Southern Vascular Former president reflects

Southern Vascular Former president reflects
The case for multidisciplinary limb salvage in face of increasing diabetes, diversifying nation



BY BETH BALES
Society for Vascular Surgery (SVS) members elected Joseph Mills, MD, of Baylor College of Medicine in Houston, Texas, as their next vice president, a result announced during the Virtual Annual Business Meeting last month.
He now joins a line of succession that includes the new and incoming SVS President Ali AbuRahma, MD, and Presidentelect Michael C. Dalsing, MD,
DRAMATIC INCREASES IN RATES OF DIABETES
particularly among Black females—through 2060 underscore the importance of a multidisciplinary team approach to limb salvage, according to Vincent Rowe, MD, professor of vascular surgery and endovascular therapy in the Keck School of Medicine at the University of Southern California (USC), Los Angeles.
Rowe was speaking before the Pacific Northwest Endovascular Conference (PNEC) in Seattle during which he made the case for the multispecialty method—why it works and how other centers might go about embracing it rather than fighting it. To that end, he informed the PNEC gathering (May 27–28), when he first started to talk on the topic a few years ago, his institution did not
who will follow AbuRahma in the presidential chair next year. The digitally hosted business meeting took place June 16.
Mills is chief of the division of vascular surgery and endovascular therapy at Baylor. He was previously professor and chief of vascular surgery at the University of Arizona College of Medicine and co-director of the Southern Arizona Limb Salvage Alliance (SALSA).

BY BHAGWAN SATIANI, MD
ANTHONY VALDÉS, MBA, THE PRESIDENT OF Tampa, Florida-based Collaborative Health Systems, declares that what physicians want is to “deliver great clinical outcomes, get paid fairly for that care, and stay independent.” It is becoming clearer with every passing year that, while we do, for the most part, deliver great clinical outcomes, and many physicians do not think we get paid fairly for providing that care, the hopes of remaining independent appear to be fading for many of us surgeons. And by physician independence, I am assuming that implies autonomy to make decisions in all things related to the practice of medicine.
Over time, some of us may feel we are facing up to a state of what might be called thralldom—or held in a kind of bondage-type relationship—and we are, thus, looking for other options. In general, other than to retire early, the conventional choices left to us are perhaps to remain independent within a specialty or multispecialty group; accept employment in an academic, private or government health system; choose another career; or seek out novel ways to remain in practice.
Novel options may include to stay in practice but consider non-traditional or even provocative paths. While office-based labs (OBLs) and ambulatory surgery centers (ASCs) are now mainstream, new actors are in play.
Putting the traditional deep-pocket potentates to one side, some colleagues have taken up employment with device makers, pharmaceutical companies, and even Wall Street outfits. The job may start part-time, but, if both parties are satisfied, the physician acquires some relevant new knowledge or a business degree, and then segues to
an executive role that comes fully equipped with stock options. And now there are even newer, more powerful capitalist players with deeper pockets still. Amazon, with a current market cap exceeding $1.7 trillion, is launching Amazon Care for its employees in all 50 U.S. states, hiring 3,000 new corporate types and offering virtual care just as a start. Not so long ago, the mega insurer UnitedHealth Group, which already has 30,000 employed or affiliated physicians (Optum), completed a $4.9-billion acquisition of DaVita Medical Group, which employs 13,000 physicians. It is now well on the way to becoming the largest single employer of physicians.
Probably the biggest earthquake was the entrance of private equity players. These outfits can be lucrative sources of funding whose methods involve investing institutional capital in order to purchase operating entities, as in physician practices. Our recent review of the pros, cons and risks of being part of a private equity structure is concerning.1 COVID-19 has had a deleterious effect on the number of deals in North America, with buyout volume and value both dropping in 2020, the latter by 25% to $34.7 billion from 2019. Although it is still early, employment with private equity-owned practices is the newest but untested kid on the block. Provider (oh how I abhor that term!) deals were the most frequent, falling to 52% of all deals—the relevant figure was 60% in 2019.
Growth has occurred in other sectors of healthcare: information technology, telehealth support, payors, medical technology companies, biopharma and life sciences in general, and next-generation models of care like home care. What does strike as particularly surprising

Putting the traditional deeppocket potentates to one side, some colleagues have taken up employment with device makers, pharmaceutical companies, and even Wall Street outfits
is that, in the provider area, surgical-type practices are represented in the majority (>50%). Granted, most could be classed as either ophthalmology, ear nose and throat (ENT), or dermatology, but specialty surgery practices may not be far behind. So why are private equity outfits attractive to physicians? For doctors who are either looking for an exit or not risk averse, there is an opportunity to be a participant in the private equity companies’ playbook. This means bringing in new management, creating efficiencies, offering and delivering more services, negotiating with payors for higher reimbursement, and micromanaging finances with the aim of selling the practice. This, of course, results in a share of the hefty profit yield a few years down the line. Although the
continued on page 6
VASCULAR SPECIALIST
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD, Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Marie Drudi, MD
Executive Director SVS Kenneth M. Slaw, PhD
Director of Membership, Marketing and Communications Tara J. Spiess CAE
Managing Editor SVS Beth Bales
Marketing & Membership Specialist Anna Vecchio
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA Publishing. Content for the News From SVS is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA Publishing will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein.
The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com.
For missing issue claims, e-mail subscriptions@bibamedical.com.
Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA Publishing.
Printed by Elk Grove Graphics
©Copyright 2021 by the Society for Vascular Surgery
Published by BIBA Publishing, which is a subsidiary of BIBA Medical Ltd.
Publisher Roger Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Jocelyn Hudson, Suzie Marshall, Will Date and Jamie Bell
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to
BY BRYAN KAY
The World Federation of Vascular Societies (WFVS) has entered a new era of transformation, seeking to better pave the way for disparate vascular surgeons and societies to disseminate the latest science and best practices to every corner of the globe.
In what is planned to be a two-year transitional period, the WFVS will now be housed administratively under the aegis of the Society for Vascular Surgery (SVS) and led by new SecretaryGeneral Palma Shaw, MD, the current chair of the SVS International Relations Committee.
The WFVS, currently led by Australiabased President Peter Subramaniam, MBBS, is an amalgam of membership societies from every continent, including the SVS in North America, the European Society of Vascular Surgery (ESVS) and the Asian Society for Vascular Surgery. Its core mantra involves connecting member societies in order to foster international scientific discourse, share knowledge of effective therapies and interventions, and impart developments in vascular specialist training strategies.
Previously, the federation would host an annual meeting in the home country of the reigning president, who would also assume its administrative home, with member society participants travelling from across the world to attend.
In the new era, Shaw and SVS staff will seek to establish a sustainable future for the WFVS through a fixed administrative abode as well as ongoing live meeting events housed on a digital platform. The plans are the result of a memorandum of understanding recently agreed between the WFVS, the SVS and the ESVS.
“The WFVS mantra will remain the same but this is, in fact, an evolution,” explains Shaw, a professor of surgery at the State University of New York, a member of the division of vascular surgery at Upstate Medical Center in Syracuse, New York, and also the program director of the vascular fellowship at the same institution, in an interview with Vascular Specialist Shaw was tapped for the role of secretary-general by outgoing SVS President Ronald L. Dalman, MD, and Executive Director Kenneth M. Slaw, PhD, owing to her experience on the International Relations Committee. She is believed to be the first female leader within the organization, and will be joined by Wei Zhou, MD, a professor
of surgery and the chief of the division of vascular surgery at the University of Arizona College of Medicine-Tucson, Arizona, who will be the second SVS representative to the WFVS council of officers.
The post-pandemic era of virtual meetings helped inform the need for a digital-based future for WFVS meetings, said Shaw. “We’re proposing that there is a migration from an annual WFVS live event to an ongoing digital platform,” she continues. “The support provided will be such that we will help transition the WFVS to a sustainable, virtual, digital platform, and it won’t be anticipated that members are obligated to attend live events or meetings, although we can hold live meetings if we choose to.
“Additionally, there has been this rotating administrative home housed wherever the president is, and it would change every year. It really wasn’t providing a lot of stability for this society. So, the governance and administrative home needed to be set and established. Also, they didn’t have resources, because they don’t really charge dues, with the $1,000-a-year fee for each society not really amounting to much except to support the website. We also thought the mission could be broadened.”
Governance of the WFVS will be retained by the Federation Council through its soon-to-berevised bylaws and constitution. The transformation will include a new website and the recruitment of a part- or fulltime international relations manager. Shaw will remain in post for the duration of the two-year transition, working alongside Slaw with the ultimate goal of long-term sustainability and completing the Federation’s digital re-birth.
“It’s an aggressive lift but I think it’s very exciting and very doable,” comments

Shaw, who feels particularly prepared for the secretary-general role having taken up the reins mere days after graduating with an executive MBA. “I’ve had many conversations with the existing leadership, the president, the outgoing secretarygeneral, all of the council members.”
A presidential changing-of-the-guard is due in October, and a secretary-generalelect is also in place in the form of Juan Paolini, MD, the current treasurer of the Latin American Association of Vascular Surgery. The new set-up will be reassessed in two years, with a pulse-check coming at the 2022 Vascular Annual Meeting
“We’re proposing that there is a migration from an annual WFVS live event to an ongoing digital platform” — Palma Shaw
(VAM), where a WFVS session is planned.
“The reality is, I don’t think that, even in this era, even when COVID goes away, we can go back to live meetings for the WFVS every year,” reflects Shaw. “Think about the limitations of requiring people to travel all over the world—from Australia to go to Boston, or from India to go to Australia or South America. The last in-person WFVS meeting, which I went to in 2018, was wonderful, but people had to travel from places like Australia to South America. The distances can be great.
“What we can actually do—and I really think this is the way things are going—is we use a virtual platform to hold things together, to educate and communicate to keep moving things forward, and then we have periodic in-person meetings.”
The fundaments of spreading up-todate developments in vascular science to those pockets of the globe that might not otherwise have access to the latest best practice remain at the core of WFVS, adds Shaw. “Out of this terrible pandemic, we’re going to capitalize on a lot of good things that we’ve learned to optimize our strategy, to work together in a societal way, to disseminate information to those people that have not,” she says. “There are people, for example in Africa, in the Philippines, and in other parts of the world, who don’t have the means to have the latest information. Some don’t have a society to represent them. There are people practicing vascular surgery who can’t leave where they are because they might be the only vascular specialist in the whole region. They can’t go to a vascular meeting or attend the SVS meeting to learn the latest.
“This is a collaborative effort to organize the vascular societies with resources, to reach those still developing: All of the societies, which are designed mostly by continent, and their leaders collaborate and exchange ideas so that everybody benefits—so no one continent is held back. We bring everybody together on the virtual platform, increasing our communication dramatically by doing so.”

number of practices owned by private equity players is unknown, the Medicare Payment Advisory Commission (MedPAC) estimates these entities bought at least 2% between 2013 and 2016, after which acquisitions picked up. Paul Ginsburg, MedPAC vice-chairman, recently noted: “Private equity is more aggressive. The loopholes in our payment systems will be exploited more rapidly.” Federal and state prosecutors are now investigating private equity companies over excessive loans from the Small Business Administration’s COVID-19 Paycheck Protection Program. Another new term we may become familiar with is the special purpose acquisition company (SPAC). This is another option for private equity-owned medical groups looking to exit arrangements after three-to-seven years as an alternative to an initial public offering (IPO). SPACs avoid the labor-intensive IPO process by allowing a shell
The case for multidisciplinary limb salvage in face of increasing diabetes, diversifying nation
have such a limb salvage program, leading him to declare that his talk should actually be entitled, “How we realized we needed to build one.”
An overall growth in the number of people developing diabetes looms large, explained Rowe. “We found out that we needed the program when we started seeing a lot cases such as this case here,” he said, pointing to a slide depicting major tissue damage to the foot. “These are cases of combined problems with circulation and the foot in terms of tissue loss and deep infection. The reason why we were seeing more of these things was because of the exponential growth of diabetes.”
Rowe referenced some key statistics: More than 34 million people of all ages—about one in 10—have diabetes, and 88 million adults, or one in three, have prediabetes. Diabetes complications are increasing for young adults aged 18 to 44 and middle-aged adults aged 45 to 64. Diabetes is more common among Asians, non-Hispanic Blacks, and Hispanics than non-Hispanic whites. Nearly one in five adolescents aged 12 to 18 and one in four young adults aged 19 to 34 have prediabetes
“The patients we have talked about, mainly for peripheral vascular disease, who have worse outcomes are Black and Hispanic,” Rowe continued. “We’re seeing that diabetes is more common in that group. This is not only going to increase the complexity of these patients with

corporation to take the company public. The existential question for doctors is this: How do we take control of our own destiny? Or has the horse bolted from the barn already? Are we now on the road to what Friedrich Hayek called the road to serfdom? A lot depends on how the current generation of physicians sees the security of employment in exchange for the freedom of owning their own practices. While we deal with conflicts of interest regularly, the pressure to produce is a step up from work relative value unit (wRVU)-based compensation models
The existential question for doctors is this: How do we take control of our own destiny? Or has the horse bolted from the barn already?
diabetes, but it’s going to make the overall outcomes that they have worse, because there will be more of them. It’s sort of a doubling project, where there’s going to be more patients with the problem and then more disease presence.”
Referencing sourced data, Rowe took a look at the pediatric population, explaining: “We’re dealing with a more diverse nation. The total population of people considered minorities is about 38%. But for children under five, it’s about 50%. That’s from 2014, so I’m sure that has increased. We are going to have a more diverse nation and we have to be prepared for that, especially if the diversity is involving patient groups that are at risk for diabetes. We have tracked the increase in diabetes up to 2060, and the prevalence was shown as going to increase, especially a prediction among Black females that there was going to be a huge increase, and an increase in those identified as Black males. These groups are going to be the ones we’re dealing with in terms of trying to treat their lower-extremity problems.”
The argument in favor of a limb salvage program extends to five-year mortality rates among patients who undergo a major amputation, noted Rowe. These patients are more likely to die in five years than people with a host of cancers, excluding lung cancer. “Once you deal with a patient who gets an amputation, their life expectancy goes down dramatically.”
and may be a leap too far. Are we ready for the intense probes that will surely follow? Will we be just about anyone’s chauffer? At this juncture, I would recommend reading Carl Hauser’s thought-provoking presidential address at the Western Trauma Association.2
References
1. Satiani B., Zigrang T.A., Bailey-Wheaton J.L. Should surgeons consider partnering with private equity investors? The American Journal of Surgery. 2020 Dec 19; S00029610(20)30806-0. doi: 10.1016/j.amjsurg.2020.12.028.
2. Hauser C. Ownership. J Trauma Acute Care Surg. 2017. Volume 83, Number 5
BHAGWAN SATIANI is professor emeritus in the division of vascular diseases and surgery in the College of Medicine at The Ohio State University, Columbus, Ohio. He is an associate medical editor of Vascular Specialist.
At the outset of the program at USC, the various specialties were siloed. “When we looked at things, we just saw them differently, and couldn’t agree,” he said. Then the BEST-CLI (Best endovascular vs. best surgical therapy in patients with critical limb ischemia) trial came along, highlighting the need for two different specialties to be involved with CLI patients in some of the major medical centers.

“We wanted to be a part of the trial, so in 2014 it forced myself and a cardiologist to join forces,” Rowe explained. “Since we did that, under the aegis of the trial, we began working much closer together, and doing better for our patients as a team.”

“We are going to have a more diverse nation and we have to be prepared for that, especially if the diversity is involving patient groups that are at risk for diabetes”—
Vincent Rowe

In the meantime, Rowe observed, since the turn of the century the number of publications dealing with the multidisciplinary approach to limb salvage has skyrocketed. Most of those studies show a lowering of amputation rates after the establishment of a limb salvage program, Rowe added. The USC Limb Salvage Center contains vascular surgeons,
interventional cardiology, vascular medicine, a nurse practitioner, a research coordinator, fellows from vascular surgery and vascular medicine, podiatry, plastic surgery, wound care specialists, endocrinology practitioners and nutritionists, among others. Crucial roles are played by podiatry and plastic surgery, Rowe said, along with wound care, nutrition and physical therapy. “And I don’t think we use this team enough: the endocrine specialists.” David Armstrong, DPM, co-director of the USC Limb Salvage Center, dubbed the service the “Hot Foot Line.” Patients call the line, with subsequent wounds assigned to podiatry if they bear good circulation and are mainly due to infection, and sent to vascular surgery should there be an issue with circulation. Rowe and colleagues compared patient outcomes from before the start of the program when practitioners siloed, to afterwards when they were combined into a limb preservation clinic.
“We saw benefits in the amputations rates in high amputations rates, or high up the leg, and we saw a decrease in low amputations as well. We also saw an improvement in the metric from the highto-the-low ratio.”
The USC team’s data is not yet published but Rowe and colleagues conclude that the multidisciplinary approach to limb salvage bears a number of benefits, including in amputation rates and length of stay. Rowe also touched on limitations. “One of the main ones is staffing and clinic space, as well as operating time, because we end up doing a lot of shared procedures,” he said. “I’ll do something to help the circulation, and then the podiatrist will come in and clean up a part of the foot, or do a partial foot amputation, all in the same setting, so it prolongs the operating time.”

BY BRYAN KAY
The first time Bruce A. Perler, MD, attended the Southern Association for Vascular Surgery (SAVS) annual meeting, he was a young faculty member who had already started developing the keen interest in carotid disease for which he is now well known, but otherwise a selfdescribed “nobody” in the company of greatness.
It was 1986, and he was attending an evening reception, when, from across the other side of the room, he spotted Jesse E. Thompson, MD, “the dean of carotid disease,” who, to Perler’s surprise, suddenly walked across to introduce himself to the up-and-comer. “Then he led me back across the room to meet his wife,” remembers Perler. “Here’s this major hero of mine, this iconic figure in vascular surgery, talking to a nobody.” It was a seminal moment for Perler, an interaction epitomizing to him the culture of SAVS, “what makes it such a special organization—not just great science, but the collegiality, friendship and mutual respect.”
The encounter might be viewed as a portentous moment in the career of the Johns Hopkins Hospital, Baltimore, Maryland, Julius H. Jacobson II, MD, endowed chair in vascular surgery, vice-chair for clinical operations, and chief emeritus of the division of vascular surgery and endovascular therapy. Thompson was the first-ever recipient of the prestigious Rudolph Matas Lifetime Achievement Award, which SAVS bestows to recognize a lifetime of excellence, achievement and contributions to the field of vascular surgery. Now, Perler joins a small band of Matas awardees as the latest following in the wake of the man for whom the accolade is named and who was once hailed “the father of vascular surgery.”
Perler’s route to the gilded award is not inconsiderable. The list of career milestones and accomplishments belonging to him require breathless delivery to achieve relative brevity. But incoming Society for Vascular Surgery (SVS) President Ali AbuRahma, MD, one of a trio of former SAVS presidents behind his nomination, makes a fist of it in his formal letter of recommendation.
A sampling: Vascular chief. SVS president. A consultant to the Circulatory System Devices Panel of the Food and Drug Administration (FDA). Executive vice president of the American Board of Surgery-Vascular Surgery Board (ABS-VSB). Chair of the SVS Foundation. President of the Eastern Vascular Society. And, the most relevant past role in the context of AbuRahma’s compiling of the list: SAVS president.
“It seems that we tend not to see much of the past presidents, but not Dr. Perler,” AbuRahma commented in his letter. “In spite of Dr. Perler’s busy schedule, he has not
missed one single [SAVS] meeting over the past 25 years. In summary, I believe Dr. Perler is most deserving of the Matas award given all that he has done, not only for the SAVS, but the field of vascular surgery.”
Rarely bestowed honor
Gilbert R. Upchurch Jr., MD, the immediate past SAVS president, who formally handed Perler the award, pointed out the accolade is not given yearly but to individuals who have shown continued and persistent leadership to the Society over the years—last being awarded in 2017.
“Dr. Perler has accomplished everything there is to accomplish in vascular surgery,” he said. “He is a brilliant scholar with a quick wit. He is functionally undefeated in any debate regarding vascular surgery as his debate skills are unparalleled. He has edited the JVS and presently serves as the editor of Rutherford’s Vascular Surgery and Endovascular Therapy. He remains a tireless supporter of the SAVS.”
Yet Perler himself, presented with this list, first returns to his presence in the company of Thompson 35 years ago, commenting, “I’m obviously proud of my contributions to the specialty and the leadership positions I’ve been entrusted with over the years, but, ultimately, I still consider myself primarily and, most importantly, to be what I was in 1986, a vascular surgeon,” he tells Vascular Specialist. His career interests cover the entirety of the vasculature and beyond to vascular surgery’s place in the firmament of medicine. “I take care of the totality of vascular disease but I’ve always had a special interest in carotid disease and stroke prevention,” he continues. “I feel truly blessed to be a vascular surgeon, and to be entrusted to care for the vascular surgical needs of my patients. I’m a great fan of James Collins, the business writer, who wrote something along the lines of, ‘It’s impossible to have a great life unless it’s a meaningful life, and it’s difficult to have a meaningful life without meaningful work.’ I can’t think of more meaningful work, or a better way to spend one’s professional life, than caring for the surgical needs of our patients.”
an incredibly important financial asset of the Society for Vascular Surgery, and I’m very proud of the nearly eight years that my co-editor, Tony Sidawy, MD, and I had, and the condition in which we left the journal, and also that we started two new journals, the Journal of Vascular Surgery: Venous and Lymphatic Disorders, and the SVS’ first open access journal, the Journal of Vascular Surgery: Cases and Innovative Techniques.”
Looking ahead, Perler sees a bright future for the vascular specialty. “These are tough times for medicine in general and tough times for vascular surgery, but I think it was Albert Einstein who said, ‘In difficulty lies opportunity,’” he says. “I think vascular surgery has enormous opportunity moving forward. The patients we serve are only going to increase in number, we’re one of the—if not the—most innovative specialties in medicine and surgery. New treatments, whether they be technological or medical, stem cell or the use of artificial intelligence, I think the future is bright. It’s really incumbent upon us senior surgeons to encourage as many bright young people to become interested in the field, get them into the field, and make those contributions.”
‘Be yourself’
“I’ve always believed the toughest thing in the world is to try to be somebody you’re not. The easiest thing to do is to be yourself, and that’s how I’ve conducted my professional life”
— Bruce A. Perler
Perler holds up vascular surgery as a singular discipline within the treatment of the vasculature. “We’re truly unique among those who care for vascular disease,” he says. “I talk often about vascular surgery exceptionalism—not that we’re better than the others; we’re not; but we are unique in so many ways. We’re exclusively devoted to the care of vascular disease; we provide the totality of care— medical therapy, endovascular and open surgery— and we follow our patients for life. I literally have patients I’ve been following for 20 years or longer.”
Perler considers himself fortunate to have been entrusted with numerous leadership positions, but one role in particular stands out. “I think one of the most important jobs I’ve ever had was to be co-editor of the Journal of Vascular Surgery, which not only symbolizes vascular surgery leadership in the care of circulatory disease, but as
For those potential future vascular surgeons, Perler has a message: Seize on opportunities when they present themselves. He also offers pearls of wisdom for the vascular career beyond. “I’ve always believed the toughest thing in the world is to try to be somebody you’re not,” Perler says. “The easiest thing to do is to be yourself, and that’s how I’ve conducted my professional life. I’m honest, I think I do the right things for the right reasons, and try to treat people right. I think people pick up on that, they recognize that, and that’s how you get to be asked to be president of this, or editor of that. Once given those opportunities you have to deliver. I’ve observed that people aspire to positions of leadership for one of two reasons: Some people want to be something, and other people people who want to do something are the opportunities and give it all you have.
award, for this old burned-out taxi
still carries his taxi driver’s license in his wallet to remind him of his roots, is enormously humbling and kind of
FRANK R. ARKO III, MD
Intravascular ultrasound (IVUS) is now used in a wide variety of peripheral vascular interventions after having first been utilized in coronary circulation in the late 1980s. The increased complexity of endovascular interventions has required improved imaging, and IVUS is the one tool besides angiography that can easily allow direct visualization of the vessel and improve outcomes. IVUS-guided interventions resulted in a significantly larger mean diameter while reducing the odds of TLR (target lesion revascularization) at 6-, 12-, 18-, 24-, months in coronary studies. Lesions at high risk were studied in a randomized controlled trial of 150 patients. IVUS use resulted in larger minimal lumen gain, a lower six-month restenosis rate, while TLR at 12 months was also significantly decreased.1
THE USE OF IVUS IN PERIPHERAL interventions, while not randomized, has demonstrated improved outcomes—for example, in aortoiliac occlusive disease.2
In a retrospective analysis of 1,198 patients (28% critical limb ischemia [CLI]) to investigate whether IVUS improves primary patency following nitinol stenting for TASC II A–C femoropopliteal lesions, 2,324 propensity score-matched patients were compared with those treated without IVUS. IVUS was used in 22% of the overall population—in those with more severe TASC classification— with a mean follow-up of 1.9 +/– 1.5 years. Five-year patency was 65% compared to 35% for patients with and without IVUS (p<0.001), respectively.3
Case review

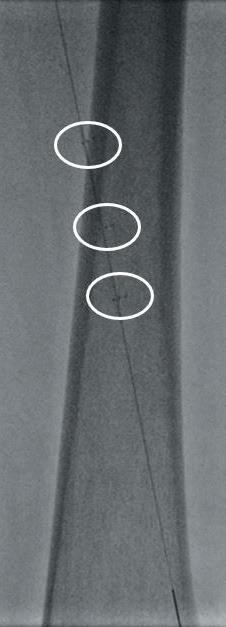
Here, we present a case of a severely limited claudicant who presented with three years of worsening calf pain. The patient was a prior smoker who was treated with maximum medical therapy and a walking program. This initially improved the symptoms, but after three months she regressed. Exercise anklebrachial indices (ABIs) were performed. At rest, the ABI on the left leg was 0.67. With exercise this decreased to 0.17. On the angiogram, there was a long segment stenosis of the superficial artery (SFA), but otherwise there were threevessel runoffs to the foot (see figure 1). Pre-intervention IVUS was used to size the diameter of the SFA through the long segment of diseased artery. Predilatation was performed followed by


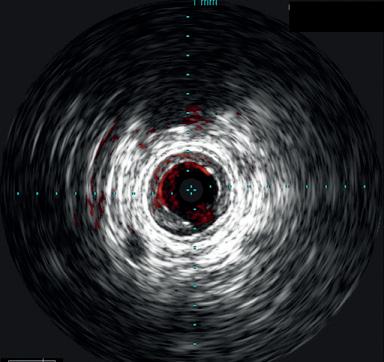
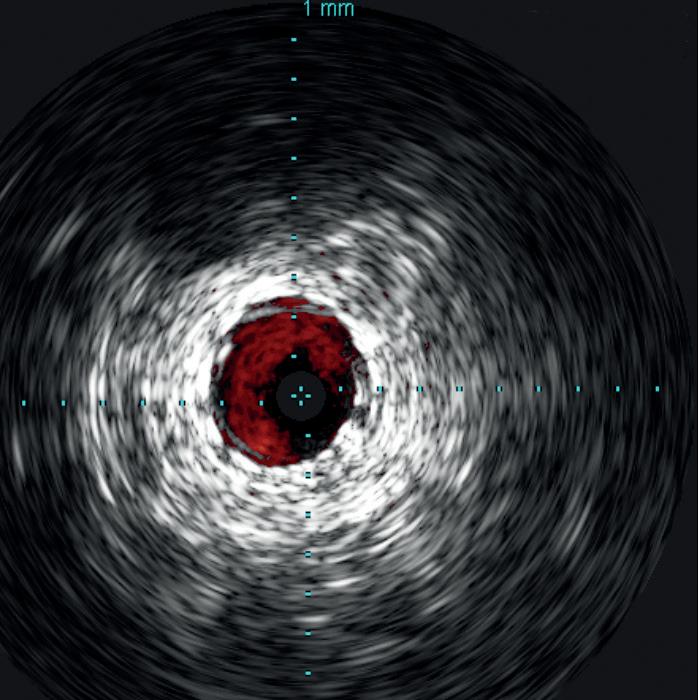
the Stellarex drug-coated balloon (DCB). Completion arteriogram showed marked improvement in flow but a possible dissection in the mid-segment of the SFA. IVUS’ unique ChromaFlo feature was then used to identify and confirm the areas of dissection (see figure 2) Most of the vessel had significant luminal gain but there were multiple areas of short-segment dissection. These were then treated with placement of a total of six Tack Endovascular System implants. The Tack implants were then post-dilated using plain old balloon angioplasty (POBA). Completion angiogram and IVUS (see figure 3) demonstrated resolution of the dissections. Follow-up ABI was 0.95 at rest.
The benefits of utilizing IVUS have been shown in the literature. In nearly every vascular bed studied, we have seen an improvement in overall outcomes. Over the last several years, especially with the introduction of DCBs, as well as atherectomy, there has been a move away from utilizing the use of stents to minimize in-stent restonosis, stent fractures and stent thrombosis. The Tack system optimizes percutaneous transluminal angioplasty (PTA), especially with DCB therapy, to individually treat dissections and to avoid the need to place long segments of stents. In reviewing data on PTA with Tack and PTA alone, there was a marked improvement in the primary patency of 67–87% in patients treated with a DCB compared to 95% 12-month patency in patients treated with DCB and Tack.4 This case shows the
“The case example shows how these systems can be combined to improve outcomes and improve long-term patency by seeing within the vessel”
utility of utilizing IVUS with a DCB to allow for treatment with the Tack system, minimizing the need for longer stents.
The newly developed Reconnaissance PV .018 OTW IVUS has several benefits that allow for improved image quality and durability, and enhanced catheter design with an over-the-wire platform. It is easily deliverable through complex lesions due to enhanced tapered tip, improved hydrophilic coating, and is 5F compatible.
It is constructed with a stainless-steel shaft for improved pushability. The over-thewire design also allows for fluid infusion up to 300psi, easy guidewire exchanges between 0.014 and 0.018, and an extra 15cm working length.
The Tack system is a first-of-its-kind dissection repair device that allows for precision treatment of peripheral arterial dissections following balloon angioplasty in both above- and below-knee lesions. The device comes in various sizes. There are four or six preloaded Tack implants for the below- and above-knee systems, respectively. The system is accurate to <=1mm deployment. The Tack itself is made out of nitinol with gold markers. It has been studied in the TOBA trials.4–6 These studies demonstrate that post-PTA dissection repair with the Tack system improves outcomes for both POBA and DCB angioplasty for patients with peripheral arterial disease (PAD) and CLI. The case example shows how these systems can be combined to improve outcomes and improve long-term patency.
1. Medical Advisory Secretariat. Intravascular ultrasound to guide percutaneous coronary interventions: An evidencebased analysis. Ont Health Technol Assess Ser. 2006;6(12):1–97. Epub 2006 Apr 1. PMID: 23074482; PMCID: PMC3379536.
2. Arko F., Mettauer M., McCollough R., et al. Use of intravascular ultrasound improves long-term clinical outcomes in the endovascular management of atherosclerotic aortoiliac occlusive disease. Journal of Vascular Surgery. Apr 1998; volume 27, issue 4, P614–623.
3. Iida O., Takahara M., Soga Y., et al Efficacy of intravascular ultrasound in femoropopliteal stenting for peripheral artery disease with TASC II class A to C lesions. J Endovasc Ther. 2014 Aug;21(4):485–92. doi: 10.1583/144721R.1. PMID: 25101575.
4. Brodmann M., Wissgott C., Brechtel K., et al. Optimized drug-coated balloon angioplasty of the superficial femoral and proximal popliteal arteries using the Tack Endovascular System: TOBA III 12-month results. Journal of Vascular Surgery. Volume 72, Issue 5, 2020, Pages 1636–1647.
5. Gray W., Cardenas J., Brodmann M., et al. Treating post-angioplasty dissection in the femoropopliteal arteries using the Tack Endovascular System: 12-Month results from the TOBA II study. JACC 2019 Dec, 12(23) 2375–2384.
6. Geraghty P.J., Adams G.L., Schmidt A., et al, on behalf of the TOBA II BTK Investigators. Twelve-month results of Tack-optimized balloon angioplasty using the Tack Endovascular System in belowthe-knee arteries (TOBA II BTK). Journal of Endovascular Therapy 27.4 (2020): 626–636.
FRANK R. ARKO III is chief of vascular and endovascular surgery, and co-director of the Aortic Institute at Sanger Heart & Vascular Institute, Atrium Health, in Charlotte, North Carolina. Arko has been compensated for his services for Philips’ further use and distribution.
BY BRYAN KAY
STENTING REDUCED MORTALITY RISK IN patients undergoing interventions for peripheral arterial disease (PAD) by more than 30% when compared to plain balloon angioplasty, and 40% contrasted with atherectomy, a recent propensity-matched analysis found.
The Vascular Quality Initiative (VQI)-derived data drew sharp conclusions from lead investigator of the study, Dipankar Mukherjee, MD, who trailed his probe into the effects of PAD interventions on survival to most recent follow-up by highlighting that most of these procedures involve claudication patients.
“Expensive interventions do not necessarily correlate with good results,” Mukherjee told attendees of the International Symposium on Endovascular Therapy (ISET) held in Miami (May 9–11), where he presented his findings. “What has been good for the bottom line of the OBL [office-based lab] may be fatal for the patient. We recommend a critical reappraisal of the treatment paradigm for PAD patients presenting with claudication. We believe the current CMS [Centers for Medicare & Medicaid Services] reimbursement for atherectomy has resulted in unintended consequences.”
Mukherjee, chief of vascular surgery at Inova Fairfax Hospital in Falls Church, Virginia, earlier set out the current context of PAD interventional practice: While PAD
interventions double every decade, the more severe form of the disease, critical limb ischemia (CLI), occurs in only a small percentage. More than a decade ago, there were CMS payment system changes governing the outpatient setting. That led to the rise of the OBL, where most PAD interventions are now carried out. Atherectomy, most frequently performed in OBLs, is the most highly compensated PAD intervention.
For the study, Mukherjee and colleagues plumbed the VQI database for claudication and CLI interventions performed between May 2011 and February 2020. Procedures were classified as either balloon angioplasty alone, stenting with and without a balloon, and atherectomy with or without stenting or a balloon. The researchers compared three cohorts: those receiving balloon angioplasty vs. those who underwent stenting; patients who received balloon angioplasty vs. patients undergoing atherectomy; and those who had a stent placed vs. atherectomy.

“We recommend a critical reappraisal of the treatment paradigm for PAD patients presenting with claudication” — Dipankar Mukherjee
A total of 15,281 patients were included: 9,441 received balloon angioplasty, 3,547 got a stent and 2,293 underwent atherectomy. After propensity matching, a group of 3,047 remained to compare between balloon angioplasty and stenting; 2,016 for comparison of angioplasty and atherectomy; and 1,656 between stenting and atherectomy. Patients were almost equally divided between claudicants and CLI. Most interventions were performed in the femoropopliteal-tibial segment. Results showed a “highly, highly significant” hazard ratio (HR) of 0.7 in favor of stenting vs. balloon
angioplasty (95% confidence interval [CI], 0.6–0.82; p<0.001), Mukherjee revealed. The research team uncovered no difference between balloon angioplasty and atherectomy (HR, 1.02; CI 0.88–1.19; p=0.776 ), while stenting was found to be superior to atherectomy (HR, 0.6; CI, 0.48–0.75; p<0.001). When claudication patients were separated from those with CLI, Mukherjee and colleagues discovered a survival benefit in favor of stenting over balloon angioplasty (HR, 0.49; CI 0.4–0.59; p<0.001). They detected no difference between angioplasty and atherectomy, but their data demonstrated a “highly significant” HR of 0.55 in favor of stenting vs. atherectomy (CI, 0.43–0.69; p<0.001). “When we look at CLI alone, there was a trend toward significant,” Mukherjee added.
Discussing his findings, Mukherjee told ISET delegates that investigators have reported “almost universal evidence” of distal embolization with peripheral atherectomy. “We know that intermittent claudication has a relatively benign course with a very small annual mortality risk. I have previously shown, using ICD-9 billing data, that the results of intervention with atherectomy for patients presenting with claudication symptoms were worse than the natural history of the condition.” Mukherjee conceded there were limitations to the study, primarily owing to its observational nature, but concluded that he and colleagues had demonstrated “stenting has 30% better survival than angioplasty and 40% better than atherectomy after propensity matching.”

RISK INFORMATION

Caution: Federal (USA) law restricts the use of the system by or on the order of a physician.
Refer to Directions for Use and/or User Manual provided with the product for complete Instructions, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the product.
INDICATIONS FOR USE
The AURYON Atherectomy System is indicated for use in the treatment, including atherectomy, of infrainguinal stenoses and occlusions, including in-stent restenosis (ISR).
References: 1. Rundback J, Chandra P, Brodmann M, et al. Novel laser-based catheter for peripheral atherectomy: 6-month results from the Eximo Medical B-LaserTM IDE study. Catheter Cardiovasc Interv. 2019;94(7):1010-1017. 2. Shammas NW, Chandra P, Brodmann M, et al. Acute and 30-day safety and effectiveness evaluation of Eximo Medical’s B-LaserTM a novel atherectomy device, in subjects affected with infrainguinal peripheral arterial disease: results of the EX-PAD-03 trial. Cardiovas Revasc Med. 2020;21(1):86-92. 3. Auryon. Instructions for use. AngioDynamics; 2020.
SVS Performance Committee members Mounir Haurani, MD, and Jose Almeida, MD, weigh up the importance of patientreported outcomes (PROs) and how they can be effectively deployed in practice.
MH: Patient reported outcomes (PROs) are direct reports from the patient of their health condition, health behavior or experience with healthcare, and are not subject to interpretation by the clinician or anyone but the patient. PRO measures (PROMs) are the tools that are used to evaluate PROs.
JA: But PROs measure outcomes that aren’t relevant and we do not have many vascular disease-specific PROMs!
MH: While clinicians and other stakeholders may value traditionally measured outcomes, those often do not reflect the patient experience of healthcare. PROs provide an unadulterated assessment of the patient’s perception of their own health status. Importantly, a properly developed, validated PRO will address issues that are important to the patient.
PROMs fall into two major categories: health-related quality of life (HRQOL) and satisfaction. Most people are familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), which is a satisfaction survey that includes topics like cleanliness and
quietness of the hospital environment. I agree; those aren’t particularly relevant to vascular surgery; but, in fact, there are a number of vascular specific PROMs, such as the VascuQOL and the Peripheral Artery Questionnaire (PAQ) that can be used to assess treatment for peripheral arterial disease (PAD).
JA: Maybe you’ve convinced me that PROs have some value but collecting them sounds like just more paperwork in an endless battle against increased bureaucracy that detracts from patient care. Health and wellness task forces cite increased paperwork as a source of physician burnout. Post-op edema is clearly a real and debilitating problem that needs to be managed. Patients communicate this effectively with their voices when in the exam room. PROMs just add an additional barrier to personalized care—in that they make calculators and protocols
BY DANIEL J. BERTGES, MD, AND JENS ELDRUP-JORGENSEN, MD
Vascular specialists have long recognized that there is more to the treatment of peripheral arterial disease (PAD) than the immediate procedural success and early outcomes.
THE PATIENT EXPERIENCE SHOULD NOT ONLY be measured in clinical outcomes such as patency or mortality but subjective measures such as the impact on lifestyle. In recognition of this, the Society for Vascular Surgery (SVS) Vascular Quality Initiative (VQI) has launched a pilot program of patient-reported outcomes measures (PROM) for use with peripheral vascular interventions (PVI).
tantamount to direct communication. MH: There are ways that we can streamline the collection of PROs, such as the use of tablets that integrate with the electronic medical record (EMR) patients can fill out. Moving forward, the Centers for Medicare & Medicaid Services (CMS) will expect PROs to be measured and will use the results as performance standards for reimbursement. In order to provide the best care possible for our patients, and satisfy CMS requirements, it is important for us as vascular surgeons to be part of developing more vascular diseasespecific PROMs, as well as developing recommendations for efficiently and effectively integrating PROs into our practices. PROs will not replace quality listening, and thorough history and physical examinations. When a PRO is incorporated properly, we can use it to augment listening to and examining the patient.


MH: PROs can be used as a mechanism to quantify and discuss issues important to patients. Using standardized, validated PROMs can allow us to have a common language when speaking with all stakeholders. Having reliable data on how the patient perceives their recovery to be progressing and their ability to resume their normal activities can help us better understand the barriers they face in returning to normal.
JA: I still think that the most important postoperative outcomes are our
Beginning in April 2021, 15 sites in the United States and Canada joined the My Peripheral Arterial Disease (My PAD) pilot for PAD PROM collection.
Patients undergoing PVI for claudication or chronic limb-threatening ischemia (CLTI) will be asked to complete two health-related quality of life (QoL) surveys at three time points—pre-procedure, one-month and one year.
While there are a number of options for PROM, the VQI chose two validated QoL instruments. The EuroQol 5D-5L (EQ 5D-5L) is a general QoL survey while the VascuQol 6 (VQ-6) is a vascular disease-specific survey used for PROM in Europe and validated for English and Spanish speakers. The VQI added three additional questions from the original VQ-25 in an effort to study and improve PRO collection for CLTI.
The pilot will evaluate workflows at participating sites and aims to identify best strategies and minimize the burden of data collection.
The pilot will evaluate several methods for PROs collection, including web-based entry through personal computers, tablets and smartphones, as well as conventional, low-tech, paper forms.
Individual sites will choose their collection method and will have the option to use more than one mode of data entry. In an effort to reduce the burden of data collection at participating sites, the VQI commercial technology partner, Medstreaming/M2S, of West Lebanon, New Hampshire, will use email notifications to prompt
traditional measures like mortality and patency. Without achieving success in those traditional measures, the other issues that PROs address become irrelevant.
MH: I agree that PROs do not replace our traditional outcome measures. However, we can use PROs to improve the shared decision-making process. The difference between informed consent and shared decision-making is taking the patient’s goals into account when deciding on a treatment option. While the first question on the mind of most patients with an aortic aneurysm is, “What is my likelihood of surviving the surgery?”, the next question is often related to the recovery process. When we quantify patients’ HRQOL during the recovery process, we can use that information to help us objectively advise patients about their recovery process.
JA: The addition of PRO data will not fundamentally change the decisionmaking interaction between a doctor and an individual patient in a meaningful way. We do not know whether having this information ahead of time will better inform or instead confuse patients. Patients rely on and trust their surgeon’s experience.
MH: In general, I’ve found that most patients are grateful for more information. And PROs can be used on an individual level. For example, a great way of utilizing a PRO in your daily practice is by using it to measure change in HRQOL before and after an intervention. Sometimes it can be difficult for patients to remember how much disability they had before their operation for thoracic outlet syndrome. By using a PROM, you can quantify progress over time.
direct patient entry of PROs after obtaining their verbal consent to participate. The pilot will set the stage for future expansion of collection to all member sites in the PVI registry and eventually for rollout to cover other vascular procedures.
In the future, VQI PROs collection will enable international study in collaboration with European registries through the International Consortium of Vascular Registries (ICVR).
We envision a time when clinicians will have access to longitudinal PROs for their individual patients to better understand the impact of their treatments on their QoL. We hope this information will increase patient engagement, support shared decision-making and improve vascular care.
Beginning in April of 2021, 15 sites in the United States and Canada joined the My Peripheral Arterial Disease (My PAD) pilot for PAD PROM collection
DANIEL J. BERTGES and JENS ELDRUP-JORGENSEN were writing on behalf of the Vascular Quality Initiative Patient-Reported Outcomes Committee. Jorgensen is medical director of the VQI.
BY BETH BALES
There are new vistas in Oklahoma for those in need of vascular care.
That’s “vista” as in Vascular Volunteers In Service To All, or VISTA, a new initiative of the Society for Vascular Surgery (SVS) Foundation whose mission is “to provide better vascular care to underserved populations in the United States,” said Jens Eldrup-Jorgensen, MD. He conceived of the initiative and brought it to the foundation. He is the medical director for the SVS Patient Safety Organization Vascular Quality Initiative and chairs the VISTA Program Steering Committee. SVS member Kelly Kempe, MD, is overseeing the first VISTA pilot project, “Disparities in access to care for limb salvage: The Oklahoma Project,” working with the state’s indigenous and rural populations. It builds on current outreach efforts in the state, some of which began as part of Kempe’s 2020 SVS Foundation Community Awareness and Prevention (CAPP) grant.
For both CAPP and this new disparities project, Kempe is working with a multidisciplinary team at the University of Oklahoma. It includes the Oklahoma Primary Healthcare Improvement Collaborative (OPHIC), medical informatics, internal medicine, podiatry, vascular imaging as well as Peter Nelson, MD, professor and chief of vascular surgery at the University of Oklahoma College of Medicine in Tulsa.
Kempe surveyed primary care providers (PCPs) throughout the state, asking them to identify barriers to limb salvage in Oklahoma, which has some of the highest rates of cardiovascular risk factors associated with amputation in the country. The survey also asked PCPs if they were interested in one-on-one conversations to further elucidate the same questions. “We’re identifying the beginning point. What do PCPs see as primary barriers to specific care that leads to major amputation?”
said Kempe. “Why do our patients end up with severe chronic disease and with limb loss?”
Though the survey and qualitative data is currently being analyzed, PCPs told Kempe and colleagues they would welcome educational resources and awareness. When VISTA came up, “it made sense to utilize the community outreach data we have and keep building in our state.”
First up is to get a sense of the obstacles PCPs face, said Kempe. VISTA volunteers will meet with the practices, distribute educational materials, discuss prevention that will include important physical exam signs, and provide tools such as portable doppler ultrasound equipment to check blood flow. This will help the PCPs become more confident assessing circulation issues and providing more assistance for patients they’re worried about, Kempe said. The VISTA volunteers want to work to both increase PCPs’ awareness about warning signs and the care vascular surgeons can provide. Then, physicians will know to reach out to vascular surgeons when necessary—and be comfortable doing so, said Kempe.
Once they feel more confident assessing vascular disease, they will know who to call for help, she said. And working with them is key, being collaborative and respectful of the work already being done, she said.
The initiative’s first location of Oklahoma is deliberate. The state has very few vascular providers— only 12—plus one of the highest percentage of rural communities in the country, as well as the largest
“Why do our patients end up with severe chronic disease and with limb loss?” — Kelly Kempe
VISTA was born out of Jorgensen’s desire to reach out and do more. He said he’s always been a bit envious of colleagues who have gone overseas to do medical missionary work, he said in an appearance on the Audible Bleeding podcast. With the emphasis emerging over the past year on inequities, he brought a concept to bring modern vascular care to underserved communities to the SVS Foundation.
Refinements and revisions followed, with input from the American College of Surgeons to create VISTA. VISTA’s goal is awareness and prevention, and its initial project grants support initiatives that emphasize risk assessment and focus on bringing vascular care to areas of need.
VISTA organizers reached out to industry and corporate partners, many of whom had unspent funds when the COVID-19 pandemic forced cancellation of virtually all meetings, he said. “We were able to bring the VISTA idea to industry and say, ‘We have a project that addresses social disparities. Would you be interested in funding it?’ And actually, we got very quick turnaround on that.
“Interestingly, talking to corporations, we found out that their new employees want to know what the companies are doing to address social disparities,” said Jorgensen. “This is a really a very opportune time for us.”
While Abbot is funding Kempe’s project, Boston Scientific is providing funding for two additional pilot projects.— Beth Bales
Native-American population in the country. Patients typically show up late in the disease process, when treatment options are more limited, doctors said. Collaborating with the local community, cardiologists, cardiothoracic, general, and vascular surgeons all will work to provide necessary care and resources. “The goal is to have active, ongoing outreach among practices, such that our understanding of the potential needs can evolve and our ability to both empower local caregivers and then provide referral support can grow,” said Kempe.
In the late summer and early fall, team members will begin holding the first in-person visits with targeted practices. After screening, patient education will also be provided. “Oftentimes encouraging medical management, including diabetes care, stopping smoking and taking medication can potentially halt the disease,” said Kempe. “We discuss all avenues of prevention and do all we can so the disease doesn’t progress, and promote early detection when intervention may be warranted.”
As time goes on, the VISTA team will check back with the practices and physicians to find out what’s working and what they as volunteers can do better. Ultimately the model will be expanded to include information and assessment for aortic aneurysms, carotid disease and stroke, venous disease and hemodialysis needs.
“I want to emphasize how grateful I am to be a part of this project,” said Kempe. She thanked the SVS Foundation and said she’s grateful to have Nelson in her corner, as someone “who’s interested in doing things a little bit outside what some people consider research.” She said she believes community awareness work “is where sometimes we can have the biggest impact. If we can help patients, it’s a great honor.”
For more information on VISTA, visit vascular.org/VISTA.

The Eastern Vascular Society is excited to host its 35th Annual Meeting as a hybrid: in person at the BELMOND Charleston Place in Charleston, SC, as well as broadcast virtually in the comfort of your own home and archived on our website.
Registration Types
Member Physician
Non-Member Physician
Allied Health Member
Allied Health Non-Member
Candidate Member
Residents/Fellows/Students
WE ARE HYBRID! Virtual or In-Person
Don’t miss important topics across vascular surgery through a combination of abstracts, invited talks, industry sponsored mini symposiums, and debates! Please reference EVS to take advantage of the group rates (until Aug 21)
Reserve your room at the BELMOND Charleston Place

BY PETER CONNOLLY, MD, AND MARK MATTOS, MD
Let’s be clear here: Political action committees (PACs) are a good thing. Whether or not you like the concept, they create an opportunity for more people to be involved in the political process.
CONTRIBUTIONS BY PACs HAVE increased dramatically over the last decade. In 2020 nearly $500 million were donated to political campaigns. Given the magnitude of monies involved there is certainly some expectation that political donations will return some yield of political influence. Understanding the rationale of PAC donations, there are two main ways they are utilized: 1. The PAC hopes to influence the course of legislation by educating legislators on why they should take a specific action on a piece of legislation, such as co-sponsorship or voting for legislation when it is considered in committee or for passage. 2. The PAC
provides campaign contributions to those running for election who support the issues by having articulated policy positions that concern PAC members.
Patterns of PAC distributions tend to be directly proportional to elected officials’ influence on Capitol Hill. You need only look at the key members of the House of Representatives Ways and Means Committee, who receive the largest proportion of PAC donations, to appreciate PACs’ role in affecting the legislative process (see opensecrets.org).
There are 112 physician PACs, which gave $21 million in 2019–2020. While some of these PACs share common legislative interests, such as the relief from Prior Authorization requirements, there are a multitude of different legislative priorities for all of these groups. It is important for the SVS to have a voice in this element of the education process with members of Congress who sit on committees with jurisdiction over healthcare policy issues. In our time being associated with the SVS PAC, it has become apparent that we will have greater influence on Capitol Hill with more direct engagement of our elected officials.
To that end, the Society for Vascular Surgery PAC (SVS PAC) and its committee, the SVS Government Relations and the SVS Advocacy and Policy Council have engaged in a tour-de-force advocacy campaign to bring the SVS legislative agenda front and center to our elected officials. During the 2019–2020 election cycles, the SVS PAC represented the SVS at nearly 25 events with members of
BY BETH BALES
The Society for Vascular Surgery (SVS) has scheduled two Town Halls for the summer—one to cover vascular surgeon wellness programs (July 13) and the other to discuss the SVS’ first-ever appropriate use criteria (AUC) guidelines being developed on intermittent claudication. (Aug. 5).
“ADVANCING VASCULAR SURGEON WELLNESS” will begin at 6 p.m. Central Daylight Time July 13. Register at vascular.org/WellnessTownHall.
The Wellness Task Force will share updates about its initiatives to improve wellness for vascular surgeons, including the new surgeon coaching program, being developed by the SVS and the Academy for Surgical Coaching, which provides vascular surgeons with active support from other vascular surgeons. The volunteer
Congress. We are on target to match or exceed that number in just the first six months of the 2021–2022 election cycle.
SVS members representing 13 states recently met with Reps. Dr. Kim Schrier (D-Washington), Ron Kind (D-Wisconsin), Stephen Horsford (D-Nevada) and Lizzie Fletcher (D-Texas), to discuss numerous legislative priorities for vascular surgeons. SVS members engaged in a spirited dialogue with these officials, reviewing many of the hurdles that we as vascular surgeons face in the politics of medicine as well as discussing lawmakers’ perspective from Capitol Hill.
112 physician PACs $21 million gave in 2019–2020
It’s not all about the donations, but donations do bring opportunity
The takeaway was pretty clear—effective political influence only works if you have good advocacy. It’s not all about the donations, but PAC donations do bring opportunity
Legislative priorities discussed included protecting patients’ timely access to care, prior authorization reform, holding physicians harmless from Medicare cuts, stopping the practice of surprise billing, support for increasing the number of residency positions, support for telemedicine, increasing physician/surgeon wellness, and educating them on the breadth and value of vascular surgery.
While having a PAC is an important
coaches are being trained this summer. Other topics will include subjects that have caused surgeons stress, including dealing more successfully with electronic medical records (EMRs), wellness and malpractice, the government’s role in physician wellness and reducing work-related pain and discomfort. Panelists include Dawn Coleman, MD, and Malachi Sheahan III, MD, task force co-chairs; London Guidry, MD, chair of the SVS Electronic Medical Records Subcommittee; Andrew Meltzer, MD, chair of the SVS Malpractice Support Subcommittee; Niten Singh, MD, chair of the SVS Coaching Subcommittee; Megan Tracci, MD, chair of the SVS Government Relations Committee; and Max Wohlauer, MD, chair of the Ergonomics Subcommittee.
The Aug. 5 Town Hall will discuss the “Society for Vascular Surgery appropriate use criteria for intermittent claudication.” This is the SVS’ first AUC and SVS members are leading this multidisciplinary work group, which includes members of both the American College of Cardiology and the Society of Interventional Radiology participating on the rating panel for a multidisciplinary approach. Panelists will include Kim Hodgson, MD, past SVS president; Larry Kraiss, MD, past chair of the SVS Quality Council; Jessica Simons, MD, chair of the new SVS Quality Improvement Committee; Jeffrey Siracuse, MD, past chair of the SVS Appropriateness Committee; and Karen Woo, MD, chair of the SVS Intermittent Claudication Appropriate Use Criteria Work Group.
The Town Hall will address appropriateness, the process and methodology of creating appropriate use criteria. Register at vascular.org/AUCTownHall.
tool for advocacy efforts, grassroots actions where SVS members contact their lawmakers are also critical. Having large numbers of SVS members respond to our call for help last year in contacting lawmakers was a big reason the Medicare cuts were halted for 2021. To that end, the SVS PAC, Government Relations Committee and the Policy and Advocacy Council are sponsoring a Washington, D.C., virtual fly-in event on July 21, as part of a concentrated Grassroots Advocacy Week. This virtual event will match and connect 40 to 50 SVS members with their respective members of Congress for direct and frank conversations about the challenges vascular surgeons faced in 2020 and looming obstacles we will face going forward in 2021 and 2022. Advocacy is key, but it is a volume game; we can’t do it alone. Please consider making a donation to the SVS PAC (visit vsweb.org/PAC) and marking your calendars for the week of July 19 to participate in our week of grassroots action to give the SVS the strongest voice possible in the nation’s capital.
PETER CONNOLLY and MARK MATTOS are co-chairs of the SVS Political Action Steering Committee.

Upcoming SVS Town Halls cover wellness programs and appropriate use criteria




Specialised source of news and education in the field of renal disease management
Breaking news, in-depth analysis, and leading opinion from key industry figures
Steered by globally-renowned physicians to monitor the latest innovations and controversies alike in the kidney care field
Industry updates and real-time event coverage via social media, videos and more on print and digital platforms
Visit www.renalinterventions.net and click ‘Subscriptions’ for complimentary print subscription* and e-newsletter subscription**
*Available for US and EU readers only **Available worldwide
BY BETH BALES
To better meet the needs of Society for Vascular Surgery (SVS) members who practice in the community setting, the SVS has approved a proposal to evolve its Community Practice Committee to a new Community Practice Section.
THE CHANGE PROVIDES MORE OPPORTUNITY than a committee with limited membership can, said Daniel McDevitt, MD, section chair. The new section integrates the existing Section on Outpatient and Office Vascular Care (SOOVC) and brings together the whole of the community practice environment.
The Community Practice Section will be optimally
positioned to further enhance SVS efforts in education, advocacy, quality practice, ethics, research and member value from a community practice perspective.
SVS traditionally was more focused on the specialty’s science, said McDevitt. However, time has brought changes not only to the Society itself but also to medical care and society in general: Today, more and more SVS members are delivering patient care in community settings, he said.
Community practitioners comprise a significant percentage of SVS membership, he said. Change has come quickly within the past five or so years to provide more programs and education for these members.
The Community Practice Committee chair was named to the SVS Executive Board to directly represent those members’ interests. Webinars and sessions of interest at the Vascular Annual Meeting (VAM) have increased in number over the years. And with continuing need, SVS leadership embraced the idea of creating a separate section to help community surgeons meet some of the challenges they face.
He cited last year’s advocacy to fight 7–10% Medicare reimbursement cuts. Some of the Section’s first activities will take place at VAM. Thursday afternoon features content devoted entirely to the clinical and business practices of the outpatient vascular lab. Saturday will feature a three-hour postgraduate course of interest to community practitioners: “Emergency vascular care in the community hospital: What is safe and reasonable?”
During the Thursday session, the Section leaders also will present the Excellence in Community Service Awards for both 2020 and 2021.
“We are really an inclusive society that represents surgeons in a variety of venues”
— Daniel McDevitt
McDevitt praised SVS Immediate Past President Kim Hodgson, MD, and Ronald L. Dalman, MD, current SVS president, for their endorsement of the proposal. “We are really an inclusive society that represents surgeons in a variety of venues,” McDevitt said. “We all appreciate the Society embracing representing the entire vascular community.”
“We have a lot of ideas as well as content,” said McDevitt. Many external factors create stress and affect members’ ability to practice, including scope-ofpractice, billing and legal concerns, outpatient-based facilities, new employment models, increasing workloads and decreasing reimbursements. “To address these concerns, we need a more robust level of membership engagement. It’s important to have the strong representation SVS provides to advance our cause.”
BY BRYAN KAY
The ability to pivot in the face of changes to reimbursement while still meeting the needs of patients is a key facet of success in the office-based lab (OBL) setting. That was among the key messages delivered by Brian DeRubertis, MD, professor of surgery at UCLA School of Medicine in Los Angeles, in a talk delivered at the Pacific Northwest Endovascular Conference (PNEC) in Seattle (May 27–28) focused on reimbursement issues in the context of OBLs—and whether or not this mode of outpatient setting can weather the challenges.
To demonstrate his point, DeRubertis used the example of arteriovenous (AV) access procedures for dialysis patients.
“Reimbursement issues are always key to the OBL setting,” he explained. “Just like any hospital setting, you need to make sure your reimbursements are enough to sustain the model. Reimbursements have been decreasing in recent years. There is often discussion of large decreases in
reimbursement or large changes, but there have not been significant changes over the last few years, in my opinion. We have seen a decrease by a few percentage points in various procedures each year. Now that does change—there are some procedures, such as AV access procedures for dialysis, which took somewhat major changes a couple of years back. I think as physicians we need to be aware of what these changes are to make sure the reimbursement is still
The Community Practice Section is the third of its kind. Understanding the need and desire for groups of members with a common interest to find and engage with one another beyond the scope of committee work, in 2017 the SVS Executive Board established “Sections” as a new organizational model. Any group of 40 members of the SVS with a common interest or discipline can petition to become an SVS section and if approved, provide “added value” for their cohort of members in a variety of ways. Before now, since 2017 only two sections were formed, the PA Section in 2017, and the Outpatient and Office Based Care Section, better known as SOOVC, in 2019.
sufficient enough that we’re providing care for patients in a way that we think is the right way to care for them.”
DeRubertis said it was important to highlight some of the benefits of providing care in the office-based outpatient setting. He referenced physician flexibility; autonomy and independence in care provision; the speed at which patients can be transported into the procedural suite; a nimble nature that enables adaptability to community needs; and increased safety.
Reimbursement challenges often rest on an ability to react to change, he noted, returning to the example of decreased payments for AV access procedures in the the OBL arena.
“But they increased in the ASC [ambulatory surgery center setting],” DeRubertis pointed out. “So some physicians have converted and gone through the process of converting their
Brian DeRubertis
OBL to ambulatory surgery centers, which has a different set of requirements and regulations, but in some ways that’s maybe a good trend going forward for some centers.
“So I think the real key is being aware of reimbursements, and being able to pivot to make sure that it is in concordance with a model that allows us to treat our patients the right way.”
DeRubertis also touched on the ways in which COVID-19 demonstrated other OBL benefits.
While in a hospital patients attending for a lower-extremity angiogram might interact with as many as 30 different staff members, the equivalent number in an OBL or ASC might be just five to seven, he said. “So during such an unusual time like the pandemic, having that real simplicity and pareddown support staff really helped protect both patients and staff from COVID-19 transmission.”

BY CHRISTOPHER AUDU, MD
In academia, the start of summer brings about new beginnings and a changing of the guard. Chief residents and senior fellows graduate and start new jobs. This month, we decided to pick some of their brains to share their lived experiences and lessons learned for those who will be transitioning. Although 2020 was an unusual year to be a senior trainee in vascular surgery given the clinical repurposing that occurred due to COVID-19, there are still lessons to glean from the experience of our graduates.
CONTRIBUTING TO THIS COLUMN
are Zachary Wanken, MD, a Dartmouth integrated vascular residency graduate and new Washington University, St. Louis, vascular surgeon; Ignatius Lau, MD, a Mt. Sinai integrated vascular residency graduate and now vascular surgeon in Northern California; Brandon Downing, MD, a Washington University, St Louis, integrated vascular graduate and newest Community Health Network, Indianapolis, Indiana, vascular surgeon; and Laura Maria Drudi, MD, who recently became a University of Montreal, Canada, vascular surgeon. Juggling the final years of training and an active job search takes deliberation and discipline. Here’s what our columnists had to share about doing both with aplomb.
ZW: My #1 goal during my senior year was to make sure I became independently capable as an operative surgeon, both technically and from a decision-making standpoint. To that end, I scrubbed the most complex cases on our schedule and made sure to scrub a wide breadth of cases, too.
IL: Success as a chief resident or senior fellow boils down to operating as much as possible. The best learning occurs in the trenches of the operating room (OR), where mistakes may be made, near misses are discussed and emergencies are handled deftly. This stuff isn’t written in books. The only way to gain this knowledge is to increase the total number of cases that you do. As a chief, I chose high and low complexity cases to prepare me for what was to come.
LMD: The final year of training in Canada amidst a pandemic was challenging. I had to juggle chief responsibilities, studying for the Royal College of Physicians and Surgeons of Canada licensing exam, fellowship planning, and managing my soon to be surgical practice. Therefore, my priority in my final year was to ensure I was a competent surgeon. I knew the case history, operative planning, and divided tasks during the cases to ensure all members in the team had an opportunity to learn and participate. As a result, that year I became a leader in and out of the OR and my confidence grew exponentially.
BD: For your own training, it is important to continue to do the little cases because you will likely be doing far more “smaller” cases at the beginning of your career. My co-contributors have made some very excellent points. My only addition is to be mindful that the last few months of training can lead to burnout. Scheduling a vacation during those times is not a bad idea.
Develop your soft skills
ZW: My last two years, I focused on developing my management, leadership and teaching skills. This gave me useful experience in a safe environment where I could lean on the experience of my attendings. Focusing on these skills also gave me insight into the type of job I wanted.
LMD: Throughout training, I participated in several professional, leadership and educational development activities through the likes of the SVS. I always

strive to be a better physician, surgeon and person for my patients, my colleagues and myself. I developed a reputation of being a compassionate and empathetic surgical leader. In terms of management skills, I feel it is a constant struggle for me to balance and integrate the various aspects of my life and career. Rather than view this balancing act as a struggle, I choose to see it as an adventure.
BD: To be successful in your final year of training, it is very important that you continue to support the workflow of all trainees to keep morale high for all. As you know, surgery takes a team effort, and now you play a major role in making that team function.”
Know your career phenotype
ZW: From my experience, the delineation between academic practice and private practice is an oversimplification. I think the job landscape actually offers a great variety of positions that don’t fit neatly within the traditional academic or private practice models. Therefore, it is more important to focus on what you want out of a job or career. For example, many academic or private practice jobs
“I think the job landscape actually offers a great variety of positions”
incorporate research, trainee education, clinical trials, etc. I would recommend reviewing all available options.
IL: First, you have to figure out what pathway you may want to pursue. There are timelines to consider also. For instance, academic jobs tend to be available in the winter and later when budgets are released. Private practice jobs, on the other hand, can become available as early July of your final year. Prospective private practice employers may want an answer within a month of an offer, which can be challenging if you’re considering multiple options..
LMD: Throughout my vascular surgery training I made an intentional effort to brand my name and image, knowing that I have always wanted to become an academic vascular surgeon, and knowing that the job market is limited in Canada. However, I followed my passions and
opportunities opened up for me to pursue the career I wanted. Through my postgraduate training in epidemiology, I became an expert in frailty and vulnerability for patients with PAD. My branding came from several years of attending conferences, networking with vascular trainees and faculty, presenting research, and volunteering on committees.
Leverage your network
IL: Once the last year of training starts, meet with the chief of your division or section, and with trusted mentors to ask for references and to tap into the connections that they have. Be honest with them about your goals and what you’re looking for in a job. Make an effort to go to conferences in person and meet people. Sometimes, the first interview happens at these meetings. Pro tip: Meet with the representatives from each of the device companies that you have come to know and work with over the years. More often than not, they will have colleagues in the region of the country where you may be considering.
ZW: Visiting your potential new job location, if you haven’t lived there before, is important. Also important is speaking with graduating residents/fellows or erstwhile partners of your new practice. LMD: I have continuously networked with the vascular surgery community. I attended my first VAM in 2011 and always attended even when I wasn’t presenting. I became passionate about vascular outreach. I even became a simulation instructor. I further engaged in committees that were meaningful to me given my lived experiences. I am truly looking forward to growing alongside the incredible mentors and sponsors who have been by my side along the way.
CHRISTOPHER AUDU is an integrated vascular surgery resident at the University of Michigan in Ann Arbor, Michigan.
BY ANNA VECCHIO

SINCE THE INAUGURAL #SVSTWEETCHAT
that covered early career advice went live on Twitter in April, the monthly social media initiative has proven to be a valuable and interactive resource for the vascular surgeon community. It even inspired an episode of the increasingly popular Audible Bleeding, the vascular surgery podcast and formal entity of the Society for Vascular Surgery (SVS).
Members of the SVS Social Media Committee continue to update Twitter users on the progress of the chats through their personal accounts as well as the SVS social media channels.
The #SVSTweetChat has been well-received by panelists and participants—more than 360,000 users saw #SVSTweetChat in their timeline or search results during the May tweet chat covering radial access for the vascular surgeon.
Engagement levels have significantly increased since April’s Tweet edition, which earned more than 16,000 impressions. The success of the new social media initiative has inspired more members of the vascular community to get involved and keep the #SVSTweetChat conversation going on social media.
The April chat that inspired an episode of Audible Bleeding was part one of “So you’ve matched into vascular ... now what?” Hosts Matt Chia, MD, and Ali Irshad, MD, sat down with Regina Husman, MD, and Kirthi Bellamkonda, MD, to discuss how newly matched vascular residents can set themselves up for success in their residencies.
“We reached out on Twitter and asked the audience to send us questions for this episode … We want to thank Meryl Logan, MD, for inspiring this episode with the #SVSTweetChat,” said Chia.
Thirty-six Twitter users participated in the May tweet chat and more than 150 tweets featured the #SVSTweetChat hashtag. The @VascularSVS Twitter account gained 10 new followers within 24 hours of the chat.
Chats are held on the third Thursday of each month. The next tweet chat will kick off at 8 p.m. Central Daylight Time Thursday, July 15, with a new set of panelists to discuss percutaneous vs. traditional arteriovenous fistula creation.
To participate, log in to Twitter at the time of the chat, search for #SVSTweetChat in the search bar at the upper right and look for the latest thread of tweets. To respond and engage with the chat, include the hashtag, #SVSTweetChat, in each response.
PRACTICING VASCULAR SURGEONS, LEARN ALL about preventing and managing type II endoleaks—a common situation faced by specialist—from the experts on July 15. Benjamin Jackson, MD, will moderate the session, alongside panelists Wei Zhou, MD, and Sunita Srivastava, MD.
Participation is limited to 100 people so attendees have the opportunity to talk with the experts, asking questions, as well as relaying stories of their own cases and complications.
“Type II endoleak prevention and management,” from 7 to 8 p.m. Central Daylight Time, is the final of the four-session “Meet the Experts Webinar Series,” tackling a topic relevant to vascular surgeons in practice.
Vascular surgeons often confront type II endoleaks in patients who have undergone endovascular aneurysm repair (EVAR). The optimal treatment and prevention of this common problem is uncertain, and different vascular surgeons manage type II endoleaks differently.
Furthermore, some of these common endoleaks might be prevented by deploying embolization techniques or other measures at the time of the initial aneurysm repair, but indications to prophylactically treat lumbar vessels or the inferior mesenteric artery are uncertain. Part of the webinar will cover identification of indications for conversion to open aneurysm repair.—Beth Bales
Don’t miss out on learning how to better manage and prevent type II endoleaks. Learn more and register at vascular. org/MeetExperts.
Robyn Macsata, MD, 50, suddenly, May 21. She was chief of vascular surgery and associate professor of surgery at the George Washington University, Washington. D.C. George Washington University Surgery posted online, “Her extraordinary legacy as a gifted surgeon, dynamic educator and supportive mentor will live on here at [George Washington] and in the lives of all of those she touched … [hers was] a life of excellence and a legacy that will live on in our community and beyond.”
Macsata received Society for Vascular Surgery Distinguished Fellow designation in 2019.—Beth Bales
A NEW SOCIETY FOR VASCULAR SURGERY (SVS) OnDemand course, “Thoracoabdominal aneurysm repair” is now available on the Education Portal for members. It is one of eight courses now available in the “Vascular Atlas” section of SVS OnDemand. The Atlas is an online medical resource, with new courses added on a rolling basis, that provide up-to-date information to assist in patient care. SVS members update the courses.
Christopher Abularagge, MD, and James Black III, MD, both of Johns Hopkins Medicine, Washington, D.C., teach the thoracoabdominal aneurysm repair course. As is the case with all eight selections, it covers such factors as indications, pertinent anatomy, equipment needed, key steps, complications and more. Other courses include “Hemodialysis access creation with upper extremity AV fistula,” by Bradley Bowles, MD, Michael Williams, MD, and Matthew R. Smeds, MD; “Renal artery stenting,” from Efthymios Avgerinos, MD; “Popliteal venous aneurysm by closed venous plication,” delivered by Andrea Obi, MD, Thomas Wakefield, MD, and Dawn Coleman, MD; “Thoracic outlet syndrome,” from Ying Wei Lum, MD, and Christopher J. Abularrage, MD; and “An approach to wound care for vascular surgeons, by Michael Go, MD. Any SVS member in good standing may view the Vascular Atlas courses. Start by visiting vascular.org/Education.—Beth Bales