

16 News From SVS
Plan now to

Plan now to
BY JOHN F EIDT, MD
ASSOCIATE MEDICAL EDITOR, VASCULAR SPECIALIST
Every surgeon has experienced the anguish of an adverse outcome. The patient with an elective aneurysm who dies on the table, the asymptomatic carotid patient that has a stroke in the recovery room, the cosmetic varicose vein case that has a pulmonary embolus. Driving home alone, we tell ourselves that we did our “best,” but lingering in the dark shadows of our minds are the nagging questions: What should I have done differently? Am I really a safe surgeon? Should I quit and get a job with “industry”? What if I get sued? How should I deal with the family? Will I get fired? Our houses are dark when we arrive

Please

BY DAWN M. COLEMAN, MD ON BEHALF OF THE SVS WELLNESS TASK FORCE
Following a series of Vascular Specialist pieces highlighting the crisis of surgeon burnout and the unique challenges that face vascular surgeons, the SVS Wellness Task Force was formed in 2017. Recognizing that burnout may compromise recruitment and retention into our specialty, a particular threat at a time when our specialty faces projected increasing physician workforce needs, and that data suggest physician
burnout compromises both patient quality of care and overall satisfaction, the task force was charged with proactively addressing vascular surgeon burnout. Our task force, comprising 21 engaged SVS members from across the country, has been working with strong support from leadership and administration to identify potential SVS targets for meaningful change.
The year 2018 was one of information gathering as we attempted to clarify the severity of the problem and perceived member needs. We are grateful to our members

BY MALACHI SHEAHAN III, MD MEDICAL EDITOR, VASCULAR SPECIALIST

SDR. SHEAHAN
everal months back I wrote (another) editorial regarding burnout. I tried to put aside all of the surveys and statistics and get to the true human cost that burnout extorts. While the result was adequate, it will never be published. Just after finishing, I received a letter that made my efforts obsolete. What follows here is raw, unedited, and at times difficult to read. The author has not asked for anonymity, indeed he has left several identifying pieces of information, but I will keep this off the search engines at least. To me, this story illustrates that no matter how far we think we have veered from the road, there is always a path back.
BY ANONYMOUS
Iwrite this on my 7-year sobriety date, and after reading the presidential address given by Dr. Sam Money at last years’ SAVS meeting. I have not shared my story with my vascular peers – even in the discussions and breakaway sessions on surgeon burnout and attrition at society meetings because of the mix of emotions this stirs in me. It lacks humility to say, “look at me” because I could fall apart tomorrow, and this is the reasoning that helps me stay sober. I write this believing that sharing my experiences may lead to ideas for others in our stressful profession.
I always wanted to be an academic surgeon, and I earned the Founder’s Award from the Southern Association for Vascular surgery (SAVS), the Raymond Alexander Award from the American Association for the Surgery of Trauma (AAST), the Young Investigator’s Research Award from SVS, and the EJ Wiley Travelling Fellowship from the SVS. I had been granted a Fulbright Scholarship for research in upper-extremity neurovascular disorders just months prior to being deemed unfit for practice. My professional life included many false summits, and each success was just a short sweet moment. I always returned to a core need for something I couldn’t identify, much less
VASCULAR SPECIALIST Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD., Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Drudi, MD.
Executive Director SVS Kenneth M. Slaw, PhD.
Interim Director of Membership, Marketing and Communications
Angela Taylor
Managing Editor SVS Beth Bales
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of health care policy. Content for Vascular Specialist is provided by Frontline Medical Communications Inc. Content for the News From the Society is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and Frontline Medical Communications Inc. will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein.
satisfy. I felt like a visitor to my normal life of family, church, community, and home living.
Vascular training selects and trains us to be “invincible,” “invulnerable” to the foibles of mere mortals, and supremely self-confident. Despite my professional successes and conformity to the ideal, I felt a pervasive but indefinite inadequacy on the inside. Following spine surgery, exacerbated by all the standing and lead protection, I still had pain and began to rely increasingly on hydrocodone. I destroyed friendships, alienated partners, and damaged my family as the narcotics became my primary driving force.
I was arrested on Oct. 31, 2011, for diverting narcotics for my own use. I remember explaining to my three daughters (in their Halloween costumes) what had occurred, what an arraignment was, and finally about my addiction. I called relatives and friends to tell them before my bow tie and face appeared in Busted magazine the next morning. I did several important things that week, although I cannot remember the week at all.
In November of 2011, I was naturally terminated from my practice, entered a 90-day rehab program, and spent a year working on myself and my family: state medical board monitoring; counseling and 12-step
POSTMASTER Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 10255 W Higgins Road, Suite 280, Rosemont, IL 60018-9914.
RECIPIENT: To change your address, contact Subscription Services at 1-800-430-5450. For paid subscriptions, single issue purchases, and missing issue claims, call Customer Service at 1-833-836-2705 or e-mail custsvc.vasc@fulcoinc.com.
The Society for Vascular Surgery headquarters is located at 633 N. St. Clair St., 22th Floor, Chicago, IL 60611. Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by Frontline Medical Communications Inc., 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609. Phone 973-206-3434, fax 973-206-9378
Subscription price is $230.00 per year.
National Account Manager Valerie Bednarz, 973-206-8954, cell 973-907-0230, vbednarz@mdedge.com
Digital Account Manager Rey Valdivia 973-206-8094 rvaldivia@mdedge.com
Classified Sales Representative Drew Endy 215-657-2319 cell 267-481-0133 dendy@mdedge.com
Senior Director of Classified Sales Tim LePella, 484-921-5001, cell 610-506-3474, tlapella@mdedge.com
Advertising Offices 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609 973-206-3434, fax 973-206-9378
Letters to the Editor: VascularSpecialist@vascularsociety.org
Editorial Offices: 2275 Research Blvd, Suite 400, Rockville, MD 20850, 240-221-2400, fax 240-221-2548
©Copyright 2019, by the Society for Vascular Surgery


Scan this QR Code to visit vascularspecialistonline.com
meetings; yoga; cardio. This was the toughest thing I have ever done. I discovered that issues within me were more challenging than the drink and pills. After all of that, I learned that the key to staying well has been to remember daily what I am.
The vascular societies tend to discuss “burnout” broadly. The term needs a better disciplined definition. Is it “chronic fatigue syndrome,” which has an IDC-10 code R53.82, or a euphemism to talk politely about the destructive consequences of the profession we have chosen?
The burnout that I understand walks lockstep with addiction and alcoholism, frequently accompanied by disruptiveness and offensive behaviors. Little appears to have been written on this within our societies; but, I know I am not the only vascular surgeon who has torched out because of substance abuse, or depression, or other stress-related reasons.
I am also unaware of explicit guidelines within our profession for the management of the casualties – only academic musings about fatigue and the associated attrition. Older papers, and state boards, focus primarily on patient safety, not the recovery of the impaired surgeons. On my journey to restoration, I found few resources within the surgical community. I felt that I got better without the assistance of my
FRONTLINE MEDICAL COMMUNICATIONS SOCIETY PARTNERS
Director, FMC Society Partners Mark Branca
Editor in Chief Mary Jo M. Dales
Executive Editors Denise Fulton, Kathy Scarbeck
Managing Editor Mark S. Lesney
Creative Director Louise A. Koenig
Director, Production/Manufacturing Rebecca Slebodnik
Corporate
President/CEO Alan J. Imhoff
CFO Douglas E. Grose
SVP, Finance Steven J. Resnick
VP, Operations Jim Chicca
VP, Sales Mike Guire
VP, Society Partners Mark Branca
VP, Editor in Chief Mary Jo M. Dales
VP, Editorial Director, Clinical Content Karen Clemments
Chief Digital Officer Lee Schweizer
VP, Digital Content & Strategy Amy Pfeiffer
President, Custom Solutions JoAnn Wahl
VP, Custom Solutions Wendy Raupers
VP, Marketing & Customer Advocacy Jim McDonough
VP, Human Resources & Facility Operations Carolyn Caccavelli
Data Management Director Mike Fritz
Circulation Director Jared Sonners
Corporate Director, Research & Comms.
Lori Raskin
Director, Custom Programs Patrick Finnegan
In affiliation with Global Academy for Medical Education, LLC
President David J. Small, MBA

colleagues. The best I can tell, I got a second chance at my career because of my favorable risk/monetary gain ratio to a needy hospital which I accepted as a dicey leg up.
My initial return to work was a 2-year odyssey of building up a peripheral program where three surgeons had recently failed before. I learned a lot about ethics, hospital administration, and the rationale behind the Stark Law. I was buoyed by having patients come up to 6 hours into Appalachia for me to do aortic endograft cases and rib resections, as well as 40 EVARs in 2 years. A 14-year-old girl was referred from the institution that fired me: She responded well to thoracic outlet decompression and went on to volleyball stardom, became high school valedictorian, received a university scholarship, and declared a premed major – to become a vascular surgeon!
Imagine bringing your 14-year-old daughter to literally one of the worst hospitals in the country (U.S. News and World Report, 2011) to have an addict operate on her because you heard he was good! It is possible to dig out of these problems – we just need a better process within the profession to do so.
My postrecovery professional highlights include being rehired by the institution that fired me and continuing a full breadth of vascular surgical care as the division chief. I am currently the secretary of the state vascular society (president-elect 2019). The lows include criminal trial and plea bargain to class III misdemeanor, divorce, bankruptcy, and the death of my father. To remember what I am, I go to AA meetings and talk to an addiction counselor, and I have requested continued random urine drug screening (UDS). I have ensured there would be no gap in UDS for 7 years. I did this purely for my protection, through personal accountability, and as proof of sobriety to any doubters.
Being “broken” has made me a better dad, better technical surgeon, and better decision-maker, and it has made me likable to my patients and peers. Being broken also led to the dissipation of my relationships with vascular colleagues; one of them called me on the rehab wall phone to see “if the story was true.”
Within a week my schedule went from academic conferences and complex aortic cases to riding the “druggy buggy” and befriending my new peer group, including a 19-year-old roommate who responded to every question with “word.” Costs exceeded $200,000 the first year of recovery, not including lost income. It qualified as a “life-changing event.”
I doubt I am very different from everyone else who pounds out a career treating gangrene around the clock. The institutional policies are clear: Self-report if you are not in compliance with policy regarding sobriety and disruptive behaviors –which will result in a report to the medical board, and suspension or termination. For me, self-awareness was unreliable during my impairment, and the overwhelming emotion was fear. I lied to my staff chairman twice when he asked if I was taking “anything.” In retrospect I wonder why he did not intervene. In this instance, that which seems harsh is paradoxically merciful, because the natural history of addiction is much crueler.
Could there have been a safer path to help, with earlier intervention if my colleagues had a way to redirect my course? This question seems unfair, and truly I have no attitude of blame. However, I am wondering why we have not developed the processes needed to help each other out in these difficult matters, akin to or resultant from “burnout.”
During impairment, my personal thinking was as follows:
“My lumbar disk needing repair is simple to understand, and not moral-
ly loaded – except that I cannot leave my post since I am irreplaceable. I don’t want to face my trajectory toward illness and death. Furthermore, how will I pay my kid’s tuition, club dues, and the mortgage if I take time out to get better? I got shamed for illness during surgical training – is it not true that absence is weakness and puts upon my colleagues?”
My self-management was pills, nighttime drunkenness, hatefulness, resentment, and anhedonia, as well as disabling anxiety at the unsolvable thought loop.
For me, burnout, substance abuse, and physical disability were all part of the same cycle. I submit that we all see potential for these frailties in ourselves and we are either empathetic or reviled when we see it in our colleagues. Because of my life lessons, I am my brother’s/sister’s keeper within the fellowships of medicine. To understand why I say this requires understanding the dynamics and intercollegial attitudes toward the pressures put upon us by the specialty we trained so hard to enter.
I consult with a legal advocacy group that treats impaired judges. The legal community teams up to intervene on impairment early to prevent consequences on past judgments and public backlash. A good illustration is that of a judge who was an opiate addict whose access to pills involved parolees. This scandal resulted in disputes over his decisions, state costs, and loss of solitude amongst both the accused and the victims. I argue that the consequences are similarly grave in our profession. We can look at established programs for modeling our own.
A consortium of colleagues with standing in the vascular societies currently discusses these issues. We could generate anonymous surveys that probe deeply into attitudes, experiences, and yes – feelings that relate to our frailties. We can review
work outside our narrow profession to design an intervention process –other specialties, other professions, state monitoring data, and administrative literature.
One possible algorithm for the atrisk surgeon:
1. Contact the SVS-sponsored task group representative to assess the surgeon.
2. Craft a plan for help that permits constructive-therapeutic intervention, and yet complies with institutional policy and state laws.
3. Create a separate professional disability insurance policy that helps make the path to recovery more appealing to the impaired surgeon who really cannot think clearly.
4. Retain attorneys with expertise in protecting the interests of the surgeon as treatment is set up.
5. Contact locum tenens employed vascular surgeons who can help fill the manpower void during this destabilizing period to soften impact on the group.
6. When stable recovery is achieved, determination is made for return to prior duties versus transfer to a location that will value the surgeon’s recovery as much as the surgeon’s productivity.
While this testimony of my experiences carries some risk for me, my story of recovery may benefit my suffering brethren. When I was successful in the societies through hard work and influence channeling, I was rewarded and valued as an asset to the profession. When I needed help at the lowest point in my life, I honestly got very little from my professional societies. My personal “research” may make this topic relevant beyond an academically sterile podium talk or a throwaway journal article.
I am happy to be my brother’s keeper although I cannot be my own keeper – such is the complex system of professional stress, addiction, and recovery. ■



POTENTIAL ADVERSE EFFECTS
The potential adverse effects (e.g., complications) associated with the use of the device are: abrupt vessel closure; access site pain; allergic reaction to contrast medium, antiplatelet therapy, or catheter system components (materials, drugs, and excipients); amputation/loss of limb; arrhythmias; arterial aneurysm; arterial thrombosis; arteriovenous (AV) fistula; death; dissection; embolization; fever; hematoma; hemorrhage; hypotension/hypertension; inflammation; ischemia or infarction of tissue/organ; local infection at access site; local or distal embolic events; perforation or rupture of the artery; pseudoaneurysm; renal insufficiency or failure; restenosis of the dilated artery; sepsis or systemic infection; shock; stroke; systemic embolization; vessel spasms or recoil; vessel trauma which requires surgical repair.
Potential complications of peripheral balloon catheterization include, but are not limited to the following: balloon rupture; detachment of a component of the balloon and/or catheter system; failure of the balloon to perform as intended; failure to cross the lesion.
Although systemic effects are not anticipated, potential adverse events that may be unique to the paclitaxel drug coating include, but are not limited to: allergic/immunologic reaction; alopecia; anemia; gastrointestinal symptoms; hematologic dyscrasia (including leucopenia, neutropenia, thrombocytopenia); hepatic enzyme changes; histologic changes in vessel wall, including inflammation, cellular damage, or necrosis; myalgia/arthralgia; myelosuppression; peripheral neuropathy. Refer to the Physicians’ Desk Reference for more information on the potential adverse effects observed with paclitaxel. There may be other potential adverse effects that are
continued from page 1
who have helped with this effort – for their time, for their insight, and for sharing their stories (some of which have been deeply personal). Two large-scale surveys were circulated to active SVS membership, both created with the assistance of the Mayo Clinic’s Division of Health Policy and Research.
The first survey was designed with a framework of validated wellness tools and well-described risk factors for burnout, then further “personalized” to incorporate unique challenges to the vascular surgeon. About 32% of our membership responded to this survey and alarmingly, when considering nonretired active SVS members, approximately one-third self-described depressive symptoms, 35% met criteria for burnout, and 8% self-reported suicidal thoughts in the last 12 months.
The second survey has only recently closed, focusing on the ergonomic challenges that we face across the spectrum of complex open and endovascular cases. Recognizing existing data that chronic pain and physical disability are associated with burnout, these data will be linked back to the original survey responses for association. Certainly there is more to come.
Concurrent with our survey initiatives, many of you participated in a Wellness Focus Group during VAM 2018. These focus groups intentionally considered the diversity of our membership across age, gender, practice setting, and region, revealing several important themes that threaten our wellness. It was no surprise that the EMR was identified as a clear threat to vascular surgery well-being and that this is not unique to our specialty. Importantly, our membership collectively feels “undervalued” at an institutional

Dr. Coleman is an associate professor of vascular surgery at the University of Michigan, Ann Arbor.
• Drafting a “public reply” to the Office of the National Coordinator for Health Information Technology’s “Strategy on Reducing Burden Relating to the Use of Health IT and EHRs” initiative.
• Collaborating with national experts to establish peer-support tools and SVS networking opportunities that may help members cope with adverse outcomes and strategize the delivery of complex care.
• Identifying institutional best practices for surgeon wellness for broad dissemination.
continued from page 1
home. We sit alone in living rooms silently mulling over the events of the day. Our spouses have seen this before and will offer sincere consolation, but will never really know how it feels. So we do what surgeons are trained to do – we suck it up and hide our feelings. As the Brits say: “Keep calm and carry on!”
A few years ago, I operated on a young woman with suspected median arcuate ligament syndrome. She had experienced temporary improvement after laparoscopic release of the median arcuate ligament at an outside hospital, but her symptoms returned after a few months.
Initially, I attempted to place a stent in the celiac artery from the groin but failed to establish a stable access sheath. Rather than choosing a brachial approach, I recommended open repair. The next day in the operating room, I was surprised to find a distinct blue tint to the adventitia of the celiac and hepatic arteries typical of dissection. After opening the common hepatic artery, I discovered that the dissection continued well into the bifurcation of the proper hepatic artery, forcing me to clamp the gastroduodenal artery, the primary collateral pathway to the liver. Within minutes, the
level. Specifically given the scope of comprehensive vascular care that we provide patients, a large part of our work includes both unpredictable acute vascular surgical care (such as intraoperative consultations for vascular trauma) and
The Wellness Task Force is now strategizing efforts for change and supporting ongoing SVS initiatives.
remedial salvage operations to manage vascular complications inflicted during care received from other physicians. This effort leaves us with little control over our time, often without perceived reciprocal clinical support, institutional support, or compensation.
Given these data, the Wellness Task Force is now strategizing efforts for change and supporting ongoing SVS initiatives. Our Task Force is currently:
• Collaborating with key EMR stakeholders with the goal of creating tools that can be shared across the specialty and addressing best practices for system-level support.

Dr. Eidt is a vascular surgeon at Baylor Scott & White Heart and Vascular Hospital, Dallas.
• Supporting existing SVS initiatives that include the PAC/APM task force, branding initiatives through the PPO as we work to “own our space” and leverage our specialty and the community practice committee as the Society works proactively to optimize workload, fairness, and reward on a larger scale for membership.
We encourage everyone to stay tuned for periodic Vascular Specialist “Wellness Features” and to attend the Wellness Session at the 2019 VAM for interim progress that will feature the following discussions.
• (Re)Finding a meaningful career in vascular surgery.
• Ergonomic challenges to the vascular surgeon and strategies to mitigate the resulting threat of disability.
• EMR best practices to optimize efficiency.
• The role of peer support in vascular surgery, including the mitigation of second victim syndrome.
Surgeon burnout is a real threat to our workforce and the well-being of our colleagues and friends. Risk factors are multifactorial and will require broad, system-level change. The SVS remains fully committed to enhancing vascular surgeon wellness and this Task Force is grateful for your ongoing engagement and support. ■
the next 3 days, leaving me depressed, anxious, and sleepless. I hated making rounds on her. Her husband was invariably lying on a couch in her room, pictures of her children taped to her headboard. I reached out to hepatology and transplant surgery hoping for some encouragement. My partners patted me on the back and reminded me that they’d all been in similar binds. I swore to myself that I’d never do another operation on a patient with median arcuate ligament syndrome.
liver turned a nauseating purple black. I urgently constructed an aorto-hepatic bypass with vein using 8-0 suture to try to tack the dissection flap into place distally. I tried to ignore the dire appearance of the liver as I worked, but I was fearful that my distal anastomosis would be inadequate. When I took off the clamps, the liver improved slightly but remained bruised. The finding of a Doppler signal distal to my anastomosis gave me some hope but I remained fearful about the viability of the liver.
Postop, I found her husband in the waiting room with two small children. I explained the potentially catastrophic circumstances and prepared him for the possibility that she might need a liver transplant. He was stunned and angry but mostly silent. Her liver function tests (LFTs) deteriorated over
On the morning of the fourth postop day, her LFTs miraculously reversed course and she made an uneventful recovery. But I was scarred. To this day, when I see the diagnosis of median arcuate ligament syndrome on a chart in the office, I shudder. I remember the color of her liver – like the deep blackness of the abyss.
Some patients leave a scar on you. But how we, as surgeons, deal with adversity is largely unknown. Each of us has to discover through trial and error the most effective way to respond to unwanted outcomes. We model ourselves after our teachers, mentors, and chief residents. Some of us have enlightened, sympathetic partners to turn to for consolation, advice, and “competent critique.” But others may be isolated in solo practice or in shared-expense practice models where “partners”
Patients continued on following page
BY LAURA M. DRUDI, MD
RESIDENT/FELLOW EDITOR, VASCULAR SPECIALIST
As I reflect upon the past year, 2018 has certainly made a mark for addressing burnout among medical professionals, enforcing wellness, and targeting implicit and explicit gender bias in medicine and surgery.
Looking back, I entered surgery with a dream to change the culture of surgery. I knew I didn’t fit the traditional mold of an aggressive or arrogant surgeon. But I thought that my empathetic, open, and compassionate ways may spark a change in paradigm for that traditional surgical ideology. However, what I encountered as I made my way on this long, ever-winding journey was a system, culture, and tradition that beats you down, and what I thought were my strengths were quickly turned into weaknesses. As I grew and matured, this loss of identity in a culture of depersonalization surrounded by gender bias, for me, was a perfect recipe leading straight to burnout. However, this was an impetus for change, to be that voice and spark for a cultural transformation of surgery and for the women who work in the specialty.
More women are entering medical and surgical specialties. However, despite the advances made there are still clear gender-based disparities influencing overall wellness and work satisfaction. For instance, a study by Meyerson et al. demonstrated that female residents receive less operating room autonomy than male ones. I see it daily within my own curriculum and in observing other female residents in other surgical specialties. Furthermore, female residents are less often introduced by their physician titles, compared with their male counterparts, are often confused as nonphysicians, and are perceived as being less competent. This influences, to no small extent, overall confidence. It’s discouraging and disheartening to have worked so hard and yet still be treated in a sexist paradigm. And to top it all off, female physicians face a motherhood penalty.
continued from previous page
may actually be competitors.
Some of the same traits that make us effective surgeons – autonomy, courage, and leadership –also make us particularly unlikely to seek outside counsel. We fear that acknowledging our humanity will be perceived as a sign of weakness. While it has become common practice in most hospitals to have programs for so-called “second victims” – for example, emergency workers, nurses, and others caring for victims of the Boston Marathon bombing – it is uncommon for surgeons to take advantage of these resources. Surgeons tend to rely on each other, like soldiers in battle, for advice, consolation, and improvement. Professionals call it “peer support” and it forms the basis of some successful peer-to-peer rehabilitation programs.

Dr.
Drudi is a vascular surgery resident at McGill University, Montreal, and the resident medical fellow of Vascular Specialist.
In a recent study by Magudia et al., out of 12 top medical institutions that provided maternity leave, only 8 did so for residents with a grand total of 6.6 weeks on average. Furthermore, women with children or women who plan to have children have constrained career opportunities and are less likely to get full professorship or leadership positions. Anecdotally, a surgeon in passing semijokingly told me that, if I were to take a specific academic vascular position, I may have to sign an agreement not to get pregnant ... probably not the job for me.
It’s appalling that, in this day and age, these explicit beliefs still exist, but what scares me more are all the implicit unconscious biases that affect all women not only in surgery but in medicine as well.
Looking back, 2018 is a year of beginning difficult conversations about physician and surgeon wellness, burnout, and gender bias. What’s obvious is that there is a hell of a lot of work to do. But change is slowly starting. We are now recognizing what the issues are, and the next step is to take action. It’s difficult to steer big ships, but there is an active community investing in strategies to improve the cultural scope of surgery and supporting and valuing women and what they have to offer. ■
References
Magudia K et al. JAMA. 2018;320(22):2372-4.
Meyerson SL et al. J Surg Educ. 2017;74(6):e111-18.
Audible Bleeding is a new podcast from the Vascular Surgery Fellowship Program at New York Presbyterian - Cornell / Columbia. Recent episodes have featured Frank Veith, Thomas Forbes, and Vascular Specialist Medical Editor Malachi Sheahan. Available through Apple, Spotify, and Google. www. audiblebleeding.com.
CACVS: Controversies and Updates in Vascular Surgery
The meeting is being held at the Marriott Rive Gauche Hotel, Paris, France, Feb. 7-9, 2019. CACVS is an international postgraduate course for vascular surgeons, cardiac surgeons, vascular radiologists, and trainees. The course is devoted to all aspects of vascular diseases and their treatments, with a special focus on the most recent available data from on-going or recently published trials.
The Charing Cross Symposium will be held Apr. 15-18, 2019, in London. The symposium assembles a world-class faculty to address key issues in vascular and endovascular treatment and to challenge the available evidence in order to reach a consensus after discussion with an expert audience.
The Congress is being held at the Lowes Miami Beach hotel, Miami Beach, on Apr. 25-27, 2019. This CME event covers the treatment of superficial and deep venous disease, including topics from sclerotherapy optimization to managing thrombophilias and discussing clot-bursting strategies.
Over the next few months, we hope to initiate a dialogue among members of the SVS community about how we can learn to best care for one another. Few of us have any formal training in how to ask for or provide assistance. We hope that you will share your stories, techniques, and best practices.
Vascular surgery is undoubtedly an immensely rewarding career, but it can bring with it very intense personal challenges.
Who do you turn to for advice in times of adversity? A spouse, trusted senior partner, a mentor, a defense lawyer, a priest, a bottle? How do you respond to your partners facing adversity? How do
you recognize in yourself, or your colleagues, that an adverse outcome has affected your ability to deliver safe, compassionate care? How do you listen for telltale signs that substance abuse, depression, or suicidal ideation have entered the equation? And what should you do next?
I’m sure that, like me, most of you are burned out on burnout. And while I don’t diminish the importance of personal resilience, I also think that we as surgeons can learn to be better caregivers for each other. That we can learn from others how to ask the right questions, and how to be more attentive listeners. Vascular surgery is undoubtedly an immensely rewarding career, but it can bring with it very intense personal challenges. Through the resources of the SVS, we hope to raise awareness of the importance of peer support, to provide a forum to share our stories, and to develop programs that will assist each of us in acquiring the tools and skills to be better partners. Your comments are encouraged. ■
BHAGWAN SATIANI, MD ASSOCIATE MEDICAL EDITOR, VASCULAR SPECIALIST
The Merriam-Webster dictionary defines value as “the regard that something is held to deserve; the importance, worth, or usefulness of something” and “relative worth, utility, or importance.” We usually assess our professional worth by how we are treated at work. In social valuing framework, we are given social status based on how others regard us for who we are, what we do, and what we are worth. This is described as “felt worth,” which encapsulates our feelings about how we are regarded by others, in contrast to self-esteem, which is more of an internally held belief.
Our power came from our relationship with our patients and our ability to communicate and influence our patients, peers, and administrators. As owners of our practices and small businesses, our currency with hospitals and lawmakers was our ability to bring revenue to hospitals and patient concerns directly to legislators. Practicing in more than one hospital made us more valuable and hospitals battled with each other to provide us and our patients the latest tools and conveniences. In return, we gave our valuable time freely without compensation to hospitals as committee members, task force members, and sounding boards for the betterment of the community. If I were a conspiracy theorist, which I am not, and wanted to devalue physicians I would seek to weaken the physician-patient bond. The way to implement this would be for a single hospital employer to put us on a treadmill chasing work relative value units, give us hard-to-accomplish goals, and keep moving the goalpost. Like I said, I do not believe in conspiracies.
The tsunami of byzantine regulations, Stark laws, and complicated reimbursement formulas has sapped our energy to counter the devaluation. Some are glad to see physicians, particularly surgeons, get their comeuppance because we are perceived as having large egos. This may be true in some instances. Yet, it turns out that the top three job titles with the largest egos are private household cooks, chief executives, and farm and ranch managers.1
Physicians are also reputed to be possessing dominant leadership styles and seen as bossy and disruptive. Hence, we are made to have frequent training in how to ameliorate our disruptive behavior tendencies. Again, this may be true in a few cases. However, while reports mention how many people witness such unacceptable behavior, there are no valid data about the incidence in practicing physicians. Research also does not support the view that physicians have dominant and aggressive personalities leading to such behavior.
One of the leading interpersonal skills model is Social Styles. We happen to teach this to our faculty at the Ohio State Medical Center’s Faculty Leadership Institute. Turns out that physicians and nurses are almost equally placed into the four quadrants of leadership styles: driving, expressive,

Dr. Satiani is professor of clinical surgery in the division of vascular diseases and surgery at Ohio State University, Columbus. He blogs at www.savvy-medicine. com. Reach him on Twitter @savvycutter.
amiable, and analytical. I found similar findings in our society members participating in a leadership session I moderated. Indeed, we rank very high on “versatility,” a measure that enables us to adapt our behaviors to fit with our patients and coworkers.
Reported burnout rates of 50% in physicians may or may not be accurate, but burnout is real and so is depression and so are physician suicides. I have witnessed six physician suicides in my career thus far. Teaching resilience, celebrating doctor’s day, and giving out a few awards are all interventions after the fact. Preventive measures like employers and hospitals prioritizing removing daily obstacles, eliminating meaningless work, providing more resources to deal with EMRs, and making our lives easier at work, so we can get to our loved ones sooner would help.
Physicians have been largely excluded from participating in the health care debate. We want to see empirical evidence before we sign on to every new proposed care model. Otherwise, we cling on to the status quo, and therefore, decision makers tend to leave us out. More important, value-based payment models have not thus far led to reduction in the cost of health care. Despite poor engagement scores at major health systems, physicians are “managed” and sidelined, and mandates are “done to them, not with them.”
In my 40-year career, our devaluation has been a slow and painful process. It started with being called a “provider.” This devalues me. Call me by what I am and do. Physician. Doctor. That is what our patients call us. But, we have been pushed to acquiesce. So, why do physicians undervalue themselves and are unable to be confident of their value to employers and hospital executives?
Some have theorized that physicians have low self-esteem and that denial and rationalization are simply defense mechanisms. The low self-esteem is traced back to medical student days and considered “posttraumatic” disorder. In one study of 189 medical students, 50% reported a decrease in their self-esteem/confidence. The students blamed their residents and attendings for this reaction. Some degree of intimidation may continue into training and employment where it may be part of the culture. We need to change this cycle and treat our students, residents, and mentees with respect as future peers.
Another aspect is related to our own well-being. Most physicians value their patient’s health more than their own. That concept is drilled into us
throughout our life. Our spouses complain that we care more about our patients than we do for our families. We often ignore warning signs of serious issues in our own health, always downplaying textbook symptoms of burnout, depression, and even MI. Being too busy is a badge of honor to indicate how successful and wanted we are. This also needs to change.
Sheryl Sandberg in her book “Lean in” discusses the “tiara syndrome,” mainly referring to women. I would suggest that this applies to a lot of physicians, both men and women. Physicians tend to keep their heads down, work hard, and expect someone to come compliment them and place a “tiara” over their head. We may be wary of being called “self-promoters.” Sometimes it is cultural baggage for immigrant physicians who are taught to not brag about their accomplishments. It may behoove us to judiciously make peers and leadership aware of our positive activities in and outside the health system.
Some see physicians not as “pillars of any community,” but as “technicians on an assembly line” or “pawns in a money-making game for hospital administrators.” This degree of pessimism among physicians in surveys is well known but there is good news.
In a 2016 survey based upon responses by 17,236 physicians, 63% were pessimistic or very pessimistic about the medical profession, down from 77% in 2012.2 In another poll, medical doctors were rated as having very high or high ratings of honesty and ethical standards by 65%, higher than all except nurses, military officers, and grade school teachers.3 When the health care debate was at its peak in 2009, a public poll on who they trusted to recommend the right thing for reforming the health care system placed physicians at the very top (73%) ahead of health care professors, researchers, hospitals, the President, and politicians. Gallup surveyed 7,000 physicians about engagement in four hierarchical levels: Confidence, Integrity, Pride and Passion. Physicians scored highly on the Pride items in the survey (feel proud to work and being treated with respect).4 In other words, if we are treated well, we feel proud to tell others where we work.
Finally, like many I may consider myself an expert in all sorts of things not relevant to practicing medicine. Yet, I respectfully suggest we stay away from political hot potatoes like nuclear disarmament, gun control, climate change, immigration, and other controversial issues because they distract us from our primary mission. I would hate to see us viewed like Hollywood. ■
References
1. www.chicagotribune.com/business/ct-payscaleego-survey-0830-biz-20160829-story.html.
2. www.medpagetoday.com/primarycare/generalprimarycare/60446.
3. https://nurse.org/articles/gallup-ethical-standards-poll-nurses-rank-highest/.
4.https://news.gallup.com/poll/120890/healthcare-americans-trust-physicians-politicians.aspx.

Carotid artery disease higher in the neck may be difficult to treat with CEA.
TCAR may be your option. With thousands of real world patients studied, TCAR has shown to be a safe and clinically effective alternative to CEA. A high cervical lesion in the carotid artery
Other patients who could benefit from carotid revascularization through robust reverse flow include:*
• AGE ≥75
• CONGESTIVE HEART FAILURE
• ≥2 DISEASED CORONARIES WITH ≥70% STENOSIS
• SEVERE PULMONARY DISEASE
• SURGICALLY INACCESSIBLE LESION
• PRIOR HEAD/NECK SURGERY
• RESTENOSIS POST CEA
• IRRADIATED NECK
• CONTRALATERAL OCCLUSION
• BILATERAL STENOSIS REQUIRING TREATMENT
• SEVERE TANDEM LESIONS
*Reimbursement eligible criteria for the TCAR Procedure per the Medicare National Coverage Determination (20.7) on PTA including CAS
Please
BY AMY B. REED, MD APDVS PRESIDENT
In 2015 the Association for Graduate Medical Education (ACGME) began requiring programs to educate and instruct residents and fellows in areas of well-being. A myriad of education tools became available for programs directors (PDs) on self-care, resiliency, battling sleep-deprivation, and how to spot depression in a trainee. Almost overnight PDs were expected to become experts themselves on these topics or find someone who was. Yet what about the educating the educator? Training the trainee? Might it not be a far cry to say that many in our midst were equally in need of education and tools on how to handle our own issues with resiliency, depression, and care-giving fatigue? Could we effectively model exemplary behavior to our own residents and fellows?

Dr. Reed is a professor and chief of the division of vascular surgery at the University of Minnesota, Minneapolis.
2017 APDVS meeting where PDs discussed the incredible burden from the electronic health record, the increasing number of training program rules and bloated requirements, and the snowballing requirements from hospital administration regarding supervision and record keeping. Dr. Sinsky’s talk highlighted that more than 70% of faculty / physician burnout is due to system issues that need addressing from an administrative standpoint in health systems – not more yoga!
The Association of Program Directors in Vascular surgery (APDVS) brought Christine A. Sinsky, MD from the American Medical Association (AMA) to the 2018 APDVS meeting to speak on “Physician Well-Being: Bringing the Joy Back to Practice.” This was in response to the overwhelming response and discussion from the floor at the
Having taken the SVS “burnout” survey, I felt that it really never got into the “whys” of what was making individuals burn out. It dealt more with the consequences of the whys rather than the whys themselves, and it is these whys that must be addressed to assist in the prevention of burnout. I would like to comment on my experience of some, certainly not all, of the possible whys related to both inherent stressors and “administratorinduced stressors” encountered in my 42-year vascular surgery practice that can easily cause burnout.
I believe there are several major areas that need to be evaluated to understand the causes of burnout because the complexities of today’s practice environment demand a different approach to the practice of vascular surgery for the well-being of the vascular surgeon. These complexities include the emotional baggage inherent in a practice, practice structure, unpredictable time-management issues of running a practice, and hospital administration’s decisions creating unintended consequences for the vascular surgeon. By its very nature, vascular surgery is a difficult field with many inherent stressors, endovascular innovations notwithstanding. The initial emotional stressors may well be those of dealing with elderly patients with multiple severe comorbidities, poor outcomes, and the ensuing consequences. With the aging of the
population, these stressors will only increase, yet compensation to treat these feeble patients has yet to rise to a level commensurate with the risk factors and complications the surgeon must deal with. Over time this will take its toll on some.

The APDVS is committed to working on making the lives of our PDs – as well as our vascular trainees – easier. Sharing evaluation and interview forms, as well as curriculum presentations help keep PDs from recreating the wheel at midnight. Sharing tips and tricks in our training programs, helping each other out, and highlighting best practices can help all of us get out of the hospital and onto the yoga mat! ■
the work and split the gain equally in return for the most valuable commodity of all: free time.
Time management is of paramount importance in completing a schedule, yet the paradox of the vascular world is its inherent un-
By its very nature, vascular surgery is a difficult field with many inherent stressors, endovascular innovations notwithstanding.
Which practice pattern one chooses to utilize – solo, group, or employed – also plays an important part. The presence or absence of appropriate help and backup for difficult cases, call coverage, and partnership financial packages can be either very stress producing or stress relieving. Are practice responsibilities and finances equally split so as to achieve a reasonable lifestyle, or is there a hierarchy of work and financial gain by which some must shoulder more of the burden for less pay than others? This is the beginning of the income versus lifestyle conflict and becomes a seriously stressful trap when one is short sighted and does not go for the long term. In our practice, we rotate
predictability. There are difficult, time-consuming cases; unexpected, recurrent vascular problems in the same patient; urgent consults needing treatment within a few days; and the inevitable emergency room call for immediate treatment, day or night, for an embolism, vascular trauma, or ruptured aneurysm – not to mention the hospital committees or other responsibilities in the everyday life of a vascular surgeon.
One’s schedule requires dedicated time and attention yet the urgent/ emergent issues interrupting one’s daily schedule ensures that the only predictability is unpredictability. This is a source of burnout. My experience over the years has been
that about 25% of our practice load comes on an urgent to emergent basis, often causing considerable scheduling problems both in the operating room and at the office – again, issues that can cause tremendous stress for many. Without a large group, these constant stressors become difficult to shoulder.
Then there are the hospital-induced stressors caused by poorly conceived administrative decrees. One example is when emergency rooms need vascular services but no contracts are offered to secure these services, in which physicians are merely expected to provide 24/7 services. Once a physician has been called in for a case in the middle of the night, the stress of carrying on the next day becomes greater for that physician unless a system is in place for designated calls, which some larger groups have worked out.
Another example is the tendency to grant interventional privileges to those incapable of treating their operative complications without any consideration for who would reimburse those who come in after and how. Why is it assumed that vascular surgeons would/should take time out of their practice to answer the call without any additional compensation? If the compensation from these service lines is so lucrative, then compensation in the form of contracts needs to be offered to those who can provide the necessary
LESIONS ACROSS THE ELBOW
Thrombosed AV grafts
Complex iliac lesions
In-stent restenosis of the SFA
PTA failures of AV graft lesions
Long SFA lesions
Chronic total SFA occlusions






Physicians are achieving durable outcomes across the elbow with fewer reinterventions in rapidly failing AV access circuits. See the NEW case study at goremedical.com/viabahn/elbow
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® Endoprosthesis is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery de novo and restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 –7.5 mm, in superficial femoral artery in-stent restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 6.5 mm, and in iliac artery lesions up to 80 mm in length with reference vessel diameters ranging from 4.0 – 12 mm. The GORE® VIABAHN® Endoprosthesis is also indicated for the treatment of stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous (AV) access grafts.
CONTRAINDICATIONS: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is contraindicated for noncompliant lesions where full expansion of an angioplasty balloon catheter was not achieved during pre-dilatation, or where lesions cannot be dilated sufficiently to allow passage of the delivery system. Do not use the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface in patients with known hypersensitivity to heparin, including those patients who have had a previous incidence of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at goremedical.com for a complete description of all warnings, precautions and adverse events. Only
Images courtesy of Minneapolis Vascular Physicians. Used with permission. W. L. Gore & Associates, Inc. | Flagstaff, AZ 86004 | goremedical.com Products listed may not be available in all markets.
®, VIABAHN®, and designs are trademarks of W. L. Gore & Associates. © 2018 W. L. Gore & Associates, Inc. AX1547-EN1 DECEMBER 2018
BY VIVIAN GAHTAN, MD CHAIR, VASCULAR SURGERY BOARD-AMERICAN BOARD OF SURGERY
Maintenance of Certification (MOC) is an American Board of Medical Specialties (ABMS) requirement for their 24 member boards. The MOC process has received much criticism, especially in recent years. To date, a 5-hour exam at a secure testing center every 10 years covering comprehensive vascular surgery knowledge has been the routine. This requirement had the surgeon take off a day from work for the exam, in addition to the time it took to prepare. Burnout, at least in part, is related to the sheer volume of busywork not directly relevant to being a practicing surgeon.
The American Board of Surgery is sensitive to both the relevance of MOC and needs of the diplomate, and is striving to make appropriate changes. Diplomates were surveyed regarding MOC and the accompanying exam in both 2016 and 2017. Using this input, the development of the 10-year exam format was studied carefully by the board directors and executive staff, all of whom are active in the clinical practice of surgery, and a new process now known as Continuous Certification was introduced. The intent of the new Continuous Certification Assessment (to replace the every-10-year MOC exam) is to be an activity that is convenient, timely, and more reflective of the surgeon’s daily practice. The assessment is to be done every 2 years and is online, open book, and taken at a place of the examinee’s choosing, such as the home or in the office. Another key feature of the continuous certification process is that the total number of CME required is decreased and the self-assessment requirement is eliminated.
In November 2018, I took the first General Surgery Continuous Certification Assessment. There was approximately a 2-month window to register, and online registration was simple, taking only about 15 minutes to complete. All the references were listed on the ABS website and the vast majority were open access and directly linked to the article. For those articles that were not open
Burnout from page 10
services to treat the inevitable complications. This will in some way help compensate for time lost in the vascular surgeons’ practices.
The contracts should reflect the value to an institution vascular surgeons bring for their presence, including ED coverage for most if not all of the service lines, such as cardiology, radiology, orthopedics, gynecology, and general surgery. This also includes

Dr. Gahtan is professor and chief, division of vascular surgery and endovascular services, State University of New York Upstate Medical University, Syracuse.
access, there was a link to the PubMed abstract. I downloaded all of the articles (actually this part my assistant did) and requested five articles from the library. I did not review the articles in advance, but used them when going sequentially through the assessment questions. Depending on
Overall, there has been much positive feedback. Of the 2,164 diplomates taking the Continuous Certification Assessment, only 21 were unsuccessful.
the article, I read it or looked up the specific aspect I was looking for. I worked on the test three different times – at the airport during a long layover, at home, and at my office. After answering each question, I received feedback on what was the correct answer and a one-paragraph explanation which I read completely. After completing all 40 questions, each question for which I had an incorrect answer (not more than 1 or 2 of course, Ha!) was shown again with the opportunity to answer the question. The total time it took me was about 4.5 hours. All in all, it was a good experience, and I learned something. The general surgery assessment is modular.
issues arising from the house staff inserting lines and from subsequent renal failure, as well as for angio-access patients who need immediate vascular backup to treat the vascular complications encountered.
In addition, these contracts should acknowledge the revenue generated by the presence of a vascular service line. With the burnout rate and unpredictable lifestyle, one would be
Twenty questions (half) were core surgery topics, and the other 20 questions came from one of four specialty modules of the examinee’s choice – breast, abdomen, alimentary tract, or comprehensive general surgery. I took the core and the abdomen modules. The core topics were, for the most part, areas that a surgeon who does patient care would find relevant (for example, perioperative management of a patient on corticosteroids, postoperative delirium, and prophylaxis for venous thromboembolism).
A couple of other details should be mentioned about this new process. From the time of initiation of the assessment, there are 2 weeks allocated for completion. One needs 80% correct to pass. If the examinee receives less than 80% but higher than 40% on the first assessment attempt, he/she will have a second attempt to answer the questions that were incorrect on the first try. If a cumulative score of less than 80% is achieved after the second attempt, a grace year will be provided, which is an extension of certification for 1 year with the opportunity to take the next year’s assessment. If after the grace year (four attempts) the diplomate is unsuccessful, then a secure exam is required to regain certification.
Overall, there has been much positive feedback. Of the 2,164 diplomates taking the Continuous Certification Assessment, only 21 were unsuccessful. Therefore, the pass rate was over 99% for the inaugural year. The average examinee took just over 3 hours to complete the assessment.
In 2018, the 10-year recertification examination in vascular surgery with 10 years of credit was given for the last time. The Vascular Surgery Continuous Certification Assessment is in preparation now and will roll out in the fall of 2019. It will follow a format similar to general surgery with 40 questions on a number of topics in vascular surgery. However, the vascular surgery assessment will not be modular. This activity will incorporate general knowledge (for example, from consensus guidelines), as well as late breaking trials. So far, this process looks to be a better one, as well as more efficient and relevant for the busy surgeon. ■
concerned that vascular surgeons could be on the endangered species list; and given the current shortage of vascular surgeons, don’t our numbers reflect this concern?
There are no easy solutions because the field is a difficult one and is undercompensated for the risks assumed and services provided, which makes it an unattractive specialty, especially in today’s lifestyle-conscious generation. The vascular specialty is embattled, and the human toll extracted in the field speaks for itself. The rewards must improve to make
things more appealing, and this will lead to an increase in the number of vascular surgeons, and more will join in groups to mitigate the effects of the stressors of the field. Until then, vascular surgeons need to demand that they receive fair compensation for their availability and the coverage they provide, which allows many other departments and specialties to function. This reality must be acknowledged and compensated. ■
Carlo A. Dall’Olmo, MD Michigan Vascular Center Flint
BY BRUCE JANCIN MDEDGE NEWS REPORTING FROM THE NORTHWESTERN VASCULAR SYMPOSIUM
CHICAGO – Home-based exercise for peripheral arterial disease–related walking limitations works at least as well as – and arguably better than – the supervised outpatient hospital clini–based treadmill exercise programs of the type approved for coverage by the Centers for Medicare & Medicaid Services in 2017, Mary M. McDermott, MD, said at a symposium on vascular surgery sponsored by Northwestern University.
“The prevailing thinking is that supervised treadmill exercise is more effective than home-based exercise for PAD. And for the outcome of treadmill walking that is true. But for the outcome of 6-minute walking distance, which I would argue is more relevant to walking in daily life, home-based exercise programs appear to be better. Supervised treadmill exercise interventions preferentially improve treadmill walking performance, and that doesn’t translate as well to walking in daily life. Home-based exercise, where patients walk in a corridor or on the ground, is more relevant to the type of walking that they want to do,” explained Dr. McDermott, professor of medicine at the university as well as a leader in the field of research on exercise as a treatment for PAD.
However, she added a caveat regarding homebased exercise for symptomatic PAD: For it to be

Leg Study (GOALS) – a 6-month group-mediated cognitive-behavioral intervention in which PAD patients built up to walking at home for up to 50 minutes per session 5 days per week – 6-minute walking distance (6MWD) remained significantly better than in controls at follow-up after completion of the intervention. In fact, 6MWD actually increased further between 6 and 12 months in the home exercise group (J Am Heart Assoc. 2014 May 21;3[3]:e000711. doi: 10.1161/JAHA.113.000711). Dr. McDermott was the lead author for this study.
• The exercise program must consist of 12 weeks of thrice-weekly sessions.
• It has to be prescribed by a physician following a face-to-face meeting with the patient during which the physician provides education on cardiovascular risk prevention.
• An additional 36 sessions of supervised exercise can be obtained with a written note of justification by the physician following completion of the initial 12 weeks.
• The sessions must take place in a physician’s office or an outpatient hospital setting.
• The exercise has to be supervised by a physician, physician assistant, or nurse specialist.
• The exercise must be delivered by qualified personnel trained in basic and advanced cardiac life support as well as exercise therapy for PAD.
effective it must incorporate proven behavioral change techniques, including goal setting, monitoring progress, accountability to a coach, and face-toface visits at least once per month.
“It seems you can’t just tell PAD patients to go home and walk because most of them won’t do it,” observed Dr. McDermott, who is a general internist and geriatrician.
Home-based exercise programs aren’t reimbursed by the CMS. But studies by Dr. McDermott and other investigators indicate that the results are more durable than for supervised treadmill exercise. For example, in the Group Oriented Arterial
In contrast, another study by Dr. McDermott now in press for the same journal found that the improvement in 6MWD achieved in PAD patients over the course of a 6-month supervised treadmill exercise program was not maintained during the next 6 months after completion of the intervention. Indeed, 6MWD showed a steady decline from its apex at the intervention’s conclusion, such that at the 12-month mark it was no longer significantly different from that of the control group, according to Dr. McDermott.
The Society for Vascular Surgery recommends a supervised exercise program as first-line therapy
for PAD patients with intermittent claudication, with a Class I Level of Evidence A designation. Home-based exercise also gets a Class I recommendation, albeit with Level of Evidence B.
Dr. McDermott believes a home exercise program makes the most sense for PAD patients after their CMS benefit for a supervised clinic-based program has run out, or for patients – and there are a great many – who either can’t or don’t want to participate in a supervised program. She and others who’ve led randomized controlled trials of supervised exercise programs have found that close to 70% of eligible PAD patients decline to participate because of the inconvenience of going to the hospital outpatient facility at least three times per week or for other reasons.
“Also, it’s important to recognize that attendance can be a challenge, even when supervised exercise is covered by insurance. In our randomized trials, where we provide transportation, we still see only 65%-70% adherence to attendance,” she noted.
She stressed that it’s crucial for physicians and surgeons to educate their PAD patients about what to expect from an exercise program, be it supervised or home based.
“It’s not like revascularization, where they’re going to feel better in their walking immediately. It really takes a commitment. Four to six weeks is usually required before patients begin to experience a benefit, and I think it’s really important for patients to know that so they don’t get discouraged in the first couple of weeks,” Dr. McDermott said.
Turning to the key evidence-based behavioral change techniques shared by successful home-exercise programs for PAD, she noted that the GOALS trial intervention utilized weekly group sessions in which simple cognitive-behavioral self-regulatory techniques were used to help patients set and stick to home-based walking goals. A similarly positive randomized controlled trial by investigators at the University of Oklahoma utilized once-monthly group meetings at the medical center (J Am Heart Assoc. 2014 Sep 18;3[5]:e001107. doi: 10.1161/ JAHA.114.001107).
In contrast, in the recent HONOR randomized clinical trial, where Dr. McDermott and her coinvestigators tested whether a home-based exercise intervention in which the active treatment group utilized a Fitbit wearable activity monitor and telephone coaching over the course of 9 months, the results proved disappointing. The intervention was no more effective than was usual care at improving 6MWD (JAMA. 2018 Apr 24;319[16]:1665-76).
“One of the things I learned from doing this trial is that for a home-based exercise intervention in PAD to be successful, it’s not easy and there really needs to be some ongoing contact with a coach or nurse or a staff member that the patient feels accountable to. A wearable device is not a durably effective motivator for PAD patients. I think the reason this trial didn’t work so well is that most
Exercise continued on following page
BY ALICIA GALLEGOS MDEDGE NEWS
Apatient is suing you. Now what? Legal experts warn that a doctor’s first steps after a lawsuit can dramatically impact the outcome of the case. Below, medical malpractice defense attorneys share the most important do’s and don’ts for physicians after they receive a lawsuit notice.
• Do contact your insurer and/ or risk manager. Once you receive notice of a lawsuit, the first step is calling your medical malpractice insurer and/or risk manager, said Steven Fitzer, a medical liability defense attorney based in Tacoma, Wash. The insurer and risk manager will take the matter from there and advise your next moves. Resist the urge to disregard the notice and hope that the challenge goes away when the patient is no longer angry, he said. Failing to notify the insurer in a timely manner could be a policy violation and affect current or future coverage.
• Don’t contact the plaintiff/patient or patient’s family. Instinctively, many physicians feel compelled to call the patient and attempt to settle the conflict verbally, particularly if they have had a longstanding relationship, Mr. Fitzer said in an interview. Don’t do it. “In 42 years, I’ve never come across a physician who successfully talked somebody out of a lawsuit, once it was started,” he said. “It’s a pipe dream.” Keep in mind that conversations with patients after a lawsuit filing can be used against doctors in court and certain words can easily be misconstrued as admissions of guilt.
continued from previous page

• Do secure all medical records pertaining to the case. Obtain and print copies of all information relevant to the patient’s suit, such as history, billing records, letters, and medical chart. Store the data in a secure location in preparation for transferring to the insurer and/or attorney, said Michael Moroney, a medical liability defense attorney based in Teaneck, N.J.

• Don’t access or change the record. It may seem tempting to review the plaintiff’s medical record and fix any errors found. However, accessing the patient’s electronic data can appear as an attempt to manipulate or delete relevant data, said Joshua R. Cohen, a medical liability defense attorney based in New York.
“Avoid accessing [the] EMR or PAC system [and] leaving a digital fingerprint,” he said in an interview. “For example, if a radiologist is sued for an alleged failure to diagnose breast cancer, they should not open that study on their computer as an audit trail will show that. Worse is when they start making measurements after the lawsuit which are now discoverable as part of the lawsuit.”
Leave the record alone and let the attorneys handle the data, he advised.
followingof it was by telephone and it was easy for patients to avoid our calls if they weren’t walking. Patients were initially really enthusiastic about the Fitbit, but we found that over time they stopped wearing it,” she said.
Dr. McDermott heartily endorses the Society for Vascular Surgery’s Class I recommendation that all PAD patients with intermittent claudication should exercise regularly, including those who’ve undergone revascularization procedures. Numerous clinical trials have demonstrated additive clin-

• Do discuss the patient case openly with your attorney and risk manager. Honesty about all aspects of a medical case from the start sets the right tone for a positive relationship between doctor and attorney, experts say. Help your attorney understand the medicine so that they can speak intelligently about the details to the court and any retained experts, Mr. Fitzer recommended. If disagreements continually arise among physicians and attorneys, and the match fails, consider speaking to the insurer about changing attorneys.
• Don’t discuss the case. As Mr. Fitzer puts it, “loose lips sink ships.” Physicians lose confidentiality protections when they talk about lawsuit details with third parties, and those conversations could come back to haunt them. This includes colleagues and staff members in the patient’s care loop, said Catherine Flynn, a medical liability defense attorney also based in Teaneck. The third parties could later be questioned by the plaintiff’s attorney about the case.
“It’s like that kid game of telephone where you say something to the nurses and then a year later, they’re deposed, and their recollection is very different,” Ms. Flynn said in an interview. “It turns into something that you did not say.”
Your spouse is the exception. Most states protect conversations among spouses and bar husbands and wives from having to testify against their spouse.
ical benefits for opening the peripheral artery and strengthening skeletal muscles.
Uptake of supervised exercise programs for symptomatic PAD since the CMS coverage decision is quite variable regionally. Integrating new programs into existing cardiac rehabilitation facilities is a natural fit because staff members are very familiar with structured treadmill exercises already on site, but some freestanding programs are run by vascular surgery groups or cardiologists.
“I think part of the reason it hasn’t been taken up faster is that the reimbursement is such that you’re not going to make money on it,” Dr. McDermott said.
Asked if all patients with PAD should undergo
• Do alert staff to the lawsuit and track any document requests. Following a lawsuit notice, inform staff that a claim has been filed by a patient – without going into detail. Be alert to document requests by nonpatients and make sure your attorney is aware of such requests. For example, some plaintiffs hire a private investigator to contact the medical practice and attempt to obtain records, Mr. Moroney said. In other cases, the plaintiff’s attorney or their paralegal tries to get copies of the medical chart or billing records.
• Don’t release any patient data to third parties. Ensure that staff members do not provide any patient information to the plaintiff’s attorney or other third parties, Mr. Moroney said. All relevant records should go through your attorney. No questions about the patient or the circumstances of the complaint should be divulged by the doctor or staff members to any third party, he said.
• Do seek emotional support from family and friends. Facing a lawsuit can be draining, both physically and mentally. Make time for self-care and lean on loved ones when needed, Mr. Fitzer said. Sharing your feelings –without going into detail about the case – can help relieve stress and reduce the emotional strain.
• Don’t isolate yourself. “This can be an isolating experience,” Mr. Fitzer said. “You need support. You need reinforcements. Take care of yourself and your family – they are your biggest source of support.” ■
an exercise treadmill test before embarking on an exercise program, Dr. McDermott replied, “I’m part of a writing group for the American Heart Association on how to implement these new guidelines. We’re not formally recommending a stress test. Some cardiologists on the panel suggested that it should be individualized based on patient history and symptoms. If they’re having symptoms of chest pain or they have a significant cardiac history, go ahead with a stress test. I don’t think it’s going to be recommended as a routine practice, but it’s safest to get a stress test.”
She reported having no financial conflicts regarding her presentation. ■
bjancin@mdedge.com


EXPERIENCE THE DIFFERENCE IN




























Choose the distinctive performance of our balloon dilatation catheters
Complete support for complex BTK cases
PINNACLE® DESTINATION®
Guiding Sheath

Support Catheters
Engineered to provide best-in-class PUSHABILITY* with a small profile for accessing target lesions1 Demonstrated excellence in CROSSABILITY with a low deflation time1
*Tested against select leading competitors

ADVANTAGE® Peripheral Guidewires
GOLD Hydrophilic Coated Guidewire
When RX tested against Boston Scientific Sterling™ Monorail™ and OTW tested against Bard Ultraverse® 0.018"

This year’s Vascular Annual Meeting will have a new and elegant air about it, with the introduction of a Gala to benefit the SVS Foundation. It is replacing the traditional President’s Reception, at the request of SVS President Michel S. Makaroun. Dr. Markaroun wants an event to not only celebrate with colleagues but also to benefit a cause close to his heart, the SVS Foundation.
Tickets are $250 each, of which $150 is a tax-deductible contribution to the SVS Foundation’s general Greatest Need Fund.
The Gala will be held Friday, June 14, at the Gaylord National Resort & Convention Center, the site for VAM. The evening will include:
• A Silent Auction, in which any member (or friends) can participate via an online portal through the duration of the event. The Silent Auction will open several weeks before the meeting.
• Cocktails and dinner.
• A program, including entertainment.
“Other medical societies host galas at their annual meetings. I wanted something similar to bring our leadership and membership together to celebrate vascular surgery as a specialty,” said Dr. Makaroun.
“And bringing people together will benefit the signature work of the SVS Foundation,” he said, “Its various grants, scholarships and projects touch
R
every single SVS member, whether in academia or private practice.”
Many of the details are still in the planning stages but the link to purchase tickets, plus the opportunity to donate auction items, should be available later this month.
In the meantime, Dr. Makaroun urges members to be gearing up for a great time. “This will be a signature event of the Vascular Annual Meeting,” he said. “Much as the Presidential Address brings everyone together in one place, so will our gala.”
The 2019 Vascular Annual Meeting will be June 12 to 15 at the Gaylord National Resort and Convention Center in National Harbor, Md., just outside Washington, D.C. Scientific sessions

will be June 13 to 15 and exhibits will be June 13-14. Registration and housing will open in early March. ■
egistration is now open for The SVS’s Vascular Research Initiatives Conference (VRIC) 2019. VRIC will be held this year on May 13 in Boston, Mass., the day before the American Heart Association’s (AHA) Vascular Discoveries meeting (previously known as ATVB meeting). VRIC is the premier vascular venue for emerging vascular science and translational research important to vascular patients, and VRIC welcomes both clinicians and clinician scientists interested in developing future therapeutics and devices for vascular patients.
• Atherosclerosis, arterial injury and diabetes, a session designed to be of interest through the vascular surgeon community
Updates from young vascular surgeon-scientists on KO8 projects:
• Mohamed Zayed, MD, PhD; Washington University

VRIC’s theme this year is “Hard Science: Calcification & Vascular Solutions.” VRIC presenters also have the opportunity to present their work on Tuesday night as a poster at Vascular Discoveries.
“We are particularly excited to host VRIC in Boston, which has such a rich tradition for vascular surgery. As such, the SVS Research and Education Committee is working with the AHA and our local programming committee to provide cutting-edge scientific sessions and social programming to best assist both junior and established surgeon investigators to pursue meaningful research and form collaborations broadly with world renowned scientists,” said Dr. Luke Brewster, committee chair.
“On behalf of the R&E committee, we are particularly grateful to vascular surgeons Peter Henke, Keith Ozaki and Raul Guzman for help integrating SVS members and vascular topics into Vascular Discoveries and for help establishing the local program committee for this destination event for vascular surgeon-scientists,” he added.
Highlights of VRIC include:
VRIC abstract sessions:
• Aortopathies and novel vascular devices
• Vascular regeneration, stem cells and wound healing
• Mechanisms and advanced therapies for venous disease
• Karen Woo, MD, MS; University of California Los Angeles Alec Clowes Lecture:
• Cecilia Giachelli, PhD, will present the Third Annual Alexander W. Clowes Distinguished Lecture. She is the W. Hunter and Dorothy Simpson Endowed Chair of Biomedical Engineering at the University of Washington. She is an expert in vascular calcification, the past-president of North American Vascular Biology (NAVBO) and a friend/colleague of the late Dr. Clowes. Translational Session: Hard Science: Calcification and Vascular Solutions
• VRIC’s translational session will include keynote presentations from experts in vascular calcification and provide a forum for attendee input into solutions for this crippling problem. Vascular calcification experts Raul Guzman, MD, Dwight Towler MD, PhD, and Elena Aikawa MD, PhD will speak on the knowns and unknowns of this devastating disease.
“We are emphasizing that this venue is the place to discuss your research and develop your professional networks throughout the day,” said Dr. Brewster. Specifically, and new to VRIC 2019, organizers plan a “walk-about lunch” during which attendees can mingle between tables and preview VRIC posters prior to the cocktail reception that evening. “VRIC provides a forum for re-visiting old friendships and initiating new ones for dedicated surgeon-scientists of all ages,” said Dr. Brewster. “By liberating the lunch hour, we hope to create an additional hour for networking and scientific discussion for our attendees.” For more information, visit vsweb.org/VRIC19 ■
Rosemont Move Offers Room to Grow Programming, Value A new Quality Council. A new Appropriateness Committee. Task forces exploring workforce shortages in vascular surgery, burnout and wellness, and a vascular center verification program for inpatient and outpatient settings. A new Section within the Society for Vascular Surgery for physician assistants and another in process for Outpatient Vascular Care. A member engagement and networking site. A management home for the Society for Vascular Nursing, Delaware County Vascular Society and Association for Program Directors in Vascular Surgery. An expanded SVS Foundation mission.
These are just a handful of the new initiatives launched recently, aimed at building and sustaining additional value for SVS members and the specialty.
“We are in a time of significant programmatic expansion and outreach to offer more services to our members,” said SVS President Dr. Michel S. Makaroun. “We are expanding our Vascular Quality Initiative with new registries, introducing a revolutionary verification program for vascular centers and looking at tackling appropriateness of care, just to name a few endeavors.”
Programming, of course, means people to help run them on the SVS side. That’s just one impetus for the Society’s upcoming move in February to a new and larger headquarters in Rosemont, Ill., near O’Hare Move continued on following page
Applications for many SVS and SVS Foundation awards, grants and scholarships are due Feb. 1 and March 1. Visit vsweb.org/ Awards for more information on these and all SVS and SVS Foundation awards.
Feb. 1 Deadlines
SVS
Excellence in Community Service Award: A new award to honor a member with a minimum of 20 years as a practicing vascular surgeon who has exhibited outstanding leadership within his or her community as a practicing vascular surgeon.
SVS/ACS Health Policy Scholarship: An $8,000 award to attend the Executive Leadership Program in Health Policy and Management at Brandeis University in June.
SVS Foundation
Student Research Fellowship: Designed to stimulate laboratory and clinical vascular research by undergraduate and medical students registered at

universities in the United States and Canada.
March 1 Deadlines
SVS
Lifetime Achievement Award: SVS’ highest honor, recognizing an individual’s outstanding and sustained contributions to both the profession and to SVS.
Medal for Innovation in Vascular Surgery: Honoring an individual or individuals whose contributions have had a transforming impact on the practice or science of vascular surgery.
Distinguished Fellow: Designation bestowed on members who have distinguished themselves through sustained and substantial contributions in two of these categories: research, service or education.
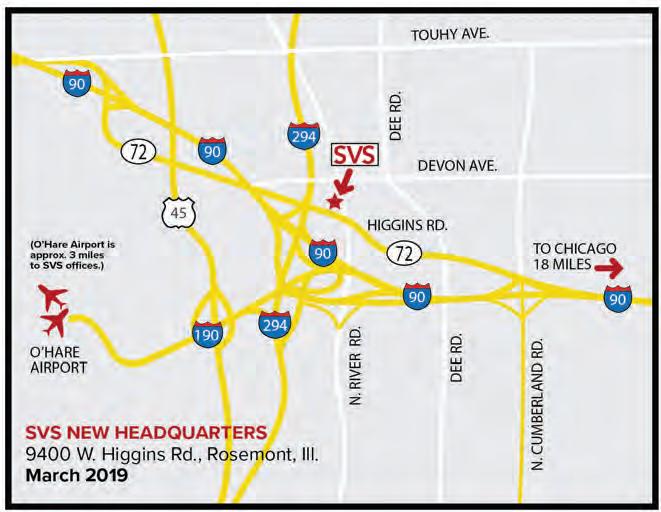
continued from previous page
International Airport.
“We’re a growing, thriving organization, evolving to keep pace with the specialty,” said SVS Executive Director Kenneth M. Slaw, PhD. “So where our members see the need, we are following with the creation of task forces, study of issues and implementation of programs.”
One such venture, currently in planning and exploration with members, is a revitalized branding initiative. The multi-faceted campaign will include messaging that positions vascular surgeons as comprehensive care experts and creating
referral materials for primary care providers and other physicians as well as educating the public about why a vascular surgeon is the logical and perfect choice to provide their care. SVS members involved in the project met earlier this month to begin mapping out an implementation plan.
The new headquarters, at 9400 W. Higgins Road, offers the space and amenities to keep up with both current and future needs, said Dr. Slaw. “It’s member-centric; it’s only 10 minutes from O’Hare and members will be able to easily drop in and work with staff or hold council and committee meetings.
“It’s the start of a whole new chapter in the history of the SVS.” ■
Women’s Leadership Training Grant: Designed to identify and provide $5,000 awards to women who want to develop and sharpen leadership skills. Three awards are provided at three levels of experience. (See story on 2012 recipient Dr. Ruth Bush below.)
SVS Foundation
Community Awareness and Prevention Project Grant: In only its second year, providing grants of up to $3,000 for vascular surgeons to conduct community-based projects that emphasize patient education and risk assessment and advance awareness of vascular health.
E.J. Wylie Traveling Fellowship: Named for the late, great Dr. Edwin Jack Wylie (1918-1982), a pioneering giant in vascular surgery, this fellowship enables the recipient to visit of number of vascular surgery centers worldwide.
Clinical Research Seed Grants: Providing direct support for pilot clinical projects which potentially could grow into larger studies fundable by industry or governmental sources ■
From how to deal with type II endoleaks to what you wish you’d known about vascular surgery during med school, SVS members are chiming in online, on SVSConnect
This new online community is the place to be for collaboration, engagement and communication. On SVSConnect, members can start and participate in discussions on any topic they wish, and can also ask general questions of SVS and SVS leadership.
The member-only site also makes it easier and more efficient for members to

find each other, communicate, network and engage with the SVS. For now, there is a single forum, to get members signed up and familiar with the website. SVS will soon develop smaller, private communities where committees, sections and other interest groups can collaborate, store documents and accomplish their work more easily.
Join the conversation at vsweb.org/ SVSConnect ■
Medical school and rigorous surgical training traditionally do not include advanced instruction in leadership skills, yet they are integral to achieving career success.
Ruth L. Bush, MD, JD, MPH, knew that despite increases in the number of women entering science and medicine, “few women exist in academic leadership positions.” And though her institution at the time— Baylor Scott & White Medical Center in Temple, Texas — had an executive leadership program, there was nothing specifically for women to navigate leadership in the clinical or academic environment,
she said.

In 2012, Dr. Bush, then Associate Dean for Medical Education with oversight of Temple’s residency programs, received one of three annual SVS Women’s Leadership Training Grants (see story above). It led to creating an institutional Women’s Leadership Advisory Council to foster and promote leadWomen continued on following page DR. BUSH
In Memoriam
Robert M. Blumenberg, 84, Dec. 2, 2018. Dr. Blumenberg treated combat casualties during the Vietnam War. During his surgical career, he was president of the Society for Clinical Vascular Surgery, authored numerous clinical papers and wrote “Scalpel!: Memoirs of a Surgeon.”

Do you know of an SVS member who has passed away? Please let us know at communications@vascularsociety.org.
Spotlight
Editor’s Note: Spotlight highlights significant honors and achievements our members receive, medical and otherwise. Send information (with “Spotlight” in the subject line) to communications@vascularsociety.org.
SVS Vice President Dr. Ronald Dalman has been named associate dean for market development of the Stanford University School of Medicine.
SVS members Dr. Edith Tzeng and Vascular Surgery Fellow Luka Pocivavsek are members of a research team led by the University of Pitts-

burgh studying whether the “active wrinkles” on an artery’s interior surface may help improve synthetic graft design and create an alternative to autologous grafts for bypass surgery. The team has received an R56 grant of more than $450,000 from the National Institutes of Health to fund clinical translation work. ■
The first membership application deadline for 2019 is March 1. SVS membership provides extensive benefits, including free or reduced-rate subscriptions to the Journal of Vascular Surgery. Active members also may use our new designation, Fellow of the Society for Vascular Surgery (FSVS). See all membership benefits at vsweb.org/MemberBenefits
continued from previous page
ership training and mentoring of junior women leaders.
She worked with a research leader and member of the Institutional Review Board to design a survey focused on leadership topics which was sent to women leaders around the country: Had they had formal mentorship and when? What type of mentors? Had they ever had a professional career coach? Had they been a mentor themselves?
Her results showed that though mentorship was available to nearly all of the 19 respondents (of 20 contacted), less than half currently had a mentor and were themselves mentoring junior faculty and postgraduate trainees.
And while leadership training was available to nearly all of them, 84.2 percent acknowledged that specific career advising and long-term mentorship would be valuable. The
Young surgeons currently in their fourth year of Candidate membership — vital members of the Society for Vascular Surgery — need to now apply for Active membership. These specific Candidate memberships expired Dec. 31, 2018; transition to Active Membership is not automatic. Apply today at vsweb. org/Join ■
survey pointed to networking, professional career planning and strong female role models as being most valuable to professional development.
The advisory council was then designed around the identified needs for junior staff, including mentoring.
“Even if you’re expected to become a mentor yourself, you still need guidance and professional development.”
When Dr. Bush received her SVS grant, it was at the senior level, for those 10 years or more out of training. Leadership development opportunities seem to be plentiful early in a surgeon’s career, she point-
On Nov. 1, 2018, the Centers for Medicare and Medicaid Services (CMS) released the 2019 Physician Fee Schedule (PFS) and Quality Payment Program (QPP) final rule.
This final rule makes payment and policy changes to the Quality Payment Program, starting Jan. 1.
The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) advances a forward-looking, coordinated framework for clinicians to successfully participate in the QPP, which rewards value in one of two ways:
• The Merit-based Incentive Payment System (MIPS).
• Advanced Alternative Payment Models (Advanced APMs).
As there is no vascular surgery-specific APMs (the Society for Vascular Surgery is working to develop one), most SVS members will continue to participate in the MIPS program this year. Changes for 2019 include:
ed out. “But even if you’re expected to become a mentor yourself, you still need guidance and professional development. This is a life-long process,” she said.
Without the grant, she said, “I don’t know that I would have recognized that institutional programs really need to be specifically developed targeting women. Now, eight years later, I think we still need these programs. They will increase diversity among leaders both among women and men. It’s a chance to foster and promote leadership among people who may not have thought they could BE a leader.”
Now Associate Dean for Medical Education at the University of Houston College of Medicine (under development), she is mentoring and advising undergraduate students. She finds it gratifying and empowering to help others succeed, she said. “It’s not about you sometimes. It’s about watching trainees excel and move past you and feel proud that you were a part of their success.” ■
CMS is expanding the MIPS-eligible clinician definition to new clinician types including physical therapists, occupational therapists, qualified speech-language pathologists, qualified audiologists, clinical psychologists and registered dietitians or nutrition professionals. If a practice or group employs any of these clinicians, the practices must report the various elements of the MIPS program and the clinicians will count toward the clinician total for being considered a small practice.
CMS added a third criterion for physicians to qualify for the low-volume threshold – providing 200 or fewer covered professional services to Part B patients. However, given the typical patient population age, most vascular surgeons will not be able to opt out of QPP. A new CMS policy allows physi-
QPP continued on following page
cians to opt-in to participate in MIPS or create virtual groups and receive corresponding payment bonuses or penalties if they meet or exceed one or two — but not all — the low-volume threshold elements (i.e., have less than or equal to $90,000 in Part B allowed charges for covered professional services, provide care to 200 or fewer beneficiaries, or provide 200 or fewer covered professional services under the PFS). As QPP is a budget-neutral program, this could help increase the available funds for the bonus pool for SVS members.
CMS set the 2019 performance threshold for determining bonuses or penalties in 2021 at 30 points and the “exceptional performance” threshold at 75 points, a 100 percent increase from 2018’s 15 points threshold. SVS members will need to participate in all elements of MIPS in 2019 to ensure they reach the 30-point threshold. In previous years, just participating in the Clinical Improvement Activities portion would have been enough to avoid a penalty.
This is the first year physicians may be scored for purposes of the MIPS quality and cost performance categories based on their attributed hospital’s performance in the Hospital Value-Based Purchasing (VBP) Program. Facility-based scores for the 2019 performance period/2021 payment determination are based on the 12 measures included in the fiscal year 2020 Hospital VBP Program.
National Provider Identifiers billing under the group’s Tax Identification Number must be eligible for facility-based measurement as individuals, and the group must submit data in the Improvement Activity or Promoting Interoperability categories.
(previously Advancing Care Information)
CMS has eliminated the base, performance and bonus scoring structure used in MIPS’ first two years, instead scoring physicians on a 100-point scale at the individual measure level.
CMS is also maintaining the hardship exceptions for this performance category.
However, CMS is requiring all physicians to use 2015 Certified EHR Technology (CEHRT) in 2019. Physicians who lack access to 2015 Edition CEHRT will be able to request a hardship exception.
CMS is adding two new measures — scored as bonus points in 2019 — to the e-Prescribing objective of the Promoting Interoperability Program: Query of Prescription Drug Monitoring Program and Verify Opioid Treatment Agreement.
A combination of data collection types for the quality performance category is allowed. CMS will score the measure based on the most successful collection type. The multiple-submission type option does not apply to web-interface reporters.



There is no election or opt-in required for facility-based scoring, nor is there an opt-out option. Instead, facility-based scoring automatically applies to MIPS-eligible clinicians and groups that qualify and would benefit by having the facility-based score. However, facility-based physicians may opt to participate through traditional MIPS and CMS will pick the best score to make a payment determination. This may be an option for employed vascular surgeons who believe they have more input in the hospital quality measure programs. For facility-based scoring, physicians must perform 75 percent of their services in inpatient, on-campus outpatient or emergency room settings, and must have at least one service billed with the place of service code used for inpatient (21) or emergency room (23). To be scored as a group, 75 percent or more of the
CMS also is limiting the claimsbased reporting option to individuals in small practices. However, CMS expands the claims-based reporting option to allow small group practices (15 or fewer eligible clinicians) to report via claims.
Completeness Criteria, Threshold and Scoring
CMS maintains that for a physician to be successful in reporting on a measure, he or she must meet the data completeness criteria of 60 percent of all denominator eligible patients and must report a minimum of 20 cases. Physicians reporting via claims must report on 60 percent of Medicare Part B patients only and on a minimum of 20 cases.
If a measure has a benchmark and a physician meets the data completeness criteria, he is eligible to receive three to 10 points based on performance compared to the benchmark. If a physician fails to meet the criteria, he is only eligible to receive one point. Small practices would continue to receive three points if they do not
continued from previous page QPP continued on following page
Trends of Death Due to rAAA: Ruptured aortic aneurysms have a mortality risk of nearly 90 percent, but the mortality rate in the United States is understudied, according to an article in the February Journal of Vascular Surgery
Researchers conducted a retrospective analysis of national death certificate data and found a “significant decline in death due to rAAA during the past 17 years,” primarily because of a decrease in the incidence of fatal rAAA. There were “significant differences between site, age, sex, races and geographic location.”
BY EMILIA KROL, MD ON BEHALF OF THE LEADERSHIP DEVELOPMENT AND DIVERSITY COMMITTEE
Ihad the privilege of interviewing Dr. Cynthia Shortell, Professor and Chief of Vascular and Endovascular Surgery, and Chief of Staff of the Department of Surgery at Duke University Medical Center in Durham, N.C.
They noted the study’s limitations and said more research is needed on the effectiveness of population-based screening for AAA in women. Read this article free through March 31 at vsweb.org/JVS-rAAAtrends ■
Dr. Shortell, a native New Yorker, earned her AB from Dartmouth College and MD from Weill Cornell Medical College. Upon completion of training that included a general surgery residency, a research fellowship in hematology and a vascular surgery fellowship at the University of Rochester (URMC)/Strong Memorial Hospital, she was invited to join the URMC faculty. She remained in Rochester until 2005, when she accepted a position with Duke as chief of vascular surgery.
During her tenure at Duke, Dr. Shortell has garnered an increasing number of leadership roles by
Access hundreds of sessions for one year
See those you missed, watch others again — even download materials
Just $199 for VAM attendees $499 for non-attendees
To purchase, visit vsweb.org/OnDemand18
virtue of her integrity, insight and vision. Most notably she has served as the program director of the Vascular Surgery Residency, vice chair of Faculty Affairs and currently as Chief of Staff for the Department of Surgery. She has served as a principal investigator in numerous clinical trials, and she has published more than 100 articles in peer-reviewed journals, 32 book chapters, three books and countless abstracts and presentations. In addition to her brilliant clinical and academic career, Dr. Shortell is a leader in the changing face of our specialty. As a longstanding, dedicated and active member of the Society for Vascular Surgery, she has served as chair for both the Committee on Women’s Issues and the Education Council.
There were no female surgeon role models for me. But, I did regard one of the older general surgeons I worked with as somebody I could truly look up to. I considered him my role model, a mentor who looked out for me, though he didn’t act as a career advisor.


Q: How did you build up to your current role over the years?
Q: At what point in your career did you know that you wanted to take up a leadership role?
A: I don’t believe I can define a specific moment. When I was in residency it was quite unusual for a woman to train in a vascular fellowship, not to mention lead in surgery. I was more in survival mode then, not even contemplating a future in leadership.
continued from previous page
meet the criteria. The Quality Category will be weighted at 45 percent in 2019, a reduction of 5 percent.
Cost Category Weight Now 15 Percent of final Score
Despite protests from the SVS and many other medical organizations, CMS increased the cost category weight in MIPS to 15 percent. The final rule retains the two existing cost measures (Medicare Spending Per Beneficiary and Total Per Capita Cost of Care) with no changes and adds eight new episode-based measures in 2019, including one that SVS’ Quality and Performance Measures Committee helped develop. All the measures include both Part A and Part B costs and are calculated
A: Although I never had any formal leadership training, I’ve maintained a strong academic presence in our field for many years due to my research interests and national societal memberships. My formal leadership experience developed as those societal involvements deepened and my institutional commitments broadened. At Duke, I collaborated with research teams, became involved in the process of applying for grants, led our vascular laboratory as its medical director, served as the program director of our vascular residency and advanced our section status to the rank of division. Over time, by accepting and successfully managing increasing responsibilities, I have built a reputation as an individual who is reliable, Leadership continued on following page
from administrative claims.
Five of the new cost measures are tied to costs associated with a particular procedure (elective percutaneous coronary intervention, knee arthroplasty, revascularization for lower limb ischemia, routine cataract removal with IOL and screening colonoscopy). Three (intracranial hemorrhage or cerebral infarction, simple pneumonia with hospitalization and ST-Elevation Myocardial Infarction with PCI) involve costs associated with an acute inpatient medical condition. Procedural episodes are attributed to any physician who billed one of the “trigger” procedure codes, and any physician with at least 10 episodes in each measure is scored on it. For more information on this final rule and to check your individual or practice enrollment status, visit www.qpp.cms.gov ■
BY TED BOSWORTH MDEDGE NEWS REPORTING FROM VEITHSYMPOSIUM
NEW YORK – It is well known that reoperative carotid endarterectomy can be technically challenging because of the scarring left from the initial procedure, but an analysis of a large database presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation also revealed that the risk of complications, particularly stroke, is greater.
When “redo” carotid endarterectomies were compared with the index primary procedure collected in the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database, the odds ratio for stroke was several times greater (odds ratio, 3.71; P = .002) on univariate analysis, reported Jeffrey J. Siracuse, MD, associate professor of surgery and radiology at Boston University.
Previous single-center reports of redo endarterectomies “showed
continued from previous page
terrific results, really no perioperative stroke or morbidity, but this is older data from a different era,” said Dr. Siracuse, who undertook this study to determine whether “real-world” data would tell a different story.
In this study, 75,943 primary carotid endarterectomies and 140 redo procedures were identified in the ACS NSQIP database and compared. The redo population had a significantly higher incidence of end-stage renal disease (3.6% vs. 1.1%; P = .004), but history of stroke, whether with deficit (20.8% vs. 15.4%) or without (11.5% vs. 9.1%), was numerically higher among those undergoing a primary procedure even though these differences did not reach statistical significance. Baseline demographics and comorbidities were otherwise similar.
Presumably because of the difficulty of recanalizing scarred tissue, the mean procedure time for redos was longer than that for the primary procedures (137 vs. 49 minutes;
committed, collaborative and effective. As a result, when the position opened up, my name was among the potential candidates.
Q: According to the surveys, the qualities that make a credible leader include: honesty, forward-looking, inspiring, competence, intelligence and broad-mindedness. That seems like a very general statement. What would you say your credibility depends on? Do you think you can narrow it down?
A: Candor and forthright communication are very important. Fairness is key. People need to know that regardless of your personal feelings on an issue, you will act impartially and not allow emotion to cloud your judgment.
Q: What is the most important skill any successful leader should have, in your opinion?
A: A common, significant obstacle to a leader’s success is lack of empathy, unwillingness to listen to others’ points of view. Organizations are comprised of people with various concerns, abilities, needs and biases. Successful leadership requires the skill to acknowledge and appreciate the different perceptions held by those individuals. If one
P less than .001), but there were no significant differences in the rate of surgical site infections (0.7% vs. 0.3%; P = .482), return to the operating room (3.6% vs. 4%; P = .853), or 30-day readmissions (2.1% vs. 6.9%; P = .810) for the redo and index procedures, respectively.

Although perioperative MI rates were higher in the redo group (2.1%) than in the primary endarterectomy group (0.9%), this difference did not reach statistical significance (P = .125). However, a multivariate analysis associated redo carotid endarterectomy procedures with a nearly threefold increase in risk of a composite of major adverse cardiovascular events when compared on a multivariate analysis (OR, 2.76; P = .007), Dr. Siracuse reported.
For the surgeons considering a
is unwilling to evaluate a problem from another perspective, then resolution is highly unlikely and your group will be subject to constant conflict. In my opinion, empathy is definitely an essential skill for problem-solving and, thus, leadership success.
Q: The image of a macho leader is still prevalent in our culture. How did you manage to stay true to yourself in your current role?
A: Remaining true to yourself requires first and foremost knowing and accepting who you are. I believe striving to become the very best version of yourself is a lifelong pursuit that requires effort and frequent reevaluation. Hopefully, experience brings wisdom and that wisdom should help you realize that flexibility in dealing with individuals is an essential characteristic for strong leadership. A leader must be approachable, open-minded and willing to listen. You must recognize who thrives when nurtured and who succeeds under more rigid guidance. Maintaining relevance and longevity in one’s career requires foresight and the resilience to adjust your course when necessary. It’s unnecessary, and often counterproductive, to maintain the harsh leadership style of an unapproachable façade. Quite the opposite — I think it’s important in this day and age to demonstrate that nice and nurturing do not at all imply a weak, indecisive nature. I believe employing empathy requires strength and confidence, and does not sacrifice excellence or your core values. ■
redo carotid endarterectomy, these data “inform a risk-benefit analysis,” according to Dr. Siracuse, but he also said that redo procedures still should be considered a viable strategy when considered in the context of other options.
Presenting a case he performed just prior to the VEITHsymposium, Dr. Siracuse displayed CT images that showed internal and common carotids with more than 75% stenosis in an 80-year-old women 7 years after a primary carotid endarterectomy. The tight stenoses and the evidence of substantial intra-arterial debris were concerns, but a decision to perform a redo endarterectomy was reached after other options, including stenting, were considered.
“She did great. She went home and has had no more symptoms,” Dr. Siracuse reported. “The point is you still have to take these [potential redo endarterectomies] on a case-by case basis.”
Dr. Siracuse reported he had no financial relationships relevant to this study. ■

BY TED BOSWORTH MDEDGE NEWS REPORTING FROM VEITHSYMPOSIUM
NEW YORK – The rates of carotid artery revascularization with either endarterectomy or stenting declined precipitously over a recent 15-year period, at least among Medicare feefor-service beneficiaries, according to data presented at a symposium on vascular and endovascular issues sponsored by the Cleveland Clinic Foundation.
A reduction in carotid endarterectomies (CEA) largely accounted for the decline during 1999-2014 although there was a cumulative decline in all carotid revascularization procedures when rates of CEA and stenting were combined, according to Brajesh K. Lal, MD, professor of surgery, University of Maryland Medical System, Baltimore.
In 1999, when enthusiasm for CEA appears to have peaked, 81,306 pa-
tients received this procedure, but a steady decline was observed until 2014, when 36,325 patients were being treated annually in the Medicare database. When calculated as endarterectomies per 100,000 beneficiaries, the rate declined from 298 to 128 (57%; P less than .001) over this 15year period.
The number of stenting procedures had not reached its peak in 1999, when 10,416 were performed. Rather, the number performed annually nearly doubled to, 22.865 by 2006. However, it then began to decline and reached 10,208 by 2014, which was slightly fewer than in 1999, according to Dr. Lal.
These trends have been observed even though outcomes are getting better, at least for CEA, according to Dr. Lal. From the same pool of data, there was a 31% (1.1% vs. 1.6%) reduction from 1999 to 2014 in mortality at 30 days following CEA. For a composite of ischemic stroke and

all-cause mortality, the rate fell 29.5% (3.1% vs. 4.4%). Both reductions were called statistically significant by Dr. Lal.
The improvements in CEA outcomes were observed even though “the treated patients got sicker when looking at comorbidities and risk factors, particularly hypertension, renal insufficiency, and diabetes,” Dr. Lal said.







Outcomes also improved among patients undergoing carotid stenting in general, although the patterns were described as “more complex.” In general, there was steady improvement on outcomes during 1999-2006, but there was no further gain and some lost ground during 2006-2014. For example, ischemic stroke or death fell from 7.0% in 1999 to 4.8% in 2006, but it had climbed back to 7.0% by 2014 with no net change when the first and last year were compared.
However, with risk adjustment, there was a reduction in in-hospital mortality (1.13% vs. 2.78%) over the study period for patients undergoing carotid stenting, according to Dr. Lal, who said this reached statistical significance. Like the CEA group, there was more comorbidity among those treated with stenting at the end, relative to the early part of the study period.
In the stenting group, patients with symptomatic carotid disease rose from 14.4% in 1999 to 25.9% in 2014. This tracks with Medicare policy, which required patients after 2005 to have symptomatic disease for
reimbursement, according to Dr. Lal. Prior to 2005, reimbursement was granted for patients participating in clinical trials only.
The rates of carotid revascularization are not evenly distributed geographically in the United States, according to the Medicare data. Endarterectomy in particular has been more common in the south and Midwest than on either coast. This was true in 1999 and remained so in 2014. The distribution was similar for stenting, although it was also relatively common in the southwest in the early part of the study period.
In the beginning of the study, the increased rate of stenting might have contributed to the decline in endarterectomy, but there are several other factors that are implicated in the observed trends, according to Dr. Lal. He suggested that decreasing reimbursement for the performance of these procedures, better clinical management of risk factors, and advances in medical therapy. He cited a physician survey that showed a growing preference for medical management over invasive procedures in patients with high-grade stenosis and indicated that this last factor might be a particularly important driver of the decline in revascularization referrals for asymptomatic carotid disease.
The degree to which these Medicare data are representative of overall trends in the United States is unclear, but Dr. Lal called for further work to understand the forces that these data suggest are driving the changing patterns of carotid revascularization.
BY WILL PASS MDEDGE NEWS
FROM ANNALS OF THE RHEUMATIC DISEASES
IgA vasculitis, also called Henoch-Schönlein purpura, increases risks for hypertension and chronic kidney disease (CKD), according to a retrospective study of more than 13,000 patients with IgAV.
In patients with adult-onset IgA vasculitis (IgAV), mortality risk is also increased, reported first author Alexander Tracy and his colleagues at the University of Birmingham (England).
“Long-term health outcomes of adult-onset IgAV are not well characterized,” the investigators wrote in Annals of Rheumatic Disease. “Most evidence regarding complications of IgAV in adults derives from case reports and case series; there is need for controlled epidemiological studies to address this question.”
The retrospective study compared 2,828 patients with adult-onset IgAV and 10,405 patients with childhood-onset IgAV against sex- and agematched controls. Patients diagnosed at age 16 years or older were classified as having adult-onset disease.
The investigators drew their data from The Health Improvement Network database, which includes 3.6 million active patients from more than 675 general practices in the United Kingdom. Patients in the present study were diagnosed with IgAV between 2005 and 2016. After diagnosis, participant follow-up continued until any of the following occurred: outcome event, patient left practice, death, the practice stopped contributing data, or the study ended.
Primary outcomes for adult-onset patients were venous thromboembolism (VTE), ischemic heart disease, hypertension, stage 3-5 CKD, stroke/transient ischemic attack, and all-cause mortality. Primary outcomes for patients with childhood-onset disease were limited to CKD, hypertension, and VTE.
The incidence of childhood-onset IgAV was 27.22 per 100,000 person-years, whereas adult-onset disease was much less common at 2.20 per 100,000 person-years. Mean age at onset of childhood IgAV was 6.68 years. The adult-onset group had a mean age at diagnosis of 38.1 years.
Compared with controls, all patients with IgAV, regardless of onset age, had increased risks of
hypertension (adult-onset adjusted hazard ratio, 1.42; P less than .001; childhood-onset aHR, 1.52; P less than .001) and CKD (adult-onset aHR, 1.54; P less than .001; childhood-onset aHR, 1.89; P = .01).
Patients with adult-onset IgAV showed increased risk of death, compared with controls (aHR, 1.27; P = .006). No associations were found between IgAV and stroke/transient ischemic attack, VTE, or ischemic heart disease.
“These findings emphasize the importance of blood pressure and renal function monitoring in patients with IgAV,” the investigators concluded. “Our data also suggest that IgAV should not be considered a ‘single-hit’ disease, but that clinicians should monitor for long-term sequelae. Further research is required to clarify the cause of hypertension in patients with IgAV, and to investigate whether such patients suffer from additional long-term sequelae than that are currently unrecognized.”
The investigators reported no funding sources or conflicts or interest.
SOURCE: Tracy A et al. Ann Rheum Dis. 2018 Nov 28. doi: 10.1136/annrheumdis-2018-214142.










The GORE® EXCLUDER® Device family demonstrates our commitment to advancing EVAR treatment solutions in new and innovative ways.
The most-studied* EVAR stent graft, designed for durable outcomes.
GORE® EXCLUDER® AAA Endoprosthesis


The only FDA approved, all-in-one iliac branch solution.
GORE® EXCLUDER® Iliac Branch Endoprosthesis











zone length of at least 10 mm; internal iliac artery treatment diameter range of 6.5–13.5 mm and seal zone length of
10 mm; adequate length from the lowest major renal artery to the internal iliac artery to accommodate the
endoprosthesis length, calculated by adding the minimum lengths of required components, taking into account appropriate overlaps between components. GORE® EXCLUDER® AAA Endoprosthesis Components used in conjunction with GORE® EXCLUDER® Iliac Branch Endoprosthesis: TrunkIpsilateral Leg Component. The Trunk-Ipsilateral Leg is intended to provide proximal seal and fixation for the endovascular repair of the aneurysm. Contralateral Leg Endoprosthesis Component. The Contralateral Leg Endoprosthesis is intended to bridge the GORE® EXCLUDER® Device Trunk-Ipsilateral Component to the GORE® EXCLUDER® Iliac Branch Endoprosthesis following deployment of the GORE® EXCLUDER® Iliac Branch Endoprosthesis. Additionally, the Contralateral Leg Endoprosthesis is intended to be used for distal extension of the Iliac Branch Component in the external iliac artery. The Iliac Branch Component can treat external iliac artery diameters up to 13.5 mm. This ability to extend the Iliac Branch Component distally with any Contralateral Leg Endoprosthesis expands the external iliac



