Landmark trial finds benefit from carotid stenting
By Bryan Kay
02 From the Editor
2 From the editor
Malachi Sheahan III issues a call for call pay
A modest proposal: Let’s eat the trauma surgeons
8-9 Comment & Analysis Surgeons on the frontlines: A tale of unspeakable horror and an thirst for freedom
11 Leadership SVS celebrates ascendency of former president to ACS presidency
31 The Alzheimer’s study A new pathway for preventing dementia?
16 Paclitaxel SWEDEPAD: ‘We need to look at the evidence’
33 Drug-coated technology IN.PACT AV DCB shows sustained and superior performance compared to PTA through three years
18 VQI SVS smoking cessation initiative aligns with national cancer society effort to curb habit
www.vascularspecialistonline.com
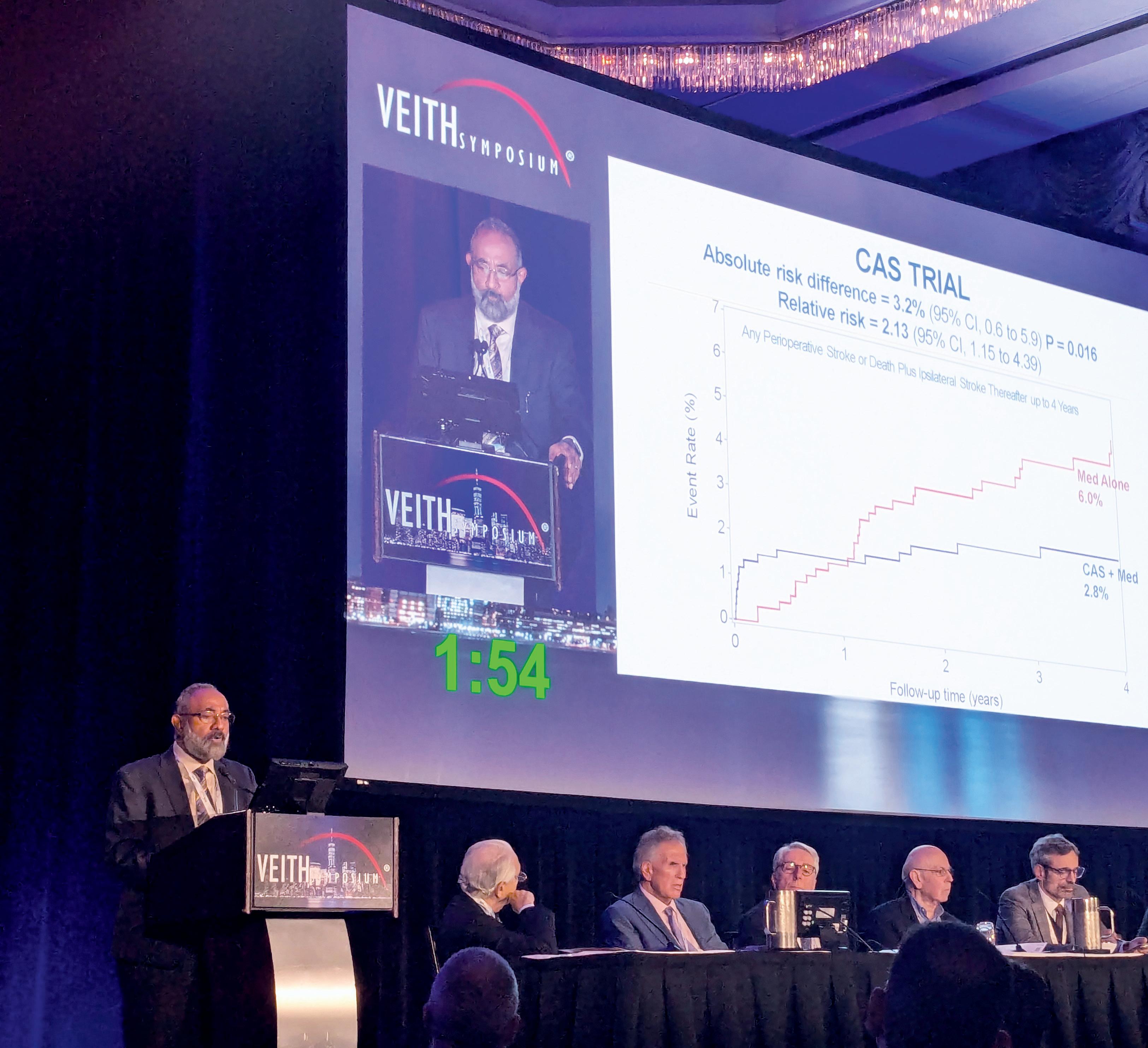
THE NATIONAL INSTITUTES OF HEALTH (NIH)-funded CREST-2 study has found that, for people with high-grade asymptomatic carotid artery stenosis who have not experienced recent stroke symptoms, a carotid artery stenting (CAS) procedure—combined with intensive medical therapy—significantly lowered stroke and death rates compared with medical therapy alone. The more traditional “gold standard” approach of carotid endarterectomy (CEA) did not show the same benefit, however.
These first “game-changing” results outlining four-year outcomes were presented at the 2025 VEITHsymposium in New York City (Nov. 18–22) by CREST-2 co-principal investigator Brajesh K. Lal, MD, a professor of surgery at the University of Maryland in Baltimore. Earlier the same day, the data were delivered at the 2025 Society of Vascular and Interventional Neurology (SVIN) annual meeting in Orlando, Florida (Nov. 19–22) by James Meschia, MD, a vascular neurologist at the Mayo Clinic in Jacksonville, Florida. The trial results were also published in the New England Journal of Medicine
Lal outlined how the study’s two simultaneously-running randomized controlled trials (RCTs) comparing CAS plus medical therapy to medical management alone, and CEA plus medical therapy to medical management alone, enrolled 2,485 patients from 155 sites across five countries.
In the CAS trial, stroke and death rates out to four years were 6% in patients who were assigned medical management and 2.8% when CAS was added, Lal told VEITH 2025. “The absolute risk difference of 3.2% in favor of CAS was statistically significant,” he said.
In the CEA trial, stroke and death out to four years was 5.3% in the medical therapy group and 3.7% when CEA was added, Lal continued.
See page 4
ONE-YEAR RESULTS FROM IVC STENT CLINICAL TRIAL SHOW POSITIVE SAFETY AND EFFICACY DATA
By Bryan Kay
TWELVE-MONTH RESULTS from the clinical trial assessing a dedicated venous stent for the treatment of symptomatic inferior vena cava (IVC) obstruction with or without combined iliofemoral obstruction showed the device exceeded its performance goal for freedom from a composite of efficacy and safety events.
The data from 89 patients were presented at The VEINS 2025 (Nov. 1–2) in Las Vegas, by Stephen Black, MD, from King’s College London in London, England.
The prospective, multicenter, non-randomized, single-arm trial of the Viabahn Fortegra (Gore) venous stent—formerly known as Viafort—represents the first such independently adjudicated study examining the use of venous stent placement for the treatment of symptomatic iliocaval venous obstruction, Black told The VEINS 2025.
The overall rate of freedom from composite primary endpoint events was 74.7%, exceeding the 58% performance goal.
The composite is made up of freedom from loss of primary patency stent embolization through 12
See page 8
Brajesh K. Lal delivers CREST-2 results
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Managing Editor, SVS
Killian Meara
Senior Director for Public Affairs and Advocacy
Megan Marcinko Communications Specialist
Marlén Gomez
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell and Éva Malpass
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America 155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. | Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. | Printed by Ironmark |
Medical editor Malachi Sheahan III, MD, makes the case for surgeon call pay, a remuneration he says should be understood more as compensation than reimbursement.
The strongest desire of my early youth was to attain an Atari 2600TM video game console. A goal I finally unlocked with the financial windfall of my First Communion. As I opened the box, visions of Pac-Man, Space Invaders and Asteroids danced in my head. The cruel reality, however, was that the console only came with some janky free games—Breakout, Combat and Basic Math (yes, really). To unlock all of the 16-bit goodness that was now at my fingertips, I would need more than my paltry allowance. I would need a job. Since I was an 11-year-old boy with no perceivable skills, my options were limited to paperboy or some kind of Artful Dodger situation. I opted for the former.
To work at that age in New York required a special permit, so my father took me down to the local government offices. A sign on the wall listed the only two exceptions to the 14 minimum-age work requirement: paper carrier and child model. Since my orthodontic situation at the time could be generously described as “unfortunate,” it wasn’t too hard for the state workers to guess which forms I needed. My subsequent 45-year run in capitalism has taught me many lessons about the free market, but perhaps most germane to this editorial: it is hard to get paid for something you are already doing for free.
Justification for call pay
The very concept of call pay is often met by (feigned?) confusion from hospital administrators. Call pay should not be seen as reimbursement for work performed but rather compensation for the burden of being available. Call is not a passive activity; it restricts a surgeon’s freedom and imposes psychological stress, regardless of whether an operation is ultimately performed. That is the essence of surgical call: the omnipresent possibility of catastrophe. Call it Schrödinger’s retrohepatic caval injury. A vascular surgeon on call will often sacrifice sleep, family time and the ability to rest and recover. This availability is a service to the hospital, other physicians and the community at large. Like any professional service, it warrants payment.
a page. Back then, call coverage was often tied to admitting privileges. You wanted to operate at Hospital X? You took call. No questions asked. No compensation offered. By 1995, the rate of inpatient operations had dropped 14% from 1980, but the combined rate of inpatient and ambulatory procedures had increased by 70%. That’s not just growth—it’s a workload explosion. And who absorbed that growth? The surgical workforce.
The 1990s also marked the beginning of serious concern about surgeon supply. A longitudinal analysis of the general surgery workforce showed that between 1981 and 1991, the number of rural surgeons remained flat while urban numbers grew modestly. But the age distribution shifted: fewer young surgeons entered the field, and the average age crept upward. By 2005, only 16.2% of general surgeons were under age 40, compared to 25.1% in 1981.
This aging workforce was expected to cover more cases, more call and more administrative duties—all without additional compensation. The seeds of burnout were sown in this era, fertilized by rising malpractice premiums, declining autonomy and the slow erosion of professional respect.
In the halcyon days of medicine,
call was a badge of honor. Surgeons were summoned from dinner parties, golf courses and, occasionally, their own weddings
A call pay system provides inherent compensation for surgeons who step up to cover others taking vacation, on maternity/paternity leave or taking sick time. When compensation is transparent and equitable, resentment declines. Departments stop fighting over who “covers more” or who “gets stuck” on weekends.
A brief history of unpaid heroism
Let’s rewind. In the halcyon days of medicine, call was a badge of honor. Surgeons were summoned from dinner parties, golf courses and, occasionally, their own weddings. They arrived in tuxedos, operated in loafers, and returned to the reception with blood on their cuffs and applause in their ears.
It was romantic. It was cinematic. It was unpaid.
The tradition of uncompensated call dates to the post-World War II era, when most physicians were independent contractors, and hospitals were grateful for any warm body willing to answer
Hospitals in the 1990s were under pressure to cut costs. Managed care organizations pushed for shorter stays, fewer procedures and tighter reimbursement. The shift to outpatient surgery was supposed to save money—but it didn’t reduce the need for surgical expertise. Instead, it fragmented care and increased the complexity of scheduling, coverage and continuity. As call became more frequent and more fragmented, especially with the rise of multi-hospital systems, burnout began to rise. Until recently, however, this was dismissed as a personal failing rather than a systemic issue. But the science is clear: surgeons with more frequent call report higher rates of insomnia, depression and early retirement. The American College of Surgeons (ACS) reported in 2024 that even home call measurably disrupts sleep cycles and increases burnout risk among acute-care surgeons. Fast forward to the 2000s. Hospitals began acquiring practices, and physicians became employees. The shift from autonomy to employment brought new expectations—and new frustrations. Call was no longer a favor—it was a line item. But unlike base salary, it remained nebulous, inconsistent and, in many cases, non-existent. The new compensation models lagged behind reality, failing to account for the expanded scope and intensity of surgical labor.
Hospitals love to talk about value-based care. But when it comes to call, the value is often one-sided. Surgical departments generate up to 70% of hospital revenue, yet surgeons are expected to provide 24/7 coverage as part of their “professional duty.”
EMTALA—the Emergency Medical Treatment and Labor Act—has also had a profound and lasting impact on surgical call coverage in the U.S. Enacted in 1986 to prevent “patient dumping,” EMTALA mandates that any hospital with an emergency department must provide a medical screening exam and stabilizing treatment to anyone who presents with an emergency medical condition, regardless of their ability to pay.
Under EMTALA, hospitals are legally required to maintain a list of on-call physicians who can provide further evaluation and treatment for patients with emergency medical conditions. This includes surgical specialists such as trauma surgeons, vascular surgeons, neurosurgeons and orthopedic surgeons.
The law doesn’t just apply to hospitals—it also places obligations on individual physicians. If a surgeon is listed on
continued on page 4
SAFETY IS OUR DNA. AND MOA.
From our early egg-cracking experiments that fractured hard shells but preserved soft membranes to treating one million patients worldwide, Shockwave IVL has sparked a new era of safety for the treatment of calcified arterial disease. Our MOA is clinically-validated in over 20,000 published patient outcomes across over 500 journal articles.
Evidence Differentiated by Post-IVL Safety Outcomes
Consistently Low Post-IVL Rates of Serious Angiographic Complications Evaluated by Core Lab Across All Studies
NR=not reported.
1. Final results, post-IVL outcomes not reported. Brodmann, M., et al. J Am Coll Cardiol. 2017;70(7):908-10; 2. Final results, post-IVL outcomes not reported. Brodmann, M., et al. Catheter Cardiovasc Interv. 2019;93(2):335-42; 3. IVL arm, Tepe, G., et al. J Am Coll Cardiol Intv 2021;14:1352-61; 4. Armstrong, E.J., et al. J Endovasc Ther. 2024. doi:10.1177/15266028241283716; 5. Chandra, V., et al. J Vasc Surg. 2024. doi:10.1016/j.jvs.2024.11.003; 6. Corl, J.D. (2024). Primary outcomes of the FORWARD IDE and Feasibility Studies. VIVA Late-breaking clinical trial presentation, Las Vegas, NV; 7. Final results, post-IVL outcomes not reported. Brinton, T.J., et al. Circulation. 2019;139:834-36; 8. Ali, Z.A., et al. Circ Cardiovasc Interv. 2019;12:e008434; 9. Hill, J.M., et al. J Am Coll Cardiol. 2020;76:2635-46; 10. Saito, S., et al. Circ J. 2021;85:826-33; 11. Hill, J., et al., Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease, Journal of the American College of Cardiology, 2020; 101016
LANDMARK TRIAL FINDS BENEFIT FROM CAROTID STENTING
“The absolute risk difference was still in favor of CEA; however, it did not reach significance.”
Lal explained: “The patterns of differences in the CAS and CEA trials were mirrored in the 44-day periprocedural period; however, in the post-procedural period starting 45 days out to four years, both CAS and CEA performed better in terms of preventing stroke and death compared to their respective medical management groups.”
Concluding, Lal emphasized how the absolute difference favoring CAS was significant, with “31 people with high-grade asymptomatic carotid stenosis needed to be treated to prevent a primary event at four years in the trial.”
FROM
THE EDITOR A CALL FOR CALL PAY
the call schedule and fails to respond in a timely manner, they can face civil penalties of up to $50,000 per violation, and even exclusion from Medicare participation. This makes call coverage not just a professional duty, but a federal legal requirement.
While EMTALA was designed to protect patients, it has created significant challenges for hospitals and physicians.
Increased call burden: Hospitals must ensure 24/7 coverage, often relying on a small pool of specialists. This leads to frequent and intense call schedules, especially in high-acuity specialties.
Uncompensated labor: EMTALA does not require hospitals to pay physicians for being on call. Many institutions still treat call as a “shared duty,” especially among employed physicians, despite the legal and clinical demands.
Recruitment and retention issues: Surgeons are increasingly unwilling to accept positions with heavy call obligations and no compensation. This is particularly true in trauma and acute care surgery, where burnout rates are high.
Legal risk: Hospitals and physicians alike face liability if EMTALA obligations are not met. This includes fines, lawsuits and reputational damage.
Data
Hospitals depend heavily on surgical departments for financial viability. Surgical services account for up to 70% of total hospital revenue and over 60% of operating margins. Elective and emergency surgeries generate substantial downstream revenue through diagnostics, inpatient care and rehabilitation. Yet, the surgeons who drive this revenue often do so without fair compensation for their oncall availability.
Only 33% of general surgeons report receiving call pay, compared to 43% of orthopedic surgeons and 39% of neurosurgeons. Only about 19% of academic surgeons report receiving call pay, compared to roughly 30% in
continued from page 1
Thomas Brott, MD, co-principal investigator and a professor of neurology at the Mayo Clinic College of Medicine in Jacksonville, Florida, followed Lal at the VEITH 2025 podium to tackle whether the CREST-2 evidence is conclusive or further study is needed.
“In one generation, since ACAS, we’ve gone from medical risk of 11% to a risk of 6%, which is remarkable, particularly in light [of the fact] that today our surveillance is via MRI [magnetic resonance imaging] in almost all instances,” he said.
“The trial shows CAS is effective, Brott continued, with its stroke and death rate “one half of medicine alone.” As for CEA, he said, “there is a difference, but it did not reach statistical significance.”
continued from page 2
private practice. Sources vary in terms of the prevalence of call pay, however. A 2024 SullivanCotter report showed that, between 2007 and 2012, the proportion of U.S. hospitals providing some form of oncall stipend increased from 48% to 63%.
According to the recent SVS/Phairify compensation study, the vast majority (93%, 660/708) of vascular surgeons took first call for vascular issues at their institutions, of which 64% (422/660) were on call on average one in four weekday nights and weekends. Most respondents (80%, 545/682) were not paid for primary call separate from their salary.
The Medical Group Management Association (MGMA) 2024 report based on 2023 data shows the median daily rate for on-call compensation for vascular surgeons is $1,000 per 24 hours. The same data source shows that the most popular method of call payment calculation is a daily rate (45%), followed by hourly (31%) and then an annual stipend (11%). Many systems will vary their rate by acuity metrics such as number of emergency room referrals per week or number of emergent procedures performed annually.
For a full picture of the call pay landscape, several sources are available: Specialty compensation and call-stipend surveys (SullivanCotter, MGMA DataDive) that report employer-paid stipends and on-call practices across hundreds of hospitals and dozens of specialties are the gold standard for benchmarking institutional stipends. Commercial locumtenens and staffing reports (CompHealth, Locumstory, Barton Associates, Sermo) disclose what hospitals pay external providers for temporary coverage—a revealing market price for guaranteed availability. And there are also specialtyfocused surveys on call burden and compensation (e.g., Buckhead FMV/ BFMV call surveys) that combine burden metrics (days on call, phone volumes) with stipend data.
Many of these are behind a paywall that exceeds my modest investigative
So, Brott asked, are future studies needed?
“Yes of course,” he said, going on to list several areas in need of scrutiny, among them carotid plaque risk, patients with higher risk features, carotid stent optimal design, flow reversal as well as the optimal regimen of medical therapy.
“The elephant in the room in one of these areas of further study is TCAR [transcarotid artery revascularization]: no level-1 evidence. But a randomized controlled trial showing a drop in risk that you would consider clinically significant over four years would require a sample size of 4,400 patients,” he added. “Discoveries will happen, but rock-solid validation may not be feasible via RCTs in patients with asymptomatic carotid disease.”
journalism budget, but you can be assured your hospital administrator has access. Call pay arrangements must comply with federal regulations, including the Stark Law and Anti-Kickback Statute. The Office of the Inspector General (OIG) has issued several advisory opinions regarding call pay. To summarize, call pay can’t be used as a kickback from the hospital to physicians for bringing their patients to that institution.
Special circumstances
Hospital employment: Hospital-employed physicians often have a minimum number of uncompensated calls per month, with additional payment for calls exceeding this number. The problem is establishing how much call is expected with base compensation. It is difficult to find an industry standard for the frequency of either general or vascular surgery call. However, an article from Kim Mobley, managing principal and physician compensation practice leader at Sullivan, Cotter and Associates, Inc., cites the average and typical frequency as one in five days. Therefore, calls exceeding six per month should be expected to be compensated in a hospital-employed model.
Trauma center coverage: In the U.S., trauma centers are designated by regional governments and most rely on the standards set by the ACS. The ACS publishes its requirements in the Resources for Optimal Care of the Injured Patient manual. It is explicitly stated that for all Level I and Level II adult and pediatric trauma centers, “expertise in vascular surgery” is mandatory and must be provided with continuous 24-7365 availability. This is categorized as a Type I standard, meaning verification is automatically withheld if it is not met.
Tertiary care centers: In tertiary care centers performing complex procedures, it is essential to have a plan in place to deal with vascular complications related to procedures performed by other specialties
such as cardiology, radiology, general surgery, interventional nephrology, surgical oncology, orthopedic surgery, or interventional neurosurgery. A simple work relative value unit (wRVU) model undervalues this work as the assisting vascular surgeon will likely need to disrupt their own clinic and operative schedule. Therefore, additional compensation should be provided for these services. Studies have shown that cases in which a vascular surgeon assists another specialist have high contribution margins and case mix indices.
The call for call pay
Ultimately all politics are local. To make the appeal for call pay you will have to sell it to your C-suite. So, in their own terms, here is a summary of the benefits of paying vascular surgeons for call.
1. Improving surgeon retention will avoid costly recruitment and onboarding expenses. Retention also stabilizes surgical service lines that generate significant hospital revenue.
2. Preservation of trauma designation.
3. Revenue capture: surgeons on call admit and treat emergent cases rather than transferring them, which increases inpatient and procedural revenue. Highacuity cases often drive downstream revenue (intensive care unit [ICU] stays, imaging, follow-up procedures).
4. Risk mitigation by avoiding EMTALA violations and malpractice claims.
5. Cost vs. ROI: a single, high-revenue emergency case can offset weeks of call pay stipends, making the investment commercially reasonable. The locum market’s premium shows hospitals will pay to avoid gaps, supporting the argument that predictable stipends are an investment. Data from staffing and compensation reports show dramatic locum rate spikes in undercovered specialties—a market inefficiency that fixed stipends can reduce.
MALACHI SHEAHAN III serves as the medical editor of Vascular Specialist
Confirm your Vascular Specialist digital subscription
Dear reader:
We are reaching out to share important news regarding your digital subscription for Vascular Specialist. Today, you are receiving Vascular Specialist digital content from BIBA Medical, the current publisher of the newspaper. Beginning in January, the Society for Vascular Surgery (SVS) will take over full production—print and digital—of Vascular Specialist. In preparation for this transition, we are asking all digital subscribers to confirm their subscription for 2026.
Click here to confirm your digital subscription and receive online Vascular Specialist content from the SVS.
You also have the opportunity to remain a subscriber of BIBA Medical. Click here to continue receiving content from BIBA Medical.
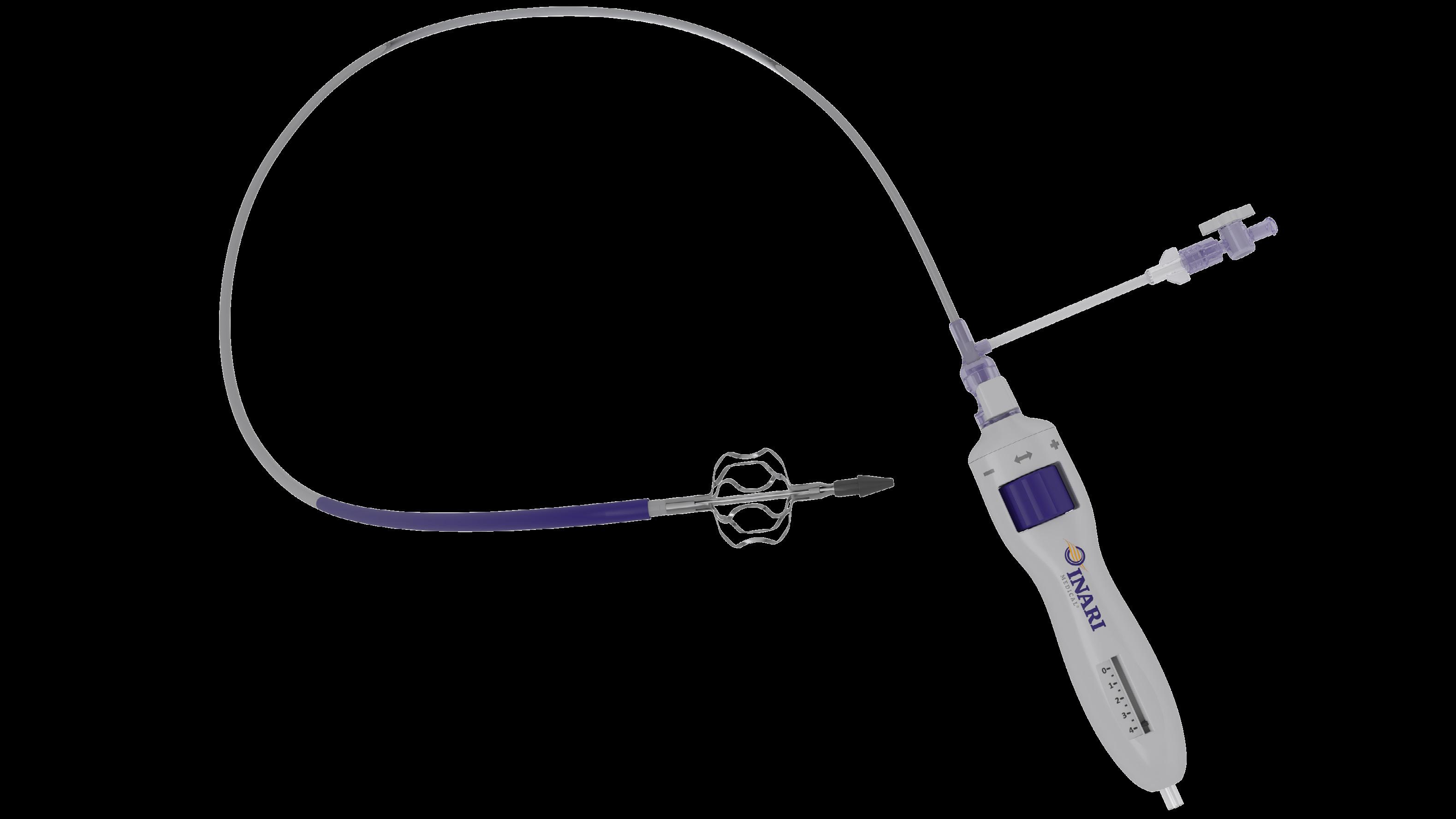
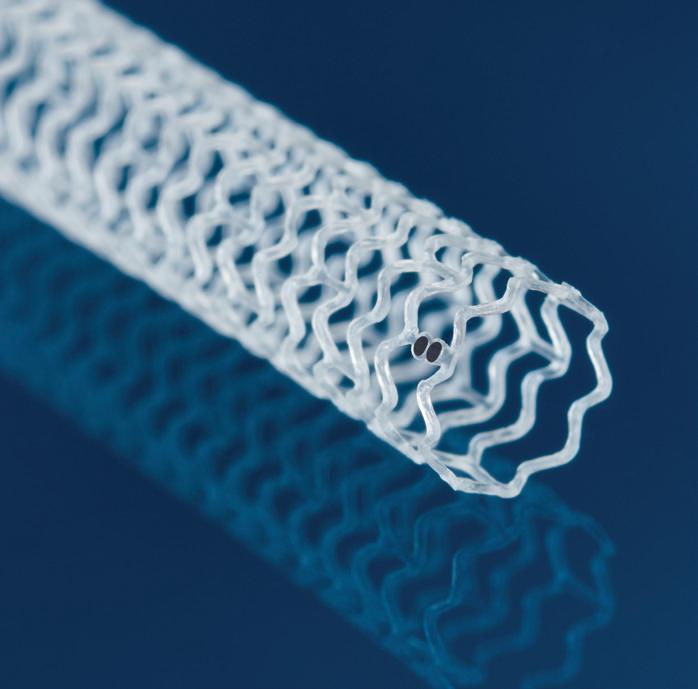
RevCore™ Thrombectomy Catheter
The First Mechanical Thrombectomy Device for Venous Stent Thrombosis
Indications For Use:
The RevCore Thrombectomy Catheter is indicated for (1) The non-surgical removal of thrombi and emboli from blood vessels (2) Injection, infusion, and/or aspiration of contrast media and other fluids into or from a blood vessel. The RevCore Thrombectomy Catheter is intended for use in the peripheral vasculature. Refer to IFU for complete Indications for Use, contraindications, warnings, and precautions.
Caution: Federal (USA) law restricts this device to sale by or on the order of a physician. All trademarks are property of their respective owners.
Stent maintenance: Sustaining long-term patency in the deep venous system
As venous stenting becomes more common, the focus must now shift to what occurs after the procedure, according to consultant vascular surgeon Stephen Black, MD, FRCS. The concept of stent maintenance is key, acknowledging that venous stents—once implanted—will require lifelong monitoring to maintain their function.
“When we stent venous patients, we have to remember that their life expectancy is completely different from patients with arterial disease,” says Black, from Guy’s and St Thomas’ NHS Foundation Trust in London, England, and professor of venous surgery at King’s College London. “These are people who will often live with their stents for 30, 40, even 50 years. It’s unrealistic to think that there will never be a need for ongoing follow-up, or that we can discharge them from care after a year or two.”
Unlike arterial or coronary disease, where long-term mortality remains high, venous patients typically live long, active lives after intervention. “The mortality after venous procedures is extremely low,” Black explains. “That means we have to think about what lifelong care looks like for these patients.”
Why surveillance matters
The first few weeks after stent implantation represent a critical window for detecting early stent failure. “Most stents that fail do so early,” explains Black. To better understand and mitigate this risk, his team at Guy’s and St Thomas’ analyzed a decade of surveillance data from 348 patients with chronic post-thrombotic syndrome (PTS), representing more than 500 treated limbs. The findings were clear: re-intervention occurs early, with nearly 50% taking place within six weeks and two-thirds prompted by ultrasound surveillance rather than symptoms, resulting in an acute presentation. A two-week surveillance scan proved highly pre dictive of long-term outcome. Pa tients with >50% in-stent reste nosis had significantly poorer patency even after re-in tervention (p<0.0001), while 30–50% in-stent stenosis was also as sociated with higher re-intervention rates (p=0.0019). “These early scans allow us to identify high-risk patients and act before stent occlusion
occurs, improving long-term secondary patency,” says Black. At St Thomas’ Hospital, the standard ultrasound surveillance protocol for venous stents is one day, two weeks, six weeks, three months, six months and one year post-intervention. “Patients with early in-stent restenosis need closer imaging and perhaps earlier intervention,” Black explains. This approach, he says, will make post-stent care more efficient and better targeted.
Black emphasizes that even in patients who initially do well, circumstances can change. “Life happens,” he says. “A patient might do perfectly fine for years on anticoagulation, but if they have children, or undergo another surgery where anticoagulation needs to be interrupted, they can develop in-stent restenosis.”
Understanding and defining in-stent restenosis is becoming increasingly important. “We’re starting to look at what constitutes in-stent restenosis and what tools we can use to tackle it,” Black says. “It’s been encouraging to see innovation in this space. Technologies like the RevCore Thrombectomy Catheter and VenaCore Thrombectomy Catheter (Stryker/Inari Medical) are part of an expanding toolkit, but we’re still in the early stages.”
Pairing technologies for the future
“Simply debulking the stent is not enough,” Black continues. “We also have to think about what adjunctive technologies we need, whether that’s improving vessel inflow, addressing wall inflammation, or enhancing the biological environment to keep stents patent over time.
“Debulking technology will need to be paired with other tools. Once a stent occludes, it can be almost impossible to cross. You can have the best device in the world, but if you can’t get through the occlusion, you can’t
use it. So we need to think about how we cross more effectively and what adjunctive tools will make that achievable.”
He also raises the possibility that stents themselves may alter venous biology over time. “A vein is a capacitance vessel. It’s designed to expand and contract depending on flow,” he explains. “Once you stent it, that adaptability is gone. That may be one of the reasons we see progressive stenosis develop years later.”
Evolving toward biological solutions
Looking ahead, Black envisions new ways to support stented veins and maintain physiologic flow. “We may have to think about
how we modulate flow through intermittent pneumatic compression, muscle stimulators or other existing technologies,” he says. “But more interestingly, bioabsorbable materials might play a role. A stent that restores flow, then dissolves, could return the vessel to normal function without lifelong maintenance. We’re not there yet, but it’s something to watch closely.”
Ultimately, Black emphasizes that stent maintenance is a lifelong commitment. “Once we place a stent, we take on the responsibility to look after that patient for as long as they live,” he says. “We have to understand what lifelong management really looks like and make sure we’re ready to deliver it.”
This article is sponsored by Inari Medical. The HCPs sharing their views and opinions here express their experience with Inari Medical devices. The HCPs’ opinions of these devices were formed independently of Inari Medical and may not represent every experience or outcome with the devices. Indications For Use: The RevCore thrombectomy catheter is indicated for (1) the non-surgical removal of thrombi and emboli from blood vessels and (2) injection, infusion, and/or aspiration of contrast media and other fluids into or from a blood vessel. The RevCore thrombectomy catheter is intended for use in the peripheral vasculature. The VenaCore Thrombectomy Catheter is indicated for (1) the non-surgical removal of thrombi and emboli from blood vessels; and (2) injection, infusion and/or aspiration of contrast media and other fluids into or from a blood vessel. The VenaCore Thrombectomy Catheter is intended for use in the peripheral vasculature. Review complete Instructions for Use, Indications for Use, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the product. Caution: Federal (USA) law restricts this device to sale by or on the order of a physician. For all non-Inari products, please refer to
Stephen Black
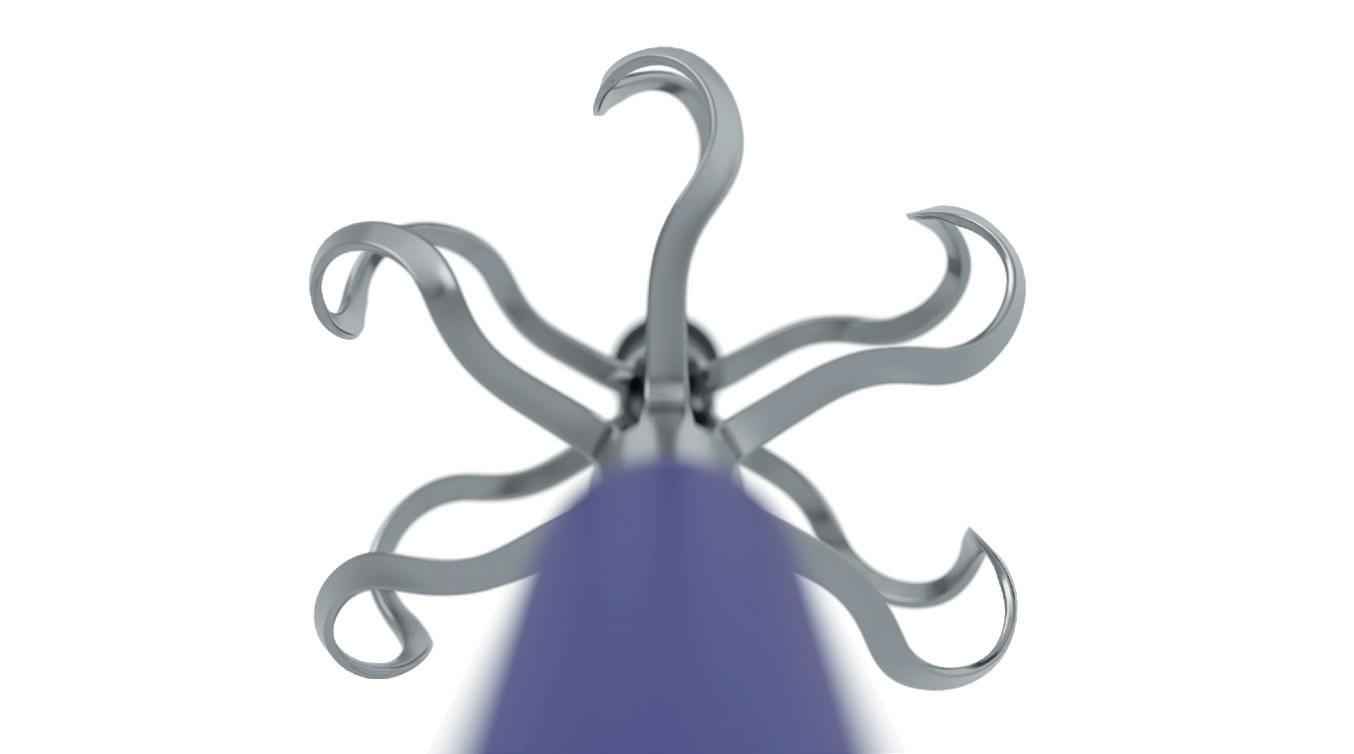
From top: The RevCore device, tip close up and device simulated in anatomy
PULMONARY EMBOLISM
PERT, AI AND THE RISE OF THROMBECTOMY DEVICES: ‘PERT LEADS TO MORE ADVANCED
THROMBECTOMY REMOVAL THERAPIES,
By Bryan Kay
LOWER HOSPITAL STAYS’
THE INCREASING SOPHISTICATION of the device space for the treatment of pulmonary embolism (PE) aligned with advances in the deployment of pulmonary embolism response teams (PERTs) are among factors leading to notable improvements in care, according to leading vascular surgeon Patrick Muck, MD.
The chief of vascular surgery at Good Samaritan Hospital in Cincinnati, Ohio, has led a number of recent papers exploring the addition of artificial intelligence (AI) to the PERT at his institution and subsequent gains derived from the move.
The most recent data presented at the 2025 Midwestern Vascular Surgical Society (MVSS) annual meeting in Cincinnati (Sept. 18–20) showed that the use of AI technology to diagnose a patient with a PE can lead to earlier anticoagulation and intervention in the appropriate patient, and that, with improved time to treatment of PE using AI, there may also be a decrease in mortality. “There are probably 20-plus devices either already available or going
to be available soon,” observes Muck during an interview at the recent 2025 VEITHsymposium in New York City (Nov. 18–22), where he moderated a pair of sessions covering thrombectomy devices across both the arterial and venous systems. “The reason there are so many devices is that PE is such an unmet need and it is the number one cause of preventable death for in-hospital patients. That, coupled with the fact these devices are decreasing the need for adjunctive thrombolysis, is exciting.”
Muck says his team have presented at the likes of MVSS, the PERT Consortium and, again next year at the 2026 American Venous Forum (AVF) in Denver, Colorado (Feb. 28–March 4), data showing that, with PERTs, “it is not so much door-tothrombectomy time” where AI proves its worth. “What makes it so important is that it allows for rapid diagnosis, which leads to rapid communication amongst the PERT team members, which leads to more rapid initiation of anticoagulation,” he
explains. “That’s the real benefit of AI. It’s not like door-to-balloon in MI [myocardial infarction], or some aspects of the stroke service, but door-to-diagnosis and thereby door-to-triage time.”
The addition of AI shows up in patient outcomes, Muck continues. “We know that every hour that a patient is not anticoagulated with a pulmonary embolism, mortality goes up. The patient can go through the CT [computed tomography] scan and, within six minutes, typically you can get a diagnosis or an AI alert of a positive PE, which then sets off a communication amongst the team members, which leads to quicker triage and thereby anticoagulation. As for PERT, plenty of publications show that centers that have a PERT have a higher usage of advanced thrombectomy devices,
shorter hospital length of stay, as well as lower mortality.”
Muck and colleagues launched their own PERT at Good Samaritan in January 2013 and added AI to the system in 2022, deploying the Viz.ai detection software.
“It takes a village of people coming together to offer the best-in-class
at one of his kids’ lacrosse or soccer games, armed with his computer in the event he would receive an alert for a patient with a PE. With time of the essence, he’d then have to navigate logging on, firewalls then a CT scan before being able to provide an opinion on the best therapy for the patient at hand. Now, with the AIdriven notification sent to his phone, the turnaround is revolutionized.
continued from page 1
months of follow-up; freedom from device- or procedurerelated death; clinically significant pulmonary embolism confirmed via computed tomography angiography (CTA); device- or procedure-related vascular injury requiring surgical or endovascular intervention; and device- or procedure-related major bleeding events through 30 days.
Additionally, there was “a significant improvement in patient pain levels from baseline to 12 months, as seen by a mean reduction in the rVCSS [revised Venous Clinical Severity Score] pain score of less than or equal to
1,” Black revealed.
Some 94.3% of patients in the trial had lesions spanning three-vessel regions—the IVC and bilateral iliofemoral, he said. U.S. enrollment is now complete, Black added.
Gore is seeking an indication for use of the device in the IVC under the Food and Drug Administration (FDA) Breakthrough Device program.
The Viabahn Fortegra is being studied under two investigational device trials, with the other assessing its use for treatment of symptomatic iliofemoral venous obstruction at sites in the U.S.
“What makes it so important is that it allows for rapid diagnosis, which leads to rapid communication amongst the PERT team members, which leads to more rapid initiation of anticoagulation”
PATRICK MUCK
“In two minutes, I’ve logged in to the app, I can see a high-resolution CTA [CT angiography], the AI program gives you the RV-LV [right ventricle-left ventricle] ratio, the patient demographics and vital signs, and it’s like being right there next to the patient. It’s amazing,” he adds.
The Vascular Annual Meeting (VAM) has previously showcased how AI can shave considerable time off the process of determining management for individual patients. “You can make a diagnosis, put a plan together, discuss with members of the PERT team in real time, expedite consensus decision-making and treatment logistics far more efficiently,” Dennis Gable, MD, commented during VAM 2023.
Care for IC considered ‘inappropriate’ found to be common, putting patients at ‘increased’ risk
IN A MULTI-INSTITUTIONAL COHORT
OF patients with intermittent claudication (IC), care deemed inappropriate, or where the risk outweighs the benefit, by the SVS appropriate use criteria (AUC) for the management of IC was “common” and associated with increased risk of symptom recurrence, reintervention and amputation, a retrospective review showed.
Furthermore, in patients with mild-to-moderate lifestyle limitation, appropriate treatment was associated with no amputation, whereas inappropriate treatment was associated with a greater than 8% incidence of major amputation.
The data were presented at the 2025 Western Vascular Society (WVS) annual meeting (Sept. 14–17) in Ojai, California by Christine Mavilian, MS, a medical student at the University of California, Los Angeles (UCLA), attracting first place in the Robert Hye Memorial Best Resident/Trainee Competition. The review included 372 patients treated for claudication between 2005 and 2024 at seven institutions. Some 65% (245) were placed in the appropriate and indeterminate category, and 35% (127) the inappropriate. At two years from
initial presentation, 57% were free from invasive intervention in the appropriate/indeterminate group compared to 19% in the inappropriate group, the UCLA researchers found. “Following revascularization, patients in the inappropriate group experienced significantly higher rates of symptom recurrence and significantly higher rates of reintervention,” Mavilian told WVS 2025.
“At two years post-revascularization, freedom from symptom recurrence was 60% in the appropriate/indeterminate group compared to 49% in the inappropriate group. This approached statistical significance. At five years post-revascularization, 72% in the appropriate/indeterminate group were free from reintervention compared to 44% in the inappropriate group.
“A total of 157 patients presented with mild-tomoderate lifestyle limitation, and, in this group, no patients categorized appropriate/indeterminate had an amputation, compared to patients categorized as inappropriate, who had a major amputation rate of 8.4% and prior amputation rate of 7.6%.” Bryan Kay
Stephen Black
Patrick Muck
How likely are your surgical patients to have disruptive bleeding?
Confidence in THE Doppler that Works Surgical Doppler System
“Immediate confirmation of technical success.”
– Dr. McGinigle, Vascular Surgeon at University of North Carolina at Chapel Hill
RELIABILITY
Single-use probe predictably works every time
SAFETY
Sterile probe is ready to use & reduces cross contamination
“WE ARE THE FIRST MAJOR U.S.based surgical society to present this topic to our membership. Once again, vascular surgery is leading the way,” said Carlos Pineda, MD, a member of the SVS Cultural Competency Committee (CCC), formerly known as the DEI (Diversity, Equity and Inclusion] Committee. Pineda was speaking during opening remarks at the committee’s fourth annual summit, entitled “Neurodivergence for the Vascular Surgeon.” The virtual event, held on Oct. 18, placed vascular surgery at the forefront of a growing movement to recognize and support neurodivergent professionals in healthcare. The summit introduced attendees to the concept of neurodiversity, an umbrella term that includes conditions such as autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD) and dyslexia.
While industries like technology and finance have made strides in embracing neurodivergent talent, medicine— particularly surgical specialties—has only recently begun to explore this area.
LEADERSHIP
The idea for this summit’s theme was sparked by a conversation within the CCC last fall. Pineda recalled how
William Schutze, MD, an SVS member and volunteer, was moved by the 2024 presidential address at the Southern Association for Vascular Society (SAVS) annual meeting. During the talk, David L. Cull, MD, shared his personal experiences with a learning difference.
extraordinary abilities that, when recognized and supported, can help advance our specialty and improve care for our neurodivergent patients.”
Scott Humphries, MD, medical director of the Colorado Physician Health Program (CPHP), opened the neurodiversity summit with a primer on neurodivergence, exploring its scientific underpinnings and the stigma that often surrounds this topic.
“By understanding this topic better, we’ll be able to help our colleagues, trainees and students who are neurodivergent”
“To hear a firsthand, honest account from a respected vascular surgeon about the challenges and strengths associated with learning differences was both fascinating and eyeopening,” said Pineda. “By understanding this topic better, we’ll be able to help our colleagues, trainees and students who are neurodivergent. Many possess
perspective. Diagnosed with autism in his mid-40s, Henderson shared how his neurodivergence shaped his approach to medicine.
“When we look at neurodivergency, we’re looking at where someone falls on a spectrum,” said Humphries. “It’s not about drawing hard lines, but understanding how traits can affect daily life, and when individuals may need additional support.”
CARLOS PINEDA
As a psychiatrist, Humphries emphasized that while neurodivergent conditions are often straightforward to treat, overconfidence in diagnosis can lead to missteps.
James Henderson, MD, FHEA, a consultant on neurodivergence, a surgeon and deputy lead of Autistic Doctors International, offered a personal
LEADERSHIP DEVELOPMENT PROGRAM COHORT 6 CELEBRATES GRADUATION
THE SIXTH COHORT OF THE SVS LEADERSHIP DEVELOPMENT PROGRAM (LDP) gathered Oct. 19–20 in Rosemont, Illinois, for a capstone workshop and graduation ceremony, marking the culmination of an intensive, months-long journey in leadership training for vascular surgeons.
The LDP is an immersive, experiential program designed to equip vascular surgeons with the tools and strategies needed to lead effectively within their practices, hospitals and professional societies. The curriculum blends evidence-based instruction with real-world application, fostering a dynamic environment where participants engage in problem-solving, mentorship and peer-to-peer learning.
Gabriela Velazquez, MD, chair of the LDP, emphasized the program’s unique ability to build a strong, supportive network among participants. “In the LDP, you build this community of people who are really invested in a leadership journey—not just to navigate how things work in their institutions, but to seek support as they overcome challenges in their careers and other opportunities that come their way,” Velazquez said.
Graduates of the LDP report increased confidence in leadership roles, improved negotiation skills and a greater likelihood of taking on leadership positions within professional societies. Marlén Gomez
For more information, visit vascular.org/LDP
“To me, autism is simply a way of being,” he said. “It’s not something that can or should be cured. We just perceive and interact with the world differently, and that diversity of thought can be a strength.”
Henderson reminded attendees that neurodivergence is deeply individual. “If you’ve met one [autistic person], you’ve met only one [autistic person],” he said.
Omid Jazaeri, MD, vice-chair of the CCC, shifted the focus to patient care, highlighting how neurodivergence affects not only providers but also the patients they serve. With 15–20% of adults estimated to be neurodivergent—many undiagnosed until later in life—Jazaeri emphasized the importance of adapting care strategies in vascular surgery where the patient population skews older.
“Caring for your neurodivergent patient isn’t extra work. It’s essential work. It’s work that you must do to accommodate for them,” he said.
In the summit’s closing session, Jazaeri called for a shift in mindset: “We need to move away from framing neurodivergence as a deficit. It’s a difference—one that enriches our profession.”
SVS honors Anton Sidawy appointment as ACS president
THE SVS CONGRATULATES ANTON N. Sidawy, MD, FACS, DFSVS, on his appointment as the 106th president of the American College of Surgeons (ACS). His installation took place during the ACS Clinical Congress in Chicago (Oct. 4–7).
Sidawy, an SVS past-president (2010), was also honored earlier this year with the SVS Lifetime Achievement Award. He was recognized for his decades of transformative leadership, contributions to vascular surgery, and distinguished service that also includes presidencies of the Eastern Vascular Society and the Society for Clinical Vascular Surgery.
Sidawy has continued his involvement in SVS matters as a past president, playing a key role in the creation of the Vascular Verification Program (VVP). Launched in 2023, the program is a joint initiative between the SVS and ACS that provides hospitals with a framework for improving vascular care through rigorous standards and oversight.
A prolific academic, Sidawy has published 200 peer-reviewed manuscripts
and edited several textbooks, including the 9th and 10th editions of Rutherford’s Vascular Surgery and Endovascular Therapy He also served as editor-in-chief of the Journal of Vascular Surgery (JVS) group of peer-review publications.
Sidawy’s chosen theme for his ACS presidency, “The House of Surgery: A Home to All Surgeons,” reflects the ACS commitment to inclusivity and collaboration across surgical disciplines and practice environments.
In his ACS presidential address, Sidawy outlined the overarching issues facing surgery and emphasized that “professional organizations representing individual surgical specialties, such as the SVS, are essential in unifying each specialty to speak with one voice.”—Marlén Gomez
Carlos Pineda
Anton N. Sidawy
COMMENT& ANALYSIS
THE OUTPATIENT
Changing the game in knee osteoarthritis: A vascular approach
Chinmay Shelgikar, MD, discusses the benefits of vascular surgeons performing geniculate artery embolization.
GENICULATE ARTERY
embolization (GAE) is an intra-arterial, catheter-based procedure used to treat chronic knee pain that is caused by osteoarthritis (OA). It targets the distal branches of the geniculate arteries supplying the synovium and joint capsule of the knee and then occluding the distal vessels.
A salient pathological feature of knee OA is low-grade chronic inflammation, often accompanied by abnormal angiogenesis in the synovium and adjacent structures. It is hypothesized that these new, fragile blood vessels play a role in pain generation by carrying inflammatory mediators and sensitizing nearby nerves.
The technique of GAE is relatively straightforward. It can either be done through an antegrade or retrograde common femoral access using a 5F sheath. Often, the genicular vessels can be selected with a 4F catheter. This is usually followed by a microcatheter into the distal
CORNER
STITCH
branches and then selective embolization using 100-to-300micron embospheres. Typically, three-to-four vessels are selected to be embolized. To avoid nontarget embolization, it is essential to do a thorough diagnostic angiogram to make sure that the geniculate vessels do not collateralize to the popliteal artery or the recurrent anterior tibial artery.
The procedure typically takes oneto-two hours and is performed under conscious sedation in an office-based lab (OBL) or hospital outpatient setting. Most patients can return home the same day and resume normal activities within a few days. GAE does not alter the structural integrity of the knee, making it an appealing option for patients who are not candidates for surgery or wish to delay knee replacement. Long-term clinical studies are still ongoing; however, one-year data appear promising.
Patient selection for GAE is crucial. They should be fully worked up by
HOW IMPORTANT IS COMPLEX ENDOVASCULAR AORTIC
TRAINING IN THE CURRENT LANDSCAPE?
By Saranya Sundaram, MD
JUST A FEW YEARS AGO, IT WAS COMMONLY accepted that training in complex endovascular aortic operations depended heavily on the location and practice of the institution where residents/fellows trained. If vascular surgeons at a particular institution participated in these procedures, it was often with multiple vascular surgery attendings scrubbed or with interdisciplinary participation from either interventional radiology or cardiothoracic surgery. Trainees at high-volume institutions had the benefit of being able to participate in these procedures, but expertise did not necessarily affect board certification or job availability. This is not to say either of those outcomes are affected by comfort with complex endovascular aortic procedures today. However, with the landscape of who we treat and what we treat them with constantly shifting, it’s an important aspect of training to re-assess. New data on longterm follow-up after acute dissection now suggest early intervention may have benefit to aortic-specific survival
orthopedic surgery or physical medicine and rehabilitation (PM&R) specialists. Direct patient referrals should be avoided. There are several benefits for vascular surgeons to learn this procedure. From a technical perspective, it is good practice for keeping up with microcatheter skills and embolization techniques. These skills can be then extrapolated to other vascular bodies, including the prostate, liver and for treatment of arteriovenous malformations.
It is also an important way to collaborate with specialties with which we don’t normally share patients and would facilitate a symbiotic relationship with our orthopedic surgery colleagues. Commonly, we only know them when a vascular complication occurs in one of their patients. Additionally, a tighter working relationship with PM&R may help
In the era of decreasing reimbursement for PAD work, this can be an important way to financially supplement a vascular practice
and delayed disease progression. 1 Publications have suggested a higher incidence of branch involvement in younger patients presenting with acute aortic dissection.2 And survival rates predict over 70% survival of both those fixed and unfixed, suggesting more chronic dissections may present requiring further intervention. Even in the abdominal aneurysm sphere, an increasing number of commercially available branched devices have been placed in patients that may eventually require repair. And proximal degeneration of prior infrarenal repairs continues to necessitate proximal branched endograft extensions to achieve appropriate seal. Prior branched interventions such as snorkels—even physician-modified endografts—are not immune to endoleak and need for revision.
Not all trainees want to or plan to participate in complex endovascular aortic interventions in their future practice. But that does not negate the increased interest in those who can demonstrate competence in “backtable” endograft modification or comfort with in-situ laser fenestration, endoleak evaluation/repair, or deployment of off-the-shelf branched endografts.
From speaking to several graduates who went to practice at mainly community or private settings, even they have been asked to participate or manage patients requiring “complex endovascular aortic techniques” because of their training background/procedural comfort. It’s clear that the patient need is present; with continued shortage in vascular
increase peripheral arterial disease (PAD) volumes as well. Finally, in the era of decreasing reimbursement for PAD work, this can be an important way to financially supplement a vascular practice, especially for those working in an OBL. In general, the patients best suited for this procedure are those who have moderate-to-severe osteoarthritis who have failed conservative treatments such as physical therapy, intra-articular corticosteroids, geniculate nerve ablation or hyaluronic acid injections. It is not recommended for patients with advanced joint destruction, extensive bone-on-bone changes, or those with active infections or coagulopathies. The procedure is fully covered for Medicare recipients under the CPT code 37242. Private payors often require a prior authorization but denials are less common given the cost of knee replacement surgery.
Potential risks of this procedure— including embolization and access-site injuries—are rare. Most commonly, patients will have post-embolization syndrome, including skin discoloration, knee swelling, and more pronounced knee pain for the first few weeks. This improves significantly and, at one-month follow-up, most patients do not have any significant symptoms.
CHINMAY SHELGIKAR is a vascular surgeon with Trinity Health IHA Medical Group in Ann Arbor, Michigan.
surgeon availability, it makes sense increasingly complex aortic pathology has been identified at non-academic practices. It’s only a matter of time before these patients find a practitioner who can offer them an appropriate intervention, which could now be dictated by graduating trainee comfort with these practices.
A few years back, trainees were advised to interrogate program comfort with open intervention to ensure they received a well-rounded surgical training. As the landscape of vascular surgery continues to change, it may now be important for trainees to determine if they will have adequate exposure to complex aortic techniques, especially if they desire to work at a high-volume academic or community practice with general call. Though, at the moment, comfort with these techniques only serves to benefit trainees in what they can offer to their future practices.
References
1. Nienaber CA et al; INSTEAD-XL trial. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013 Aug;6(4):407–16
2. Wu S et al. Age-related differences in acute aortic dissection. J Vasc Surg. 2022 Feb;75(2):473–483.e4
SARANYA SUNDARAM is Vascular Specialist resident/fellow editor and of the Corner Stitch column.
Chinmay Shelgikar
Saranya Sundaram
Flixene Vascular Graft
The Right Graft for AV Access
Designed for getting it right
The right graft for long lasting durability and proven reliability
The right graft for safe graft placement
The right graft for suturability and handling
The right graft for early cannulation
COMMENT& ANALYSIS
MISSING A STEP? SEARCHING FOR MEANING IN CLAUDICATION RESEARCH
INTERMITTENT CLAUDICATION (IC) IS THE most common symptomatic manifestation of lower extremity peripheral arterial disease (PAD). Despite its prevalence, IC remains a condition more often overtreated than understood.
The natural history of IC is generally benign, with major amputation risk less than 1% per year; the risk of death from cardiovascular causes is substantially higher than the risk of limb loss.1 As such, first-line management, as outlined in the SVS appropriate use criteria (AUC) and clinical practice guidelines (CPG) is education, optimal medical therapy (OMT) and structured exercise therapy.2,3 Despite this, patients and providers are often focused on modest leg symptoms and unsubstantiated fears of limb loss, rather than reducing risks of cardiovascular morbidity or acknowledging limited long-term benefit of IC interventions.
Enthusiasm for revascularization in IC often arises from a genuine desire to improve patient disability. There are patients for whom revascularization can deliver meaningful symptomatic improvement; the challenge lies in identifying those individuals and providing counseling on the risks and benefits, amid a limited evidence base. Accurately predicting the magnitude and durability of improvement for each patient experiencing IC is central to informed decision-making—yet the data needed to support these everyday clinical discussions remain shockingly sparse.
Evidence from randomized controlled trials (RCTs) and cohort studies consistently shows that invasive treatments for IC offer, at best, short-term improvements in walking performance without sustained quality-oflife (QoL) advantage over exercise or OMT. Few RCTs exist that compare management strategies, and those that have been executed are modest in size and scope. In addition, studies show that many endovascular interventions for IC fail to meet minimum efficacy standards, while risks of reintervention and disease progression increase over time.4,5 Selecting patients most likely to benefit from revascularization therefore requires
A team of leading vascular surgeons in the care of patients with PAD weigh up evidence for the treatment of claudication, calling for research focused on clarifying who should be revascularized, and who should continue with medical management and exercise therapy.
both time and nuance, and a willingness to acknowledge the limitations of current evidence and prioritize shared decision-making, grounded in realistic expectations. While this background would suggest that a minority of IC patients would benefit from revascularization, the numbers tell another story. Medicare‐allowed charges for IC have increased by roughly $12 million per year between 2011 and 2022,6 indicating that revascularization for IC is on the rise. This observation has not escaped public attention, with the New York Times and ProPublica
“Using major amputation as a primary endpoint for comparative effectiveness studies in IC implies that amputation prevention is the treatment goal in IC, which is a dangerous false flag”
both having published investigative reports chronicling the rapid expansion and questionable practices of outpatient vascular care.7–11 The ability to provide less invasive endovascular interventions in ambulatory settings, with low procedural risk, has understandably driven the market growth. How do we ensure that patients and physicians receive the best information for these treatment decisions?
The 2024 SVS CPG update on the management of IC identified seven major research gaps, the top three concerning the role of revascularization.2 A PubMed search yields over 175 IC-related publications in 2025 alone, yet quantity has not translated to quality in IC research. In the absence of prospective trials, numerous researchers have conducted retrospective analyses using various sources of observational data, such as procedural registries and administrative datasets. This approach
limits study design to available datapoints, rather than the appropriate ones. It can lead to posing questions that the data were never designed, or equipped, to properly answer. A recent example exhibiting this fundamental flaw was published in JAMA Network Open, a journal with an impact factor of 9.7, wherein the authors used major amputation as the primary endpoint for a comparison between open and endovascular revascularization strategies for IC.12
The primary endpoint for a comparative effectiveness study should be directly related to the intervention’s purpose. Meaningful outcomes in IC should focus on patient priorities of walking performance, symptom relief and health-related QoL. Using major amputation as a primary endpoint for comparative effectiveness studies in IC implies that amputation prevention is the treatment goal in IC, which is a dangerous false flag. It is a safety endpoint, not an efficacy endpoint. While risks of limb loss and mortality are expected to be low, recurrent symptoms, repeat procedures and potential hastening of disease progression to chronic limb-threatening ischemia (CLTI) are common adverse outcomes that should be ascertained in any study of invasive treatment for IC.
High-quality studies derived from large databases leverage the statistical benefits of sample size but interpret findings in the context of clinical relevance. In the referenced study, the authors reported one-year amputation rates of 0.6% and 0.9% for endovascular and open surgery, respectively, focusing on the statistically significant but clinically meaningless difference in what are, quite thankfully, acceptably low rates of a catastrophic outcome. The study’s conclusion—that “patients with claudication may benefit most from endovascular-first intervention and subsequent open bypass using reversed GSV [great saphenous vein] conduit”—reads as a troubling endorsement of endovascular overuse at risk for being taken out of context. The study design’s inappropriate emphasis on amputation risk rather than patient-centered outcomes for IC or adherence to the SVS AUC for IC perpetuates fear-driven treatment patterns that may lead to harm. In addition, there was a missed opportunity to underscore the alarming finding that 13.2% of patients in the study underwent tibial endovascular interventions for IC, a practice deemed to universally carry more risk than benefit by the SVS AUC.3
As noted above, research using any large administrative and/or procedural database (e.g., Medicare, the American College of Surgeons [ACS] NSQIP, Nationwide Inpatient Sample, etc.) carries significant challenges and limitations. With respect to the SVS Vascular Quality Initiative (VQI) specifically, it is a procedural registry, resulting in an inherent treatment selection bias in the data. Compounding this, the “long-term” (i.e., one-year) outcomes in the VQI are notoriously incomplete, illustrated by the referenced paper where the chosen endpoint of major amputation was missing in 40% of the endovascular cohort. The reported 99% one-year patency for open bypass is likewise an implausible result that undermines confidence in the study itself.
We need contemporary research focused on clarifying who is likely to attain a meaningful benefit from revascularization for IC, and who should continue with medical management and exercise therapy. Patient factors such as age and comorbidities, functional capacity and anatomic factors (level and complexity
continued on page 16
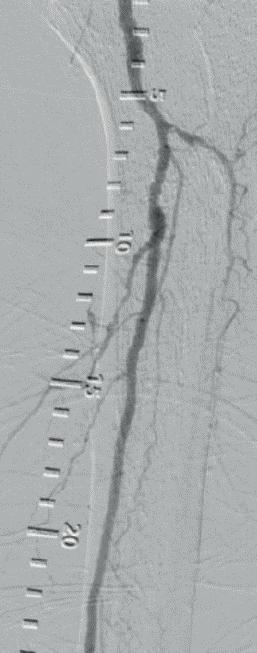
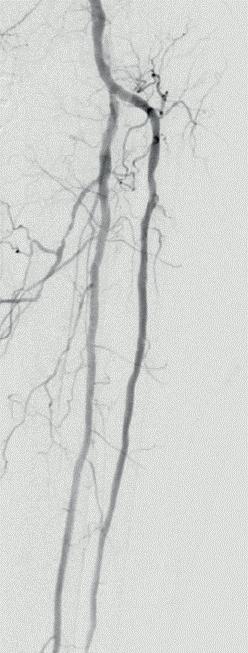
Cracking CLTI: How Shockwave Javelin
intravascular lithotripsy is opening up new frontiers in heavily calcified peripheral arterial occlusive disease
Three vascular surgeons discuss how and when they deploy the transformative Shockwave Javelin first-of-its-kind Forward Intravascular Lithotripsy (IVL) Platform in cases of heavily calcified peripheral vascular occlusive disease.
Viewpoints on when and how to use Shockwave Javelin vary, but one insight unites them: prior to its emergence there were limited options available to get through the sorts of severely calcified lesions the device opens up. Or, as Sung Yup Kim, MD, an associate professor of surgery at Mount Sinai Health System in New York, puts it: “In the past we have used balloons, we have used orbital atherectomy, cutting balloons with no major success, nothing would track in these areas, and there were cases where we just had to abort and think about an open option. Shockwave Javelin allows us to deliver endovascular therapy for these patients.”
Paul Foley
“At the outset, how we thought we were initially going to use Shockwave Javelin is not how it has turned out to be.” The words of Paul Foley, MD, director of the vascular lab at Doylestown Hospital in Doylestown, Pennsylvania, as he assesses the evolution in his use of the Shockwave Javelin, from initial study in the FORWARD PAD investigational device exemption (IDE) trial, through limited market release and, earlier this year, the launch of the platform in the U.S. Understanding now what the device can do, Foley sees Shockwave Javelin as a routine IVL delivery device in tibial vessels and below the ankle, which is also able to tackle some of the most challenging disease.
That broader canvas for the Shockwave Javelin platform includes use as a primary IVL modality. In the limited market release phase of Shockwave Javelin, the conventional wisdom went that “if you had a boulder of calcium that you couldn’t get across, this was going to be the savior device,” Foley explains. “And, certainly, that’s one piece of Shockwave Javelin.”
However, after more experience Foley has found Shockwave Javelin’s role to be more nuanced and depends on the vessel bed, he says. In the femoropopliteal space, the Shockwave Javelin works best as facilitator, “modifying calcium to facilitate the next step”. In the tibial vessels, Foley continues, a good outcome is defined as successfully
crossing the lesion while delivering pulses. “I don’t see Shockwave Javelin simply as a method of crossing the uncrossable anymore; I see it as way more than that. When I look at a calcified, highly stenotic tibial vessel, Shockwave Javelin is now my knee-jerk device.” Below the ankle, Foley says, the Shockwave Javelin is breaking new ground by effectively crossing through vessels previously unpassable by any other method.
Shockwave Javelin is proving to be a multi-tool for patients with chronic limb-threatening ischemia (CLTI), he adds. While vessel bed may vary, the success of the product lies in modifying plaque while achieving luminal gain and a reduction in diameter stenosis—and doing so safely without a high risk of angiographic complications, perforation or distal embolisation.1
Kenneth
Tran
practice in cases involving the femoropopliteal vessel bed. These patients will tend to have either a low segmental chronic total occlusion (CTO) or a couple of focal areas where no devices will track, he explains.
“These are cases where we already have a wire through, there is a rock sitting there, and, with Shockwave Javelin on that spot, we crack open the area, apply some forward pressure, and then try to crack the calcium distal to that. We maintain Shockwave Javelin for one or two cycles in one spot that is really, really calcified and heavy. Then, in the next few cycles, we are moving forward with Shockwave Javelin.”
Kim doesn’t see the platform as a crossing device. “It is not a case of when you can’t go through a CTO, and you use Shockwave Javelin and try to tunnel a channel through severe calcium,” he says. “I don’t think that’s the purpose of Shockwave Javelin.” Kim tends to encounter trouble with femoropopliteal lesions most often at the Hunter’s canal, where the artery sometimes bends at the popliteal facia. “If you have a severe calcium there, the bend is a killer with a rock-hard calcium,” Kim says.
Step forward Shockwave Javelin: in this small portion of cases, too, the device has proven successful, he adds.
Access points
For Kenneth Tran, MD, a clinical assistant professor of surgery at Stanford Health Care in Stanford, California, Shockwave Javelin has proven an important precursor in complex cases. “It’s not intended to be used as the primary IVL technology—I think of it as enabling me to do my next step in my treatment algorithm, where I can’t deliver the device I’m trying to deliver,” he says. In below-the-knee (BTK) lesions, Tran sees its use as often initial vessel prep, such as to advance an intravascular ultrasound (IVUS) catheter or Shockwave E8 IVL balloon. However, he recognizes instances in which Shockwave Javelin has a role to play as the go-to IVL catheter. “For isolated lesions that are very small, I have had success using the Shockwave Javelin as the sole lithotripsy device,” says Tran.
Sung Yup Kim
On the other hand, Kim sees Shockwave Javelin make the biggest difference in his
Views on optimal access vary. While Kim prefers a contralateral approach for precision to traverse tough lesions, both Foley and Tran err toward an antegrade access.
“If there is no inflow disease, no disease in the common femoral artery, no disease in the femoropopliteal region that I think is significant, so that, going in, there is going to be a high likelihood I’m doing a below-knee or a tibial or even a pedal artery intervention, I approach all of those cases from an antegrade approach,” says Foley. “And I don’t have any hesitation to do that because I believe that, with an antegrade approach for below the knee, especially for calcified lesions, really stenotic or at least occlusive lesions, you have a much better chance of getting across them. You get much better pushability and tactile feedback than you would if you were going up and over from a contralateral approach.
“But in any patient in whom I’m doing an antegrade approach where I know I’m going to be working below the knee, I always have the foot prepped out so that I have a low threshold of approaching from a retrograde pedal access as well.”
Shockwave Javelin provides more flexibility in terms of the level of support available while across a lesion, Tran says. In the BTK space, the antegrade approach allows for more pushability, but some anatomically inappropriate patients enforce the up-andover access of the contralateral approach. The platform is a unique tool that can be used to modify calcium previously beyond what was available in his PAD toolkit, Tran says. “This has enabled treatment of
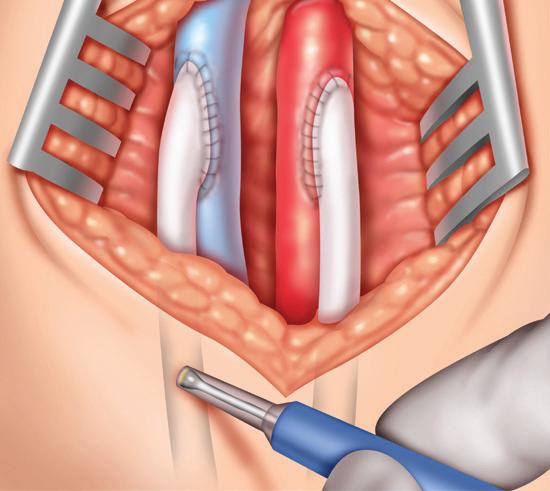
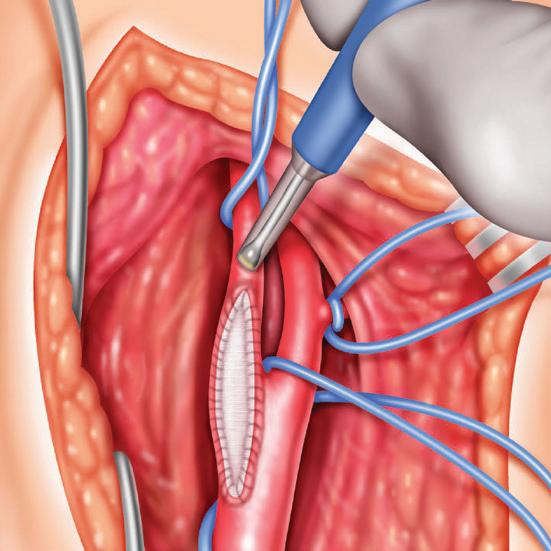
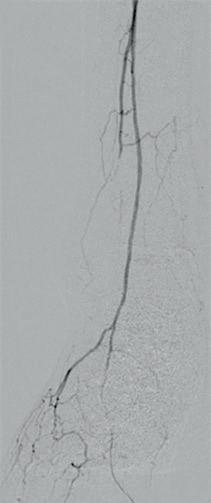
3: Definitive therapy, AT and DP treated with a 2.5x150mm angioplasty balloon a) Completion angiogram of AT b) Completion angiogram of DP
more complex tibial lesions from an up-andover approach. It has also allowed us to be able to treat more complex lesions more thoroughly with larger profile devices.”
Reference 1. Corl J et al. FORWARD PAD IDE/feasibility studies: Primary endpoint analysis of a novel non–balloon-based peripheral IVL catheter. J AmColl Cardiol Intv. 2025 Feb, 18 (3) 398–399
Updated safety information for the Shockwave advertorial: In the US: Rx Only. Prior to use, please reference Instructions For Use for information on indications, contraindications, warnings, precautions, and adverse events. www. shockwavemedical.com/IFU
PAUL FOLEY, SUNG YUP KIM and KENNETH TRAN are paid consultants of Shockwave Medical. The views expressed are their own opinions, reflect their daily medical practice and do not necessarily represent Shockwave Medical SPL-78322 Rev. A
Paul Foley
Sung Yup Kim
Kenneth Tran
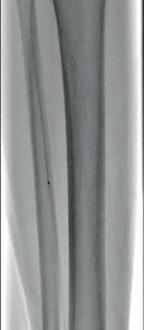
Figure 1: Diffuse calcified occlusive disease on pre-procedural arteriogram
a) Anterior tibial (AT) artery b) Dorsalis pedis (DP) artery
Figure 2: Shockwave Javelin in therapy a) In the AT b) In the DP
Figure
‘We need to look at the totality of evidence’: Panelists examine SWEDEPAD mortality signal
By Jocelyn Hudson
THERE WAS STANDING ROOM ONLY IN A FOCUSED session on the SWEDEPAD registry-based randomized controlled trials in claudication and chronic limb-threatening ischemia (CLTI) during the 2025 Vascular Interventional Advances (VIVA) conference (Nov. 2–5) in Las Vegas. Panelists discussed the implications of the latest findings.
Joining the session remotely, Joakim Nordanstig, MD, a vascular surgeon at the University of Gothenburg, in Gothenburg, Sweden, opened proceedings with a summary of the SWEDEPAD findings, which he and co-principal investigator Mårten Falkenberg, MD, a vascular surgeon at Sahlgrenska University Hospital and the University of Gothenburg, first shared at the 2025 European Society of Cardiology (ESC) congress (Aug. 29–Sept. 1) in Madrid, Spain. Results were simultaneously published in The Lancet Nordanstig reiterated that drug-coated balloons and stents
were not associated with reduced risk of amputation or improved quality of life compared with uncoated devices in the SWEDEPAD 1 and 2 trials. He added that higher fiveyear mortality with drug-coated devices in patients with intermittent claudication was noted.
Subsequently, Eric Secemsky, MD, director of vascular intervention at Beth Israel Deaconess Medical Center in Boston, took to the podium to consider the SWEDEPAD results on paclitaxel safety and efficacy in the context of real-world data pointing to the contrary, including that from Secemsky and colleagues’ recently published and Food and Drug Administration (FDA)-commissioned SAFE-PAD study.
“Obviously, we have to take SWEDEPAD seriously because it’s a prospective trial,” Secemsky remarked, before stressing that clinicians “need to be thoughtful of all the other evidence we have to support the safety of paclitaxel.”
Secemsky also questioned the relative importance of a mortality signal to patients. He highlighted data showing that, on average, patients would accept a device offering a reduction in two-year clinically driven target vessel revascularisation (CD-TVR) risk from 30% to 10% and a reduction in five-year CD-TVR risk from 40% to 30% if the five-year mortality risk increase was less than or equal to 4.6%.
During a panel discussion following the two presentations, session co-moderator Joshua Beckman, MD, chief of vascular medicine at UT Southwestern Medical Center in Dallas, asked Nordanstig for his reaction to the “total dataset.”
“We need to be careful and we need to look at the totality of evidence,” Nordanstig responded, before noting that the SWEDEPAD team is “planning further scrutiny of the evidence.”
However, he did profess to being “more concerned about the lack of effectiveness [of drug-coated devices] than the mortality signal in SWEDEPAD 2.”
COMMENT& ANALYSIS
CONTINUED FROM PAGE 14
Secemsky
“Obviously, we have to take SWEDEPAD seriously because it’s a prospective trial [but we also] need to be thoughtful of all the other evidence we have to support the safety of paclitaxel”
ERIC SECEMSKY
of disease; unilateral versus bilateral) must be accurately captured and taken into consideration. Large datasets such as the SVS VQI can complement prospective IC research if used thoughtfully but require significant improvement in capture of relevant datapoints and/or linkage to other datasets (e.g., VQI-VISION) to address key questions in long-term outcomes (which SVS guidelines13 have defined as at least two years). The referenced study is far off base in its endpoint, data quality and analysis, and will likely be interpreted by those with bias towards intervention as affirmatory.
The vascular community has a duty to our patients to uphold the highest standards of clinical care and research. Any amputation after an IC intervention
likely represents avoidable iatrogenic harm. The recent SVS CPG update2 highlights the importance of shared decision-making in IC with a full understanding of the individual risks and benefits for intervention. The mission of the SVS VQI is to “improve the quality, safety, effectiveness and cost of vascular healthcare.” To achieve this goal, clinical care and research must prioritize patient-centered outcomes, rigorous study designs and appropriate care that minimizes procedural overuse. We must resist the easy path of procedural justification disguised in the language of data science—our field doesn’t need more volume, it needs more meaning.
References
1. Dormandy J, Heeck L, Vig S. The natural history of claudication: risk to life and limb. Semin Vasc Surg. Jun 1999;12(2):123–37
2. Conte MS, Aulivola B, Barshes NR et al. Society for Vascular Surgery Clinical Practice Guideline on the management of intermittent claudication: Focused update. J Vasc Surg. Aug 2025;82(2):303–326 e11. doi:10.1016/j.jvs.2025.04.041
3. Woo K, Siracuse JJ, Klingbeil K et al Society for Vascular Surgery appropriate use criteria for management of intermittent claudication. J Vasc Surg Jul 2022;76(1):3-22 e1. doi:10.1016/j. jvs.2022.04.012
4. Bath J, Lawrence PF, Neal D et al Endovascular interventions for claudication do not meet minimum standards for the Society for Vascular Surgery efficacy guidelines. J Vasc Surg. May 2021;73(5):1693–1700 e3. doi:10.1016/j. jvs.2020.10.067
5. Thanigaimani S, Phie J, Sharma C et al Network Meta-Analysis Comparing the Outcomes of Treatments for Intermittent Claudication Tested in Randomized Controlled Trials. J Am Heart Assoc May 4 2021;10(9):e019672. doi:10.1161/ JAHA.120.019672
6. Dun C, Stonko DP, Bose S et al. Trends and Factors Associated With Peripheral Vascular Interventions for the Treatment of Claudication From 2011 to 2022: A National Medicare Cohort Study. J Am Heart Assoc. Jul 16 2024;13(14):e033463. doi:10.1161/JAHA.123.033463
7. Creswell J, Abelson R. Medicare Payments Surge for Stents to Unblock Vessels in Limbs. New York Times. Jan 29, 2015. Accessed April 8, 2021
8. Thomas K. They Lost Their Legs; Doctors and Healthcare Giants Profited. New York Times. July 16, 2023. Accessed May 2, 2025. https://www.nytimes. com/2023/07/15/health/atherectomyperipheral-artery-disease.html
9. Waldman A. Researchers Warned of Possible Vascular Procedure Abuse. . ProPublica. December 12, 2023. Accessed March 16, 2024. https://www.propublica. org/article/researchers-warned-ofpossible-vascular-procedure-abusedoctors-pushed-back
10. Waldman A. Steak Dinners, Sales Reps and Risky Procedures. ProPublica February 16, 2023. Accessed March 16, 2024. https://www.propublica.org/article/ medtronic-medical-device-kickbackslawsuit-kansas
11. Waldman A. In the “Wild West” of Outpatient Vascular Care, Doctors can Reap Huge Payments as Patients Risk Life and Limb. ProPublica. May 24, 2023. Accessed May 2, 2024. https://www. propublica.org/article/maryland-dormuminimally-invasive-vascular-medicaremedicaid
12. Bellomo TR, Jabbour G, Manchella M, et al. Endovascular Therapy, Open Surgical Bypass, and Conduit Types for Index Treatment of Claudication. JAMA Netw Open. Oct 1 2025;8(10):e2533352. doi:10.1001/ jamanetworkopen.2025.33352
13. Society for Vascular Surgery Lower Extremity Guidelines Writing G, Conte MS, Pomposelli FB et al. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J Vasc Surg. Mar 2015;61(3 Suppl):2S-41S. doi:10.1016/j.jvs.2014.12.009
Authored by BENJAMIN S. BROOKE, MD, MICHAEL S. CONTE, MD, ELIZABETH L. GEORGE, MD, JENS ELDRUP-JORGENSEN, MD, LEIGH ANN O’BANION, MD, KAREN WOO, MD, and JESSICA P. SIMONS, MD.
Eric
META-ANALYSIS: DRUG-COATED DEVICES SHOW COMPARABLE AGGREGATE OUTCOMES TO NONDRUG-COATED DEVICES IN CLTI
By Killian Meara
DRUG-COATED BALLOON (DCB) angioplasty appears to offer similar benefits as plain old balloon angioplasty (POBA), with or without stenting, for patients with chronic limb-threatening ischemia (CLTI) who are undergoing endovascular femoropopliteal segment lower extremity revascularization, according to new meta-analysis data presented at the annual meeting of the Canadian Society for Vascular Surgery (CSVS) in Ontario, Canada (Sept. 26–27).
Investigators from University of Toronto, Canada, led by senior author David Szalay, MD, associate professor in the department of surgery, conducted a meta-analysis that analyzed data from six clinical trials comparing POBA with DCB for the treatment of the femoropopliteal segment in patients with CLTI.
The study looked at four key outcomes: freedom from major amputation, major adverse limb events, the need for additional
procedures and mortality. The goal was to see whether using drug-coated devices, which release the medication paclitaxel, led to better results than using plain balloons. Data was gathered from Embase, MEDLINE, and relevant articles cited in major guidelines.
Findings showed there was no statistically significant difference in limb events or mortality between DCB or POBA. After synthesizing evidence using the GRADE tool, all key endpoints except mortality were rated with a moderate-to-high degree of certainty.
“The results show there isn’t a statistically significant difference in terms of the four outcomes we analyzed when comparing a drug-coated device to a plain balloon angioplasty,” said first author Allen Li, MD, a second-year integrated vascular surgery resident at the University of Toronto.
Though the absence of a clear difference might appear to narrow the decision-
making process, co-author Arshia Javidan, MD, a fifth-year integrated vascular surgery resident at the University of Toronto, said the implications are far more nuanced due to the complexity and heterogeneity of the CLTI population. “It will always depend on the specific patient and their anatomy rather than a large paintbrush that we can sweep across the whole field and say we should or shouldn’t use [paclitaxel] in these scenarios,” said Javidan.
Li and Javidan both emphasized that the study’s overall strengths and limitations should be considered when interpreting the results. “One of the biggest limitations of the study, and with every high-level meta-analysis, is that it is not patient-level data,” said Javidan. “These are outcomes taken in aggregate where you lose so much of the granularity that exists in making these decisions.”
The study contributes to ongoing discussions about using drug-coated devices in clinical practice. Javidan said patients with CLTI are high-risk and prone to restenosis, and paclitaxel effectively targets neointimal hyperplasia. While
previous research raised concerns about increased mortality with paclitaxel, he said that this has not been consistently supported by later data. “The messaging around paclitaxel-coated devices is that it really is patient dependent,” said Javidan. “You have to choose the right device for the right patient.”
Javidan noted that the ongoing debate around paclitaxel is compounded by foundational issues in how research is conducted. “Our ability to synthesize evidence through meta-analysis is fundamentally limited by the heterogeneity in how major trials define their patient population, their endpoints and even the anatomy of the lesions they are treating,” he said. “Adopting universal classification and anatomic standards, like WIfI and GLASS, and demanding precise definitions for endpoints are not academic exercises — they are essential for delineating clinical truth and improving patient safety.”
Despite this and other challenges, Li and Javidan said the field has made significant progress over the past decade. “We’ve come together and have come up with what is close to global consensus guidelines on a lot of these definitions,” Javidan said.
Li and Javidan also pointed to future directions in CLTI research, including the use of large-scale databases like the Vascular Quality Initiative (VQI) for patient-level analyses.
Allen Li, David Szalay and Arshia Javidan
SVS SMOKING CESSATION INITIATIVE ALIGNS WITH NATIONAL CANCER SOCIETY EFFORTS TO CURB HABIT
By Marlén Gomez
VASCULAR SPECIALISTS HAVE BEEN EXPANDING efforts to combat tobacco use through the SVS Patient Safety Organization (SVS PSO), which is leading a targeted campaign to help patients quit smoking and reduce their risk of
proved five-year survival rates by increasing the use of antiplatelet agents and statins. That initiative achieved nearly 90% compliance across 18 VQI regions, demonstrating the impact of data-driven quality improvement.
The smoking cessation initiative focuses on two key reporting measures: preoperative smoking status, identifying patients who are actively smoking within one month of their vascular procedure; and smoking cessation at follow-up, tracking whether patients have quit smoking between nine and 21 months after their procedure.
SVS VQI data show that about 32% of patients across registries successfully quit smoking between their procedure and long-term follow-up. These results underscore the importance of targeted in
Cessation Quick Tips.” Clinicians are also encouraged to pursue Certified Tobacco Treatment Specialist certification to enhance their ability to counsel patients effectively. Since its launch, CAN-DO has gained momentum across all 18 VQI regions. Centers have created regional and national charters, developed billable smart phrases for electronic health records and contributed abstracts to the VQI at the SVS Vascular Annual Meeting (VQI@VAM). As of 2025, 30 charters have been established, and the initiative is set to become part of the SVS VQI Participation Awards in 2026.
“This level of engagement reflects the vascular community’s commitment to improving patient outcomes through behavioral change,” said Nikolaos Zacharias, MD, medical director for qual
Nikolaos Zacharias
Esprit BTK:
Drug-eluting resorbable scaffold poised as first-line therapy for below-the-knee CLTI
“We now have something on label and FDA [Food and Drug Administration] approved that we can use as a first-line therapy for tibial vessels,” Richard Pin, MD, chief of vascular surgery at Southcoast Health in New Bedford, Massachusetts, tells Vascular Specialist, designating a primary role for the Esprit BTK everolimus-eluting resorbable scaffold system (Abbott) in the treatment of below-the-knee (BTK) chronic limb-threatening ischemia (CLTI).
In this interview, Pin highlights his extensive clinical experience with Esprit BTK and shares how the device is fundamentally changing clinical practice for a challenging disease state where timely intervention is key.
Tackling tibial vessel disease
According to Pin, one of the most pressing unmet needs in the treatment of CLTI relates to tibial vessel disease. Moreover, “time is critical” in these patients, Pin says—many of whom are referred from wound care centers—to prevent tissue loss and amputation.
Esprit BTK, Pin remarks, has “helped tremendously” in the tibial vessels, offering a “new weapon in the armamentarium” and a more durable treatment option able to keep vessels patent over a longer period of time than angioplasty thanks to its radial strength and sustained everolimus elution, all while leaving nothing behind. “Often, tibial vessels are the culprit in terms of recurrent disease, recurrent wounds, and now we have a durable option to treat that,” he says.
Pin underscores that for patients with CLTI—many of whom are poor surgical candidates due to comorbidities and lack of suitable bypass conduit—balloon angioplasty alone often falls short. Esprit BTK offers a transformative alternative, Pin claims, combining recoil resistance and everolimus elution with the long-term benefits of a bioresorbable scaffold, giving physicians a more effective and durable option to restore perfusion and preserve future treatment options.
Reduced reinterventions
Pin’s views on Esprit BTK rest on vast clinical experience, with his institution being part of the landmark LIFE-BTK randomized controlled trial (RCT)—for which twoyear data were presented at VIVA 2024—as well as the LIFE-BTK pharmacokinetics sub-study and the device’s post-approval study (PAS). “Our experience with Esprit BTK has been pretty extensive,” he says, “despite the short time that it’s been on the market.”
Summarizing some of the headline findings from the available data, Pin details a
31% superiority versus balloon angioplasty in terms of limb salvage and primary patency at one year, with sus tained benefits through two years. 1,2 Most im portantly, he highlights a significantly reduced need for patients to return to clinic for a reintervention following treatment with the Esprit BTK, with 90.3% of Esprit BTK patients not requiring a reintervention through two years in the trial.2,3 “Those were the things that were borne out through the clinical trial, and, from an anecdotal standpoint, those are the things we see first-hand when we’ve been using Esprit BTK,” Pin says.
at his center and at wound care facilities. He details that this integrated follow-up approach—combining regular wound assessments with ultrasound and ankle brachial index (ABI) surveillance within the first one to three months—enables early monitoring and supports optimal healing. In addition, Pin remarks that the structured, ongoing follow-up every three to four months until wound resolution reflects the confidence clinicians have in Esprit BTK’s ability to promote durable vessel patency and sustained wound improvement, far beyond what balloon angioplasty alone can offer.
Pin is confident the device will continue to bring about positive long-term results, with three-year data from the LIFE-BTK trial due this autumn.
Key features: A first-ofits-kind device
“ Once you start working on tibial vessels often, you know that they’re going to recoil. It’s not a question of if, it’s when, and the scaffold really prevents that from occurring ”
The main therapy available prior to Esprit BTK has been balloon angioplasty, Pin shares, highlighting several limitations to this approach in a recounting of his treatment algorithm: “We would do our angiogram and try to open up any tibial vessels with angioplasty alone, and if that didn’t give us a satisfactory result, then we were talking about doing something off label, which was putting a coronary stent into a tibial vessel to support a dissection or recoil in the vessel that wasn’t adequately treated with angioplasty alone.” However, Pin continues, a permanent metallic implant has not been rigorously studied in an RCT in the tibials, and can compromise future treatment options, affecting limb salvage and patency.
RICHARD PIN
Pin underlines several unique features of the Esprit BTK that he sees as crucial to its success so far. He highlights, for example, the fact that it is the first device of its kind to be approved by the FDA for treatment of the tibial vessels and, uniquely, can address both the mechanical and biological needs to effectively treat CLTI. Pin reiterates that the scaffold provides the support to treat recoil or dissection from balloon angioplasty, with radial strength equivalent to a metallic stent within the first six months. 4 On this point, Pin states that recoil is a significant issue when treating tibial vessels and is therefore something that must be addressed for optimal treatment: “Once you start working on tibial vessels often, you know that they’re going to recoil. It’s not a question of if, it’s when, and the scaffold really prevents that from occurring.”
Pin underlines another key feature in that the sustained three-month period of everolimus elution from Esprit BTK is able to suppress any kind of hyperplasia as well as any longer-term issues with stenosis, therefore maximizing patency.1
want to go back and need to treat something else, there isn’t a piece of metal that may compromise, for instance, a distal bypass sometime down the road.”
CASE PRESENTATION
A 70-year-old male with diabetes and end-stage renal disease. Prior left foot transmetatarsal amputation (TMA) with previous angioplasty performed three months prior in anterior tibial (AT)/peroneal arteries. Ongoing open wound at TMA.
Pre-intervention
Final angiogram
Pin notes that the resorbable and novel nature of Esprit BTK resonates strongly with patients—many of whom have previously received permanent metallic stents. “They’re very interested,” he says. “A lot of these patients have had other stents put in before, and they’ve been told that these are for life. And here we are, with something that’s resorbable, it definitely piques peoples’ interest. This is really something patients find cutting edge in terms of technology.”
Reflecting on his experience with Esprit BTK, Pin emphasizes the meaningful difference it has made in the lives of his patients. “Esprit BTK has truly changed outcomes for the patients I treat,” he shares, highlighting the device’s role in improving healing and preserving limbs in a population with limited alternatives. He advocates for its use as a first-line therapy, citing its unique ability to combine effective revascularisation with long-term vessel preservation—something traditional therapies often fail to deliver. For patients facing the devastating consequences of CLTI, Pin summarizes, Esprit BTK offers new hope where few options exist.
References
1. Esprit™ BTK Everolimus Eluting Resorbable Scaffold System Instructions for Use (IFU). Refer to IFU for additional information
Pin emphasizes the long-term advantages of Esprit BTK, noting that patients treated with the device are closely monitored both
Pin highlights one of Esprit BTK’s most transformative features is its bioresorbable scaffold that “leaves nothing behind.” 5 Unlike permanent metallic implants, he explains, “over the course of three years, the scaffold is going to dissolve, and so you don’t really have anything that is going to be a long-term irritant to the vessel. Or, if you
2. DeRubertis BG et al. Two-Year Outcomes of the LIFE-BTK Randomized Controlled Trial Evaluating the Esprit™ BTK Drugeluting Resorbable Scaffold for Treatment of Infrapopliteal Lesions, VIVA 2024
3. Reintervention defined as CD-TLR
4. Data on file. Testing done with XIENCE Sierra™ 3.5x38 mm at nominal
5. Excluding platinum markers
Esprit BTK
Esprit™ BTK Everolimus Eluting Resorbable Scaffold System
INDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
CONTRAINDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is contraindicated for use in:
• Patients who cannot tolerate, including allergy or hypersensitivity to, procedural anticoagulation or the post-procedural antiplatelet regimen.
• Patients with hypersensitivity or contraindication to everolimus or structurally related compounds or known hypersensitivity to scaffold components poly(L-lactide), poly(D, L-lactide), and platinum.
WARNINGS
This device is intended for single use only. Do not reuse, reprocess, or re-sterilize. Note the product “Use-by” date on the package. Reuse, reprocessing, or re-sterilization may compromise the structural integrity of the device and / or delivery system and / or lead to device failure, which may result in patient injury, illness, or death. Reuse, reprocessing, or resterilization may also create a risk of contamination of the device and / or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device and / or delivery system may lead to injury, illness, or death of the patient.
• The Esprit™ BTK System is intended to perform as a system. The scaffold should not be removed for use with other dilatation catheters.
• The Esprit™ BTK System should not be used in conjunction with other non-everolimus drug eluting devices in the same vessel as the Esprit™ BTK Scaffold.
• It is not recommended to use this scaffold to treat lesions located at any joint or other hinge points, such as the knee or ankle. The recommended region for below-the-knee (BTK) treatment with the Esprit™ BTK Scaffold is the infrapopliteal arteries at a location ≥ 10 cm above the proximal margin of the ankle mortise. The Esprit™ BTK Scaffold has not been tested for use outside the recommended implant locations.
This product should not be used in patients with aneurysms immediately adjacent to the scaffold implantation site.
• Insertion of the Esprit™ BTK System and implantation of the scaffold should be performed only under fluoroscopic observation with radiographic equipment providing high resolution images.
Quantitative imaging is strongly recommended to accurately measure and confirm appropriate vessel sizing (reference vessel diameter ≥ 2.5 mm). If quantitative imaging determines a vessel size < 2.5 mm, do not implant the Esprit™ BTK Scaffold.
• Adequate lesion preparation prior to scaffold implantation is required to ensure safe delivery of the scaffold across the target lesion. It is not recommended to treat patients having a lesion that prevents complete inflation of an angioplasty balloon.
• Successful pre-dilatation with residual diameter stenosis of < 30% by visual estimation is required for treatment of the target lesion; < 20% by visual estimation is preferred.
• Ensure the scaffold is not post-dilated beyond the allowable expansion limits.
• Use of appropriate anticoagulant and / or antiplatelet therapy per standard of care is recommended for use of this scaffold system.
• This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
Judicious selection of patients is necessary, since the use of this device carries the associated risk of
scaffold thrombosis, vascular complications, and / or bleeding events.
PRECAUTIONS
• Scaffold placement should not be performed in patients with known allergies to contrast agent that cannot be medically managed.
• It is not recommended to treat patients having a lesion with excessive tortuosity proximal to or within the lesion.
• When multiple scaffolds are required, only combinations of Esprit™ BTK Scaffolds must be used. Any potential interaction with other drug-eluting or coated devices has not been evaluated.
• The delivery system is intended for deployment of the scaffold only and should not be used to dilate other locations.
• Implantation of the scaffold should be performed only by physicians who have received appropriate training.
• As with all catheter-based procedures, scaffold placement should be performed at facilities where patient can be prepared for necessary intervention and / or surgical removal of the device and vessel repair as per facility protocol.
• Pre-dilatation should be performed with an angioplasty balloon. Cutting or scoring balloons can be used per physician discretion, if the lesion appears to be mildly calcified.
• Failure to pre-dilate the vessel may impair nominal / optimal scaffold delivery.
• Implanting a scaffold may lead to dissection of the vessel distal and / or proximal to the scaffold, requiring additional intervention.
Note: In cases of bailouts, bailout treatment of the target lesion can be done using the Esprit™ BTK Scaffold of the appropriate length. If an appropriate length Esprit™ BTK Scaffold is not available, physicians should use standard of care.
• An unexpanded scaffold may be retracted into the introducer sheath one time only. An unexpanded scaffold should not be reintroduced into the artery once it has been pulled back into the introducer sheath.
• Post-dilatation is strongly recommended for optimal scaffold apposition. When performed, post-dilatation should be performed at high pressure (> 16 atm) with a non-compliant balloon up to 0.5 mm larger than the nominal scaffold diameter.
Use an appropriately sized non-drug coated balloon to pre-dilate the lesion. When treating a long lesion, scaffold the distal portion of the lesion prior to scaffolding the proximal portion of the lesion. Ensure that the scaffolded area covers the entire lesion / dissection site and that no gaps exist between scaffolds.
• The extent of the patient’s exposure to drug and polymer is directly related to the number of scaffolds implanted. The safety of everolimus, polymer, and polymer breakdown products was evaluated in preclinical studies and the biocompatibility assessment of the Esprit™ BTK Scaffold.
• The safety and effectiveness of the Esprit™ BTK Scaffold in patients with prior brachytherapy of the target lesion or the use of brachytherapy for treatedsite restenosis in the Esprit™ BTK Scaffold have not been established. Both vascular brachytherapy and the Esprit™ BTK Scaffold alter arterial modeling. The potential combined effect on arterial remodeling by these two treatments is not known.
• The safety and effectiveness of the Esprit™ BTK System have not been established in clinical trials with the use of either mechanical atherectomy devices (directional atherectomy catheters, rotational atherectomy catheters) or laser atherectomy catheters. Formal drug interaction studies have not been performed with the Esprit™ BTK Scaffold because of limited exposure to everolimus eluted from the scaffold.
Everolimus, the Esprit™ BTK Scaffold’s active pharmaceutical ingredient, is an immunosuppressive agent. Therefore, consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression.
• Oral everolimus use in renal transplant and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglyceride levels, which in some cases required treatment.
• Non-clinical testing has demonstrated the Esprit™ BTK Scaffold is MR Conditional. A person with the Esprit™ BTK Scaffold may be safely scanned under the following conditions. Failure to follow these conditions may result in injury.
Static magnetic field strength of 7 Tesla or less
• The Esprit™ BTK Scaffold should not migrate in this MRI environment. MRI at 7 Tesla or less may be performed immediately following the implantation of the Esprit™ BTK Scaffold.
POTENTIAL ADVERSE EVENTS
Potential adverse events include, but are not limited to: Allergic reaction or hypersensitivity to contrast agent, anesthesia, scaffold materials (poly[L-lactide] [PLLA], poly[D, L-lactide] [PDLLA], platinum, or everolimus), and drug reactions to anticoagulation or antiplatelet drugs
• Vascular access complications which may require transfusion or vessel repair, including:
CAUTION: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use, inside the product carton (when available) or at manuals.eifu.abbott for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. This material is intended for use with healthcare professionals only.
Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs.
Information contained herein for DISTRIBUTION in the U.S. ONLY.
Abbott
3200 Lakeside Dr., Santa Clara, CA 95054 USA, Tel: 1.800.227.9902
™ Indicates a trademark of the Abbott Group of Companies.
The risks described below include the anticipated adverse events referenced in the contraindications, warnings, and precautions sections of the everolimus labels / SmPCs and / or observed at incidences ≥ 10% in clinical trials with oral everolimus for different indications. Refer to the drug SmPCs and labels for more detailed information and less frequent adverse events.
• Bleeding and coagulopathy (including hemolytic uremic syndrome [HUS], thrombotic thrombocytopenic purpura [TTP], and thrombotic microangiopathy; increased risk with concomitant cyclosporine use)
Constipation
• Cough
• Diabetes mellitus
Diarrhea
• Dyspnea
• Embryo-fetal toxicity
• Erythema
• Erythroderma
• Headache
• Hepatic artery thrombosis (HAT)
• Hepatic disorders (including hepatitis and jaundice)
• Hypersensitivity to everolimus active substance, or to other rapamycin derivates
• Hypertension
• Infections (bacterial, viral, fungal, or protozoan infections, including infections with opportunistic pathogens). Polyoma virus-associated nephropathy (PVAN), JC virus-associated progressive multiple leukoencephalopathy (PML), fatal infections and sepsis have been reported in patients treated with oral everolimus.
• Kidney arterial and venous thrombosis
• Laboratory test alterations (elevations of serum creatinine, proteinuria, hypokalemia, hyperkalemia; hyperglycemia, dyslipidemia including hypercholesterolemia and hypertriglyceridemia; abnormal liver function tests; decreases in hemoglobin, lymphocytes, neutrophils, and platelets)
• Lymphoma and skin cancer
• Male infertility Menstrual irregularities
• Nausea
• Nephrotoxicity (in combination with cyclosporine) Non-infectious pneumonitis (including interstitial lung disease)
• Oral ulcerations
• Pain
• Pancreatitis
• Pericardial effusion
• Peripheral edema
• Pleural effusion
• Pneumonia
• Pyrexia
• Rash
• Renal failure
• Upper respiratory tract infection
• Urinary tract infection
• Venous thromboembolism
• Vomiting
• Wound healing complications (including wound infections and lymphocele)
There may be other potential adverse events that are unforeseen at this time.
VIVA 2025
Compiled by Bryan Kay and Jocelyn Hudson
‘Excellent’ oneyear outcomes from ROADSTER 3 show TCAR is ‘safe and effective’
ONE-YEAR OUTCOMES IN THE ROADSTER 3 post-approval study to evaluate the safety and effectiveness of transcarotid artery revascularization (TCAR) using the Enroute stent and neuroprotection system (Boston Scientific) in standard-surgical-risk patients revealed a 1.5% intention-to-treat rate of composite major adverse events (1.3% per protocol).
Delivering the results at the 2025 Vascular Interventional Advances (VIVA) conference (Nov. 2–5) in Las Vegas, Meghan Dermody, MD, chief in the Division of Vascular Surgery at Penn Medicine Lancaster General Health in Lancaster, Pennsylvania, also reported an intention-to-treat ipsilateral stroke rate between 31–365 days of 0.6% (0.7% per protocol).
The results were drawn from patients enrolled between September 2022 and June 2024—344 intention to treat and 219 per protocol—at 48 U.S. sites. The primary endpoint was the hierarchical composite incidence of major adverse events, defined as stroke, death or myocardial infarction
DISEASE
By Bryan Kay and Jocelyn Hudson
ENVVENO MEDICAL HAS announced that it received an “unfavorable” decision from the US Food & Drug Administration (FDA) in response to its supervisory appeal of the “notapprovable” letter it received on Aug. 19 in response to its premarket approval (PMA) application for the VenoValve device, a surgical replacement venous valve for treating severe deep chronic venous insufficiency (CVI).
The supervisory appeal upheld the review staff decision in the not-approvable letter that the VenoValve did not meet the standard of reasonable assurance of safety and effectiveness, enVVeno reported.
“Although the appeal decision was not the result we are looking for, it did provide
within 30 days and ipsilateral stroke from 31 to 365 days post procedure. The rate of stroke/death/MI at 30 days was 0.9% (0.6% per protocol), with a 30-day stroke rate of 0.9% (0.6% PP).
“ROADSTER 3 is the first independently adjudicated, prospective study evaluating TCAR in a standard-surgical-risk population,” said Dermody, who first presented 30-day outcomes from the study at VIVA 2024. “Results demonstrate that TCAR is safe and effective, with excellent clinical outcomes.”
The 30-day outcomes represented the lowest reported in a standard-surgical-risk population, she added.
PERFORMANCE III
demonstrates ‘very low’ 30-day
event rates for dual neuroprotection in TCAR
THIRTY-DAY RESULTS FROM THE PERFORMANCE III study of integrated embolic protection (IEP) in transcarotid artery revascularisation (TCAR) demonstrate “very low” 30-day event rates. Sean Lyden, MD, chair of vascular surgery at the Cleveland Clinic in Cleveland, Ohio, shared this finding during a late-breaking trials session at VIVA 2025.
The prospective, multicenter PERFORMANCE III study evaluated the safety and effectiveness of the Neuroguard IEP system (Contego Medical), 70cm carotid stent and the Neuroguard IEP embolic protection system for direct TCAR in 146 patients across 26 clinical sites. The Neuroguard IEP embolic protection system includes both a direct access kit and a blood flow reversal system.
“The 30-day event rates in the PERFORMANCE III study are the lowest reported in a prospective, multicenter carotid artery revascularisation study,” said Lyden, who is
valuable insight into the criteria that would be necessary for approval of enVVe, our nextgeneration transcatheter based replacement venous valve,” said Robert Berman, enVVeno Medical’s CEO. “enVVe should have a different safety profile than an open surgical device and is ready for human testing. Assuming that we can reach alignment with the agency on achieveble endpoints for enVVe, it makes sense to turn our attention and devote our resources to enVVe.”
Meanwhile, data on the VenoValve device continued apace at the podium during the fall.
At the 39th European Society for Vascular Surgery (ESVS) annual meeting (Sept. 23–26) in Istanbul, Turkey, SAVVE trial principal investigator Matthew Smeds, MD, of Saint Louis University in Saint Louis, Missouri, shared a new finding that the novel bioprosthetic valve’s impact on ulcer area reduction and symptoms is
co-national principal investigator of PERFORMANCE III. In the PERFORMANCE III study, the 30-day stroke rate was 0% per the intention-to-treat analysis, with zero myocardial infarctions, zero cranial nerve injuries, zero neurological deaths, and zero stent thromboses reported. The primary endpoint of major adverse events through 30 days was 0.69% (intention-to-treat) and 0% (per-protocol), which Lyden noted was significantly lower than the predefined study performance goal.
PROMISE III: Six-month
data ‘reinforce’ case for TADV in no-option
CLTI patients
SIX-MONTH OUTCOMES AMONG NO-OPTION chronic limb-threatening ischemia (CLTI) patients treated using transcatheter arterialization of the deep veins with the LimFlow system (Stryker/Inari Medical) in the PROMISE III trial showed a 81% rate of amputation-free survival.
Principal investigator Daniel Clair, MD, chair of vascular surgery at Vanderbilt University in Nashville, Tennessee, delivered the primary safety endpoint result from PROMISE III at VIVA 2025. He told attendees that the six-month data for the “only purpose-built system that is FDA [Food and Drug Administration]-approved for treatment” of no-option CLTI “reinforce the evidence for TADV with the LimFlow system” among this patient group.
A total of 100 patients (103 limbs) underwent TADV between 2022 and 2024 in PROMISE III. All included limbs had non-healing ulcers or gangrene, with 75% Rutherford class 5 and 25% class 6. Technical success was 97%.
At six months, limb salvage was 87%, survival was 93.8%, and approximately 80% of wounds were completely healed or healing, Clair added. The median pain score was 2, “significantly decreased” from 6 at baseline (p<0.0001).
dependent upon ulcer location. Smeds shared that the U.S. pivotal study of the device assessed 61 ulcers in 43 of the 75 patients enrolled in SAVVE. The presenter specified that, of these 43 patients, 65% had ulceration above the malleolus and 35% had ulceration below. He noted that average starting ulcer size was larger in the above-malleolus location as compared to the belowmalleolus location. Smeds stated that, when stratified by location, average ulcer size reduction was 12cm in ulcers above the malleolus, while the corresponding figure was 3.3cm in those below the malleolus. In terms of ulcer duration, Smeds revealed that patients who had had an ulcer for less than a year at baseline had a more significant reduction in ulcer size. Smeds concluded that the VenoValve device appears to have a positive effect on ulcer healing, particularly in patients with
ulcers of less than one-year duration. He added that the impact of ulcer healing as well as patient-reported symptoms and quality of life is more substantial in patients with ulcers above the ankle and that this occurs within one month of device placement.
Similarly, at the 2025 annual meeting of the Western Vascular Society (Sept. 14–17) in Ojai, California, data was presented by Adam Surti, MD, a general surgery resident at Cedars Sinai Medical Center in Los Angeles, show that among 44 patients in the SAVVE trial classified as having C6 disease, 31 had ulcers for more than one year. At two-year follow-up, 35 C6 patients remained in the study, and, for patients with ulcer duration greater than one year, ulcer area reduction was 1.8cm2 at one year and 0.3cm2 at two years. Ulcers located above the malleolus showed the most significant healing, with area decreasing from 12 to 3.8 cm2. Ulcer recurrence rates at two-year follow-up was 7%, notably lower than the 15%–44% recurrence rates reported in literature, Surti reported.
Meghan Dermody
Matthew Smeds (top) and Adam Surti
NESVS 2025
Grappling with the workforce challenges of the future
By Bryan Kay
IT’S ONE OF THE ENDURING REASONS GIVEN cross-generationally in answer to the question, “Why vascular?” It goes something along the lines of, “I value that vascular surgeons have longitudinal relationships with their patients.”
That was the message from Jessica Simons, MD, the 2024–25 president of the New England Society for Vascular Surgery (NESVS), a professor of surgery at UMass Chan Medical School in Worcester, Massachusetts, and the institution’s integrated vascular surgery residency program director.
Simons was giving her outgoing presidential address at the 2025 NESVS annual meeting in Providence, Rhode Island (Sept. 26-28) on the topic of generational change in vascular surgery, exploring the values of each generation and those that endure in the context of the future of the vascular workforce.
Amid workforce pressures and some researchers predicting a surplus of vascular surgeons deeper into the future, Simons questioned how care delivery will look. “Given that surgeons are pulled in so many directions, yet seek a reduced clinical workload, we likely need that surplus of surgeons that some researchers are projecting and maybe more so,” she said. “How can we maintain continuity with and accountability to our patients without working 24/7, 365 or even 80 hours a week?”
Fundamentally, she asked, can
adaptations to work be made so that surgeons can meet their personal goals without compromising patient care? Simons explored shifting attitudes toward work across generations—Baby Boomers and Gen X, Y and Z—which roughly goes like this, she said: “Boomers live to work, Gen X works to live, Gen Y wants to live, live, live and work as they need to.”
“One of these isn’t better than the other,” Simons added. “Everyone in vascular surgery works pretty darn hard. But attitudes toward work have changed. And the example of blurred work-life boundaries is particularly interesting.”
While acknowledging her attitude reflects the generation from which she comes, Gen X, Simons underscored that “our work-life balance equation has to reflect that it is not just about me and my home life.”
How is this achieved? she pondered.
“How do we meet the demands for patient care while meeting the demands for life outside of work, all while stretched thinner than ever across healthcare and experiencing a shortage of surgeons? It sounds pretty impossible. But I would argue this is a group that likes impossible challenges.”
But the basic tension underlying the question is the same as the one Gen X saw as their parents confronted a rapidly evolving culture and home and work-life dynamics, Simons added—“a conundrum that is shared across generations.”
In common with the answer to “Why vascular?”, “we have more in common than we realize,” she told NESVS 2025. Some values, such as the altruism that might be contained in a desire to engage in longitudinal care, are conserved across generations, she said.
‘WHAT
I TALK ABOUT WHEN I TALK ABOUT VALUE’
OUTGOING WESTERN VASCULAR
Society (WVS) President Ahmed AbouZamzam Jr., MD, provided a possible prescription for value in vascular surgery that goes beyond the monetary value assigned to the profession.
Using the memoir of Japanese writer Haruki Murakami, What I Talk About When I Talk About Running, to illustrate the point, Abou-Zamzam told attendees of the 2025 WVS annual meeting (Sept. 14–17) in Ojai, California, how the author “reflects how running has shaped his writing and his writing has impacted his running.”
Just as vascular surgery takes hard work, dedication and persistence, Abou-Zamzam said he considers how he could say the same about his own passion for running and how it overlaps with his working life.
“I hear people say, we are not valued [as vascular surgeons],” he said. “I think it is because we are using the word differently … we may be misunderstanding each other.” While efforts to demonstrate the monetary value vascular surgeons bring to the healthcare system are well chronicled, Abou-Zamzam added, “there is so much more to value when I talk about value.”
For him, that can mean there are certain joys for which there may not be a monetary value. “My favorite part is walking out of the OR [operating room] and going to talk to the patient’s family,” he said. “I mean, I don’t know anybody who can do anything better than when you see the relief on their faces. I think we have to look at these things and everyone find that satisfaction. And that’s what I seem to be thinking about when I think about value.”—Bryan Kay
Jessica Simons
Ahmed Abou-Zamzam
SOCIETY BRIEFS
Compiled by Marlén Gomez
SVS Foundation funds vascular initiatives to the tune of nearly $360,000 last year
THE SVS FOUNDATION’S 2025 ANNUAL report details a year of significant progress in research, education and advocacy aimed at improving vascular health worldwide.
The foundation awarded more than $359,000 in grants during the 2024–2025 cycle, continuing its legacy of supporting research and training. Since 1987, the SVS has provided nearly $16 million in funding to advance vascular science and prepare future leaders in the field.
The report underscores the foundation’s mission to optimize vascular health through research, education and programs that prevent and treat circulatory disease.
Among the year’s milestones was the creation of the Enrico Ascher Vascular Innovation Institute, which will officially launch at the 2026 Vascular Annual Meeting (VAM). The institute is designed to foster innovation, mentorship and education in vascular surgery, offering seed funding for new ideas and hosting the Roy Greenberg Distinguished Lecture and SVS Medal of Innovation.
The report also highlights the Vascular Health Step Challenge, which marked its fourth year with its first in-person event. More than 100 participants joined a walk at Stanford University, contributing to a global effort that logged 47,806 miles and raised $78,000 to promote awareness of peripheral arterial disease (PAD).
Financially, the foundation reported $8.1 million in total liabilities and equity, with 51% of funds spent on programs. Contributions came primarily from industry (60%), followed by individual donors (25%) and foundations or societies (15%). All board members contributed, along with 31% of active members.
For more information, visit vascular.org/ SVS-Foundation
Abstract submissions open for VAM 2026
THE SVS INVITES AUTHORS TO SUBMIT abstracts for the 2026 Vascular Annual Meeting (VAM 2026) by Jan. 7, 2026, at 3 p.m. Central Time. The event, held at the Hynes Convention Center in Boston (June 10–13), will feature the latest advancements in vascular surgery and offer a platform for researchers and practitioners to share their innovative work.
Researchers are invited to submit both traditional abstracts and video presentations. Scientific abstracts account for nearly 50% of the daily programming, offering a significant opportunity to present your work to leaders in the field and to advance vascular care.
Learn more at vascular.org/VAM
SVS FOUNDATION DONORS TURN OPPORTUNITY INTO LIFELONG IMPACT
THE SVS FOUNDATION IS MARKING A MILESTONE IN THIS YEAR’S Celebration of Science year-end giving campaign, as former awardees have now contributed amounts exceeding the support they once received.
Julie A. Freischlag, MD, exemplifies this spirit of generosity after receiving $12,000 in early-career funding for the E.J. Wylie Traveling Fellowship. The fellowship allowed her to visit Yale University to observe the basic science laboratory of Bauer Sumpio, MD, PhD, and to visit Australia to observe clinical vascular surgery in Sydney, Melbourne and Geelong. Over the years, she has contributed almost three times the award amount to the SVS Foundation.
Ronald Dalman, MD, who also received the E.J. Wylie Traveling Fellowship, has contributed more than triple what he received in funding over his lifetime. He said his decision to give stems from a deep belief in the foundation’s mission.
James H. Black, MD, another Wylie recipient, said his contributions reflect the lessons he learned early in his career: collaboration and continuous learning.
Joseph L. Mills, MD, received the Wylie award in 1993, a recognition that he credits with laying the foundation for his academic career. Additionally, he was awarded a VISTA grant from the foundation, which enabled his team to conduct essential follow-up research on a Patient-Centered Outcomes Research Institute (PCORI) study focused on preventing amputations in underserved and economically disadvantaged individuals with diabetes. This opportunity also allowed him to mentor the next generation of researchers specializing in peripheral vascular disease. Between 2015 and 2025, Mills received $45,500 in funding and has since surpassed his own award amount.
Research funding remains scarce, and the SVS Foundation relies on donors’ contributions to sustain programs that foster discovery and education. These gifts fund fellowships, research grants and initiatives that help vascular surgeons tackle complex challenges. “One needs resources for mentors to teach the next generation, and donors can direct those resources to exciting and worthwhile projects, as there is never enough research funding available—especially now,” Freischlag said. “Giving back makes one feel proud that you can help someone else achieve their dream.”
Matthew Eagleton, MD, SVS Foundation board chair, said: “We ask a lot of our members. We ask for time. We ask for money. We ask for support,” Eagleton said. “For some of you, we are going to make an additional ask—consider giving back.”
For more information, visit vascular.org/SVS-Foundation
Froedtert Hospital first in Wisconsin to earn national vascular verification
FROEDTERT HOSPITAL HAS become the first hospital in Wisconsin to receive national verification as a Comprehensive Inpatient Vascular Center through the American College of Surgeons (ACS) Vascular Verification Program (VVP), in partnership with the SVS.
the Society for Vascular Surgery is a testament to our team’s unwavering commitment to excellence in patient care,” said Peter Rossi, MD, associate director of the Heart and Vascular Service Line for Froedtert and the Medical College of Wisconsin health network, as well as division chief of vascular and endovascular surgery.
The designation also recognizes Froedtert Hospital as an ACS Surgical Quality Partner, a title awarded to institutions that meet rigorous standards in surgical care and demonstrate a commitment to continuous quality improvement.
“Achieving vascular verification from the American College of Surgeons and
NIH-funded WARRIORS trial advances toward launch
THE NATIONAL INSTITUTES OF Health (NIH) has approved funding for the WARRIORS international randomized controlled trial comparing endovascular aneurysm repair (EVAR) with watchful waiting in women with small abdominal aortic aneurysms (AAAs) measuring 4–5.5cm.
In the U.S., the trial will leverage the SVS Vascular Quality Initiative (VQI) endovascular aneurysm repair (EVAR) and vascular medicine registries to collect data at treatment and at one- and five-year follow-up. Patients will provide consent to the data-coordinating center at the University of Alabama at Birmingham to receive their identified data. This center will oversee site selection, contracts and data queries.
Adam Beck, MD, chair of the SVS Vascular Quality Initiative (VQI) and U.S. principal investigator for the WARRIORS trial, emphasized the importance of both the scientific question and the innovative use of registry infrastructure.
“This trial addresses one of the most important unanswered questions in aortic disease—how best to care for women with small AAAs. Integrating VQI registry data directly into a national and international randomized study allows us to streamline site selection and dramatically enhance data collection efficiency. This model has the potential to accelerate enrollment, reduce cost and fundamentally change how large-scale vascular trials are conducted,” said Beck.
The trial is a study outside of the SVS Patient Safety Organization (PSO) but uses the VQI registries for data collection with SVS PSO permission.
“This recognition reflects the skill, collaboration and dedication of our multidisciplinary team in providing the highest standards of vascular care to our community.”
The VVP is an evidencebased initiative designed to help hospitals build and strengthen quality improvement infrastructure within their vascular disease programs. Hospitals interested in pursuing verification through the AVS-SVS Vascular Verification Program can find more information and help at vascular.org/VVP
The U.S. arm of the WARRIORS trial plans to enroll 350 patients across 35 sites. Fivos, the SVS PSO’s technology partner, will support registry development, create custom variables and provide training for participating centers. Data will be transmitted quarterly for three years during enrollment and annually for five years of long-term follow-up, for a total project duration of eight years. The NIH-funded trial is expected to clarify whether early intervention with EVAR offers benefits over surveillance in women with small AAAs— a question with significant implications for clinical practice.
Adam Beck
New era beckons: Vascular Specialist moves in-house as new chapter opens for SVS official newspaper
By Bryan Kay
MALACHI SHEAHAN III, MD, HAS BEEN AT THE helm of Vascular Specialist for more than seven years. In that time, it is fair to say the newspaper—the official voice of the SVS—has evolved. About a year and a half after he took over at the helm in the summer of 2018, the title changed publishers. With the swap in publishing partner came a new tone and editorial strategy.
Now, another new era beckons for Vascular Specialist, which mails out monthly to each of the Society’s members. From Jan. 1, the SVS will publish the title in-house after six years of a publishing partnership with London, Englandbased medical media and event company BIBA Medical, owners of the globally renowned Charing Cross (CX) International Symposium founded by the late vascular surgery luminary Roger Greenhalgh, MD.
And Sheahan, Vascular Specialist’s medical editor with overall editorial oversight for the paper, sees opportunity for further evolution in the title’s voice. Six years ago, when he last confronted an unknown Vascular Specialist future, he wasn’t quite sure what to expect. But, says the chair of vascular surgery at Louisiana State University (LSU) in New Orleans, the partnership with BIBA Medical breathed new life into the paper.
“For the first time, we really started producing our own content rather than commenting on news we got from the wires, so to speak—that really limited the scope of what we could cover,” Sheahan recalls. “A majority was cardiologyrelated, medical-related. Of course, that is interesting—but we could never really cover content on-site at the vascular surgery regional meetings like we do now, or at VESS [the Vascular and Endovascular Surgery Society], or at SCVS [the Society for Clinical Vascular Surgery]. All of that came on with BIBA.”
Over the last six years, Sheahan says, Vascular Specialist was able to build its own brand. With the title now moving
IN MEMORIAM
in-house to the SVS, with the Society now acting as both owner and publisher, the chief editor hopes to be able to further flesh out that brand. “Now we cover breaking science in the vascular surgery world directly, and we bring a different flair, much more of a voice,” he reflects. “What are we? We are not a journal, not strictly a newspaper, and not quite a magazine. I would say we are much more ‘of the specialty,’ a must-read for folks who want to stay up to date with what is happening with the vascular specialty: the science, the regionals, the politics of it, anything controversial, government relations, really new content. In the longer term, we plan to do more mapped-out content, with more lead time, and more special issues.”
To that end, Vascular Specialist will move from a 12-issue publishing schedule to a nine-times-per-year title that places
“We are much more ‘of the specialty,’ a must-read for folks who want to stay up to date”
MALACHI SHEAHAN III
a laser focus on specific areas of vascular surgery, such as peripheral arterial disease (PAD) and venous disease. The paper has a new managing editor, Killian Meara, who will assist the medical editor in setting the editorial agenda. Sheahan also wants to broaden the range of voices that appear as guest editorialists, columnists and commentators.
“The paper now is how I have envisioned us one day to be: to be the newspaper for vascular surgery and for the specialty, and for anyone who is interested in it,” he says. “We have been able to increase our medical student readership, our trainee readership—creating content for
CLYDE BARKER, PIONEERING VASCULAR SURGEON AND PENN MEDICINE TITAN, DIES
CLYDE F. BARKER, MD, A towering figure in American surgery and a transformative leader at Penn Medicine, died peacefully at his home on Oct. 2, surrounded by family. He was 91. “So ended an era,” said Ronald DeMatteo, MD, chair of surgery at the University of Pennsylvania. “Surgeon, innovator, scientist, leader, administrator, counselor, husband, father, athlete, historian and friend. The term ‘giant’ is often applied to individuals who make important contributions to medicine or
medical education. That label seems insufficient to describe Dr. Barker. Rather, he was a titan.”
Barker dedicated 67 years to Penn Surgery, beginning his general surgery training in 1958 and never leaving.
He became a professor in 1973 and chief of vascular surgery in 1981. From 1983 to 2001, he served as the John Rhea Barton professor and chair of surgery,
them. We want to cover the specialty completely. I want to have more associate editors and more voices involved, so that it is not just me and my voice.
“We want to have more recurring writers, more vascular surgeons who will give the newspaper a different flavor and a different perspective than I can—a different sensibility and opinion, hopefully, from the way I think, so that we can be more well-rounded, I would say, and especially in the editorial process.”
And Sheahan, who now also serves as SVS secretary and is chair of the Vascular Surgery Board (VSB) of the American Board of Surgery (ABS), won’t be heading anywhere any time soon. He will remain as medical editor and as a popular and regular author of the page 2 editorial, a coveted spot which is the preserve of the paper’s chief editor to either write or commission. As for any perceived conflicts assigned to him? They remain just that: perception over reality, he says.
“I don’t see any of my other roles, for instance, necessarily as conflicts because they all serve the specialty, and everything I have written has been written in deference to the specialty—what would be best for vascular surgeons and their patients—and I don’t think there are true conflicts there,” he says. “But it is definitely time to bring more voices in. Everyone is going to write from the perspective of the specialty, of course; we may disagree, but that is the goal. Just having other views, different views, from different societies, will always be helpful to counteract any perceived conflicts of interest I might have.”
No greater testament to that is in evidence, perhaps, than editorials Sheahan has written in recent years taking a look at areas such as trauma surgery and cardiology where they intersect with vascular. To counter his own voice, he invited a trauma surgeon counterpart to write a rebuttal. It went over so well that he found himself accosted once again, more than three years later, at the recent American College of Surgeons annual meeting, by a trauma surgeon keen to remark on the two articles.
shaping generations of surgical leaders and researchers.
Born in Salt Lake City, Utah, Barker graduated from Phillips Exeter Academy and Cornell University, later earning his medical degree from Cornell Medical School in Manhattan, New York. A nationally ranked amateur tennis player, he brought the same discipline and boldness to the operating room.
He performed the first kidney transplant at the Hospital of the University of Pennsylvania and led Penn’s transplantation of clinical care and research.
Collaborating with immunologist Rupert Billingham, Barker contributed seminal papers on immune tolerance. His work with Ali Naji,
MD, yielded two Science publications that advanced understanding of autoimmunity in diabetes and tolerance induction in islet transplantation. Barker’s research was continuously funded by the National Institutes of Health (NIH) for 25 years, including five R01 grants and an NIH Merit Award. He published more than 400 papers and served on editorial boards, including that of Annals of Surgery
Beyond Penn, Barker held leadership roles in nearly every major surgical society, including presidencies of the American Surgical Association, American Society of Transplant Surgeons, Halsted Society, International Surgical Group, and the Philadelphia Academy of Surgeons. He also chaired the Board of the William Maul Measey Foundation and served as president of the American Philosophical Society.—Marlén Gomez
Clyde F. Barker
Malachi Sheahan III
CLINICAL&DEVICENEWS
Compiled by Bryan Kay and Jocelyn Hudson
ViTAA Medical announces FDA 510(k) clearance for aortic planning platform
VITAA MEDICAL HAS ANNOUNCED THAT THE FOOD and Drug Administration (FDA) has granted 510(k) clearance for AiORTA Plan, which the company describes as a “fully automated, hyper-precise aortic surgery planning solution.”
The tool aims to automate key preoperative measurements and streamline aortic case preparation by generating a complete aortic plan in minutes in a web-based system, producing automated aneurysm segmentation, centerline extraction, precise diameter and angulation measurements, and instant volumetric modeling.
The other elements of ViTAA’s broader AiORTA platform— which also includes AiORTA Maps and AiORTA Watch—are currently in multicenter clinical studies. Maps is a diagnostic aid that aims to produce patient-specific vessel strength analysis, while Watch looks to provide longitudinal monitoring for early complication detection.
“Regulatory clearance of AiORTA Plan validates our approach of combining automation with precision medicine,” said Randy Moore, MD, a vascular surgeon at the University of Calgary in Alberta, Canada, and chief medical officer at ViTAA Medical. “As we continue our international clinical studies for AiORTA Maps and AiORTA Watch, we’re focused on delivering solutions that help physicians see beyond outdated size guidelines and gain insights into vessel behavior that can inform decision-making throughout the patient journey.”
Frank J. Veith, MD, vascular pioneer and chair of the
Elucid launches PlaqueIQ image analysis software for carotid arteries
ELUCID LAUNCHED ITS PLAQUEIQ IMAGE analysis software for the quantification and classification of plaque morphology in the carotid arteries. According to the company, as the “first and only” computed tomography (CT)-based plaque analysis software indicated for the carotid vasculature, PlaqueIQ may help physicians diagnose carotid plaques at risk for rupture, and develop patient-specific treatment pathways to monitor and prevent stroke.
“The ability to characterize plaque composition precisely revolutionizes carotid stroke risk assessment,” said David Deaton, MD, an adjunct associate professor of surgery at the University of Pennsylvania in Philadelphia. “Plaque composition has long been recognized as a critical risk element for stroke but was not available with conventional imaging techniques. Precise determination of plaque composition supersedes the traditional stenosis assessment and allows a more accurate identification of patients at highest risk for carotid stroke, and facilitates procedural choice and planning.”
PlaqueIQ is a Food and Drug Administration (FDA)-cleared tool that provides non-invasive plaque analysis based on objective histology, offering physicians “CT Virtual Histology,” Elucid claims. The software delivers quantification and classification of plaque morphology and is described in a press release as being “uniquely capable” of identifying and quantifying lipid-rich necrotic core—a plaque type strongly linked with both cardiovascular and cerebrovascular risk.
AiORTA Plan
VEITHsymposium, who performed the first endovascular aneurysm repair (EVAR) of an abdominal aortic aneurysm (AAA) in the U.S. three decades ago, hailed the approval as a milestone. “This is an important advance,” he said. “AiORTA Plan can streamline how physicians prepare for complex aortic procedures, and as the broader AiORTA platform matures with Maps and Watch in clinical evaluation, it has the potential to transform individualized care by providing critical insight.”
01: 4.5” x 5.625”
Shape Memory Medical announces midway milestone in AAA-SHAPE pivotal trial
SHAPE MEMORY MEDICAL HAS reached 50% enrollment in its ongoing AAA-SHAPE pivotal trial, the company recently revealed.
AAA-SHAPE is a prospective, multicenter, randomized, open-label trial to determine safety and effectiveness of the investigational Impede-FX RapidFill device to improve abdominal aortic aneurysm (AAA) sac behavior when used in conjunction with elective endovascular aneurysm repair (EVAR).
The patient—the 90th to undergo treatment in the trial—was treated by principal investigator Aleem Mirza, MD, a vascular surgeon at Orlando Health Heart and Vascular Institute in Orlando, Florida.
AAA-SHAPE will enroll 180 patients with infrarenal AAAs across up to 50 sites in the U.S., Europe and New Zealand.
Study participants will be randomized 2:1, either to EVAR plus sac management with Shape Memory’s Impede-FX RapidFill (the treatment arm) or to standard EVAR (the control arm). Key endpoints will compare sac diameter and volume change, endoleak rates, and secondary interventions.
InterVene receives FDA 510(k) clearance for Recana thrombectomy system
INTERVENE RECENTLY REVEALED it has received 510(k) clearance from the Food and Drug Administration (FDA) for the Recana thrombectomy catheter system, which is designed for the treatment of venous in-stent restenosis and native vessel obstructions.
A press release notes that Recana is a fully integrated system featuring a debulking catheter, introducer and collection sheaths, and nitinol collection baskets designed to simplify challenging venous procedures for physicians and improve clinical outcomes.
“The long-term consequences of venous obstructions and occlusions can be devastating for patients,” said William Marston, MD, vascular surgery division chief at the University of North Carolina at Chapel Hill.
“Based on my pre-clinical experience, I believe the Recana system represents a promising treatment option that overcomes key limitations of traditional recanalization methods.”
InterVene shared that it had designed Recana’s integrated system of complementary components to enable single-session treatment, reduce the need for additional devices, and improve procedural efficiency.
GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surfacea
Consult Instructions for Use eifu.goremedical.com
Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery de novo and restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 7.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery in-stent restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 6.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in iliac artery lesions up to 80 mm in length with reference vessel diameters ranging from 4.0 – 12 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is also indicated for the treatment of stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous (AV) access grafts. CONTRAINDICATIONS: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is contraindicated for non-compliant lesions where full expansion of an angioplasty balloon catheter was not achieved during pre-dilatation, or where lesions cannot be dilated sufficiently to allow passage of the delivery system. Do not use the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II.
GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surfacea,b
Evan Brownie, MD Murray, Utah
TRUSTED BY THOSE WHO TREAT COMPLEX CASES
Kiang, MD Loma Linda, California
Erie, Pennsylvania
In complex cases, experience and evidence make all the difference. Proven across SFA lesions with average lengths of 24 cm and 87% TASC C or D, the VIABAHN® Device demonstrated excellent patency and durability with 76% 5-year freedom from target lesion revascularization.1 Discover how practicing physicians apply these results to guide treatment of SFA disease. Watch the videos.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
a As used by Gore, Heparin Bioactive Surface refers to Gore’s proprietary CBAS® Heparin Surface.
b Also referred to as the GORE® VIABAHN® Endoprosthesis with PROPATEN Bioactive Surface in some regions.
1. Iida O, Ohki T, Soga Y, et al. Five-year outcomes of the GORE VIABAHN Endoprosthesis for the treatment of complex femoropopliteal lesions from a Japanese post-market surveillance study. Vascular Medicine 2024;29(4):416-423
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.