MORE THAN HALF OF MEDICAL STUDENTS ALTERED MATCH RANKING ORDER AFTER POST-VIRTUAL INTERVIEW SITE VISITS, APDVS SURVEY FINDS
By Bryan Kay
AMID THE BUILD-UP TO residency Match Day 2024, the Association of Program Directors in Vascular Surgery (APDVS) has delivered data from a VISIT (Vascular In-Person for Students in the Match Trial) pilot study that took place last year showing some 57% of medical students who took part changed their rank list of integrated vascular surgery programs based on postvirtual site visits to institutions on their radar.
The headline finding emerged during the 2024 Southern Association for Vascular Surgery (SAVS) annual meeting in Scottsdale, Arizona (Jan. 24–27).
“These VISIT data show that a visiting process with a locked ranking order list can really provide meaningful data to applicants—I say that in the context of 57% of them changing their rank lists following these visits,” said co-first author David Rigberg, MD, vascular surgery program director at the University of California, Los Angeles (UCLA), who was presenting on behalf of the APDVS executive council.
The study was launched after the Association of American Medical Colleges (AAMC) released a position paper stressing the importance of diversity, equity and inclusion (DEI) practices, in-person interview affordability, and the environmental
See page 4
SAVS 2024
A JOURNEY TO THE HEART OF DEI LIKE NO OTHER
David L. Cull, MD, delivers a captivating presidential address, laying bare his own challenging journey as a vascular surgeon and the hidden lessons on diversity, equity, and inclusion his life story may hold
By Bryan Kay
2 Guest editorial Russell Samson, MD, puts forward a proposal to save vascular surgery
4 AAA and complex repair ‘We need more evidence,’ says UChicago vascular chief
6 Appropriateness Vascular Verification Program green-lights first three outpatient centers
17 ‘Get a Pulse on PAD’ SVS joins multispecialty public awareness campaign
www.vascularspecialistonline.com
Like nearly everyone else assembled, when Alan Lumsden, MD, took to the podium to deliver the customary presidential address preamble, he had little idea of the allegorical story that was to follow. Not even the program book quite captured what lay in store. “How my perspective on diversity, equity and inclusion has changed after I removed the log from my eye,” reads the entry under the presidential address in the 2024 Southern Association for Vascular Surgery (SAVS) annual meeting guide. The title of the 2024 SAVS presidential address,
See page 8
a meeting highlight, of course suggested a diversity, equity, and inclusion (DEI)-related topic, Lumsden—whose job it was as president-elect to introduce the sitting president—later shared. But what he and many others did not expect was the jaw-dropping tale of the lens with which 2023–24 SAVS President David L. Cull, MD, now looks at DEI through. Even for Lumsden, after he had just included in his introductory roast details of Cull’s early academic struggles, the presidential address caught him slightly off-guard. For, Cull revealed—bringing the true meaning
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | Professor HansHenning Eckstein, MD | John F. Eidt, MD
| Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Christopher Audu, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Executive Director SVS Foundation
Rupa Brosseau
Manager of Marketing
Kristin Spencer Communications Specialist
Marlén Gomez
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Global Sales Director Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. | Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. | Printed by Ironmark |
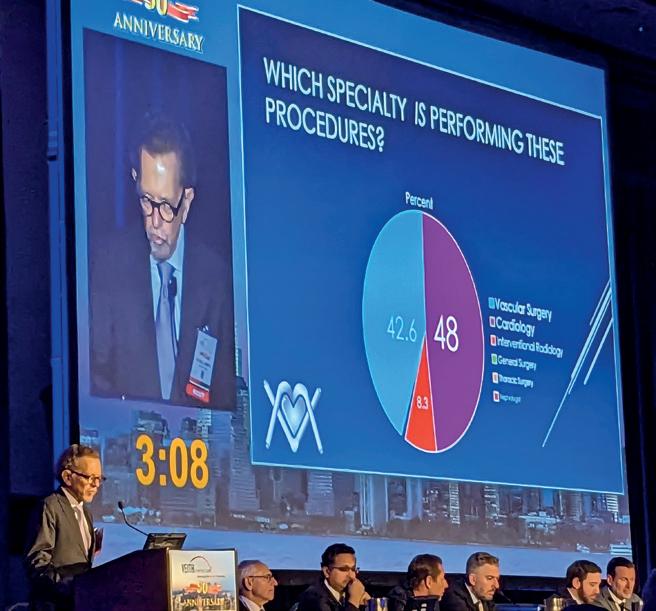
In response to recent articles in the lay press suggesting vascular surgeons were performing unnecessary procedures, Vascular Specialist medical editor, Malachi Sheahan, has asked me to write an editorial based on a talk I presented at the 2023 VEITHsymposium. At that meeting I provided data demonstrating which specialties are treating vascular patients and the rate of insurance denials dependent on provider specialty. I was originally reluctant. I had stopped writing editorials for Vascular Specialist because I had said all that I had on my mind. I was also concerned that, eventually, I would write a piece that readers would find so controversial that I would never be able to show my face in public again.
Well, here it is. I am going to come right out and say it in big, bold, black-and-white letters: “We need the insurance industry to save vascular patients and vascular surgeons.”
To those few of you still reading, please stay with me. I am not suggesting that we continue the current system of prior authorization, since it is time-consuming, expensive, a nuisance for the provider and patient, and still does not guarantee quality care. Rather, I am going to propose a different system that I think has merit.
But first, here is some background as to how I came to the unfortunate conclusion that these companies could be the answer and not the problem. This will require that I detail some of the data that I addressed at the VEITHsymposium and my takeaway from the recent barrage of articles about unnecessary atherectomy. Further, how an American Board of Vascular and Endovascular Surgery (ABVES) aligns with my proposal, and why I keep urging that the Society for Vascular Surgery (SVS) change its name to the American College of Vascular and Endovascular Surgery (ACVES).
First, which specialty is responsible for most of vascular surgery in the United States? For the last two years I have been involved in developing and overseeing a major insurance carrier’s 100% outpatient Medicare Advantage prior authorization (PA) program involving 10 endovascular codes dealing with iliac, femoropopliteal and tibial arteries (Codes 37220–372230), and recently all vascular surgery. Medicare Advantage programs are now insuring more than 50% of all Medicare participants, so my experience has provided me a good overview of who is doing what and why. Cardiologists accounted for 48% of the requested PAs, with 42.6% from vascular surgeons, 8.3% from interventional radiologists, and 1% from general surgeons, thoracic surgeons, or nephrologists. There was a geographic variation with vascular surgeons, cardiologists, and interventional radiologists requesting, for example, 40%, 53%, and 6% PAs in Florida; 42.6%, 28.7%, and 28.7% in Texas; and 63%, 26%, and 11% in New York State, respectively. Irrespective of the variation, these data clearly show that, overall, vascular surgeons are probably doing less than half of the vascular procedures in the U.S. Now that the Centers for Medicare & Medicaid Services (CMS) has approved carotid stenting for asymptomatic patients, it is likely that cardiologists will take away even more procedures.
Russell H. Samson
Diminishing voice
The fact that cardiology is now dominant has enormous repercussions. It diminishes the
voice of vascular surgeons such that government entities, insurance companies, the lay press, and the public will turn to cardiologists and their societies for information, advice and treatment. This must have a negative impact on the viability of vascular surgeons’ practices and on patients’ health. Now, why do I say that it will affect patient health?
Since many of these latter requests are coming out of Florida, I suspect that May-Thurner syndrome must be caused by mosquito bites since this would be the only way this epidemic could be explained
The answer to that also comes from my program, which has evaluated well over 20,000 requests for PA. Last year I presented a small sample of 1,488 PA requests (946 original PA, 172 peer-to-peer, and 370 appeals) for outpatient procedures from 20 states, with New York, Texas and Florida accounting for the majority. All PAs were evaluated predominantly by vascular surgeons or, on occasion, Boardcertified interventional cardiologists. Subsequent peer-topeer discussions were performed by vascular surgeons. Let me assure you that this program was initiated because the company was convinced that abusive practices were causing harm not only to its bottom line, but also to its members’ (patients’) health and well-being. Since there is only one Local Carrier Determination (LCD 35998) dealing with noncardiac stents, and since that LCD can only be used in six states for outpatient care, most insurance companies have developed their own documents outlining indications and appropriate use criteria. Some also use proprietary guidelines such as InterQual.1 For the most part, these are carefully researched, well-written attempts to curtail unnecessary procedures, yet ensure that necessary ones are authorized. Our program predominantly used InterQual but also SVS appropriate use guidelines,2 as well as guidelines sponsored by the American College of Cardiology and American Heart Association.3 Overall denial rates were 44.8% for initial PAs, 45.8% for peer-to-peers, and 41% for appeals. Denials were more frequent for PA requests from cardiologists (56%) than interventional radiologists (47%) and vascular surgeons (30%). Admittedly, some denials were for lack of information or incorrect coding, but many were because patients were being rushed to the office-based lab (OBL) without attempts at conservative therapy. Some case scenarios attributed to cardiologists and interventional radiologists may shock even the most jaded reviewer. For example: a request to perform tibial atherectomy for claudication on a dialysis patient who one month previously had the peroneal artery perforated requiring two units of blood transfusion, fasciotomy, and resultant myocardial infarction; superficial femoral artery (SFA) and tibial atherectomy performed via pedal approach yet no prior or post attempt to treat proximal complete occlusion of the common iliac, external iliac and common femoral arteries; a patient with clearly defined significant femoropopliteal and tibial disease and a leg ulcer booked for an arteriogram but first having bilateral saphenous vein ablations thus destroying the potential for a tibial saphenous vein bypass; and now that we are reviewing all aspects of vascular surgery, an epidemic of PAs to treat “May-Thurner syndrome” affecting octogenarians with bilateral ankle swelling and congestive heart failure.
Since many of these latter requests are coming out of Florida, I suspect that May-Thurner syndrome must be caused by mosquito bites, as this would be the only way this epidemic could be explained. Further, radiologists are now offering endovascular embolization of genicular arteries to treat arthritis of the knee. In one case, the radiologist performed one of these procedures on a knee contralateral to a below-knee amputation and where the SFA was already showing evidence of atherosclerosis. What an amazing indictment that about half of all requests from these other specialists were denied.
Need I say more about how the expanded role of cardiologists will affect vascular patients?
Well, if this is not sufficient, what about all the recent articles in the lay press? There is now
an avalanche of material detailing the abusive use of atherectomy predominantly by cardiologists. However, as our PA program highlights, it is not just atherectomy but all the peripheral endovascular procedures.
‘Operate, Medicate and Dilate’
We must also recognize that, unfortunately, vascular surgeons accounted for 30% of the denials in this Medicare Advantage program. In a past editorial for Vascular Specialist, I made it abundantly clear that I believed that vascular surgeons, like the Knights of the Round Table (or more aptly, the rectangular table?) in the Arthurian legend, follow a chivalrous code of honor that guides us in placing a patient’s well-being ahead of financial reward. We ride out, catheter, stent and knife at the ready to defeat the malevolent atherosclerotic enemy. We proudly fly our banner proclaiming that only we “Operate, Medicate and Dilate.” We denounce other specialists involved in vascular care as Dark Knights whose evil intent is to plunder, their poor behavior induced by disparate payment schedules that favor dilating, rather than operating or medicating.
Yet, I am now chagrined to acknowledge that we too have knights who forsake their code of chivalry— vascular surgeons who value the attainment of wealth or prestige as their raison d’être. Perhaps a few examples of PAs requested by vascular surgeons will highlight that not all vascular surgeons follow appropriate guidelines: a stroke patient is wheelchair-bound and has no complaints relating to her legs but the duplex scan shows a “serious” SFA 80% occlusion that, if it occludes, can cause amputation; a request to treat an occluded anterior tibial artery at the same time as an SFA endovascular treatment for claudication, yet the posterior tibial and peroneal arteries are widely patent; an iliac angioplasty for claudication in a patient on home oxygen with limiting shortness of breath while being treated concomitantly for lung cancer; and four repetitive procedures within six months to treat recurrent right SFA occlusions with a patent popliteal and two-vessel runoff, yet no discussion of a surgical alternative? We need to make these “Dark Knights” aware of how their actions have a negative effect on the rest of us. Because, if left unchecked, castigation in the media and government action will punish all vascular surgeons and our legendary contributions to the management of vascular disease will fade from memory, just like Arthur and his knightly court.
Before I move on, let me speak to those of us who try to follow exemplary practice. Let us look deeply at our own experience and assess whether the following scenarios may be impacting what we do. In general, endovascular procedures are much easier to perform than open surgery, so a stent rather than a bypass. Complications may not be as devastating, so perhaps an inclination to intervene earlier in the disease process. As endovascular procedures replace open surgeries, new graduates and even older surgeons may begin to feel uncomfortable performing complex surgeries, so an angioplasty when a bypass may be preferable. Use a well-reimbursed new technology, though unproven, since it has a novel cache that can be advertised to referring physicians. Do some of these scenarios seem familiar?
Now let us return to the articles that were published in the New York Times and ProPublica since they are painting vascular surgeons with the same paint brush as cardiologists. It would take a highly educated layperson to realize that vascular surgeons accounted for very few of the 200 or so accused of overutilization since the word used most frequently is “vascular” not “cardiology,” and the authors often referred to the procedures as surgeries. So perhaps for the first time, the lay public is becoming aware of vascular surgeons, but surely this is not the way we had hoped? Let’s face it, the magician David Copperfield could not make vascular surgeons more invisible than we are now. Dr. Alan Dietzek, in his presidential address to the Society for Clinical Vascular
Surgery,4 titled his first chapter, “The anonymity of our specialty,” and the following quotation remains true today. “Why are we still not recognized as the go-to physicians for the treatment of vascular disease? Why are we still fighting a battle for recognition that never seems to end? When will it change and how can we change it? Will our specialty survive?” Alan goes on to make an impassioned case for an American Board of Vascular Surgery (ABVS) independent from the American Board of Surgery (ABS), and he has remained committed to this quest.
I am suggesting that it rather be named the American Board of Vascular and Endovascular Surgery. Recently, cardiologists have approached the American Board of Medical Specialties (ABMS) requesting that their Board separate from the American Board of Internal Medicine, thus establishing a separate Board of Cardiovascular Medicine. If vascular surgery does not achieve its own Board first, it will finally relegate vascular surgeons to being second-class purveyors of vascular treatment. Soon, I suspect the American College of Cardiology will adopt the name “American College of Cardiovascular Medicine.” That will be even more devastating; however, we cannot prevent it from happening. What we need instead is to immediately adopt a name change for the SVS. Some years ago, when the logo of the SVS was about to change, I suggested it was an opportune time to give up on the name Society for Vascular Surgery and rather become the American College of Vascular and Endovascular Surgery (ACVES). This has an imprimatur that will result in respect for its members and its messaging. It is more important now than ever before. Now, some will say it is too costly to change the name of the SVS and to have a separate ABVES. Stay tuned because my proposal will also pay for these changes. Together with the American Board of Vascular and Endovascular Surgery (ABVES), these renamed and new organizations will restore our preeminent position as the primary thought leaders and providers of vascular care.
To summarize, it is apparent that cardiology is taking over much of the management of vascular surgery patients in the U.S. The quality of their care is suspect. However, we must admit that some vascular surgeons do not offer optimal care either. Part of the reason for cardiologists’ increasing supremacy is that vascular surgeons have failed to market who they are and what they do. By allowing the ABS to represent vascular surgeons, we have abrogated our ability to stand as a unique entity. The SVS has not been aggressive in marketing vascular surgeons and even the name of the Society does not assure that vascular surgeons are the go-to specialists for vascular interventions. Insurance companies are aware of an increasing number of unnecessary procedures and are ramping up prior authorization programs. Hence my proposal.
Program of spot-checks
surgeons who have been rigorously trained by a program developed by the ABVES. The reviewers will be required to be thoroughly versed in Medicare rules as they apply to vascular surgery, the various LCDs and their jurisdictions, and appropriate use guidelines and peerreviewed manuscripts selected by the ABVES. Before being accredited as a certified reviewer, they will have to undergo a test developed and run also by the ABVES. The program will also assist in procuring and paying for state licensure where necessary. Appropriate insurance will also be provided. Importantly, these reviewers will be well compensated for their work. All would have to sign an agreement that they will not review a potential competitor, or someone closely affiliated. A peer-to-peer will be mandatory before any denial. The goal should be remedial education and not punishment. Denials will be reviewed by a second reviewer before a final determination. Denials will not be considered evidence of negligence but rather noncompliance with insurance standards. Vascular surgeons who provide appropriate care will not be required to undergo a similar review in the following year. Providers who fail such a review will undergo further spot checks at six monthly intervals until they are seen to comply with appropriate standards of care. Continuing abusive behavior may warrant exclusion from Medicare or the insurance carriers’ panel. The ACVES, being primarily responsible for this program, will market it to the various insurance carriers who, if they agree to participate, will pay a premium over the costs to be divided by the ABVES and the ACEVS.
If vascular surgery does not achieve its own Board first, it will finally relegate vascular surgeons to being secondclass purveyors of vascular treatment
The program has multiple benefits. The ACVES and the ABVES will be provided with a source of income that will keep these organizations solvent for the foreseeable future. Payers will see a significant reduction in the cost of provider oversight, a drastic reduction in the number of costly unnecessary procedures, and, by improving the health of their members, a further reduction in expenses. Vascular surgeons will not have to put up with time-consuming, expensive and frustrating PAs. Most importantly, they will be able to advertise to patients that they voluntarily agreed to a program of oversight and that their services have met the highest standard of peer review. Further, insurance carriers choosing providers for their panel will likely seek only those who are part of this program. This will guarantee that vascular surgeons are once again promoted as the appropriate providers of vascular services. Most importantly, the standard of care for vascular patients will be vastly improved. I am hopeful that eventually cardiology and interventional radiology will partner with us to improve the vascular health of the nation.
I propose that the American College of Vascular and Endovascular Surgery, in conjunction with the ABVES, develop the following program. Member vascular surgeons agree to have 10 procedures a year spot-checked randomly by the carrier after the procedures have been completed. In return, participating physicians will not require PAs for their patient procedures and surgeries. The review will include actual images rather than just reports since the written word can manipulate the truth, but images do not lie. If patients had wounds or varicose veins, photographs would also be provided. The review will be performed by Board-certified vascular
2. Society for Vascular Surgery appropriate use criteria for management of intermittent claudication. Journal of Vascular Surgery volume 76, issue 1, p 3–22 April 2022
3. ACC/AHA/SCA/SIR/SVM 2018. Appropriate use criteria for peripheral arterial intervention. Journal of the American College of Cardiology volume 73 No2 2019
4. Dietzek A. Vascular surgery is the best kept secret in medicine and my thoughts on how we can change that. Journal of Vascular Surgery Vol. 69 Issue 1 p 5–14 Published in issue: January, 2019
RUSSELL H. SAMSON is president of The Mote Vascular Foundation and past medical editor of Vascular Specialist
FROM THE COVER MORE THAN HALF OF MEDICAL STUDENTS ALTERED MATCH RANKING LIST AFTER POST-VIRTUAL INTERVIEW SITE VISITS, APDVS SURVEY FINDS
continued from page 1
impact of interview travel in the wake of the COVID-19 pandemicinduced re-arrangement of the Match process landscape.
COVID-19 yielded a transition to the virtual interview, but as the pandemic receded the AAMC continued to recommend the virtual interview process, Rigberg noted.
In light of debate over whether or not to return to in-person interviews, or the potential for a third way involving a hybrid approach, through the VISIT pilot study the APDVS sought to answer the question: Do post-virtual interview site visits that take place after participating programs have already locked in their student rank lists provide benefit to applicants in the Match process?
The study findings prompted incoming SAVS President Alan Lumsden, MD, chair of the Department of Cardiovascular Surgery at Houston Methodist in Houston, Texas, to emphasize the value of in-person visits, which, he said, “can’t be replicated by online interviews.”
“To me, unfairness is asking a medical student to commit five years of their life to an institution, and the first day they walk through is for orientation,” he added. “The risk is more on the applicant side than it is on the institution side.”
Some 21 of the 74 integrated vascular surgery residencies in the U.S. that took part in the 2023 National Resident Matching Program participated in the study, which involved a survey being disseminated to both the applicants and
the institutions’ program directors.
The post-virtual interview site visits took place within the month between programs locking their rank lists and students submitting their own ranking lists. The validated surveys were then later sent out, with the main question being probed whether in-person visits after virtual interviews impacted rank lists.
“The answer was a resounding yes,” reflected Rigberg. Among the 57% who answered that they changed their rank lists, 37% increased a program’s rank after a visit. Another 10% said visits had no impact.
to act upon,” explained Rigberg.
On the question of whether or not applicants would recommend a return to in-person interviews, the data showed a near 50-50 split among respondents, he continued, emphasizing that the medical students participating had decided they “wanted to visit in person and did so.”
“An additional 33% stated that although they did not change their rank list, [visits] affirmed their rank list, so they sent their rank list in with more confidence,” Rigberg said.
The most common factor affecting decisions to change was esprit de corps—”so that relationship between attendings and trainees that you really have trouble seeing in a Zoom-type format,” added Rigberg.
The survey results also demonstrated that 21% of programs would have—if they could—changed their rank lists following the in-person visits.
“We don’t have granular data on whether this [movement] was up or down, but it is important to recognize the programs are locking themselves into something where they are getting information that they might not be able
Among the program directors asked the same question, “interestingly enough, about 20% were kind of agnostic on it. Then there was a 37-37 split between ‘yes’ and ‘no’ about returning to in-person interviews. Again, there is some selection bias there as these are programs that wanted to have a program where they had some type of in-person visit,” Rigberg added.
“ These VISIT data show that a visiting process with a locked ranking order list can really provide meaningful data to applicants”
DAVID RIGBERG
Fifth edition of SVS leadership program reaches capacity
THE FIFTH COHORT IN THE SOCIETY for Vascular Surgery (SVS) Leadership Development Program (LDP) reached capacity in early February due to limited space and high interest from members.
According to LDP faculty, the curriculum draws from the highest quality evidence-based model of leadership contained in the Jim Kouzes- and Barry Posner-penned book, The Leadership Challenge, with an intense focus placed on applying this knowledge into the world of real-life challenges.
Manuel Garcia-Toca, MD, Faisal Aziz, MD, Dawn M. Coleman, MD, Randall R. DeMartino, MD, Kristina Giles, MD, and SVS Executive Director Kenneth M. Slaw, PhD, will lead the program.
“We all will have an opportunity to be leaders in some way shape or form as our careers evolve,” said LDP graduate Leigh Ann O’Banion, MD. “The LDP is a great way to learn from your colleagues and develop a foundational skill set that will be a valuable tool throughout your career!”
Garcia-Toca, who chairs the SVS LDP, added: “The direct correlation between effective leadership and improved patient outcomes makes this program beneficial not just for the surgeons themselves but also for the broader healthcare community they serve.”—Kristin Spencer
AAA and complex repair: ‘We need more evidence,’ says UChicago chief
By Jocelyn Hudson
Arandomized controlled trial (RCT) of open repair versus endovascular aneurysm repair (EVAR) for the treatment of abdominal aortic aneurysms (AAAs), as well as head-tohead trials for additional information on EVAR and complex repairs, are warranted. This was the main conclusion of Ross Milner, MD, during a presentation he delivered as part of an ”‘EVAR Developments” session at the recent Critical Issues America (CIA) annual meeting (Feb. 2–4) in Miami, Florida.
The professor of surgery and chief of the Section of Vascular Surgery at the University of Chicago Medicine in Chicago opened his talk with reference to a 2020 Journal of Vascular Surgery paper by Konstantinos Spanos, MD, and colleagues titled “A new randomized controlled trial on abdominal aortic repair is needed.”
In response to this need, Milner highlighted that Medtronic has launched three trials—HERCULES, ADVANCE and SOCRATES—the latter being the main focus of Milner’s talk at the CIA meeting. He homed in first on HERCULES. The purpose of this multicenter, global, randomized controlled postmarket trial, he shared, is to compare endosuture aneurysm repair (ESAR) to standard EVAR in the treatment of AAAs with wide proximal necks, and will be the first comparative trial to do so. He noted an enrollment goal of 300 patients at 40 sites across Europe and the U.S. Milner then turned his attention to ADVANCE, which he said is the first EVAR head-to-head RCT looking at
aneurysm sac regression outcomes between two devices.
“The ADVANCE clinical study will progress the work of sac regression as a key early indicator of long-term outcomes,” he remarked. The study will “bring EVAR evidence into the current decade,” Milner added, and “empower physicians to make precise, evidence-based clinical decisions that improve patient outcomes.”
SOCRATES, meanwhile, will focus on treatment modalities for an especially complex group of AAA patients. Its purpose, Milner elaborated, is to compare the safety and performance of ESAR versus fenestrated EVAR (FEVAR) for the treatment of AAA patients with infrarenal aortic proximal neck lengths of 4–15mm and minimal proximal sealing zone lengths of 8mm.
“Hostile aortic necks can lead to a loss of proximal seal over time,” he said by way of background to the study, detailing that short necks are associated with increased risk of type Ia endoleak and secondary procedures. Milner noted that there are two treatment options available here: extending the sealing zone proximally or reinforcing the sealing zone. SOCRATES will compare the two.
The trial will be conducted at up to 40 sites in the U.S. and
Ross Milner
Europe, with Milner listing Austria, Belgium, France, Germany, Italy, The Netherlands, Spain and Switzerland as the European countries participating in the trial.
In terms of patient selection, Milner relayed that at least 204 patients are due to be randomized (1:1) and evaluated for non-inferiority. Patients will be treated by one of two methods: ESAR with Medtronic’s Endurant II/IIs with Heli-FX EndoAnchor implants, or FEVAR with either Cook’s Zenith fenestrated stent graft system or—in Europe only—Terumo’s fenestrated Anaconda equivalent.
“[SOCRATES] will be the first comparative trial of ESAR and FEVAR in the treatment of patients ineligible for standard EVAR due to challenging anatomical criteria but within the IFUs [instructions for use] of the two treatment modalities,” Milner summarized. He added that the trial is actively enrolling.
The latest update from the trial, Milner shared, is from August of last year, when the first U.S. patient was treated in the study by co-principal investigator Brant W. Ullery, MD, in Portland, Oregon.
“We need more evidence,” Milner said in his closing statement, looking at the field of AAA repair as a whole. Looking forward, he specified that an RCT of open repair as compared to EVAR—as well as FEVAR and branched EVAR (BEVAR)—is needed, and that head-to-head trials “will ideally provide additional safety and efficacy information for EVAR and complex repairs.”
David Rigberg
LANDMARK BEST-CLI TRIAL GAINS RECOGNITION AS TOP CARDIOVASCULAR ADVANCE IN 2023
By Marlén Gomez
THE AMERICAN HEART ASSOCIATION (AHA) has named the BEST-CLI (Best endovascular vs. best surgical therapy in patients with critical limb ischemia) trial one of the top cardiovascular advances of 2023. This study—led by vascular surgeons Alik Farber, MD, and Matthew T. Menard, MD, and interventional cardiologist Kenneth Rosenfield, MD—compared open and endovascular treatments for chronic limb-threatening ischemia (CLTI) and was aimed at exploring the effectiveness of each treatment modality.
“First and foremost, it brought surgery back into the discussion of CLTI care against a backdrop of a progressive decline in the use of surgical bypass and a dramatic escalation of the use of endovascular therapy,” commented Menard.
“Given the primary finding that surgery was more effective at preventing the main endpoint of major adverse limb events [MALE] or death, it was a wakeup call of sorts to the vascular surgical world in terms of the ongoing importance of surgery as a treatment option.”
Menard, from Brigham and Women’s Hospital, and his counterpart Farber, at Boston Medical Center, both in Boston, brought
together their expertise in vascular and endovascular surgery to embark on a journey that spanned well over a decade. The duo initiated the idea for the BEST-CLI trial in 2007, during a break at the New England Society for Vascular Surgery annual meeting that year, recognizing the need to address the uncertainty surrounding the optimal treatment for CLTI patients. Rosenfield, from Massachusetts General Hospital, joined before the trial was approved and provided an interventionalist perspective to the project.
Farber said that neither he nor Menard had experience conducting clinical trials when they first conceptualized the idea. However, reaching out to the Society for Vascular Surgery (SVS) leadership proved crucial in securing the necessary support to turn their vision into reality.
The trial began enrolling patients in 2014 and concluded in 2019, though it encountered numerous challenges and roadblocks. Despite the complexities involved, Rosenfield acknowledged the enthusiasm within the medical community to answer the question of the optimal treatment for CLTI. To pursue the trial and provide impetus over the ensuing decade, the investigators confirmed
Vascular Verification Program green-lights first three outpatient centers
By Marlén Gomez
THE AMERICAN COLLEGE OF SURGEONS (ACS) and the Society for Vascular Surgery (SVS) have verified the first three outpatient centers under the newly launched Vascular Verification Program (Vascular-VP), with initiatives that focus on ensuring the highest quality of vascular surgical and interventional care in both inpatient and outpatient settings.
The verified centers, namely Albany Medical Center Vascular Outpatient Lab in Albany, New York, Total Vascular Care in Brooklyn, New York, and Michigan Vascular Center in Flint, Michigan, have demonstrated their commitment to improving patient outcomes and delivering treatment, said Clifford Y. Ko, MD, director of the ACS division of research and optimal patient care.
“These three centers have, first as pilot sites and now as verified centers, established themselves as leaders in outpatient vascular
the high degree of equipoise associated with the two standard-ofcare open surgery and endovascular treatment strategies through a survey conducted early in the process. Involving over a thousand investigators across 150 sites worldwide, the trial required a substantial commitment to complete.
we, as a community of physicians and caregivers, are unclear about best practices,” added Farber.
“The SVS has been critical, from the first outreach we undertook in 2009 to the support provided by every one of the SVS presidents since that time. They not only formally endorsed the trial,” said Farber, “they played a key role in our successful fundraising effort towards the end of the trial. They also helped us throughout the process by allowing us to showcase the trial in publications such as Vascular Specialist, within Society-sponsored webinars and at the SVS annual national meetings.”
The trial’s secondary findings, unveiled at the 2023 Vascular Annual Meeting (June 14–17) in National Harbor, Maryland, revealed that both open and endovascular procedures were equally safe for CLTI patients, and that, notably, the major adverse cardiovascular event (MACE) and mortality rates were similar between the two study arms.
Farber stressed the study’s broader implications, noting its impact on raising awareness and interest in CLTI care, and in reinforcing a focus on CLTI globally, especially in the context of the increasing prevalence of diabetes.
“It’s the patient that suffers the most when
care. They have paved the way for many more centers to join us in their journey to continuous improvement by using data and ACS standards and resources to deliver the best possible patient care,” said Ko.
The Vascular-VP, a collaborative effort between the ACS and SVS, offers two levels of participation, one for inpatient and one for outpatient centers. Built on a foundation of quality metrics, program resources, facility standards, and service provisions, the program emphasizes data collection and quality improvement activities. The shared standards across all levels ensure a comprehensive and standardized pathway for centers to enhance their vascular care infrastructure.
“This is a tremendous initiative and joint effort between the SVS and the ACS to address a very important issue in today’s healthcare landscape, as much care is now being delivered in the outpatient setting. These three verified centers are at the forefront of efforts to improve, monitor and optimize the outcomes of outpatient care for patients with vascular disease,” said SVS President Joseph L. Mills, MD. To achieve verification, the three centers met
“We owe an incredible amount of gratitude both to the patients who were brave enough and generous enough to allow us to investigate this clinical problem through their experience, and to all the investigators, including many SVS members, who worked so hard to see the trial through to completion. The benefits of BEST will continue to be paid forward, as the wealth of generated data will serve as a foundation on which we as a community can base future efforts to better understand the numerous unanswered questions that remain in CLTI care.”
“First and foremost, it brought surgery back into the discussion of CLTI care against a backdrop of a progressive decline in the use of surgical bypass and a dramatic escalation of the use of endovascular therapy”
MATTHEW T. MENARD
the standards outlined in the Optimal Resources for Vascular Surgery and Interventional Care—Outpatient Standards framework. This set of standards addresses essential elements of vascular surgical care and quality, ensuring that verified centers maintain the highest standards in patient care.
“Participating in Vascular-VP brought together a lot of our resources, including nursing, vascular lab, office-based lab, front desk and others, to improve the care we are providing to the vascular patient,” said Anil Hingorani, MD, FACS, a vascular surgeon with Total Vascular Care.
“These resources have helped set us apart from our competitors. It’s not just the quality or safety in this competitive market; you must be aware it’s a continuous cycle of looking at your results to find solutions and improvements to improve patient quality.”
Their Vascular-VP verification gives these centers the status of ACS Surgical Quality Partners, which signifies their commitment to continuous improvement, adherence to rigorous standards and dedication to delivering quality care. Patients seeking services at Surgical Quality Partner centers can trust that they are receiving care of the highest standards in surgical quality.
Both inpatient and outpatient centers interested in joining this initiative and continuing their vascular service quality improvement journey are encouraged to make an application online.
Learn more about the Vascular Verification Program at vascular.org/Verification
Alik Farber Matthew T. Menard
Joseph L. Mills (left) and Anil Hingorani
Every day, you perform a wide variety of complex vascular procedures, and you need a variety of grafts. Getinge delivers a comprehensive portfolio of vascular grafts and patches in a range of materials and coatings—from hybrid and ePTFE to heparin bonded and collagen. Backed by evidence, a long history of use, and continued investment and innovation in vascular graft technology, Getinge is the only graft portfolio you need.
www.getinge.com
SOUTHERN VASCULAR FROM
THE COVER SAVS 2024: A JOURNEY TO THE HEART OF DEI LIKE NO OTHER
continued from page 1
of “the log from my eye” phrase into focus—he has considerable experience of the benefits of gaining acceptance: he has battled a learning disability his entire life. Until this moment, it had been a battle that took place privately, concealed from most of those professionally close to him. Yet that in itself carried the point, Cull told those gathered. The challenges he worked to overcome were hiding in plain site. In turn, the idiosyncrasies to which his learning disability gave rise posed a different kind of challenge to his colleagues. A couple of years ago, this led to an epiphany for Cull: his story represented that of a DEI beneficiary.
Cull, from the University of South Carolina School of Medicine in Greenville and formerly vice president of academic and clinical integration at Prisma Health, almost did not give the presentation. Tucked in his pocket as he followed Lumsden to the podium was an alternative address, there in case he decided to “bail” on the topic upon which he’d settled. As a Baby Boomer, a male and a surgeon, he has tendency not to share, he said. But the force of the moment, the divisiveness to which those three letters—DEI—can sometimes lead, helped compel him to overcome his discomfort.
Raised in rural Virginia, Cull said he grew up inculcated with the mantra that “hard work and success were strongly linked,” and insulated from the cultural shifts that began taking place during his formative years. By the time he arrived in Greenville to start practice, he brought with him that sort of bias, he said, and that formed the bedrock of his views on DEI.
“The segregated bubble in which I lived resulted in several biases which I carried with me to Greenville in 1997 when my vascular surgery practice began,” Cull said. “These biases dominated my perspective on DEI for the first decade in Greenville.”
Until 2008. That’s when he first took part in DEI training as he entered the leadership of his institution’s Department of Surgery. Lots of reading, conversations with his adult children and their spouses, as well as roles in DEI initiatives eventually helped shift his views.
Whereas before Cull held beliefs in keeping with the hard-work-yields-success mantra—such as people should fit and feel comfortable in a work environment, more women surgeons would harm the culture of surgery, LGBTQ discussions are uncomfortable and best avoided—now he’d evolved to adopt two core beliefs. “Systemic racism, sexism, and bias toward sexual orientation exist, and efforts to fix them are just and worthwhile,” he said. “And diversity strengthens businesses, organizations and our society.”
These were intellectual decisions, not based on personal experiences, and many surgeons of his generation and gender might have embarked upon similar journeys, Cull reflected. At this point, skeptics might object and suggest his transformation “was more an indoctrination than an education,” he continued.
Not long after his perspective on DEI reached a point of transformation, Cull also finally began to accept, within himself—if not publicly outside a small circle of
close friends and partners—the fact he had a learning disability. Up to that point, he had developed a particular way of avoiding this explanation for his struggles. It had been long in the making: Cull was first diagnosed back during the latter part of his surgery residency at Wilford Hall Medical Center in San Antonio, Texas.
During his presidential introduction, Lumsden trailed the early educational struggles Cull had encountered in elementary and middle school. “He studied a lot, but that was not reflected in his grades,” Lumsden quipped, revealing report cards with less-than-flattering scores. “With scores like this he was probably not exactly destined for surgery, but a big turnaround was made academically.”
What Lumsden was not to know was the true nature and scale of the source of the issue.
Following him, Cull revealed all, detailing the learning disability from symptom to diagnosis to aftermath. What he had was expressive and receptive language processing disorder. The disability meant he struggled to translate thought into speech. That explained the need to write down even basic instructions because of an inability to follow verbal instruction. An inability, for example, to present off-the-cuff on rounds, or respond to even basic questions for which he knew the answer. The poor grades early on. The necessity to work harder than his peers to attain required levels. Yet, at the point of diagnosis, he refused to accept that he had the disorder in question. “I considered a disability as uncorrectable, and if disclosed might be seen as an excuse for poor performance or something I was trying to use for secondary gain,” he told SAVS. “I found it more comfortable to accept I was on the lower end of the bell curve for intelligence compared to my colleagues.”
to develop step-by-step instructions for every one of these operations. That lent him great confidence as he entered practice in Greenville and tackled the first few years of his career as a vascular surgeon.
However, the specter of the endovascular revolution loomed. Ultimately, the complex range of catheters, wires, stents and balloons, as well as procedural bailouts, it yielded was not an arena to which Cull could re-tool his adaptive techniques in order that he could continue to thrive. “My partners would tell you that after considerable effort and time with them in the endovascular suite, I was never able to advance beyond the most basic endovascular skills,” he said.
Instead, he found ways in which he could maximize his value to his group wherever he could, taking on “less appealing areas to my partners.” He found a home in the likes of vascular access and amputation, for instance, and thrived as a teacher.
“They focused on what I could do rather than what I couldn’t do and they accepted me as a full partner”
DAVID L. CULL
That’s where that early grounding in rural Virginia re-entered the lexicon: you overcome those shortcomings with hard work because “hard work is highly valued in the surgery culture,” he said. “I held tightly to this less-intelligent narrative for most of my surgery career.”
Despite at this point being unwilling to accept he had a learning disability, Cull had nevertheless already developed a retinue of techniques to help him adapt. Characteristics for which he would become well known were formed in this crucible. Extensive preparation. Meticulous planning. Never, ever procrastinating. Later, in leadership roles, he would similarly incorporate adaptive techniques aimed at thriving. “My partners would not recognize these techniques as adaptations to my disability because I had not disclosed my disability to them. Instead they would recognize them as endearing David Cull quirks,” he explained.
The era prior to the endovascular revolution lent itself well to Cull’s abilities. During the late 1980s and 1990s, he said, “vascular surgery only required learning 10–12 operations, and the indications were well established. This narrow focus was a factor in me choosing vascular surgery, for it was a field I felt I could master.”
The high case volume he experienced at Eastern Virginia Medical School during his fellowship allowed him
All of which leads up to this moment of public revelation. “It has taken me more than 25 years to accept I have a learning disability, and I have been successful at hiding this disability from everyone except a handful of close friends and colleagues,” he confided. “Even today I have difficulty disclosing this, because, for my entire career, I have been inculcated into a surgical culture that hasn’t seen diversity as a strength, rather as a weakness.”
The year 2022 held an even deeper reckoning for the now retired surgeon. That was the year in which Cull realized his was a story of diversity and its benefits. In recent years, he recalled trying to explain to senior partners the characteristics of his disability that prevented him from being able to perform endovascular interventions. All he got in return were blank looks. After first being bothered by the response, he eventually came to realize they were unflinching because his value to the group had been long established. “They focused on what I could do rather than what I couldn’t do, and they accepted me as a full partner,” Cull noted.
He drew on an example of how this inclusion played out in practice. Whenever he took vascular call and an emergency requiring an endovascular intervention reared its head, those same partners, if in town, always would be on deck to lend a hand, Cull said. “How I was treated by my partners is what a diverse, equitable and inclusive environment looks like. I was fortunate to have landed in a practice where I thrived and gained fulfillment from doing what Bill Marston called the routine work of vascular surgery.”
Back on the subject of the title Cull chose for his presidential address, suggestive of a DEI topic but clearly representing something more, he explained how he settled on the particular wording. “The title came from the realization two years ago that my story is a diversity, equity and inclusion story, and I can use my experiences to gain insights into what it must be like in our profession and in our society to be a woman, a person of color, a member of the LGBTQ community or a disabled person,” he told SAVS as he came to the end of his address. “While my experiences have given me new insight, I can’t fully understand their life experience because I have had the advantage of being a White male who was able to hide his disability over a 30-year career—and was given the benefit of the doubt when I failed.”
OPEN REPAIR
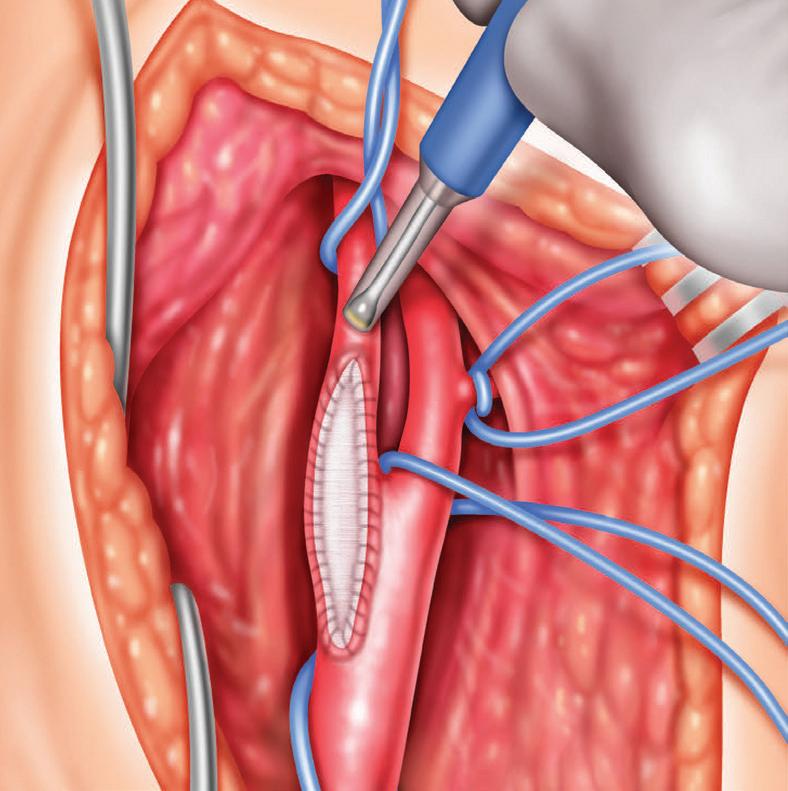
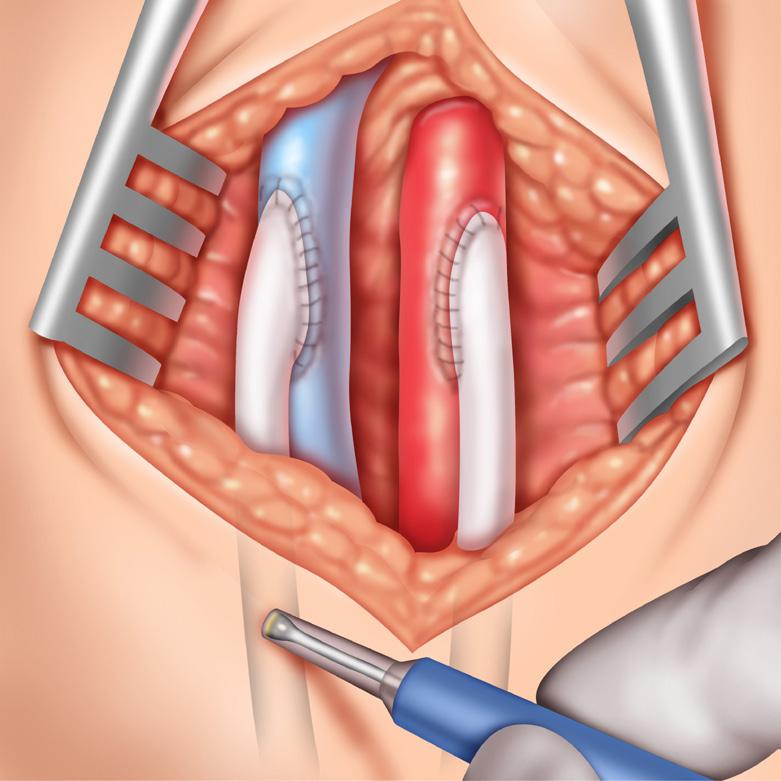
Reevaluating aortoiliac endarterectomy: Case series shows ‘acceptable durability’
By Bryan Kay
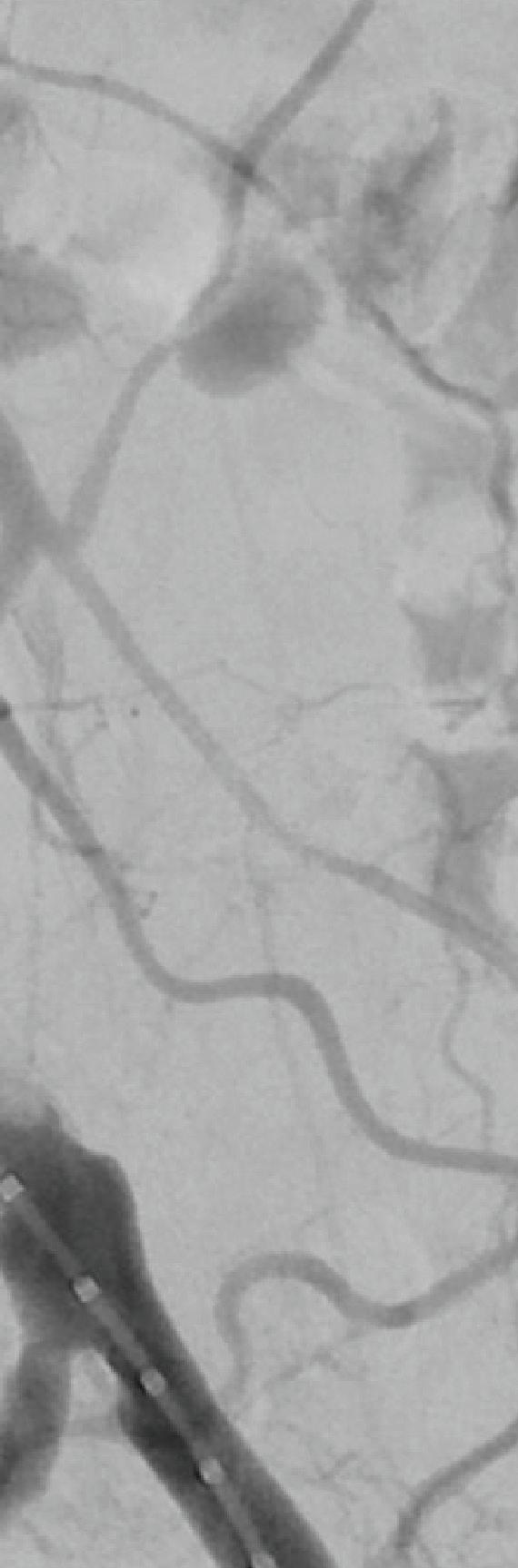
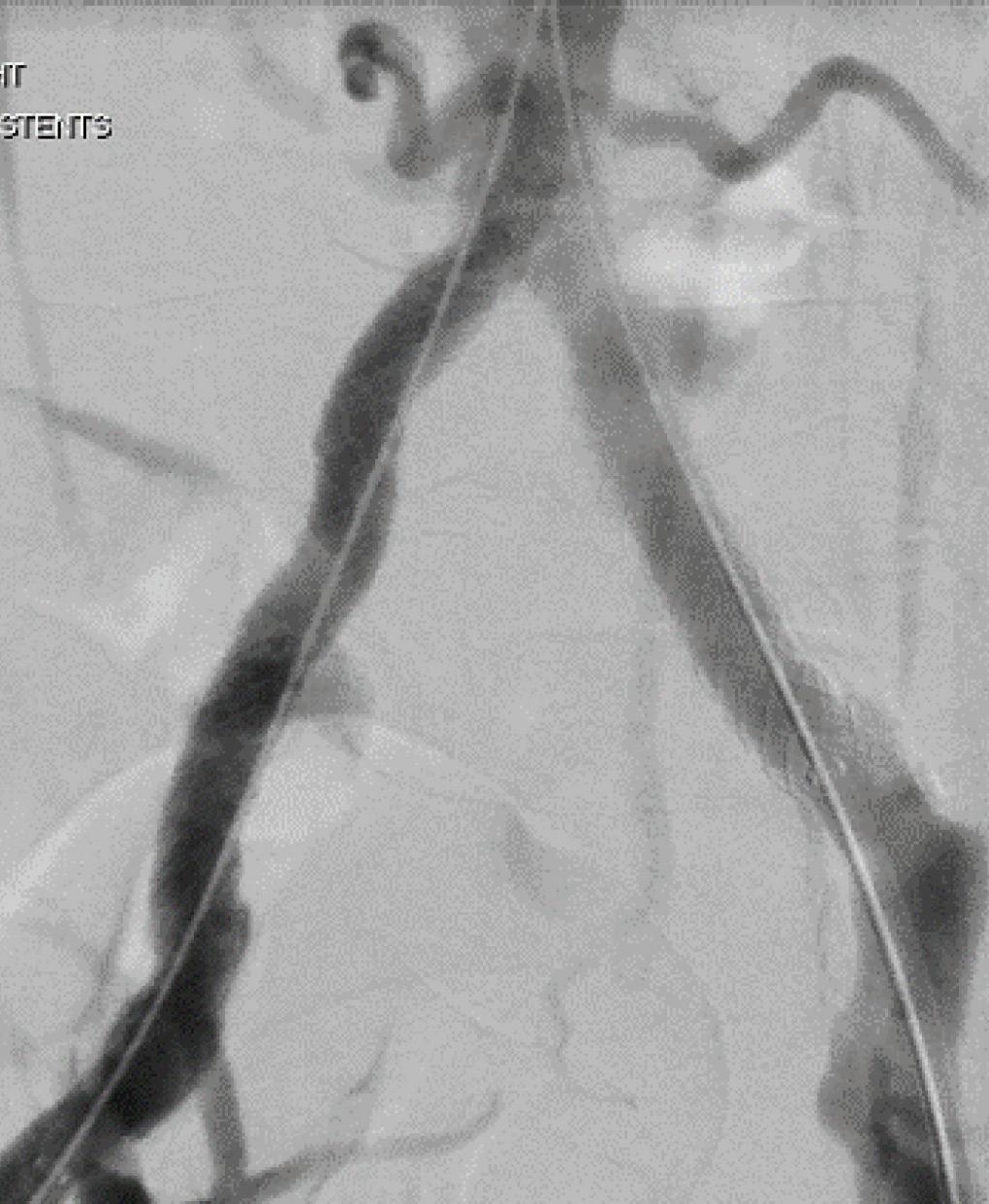
THE UNCOMMONLY PERFORMED aortoiliac endarterectomy—one of the open procedures on which the vascular surgical specialty was founded— surgery provides acceptable durability in patients with smaller native vessels, especially among females, a 25-patient case series review performed at Louisiana State University (LSU) Health Sciences Center in New Orleans has shown.
Results from the analysis, presented at the 2024 Southern Association for Vascular Surgery (SAVS) annual meeting in Scottsdale, Arizona (Jan. 24–27) by Shivik Patel, MD, demonstrated freedom from major adverse limb events of 89% and 81% at two- and three-years post-procedure, while primary and secondary patency three years out were 86% and 89%, respectively.
The aortoiliac occlusive disease patient sample, from 2006–2022, was 72% female
with a mean age of 53.6 years. “Two of these patients had early post-operative thrombosis, and both of those patients had undergone procedures in an acute limb ischemia type of event,” explained Patel, a former vascular resident at LSU and now attending surgeon at WellSpan Health in York, Pennsylvania.
“Among the patients who underwent the procedure in an elective circumstance, there was one instance of late reintervention that was needed, but, overall, this series shows pretty durable outcomes after three years.”
A subanalysis involving mean aortic and iliac diameter measurements further demonstrated that the patient cohort had smaller native vessels than the means of a general population, Patel continued. “We went through all of the patients imaging and measured their juxtarenal aorta, their infrarenal aorta, distal aorta and bilateral
iliac arteries, as we wanted to compare our group to standard population means for the age group,” he said. “We saw that our aortic diameters and iliac diameters were less than those means.”
Patel conceded study shortcomings, principally the lack of a control group. “Our study involved most predominantly females, which could provide some bias in terms of having a mostly female sample, but I think it speaks to benefit something like this can have in the female population,” he added.
Patel argued that given the procedure’s relatively uncommon use in practice, the 25-patient sample provides a “fairly robust” dataset with which to introduce numbers suggesting a role among a specific patient group.
“We have noticed, especially in my clinical experience, in patients in whom we place stents in their smaller vessels, they are not going to have the durability, and, down the road, you’re going to be placing a aortobifemoral bypass,” he noted. “If you have a reason to avoid a large prosthetic graft, as in an aortobifemoral graft, or avoiding femoral incisions, this is a very durable procedure to
do if you have isolated aortic and iliac disease, as long as the patient has acceptable operative risk.”
Patel sees his dataset, for a procedure first performed in the early 1950s, and described in a 2006 Annals of Vascular Surgery paper as “almost a lost art,” as a moment for repose. “This is an opportunity for us to reevaluate one of the traditional operative techniques our specialty is founded on and to make sure we don’t forget about procedures like it,” he said. “They may come back to play a role, and aortoiliac endarterectomy is a surgery I think may re-emerge as a more popular option in patients with specific anatomic specifications.”
“Aortoiliac endarterectomy is a surgery I think may re-emerge as a more popular option in patients with specific anatomic specifications”
Shivik Patel
DIALYSIS ACCESS
AS TEMPORAL TRENDS IN
HEMODIALYSIS ACCESS CREATION EMERGE, NOTION OF AV FISTULA SUPERIORITY COMES UNDER SCRUTINY
The 2024 Southern Association for Vascular Surgery (SAVS) annual meeting (Jan. 24–27) hears three separate talks—two scientific papers and one from an invited guest lecturer—that separately and from different angles checked the pulse of the arteriovenous fistula (AVF)-first era. By Bryan Kay
SANDWICHED NEATLY BETWEEN two complementary dialysis access papers on the SAVS 2024 program, a prominent nephrologist and chair of the taskforce responsible for the 2019 update of the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines delivered a point-by-point take down of the myths that she says surround the idea that AVFs are superior to arteriovenous grafts.
Charmaine Lok, MD, a professor at the University of Toronto in Canada, and medical director of the chronic kidney diseases and vascular access programs at Toronto General Hospital, was delivering the Scottsdale, Arizona-hosted meeting’s Jesse E. Thompson, MD, Distinguished Guest Lecture, the first non-surgeon to do so.
Taking attendees on a tour through the literature, she sought to debunk key aspects around why AVFs are accepted as superior to AV grafts, Lok challenged the argument that fistulas last longer than grafts. However, she said, the key data from which that assertion is derived do not compare all fistulas created vs. all grafts created. “They’re comparing fistulas that actually worked to all grafts,” she explained, making it a “flawed, biased analysis.”
After repeating the analysis, she found that after accounting for primary failure, there was no difference between fistulas and grafts—which was “true for both forearm and upper-arm fistulas.” Lok added, “And when we looked at upper-arm access only, there was no
difference between fistulas and grafts, whether or not we include or exclude pri mary failures.” Randomized controlled trial data tell a similar story, she said. In one, grafts “actually had superior sur vival [or lasted longer] compared to fis tulas for both primary patency as well as secondary patency.”
Turning to the idea that fistulas have fewer complications, Lok pointed to a rare study in this area that focused on infection rates: among 200,000 patients, the inves tigators found that, between fistulas and grafts, the rate was the same, she said.
Moving on to the similar contention that fistulas require fewer interventions than do grafts, Lok drew on a study she said summarizes the evidence thus far: “Patency outcomes of fistulas and grafts is a trade-off between non-maturation and long-term outcomes,” she explained, also pointing to evidence from a study with fol low-up out to six years showing that 50% of fistulas needed more interventions be fore use versus only 17% of grafts.
As for the proposition that AVFs lower costs, she pointed to evidence that demon strated fistulas cost less only when the AVF maturation rate was greater than 82%.
“We have already shown you that that is not happening—our fistula maturation rate was only about 40%,” Lok noted.
Finally, she rested on the idea that fis tulas are associated with lower mortality when compared with grafts. She cited a study that demonstrated mortality risk was best with fistulas compared to cath eters and grafts. Ultimately, Lok said, the higher mortality in those subjects was at tributed to the higher comorbidity burden of patients receiving these access types. It boiled down to selection bias, she added.
Which led her to two ultimate ques tions: What do you think of fistulas now? she asked. Are they really that superior?
“It all depends on your point of view,” Lok said. “Fistula-first was a popula tion-based perspective versus the patient
Charmaine Lok
Bright Benfor
James J. Fitzgibbon
Reach for the Doppler that Works Every Time
The Trans-Q-taneous Intraoperative “TQI” Doppler System is the Doppler you can rely on for all your surgical needs.
VTI’s single-use surgical Doppler probes provide a high degree of reliability since probe failure due to reprocessing is eliminated. RELIABLE
COST EFFECTIVE
The hidden costs associated with reusable probes, including reprocessing and lost OR time due to probe malfunctions, are eliminated.
MULTI-FUNCTIONAL
Provides real-time intraoperative and transcutaneous evaluation of blood flow, for ALL your surgical needs.
Be Confident in Your Doppler!
Call 800-550-0856 or visit us at VTI-online.com to learn more about our Doppler, including a complimentary analysis of your “hidden costs”. Find out why the TQI Doppler provides a high degree of performance reliability and is a more cost-effective solution for ORs.
Visit our TQI product page on our website.
COMMENT& ANALYSIS
AAA REPAIR
ESVS 2024 CLINICAL PRACTICE GUIDELINES ON THE MANAGEMENT OF ABDOMINAL AORTOILIAC ARTERY ANEURYSMS— WHAT’S NEW?
The updated European Society for Vascular Surgery (ESVS) 2024 clinical practice guidelines for the care of patients with aneurysms of the abdominal aorta and iliac arteries, have been published in the European Journal of Vascular and Endovascular Surgery. Here, Anders Wanhainen, MD, from Uppsala, Sweden, and Isabelle Van Herzeele, MD, from Ghent, Belgium highlight some important updates from the new document.
The ESVS 2024 guidelines document on the management of abdominal aortoiliac artery aneurysms was developed over a three-year period by a writing committee comprising of 16 aortic experts from 12 European countries.
By summarizing and evaluating the currently best available evidence, 160 recommendations for the evaluation and treatment of patients have been formulated and graded according to a modified European Society of Cardiology (ESC) grading system, where the strength (class) of each recommendation is graded from I to III and the letters A to C to mark the level of evidence (LoE).
Compared to the previous 2019 version, 59 recommendations are completely new, 49 have been revised, and only 52 recommendations have not been changed. Importantly, only 10/160 (6%) recommendations are based on level A evidence, while 112 (70%) recommendations are supported by level C evidence or based on consensus.
Screening and management of small AAAs
Because of changing epidemiology, with the decreasing prevalence of abdominal aortic aneurysm (AAA), a thorough re-evaluation of the screening recommendations has been made. Although screening of high-risk groups remains highly recommended (class I, level A), the target groups have not been included in the recommendations, but should be made depending on local conditions, such as prevalence of the disease and life expectancy.
People who have first-degree relatives with AAA, with other peripheral aneurysms or organ transplant recipients are established high-risk groups that should be subject to screening. Older men, especially those with a history of smoking,
gender differentiation of the indication for repair. Nevertheless, it may be reasonable to take gender and body size into account, in the same way as for AAA.
Elective AAA repair
The existing randomized controlled trials (RCTs) comparing open surgical repair (OSR) and endovascular aneurysm repair (EVAR) are partly outdated and not entirely relevant for today’s situation. It is therefore necessary to also include more recent case series and registry studies in the overall evaluation. Thus, despite data from multiple RCTs and meta-analyses, representing the highest level of evidence, the existing LoE was rated as mediocre (level B). Overall, evidence suggests a significant short-term survival benefit of EVAR over OSR, with similar long-term outcomes out to 15 years of follow-up. Thus, the impetus towards EVAR as the preferred treatment modality for AAA in most patients is retained in the 2024 guideline.
included. All patients are recommended for early postoperative CTA imaging (within 30 days) to assess the presence of endoleak, component overlap and sealing zone length.
Patients stratified as at low risk of complications should be considered for low frequency imaging follow-up during the first five years. Patients deemed at high risk should instead be managed more actively with intensified and/or additional imaging or consideration of treatment.
New and updated recommendations on the management of endoleaks are presented, and a suggested diagnostic step up for occult undetermined endoleaks is described, where the option of conversion to OSR with stent graft explantation is highlighted.
Complex AAA
also remain a suitable target group in many settings. But, in populations with extremely low smoking prevalence, the incidence of AAA is so low (<1%) that the value of screening can be questioned. There is also lack of support for screening women and people with cardiovascular disease. The importance of cardiovascular risk factor management in patients with small AAAs has been strengthened. Based on a comprehensive analysis of the available evidence, it is not considered to be justified to restrict the use of fluoroquinolone antibiotics in patients with AAA as was previously suggested by the Food and Drug Administration (FDA) and European Medicines Agency (EMA). Similarly, these guidelines advise against restricting exercise and sexual activity in patients with AAAs.
Indication for repair
In line with the evidence, a clear negative recommendation is now issued for the repair of AAA <55mm in men and <50mm in women. The diameter threshold for when repair can be considered is maintained at 55mm for men and 50mm for women; however, the recommendations have been downgraded due to the lack of supporting high-quality evidence. Furthermore, it is clarified that the diameter threshold for considering repair should preferably be based on the ultrasound measurement, while computed tomography angiography (CTA) for treatment planning is only recommended when the diameter threshold has been met on ultrasound.
Given the natural history of iliac artery aneurysms with slow growth rates and the very low risk of rupture below 40mm in diameter, the writing committee considers it justified to raise the recommended diameter threshold for surgical repair to 40mm. There are no data to suggest any
Following reports of failing devices in EVAR, these guidelines advocate the use of devices with proven durability, and advise against EVAR outside the manufacturer’s instruction for use (IFU) in the elective setting. Long-term followup in prospective registries of updated devices based on established platforms is recommended as before, but with the increased requirement for 10 years of durability data.
Due to the lack of evidence of a clinically relevant benefit, routine preemptive coiling of side branches or non-selective aneurysm sac embolization before EVAR is not recommended, and, in OSR of AAA, routine use of antimicrobial coated grafts to prevent aortic graft infection is not recommended.
The previously preferred endovascular approach for iliac aneurysms has been amended. Neither technique is generally considered superior to the other, but instead the choice of surgical technique for iliac aneurysm repair should be based on patient and lesion characteristics.
Ruptured AAA repair
The benefit of EVAR for ruptured AAA has been demonstrated in RCTs and large cohort studies, which is why the recommendation for EVAR as the first option in rAAA remains as class I, whereas it is considered justified to upgrade the LoE to level A.
The recommendation of using aortic balloon occlusion for proximal control is downgraded due to the uncertainty of its effect, while the recommendation for vacuum assisted open abdominal closure has been upgraded, with the addition of mesh traction.
EVAR follow-up
An updated recommended follow-up algorithm after standard EVAR has been
The coverage of complex AAAs has been expanded significantly to reflect advances in technology since 2019 and now covers the management of juxta- and pararenal AAAs, as well as suprarenal AAAs and type 4 thoraco-abdominal aortic aneurysms (TAAAs). Treatment recommendations have been updated based on an increasingly comprehensive body of knowledge, including preliminary data from the most recent UK COMPASS trial. Endovascular repair with fenestrated and branched endografts is considered to have some benefit and is advocated in patients with high surgical risk and complex anatomy.
Further updated recommendations have been issued on preservation of renal function, prevention of spinal cord ischemia, and new technologies such as off-the-shelf branched devices, physicianmodified endografts (PMEGs), and in situ fenestration.
Parallel graft techniques should only be considered as an option in the emergency setting, or as a bailout, and ideally be restricted to ≤2 chimneys. The use of new techniques and concepts for treatment of complex AAAs is not recommended in routine clinical practice.
Centralization
The firm evidence of a volume-outcome relationship of surgical repair in general, and AAA repair in particular, makes it necessary and justifiable to continue centralization of AAA repair. The recommended minimum yearly caseload has been upgraded to at least 30 standard AAA repairs per center (no less than 15 each for OSR and EVAR), and a consensus recommendation on a minimum yearly caseload of 20 complex AAA repairs has been added. Rare and complex conditions, should only be managed in highly specialized centers.
ANDERS WANHAINEN and ISABELLE VAN HERZEELE are chair and co-cjair of the ESVS guideline writing committee.
CORNER STITCH
“Where are you from? Where are you really from?”
Vascular resident Saranya Sundaram, MD, shares a story of finding cultural understanding and community.
“IT’S SUNDARAM, S-U-N…” I’M INTERRUPTED by a nurse asking me if I’d like to call anesthesia for an airway. I quickly nod and ask them to grab the crash cart.
“I’m sorry, you said… S-U-N-D-A-M?” the radiology resident repeats over the phone.
“No, I said S-U-N-D-A-R-A-M.” Another nurse asks me if this was the central line I wanted, and I give a thumbs up. They let me know they are still struggling to get another IV, but they could push the calcium through the remaining 16 gauge in the left arm. I tuck the phone against my shoulder and start grabbing the ultrasound, some flushes and gauze.
“I’m sorry, I still can’t find you. Can you spell it again?” he says a little louder over the phone, to get my attention. “It’s, what, S-U…” I try cutting him off, asking if there’s another way to look me up. I understand he needed my name for the wet read and thanked him for letting me know about the
subdural on bed 11, but I had a man in the ICU a full minute into chest compressions, and I needed to get control of the room. He starts to argue, though I was saved by my intern who, after witnessing my frustrated expressions from across the room, grabbed the phone from me and promised to handle it. I thanked him quietly and refocused on the room.
I find myself back at this experience every once in a while. Sometimes, it’s while reflecting on my own, at home snuggled up with my dog, about the general absurdity of the situation. Yes, the absurdity that while running my first code as ICU chief, I was spelling my last name to a person who couldn’t be bothered to figure it out.
If I really thought about it, there wasn’t a clinic where I hadn’t gotten the I-know-you-aren’t-from-around-hereand-I’m-going-to-figure-you-out stare. And I had grown accustomed to the questions that followed—“Where are you from?” “Where are you really from?” And the occasional and bold, “You’re Indian right?”
In truth, Charleston wasn’t much different from the towns that I grew up in. My parents were deeply religious South Indians who just happened to settle on sleepy Carbondale, Illinois, as their opportunity for a life in America. Regardless, my parents had always been good at finding “the community,” even in places like Emporia, Kansas, where their children were born, or Grand Rapids, Michigan, where they grew up. It wasn’t until my later years that I realized my parents and brother were the only aspect of “the community” I needed. With thousands of miles now separating us, that quiet comfort of feeling seen and understood felt farther than it had ever been. But I’d like to think my time on research this year has allowed me a certain clarity. That out-of-place feel-
ing is dealt more subtly outside of the hospital. And without the defense mechanism clinical efficiency had allowed me, I am forced to think about things as they happen and also pay more attention to how the people around me respond to similar situations.
Two of my co-residents have found ways to make themselves feel a little more at home, trying all the Vietnamese pho spots they happen upon or finding the best beef broccoli in Charleston at the back of a Chinese grocery store. And I realize now that spending time with them has always brought me closest to that feeling of community. Thinking back, things like the annual “Happy Diwali” phone calls from my program director were opportunities to be a part of “the community,” even if I didn’t realize it at that moment. It wasn’t until I was in the middle of a debriefing with one of my attendings, who happens to be one of a few Black female surgeons practicing in South Carolina, that it hit me—that feeling of “otherness” could be shared and understood across vastly different backgrounds.
I’ve started to lean into that clarity and the people who may not look like me but can understand me. The comfort that I have found from shared experiences has been life and outlook altering. Every once in a while, yes, I get that twinge of discomfort when I use a nickname at restaurants or spell my name over the phone. But I notice myself smiling more when I think about how much my co-residents or attendings would enjoy hearing about this new absurdity. And, for a moment, I realize that I have found my own sense of community.
SARANYA SUNDARAM is a vascular surgery resident at Medical University of South Carolina in Charleston.
The basics of budget neutrality, code valuation and physician payment GOVERNMENT GRAND ROUNDS
By Natalie D. Sridharan, MD, and Nicolas J. Mouawad, MD
SO, WHAT IS BUDGET NEUTRALITY and how does it affect physician payment?
The Medicare Physician Fee Schedule (PFS) is a resource-based relative value scale (RVS) payment system, where relative value units (RVUs) are based on resource costs associated with physician work, practice expense and malpractice. The PFS has a budget neutrality requirement that has been in place since 1992. Budget neutrality is the federal mandate that requires an upward adjustment in expenditures in one area of the Medicare program to be offset by a downward adjustment in other areas. In the simplest terms, budget neutrality requires that the Centers for Medicare & Medicaid Services (CMS) make an overarching negative adjustment to the PFS to counterbalance any increases in PFS resources that CMS implements. This process occurs by implementing changes to the conversion factor (CF). The CF, a national dollar multiplier, is used to “convert” geographically adjusted Relative Value Units (RVU) to determine the Medicare-allowed payment amount for a particular physician service.
A significant budget neutrality adjustment went into effect in 2021 as
a result of the revaluation of office/ outpatient evaluation and management (E/M) codes within the PFS. However, coordinated advocacy efforts across the provider community resulted in Congress advancing legislation to mitigate the impact of the budget neutrality adjustment. They have taken similar action in each of the following years. Efforts to reverse the 2024 reduction in the PFS are still underway.
How are codes valued?
The American Medical Association (AMA) Relative Value Scale Update Committee (RUC) is an expert panel of physicians and healthcare professionals that makes recommendations to the federal government on the resources required to provide medical services. Medical services are described by Current Procedural Terminology (CPT) codes. CPT codes offer doctors and healthcare professionals a uniform language for coding medical services and procedures to streamline reporting, and increase accuracy and efficiency. CMS reviews RUC recommendations and determines the RVUs for CPT codes.
The AMA CPT panel meets three
times per year in sequence with the RUC meetings. The CPT panel debates and approves new procedural codes, revises existing codes, and deletes obsolete ones. Typically, a code that has been revised or newly approved by the CPT panel will then be reviewed at the next RUC meeting for new or revised valuation.
Medical specialty societies such as the SVS—with 20% AMA membership and recognized by the AMA House of Delegates—nominate a specialty society member to advocate on behalf of their membership for appropriate values for medical services they provide.
These “RUC Advisors” present survey data to the AMA RUC panel. This panel is made up of physicians and other healthcare professionals.
There are 29 seats on the RUC. The majority of seats are filled by delegates from medical specialty societies. The RUC meets three times per year. Historically, greater than 90% of RUC recommendations were adopted by CMS, although that percentage fluctuates.
The survey data that the advisors present to the AMA RUC panel come from RUC surveys that the specialty societies disperse to the membership. The panel
determines the questions and timeline for completion. The surveys include questions related to physician time, intensity, typical patients and pre-/postoperative care. The specialty society’s RUC advisor and coding committee review the data and prepare recommendations for the RUC panel.
Crucial role
Budget neutrality plays a critical role in these discussions; increasing the value of a particular code will result in a corresponding across-the-board decrease in reimbursement for all other procedures.
The exploration of topics such as budget neutrality and the valuation of CPT codes explains the crucial role these factors play in shaping healthcare reimbursement policies.
By highlighting how these processes occur, we hope to equip early-career vascular surgeons with the knowledge and insight necessary to actively engage in advocacy efforts and thereby contribute to the evolution of healthcare policies that directly impact their practice.
NATALIE D. SRIDHARAN and NICOLAS J. MOUAWAD are both graduates of the SVS Advocacy Leadership Program.
23–25 APRIL 2024
TUESDAY-THURSDAY
NEW VENUE, E xCeL LONDON, UNITED KINGDOM
• BASIL-3 Podium First Presentation:
Putting BASIL-3 in context
Tuesday, 23 April
• NEW!
Challenging Cases Session: Presentations from societies around the world Thursday, 25 April
• Late Breaker: BEST-CLI vs BASIL 2 - outcomes when comparing apples with apples Thursday, 25 April
‘VOICES OF VASCULAR’ CAMPAIGN CELEBRATES DIVERSITY FOR BLACK HISTORY MONTH
By Marlén Gomez
During Black History Month, the Society for Vascular Surgery (SVS) Foundation will shine a spotlight on the contributions of Black vascular surgeons through its “Voices of Vascular” campaign. This initiative is dedicated to recognizing the diverse voices within the SVS and promoting awareness of various cultures and communities.
The “Voices” campaign—whose presenting sponsor this year is Boston Scientific— spans multiple months, each dedicated to acknowledging different facets of diversity.
Following Black History Month in February, the campaign extends its focus to Women’s History Month in March, Asian American and Pacific Islander Heritage Month in April, Pride Month in June and National Hispanic Heritage Month from mid-September to mid-October. The goal is to engage members and the public in sharing crucial information about each highlighted group, fostering awareness and appreciation for their unique contributions.
Recognizing the campaign’s impact, the SVS and its Foundation received the Profile of Excellence Award from the American Association of Medical Society Executives (AAMSE) last September. This annual award program honors member organizations
achieving excellence in areas such as diversity, equity, and inclusion (DEI), advocacy, communications, education, membership and leadership.
For Black History Month, the SVS has curated a series of profiles spotlighting the accomplishments and stories of Black vascular surgeons.
One featured professional for the 2023 initiative was Channa Blakely, DO, who was matched into vascular surgery in Galveston, Texas. Currently finishing up her residency at the University of Texas Medical Branch, Blakely recognized the implicit trust and understanding she shares with patients who look like her. As an African American woman in a surgical specialty, she emphasized the importance of her role in building connections with patients.
“I find that my patients express their pride and the comfort of me having a similar background to them. They often look at me for reassurance,” said Blakely.
The profiles aim to inspire the next generation of vascular surgeons and underscore the significance of diversity within the medical community. Daemar Jones, a fourth-year medical student at Texas Tech University Health Science Center School of Medicine,
was featured for 2024 Black History Month. Jones, a 2023–24 social media ambassador for the SVS, emphasizes the impact of scholarships and donations to the Foundation that support physicians and students.
“Coming from me—a student who had all odds statistically [against him] as someone who’s not supposed to be here—if I get a Match acceptance, I aspire to advance my career academically and become an academic mentor. My goal is to be a resident with skills that impact my community. Those are the aspirations that drive me forward, and I am determined to break barriers and inspire the next generation,” said Jones.
The “Voices” campaign serves as a valuable resource for those interested in gaining insights into the multifaceted world of vascular surgery and the individuals shaping its future.
To learn more about “Voices of Vascular,” visit vascular.org/VoicesOfVascular
“I find that my patients express their pride and the comfort of me having a similar background to them. They often look at me for reassurance”
CHANNA BLAKELY
Make a ‘PLAN’ for CLTI by tuning into new webinar
AN UPCOMING WEBINAR IS SET TO provide insights for healthcare professionals aiming to enhance their expertise in treating patients with chronic limb-threatening ischemia (CLTI).
Titled “Structured Decision-Making in the CLTI Patient: Understanding the PLAN,” the webinar’s goal is to delve into patient risk assessment, limb severity evaluation, and anatomic complexity considerations. Registration for the online session is now open and will be held at 6 p.m. CST on Feb. 27.
Organized through a grant from the Council of Medical Specialty Societies (CMSS), focused on fostering diagnostic excellence, the webinar seeks to explore the complexities of CLTI treatment through the lens of the PLAN algorithm (patient risk, limb severity, anatomic complexity).
According to webinar moderator Michael Conte, MD, professor and chief, Division of Vascular and Endovascular Surgery at the University of California, San Francisco, the webinar’s focus on the PLAN algorithm aligns with the global vascular Guidelines in CLTI, emphasizing the importance of a systematic approach to patient-centered decision-making.
For more information on the webinar, visit vascular.org/PLAN.—Marlén Gomez
Audible Bleeding podcast expands horizons with new senior editor
IBy Marlén Gomez
n the fast-evolving landscape of medical education, podcasts have emerged as a powerful medium for disseminating knowledge and fostering community among professionals. Among these, Audible Bleeding has carved a niche as an auditory experience and formal publication dedicated to shaping the minds of early-career surgeons.
Founded in 2018, the podcast has seen remarkable growth, culminating in 204,841 downloads in 2023. It boasts an average of 561 unique daily listeners, indicating a steady and engaged audience within the surgical community.
Popular Audible Bleeding sub-series include “Lost in Translation,” which explores how vascular surgeons and patients communicate, and Journal of Vascular Surgery (JVS) “Author Spotlights,” which discuss that month’s articles in the JVS journals.
Last year marked a pivotal moment for the podcast as Imani McElroy, MD, a member since 2021, became the senior editor. Currently a senior general surgery resident at Massachusetts General Hospital in Boston, McElroy’s passion for addressing healthcare disparities stems
from her firsthand experiences in San Francisco. Her research interests, spanning implementation sciences and examining racial/ethnic and gender disparities within healthcare and vascular surgery, align with the podcast’s commitment to equity.
“I am excited to contribute to the educational mission of Audible Bleeding. We are currently working on streamlining procedures to ensure consistent, high-quality content. My goal is to foster collaboration, making Audible Bleeding a hub for knowledge exchange within the vascular surgery community,” said McElroy.
In 2024, the podcast will introduce two new sub-series to diversify its content. The SVS Sub-Section on Outpatient and Office Vascular Care (SOOVC) will delve into developing a series of office-based lab (OBL) podcasts. In contrast, the “Managing, Organizing, and Navigating Investment Choices for Economic Success (MONIES)” sub-series will explore managing finances for medical professionals. These additions aim to cater to the audience’s diverse needs.
As McElroy steps into her role, Adam Johnson, MD, the podcast founder, expressed his confidence in the transition, stating: “I am thrilled to welcome Dr. McElroy as the senior editor. Her dedication to addressing disparities and robust research background make her the ideal leader for the podcast’s next chapter. I look forward to seeing the podcast flourish under her guidance.”
Listen to the Audible Bleeding on the podcast website, available at: www.audiblebleeding.com
SVS WEBINAR AIMS TO TACKLE UPCOMING CHANGES TO CMS REPORTING REQUIREMENTS
THE SVS WILL HOST A WEBINAR FEB. 29 TO HELP EQUIP members with insights on impending Centers for Medicare & Medicaid Services (CMS) reporting requirements that impact vascular specialists.
Jessica Simons, MD, chair of the SVS Quality Improvement Committee, emphasized vascular surgeons’ role at the intersection of high-quality patient care and the financial viability of their practices.
“The SVS Quality Measures and Performance Committee [QPMC] is actively engaged in developing vascular-specific Merit-based Incentive Payment System (MIPS) Value Pathways (MVPs) designed to optimize reporting and payment structures for our dedicated vascular specialists,” said Simons.
The webinar—“How Medicare Quality Requirements Will Impact Reimbursement”—aims to address the financial challenges posed by changes in reimbursement and government policies. Simons stressed the importance of adapting to current and future requirements to maintain high standards of care and ensure financial sustainability within the field.
CMS mandates that all healthcare providers, irrespective of their practice setting, submit quality measures through either MVP, MIPS or an Alternative Payment Model (APM). Effective reporting and compliance require the development of vascular-specific pathways as upcoming requirements have the potential to impact all SVS members.
In a collaborative effort, the SVS QPMC and the Quality Improvement Committee will provide insights during the webinar. Register for the webinar at vascular.org/QMPCwebinar
SOCIETY BRIEFS
Compiled by Marlén Gomez, Kristin Spencer and Bryan Kay
‘Get a Pulse on PAD’
IN PARTNERSHIP WITH THREE OTHER medical societies in the vascular disease space that form the PAD Pulse Alliance, the SVS is taking part in a peripheral arterial disease (PAD) public awareness campaign called “Get a Pulse on PAD.”
Alongside the Association of Black Cardiologists (ABC), the Society for Cardiovascular Angiography & Interventions (SCAI) and Society of Interventional Radiology (SIR), the group aims to educate people on PAD risk factors and potential symptoms, as well as encourage patients to advocate for their own health with their doctors.
The awareness campaign, taglined “Kick Off the Conversation,” launched as the PAD Pulse Alliance released survey data showing that 70% of Americans are unaware of the disease, contributing to the 400 amputations performed each day in the U.S.
“The collaboration among these medical societies is a testament to the devastating impact PAD can have on people, families and whole communities if not diagnosed and treated early, and importantly, early treatment usually consists of medication and lifestyle changes,” said SVS President Joseph L. Mills, MD. “We hope that care teams will continue to collaborate to ensure early and proper diagnosis with the ultimate goal of improving outcomes for patients.”
The PAD Pulse Alliance has also created a website and patient toolkit at PADPulse.org
SOUTHERN VASCULAR ELECTS FIRST WOMAN PRESIDENT-ELECT
THE SOUTHERN ASSOCIATION FOR Vascular Surgery (SAVS) elected Margaret (Megan) Tracci, MD, to become its first woman president for the 2025–26 cycle.
Tracci, a professor of surgery at the University of Virginia in Charlottesville, will serve as SAVS president-elect during 2024–25. Tracci is a past president of the Virginia Vascular Society.
Alan Lumsden, MD, the Walter W. Fondren III Presidential Distinguished Chair of the DeBakey Heart & Vascular Center at Houston Methodist, is the 2024–25 SAVS president.
Lumsden took over from David L. Cull, MD, professor of surgery at the University of South Carolina in Greenville, at the SAVS business meeting, which took place at the end of the association’s 2024 annual meeting in Scottsdale, Arizona (Jan. 24–27).
JVS-CIT RELEASES SPECIAL ISSUE ON GENETIC ARTERIOPATHY
THE JOURNAL OF VASCULAR SURGERY CASES, INNOVATIONS AND Techniques (JVS-CIT) has published its latest virtual special issue, which covers genetic arteriopathy. This is the second special issue published in the journal. JVS-CIT currently plans to publish four per year.
JVS-CIT editors report that there are data showing manuscripts published in virtual special issues have a higher number of publications and are read more often.
The latest special issue theme is dedicated to the diagnosis of underlying aortopathy or arteriopathy etiology, and management of these conditions. The two guest editors are Sherene Shalhub, MD, of Oregon Health and Science University, and J. Westley Ohman, MD, of Washington University School of Medicine.
“Drs. Shalhub and Ohman are national thought-leaders in the management of genetic arteriopathies and were the key to making this issue possible,” said JVS-CIT Editor-in-Chief Matthew Smeds, MD. “They have been able to provide insight into the topic that would have otherwise been missing and helped put together a valuable resource for all vascular surgeons.”
The editorial board and guest editors of JVS-CIT spent six months recruiting content for the genetic arteriopathy issue. It contains 14 case reports and short communications. It can be found at vascular.org/ JVSCITvsiGenetic
JVS-CIT is currently recruiting manuscripts for the next two virtual special issues. The topics being studied include aortic dissections, guest edited by Firas Mussa, MD, and Bernardo Mendes, MD, and vascular trauma, guest edited by Mario D’Oria, MD, and Erica Leith Mitchell, MD. Release dates will be announced soon.
New editorial team selected for Rutherford’s 12th edition
THE SVS EXECUTIVE BOARD HAS appointed the editorial team for the upcoming 12th edition of Rutherford’s Vascular Surgery and Endovascular Therapy. The team now includes Linda Harris, MD, Audra Duncan, MD, and Peter Henke, MD.
Duncan and Henke, alongside Harris, will work with 11th edition editors
Tony Sidawy, MD, Bruce Perler, MD, to prepare the new editorial team for their upcoming tasks.
SVS President Joseph L. Mills, MD, expressed gratitude for the new appointments made to lead the title.
“The Publications Committee and
JVS group openaccess papers
Executive Board had a very difficult decision on its hands with three stellar proposals,” noted Mills. “All would do an outstanding job, and we thank them for their vision and interest in improving Rutherford’s. Drs. Harris, Duncan and Henke are uniquely positioned to take Rutherford to the next level.”
Speaking on behalf of the editorial team, Harris said: “We are excited and honored to have been selected to edit Rutherford’s 12th edition. We look forward to ensuring that it remains our ‘Vascular Bible’ for years to come.
“We expect to continue to innovate so that Rutherford’s is seen as the go-to book for all generations of learners.”
Rutherford’s 11th edition will come out during fiscal year 2025–26, when planning for the textbook’s 12th edition begins.
SVS MEMBERS ARE URGED TO PAY THEIR DUES PROMPTLY TO maintain their SVS membership before suspensions roll out starting in midFebruary. Membership renewal ensures access to a comprehensive SVS membership experience.
To ensure uninterrupted access to these benefits, members are urged to renew their membership before Feb. 15. Suspension emails will be sent out on that date, and renewals can be completed at vascular.org/Invoices
THE JOURNAL OF VASCULAR Surgery (JVS) editors announced the open-access articles available in the flagship title’s March 2024 issue. The relevant papers are: “Creating hemodialysis autogenous access in children and adolescents” (vascular. org/JVShemodialysis); “Safety and efficacy of mechanical aspiration thrombectomy for patients with acute lower extremity ischemia” (vascular. org/JVSsafety); “Safety and learning curve of percutaneous axillary artery access for complex endovascular aortic procedures” (vascular. org/JVSLearningCurve); and “Preoperative predictors of non-home discharge after F/BEVAR of complex abdominal and thoracoabdominal aortic aneurysms” (vascular.org/ JVSpreoperative).
JVS-Venous and Lymphatic Disorders, now a fully open access peer review title within the JVS stable, is available at www.jvsvenous.org
VAM 2024 pricing now available
PRICING INFORMATION FOR THE 2024 Vascular Annual Meeting (VAM 2024) is now available. The event, scheduled in Chicago from June 19–22, is promoted as the year’s premier educational event for all vascular professionals. Organizers urge prospective attendees to secure funding from their institutions before the March registration launch.
VAM 2024 will reintroduce last year’s tiered registration model with an early registration period, a concept that was reintroduced to VAM for the 2023 conference. Early-bird registration will take place from March 20–April 10. After the April 10 deadline, prices will increase to the advance registration rate, which will last through June 17. An increased, on-site registration fee will be available to anyone who cannot register for VAM 2024 in advance.
The tiered registration model offers a significant discount for SVS members, which organizers say is consistent with other SVS education offerings. Individuals who register for the meeting before applying for SVS membership will be eligible to receive the refunded difference if the application is submitted. All membership applications are subject to approval. Visit vascular.org/Join to become a member.
Make a plan to secure your funding for VAM 2024 so you can register early and save. Visit vascular.org/VAM24Pricing to learn more.
Margaret Tracci
THE MOST COMPLETE ONE-DAY ENDOVASCULAR CONFERENCE
MAY 24, 2024
HYATT REGENCY SEATTLE | SEATTLE, WA
The 2024 Pacific Northwest Endovascular Conference will offer its signature interactive learning format, 80+ key opinion leaders on faculty, focused breakout sessions, resident competition and Simulation Summit live in Seattle.
PROGRAM HIGHLIGHTS:
• One-day Powerhouse Program
• 9 CME Credit Hours
• Three Focused Breakout Sessions
MAIN SESSIONS
• Aortic – Modern Management
• Lower Extremity
• Venous
• Physician Practice & Education
• Technical Pearls, Techniques and Tips
MAY
23,
9 CME HOURS
• Simulation Summit for Vascular Trainees
• Resident Competition
• International Abstract Session
• Exhibit Hall and Networking
• Industry Satellite Sessions
CONCURRENT SESSIONS
• Updates on Vascular Surgery for Advanced Practice Providers
• Limb Preservation & Wound Care
• The Business of Vascular Surgery
2024 SIMULATION SUMMIT FOR VASCULAR TRAINEES
Scholarship includes:
• Registration to Summit & PNEC
• Lodging at the Hyatt Regency Seattle
• Travel reimbursement (U.S.-based)
CLINICAL&DEVICENEWS
By Jocelyn Hudson
million) in funding to develop a novel artificial intelligence (AI)-based computed tomography (CT) technology that has the potential to promote climate neutral and sustainable healthcare.
The international, transdisciplinary NetZeroAICT Consortium is headed up by Regent Lee, MBBS, a vascular surgeon scientist at Oxford University Hospitals NHS Foundation Trust and associate professor of vascular surgery at the University of Oxford in Oxford, England.
According to the multidisciplinary group—which further includes Vicente Grau, professor of engineering science at the University of Oxford—the new technology (CT Digital
FDA approves breakthrough device for complex aortic aneurysms
GORE HAS ANNOUNCED FOOD AND Drug Administration (FDA) approval for the Gore Excluder thoracoabdominal branch endoprosthesis (TAMBE), which the company states is the first off-the-shelf endovascular solution for the treatment of complex aneurysmal disease involving the visceral aorta.
“Until now, endovascular treatment options were limited as alternatives to open surgical repair,” said Mark A. Farber, MD, national principal investigator. “TAMBE is an innovative first step forward that enables us to provide care that’s both effective and timely for complex aneurysm repair.”
First patient enrolled in HERCULES trial
Contrast) can make CT scans “safer, faster, more equitable and more sustainable.”
Lee provided a high-level description of how the technology works: the idea is to use AI to enhance non-contrast CT scans with the aim of getting the equivalent outcomes to a contrast scan. He elaborated: “When you do a contrast CT scan, you typically go through the scan twice. The first time, you have a non-contrast CT, and then, based on that non-contrast CT, the radiologist will calculate how tall you are, etc., and calculate the timing of the injection of the contrast. Next, the patient gets scanned a second time to get the contrast-enhanced CT. What we propose is that with AI, we would only require the first noncontrast CT scan. We can extract high-level information from the non-contrast CT scan using AI, overlay where contrast should be on the native non-contrast scan and display it as a digital contrast enhanced scan, without the need for the second scan.”
Regent Lee
The funding received will allow the researchers to move forward with development of the technology. Lee anticipates that the team will face some challenges along the way. He highlights, for example, that clinical acceptance may take time. “What we are proposing to do is quite radical,” he said. “Essentially we are proposing a complete change of how radiology services can be delivered, and there will be questions and reluctance amongst the clinicians to get used to this new way of looking at images.” He likened the task of launching the technology as “almost like trying to introduce a new language into the profession.” Lee also mentioned that patients may be fearful of using an entirely new method of imaging to treat them.
Viabahn VBX stent graft receives FDA approval
GORE REPORTED RECENT FOOD AND Drug Administration (FDA) approval of a lower profile Viabahn VBX balloon expandable endoprosthesis (VBX stent graft) for the treatment of complex iliac occlusive disease.
THE FIRST PATIENT HAS BEEN ENROLLED into the HERCULES trial, which compares endosuture aneurysm repair (ESAR) to standard endovascular aneurysm repair (EVAR) in the treatment of abdominal aortic aneurysms (AAAs) with wide proximal necks.
HERCULES is an investigator-driven trial led by Michel Reijnen, MD, a consultant vascular surgeon at Rijnstate Hospital in Arnhem, The Netherlands, and Konstantinos Donas, MD, head of the Department of Vascular and Endovascular Surgery at Asklepios Clinic Langen in Langen, Germany, in collaboration with Medtronic. Rijnstate Hospital is sponsoring the trial.
The company detailed in a press release that no changes to the stent design were made to achieve the lower profile. The device will be rolled out to the U.S. market over the coming months and is also being studied in the TAMBE trial.
First procedures announced in study of novel peripheral IVL system
FASTWAVE MEDICAL HAS announced the successful completion of enrollment for its first-in-human (FIH) study of the company’s peripheral intravascular lithotripsy (IVL) technology.
The prospective, single-arm study aims to assess the safety and performance of FastWave’s IVL system in patients with peripheral arterial disease (PAD) of the superficial femoral or popliteal arteries with moderate-to-severe calcium.
In a press release announcing the new funding, Lee commented on the wider significance of the consortium’s work: “The combined NetZeroAICT Consortium expertise will enable us to develop and deploy trustworthy ‘green’ AI software as a medical device with the ultimate goal to reduce the environmental footprint from CT imaging.
“European patients will have access to safer, faster, equitable and sustainable healthcare delivery while the healthcare systems strengthen their alignment with the European Green Deal. This is a new era of translational research. In addition to improving patients’ health, our aspiration is to improve planetary health for future generations.”
“Essentially we are proposing a complete change of how radiology services can be delivered, and there will be questions and reluctance amongst the clinicians to get used to this new way of looking at images”
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis is indicated for the treatment of de novo or restenotic lesions found in iliac arteries with reference vessel diameters ranging from 5 mm – 13 mm and lesion lengths up to 110 mm, including lesions at the aortic bifurcation. CONTRAINDICATIONS: Do not use the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
LONG-TERM DURABLE CLINICAL OUTCOMES IN COMPLEX AORTOILIAC OCCLUSIVE DISEASE
Sustained clinical effectiveness through five years1:
primary patency per lesion
freedom from target lesion revascularization per subject
1. Holden A, Takele E, Hill A, et al. Long-term follow-up of subjects with iliac occlusive disease treated with the Viabahn VBX Balloon-Expandable Endoprosthesis. Journal of Endovascular Therapy. In press.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
Please see accompanying prescribing information in this journal. Products listed may not be available in all markets.