MENTAL HEALTH IN UKRAINE: DISPLACEMENT, VULNERABILITIES AND SUPPORT
THEMATIC BRIEF
NOVEMBER 2024
TABLE OF CONTENTS
SYMPTOMS OF DEPRESSION AND INDIVIDUAL RISK FACTORS
MENTAL HEALTH AND DISPLACEMENT
SOCIO-ECONOMIC VULNERABILITIES
SUPPORT NEEDS
RECOMMENDATIONS FROM IOM MHPSS
UKRAINE PROGRAMMING
INTRODUCTION
As of October 2024, an estimated 3.6 million people remain internally displaced in Ukraine, while 4.3 million previously displaced people have returned to their primary place of residence (IOM GPS R18). The war continues to have a significant impact on the country’s economy and on people’s livelihoods and living standards. Ukrainians often struggle to meet their basic needs, including food (reported as a need by 22% of respondents), with more than half (52%) of the population resorting to crisis or emergency livelihoods-based coping strategies that may significantly affect their resilience and well-being in the long term. IDPs, in particular, face insecure housing tenure, higher levels of unemployment, and are more likely to rely upon social assistance for a proportion of their household income. On the other hand, almost a third of returnees interviewed for General Population Survey (GPS) reported struggling to access income earning opportunities (31%), and 22 per cent reported limited access to adequate education, indicating the difficulties encountered to rebuild their lives
BRIEF METHODOLOGY
The data presented in this report was commissioned by the International Organization for Migration (IOM) and collected by Multicultural Insights as part of Round 17 of the General Population Survey (GPS). Data was collected through phone-based interviews, with respondents identified through a nationally representative screening survey of 40,000 individuals. Round 17 data includes interviews with 1,488 IDPs, 1,188 returnees, and 1,800 non-displaced individuals carried out between 13 July and 12 August 2023. IDPs are defined as people who left their homes or are staying outside their habitual place of residence due to the full-scale invasion in February 2022, regardless of whether they hold registered IDP status. Returnees are defined as people who returned to their habitual residence after a significant period of displacement (minimum of two weeks since February 2022). All remaining individuals are considered non-displaced. All interviews were conducted using a random-digit-dial (RDD) and computer-assisted telephone interviewing (CATI) approach, generating results with an overall margin of error of 1.35% [CL 95%]. The survey included all of Ukraine, excluding the Crimean Peninsula and the areas of Donetska, Luhanska, Khersonska, and Zaporizka Oblasts under the temporary military control of the Russian Federation where phone coverage by Ukrainian operators is not available. For further details, please refer to the Methodological Note
The Patient Health Questionnaire-2 (PHQ-2) was used to identify symptoms of depression among respondents. The PHQ-2 consists of two questions assessing symptoms of depression:
1. Over the last two weeks, how often have you experienced little interest or pleasure in doing things?
KEY FINDINGS
• Thirty-eight per cent of respondents are at high risk of depression (PHQ-2 score of 3+). These symptoms were more commonly reported by women (42%) and persons with self-reported disabilities (45%).
• The reported experience of symptoms of depression was highest among IDPs (50%), followed by returnees (42%), and the nondisplaced (35%). The risk of depression was more common in individuals considering to move from their current location, in the short or long term.
• Unemployed individuals appeared to be at higher risk of depression (54%). Household-level vulnerabilities, such as the use of severe coping strategies and the presence of persons with chronic illnesses, were also correlated with higher rates of those reporting symptoms of depression.
• One third of individuals who reported being at high risk of depression mentioned the need for psychological support. Individuals who reported symptoms of depression also identified a lack of access to basic goods and services at higher proportions than individuals without symptoms of depression.
in their areas of origin, while the entire population is impacted by the broader socio-economic consequences of the war (IOM GPS R17).
The protracted nature of the conflict and the uncertainty about the future it creates, together with unfavorable economic conditions, are expected to have a significant and lasting impact on the mental health of the Ukrainian population. Against this backdrop, this brief provides an overview of the population groups most at risk of experiencing symptoms of depression, examining factors such as gender, age, and disability. It also explores the relationship between mental health and displacement status, as well as individual and household-level socioeconomic characteristics, and outlines support needs. Finally, the brief presents recommendations for mental health and psychosocial support (MHPSS) programming across Ukraine, aiming to inform targeted assistance to address the pressing mental health challenges facing vulnerable populations affected by conflict.
2. Over the last two weeks, how often have you felt down, depressed or hopeless?
(Answer options: Not at all, Several days, More than half the days, Nearly every day, Do not know)
The responses to these questions are combined to yield a final score. The final PHQ-2 score can range from 0 to 6, with a score of 3 or greater considered likely to indicate a higher risk of depressive disorder. In the following, both the final PHQ-2 scores and the results obtained from each of the two questions individually are presented. For ease of understanding, respondents found to have a PHQ-2 score of 3 or higher are categorised as reporting ‘symptoms of depression’. The results of the PHQ-2 analysis may give an indication of the possible prevalence of depressive disorder in the population and, more importantly, possible differences between population groups, but do not represent precise estimates for which further screening would be required.
Limitations: The exact proportion of the excluded populations is unknown. Those currently residing outside the territory of Ukraine were not interviewed, following active exclusion. Minors were also not assessed. The sample frame is limited to adults that use mobile phones. It is unknown if all phone networks were fully functional across the entire territory of Ukraine for the entire period of the survey; therefore, some respondents may have had a higher probability of receiving calls than others. Residents of areas with a high level of civilian infrastructure damage may have a lower representation among the sample.
SYMPTOMS OF DEPRESSION AND INDIVIDUAL RISK FACTORS
KEY FINDING 1: Symptoms of depression were reported by a significant proportion of respondents, especially by women and persons with disabilities.
Two in five respondents reported experiencing symptoms of depression (PHQ-2 score of 3+) during the two weeks prior to data collection. Gender and self-reported disability were the individual characteristics associated with the most important differences in the rate of reporting symptoms of
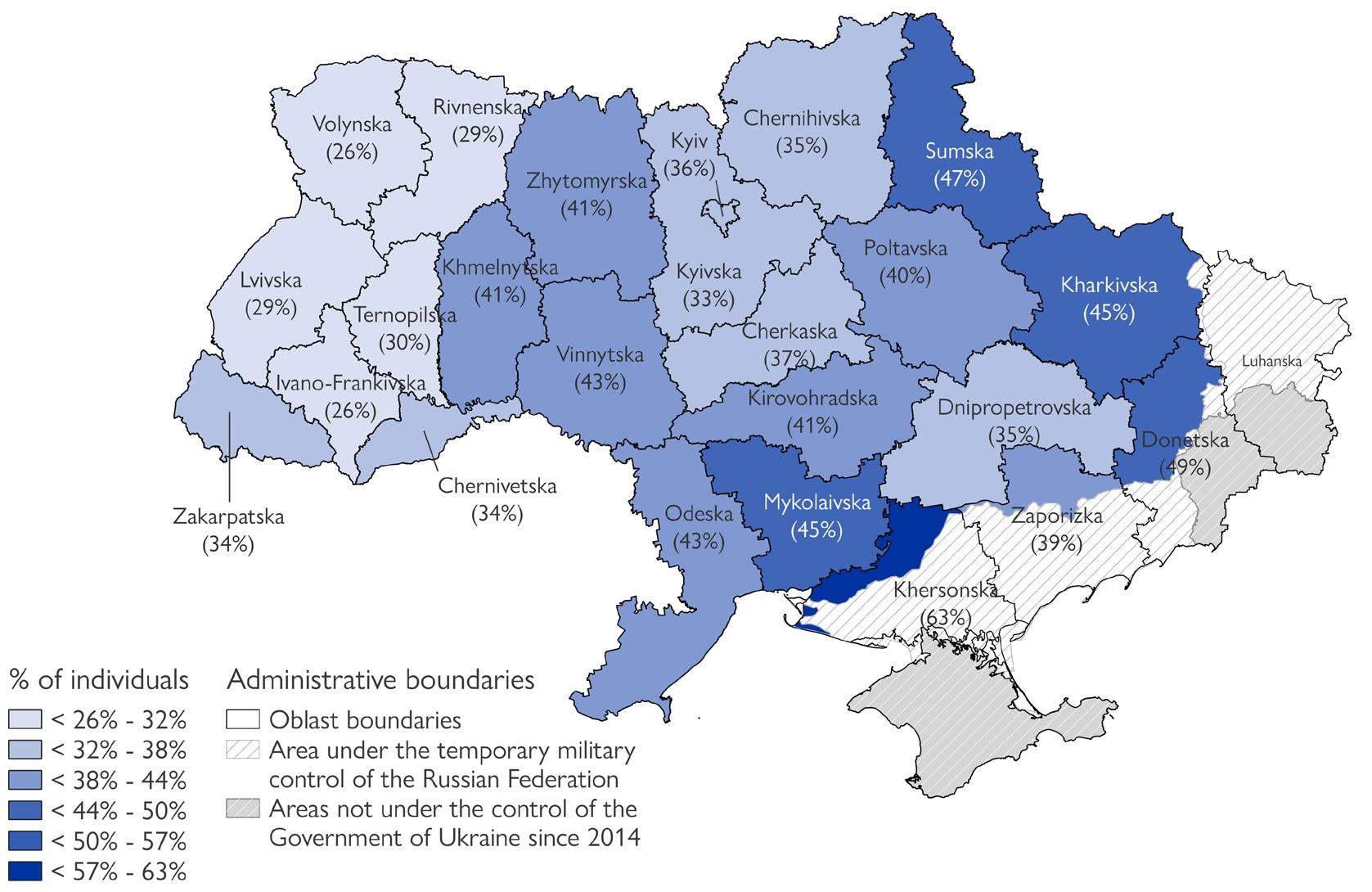
depression. Results varied across the country, with the lowest proportion of respondents reporting symptoms of depression found in the Western oblasts1, and the highest proportion found in the Southern oblasts2, as well as in frontline oblasts.
38%
of all respondents may be at high risk of depression (PHQ-2 score of 3+)
45% of respondents with self-reported disabilities mentioned having experienced symptoms of depression (PHQ-2 score of 3+), compared to 37 per cent of individuals without self-reported disabilities.
This was primarily driven by the difference between the proportion of persons with self-reported disabilities (44%) and without selfreported disabilities (34%) mentioning that they had felt down, depressed or hopeless more than half the days or nearly every day during the previous two weeks.
29%
of respondents reported having experienced little interest or pleasure in doing things more than half of the time or nearly always in the two weeks prior to data collection
of respondents reported having felt down, depressed or hopeless more than half of the time or nearly always in the two weeks prior to data collection 35%
DIFFERENCES BY GENDER
Women were significantly more likely to report having experienced symptoms of depression than men. While this may indicate that men are more reluctant to discuss mental health issues due to traditional models of masculinity, it reflects a global pattern of higher prevalence of depression among women.3 Age was also associated with different proportions of individuals reporting symptoms of depression, with the highest proportion found among respondents aged 46-59 (18%). The intersection of gender and age resulted in older women (46+) being the group most likely to report having experienced symptoms of depression.
3 See e.g. WHO, Depression Fact Sheet, March 2023, available here
1: % of individuals with a PHQ-2 score of 3+, by respondent gender and age
Map 1: % of individuals reporting symptoms of depression (PHQ-2 score of 3+), by oblast
Figure
MENTAL HEALTH AND DISPLACEMENT
KEY FINDING 2: IDPs and individuals who intended to leave their location in short or long term were more likely to report symptoms of depression.
The proportion of respondents who reported having experienced symptoms of depression was highest among IDPs (50%), followed by returnees (42%) and the non-displaced (35%). These proportions increased when displacement was combined with other characteristics, most notably a respondent’s gender and, in the case of returnees, the time since return. Among IDPs, such differences were less pronounced, potentially indicating this group to be at higher risk, irrespective of compounding factors.
Additionally, symptoms of depression tended to be more commonly reported by individuals considering to move, in the short or long term, including if the
2: % of respondents reporting having experienced little interest or pleasure in doing things, or felt down, depressed or hopeless, more than half of days or nearly always in the two weeks prior to data collection, as well as % of individuals with a final PHQ-2 score of 3+, by displacement status
intention was to return to their area of origin. Conversely, symptoms were less commonly reported by those intending to remain in their current location, especially if they had the intention to integrate (in the case of IDPs). Notably, among individuals planning to relocate in a new location, 45 per cent of those at high risk of depression (PHQ-2 score 3+) planned to move abroad, compared to 24 per cent of those not reporting such symptoms. Finally, IDPs currently residing in the Southern oblasts4 were most likely to report having experienced symptoms of depression (46%), followed by IDPs in the East5 and the Center6 (both 40%), while the lowest proportion of respondents reporting such symptoms was recorded in the Western macro-region (31%)7
COMPOUNDING FACTORS: GENDER & DISABILITY
46%
39%
COMPOUNDING FACTORS: TIME SINCE RETURN
of returnees who had returned to their area of origin within the three months prior to data collection experienced symptoms of depression.
of returnees who had returned to their area of origin within the year prior to data collection experienced symptoms of depression, compared to 40 per cent of returnees who had returned more than a year before data collection.
4: % of individuals with symptoms of depression (PHQ-2 score of 3+), by displacement status and short-term movement intentions8
Gender differences in the prevalence of symptoms of depression were relatively small among IDPs (53 per cent of women and 46 per cent of men). However, among returnees and the non-displaced population, women were approximately one-third more likely to report symptoms of depression: of returnee women experienced symptoms of depression, compared to 34 per cent of returnee men. of non-displaced women experienced symptoms of depression, compared to 30 per cent of non-displaced men.
Similarly, self-reported disability played a more important role as a compounding factor among returnees and the non-displaced population, compared to IDPs.
Figure 3: % of respondents reporting symptoms of depression (PHQ-2 score of 3+), by displacement status and self-reported disability
disability No self-reported disability
Figure 5: % of IDPs at high risk of depression (PHQ-2 score of 3+), by mobility intentions beyond the 3 months after data collection
8 Data for the non-displaced population was not representative.
Figure
Figure
SOCIO-ECONOMIC VULNERABILITIES
KEY FINDING 3: A correlation was found between mental health and livelihoods, with unemployment and the use of severe coping strategies being associated with a higher rate of reporting symptoms of depression.
The risk of depression was highest among unemployed individuals, and lowest among the self-employed. This was especially true for unemployed returnees, among whom the rate of reporting symptoms of depression reached higher levels than among unemployed IDPs.
Results also showed that the proportion of respondents reporting symptoms of depression was significantly higher among individuals living in households that were struggling to meet their basic needs and therefore resorting to the
INDIVIDUAL LEVEL
of unemployed individuals reported having experienced little interest or pleasure in doing things more than half the days or nearly always in the two weeks prior to data collection.
of unemployed individuals reported having felt down, depressed or hopeless more than half the days or nearly always in the two weeks prior to data collection.
HOUSEHOLD LEVEL
VULNERABLE HOUSEHOLD MEMBERS
The share of respondents reporting symptoms of depression was significantly higher in households with at least one person with a disability or with a chronical illness.
of individuals in households with persons with disabilities reported symptoms of depression, compared to 34 per cent of individuals in households without persons with disability. of individuals in households with chronically ill members reported symptoms of depression, compared to 31 per cent of individuals in households without chronically ill members.
adoption of severe livelihoods-based coping strategies, reaching 60 per cent among IDPs in these cases, and around 55 per cent among both returnees and the non-displaced. Equally, the presence of chronically ill household members was correlated with a rise in the proportion of respondents reporting symptoms of depression to 60 per cent, 50 per cent, and 44 per cent among IDPs, returnees, and the non-displaced, respectively, while 46 per cent of respondents overall who were living in households with persons with disabilities reported symptoms of depression.
Retired,
In
In paid work for an employer (employee)
My
My own business, self-employed, working for family business
COMPOUNDING FACTORS: GENDER AND DISABILITY
Across the four types of occupation shown in Figure 6 (which account for 84% of female respondents and 91% of male respondents), with the exception of self-employment, female respondents reported having experienced symptoms of depression at notably higher proportions than male respondents.
On the other hand, there was no significant difference in the reported experience of symptoms of depression between individuals in paid work with or without self-reported disability. However, a significant difference based on self-reported disabilities was observed among retired individuals: 50 per cent of retired persons with disabilities reported symptoms of depression, compared to 37 per cent of those without disabilities. This may indicate that among individuals with disability, the ability to earn an income can positively impact mental health outcomes.
Figure 7: % of individuals reporting that they experienced little interest or pleasure in doing things, or felt down, depressed or hopeless, at least half the days or nearly always in the two weeks prior to data collection, as well as % of individuals with symptoms of depression (PHQ-2 score of 3+), by severity of coping strategies employed by the household during the 30 days prior to data collection
Figure 6: % of respondents at high risk of depression (PHQ-2 score of 3+), by displacement and main employment status categories
SUPPORT NEEDS
KEY FINDING 4: Population groups with a higher risk of depression reported a higher need of both psychological and other types of support.
One third of individuals at high risk of depression mentioned needing psychological support for themselves or someone in their households. Overall, the high-risk population groups identified earlier in this brief more frequently reported needing mental health support than others. However, an exception to this trend was represented by the fact that returnees reported higher needs for psychological support compared to IDPs, who however more commonly reported symptoms of depression.
of individuals overall reported themselves or someone in their household to be in need of psychological counselling.9 This figure increased to 23 per cent in the case of women.
DISPLACEMENT STATUS AND MOBILITY INTENTIONS
Figure 8: % of respondents reporting themselves or someone in their household as needing psychological counselling, by displacement status
Individuals reporting symptoms of depression also mentioned lacking access to a broader range of basic goods and services, notably medicines and healthcare, than individuals without symptoms of depression, highlighting the importance of holistic interventions that combine support of basic needs with the provision of mental health services.
of individuals reporting symptoms of depression mentioned that they or someone in their household were in need of psychological counselling, compared to 11 per cent of individuals not reporting symptoms of depression.
25% 26%
of individuals in households with persons with disabilities reported themselves or someone in their household to be in need of psychological counselling.
of individuals in households with chronically ill persons reported themselves or someone in their household to be in need of psychological counselling.
9: % of respondents reporting themselves or someone in their household as needing psychological counselling, by displacement status and movement intentions in the three months following data collection10
Figure 10: % of respondents reporting themselves or someone in their household as needing psychological counselling, by level of severity of livelihoods-based coping strategies the household in the 30 days prior to data collection
SUPPORT NEEDS
Individuals reporting symptoms of depression mentioned greater lack of access to basic goods and services. Hence, besides mental health support, individuals reporting symptoms of depression may need broader support to help them regain access to basic goods and services and re-establish a sufficient level of mental and material resilience.
Figure
Figure 11: % of respondents reporting a lack of access to different basic goods and services
RECOMMENDATIONS FROM IOM MHPSS UKRAINE PROGRAMMING
ABOUT IOM UKRAINE MHPSS
IOM in Ukraine implements a comprehensive MHPSS programme aimed at enhancing the psychological well-being and resilience of individuals affected by war and displacement. The programme offers a wide range of services, including community and family support activities across Ukraine, focused and specialized support both in person and through the IOM Emotional
RECOMMENDATIONS (ABRIDGED):
The following recommendations for IOM MHPSS programming in Ukraine propose a comprehensive, multitiered response to address the pressing mental health challenges facing vulnerable populations affected by conflict. These strategies aim to provide immediate relief while addressing the socio-economic drivers of mental health challenges, fostering resilience and well-being across affected communities.
Tailored Support for High-Risk Groups: Given the complex interplay between personal, social, and economic stressors, it is recommended that IOM enhance specialized MHPSS services for high-risk groups—including IDPs returnees, women, and individuals with disabilities—who are experiencing disproportionately high rates of depressive symptoms.11 This approach includes utilizing the Patient Health Questionnaire-9 (PHQ-9) to further assess individuals who scored 3 or more on PHQ-2. Applying PHQ-9, a validated measure for assessing the severity of depression, can aid in early identification and appropriate intervention by helping staff detect those in need of immediate, specialized MHPSS services. Moreover, IOM should consider expanding women-only support groups that focus on gender-specific challenges, such as caregiving and economic needs;12 establishing proactive outreach to households with disabled and chronically ill members;13 and developing reintegration programs for returnees that include psychological support, job placement assistance, and health services to address their unique stressors, such as displacementrelated trauma.14 Where possible and appropriate, IOM MHPSS teams should integrate these groups into community-based psychosocial activities.
Support Hotline, as well as capacity-building initiatives for government partners, MHPSS professionals, and volunteers. IOM and its implementing partners have provided 214,683 MHPSS services to more than 65,000 individuals between 24 February 2022 and 15 October 2024 through in person and remote services, including through the IOM Emotional Support Hotline.
3. 4. 5.
Expanding Access to Services in Conflict-Affected and Remote Areas: With mental health needs particularly acute in frontline and remote regions with limited access to services, it is recommended to expand MHPSS accessibility through mobile MHPSS units, remote services and community-based MHPSS centers.17 Mobile units, run by IOM MHPSS and Health teams, could bring mental health assessments, psychological first aid, and counseling to underserved areas, while remote options, such as the IOM Emotional Support Hotline, while not a panacea, expand access to services and help overcome conflict-related mobility restrictions. Furthermore, community centers could provide safe spaces for both displaced and local populations, integrating psychosocial support and livelihood resources.18
Community-Level Campaigns to Reduce Stigma: Recognizing that stigma, especially among men, hinders help-seeking behaviors, IOM MHPSS teams are recommended to continue and expand targeted awareness campaigns to normalize mental health care within communities. Culturally sensitive messaging that frames mental health care as resilience-building for men, peer-led support initiatives where trained community members act as mental health ambassadors, and integrating mental health education into school curricula aim to create early and lasting shifts in perceptions about mental health.19
Cross-Sectoral Coordination for Holistic Service Delivery: The evaluation demonstrates that respondents with depressive symptoms report a need for not only psychological support but also essential goods and healthcare, underscoring the value of a coordinated, cross-sectoral response.20 It is recommended that all IOM teams establish and expand integrated service hubs in highneed areas, where individuals can access MHPSS, healthcare, and livelihood support in one location. Without this cross-sectoral support, the drivers of respondents’ needs may not be addressed in any durable way. Strengthening data sharing and regular coordination meetings among MHPSS providers, healthcare organizations, and livelihood agencies through cluster fora will help ensure seamless service provision, comprehensive coverage, and minimized duplication, facilitating a cohesive response to both mental health and material needs.21 1. 2.
Integration of MHPSS with Livelihoods Support: Acknowledging the strong correlation between economic insecurity and poor mental health, integrating economic and livelihood support within MHPSS services is critical to reduce financial stressors that exacerbate mental health risks.15 Recommendations include creating vocational training and employment support partnerships, with embedded MHPSS staff to address psychological barriers, following IOM’s MLI manual, and offering financial assistance, such as small grants and cash transfers, to help households reduce the need for severe coping strategies.16 For those already receiving financial support, IOM teams, including but not limited to IOM MHPSS, should establish and expand referral pathways to MHPSS services that can bolster positive coping mechanisms and build social support networks.
11 International Organization for Migration (IOM), 2022. Manual on Community-based Mental Health and Psychosocial Support in Emergencies and Displacement - Second Edition. IOM, Geneva. IOM
12 Charlson, F., van Ommeren, M., Flaxman, A., Cornett, J., Whiteford, H., & Saxena, S. (2019). New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. The Lancet, Retrieved from The Lancet
13 Amedari, M. K. I., 2020. Mental health support for IDPs in Northeast Nigeria. Bibalex
15 Baingana, F. K., Bannon, I., & Thomas, R., 2005. Mental health and conflicts: Conceptual framework and approaches. World Bank
16 IOM, MHPSS And Livelihood Integration (MLI) Manual, March 2022. IOM
17,18 International Organization for Migration (IOM), 2022. Manual on Community-based Mental Health and Psychosocial Support in Emergencies and Displacement - Second Edition. IOM, Geneva. IOM
19 Ibid; Inter-Agency Standing Committee. (2019). IASC Community-Based Approaches to MHPSS Programmes: A Guidance Note IASC
20 Baingana, F. K., Bannon, I., & Thomas, R., 2005. Mental health and conflicts: Conceptual framework and approaches. World Bank
21 Alaka, A. I. (2023). The protection of vulnerable groups in armed conflict. Retrieved from ResearchGate.; Inter-Agency Standing Committee. (2019). IASC Community-Based Approaches to MHPSS Programmes: A Guidance Note IASC