What the Society is doing for vascular surgery in D.C. as election arrives
3
JVS ASSOCIATE EDITOR
Ulka Sachdev-Ost recalls her mother's career
10
COVID-19 ALI amid the pandemic
Members asked; SVS listened.
The Society for Vascular Surgery (SVS) has launched a Branding Toolkit to help its members brand the specialty in order to elevate and differentiate their practices.
TANATOMY OF A BRANDING CAMPAIGN: MAKING VASCULAR SURGERY MORE VISIBLE
BY BETH BALES
27
AMPUTATIONS
Value of podiatry in limb salvage
his first set of branding tools tells referring physicians what vascular surgeons do and why they are critical partners when it comes to treating their patients with circulatory disease.
With the toolkit, vascular surgeons also can emphasize to other healthcare professionals that surgery is only part of the repertoire of treatment they offer.
The tools, to help members communicate about the comprehensive care they provide, have been in development for more than two years, said Joseph Mills, MD. He led the branding effort as chair of the Public and Professional Outreach Committee.
SVS members identified branding as their No. 1 initiative in 2018, he said. Subsequent research identified confusion among patients as well as other physicians with respect to which medical specialty best treats vascular issues and highlighted the misconception that surgery is the only treatment modality vascular surgeons offer.
To address these issues, the branding effort emphasizes two main concepts, said Mills: “We provide comprehensive care, and surgery is only part of our story. No one else providing components
“We provide comprehensive care, and surgery is only part of our story”— Joseph Mills
of vascular care is trained and capable of offering all of the available options and long-term follow-up care that we can do.
“No one wants to get rid of the essential fact that we’re surgeons—but we’re not only that. We don’t just solve patients’ acute problems. We provide care for their vascular disease for the rest of their lives.”
In many instances, he noted, “we are viewed as highly technical surgeons who are relied upon for episodic interventions.
“So to brand ourselves properly, the key message going forward is that we must do what we say we do, which is to provide comprehensive and longitudinal care.”
THE BIG PICTURE
Give people a fair chance and watch the results
BY BHAGWAN SATIANI, MD
TEN YEARS AGO WHEN WE WROTE A PAPER ON diversity that was published in the Journal of Vascular Surgery (JVS), it barely caused a ripple. Entitled “Diversity in membership and leadership positions in a regional vascular society,” it was co-authored by Patrick S. Vaccaro, MD, and Michael R. Go, MD. We are, respectively, of South Asian, Caucasian and Southeast Asian/Pacific Islander backgrounds.
I am not sure whether my co-authors got any feedback, but I perceived negative vibes that may have hurt my academic aspirations. Our work was 10 years ahead of its time. Perhaps times were changing, but within three years our regional society had its first female president and one of North African descent.
Our work was provocative but may have been misunderstood. My frustration with how things were year after year led to an effort to look at the data to understand the homogeneity of our officers.
It did not petition for a quota system; neither did it suggest there had been a deliberate plan to keep others out. G. Patrick Clagett, MD, then SVS president, had asked Frederick Beavers, MD, and I to co-edit a JVS diversity supplement, and insisted that the work be included. I agreed with some trepidation and concern about how it would be interpreted.
In 2008, by our estimate our regional vascular society had 68% of members in private practice. Only 5.7% of members were female, 1% were African Americans and even fewer were Latinos.
After reviewing 30 years of member records by academic/private practice, gender, race and ethnicity, we concluded that private practitioners, women, and ethnic and racial minorities were underrepresented in senior leadership positions. These groups were appointed to junior councilor roles—like I was—but did not progress to senior leadership positions.
We were careful to note: “Our findings should not be
taken to mean that the lack of diversity in membership or leadership positions necessarily implies a conscious or planned strategy to exclude diverse members. Rather than a ‘glass ceiling,’ which implies an active effort to exclude women and minorities, our findings are consistent with Blakemore’s postulate of ‘cumulative disadvantages.’”
Additionally, after a review of the diversity literature, we suggested: “Similar attraction and self-categorization theories suggest that people are more likely to associate themselves with people of similar demographic
I insisted that our faculty would do fine without any of us putting our feet on the scales for anyone
characteristics, including age, race and gender. Self-formed groups such as professional societies, particularly work groups, tend to organize themselves along homogenous lines. On the other hand, randomly formed groups generally exhibit more diversity.”
We determined that the literature was consistent that individuals preferred to interact with members “who are of their own kind.”
This supported our bias that groups “in the know” were much more likely to benefit from the organization. We suggested several actions by the society to advance diversity of all kinds, not just gender, race and ethnicity, but also of thought and practice type. Finally, my fellow authors and I concluded our paper with a plea that “other than the issue of fairness, why should professional organizations such as the [Midwestern Vascular Surgical Society] alter course? A possible answer is self-
preservation.” The world has since moved on to some degree. The biggest gains in healthcare occupations in the United States have occurred in areas other than among physicians. A lack of opportunity and mentorship are still significant obstacles in the way of giving qualified people a fair chance to progress.
When starting a Faculty Leadership Institute (FLI) at my institution, I was buttonholed by many diversity advocates in an effort to make sure that the groups had adequate minority and female representation.
My answer was consistent with my political philosophy: equality for all. I insisted that our faculty would do fine without any of us putting our feet on the scales for anyone. We made sure our call for applications got wide publicity in person, in newsletters and in emails, especially for high-potential women and minorities.
I was right. Their representation was better than their respective share of the faculty in the medical center. But if it were not for personally reaching out to some faculty who were reluctant to apply, thinking they had no chance of getting in, our goal of the best possible cohort would not have been achieved.
A relatively newly-hired African American sub-specialty surgeon was appointed as an interim division director, and had been overwhelmed at even the mere thought of applying. It took some arm-twisting to get him to do so. The extra education for this high-potential faculty member became very useful in his role, and he is flourishing several years later. Several men and women also needed face-toface conversations about the opportunities the FLI could provide them. All we needed to do was reach out to people and give everyone a fair chance.
In essence, that is all people are asking for.
Bhagwan Satiani is professor emeritus in the division of vascular diseases and surgery, the department of surgery, in the College of Medicine at The Ohio State University. He is an associate medical editor of Vascular Specialist.
VASCULAR SPECIALIST
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD, Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Drudi, MD
Executive Director SVS Kenneth M. Slaw, PhD
Director of Membership, Marketing and Communications Angela Taylor
Managing Editor SVS Beth Bales
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA Publishing. Content for the News From SVS is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA Publishing will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein.
The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com.
For missing issue claims, e-mail subscriptions@bibamedical.com.
Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA Publishing.
Published by BIBA Publishing, which is a subsidiary of BIBA Medical Ltd.
Publisher Roger Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Jocelyn Hudson, Suzie Marshall
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe 526
Bhagwan Satiani
New JVS associate editor for diversity follows in the footsteps of her mother
BY BRYAN KAY
It took Journal of Vascular Surgery (JVS) associate editor Ulka Sachdev-Ost, MD, a while to realize just how much of an impact her mother’s journey in medicine had had on her own career.
Sachdev-Ost reveals an intriguing backdrop to an appointment that came about in the wake of a controversial JVS paper on younger vascular surgeons and supposed “unprofessional behavior,” which raised the specter of a lack of diversity in vascular surgery and medicine. The brand new JVS role is, of course, focused on diversity, equity and inclusion. For Sachdev-Ost, chief of vascular services at UPMC MageeWomens Hospital in Pittsburgh, the emphasis carries extra meaning. Because when her parents arrived in the United States from India as immigrants, they were both surgeons intent on continuing to pursue the surgical field. But while her father would carve out a career in neurosurgery, a different path was to beckon for Sachdev-Ost’s mother.
As Sachdev-Ost describes, the journey of the late Ranjit K. Sachdev was a tale of thwarted ambition. Yet, as she tells Vascular Specialist shortly after taking up the position at JVS, a roadmap for her own ascent emerges—a drive for the surgical arena deferred just a single generation.
“I’ve told this story to other people because it really did have such a profound impact on me,” explains Sachdev-Ost, also associate professor of vascular surgery at the University of Pittsburgh. “When my parents came to the United States, my mother—in some way, shape or form— got the message that she should not pursue a surgical field because it would be inconsistent with wanting to raise a family; and, especially if her husband was a surgeon, it just would be an ‘impossibility.’ And so, she ended up doing pathology.”
For Sachdev-Ost, her mother’s
experience eventually bore a hole. “She would tell me this story so many times, because it clearly bothered her that she made this change to an essentially nonclinical field, and because she had been told that she really just shouldn’t pursue surgery,” Sachdev-Ost recalls. “So, when I decided to do surgery, having her blessing to do so was really important to me. And it was actually the thing that, in the end, made me really excited about going into a surgical field. I’ve always kind of had a chip on my shoulder because of her.”
Sachdev-Ost’s associate editor duties are wide-ranging. Early efforts will focus on initiatives like broadening the reviewer pool of the JVS body of publications. “That’s a great way to diversify the people who are getting the first reads of the papers that are coming through the journals,” she says. “If you can diversify a reviewer pool, you can get different viewpoints and things that maybe traditional reviewers might not have thought of. That also increases the number of people who then become part of the Editorial Board. Just on social media, you can tell there are plenty of people who are ready and willing to be reviewers.”
In addition to her mother’s influence, Sachdev-Ost’s career has also drawn inspiration from the women surgeons she encountered during her time as a trainee at Mount Sinai in New York City. She watched on as they carved out success in surgery and as teachers while also raising families. “A lot of people really need that role model to feel like they belong in that space as well,” Sachdev-Ost says. “It was very important to me, and I think it’s very important to the next generation. I can tell you that I see that from my teaching
Freischlag unveiled as ACS president-elect
BY BRYAN KAY
Julie Ann Freischlag, MD, the first and so far only female president of the Society for Vascular Surgery (SVS), will be the next president of the American College of Surgeons (ACS).
“When my parents came to the United States, my mother—in some way, shape or form—got the message that she should not pursue a surgical field because it would be inconsistent with wanting to raise a family”—Ulka Sachdev-Ost
experience: I have so many women, so many women of color, who say when they do a rotation with us, ‘I didn’t realize that this could be something that I could actually do.’ I love being that role model for people, and I think a lot of people feel the same way.”
Vascular surgery occupies a key vantage point, Sachdev-Ost observes. “We have a particular view of health disparities, because a lot of times we are treating disease reflective—how do I put this— of a lack of medical attention.” As she settles into the position, she’s looking forward to pursuing editorials that highlight issues with particular impact for underrepresented minorities in medicine.
“I’m looking at a lot of what we do as vascular surgery—we should be trying to work ourselves out of a job. Like I said, a lot of what we deal with is late-stage disease. Is there a way that, if we targeted people a little bit earlier, or if we even did
THE WINSTON-SALEM, NORTH CAROLINA -based vascular surgeon was elected to serve as the 2020–2021 president-elect of the American College of Surgeons (ACS), a development announced at the ACS Clinical Congress 2020 (Oct. 3–7). Freischlag’s one-year term as president starts in October 2021.
Currently, Freischlag is CEO of Wake Forest Baptist Health and dean of Wake Forest School of Medicine in Winston-Salem, leadership roles she assumed in 2017 after nearly 30 years as a practicing surgeon and educator at medical institutions across the U.S.
Freischlag’s past faculty and hospital appointments include serving as professor of surgery and vice-chair in the section of vascular surgery at the Medical College of Wisconsin, Milwaukee, and professor of surgery and William Stewart Halsted Professor, chair and surgeon-in-
more on the educational side, then people wouldn’t necessarily need to have bypasses? People wouldn’t necessarily need to have amputations.” Ultimately, Sachdev-Ost doesn’t see herself as a diversity expert. “The same thing applies: that I’m hoping I work myself out of a job, that this doesn’t necessarily become a position that we have to have, because we’ve already achieved a certain level of diversity amongst the review process, the editorial process, and the writing process,” she says. “That may be who-knows-how-long down the road, but that’s the goal.”
A road whose route traces back to an ambitious mother. “I didn’t realize how impactful it was on me, but it really was,” Sachdev-Ost says, recalling her mother’s journey once more. “There are so many times that I think about that. She was a surgical person in every way. So, for her to not do it really bothered her—and it had such a huge impact on me.”
chief at the Johns Hopkins University School of Medicine in Baltimore.
She has been a surgeon-scientist throughout her career, and is considered an internationally renowned expert in the diagnosis and treatment of thoracic outlet syndrome. Freischlag was also a national investigator of the OVER (Open versus endovascular repair) Veterans Affairs Cooperative Study, a multicenter randomized trial on the repair of abdominal aortic aneurysms (AAAs). She has also led or participated in research on topic areas including vascular grafts and peripheral vascular disease.
A Fellow of the American College of Surgeons (FACS) since 1991, Freischlag has served in various leadership roles within the organization, including as a governor (2000–2006) and secretary (2002–2006). She was the 2013 president of the SVS.
Anatomy of a branding campaign: Making vascular surgery more visible
Continued from page 1
“We’ve worked hard to figure out how to create a practical toolkit with easily downloadable branding materials that can be customized so that each member can use them,” said Kenneth M. Slaw, PhD, SVS executive director. “And we’ve created the toolkit in such a way that members, as they use it, will continue to build it and improve it going forward.”
Members can personalize elements of the toolkit by adding their practice name, logo, contact information and even photos to the materials. They can download the materials immediately and/or order professionally printed materials through an online system. Branding videos—including a two-minute state-of-the-specialty video offering a broad overview of vascular surgery and five shorter snippets—can be used on member websites and on their social media feeds.
Vascular conditions
Condition-specific fliers have also been created to help members educate referral sources about the most appropriate care and referral for key vascular conditions, currently including abdominal aortic aneurysms, chronic limb-threatening ischemia and diabetic foot ulcers. “We picked conditions that were common and for which we have recently updated guidelines,” said Mills.
Additional condition-specific fliers are being planned, to include carotid and venous disease, thoracic outlet syndrome, and dialysis access, said Mills. Members are encouraged to suggest other topics.
The initiative is of such importance that Ronald L. Dalman, MD, SVS president, included it in the E. Stanley Crawford Critical Issues Forum in June, part of SVS ONLINE. It was part of an overall discussion of vascular surgery and its future within the U.S. healthcare system.
During the session, Mills discussed how vascular surgeons fit into the American healthcare system, what the role of the vascular specialist should be, and how vascular surgeons can differentiate themselves from other specialties with occasionally overlapping interests, said Dalman. The branding tools, he said, “are going to help us understand and position vascular surgery in such a way that our colleagues in the health system, and leaders in American healthcare who might not be physicians themselves, can understand what we do.”
The branding tools that are part of the initial release of the toolkit consist of the SVS member logo; the “Surgery is only part of our story” brand video;
Vascular surgeons are often viewed through the prism of episodic interventions, not the longitudinal care they provide
“We've worked hard to figure out how to create a practical toolkit with easily downloadable materials”—Kenneth M. Slaw
copy that can be featured on a member’s practice website; a referral brochure, to date geared to both podiatrists and primary care physicians; and referral source flyers. Additional tools to help SVS members engage with other referral audiences, hospital leadership, patients and consumers will be added over time.
Member input
Project leaders consulted with many members at multiple steps along the way,
including at the 2019 Vascular Annual Meeting (VAM), where members were urged to look at possible ads, fliers and other materials as they were being envisioned, developed and finalized.
“Surgery is only part of our story” resonated and became the key theme and meme for this branding initiative.
Branding consultant Springboard Brand & Creative Strategy and SVS staff held a number of photo shoots, capturing members in action. The results are true-to-
Putting the toolkit into action
William Shutze, MD, a member in community practice in Dallas, has lost no time in putting the new SVS member Branding Toolkit to use.
In fact, he was experimenting with it during the SVS Town Hall in mid-September at which it was introduced.
“One of the first things I did was download the member branding banner,” he said. “I have actually embedded that into my work templates on electronic health records at the hospital.” The red banner is larger than his signature and stands out, he said. “I’m hoping the idea will catch on and others will be inspired to do the same thing. It’s a powerful statement.”
He also has taken the audio file from the longer branding video and is now using it for the practice’s “hold” music. “It’s the right length and it gets the message out that we need to send.” He has customized the “leaderboard digital banner” for primary care physicians with pictures of himself and two of the 14 surgeons in the practice. This has become the footer for all correspondence with a referring physician. “It’s in my computer; I just drag it onto the correspondence; I don’t have to create it every time.”
life images that reflect the full spectrum of care provided by vascular surgeons.
Members can obtain initial log-in instructions to help set up their toolkit account at vsweb.org/1stBrandingLogin. After resetting their password, they will receive an email from the system with a temporary password and a link for login. Members should treat their access credentials with the same security measures they use with any other SVS accounts. For additional help see the Quick Reference Guide and the How-to Video, at vsweb.org/Branding.
In your hands
Both Mills and Slaw emphasized that members need to take the next steps to use the toolkit in order for branding to be effective. “This is really where it all begins,” said Slaw.
“We’re giving our members the tools they need to have effective conversations in their own local markets with referral sources,” said Mills. “Use them! Make a difference for yourselves and our profession by getting this message out in different ways and as often as you can.”
Mike Chapman, an account director at Springboard, called the SVS Branding Toolkit new ground. “To my knowledge there is no medical society in the country that has developed what SVS has just developed here,” he said. SVS will post branding messages at the national level. But the lasting impact will come from the grassroots, said Slaw. “There is nothing the SVS can do that will be more powerful than individual members going out locally using the tools to get our message out.”
Additionally, Shutze has customized the fliers and begun doing some selected targeting. “For this to be as impactful as it can be, there’s going to have to be widespread adoption by the members,” he said. “We need to flood the workplace with these branding messages. That’s how branding works.”
He’s also interested to see how other SVS members use the tools. “I’m eager to see the creative ideas they come up with,” he said.
Fliers covering more vascular conditions will be added. SVS and Springboard will begin targeting consumers, “raising awareness of what we really do,” said Joseph Mills, MD, who leads the SVS effort. Following that initiative will be a campaign aimed at medical students and residents.
Another effort will target CEOs and hospital administrators. “Most of the public fails to realize how much we do,” said Mills of how vascular surgeons add expertise in OBGYN, urology and trauma cases, among other specialties. “They don’t realize how much support we provide.”
For more information, visit vsweb.org/Branding. For login help email membership@ vascularsociety.org.
William Shutze
Family history risk of AAA increases incrementally based on degree of relation, study finds
BY BRYAN KAY
There is an incremental increase in the risk of an abdominal aortic aneurysm (AAA) among those with a family history of the disorder based on degree of relation—with a significantly higher risk found in patients who have a first-degree relative with an AAA.
THE FINDINGS WERE DELIVERED during a scientific session at the Western Vascular Society (WVS) virtual annual meeting (Sept. 27–29), covering familial risk of AAA and the implications for population screening, by Claire Griffin, MD, an assistant professor of vascular surgery at the University of Utah in Salt Lake City. AAAs are the 13th leading cause of death in the U.S., with a prevalence of 4–8%, Griffin observed. Current U.S. Preventative Services Task Force (USPSTF) guidelines recommend a one-time abdominal ultrasound to screen for AAAs in men
College of Physicians, both of which do the majority of screening in patients,” she said during her talk. “The 2009 Society for Vascular Surgery (SVS) practice guidelines did recommend screening in patients with a history of AAA in their family but this has not been widely practiced.”
AAAs derived from
UTAH
aged 65–75 who have ever smoked, with the main risk factors for AAA being male sex, a history of smoking and family history. However, no screening is recommended for women who have smoked, and there are no specific screening recommendations from the USPSTF for a family history of AAA, she said. “The USPSTF screening guidelines are adopted by both the American Academy of Family Physicians and the American
Population Database:
Griffin and colleagues at the University of Utah hypothesized that the Utah Population Database—which she described as a unique resource with extensive relevant data—could provide “a robust and relative patient cohort to answer the true familial risk of AAA in a low tobacco use environment.”
250,000 cases (after exclusions) and 2.8 million controls
All patients in the database with a diagnosis of AAA were included and matched with 10 age and sex controls. After exclusions, almost 250,000 cases and their relatives were matched to 2.8 million controls. “A fixed effects model was used including the co-factors of time to diagnosis, type of relative, sex of relative, ethnicity and birth cohorts as non-
Preoperative risk score tool for rAAA 30-day mortality is accurate, new study finds
BY BRYAN KAY
An entirely preoperative risk-scoring tool for the prediction of 30-day mortality after a ruptured aortic abdominal aneurysm (rAAA) was found to be accurate after a retrospective review of a prospectively collected database at Harborview Medical Center in Seattle.
THE CALCULATOR HAS PROVEN TO be a valuable aid in preoperative counseling and in decision-making over transfers for treatment, which represented the majority of the patients studied by a University of Washington (UW) research team. The results were delivered during the Western Vascular Society (WVS) virtual annual meeting (Sept. 27–29).
In addition, the study’s findings have been confirmed at a number of other institutions, UW vascular surgery resident and first-named author Jake Hemingway, MD, told attendees.
The high morbidity and mortality associated with rAAAs means a significant mobilization of both prehospital and in-hospital resources are oftentimes
necessary, he said. Though various risk-scoring tools have been created, their reproducibility and effectiveness vary, with some overly complex and not practical for use, Hemingway continued. “Others rely on intraoperative and postoperative variables that are entirely worthless to the patient prior to the operation. And some of them are simply not accurate outside of the initial study that created them.”
The Harborview risk score, first published in the Journal of Vascular Surgery (JVS) in 2018, is entirely preoperative. The original publication of the score (range: 1–4) found a 30-day mortality of 22% if patients had 1 point through 100% mortality if all four factors were present. In the latest study, the investigators hypothesized that despite advancements in endovascular methods and improved mortality after rAAA repair, the score would remain accurate.
They included all patients who presented to the institution with a rAAA from January 2002–December 2018. They were divided into three cohorts: those patients who belonged to the pre-endovascular aneurysm repair (EVAR) era (January 2002–July 2007), the pre-risk score use era (August 2007–October 2013), and the modern era (November 2013–December 2018). The risk score itself is based on the data gathered from the first two cohorts. During the period studied, 417 patients were treated for rAAAs, with 391 undergoing an operation: 133, 152 and 106 from cohorts one, two and three, respectively. “On univariate analysis, we see that open surgical repair is associated with an increased risk of 30-day mortality (odds ratio [OR] 2.8, 95% confidence interval [CI] 1.80–4.40; p<0.0001), and being repaired in a later cohort— either two or three as compared to one—is associated with a decreased risk of mortality,” Hemingway said.
interacting terms, and an interaction model between relative type, age group and sex of relative,” Griffin explained.
The researchers found that the risk of AAA diagnosis increased in an incremental fashion based on degree of relation to the case, with a hazard ratio (HR) of 3.02 for first-degree relatives (95% confidence interval [CI], 2.75–3.31; p<0.001), 1.60 for second-degree relatives (95% CI, 1.42–1.72; p<0.001), and 1.33 for first cousins (95% CI, 1.26–1.42; p<0.001). They also found the age at diagnosis was “noticeably earlier” in the cases and relatives compared to control groups, with a HR of 8.3 (p=0.03) for those aged 0–33 and 4.65 for 55–64 (p<0.001).
Concluding, Griffin told the meeting: “There’s a significantly higher risk of AAA in patients with a first-degree relative with a diagnosis of AAA, and age at diagnosis is often younger than current widespread screening guidelines recommend. This lends further weight to the SVS practice guidelines from 2009, and can hopefully be used to push for more widespread adoption of screening in patients—both male and female—with a positive first-degree-relative family history, even in the absence of a history of smoking.”
“Regarding the risk score, we see that not only is each individual component associated with increased 30-day mortality, but so too is the Harborview risk score as a whole (p<0.0001). Other variables associated with an increased 30-day mortality include heart rate greater than 110 and INR [international normalized ratio] over 1.8.”
The investigators found that over time a higher proportion of repairs were carried out using an endovascular approach; there was a slight decrease in risk score for both open and endovascular patients; there was no difference in risk score between the two groups across all three cohorts; and 30-day mortality decreased from 58.6% in cohort one down to 35% in both two and three.
“This is driven both by an increased adoption of endovascular techniques but also by a decrease in the mortality of open repair, which decreased by 58.7% to 40% in cohort three,” Hemingway said. “When we look specifically at the risk score within the modern cohort, we see that when we look at all patients combined, as well as by repair type, that an increase in a Harborview risk score is associated with an increased 30-day mortality [combined (p<0.0001), open repair (p<0.0003) and EVAR (P<0.0001)].”
“Following the institution of an EVAR-first approach, mortality dropped from 58% to 35%”—Jake Hemingway
The research team concluded that the Harborview risk score is accurate among the modern patients studied.
Hemingway said: “This represents the largest singleinstitution experience with rAAA in which we saw over triple the odds of 30-day mortality following open surgical repair compared with EVAR.
“We also saw that following the institution of an EVAR-first approach, mortality dropped from 58% to 35%, which is likely a reflection of both increased adoption of endovascular techniques but also due to improved mortality following open AAA repair.”
Study identifies new genetic factors associated with AAA risk
BY JOCELYN HUDSON
The American Heart Association (AHA) recently announced the publication of a study identifying 14 new genes linked to an increased risk of abdominal aortic aneurysm (AAA).
PREVIOUS STUDIES HAVE DETECTED 10 locations in the human genome associated with potential AAA risk. But this new work, published in the AHA’s journal Circulation, more than doubled that number to a total of 24 genetic factors associated with AAAs.
“This new information can enhance screening protocols and help identify individuals at risk for abdominal aortic aneurysm,” one of the study’s authors, Philip S. Tsao, PhD, of Stanford University School of Medicine and
the Veterans Affairs (VA) Palo Alto Health Care System, California, said in a news release.
According to the AHA, the study used the world’s largest genetic biobank, the Million Veteran Program, which was created in 2011 to study how genes affect the health of U.S. military veterans. Researchers tested about 18 million DNA sequence variants among more than 7,500 AAA cases and 172,000 veterans who did not have the condition.
The work factored in the effects of blood pressure, finding that a genetic predisposition for an increase of 10mmHg in diastolic blood pressure increased the risk. “We were surprised that diastolic blood pressure, as opposed to systolic blood pressure, is likely of greater significance in the development of abdominal aortic aneurysm,” Tsao said.
The data also showed that 19 of the 24 genetic risk variants for the condition pointed to an increased risk for aneurysms in other parts of the body.
Researchers created a “polygenic risk score” that helped identify groups of people more likely to develop AAAs, regardless of known risk factors such as smoking and family history. The authors said the report is limited because the database primarily includes veterans of European ancestry. They suggest that as genetic technology advances, research includes more samples from people with diverse backgrounds to limit the chance of ethnic disparities in precision medicine.
‘Fundamental differences’ in patient outcomes after open
AAA detected across three national registries
BY BRYAN KAY
An investigation of differences in patient outcomes following open repair of abdominal aortic aneurysms (AAAs) found in three national registries showed that mortality rates were lower for those contained in the Vascular Quality Initiative (VQI).
Researchers at Brigham and Women’s Hospital in Boston discovered “fundamental differences” between patient profiles, payer mix and outcomes in the databases—differences that persist “despite adjusting for these patient factors.”
The findings, presented during a rapidfire session at the New England Society for Vascular Surgery (NESVS) virtual annual meeting (Sept. 11–12), were derived from a comparative analysis of open AAA repair outcomes across the three registries.
Large national databases are increasingly used to monitor adherence to quality benchmarks of care, presenter Rebecca E. Scully, MD, a vascular and endovascular surgery fellow at the institution, told the meeting. “However, wide variability has been previously demonstrated between various datasets.”
Using open AAA repair as a model, Scully et al identified individuals undergoing the procedure electively from 2013–2016 in the VQI, the American College of Surgeons National Surgical Quality Improvement Program (ACS
NSQIP), and the National Inpatient Sample (NIS), a large publicly available all-payer inpatient database.
Key among their findings, Scully and colleagues discovered, were data related to mortality, which she said “varied significantly between groups.” They found in-hospital mortality of 3.3% in the VQI, 4.5% in NSQIP and 5.5% in NIS—differences that persisted at 30 days with 5% for NSQIP and 3.5% for the VQI. Meanwhile, she noted, the VQI was the only dataset that reported 90-day mortality, found to be 4.8%.
When adjusting for age, gender, race and comorbidities, the odds of inpatient mortality remained “significantly different,” with the higher odds reported among patients in the NIS and NSQIP datasets (NSQIP vs. VQI: odds ratio [OR] 1.5, 95% confidence interval [CI] 1.2–1.9; p=0.001. NIS vs. VQI: OR 1.8, 95% CI, 1.4–2.4; p<0.001), Scully said.
As well as mortality, the research team also looked at length of stay and discharge disposition outcomes. In terms of baseline statistics, Scully reported significant
18 million DNA sequence variants tested among:
more than 7,500 AAA cases and 172,000 military veterans
differences in race distribution and primary insurer, with individuals in NIS more likely to have Medicare compared to the VQI. Additionally, the same was true of comorbidities across the three datasets, she said. “We captured procedure-specific variables; however, availability of these data was limited primarily to the VQI, and serves to highlight that specific procedure data was not available in the NIS or NSQIP, including approach or clamp position,” Scully noted. Length of stay varied from slightly over nine days in the VQI to 10-and-a-half days for patients captured in NSQIP (p=0.003).
Disposition at discharge also varied between groups, with 76% of patients sent home in the VQI to 73% in NIS and NSQIP (p<0.001).
Concluding, Scully said the differences their analysis detected may reflect the varying choices
questions from session moderators
presentation.
Dardik asked whether the better results shown in the VQI indicated more vascular surgeons using the database. “Part of it is NIS is a completely administrative dataset, and the VQI and NSQIP are QI databases, so we decided to focus on inpatient mortality as a pretty binary outcome,” Scully answered. “Part of it is differences between the two populations, within the populations captured in the NIS and captured in the VQI and NSQIP, and I think part of it is differences in institutions who have elected to be part of the VQI compared to NIS, which is a national sample.”
Shaw wondered whether the research suggested a need for one unified database, adding that the VQI seemed
“It has expanded and continues to expand. Participation in QI registries like VQI that capture more granular data would I think allow for—based on these data potentially—better care to be delivered to patients”—Rebecca E. Scully
made by institutions over which quality improvement (QI) registries they participate in.
“It’s crucial to take this into account when discussing policy decisions and national guidelines based on these data repositories.” Scully went further after
more complete. “It has expanded and continues to expand,” Scully responded. “Participation in QI registries like the VQI that capture more granular data would I think allow for—based on these data— potentially better care to be delivered to patients.”
Alan Dardik, MD, and Palma Shaw, MD, at the end of her
‘Nearly nothing’ in surgery will go untouched by AI in the
future, ACS Clinical Congress hears
BY BRYAN KAY
Almost nothing will go untouched by artificial intelligence (AI) in healthcare and surgery, notably in the quickly evolving world of vascular and endovascular surgery, Elsie Gyang Ross, MD, told the American College of Surgeons (ACS) Clinical Congress (Oct. 3–7), which was held virtually.
THE ASSISTANT PROFESSOR OF vascular surgery and research scientist with a focus on machine learning at Stanford University Medical Center in Stanford, California, was delivering a presentation on the current state of surgical AI in which she outlined the solutions either currently available or on the horizon across pre- intra- and postoperative care.
Ross ran through applications in radiology, pathology and vascular surgery; across intraoperative imaging and bleeding, robotic surgery, and postoperative acute care; as well as palliative care.
Though many solutions remain unavailable, she said, the application of AI in healthcare is accelerating.
“Currently, there are limited applications of AI for the surgical patient when we’re looking purely at clinically available commercial solutions,” Ross told the ACS Clinical Congress. “[But] many new applications are on the horizon, making this a very exciting time in the development phase of surgical AI.”
Ross defines AI as the application of mathematical algorithms toward automated problem-solving. “You can call the algorithms any number of things, such as learning algorithms—as a matter of fact a logistic regression can be applied toward automated problem solving, and this system can be considered AI as well—but the idea is you’re using some mathematical tool to automate a decision or process.”
In healthcare, that can mean minimalto-no automation, to partial automation such as assistive surgery, all the way to fully automated surgery. Machine learning algorithms put to work include supervised learning, unsupervised learning and deep learning, Ross explained.
At present, the field is in the process of figuring out “how to augment the abilities of humans who are doing the day-to-day work of taking care of patients,” she said.
Radiology has seen the most progress in use and application of AI, Ross went on, giving the example of a collaboration between the University of San Francisco and GE Healthcare to address lags in X-ray reads during critical time windows as a case in point. They developed AI software that can “identify pneumothorax on a chest X-ray and alert the technologists and radiologists, and bring the X-ray up the queue so that it’s read much quicker than it normally would be.” This solution gained Food and Drug Administration (FDA) clearance in 2019, she added.
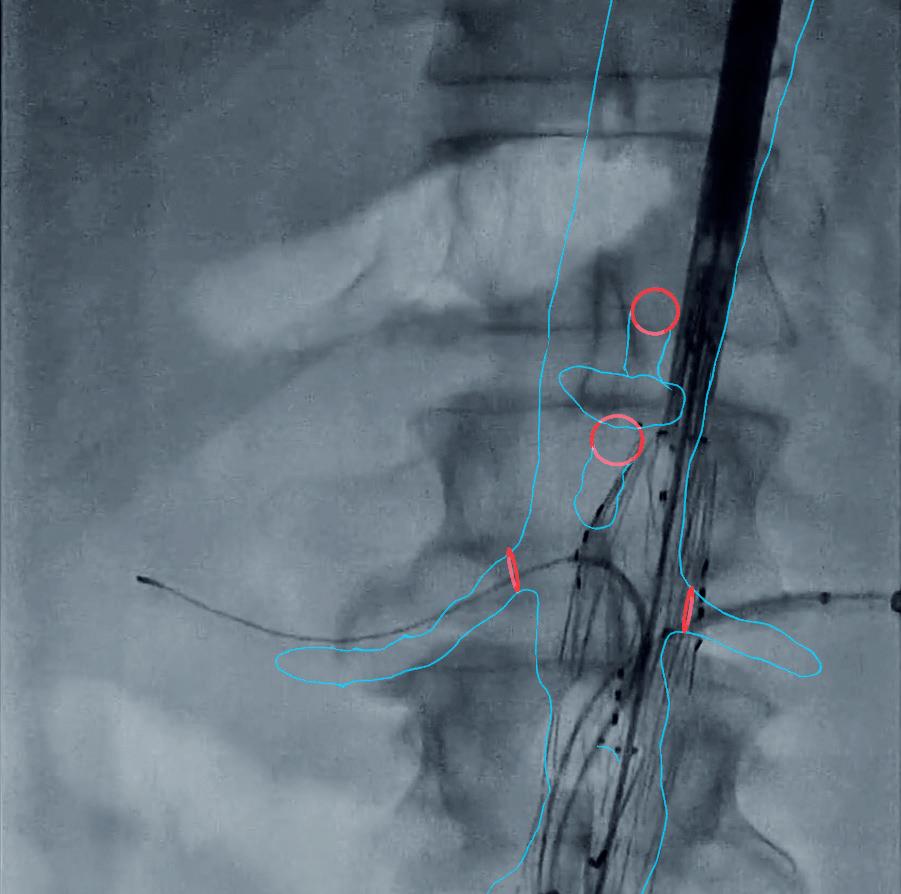
“The field of vascular surgery and the endovascular repair of abdominal aortic aneurysms has been quickly evolving.
As we’ve been able to fix more complex aneurysms, we’ve needed intraoperative assistance for the proper placement of stent grafts,” Ross continued.
One example includes a Cydar Medical AI solution to model how vessels move and are deflected by the introduction of different wires and instruments, she said.
“Preliminarily, use of this technology has been found to decrease important metrics for vascular surgeons, such as radiation exposure, fluoroscopy time and procedure times.”
Elsewhere, in the sphere of intraoperative bleeding AI technology has been employed to quantify blood loss based on the soilage from lap pads.
“And at least in the obstetrics literature, this solution has been preliminarily shown to improve time to identifying hemorrhage, leading to a reduction in delays in intervention,” Ross told the ACS gathering.
“And while we can talk all day about robotic surgery and AI,” she said, “I want to highlight that not only are AI solutions being developed for robots, but there is robotic hardware now being developed in synergy with AI software. In Microsure’s case, they have developed the world’s first microsurgery robot with software and
hardware that can stabilize a surgeon’s movements to allow for more precision across a broader spectrum of surgeon’s skill. In recent reports, this technology platform has been used to successfully perform lymphatic surgery.”
Applications in postoperative acute care is another important area where AI can lead to improved patient outcomes once solutions become commercially available, Ross went on.
“Though computer vision is often discussed for intraoperative possibilities, recent work shows that computer vision will play a big role in postoperative care as well,” she said.
Researchers at Stanford demonstrated that depth cameras placed in intensive care units (ICUs) were able to accurately quantify patient mobility in the ICU.
“That can be extremely important in recovery,” Ross continued. “Their AI model could also decently identify how many personnel were required to enable such patient movement. We currently have multiple more cameras going up in our ICUs that will use depth and heat mapping amongst other capabilities to monitor ICU care and recovery.”
Lastly, Ross touched on AI and palliative care.
“Applying deep learning algorithms to the task of identifying which patients will die within three to 12 months can provide pretty accurate results”— Elsie Gyang Ross
“As surgeons, we’d love it if we could save everyone, but, in reality, we do have to make difficult decisions about individual patients,” she said. “We’re so close to these decisions sometimes it can be hard to see the patient holistically or in busy practices it can be difficult to make these assessments as well. Even though it sounds counterintuitive, computational algorithms can help. Applying deep learning algorithms to the task of identifying which patients will die within three to 12 months can provide pretty accurate results. We currently have such a model running here at Stanford, which helps our palliative care teams prioritize patients to see and consult once they have permission from treatment teams. This is all to say nearly nothing will go untouched in the AI world in the future.”
For those perhaps wary of a complete machine takeover, Ross had some words of solace. “If you take nothing else away from this talk, based off the current state of AI, surgeons still have great job security,” she quipped as she concluded.
Elsie Gyang Ross
Cydar Medical's AI solution, which models vessel movement
NYC study shows 50% limb salvage rate in COVID-19 patients with ALI during pandemic peak
BY BRYAN KAY
Data gathered from patients presenting with acute limb ischemia (ALI) during the peak of the COVID-19 pandemic at the heart of New York City—a U.S. epicenter—demonstrated a 50% rate of limb salvage as well as a 70% 30-day mortality rate, with 20% of that number among patients in whom revascularization was attempted.
The research was conducted by investigators at New York-Presbyterian Queens hospital, and delivered by Vina Chhaya, MD, a resident at the institution, during a recent session of the ongoing Eastern Vascular Society 2020 Virtual Meeting (Oct. 7–Nov. 18), a digital replacement for its annual gathering.
The research team was seeking to document its experience with revascularization related to ALI among COVID-19-positive patients across a 10-week period spanning March–May, the height of the Big Apple’s epidemic.
Chhaya explained: “The virus has systemic effects, including a disseminated intravascular coagulopathy associated with increased mortality risk. The exact pathology of this hypercoagulability is not completely elucidated, but proposed mechanisms include properties of the virus itself, a sepsis-mediated activation of the complement cascade, endothelial dysfunction, and antiphospholipid syndrome, as the virus induces the development of reactive antiphospholipid antibodies, predisposing patients to hypercoagulability.
“Data published to date focusing on hypercoagulabilityinduced acute limb ischemia from Covid-19 is primarily from Italy and consists of single-center cohorts of around 20 patients,” she said. “Notably, the Italian experience highlights the significant increase of acute limb ischemia in COVID patients but also demonstrates favorable revascularization and survival-to-discharge outcomes. Given the associated dynamic coagulopathy, D-dimer has also emerged as a marker of thromboembolism that guides surveillance and timing of initiation of anti-coagulation.”
the city was fighting the coronavirus during the peak. Queens county itself recorded 71,000 cases and more than 6,000 deaths, Chhaya noted. Resources, she said,
“The virus has systemic effects, including a disseminated intravascular coagulopathy associated with increased mortality risk”—Vina Chhaya
we examined vasopressor use, the maximal level of respiratory support utilized during hospitalization, and functional status as documented in the patient chart,” explained Chhaya. “Surprisingly, the majority of our cohort did not require vasopressors, and 70% of patients used noninvasive positive pressure ventilation, with only two patients requiring intubation.”
Variables included body mass index (BMI), age and GOFAR score, a metric that predicts survival to discharge with good outcome following in-hospital cardiac arrest or attempted resuscitation. “This score was used as a guide by our palliative care teams during the pandemic to have an objective measure for all critically-ill patients, and we included it in our dataset.”
Results showed that GOFAR scores appeared to be higher among the mortalities (mean: 27.6, 95% confidence interval [CI] 16.9–38.4) and lower for those who received interventions (mean: 14.8, 95% CI -1.52–31.2). D-dimer levels were noted to be elevated for the entire cohort (mean: 5,424ng/ml, 95% CI 1,199–9,648) and higher among the death subset (mean: 6,674, 95% CI -2,401–15,751). “Only three in our cohort had values less than 1,500ng/ml,” she said.
Among the intervention subset, the majority of the occlusion sites were in the lower extremity, with three in the infrapopliteal region. One patient received a bilateral below-the-knee amputation. Four of the five had Rutherford classification 2B or 3 ALI, two re-occluded and one patient died. Of those who re-occluded or died, all had Rutherford classification 2B or 3. Of the death subset, only one received a revascularization, with 80% of occlusions proximal, and all either Rutherford 2B or 3. Among this group, the survival-to-discharge probability as calculated by the GOFAR score was less than 3%.
New York-Presbyterian Queens is an academiccommunity hybrid hospital located at the heart of where
CDC codifies CLI, CLTI in ICD-10-CM
BY BRYAN KAY
The Centers for Disease Control and Prevention (CDC) has approved a proposal to distinctly recognize critical limb ischemia (CLI) and critical limbthreatening ischemia (CLTI) in the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM).
A COALITION ORGANIZED BY THE CLI Global Society worked in close
were limited and placed “tremendous strain” on the area’s healthcare system. The study, based on a retrospective short review, scrutinized an institution with 535 beds, 2,232 COVID-19 patients, and 577 deaths. Some 14 cases of ALI were diagnosed, 10 of them among those with COVID-19—which, Chhaya speculates, was likely an underestimate given “the severe critical illness and deaths resulting from hypoxic respiratory failure as well as patients with chronic peripheral arterial disease avoiding the hospital at this time.”
Of the 10, 60% were Caucasian or Hispanic, seven were male, all were over the age of 50, and the main comorbidities recorded were hypertension and diabetes. The 10-patient cohort was further broken down into two subsets: interventions (n=5) and deaths (n=5).
“To understand how critically ill our 10 patients were,
partnership with the vascular specialist community to develop the proposal, and involved the society’s own Robert A. Lookstein, MD, and Barry T. Katzen, MD. Other members included Sean Roddy, MD, of the Society for Vascular Surgery (SVS), Mitchell Weinberg, MD, of the Society for Vascular Medicine, Bulent Arslan, MD, of the Society of Interventional Radiology, and Mehdi Shishehbor, DO, of the Society for Cardiovascular Angiography and Intervention (SCAI).
The ICD-10-CM is a worldwide standard reference set of disease codes used to report medical services provided to patients. The announcement is being hailed as a major step forward in tracking patient treatments and outcomes for CLI and CLTI, which affect millions of patients around the world.
The goal of this initiative is to support coding professionals, educators, compliance staff and physicians to identify
Concluding, Chhaya said: “Overall, our data show a 50% limb salvage rate and a 70% 30-day mortality rate, with 20% among those patients receiving intervention. Despite our resource limitations during the peak of the pandemic, our team managed to perform a total of nine revascularization interventions, with four of those in COVID-positive patients initially presenting as Rutherford 2B or 3 ALI.”
She added: “Our data also support what has already been published, namely that D-dimer levels are higher in COVID-positive patients and especially so in those with acute limb ischemia as our cohort had a mean of over 5,000ng/ml. Finally, our high rates of morbidity and mortality are secondary to severe inflammatory response dates, leading to hypercoagulability as well as the critical illness seen in COVID-19 patients.”
and accurately report CLI and CLTI in clinical documentation, electronic medical records and medical billing in order to track and monitor patient treatments and outcomes in the future. “This effort is a first step in building awareness of the
“These dedicated codes are critical in our goal to improve quality of life by preventing amputations and death due to CLI”— Barry T. Katzen
complexity associated with caring for patients who suffer from CLI within public and commercial payers and the broader healthcare community,” said Katzen, board chair of the CLI Global Society, which was formed to help improve quality of life by preventing amputations and death due to CLI. “These dedicated codes, now newly identified for CLI, are critical in our goal to improve quality of life by preventing amputations and death due to CLI.”
Lookstein, chair of the Vascular Societies Workgroup and CLI Global Society board member, said: “[We] look forward to continued partnership as we launch initiatives to educate our membership, our hospitals and healthcare provider staff regarding these changes,” Lookstein explained. “They have the potential to positively impact the care we provide to these extremely vulnerable patients across the United States and around the world.”
DCBs lead to reduced mortality, amputation through four years after femoropopliteal revascularization, new analysis finds
BY BRYAN KAY
Patients treated with a paclitaxel-coated balloon saw greater survival, freedom from amputation and amputation-free survival through four-year follow-up after their initial femoropopliteal revascularization operation than those who received treatment using an uncoated device, researchers behind a propensitymatched retrospective review at University Hospitals Cleveland Medical Center, Ohio found.
THE STUDY FURTHER SHOWED that freedom from target-lesion revascularization was higher in paclitaxel patients through three-year follow-up. These latest findings, presented by Alexander H. King, MS, of UH Cleveland’s division of vascular surgery and endovascular therapy, emerged during a session on peripheral arterial disease (PAD) at the Eastern Vascular Society (EVS) virtual annual meeting (Oct. 7–Nov. 18). They relate to previous data showing that the IN.PACT Admiral DCB had a
significant advantage in overall survival, amputation-free survival and targetlesion revascularization (TLR) after femoropopliteal artery treatment through four-year follow-up when compared to uncoated balloons in a head-tohead comparison between two discrete paclitaxel-coated devices, delivered a month previously at the Midwestern Vascular Surgical Society (MVSS) virtual annual meeting (Sept. 9–12). King et al told the MVSS gathering that the other DCB studied, the Lutonix (BD Bard), showed
Vascular surgeons encouraged to consult paclitaxel talking points document
BY BRYAN KAY
Vascular surgeons are being encouraged to take consideration of a set of talking points about the risks and benefits of paclitaxel-equipped devices—developed by a multispecialty panel of medical societies—in discussions with their patients.
The document is the work of the Multi-Specialty and Multi-Society Coalition for Patient Safety With Paclitaxel Technologies, which includes three leading vascular surgical membership bodies: the Society for Vascular Surgery (SVS), the Vascular and Endovascular Surgery Society (VESS) and the Society for Clinical Vascular Surgery (SCVS).
The Food and Drug Administration (FDA) tasked the coalition with putting together bullet points that reflect the current evidence around the hot button topic of paclitaxel devices.
On the SVS side, Jens Eldrup-Jorgensen, MD, and Daniel Bertges, MD, were involved in the discussions that led to the finished document. They were joined by James Black, MD, from VESS as well as Jean Bismuth, MD, from the SCVS.
The American College of Cardiology, the American
a less clear advantage in major outcomes compared to uncoated balloons.
At EVS, King elaborated on the research team’s single institution study of 1,419 femoropopliteal revascularization patients (treated from 2010–2019) as it pertained to four-year outcomes between those who received angioplasty with paclitaxel (using either the IN.PACT Admiral or the Lutonix) versus those treated via the same procedure without the drug (n=830 vs. 594).
The investigators compared the four-year outcome measures of all-cause mortality, freedom from major amputation, amputationfree survival and TLR. After propensity matching, the two cohorts each contained 529 patients. They found four-year survival rates were superior in the paclitaxel group at 62.1% compared to 51.8% with a plain balloon (p=0.04). On multivariate analysis age, critical limb-threatening ischemia (CLTI), chronic kidney disease (CKD), hyperlipidemia, diabetes and chronic obstructive pulmonary disease (COPD) were all associated with mortality through four years. “Importantly, paclitaxel use
4year
was not a significant factor on multivariate analysis,” observed King. Freedom from major amputation rates were 91.3% among the patients treated with a paclitaxel-coated device and 85.5% in those undergoing a revascularization procedure with an uncoated balloon. Factors related to increased risk of amputation were CLTI and CKD, King explained, and paclitaxel use was a protective factor against amputation (hazard ratio [HR] 0.53; p=0.003).
survival rates superior in paclitaxel group at 62.1% compared to 51.8% with a plain balloon (p=0.04)
As for amputation-free survival, “there was a clear benefit for patients treated with paclitaxel” with a rate of 59.3% vs. 46.4% in the uncoated device group, he said. On multivariate analysis, paclitaxel was identified as protective (HR: 0.72; p=0.002). And while TLR rates at four years were similar between the two groups (paclitaxel: 73.6%; uncoated: 71%), “paclitaxel patients had a similar advantage at one, two and three years after the initial operation.” King added that further prospective studies are warranted to identify possible factors associated with the discrepancy between clinical trial and population-based data.
College of Radiology, the American Heart Association, the Society for Cardiovascular Angiography and Interventions, the Society for Vascular Medicine and the Society of Interventional Radiology make up the remainder of the membership bodies that are represented in the coalition.
“The coalition bullet points reflect the current evidence surrounding this complex topic and is designed to help institutions and members when discussing the increased rate of long-term mortality in patients treated with paclitaxel-coated balloons and paclitaxel-eluting stents,” the coalition said.
“The statements are intended to summarize the current state of the evidence and to serve as starting points for discussion. We recognize this is a complex issue and the talking points and are not intended to take the place of thoughtful, individualized discussions with patients. “The ability to effectively communicate risk and benefit of revascularization is a key part of procedure selection. Please consider the following statement in your discussions and informed consent process.”
The Multi-Specialty and Multi-Society Coalition for Patient Safety With Paclitaxel Technologies document follows in full.
Peripheral vascular intervention talking points for informing patients about the paclitaxel safety signal
A recent meta-analysis of randomized trials suggests an increased mortality rate after two years in peripheral artery disease (PAD) patients treated with paclitaxelcoated balloons and paclitaxel-eluting stents for femoropopliteal disease compared to patients treated with uncoated balloons or bare metal stents.
The FDA recommends that physicians discuss the risks and benefits of all available treatment options with their PAD patients.
To this end, a Multi-Specialty Paclitaxel Coalition (American College of Cardiology, American College
of Radiology, American Heart Association, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine, Society of Interventional Radiology, Society for Vascular Surgery, Vascular and Endovascular Surgery Society, and the Society for Clinical Vascular Surgery), representing the majority of specialists who evaluate and treat patients with PAD, developed the following talking points, which have been reviewed by the FDA, that physicians/providers may consider when discussing PAD treatment options with their patients:
n Some balloons and stents used to treat symptoms resulting from blocked blood vessels in leg(s) are coated with the drug paclitaxel
n Research studies show that paclitaxel-coated balloons and stents improve the chance that the treated blood vessel in your leg will remain open after your treatment and lower the likelihood that you will need a repeat procedure to re-open the vessel
n However, an analysis in 2019 that combined the results from multiple studies indicated that the use of paclitaxel-coated balloons and stents may increase your chance of dying starting about 2 years after treatment. Although this analysis has limitations and further research is still ongoing, the available information as of April 2020 suggests that paclitaxelcoated device use may increase your chance of dying over the next 2–5 years compared to treatment with uncoated balloons or bare metal stents
n There may be other options for the treatment of your symptoms, including medications, exercise, balloons, stents or other devices that do not contain paclitaxel, and surgery. You and your doctor should discuss the possible risks and benefits of all treatments to identify those options that are best for you
The Multi-Specialty Paclitaxel Coalition is actively working with the FDA, medical device manufacturers, and clinical investigators to advance our understanding of the long-term safety and effectiveness of paclitaxelcoated devices.
TCT 2020 latebreaking trials session features new data on drug-coated devices
BY JOCELYN HUDSON AND SUZIE MARSHALL
Findings from a series of late-breaking trials in the endovascular field were delivered recently at TCT Connect (Oct. 14–18), the 32nd annual scientific symposium of the Cardiovascular Research Foundation (CRF), held virtually, with the first from Connie N. Hess, MD, of the University of Colorado in Aurora, featuring the results from a large subgroup analysis of the VOYAGER PAD randomized clinical trial.
The study showed neither a mortality risk nor benefit associated with the use of paclitaxel drug-coated devices in the treatment of peripheral arterial disease (PAD). The study also found that the benefit of rivaroxaban use on reducing ischemic limb and cardiovascular outcomes was consistent regardless of whether a drug-coated device was used.
Hess and team’s analysis examined the long-term safety of drug-coated devices (DCDs). It also evaluated whether rivaroxaban 2.5mg twice daily plus low dose aspirin versus low dose aspirin alone was consistent, either with or without use of a DCD.
During the qualifying endovascular lower extremity revascularization, DCD was used for 31% (n=1,358) of patients. Patients receiving DCD more frequently had prior endovascular lower extremity revascularization, had higher baseline use of dual antiplatelet therapy and statins, and were more often treated for claudication than non-DCD patients.
In the unweighted analysis, lower associated mortality was observed among patients receiving DCD versus non-DCD (2.9 vs. 3.9 per 100 patient-years; 3.5-year Kaplan-Meier cumulative incidence of 10.2% vs.13.8%). After weighting, there was no association between DCD use and mortality (3.5-year cumulative incidence 12.1% vs. 12.6%, HR 0.95, 95% CI 0.83–1.09, p=0.49). The benefit of rivaroxaban 2.5mg twice daily with aspirin compared to aspirin alone in reducing ischemic limb and cardiovascular outcomes was also consistent regardless of whether a DCD was used.
The VOYAGER PAD trial was funded by research grants to CPC Clinical Research from Bayer and Janssen.
IN.PACT 0.014 DCB
Antonio Micari, MD, University of Messina, Messina, Italy, presented firstever results from Medtronic’s IN.PACT BTK study, a feasibility study assessing the
safety and effectiveness of the company’s IN.PACT 0.014 drug-coated balloon (DCB) in critical limb ischemia (CLI) patients with chronic total occlusion (CTO) in the infrapopliteal arteries.
The IN.PACT BTK study is a prospective, multicenter, 1:1, randomized feasibility study assessing the safety and effectiveness of the IN.PACT 0.014 DCB, a 3.5μg/mm2 dose paclitaxel-coated balloon, versus conventional percutaneous transluminal angioplasty (PTA) for the treatment of CTOs in the infrapopliteal arteries. The study enrolled 50 patients at nine sites in Europe.
At nine months, patients in the DCB group experienced a reduction in sub-
“I think we are really starting to close the door on the paclitaxel controversy”—
Robert A. Lookstein
segmental late lumen loss compared to those in the PTA control group (0.59±0.94mm vs. 1.26±0.81mm, respectively, p=0.017), a 53% lower late lumen loss than the PTA control group. Using the classic late lumen loss method, subjects in the DCB group experienced lower late lumen loss compared to those in the PTA control group at nine months (0.89±0.77mm vs. 1.31±0.72mm respectively, p=0.07 ), a 32% lower late lumen loss than the PTA control group. Historically, there has not been a DCB technology that has demonstrated effectiveness in this vessel bed. According to a Medtronic press release, the data presented at TCT demonstrate that IN.PACT 0.014 may offer a clinical benefit in patients with CLI.
The IN.PACT 0.014 DCB is an investigational device that is being
evaluated in Europe, and is not currently being evaluated in the U.S.
ILLUMENATE Global
Andrew Holden, MBChB, of Auckland City Hospital, Auckland, New Zealand, reported on late safety and efficacy outcomes for the low-dose Stellarex DCB (Philips) in de novo and restenotic femoropopliteal lesions drawn from a large cohort of patients.
He revealed that four-year data from the trial show favorable safety and efficacy outcomes consistent with the ILLUMENATE randomized controlled trials, and also demonstrate similar efficacy in prespecified cohorts including different gender groups and diabetics.
ILLUMENATE Global is a prospective, single-arm, multicenter study conducted in the European Union. The patient population included those with Rutherford Clinical Classification (RCC) of 2–4 indicated for treatment of the superficial femoral artery (SFA) and/or popliteal artery for de novo or restenotic lesions. Follow-up office visits were at one, six, 12, 24, and 36-months post-procedure
and included clinical, hemodynamic, and functional outcomes. At four years, the rate of major target limb amputation was 0.8% and that of all-cause mortality was 8.1%. Clinically-driven target lesion revascularization through four years was 75.6% at day 1,460 and the subgroup analysis revealed no difference in prespecified cohorts. “The ILLUMENATE Global study supports durable long-term outcomes with the Stellarex DCB and is applicable to a complex population,” Holden told the TCT audience.
Paclitaxel controversy
“I think we are really starting to close the door on the paclitaxel controversy,” Robert A. Lookstein, MD, of Mount Sinai Health System in New York, part of the panel for the TCT late-breaking trials, commented at the end of the session. “There is clearly a lot more work that needs to be done for paclitaxel below the knee and it is encouraging to see that there is going to be work on that,” he added. “We are barely scratching the surface on drug-based delivery in the below-knee circulation, so there is a lot more work to do.”
SVS details opposition, support to CMS proposed rules
BY BETH BALES
The Society for Vascular Surgery (SVS) has submitted comment letters to the Centers for Medicare & Medicaid Services (CMS) on two proposed rules that directly affect SVS members: the Medicare Physician Fee Schedule and the Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems (HOPPS).
CMS ISSUED THE PROPOSED RULES in early August. They will be finalized on or around Dec. 1 and effective on Jan. 1, 2021. “The letters provide CMS with our
Society’s strong and detailed responses to each vascular policy point in the proposed rules,” said Matthew Sideman, MD, chair of the SVS Policy and Advocacy Council.
The proposed Physician Fee Schedule rule includes cuts that that would reduce total payments to vascular surgeons of 7%.
“These rules include cuts that will have a massive impact on vascular surgery practices for years to come,” said Sideman.
“We are fighting back with these letters, plus a partnership with 11 other surgical societies and with outreach to our own members to contact their legislators.”
The SVS letter also contains comments on the proposed rule for Quality Reporting Programs.
Physician Fee Schedule
The SVS strongly opposes the reduction in the conversion factors, from $36.09 this year to $32.26. This is lower than the 1994 factor, which would be approximately $58 in today’s dollars. This cut, paired with upcoming changes in the office/outpatient evaluation and management values in the global codes, could force surgeons who rely on providing care to Medicare patients to be unable to continue to practice.
SVS also opposes other details in the
proposed rule, including the E/M Inherent Complexity Add-on Code and CMS’s establishment in global services of a two-tiered system for evaluation and management services.
SVS offered detailed comments on toe amputation services, supply pricing and the technical expert panel related to practice expense.
The letter also addresses the Quality Payment Program, urging CMS to extend flexibility on the “extreme and
“These rules include cuts that will have a massive impact on vascular surgery practices for years to come”— Matthew Sideman
Healthcare on a precipice: SVS PAC stands ready to fight coming challenges
BY KRISHNA JAIN, MD, AND ALI IRSHAD, MD
Since 2002, the SVS Political Action Committee (PAC) has been a vehicle for advocacy specifically for vascular surgeons. As the only voice geared for vascular surgeons in Washington, D.C., it plays an instrumental role in championing pressing concerns that matter to the wider vascular surgery community.
So what exactly does the SVS PAC do? And more importantly, why should you care?
SVS PAC plays an integral role as a liaison for vascular surgeons when communicating with lawmakers on the Senate Finance, House Ways and Means, and the House Energy and Commerce committees, as well as the House and Senate Veterans Affairs Committee, and House and Senate leadership.
Aside from advocacy with various congressional committees, SVS PAC also supports congressional candidates whose positions on healthcare policies are aligned with SVS and our members. SVS support for candidates who share our views is a critical tool for achieving SVS legislative and regulatory priorities.
The PAC achieves this through monetary donations for congressional candidates—both incumbents and challengers—on a bipartisan basis.
Using a scorecard system, the committee identified members of Congress serving on congressional committees with jurisdiction over healthcare issues to cultivate for future support.
Each candidate was then evaluated on whether he or she co-sponsored or supported key SVS legislative and regulatory priorities. Visit vsweb.org/PACChart to download the scorecard.
The following legislative efforts were taken into
SVS support for candidates who share our views is a critical tool for achieving SVS legislative and regulatory priorities
uncontrollable circumstances hardship exception” through at least 2021, because of the COVID public health emergency and also agrees that CMS should delay the timeline for implementation of any Advanced Alternative Payment Models (AMPs) until at least 2022.
Other issues also are addressed. Read the complete letter at vsweb.org/21FeeSked
HOPPS
SVS opposed CMS’ proposal to eliminate the Inpatient Only list over the course of three years. Doing so will “increase patient copayments for many procedures while increasing patient risk.
In contrast, SVS does support an annual process whereby stakeholders nominate services for removal from the IPO list, and due consideration is given to patient safety and patient financial burden.”
The letter also addresses other topics, including changes to the Ambulatory Surgery Center list of covered surgical and dialysis vascular access payments. Read the complete letter at vsweb.org/21HOPPS
account in creating this scorecard, in order to hone efforts and support for politicians who advocate for patients and physicians alike:
■ Co-sponsorship of Improving Seniors’ Timely Access to Care Act of 2019 (HR 3107), legislation that reduces the burden and costs of prior authorization policies imposed by Medicare Advantage plans
■ Co-sponsorship of Resident Physician Shortage Act (HR 1763/S 348), legislation addressing the doctor shortage by adding 15,000 additional Medicare-supported residency slots over five years
■ Co-signing onto four separate congressional letters addressing the Medicare Physician Fee Schedule (MPFS) and the payment cuts to vascular surgeons in 2019 and 2020
It is through these systematic and exhaustive methods that SVS PAC gets results. In 2018 alone, we saved over $100 million in vascular ultrasound reimbursements due to successful Society advocacy supported by the political action committee.
At no time has the SVS PAC been more relevant than at this juncture. In this election year, U.S. health legislation and payment models are at a precipice. In the coming months there are proposed Medicare payment cuts ranging from 7–10%.
As we all know too well, if these cuts pass, private insurance companies will follow suit, ultimately leading to decreased payment for vascular surgery services all across the country.
This will undoubtedly affect all of us, regardless of practice patterns, geography or years in practice. The SVS PAC stands as the single strongest advocate against these myopic and unfair payment cuts. It is a proponent, not only of the member vascular surgeons but also the specialty itself and the utility it provides in health systems across the country.
The time is now! Donate to the SVS PAC today. Please go to www.svspac.org to make a contribution and to fight these cuts.
Krishna Jain and Ali Irshad are members of the SVS PAC Steering Committee.
Matthew Sideman
Correct billing in severe trauma cases can be complicated
BY THE SVS CODING COMMITTEE
The management of the severely injured trauma patient often requires delicate coordination among multiple specialties, and multiple separate operative procedures are often necessary. In particular, the clinical management of concomitant vascular and orthopedic injuries can be complicated. As a practical matter, correct billing is often a subject of debate.
HERE IS A CLINICAL EXAMPLE: A PATIENT presents in the emergency deparement after a motor vehicle collision with significant left-leg open fractures and active hemorrhage. He is taken to the operating room for exploration and repair. Vascular surgery is consulted and intra-operatively identifies the two ends of a nearly severed femoral artery, but, recognizing the complexity of repair and need for other services to provide timely definitive operative treatment, a temporary vascular shunt is placed. Because of the patient’s instability, the patient is transported to the intensive care unit (ICU) and resuscitated overnight. The following day, the patient’s leg is re-explored, the shunt is removed, and the artery is repaired with a vein patch angioplasty using contralateral autologous vein.
For the scenario described, the vascular surgeon provided two separate operative services. The first involves exposure, likely partial excision or debridement of the vessel wall, and the insertion of a shunt. The arterial exploration would be appropriately billed with
As a practical matter, correct billing is often a subject of debate
code 35703 (exploration not followed by surgical repair of artery: lower extremity). The placement of a shunt, which legitimately does require surgical manipulation of the artery proximal and distal to the injury, as well as temporary vascular control, does not have a separate CPT code. Moreover, the work of controlling arterial inflow and outflow, the proverbial “preparation of the artery,” is included in 35703.
For the second surgery, the artery is re-inspected and the definitive repair is performed. Proximal and distal control is obtained, the shunt is removed, and embolectomy catheters are passed proximally and distally to ensure patency. Embolectomy is not separately reportable in this instance as it is included in the code for definitive vessel repair. The contralateral saphenous vein is harvested, then fashioned into a patch and used to repair the artery definitively.
The most appropriate code is 35256 (repair blood vessel with vein graft lower extremity). Since the second staged procedure (35256) is performed in the global period of the initial procedure (35703), the modifier -58 would be appropriate (staged or related procedure or service by the same physician or other qualified healthcare professional during the postoperative period). In this instance, the placement of a shunt per se is not a billable event, but the remainder of the surgical maneuvers can be accurately represented by existing codes within the CPT nomenclature.
‘Smile’ to benefit SVS Foundation
The holidays are close upon us, and many Society for Vascular Surgery members will be shopping online this month and next.
The COVID pandemic has, in fact, prompted many people to do even more shopping online then before. Those who use the Amazon “Smile” website can not only purchase what they need but also benefit the SVS Foundation at the same time.
Simply start an Amazon shopping session at smile.amazon.com, with the SVS Foundation your designated charity. The Foundation will receive 0.5 percent of the cost of eligible purchases.
On your first visit, you will need to select the SVS Foundation as your charitable organization. The website will remember your selection. Remember, for the SVS Foundation to receive donations, you must start shopping on the “smile” site.—Beth Bales
In memoriam
Sunil Agarwal, MD, Feb. 2. Agarwal was professor and head of the department of vascular surgery, Christian Medical College, Vellore, India. Giancarlo Piano, MD, 63, of Chicago, Oct. 8, of COVID-19. He was a beloved vascular surgeon, teacher and mentor, and a fierce advocate for his patients.—Beth Bales
Virtual VRIC is here
Robert W. Gore dies at 83
Robert W. "Bob" Gore, PhD, the man behind expanded polytetrafluoroethylene (ePTFE) and chairman emeritus of the W.L. Gore & Associates board of directors, has died. He was 83.
A seasoned inventor and leader at the global materials science company behind a slew of medical devices, Gore passed peacefully at home following a long illness. His scientific discoveries spanned many other industries, including performance fabrics, space exploration and filtration.
Gore, a chemical engineer, took on the role of chairman emeritus role in 2018 after nearly 60 years on the Gore board, 30 as chairman. He also served as president of Gore from 1976 to 2000.
“Bob's commitment to research and development led to his 1969 discovery of a versatile new polymer form, expanded polytetrafluoroethylene (ePTFE),” Gore said in statement.
“The introduction of this groundbreaking new material opened a world of possibilities for products and further innovations.”
He is survived by wife Jane, a large family of children, grandchildren and great-grandchildren, and four siblings.—Bryan Kay
The 2020 Vascular Research Initiatives Conference is repurposed as a virtual event—and is coming to a screen near you this month.
Featuring two presentations, VRIC ONLINE 2020: From Discovery to Translation, will include the accepted oral presentations from the canceled conference as well as live question-and-answer periods. Times are 1 to 3 p.m. Central Standard Time Thursday, Nov. 5, and 7 to 9 p.m. CST Thursday, Nov. 12. Registration is free but mandatory. Visit vsweb.org/VRIC20 to register and for more information.
SVS president Ronald L. Dalman, MD, and Dr. Edith Tzeng, MD, chair of the Research Council, championed the idea to present Virtual VRIC, said Luke Brewster, MD, chair of the Basic and Translational Research Committee.
He pointed out that the committee “learned quite a bit about virtual meetings” from SVS ONLINE: “New Discoveries and Advances in Vascular Surgery” and two European sessions. “We’re pleased to bring forward these two modules to accommodate the outstanding science we had submitted to us.” Beth Bales
Membership information outlined
The end of 2020 brings deadlines for SVS membership application and payment of SVS dues.
Dues invoices have been distributed to all members via email and/or mail. Dues must be paid by Dec. 31 to maintain SVS membership and continue access to the Journal of Vascular Surgery (JVS), SVSConnect, the new Branding Toolkit and other benefits.
Graduated Candidates in Year 4: Transition to Active Membership: Graduated Candidates in year four of their “graduated candidate” membership must transition to Active membership. Only those who apply for such membership by Dec. 1 will continue to enjoy benefits without a lapse.
SVS has many new and thriving initiatives, including the just-debuted Branding Toolkit to help members promote their expertise with referring physicians, the active community on SVSConnect, wellness and leadership initiatives, a Mentor Match program and more. All are open only to SVS members.
Other additional benefits include access to the JVS peer-reviewed publications as well as a slew of clinical practice guidelines and reporting standards to facilitate exemplary patient care.—Beth Bales
Those who need hard-copy invoices may email membership@vascularsociety.org. Apply for Membership by Dec. 1: The final date this year to apply for membership is Dec. 1. The first application date for 2021 is March 1, 2021. Visit vsweb.org/Join.
Abstracts for VRIC, VAM 2021
Calling surgeons and scientists: Your research is wanted.
Submission sites are now open for two annual SVS meetings in 2021, the Vascular Research Initiatives Conference (VRIC) and the Vascular Annual Meeting (VAM).
The VRIC submission site will close Jan. 6, 2021. Conference details are still being worked out. Registration is expected to open in December. The VAM abstract submission site will open Monday, Nov. 16 and close at 3 p.m. Central Standard Time on Wednesday, Jan. 13, 2021.
Submission policies and guidelines are available at vsweb.org/Guidelines20. The meeting—which will celebrate the 75th anniversary of the Society—will be June 2 to 5 in San Diego. This year, scientific sessions will run, with educational sessions, across all four days.
Registration and housing will open in early March. The SVS continues to plan for an in-person meeting where members can learn from one another.—Beth Bales
New society
A new American Limb Preservation Society (ALPS) was launched during the recently concluded Diabetic Foot Conference (DFCon), held virtually this year from Oct. 9–10.
The organization aims to serve as an interdisciplinary bridge between patients and medical specialties, surgery, nursing, physical therapy, engineering and science for better care of the lower extremity.
SVS members in the news
Richard Lynn, MD, a vascular surgeon from Palm Beach, Florida, has been elected second vice-president-elect of the American College of Surgeons (ACS).
Alan Dardik (right), MD, of Yale University School of Medicine, New Haven, Connecticut, and Andres Schanzer, MD, of the University of Massachusetts Medical School, Worcester, are the new president and president-elect, respectively, of the New England Society for Vascular Surgery (NESVS).
S. Ahmed Hussain, MD, of Toledo, Ohio, a native of Pakistan who has lived in the United States for nearly 60 years, has written an autobiography entitled, “A Tapestry of Medicine and Life.”—Beth Bales
“Our collective goal is to eliminate preventable amputations over the next generation,” writes David G. Armstrong, MD, ALPS founding president and professor of clinical surgery at the University of Southern California, in his introduction to the group. For membership and other information, visit limbpreservationsociety.org.—Bryan Kay
Dig deep this Giving Tuesday
BY BETH BALES
Will you give on Giving Tuesday? This will be the SVS Foundation’s third year marking the annual global day of giving— Dec. 1, this year—which follows Thanksgiving and the big shopping days of Black Friday and Cyber Monday.
The day is set during the holiday season, when many people concentrate their charitable giving. With a very low-key start in 2018, with just $350 in contributions, donations picked up in 2019, with 20 donors contributing nearly $2,000. Hopes are high this year for about 2 ½ times that amount, said Peter Lawrence, MD, Foundation chair.
Here are some examples of how donations to the SVS Foundation—on any day of the year—are improving patient care: Through an SVS Foundation Community Awareness and Prevention Project grant, Leigh Ann O’Banion, MD, is helping amputees in the Fresno, California, area become ambulatory more quickly. The project, which has been interrupted by COVID-19, has so far been successful.
The Foundation grants of C. Keith Ozaki, MD, have helped him study the way blood vessels respond to physical force and the way food consumption prior to surgery
affects the response to surgical trauma.
Rural patients were able to “see” Misti Humphries, MD, via telemedicine because of an SVS Foundation Clinical Research Seed Grant. One of her thoracic outlet syndrome patients avoided a five-hour round trip but could still show the staff her progress, raising her arms up in triumph.
Omid Jazaeri, MD, spent a year visiting centers with advanced imaging and MR technologies. The ability to better understand aortopathies as they pertain to structure, stress and physiology of blood flow will help him treat his own patients more successfully.
“We simply can’t fix what we can’t see or understand,” he said. Hundreds of SVS members over the years have poured time and effort into studying diabetes, peripheral arterial disease (PAD), vascular remodeling, venous thrombus formation and other topics—all to treat or prevent vascular diseases or reduce their severity.
“My mantra is: ‘More money, more
mission,’” said Foundation chair Peter F. Lawrence, MD. “With more money, we can fund more grants, we can fund more science into the hows and whys of vascular disease, we can fund more community projects that educate the public about what vascular disease is and how we can help them. Please help the Foundation help others, by giving on Giving Tuesday.”
SVS Foundation Annual Report published
The Foundation’s 2020 Annual Report looks at the challenging year upended by the pandemic and its effect on vascular surgery, and then looks ahead to welcome 2021 in its just-published 2020 Annual.
“A Look Back, A Look Ahead” includes financial information as well as infrastructure changes to and expansion of the SVS Foundation Board of Directors. Showcased stories detail how lives of amputees and those in danger of amputation are benefiting from SVS Foundation Community Awareness and Prevention Project (CAPP) grants. Indeed, the SVS Foundation thanks all who share to make this impact possible.
The report also details deadlines for 2020–21 awards, the different Foundation funds and ways to give.
Read the report to learn how donor dollars impact patients health and wellbeing and vascular care, at vsweb.org/ FoundationReport20.
'Alea iacta est': The case for endovascular methods in vascular trauma care
BY BRYAN KAY
When Benjamin W. Starnes, MD, talks vascular trauma, he does so from a position of certain authority. As the recent Southern California Vascular Surgical Society (SCVSS) virtual annual meeting (Oct. 24–25) heard, few in modern practice can draw on the sort of experience possessed by the University of Washington (UW) chief of vascular surgery. In sum: 15 years out in the confines of military theater and another 13 back home on civvy street in the more salubrious environs of hospital operating theaters.
So his paean for the use of endovascular methods in the treatment of vascular injury, detailed in his SCVSS guest lecture, “Alea iacta est: Crossing the Rubicon in vascular trauma from battlefield to bedside,” carries considerable merit. In the context of endovascular treatment in vascular trauma care, those Latin words from Roman history, attributed to Julius Caesar after he defiantly crossed the Rubicon River, sparking civil war, are prescient. “[Caesar] famously announced, ‘Alea iacta est.’ The die is cast, we will no longer go back, and he changed the Roman Empire and the world forever,” Starnes told the meeting.
In terms of endovascular care in trauma, too, there’s
no turning back. For vascular injury’s Rubicon, read turn of the century. Around then, explained Starnes, there was a sea change. “There were improvements in imaging. It was now rapidly available and portable. There had been this strong tradition of, ‘Do we go to the operating room, or do we go to the imaging suite for angiography?’ I would submit that those two places are exactly the same place. In our hybrid operating rooms nowadays, we can do anything.”
Unlike in his military days.
Starnes’ experience—both military and civilian—is considerable and illustrative to the topic at hand. From military life, there was the time he led a surgical team dispatched to the Pentagon after the building came under attack on 9/11; from civilian practice, a status that includes leading surgeon-scientist, professor and founder of innovative vascular therapy company Aortica Corporation, now owned by Terumo.
Earlier this year, Starnes was also at the head of efforts aimed at dealing with the impact of the COVID-19 outbreak on vascular practice. He and his UW team crafted an influential set of clinical practice guidelines, and Starnes was vocal in calling on his fellow vascular chiefs across the country to take urgent measures in order to conserve resources and save lives. His military background was prominent in how he viewed the threat posed by the virus and approaches to triaging patients.
U.S. forces. Starnes showed his entrance and exit wounds from a high-velocity weapon and their stellate- or star-like shape. “These are war wounds, and they need to be aggressively debrided, otherwise the patient can die of sepsis.”
All of this serves as fuel for his current role at Seattle’s Harborview Medical Center.
From this vantage point, he operates at the only level-one trauma center for five Western states, which means a lot of vascular injuries, Starnes said.
In between times, there has been a documented increase in the use of endovascular techniques to treat vascular trauma. One paper he cited showed a positive trend related to endovascular therapy in civilian vascular injuries, particularly with regard to the thoracic aorta. “That was commensurate with an increase in survival for those patients having endovascular repair versus an open repair of a vascular injury,” Starnes observed. “The conclusions of this study were that the use of endovascular therapy in the United States has increased dramatically during the last decade, particularly among severely injured blunt force trauma patients. And endovascular therapy was associated with improved hospital mortality and lower rates of sepsis.”
SCVSS president Juan Carlos Jimenez, MD, just about managed a career synopsis when he introduced Starnes to the meeting.
“His list of military awards is impressive and inspiring, and includes the following: Combat Medical Badge, one of only two combat badges and only given to those who render medical aid while under direct hostile enemy fire on the battlefield; the Meritorious Service Medal; six Army Commendation Medals; and an Army Achievement Medal—just to name a few,” Jimenez said.
Benjamin W. Starnes saw his first combat mission as a military surgeon in Kosovo in 1999 (top right); the UW vascular chief at work in the battlefield (middle); and a repaired arm Starnes and his team at UW saved from amputation after a horrific injury (bottom)
For his part, endovascular techniques bear many merits: They can temporize lifethreatening injuries, don’t require direct surgical exposure and can serve as primary treatment. Starnes ran through its use in five vascular beds: trauma of the cervical, thoracic, axilo-subclavian, abdominal and ileo-femoral, and extremity regions. Rounding out, he described the case of a man whose mangled arm was saved from amputation—an example to illustrate the importance of maintaining open repair skills.
From back then, Starnes showed attendees some of the severe vascular trauma cases he treated in battlefield scenarios from Kosovo to Iraq. Injuries to the lower extremities, the aorta, the upper extremities, the neck. He told of spartan surroundings. Makeshift operating rooms. A power failure necessitating the deployment of a flashlight in the middle of a four-compartment fasciotomy. Limbs saved. The unrelenting backdrop of gunfire. Mistakes made and lessons learned.
On the fundamentals: War injuries—very different to civilian injuries—mean learning how to manage patients in a very different way, Starnes said. To illustrate the point, he drew on the case of the brother of the infamous Iraqi military commander dubbed Chemical Ali after the man was shot and captured by
“This is not a normal extremity,” he said, pointing to both a graphic image of the injury, then the repaired arm. “But he has grip strength, and he has his arm.” Out on the frontlines of war, on the other hand, the arm would have been amputated and burned before the day was out. “We don’t have the resources on the battlefield to do what we can do every day in our modern hybrid operating rooms and in our modern hospital systems.”
Which recalls the lecture title: Alea iacta est “Endovascular methods are now utilized to manage vascular trauma,” Starnes told the SCVSS audience. “I think that technology is behind the pace of innovation in this country. We know from multiple studies that endovascular methods have lower morbidity rates, higher success rates and reduced anesthetic requirements. And endovascular approaches to vascular trauma may be limited to certain regions of the body. And I would say that for extremity injuries, it’s pretty simple: Put up a tourniquet and do the proper repair.”
Benjamin W. Starnes
‘Significant’ value of podiatrists in vascular practice
BY BRYAN KAY
A multidisciplinary limb salvage alliance found that operating room (OR) and clinic volumes as well as work relative value units (wRVUs) all increased significantly over a three-year period after the recruitment of podiatrists into the program.
STUDYING DATA FROM 2015–2019, researchers found that although growth was initially pulled up by the addition of vascular surgeons in 2017, podiatry accounted for a 57% increase in clinic—and more than 60% jump in OR traffic—in the last two years.
The data, presented by Wei Zhou, professor and chief of vascular surgery at the University of Arizona in Tucson at the 2020 Western Vascular Society (WVS) virtual annual meeting (Sept. 27–29), comes from a study on the economic value of adding a podiatry service in a limb salvage alliance. Zhou is also co-director of the group in question: the Southern Arizona Limb Salvage Alliance (SALSA),
which was co-founded by vascular surgeon Joseph Mills, MD, and podiatrist David G. Armstrong, DPM, in 2008.
“The benefits of close collaboration between podiatry and vascular extends beyond clinical outcome. Understanding and clearly outlining the financial advantages can help bring podiatrists into a limb salvage practice,” said Zhou.
Zhou occupies an apt vantage point. The area in which her team operates is in a unique geographic location: It is home to the largest, densest population of Native Americans in the country, as well as a large Hispanic populace. Tze-Woei Tan, MBBS, one of the study co-authors, found that among Medicare beneficiaries, Native Americans have the worst diabetic foot ulcer and infection outcomes.
SALSA, a multidisciplinary “toe and flow” program now widely adopted around the world, grew out of this stark environment. The institution where they operate, Banner-University Medical Center, a safety net hospital, has a patient population comprised of nearly 40% Hispanic and Native American.
Historically—based on a study by Kay R. Goshima, MD, a SALSA team member—despite a history of aggressive infrapopliteal revascularization, nearly 50% of patients required hospital readmission within six months, and over 50% saw prolonged time healing, Zhou explained.
Zhou and colleagues studied a period during which the composition of the alliance went through significant change. The number of podiatrists went from three to one and now four, while the vascular surgeon portion moved from two to four.
Reviewing an administrative database, the investigators plumbed captured
Diabetes Awareness Month: The utility of SVS branding fliers for diabetic foot ulcers
BY BETH BALES
November is Diabetes Awareness Month. The Branding Toolkit (see cover story) can help SVS members promote the valuable care they provide those with the disease.
One of the three customizable condition fliers currently available covers diabetic foot ulcers (the other two address abdominal aortic aneurysms, or AAAs, and chronic limb-threatening ischemia, or CLTI). Surgeons can highlight awareness of diabetic foot ulcers by sending the flier—customized and personalized with contact information— to referring physicians and podiatrists. The front of the flier outlines each condition, information on when to refer a patient, and the all-important question of “why” a provider should refer a
data such as monthly OR cases, clinic encounters, inpatient volume and total wRVUs generated by the SALSA team. Some 36,000 patients were seen at the SALSA clinic and over 5,500 operative cases were performed over the period. Overall, Zhou et al found 100% growth in
patient with the condition to a vascular surgeon. The flier’s flip side includes clinical practice guidelines for diabetic foot ulcers and CLTI.
The toolkit also includes a flier—also customizable—directed to podiatrists, featuring three SVS members working with patients’ feet. Members can swap out the existing photos with ones of their own. Members can use the flier as a handout, an emailable PDF or as a fullpage print ad.
Visit vsweb.org/Branding for more information.
“The benefits of close collaboration between podiatry and vascular extends beyond clinical outcome”—
Wei Zhou
clinic visits, operative cases and wRVUs from 2015 to 2019. “The team has grown significantly over the last five years and was significant for each year,” said Zhou “The initial growth was attributed to vascular surgeons. An increase in the podiatry complement contributed to over 100% growth in the clinic volume. Podiatry in general evaluate twice as many patients in clinic than vascular surgeons. They see up to 1,000 patients a month, while vascular surgeons typically see 300–400 patients a month.”
Initial growth in patients treated in the OR, too, was initially attributed to vascular surgeons, Zhou continued. In 2019, podiatrist recruitment contributed to an additional increase of 40%, she said. “Despite podiatric procedures being shifted from vascular surgeons to the podiatrists, in 2018 and 2019 vascular surgeons continued to see an incremental growth in OR volume. When we look at total wRVU, not surprisingly podiatry had a significant increase in wRVU in 2019, and contributed to a total 40% of group wRVU.”
Summing up, Zhou observed: “Podiatrists had the greatest contribution to outpatient care—up to 70% of total clinic encounters were done by podiatrists. Podiatrists contributed to up to 40% of OR cases, inpatient consultations, total wRVUs and total charges in our group.”