THE RECENT REPORT OF AN ELEVATED risk of major amputation among patients treated with paclitaxel-coated balloons (PCBs) in the lower limbs has already seen a mixed reaction from professionals across the vascular specialty. In this special report, we hear from five expert vascular surgeons who discuss the implications of the findings made by interventional radiologist Konstantinos Katsanos, MD, and colleagues.
First, Jessica Simons, MD, Caitlin W. Hicks, MD, and Katharine McGinigle, MD, pore over the meta-analysis in question, commenting on the methodology Katsanos et al pursued, and discussing the reported results. Michael Conte, MD, and Joseph Mills, MD, also weigh in with analysis on the significance of the latest study ahead of results expected from ongoing clinical trials that look at drug-coated balloon usage in peripheral arterial disease (PAD).
FROM THE FLOOR
VAM 2021 structural changes prove hit with attendees
BY BETH BALES
It was an epic return: nearly 700 abstracts presented in six plenaries and several other forums; six concurrent sessions; six SVS breakfast sessions; three postgraduate courses; six “Ask the Experts” presentations; more than 1,000 in-person professional attendees; nearly 400 livestreaming registrants; 88 exhibitors in 154 booths; three presidents; two presidential addresses; and three annual meetings held in collaboration with each other.
THAT’S THE 2021 VASCULAR ANNUAL Meeting (VAM) by some of the numbers. But mere math can’t convey the contagious enthusiasm of participants who had waited more than two years for the chance to reconnect with colleagues and participate in education, networking and fun.
“People were extremely excited to be inperson again,” said Andres Schanzer, MD, cochair, with Matthew Eagleton, MD, of the SVS Program Committee, which oversees educational content at VAM—Schanzer chairs the committee for 2021–22. “I can’t tell you how many people
stopped one of us to tell us how happy they were to be there.”
This year’s meeting featured several important structural changes designed to minimize overlapping sessions and maximize the attendee experience. They included moving several sessions formerly held on Thursday to Wednesday, holding the three postgraduate courses on three different days, scheduling plenary sessions without conflicts, and offering a livestreaming option for those unable to travel.
Member reactions have proved the changes quite popular, said Schanzer. “Our at-home registrants really liked being able to watch the livestreamed sessions via their computers,” he said, adding that those watching remotely especially enjoyed being able to participate in live questions and answers via Zoom.
Spreading the educational content out across all four days was also a hit, with each day of the meeting wellattended. “People told us repeatedly they really liked
the structural changes, which was gratifying since it was a big change, and they were also very pleased with the educational content,” said Eagleton.
Because the 2021 meeting was moved from June to August, preparations are well under way for 2022. Both Eagleton and Schanzer urged attendees to provide their feedback on VAM 2021. “The changes we made for this year were the direct result of feedback from members,” Eagleton pointed out. “We can’t create the meeting members want without them telling us what would improve VAM.”
The presence of three presidents—current President Ali AbuRahma, MD, Immediate Past President Ronald L. Dalman, MD, and 2019–20 President Kim Hodgson, MD—reflected the transition of the SVS out from under the pandemic, adding extra energy to the meeting.
And then there is the all-important number 75: SVS leaders kicked off the year-long SVS 75th anniversary celebrations.
“The staff of the SVS is truly honored to serve our members and really went above and beyond to convene a successful, effective and safe VAM 2021,” noted
Kenneth M. Slaw, PhD, SVS executive director. “The synergy between our member-leaders and staff was extraordinary.”
For more information on VAM, visit vascular.org/VAM.
VASCULAR SPECIALIST
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD, Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Marie Drudi, MD
Executive Director SVS Kenneth M. Slaw, PhD
Director of Membership, Marketing and Communications Tara J. Spiess, CAE
Managing Editor SVS Beth Bales
Marketing & Membership Specialist Anna Vecchio
Assistant Marketing & Social Media Manager
Kristin Crowe
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA Publishing. Content for the News From SVS is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA Publishing will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein.
The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com.
For missing issue claims, e-mail subscriptions@bibamedical.com.
Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA Publishing.
Published by BIBA Publishing, which is a subsidiary of BIBA Medical Ltd.
Publisher Roger Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Jocelyn Hudson, Will Date, Jamie Bell and Anthony Strzalek
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe 526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America 155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Left to right: Ali AbuRahma, Ronald L. Dalman and Kim Hodgson
Inset: Andres Schanzer (left) and Matthew Eagleton
BY MALACHI SHEAHAN III
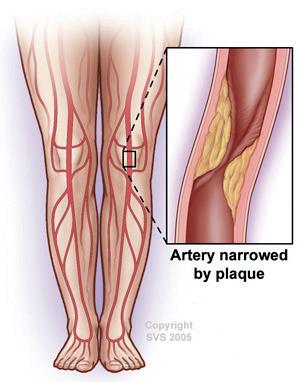
A recent meta-analysis by Konstantinos Katsanos, MD, of Patras University Hospital, Rion, Greece, and colleagues—“Risk of major amputation following application of paclitaxel-coated balloons [PCBs] in the lower-limb arteries: A systematic review and meta-analysis of randomized controlled trials [RCTs],” published in the European Journal of Vascular and Endovascular Surgery (EJVES)—warns of a possible heightened risk of major amputation after the use of PCBs in lower-extremity arteries. Vascular Specialist asked some of our nation’s leaders in the care of peripheral vascular disease to comment on the clinical implications of this study.
Jessica Simons, MD, associate professor, University of Massachusetts Medical School, Worcester, Masachussetts
Katsanos and colleagues conducted a systematic review and meta-analysis of existing data from RCTs on the effect of PCB use (in the femoropopliteal and infrapopliteal segments) on major amputation.
Using an incredibly rigorous methodology, they found compelling evidence for an increased hazard of major amputation associated with paclitaxel drug-coated balloons (DCBs) compared with plain balloon angioplasty. This effect was more pronounced among limbs treated for chronic limb-threatening ischemia (CLTI) as compared with intermittent claudication; among CLTI patients, they calculated a numberneeded-to-harm of 35 limbs.
Katsanos and colleagues demonstrated a dose-response effect. They posited a plausible biologic mechanism, including a contrast with drug-eluting stents. They concluded by saying that further investigation into the benefits and risks of paclitaxel DCBs are needed. To me, the primary question that remains is: Do we really need more studies?
As I have read the evidence supporting paclitaxel DCBs, none of it has ever been strong enough to mitigate these more recent findings. Prior to this particular study, I could have imagined some CLTI patients in whom there could be some limited role, since that group is often focused on limb salvage rather than survival. But this new analysis compels me that there is neither benefit.
PCD s Panel of vascular surgeons review latest findings on paclitaxel-coated balloons
Caitlin W. Hicks, MD, associate professor, Johns Hopkins Hospital, Baltimore, Maryland
The newest meta-analysis of PCBs by Kastanos et al, published in EJVES last month, raises concern about the use of DCBs for the treatment of peripheral arterial disease (PAD) for the second time in three years, this time with respect to major amputation risk. While the first meta-analysis, published in the Journal of the American Heart Association (JAHA) in 2018, focused on PCBs and stents, the newest meta-analysis on the topic is specific to DCBs. Similar to the original article, my personal bias after reading the abstract was one of skepticism. That feeling didn’t change much after reading the full text.
For one, nearly half of eligible studies were excluded from the analysis. The stated inclusion criteria for the metaanalysis drew from RCTs with at least six months of follow-up, which included any type of PCBs used to treat PAD in the lower extremities, and reported counts of major amputation as an endpoint.
However, when you review the PRISMA (Preferred Reporting Items for Systematic Reviews and MetaAnalyses) flow diagram that reports study exclusions, the first point that jumps out is that 19 studies were excluded for having zero major amputation events in both study arms. Only 21 studies were included in the final analysis, meaning that nearly 50% of eligible studies were excluded.
The authors performed a variety of sensitivity analyses to demonstrate replicability of their findings, but notably did not perform one including the studies
with no major amputation events, which would have reduced the event frequency substantially and likely rendered the differences between treatment nonsignificant.
My second concern with this metaanalysis is the inclusion of technology that has been actively unapproved by the Food and Drug Administration
“To me, the primary question that remains is: Do we really need more studies?” — Jessica Simons
“Similar to the original, my personal bias after reading the abstract was one of skepticism” — Caitlin W. Hicks
“The real limitation of all meta-analyses—including this one—are the trials included” — Katharine McGinigle
(FDA). For example, BD’s Lutonix DCB for below-the-knee (BTK) applications was recently rejected by the FDA for the second time in 18 months due to concerns about both clinical effectiveness and safety, yet the data from LutonixBTK was included in the meta-analysis— contributing the second largest number of
patients of all 21 studies evaluated. There are currently no FDA-approved DCBs for BTK applications, but the meta-analysis includes data from seven infrapopliteal studies that contributed outcomes for 1,355 out of a total of 3,760 limbs. While U.S. approvals are not the be-all and endall of technology, the FDA is notoriously one of the strictest regulatory bodies for new technology in the world, and the inclusion of devices that have been actively rejected by the FDA in the past is setting up the DCB group for failure.
My third main concern about this meta-analysis is the inclusion of patients with CLTI. The risk of major amputation is not the same for patients with claudication and CLTI. CLTI also comes in a variety of forms, and without some understanding of the extent of disease, comparing major amputation rates for a sample of patients with heterogenous forms of PAD is uninformed. It is notable that the risk of major amputation in trials limited to claudication patients was not different for DCBs compared to plain balloon angioplasty, although, strikingly, the authors do not report the crude risk in the claudication subgroup.
While I think it has been an important endeavor to raise the academic question of PCDs and their outcomes, the current available evidence does not convince me that current (FDA-approved) DCB devices increase the risk of major
amputation full stop. I will continue to use them selectively in appropriate patients until either an RCT or real-world data that adjusts for baseline differences in patient risk suggests otherwise.
Katharine McGinigle, associate professor, University of North Carolina School of Medicine, Chapel Hill, North Carolina I congratulate the international group of authors led by Katsanos on their recent publication in EJVES Their systematic review and meta-analysis evaluating the risk of major amputation following application of PCBs in lower-limb arteries was performed with impeccable methods
and raises important concerns. Based on 21 RCTs, they conclude that there appears to be a heightened risk of major limb amputation after the use of PCBs for femoropopiteal and/ or infrapopliteal revascularization.
The authors theorize that this may be due to downstream embolization and tissue deposition of paclitaxel that causes unsalvageable tissue damage, despite target vessel patency. I agree with the authors that this is concerning and that specific trials to evaluate limb salvage outcomes are needed. In the meantime, I must decide what to do in my practice, and those conclusions are harder to draw.
The real limitation of all meta-
(SVS) objective performance goals.
The authors report that the preponderance of trial participants were white males. That limits the generalizability of these results as we know that females are equally as likely to have PAD, and that Black females specifically have the highest rates of limb amputation after CLTI diagnosis.
Another major issue that limits my ability to interpret this data is the problem of imprecise language to define inclusion criteria trials of CLTI patients.
We need more precise information on wound size and location—and patient comorbid and anatomic factors—in order to really determine the expected risk of
‘Proceed cautiously in use of DCBs in CLTI patients with advanced WIfI stage’
BY MICHAEL CONTE, MD, AND JOSEPH MILLS, MD
paclitaxel
analyses—including this one—are the trials included. In this paper, 52% of the trial participants were claudicants.
Rather than get caught up in appropriateness-of-use criteria, adherence to medical therapy and supervised exercise programs, I chose to eliminate that half of the study population from consideration. There is simply not enough information in this paper to make decisions for the treatment of claudicants.
In general, these non-invasive interventions work and we should focus more of our attention to these therapies. If you must intervene, then avoiding drug-coated technology and the stenting of femoropopliteal lesions is easy enough if you are as equally concerned about the possible amputation and mortality risks as I am.
Taking into consideration the 11 of 21 trials including mostly patients with CLTI, the authors report a 7.2% vs. 4.7% (hazard ratio [HR] 1.56, 95% confidence interval [CI] 1.04–2.33; p=0.03) risk of limb loss with the use of PCB angioplasty versus plain balloon angioplasty over one to two years.
While there may be increased risk of limb amputation at this point using PCBs compared to deploying plain balloons, these major limb amputation rates are remarkably low.
Other registry studies report a major limb amputation rate as high as 20% within one year in patients with CLTI who are revascularized, and this is in line with the Society for Vascular Surgery
an adverse outcome, as well as whether or not a slightly higher risk is merited for each individual situation. As an example, many of the trials in this meta-analysis include “Rutherford 5/6” patients. We know that Rutherford 6 means an unsalvageable limb, so, clearly, patients with Rutherford 6 disease should not be included in a revascularization trial. This leaves the reader questioning who was actually included.
Limb outcomes are directly related to the severity of the wound at the time of revascularization, and until we start stratifying our analyses by the SVS WIfI (wound, ischemia, foot infection) wound classification system, we will not be able to determine the effect of other factors with a weaker signal, such as the paclitaxel dose administered.
To conclude, the authors raise an important concern that there may be downstream tissue effects of lower-extremity arterial paclitaxel administration. I agree with them that this is enough preliminary data to merit a dedicated trial to evaluate this specific safety question.
However, in the meantime, the majority of my patients with CLTI have a greater than 7.2% risk of limb loss within one or two years, and in cases of patients who are poor bypass candidates with moderate-large wounds and difficult-totreat lesions like below-the-knee popliteal occlusion, I think it is reasonable to continue to use drug-coated technology as part of a multipronged strategy to treat CLTI.
THE LAST SEVERAL YEARS HAVE SEEN ongoing controversy and debate about the risks and benefits of paclitaxel-coated devices (PCDs) for patients with peripheral arterial disease (PAD). The latest contribution from Konstantinos Katsanos, MD, and colleagues raises questions about potential increased risk of amputation in patients treated with paclitaxel drugcoated balloons (DCB), particularly in the context of chronic limb-threatening ischemia (CLTI). Since the 2018 publication from the same first author highlighted a potential mortality risk, several large-scale observational studies, as well as a report from the SWEDEPAD registry, have shown no discernible mortality signal.
The issue remains somewhat unsettled, and the Food and Drug Administration (FDA) has not as yet changed its most recent guidance, urging some caution and a need for more long-term data.
From my perspective, the plausibility of potential adverse off-target effects of paclitaxel has always been greater in the treated limb rather than systemically. So, this publication should engender some appropriate caution and emphasize need for greater study given limitations in the data. It should also be put into perspective from the standpoint of both risk and benefit.
First, and most importantly, as yet there is no demonstration of clinical efficacy of drug-coated balloons (DCBs) in patients with CLTI. Clearly, patients with CLTI have ongoing major unmet needs for improved and more durable vascular interventions, but so far DCBs have not shown themselves to be the answer. One wonders if this observation is part of that explanation. The recent failure of Lutonix-BTK to meet its efficacy endpoint further highlights the disappointing impact of DCBs where they are needed most: in patients with CLTI and severe tibial disease. The risk estimated by Katsanos is also very modest—i.e. less than three in 100 excess amputations—and is not controlled for important confounders such as limb severity (e.g. the wound, ischemia and foot infection [WIfI] stage). But in the absence of proven efficacy in CLTI, one should be quite cautious about any increased risk profile. Drug-eluting devices and their associated pharmacology are complex, and one should be cautious about lumping multiple unique devices, and certainly
device classes, together. The potential embolization concern is legitimate but also likely to be device and formulation specific. In the interim, I would advise caution in the use of DCBs in CLTI patients with advanced WIfI stage, larger wounds, or those needing reconstructive foot surgery. We will await the results of ongoing trials such as BEST-CLI (Best endovascular versus best surgical therapy in critical limb ischemia), BASIL-3, and SWEDEPAD to get more comprehensive data on both the risks and benefits of DCBs in CLTI.
Additionally, the paclitaxel controversies have spurred accelerated work to develop alternative drugs—for example limus agents—and delivery platforms that may yet prove to be the silver lining.
Furthermore, the amputation rate was only significantly different in the CLTI group, but not the claudicant group, and the overall amputation rate is much lower than would be expected in CLTI patients (about 4–7%)—which would correlate with only WIfI clinical stage 1, and perhaps stage 2, patients.
Unfortunately, we do not have any stratification of limb risk (WIfI) or runoff/ anatomy—e.g. the Global Limb Anatomic Staging System (GLASS)—so making any comparison of amputation risk without this and other information is difficult.
We also don’t have a good handle on the timing of the major amputations. If particulate embolization is the proposed mechanism, one would expect that to occur fairly early after intervention, but that is hard to ferret out.
“First, and most importantly, as yet there is no demonstration of clinical efficacy of drug-coated balloons in patients with chronic limbthreatening ischemia”
Michael Conte and (left) Joseph Mills
Key players behind first SVS AUC on claudication unpack details of development process
BY BRYAN KAY
Vascular surgeons have a history of going the extra mile to do the right thing for their patients. So went the theme of one of the comments sent in near the close of a recent Society for Vascular Surgery (SVS) Town Hall, during which key figures behind the Society’s first-ever set of appropriate use criteria (AUC)—set to cover the treatment of claudication—laid out some of the mechanics of bringing the upcoming document to the brink of publication.
THE SERIOUSNESS OF THE UNDERTAKING WAS laid bare at the outset of the gathering by Larry Kraiss, MD, the immediate past chair of the SVS Quality Council, who oversaw the development of the AUC. Revealing the methodology adopted to carve out the criteria as the RAND Corporation method, he duly quoted the group’s definition of appropriateness in care: “An appropriate procedure is one in which the expected health benefit exceeds the expected negative consequences by a sufficiently wide margin that the procedure is worth doing, exclusive of cost.” The RAND/UCLA (University of California, Los Angeles) method involves group decisionmaking comprised of a systematic literature review, as well as both a writing panel and a multidisciplinary rating panel. Kraiss said one of the recurring questions he faces concerns why there are two types of documents addressing quality of care—the other being clinical practice guidelines (CPGs).
Kraiss outlined how the two should interact: “When there is strong and abundant evidence to support a grade 1a clinical practice guideline either for or against a particular decision, the appropriate use criteria should generally agree with those statements because they are both using the same evidence base. However, in more nuanced clinical scenarios, CPGs may not be able to make strong recommendations given the available evidence. CPGs may therefore deliver weak or conditional recommendations, and it is in these circumstances then that AUCs explicitly recognize the lack of good evidence and mobilize expert opinion to give guidance.”
AUCs step into this void, Kraiss added. The rationale is clear: “AUCs will allow us to formally state the SVS position in the public domain and provide a means to advocate against inappropriate overuse.”
Karen Woo, MD—who co-moderated the Town Hall in early August with SVS Past President Kim Hodgson, MD, and is a member of the seven-person SVS AUC writing panel for the maiden criteria—explained the reasoning behind the selection of the RAND method.
“It’s the only standardized, validated technique for determining appropriateness, and it combines evidence with expert opinion,” Woo said. “It’s often used when we can’t perform an RCT [randomized controlled trial] in every feasible clinical scenario.”
The process behind the method is scientific, Woo continued. First comes the systematic review and metaanalysis. The writing committee creates scenarios. The rating panel then rates these across two rounds on a scale of one to nine. These range from inappropriate (1–3) to appropriate (7–9), with an indeterminate scale in between (4–6). Ultimately, the aim is to achieve a set of criteria that will result in better patient outcomes “when they are adhered to,” added Woo.
Jeffrey Siracuse, MD, the immediate past chair of the SVS Appropriateness Committee and also a member of
SVS Quality Improvement Committee, walked Town Hall watchers through the arduous process of how the definitions, scenarios and assumptions were constructed.
“The final result was a mind-numbing number of hypothetical patients to consider and ratings to render— greater than 2,200, but I think ultimately it was meaningful and manageable since there was some striking agreement on a few high levels,” she said.
Woo emphasized the importance of the scenario construction portion of the process described by Simons. “I want to highlight how important this part of the process was because everybody has to be speaking the same language so everyone can rate starting from the same place,” she said.
Kraiss provided a short overview of the fruits of the panelists’ labors: the more than 2,200 individual scenarios rated over the course of 15 hours spread across two days.
“A complete and accurate portrayal of the results will require numerous tables and accompanying narrative
the writing panel for the intermittent claudication AUC, explained how the SVS arrived at claudication for its first set of criteria. After considering a number of conditions rather than specific interventions, the Society settled on claudication since “it is a perceived need by both the public and our Society,” he said.
Siracuse also broke down the multicameral nature of the rating panel. Eleven of the 15 members were drawn from the SVS membership, with two each brought in from the American College of Cardiology (ACC) and the Society of Interventional Radiology (SIR). The panel was also drawn from a broad geographical spread, a breadth of experience levels in terms of years in practice, and a nearly even split between academic and private or community surgeons.
In terms of the writing panel’s role, Siracuse explained that the team fleshed out relevant variables deemed important, as well as definitions, scenarios and assumptions, all reviewed by the Appropriateness Committee before being sent to the rating panel.
Jessica Simons, MD, the inaugural chair of the new
describing the deliberations of the rating panel as they considered the various scenarios,” he said. “This is beyond the scope of today’s presentation; however, it is important to note again the remarkable degree of consensus achieved by the rating panel, where less than 0.5% of the scenarios met criteria for disagreement.”
Simons said next steps include peer review of the AUC manuscript by the SVS Document Oversight Committee, a public comment period, SVS Executive Board review and the eventual goal of publication in the Journal of Vascular Surgery. Woo, meanwhile, picked up on the theme of vascular surgeons doing the right thing raised by the viewer comment: “Since CMS [the Centers for Medicare & Medicaid Services] is moving towards pay for performance, perhaps if we can show that we’ve developed these criteria, that they benefit patients—that we can somehow capitalize off of that. I don’t know how that’s exactly going to happen, but I think at least—I’ll just speak for myself—I would rather go to my grave knowing that I did the right thing. And I think that was reflected in our panelists.”
Larry Kraiss
Jeffrey Siracuse
Jessica Simons
Karen Woo
Kim Hodgson
A recent SVS Town Hall revealed the intricacies of developing the AUC on claudication
less time in the OR* (compared to CEA)
Protection from stroke And
so much more
TCAR is designed to give the vascular specialist more options when treating carotid artery disease. TCAR is a complete procedural solution that is less invasive, takes less time to perform and results in significantly less risk of CNI and in-hospital MI in comparison to CEA.* All while protecting the patient from surgery-related stroke with rates as low as 0.6%.** Brighter patient outcomes through brighter clinical thinking. Silk Road Medical. Brighter. silkroadmed.com/tcar
* Malas MB, et al. TransCarotid Revascularization with Dynamic Flow reversal versus Carotid Endarterectomy in the Vascular Quality Initiative Surveillance Project [published online ahead of print, 2020 Sep 15]. Ann Surg. 2020;10.1097/SLA.0000000000004496.
** Kashyap VS, et al. Early Outcomes in the ROADSTER 2 Study of Transcarotid Artery Revascularization in Patients With Significant Carotid Artery Disease. Stroke. 2020 Sep;51(9):2620-29.
SVS focuses in on launch of vascular verification program
BY CARRIE MCGRAW
The Society for Vascular Surgery (SVS), in partnership with the American College of Surgeons (ACS), has announced that it is closing in on the launch of a future program to verify quality on the part of facilities that offer vascular care.
SVS PAST PRESIDENT KIM HODGSON, MD, referenced the Vascular Center Verification and Quality Improvement Program (VCV&QIP) during his Presidential Address at the Vascular Annual Meeting (VAM) in San Diego, California, Aug. 19.
The Society’s aim in developing the verification process and program is to indicate to patients that program reviewers investigated and verified a particular institution’s quality improvement process and that it follows high standards and protocols. Verification assures patients that the centers are taking steps necessary to consistently strive for high-quality patient care.
“It is difficult for both governmental and non-governmental agencies, including third-party payors, to determine quality and appropriateness,” said Hodgson. To address this unmet need, the SVS undertook the task of defining standards for quality, appropriateness and value for the vascular specialty. The involvement of vascular experts in defining quality and appropriateness has been pivotal in building a quality infrastructure to support members throughout the ever-changing healthcare landscape.
The SVS and ACS are working together to better define and verify high-quality and efficient care for vascular patients in both inpatient and outpatient settings,
said SVS Executive Director Kenneth M. Slaw, PhD. “The long-range goal is to have all SVS members actively engaged in quality improvement initiatives and to have this work recognized by government and private payors in efforts to reduce administrative burden through more streamlined prior authorization.”
The SVS/ACS VCV&QIP’s mission is to drive quality and value by guiding the vascular center to leverage the infrastructure necessary to perform various vascular procedures in an environment that is safe and conducive to excellent patient outcomes and to be a leader in vascular quality improvement. At its core, VCV&QIP follows six National Quality Strategies to align organizational functions to drive improvement based on the aims and priorities of the Agency for Healthcare Research and Quality (AHRQ), part of the U.S. Department of Health and Human Services. The areas are: measurement and feedback with required registry participation; certification, accreditation and regulation with required facility regulation; consumer incentives and benefit designs with thorough discussion of treatment options and consent; health information technology, working with outside software for continuation of care; innovation and diffusion with research; and workforce development with the capability of resident training.
SVS: A lesson in unity through diverse talent
BY KENNETH MADSEN, MD
Today’s emphasis on diversity is nearly inescapable, while examples of true unity seem scarcer. Is there really a way the two can co-exist or work together beneficially? Consider some of your favorite bands, or even successful sports teams. Even a cursory assessment shows that a diversity of talents and aptitudes can and do work harmoniously to create memorable music or bring home championships. Similarly, the SVS is a very diverse society that stands to benefit tremendously if unified in purpose.
As with all ACS Quality Improvement programs, the VCV&QIP began with the development of the program’s “standards,” factors felt to be critical to the success of a program and against which a program is evaluated.
Once the standards were formulated, at the SVS level Hodgson and fellow former SVS president, Anton Sidawy, MD, identified potential pilot sites, looking for both inpatient and outpatient verification levels, to apply the standards to real-world practices and fine-tune them if needed.
Surgeons visited the first pilot site, the Albany Medical Center in Albany, New York, in April. “The verification of inpatient and outpatient vascular centers is an important step in recognition of our specialized and distinct service to our patients and to our healthcare systems,” said R. Clement Darling III, MD, of the Albany Medical Center and another former SVS president. “The verification process was valuable to help us to understand what we need to provide the best longitudinal vascular care for our patients and will provide a roadmap to help institutions and payors understand the infrastructure needed to establish and maintain a comprehensive vascular service.”
In addition, verification, “will
OUR SPECIALTY BOASTS A DIVERSE RANGE OF practices—from highly specialized vascular centers of excellence to rural practices—that face a broad range of common but challenging vascular conditions. We operate efficient office-based labs (OBLs) and elegant vein practices. Our interests and aptitudes within the Society vary widely, and we all seek optimal practices that provide reasonable work-life balance while also ensuring professional satisfaction. Working in a proper setting can invigorate and energize us while acting as a level of protection from burnout. In this manner, the diversity of our practices can better ensure optimal patient care.
Our Society is diverse in social and political ideologies as well. These differences should not divide us
Beyond this we must continue to look even deeper. Our Society is diverse in social and political ideologies as well. These differences should not divide us. Rather, healthy discourse should open our eyes to future possibilities while exposing the current challenges that are our opportunities for progress. Despite and because of our diversity, we must have a seat at the legislative table and do everything possible to work for one another. The SVS Political Action Committee (PAC) is a vehicle that
demonstrate to patients and providers that we are following standards and established protocols that have been peer-reviewed for their benefit by specialty-trained vascular specialists/surgeons. I thought the process was comprehensive, fair, educational, and a true benefit to our patients and our specialty of vascular surgery,” said Darling. VCV&QIP requires institutions to examine and validate processes that should lead to the following: external credibility, improvement in quality, enhanced organizational learning, high staff effectiveness, decreased liability cost, and mitigating risk of adverse events.
The Michigan Vascular Center participated as the first office-based lab (OBL) in the pilot phase. “The Michigan Vascular Center opened its first OBL in 2005 and opened a second in 2013,” said Robert Molnar, MD, adding that the centers have been accredited by the Accreditation Association for Ambulatory Health Care (AAAHC) for more than eight years. “Our focus was always on providing care that was equivalent and even superior to that provided in the hospital setting. We felt that accreditation was important to signify our level of commitment to quality and best practice standards. When the SVS/ACS announced a vascular-specific verification program for OBLs, we wanted to participate and have our program evaluated to ensure we were providing the best possible care with the highest quality. The process allowed us to analyze what we had established and provided a process to reaffirm our commitment to quality and our patients.”
In the coming months, SVS and ACS will finalize the standards and infrastructure to provide vascular facilities with easy access to resources in order to guide them in applying for verification.
For more information on the verification program, contact Carrie McGraw at cmcgraw@vascularsociety.org.
can package these efforts and present them to elected representatives who can advocate for our needs. Some current SVS PAC efforts include: lobbying support for enacting legislation to end cuts in Medicare payments scheduled for Jan. 1, 2022; H.R. 2256/S. 834, “The Resident Physician Shortage Act”; H.R. 1667/S. 610, the “Dr. Lorna Breen Health Care Provider Protection Act”; and H.R. 3173, “Improving Seniors’ Timely Access to Care Act of 2021.” More information on these issues is available at vascular.org/VoterVoice. While the PAC is working diligently on behalf of the Society, we need engagement from our membership. The impact of our messaging is directly proportional to the percentage of the Society that participates. Of our 5,600 members less than 10% currently donate to the PAC. To those who donate, we thank you! To those who have never donated—take a chance on us, donate to the PAC, and invest in your future as well as the future success of our specialty.
KENNETH MADSEN is a member of the Society for Vascular Surgery PAC Steering Committee.
Kim Hodgson during his address
with
by
RISK INFORMATION
Caution: Federal (USA) law restricts the use of the system by or on the order of a physician.
Refer to Directions for Use and/or User Manual provided with the product for complete Instructions, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the product.
INDICATIONS FOR USE
The AURYON Atherectomy System is indicated for use in the treatment, including atherectomy, of infrainguinal stenoses and occlusions, including in-stent restenosis (ISR).
References: 1. Rundback J, Chandra P, Brodmann M, et al. Novel laser-based catheter for peripheral atherectomy: 6-month results from the Eximo Medical B-LaserTM IDE study. Catheter Cardiovasc Interv. 2019;94(7):1010-1017. 2. Shammas NW, Chandra P, Brodmann M, et al. Acute and 30-day safety and effectiveness evaluation of Eximo Medical’s B-LaserTM , a novel atherectomy device, in subjects affected with infrainguinal peripheral arterial disease: results of the EX-PAD-03 trial. Cardiovas Revasc Med 2020;21(1):86-92. 3. Auryon. Instructions for use. AngioDynamics; 2020.
‘Do we need to do a better job of making devices that fit female anatomy?’
BY BRYAN KAY
It was a burning question posed from the conference floor, and it led to some approving social media nods in its aftermath: Does the tone of conversation around the vascular anatomy of females need to morph into a discussion about the availability of devices that fit the female anatomy?
The point was provoked by another question that followed findings delivered by Scott R. Levin, MD, a general surgery resident at the Boston University School of Medicine, Boston, at the 2021 Vascular Annual Meeting (VAM) in San Diego (Aug. 18–21) suggesting female sex was associated with a higher risk of reintervention after endovascular procedures and infrainguinal bypass surgeries for intermittent claudication.
“Do we need to stop saying that women have worse anatomy than men?” came the question from Mahmoud B. Malas, MD, chief of vascular and endovascular surgery at the University of California San Diego, San Diego, in Plenary Session 6 on Aug. 21.
Malas was speaking after fellow audience member Keith D. Calligaro, MD, chief of vascular surgery and endovascular therapy at Pennsylvania Hospital in Philadelphia, rose to query Levin on two aspects of his findings. Calligaro began by referencing a question he had posed the previous day of Thomas F. X. O’Donnell, MD, senior vascular surgery fellow at Beth Israel Deaconess Medical Center in Boston, who had delivered new findings on racial disparities in the treatment of ruptured abdominal aortic aneurysms (AAAs).
“Yesterday I rose to make a comment about a paper that was presented and why women might have higher complication rates for aortic aneurysms,” he explained. “That comment was simply because some of them have smaller iliac arteries, worse access, more complications.”
Could the reason for the higher level of complications among women demonstrated in the claudication study be put down to the fact women “tend to have smaller infrainguinal arteries and therefore less durable long-term results?”
Calligaro said, further querying: “You commented women are less likely to be given statins. I’m aware of several papers that have shown women are less likely to take statins when they’re prescribed. I don’t know why. I’ve read several papers on this subject, and I don’t know that anyone really knows the reason, but that’s what a lot of the data shows.”
The data gathered by Levin and
colleagues demonstrated that female sex was associated with lower use of aspirin and statins prior to both infrainguinal bypasses and endovascular interventions. “But we don’t know based on using the database why this is the case,” said Levin. “We do know that aspirin-statin use is associated with lower rates of reintervention, and so the lower rates of aspirin-statin may have contributed to higher reintervention. We did actually control for preoperative medication in our multivariable analysis. Further prospective studies would be needed to tease out the causes of why there are these differences by sex.”
For Malas’ part, he asked Levin whether the profession needed “to do a better job of making devices that fit women,” saying it was not that women have “worse anatomy than men” but rather smaller vessels. “Is the problem, with an aneurysm or peripheral intervention, that we don’t make stuff that fits women’s anatomy better?”
Levin said that the present study— which queried the Vascular Quality Initiative (VQI) for all suprainguinal and infrainguinal bypasses as well as endovascular interventions for intermittent claudication from 2010–2020—was not able to demonstrate causes, nor did it probe specific devices. “But I think that would be useful for future studies to look at and control for specific devices,” he said.
After performing bivariable and
“Is
the problem, with an aneurysm or peripheral intervention, that we don’t make stuff that fits women’s anatomy better?” —
Mahmoud B. Malas
multivariable analyses to evaluate the association of sex with perioperative and long-term outcomes, what the chief findings of the investigation did show was that among endovascular procedures for intermittent claudication, female patients more often had iliac interventions, less often had infrainguinal interventions, and less often underwent stenting or atherectomy (all p<0.05), according to Levin et al
This was based on 64,752 endovascular interventions (62% male, 38% female sex) prized out of the VQI on claudicants. Furthermore, female patients more often had access site hematomas (3.6% vs. 2.3%; p<0.001) and stenosis or occlusion (0.3% vs. 0.2%; p=0.001). Female patients had lower one-
Mahmoud B. Malas
year reintervention-free survival (84.3% vs. 86.3%; p<0.001), with no differences in amputation or death. Female sex was independently associated with one-year reintervention (hazard ratio [HR] 1.16, 95% confidence interval [CI] 1.09–1.24; p<0.001), but not amputation or death.
Among those who underwent infrainguinal bypasses (9,314 surgeries; 70% male, 30% female), female patients had fewer infrapopliteal targets and more often received prosthetic conduits (p<0.05 for all), Levin explained. There were no differences in perioperative outcomes. Female patients had lower one-year reintervention-free survival (79% vs. 81.2%; p=0.04) with no differences in amputation or death. Female sex was independently associated with oneyear reintervention (HR 1.16, 95% CI 1.03–1.31; p=0.016), but not amputation or death.
As for suprainguinal bypasses (3,227 surgeries; 63% male, 37% female), “female patients more often underwent bypass from the axillary artery (p<0.05). Female patients had fewer perioperative surgical site infections (0.9% vs. 1.8%; p=0.048). There was no significant difference by sex for one-year reintervention, amputation, or death, even adjusted for comorbidities,” Levin added.
Levin also reported that female patients were less likely to present with independent ambulatory status preoperatively, which persisted postoperatively after endovascular interventions. Meanwhile, for endovascular interventions and infrainguinal bypasses, female patients were less often on aspirin (73.4% vs. 77.3% and 71.5% vs. 74.8%, respectively) and statins (71.8% vs. 76.7% and 73.1% vs. 76%, respectively)—all with a p value of <0.001.
Levin concluded: “Female patients undergoing interventions for claudication were less often on aspirin and statins. Interventionists treating female claudication patients should increase their efforts to maximize medical therapy, even patients exhibiting with worse baseline ambulatory function and worse function after peripheral vascular interventions. After peripheral vascular interventions and infrainguinal bypasses, female patients had increased risk of reintervention. Future research should clarify reasons for poorer intervention durability in female patients.”
Ruptured AAA disparities
The data demonstrating racial disparities among patients treated for rAAAs, delivered by O’Donnell during a special
scientific session on diversity, equity and inclusion Aug. 20, included one statistic showing that Black patients were significantly less likely to undergo transfer prior to repair compared to white patients (49% vs. 62%; p=0.002)—with rates of transfer high. “This was consistent in crude and adjusted analyses, in sub-analyses limited to only stable patients, and was not modified by insurance status, type of operation, or hospital volume,” O’Donnell revealed.
unstable to undergo repair, patients refusing repair, comorbidities such that repair would be futile?”
O’Donnell and colleagues examined all repairs of rAAA in both the VQI from 2003–2020 to evaluate transfer rates and outcomes in Black vs. white patients in the National Inpatient Sample (NIS) from 2004–2015 to examine turndown rates. They found nearly 5,000 (6.2% Black) in the former and 50,000 (6% Black) in the latter. Mixed effects logistic regression, Cox regression and marginal effects modeling were used to study the interaction between race, insurance status, type of operation— open repair vs. endovascular aneurysm repair (EVAR)—and hospital volume. There was no significant difference in perioperative mortality (Blacks 22% vs. whites 26%; p=0.098) or complications (52% vs. 52%; p=0.64), the researchers found. But O’Donnell said the data show that Black patients were significantly more likely to be turned down for repair when presenting with rAAA (37% vs. 28%; odds ratio [OR] 1.5 [1.2–1.9]; p<0.001). “There was a significant interaction between race and insurance status with respect to turndown,” he explained.
“Patients with private insurance underwent operations at similar rates regardless of race, but among patients with Medicare or Medicaid/self-pay, Black patients were less likely than whites to undergo repair (Medicare: 64% vs. 72%; p=0.001; Medicaid/self-pay: 43% vs. 61%, p=0.031).”
Furthermore, patients with Medicaid/ self-pay were less likely to undergo repair compared to patients of the same race with either Medicare or private insurance (p<0.05), O’Donnell added. He concluded: “Black patients with rAAA are poorly served by the current systems of interhospital transfer in the United States, as they less often undergo transfer prior to repair. Although postoperative outcomes appear similar, this may be false optimism, as Black patients, especially the underinsured, are more often turned down for repair even after adjustment. Significant work is needed to better understand the reasons underlying these disparities and identify targets to improve the care of Black patients with rAAA.”
Session moderator Bernadette Aulivola, MD, professor of surgery and director of the division of vascular surgery and endovascular therapy at Loyola University Medical Center in Maywood, Illinois, asked O’Donnell to explain how he and his fellow researchers defined turndown, or failure to offer an operation, elaborating, “How do you catch out whether that’s patients too
O’Donnell said: “That’s always the interesting question with something like NIS, and why we wanted to use the two databases, and that’s something you can tease out in the VQI, and we know from the VQI that the rate of presentation in terms of instability is the same, so, all things being equal, the race comorbidities were slightly higher but presentation as an unstable patient was about the same, so some of that increase in turndown may be due to the comorbid burden. But since the instability is about the same, you can’t attribute all of that.”
Calligaro, raising the same point he later asked of Levin the following day, urged caution in how the data is interpreted.
“There are several publications also showing that women are less likely to
Females were 30% less likely to undergo surgery for PAD, national database study finds
A review of more than 1 million patients receiving vascular surgery over a 16-year period identified significant sex-related disparities in the treatment of abdominal aortic aneurysms (AAAs) and peripheral arterial disease (PAD)—with females 30% less likely to undergo surgery in the case of PAD.
“The first annual Women’s Vascular Summit highlighted sex- and genderrelated knowledge gaps in vascular disease and treatment,” first author Katharine McGinigle, MD, assistant professor in the division of vascular surgery at the University of North Carolina in Chapel Hill, writes in the June edition of the Journal of Vascular Surgery (JVS). “This finding suggests an opportunity for further research to improve care and outcomes in people who identify as women, specifically”.
Speaking to Vascular Specialist, McGinigle went into more detail about the meeting and its importance: “The Women’s Vascular Summit, directed by co-author Linda Harris, [MD], is an annual meeting for medical professionals who treat vascular disease in females. For all vascular conditions, the research presented at this meeting has illustrated that there are significant sex-related knowledge gaps. Females tend to have different presenting symptoms than males, present later in the disease course, and are more often misdiagnosed.”
The research team hypothesized that once the diagnosis is made, there also would be differences in the intervention rate and type of intervention performed. The purpose of this study, therefore, was to identify all operations performed for AAA, carotid artery stenosis (CAS) and PAD in the U.S., and to provide data on sex-related disparities in treatment.
Using the Healthcare Cost and Utilization Project National Inpatient Sample, the research team identified all hospitalizations
undergo repair at the same size, and that they have a higher mortality for elective and ruptured, open versus endo,” he said. “Frankly, I don’t think it’s because women are turned down for surgery per se. One reason that comes to mind is for instance with EVARs—they may have smaller iliac arteries, worse access and higher complication rates … I’m not aware of any anatomic differences between African Americans in terms of aortoiliac anatomy but there may be other things we’re not aware of.”
O’Donnell accepted the point, explaining that his group had looked at aortoiliac anatomy previously. “What we found in the VQI at least was that Black patients—and similarly in this population as well—had more iliac aneurysms, but more often were actually treated with EVAR. That’s borne out in this dataset: Black patients were about 10% more likely to undergo EVAR. So some of it may be anatomic differences, but I don’t think that can explain a significant portion either.”
of adult patients (≥18 years old) diagnosed with AAA, CAS or PAD who underwent vascular surgery from 2000–2016. The authors specify that they used census data and sex-specific population disease prevalence estimates from the National Institute of Health and Agency for Healthcare Research and Quality to calculate the number of U.S. adults with AAA, CAS and PAD.
McGinigle and colleagues detail that there were 1,021,684 hospitalizations for vascular surgery over the 16-year study period: 13% AAA (21% female, 79% male), 40% CAS (42% female, 58% male), and 47% PAD (42% female, 58% male). Females were older than males at the time of surgery (median age, 71.3 years vs. 69.7 years) and less likely to have private insurance (18% vs. 23%). In addition, minimal differences were seen across race/ethnicity, comorbidities and hospital characteristics.
After accounting for disease prevalence, the authors report in JVS that females were 25% less likely to undergo surgery for AAA and 30% less likely to undergo surgery for PAD compared with males, were less likely to receive an endovascular procedure compared with open for AAA or CAS, and more likely to receive one for PAD.
McGinigle remarked on these findings: “We know we need to improve AAA screening rates, and now we know that even when the diagnosis is made, we need to be operating more in women. […] It appears as if females are getting more endovascular revascularizations in this study, but we caution that all of the patients in this database are admitted to a hospital, so it is likely that women are just more often getting admitted for complications for a common outpatient procedure. The gender-stratified rates of outpatient treatment are known.
“Shared decision-making around the indication for treatment is important, and in the future it will be interesting to study how females versus males make these decisions, particularly in conditions like claudication where there are not objective parameters for intervention.”—Jocelyn Hudson and Bryan Kay
Scott R. Levin
Thomas F. X. O'Donnell
Keith D. Calligaro
SVS bestows Lifetime Achievement Award on Robert B. Smith III
BY BETH BALES
Among his many professional achievements in a career of a “golden age of vascular surgery” that overlapped with the growth and maturation of the specialty and the endovascular revolution, Robert B. Smith III, MD, most remembers the “many young men and women who trained with us over those years and today excellently service patients’ needs.”
SMITH, WHO RETIRED 11 YEARS AGO, ON THE morning of Aug. 19 at the Vascular Annual Meeting (VAM) in San Diego officially received the Society for Vascular Surgery (SVS) Lifetime Achievement Award, one of the highest honors the SVS can bestow upon a member. In performing the introduction, Past President Kim Hodgson, MD, called Smith “a venerated master who has left a lasting impact on the vascular world.” He actually was named award recipient in 2020 but cancellation of the 2020 VAM moved his ceremony to 2021. Due to health issues “of my lovely wife of 68 years,” Smith accepted the award via video from his home in Georgia.
He began his career as a resident at Columbia Presbyterian Medical Center in New York, working with the famed Arthur Vorhees, MD, who invented a plastic prosthesis for correction of diseased arterial segments. “He was a great teacher who became a friend and collaborator until his death in 1992,” said Smith.
His residency, said Hodgson, “jump-started his immersion in vascular surgery where his career overlapped with the growth and maturation of vascular surgery and the endovascular revolution.”
After residency he returned to Emory University—
where he’d attended college and medical school—as a faculty member. There, Garland Perdue, MD, “congenial colleague, active role model and gifted administrator,” was also his benefactor. He and Perdue performed Georgia’s first successful renal transplant, and he helped refine the distal splenorenal shunt, a major innovation in the care of patients with portal hypertension, said Hodgson. Surgeons from across the country have visited Emory to observe the liver team performing shunt procedures.
In 1969, they started a vascular surgery fellowship, comprised of one additional year of training after general surgery training. It was “one of the earliest such programs in the country and the first to receive approval by a national accrediting agency,” said Smith. “We trained more than 60 vascular surgery residents” over more than four decades, he added, who are now working across the country and even the world. Four, in fact, followed Smith
as Emory’s head of vascular surgery: Alan Lumsden, MD, Elliot Chaikof, MD, Thomas Dodson, MD, and the current chair, William Jordan, MD. In turn, those trainees praise Smith, calling him “both a master surgeon and the go-to vascular surgeon at Emory,” said Hodgson.
“I am an admiring enthusiast for what you and your teams do on a daily basis,” Smith told the VAM audience.
“I am aware it is a great privilege to be a physician and even more a surgeon and especially a surgeon in a subspecialty that frequently is a life-, brain- or limb-saving discipline.” Receiving the award is the “highest honor of my professional career and I am profoundly grateful,” he said. “It’s a humbling experience as I join those prestigious leaders who have received this award previously.”
The award also “is an affirmation of the entire division of vascular surgery at Emory,” he added, thanking Hodgson and others “for this very special recognition.”
What is taxonomy and how does it affect vascular surgeons?
BY KEVIN MARTIN, MD
Have you ever had a bill denied for services of your assistants and not known why? Have you received cryptic messages on an explanation of payments that indicates your assistant is not allowed to bill for services? As the use of professional extenders increase, this is becoming a more frequent issue.
SEVERAL SURGEONS HAVE AIRED questions over the past year about denials on billing for their mid-level or advanced practice providers (APPs), physician assistants (PA) or nurse practitioners (NP). Some of these denials are related to taxonomy code issues. Taxonomy is the classification of providers ticking away on computers in the background, about which many physicians know little. When a provider signs up to practice after getting the appropriate license, one gets an National Provider Identifier (NPI) number but also a taxonomy code number, which goes into the Medicare Provider Enrollment, Chain and Ownership System (PECOS) and insurers’ computers. The taxonomy code tells the computer what type of provider you are. For physicians, this usually never changes, i.e., once a vascular surgeon, always a vascular
surgeon. Many physicians never even know they have a taxonomy number as this is usually handled by credentialing employees when the physician first starts work. So, the problems are not with the vascular surgeon, but with the APPs.
For PAs, there are only three taxonomy codes, but issues occur when a PA starts work with a medical practice, changes jobs, and is hired by surgeons and does not change his or her taxonomy code. Then there can be conflicts with surgical groups being told that they cannot be with other groups in risk-sharing models (accountable care organizations) as the computer sees a primary care billing from the surgical group PA (the computer thinks this is still a medical PA), which cannot be allowed. When an APP changes jobs, it is important to review and update the taxonomy code.
For nurse practitioners, there are 18
SVS branding campaign wins communications award
BY BETH BALES AND KRISTIN CROWE
The Society for Vascular Surgery (SVS) branding campaign has received a “Profiles of Excellence Award” from the American Association of Medical Society Executives for outstanding achievement by medical societies.
SVS WON ITS AWARD IN THE COMMUNICATIONS category, for “initiatives that disseminate an important message or promote a medical society’s mission through effective content and delivery methods.” The other categories are advocacy, education, leadership and membership.
The entry, “Translational branding: Applying a national brand strategy to improve your member’s local brand,” highlighted the Society’s ongoing branding campaign and Branding Toolkit to help vascular surgeons communicate their role in comprehensive vascular care to referral sources and patients, and to emphasize that “Surgery is only part of our story.” SVS works with Springboard Brand & Creative Strategy to develop the campaign and the toolkit.
taxonomy codes, and for certified clinical nurse specialists (CCNS) there are 34. None of those 52 codes specifies a surgical NP or CCNS. There can be problems with computers thinking that billings from these are medical providers rather than surgical providers.
To decrease problems, there are workarounds. None is perfect but they do allow some flexibility. First, one should be aware of these taxonomy codes and make sure that everyone is signed up with the correct code.
The following section of the Centers for Medicare and Medicaid Services (CMS) website, vascular.org/TaxonomyDataset, is a good place to start to check the taxonomy codes. The PECOS (vascular. org/PECOS) can be checked to make sure the taxonomy code is correctly listed.
This is a separate issue from the desire of some APPs to have independent practices without a collaborative agreement with a physician.
No. of taxonomy codes: PAs 3, NPs 18 and CCNS 34
APPs traditionally are considered to be working in the same field/specialty as the physicians with whom they work. The supervising physician can be listed on a claim with the APP so the computer can recognize the specialty within which the APP is working, based on the physician’s taxonomy code. There must be a collaborative agreement between the APP and the physician to use the latter’s name/ code that pulls the service to a specialty.
The Branding Toolkit, introduced a year ago, includes fliers, posters and brochures that can be customized with member logos, addresses and photos. Additional tools to help SVS members engage with additional referral audiences, hospital leadership, patients and consumers will be added over time.
“I’m proud of this award, as I am proud of the immense effort that has gone into making the campaign a reality,” said SVS Executive Director Kenneth M. Slaw, PhD.
“Members identified branding as a No. 1 initiative in 2018, and now the SVS and Springboard have given our members the tools they need to have effective conversations in their own local markets with referral sources,” noted Joseph Mills, MD, SVS vice president and former chair of the Public and Professional Outreach Committee, which worked to develop the campaign and toolkit.
“Use them,” he added. “Make a difference for yourselves and our profession by getting this message out in different ways and as often as you can.”
For those in multispecialty groups with the same tax identification number, the taxonomy code for the physician can identify the separate specialty while the APP taxonomy code is not specific enough. Depending on the site of service, the physician can also edit/amend the note after seeing the patient and take over the billing under split/ shared service. Physicians then get the credit for the billing. This may play havoc with APPs’ pay if their remuneration is heavily based on work relative value unit (wRVU)/ billing production. But some electronic medical records have a way to track the APP productivity as well as the physician billing. These are some of the ways to avoid billing problems, but making sure the taxonomy codes are correct is the first step. If there are recurrent denials on APP billing, coordination between credentialing and billing staff can alleviate/resolve many of these problems.
KEVIN MARTIN was writing on behalf of the SVS Coding Committee, of which he is a member.
as a huge opportunity to promote a vascular practice. Hundreds of SVS members have accessed the toolkit by downloading and/or customizing fliers, postcards, videos, social media ads and more. Now, the SVS wants to hear Branding Toolkit success stories.
The contest includes two categories: both the most creative and most effective uses of the toolkit. Each winner will be able to choose between admission to the 2022 Vascular Annual Meeting (VAM) or a $250 social media ad campaign.
SVS also will conduct a drawing, with the winner, selected at random, receiving one free year of SVS membership dues for 2022. To enter, members can submit any number of customized pieces from the toolkit, with each piece serving as one entry into the drawing.
Winners will be announced at the VEITHSymposium in Orlando later in November.
Our November issue highlighted the SVS branding
Brand your practice and win Meanwhile, members have the chance to tell their stories, promote their practices and spread the word about the vascular surgery specialty—and win prizes.
They simply need to use the SVS Branding Toolkit and then share how they put it to use by entering the SVS Branding Contest by Nov. 1
The Branding Toolkit represents a commitment to the branding of the vascular surgery profession and serves
“The SVS has really demonstrated a commitment to every member with the branding effort,” said Benjamin J. Pearce, MD, chair of the SVS Public and Professional Outreach Committee. “The Branding Toolkit allows each member to create a bespoke set of patient-centered and practice-oriented materials to help get the word out about vascular surgery. I encourage all members to participate in the toolkit contest and drawing, not just for the prizes, but to get firsthand experience with this resource.”
For more information on the branding campaign and toolkit visit vsweb.org/Branding.
Amputation rates higher for people with PAD who are poor or Black
BY JOCELYN HUDSON
POVERTY AND BLACK RACE WERE associated with higher rates of lowerleg amputation among people with peripheral arterial disease (PAD) who live in metropolitan areas, according to new research published in a special issue of the Journal of the American Heart Association (JAHA), an open access journal of the American Heart Association (AHA).
The analysis on PAD-related amputations is one of 16 new research studies highlighting health disparities among people from diverse population groups published in the special spotlight issue of JAHA
JAHA senior associate editor Pamela Peterson, MD, of the University of Colorado Denver, and associate editor Sula Mazimba, MD, from the University of Virginia Health System, Charlottesville, Virginia, note that while management of cardiovascular disease has reduced death rates over time, there are still “striking disparities” in the U.S. that have widened along racial, ethnic,
FDA approves expanded PAD indication for rivaroxaban plus aspirin
BY JAMIE BELL
socioeconomic and geographical lines.
“We hope that this issue of JAHA will reinforce the recent American Heart Association’s presidential advisory statement urging all stakeholders to a committed path towards transforming the conditions of historically marginalized communities, improving the quality of housing and neighborhood environments of these populations, advocating for policies that eliminate inequities in access to economic opportunities, quality education and healthcare, and enhancing allyship among racial and ethnic groups,” they wrote.
The study, “Geographic and
socioeconomic disparities in major lower-extremity amputation rates in metropolitan areas,” by Alexander Fanaroff, MD, of the University of Pennsylvania, Philadelphia, et al, is an analysis of national Medicare claims data to determine ZIP codelevel variation in rates of amputation among Medicare beneficiaries.
“We found that closer proximity to specialized PAD care within metropolitan areas does not ensure access to high quality care” — Alexander Fanaroff
“Limb amputation can be delayed and or prevented by timely and aggressive treatment. However, lack of access to specialized care may delay PAD diagnosis and limit efforts to save the limbs if it has progressed to the advanced disease stage,” explained Fanaroff.
major cardiovascular events (MACE) in patients with coronary artery disease (CAD) and major thrombotic vascular events, such as myocardial infarction, ischemic stroke, acute limb ischemia, and major amputation of a vascular etiology, in patients with PAD, including patients who have recently undergone LER due to symptomatic PAD.
The Janssen Pharmaceutical Companies of Johnson & Johnson announced in late August that the Food and Drug Administration (FDA) had approved an expanded peripheral arterial disease (PAD) indication covering the rivaroxaban vascular dose—2.5mg twice daily plus 100mg of aspirin once daily—to include patients who have recently undergone a lowerextremity revascularization (LER) owing to symptomatic PAD.
The approval is based on data from the phase III VOYAGER PAD study. According to a press release, rivaroxaban is now the first and only therapy indicated to help reduce the risks of
“For more than 20 years, many physicians have used dual antiplatelet therapy after lower-extremity revascularization due to symptomatic PAD with limited data to support efficacy and safety in this setting. Now, the VOYAGER PAD and COMPASS clinical studies have demonstrated the utility of dual pathway inhibition in targeting both platelets and thrombin in patients with PAD. These data provide a new mechanism of treatment using an evidence-based strategy for this vulnerable population,” said Marc P. Bonaca, MD, of the University of Colorado Anschutz Medical Campus, Aurora, Colorado. “This FDA approval of rivaroxaban plus aspirin is a major advancement for PAD management and sets the stage to evolve the current standard of care for patients with PAD,” he added.
Fanaroff and colleagues found that ZIP codes with a higher proportion of Black residents had higher amputation rates than ZIP codes with lower proportions of Black residents. In addition, ZIP codes with lower median household income, more residents eligible for Medicaid and worse scores on the Distressed Communities Index scale (a composite marker of socioeconomic status), had higher amputation rates compared to ZIP codes with higher socioeconomic status, even after adjusting for clinical and demographic characteristics.
“Though amputation rates are generally higher in rural areas, this finding shows that the association between lower socioeconomic status, race and amputation rate extends to major metropolitan areas as well as rural regions,” Fanaroff said. “We found that closer proximity to specialized PAD care within metropolitan areas does not ensure access to high quality care. Strategies targeted to communities with high amputation rates are also needed in urban areas to reduce these disparities.”
A recent AHA scientific statement noted sex and ethnic disparities exist in the diagnosis and treatment of chronic limb-threatening ischemia (CLTI).
Symptomatic PAD post-LER: 2.5mg of rivaroxaban twice daily plus 100mg of aspirin once reduces MALE/MACE by 15% 2.5mg 100mg
major adverse limb events (MALE) by 15% in patients with symptomatic PAD post-LER compared to aspirin alone.
The VOYAGER PAD trial saw no significant difference in thrombolysis in myocardial infarction (TIMI) major bleeding between rivaroxaban with aspirin compared to aspirin alone.
The results from the VOYAGER PAD study complement findings from the landmark phase III COMPASS trial, which also examined the dual-pathway approach of rivaroxaban with aspirin in CAD and/or PAD patients and further supports this FDA label extension in PAD patients.
Rivaroxaban now has nine indications in the U.S. The phase III VOYAGER PAD trial, which demonstrated the rivaroxaban vascular dose reduced the risk of MACE and
Data from the phase III COMPASS trial resulted in FDA approval in 2018 to reduce the risk of MACE, such as heart attack, stroke and cardiovascular death in people with chronic PAD and CAD. While there were more major bleeds with the rivaroxaban vascular dose in COMPASS, there was no significant difference in rates of fatal bleeding, intracranial bleeding or symptomatic bleeding into a critical organ.
Meanwhile, new data from VOYAGER PAD presented at the 2021 Vascular Annual Meeting (VAM) suggested rivaroxaban plus aspirin should be considered after lowerextremity bypass regardless of conduit type, as reported in Vascular Connections, a sister publication of Vascular Specialist
Save the date for new PAD skills workshop
BY BETH BALES
September is National PAD Awareness Month, and the Society for Vascular Surgery (SVS) will spend the month not only calling attention to causes and treatment for the disease, but also planning a peripheral arterial disease (PAD) skills workshop.
THE HANDS-ON WORKSHOP, aimed at practicing surgeons, includes more than 10 hours of didactics, smallgroup sessions and four hours of skills training. It will be held Feb. 11 and 12, 2022, at the Orthopedic Learning Center (OLC) in the SVS headquarters office building in Rosemont, Illinois. To be able to provide individual and personalized attention, attendance is
SVS draws attention to Medicare cuts as PAD Awareness Month kicks off
limited to 75 attendees. Members have long requested such a workshop because they treat PAD patients frequently but don’t necessarily have the latest skills and knowledge, said Vikram Kashyap, MD, program chair alongside Patrick Geraghty, MD, with additional planning coming from Daniel McDevitt, MD.
Fifteen “top-notch” surgeon-instructors will teach, the doctors said.
THE SOCIETY FOR VASCULAR SURGERY (SVS) has mobilized a special task force to take action on proposed cuts by the Centers for Medicare and Medicaid Services (CMS) that would severely hammer vascular care, potentially harming access to specialty care. The SVS Task Force on CMS Payment Cuts, cochaired by Matthew Sideman, MD, and William Shutze, MD, is working with a number of other specialty societies and coalitions to submit both technical letters and letters of personal stories from physicians as to how these proposed cuts will impact patient care.
UCLA-SVS review course less than month away
There’s less than a month left to register for the Sixth Annual UCLA-SVS Symposium set to take place Oct. 1 to 3 at the Beverly Hilton in Beverly Hills, California.
“A COMPREHENSIVE REVIEW AND UPDATE OF
What’s New in Vascular and Endovascular Surgery” offers a valuable, in-depth review of the specialty for those preparing to take the vascular board examinations as well as providing the basic didactic education for vascular residents and fellows in training.
The Division of Vascular and Endovascular Surgery at UCLA and the Society for Vascular Surgery offer the course jointly. More information, including the course description, faculty, agenda, objectives, accreditation and more, is available at vascular.org/ Symposium21.—Beth Bales
“Surgeons like being trained by surgeons who they know, who can speak clearly about the advantages of different therapies and different clinical settings,” said Kashyap.
Community practitioners do not typically have a great many opportunities for hands-on instruction, added McDevitt, chair of the new SVS Community Practice Section.
“Our surgeons read about techniques but need a comfort level when they start executing them,” he said. “Educational opportunities are limited, as is the ability to try equipment unimpeded.”
In addition, new devices are introduced frequently. “Surgeons need to know ‘where does this new device fit into my practice,’” said Geraghty. “They want clear feedback and advice.”
The workshop will feature only approved devices grouped by areas of different facets of participants’ clinical practices.
CMS’ proposed physician fee schedule, if implemented as proposed, will result in a devastating 11.4% cut to vascular surgery. That cut incorporates changes to the conversion factor, the fourth and final year of the market update to supplies and equipment, and a new proposal to update clinical labor pricing. This year’s drop is reinstating the cut that Congress prevented last year, which further emphasizes the need for continued congressional intervention to protect patient care, advocates have said. By some estimates, vascular surgical procedures are set to incur some of the steepest cuts under the proposed rule.
CMS cuts are particularly harsh for revascularization services, especially in the office setting or OBLs, with some cuts estimated up to 22%. SVS is mobilizing members and all resources possible in an attempt to educate CMS on the impact of these cuts on patient lives and the business of running an effective private
First patient enrolled in AAA-SHAPE Netherlands study Shape Memory Medical has announced the initiation of AAASHAPE Netherlands, the company’s prospective, multicenter early feasibility study of the Impede-FX RapidFill device when used for abdominal aortic aneurysm (AAA) sac management during elective endovascular aneurysm repair (EVAR). The Dutch study’s first procedure was performed by Michel Reijnen, MD, a vascular surgeon at Rijnstate Hospital in Arnhem, The Netherlands. Ted Ruppel, president and chief executive officer of Shape Memory Medical said, “The addition of Dutch sites to the AAA-SHAPE program accelerates our ability to evaluate Impede-FX RapidFill and its potential to improve sac regression in AAA patients following EVAR.” The study will enroll up to 15 patients across three centers in The Netherlands.— Jocelyn Hudson
Workshop topics will cover the entire gamut of PAD, including the latest tools and treatments such as deep vein arterialization, tibial interventions, intravascular ultrasound (IVUS) and intravascular lithotripsy. Of note, cadaver specimens, table-top models and hands-on deployment will be utilized to optimize the sessions.
Additional didactics on national trends in open and endovascular therapies, treatment settings, complications, plus billing and coding will be highlighted.
Adding this training is an important step for the Society and its members, said Kashyap. “Every day, every month, we have tremendous changes in treating occlusive disease. Feedback from the Vascular Annual Meeting (VAM) showed that members want really hands-on, detailed information on advanced endovascular techniques.”
Registration will open the first week in November. Look for information in the Pulse biweekly electronic newsletter, on social media and other SVS channels.
practice. “If these cuts go into effect, we may lose a large percentage of private practices as they simply will no longer be able to sustain sufficient margin to pay for employees, supplies and office space,” noted Shutze.
The proposed cuts are also being driven by a provision that purports to update clinical labor data, with an anticipated severe impact on cardiology, vascular surgery, venous, radiation oncology and radiology practices. Earlier this summer, the Surgical Care Coalition—of which the SVS is a member—said the fee schedule failed to address pending cuts to surgical care and continued to threaten patient care by reaffirming “previously imposed misguided cuts.”
“We believe we understand what CMS is trying to do, but the methodology and focus is sufficiently flawed and harmful to the mainstream of Medicare recipients who are in need of vascular care, that implementation must be halted,” said Sideman. Bryan Kay
Spotlight:
Daniel Clair, MD, has been named the inaugural chair of the newly formed Department of Vascular Surgery in the Section of Surgical Sciences at Vanderbilt University Medical Center and professor of vascular surgery in the Vanderbilt University School of Medicine, Nashville, Tennessee. His appointment is effective Oct. 1.
Member Rajesh Malik, MD, has been appointed chief of vascular surgery at New York-Presbyterian Brooklyn
Methodist Hospital. He is an assistant professor of surgery (interim) at Weill Cornell Medicine. In his new role, Malik will lead the expansion of vascular surgery services at the hospital. He is a founding member of the South Asian American Vascular Society.
Caitlin W. Hicks, MD, and Linda Harris, MD, are editors of the new book Vascular Disease in Women: An Overview of the Literature and Treatment Recommendations, which highlights the epidemiology, natural history and treatment of vascular disease in women. Scott Kujath, MD, has been named the new medical staff president of North Kansas City Hospital in Kansas City.
Corner Stitch
In this month’s trainee column: Mindfulness and wellbeing
The art of surgery in the present moment
BY ANNA KINIO, MD
As a young surgeon-in-training, and a millennial, the concept of mindfulness and wellbeing perfuses my day-to-day life. Reminders of the importance of “being present” and “taking care of yourself” come from all directions: in newsletters, inspirational quotes on social media and advertisements offering everything from yoga classes to aromatic diffusers. I am as guilty as the next person of falling for this materialistic version of wellbeing, buying the agenda with inspirational quotes that will surely change my life, or signing up for a meditation app that I use religiously for a week before letting it fall by the wayside.
BUT BEYOND THIS SUPERFICIAL and easily marketable concept of mindfulness, I do believe that the art of being present has an important place in our lives, and especially in the operating room (OR). As someone with a constant stream of self-talk, much of it negative, I was forced to address this head-on in my second year of residency. As Henry Ford famously put it—“Whether you think you can or you think you can’t, either way you are right”—and I decidedly thought
that I could not. In the OR, I would live in fear of performing in front of my staff. The nerves would start the night before and increase until I was in the OR, shaking and berating myself harshly for performing so poorly, sometimes also playing a script of what I was sure the staff were thinking in my head. Clearly this did nothing to help my surgical prowess, and led to even simple acts becoming tense and poorly executed. Understanding the concept of
Insights from the VAM 2021 floor: The future of vascular surgery
BY KRISTIN CROWE AND ANNA VECCHIO
The Vascular Annual Meeting (VAM) presents great opportunities for medical students and residents who aspire to be vascular surgeons to network with, engage with and learn from vascular surgeons from all over the world. After a long day of vascular education, many of these VAM 2021 attendees gathered at the General Surgery Resident and Medical Student Reception Aug. 18, the first day of the meeting. The reception presented a chance for future vascular surgeons to build connections and network with their peers.
They shared what brought them to this year’s VAM,
mindfulness has traditionally been difficult for the surgical community, which is ironic given the great amount of mindfulness that occurs in a surgical theater. As Carter C. Lebares, MD, director of the UCSF Center for Mindfulness in Surgery in San Francisco puts it: “mindfulness consists of specific cognitive skills including interoception (an awareness of passing thoughts, emotions and sensations), emotional regulation (development of nonreactivity in response to stimuli) and metacognition (conscious awareness of one’s cognitive control processes).”
will start making mistakes. While the studies on mindfulness in surgery remain small, research confirms the positive effects of mindfulness-based training that seems intuitive. Studies show that using mindfulness training can improve executive function scores, increase the speed of motor skills, improve working memory, and lower stress and surgeon burnout.
“The nerves would start the night before and increase until I was in the operating room, shaking and berating myself harshly for performing so poorly”
It is clear that these skills are already being put to use in the OR by many of the attendings with whom we work. They may be recognized as those who are able to obtain the “flow state” where total focus on the present activity leads to complete union with the task at hand.
Beyond achieving this desirable state, the implications of the surgeon’s mindfulness-based skills extend beyond him or herself. The surgeon who can take a breath and calmly deal with intraoperative bleeding will create a better working environment than the surgeon who starts cursing, worrying that his or her patient will die, and barking at the assistant and anesthesiologist, who in turn
and some advice they would give to their younger selves, as well as to anyone just starting out in the medical field—student or otherwise.
“I worked on a project with Thomas Forbes, division chair and professor at the University of Toronto. The project was accepted for presentation at VAM, which intersected my involvement with the project and my interest in vascular surgery. It was perfect,” said Allen Li, a medical student at the University of Ottawa, Canada.
“Don’t be afraid to be involved and to do things that you want to do,” advised Jessica Nguyen, a medical student at Queens University, Kingston, Ontario, Canada. Nguyen encouraged students not to “mute themselves,” and encouraged them to speak up and truly get involved.
A group of rising fourth-year medical students had the occasion to meet and connect with each other for the first time at VAM, touching on what they were most looking forward to at the in-person meeting.
SVS Diversity Medical Student VAM Travel Scholarship recipients Falen Demsas, Ariel Francois and Aderike Anjorin talked of their excitement at the
As for my journey, it continues to be a work in progress, but I am happy to be evolving away from the anxiety-ridden and overly self-conscious version of myself. Lots of practice on my surgical skills has helped, but so has working on being fully present when performing a task in the OR. For me this is the true value of mindfulness, far from the commercialized idea that we put on a pedestal. I think that, as a specialty, we will only gain value in recognizing mindfulness as a skillset that needs to be actively developed and worked on for a fully balanced surgical training.
I know for my part it is a muscle which I will continue flexing every day. After all, the present moment is all we truly have.
ANNA KINIO is a vascular surgery resident in the department of surgery at McGill University in Montreal.
prospect of meeting other like-minded people who share a similar interest and passion for the future of the vascular surgical specialty.
“VAM has given me the invaluable opportunity to meet fellow students and see the latest research in the field,” said Anjorin, who is currently taking a research year at Duke University School of Medicine in Durham, North Carolina.
“VAM gives a great feel for the culture of different programs. Most interviews will be virtual for this year, so having the opportunity to meet anyone I can and find my place in the field is very valuable,” said Deena El-Gabri, a fourth-year medical student at the University of Wisconsin.
“Most interviews will be virtual for this year, so having the opportunity to meet anyone I can and find my place in the field is very valuable” — Deena El-Gabri
Ashley K. Vavra, MD, and Christopher J. Smolock, MD, talk to Vascular Specialist about why they decided to collect patientreported outcomes (PROs), how they got started with them and the challenges they have faced. Vavra is a member and Smolock a recent member of the Society for Vascular Surgery (SVS) Performance Measures Committee.
Why did you decide to collect patient-reported outcomes?
AV: My feeling is that PROs are a way to help us as vascular surgeons better set expectations among the patients who we treat for how a vascular disease or treatment will affect their day-to-day life. As we learn more, I am hopeful that PROs will also help us learn how to better define the success of particular treatments or interventions.
CS: Seeing patients in long-term followup, it became apparent that a technically successful and complication-free intervention or operation did not always correlate positively with a patient’s quality of life (QOL) throughout recovery. A striking example of this paradox is in acute aortic dissection patients who are treated by means of percutaneous endografts.
How did you get started?
AV: I first looked at the literature on PROs in vascular surgery patients. However, the more I read, the more questions I had about which measures to collect and how to collect them. I found it helpful that the SVS released reporting guidelines for thoracic outlet syndrome that included two recommended PRO measures for collection; I used that as a starting point.
CS: We began using general QOL/ PRO surveys in retrospective research studies, one of which involved patients with total aortic replacement in multiple modalities over multiple stages. We began
USPSTF expands prediabetes, type 2 diabetes screening recommendation
The United States Preventive Services Task Force (USPSTF) has issued an updated recommendation statement suggesting that clinicians screen for prediabetes and type 2 diabetes in overweight or obese adults aged 35–70 years—capturing adults at an age bracket five years younger than that contained in the previous advisory from 2015.
THE B-CLASSED RECOMMENDATION MEANS THE USPSTF BELIEVES there is high certainty the net benefit from the offer or referral for effective preventive interventions is moderate “or there is moderate certainty that the net benefit is moderate to substantial.”
The update is based on a systematic review aimed at evaluating screening for prediabetes and type 2 diabetes in asymptomatic, non-pregnant adults as well as preventive interventions for those with prediabetes.
“Based on data suggesting that the incidence of diabetes increases at age 35 years compared with younger ages, and on the evidence for the benefits of interventions for newly diagnosed diabetes, the USPSTF has decreased the age at which to begin screening to 35 years,” the statement reads.
Furthermore, evidence on the optimal screening interval for adults with an initial normal glucose test result is limited, with cohort and modeling studies suggesting that “screening every three years may be a reasonable approach for adults with normal blood glucose levels.”
USPSTF members led by Karina W. Davidson, PhD, of Feinstein Institutes for Medical Research at Northwell Health, Manhasset, New York, authored the recommendation, which was recently published in the Journal of the American Medical Association (JAMA). “Screening asymptomatic adults for prediabetes and type 2 diabetes may allow earlier detection, diagnosis, and treatment, with the ultimate goal of improving health outcomes,” the authors wrote. The update replaces the 2015 USPSTF recommendation statement.—Bryan Kay
approaching extensive aortic repairs in this manner, presuming an advantage for the multi-stage, multi-modal approach in survival and QOL. Instead, we observed that patient QOL was not necessarily better than single-stage, open surgery.
How do you collect the PROs?
AV: I started collecting PROs prospectively using a paper form that is then entered in the electronic medical record (EMR). However, our institution has now set up a method of electronic collection for patients through the patient portal of our EMR.
CS: We started collecting prospectively and electronically for some patients during outpatient check-in but are still working through this process.
How do you use them with patients?
AV: So far, I have only used them on an individual patient basis and discussed trends if they are available.
CS: I use retrospective QOL data following aortic interventions to inform patients of potential challenges post-procedure that might seem counterintuitive. This has been especially helpful for our patients who experience weeks to months of malaise after a percutaneous intervention for
aortic dissection, as it educates them on this expected outcome. The minimally invasive nature of such a procedure does not necessarily prepare the patient for a prolonged period of convalescence.
What challenges have you faced?
AV: The first challenge is response rates, and I have found that having an option to collect measures while patients are in the office is helpful. Another challenge is how to use the data. Since I have yet to analyze the data from our own experience and there aren’t benchmarks to help guide interpretation, I find it challenging to know exactly how to counsel patients on their results. Hopefully, this will improve as we learn more about how specific measures correlate with vascular disease and treatments.
CS: We are working on incorporating disease-specific PROs for each of the entities we treat. We also need to broaden the reach of this to the majority of our outpatient visits in a way that is not onerous to the patient or the provider.
“I find it challenging to know exactly how to counsel patients on their results.”—