home washing machines may be insufficient for decontaminating healthcare worker uniforms, and in fact may be contributing to the spread of hospitalacquired infections and antibiotic resistance. As such, the researchers argue that laundering guidelines given to healthcare workers should be revised.
Such revision, the researchers say, should aim to ensure that home washing machines are cleaned effectively or, alternatively, that — to improve patient safety and control the spread
of antibiotic-resistant pathogens — healthcare facilities should use onsite industrial machines to launder uniforms. “Our research shows that domestic washing machines often fail to disinfect textiles, allowing antibiotic-resistant bacteria to survive,” the researchers said.
“If we’re serious about transmission of infectious disease via textiles and tackling antimicrobial resistance, we must rethink how we launder what our healthcare workers wear.”
The study, ‘Domestic laundering of healthcare textiles: disinfection efficacy and risks of antibiotic resistance transmission’, has been published open access in PLOS One and you can read it at doi.org/10.1371/journal. pone.0321467.
Featured Products
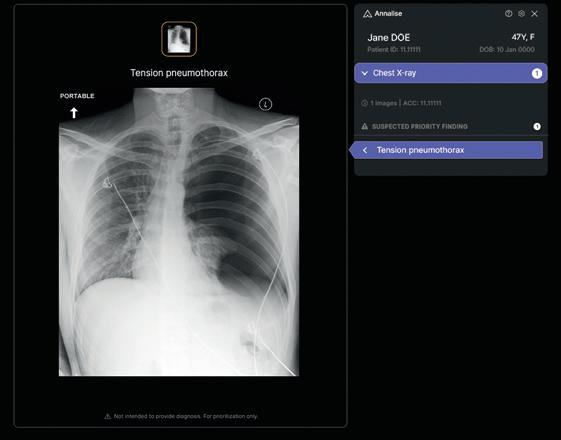
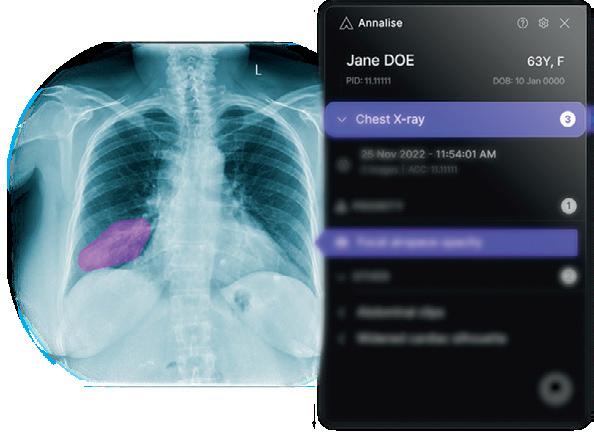
AI chest X-ray
The Harrison.ai Annalise Enterprise CXR module is intended to assist clinicians with the interpretation of radiological imaging studies.
It is designed to empower busy clinicians to do their best work, especially when they’re under pressure, detecting up to 124 findings on chest X-rays. The technology analyses up to three images per study, including frontal and lateral images.
Its features include a customisable user interface that is designed to integrate seamlessly into PACS and RIS, and to be used comfortably in under-10 studies. A confidence bar displays the likelihood of the finding and uncertainty of the AI model, assisting clinicians to interpret with confidence.
It is also available with an automated draft reporting feature, Annalise Reporting, which is designed to make radiology reporting quick and easy, creating complete, editable draft reports ready for radiologists to review and sign off.
Harrison.ai harrison.ai
ai174242756624_Nursing Innovations AD.pdf 1 20/03/2025 10:39:26 AM
ASCVD QI toolkit and CPD activities
LipidPlan in a box is intended to support GPs and primary care teams in undertaking quality improvement (QI) activities to improve the quality of care for their patients with atherosclerotic cardiovascular disease (ASCVD). Developed with the guidance of a multidisciplinary steering committee of primary care experts and sponsored by Novartis Australia, it is designed to be easy to access online, and is available in two formats.
First, a QI toolkit — an interactive PDF with tools and resources to help implement Plan-Do-StudyAct (PDSA) cycles within practice. The interactive PDF toolkit is designed to equip primary care providers with the tools and resources to facilitate better low-density lipoprotein cholesterol (LDL-C) management QI activities by engaging public health networks to prioritise local needs, assembling an implementation team, implementing PDSA cycles within practice and adopting the most effective strategies across the clinic. This is not a Royal Australian College of General Practitioners (RACGP)-approved continuing professional development (CPD) activity.
Second, online RACGP-accredited CPD activities — a series of seven standalone RACGP-accredited mini audits to implement within practice. (These are RACGP-approved CPD activities under the RACGP CPD Program and comprise three activity types to provide a total of 8.5–10.5 hours of CPD each).
European researchers are calling for a reassessment of healthcare guidelines after revealing that an ICU disinfectant procedure used in certain countries may increase antibioticresistant infection risk.
‘Universal decolonisation’ is a preventive procedure applied to patients upon admission to intensive care in which the entire body is disinfected with chlorhexidine — a commonly used antiseptic also employed to sanitise hospital surfaces and medical devices — and an additional nasal treatment is administered with another disinfectant, mupirocin. The procedure is at the centre of a study published in The Lancet Microbe
“Our research highlights the unintended consequences of universal decolonisation in a global context where antibiotic resistance is an increasing threat,” said Marco Oggioni, one of the authors of the study and a professor at the Department of Pharmacy and Biotechnology at the University of Bologna.
“Coordinated efforts to prevent antibioticresistant infections are crucial, but they must not prevent us from critically re-evaluating the tools we use to achieve these goals.”
Introduced in the 1990s, universal decolonisation has proven effective in curbing the spread of methicillin-resistant Staphylococcus aureus (MRSA, a bacterium resistant to certain antibiotics that can cause severe infections), reducing MRSA infection rates from 30–40% to below 5% in many
countries — Scotland included, which is where this study was conducted.
“Currently, UK healthcare facilities take different approaches: some hospitals apply universal decolonisation to all patients, while others take a more targeted approach, decolonising only those who test positive for MRSA,” Oggioni explained. “As a result, hospitals adopting universal decolonisation use significantly larger volumes of disinfectants such as chlorhexidine and mupirocin.”
In the study, researchers focused on two Scottish hospitals using these different approaches, comparing bacterial infection levels and antibiotic resistance rates among ICU patients over a 13-year period. They found higher rates of infection caused by the superbug methicillin-resistant Staphylococcus epidermidis (MRSE) in the hospital practising universal decolonisation; MRSE being less well-known than MRSA, but increasingly common and resistant to several types of antibiotics.
“Our findings show that the excessive use of disinfectants in universal decolonisation may not improve infection control, and instead leads to a rise in MRSE infections,” said
Professor Karolin Hijazi from the University of Aberdeen, who coordinated the study. “In intensive care settings where the risk of MRSA infection is low, indiscriminate use of decolonisation procedures may not only be ineffective but also potentially harmful.”
According to Oggioni, this applies to regions where MRSA prevalence is low, like Scotland. “In Italy, however, MRSA infection risk remains high despite a downward trend, which means both targeted and universal decolonisation are still necessary,” Oggioni said. “We’ll need to reduce MRSA prevalence in Italy before we can reassess the risks and benefits of these intervention procedures.”
A reassessment of current practices in light of the evolving epidemiological landscape is therefore being called for by the study’s researchers, who believe new standardised guidelines are needed to identify the most effective decolonisation treatments — weighing both the benefits in infection control and the potential impact on antibiotic resistance.
‘Universal versus targeted chlorhexidine and mupirocin decolonisation and clinical and molecular epidemiology of Staphylococcus epidermidis bloodstream infections in patients in intensive care in Scotland, UK: a controlled time-series and longitudinal genotypic study’, has been published open access in The Lancet Microbe and you can read it at doi. org/10.1016/j.lanmic.2025.101118.
around lung disease and cancer Stigma must go
The stigma for people diagnosed and living with lung disease or cancer is a heavy physical and emotional burden. It can leave people feeling isolated, ashamed and — worse still — be the reason they hesitate or don’t seek much-needed help.
Data from Lung Foundation Australia’s Lived Experience Survey showed the debilitating effect stigma has on patients. The survey, with responses from 1034 people living with a lung condition and 149 carers, alarmingly showed the levels of stigma had increased since 2020, including the stigma patients felt from health practitioners.
It simply isn’t good enough. The stigma around lung disease and cancer must go.
Alongside Lung Foundation Australia, health professionals must play an active role in helping to remove stigma and create more supportive environments for those living with lung disease.
Language matters
Research presented at the Australian Lung Cancer Conference 2025 by Dr Shiho Rose and her team showed that stigmatising language — including blame-focused terms and moralising narratives — remains prevalent in media coverage. But we know this extends into treatment rooms, doctors’ surgeries and everyday interactions when a patient is diagnosed with a lung disease. The language we use when talking about lung disease matters.
Better communication, education and advocacy are essential to make sure stigma is removed and greater empathy is given
to patients. Lung disease is complex. Research is showing us that the first 1000 days of someone’s life can set the course of their lung health for life. Exposure to environmental conditions in early life can increase chronic diseases risk, regardless of whether a person smokes or not.
Likewise, we need to make a dedicated effort to highlight the advancements in treatment and research that are contributing to the growing number of people who live longer and better. We should spend more time focusing on the positive and less time dwelling on the negative.
Cultivating empathy and understanding
We need to acknowledge the experiences of patients without judgment. Too often people diagnosed with or living with lung disease are immediately blamed for causing it themselves, rather than offered concern. It isn’t good enough.
Empower your patients in their care decisions and encourage them to have agency in their health. Understand that
charities like Lung Foundation Australia are your allies in supporting your patients and able to offer them connection, support and community.
Connection and community
Connection and community are paramount when living with a lung disease. Patients need access to health professionals who specialise in lung disease and can offer genuine and practical advice on how to cope with the emotional challenges of their diagnosis.
Support from specialist lung cancer nurses, for example, has proven impacts, including:
• reduced avoidable ED presentation
• improved cancer service alignment with optimal lung cancer care
• improved value and quality of patientcentred lung cancer care
• improved access to lung cancer treatment and timeliness of treatment
• increased receipt of anticancer therapy
• strengthened patient capacity to self-manage
• improved outcomes for patients and carers affected by lung cancer (cancer outcomes, quality of life and wellbeing).
Why is it not yet standard practice that patients with lung disease or cancer are given the same opportunities for support, quality of life and survival that people with other cancers have?
Stigma breeds inequality
The stigma around lung disease and cancer has held back research investment and community empathy for too long, resulting in greater inequality in treatment, progress and care.
Regardless of how a patient’s diagnosis came about, they still deserve the gold
standard of care that patients with breast, bowel or prostate cancer, or those in city locations, receive. Cancer is cancer, and all Australians deserve to have access to a full range of treatments.
Lung Foundation Australia believes the soon-to-launched national lung health screening program will transform the way lung health and disease are viewed in the community. We want the service to normalise having your two-yearly lung screening just as much as people know to schedule their mammogram after turning 40 or making sure you “slip, slop, slap, seek and slide” before heading outdoors.
We can’t advocate on behalf of the lung cancer community alone. We need the help of health practitioners nationally. Be the voice that advocates for policy changes that promote lung health screening and research, share knowledge and resources to ensure that patients are supported preand post-diagnosis, and speak out against stigma you see in action.
Together we can make the first question someone is asked after sharing their lung cancer diagnosis, “I’m sorry you’ve been
given a cancer diagnosis. Is there anything I can do to help?” rather than “Oh, do you smoke?”
Let’s work together to break down the walls of stigma and empower individuals to live better, regardless of their diagnosis.
In July 2025, the National Lung Cancer Screening Program launched. Learn more at www.lungfoundation.com.au/advocacy/ national-lung-cancer-screening-program.
Integrated securement dressing
The SorbaView SHIELD multi-layer dressing and catheter securement system is designed to provide a comprehensive vascular access management solution to manage dwell time, infection rates and associated costs.
Designed to provide built-in, breathable stabilisation with a secure hold, it features soft fabric to conform comfortably with skin movement, deep notches to help seal tubing in place, and tabs and perforations to increase versatility and facilitate easy removal.
With a large window for thorough assessment of insertion site, it also has contoured edges to help prevent dressing from peeling up and SHIELD technology with a stabilisation device, designed to prevent tugging forces from reaching the catheter.
Other features include a reinforced ‘collar’, to keep hubs locked firmly in place; a viral and bacterial barrier film; an absorbent pad that wicks moisture away from the insertion site; and, available on certain designs, secondary closure pieces that enhance stability.
Medline International Two Australia Pty Ltd www.medline.com.au
Mark Brooke, Chief Executive Officer of Lung Foundation Australia
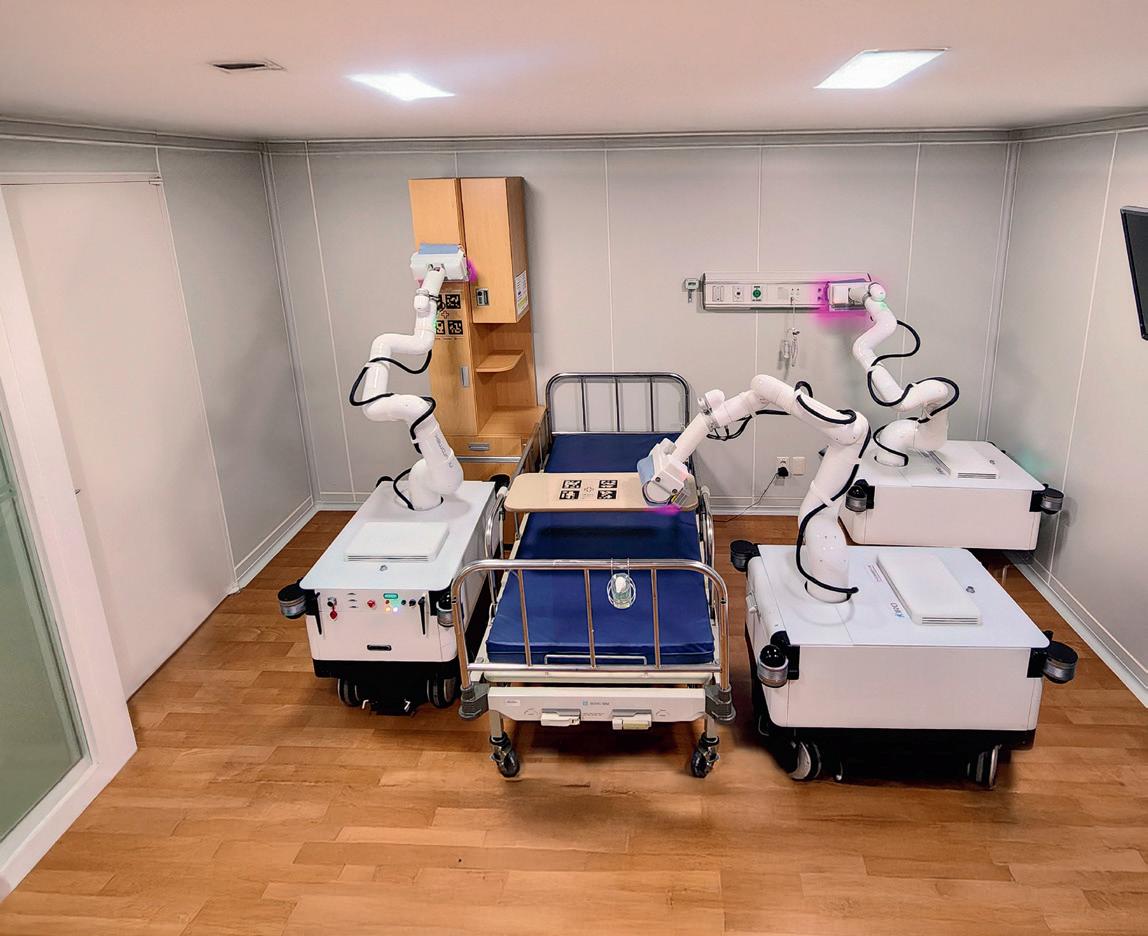
Robot automates hospital disinfection processes
Thorough disinfection, particularly within hospital environments, was shown to be critical during the COVID-19 pandemic, which also highlighted concerns surrounding labour shortages due to physical fatigue and risk of exposure to pathogens. Additionally, as human performance can be inconsistent and individuals’ compliance with manually conducted disinfection tasks tends to vary, South Korean researchers from POSTECH (Pohang University of Science and Technology) turned to robot technology; seeking to better existing solutions — such as UV-C robots and hydrogen peroxide vapour systems — that have limitations in completely removing contaminants hidden in obscured or hard-to-reach areas.
What they came up with is an ‘intelligent autonomous wiping and UV-C disinfection robot’ capable of both navigating hospital environments and performing disinfection tasks — its dual disinfection system being a key feature. This dual system works by, first, utilising a robotic manipulator to physically wipe surfaces and remove contaminants, and second, employing UV-C irradiation to disinfect hard-to-reach corners and narrow spaces. To minimise operational failures, precision control algorithms are used. While to ensure sustained disinfection operations, a self-sanitising station and wireless charging system has been integrated.
CASE STUDY
Real-world testing of the robot’s performance was undertaken at Pohang St. Mary’s Hospital, with bacterial culture experiments conducted by the research team — to confirm the effectiveness of disinfection, with repeated autonomous operations carried out to verify its long-term usability in clinical settings. The automation of
time-consuming and repetitive disinfection tasks is a key advantage of the robot, as is its ability — unlike variability in human performance — to disinfect with consistent precision, significantly reducing the risk of infection within the hospital.
POSTECH
www.postech.ac.kr
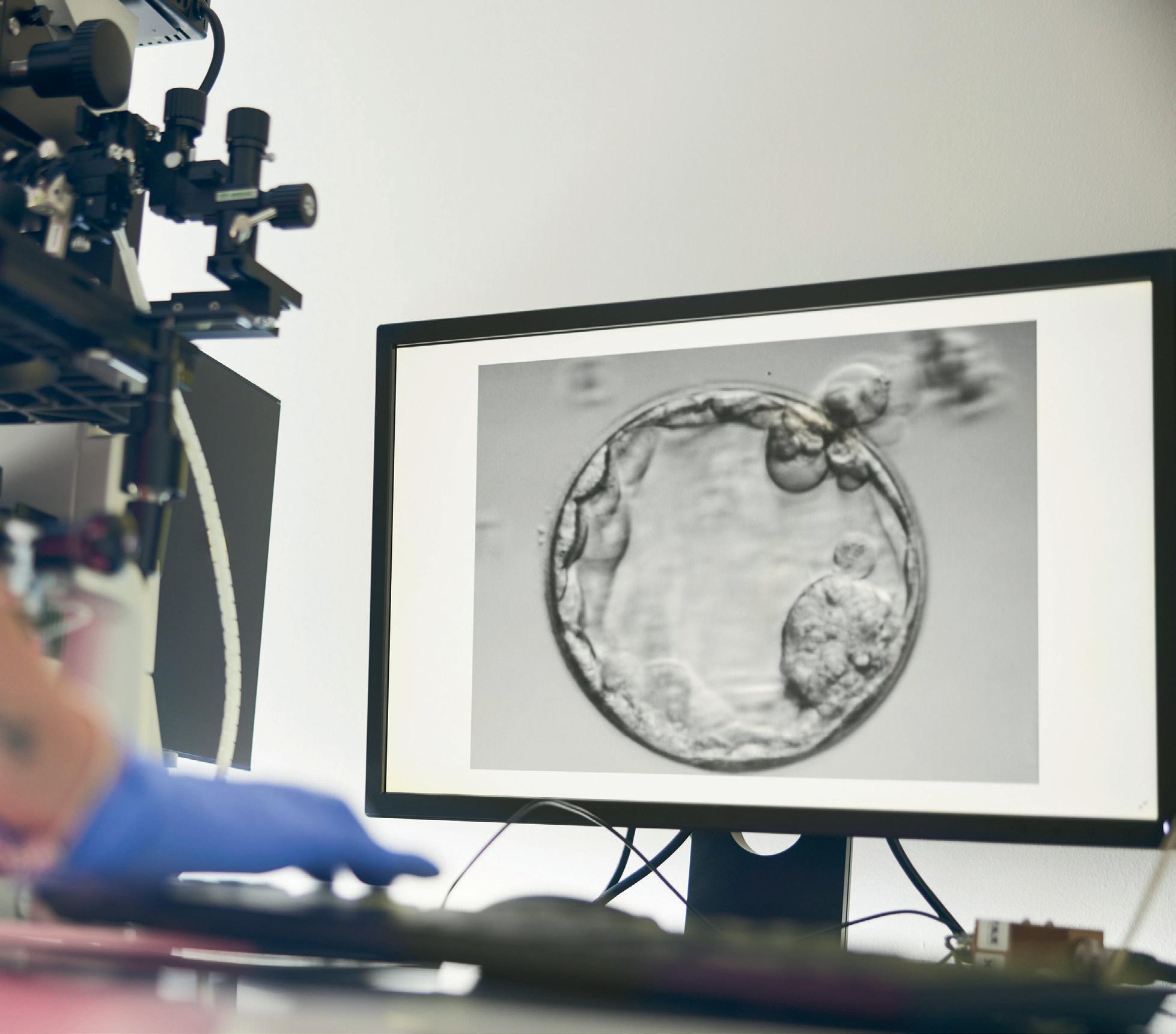
Improving success rates: lactic acid in IVF
PROFESSOR DAVID GARDNER AM*
The co-author of research published this year in Biomolecules explains how the metabolism of the embryo could be a major component determining the success of implantation in IVF.
The process of embryo implantation, a key process in the establishment of a successful pregnancy, is complex. With approximately one in six couples in Australia facing infertility, many turn to IVF as a pathway to parenthood. While IVF success rates have significantly improved over the last 45 years — since the birth of the first test-tube baby — and around 5% of Australian children are born via IVF, more than half of couples attempting IVF are unable to establish a pregnancy. Our recent research1 suggests that the metabolism of the embryo could be a major component determining the success of implantation.
Invasion of the uterus by the embryo
Dr Kathryn Gurner — a clinical research embryologist and my co-author on this research — and I have been investigating how the unique metabolic functions of the late-stage preimplantation embryo (known as the blastocyst) can control events key in the uterus to promote implantation.
Implantation is a curious biological phenomenon as it represents the invasion of the mother’s uterus by the blastocyst stage embryo, an entity which is not considered as ‘self’ by the woman but rather is recognised as a foreign body. This raises fundamental questions like “how does the blastocyst
prevent immune rejection by the woman” and “how does it then go on to create its own blood supply?” — a phenomenon referred to as angiogenesis.
From biochemistry to the blastocyst
While many researchers around the world have considered the process of implantation from the perspective of uterine signalling, Gurner and I have instead considered the potential role of the blastocyst’s unique metabolism; that being its capacity to form lactic acid even when given ample oxygen to oxidise it, in this intricate process.
This unusual metabolic characteristic is referred to as aerobic glycolysis and is a metabolic trait also seen in invasive tumours. By examining the mechanisms employed by cancer cells, we were able to explore whether the blastocyst utilises similar processes for implantation — with findings suggesting that this indeed seems to be the case.
Lactic
acid — more than a by-product of the gym
Often associated with the burn of an intense workout, lactic acid is widely regarded as a byproduct of anaerobic metabolism, occurring when oxygen is in short supply — such as in muscles during a sprint or heavy exercise.
However, in the case of the embryo, it transpires that lactic acid produced by the blastocyst is used to deliberately create a specific microenvironment around the embryo characterised by low pH and high levels of lactate. Essentially, the blastocyst forms a small acidic cloud around itself, which facilitates a number of crucial events in the early stages of implantation.
The initiation of implantation by lactic acid
In the initial phases, this acidic environment helps transition the uterus into a receptive state for implantation, a process known as
endometrial receptivity. By influencing the function and expression of key genes within endometrial cells, lactic acid promotes changes that allow the uterine lining to become more hospitable for the attaching embryo.
Lactic acid also facilitates the blastocyst’s invasion of the uterus by driving alterations in gene and protein expression that encourage its penetration into the endometrial tissue. This invasion is crucial for embedding the embryo deeply within the uterine lining, ensuring proper nutrient exchange and sustained development.
Additionally, as endothelial cells — progenitors of blood vessels — and various immune cells within the uterine environment absorb lactate produced from the blastocyst, their function/ behaviours adapt to promote implantation. In endothelial cells, this leads to an increase in the formation of new blood vessels, ensuring the embryo secures a consistent oxygen and nutrient supply.
Meanwhile, lactate uptake by immune cells influences the maternal immune response by dampening immune activator cells and increasing molecules that suppress immune activity. This adjustment prevents the embryo from being recognised as a foreign entity, facilitating successful implantation.
In conclusion
These discoveries highlight the intricate role of lactic acid in shaping the uterine environment during the earliest phases of pregnancy. While this research provides exciting insights, there is still much to uncover about lactate signalling in the uterus — and consequently this will help create ways in which we can pretreat patients to enhance uterine receptivity.
1. Gurner KH, Gardner DK. Blastocyst-derived lactate as a key facilitator of implantation. Biomolecules. 2025;15(1):100. doi: 10.3390/biom15010100
*Professor David Gardner AM is Scientific Director of Melbourne IVF and Director of ART, Scientific Innovation & Research at Virtus Health.
In Conversation
with Dr Kathryn Zeitz
AMY SARCEVIC*
As she approaches one year in the role, Hospital + Healthcare speaks with Australian College of Nursing CEO Dr Kathryn Zeitz to learn where we’re at — and where we need to go — with nurses’ scope of practice.
Dr Kathryn Zeitz FACN is about to mark her first anniversary as CEO of the Australian College of Nursing, and if she could summarise her year in one word, it might be ‘eventful’.
With ambitions to increase the scope of nursing and midwifery practice, Zeitz — who is also an Adjunct Professor — has been tirelessly advocating for reform.
And while funding and regulatory models are still holding these sectors back, there is growing recognition that nurses and midwives are currently underutilised.
“Nurses make up more than half the healthcare workforce and have enormous untapped potential,” she said. “We are competent at supporting preventative care and the management of complex comorbidities.
“We’re also the most geographically distributed. You’ll find us in the most remote communities, where you won’t find other health service providers.
“So, nurses are a critical part of Australia’s healthcare solution.”
Relieving the burden
Zeitz says advanced nurses can deliver preventative and post-diagnostic care “readily and cost-effectively”, complementing GPs, specialists and other members of a multidisciplinary care team. She says this is an asset to an under-resourced system.
“I come from a world of hospital ramping and I don’t think there’s any jurisdiction that isn’t being touched by this. Almost everywhere you look it’s often a six week wait to see your GP; a month to access allied health.
“We have this tsunami of chronic disease coming and the cost of delivering care in acute settings is not sustainable. We’re on track to have a 70,000 shortfall in nurses by 2035.
“We need to do something different,” she said.
Reconceptualising nursing
For Zeitz, something different means a rethink in how nurses are conceptualised and a shift in policy to reflect that.
We have this tsunami of chronic disease coming and the cost of delivering care in acute settings is not sustainable. We’re on track to have a 70,000 shortfall in nurses by 2035. We need to do something different.
She believes discrepancies in local regulation are restricting growth in the nursing profession.
“Say I’m a remote area nurse working in Outback Australia. There is a whole lot of work that I can do. I can put in intravenous lines; I can do full comprehensive assessments; I can provide complex wound care.
“But if I were to move interstate and work in a major metropolitan setting, I might not be allowed to do that. There is a lack of consistency between jurisdictions and care settings on the type of work nurses can do.”
Overshadowing this is what Zeitz calls an outdated funding model that “severely limits nurses’ scope of practice”.
In the current system, acute hospitals receive activity-based funding from their state, while most primary care services are funded mainly by the Commonwealth’s Medicare Benefits Schedule (MBS).
“The majority of that primary care funding is going to GPs or the medical practice and there are very few opportunities for nurses who work in the primary setting to establish independent services and relieve the pressure on the system,” Zeitz said.
Lack of incentive
Kylie is a registered nurse, who works in a GP clinic — and is a case in point.
She is a credential diabetes educator and is undertaking study to become a nurse practitioner. She manages complex chronic conditions, provides wound care and supports preventative health. She is often delivering 30-minute consultations for individual patients.
Despite her expertise, Medicare pays just $14.00 for one of the few MBS items a registered nurse can access — chronic disease support.
“It doesn’t matter how long Kylie spends on those services, $14.00 will be the limit,” Zeitz said.
“For wound care, the doctor just needs to pop in, say hello to the patient and check how they are going for that encounter to be billable through the practice. Meanwhile, Kylie delivers all the actual care.
“And, yes, she’s getting a salary, but there is no financial incentive for her to undertake independent practice and do that work.
“This undervalues Kylie’s work in easing healthcare pressures; and it wastes doctors’ time.”
A push for blended funding
A blended funding model that is less heavily weighted towards MBS funding could counter this issue and enable Kylie to work at her full scope of practice.
Such models — which include capitation, bundled and performance-based payments — have already been recommended in independent reviews, and ACN is now advocating for their enactment.
“This would give nurses a funding stream to work independently, particularly in chronic disease management,” Zeitz said.
“We see this as the best way forward and a ticket to so many of the outcomes we are looking to achieve in health.
“We are deeply committed to seeing this become a reality.”
In the driving seat
While Zeitz may not have yet reached the finish line, she is pleased to now be driving a vehicle that will help her get there.
“After working many years in public health, it was frustrating not being able to turn service delivery around to benefit our community. Taking the helm of ACN and having that opportunity is a real honour,” she concluded.
*Amy Sarcevic is a freelance science and technical writer who regularly writes for Hospital + Healthcare. She has an academic background in psychology.
Healthy heights vertical hospitals on the rise
BRUCE CROOK*
If you’ve ever received care on the 30th floor of a hospital in Houston, Hong Kong or London, you know the experience is both unique and transformative. Yet, as a healthcare architect explains, these towering, 140-metre-plus healthcare facilities are no longer anomalies — they’re becoming a global standard.
Throughout my international career as a healthcare architect, I’ve had the privilege of designing numerous high-rise hospitals. My work has taken me across continents — from Singapore and Southeast Asia to Northern Europe and North America — where I’ve observed firsthand the burgeoning trend of vertical healthcare design.
Urban centres worldwide are grappling with challenges like limited land availability, traffic congestion and the need for increased public and pedestrian spaces. Vertical, high-density developments offer a compelling solution,
not just in commercial and residential sectors but increasingly in education, research and healthcare facilities.
Hospitals are embracing verticality to enhance clinical effectiveness, streamline support services and, most importantly, improve patient outcomes and accessibility. This shift isn’t entirely new; the trend traces back to structures like Guy’s Hospital in London, which held the title of the world’s tallest hospital from 1974 until 1990. It was later surpassed by the O’Quinn Medical Tower in Houston and then by Hong Kong’s Li Shu Pui Building.
So, what’s driving this ascent in hospital design? Several advantages come to mind:
• Efficient land use — vertical designs make optimal use of limited urban land, allowing for a greater concentration of clinical disciplines, educational and research facilities, and support services within a smaller footprint.
• Enhanced patient care — by grouping related services on the same floors, vertical hospitals reduce the need for patients to move between departments, streamlining care and improving the patient experience.
• Staff efficiency — vertical layouts minimise the time staff spend moving between floors or departments, enhancing response times and overall patient care.
• Optimised workflows — these hospitals facilitate logical workflows, minimising unnecessary movement and maximising operational efficiency. This is particularly beneficial when integrating automated logistics-support robots and vertical transport systems.
• Healing environments — upper-floor patient rooms offer expansive views and increased natural light, creating a more pleasant environment for both patients and staff.
• Integrated green spaces — incorporating rooftop gardens and stacked balconies supports recovery and provides respite areas for staff, aligning with research that highlights the positive impact of biophilic design on wellbeing and recovery rates.
• Improved accessibility — strategically placed elevators, ramps and staircases enhance movement throughout the facility for both patients and staff.
The rise of vertical hospitals represents a significant evolution in healthcare design, addressing the pressing needs of modern urban environments while prioritising patient care and staff efficiency. As cities continue to grow and space becomes increasingly scarce, I believe we’ll see more healthcare facilities reaching for the skies.
The Tower Wing (centre) of Guy’s Hospital in London, designed by Watkins Gray for the NHS, is one of the world’s tallest healthcare buildings, despite being overshadowed by its 309m+ tall neighbour, The Shard — the city’s highest tower.