

Progress with limits: Female surgeons still face uneven playing field
By Maria Gifford
For decades, vascular surgery had few female surgeons. The specialty carved out its territory with increasingly sophisticated techniques, but the operating rooms where surgeons performed carotid endarterectomies and aortic repairs remained overwhelmingly male. Only in recent years have women started entering the field in significant numbers.
Today, women comprise 14.6% of practicing vascular surgeons. But as more enter the profession, they aren't getting equal access to the complex, career-defining cases that make vascular surgery what it is.
Britt Tonnessen, MD, associate professor of vascular surgery and associate program director of the vascular residency program at Yale School of Medicine, has a career spanning nearly 20 years. Over that time, she has observed talented female surgeons struggle to secure the same volume and complexity of cases as their male counterparts despite identical training and credentials. When a study was published in the Journal of Vascular Surgery (JVS) in June 2025 documenting how significant these disparities are, Tonnessen felt the data deserved a response.

"The current study brought forth important data that should raise questions and concerns as to why highly trained female surgical subspecialists had lower volume of cases when compared to men, despite an uptick over time," said Tonnessen.
Tonnessen co-authored a letter to the editor published in JVS in November 2025, which not only acknowledged the problem but calculated what the disparities actually cost female surgeons.
Numbers behind the gap
The study analyzed medical claims data from the Centers for Medicare and Medicaid Services from 2017 to 2021, examining who performs common vascular procedures across all specialties.
The findings showed that board-certified vascular surgeons performed the highest percentage of major vascular procedures: 68.6% of open infrarenal aortic interventions, 65.2% of endovascular aneurysm repairs (EVARs), 59.1% of carotid endarterectomies, 60.3% of open arteriovenous fistulas, 59.3% of endovascular arteriovenous fistulas, 71.4% of open infrainguinal interventions, and 45.7% of endovascular infrainguinal interventions.
The majority of all procedures were performed by male vascular surgeons, ranging from 88.3% to 94.7% depending on the procedure type. However, vascular surgery demonstrated the greatest increase in procedures performed by women over the five-year period.
Female vascular surgeons performed between 6-10% of endovascular aortic repairs and carotid endarterectomies over the study period. Considering women comprise only 14.6% of vascular surgeons overall, that still represents a significant deficit. An additional 4-7 EVARs and 7-14 carotid endarterectomies per year should be going to female vascular surgeons but aren’t.
The letter noted that surgical complexity is linked to work relative value units (RVUs) — a metric used to measure the value of medical services for physician compensation and billing — and potentially widens the pay gap in productivity-based practice settings. Higher complexity surgical procedures generate more RVUs while lower complexity procedures generate fewer.
See page 14


PREMATURE PAD TIED TO HIGHER AMPUTATION RATES
By Killian Meara
PATIENTS WITH PREMATURE peripheral arterial disease (PAD) face a significantly increased risk of mid- and late-term major amputation, according to a new analysis of the linked Vascular Quality Initiative and Medicare dataset (VQI-VISION). The research was presented at the 2026 annual meeting of the Southern Association for Vascular Surgery (SAVS) in Paradise Island, the Bahamas (Jan. 21–24).
Premature PAD is defined by onset before 50 years of age and only represents about 1.6% of cases. Olamide Alabi, MD, lead author on the study and associate professor of surgery at Emory University School of Medicine in Atlanta, Georgia, said that some anecdotal data suggests these patients have worse outcomes after revascularization. “We wanted to look within the VQI, which is the largest vascular surgery registry, to determine if that was in fact the case,” she said. The study looked at over 15,000 patients who underwent endovascular peripheral vascular intervention (PVI) for arterial occlusive disease between January 2017 and December 2018. Demographics, outcomes, and characteristics were analyzed between premature PAD and traditional-age patients. Primary outcomes were the risk of major
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD | Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD | James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Managing Editor Killian Meara kmeara@vascularsociety.org
Assistant Editor Maria Gifford
Design Madison Spadafino
Advertising Nicole Schmitz nschmitz@vascularsociety.org
Letters to the editor vascularspecialist@vascularsociety.org
Published by the Society for Vascular Surgery
FROM THE EDITOR
Fear and loathing in a post-CREST-2 world

Medical editor Malachi Sheahan III, MD, reflects on the release of the CREST-2 results and considers what they may mean for clinical practice.
As you likely know, the long-awaited CREST-2 trial results were recently released. While panic and jubilation erupt among different tribes of our fractured health care system, the findings demand a measured scientific look. Of course, you didn’t come to me for that, so I’ll point you in the direction of the official SVS response published by AbuRahma, Schermerhorn, and Calligaro in the December JVS (see page 18). What follows is my (very biased) opinion, FAQ style.
What was the design of CREST-2?
Two parallel, observer-blinded randomized controlled trials (RCTs) in patients ≥35 years with ≥70% asymptomatic carotid stenosis. One compared intensive medical management (IMM) alone vs. IMM + carotid artery stent (CAS), the other IMM vs. IMM + carotid endarterectomy (CEA). Primary endpoints: stroke or death within 44 days, plus ipsilateral ischemic stroke up to 4 years.
What were the main outcomes for CAS?
At 4 years risk: 6.0% in IMM vs. 2.8% in CAS + IMM (P = .02).
Periprocedural risk: 1.3% with CAS. Number needed to treat was 31.
What were the main outcomes for CEA?
Four-year composite: 5.3% IMM vs. 3.7% CEA + IMM (P = .24).
Periprocedural: IMM had 3 strokes; CEA had 9 strokes.
How did CAS compare to CEA?
Both had lower risk of stroke at four years than IMM but only CAS reached significance. Both had low rates of disabling stroke rates.
What was considered intensive medical therapy?
BP <130 mmHg, LDL <70 mg/dL, lifestyle optimization.
How close was CEA to achieving statistically significant improvement over IMM?
–Social media starts here “Verdict is out!!!!! #CREST2 RESULTS FAVORING CAS!!!” and devolves quickly.
Wait, the periprocedural stroke risk was 1.3% with CAS? Is that typical?
No, it is historic. This is by far the lowest reported in any randomized carotid revascularization trial with independent outcome adjudication. Stent enthusiasts will credit improvements in device technology, imaging, and medical management. Skeptics will note that the credentialing process was incredibly rigorous with about half of the prospective interventionalists rejected. Conversely, about 90% of the surgeons were accepted.
Life in the medical arms of this trial seems nice. How can I move there?
I know right? Free meds! Lifestyle coaches! I’ve got patients trying to light up Marlboros in the PACU while their family is trafficking Popeyes to their bedside. This trial shows us the promise of medical therapy, but not necessarily our reality. And even in this ideal scenario, the results may not be as dramatic as they appear. As the official SVS response points out, the annual stroke risk with medical therapy in the (now ancient) Asymptomatic Carotid Artery Study was 2% and decreased to 1% over time. In CREST-2, medical management yielded an annual stroke rate of 1.7% in the CAS trial and 1.5% in the CEA trial.
What about TCAR?
Enrollment began in 2014, before the widespread use of TCAR. Since TCAR has never been studied in a randomized controlled manner, this remains an open, but important question as this technique is favored by many vascular surgeons for asymptomatic lesions.
Go ahead. Unload the rest of your nitpicks here. Thank you! Don’t mind if I do:
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society. The Society for Vascular Surgery will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. |
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | RECIPIENT: To change your address, e-mail vascularspecialist@ vascularsociety.org | For missing issue claims, e-mail vascularspecialist@vascularsociety.org | Vascular Specialist (ISSN 1558-0148) is published by the Society for Vascular Surgery. | Printed by Ironmark ©Copyright 2025 by the Society for Vascular Surgery
Follow Vascular Specialist on socials vascularspecialist vascular-specialist-online vascularonline
A tipping point analysis showed that six more strokes in the IMM group would have given this result. Some back-of-the-envelope math suggests that if 29 strokes occurred in the 600 medical group patients at four years, stroke reduction with CEA would have achieved significance. Interestingly, there were 28 strokes in the 600 medical group patients in the CAS trial.
Did CAS outperform CEA?
No. These were two separate trials with different inclusion criteria. A direct comparison between CAS and CEA cannot be made. As I pointed out, it appears the benefit of CEA would have achieved significance had it been compared to the same medical management group as CAS. Over the past 15 years, seven of the eight randomized controlled trials directly comparing these two modalities demonstrated a persistently increased incidence of 30-day stroke with CAS over CEA (including CREST-1 by the way). A finding reinforced by real world VQI data. Anyone claiming that CAS outperformed CEA in CREST-2 would be using the same transitive property logic fail that led my son to claim his soccer team was the best since they beat the eventual champs (ignoring their 0-12 record against the rest of the division).
With these results so close I am sure the conclusions drawn by other specialties have been tempered?
My sweet summer child. From the New England Journal of Medicine
– “We can conclude that there is no longer a role for routine carotid endarterectomy in persons with asymptomatic stenosis.”
Here is a just a sample of the headlines seen on page 1 of a Google search:
– A New Asymptomatic Carotid Stenosis Paradigm?
– Long-Awaited CREST-2 Results Bolster Stents for Asymptomatic Carotid Stenosis
– CREST-2 Shows Reduced Stroke Risk With Carotid Artery Stenting Plus Intensive Medical Management; No Added Benefit Seen With CEA
– Carotid Stenting Makes a Strong Showing in the CREST-2 Registry
– Asymptomatic Blocked Carotids Don't Need Surgery, Large Trial Shows
– The antiplatelet protocols were more aggressive in the CAS arm than that required for CEA.
– The design was intent-to-treat. Nearly 20% of the patients assigned to medical management eventually underwent a carotid revascularization.
– About two thirds of the patients enrolled had a carotid stenosis of 70-79%. My personal practice is not to perform routine CEA in asymptomatic lesions less than 80%.
So, what can we conclude from CREST-2?
Look, sequels can be difficult to pull off. For every Godfather II we get a dozen Deuce Bigalow European Gigolos. Still, CREST-2 was meticulously designed and implemented. It is now up to us to interpret these results in our real-world settings. We have data from thousands of patients enrolled in carotid revascularization trials. The CREST-2 results should enhance this abundance of knowledge, not replace it wholesale.
Clearly medical management is and remains the cornerstone of therapy. Get the LDL under 70, push the SBP below 130, stop smoking, and deploy a PCSK9 inhibitor when statins fail. For interventions, scrutinize your own outcomes. If your complication rates drift above trial level performance, you are not doing CREST-2, you are doing roulette. For every provider who interprets these results as an indication to routinely stent asymptomatic lesions, there is at least a 50% chance the CREST-2 investigators would not credential them. No matter what technique you employ, the margin of benefit for carotid revascularization in asymptomatic lesions is razor thin. Following CREST-2, it does not seem like a leap to suggest that patient selection and provider skill matter as much or more than the type of intervention employed. How payers weaponize the CREST-2 findings remains to be seen. Blanket denials for asymptomatic revascularization is obviously a possibility. A better and more evidence-based approach would favor a requirement for registry-anchored proof of outcomes. CEA isn’t dead, but a strict diet is likely.
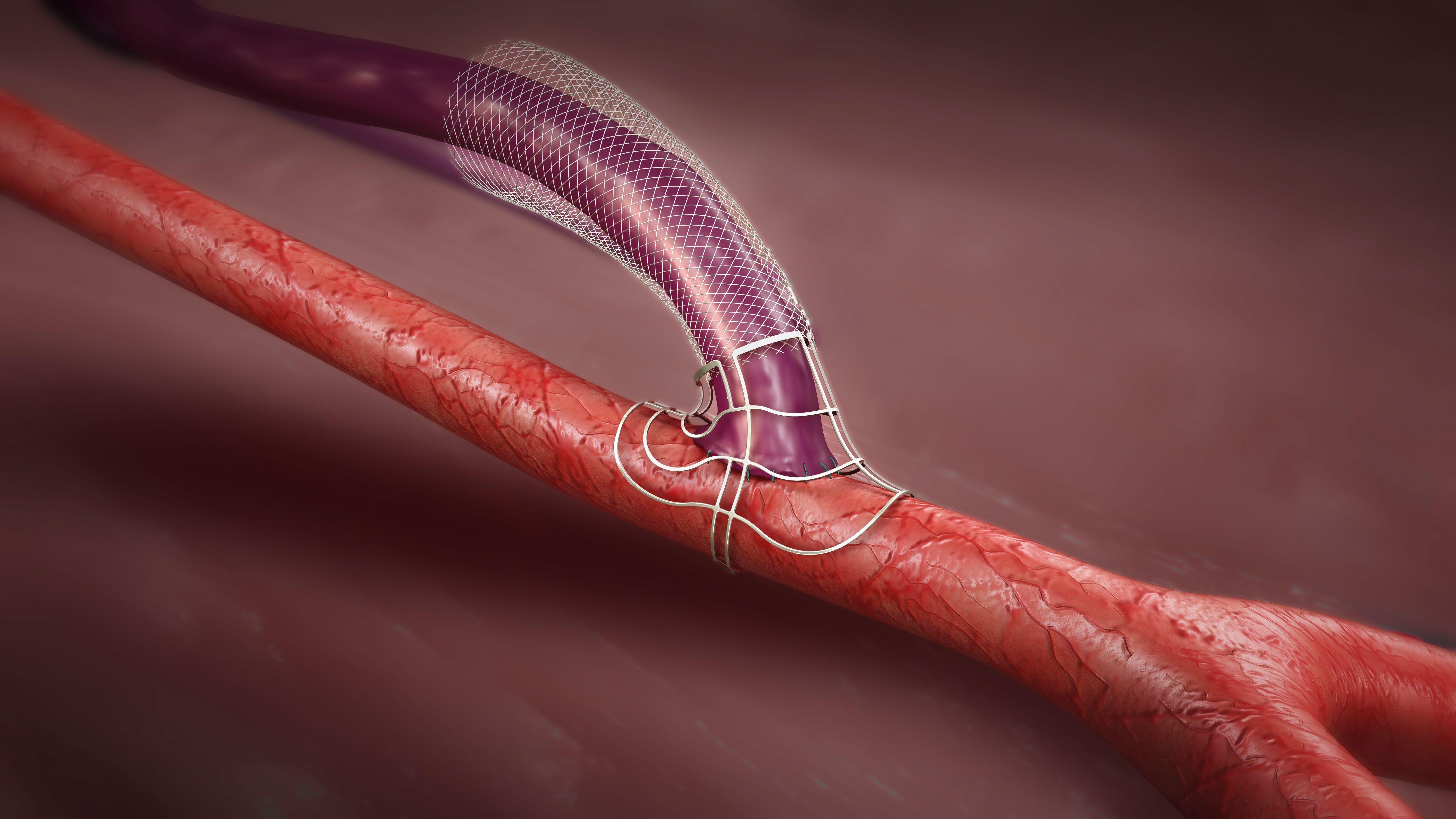
EU/UK: The VasQ device is intended for use as subcutaneous arteriovenous conduit support for vascular access.
US: VasQ is intended for use as an external support for upper extremity arteriovenous fistulas created for vascular access by means of vascular surgery.
Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions and adverse events available at https://laminatemedical.com/eIFU




BLOOD PRESSURE CONTROL CRITICAL FOLLOWING PAD REVASCULARIZATION, STUDY SHOWS PAD
By Maria Gifford and Killian Meara
A recent study suggests vascular surgeons may be overlooking a crucial element of post-procedural care: blood pressure management. The data, presented at the 2026 annual meeting of the Southern Association for Vascular Surgery (SAVS) in Paradise Island, the Bahamas (Jan. 21–24), found good hypertension control directly impacts amputation free survival (AFS) rates following revascularization for peripheral arterial disease (PAD).
The single-center study was led by researchers from the University of Michigan, Ann Arbor and examined 1,962 patients over nine years who underwent open and endovascular lower extremity revascularization. Findings showed patients with hypertension were at higher risk of amputation or death compared to those who maintained normotensive blood pressure levels, despite being prescribed antihypertensive agents.
the findings should prompt vascular surgeons to reconsider their approach to hypertension.
“Blood pressure management is often neglected because it’s something that is chronic,” said Henke. “It requires repeated visits often, and it requires expertise that is sometimes out of the standard teaching that vascular surgeons get. We typically just don’t know how to manage it as well.”

Henke, MD
The study tracked AFS as the main outcome and patients were classified as normotensive (<130 mmHg), Stage I hypertension (130-140 mmHg), or Stage 2 (140+ mmHg). The results showed that normotensive patients had significantly better AFS compared to hypertensive patients. “The take home message is we really should focus on trying to get our patients in the normal intensive range as best as possible,” said Henke.
was actually associated with decreased AFS,” said Henke. “It’s a matter of patients taking their medication, and we think that reflects medication adherence.” He added that sometimes patients can be on medications but remain persistently hypertensive. “They may be trying to take them, or they’re taking them and need additional medicines added,” he said.
Henke said that the path forward involves better coordination between clinicians. “The big opportunity here is to pair with our vascular medicine colleagues that are specialists in this area to manage hypertension, as well as more aggressive lipid management.”
Although vascular medicine is part of fellowship and residency training, only recently has it been emphasized, said Henke. He added vascular surgeons have historically been focused on claudication and long-term management. “Many of us, myself included, probably think someone else is taking care of [blood pressure management] and refer them back to their cardiologist, vascular medicine doctor, or primary care physician,” said Henke. “We just really haven’t paid as close attention to it as we should.”
According to Henke, vascular surgeons now pay attention to antiplatelet therapies and lipid management much better than in the past. Hypertension should also get the same level of awareness. Looking ahead, Henke believes that more research to compare blood pressure management with routine care would be beneficial.
“One idea would be to have a prospective cohort of patients who have intensive medical management after their procedure as compared to routine care,” said Henke. “That could be a randomized controlled pragmatic study where you have some centers where vascular surgeons are paired with cardiology, vascular medicine or primary care and they coach the patients or follow up monthly to get some type of virtual readings of their blood pressure on a more intensive basis. I think that would be interesting to see.”
Peter Henke, MD, senior author on the study and section head of vascular surgery at the University of Michigan, Ann Arbor, said
The data also found patients whose blood pressure readings fluctuated between visits showed decreased AFS compared to those with consistent readings. “Wide variability
Dementia patients see worse outcomes after AAA repair
By Killian Meara
A cohort study using national Medicare data found patients with Alzheimer’s disease and related dementias face significantly higher risks across different outcomes after elective abdominal aortic aneurysm (AAA) repair. The data were presented at the 2026 annual meeting of the Southern Association for Vascular Surgery (SAVS) in Paradise Island, the Bahamas (Jan. 21–24).
Led by researchers from Brigham and Women’s Hospital in Boston, Massachusetts, the study is the first to evaluate outcomes of AAA repair specifically in patients with dementia. “We included 42,733 patients in our study, and of those, 4.3% had dementia,” said co-investigator Samir K. Shah, MD. “Overall, around 80% underwent endovascular aneurysm repair (EVAR). A greater percentage of patients with dementia, 89.1%, underwent EVAR.”
Researchers sought to test if EVAR among high-risk patients with dementia was safe due to it being less invasive. “There’s a common understanding that endovascular repair is a less physiologically stressful alternative to open repair, and therefore is a ‘safe’ procedure,” said Shah, an assistant professor in the division of vascular surgery and endovascular therapy at the University of Florida. “There has been no study focused solely on aneurysm outcomes amongst patients with dementia that we identified. This is the first one ever.”
The results suggest EVAR isn’t necessarily a low-risk procedure for this population. “Across the board, patients with dementia had worse outcomes,” said Shah. Thirty-day mortality was found to be 6.9% in patients with dementia
Vascular surgery training should incorporate some curriculum on medicine management, said Henke. “It doesn’t mean vascular surgeons are going to manage hypertension for a living but being more aware of it and knowing when to add a medication that’s safe should be part of the practice,” he added.
compared with 3.6% in those without the disease. Inpatient complications occurred in 23.5% of dementia patients versus 17.9%, and 90-day readmission rates were 30% compared with 19.7%. “After adjustment, that remained true,” Shah added.
The researchers also calculated time at home ratio, which measures how much time a patient spends at home rather than in hospitals or nursing facilities the year following a surgery. “Most patients with dementia are community dwelling,” said Shah. “People have this idea that patients with dementia are primarily institutionalized, and across any number of studies, that’s been shown not to be the case. We found that the time at home ratio is lower among patients with dementia.”
Shah emphasized the study’s purpose is not to tell clinicians whether to operate, but to inform discussions. “It would be an error to look at this data and see it as prescribing a specific way of treating or not treating patients,” he said. “What we want is to calibrate decision-making with the data. Aneurysm repair is done for life extension, not life improvement. Because that’s the case, it’s especially important for patients and their caregivers to understand the impact that undergoing this operation will have.”
Shah said the findings should serve as a framework for shared decision-making. “If after understanding all of the data, patients and their caregivers say it is consistent with what they want, then I think by all means they should do it,” he said. “I see our data as a tool to help align care with patient goals.”
The study also highlights a broader problem. According to Shah, cognitive impairment in vascular patients is common but often undiagnosed. “We have a separate paper that was published last year in the Annals of Vascular Surgery that showed amongst patients in our vascular surgery clinic with no diagnosis of Alzheimer’s disease, traumatic brain injury, or any other sort of dementia or cognitive impairment, there was a 77% incidence of mild or moderate cognitive impairment as measured by the Montreal Cognitive Assessment,” he said. “That’s spectacular. That’s three out of four patients who have nothing on
“The big opportunity here is to pair with our vascular medicine colleagues that are specialists in this area to manage hypertension, as well as more aggressive lipid management.”
PETER HENKE, MD
their chart that have a problem that we can detect using a validated tool.”
Understanding a patient’s cognitive baseline is critical for accurate counseling and risk assessment, said Shah. “If people have this condition and we don’t pick up on it, then we won’t be counseling patients with the most accurate data,” he added. “We won’t have an appropriate understanding of their near-term and longer-term risks.”
The findings support the idea that coordinated, multidisciplinary care could lead to better postoperative results. “In an ideal world, we would be working with primary care doctors, with geriatricians, with family members or other caregivers who know the patient well and understand their goals,” said Shah. “Oncologists routinely do this with surgeons, radiation oncologists, medical oncologists and others to come up with the best possible solution for the patient.”
Shah said the next step is to gather more patient-centered data, such as information on pain, mobility, mood and quality of life. “We have mortality, readmissions and major complications data, but what we don’t have is what laypeople would consider patient-centered data,” he said. To address that, his group has begun giving patients smartwatches that collect data on movement, sleep, pain and mood, merging that information with clinical records. “If patients had that kind of data, they could make decisions that are as close to ideal as possible,” he said.

Peter
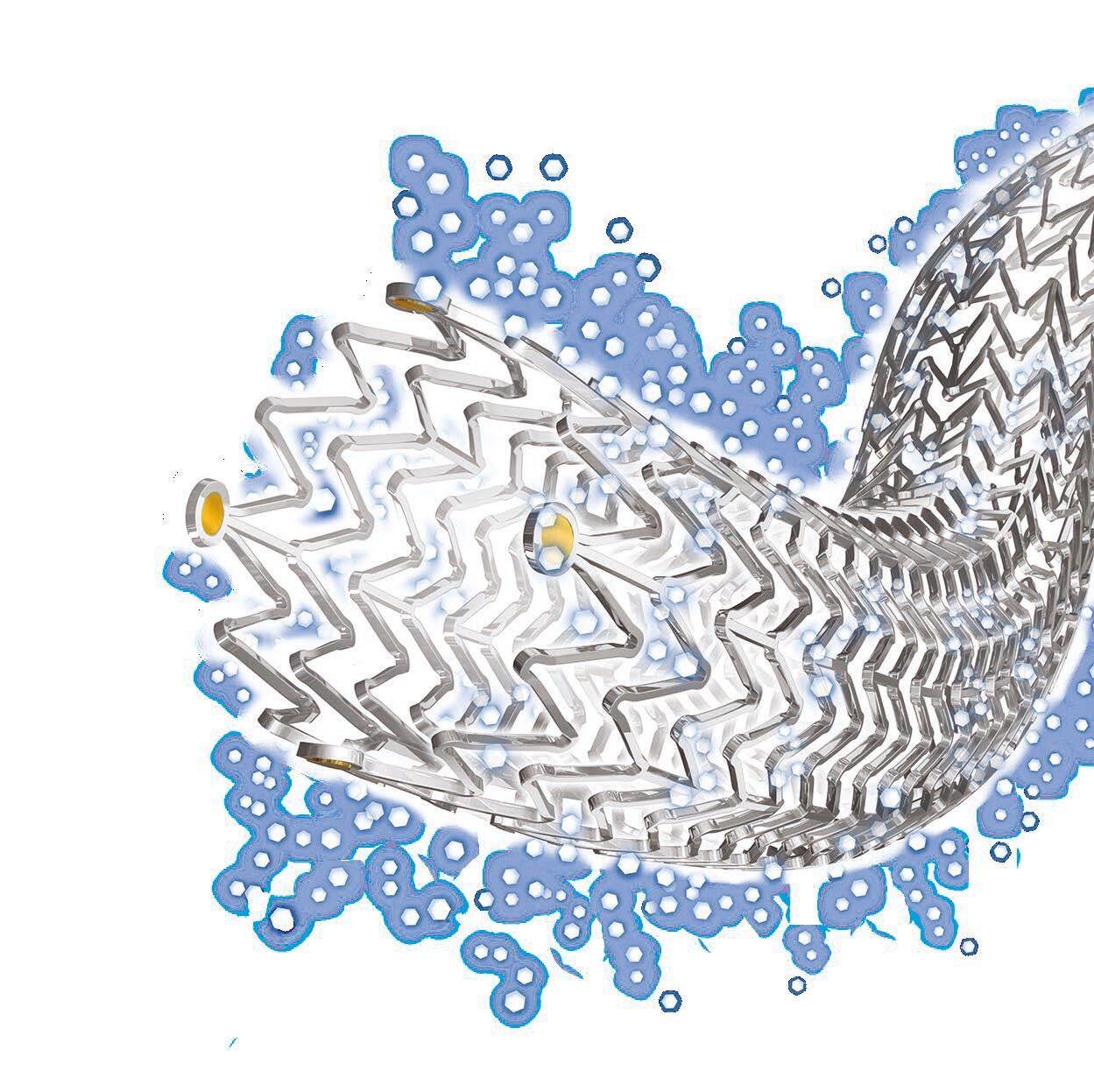
Nothing beats Zilver® PTX®.
Real-world REALDES study shows lower rate of instent occlusions with Zilver PTX than Eluvia®.1
There is no difference in primary patency or CD-TLR between Zilver PTX and Eluvia, despite the fact that longer lesions were treated in the Zilver PTX arm.
FROM THE COVER: PREMATURE PAD TIED TO HIGHER AMPUTATION RATES
amputation and mortality at 30 days, 90 days, and one year.
Results found premature PAD patients have a higher disease burden, including increased prevalence of obesity, diabetes and advanced kidney disease. They were also more likely to have a prior history of amputation and were less likely to receive guideline-directed medical therapy. “Statins save limbs and lives,” said Alabi. “If you are a patient with PAD and you are not on them, your life will be shorter and you certainly have a higher risk of losing your leg.”
Among the 351 patients with premature PAD, major amputation rates were higher at each time point. They also experienced a shorter mean time-to-amputation when compared to older PAD patients. Despite a mean age difference of 28.3 years, the data found there was no significant difference in all-cause mortality and a similar mean time-to-death between the two groups. “These younger patients are equally likely to die and die within the same timeframe after their revascularization as the older group of patients,” said Alabi. “That’s concerning.” Alabi said the increased amputation rates point to issues in early detection. “It’s clear that patients with premature PAD are not being found early enough,” she said. The research also found that these patients were more likely
LEGACY
continued from page 1
to present with chronic limb-threatening ischemia (CLTI). “We’re not missing the majority of patients,” said Alabi. “But we’re certainly missing a large group of patients who could potentially have their limbs saved and could potentially have longer lifespans.”
Another finding from the study showed that minority groups were more prevalent in the premature PAD group. “We already know that Black patients with PAD have higher rates of amputation,” said Alabi. “The same is true within the premature PAD group.” There was also a higher proportion of women. “Women are always the ones described as having atypical symptoms,” said Alabi. “If we’re waiting until they have symptoms, which tends to be the end stage manifestation of PAD, we’ve already missed the boat.”
The findings add to the growing amount of data that show a need for better screening, said Alabi. “I don’t think screening should be limited to age 65,” she said. “If you have certain risk factors, particularly diabetes and chronic kidney disease, you should be screened for PAD.” Alabi added that several national screening initiatives are underway, but many still restrict eligibility based on age.
In addition to screening, Alabi said improvements in guideline-directed medical therapy for these patients needs to become a priority. However, she said diagnosis remains
ROBYN MACSATA LECTURESHIP TO DEBUT AT 2026 APDVS ANNUAL MEETING
By Marlén Gomez
The Association of Program Directors in Vascular Surgery (APDVS), in collaboration with the Society for Vascular Surgery (SVS) Women’s Section and the SVS Foundation, will launch the inaugural Robyn Macsata Lectureship at the APDVS Annual Meeting, March 6–7, 2026, in Rosemont, Illinois.
The lectureship, the first named lecture in APDVS history, will be presented annually to honor excellence in education, mentorship and innovation within vascular surgery. Patricia L. Turner, MD, MBA, FACS, executive director and CEO of the American College of Surgeons (ACS) and a nationally recognized leader in minimally invasive surgery, will deliver the lecture.
“This initiative is a powerful testament to Robyn’s legacy and the values she championed,” said Anton Sidawy, MD, MPH, DFSVS, past chair of the Department of Surgery at George Washington University and one of Macsata’s closest mentors. “Robyn clearly left an indelible mark not only on the field of vascular surgery but also on the lives of those she trained and worked alongside. She had such a positive outlook on life that my wife used to call her ‘Sunshine.’”
Robyn Ann Macsata, of Torrington, Connecticut, passed away unexpectedly at her home in Washington, D.C., on May 21, 2021, at the age of 50. To everyone who knew her, Macsata held a deep commitment to education and

the biggest challenge. “We have to know they have PAD for them to be prescribed these medications,” said Alabi. She emphasized the importance of patient education, noting that many patients with PAD don’t even know the name of their disease, which she said is likely due to a lack of appropriate counseling.
“We need to liberally provide screening for these patients because we could literally save their lives and limbs,” said Alabi. “It’s really bad for you if you lose your leg. But it’s actually bad for our communities and it’s bad for the health care system. If you lose your leg, that is somebody out of the workforce, that is someone who can no longer be the breadwinner for their family. There are very real costs to these individuals, to their families, but also to the greater society.”
“These younger patients are equally likely to die and die within the same timeframe after their revascularization as the older group of patients. That’s concerning.”
OLAMIDE ALABI, MD

mentorship that defined her career. After completing her vascular surgery training at Georgetown University/MedStar Washington Hospital Center, Macsata spent 11 years at the Veterans Affairs Medical Center in Washington, D.C., where she served as chief of vascular surgery and program director for the MedStar Georgetown University Hospital/ Washington Hospital Center vascular surgery residency and fellowship program.
Macsata later became the chief of vascular surgery and associate professor of surgery at George Washington University Hospital, where she worked alongside Sidawy.
“Robyn was my first fellow, so she called herself ‘Number One,’ and she was so proud of that title,” said Sidawy. “During her fellowship with me, her father passed, so she started calling me ‘Papa,’ which was picked up by the rest of the fellows. Robyn was like a daughter to me; so by honoring her memory, you are honoring me as well.”
Macsata’s influence extended far beyond the operating room. A steadfast advocate for women in surgery, she inspired countless physicians to pursue their goals with confidence and integrity. Her mentorship empowered others to find their voice, embrace their strengths, and contribute meaningfully to advancing vascular surgery.
“Robyn was the kind of friend that we all need: loyal, fun and always inclusive, bringing people together,” said Palma
Shaw, MD, DFSVS, who trained alongside Macsata. “She was a friend of mine for close to 20 years. We trained at the same time in vascular surgery, and she always made everyone feel welcome.”
The lectureship reinforces the Society’s tradition of recognizing exceptional achievement in vascular surgery, education and research.
“I believe this lectureship represents a defining moment for our organization and the broader vascular surgery community. It will serve as a centerpiece for inspiration, reflection and dialogue; an annual reminder to our membership that education and mentorship are the cornerstones of our specialty. By elevating these values through a named lectureship, we create a lasting platform that celebrates excellence and challenges us to innovate in how we train and support future generations of vascular surgeons,” said Dawn Coleman, MD, DFSVS, the 2026 APDVS president. Coleman hopes that the lectureship becomes a yearly moment at the APDVS meeting where attendees can come together to celebrate Macsata’s ideals and recommit to them.
Turner’s inaugural lecture will set the tone for what organizers envision as a cornerstone of the APDVS meeting.
“Choosing Dr. Patricia Turner for the inaugural lecture was intentional; her leadership and advocacy mirror Robyn’s legacy and will inspire all of us to carry that torch forward,” said Coleman.
For those who knew Macsata personally, the creation of this lectureship is both a celebration and a reminder of her enduring impact. “Robyn was a stalwart for vascular surgery and the training of vascular surgeons,” Sidawy said. “It is very fitting for this lecture to be sponsored by the APDVS and the Women’s Section in SVS.”
Christopher J. Abularrage, MD,
DFSVS, a mentee and friend, echoed that sentiment. “We spent many hours talking about vascular surgery trainees, different programs and all aspects of vascular surgery. Eventually, our conversations would turn to life in D.C., since we both spent so much time there. She was truly a wonderful person, taken from us much too soon,” he said.
The two spent time together at Washington Hospital Center, where Macsata was a fellow and Abularrage was a general surgery resident interested in vascular surgery. He credits her for taking the time to guide him through the operations. Over the years, they served together on committees within the Eastern Vascular Society (EVS) and the SVS. “She loved vascular surgery and teaching, and I hope that this lectureship in perpetuity brings her verve for the specialty and for teaching new trainees to help recruit them into vascular surgery. That’s what her specialty was: piquing interest in young trainees to go into vascular surgery,” said Abularrage.
“The SVS Women’s Section Steering committee has discussed for several years how best to preserve the memory of Dr. Macsata and celebrate her legacy,” said Audra A. Duncan, MD, chair of the SVS Women’s section. “It is so fitting to be able to finally do this in collaboration with the APDVS, as education was where Robyn really shined. I was honored to have her as a friend and colleague, but also now to have her legacy memorialized. I hope those who knew her can use this lectureship to convey to future generations in the SVS Women’s Section, and the SVS at large, the importance of educating with positivity and inclusion which were Robyn’s strong values.”
To make a gift in support of the Macsata Lectureship, visit vascular.org/macsata.
Olamide Alabi, MD














VASCULAR RESEARCH
SVS FOUNDATION AWARDS GRANT TO STUDY PREGNANCY OUTCOMES, PAD RISK
The Society for Vascular Surgery (SVS) Foundation has awarded its Vascular Care for the Underserved (VC4U) Project Grant to a study examining the link between reproductive history and peripheral artery disease (PAD). The project, titled “Linking Reproductive History to Vascular Health: Understanding Peripheral Artery Disease Risk After Adverse Pregnancy Outcomes,” is led by Katherine M. Reitz, MD, and Natalie Domenick Sridharan, MD.
The VC4U grants fund initiatives to close gaps in vascular care delivery across the United States. This year, the SVS Foundation partnered with the SVS Women’s Section to prioritize research on women’s vascular health — an area historically underrepresented in clinical studies.
“The SVS Foundation is proud to support trailblazing research that ensures women are included in vascular studies,” said Catherine Lampi, SVS Foundation director. “This award was made possible through the generosity of our donors, and we look forward to continuing to partner with the SVS Women’s Section to fund projects like this that advance equity and improve outcomes for all patients.”
PAD affects more than 200 million people worldwide and up to 10% of adults in the United States, according to the 2019 Global Disease Burden Collaborators. Prevalence is higher in women than men, but women remain underrepresented in PAD research and clinical trials. This lack of inclusion has contributed to the absence of sex-specific guidelines for reducing limb loss and cardiovascular mortality, both doctors explained in their project.
“The award is a generous seed funding that allows us to get additional preparation for research and will help us continue to grow in our research interests and in exploring women’s health, as it synergizes with PAD. This will help us continue to apply to more funding sources and continue
to increase the amount of information we can put behind these efforts,” said Reitz.
Recent evidence links adverse pregnancy outcomes (APOs) — including hypertensive disorders, preterm delivery, gestational diabetes, placental abruption and pregnancy loss — to increased short- and long-term risk of atherosclerotic cardiovascular disease. The American Heart Association (AHA) recognizes APOs as predictors of cardiovascular morbidity and mortality and calls for early postpartum interventions. APOs affect one in five pregnancies, with rates rising in the United States.
Despite this evidence, the relationship between APOs and PAD remains unexplored. Obstetric history is rarely included in vascular evaluations, limiting clinicians’ ability to identify sex-specific risk factors. Understanding this connection could enable earlier diagnosis and targeted interventions to reduce complications in high-risk women.
The study will focus on Western Pennsylvania, where tobacco use, hypertension and diabetes disproportionately affect low-income neighborhoods and racially and ethnically minoritized populations. Both rural Appalachian and urban Pittsburgh communities face heightened risk for APOs and PAD. Magee-Womens Hospital, which handles more than 10,000 deliveries annually, serves these vulnerable populations.
“More than anything, knowledge is power and knowing that these pregnancy outcomes are associated with adverse events, we can screen patients. We can continue to study it. We can continue to improve patient outcomes and try to get the outcomes for women, at least approaching those for men,” said Reitz.
Using electronic health records and the Magee Obstetric Maternal & Infant (MOMI) Database, investigators hypothesize that APOs are associated with early PAD development and adverse outcomes following lower extremity revascularization. The study has two aims:
Aim 1: Identify APOs linked to early PAD onset and longterm major adverse limb events and cardiovascular events among women undergoing PAD treatment. Researchers will integrate data from 8,104 female PAD patients treated between 2016 and 2024 with APO data from more than 300,000 live births recorded from 1985 to 2019.
Aim 2: Explore barriers and facilitators to implementing a structured obstetric history tool in electronic health records. Guided by the Consolidated Framework for Implementation Research, the team will interview clinicians, EHR developers and patients to design a
sustainable process for integrating sex-specific history into vascular care.
Sridharan said the team will be working with the Clinical and Translational Science Institute at the University of Pittsburgh, where the grant funds will help them begin, asking the women questions and documenting their history.
“We’ll be having a summit with multiple stakeholders who are involved in women’s health and patient care and possibly even some patients themselves to see how we can integrate this history intake tool and the process of asking these important women’s health history questions to patients in a way that is acceptable and sustainable,” she said. “We’re going to do it in a very structured way to make sure that it fits into the clinic flow so that it’s not disruptive, it’s acceptable to patients, it’s integrated into our EMR so that we can collect this data hopefully for many years to come and identify the risk factors that are relevant to our patients so that we can intervene on them earlier in life.”
The team is based at a high-volume academic medical center anchored by UPMC Magee-Women’s Hospital, one of the largest women’s hospitals in the country. The system performs nearly 1,000 lower extremity revascularizations annually, 40% of which involve female patients, and about 1,200 carotid interventions, more than half of which include women.
Reitz and Sridharan also lead a vascular screening clinic for underserved patients. Seed funding from the Eastern Vascular Society (EVS) enabled a bi-monthly clinic serving unhoused and uninsured individuals in Pittsburgh, providing diagnostic and preventive services.
By investigating the link between APOs and PAD and creating a framework for integrating obstetric history into vascular care, the project aims to inform sex-specific risk factors and improve outcomes for women. Findings could lead to scalable strategies for early diagnosis and intervention, ultimately reducing disparities in vascular health.
“We see this as something that can potentially be rolled out to other providers, whether that is gynecologists, women’s health providers or cardiologists. We’re hopeful that this knowledge and the tools that we create from the studies that come from this grant are something that can be used to help inform other providers and provide screening tools for them, as well to help capture these patients earlier, possibly get them vascular referrals earlier or possibly get them on medications for prevention of vascular disease and adverse outcomes,” said Sridharan.
KATHERINE M. REITZ, MD

“The award is a generous seed funding that allows us to get additional preparation for research and will help us continue to grow in our research interests and in exploring women’s health, as it synergizes with PAD. "
NATALIE DOMENICK SRIDHARAN, MD

We’re hopeful that this knowledge and the tools that we create from the studies that come from this grant are something that can be used to help inform other providers and provide screening tools for them."
BOLDER
CMS Introducing the Vascular Surgery MIPS Value Pathway: A new era for meaningful, specialty-driven quality reporting
By Caitlin W. Hicks MD, MS, and William P. Shutze, MD
THE CENTERS FOR MEDICARE & MEDICAID Services (CMS) recently finalized a new Merit-based Incentive Payment (MIPS) System Value Pathway (MVP) specifically for vascular surgery — an important milestone for our specialty and the Society for Vascular Surgery (SVS).
Developed by the SVS Quality and Performance Metrics Committee (QPMC) under the leadership of Evan Lipsitz, MD, and Caitlin W. Hicks, MD, MS, with invaluable support from SVS Manager of Quality Improvement and Practice Carrie McGraw, the Vascular Surgery MVP has been officially incorporated into the CMS 2026 Final Rule. This milestone represents years of dedicated effort to ensure that vascular surgeons at last have a reporting pathway that reflects our practice, reflects meaningful outcomes for vascular patients, and reduces the administrative burden of traditional MIPS.
For many vascular surgeons, the mechanics of the Quality Payment Program (QPP) and MIPS felt opaque and disconnected from day-to-day clinical care. Yet these programs shape reimbursement, influence public reporting, and increasingly inform CMS’ understanding of quality care. The Vascular Surgery MVP offers a coherent reporting pathway for vascular surgeons that organizes measures around the work we actually do on behalf of our patients and creates a more straightforward, clinically grounded reporting experience.
Understanding the MVP framework MVPs were created to address well-recognized limitations of traditional MIPS, which often required clinicians to select measures from an excessively broad and often clinically irrelevant menu. MVPs replace this approach with narrowly defined specialty-specific sets of measures that align quality, cost, improvement activities, and interoperability requirements under a consistent framework. Beginning with the 2026 performance year, vascular surgeons will be able to report using the new Vascular Surgery MVP. CMS anticipates MVPs will become the dominant reporting mechanism for all clinicians in future years.
How the Vascular Surgery MVP was built
The SVS QPMC developed the Vascular Surgery MVP through extensive review of available MIPS measures, registry experience, and continuous dialogue with CMS. The committee prioritized measures that reflect the conditions we treat most frequently, that have a strong evidence base, and that distinguish meaningful variation in performance.
This work was grounded in a simple goal: to create a high-value pathway that accurately reflects the complexity and quality of vascular surgical care and can be adopted successfully across diverse practice settings.
What components will vascular surgeons report under the MVP?
The Vascular Surgery MVP, as all MVPs, includes four core components: quality, cost, improvement activities, and a foundational layer (population health and promoting interoperability). Each category has defined reporting expectations (Table), which are consistent across all MVPs and easier to navigate than the traditional MIPS structure.
Quality category: Must report four measures (at least one outcome measure)
Under this MVP, vascular surgeons select four quality measures from a curated set, with at least one required to be an outcome measure. The quality measures are organized across clinical areas central to vascular practice. They include procedure-specific outcomes for endovascular aneurysm repair and carotid artery revascularization; postoperative outcomes such as unplanned reoperation, readmission, and surgical site infection; dialysis access functional outcomes; communication-focused measures such as closing the referral loop; and broader patient-centered care practices like glycemic assessment, tobacco cessation, medication reconciliation, and cardiovascular risk reduction.
The structure of the MVP quality category ensures a clinically meaningful approach to quality reporting: surgeons choose from measures that are already common in perioperative and vascular quality frameworks, rather than from an overwhelming list untethered to our specialty.
Cost category: CMS-calculated, and all MVP-specific cost measures apply
The cost component of an MVP does not require manual reporting. CMS calculates performance using administrative claims, and all cost measures linked to the MVP apply automatically. For vascular surgery, these include episode-based costs for revascularization for chronic limb-threatening ischemia, hemodialysis access creation, and the Medicare Spending per Beneficiary (MSPB) measure. These episodes are directly aligned with common vascular procedures and reinforce responsible resource utilization within high-risk patient populations.
Improvement activities: Attest to one activity
Clinicians attesting under the Vascular Surgery MVP will select one improvement activity from a focused list that includes patient-reported outcome tool implementation, perioperative care coordination, telehealth to expand access, medication and anticoagulation management, advance care
planning, and participation in patient safety organizations. Because the MVP tightly links improvement activities to the overarching goals of the pathway, the options to report on improvement activities are more intuitive and clinically aligned than those in traditional MIPS.
Foundational layer: Population health + promoting interoperability
All MVPs include a foundational layer with two parts: –Population Health: CMS automatically assigns the higher of two claims-based population health measures, requiring no action from the reporting clinician.
–Promoting Interoperability: Clinicians must report the same electronic health record–based measures required under traditional MIPS unless they qualify for reweighting.
Why this MVP matters for vascular surgeons
The Vascular Surgery MVP brings clarity and vascularspecific clinical relevance to a government-mandated quality reporting program that has historically felt fragmented and burdensome. By narrowing reporting to measures that reflect the essential domains of vascular practice, it creates a structure that aligns federal reporting with the way we conceptualize quality and outcomes as a specialty. It also reduces the administrative lift by restricting the number of measures required and streamlining selection.
Importantly, the Vascular Surgery MVP positions the SVS to shape national definitions of quality more effectively. The curated measure set highlights the risk profile and complexity of the patients we treat while reinforcing the specialty’s commitment to evidence-based, high-quality care.
What’s next for the Vascular Surgery MVP?
The inclusion of the Vascular Surgery MVP in the 2026 Final Rule is both a milestone and a beginning. It marks the first time vascular surgery has had a dedicated, specialty-aligned pathway within MIPS, and is a reporting pathway shaped by vascular surgeons for vascular surgeons. As CMS continues moving toward MVP-centered reporting, this new option ensures our specialty is represented accurately and fairly within national quality programs.
The SVS encourages its members to familiarize themselves with the structure and requirements of the Vascular Surgery MVP before the 2026 reporting year. The SVS QPMC is diligently working to develop additional quality measure that will further support our members’ meaningful reporting experience. Our ultimate goal is for the Vascular Surgery MVP to serve not only as a CMS compliance mechanism, but as a meaningful reflection of the value vascular surgeons bring to patient care every day.
Table. Overview of reporting requirements for clinicals reporting through an MVP A summary of the Vascular Surgery MVP can be found on the CMS website:
Requirements
Must report 4 quality measures, including ≥1 outcome measure (or high-priority measure if no outcome is available).
Cost All MVP-specific cost measures are automatically calculated by CMS using administrative claims; clinicians do not submit anything manually.
Improvement Activities Must attest to 1 improvement activity (unless the practice qualifies for special status allowing fewer).
Foundational Layer Includes Population Health measures (CMS calculates automatically) and Promoting Interoperability (PI) requirements. Clinicians must report PI measures unless exempt.

Stay tuned for a related Audible Bleeding Episode that will offer a Q&A on pertinent questions about the MVP!
Other related and valuable resources can be found at:

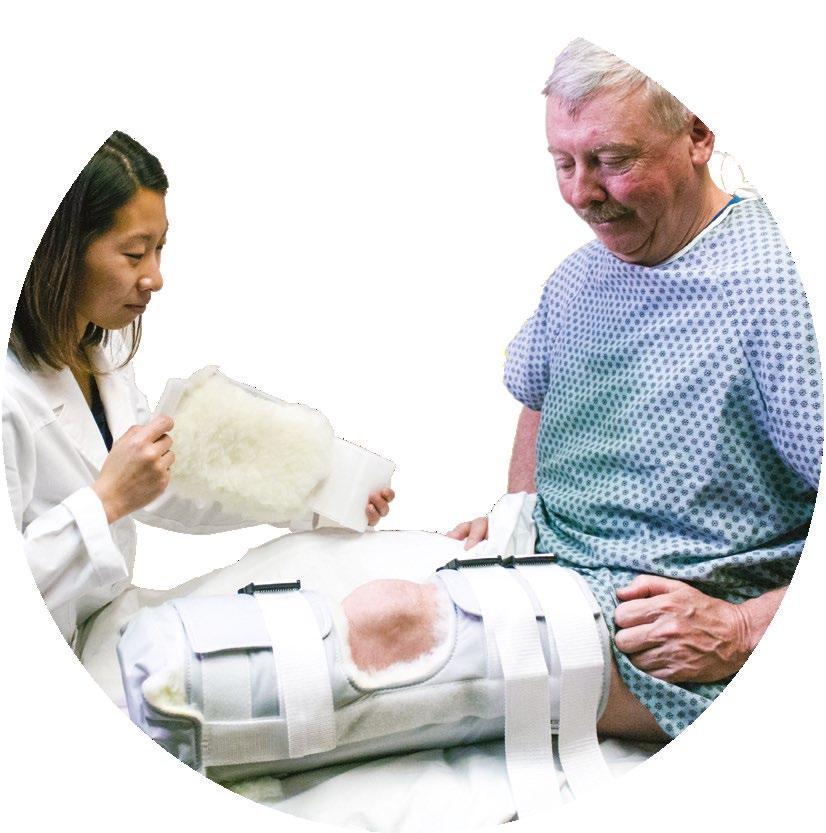

BKA PROTECTOR


ROOKE VASCULAR BOOT
You may recognize our name from this product. Rooke Vascular Boots have been warming and protecting patients’ feet for over 3 decades. Rooke Boots provide natural warmth which studies have shown may increase perfusion and Tcpo2’s while completely off loading the heel.
The Rooke BKA Protector is a rigid removable device with ample, soft padding all around to protect your patient from possible dehiscence when they fall. (AKA size also available)

CODING UNDERSTANDING THE NEW LOWER EXTREMITY REVASCULARIZATION CPT CODES
By Benjamin Lerner, MD
Lower extremity revascularization (LER) describes the work of reestablishing blood flow through stenotic or occluded blood vessels from the level of the iliac arteries to the level of the feet. It does not describe work for other pathologies such as aneurysms and does not include any work proximal to the aortic bifurcation.
The LER code set was last revised in 2011 when a comprehensive set of new lower extremity codes was created. This code set incorporated a new CPT construction of vascular territories and represented the change from component coding of each individual portion of the procedure to bundled coding of each intervention. As several of these codes were found to have high utilization, the Centers for Medicare and Medicaid Services (CMS) asked the professional societies that perform the procedures to formulate an action plan to address this finding.
A multi-year project was undertaken with a goal of modernizing the CPT code set to reflect modern practice and also to recognize the increasing burden of work, cost, and risk of treating arterial pathology that is addressed by LER. The result is a new 46 code set. The new LER code set continues to be built around reporting interventions based on arterial territory and vascular technology, however it now also recognizes (and requires documentation of) the complexity of the lesion treated. This article will provide an overview of these changes, as well as a tutorial for the new coding structure.
There are four major changes to the LER code set effective Jan. 1, 2026. These are:
– The addition of complexity to lesion definition
– The separation of the femoral-popliteal territory into two distinct territories
– The addition of an inframalleolar territory
– The addition of an add-on code for intravascular lithotripsy when performed in the iliac and femoral-popliteal territories
Complexity
Perhaps the most noticeable change in the LER code set is the introduction of complexity into reporting. Complexity is designed to reflect the additional skill, time, cost, and risk associated with more complex arterial lesions. While many different specialists and societies have thoughtful and validated models for lesion complexity, a binary system was created for CPT coding purposes to allow for unambiguous interpretation of lesions and consistency of reporting. Lesions are to be reported as either straightforward, which indicates any hemodynamically significant stenosis which
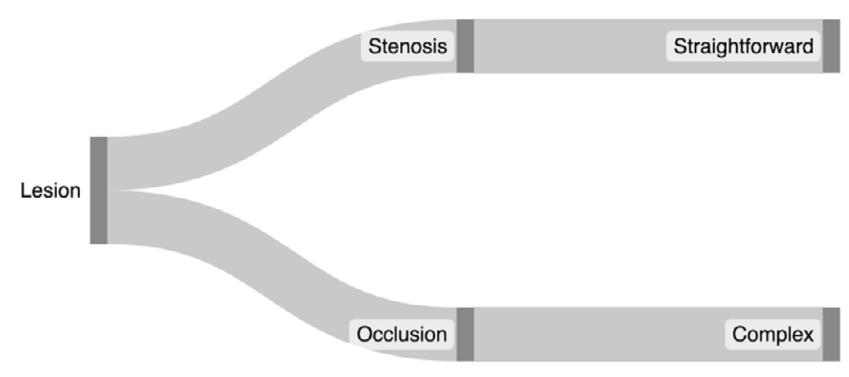




still allows blood to traverse the lesion, or complex which is defined as an occlusion (Figure 1).
An occlusion is the complete absence of blood flow through the lesion in question. Terms such as “subtotal occlusion” or “partial occlusion” are now inaccurate and obsolete for CPT reporting; “occlusion” only refers to the complete absence of blood flow through a lesion and is only appropriately reported when complete absence of blood flow is documented.
Complex lesions are considered to require more work than straightforward lesions, and therefore should be reported when multiple vessels within a single territory are treated.
Intravascular lithotripsy
New for 2026, Intravascular lithotripsy (IVL) may be reported when performed in the iliac and femoral popliteal territories. This is a novel technology in which a specialized balloon delivers ultrasonic waves that are produced from an attached power source. IVL is reported with an add-on code when used in the iliac or femoral-popliteal territories and may be reported in addition to any of the other above technologies.
How to code lower extremity interventions in 2026
Iliac
The iliac territory is comprised of 3 vessels: the common iliac, the external iliac, and the internal iliac (sometimes referred to as the hypogastric) artery. If more than one intervention is performed in the iliac territory the most superior hierarchical intervention the CPT hierarchy is reported as the “initial vessel” and any additional reportable interventions are reported with an appropriate add-on code. It is important to remember that bilateral iliac interventions in the same operative setting (e.g., bilateral common iliac artery stenting) are reported with a -50 modifier and not with an add-on code.
Angioplasty and stenting when performed in the iliac territory are reported with the corresponding technology and complexity code. Atherectomy, if performed in the iliacs, is to be reported with the Category III code 0238T. IVL is a novel technology that may now be reported in the appropriate territory, including when it is used in the iliac vessels. IVL in the iliacs is reported with the add-on code +37262 in addition to the appropriate base code (Page 2 of the Lower Extremity Revascularization (LER): How to Code Starting 1/1/2026 pamphlet).
Femoral-Popliteal
The femoral-popliteal territory extends from the proximal common femoral artery to the first tibial vessel below the knee, which is typically the origin of the anterior tibial artery. The femoral-popliteal territory is anatomically the longest arterial segment of the leg, however prior to 2026 all interventions performed in this territory were reported with a single code. There have been significant advances in
the endovascular treatment of this territory, therefore the code set was modified to allow for discreet interventions in the common femoral and profunda femoris which combined are considered distinct vessels for CPT purposes from the superficial femoral artery (SFA) and popliteal. Therefore, the femoral-popliteal territory is now defined as two separate territories: the common femoral/profunda and the SFA/ popliteal vessels.
All technologies may be reported in the femoral-popliteal territory, and IVL may be reported with the add-on code +37279 when performed (Page 3 of the pamphlet).
Tibial
In 2026 the tibial territory continues to consist of three vessels: the anterior tibial, the posterior tibial, and the peroneal. The tibio-peroneal trunk is considered a proximal continuation of either the peroneal or the posterior tibial artery and is not considered a 4th tibial vessel; any intervention on the peroneal or the posterior tibial artery which also includes the tibio-peroneal trunk is considered one vessel for CPT reporting purposes.
IVL in the tibial territory does not have a Category I CPT code, and when performed in the tibial vessels may be reported as tibial angioplasty, or with the unlisted vascular surgery code 37799 (Page 4 of the pamphlet).
Inframalleolar
Prior to 2026, the distal continuations of the tibial vessels below the ankle were considered part of the more proximal tibial vessel. Since 2011, interventions in the inframalleolar segment have become common, particularly in the treatment of critical limb ischemia and limb salvage. To reflect this important work CPT now allows for reporting of angioplasty of straightforward and complex lesions when performed in the inframalleolar territory. The vessels of the Inframalleolar territory are the dorsalis pedis (the distal continuation of the anterior tibial) and the plantar artery (the distal continuation of the posterior tibial artery). CPT allows for reporting of angioplasty of straightforward and complex lesions of the Inframalleolar vessels when performed (Page 5 of the pamphlet).
The new LER code set for 2026 completely replaces the current CPT codes. Individual payors may set their own timelines and schedules for implementation; however, our understanding is that for Medicare beneficiaries this change will be effective January 1, 2026, rendering CPT codes 37220 through 37239 obsolete.
While local coverage determinations and individual carrier payment policy can and do affect reimbursement, providers and their coding/billing teams should work together to ensure adequate documentation and accurate coding to align with the new LER code set. The Coding and Reimbursement team of the Society for Vascular Surgery is committed to keeping its membership updated and at the forefront of all changes to the reporting of vascular procedures.

FROM THE COVER: PROGRESS WITH LIMITS: FEMALE SURGEONS STILL FACE UNEVEN PLAYING FIELD
In productivity-based compensation models, physicians who perform more high-RVU procedures earn more. This makes the disparity in surgical-case complexity a direct financial concern.
"In the fee-for-service and RVUcentric models of employment, such a differential has significant financial implications," said Tonnessen.
women surgeons that translates to longer appointment times and emphasis on 'softer' and nonoperative skills," said Tonnessen. "Collectively, such expectations place additional burdens on female surgeons and can lead to practice dissatisfaction and burnout."
Vascular surgery’s lead in female recruitment
When it comes to improving gender
acknowledging ongoing responsibility.
"As a specialty, vascular surgery has made an intentional effort to add women to our workforce," said Sheahan. "I am especially proud of the recruitment scholarship program of the Southern Association for Vascular Surgery, where 70% of the recipients who went on to match in vascular surgery were women."
"It would be foolish, however, to just blindly add women to our trainee
show growth in female representation. "In terms of a meaningful benchmark by 2030, if the proportion of women performing vascular procedures meets the trend of women matriculating from medical school, this would be a considerable stride," she said.
The study examined practicing vascular surgeons, not trainees. The 56% increase in female trainees from 2007 to 2016 hasn't yet fully filtered into the workforce data.

vascular
surgery
Tonnessen's letter addressed a larger issue: Why are female surgeons performing fewer carotid, aneurysm, and bypass procedures?
"Some may speculate that women in vascular surgery are less interested in these cases or choose less vigorous schedules," the letter said. "Such explanations are convenient but do not resonate."
The real answer, Tonnessen says, lies in referral patterns shaped by implicit bias. Research shows that surgeon gender influences case referrals.
"Extrapolating, this practice potentially affects operative referrals that come from colleagues in other male-dominated specialties such as cardiology, cardiothoracic surgery, and orthopedics," said Tonnessen. "Women in vascular surgery also may be presumed to be experts in some areas like leg veins, for example, but not in aortic disease."
Studies cited in the letter show that female surgeons experience a decrease in referrals after a single complication — a penalty that male surgeons don't face. Female surgeons also receive more nonoperative referrals.
"Patients and referring clinicians may have different expectations for
recruit and retain female surgeons means depleting the talent pool during a growing physician shortage. And female surgeons have outcomes on par with male surgeons. A 2022 Canadian study showed decreased mortality and readmissions among female surgeons.
A path to equity
"Leaders and administrators play a critical role to promote their women surgeons' expertise and to address the inevitable biases that arise," said Tonnessen. "Practice patterns can be proactively reviewed, such as distribution of unassigned referrals and allocation of resources such as support staff, marketing, and operative block time."
Trinh emphasizes intervention at the earliest stages. "This starts at the medical school level, when most students' interest in surgery begins," she said. "I remember being a medical student and a lot of my friends said they didn't want to do surgery because of the lifestyle or the stereotype that the specialty wasn’t women-friendly."
Malachi Sheahan III, MD, chair of the Department of Surgery at Louisiana State University Health Sciences Center in New Orleans and medical editor of Vascular Specialist, noted the field's progress while
"I think as more female trainees enter the workforce, the number of procedures performed by women will continue to increase and near the trend seen with medical school graduates," said Trinh.
But achieving equity requires more than waiting for demographics to shift. It requires acknowledging that highly trained female surgical subspecialists face barriers their male counterparts don't — barriers that manifest in case volumes, RVU generation, compensation, and career satisfaction.
"Women in vascular surgery deserve equitable access to expertise-building cases," Tonnessen wrote in the letter. The data show progress, but the imbalance underscores barriers that still need to be dismantled — case by case, referral by referral.
Complex Wound Care Masterclass Workshop


Solutions Through Science AVF 2026

February 28-March 4, 2026
Sheraton Downtown • Denver, Colorado
ALL SPECIALTIES WELCOME!
The American Venous Forum invites you to join colleagues from around the world for the 38th Annual Meeting, taking place February 28-March 4, 2026, in Denver, Colorado. This premier event offers cutting-edge education, hands-on learning, and unparalleled networking for all professionals in venous and lymphatic disease care.
WHY ATTEND:
• Hear the latest clinical and scientific updates in venous and lymphatic medicine
• Engage in interactive sessions, abstracts, and case discussions
• Connect with experts and industry leaders shaping the future of venous health
• Dedicated programming for Advanced Practice Providers and Physicians-in-Training

International Group Photo at the 2025 Annual Meeting
2025 year in review:
Message from the SVS president and executive director
As the Society for Vascular Surgery (SVS) moves into 2026, SVS President Keith Calligaro, MD, and SVS Executive Director Kenneth M. Slaw, PhD, thank the community and highlight key accomplishments, priorities, and progress guiding the SVS and specialty forward.

The world is moving around us at blinding speed and we seem to live and work in a continuous series of “blinks," each blink a little different than the last. With the speed of change howling around us it is ever more important to hold tightly to what “anchors” us: Our Purpose/Mission; Our Ethics, Core Values, and Culture; Our Members and our Relationships. While we anchor, it is equally important for us to fix our gaze firmly on our future.
As SVS leaves 2025 and crosses the threshold into 2026, first and foremost, we want to extend our thanks, gratitude, and appreciation, to every SVS member for your support of patients, our Specialty, and Society; and our incredible volunteers and elected and appointed leaders for keeipng SVS focused, directed, and moving forward. Without our team of talented professional Staff, none of the accomplishments we have achieved could have been realized. It is the optimal balance of member drive, ideas and energy, with the talented expertise in the Staff, that moves the SVS and our Specialty forward.
Thank you to all.
2025 transcends the Presidencies of Matt Eagleton and Keith Calligaro, and it has been another year of focus on “big things” and “big accomplishments”
2025 began with the SVS Strategic Board (SBOD) beginning to develop a vision for SVS 2030 and beyond. The SBOD completed a SWOT (Strength-Weakness-OpportunityThreat) exercise to provide focus for initiatives and resources. Strengths highlighted the SVS membership and professional staff dedicated to creating and sustaining highest quality science, intellectual property, and programs.
Weaknesses focused on perceived fragmentation amongst members and vascular surgery societies leading to an overabundance of intersecting program choices while members have increasingly finite funds, time, and energy.
Opportunities for SVS focused on national Branding and Public/Media Relations efforts expanding awareness of vascular surgery, leading/driving HC system change, providing career support for members at all stages, investing in innovation, and demonstrating the power of Quality Improvement through real world evidence.
Threats focused on competition with other specialties in crowded vascular markets, sustaining interest and value in engagement with an increasingly diverse membership, a broken HC system leading to declining payment, financial limitations, burnout and workforce shortages.
The SVS Board, Council, Committee and Section leadership went to work to address these priorities in accordance with a new Strategic Plan Framework that organizes the work of SVS into 4 primary mission priorities: Advancing Clinical Excellence; Strengthening the Specialty; Strengthening Member Value and Engagement; and Strengthening the SVS as a Medical Society.
We are pleased to share just a few exciting highlights, accomplishments, and actions in 2025:
Advancing clinical excellence
SVS and vascular surgery have a new MIPS quality measure to increase payment
The SVS Quality and Performance Metrics Committee (QPMC), led by Evan Lipsitz, MD, and staffed by Carrie McGraw, RN, developed, submitted, and achieved milestone approval by CMS of a new MIPS MVP Measure that combines collection of data for 5 common procedures: AAA, Carotid, Venous, CLTI and HD access. This will reduce reporting burden and improve payments for vascular surgeons.
SVS sets the standard for quality in vascular disease care
The SVS continuously has 12-14 Clinical Practice Guidelines (CPGs) and Best Practice Documents in the active pipeline. In 2025 two Clinical Practice Guidelines were approved and published:
– Ketteler E, Cavanagh SL, Gifford E, et al. The Society for Vascular Surgery expert consensus statement on pain management for vascular surgery diseases and interventions. J Vasc Surg. 2025;82(1):1-31.e2. PMID: 40154930;
– Conte MS, Aulivola B, Barshes NR, et al. Society for Vascular Surgery Clinical Practice Guideline on the management of intermittent claudication: Focused update. J Vasc Surg. 2025;82(2):303-326.e11. PMID: 40316185.
On deck for 2026: Blunt Thoracic Aortic Injury CPG, Type B Aortic Dissections CPG; Genetically Triggered Aneurysms CPG; Vascular Scope of Work position statement. Finally, the following documents in collaboration with other Societies have been endorsed:
– CC/AHA/ASE/ASNC/SCCT/SCMR Advanced Training Statement on Advanced Cardiovascular Imaging; ACR Recommendations from the Blue Ribbon Panel on Fluoroscopy Safety; 2)
– 2026 ACC/AHA Clinical Performance and Quality Measures for Patients With Peripheral Artery Disease. Britt Tonnesson, MD (Chair, Document Oversight Committee) has been instrumental in prioritizing and improving the speed toward publication of CPGs and documents in the pipeline. We owe a debt of thanks to the DOC Committee and Reva Bhushan, PhD, Director of Quality Practice.
JVS-Vascular Science indexed
SVS’s Basic Science Journal achieved a major milestone and was accepted for indexation in the Web of Science and earned an initial Impact Factor of 2.0! Our gratitude goes to Alan Dardik, MD, the founding and now outgoing Editor-in-Chief of the journal and Phil Jackson, Director of Publications.
SVS PSO/VQI continues to achieve new heights as cornerstone of quality
The SVS Patient Safety Organization (PSO/VQI) continues to set the highest standard for registries and use of real world data to improve quality of care:
– The PSO/VQI established the LEAF Program (Long-term EVAR Assessment and Follow-Up (LEAF) a surveillance protocol created in collaboration with participating device manufacturing companies to provide the first and only registry-based surveillance protocol, designed in collaboration with the FDA, for the evaluation of longterm outcomes 10 years after EVAR.
– The SVS PSO launched a first of its kind registry-based national program on smoking cessation. This National Quality Initiative is helping centers launch Smoking Cessation Quality Improvement programs, which then can be tracked through the VQI, and is providing a cadre of resources to assist Vascular Care teams help patients stop smoking.
– The PSO, in collaboration with APDVS, launched a new Fellowship in Training (FIT) program for residents and fellows in vascular surgery. Advancement through the 12 to 18 month program provides the FIT applicant opportunity to present their work during VQI@VAM with potential selection for a highly coveted Jack L Cronenwett Scholarship (5 awarded annually) to continue research and/or work more closely with VQI/PSO staff and committees.
– SVS PSO also achieved a milestone in RWE Clinical Trials in 2025 as the National Institutes of Health (NIH) has approved the SVS PSO/VQI as the data collection mechanism for the WARRIORS Trial. WARRIORS is an international randomized trial comparing endovascular aneurysm repair (EVAR) with watchful waiting in women with small abdominal aortic aneurysms (AAAs) measuring 4 to 5.5 centimeters. Adam Beck, MD, chair of the PSO Executive Committee, will serve as the U.S. principal investigator.
– The VQI is working with a select group of centers in Michigan to launch a randomized trial on Dual Anti-Platelet Therapy. The study is formally named: “Vascular Trial Associated Registry Pilot (VSTAR-P): Antiplatelet therapies for patients undergoing lower extremity endovascular revasculaization.” The main objective of this study is to create an investigator-initiated, multicenter, open label, randomized trial to evaluate 1 month vs. 6 months of DAPT in patients undergoing lower extremity endovascular revascularization. This will demonstrate the feasibility (e.g., data completeness, recruitment rates, completion rates, adherence, etc.) of conducting such a trial nested within the VQI-PVI registry and to collect pilot event data to serve as preliminary evidence to secure funding for the large-scale, fully powered trial. This study is designed as a prospective, investigator-initiated, open-label randomized clinical trial involving collaboration between Corewell Health and Henry Ford Health.
SVS education drives clinical excellence
In 2025, SVS reached 2,648 vascular providers with its educational programs. Our flagship educational event, the VAM, was held in New Orleans, and provided over 1,400 attendees with outstanding education, fun, and surprises, when 30 minutes before the opening Plenary “the lights went out in New Orleans.” Extraordinary leadership by Matt Eagleton, MD, SVS President, Jason Lee, VAP Program Chair, and Claudie Sheahan, VAM PGE Chair, Lisa Cohen, Director of Education and Courtney Miller, Director of Meeting, transitioned the opening within 30 minutes to new space and added some comedic commentary to launch the program. In other SVS Educational events:
– SVS launched online availability of its Wound Care Curriculum, reaching the first 120 multidisciplinary providers, with the Live Workshop to be held June 12 in Boston at VAM 2026.
– The Vascular Research and Innovation Conference (VRIC) attracted over 100 research scientists this year to present the best basic science in vascular disease.
Keith Calligaro, MD SVS PRESIDENT
Kenneth M. Slaw, PhD SVS EXECUTIVE DIRECTOR
– The SVS Leadership Development Program completed Cohort 6 with 27 attendees, now having reached over 130 SVS members.
– The CPVI (Hands On Skills Course) provided 50 SVS members with a stellar opportunity to build their skills with new devices and technology.
– The SVS Coding Course had record attendance of 275 in 2025 with a deep dive on the new Lower Extremity Codes.
– SVS launched its updated and refurbished VascuLEARN platform where you can find recordings and resources from the above listed programs as well as Surgical Exposure videos – from the How I do it sessions at VAM, Microlearnings on a variety of practice management, leadership, and clinical topics, SVS webinar replays, industry links, webinars, videos, and resources, and Vascular Post Op Pearls from the Society for Vascular Nursing.
New women’s research grant awarded
The SVS Foundation, in partnership with the SVS Women’s Section, launched a new grant opportunity focused specifically on Women’s Vascular Health Research. The Women’s Vascular Health Research Grant was created to address the unique vascular health needs of women and to confront the longstanding underrepresentation of women in vascular research and clinical trials. Congratulations to Katherine Reitz, MD, and Natalie Sridharan, MD, who received the award for their project "Linking Reproductive History to Vascular Health: Understanding Peripheral Artery Disease Risk After Adverse Pregnancy Outcomes."
Strengthening the specialty
Payment advocacy remains top priority/focus
The Centers for Medicare and Medicaid Services released its CY 2026 physician fee schedule proposed rule. Overall, vascular surgeons are slated for a combined increase of 5%. Through the efforts of the SVS’ Coding Committee (David Han, Chair). In addition due to herculean efforts of the SVS RUC/CPT advisors, Matthew Sideman, Ben Lerner, Sean Roddy, Sunita Srivistava, the CMS proposed Rule accepts the physician work recommendations for all 46 new lower extremity codes. However, CMS is also proposing to significantly lower the RUC-recommended work values for thoracic branched endovascular services (2.5% decrease). The importance of having strong leadership and representation in Coding, RUC/CPT cannot be understated.
Public awareness (branding) of vascular surgery hits new heights
The SVS is now in an entirely different league when it comes to branding our specialty and leveraging media relations. The SVS “Highway to Health” Campaign has generated close to 4 billion media impressions as our members take to podcasts, TV, and print media to let the public know who we are. Enormous thanks go to Bill Shutze, MD, and Anahita Dua, MD, for being our early adopters, and we owe a debt of gratitude to Megan Marcinko, Sr. Director for Public Affairs, for leading our efforts.
SVS launches first-ever advocacy conference
Thanks to the leadership of Megan Tracci, and again, Megan Marcinko, Sr. Director of Public Affairs, the SVS convened its first-ever Advocacy Leadership Conference in Washington, DC, on September 14-16, 2026. Over 50 SVS members stormed the Hill to fight for optimal vascular patient care.
SVS EB updates disciplinary policy for expert witness testimony
Refinements and alignments to new legal requirements led to this update. As a reminder, disciplinary measures may be taken against any SVS member who serves as an expert witness and who is found to provide fraudulent testimony. Much thanks to Michael Rohrer, MD, Chair, Professional Conduct Committee for his balanced leadership and hard
work. If you wish to file a complaint please contact Dr. Rohrer (Michael.rohrer@providence.org) or SVS Executive Director, Kenneth M, Slaw, PhD (kslaw@vascularsociety.org).
Decision
on board certification model
One of the more momentous decisions in 2025 by the EB was a final recommendation following 18 months of study of the preferred model for vascular surgery board certification. In July the EB recommended, based on member survey data and 18 months of analysis, to continue supporting the current Federated Vascular Surgery Board model. As the potential for a new CV Board still remains on the horizon, the EB continues to monitor and study the need to remain prepared to respond should events warrant such action.
Vascular Specialist comes back home
In another milestone, SVS is now the proud self-publisher of Vascular Specialist! SVS will begin self-publishing Vascular Specialist in January/February, 2026. SVS Secretary Mal Sheahan, MD, continues as medical editor and SVS will be actively seeking a group of new assistant editors.
Strengthening member value and engagement
SVS continues to explore sections as model to build sdded value
In 2025, the SVS Women’s Section was approved by the Board as a Full-Standing Section, joining the Young Surgeon Section, and three new Provisional Sections were approved: The Senior Section, the Pediatric Care Section and the Arab-American Section. The Board established a new Work Group led by SVS Vice-President Andy Schanzer, MD, to clarify and re-define the role of Sections moving forward into the future.
Launch of the Ascher Vascular Innovation Institute
The SVS Foundation proudly launched the Enrico Ascher Vascular Innovation Institute, established with the generous support of the Ascher family. Its mission is to cultivate a culture of innovation within the vascular community by providing mentorship from experienced surgeon-innovators, offering educational programming in key areas of innovation, and delivering seed funding to support promising new ideas. Anchored at VAM, the Institute aims to build a vibrant community of innovators.
New lectureships established to honor Drs. Moore and Macsata
– The Wesley S. Moore Lecture in Vascular Surgery was established by the Board. This lectureship, supported by individual member donors to a fund in the SVS Foundation, will be rotated into the Vascular Annual Meeting, honors Dr. Moore’s profound contributions in education, patient care, and the specialty of vascular surgery.
– The Robyn Macsata Lectureship was established by the Boards of the SVS and APDVS. In partnership with the Association of Program Directors in Vascular Surgery (APDVS) and the SVS Women’s Section, this Lectureship will debut at the 2026 APDVS Annual Meeting, and celebrates Dr. Macsata’s extraordinary legacy as a teacher, mentor, and leader. It honors her unwavering commitment to excellence in education, patient care, and the development of the next generation of vascular surgeons.
Strengthening the SVS as a medical society
New officers elected and SVS members pass bylaw Referendum
In the 2025 Elections, Andres Schanzer, MD, was elected Vice President and Malachi Sheahan, MD, was elected Secretary. In addition members ratified two key changes in SVS Bylaws. First, the composition of the Executive Board was expanded from nine to 11 members, with the addition
of 5 At-Large Members joining the 6 SVS Officers including Chelsea Dorsey, MD, Yazan Duwayri, MD, Katherine Gallagher, MD, Vik Kashyap, MD, and Rob Molnar, MD. Second, the Senior Membership category, historically based on retirement status, was updated to a new multi-tier Legacy Membership category based on age.
Strengthening SVS for 2030 and beyond
The Executive Board has embarked on a series of initiatives to strengthen governance, strategic focus and scope:
– The EB is completing a self-assessment of governance function as well as individual board member assessment. This includes assessment of the Board President and Executive Director.
– The SVS is conducting a comprehensive evaluation and prioritization of programs and services with the help of an external consultant. The goal of the EB is to explore new models of efficiency so that SVS can continue to grow membership value and explore new worthwhile initiatives while minimizing the future need for increasing dues and program fees. The SVS has grown in complexity the past 10 years.
– SVS Vice President Andy Schanzer, MD, started serving as Chair of a regular meeting of the five SVS Council Chairs and six Section Chairs respectively, to address strategic priorities and collaboration across all Councils and Sections.
– To ensure the SVS continues to function at a high-level should there be a transition or change in top Staff leadership, the EB approved a comprehensive blueprint document clearly delineating a future transition plan when needed.
– SVS President-elect Linda Harris, MD, led a Working Group exploring the evolution of Vascular Society Relations and Engagement which suggested sunsetting the current SBOD and instead creating an Advisory Council of Vascular Surgery Societies to focus on strategies affecting all vascular societies to be co-chaired by the SVS President-elect and Vice President and to establish a new Executive Board Strategic Planning Committee to continuously work on 3-5 year strategic planning for SVS, chaired by the SVS Presidentelect. If the EB and the SBOD approve, there will be a Bylaws Referendum included in the election ballot for ratification in June 2026.
– SVS President-elect Linda Harris is leading a Work Group to examine the value and strengthen relationships with Regional and National Vascular Surgery Societies as well as External Societies seeking relationships with the SVS.
VOYAGE scholarship program lifts off
The SVS Foundation, in partnership with the SVS Young Surgeons Section, launched the VOYAGE Scholarship Program to support early-career vascular surgeons. In its inaugural year, the Foundation awarded 30 scholarships, supporting participation in the Vascular Annual Meeting (VAM), the Leadership Development Program, the Coding and Reimbursement Workshop, the CPVI Skills Course, and the Advocacy and Leadership Conference.
This is just a small sample of the exciting work that was going on in your SVS in 2025. 2026 looks to be just as exciting and full of accomplishments. Thank you for your continued membership and support.
SVS responds to CREST-2 findings on carotid stenting, endarterectomy
THE SOCIETY FOR VASCULAR SURGERY (SVS) has issued a detailed commentary in response to the results of the CREST-2 trial, which were presented at the 2025 VEITH symposium in New York City (Nov.
18–22) and the Society of Vascular and Interventional Neurology (SVIN) annual meeting in Orlando, Florida (Nov. 19–22).
CREST-2 evaluated treatment strategies for patients with high-grade asymptomatic carotid artery stenosis and no recent stroke symptoms. Researchers enrolled 2,485 patients with 70% or greater stenosis and randomized them to receive intensive medical therapy alone or in combination with either carotid artery stenting (CAS) or carotid endarterectomy (CEA). Medical management included strict control of blood pressure and lipids, smoking cessation, weight management, and medication adherence.
The study found CAS combined with medical therapy significantly reduced the risk of stroke and death compared with medical therapy alone — 2.8% versus 6.0%. In contrast, CEA plus medical therapy showed a 3.7% event rate compared to 5.3% with medical therapy alone, a difference that was not statistically significant.
Periprocedural risks were low and disabling strokes were rare across all groups. CAS benefits were consistent across age, sex, and risk-factor subgroups.
SVS President Keith Calligaro, MD, DFSVS, noted in a recent SVS Connect forum post that the findings carry “far-reaching clinical and medico-legal implications.”
The SVS commentary, authored by Calligaro; Ali AbuRahma, MD; Marc Schermerhorn, MD; and the SVS Executive Board, emphasizes that while CREST-2 adds valuable data, its conclusions should be interpreted in the context of real-world practice.
The statement highlights concerns about the generalizability of intensive medical management, the absence of transcarotid artery revascularization (TCAR) in the trial and the importance of individualized treatment decisions based on anatomy and risk profile. It also underscores that CEA and TCAR remain critical options for selected patients and that CREST-2 does not alter the current standard of care.
COMMENTARY BY THE SOCIETY FOR VASCULAR SURGERY REGARDING CREST-2
By Ali AbuRahma, MD (Past President, Society for Vascular Surgery), Marc Schermerhorn, MD (Past Chair, Society for Vascular Surgery Document Oversight Committee), Keith Calligaro, MD (President, Society for Vascular Surgery) and the Society for Vascular Surgery Executive Board
THE PURPOSE OF THIS commentary is to critically examine the CREST-2 results, discuss their implications for clinical decision-making for asymptomatic carotid artery disease, and guide clinicians toward optimizing patient outcomes. Patients with severe carotid stenosis have several treatment options available, including transfemoral carotid artery stenting (TF-CAS), transcarotid artery revascularization (TCAR), and carotid endarterectomy (CEA), all along with best medical therapy. Vascular surgeons are uniquely trained to offer all of these modalities and offer an approach through a collaborative process involving vascular medicine physicians and primary care teams, using risk stratification principles outlined in the Society for Vascular Surgery (SVS) Carotid Guidelines.1 We congratulate the CREST-2 investigators for a well-designed and exhaustive study. However, there are several issues with their conclusions that warrant careful examination and discussion.
Real-world clinical database:
The only database to evaluate real-world outcomes of TF-CAS, TCAR, and CEA is the Society for Vascular Surgery Vascular Quality Initiative (VQI). This registry is a multi-disciplinary database used as the primary repository of data regarding carotid stenting and endarterectomy. The VQI is comprised of vascular surgeons, cardiologists, radiologists, neurosurgeons, and other specialties performing carotid artery stenting and CEA. Based on VQI data, and multiple published articles that include thousands of patients, superior outcomes of both CEA and TCAR compared to TF-CAS have been consistently demonstrated in standard and high-risk asymptomatic and symptomatic patients. We strongly encourage physicians performing TF-CAS, TCAR, or CEA to join the VQI to accurately track real-world
outcomes among specialists and procedures. Ongoing participation across specialties will help ensure the VQI continues to generate high-quality real-world evidence that informs practice and supports the best possible patient care moving forward.
Real-world medical management:
The best medical management in CREST-2 is unlikely to be replicated by real world physicians and patients outside of a controlled study such as this one. Medical management has not progressed as far as once surmised, as the annual stroke risk in Asymptomatic Carotid Artery Study (ACAS) was 2% per year and decreased to < 1% over time.2 However, even with the most highly resourced and aggressive medical management targets, medication payments, routine checkin phone calls, and lifestyle coaching, CREST-2 achieved an annual stroke risk with medical management of 1.7% in the TF-CAS arm and 1.5% in the CEA arm of the trial. Thus, even with what is likely non-reproducible medical management, revascularization had a small benefit. If medical management from the trial is not generalizable, the benefit of revascularization could be even greater.
The role of TCAR:
The authors point out that TCAR was not evaluated because it had not yet been broadly implemented when CREST-2 began. However, TCAR has since become widely disseminated and is now a central component of carotid revascularization practice in the United States; thus, any modern evaluation of treatment options must include this technology. TCAR has been shown to result in lower stroke and death rates compared to TF-CAS in both high-risk and standard risk populations.3,4 Compared to CEA, TCAR has repeatedly demonstrated similar rates of stroke and death but with lower rates of myocardial
infarction (MI) and cranial nerve injury.5 TCAR has also been shown to be as safe as CEA and significantly safer than TFCAS in octogenarians.6-8
Results of other trials:
The stroke rate for TF-CAS has been reported to be twice that of CEA in nearly all randomized trials preceding CREST-2, with statistically significant differences most consistently observed in symptomatic patients, who have higher baseline event rates. The asymptomatic trials were underpowered to detect a difference in stroke. When Strauss et al evaluated over 100,000 CEA, 50,000 TCAR, and 25,000 TF-CAS procedures, TF-CAS had a 50-90% higher stroke rate than CEA and TCAR, even in asymptomatic patients.9
Selective interventionalist and anatomic factors favoring TF-CAS in CREST-2:
There were notable differences in operator selection and anatomic considerations between TF-CAS and CEA. Potential interventionalists had to submit 100 TFCAS operative notes with at least 25 cases performed in the past year; only 50% of applicants were accepted. Potential surgeons had to submit 50 CEA operative notes over any time period; 90% of applicants were accepted. Exclusion criteria from the TFCAS arm included unfavorable anatomy or disease in inflow vessels (aortic arch imaging where the investigator believed the sheath, protection device, and stent could not be delivered safely, such as type 3 arch and especially in patients over 70 years; innominate or common carotid artery severe angulation, tortuosity, calcification, or stenosis) or in the internal carotid artery (circumferential calcification, lesions > 2 cm long). These exclusion factors would play a much less important, if any, role when considering CEA and TCAR.10,11
These stringent and uneven exclusion factors create a study population that differs meaningfully from real-world patients, making the results less applicable to routine clinical decision-making.
Learning curve of interventions: Multiple studies have demonstrated the long learning curve associated with TFCAS; at least 50-100 cases are required for early proficiency.12,13 The same has not been demonstrated with TCAR, where those performing their first cases had no increased risk of stroke or death compared to those with extensive experience.14 We have concerns that less experienced TF-CAS interventionalists will apply CREST-2 recommendations to a broad swath of asymptomatic patients without the same careful selection of low-risk anatomy. Also, resident involvement in both TCAR and CEA has not been demonstrated to increase adverse events, while the same has yet to be demonstrated for TF-CAS.15
Continued utility of CEA:
Depending on individual risk factors and anatomy, CEA is still appropriate for selected asymptomatic patients.1,2 Metaanalysis of several randomized trials showed superiority of CEA over TF-CAS in terms of stroke and death. Kakkos et al summarized nine randomized carotid trials and concluded that a stroke/death rate at 30-days was significantly higher for TF-CAS (2.9%) than CEA (1.9%, OR 1.6; p =.044); the 30-day stroke rate was significantly higher for TF-CAS (2.9%) than CEA (1.8%, OR 1.6; p =.032); the 30-day MI rate was non-significantly lower for CAS (0.66%) vs CEA (1.5%, OR 0.5; p =.105); and the stroke/death rate at 30-days plus ipsilateral stroke during one year follow-up was significantly higher for TF-CAS (3.6%) than CEA (2.4%, OR 1.5; p =.04).16 Saratzis reported a meta-analysis of 6,659
patients in the four largest randomized controlled trials (ACT-1, ACST-2, CREST-1, SPACE-2) and noted the 30-day stroke/ death/MI rate was not significantly different between CAS and CEA (3.5% vs 3.1%; OR 1.18; p=0.25), but the 30-day “any” stroke rate was still higher after CAS (3.0% vs 1.95%; OR 1.61; p=0.0046), as was the 30-day stroke/death rate (3.1% vs 2.2%; OR 1.47; p=0.017).17 Once the perioperative period had elapsed, the four RCTs documented that ipsilateral strokes were very low after CAS or CEA (0.4-0.5/yr after TF-CAS and 0.2-0.5/yr after CEA). Recently the Asymptomatic Carotid Surgery Trial (ACST-2) reported a similar disabling stroke/death prevention rate between CEA and TF-CAS but noted a much higher number of minor strokes in TF-CAS compared to CEA subgroups (48 vs 29).18
Different outcomes in each medical arm:
CREST-2 was not designed to compare TFCAS vs. CEA since there were two separate medical arms. Of note, the medical arm of the TF-CAS study had 6.0% stroke and death rate at 4 years in contrast to 5.2% in the surgical arm patients who had medical therapy. If the same patients in the medical arm of the TF-CAS study were used compared to the CEA patients, the difference might have been more significant. At the interim analysis, the CEA arm showed more favorable outcomes than TF-CAS. However, there were six late stroke events in the CEA arm 2-4 years post op that were unrelated
to the procedure or carotid re-stenosis or re-intervention. Because these strokes occurred years after surgery and were not linked to re-stenosis or reinterventions, it is difficult to understand how they meaningfully reflect the comparative performance of the treatment options. Moreover, with event rates this low, even a small number of unrelated outcomes can disproportionately influence the apparent differences between treatment arms.
Limitations of each intervention:
TF-CAS, TCAR, and CEA each has their own limitations and drawbacks.10
Carotid stenting with either TF-CAS or TCAR is less favorable with heavy calcification, angulation, or tortuosity of the ICA compared to CEA. TF-CAS may be contraindicated or pose higher risk for diseased, tortuous, or angulated aortic arch inflow vessels. TCAR is less favorable if there is a low carotid bifurcation or disease at the common carotid puncture site. CEA is less favorable when there is severe cardiac or pulmonary disease, neck radiation, prior major neck surgery, very cephalad lesions, cervical spine immobility, contralateral vocal cord paralysis, and possibly contralateral internal carotid artery occlusion. These strengths and weaknesses underscore the value of having all revascularization strategies available, allowing clinicians to match each patient with the modality best suited to their anatomy, risk profile, and goals.
Conclusions:
Carotid interventions are perhaps the most widely studied of all medical procedures. While CREST-2 certainly adds to this abundance of data, the results are not so overwhelming as to cast aside our wealth of accumulated knowledge. We therefore wish to emphasize that the findings and recommendations in CREST-2 do not change the standard of care. We agree with the CREST-2 findings that medical management of all patients with carotid disease should be optimized and that TF-CAS procedures performed by highly trained, experienced interventionalists in carefully chosen patients may be appropriate treatment. However, TCAR and CEA continue to play an important role in appropriately selected patients with asymptomatic carotid disease.
References
1. AbuRahma AF, Avgerinos ED, Chang RW, Darling RC 3rd, Duncan AA, Forbes TL, Malas MB, Murad MH, Perler BA, Powell RJ, Rockman CB, Zhou W. Society for Vascular Surgery clinical practice guidelines for management of extracranial cerebrovascular disease. J Vasc Surg. 2022;75(1S):4S-22S.
2. Poorthuis MHF, Solomon Y, Herings RAR, Visseren FLJ, Kappelle LJ, Bots ML, Rissanen I, de Borst GJ. Temporal Trends and Determinants of Stroke Risk in Patients with Medically Treated Asymptomatic Carotid Stenosis. Stroke. 2023 Jul;54(7):1735-1749.
3. Schermerhorn ML, Liang P, Eldrup-Jorgensen J, Cronenwett JL, Nolan BW, Kashyap VS, Wang GJ, Motaganahalli RL, Malas MB. Association of Transcarotid Artery Revascularization vs Transfemoral Carotid Artery Stenting With Stroke or Death Among Patients with Carotid Artery Stenosis. JAMA 2019;322:2313-2322.
4. Liang P, Cronenwett JL, Secemsky EA, Eldrup-Jorgensen J, Malas MB, Wang GJ, Nolan BW, Kashyap VS, Motaganahalli RL, Schermerhorn ML. Risk of Stroke, Death, and Myocardial Infarction Following Transcarotid Artery Revascularization vs Carotid Endarterectomy in Patients with Standard Surgical Risk. JAMA Neurol. 2023;80:437-444.
5. Malas MB, Dakour-Aridi H, Kashyap VS, Eldrup-Jorgensen J, Wang GJ, Motaganahalli RL, Cronenwett JL, Schermerhorn ML. TransCarotid Revascularization with Dynamic Flow Reversal Versus Carotid Endarterectomy in the Vascular Quality Initiative Surveillance Project. Ann Surg 2022;276:398-403.
6. Malas MD, Elsayed N, Naazie I, Dakour-Aridi H, Yei KS, Schermerhorn ML. Propensity score-matched analysis of 1-year outcomes of transcarotid revascularization
with dynamic flow reversal, carotid endarterectomy, and transfemoral carotid artery stenting. J Vasc Surg 2022;75:213-22.
7.Naazie IN, Cui CL, Osaghae I, Murad MH, Schermerhorn M, Malas MB. A Systematic Review and Meta-Analysis of Transcarotid Artery Revascularization with Dynamic Flow Reversal Versus Transfemoral Carotid Artery Stenting and Carotid Endarterectomy. Ann Vasc Surg 2020;69:426-436.
8. Mehta A, Patel PB, Bajakian D, Schutzer R, Morrissey N, Malas M, Schermerhorn M, Patel VI. Transcarotid artery revascularization versus carotid endarterectomy and transfemoral stenting in octogenarians. J Vasc Surg 2021;74:1602-1608.
9. Straus S, Yadavalli SD, Allievi S, Sanders A, Davis RB, Malas MB, Wang GJ, Kashyap VS, Cronenwett J, Motaganahalli RL, Nolan B, Eldrup-Jorgensen J, Schermerhorn M. Seven years of the transcarotid artery revascularization surveillance project, comparison to transfemoral stenting and endarterectomy. J Vasc Surg 2024;80:1455-1463.
10. AbuRahma AF, Avgerinos ED, Chang RW, Darling RC 3rd, Duncan AA, Forbes TL, Malas MB, Perler BA, Powell RJ, Rockman CB, Zhou W. The Society for Vascular Surgery implementation document for management of extracranial cerebrovascular disease. J Vasc Surg. 2022 Jan;75(1S):26S-98S.
11. Howard VJ, Meschia JF, Lal BK, Turan TN, Roubin GS, Brown RD Jr, Voeks JH, Barrett KM, Demaerschalk BM, Huston J 3rd, Lazar RM, Moore WS, Wadley VG, Chaturvedi S, Moy CS, Chimowitz M, Howard G, Brott TG; CREST-2 study investigators. Carotid revascularization and medical management for asymptomatic carotid stenosis: Protocol of the CREST-2 clinical trials. Int J Stroke 2017;12:770-778.
12. Gray, W.A. ∙ Rosenfield, K.A. ∙ Jaff, M.R. Influence of site and operator characteristics on carotid artery stent outcomes: analysis of the CAPTURE 2 (Carotid ACCULINK/ACCUNET Post Approval Trial to Uncover Rare Events) clinical study. JACC Cardiovasc Interv. 2011; 4:235-246.
13. Jabbour G, Yadavalli SD, Straus S, Sanders AP, Rastogi V, Eldrup-Jorgensen J, Powell RJ, Davis RB, Schermerhorn ML. Learning curve of transfemoral carotid artery stenting in the Vascular Quality Initiative registry. J Vasc Surg 2024;80:138-150.
14. Kashyap VS, King AH, Liang P, Eldrup-Jorgensen J, Wang GJ, Malas MB, Nolan BW, Cronenwett JL, Schermerhorn ML. Learning Curve for Surgeons Adopting Trans-carotid Artery Revascularization Based on the Vascular Quality Initiative-Trans-carotid Artery Revascularization Surveillance Project. J Am Coll Surg. 2020 Jan;230(1):113-120.
15. Cremonesi A, Setacci C, Bignamini A. Carotid artery stenting: first Consensus document of the ICCS-SPREAD joint committee. Stroke. 2006; 37:2400-2409.
16. Kakkos SK, Kakisis I, Tsolakis IA, Geroulakos G. Endarterectomy achieves lower stroke and death rates compared with stenting in patients with asymptomatic carotid stenosis. J Vasc Surg. 2017 Aug;66(2):607-617.
17. Saratzis A, Naylor R. 30 Day Outcomes After Carotid Interventions: An Updated Meta-analysis of Randomized Controlled Trials in Asymptomatic Patients. Eur J Vasc Endovasc Surg. 2022 Jan;63(1):157-158.
18. Halliday A, Bulbulia R, Bonati LH, Chester J, CradduckBamford A, Peto R, Pan H; ACST-2 Collaborative Group. Second asymptomatic carotid surgery trial (ACST-2): a randomized comparison of carotid artery stenting versus carotid endarterectomy. Lancet. 2021 Sep 18;398(10305):1065-1073.





Compiled by Marlén Gomez
DEADLINE NEARS FOR SVS FOUNDATION RESEARCH AWARD
The Society for Vascular Surgery (SVS) Foundation is accepting submissions for two major research awards that advance vascular science and support early-career physicians.
The James S.T. Yao Resident Research Award honors publication-quality, original scientific work by physicians early in their training. Eligible research should focus on the biology of vascular disease and potential translational therapies and must be unpublished in manuscript form. The deadline for the award is Jan. 12 at 11:59 p.m. Central Time. The SVS Research Council will select one recipient to present their work during a Scientific Session at the 2026 Vascular Annual Meeting (VAM). The award includes $5,000 and a one-year complimentary subscription to the Journal of Vascular Surgery (JVS). Details are available at vascular.org/yaoaward.
The Clinical Research Seed Grant supports patient-oriented clinical research projects with potential for larger future funding. This one-year, $25,000 grant is available to earlycareer vascular surgeons. Eligible projects include clinical trials, ancillary studies, mechanism-focused research, diagnostic tool development and initiatives addressing care disparities. Applications are due March 1 at 11:59 p.m. Central Time. Learn more at vascular.org/seedgrant
Register for the Complex Wound Care Masterclass

REGISTRATION FOR THE “COMPLEX Wound Care Masterclass Workshop
2026: Debridement, Dressing, and Oxygen Therapy” opens on Feb. 10. The Society for Vascular Surgery (SVS), in collaboration with the Society for Vascular Nursing (SVN) and the American Podiatric Medical Association (APMA), developed this program to offer an interprofessional wound care curriculum designed specifically for vascular care teams. The course consists of an online module featuring 27 instructional videos, along with a hands-on workshop scheduled for Friday, June 12, coinciding with the Vascular Annual Meeting (VAM).
To learn more, visit vascular.org/woundcare.
SVS INTRODUCES FREE QUALITY IMPROVEMENT CONSULTING PROGRAM
THE SOCIETY FOR VASCULAR SURGERY (SVS) HAS LAUNCHED THE Quality Improvement (QI) Consulting Program, a new initiative designed to help members develop and manage quality improvement projects. The program is offered through the SVS Quality Improvement Committee (QIC) and is available at no cost to members.
The QI Consulting Program guides at every stage of a quality improvement project. The program includes assistance with getting started, troubleshooting challenges and sharing project outcomes. The goal is to offer expert feedback and support as members navigate an evolving healthcare environment and meet regulatory requirements.
The program can help members begin projects by developing problem statements, identifying stakeholders, selecting measures and creating project charts. It also offers advice on project management, such as choosing a QI methodology, organizing timelines and developing communication plans.
Members can receive guidance on defining success by establishing process measures, tracking interventions and displaying data for team review. Consultants can also assist with troubleshooting when interventions do not work as expected and improvement is still needed. The program also helps members amplify success by creating dissemination plans and preparing for presentations or publications.
The QI Consulting Program does not include data analysis, complete project mentorship or formal QI instruction.
The QIC will accept applications during the first two weeks of each month and will select up to five projects at a time. Fellows and residents may participate in the program, but their attending physician must submit the application and be an active SVS member in good standing.
For more information or to apply, visit vascular.org/QI-Consulting
SVS compensation study closes Jan. 31
AS THE NEW YEAR BEGINS, MEMBERS OF THE SOCIETY FOR VASCULAR Surgery (SVS) have until Jan. 31 to participate in the SVS Compensation Study, a 15-minute survey designed to provide enhanced power-searching capabilities, comparative functionality and expanded career reach.
The study, conducted in collaboration with Phairify — a web-based data collection and visualization platform — requires members to enter their 2023 financial information. In February, data collection for the 2024 study will begin.
The initiative aims to help SVS members make informed career decisions by offering exclusive access to detailed information specific to their specialty and practice situations. The survey covers a wide range of topics, including compensation, call frequency, productivity, bonuses, benefits and practice settings.
SVS launched the compensation study in 2023 in response to member requests for greater transparency and data-driven insights into vascular surgery compensation. The study is an SVS member benefit and is fully anonymous, allowing participants to provide information without privacy concerns.
Members who previously participated are encouraged to log back in and update their data for 2024.
Those interested in participating or updating their information can visit vascular.org/compensation
LATE-BREAKING ABSTRACTS RETURN FOR VAM26
The Vascular Annual Meeting (VAM) will again feature late-breaking abstracts, offering researchers a chance to present the latest findings in clinical and nonclinical science. These abstracts highlight cutting-edge data and innovative studies that bring timely insights to the forefront of the program. The submission window runs from Feb. 4 to March 2. VAM26 provides multiple opportunities to share work, ideas and research, including education sessions, posters and named lectures.
To learn more, visit vascular.org/VAM.
SVS membership renewal ensures continued access, benefits
Society for Vascular Surgery (SVS) member dues were due Dec. 31. SVS members are encouraged to renew their memberships to maintain uninterrupted access to the Journal of Vascular Surgery (JVS) portfolio, exclusive discounts on events, educational programs and meetings, and SVS-led communications such as Vascular Specialist. Renewal also provides ongoing networking opportunities through SVS Sections and SVSConnect. Membership dues provide members with access to the SVS’s national branding campaign, Highway to Health, which promotes the visibility of vascular surgery among patients, referring providers and health system leaders.
To renew, visit vascular.org/join
VESAP6 KEY TO CERTIFICATION FOR VASCULAR SURGEONS
Start the new year by investing in your professional growth with the sixth edition of the Vascular Education and Self-Assessment Program (VESAP6) from the Society for Vascular Surgery (SVS). This comprehensive online resource offers more than 600 questions, detailed rationales and references across multiple modules, an essential tool for vascular specialists committed to lifelong learning. VESAP6 is a digital aid for vascular surgeons in preparing for qualifying, certification and recertification examinations and to remain current in the specialty of vascular surgery and endovascular therapy. The program continues to meet Continuing Medical Education (CME) credit/maintenance of certification (MOC) requirements of the American Board of Surgery (ABS) in Vascular Surgery and provides AMA PRA Category 1 Credits™ with self-assessment. VESAP6 also supports the Registered Physician in Vascular Interpretation (RPVI) certification and recertification through dedicated Vascular Lab modules.
Available in both desktop and mobile formats, the program includes modules on critical topics such as aortoiliac disease, cerebrovascular disease, dialysis access management, radiation safety, renal and mesenteric vascular disease, upper and lower extremity vascular disease and more. VESAP6 will expire on March 26, 2027.
Learn more at vascular.org/VESAP.
COMMENT& ANALYSIS
Phaedro’s dog and Dr. Oz: Reclaiming physician leadership in health care
By Arthur E. Palamara, MD, FACS
THE NOVEL I, CLAUDIUS, IS A HISTORICAL fiction written by Robert Graves in 1934. Daily life amidst Rome’s political decay during the despotic regimes of Augustus, Tiberius and Caligula is richly described. Claudius’ grandmother was the sinister Livia who manipulated these figures to secure her own power and aspired to become a goddess. Regretfully for her, Livia never achieved that status but was nevertheless named Queen of Heaven. Since she killed most of her adversaries, the threshold for becoming a celestial queen, back then appears rather low.
Although unwilling to become emperor, Claudius agreed only to save his wife and unborn child. It is no less than a miracle since — as a child — he survived malaria, colitis, rashes, and walked with a limp, from him we derive the word claudication. But this essay is not about the Emperor Claudius nor the politically unsettled time of the darkening Roman Republic, but about a parable contained within the novel: a story that may have bearing on today’s medical dystopia.

The dog was so trusted that his master sent him to the meat market to fetch a package of meat and return it to his master. He had such confidence that the dog would never betray his trust. The master gazed from his window watching in horror as his dog was beset by a pack of mongrels. He realized immediately that his faithful dog never had a chance to protect the meat. As the scuffle ensued, Phaedro observed his dog emerge from the scuffle with a large piece of meat which the dog began to eat and finish on the spot while the pack continued to squabble. When the dog arrived home, Phaedro did not castigate the animal for eating the meat but praised him for his intelligence, successfully dealing with a horrific situation over which he had no control.
the price of the same medication manufactured and shipped from Europe is four times the price when sold in the United States.” President Trump was congratulated for using his negotiating skills to compel the industry to lower prices.
– He did not mention what was going to happen to the patients in the Affordable Care Act who are going to face stiff increases in their premiums next month. (His speech was given before President Trump floated the idea of continuing the financial supplements/tax credits for another two years.)
– He did not mention the anticipated 6.7% increase in health care insurance premiums anticipated for 2026.
“Since health care cannot exist without doctors, it appears the moment has arrived for us to reassume our leadership role."
In 1988, I wrote an essay for the Broward County Medical Association RECORD describing the insidious deterioration of health care that was slowly enveloping our profession. HMOs were becoming popular as non-medical financiers learned how to enrich themselves at patient/physician’ expense. Then, as now, everything bad in health care has its origins in South Florida. The paramount example is IMC, International Medical Centers, whose CEO Miguel Recarey Jr. swindled Medicare and Medicaid out of $781 million dollars intended to provide care for 197,000 enrollers but failed to pay doctors. Although later indicted by the Department of Justice, he fled to Spain with $300-400 million missing. He was arrested in Spain but was never extradited to the United States. Some very high-level politicians sighed a great sigh of great relief. Without question, Mr. Recarey and others were harbingers of things to come and with it, the dethroning of physicians from our august position as leaders in health care.
ARTHUR E. PALAMARA, MD, FACS
On November 17, at the 2025 Interim Meeting of the American Medical Association, delegates had the opportunity to listen to a speech from CMS Administrator Mehmet Oz. Well aware that deeply held feeling concerning the current administration existed, delegates were warned that inappropriate conduct would not be tolerated. Security was tight and guards in dark clothing were positioned around the room. As it turned out, none were needed. The crowd of physicians was polite. Dr. Oz spoke physician to physician, glumly presenting a realistic description of the decomposing status of American health care. Among the highlights:
– Medicaid: CMS estimates that 6.1 million out of 20 million people could work but don’t(?)
– He mentioned (twice!) that South Florida is the capital for Medicare/Insurance fraud in the United States.
– There are too many people on the Affordable Care Act. At least a quarter never use it. (Surprisingly, all of us have automobile insurance but hope never to use it. Perhaps he meant that insureds don’t go in for annual wellness examinations?)
– There are too many codes in ICD-10.
– His solution for the prior-authorizations scourge is to give Gold Cards to 50% of the doctors who deliver medically necessary care/procedures. (The implication suggests that 50% of physicians fail to practice according to the standards of their specialty.)
– He did not mention President Tump’s accusing the insurance industry of charging too much and reaping enormous profits. He did offer that the current administration prefers negotiation rather than other forms of pressure.
– His concluding argument is that doctors need to play a more assertive (my word) role in health care as we seek solutions. He felt that we need to create a more “Quality Driven Payment System,” and the MIPS was not working.
– Lastly, he feels that expanding Accountable Care Organizations is a potential solution.
Dr. Oz coming to the American Medical Association suggests that the administration is keenly aware that our current health care system is unsustainable and would have physicians become more engaged in achieving the solution.
Regretfully, health care does not appear to be among the president’s priorities.
Getting back to Phaedo, his intelligent pup slipped out of the pack leaving the remaining cubs to fight among themselves. Since health care cannot exist without doctors, it appears the moment has arrived for us to reassume our leadership role. It has taken 37 years, but a cascade of events exposes our opportunity to reassume our position as stewards of the profession.
It will be challenging, often painful and confrontational, but the rewards great. Nor is it a coincidence that the most successful hospital systems in the country have doctors with major leadership roles. Instead of tinkering around the edges, doctors need to take the helm. Before it is imposed on us by others with less integrity.
We may have to “bark” a little, but it will be worth it.
(Examples are too numerous to site.)
Back to ancient Rome: Phaedro was a rich nobleman who lived in the internecine world of brutal Roman politics in the first century AD. He had a dog, a very faithful, honest, obedient animal representing qualities obviously not shared by leading Romans of his day.
– Doctors are retiring at age 61. He opined that doctors working an additional 3 years would reduce health care expenditures $1 trillion.
– He mentioned CMS successful negotiations with the pharmaceutical industry bringing the cost of GLP-1 inhibitors down to reasonable levels. “It is wrong that
ARTHUR PALAMARA is a vascular surgeon practicing in Hollywood, Florida. He is active in county, state and national medical organizations.
COMMENT& ANALYSIS
THE OUTPATIENT
A CRITICAL MOMENT FOR PHYSICIAN PAYMENT: WHAT VASCULAR SURGEONS NEED TO KNOW
By Joe Haurani, MD and Chinmaya Shelgikar, MD
THE 2026 MEDICARE PHYSICIAN FEE SCHEDULE finalized on Oct. 31 represents more than a routine payment update. The introduction of a 2.5% “efficiency adjustment” coincides with broader Congressional and administrative scrutiny of how physician services are valued under Medicare. Understanding these converging forces is essential for vascular surgeons who want to influence the future of payment policy.
The immediate ask is simple: visit https://vascular.org/advocacy/grassroots-advocacy to send a message to your representatives. It takes 30 seconds. But the larger issue deserves your attention — we’re facing a potential restructuring of the entire physician payment system.
Three converging policy developments
The efficiency adjustment

CMS implemented a 2.5% reduction in work RVUs for nearly all non-time-based codes, premised on the assumption that surgical procedures have become more efficient over time. This adjustment will recur every three years with no established floor.
The evidence suggests otherwise. A 2025 Journal of the American College of Surgeons study analyzed 1.7 million operations across 249 CPT codes and 11 surgical specialties. The findings: 90% of CPT codes had the same or longer operative times in 2023 compared to 2019, with overall times increasing by 3.1%.
For vascular surgery specifically, the migration of straightforward cases to endovascular approaches means patients requiring open bypass or aneurysm repair now represent a more complex cohort. Add endemic OR staffing challenges, supply chain disruptions, and scheduling constraints, and the assumption of universal efficiency gains becomes difficult to support.
For employed surgeons with RVU-based compensation — which represents a growing majority — this adjustment directly affects personal income
Upcoming programming for medical students, residents and fellows CORNER STITCH
By Saranya Sundaram, MD
A warm welcome all to 2026! To start off the new year, we wanted to provide a list of programming, scholarships and events coming up this year. Though the deadlines for some of the events earlier in the year have passed, most of these events occur on an annual basis, so keep an eye out for details on how to apply for the next year’s conference! Please note that this is not a comprehensive list.
without a corresponding reduction in workload or complexity.
Congressional investigation of the AMA/RUC system
Sen. Bill Cassidy, chairman of the Senate Health, Education, Labor and Pensions Committee, has requested information from the American Medical Association regarding CPT code development, licensing fees, and the organization’s influence on Medicare payment rates. Cassidy provided a Dec. 15 deadline and indicated willingness to use additional investigative tools if voluntary cooperation is insufficient.
On Dec. 9, Cassidy expanded this inquiry by launching a questionnaire for healthcare providers, payers, and health IT companies to document how CPT licensing fees and royalty structures affect their operations.
The RUC (Relative Value Scale Update Committee) is the primary mechanism through which specialty societies provide input to CMS on the relative value of physician services. Questions about its future create uncertainty about how physician input will be incorporated into payment decisions going forward.
Administrative plans for payment reform
Health and Human Services Secretary Robert F. Kennedy Jr. has indicated interest in reforming Medicare’s physician payment structure, with particular focus on shifting resources from procedural services toward chronic disease prevention and management. Reports suggest Kennedy is exploring options to reduce the AMA’s role in determining Medicare payments, potentially transferring more authority directly to CMS. Kennedy has raised concerns about transparency and CMS oversight of RUC operations, as well as broader questions about whether the current system appropriately balances incentives between specialized procedures and primary care services.
Why these developments matter
These three initiatives — CMS’s efficiency adjustment, Congressional investigation, and administrative reform proposals — appear coordinated in timing if not in explicit collaboration. Multiple stakeholders have identified similar concerns about the current payment system, which suggests momentum for change.
The challenge for surgical specialties is ensuring that reforms address legitimate structural problems (lack of inflation adjustment since 1992, budget neutrality pitting specialties against each other) rather than simply
Events (open attendance)
Vascular Annual Meeting Residency and Fellowship Fair
Who: Medical students and general surgery residents interested in applying to either an integrated vascular surgery residency or an accredited vascular surgery fellowship
When: Friday, June, 12 2026 (Vascular Annual Meeting)
Details: Must register for the vascular annual meeting to attend
Journal of Vascular Surgery Online Journal Club (Virtual)
Who: Vascular surgery trainees, all interested in vascular surgery are welcome to attend
When: Second week of each month
Details: https://vascular.org/vascular-specialists/ research/journals/jvs-online-journal-club
redistributing a fixed pool based on assumptions that don’t match clinical reality.
The efficiency adjustment represents payment policy that contradicts empirical data, particularly the JACS study showing increased operative times. While primary care services are largely exempt, the policy risks creating further divisions between primary care and specialty physicians rather than addressing the broader drivers of Medicare spending growth — administration, pharmaceuticals, and facility fees.
The efficiency adjustment combined with the 50% reduction in indirect practice expense for hospitalbased services means facility-based procedures face approximately 7% payment reductions. For vascular surgeons who perform significant work in hospital settings, this creates compounding financial pressure.
The path forward

The Medicare physician payment system is entering a period of significant scrutiny and potential reform. This creates both risk and opportunity. The risk is that changes occur without adequate input from surgical specialties, particularly smaller fields like vascular surgery. The opportunity is to help shape reforms that address legitimate structural problems while maintaining appropriate valuation for complex surgical care.
Our RUC representatives have consistently advocated effectively for vascular surgery. They need grassroots support to maximize impact during this critical period. Take 30 seconds today to complete the Voter Voice. More importantly, continue to stay engaged whether you agree or not, your opinions and voice help shape our society’s future. Consider what additional contributions you can make — sharing practice data, responding to stakeholder inquiries, or identifying codes needing revision.
The efficiency adjustment took effect January 1, 2026. Congressional and administrative reviews of the broader payment system are ongoing. The window for input is narrow. Whether you view current developments as concerning or see potential for constructive reform, active participation in the policy process is essential.
JOE HAURANI is a vascular surgeon and a professor in the division of vascular surgery at East Carolina University. CHINMAYA SHELGIKAR is a vascular surgeon at Trinity Health IHA Medical Group in Ypsilanti, Michigan.
Meeting-based programs/ travel awards
Pacific Northwest Endovascular Conference Simulation Summit for Vascular Trainees
Who: Senior cardiothoracic fellows, peripheral intervention fellows, vascular fellows, and PGY-5 integrated vascular residents
When: Applications will reopen in winter of 2026
Midwest Vascular Surgery Society Technology & Technique Vascular Simulation Program
Who: Vascular surgery fellows or integrated vascular surgery residents, priority is given to those in their final years of training
When: Applications will reopen fall of
2026, typically due in August
SVS General Surgery Resident/Medical Student VAM Travel Scholarship
Who: Medical students and general surgery residents with an interest in vascular surgery by facilitating their attendance at the 2026 SVS Vascular Annual Meeting (VAM)
Deadline: Applications will reopen in summer of 2026, typically due in September
Southern Association for Vascular Surgery Sizing Showdown & Hands-on Course
Who: Current Vascular trainees, preference given to those in programs within SAVS region
Deadline: Applications will reopen in summer of 2026, typically due in November
Joe Haurani, MD
Chinmaya Shelgikar, MD
Vascular & Endovascular Surgical Society Vascular Fellows Program
Who: current Vascular trainees, preference given to senior residents/fellows
Deadline: Applications will reopen in summer of 2026, typically due in November Society for Clinical Vascular Surgery Fellow & Chiefs or Rising Seniors Residents Program
Who: current Vascular trainees, either rising to their final years or in their final year Deadline: Applications will reopen in summer of 2026, typically due in November
Awards/fellowships
James S.T. Yao Resident Research Award (SVS Foundation)
Description: “The James S.T. Yao Resident Research Award is designed to provide special recognition of publicationquality original scientific work that has been unpublished in manuscript form. The recognition includes a VAM Scientific Session presentation before the membership of the Society for Vascular Surgery (SVS), a $5,000 award and a one-
year complimentary subscription to the Journal of Vascular Surgery.”
Deadline: Jan. 26, 2026, 11:59pm CST
Details: https://vascular.org/svsfoundation/programs-and-awards/jamesst-yao-resident-research-award Student Research Fellowship (SVS Foundation)
Description: “The SVS Foundation Student Research Fellowship stimulates laboratory and clinical vascular research by undergraduate college students and medical school students registered at universities in the United States and Canada. The intent of the fellowship award is to further the student’s education and introduce the student to the application of rigorous scientific methods to clinical problems and underlying biologic processes important to patients with vascular disease… Each fellowship consists of a $3,000 award and a one-year complimentary subscription to the Journal of Vascular Surgery.”
Deadline: Feb. 1, 2026, 11:59pm CST
Details: https://vascular.org/svs-
CLINICAL&DEVICENEWS
Compiled by Killian Meara
Fluidx completes enrollment for pivotal trial evaluating GPX embolic device
A pivotal trial evaluating the safety and efficacy of the GPX embolic device for peripheral vascular embolization has completed enrollment, Fluidx Medical technology announced in a release.
The prospective, multicenter, multinational, investigational device exemption (IDE) study enrolled 114 patients across 18 sites in the United States, Canada and New Zealand. In the trial, GPX was delivered through over 20 different microcatheter configurations and demonstrated broad compatibility across a wide range of commonly used delivery devices.
Fluidx previously announced results of a prospective, single-arm, open-label, multicenter, early feasibility study of the GPX device in May 2024. The trial, which was a first-in-human study, showed the device achieved 100% technical success and high usability scores from physicians for ease of preparation, deliverability, and visibility. The study was published in the Journal of Vascular and Interventional Radiology (JVIR)
“Completing enrollment is a critical milestone for the study, and we thank the investigators and patients who made it possible”, said Michael Darcy, MD, professor of radiology at Washington University and national principal investigator on the study. “If the GPX trial can confirm the positive results of the earlier study published in JVIR, it could help establish GPX as an important new tool in embolic therapy. We look forward to sharing this data with the interventional community.”
FDA clears Bendit17 steerable microcatheter
The Food and Drug Administration (FDA) granted 510(k) clearance to the Bendit17 steerable microcatheter, Bendit Technologies said in a release. The approval makes the catheter the smallest available on the market.
The device provides enhanced steerability and precision that enables controlled navigation through complex anatomies while maintaining stability and control. It was designed for use in a wide range of vascular procedures.
"FDA clearance of the Bendit17 is a major milestone for our team and a meaningful advancement for clinicians seeking greater control and navigational precision in complex vascular procedures,” said Oz Cabiri, CEO of Bendit, in the release. “The device's capability to navigate with or without a guidewire represents a significant technological leap forward. Our mission is to push the boundaries of what is possible in endovascular care, and the Bendit17 embodies that vision.”
The company said the approval of Bendit17 “marks a significant step forward in advancing precision and accessibility in neurovascular and peripheral endovascular interventions.” It also said it is in the final stages of production and plans to initiate its first U.S. commercial clinical procedures in January 2026.
foundation/programs-and-awards/ student-research-fellowship VQI Fellowship in Training (FIT) Program (Vascular Quality Initiative)
Description: “A program designed to train young vascular surgeons, physicians and clinicians on ways to improve quality of care and patient outcomes using registry data is now preparing for its fourth cohort. The Society for Vascular Surgery Patient Safety Organization (SVS PSO) launched the Vascular Quality Initiative Fellowship in Training Program, or “VQI FIT,” in 2022 to foster a deeper understanding of vascular quality processes and metrics among residents and fellows”
Deadline/Details: For further information please contact Betsy Wymer, Director of Quality, at bwymer@svspso.org, Dr. Adam Johnson at adam.johnson@duke.edu, or Dr. Nikolaos Zacharias at nzacharias@ mgh.harvard.edu.
Vascular & Endovascular Surgical Society Resident Research Award
Description: “One $12,500 grant for
01: 4.5” x 5.625”
basic/translational science, educational, clinical or health outcomes research will be awarded during the VESS annual winter meeting. The VESS Resident Research Award is specifically designed to help residents in training initiate projects during protected academic development time that will lead to future academic potential toward extramural funding for basic or clinical research. Eligible candidates must identify with an accredited general or integrated vascular surgery residency program. Within the award application, along with a proposed academic development plan, a VESS Active Member must be identified as either the dedicated research mentor, sponsor or collaborative investigator on this project.”
Deadline/Details: Applications will reopen in spring of 2026, typically due in October. All required materials, in a single PDF document, are electronically submitted to vess@administrare.com.
GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surfacea
Consult Instructions for Use
eifu.goremedical.com
Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery de novo and restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 7.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery in-stent restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 6.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in iliac artery lesions up to 80 mm in length with reference vessel diameters ranging from 4.0 – 12 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is also indicated for the treatment of stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous (AV) access grafts. CONTRAINDICATIONS: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is contraindicated for non-compliant lesions where full expansion of an angioplasty balloon catheter was not achieved during pre-dilatation, or where lesions cannot be dilated sufficiently to allow passage of the delivery system. Do not use the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II.
aAs used by Gore, Heparin Bioactive Surface refers to Gore’s proprietary CBAS® Heparin Surface. Products listed may not be available in all markets. © 2025 W. L. Gore & Associates, Inc. All rights reserved. All trademarks referenced are trademarks of either a member of the Gore group of affiliated companies or their respective owners. “Together, improving life” mark and design are trademarks of a Gore company. 25PL1153-EN01 AUGUST 2025



OPTIMIZING ARTERIOVENOUS (AV) ACCESS MAINTENANCE OUTCOMES




















The VIABAHN® Device is guideline-aligned1 and data-backed to reduce reinterventions.2,3
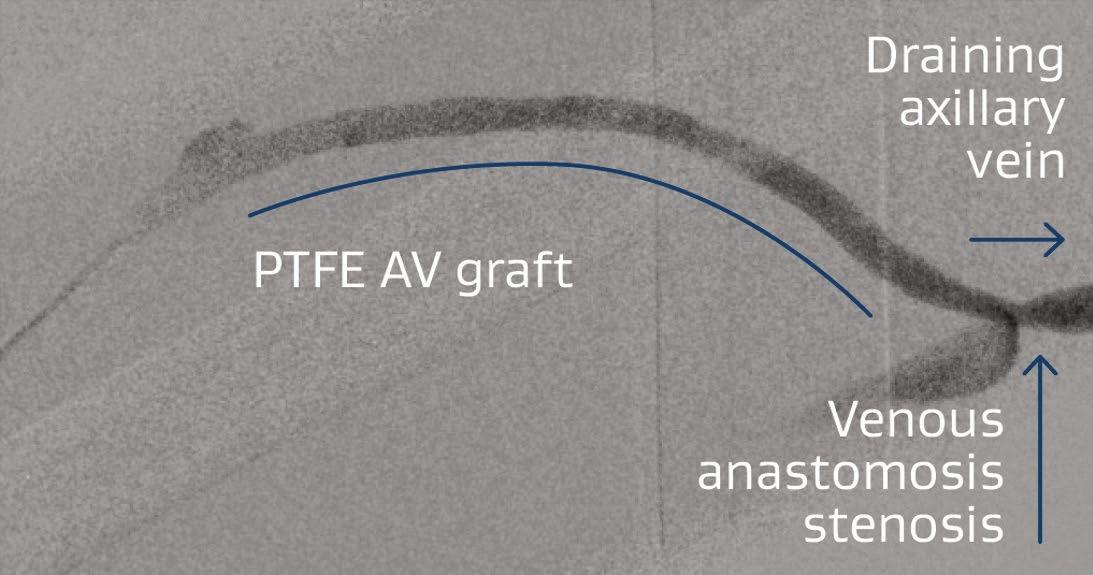
Right brachialaxillary AV graft with stenosis at the venous anastomosis. Lesion was initially treated with PTA.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
a As used by Gore, Heparin Bioactive Surface refers to Gore’s proprietary CBAS ® Heparin Surface.

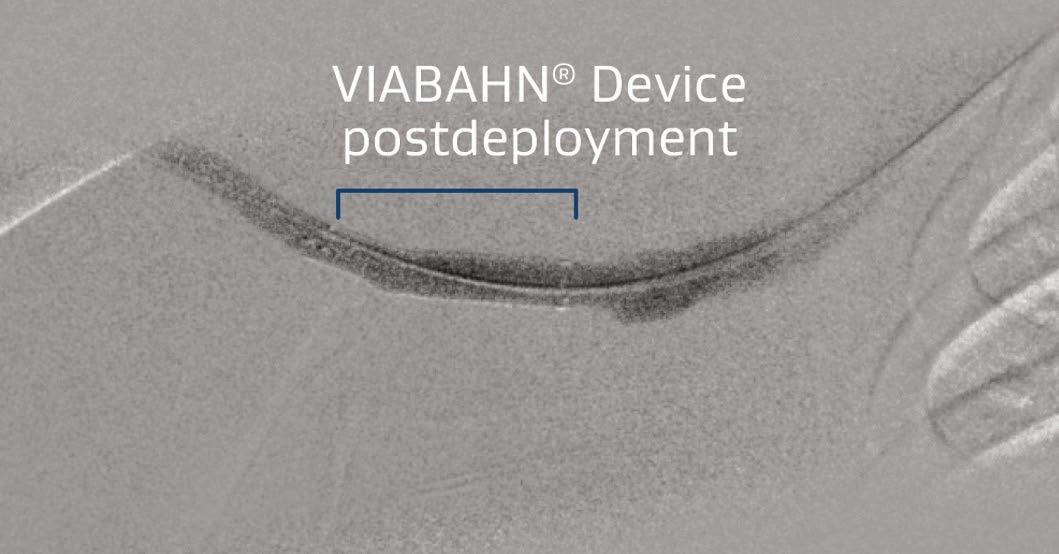
Placement of the VIABAHN® Device improved flow and resolution of recoil.
GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surfacea See the evidence Images courtesy of Daniel V. Patel, MD. Used with permission.
1. Lok CE, Huber TS, Lee T, et al; KDOQI Vascular Access Guideline Work Group. KDOQI Clinical Practice Guideline for Vascular Access: 2019 update. American Journal of Kidney Diseases 2020;75(4) Supplement 2:S1-S164. 2. Mohr BA, Sheen AL, Roy-Chaudhury P, Schultz SR, Aruny JE. REVISE Investigators. Clinical and economic benefi ts of stent grafts in dysfunctional and thrombosed hemodialysis access graft circuits in the REVISE Randomized Trial. Journal of Vascular & Interventional Radiology 2019;30(2):203-211.e4. 3. Vesely T, DaVanzo W, Behrend T, Dwyer A, Aruny J. Balloon angioplasty versus Viabahn stent graft for treatment of falling or thrombosed prosthetic hemodialysis grafts. Journal of Vascular Surgery 2016;64(5):1400-1410.e1.
Please see accompanying prescribing information in this journal. Products listed may not be available in all markets. © 2025 W. L. Gore & Associates, Inc. All rights reserved. All trademarks referenced are trademarks of either a member of the Gore group of affiliated companies or their
