Double whammy: Society set to stage pair of Annual Business Meetings this month
Herbert Dardik, vascular luminary and lowerextremity bypass pioneer, dies at 84
BY BRYAN KAY
THE VASCULAR SURGERY world has lost one of its leading lights. Herbert Dardik, MD, a giant of the specialty renowned for his innovative work on the umbilical vein graft and as a champion of emerging vascular surgeons, has died. He was 84.
For almost 50 years, Dardik was an omnipresent figure at Englewood Hospital and Medical Center in Englewood, New Jersey, where he rose to become the institution’s chief of vascular surgery, and, in 2016, its chief emeritus of vascular surgery and general surgery.
In 1978, he founded the hospital’s first vascular surgery fellowship program, much later chipping in to help revive it. Retiring from clinical practice in 2017, Dardik remained a familiar presence at the hospital until a year ago. He died of natural causes. He is survived by his wife of more than 60 years, Janet, and children, Alan (also a vascular surgeon), Michael and Sharon.
To drain or not to drain? That is the question
Vascular surgeons from across world report on early response to pandemic
BY BRYAN KAY
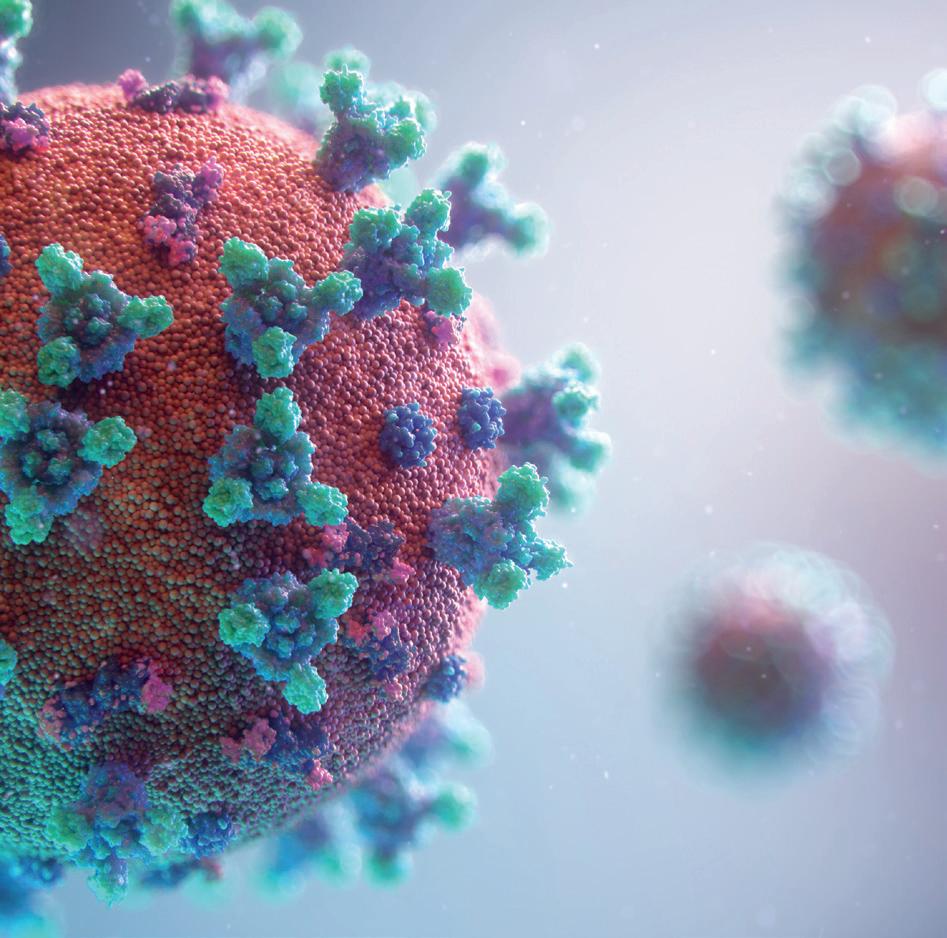
The seismic impact of the novel coronavirus on vascular surgery across the globe continues to be absorbed. Practice changed, and the specialty pivoted to meet the challenges posed head on.
Last month, Vascular Specialist explored the Society for Vascular Surgery response and the different ways surgical practices in U.S. hotspots had been hit.
In this month’s issue, we point a wide lens on the vascular landscape, producing an in-depth special report
that chronicles the early experiences of vascular surgeons in key countries across the globe and cities dotted around North America. A team led by Matthew Smith, MD, Laura Marie Drudi, MD, and Erica Leith Mitchell, MD, introduce these global perspectives about how they and their colleagues in far-flung locations tackled the pandemic as it arrived on their doorsteps. This is vascular surgeons in the thick of the crisis—in their own words.
Letter from NYC: Lessons learned ahead of possible future waves of COVID-19
BY NICHOLAS J. MORRISSEY, MD
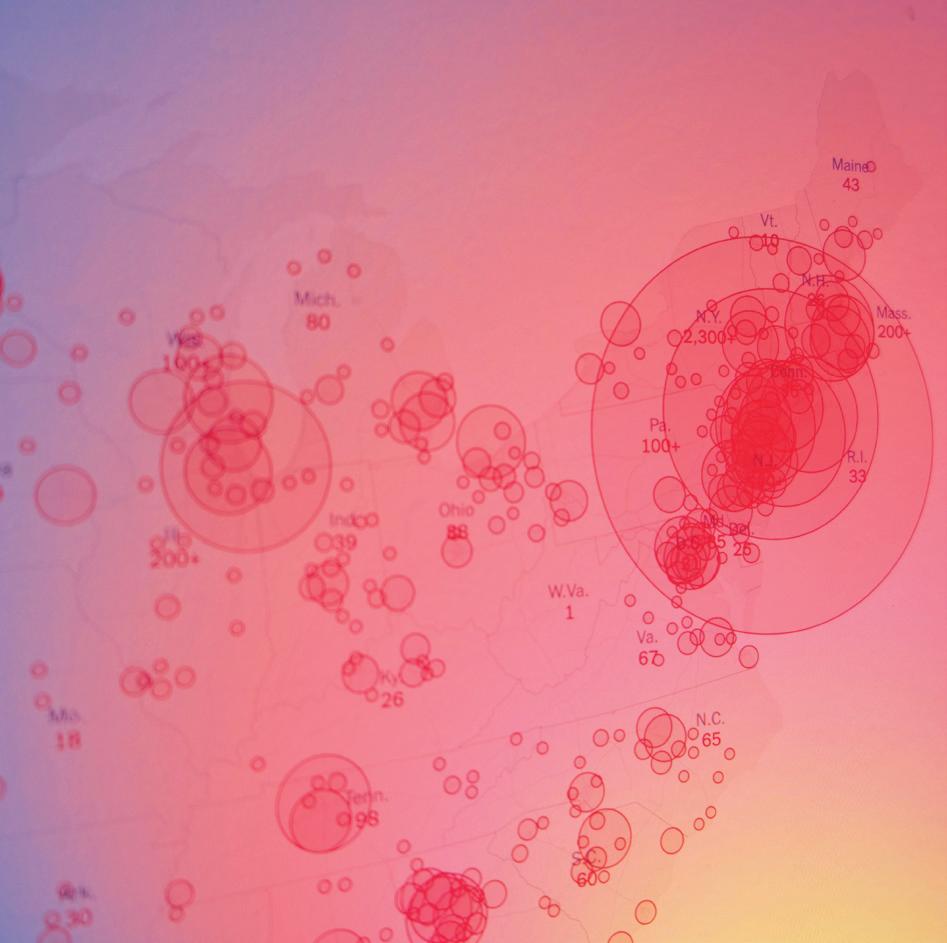
On March 1, I drove down the Connecticut Turnpike in a rental car with my three sons. We had just left a somber family event, and I was listening to the news with eagerness as the initial COVID-19 invasion of the Pacific Northwest seemed poised to overflow across the United States. The first potential New York patient was being tested, while one confirmed case was identified in Rhode Island. After that peaceful day, the next two months exist in my mind’s eye as a blaring tidal wave of pain, death and unrest.
The second case, in Westchester County, was located a mere 15 minutes outside the city, and, given the early stage of the U.S. experience, testing and isolation were well under the radar. The patient's travels were vast and inoculating. Symptomatic and asymptomatic carriers logarithmically rained this disease to the south, where our most vulnerable and physiologically susceptible lived in high density. This was the beginning of the disparate destruction of people by the single-stranded RNA virus, apparently bringing the most modern civilization to its knees. So many societal issues illuminated by the COVID-19 flashlight were on display from day one. The haves whose jobs were not essential fled to their well-spaced out homes away from the cesspool of virus—often to the dismay of the natives who feared Gotham’s invasion would bring virus to their miniscule healthcare system.
Here in Manhattan—or, more precisely, here at Columbia University Irving Medical Center—the mission was clear. Daily predictions assured us we were in for an onslaught of sickness and contagion
unlike any that had been seen in a century. The department of surgery faculty, without hesitation, offered up their services to be redeployed in any capacity the strategists felt appropriate.
MEDICAL SWAT
A team of acute care surgeons and general surgery residents invented the SWAT team—Surgical Workforce and Access Team. The group was staffed 24/7, and included an attending and two residents. Almost all surgeons took their share of 12-hour shifts, deploying to the emergency department and to the various intensive care units (ICUs) that were constructed hastily yet efficiently in all corners of our institution. We placed several hundred lines, tubes, etc. One thing to bear in mind—peculiar to our institution—is that the entire hospital enterprise had just a month earlier gone live with the Epic electronic medical record (EMR) across all campuses. It was an impressive lift to get all practitioners up to speed and working on Feb. 1, and the onslaught of a global pandemic threatened to overwhelm the nascent facility we demonstrated
with our new tools. What happened from March forward was fairly remarkable. Epic natives constructed COVID-19 specific workflows, helping bring the naïve up to speed rapidly.
Pandemics and public health crises are not things we celebrate, but our responses to them can and perhaps should be. My institution, in ways even beyond the spirit suggested in this writing, performed admirably and with complete support in ways that make me exquisitely proud.
The faculty in all departments rapidly assimilated and selflessly redeployed around the institution in varying roles. The department of surgery faculty spent weekend free time reviewing critical care and ventilator management in preparation for taking on roles in the ever-burgeoning ICUs.
POP-UPS
Early on in the process, while we saw the onslaught steaming towards us from afar, almost the entirety of our operating room (OR) suites were converted to pop-up ICUs. I still recall the first moment I peered into “my” OR. The surgical lights were unceremoniously pushed toward the ceiling, made unnecessary by the retooling of this once familiar space. The tape on the floor outlined space for up to six beds, and the ventilators of varying sizes and shapes were at the ready. Ventilators were to be our limiting factor, this was the message we received from Italy and our governor. Every available anesthesia machine was quietly placed in position alongside beds topped with crisp linens: the calm before the swarm. Within a week, I began the first of about 15 ICU shifts. We all volunteered in one way or another for these 12-hour shifts.
VASCULAR SPECIALIST
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD, Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Drudi, MD
Executive Director SVS Kenneth M. Slaw, PhD
Director of Membership, Marketing and Communications Angela Taylor
Managing Editor SVS Beth Bales
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA Publishing. Content for the News From SVS is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA Publishing will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein.
The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com.
For missing issue claims, e-mail subscriptions@bibamedical.com.
Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA Publishing.
Published by BIBA Publishing, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Dawn Powell, Jocelyn Hudson
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe 526 Fulham
Nicholas J. Morrissey
That first night was surreal. My “room” was now full. The beds contained intubated, sedated patients with feeding tubes, towers of drips and renal replacement modules. The noise of the airflow systems was a deafening reminder of just how quickly and completely our native spaces were turned into unrecognizable entities. The space, the lights, the scrub sink all immediately reminded me that, yes, this is where I now live.
Every shift brought new experiences as we responded to data learned from the previous few days: treatments, vent weaning, sedation, coagulation, cardiomyopathy, renal failure. The N-95 masks, always present, gave rise to hypercarbic headaches post-shift—only the first layer in the uniform of safety. Surgical masks were followed by bouffant cap and face shield. Anxiety peaked
when you entered a room without these pieces of equipment. Or perhaps when an endotracheal tube disconnected such that the HEPA filter was not on the patient side. Many weeks later, as I remain healthy and do my 9-mile runs to assure lung function is intact, I am convinced that I was perhaps safer swimming in the COVID-19 broth than many of my fellow citizens meandering on the outside.
TRANSFORMED
One evening, I donned my layers of personal protective equipment (PPE) and placed an iPad into a Ziploc-type apparatus. I walked into the room and pushed a button to connect via FaceTime to a patient’s wife. It was Easter weekend. I held the screen to his face, and she saw him, intubated and asleep. She wept and prayed, in Spanish reassuring
So many societal issues illuminated by the COVID-19 flashlight were on display from day one. The haves whose jobs were not essential fled to their well-spaced out homes away from the cesspool of virus—often to the dismay of the natives who feared Gotham’s invasion would bring virus to their miniscule healthcare system
him that she had recovered from her COVID-19 bout and that the children and grandchildren were doing fine. So many times she said, “I love you,” and her tears flowed in HD across the screen. I was as close as I could be to his face to try to minimize the infinite distance between the two loves. I looked around the space, the space in which a year ago, at 2 a.m., a fellow and I repaired a gunshot wound to an axillary artery with a saphenous vein graft. This same space so transformed—unrecognizable save for the obvious small, well-placed landmarks that made it unmistakably “my” room. That was our first face-to-face patient-family encounter, and I recounted it to my colleagues as perhaps the most emotionally intense moment of my career. I can report that, after several weeks, this gentleman was reunited with his family, in person, at home.
On a personal level, my three sons,teenagers all, who were being educated via Zoom and webbased classes, certainly had to be protected from my potential as a vector of disease. As with many of us, a decision was made to have my parental relationship exist via FaceTime, with daily chats, homework help and discussions that normally occurred in person. It's a small price to pay to protect them from some of the ravages we are only just detecting regarding pediatric COVID-19. My personal situation did not require a reconfiguring of living arrangements but several colleagues ended up holing up in dorm rooms and other temporary housing in order to engage in the mission while protecting their families. I suspect my experience is echoed around the country and the world. In wave one, we seemed to be running a few steps ahead of the tidal wave. I am hopeful that if there are more, what we have accumulated in knowledge, equipment and collaborative spirit will keep us comfortably ahead of the onslaught.
Nicholas J. Morrissey is associate professor of surgery in the division of vascular surgery at Columbia University Vagelos College of Physicians and Surgeons in New York.
Dark times: NYC ground to a virtual halt as COVID-19 ravaged the metropolis
Across the world: Early impact of COVID-19 on vascular surgeons
BY MATTHEW SMITH, MD, LAURA MARIE DRUDI, MD, AND ERICA LEITH MITCHELL, MD
COVID-19 has changed our world and surgical practices as vascular surgeons. We have been faced with unforeseen challenges, and the professional impact has been global. Elective procedures, the staple of our practice, have been indefinitely canceled and delayed. Clinics have been replaced by virtual encounters, and patients are only seeking hospital care when their vascular disease is severe and/or life threatening. The pandemic is taking healthcare providers far outside their comfort zones, and physicians and surgeons are being transitioned or deployed into unfamiliar or novel clinical roles. Physicians are being asked to work in unsafe conditions, where shortages in personal protective equipment (PPE) put the providers and their patients equally at risk for contracting the viral infection.
The following narratives provide witness and lay bare the stories of the earliest communal responses to COVID-19 from the point of view of vascular surgeons practicing amidst the crisis. The stories start with the experiences of vascular surgeons in Lombardy, Italy, the first place, outside of Wuhan, China, to be affected by COVID-19. We then journey to South Korea, followed by Japan, Abu Dhabi, Chile, Austria, Canada and the United Kingdom. A collection of COVID-19 vascular surgeon narratives from across the U.S. follows, with the stories starting in Seattle, the first described U.S. COVID-19 touchpoint, then moving on to New York and other states thereafter.
ITALY:
Into the eye of the storm
The first two confirmed cases of COVID-19 in Italy occurred at Spallanzani Institute on Jan. 30. The patients were from China, and were visiting Italy on holiday. They were hospitalized and isolated on Jan. 29, then successfully discharged Feb. 26. The first case of the disease resulting from secondary transmission occurred on Feb. 18 in Codogno, a municipality of Lombardy in the province of Lodi. I am an Italian vascular surgeon, born in the Lombardy municipality, but work in a hospital in Treviso in northern Italy, about 300km from Lodi. It was unfathomable to me that a COVID-19 outbreak could occur in my hospital. This is an account of my experiences during the first month of COVID-19. First week: I did my work without fear, not fully aware of the potential
A chest x-ray demonstrated findings suggestive of pneumonia; a nasopharyngeal swab was positive for COVID-19. I started to worry—Laura Nicolai
risks and severity of this infection. Second week: A case of COVID-19 on our vascular surgical service was reported. The patient was admitted for critical limb ischemia. On hospital day two, he displayed symptoms of respiratory distress. A chest x-ray demonstrated findings suggestive of pneumonia; a nasopharyngeal swab was positive for COVID-19. I started to worry. Third week: My hospital reduced elective operations and focused on increasing capacity in intensive care. Our hospital created new intensive care units (ICUs) in the operating room (OR). I was now experiencing dread, worry and loneliness. I chose to physically isolate from my family, not wanting to put them at risk, and knowing that I chose this work and profession. Despite the risk of working with COVID-19 patients, I remained passionate about my profession but found that I was constantly trying to mitigate my anxiety, uncertainty, and fear of contracting the disease. Fourth week: I performed a popliteal artery and tibial thromboembolectomy in an infected man, aged in his 60s, for acute limb ischemia. Post-operatively, he was initiated on unfractionated heparin. Despite this, two days later he redeveloped ipsilateral acute limb ischemia
and worsening COVID-19 pneumonia. He was transferred to the ICU after I took him to the OR for re-do popliteal and tibial thromboembolectomy. Unfortunately, eight hours post-operatively he again redeveloped acute ischemia. Thinking the recurrent thrombosis was due to pedal microvasculature thrombosis, I performed popliteal and tibial thromboembolectomy (for the third time) and plantar artery thromboembolectomy with concomitant arteriovenous fistula (AVF) creation to the tibial vein. Anticoagulation with heparin was continued. At 23 days, the patient is in the ICU with a tracheotomy and salvaged foot. He has triphasic Doppler signals and a patent AVF.—Laura Nicolai, MD, vascular surgery unit, Cà Foncello Hospital
SOUTH KOREA:
Land of the Morning Calm
South Korea was one of the first countries outside of China hit hard by the COVID-19 outbreak. Our first case occurred on Jan. 20. A steep rise in patients was seen from Feb. 19 onwards and continued throughout the month of March. By the beginning of April, our daily incidence of new COVID-19 cases finally stabilized, but now we are facing a resurgence in newly diagnosed cases as Korean citizens living abroad return. As a vascular surgeon working around Seoul, I did not have to change any of my daily practices during this period primarily as many cases (more than 80%) in Korea centered around Daegu and Gyeongbuk province. As in the case of Wuhan, our country managed to contain the outbreak, thus preventing a nationwide spread.
This experience has allowed the Korean people to remain relatively calm and unaffected by the outbreak, especially since Koreans have no objection to wearing masks and social distancing. The rapid development of a diagnostic tool for COVID-19, and the large number of diagnostic tests performed, has allowed for appropriate selfisolation of potential candidates. Additionally, an effective quarantine system and rapid assessment of potential close contacts has limited the spread of the virus. In the city of Daegu and Gyeongbuk province, where the newly diagnosed patients outnumbered the hospital facilities, several hospitals were designated as COVID-19 inpatient hospitals, allowing for all symptomatic patients to be admitted to these facilities. At our hospital preventive measures were taken from the start. By the end of the first week, all conferences were canceled for an indefinite period. Medical personnel were advised not to engage in activities involving a crowd, including dining events. All travel abroad was prohibited, and personnel with recent travel to either China or any other country with COVID-19 were evaluated for symptoms. All outpatients were screened for respiratory symptoms and fever, and, if positive, were guided to a separate outpatient facility for isolation from other patients. By the fifth week, the period with the greatest rise in cases, a ward was specially designated for suspicious COVID-19 patients. Based on these preventive and isolation measures, the hospital maintained its
Laura Nicolai
Hyung Sub Park
During the period of the COVID-19 outbreak, our outpatient numbers only decreased by 20–30% Hyung Sub Park
usual function, and, as such, our daily practice was not affected. During the period of the COVID-19 outbreak, our outpatient numbers only decreased by 20–30%, and hospital admissions and operative cases remained relatively constant. Despite the relatively larger number of COVID-19 patients, vascular surgeons in the region continued practice as usual. Cases that could be delayed, without causing harm to the patient, were postponed indefinitely, while other elective cases that required a postoperative ICU stay were delayed. Urgent cases not requiring an ICU stay were performed as usual. Since mid-April, we have had less than 20 cases per day nationwide, and the government is now considering loosening up on the strict measures implemented to achieve social distancing.—Hyung Sub Park, MD, assistant professor of surgery, vascular, Seoul National University Bundang Hospital
JAPAN:
Beyond the East Sea
The East Sea separates Japan from China. The first COVID-19 patient in Japan was confirmed on Jan. 16. The patient had recently traveled to Wuhan, China. On April 7, there were 4,100 COVID-19 patients, 79 in intensive care, and 97 total deaths. In my hometown of Nagoya, 148 patients have been confirmed, with only two inpatients in Nagoya University Hospital. In my hospital, vascular surgeons are working as usual and performing elective operations. Our other medical colleagues have not yet encountered COVID-19 patients. In the three months since the first reported patient in Japan, the outbreak has only affected our capital of Tokyo. A state of emergency—without a lockdown—was declared on April 7, covering a total of five cities, including Tokyo and Osaka. Nagoya was excluded from the list. As the situation in Tokyo worsened, our perspective changed, and we prepared for the worst.—Hiroshi Banno, MD, assistant professor, division of vascular surgery, Nagoya University Graduate School of Medicine
ABU DHABI: At the heart of the UAE
The early Cleveland Clinic Abu Dhabi (CCAD) experience with the COVID-19 pandemic has been characterized by a rapid response calibrated to incoming data. Since its inception, there has been a cultivation of a culture characterized by community.
There are daily meetings called “huddles” directed at the department or institutional level, followed by a daily hospital wide huddle. Since the first cases in Abu Dhabi in February, there has been a weekly virtual town hall and a central website to collect directives, training videos and news. A daily huddle of specialists, focused around action plans for the pandemic, results in email transmission of directives hospital-wide. These remarkably clear directives provide caregivers with the ability to rapidly react to the exigencies of the pandemic. The early and broad availability of testing has benefited the Emirate of Abu Dhabi, and has been critical in saving lives and keeping the hospitals from being overcome by a surge. As a vascular department— composed of three surgeons, one cardiologist, one podiatrist, two vascular technologists, one clinical nurse coordinator and several clinic nurses and staff—our mission has shifted from frantically managing the crisis to “winning the war.” This involved adopting guidance from the Society for Vascular Surgery (SVS) and reducing our elective cases. Rapid employment by the CCAD department of information technology allowed our clinic to be safely conducted by telephone and video conference
This entire experience has made us reflect and profoundly rethink our practice strategy: vascular surgery as vascular hospitalism—Michael Park
visits via virtual telemedicine. Additionally, based on individual skills, all physicians have been assigned a secondary function in the case of a case surge. Workflows have also been modified to minimize contact with other caregivers. This entire experience has made us reflect and profoundly rethink our practice strategy: vascular surgery as vascular hospitalism. This is how we train our residents and fellows, and the term informs us on the concept of the hospital as a critical, evolved and mighty community for curing patients. In a post-pandemic world, I see the need to reprioritize our values with the collected experience of this tragedy.—Michael Park, MD, chief of vascular surgery, Cleveland Clinic Abu Dhabi
AUSTRIA: Bordering northern Italy
The southern border of Austria faces northeastern Italy. The first case in Austria was Feb. 25. This patient had recently returned from Italy. On March 10, Austria imposed travel restrictions from travelers returning from China, Iran and Italy. Not long after, on March 12, we had our first reported COVID-19 death. On March 16, we had a national shutdown. Travel was only allowed for the purchase of food or medications and to provide help for others in need. Walking outdoors within 1 km from your
home address was allowed. Our department of vascular surgery at Graz Medical University here in Graz includes 10 attendings, four residents, and two general practitioners. Between Feb. 25 and March 7, there was not much change to our work schedules, nor caseload. However, in early March, we began to develop a COVID-19 strategy. This included isolation in-hospital, clearing wards and ICU beds to make way for a surge, training all the staff on the use of PPE, and canceling all elective cases and preadmissions. On March 15, we had three attendings and one resident start self-isolation (14 days) after all returned from a high exposure area while skiing in Tyrol, Italy. The call schedules were subsequently adapted, outpatient clinics were canceled, and only emergency operations were performed. Unfortunately, during this period PPE was not available at the hospital for all personnel, including staff in the emergency department. COVID-19 testing was restricted to patients with fever, coughs and positive travel histories or recent exposure. This has certainly been a trying time, and we have encountered several challenges. First, COVID-19 testing is not widely available and reporting takes 12–14 hours. Second, we have been overwhelmed by calls from anxious patients concerned about their health—not understanding that their condition is not an emergency. Finally, staff wellbeing and mental health have been negatively affected. The professional and personal impact of this pandemic cannot be understated; efforts to address these issues need to be a priority.—Tina Cohnert, MD, department of vascular surgery, Graz Medical University
CHILE:
Along the South Pacific
My first month’s experience as a vascular surgeon working through the pandemic in the Chilean capital, Santiago, was to ensure that coverage was available should the outbreak overwhelm our hospital's capacity, as well as that of our country. We are currently on day 34 after the first case and have a total of 4,815 cases and 37 deaths. The estimated number of recovered patients is 724. The government has worked tirelessly to keep its citizens safe and healthy by selectively quarantining different areas of the country, flattening the curve. We are about two to three weeks behind the northern hemisphere Only time will tell if this trend continues in the following weeks. We work in a university-affiliated private hospital with five vascular surgeons who cover two hospitals. We are currently working in call teams of one fellow and one staff, with one surgeon as backup on week rotations. This leaves three staff at home. The staff on call rotates every five weeks, the fellows every three. We have not had any of our vascular colleagues become infected. We had a very significant reduction in our elective cases, with the only operations we are conducting being placement of perma-caths (for oncologic patients needing chemotherapy and patients needing dialysis), symptomatic and/or ruptured abdominal aortic aneurysms (AAAs), and
continued on page 6
Hiroshi Banno
Tina Cohnert
Michael Park
Francisco Vargas
Across the
globe: Early impact of COVID-19 on vascular surgeons
Continued from page 5
symptomatic carotid disease. Our outpatient clinic volume has dramatically declined to a minimum and we have started implementing telemedicine this past week. This has been a remarkably interesting experience since we have had to fight against the opinions of some of our senior members who do not approve of doing medicine without a physical exam. I believe there are benefits and pitfalls to telemedicine, but it is a tool that all specialties can use. Telemedicine will likely prove to be an excellent alternative to provide counseling, guidance and follow-up for a great number of our patients in the current setting by avoiding the risk of acquiring COVID-19.—Francisco Vargas, MD, assistant professor, department of vascular and endovascular surgery, Pontificia Universidad Católica de Chile
CANADA:
Across the northern frontier
Canada saw its first COVID-19 related death on March 9 when an elderly resident in a long-term care facility in British Columbia passed away. Early on, the vast majority (89.7%) occurred in the two most populous provinces, Quebec and Ontario, with 805 and 513 reported fatalities, respectively. During the months of March and April, the strategies in our hospitals and vascular surgery services were to mitigate what was expected to be an exponential spike in cases that would threaten to overrun our acute care services. Preservation of PPE, healthcare personnel and maximizing ICU capacity were the priorities. Elective surgical activity was immediately limited to patients who would suffer significant harm if they waited beyond a week or two. Other than emergencies, at most hospitals vascular surgery cases were limited to exceptionally large aneurysms, symptomatic carotid stenoses and severe chronic limb threatening ischemia. In Ontario, this resulted in a greater than 70% reduction of vascular surgery activity compared to the same time period last year, and a projected backlog of vascular cases exceeding 2,000 patients. At our academic institutions, our residents and fellows were organized into teams so there were “on” and “off” teams to minimize exposure. Surgeons adopted similar schedules. In tandem, there have been some potential advances in medical care, specifically the adoption of telemedicine. It is ironic it took a pandemic to prompt us to adopt existing technology. As the spring turns into summer, it’s becoming apparent that instead of an overwhelming short-term spike, most Canadian jurisdictions are facing a longerterm situation where there will be a certain level of COVID-19 activity in our communities and hospitals for the foreseeable future until a vaccine is available. Attention is presently being paid to Canadian long-term care facilities, which comprise almost half of COVID-19 deaths, and to de-escalate
the original reductions in non-coronavirus activity. Various systems have been proposed to do this, but one that allows for this necessary flexibility is the Vascular Surgery Activity Condition (VASCCON), which is modeled after the Defense Readiness Condition (DEFCON) used by the U.S. military to describe the various stages of readiness in response to an external threat. Similarly, this coronavirus pandemic is an external threat to the normal practice of vascular surgery, and in response to various degrees of COVID-19 activity and the availability of PPE and ICU resources, VASCCON describes five graduated levels of surgical activity ranging from 5 (normal practice) to 1 (no surgical activity). Levels 4 and 3 represent increasingly strict reductions in elective surgical activity while level 2 represents only truly emergency procedures. Level 1 is the untenable situation where all surgical activity ceases and even emergent patients are palliated. This system is relevant to all surgical services and offers a step-wise escalation and de-escalation of surgical restriction with an eventual return to normal activity.—Thomas Forbes, MD, professor and chair, division of vascular surgery, University of Toronto
In tandem, there have been some potential advances in medical care, specifically the adoption of telemedicine— Thomas Forbes
CANADA: Trainee perspective
Drudi
On March 14, after several weeks of being on study leave for my specialty exam in vascular surgery, I received an email saying our licensing exam was postponed to an indefinite date. My heart immediately sank. I was in my own world for several weeks, reviewing SVS guidelines, personal notes and practicing oral exams. I heard of rumblings of a virus that may be heading to our shores and, even after the World Health Organization proclaimed that we would be facing a pandemic, I would be the first to attest that I wasn’t present to the idea that we would be living today in a society of social distancing and closed international borders. I immediately returned to clinical activities to help where needed. My first week back, we were operating as usual—but this quickly transitioned to only emergent and urgent cases. We went from operating every day to, if we were lucky, operating once a week. So, with no licensing exam, and a huge decrease in surgical volume as a chief resident, I felt my skills slowly spiraling down a rabbit hole. I was staring into a void with anxiety; my exam date, my ability to pursue a fellowship in Europe. To maintain my competencies for practice. And to see my family. The more I pondered these existential questions, the more I descended into the abyss. We have not
reached the so-called peak in Montreal and my home province of Quebec, and with rising numbers of COVID-19 cases and deaths daily, it is hard to see how we will ever return to normal any time soon.—Laura Marie Drudi, MD, vascular surgery resident, McGill University
UNITED KINGDOM: Braced for impact
In the early stages, the ultimate course and impact of this pandemic and the resumption of normal vascular practice remain unknown. In the U.K, the first index case was announced Jan. 31. The first confirmed positive admission to my hospital at my hospital in Norwich, England, occurred March 14. In response to the pandemic, we modified our practice in accordance with guidance from the Vascular Society of Great Britain and Ireland and the Royal College of Surgeons. We adopted a traffic light system to prioritize vascular conditions that require interventions. Following the first admission at our hospital, we called for an urgent business meeting to make plans for service provision during the pandemic. From March 14–22, the first week, we continued to practice within the green zone (normal practice). During week two, we moved to the yellow zone (urgent and emergency cases) and moved to the orange zone (emergency cases only) in the third week. All outpatient appointments were triaged into three categories: deferred, telephone consultation and outpatient attendance. We deferred all nonurgent appointments by sending a standard letter to patients and their general practitioners. We triaged all urgent appointments into those suitable for telephone consultations and those who needed to be seen in the hospital. We continued to offer three emergency clinics per week for this purpose. We modified our call schedule to accommodate the need to cover only urgent and emergency cases. After the first week, one of our vascular surgeons was advised to self-isolate until the end of pandemic due to identified individual risks. From week four, all clinicians in the hospital would be combined in teams providing ward-based services. In this way, vascular surgeons, thoracic surgeons and urologists combine into one team to round on all patients on the two wards that they normally cover and provide care for patients regardless of their clinical presentations. Hospital-based educational events are continuing virtually with an emphasis on COVID-19 publications. We continue to retain vascular trainees, who are encouraged to read for exams, write up any research projects and train via simulation. The main challenges we continue to face are ensuring the continued supply of essential resources and PPE for those in need, and a high attrition rate among ancillary staff, resulting in reduced operating room capacity. We anticipate that we will face a long waiting list after the outbreak as our monthly open and endovascular arterial procedures equate to an average of 180–200 cases.— Wissam Al-Jundi, MD, consultant vascular and endovascular surgeon, Norfolk and Norwich University Hospital
Thomas Forbes
Laura Marie
Wissam Al-Jundi
Reacting to virus in key locations across United States
AMERICAN GROUND ZERO
The realization of the pandemic’s magnitude was chilling here in Seattle. I remember the eerily similar feeling of being confused as I watched the twin towers on 9/11. There was an initial lack of comprehension, which led to a slow realization that we were under attack. The first case in the U.S. was reported on Jan. 20 and we thought it was limited to a nursing home. Work proceeded as usual. The last normal I remember was a red eye flight from Seattle to Houston on March 5 in order to present at the Houston Aortic Symposium. It was a quick trip, and I returned that night. The airport in Seattle was eerily devoid of people. That was the moment when I began to realize the magnitude of what was happening around me. The last elective operation I undertook, a third-time groin dissection and endarterectomy, was on March 10. A series of rapid changes then unfolded: a single visitor policy, screening at hospital entrances and all elective operations canceled. The pandemic led to a national emergency. Telemedicine and zoom conferences became the norm. At some point, I had a sore throat, myalgia and fevers. When the symptoms had abated, I was tested, with a negative result. By the last week of March, Washington state had over 2,000 cases of COVID-19. During that week of call, I was consumed with rescheduling clinic patients and multiple complex urgent operations, including an infected graft removal, urgent aortic dissection repair and a complicated sarcoma resection. While these operations were urgent, we were actively thinking of preserving our PPE and resources, worrying that we could deplete what we had. The entire pandemic experience remains surreal to date, including the lack of flour and toilet paper in the stores. For now, we continue to root for our colleagues in the hot zone. And we remain cautiously optimistic we have flattened the curve here in Washington.— Sherene Shalhub, MD, division of vascular surgery, department of surgery, University of Washington
were the first city in the U.S. affected by this quickly evolving pandemic. Our hospital started officially limiting elective cases on March 17, seven weeks after the first positive case in Washington state. Prior to that, there was some confusion about what cases were allowed. We submitted operating room (OR) cases for committee approval and received weekly updates on OR status and PPE supplies, but had little information about COVID-19 patient burden. Since our usual case conferences and meetings had been canceled, I felt somewhat professionally isolated, seeking more
There were so many staffing shortages in the system that we were told to only quarantine if we became symptomatic Matthew Smith
PRIVATE PRACTICE AT US EPICENTER
As a private practice vascular surgeon in Seattle, I work at the multi-specialty clinic downtown, and operate and take call at a 340-bed community hospital nearby. We have an outpatient vascular lab and an outpatient-based lab (OBL) associated with our clinic. Our team of two vascular surgeons collaborates with the vascular group at the hospital. Lots of uncertainty and fear was in the air, as we
guidance and support from the community. We continued to see few patients at the outpatient clinic and transitioned to some telemedicine services. Two of our four vascular labs have remained open for more urgent exams. We continue to utilize the OBL for thrombosed hemodialysis access and chronic limb-threatening ischemia (CLTI). I have treated some patients who were unable to get procedures done elsewhere due to limited hospital access. Overall, I am humbled and grateful to be a
part of a community that is transforming in the face of this new changing reality.—Daiva Nevidomskyte, MD, vascular surgeon, The Polyclinic
ANXIETY IN NYC
March 2020 was the month that New York City and my vascular training ceased to function as normal. The first patient to be affected with COVID-19 in NYC was diagnosed on March 1; the second case followed two days later. The latter case was transferred to Columbia Hospital, initiating a chain of events that drastically altered my vascular training. During the first week, the hospital suggested delaying elective procedures on patients over the age of 70, or with severe pre-existing conditions, but there was little change in practice as the COVID-19 cases slowly amassed in the medical wards and ICUs. At the start of the second week, delaying elective cases became a requirement, and we were only treating patients with CLTI, dialysis maintenance and larger aneurysms. Moreover, a bypass patient developed a cough but tested negative for the virus, scaring us enough that only urgent cases were admitted to our service afterward. The rounding teams decreased from 10 people to just four in order to conserve PPE and reduce exposure. We moved all educational conferences online. At the beginning of the third week, the ICUs were rapidly filling with COVID-19 patients and half of our 32 ORs were converted into ICU beds. The surgery residents became the emergency call team for difficult lines on coronavirus patients. A CLTI patient developed a cough postoperatively and was found to be COVID-19 positive. By then, there were so many staffing shortages in the system that we were told to only quarantine if we became symptomatic. We began testing every preoperative patient, and all remaining ORs—save three—were converted to ICU beds. Now into the fourth week, we have multi-institutional educational conferences over Zoom, we watch and discuss operative videos, and we wait anxiously for daily updates. We have two patients on service, with only the fellow and a service-shared intern rounding on them. We make every effort to not admit anyone or to discharge as soon as possible—we are not even carrying out completion amputations after guillotine amputations for septic feet— because the COVID-19 census in the hospital is so
Sherene Shalhub
Daiva Nevidomskyte
Matthew Smith
Reacting to virus in key locations across United States
Continued from page 7
great and our vascular patients are so vulnerable. There is a general concern among fellows that our fellowships have been functionally terminated early.—Matthew Smith, MD, division of vascular surgery, Weill Cornell Medicine/New YorkPresbyterian Hospital
CAUTIOUS OPTIMISM IN MICHIGAN
From Bay City, I started to see the cases grow exponentially in New York and felt it mandatory to push the pendulum aggressively in mid-Michigan to help flatten the curve. So, prior to our first confirmed case, even before the surgeon general put out his notice to defer elective cases on March 16, I had already implemented a plan to defer all non-urgent referrals in the clinic followed by deferring non-urgent or emergent cases in the OR. Clinic patients were reviewed for acuity, and the clinics were downsized to a skeleton crew for only urgent referrals including CLTI, symptomatic carotid disease and all AAAs, later revised to just include AAAs over 6–8cm. There was pushback from the administration as they wanted it to be “business as usual,” but I felt strongly that this clinical decision superseded the business decision, and difficult times require difficult and drastic measures. Initially, cases were reviewed by the chief of vascular surgery for appropriateness; however, by week two, only emergent cases were allowed. Initial challenges involved explaining to the rest of the staff that this pandemic was in fact real. Hourlypaid staff and techs were worried about their jobs; sharing the science behind the flatten the curve model was crucial. It was essential to keep everyone informed of the plans, and, as such, changing our behavior was a team effort. The other critical aspect to our new treatment paradigm was to inform the patients that we were not “canceling” their operations, but rather “deferring” or “postponing” their cases until it was safe to operate again. Our initial aggressive approach has been helpful in guiding the other 13 facilities in our healthcare system. Our prompt decision-making elevated us as the health system flagship. We continue to be optimistic these efforts helped to curtail the curve and, importantly, save the lives of our community.—Nicolas Mouawad, MD, McLaren Bay Heart and Vascular
PROGRESS BEFORE THE SURGE
needed. We were asked to complete an online critical care refresher course. On March 23, the state governor announced a shelter-in-place order as we watched our colleagues in Detroit, Royal Oak and Ann Arbor report rapidly increasing cases. We created two separate vascular teams that would rotate, spending seven days in clinical work at the hospital, clinic and covering call. The second group worked from home to prevent a single exposure spreading through the department. On March 27, one of our integrated vascular residents felt ill and was confirmed COVID-19 positive the next day. Thankfully, he was able to self-quarantine at home and recovered quickly over the next 10 days. Realizing we had many patients who needed vascular lab testing to appropriately stratify them, we launched an in-home vascular testing program for high-risk patients on April 1. In the first 10 days, more than 30 patients had testing in their homes followed by a virtual visit to discuss the results. Fortunately for us, the national social distancing program, state shelter-at-home order and efforts of our colleagues to educate us— combined with the implementation of our early reduction in cases—appears to be paying off in west Michigan. We have been seeing a steady number of cases but continue to have adequate PPE, ventilators, and ICU and general beds. Our time to peak surge has been successfully pushed back by weeks, and we have had limited healthcare providers infected at this point. Due to these successful measures, we are now looking to offer surgery to some of our previously postponed patients during this new window prior to the expected surge.—Robert Cuff, MD, division of vascular surgery, Spectrum Health Medical Group
eight to nine fully-packed rooms running daily for 11 surgeons. Now we await the surge, prepare to be redeployed, or contribute in any way possible.—Vipul Khetarpaul, MD, division of vascular surgery, department of surgery, Washington University in St. Louis
SPARKING GROWTH
A state of emergency was declared on March 10, the same day of the first two confirmed cases of COVID-19. Despite being located over 140 miles from the index case, between March 10–20, in Grand Rapids, Michigan, we became trained in virtual visits, all scheduled cases were reassessed and stratified, with elective cases canceled, satellite offices closed and imaging services significantly curtailed. Our hospital set aside 10% of bed capacity to accept patients from the Detroit area if
WORKING THROUGH CONFUSION
I returned from vacation in the second week of March to a packed schedule over the three proceeding weeks, with a large CLTI patient load. Reading about the case numbers on each coast created a lot of anxiety but workflow remained normal until March 18, which was the day the first COVID-19 patient tested positive in St. Louis. There was a lot of confusion and no affirmative government action at first. I packed all the important cases left on the schedule into 7- to 10-day span and decided to cut back significantly on case volume and clinical work at this time. The following week, we had a citywide, stay-at-home order; we started to see PPE was in short supply; there was a lot of concern for our own safety; telemedicine was an emerging uncharted concept; and a couple of surgeons got infected. Testing became more widespread, we pulled our resources from two sister hospitals and adjusted our trainee schedules to protect them. For attendings, we were down a few providers, as some of us were benched or quarantined. We have been taking call once a week, but our case volume is two to three cases per day compared to our baseline of
On March 13, four days after the first COVID-19 case in our hospital in Evanston, Illinois, and six weeks after the first case in the state, our chair here called an emergency meeting as the pandemic started to blossom. A dozen conference calls later, there were guidelines on restrictive surgery, including the cancellation of elective surgeries and clinic reorganizations. A cardiology colleague with whom we worked closely came down with the virus, prompting immediate decontamination of the office. All my partners volunteered for the physician labor pool in case of overwhelming need. Then came the second week. I felt a bit sick, and quarantined myself in a hotel for two days. My only symptom was fatigue—no fever and no cough—so I returned home. We preemptively canceled cases through May, and I had to talk partners and office staff off the ledge as they were anxious about losing their jobs and being redeployed into the “fire.” I performed a complex oncologic resection case that week, along with urgent revascularizations and my last vein case for a good while. Saturday, March 21, Illinois declared shelter in place. I was on call that week and noticed a steady increase in COVID-19 patients. There were multiple emergencies—a devastating aortic arch dissection, limb and mesenteric thrombosis, and several intraoperative arterial injuries. By the fourth week, we had reduced our clinic to just one provider per week. I enjoyed the change of pace, doing WhatsApp and FaceTime clinic visits, though they were more laborious than in-person equivalents. I have been trying to stay positive, and now spend quality time with family, attending family gatherings via Zoom. I am also trying to look ahead to divisional growth at the conclusion of this pandemic with regards to recruitment, incoming fellows and research funding.—Cheong Jun Lee, MD, division of vascular surgery, Northshore University Health Systems
FLATTENING THE CURVE IN TEXAS
In Houston, the effects of the pandemic became clear on March 4, the week of the Houston Aortic Symposium. We had participants from all over the world, except from coronavirus-affected countries like Italy and China. A couple of days later, our institution issued a ban on travel. As a division and an institution, we started reducing our clinic visits, determining emergent surgeries and adjusting call schedules to protect our patients and ourselves. I took the first week of call; no elective cases were performed but emergent cases did not stop. That week I had two ruptured infrarenal aortic aneurysms, one submassive pulmonary
Nicolas Mouawad
Robert Cuff
Vipul Khetarpaul
Cheong Jun Lee
embolism (PE), a few infected arteriovenous grafts and CLTI cases. During that week, I did not have much time to catch up on local news, and barely had time between operations to eat, sleep and finish paperwork. On top of this busy schedule, I learned my brother was ill with suspected COVID-19. Eventually, he tested negative and recovered quickly, but it was unsettling being thousands of miles away, worrying about him, his family and my parents. Week three started, and I was mostly working from home. A stay-at-home order was issued, and the models started predicting a surge in Houston in mid-April. It sunk in that this may be the reality for the coming few months, so we started planning out our educational conferences and meetings for the next few months. Week four, I operated on a couple of urgent outpatients and finished telehealth training. For now, I am playing my part to flatten the curve and prepare for the surge in Houston as it comes.—Rana Afifi, MD, department of cardiothoracic and vascular surgery, McGovern Medical School at The University of Texas Health Science Center at Houston
was COVID-19 positive. As I write, I am to be tested tomorrow, so we will see what happens.—Adel Barkat, MD, Oklahoma Heart Institute
ACCLIMATING IN COLORADO
LOW NUMBERS IN THE HEARTLAND
In the middle of the country, Oklahoma has had an interesting run-in with COVID-19. Week one of the pandemic we watched the world get taken by surprise. China. Japan. Italy. But nothing to report here. By week two, New York starts to get hit hard. Still not much going on here in Oklahoma. However, my partners and I start to notice an odd increase in large clinically significant PE consults from the ICUs. We were business-as-usual until recommendations from the surgeon general and the American College of Surgeons were announced regarding the cessation of elective surgery. That same March 21, we had our first case at our hospital in Tulsa: a young medical professional who deteriorated quickly, requiring ECMO. Now COVID-19 had hit close to home, and alarms began to ring throughout the medical community in the area. Our group decided to cancel all non-urgent cases on the Sunday night—hours before the work week began. Outside of a few suspected patients who had traveled to Italy, things were noticeably quiet in town. We contacted the other vascular surgeons locally and made a unanimous decision to hold off on elective surgery, despite the low numbers. It was evident we were several weeks behind others, so we prepared for an enemy that had not yet arrived. Several more cases were admitted to our hospital in week three. As vascular surgeons, we did inpatient procedures and emergencies but for the most part we left early and waited. Week four, we entered a COVID-19 surge. Case numbers were now drastically higher in the state, along with hospitalizations. Our first coronavirus consult was a cold limb on ECMO. Several COVID-19 ECMO cannulations followed. But, again, at this point we were not yet a New York or New Orleans. My family all became sick with flu-like symptoms. As they recovered, I became ill. I then received an email informing me that a patient on whom I did a PE embolectomy two weeks prior
The first person in Colorado to test positive for COVID-19 came on March 4. I did an angiogram and ray amputation that Friday, and we had friends over for dinner. Life felt normal in Aurora. The first week, we held fellowship interviews, regular clinic and Journal Club, I with an article about the importance of social distancing. Then we saw the first COVID-19 patient at our hospital, and, by the next day, all the healthcare workers were wearing masks. Two days later, we had postponed all elective operations. The second week my daughter had a cough and a fever to 103. I performed a toe amputation on a patient with dry gangrene following revascularization the week before. I postponed an arteriovenous fistula creation as elective. Luckily, my daughter started feeling better as I balanced call and worked from home with my wife and three kids. About half my clinic patients canceled, especially the elderly and those in assisted living facilities, and I had my first virtual clinic. On the third week, a stay-at-home order was issued. It has been a whirlwind 30 days since the first person tested positive in Colorado. I look back at that dinner with friends, and it seems like an eon ago. It has been challenging to stay up to date with information given the speed at which the pandemic spreads. Another challenge has been finding ways to overcome the isolation that comes with physical distancing.—Max Wohlauer, MD, division of vascular surgery, department of surgery, University of Colorado School of Medicine
CONFLICT IN CALIFORNIA
It has been challenging to stay up to date with information given the speed at which the pandemic spreads—Max Wohlauer
but from the relative quiet of California, I feel guilt and helplessness. Hearing about struggles with central access and ECMO on group chats, I reached out to the critical care and cardiology groups at the hospital and offered to help. To my surprise and dismay, there was no organized plan. Despite multiple emails daily, true information transparency and logistical support have been sore points between medical staff and hospital administration.
California declared a state of emergency March 4 and shelter-in-place by county March 16. By March 19, the order was statewide. As a private practice vascular surgeon at a community, non-teaching hospital in Burlingame, near San Francisco, our awareness of the coronavirus epidemic was initially one more of empathy and wariness, watching what was unfolding in China and knowing we were on the “near coast.” After the cluster outbreak in Washington state, the hospital began screening patients upon arrival. When I proposed screening patients at our office, my partner disagreed, not wanting to “scare patients away.” Less than a week later, the shelter-in-place order came down and, just a few days after that, my partner agreed to a screening protocol for our patients and staff. The conflict in a small private practice between patient and staff safety, and financial stability and viability, has continued to be a struggle as the weeks have slowly passed. While elective cases were stopped early at the hospital, my partner continued to do cases at our OBL for “critical” disease, though I had decided to postpone my cases. Witnessing the crisis flare out of control elsewhere
During week three, I realized how much I missed interacting with colleagues at the hospital. Without the socializing typically done between cases or at lunch, I found limited interpersonal crossover for a physician who is not hospital-based. Social contact is still a fundamental part of the human psyche—enough that even as an admitted introvert I found myself looking forward to being on call. Now, almost at week four since shelter-in-place, the irony of hand-sewn face masks and civilian N95s juxtaposed with rationed surgical masks has become the norm. Before, I had never disinfected my desk, phone or keys, and now I do it at least once daily. Our office and vascular lab run an abbreviated schedule. Worries about being able to pay the bills are a constant presence in a not-so-small corner of my brain. While right now I feel undeservedly lucky our area has mostly avoided the first wave of disease, I know that the concerns of this last month will continue, and that our risk remains looming and real.—Stephanie Lin, MD, Bay Area Vein and Vascular Center
Rana Afifi
Adel Barkat
Max Wohlauer
Stephanie Lin
Virtual catch-up: Vascular surgery and coming around to telemedicine
BY UWE FISCHER, MD
Remote treatment of patients, so-called telemedicine, has been around since the 1940s, when it was used first for transmission of radiology images. In later years, remote interaction between physician and patient was predominantly used by medical subspecialties such as behavioral medicine and psychiatry, driven by community need and sparse physician resources. The ability to evaluate patients living in rural areas during strokes or while in remote hospital intensive care units (ICUs) has evolved and been in use for several years. But it doesn’t stop there. Several subspecialties have begun to experiment with remote patient evaluation and treatment, though the numbers are low. Even in medical fields such as general surgery, pediatric surgery and, yes, vascular surgery, the use of telemedicine visits for certain patient encounters like second opinions, postoperative and annual surveillance visits has gained attention. This is my experience.
Opportunities in crisis
The onset of the COVID-19 era has changed the virtual landscape overnight. Social distancing while maintaining social contact has become the norm from a public health and personal safety perspective. I practice vascular surgery in the Yale New Haven Health System (YNHHS). Coincidentally, I had been interested in and had begun establishing telemedicine in my practice several months before the COVID-19 crisis. This stems from the fact some of my practice is in a community/rural setting, and patients often must travel longer distances to get to the office. To address this, I wanted to establish a general vascular surgery telemedicine platform to facilitate patient care and gain direct experience on its feasibility.
Leverage infrastructure
While the infrastructure for telemedicine was already in place, provided by the electronic medical record (EMR) system used at YNHHS, establishing this service for my practice was an undertaking that took time and effort. But when the COVID-19 crisis hit the U.S in March, the health systems had to respond quickly. As part of this response, the existing Telehealth Center at YNHHS established a Telehealth Conversion Center, offering guidance for a fast and effective transition to remote care for qualifying patients. As mentioned, the infrastructure for telemedicine was present, but the patients had to be signed up for the platform, which provides access to medical records and enables a conversation via email
By the end of March, more than 80% of all patients in the YNHH system were signed up, dwarfing the previous number of enrolled patients. While this was an incredible achievement, several challenges were brought upon individual physician practices. Upcoming office visits had to be screened by the physician to determine which ones could be transitioned to a video or phone visit. Next, a medical assistant or scheduler had to check to see whether the patient was signed up for the EMR platform. They then had to make contact by phone in order to explain the change in visit type and to obtain their consent.
Providers were trained for televisits and their associated documentation and billing rules using training videos provided by the Telemedicine Conversion Center, which remained accessible for additional questions and guidance. The entire process was fast
By the end of March, more than 80% of patients in the Yale system were signed up, dwarfing the previous number of enrolled patients
or messaging with the office and the providers. This platform also gives access to video visits. In addition, patients needed to have the app for this platform installed on their smartphone in order that they be armed with the necessary technical set-up for a video visit.
Co-opt patients needs
During the first weeks, about 1,000 patients signed up daily for the EMR platform with the help of the YNHHS IT and telehealth departments.
Market success
The overall experience with Telemedicine in Vascular Surgery was positive both for providers and patients. The opportunity to have a video face-to-face meeting with their vascular surgeon during a time of lockdown and restricted access to healthcare was appreciated by patients and their families, and hope for future telemedicine opportunities was expressed.
Before COVID-19, we had started a collaboration with UT San Antonio and UT Houston to establish telemedicine services for hemodialysis patients. One specified goal was to perform the initial patient evaluation via a televisit. During this, the patient’s history, arteriovenous access options and possible contraindications to surgery would be evaluated. The patient would then be scheduled for access creation. On the day of surgery, a physical exam, vein mapping and additional ultrasound evaluation would be performed. Surgical plans could be adjusted accordingly.
Ride the wave
and efficient and, within a few days, somewhere in the region of 2,000 televisits were being performed daily throughout the system.
The transition of regular office visits to televisits in the division of vascular surgery was discussed early during the hospital system’s telehealth conversion efforts. While several mostly justified concerns were expressed, providers generally moved toward telehealth visits in a quite rapid fashion. And very soon, all faculty had converted.
The COVID-19 situation has converted this possible scenario into reality as some initial televisits have already occurred. After the lifting of hospital restrictions on semi-elective surgery, the first arteriovenous access procedures were scheduled and performed. While this approach was developed before the current crisis, it will certainly be continued with the goal of assessing its long-term feasibility. Our goal is to alleviate the burden of innumerable office visits, hemodialysis sessions and hospitalizations for this population. We plan to report our experience during the COVID-19 era and beyond. As is true for other medical subspecialties, telemedicine should be considered a standard part of practice for vascular surgeons. Clearly, certain visit types can be performed safely and efficiently using telemedicine. Especially in rural areas, the time and cost for travel to a doctor’s office can be a significant burden on patients and their relatives. We should all endeavor to decrease these burdens for our patients. By using the telehealth technology that is now widely available, we have the ability to try. After all, if it’s safe, and the right thing, it should be doable.
Uwe Fischer is an assistant professor of surgery in the vascular division at Yale College of Medicine in New Haven, Connecticut.
Call to arms: Prising back control of healthcare into hands of doctors
BY ARTHUR E. PALAMARA, MD
The Journal of the American Medical Association (JAMA) carried an editorial April 20 saluting the healthcare heroes of the COVID-19 pandemic. It relayed a story of an Italian anesthesiologist who described the early days in Lombardy, Italy, and “galvanized the world to prepare for the tsunami…to come.” In fact, anesthesiologists look into the throats of mortally ill coronavirus patients who potentially spew virus-laden droplets as endotracheal tubes are inserted into their windpipes. While anesthesiologists wear protective equipment, it is not a guarantee of their safety. Many of them have died.
Coincidentally, on April 20, Bloomberg News published a story describing buyout firm KKR & Co. and the medical firm it backs, Envision, one of the largest physician staffing companies in the United States: It was considering plans to file for bankruptcy. KKR completed a leveraged buy-out of Envision in 2018, a company that employs a large number of anesthesiologists and radiologists. Envision’s debt of $1.23 billion has been trading at deeply reduced levels, about 30 cents on the dollar. Because of the pandemic and reduced outpatient/elective surgeries, Envision’s business is down about 70%. KKR agreed to buy Envision for $9.9 billion. Envison’s assets represent little more than an assemblage of physician contracts protected by restrictive covenants. Of course, like all good businesses experiencing declining revenue, they appealed to the federal government for a bailout under the CARES Act. Doctors and patients alike will suffer the deleterious effects of this bankruptcy. Highly skilled physicians were obligated by Envision to accept a “hold back” of a third of their 2019 salary. It was to be paid as a bonus on March 30 this year. That “bonus” was canceled. Further, they are required to accept an indefinite 30% reduction in their salary. How have medical professionals been subjected to the vagaries of Wall Street? Many years ago, senior members of a South Florida-based group of anesthesiologists had larger ambitions. They sold their group to investors, then later repurchased the stock. This was done several times until they were purchased by AMSURG, later Envision, now KKR. Colleagues were sold out.
CALLED
While many lay persons may consider physicians interchangeable, reality suggests otherwise. Some doctors are better trained. Some are smarter. And some just work harder. Two examples spring to mind. The first is the pediatric cardiac anesthesiologist with years of advanced training who is called in the early morning hours to provide support for the pediatric cardiac transplant team on a precariously ill child about to undergo a heart transplant. This doctor comes and spends long, tedious hours providing care without thought of reimbursement. Or the interventional radiologist who places a catheter into a remote, microscopic bleeding intestinal artery, expertly plugging it and preventing the patient from hemorrhaging to death. This, too, is done without thought of reimbursement. We go because we are called.
Arthur
But anesthesia and surgical teams are like a finely tuned orchestra: They function well when they interact together for long periods of time. Verbal communication is unnecessary since each component has their role deeply embedded. When Wall Street disrupts this harmony, patients suffer—an outcome that is neither socially nor morally acceptable. These physicians deserve to be compensated for their many (>12) years of training, skill and dedication. Our educational system requires almost all of them to borrow more than $250,000 to pay for their education. Not to mention the usurious loan rates (7.5%) for student loans grossly exceeding the Federal Fund Rate at which banks are able to borrow money.
What do these hedge fund managers actually contribute to healthcare?
What do these hedge fund managers actually contribute to healthcare? Precious little. The answer lies in the fact that healthcare has taken over roughly 20% of our gross national product—about $3.5 trillion a year. It's too much for speculators to ignore. Market evolution has spawned four large insurance companies, physician staffing companies, pharmaceutical giants and enormous hospital systems that do battle with each other to maximize revenue. The result has been unaffordable patient costs, with per capita spending twice that of any other developed nation. Yet, by some measures, we rank 29th in outcomes.
DIVERGENCE
Which leads to an inescapable conclusion: Capitalism and the profession of medicine have differing goals. Capitalism/Wall Street exist for profitability. That is not necessarily a bad thing. Although it has warts, capitalism is better than any other economic system. But is has winners and losers. In economics, the losers declare bankruptcy and start again. In medicine, the losers die. If the goal of placing the patient at the center
of our focus is abandoned, the patient becomes the unwitting victim of high cost and diminishing skill. The patient—inevitably all of us—has the understandable desire to get better, not to be overly concerned about cost. As insurance premiums have reached unaffordable levels, patients are asked to pay more deductibles and co-pays, while a greater portion of their wages are diverted to pay for employer sponsored insurance.
What we are expressing here is concern about guaranteeing that skilled physicians are compensated relative to their training and effort. It is about freeing doctors from the penury of Wall Street overseers whose presence yield little but have the capacity to inflict great damage.
Why have hospitals preferred to deal with large corporations employing anesthesiologists, radiologists, hospitalists and emergency room doctors? Perhaps doctors found it necessary to retreat into big groups to give themselves greater negotiating power with large insurers. Perhaps administrators find it easier negotiating with corporations who speak the language of contracts and avoid the messy tedium of patient care. Healthcare is intensely personal. What can be more personal than a physician placing a very sharp knife on a patient’s body? Or the expectation that the guy who puts a tube into your windpipe also knows when to take it out, managing the medical complications in between. These are concepts unlikely to be deliberated in a board room.
PYRAMID
The COVID-19 pandemic will likely compel the nation to examine the fundamentals of healthcare, which currently appear to be controlled by corporate interests. Doctors have lost or abandoned their leadership responsibilities even when our participation is necessary. Nationally, this pandemic has placed epidemiologists temporarily atop the leadership pyramid since government has made a mess of it. The closure of the economy will likely enable physicians to exert more influence as patients find themselves unable to afford health insurance premiums but still require care.
As the saying goes: Within every crisis lies an opportunity. The opportunity for physicians to exert leadership is there for the taking. The failure of Envision/KKR and the potential for substandard care afford the American Medical Association, and state and county medical associations the chance to assume leadership. In the past, organized medicine has done precious little for employed physicians. These organizations have strenuously avoided anything that seemed even remotely critical of corporate plutocrats. Perhaps it is not too late for them to help these doctors.
In the meantime, affected hospital administrators should consider declaring a breach of contract and hire these doctors lest they slowly wander off to greener pastures. It is hard to assemble a championship basketball team or a great orchestra. It would be a shame if this expertise were eroded, and with it the institutions’ ambition for excellence.
Arthur E. Palamara
is a vascular surgeon in Hollywood, Florida, and is associated with Memorial Regional Hospital.
E. Palamara
Double whammy: Pair of Annual Business Meetings slated for 2020
BY BETH BALES
In a year full of changes, the SVS Annual Business Meeting is changing, too, with two separate virtual meetings scheduled for 2020 instead of one live event.
The sessions are set for 2 to 3 p.m. CDT, on Monday, June 15, and Saturday, June 20. All members are invited. Only Active and Senior members in good standing may vote.
At the June 15 meeting, members will vote on bylaw amendments that have been proposed, and are strongly supported by, the SVS Executive Board and Strategic Board of Directors (SBOD). Developed with the intent of enfranchising all qualified members to have a vote in their governance, the bylaw amendments would permit officer elections via online voting and institute the standard of offering voting members a choice of candidates for each open position.
Following the vote on the amendments, the SVS Nominating Committee will introduce vetted candidates for vice president and treasurer, two for each position. That, too, is a modification from years in which one candidate per position was typically presented. Online voting by itself “would be a hollow act if members were not given a choice of candidates to vote for,” said Kim Hodgson, MD, the SVS president.
Information about the candidates, including a picture and written responses to questions from the Nominating Committee, will be made available to the membership to guide them in their subsequent voting. Time to consider the candidate information is built into the election timeline.
The bylaw amendments will need to be approved by a two-thirds majority of members present at the June 15 meeting. If ratified, they will become effective immediately.
Once the bylaw amendments are approved, all Active and Senior members will be able to vote electronically in a secured voting system for vice president and treasurer.
This will occur over the following five days. Results will then be announced at the June 20 meeting.
In the very unlikely event that the amendments are not approved, the election of officers will be held in accordance with existing bylaws on June 20. This vote would be restricted to those both eligible to vote and present at the meeting on June 20.
These proposed changes reflect one of Hodgson’s first initiatives as president. “My belief is that we need to enfranchise all SVS members to vote in our elections, whether they can be present at the Annual Business Meeting or not, by allowing online voting,” he said.
SVS Foundation report
Elections are not the only items on the agendas for the meetings.
At the June 15 meeting, members will hear the SVS Foundation report and about its achievements and successes.
On June 20, members will hear updates from officers, recognize the achievements of the Journal of Vascular Surgery publications and witness the virtual passing of the presidential gavel from Kim Hodgson, MD, to Ronald Dalman, MD, as the new SVS President.
To attend the two Annual Business Meetings, members must register for SVS ONLINE: "New Advances and Discoveries in Vascular Surgery." They can do so by selecting both meeting events.
The meetings are free. Visit vsweb.org/SVS-Online in order to register.
JVS produces collection on COVID-19, vascular care
BY BETH BALES
THE JOURNAL OF VASCULAR Surgery (JVS) has introduced the COVID-19 Collection, a compilation of fast-tracked articles designed to proactively provide solutions to deliver the best care in the current COVID-19 environment. JVS has dramatically shifted communication with vascular surgeons and vascular specialists to determine ways to prevent spread of the infection, improve treatment of infected patients with co-existing vascular disease, and save the lives of both patients and healthcare professionals. The JVS COVID-19 Collection is free to access and available at vsweb.org/ COVIDCollection.
“The JVS welcomes reports on personal and institutional experiences on how to improve vascular disease management while protecting our patients and the vascular care-givers during this crisis,” said Peter Gloviczki, MD, editor-in-chief of the JVS publications.
“The series of articles is designed to collectively share best practices and communication among vascular health experts for delivering the highest quality care.”
Topics in the growing collection of informative articles include telemedicine, practice changes and the impact of treating patients with vascular health conditions and COVID-19 in areas across the world.
More than 35 articles have been fast-tracked and published to date, including “Delivering high-quality vascular care via telehealth during the COVID-19 pandemic,” a discussion of the sweeping changes to the delivery of healthcare throughout the U.S. and other parts of the world.
Both the Executive Board and the SBOD enthusiastically embraced the initiative, as did members, who made it a top 10 priority in a poll in January. The original plan was to vote on the bylaw changes in 2020 and implement the new process in 2021, Hodgson said. “Then came COVID-19 and the need to pivot.”
Hodgson—along with members of the Executive Board and SBOD—believes members will champion having an enhanced voice in officer selections. “This is a new and exciting chapter of the SVS’ future,” said Hodgson.
Going forward, online voting will be held prior to the Vascular Annual Meeting (VAM), with the winners to be announced at the Annual Business Meeting during VAM.
The full collection is at vsweb.org/COVIDCollection. To access COVID-19 resources for vascular health experts visit vsweb.org/C19Resources.
Coding event set to take place Sept. 25–26
BY BRYAN KAY
REGISTRATION HAS opened for 2020 iteration of the Society for Vascular Surgery’s Coding and Reimbursement Workshop scheduled to take place from Sept. 25–26. Though it remains scheduled as a live event at the Hyatt Rosemont Hotel in Rosemont, Illinois, the SVS is considering adjusting delivery to include a virtual component if local or national restrictions on live gatherings are in effect in September.
The workshop will cover a range of coding and reimbursement updates, including changes to endovascular stent placement outside the lower extremity and Physician Quality Reporting System (PQRS), as well as coding for intravascular embolization and retrograde intrathoracic carotid stenting. Program faculty include Sean P. Roddy, MD, professor of surgery at Albany Medical College and chief of vascular surgery at Ellis Hospital in Schenectady, New York, and Teri Romano, BSN, of Karen Zupko & Associates, a speaker and consultant in coding and reimbursement. Questions can be sent to education@vascularsociety.org. Precise times are Friday, Sept. 25, from 1 p.m. to 5 p.m. and Saturday, Sept. 26, from 7:30 a.m. to 4:30 p.m., both CDT.
Advocating for our members
BY ALI RIZVI, MD, SHERENE SHALHUB, MD, AND MEGAN TRACCI, MD
COVID-19 has altered almost all of our lives to a degree previously unimaginable. Millions of Americans continue to lose their jobs, hundreds of thousands have contracted the disease and thousands have succumbed to this virus. In hard-hit states such as New York, the governor starts each day with an enumeration of these figures. At the same time, surgeons and their patients face great uncertainty, both clinically and financially, as normal operations have slowed to a near standstill and in most parts of the country are just taking the first steps on the path forward to re-opening.
THE ANONYMOUS COVID-19 pandemic practice, anxiety, coping and support survey for vascular surgeons demonstrated that 75% of respondents in practice in the United States noted that financial concerns were a source of COVID-19related stress during the period of April 14–24. The Society for Vascular Surgery Wellness Task Force sponsored the survey.
Congress and the Centers for Medicare and Medicaid Services (CMS) have acted on many fronts to provide support for physicians and practices. The Coronavirus Aid, Relief, and Economic Security (CARES) Act was intended to inject roughly $2.2 trillion into the economy through creating initiatives such as loans through the Paycheck Protection Program (PPP) and grants through the Provider Relief Fund; or enhancing existing programs, such as the Economic Impact Disaster Loan (EIDL) program, or the Medicare Accelerated and Advanced Payment Program. In response to the challenges and concerns expressed by SVS members, the Society and volunteer surgeons and professional staff continue invaluable work advocating for the financial stability of our specialty and the resources we will need to
VESAP5 to debut this summer
BY BETH BALES
The fifth edition of the Vascular Educational Self-Assessment Program (VESAP), with a substantially enlarged section on vascular ultrasound and imaging, is expected to be introduced by Aug. 1. VESAP4 will expire on July 31.
Several changes and additions, not to mention the current travel situation, make VESAP5 valuable and set it apart from earlier versions.
These include a vastly expanded section for diagnostics and imaging, available as a separate purchase, which when successfully passed,
take care of our patients going forward. Service continues, with new town halls and regular updates. In addition, the SVS is a key participant in the newly formed Surgical Care Coalition, tasked with communicating our needs and concerns to Congress and the administration on behalf of vascular surgeons. The coalition specifically will demonstrate how the current COVID-19 crisis frames the urgent need to address the future of the conversion factor and the Physician Fee Schedule. This newly formed coalition will also work in
In this time of worsening revenue shortages due to deferred visits and procedures, the additional financial strain these cuts would impose on vascular surgery practices is unsustainable
satisfies the three-year CME requirement of American Registry for Diagnostic Medical Sonography (ARDMS) to maintain Registered Physician in Vascular Interpretation (RPVI) certification. There also are topics that align with VSCORE (the SCORE curriculum specific for vascular surgery training programs and followed by the Vascular Surgery Board).
VESAP5 covers 13 topic areas important for vascular surgeons, including the four vascular lab modules.
“VESAP5 will be useful in providing innovative and effective education through all career phases, from trainee to senior vascular surgeon,” said Amy Reed, MD, co-editor. She coedited VESAP4 with Gregory Modrall, MD.
More than 97% of the questions are new. “Consequently, they are based on current practice, trends and guidelines,” she said. “In addition, each section covers all the relevant areas that one would need to study
concert with the longtime Surgical Specialty Coalition to help build understanding among both policymakers and the public of the critical importance of what we do and the need to address the fee schedule cuts proposed to begin Jan. 1, 2021.
This will be a large task and a critical one moving forward. At this moment, the SVS and the Surgical Care Coalition are starting the process of gathering data on the impact of COVID-19 in order to develop messaging. We will also be coordinating grassroots efforts to convey to Congress the need to avoid these scheduled cuts to payment for our services. Briefly, the Medicare Physician Fee Schedule for CY 2020 included broad changes to evaluation and management (E/M) services in the clinic. Due to physician fee schedule constraints requiring budget neutrality, increased overall payments to primary care for E/M services will have to be offset by deep cuts to non-E/M services. In this time of worsening revenue shortages due to deferred visits and procedures, the additional financial strain these cuts would impose on vascular surgery practices is unsustainable.
We may ask for your help—such as to describe how your practice has been impacted or to help deliver the message to our leaders and the public. Please answer the call when you are asked by engaging in grassroots efforts to communicate with legislators on the SVS “Contact Congress” page. SVS will be sending out grassroots activations over the summer. Also, please consider supporting the SVS Political Action Committee, whose work has never been more important.
Ali Rizvi, Sherene Shalhub and Megan Tracci are members of the SVS Government Relations Committee.
to prepare for any exam or recertification or to enhance one’s own knowledge. And it’s been structured in accordance with the VSCORE topics.”
The program also is an important source of continuing medical education (CME) credits, the doctors said. “It’s going to be a while before our surgeons can obtain CMEs in person,” said Reed. “Travel has become difficult, if not restricted entirely,” said Modrall. “Between that, restricted reimbursements and the limited funds now available for CMErelated travel, VESAP5 is an excellent way to get your CMEs.”
VESAP5 Vascular Lab, which includes the four lab modules, includes 200 questions and offers 30 CME credits. VESAP5 includes both a learning and an exam mode. Owners can use learning mode to practice and can view the correct answer to questions, as well as the rationale and references. Exam mode is used for taking the exams themselves, as well as earning credits.
Meanwhile, the vascular diagnostics section, produced in cooperation with the Society for Vascular Ultrasound, can “serve as an excellent study guide for the RPVI (Registered Physician in Vascular Interpretation) exam,” according to Reed.
“It is considerably more comprehensive, with more extensive material than in past versions of VESAP,” said Modrall.
The program is valuable not only for those preparing for the RPVI exam, but also for other specialists who require imaging CMEs for continued RPVI certification, he said. “CMEs specific to ultrasound are often difficult to find and access,” he said.
VESAP5 will expire three years after its introduction. As Vascular Specialist noted in May, VESAP5 will include a companion mobile app (for Apple devices only) for offline use that syncs with the desktop version when internet connection returns. For more information, visit vsweb. org/VESAP.
To drain or not to drain? That is the question
BY GUSTAVO S. ODERICH, MD, AND EMANUEL R. TENORIO, MD
Improvements in techniques of distal organ protection decreased the risk of spinal cord injuries (SCIs) from 30% to <5% with open repair of extent I-II thoracoabdominal aortic aneurysms (TAAAs).1-4 Cerebrospinal fluid (CSF) drainage has been widely accepted as one of the most important prophylactic measures to reduce the risk of SCI during both open and endovascular TAAA repair.5 The evidence for using CSF drainage is from small prospective randomized trials published two decades ago.6, 7 The first study by Crawford and associates in 1991 randomized 98 patients treated by open extent I-II TAAA repair to CSF drainage or no drainage. The maximum volume of drainage was 50ml and was discontinued at the end of the operation. There was no difference in the rate of SCI, which was exceptionally high with (30%) or without (33%) drainage.7 Subsequently, Coselli et al reported a landmark study on 145 patients with extent I-II TAAAs who were randomized to CSF drainage in 76 patients, or no drainage in 69 patients. In that study, drainage was more liberal, averaging 65ml intraoperatively and 260ml postoperatively. The rate of SCI was reduced from 13% without drainage to 2.6% with drainage.6
Since Coselli’s randomized study, CSF drainage has been assumed the gold standard both for open and endovascular TAAA repair. However, this study was never reproduced for endovascular therapy. There is no level I data to support use of CSF drainage for endovascular therapy. Interestingly, Coselli and associates recently reported an updated experience with open repair of 1,114 patients with extent II TAAA. SCI occurred in 15% of all patients, with similar rates with or without drainage. The 15% rate of SCI was nearly identical to the 13% rate observed without drainage.6
The rationale for using CSF drainage is to reduce CSF pressure in order to optimize spinal cord perfusion pressure. Because of the associated edema that follows ischemic injury to the cord, no one argues that CSF drainage is essential to treat SCI. Despite the widespread use of CSF drainage in most reports dealing with fenestrated-branched endovascular aortic repair (FB-EVAR), the rate of SCI has been inconsistent, ranging from 2% to 50%. Paraplegia has been reported in 0% to 29% of patients.5 There are many reasons for the discrepancy in results. First, not all studies have stratified the risk of SCI by aneurysm extent, often mixing lower risk (extent IV TAAA) with higher risk groups (extent I-III TAAA). Second, endpoints are not uniformly defined. Some studies use SCI as any multifactorial lower extremity weakness, while others specify paraparesis and/or paraplegia. Lastly, investigators tend to compare their strategies to prevent SCI, which have been perfected in late experiences,
with the outcomes of patients treated without these strategies in their earlier experiences. As such, studies are plagued by learning curve biases. Therefore, for the most part the recommendations by leading investigators to prevent SCI during FB-EVAR are based on flawed studies We have used a “belt and suspenders” approach to SCI prevention, such as staging of extent I-II TAAAs,
232 patients treated by FB-EVAR using a standardized SCI prevention protocol. The risk of any SCI was 1% for pararenal, 0% for extent IV TAAA, 13% for extent III TAAA and 10% for extent I-II TAAA. Permanent paraplegia occurred in 2% of patients with extent I-II TAAAs. There were no cases of permanent paraplegia among extent III and IV TAAAs. A disappointing finding of the study
There is no question that CSF drains are of paramount importance to treat SCI. No one would argue with that. But do we need to use them prophylactically?
routine prophylactic CSF drainage, permissive hypertension, early limb reperfusion, neuromonitoring and selective temporary aneurysm sac perfusion (TAS). Tenorio and associates presented the results of this protocol at the annual meeting of the European Society for Vascular Surgery in 2018. The study included
was that two of 10 patients (20%) with SCIs had lesions caused by spinal hematomas caused by CSF drain placement. This report led us to conduct a taskforce to review the CSF drain practices and outcomes.8 Kärkkäinen and associates reported the results of this review, which included 187 patients and
240 endovascular procedures with CSF drainage. Of these, 21 patients (10%) sustained any CSF drainrelated complication.9 The risk of complication was identical to the 10% rate reported by Rong et al in a systematic review of 4,717 patients treated by 6,593 endovascular aortic procedures.10 In our report, severe complications occurred in eight patients (4%), including spinal hematomas in six patients (3%) and intracranial hemorrhage in three (1.5%). There was death caused by intra-cranial hypotension and hemorrhage due to inadvertent drain disconnection. There were a number of other problems, including case cancellations from bloody drainage, drain fracture, CSF leakage, severe headaches and blood patches. Length of stay in the intensive care unit and hospital were prolonged with CSF drainage. One out of three patients (four of 13) with SCI had spinal hematomas.9 Since that report, we changed our practice to avoid any prophylactic drainage during first stage TEVAR and FB-EVAR, including patients with extent I-II TAAAs. Instead, we recommend using therapeutic drainage for patients who develop symptoms of SCI. But is this approach of rescue drainage safe and effective? What is the risk of SCI without drainage? And how often can we actually rescue symptoms? There is limited data on endovascular repair of extent I-II TAAAs without prophylactic CSF drainage. Bidas and associates reported 142 patients treated for TAAAs, including 88% with extent II or III TAAAs. Prophylactic drainage was used in the first 78 patients, but was discontinued due to a 6% rate of severe complications. After that, 64 patients had repair without prophylactic drainage. Of these, 12 patients (18%) required rescue drainage without drainrelated complications. The risk of permanent paraplegia was 2.5% with prophylactic drainage and 1.5% with rescue drainage strategy.11 Adams and colleagues, reported on 270 consecutive patients treated by FBEVAR. Their 30-day mortality of 0.4% is the lowest ever reported. Patients had no prophylactic CSF drainage and permanent paraplegia occurred in 2% of the entire cohort and 4% of patients with extent I-III TAAAs.3 The rationale for prophylactic drainage relies on the premise that CSF drains help prevent the injury and help decrease the risk of secondary injury by optimizing spinal cord perfusion pressure. It also assumes
Gustavo S. Oderich
Emanuel R. Tenorio
Patient with epidural hematoma
that placement of CSF drains is safer before the operation starts, and may be potentially dangerous after the operation because of coagulopathy or difficult spinal anatomy, which may increase the risk of complications or even prevent its placement. Nonetheless, there are many cons to be considered. First, evidence shows that CSF drains are probably unnecessary in at least 80–90% of patients who would otherwise never develop SCI symptoms. These patients are being exposed to unnecessary risks. Second, not all drains actually function. Alqaim and associates reported non-functionality in 16% of patients who received prophylactic drainage.12 Third, SCIs can still occur with CSF drainage and in many cases does not improve at all with functioning drains. Fourth, complications from CSF drains are significant when we consider that the margin for expected complications is low. One in 10 patients have some complication, and one of three with SCIs have spinal hematomas from the drain. Finally, drains are frequently a
cause of significant discomfort.
There is no question that CSF drains are of paramount importance to treat SCI. No one would argue with that. But do we need to use them prophylactically? The rationale for an approach that applies only to therapeutic or rescue drainage is based on the premise that CSF drains can still be placed after the operation and can still effectively improve SCI. This premise assumes that placement of CSF drains after the operation is nearly always possible, it is safe and that it improve symptoms. Rescue drainage avoids all the unnecessary drains in those 80–90% of patients who would otherwise have an uncomplicated course. However, this approach has potential limitations. Patients need to have a normal coagulation profile following the operation, for instance. What remains to be answered is how often CSF drains are not able to be placed and how often rescue drainage is not effective. It seems from preliminary data that the number of patients in whom rescue drains are not able to be
5. Dijkstra M.L., Vainas T., Zeebregts C.J., Hooft L., van der Laan M.J. Editor's Choice–Spinal cord ischaemia in endovascular thoracic and thoracoabdominal aortic repair: review of preventive strategies. European Journal of Vascular and Endovascular Surgery 2018;55(6):829-41.
7. Crawford E.S., Svensson L.G., Hess K.R., Shenaq S.S., Coselli J.S., Safi H.J., et al. A prospective randomized study of cerebrospinal fluid drainage to prevent paraplegia after high-risk surgery on the thoracoabdominal aorta. J Vasc Surg 1991;13(1):36-45; discussion -6.
8. Tenorio E.R., Oderich G.S., Kärkkäinen J.M., Mendes B.C., Hofer J., Wigham J., et al. Prospective Assessment of a Protocol using Neuromonitoring, Early Limb Reperfusion and Selective Temporary Aneurysm Sac Perfusion to Prevent Spinal Cord Injury During Fenestrated-branched Endovascular Aortic Repair. European Journal of Vascular and Endovascular Surgery. 2019;58(6):e364-e5.
9. Karkkainen J.M., Cirillo-Penn N.C., Sen I., Tenorio E.R., Mauermann W.J., Gilkey G.D., et al. Cerebrospinal fluid drainage complications during first stage and completion fenestrated-branched endovascular aortic repair. J Vasc Surg 2020;71(4):1109-18.e2.
placed is small, and that most are still effective. The final answer will come from a prospective randomized trial.
References
1. Coselli J.S., LeMaire S.A., Preventza O., de la Cruz K.I., Cooley D.A., Price M.D., et al. Outcomes of 3309 thoracoabdominal aortic aneurysm repairs. J Thorac Cardiovasc Surg. 2016;151(5):1323-37.
2. Coselli J.S., Green S.Y., Price M.D., Zhang Q., Preventza O., de la Cruz K.I., et al Spinal cord deficit after 1114 extent II open thoracoabdominal aortic aneurysm repairs. J Thorac Cardiovasc Surg. 2019.
3. Juszczak M.T., Murray A., Koutsoumpelis A., Vezzosi M., Mascaro J., Claridge M., et al. Elective Fenestrated and Branched Endovascular Thoraco-abdominal Aortic Repair with Supracoeliac Sealing Zones and without Prophylactic Cerebrospinal Fluid Drainage: Early and Medium-term Outcomes. Eur J Vasc Endovasc Surg 2019;57(5):639-48.
4. Eagleton M.J., Follansbee M., Wolski K., Mastracci T., Kuramochi Y. Fenestrated and branched endovascular aneurysm repair outcomes for type II and III thoracoabdominal aortic aneurysms. Journal of Vascular Surgery 2016;63(4):930-42.
10. Rong L., Kamel M., Rahouma M., White R., Lichtman A., Pryor K., et al. Cerebrospinal-fluid drain-related complications in patients undergoing open and endovascular repairs of thoracic and thoraco-abdominal aortic pathologies: a systematic review and meta-analysis. British Journal of Anaesthesia. 2018;120(5):904-13.
11. Bisdas T., Panuccio G., Sugimoto M., Torsello G., Austermann M. Risk factors for spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. J Vasc Surg 2015;61(6):1408-16.
12. Alqaim M., Cosar E., Crawford A.S., Robichaud D.I., Walz J.M., Schanzer A., et al. Lumbar drain complications in patients undergoing fenestrated or branched endovascular aortic aneurysm repair: Development of an institutional protocol for lumbar drain management. Journal of Vascular Surgery. 2020.
Gustavo S. Oderich is professor of surgery and chair in the division of vascular and endovascular surgery at the Mayo Clinic in Rochester, Minnesota.
Emanuel R. Tenorio is an advanced endovascular aortic research fellow at the same institution.
‘Risk
prediction models can be used for targeted screening for asymptomatic carotid stenosis,’ researchers find
BY BRYAN KAY
MOST PREDICTION MODELS can “reliably” identify individuals at high risk of significant asymptomatic carotid stenosis (ACS), a new study shows.
Michael H. F. Poorthuis, MD, of the Clinical Trial Service Unit and Epidemiological Studies Unit in the Nuffield Department of Population Health at the University of Oxford, U.K., et al made the discovery in a systematic review and data validation that drew on more than half a million individuals who attended commercial vascular screening clinics in both the U.K. and U.S.
Furthermore, the best‐performing prediction models identified over one third of all cases by targeted screening of individuals in the highest decile of risk only, the researchers found.
The findings were published in the Journal of the American Heart Association
In introducing their rationale, the authors noted that ischemic stroke is the first presentation of cardiovascular disease in about 25% of cases, with 15–20% of ischemic stroke cases are associated with extracranial carotid artery stenosis. The prevalence of moderate (≥50%) and severe (≥70%) ACS in the general population has been estimated to be 2% and 0.5%, respectively, they pointed out.
“Because of this low overall prevalence, population‐level screening for ACS with duplex ultrasound is not recommended in current
guidelines,” Poorthuis et al wrote. “However, targeted screening of high‐risk individuals might be worthwhile, and risk stratification tools or prediction models have been developed to provide individualized risk estimation for ACS. Before recommending targeted screening, risk prediction tools should be assessed for discrimination, calibration and likely ability to detect false‐positive and false‐negative cases in an independent external population.”
The systematic review included studies that addressed development and/or validation of diagnostic prediction models to detect ACS of 50% or greater and assessed prediction models in both general and high‐risk populations but not in diseased populations at higher risk of ACS, the authors added.
Registry launches pair of studies on vascular complications related to COVID-19
BY BRYAN KAY
The new Vascular Surgery
COVID-19 Collaborative (VASCC) is ready to start collecting data on two projects.
The first study to emerge from the international registry, entitled “Impact of COVID-19 on scheduled vascular operations,” covers five major areas of vascular practice and conditions to include carotid, aortic, peripheral, venous and hemodialysis modules. The second, called “Thrombotic complications of COVID-19,” is investigating the virus’ connections to acute limb ischemia, acute mesenteric ischemia, stroke and symptomatic venous thromboembolism.
The main goal of the first project centers on the question: What is happening to the patients who have had their surgeries delayed?
“The primary aim is to collect deidentified data on the natural history of patients who did not undergo their scheduled surgery due to COVID-19, focusing on specific conditions where researchers expect delays to have the highest impact,” Max Wohlauer, MD—one of the surgeons involved in getting the registry up and running— tells Vascular Specialist.
“What impact is the delay in care having on patients with symptomatic carotid stenosis, or chronic limbthreatening ischemia? What happens to a patient with a 7cm abdominal
Some 975 studies were reviewed, with sic prediction models identified—three each for moderate and severe ACS.
Validation utilized data from 596,469 individuals. Discrimination and calibration were assessed.
“In the validation cohort, 11,178 (1.87%) participants had ≥50% ACS and 2,033 (0.34%) had ≥70% ACS,” the investigators continued. “The best model included age, sex, smoking, hypertension, hypercholesterolemia, diabetes mellitus, vascular and cerebrovascular disease, measured blood pressure, and blood lipids. The area under the receiver operating characteristic curve for this model was 0.75 (95% CI, 0.74–0.75) for ≥50% ACS and 0.78 (95% CI, 0.77–0.79) for ≥70% ACS. The prevalence of ≥50% ACS in the highest decile of risk was 6.51%, and 1.42% for ≥70% ACS. Targeted screening of the 10% highest risk identified 35% of cases with ≥50% ACS and 42% of cases with ≥70% ACS.”
Elaborating on their findings, the authors concluded “the present study showed that most prediction models had modest discrimination but could reliably identify a cohort of cases at high risk of ACS.”
Further, they wrote: “The prevalence of ACS in the decile(s) at highest predicted risk of ACS was considerably higher than the overall prevalence, thereby substantially reducing the number of individuals needed to screen to detect ACS. Further research should determine the optimum thresholds required for a targeted screening by considering the number needed to screen, the diagnostic yield, the absolute reduction of stroke risk by prophylactic treatment, and cost‐effectiveness of different approaches.”
SOURCE: DOI.ORG/10.1161/JAHA.119.014766
aortic aneurysm whose scheduled surgery was postponed due to COVID? What about 6cm? How about 8cm? What is happening with dialysis access?”
VASCC, launched in the wake of the global pandemic to leverage key data related to the virus, is encouraging trainees to participate in the research projects and will publish under a collaborative authorship model. Content experts from around the world are involved in developing the various modules for the data collection tool, explains Wohlauer,
“ VASCC is taking painstaking efforts to ask questions in a way that's comprehensive without being overwhelming” Max Wohlauer
who also is assistant professor of vascular surgery at the University of Colorado School of Medicine in Aurora.
“VASCC is taking painstaking efforts to ask the important questions and do it in a way that’s comprehensive without being overwhelming,”
Wohlauer says.
“We developed a tracking sheet— available to VASCC members—to help participants maintain a list of the patients whose surgeries were deferred.”
The investigators are seeking to establish whether COVID-19-induced halts in practice were either due to the directives from hospitals to only carry out emergent cases, self-administered or patient-driven.
“What is the impact on patients who avoid coming to the hospital out of fear of contracting the virus?” asks Wohlauer. “Eventually, when patients have their operations—did they do worse because of the delay?” he adds.
“We’re also going to look at specific things related to each disease process. Also, what did you do differently?”
Benefits of burnout: In search of the silver lining
BY DAVID RIGBERG, MD, AND KRISTYN MANNOIA, MD
As I donned my protective gear, I glanced through the glass doors into the intensive care unit. It was 5:30 a.m., and my fatigue was palpable. My thoughts were centered on the likely dismal outcome for the patient I was about to see and the implications my care plan would hold. The patient was in her 80s, admitted with devastating embolic events—including to her legs—leading to the need for my presence. She was presumed to be COVID-19 positive. Multiple healthcare providers had seen her over the previous 12 hours—nurses, emergency room doctors, technicians, and the like. Coloring my thoughts as I evaluated her legs was the question: “How many people will be exposed to her if I push forward with an intervention?”
This wasn’t the first time I had this concern. We had an active central line service at one of our hospitals, and I remember watching my fellow—a fully trained general surgeon—place a triple lumen catheter. A procedure he can do in his sleep. But this is my COVID stress. It is neither crippling or continuous, but I am distracted by a new variable in my clinical decision making – how will our course of action impact the clinicians performing it?
It took me a little time to realize this was even happening, and I am sure there are a thousand different ways we vascular surgeons are impacted during these trying times. While burnout is already a focus of concern in our specialty, the current situation is certainly making the topic much more personal for many. It is bad enough to worry about the patient, let alone our colleagues, staff and their families. For now, that is our new reality.
Admitting that the pandemic is impacting us is an important factor in dealing with this new stimulant to burnout. But at the risk of sounding like a Pollyanna, COVID could serve
as a springboard to bring things to the surface that we might not otherwise talk about. Normally taboo, or at least relegated to the “wellness curriculum,” concerns about our
isolation worsens outcomes of burnout.1, 2 Let’s keep encouraging one another, building each other up and reinforcing the good we see being done. The collaboration across states and countries to develop best practices for COVID central line services, for example, demonstrate what can happen on a regular basis in the vascular community. This is especially important to those of us in practices without supportive partners or partners at all. Imagine an Uncle Sam poster: You, there! You don’t have to navigate that HeRO (Hemodialysis Reliable Outflow) graft alone! Talk best practices on a Zoom social hour with colleagues across the country! Building on that, we should keep
Acknowledging the unique struggles that we as vascular surgeons are going through can be both the prevention and treatment of burnout
physical well-being and the mental toll our jobs take on us have become routine topics of conversation. Multiple peer support networks have arisen in which participants are near effusive with their encouragement for fellow vascular surgeons. Telemedicine has been more rapidly adopted than the time it usually takes the operating room to switch to cheaper sutures. The misery of this pandemic provides an opportunity to implement improvements to the system that otherwise might have taken decades to achieve.
For starters, let’s keep up the good work. Studies show that social
talking about how hard this is. Yes, for now “this” is all the baggage that comes with treating COVID-19 patients. And it really is hard. But next month “this” will be a marriage that is struggling, a complication after first rib resection or a lawsuit after a gut-wrenching mortality. Acknowledging the unique struggles that we as vascular surgeons are going through can be both the prevention and treatment of burnout Talking about our angst in front of trainees helps fight stigma. Openly identifying problems leads to development of solutions.
And finally, let’s identify areas
where the system desperately needs improvement. COVID is our cardiac stress test with the results for all to see. Let’s find the wall motion abnormalities and shore them up. Lousy electronic medical records (EMRs) have been shown to be a huge contributor to burnout. So tell administrators that telemedicine is the way of the future. Loss of a feeling of control is a central characteristic of burnout - how can we work to take the reins back from the midlevel managers and the insurance companies now that the world sees the sacrifices we make? And depersonalization is rampant as a coping mechanism for the stress we routinely undergo. But we should take this opportunity to re-center ourselves when the people in the COVID-19 units are inevitably our friends and family. We have a long way to go to address the burnout epidemic. But the solidarity we feel now is an impressive place to start.
References
1. Schwartz R., Shanafelt T.D., Gimmler C., Osterberg L. Developing institutional infrastructure for physician wellness: qualitative Insights from VA physicians. BMC Health Serv Res 2020;20(1):7. Published 2020 Jan 3. doi:10.1186/s12913-019-4783-9
2. Rogers E., Polonijo A.N., Carpiano R.M. Getting by with a little help from friends and colleagues: Testing how residents' social support networks affect loneliness and burnout. Can Fam Physician 2016;62(11):e677-e683.
David Rigberg is professor of surgery at the David Geffen School of Medicine at UCLA in Los Angeles and program director of its residency and fellowship in vascular surgery.
Kristyn Mannoia is assistant professor of surgery, vascular and endovascular surgery, and director of wellness for the division of vascular surgery at Loma Linda University School of Medicine in Loma Linda, California.