Trainee competency Diversity while in training: Is it just yet another box to check?
Skyrocketing vascular nursing costs hammer vascular division's financial bottom line
BY BRYAN KAY
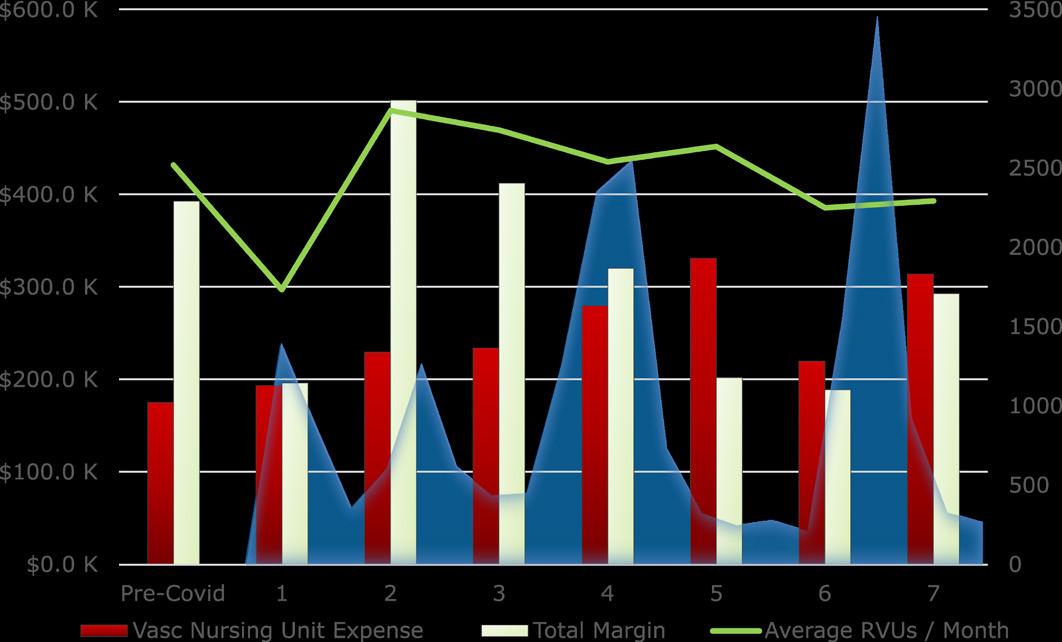
THE PROFIT MARGIN OF A VASCULAR SURGERY DIVISION at a prominent health system in New Orleans was severely eroded during the COVID-19 pandemic period—despite consistent revenue generation throughout—as nursing labor costs dramatically escalated, according to a deep financial analysis carried out by a local research team.
The investigators, led by members of the academic vascular surgery practice at Ochsner Health, looked at the division’s total profit margin across both hospital and outpatient clinics, as well as totals for vascular surgery nursing unit expenses, nursing unit
Patients treated in Food and Drug Administration (FDA)approved investigational device exemption (IDE) trials for complex thoracoabdominal aortic aneurysms (TAAAs) in the U.S. Aortic Research Consortium (ARC) had better 30day and one-year survival compared with those recorded in the real-world Vascular Quality Initiative (VQI) registry, new data presented at the 2022 Southern Association for Vascular Surgery (SAVS) annual meeting revealed.
Silence is golden—but does self-imposed silence lead to burnout?
BY BHAGWAN SATIANI, MD
Burnout is associated with silence in various contexts. It is called the silent crisis, the silent epidemic, or the silent killer. What is not talked about is the pressure or fear at work, whether professional or personal, that can lead to avoidance behavior and self-imposed silence. Surgical residents have been reported to have burnout rates >60%, and it is likely that causative factors include the pressure or fear at work. My concern has to do with silence associated with physician employees in non-clinical roles at the individual level.
TO THIS END, THE EFFECTS OF SILENCE ON burnout were studied in 600 adults.1 Four differentially motivated types of silence (acquiescent, quiescent, prosocial, and opportunistic) were studied with three components of burnout (depersonalization, emotional exhaustion, and perceptions of reduced personal accomplishment). Pro-social and opportunistic types of silence were self-imposed, whereas acquiescent and quiescent silence were forced. The authors concluded that silence likely leads to burnout, not the other way around. It is also likely that one of the critical factors leading to burnout in employed physicians is self-imposed silence. As an employee, their ability to speak out or “voice” is defined as the “discretionary communication of ideas, suggestions, concerns, or opinions about work-related issues with the intent to improve organizational or unit functioning.”2 In contrast, employee “silence” is the “conscious withholding of information, suggestions, ideas, questions, or concerns
about potentially important work- or organization-related issues from persons who might be able to take action to address those issues.”2
There is obviously some nuance to this, rather than a binary choice. Benign examples of silence include new hires choosing to be silent in order to scan the workplace and, with time, evolve into a voice. Experienced hires may start as a voice but, either from bad experiences associated with career derailment or fatigue based on learned helplessness (lack of response for change) may choose to stay silent. Also, physicians may be a voice on some and adopt silence on other issues. Furthermore, because one is a voice in meetings does not mean that person does not have hidden feelings and, similarly, the quiet physician does not necessarily imply that that physician has hidden issues they are holding inside. In addition to individual or intrinsic factors, silence may be self-imposed due to extrinsic factors. Some of us may resent being under pressure to stay silent in order to avoid personal harm, and take on passive-aggressive behavior by being a voice on easy, non-controversial issues, but withhold important and critical information from leaders.
Reasons for this self-imposed silence may be several, but primarily because it represents a danger in some way, or is seen as pointless. Job security, academic promotion, or moving up in a professional society may lead to internal pressure to inhibit expression and modify behavior, which then takes a psychological toll on the physician—especially in a personality that wants to progress but does not like making “waves.”
Is there a link between silence, psychological safety and burnout? Apparently, yes. Knol indicates that it is frequent silence, particularly “high silence” (suppression of serious flaws), that engenders burnout rather than voice reducing
Is there a link between silence, psychologic safety, and burnout? Apparently yes
it.1 Sherf and colleagues contend that we rely on our biologically based intrinsic “behavioral activation system” and “behavioral inhibition regulatory system” to assist us on when we use our voice or silence.3 The former is more of a positive state of mind and hopeful, whereas the latter is concerned with the worry, even threats, from speaking out. They also point out that individual personality traits— such as extroversion for instance—may affect outcomes. Having had experience in both the private sector as well as the academic workplace, I have observed that the latter physician is more prone to suffer burnout from pressure to remain silent, probably because one expects to express one’s thoughts and ideas freely in the learning environment. I have seen senior faculty fear for their job and career advancement if they were to speak out and displease a chair or a dean. This forced silence then becomes incorporated into the culture as younger folks watch and learn that they do not have the freedom to
continued on page 4
VASCULAR SPECIALIST
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD, Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Christopher Audu, MD
Executive Director SVS Kenneth M. Slaw, PhD
Director of Membership, Marketing and Communications Tara J. Spiess, CAE
Managing Editor SVS Beth Bales
Marketing & Membership Specialist
Amber Dunlop
Assistant Marketing & Social Media Manager
Kristin Crowe
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA Publishing. Content for the News From SVS is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA Publishing will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein.
The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com.
For missing issue claims, e-mail subscriptions@bibamedical.com.
Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA Publishing.
Published by BIBA Publishing, which is a subsidiary of BIBA Medical Ltd.
Publisher Roger Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Jocelyn Hudson, Will Date, Jamie Bell, Sarah Croft, Anthony Strzalek and Aaron Kudhail
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe 526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America 155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Bhagwan Satiani
Silence is golden— but does selfimposed silence lead to burnout?
continued from page 2
dissent. Among other stressors, inability to express ideas at work is a recipe for burnout. One could blame the general erosion of free speech, but this facet existed long before current trends.
Why is this important for hospital leaders? Leaders may not be aware that they are suppressing employee voices and fostering silence, because high silence in a health system is not only related to exhaustion and burnout, but hurts productivity. It also harms patient care in the safety and quality-of-care sphere.
Leaders are also trying to combat burnout using all the tools they have but may remain non-cognizant of the link between silence and burnout. Instead, their way of addressing burnout is of a transactional nature.
How does the leader provide psychological safety to physicians and other employees and assure their well-being? Psychological safety is described as ‘‘the degree to which people view (their) environment as conducive to interpersonally risky behaviors like speaking up or asking for help.”4
Establishing psychological safety has to be part of a cascading organizational culture. In the non-clinical areas, leaders should allow, support and commend physicians to take risks by sharing information and ideas, asking
Endurant™ II/Endurant™ IIs Stent Graft
questions, offering feedback and airing concerns. Anonymous surveys that do not ask for demographic data, may allow frank input. While supportive voices are given more weight by leaders and managers, giving physicians space to freely share their thoughts and ideas in a safe manner needs to be emphasized. Besides the resilience, as well as mindfulness training, tips on communication skills that include techniques to express thoughts in a non-threatening manner may also be useful.
Ultimately, our leaders need to be encouraged to allow respectful dissent and discussion under the umbrella of psychological safety for physician employees. Self-imposed silence is an important stressor for burnout.
References
1. Knoll M, Hall RJ, Weigelt O. A longitudinal study of the relationships between four differentially motivated forms of employee silence and burnout. Journal of Occupational Health Psychology. 2018; 24(5), 572–589.
2. Morrison, E. W. Employee voice behavior: Integration and directions for future research. The Academy of Management Annals. 2011; 5(1), 373–412.
3. Sherf EN, Parke MR, Isaakyan, S. Distinguishing voice and silence at work: Unique relationships with perceived impact, psychological safety, and burnout. Academy of Management Journal. 2021; Vol. 64, No. 1, 114–148.
4. Edmondson AC, Higgins M, Singer S, et al Understanding psychological safety in health care and education organizations: A comparative perspective. Res Hum Dev. 2016; 13:65–83.
BHAGWAN SATIANI is professor emeritus in the division of vascular diseases and surgery in the College of Medicine at The Ohio State University, Columbus, Ohio. He is an associate medical editor of Vascular Specialist.
Marston: Diversity required to deliver comprehensive care to vascular disease population
WILLIAM A. MARSTON, MD, WAS RECALLING A recent experience acting as a bone marrow donor for a family member, and the moment it dawned on him, after the harvesting procedure with a specialist in the field, the true value of the knowledge, skill and training it takes to make the routine routine in his own vascular domain. “In our world, this is devalued,” said the vascular surgery division chief at the University of North Carolina at Chapel Hill. He was addressing the 2022 Southern Association for Vascular Surgery (SAVS) annual meeting (Jan. 19–22) in Manalapan, Florida, his swansong as SAVS president. “These procedures are life and limb saving,” he told attendees. “The things that we do, we do them every day—but we don’t internalize or appreciate it.”
Marston provided a prescription for his peers struggling to fully appreciate what it is they do day after day. “Take satisfaction in providing good patient care, even if it’s not procedural. If you advise someone not to have a procedure, that may sometimes be the best thing that you could do,” he said. “Support your peers, talk to each other; we all have complications, be realistic about them.” Beware comparing yourself to podium experts, Marston said. “Most of us are experts in little, narrow things. When we talk about some great case we did, for me it might be a vena cava reconstruction. But I don’t do complex aneurysms with Mark Farber around. I don’t do retrograde pedal access. So, if you’re treating a broad selection of vascular patients, do a good job, do the best techniques you can and sleep well with it.”
He titled his address around the concept of the vascular surgeon and what might be “the right stuff” for specialists—a play on the eponymous 1980s movie about the pioneering days of the U.S. space development program and the space race’s symmetry with the swashbuckling gestation period of the vascular surgical specialty. “In the movie,” Marston said, “astronauts competed to be the first; they all wanted to be the first in space, and that had to be the best one. But I believe that today, in 2022, the right stuff should be defined by the collective success of a program to provide focused care for the largest population of patients with vascular disease possible. To achieve this, we need vascular surgeons of all backgrounds, all races, all ethnicities with the diversity to deliver care to all patients with vascular disease.”—Bryan Kay
Indications: The Endurant™ II/Endurant™ IIs bifurcated stent grafts are indicated for the endovascular treatment of infrarenal abdominal aortic or aortoiliac aneurysms. They may be utilized in conjunction with the Heli-FX™ EndoAnchor™ system when augmented radial fixation and/or sealing is required; in particular, in the treatment of abdominal aortic aneurysms with short (≥ 4 mm and < 10 mm) infrarenal necks (see Neck length definition below). The Endurant II stent graft system aorto-uni-iliac (AUI) stent graft is indicated for the endovascular treatment of infrarenal abdominal aortic or aortoiliac aneurysms in patients whose anatomy does not allow the use of a bifurcated stent graft. The Endurant II/IIs stent graft system is indicated for use in patients with the following characteristics: • Adequate iliac or femoral access that is compatible with vascular access techniques, devices, or accessories • Proximal neck length of • ≥ 10 mm; or • ≥ 4 mm and < 10 mm when used in conjunction with the Heli-FX EndoAnchor system (bifurcated stent graft only)
Note: Neck length is defined as the length over which the aortic diameter remains within 10% of the infrarenal diameter. • Infrarenal neck angulation of ≤ 60° • Aortic neck diameters with a range of 19 to 32 mm • Distal fixation length(s) of ≥ 15 mm • Iliac diameters with a range of 8 to 25 mm • Morphology suitable for aneurysm repair
Contraindications: The Endurant II/Endurant IIs stent graft system is contraindicated in: • patients who have a condition that threatens to infect the graft • patients with known sensitivities or allergies to the device materials When used with the Heli-FX EndoAnchor system, the Endurant II/IIs stent graft system is also contraindicated in: • patients with known sensitivities to the EndoAnchor implant materials. For contraindications regarding ancillary devices used with the Endurant II/Endurant IIs stent graft system, refer to the Instructions for Use provided with the device.
Warnings and Precautions: • The long-term safety and effectiveness of the Endurant II/Endurant IIs stent graft system has not been established. All patients should be advised that endovascular treatment requires lifelong, regular follow-up to assess the health and the performance of the implanted endovascular stent graft. Patients with specific clinical findings (e.g., endoleaks, enlarging aneurysms, changes in the structure or position of the endovascular graft), or less than the recommended number of EndoAnchor implants when used in short proximal necks (≥ 4 mm and < 10 mm), should receive enhanced follow-up. Specific follow-up guidelines are described in the Instructions for Use. • Patients experiencing reduced blood flow through the graft limb, aneurysm expansion, and persistent endoleaks may be required to undergo secondary interventions or surgical procedures. • The Endurant II/Endurant IIs stent graft system is not recommended in patients unable to undergo or who will not be compliant with the necessary preoperative and postoperative imaging and implantation procedures as described in the Instructions for Use. • Renal complications may occur: 1) From an excess use of contrast agents. 2) As a result of emboli or a misplaced stent graft. The radiopaque marker along the edge of the stent graft should be aligned immediately below the lower-most renal arterial origin. • Studies indicate that the danger of micro-embolization increases with increased procedure duration. • The safety and effectiveness of the Endurant II/ Endurant IIs stent graft system has not been evaluated in some patient populations. Please refer to the product Instructions for Use for details.
MRI Safety and Compatibility: Non-clinical testing has demonstrated that the Endurant II/Endurant IIs stent graft is MR Conditional. It can be scanned safely in both 1.5T & 3.0T MR systems under certain conditions as described in the product Instructions for Use. For additional MRI safety information, please refer to the product Instructions for Use.
Adverse Events: Potential adverse events include (arranged in alphabetical order): amputation; anesthetic complications and subsequent attendant problems (e.g., aspiration), aneurysm enlargement; aneurysm rupture and death; aortic damage, including perforation, dissection, bleeding, rupture and death; arterial or venous thrombosis and/or pseudoaneurysm; arteriovenous fistula; bleeding, hematoma or coagulopathy; bowel complications (e.g., ileus, transient ischemia, infarction, necrosis); cardiac complications and subsequent attendant problems (e.g., arrhythmia, myocardial infarction, congestive heart failure, hypotension, hypertension); claudication (e.g., buttock, lower limb); death; edema; EndoAnchor system (for infrarenal EVAR procedures using the Heli-FX EndoAnchor system): partial deployment, inaccurate deployment, fracture, dislodgement, embolization, stent graft damage, modelling balloon damage); embolization (micro and macro) with transient or permanent ischemia or infarction; endoleak; fever and localized inflammation; genitourinary complications and subsequent attendant problems (e.g., ischemia, erosion, femoral-femoral artery thrombosis, fistula, incontinence, hematuria, infection); hepatic failure; impotence; infection of the aneurysm, device access site, including abscess formation, transient fever and pain; lymphatic complications and subsequent attendant problems (e.g., lymph fistula); neurologic local or systemic complications and subsequent attendant problems (e.g., confusion, stroke, transient ischemic attack, paraplegia, paraparesis, paralysis); occlusion of device or native vessel; pulmonary complications and subsequent attendant problems; renal complications and subsequent attendant problems (e.g., artery occlusion, contrast toxicity, insufficiency, failure); stent graft: improper component placement; incomplete component deployment; component migration; suture break; occlusion; infection; stent fracture; graft twisting and/ or kinking; insertion and removal difficulties; graft material wear; dilatation; erosion; puncture and perigraft flow; surgical conversion to open repair; vascular access site complications, including infection, pain, hematoma, pseudoaneurysm, arteriovenous fistula, dissection; vascular spasm or vascular trauma (e.g., iliofemoral vessel dissection, bleeding, rupture, death); vessel damage; wound complications and subsequent attendant problems (e.g., dehiscence, infection, hematoma, seroma, cellulitis). Please reference product Instructions for Use for more information regarding indications, warnings, precautions, contraindications and adverse events.
CAUTION: Federal (USA) law restricts this device to sale by or on the order of a physician.
medtronic.com/aortic
trademarks of Medtronic. ™*Third party brands are trademarks of their respective owners. All other brands are trademarks of a Medtronic company. For distribution in the USA only. 11/2021
William A. Marston
Radiation protection: Lightweight shield designed to reduce eye, brain dose during complex endovascular procedures gains ground
BY SARAH CROFT
It all started with a “we should do research together; this is fascinating.” The result— the production of a prototype eyewear that decreases radiation to the eye and brain—is the more-than-decade-long toil of Melissa Kirkwood, MD, and colleagues at UT Southwestern in Dallas, Texas. From conference podium to conference podium, through endless research studies and paper-writing, Kirkwood has put in the miles to get the disposable, lightweight shield patented. Here, the UT Southwestern vascular chief tells Vascular Specialist about her journey and production of the “much-needed” device aimed at helping surgeons and interventionalists combat radiation exposure.
VS: Can you give an overview of your research journey in radiation safety so far?
MK: Yes, about 11 years ago our vascular division was flagged for having a high radiation dose case. It involved a physician modified aortic stent graft in a morbidly obese patient. Because of this, our radiation physicists had to come and speak with us as a group. I was fascinated by the topic and what they were discussing. There are so many simple things that we can do to decrease our radiation dose. After this talk with the physicists, I went up to Dr. Gary Arbique and Dr. Jeffrey Guild and said, “We should do research together; this is fascinating.” Our first project was simply looking at the radiation dose from our complex cases before and after our talk with the physicists, during which we learned some tricks to decrease dose. After controlling for multiple factors, we were able to show that by implementing simple things, you can significantly drop the radiation dose. We then looked at the risk of deterministic effects, namely skin injuries in patients following high radiation dose cases. We studied this initially retrospectively. We then started a prospective study following these patients with skin exams. What we found was skin injuries are extremely rare and are likely multifactorial, with some patient predisposing factors and not solely based on dose.
Then we progressed and looked deeper, specifically at surgeon dose. We found that factors like where the surgeon stands around the table, whether the tablemounted lead skirt is utilized, and what type of case is performed matter significantly. This paper showed that fenestrated endovascular aortic repairs (FEVARs) are by far the highest dose cases that we perform as vascular surgeons, so then we took a deeper dive looking only at FEVARs. We showed that not all FEVARs are equal in dose, and that custom-made devices require more dose than pre-manufactured devices, and the number of vessel fenestrations is a driver of increased dose. After this study, we focused on additional adjuncts to lower dose during FEVARs, such as using dual fluoroscopy with live digital zoom instead of magnification modes; employing a two-dimensional vessel navigator roadmap instead of an on-table 3D CT; and ensuring all equipment is up to date on new dose-lowering software.
Most recently, we have been focusing on what does not work for radiation. We have shown that the no-brainer surgical caps and regular leaded caps do not decrease
perfecting the design and have created a prototype, which is patented at UT Southwestern Medical Center. The eyewear attachment has been proven to decrease both eye and brain dose to the operator, and works equally well added to leaded or non-leaded routine prescription eyewear. This was recently presented at the 2021 Western Vascular Society (WVS) annual meeting.
VS: What more can you tell us about the latest data?
MK:. In this study, we have shown that when this prototype is added to leaded or non-leaded glasses, the dose to the lens, temporal lobe and midbrain is reduced by 85%, 81% and 71%, respectively. This means that interventionalists do not have to buy and wear leaded lenses anymore.
Our prototype is just as effective when added to plastic safety glasses or prescription eyewear. The device is lightweight, detachable and reversible, so it can be used for either the right or left eye/face. Only the eye that is closest to the X-ray source needs coverage. The prototype has a sleeve for the temples of the eyewear, and then the shield is molded around the operator’s face and the inferior aspect of the lenses by a conformable wire. The adhesive strip attaches to the surgical mask, eliminating any air gap between the lower face and the eyewear. It is made of lead-equivalent shielding sewn into soft cloth material. Even though it is disposable, it is not necessarily single use. I have worn it in multiple procedures without any decrease in efficacy. And the best part is, it is comfortable and there is no fogging.
We are really excited about this shield because it is an easy adjunct that can be incorporated into daily practice to improve safety. When the interventionalist goes to grab his or her hat, mask, and shoe covers, that is when to grab the eye/face shield too.
VS: Do you think your findings will change future practice?
This shield is something that should be added to the operating room routine when you are grabbing your mask and eyewear protection
brain radiation at all, because the radiation that hits the head is from scatter radiation already attenuated through the patient and not hitting the head at 90-degree angles. After discovering this we questioned the effectiveness of leaded eyewear. Sure enough, we proved that leaded eyewear does not decrease eye dose at all due to the significant air gap between the face and the leaded lens. The leaded lens can only attenuate direct X-rays to the eyes, and since all the scatter is from the patient hitting the interventionalist at angles not covered by the glasses, they are completely ineffective. However, this seemed like a solvable problem. Our first attempt at this was studying the efficacy of adding leaded shielding to the lateral and inferior aspect of the glasses. This was a success. Closing the air gap between the operator’s face and their eyes significantly decreased eye dose. But this design was heavy, uncomfortable and caused fogging. Therefore, we have been working on
MK: I hope so. Many reports have shown an increased prevalence of radiation-induced lens damage (cataracts) and brain cancer in interventionalists. The International Commission on Radiological Protection (ICRP) has set the occupational dose limit to the lens of the eye at a 20 mSv/year average over five years, with no annual dose in a single year exceeding 50mSv. Thus, the results from this study have shown that with the addition of our prototype, operators can safely perform exponentially more cases and still stay under the aforementioned ocular dose threshold. We strongly believe that our design can help mitigate some of the long-term health complications that interventionalists can experience, and hope that using our eye/face shield becomes standard practice to improve safety.
VS: Have there been any other recent developments?
MK: Not on this study, but we did just present at the 2022 Southern Association for Vascular Surgery (SAVS) annual meeting on the efficacy of lower-leg leaded garments in decreasing lower-body radiation dose during FEVARs. We also presented some new data on the CLEAR-MAX imaging technology system and how it lowers radiation dose on Siemens systems. Next steps are working with UT Southwestern to find a commercialization partner to bring the product to market. Stay tuned!
Melissa Kirkwood
How an aortic ally can help physicians optimize patient outcomes
BY KIMBERLEY WUNDER, PHD
The aorta is special. As one of the most complex and critically important vessels of the vascular system, the aorta presents unique challenges. As such, it deserves an investment in constant and specialized care to ensure optimal patient outcomes.
I’VE OFTEN HEARD THE QUESTION
“What is the device manufacturer’s role beyond providing products?” Clinicians benefit greatly from a device manufacturer relationship that provides much-needed clarity on recommended solutions for their patient. From highly responsive device delivery, to deeply specialized technical expertise, to complete consultative discussions, physicians need to know they can count on their medical device provider as a source of integral support. Physicians need an aortic ally who is equally invested in achieving the best possible outcomes for patients.
Whether a vascular or cardiothoracic surgeon is performing an endovascular aneurysm repair (EVAR) or thoracic EVAR (TEVAR) procedure, they need to feel they can trust and rely on the device, as well as the manufacturer’s clinical and
Kimberley Wunder
technical knowledge that support the use of that device.
For example, a trusted aortic ally supports the physician well beyond the acquisition of a product, providing technical expertise for their device of interest and supporting clinical decision-making by sharing their knowledge of clinical trials and outcomes. What type of experience and knowledge does the clinical or sales representative offer? How many cases do they support on average? They should be able to rely on their aortic ally for timely responses, trusted information, and essential technical device proficiency for EVAR and TEVAR procedures, literature case studies, and device specificity for unique anatomies and cases.
“How does a medical device manufacturer evolve to demonstrate commitment to innovation and valuable experiences to provide the best outcomes for patients?”
How does a medical device manufacturer evolve to demonstrate commitment to innovation and valuable experiences to provide the best outcomes for patients? A good aortic ally is committed to the development, support and refinement of physician-supportive resources. Such resources include case studies and educational webinars to share
surgical expertise, thought leadership on cutting-edge research, clinical trial developments, and the latest product innovations, demonstrations and videos of device use, product information and literature, and peer recommended techniques. This array of supporting resources should be simple to navigate, have practical application, and be succinct and easy to share with physician peers.
In today’s fast-moving surgical landscape, this means device manufacturer support that goes beyond products and considers holistic solutions that can be tailored to different types of patients. Equally important is an understanding of aortic device limitations in critical cases. A device manufacturer committed to the best patient outcomes includes a sales force with a focus on supporting physicians in choosing the right product for each patient, even when that product is not their own.
Ultimately, an aortic ally combines innovation with reliability for solutions that deliver real-world improvements to the lives of patients with aortic disease.
Visit goremedical.com/aorticsupport to find out how an aortic ally can help you.
KIMBERLEY WUNDER is a Clinical Application Specialist at W. L. Gore & Associates, delivering clinical and operational expertise, and providing education and training support within the aortic product portfolio to clinical end-users. She is passionate about engaging with customers, and accelerating research and development efforts into improved clinical outcomes.
US ARC IDE registry reports better survival vs. real-world data after endovascular repair
continued from page 1
Results from the consortium’s retrospective analysis of U.S. ARC and VQI procedures carried out between 2011–2019 were delivered by Ryan Heslin, BS, a medical student at the University of South Alabama College of Medicine in Birmingham, Alabama, with senior author Adam Beck, MD, vascular division director at the University of Alabama at Birmingham and one of the IDE investigators, present as a moderator of the scientific session in which the paper featured.
The research team aimed to compare the real-world setting of the Society for Vascular Surgery (SVS) VQI database to that of the now 10-strong physician-sponsored U.S. ARC trials in order to evaluate the effect of custom-built or off-theshelf fenestrated/branched endovascular devices. Despite the fact there are no commercially available devices for the repair of TAAAs in the U.S., an increasing number of patients are felt to be at high risk for open repair and are therefore undergoing endovascular repair, Heslin noted.
“These data are collected in the SVS VQI registry,” he said. “The U.S. Aortic Research Consortium has access to these custom-built branched/fenestrated endovascular devices that are designed to match patients and are not present in the VQI.”
The analysis of 3,212 patients—all of whom underwent elective procedures for asymptomatic, non-ruptured aneurysms, and had defined zones of endograft
deployment—showed a 30-day mortality rate of 6.1% in the VQI vs. 2% in the U.S. ARC for Crawford classification system extent 4 TAAAs. At one year, the equivalent rates were 12.3% (VQI) vs. 8.4% (ARC). Similarly, 30-day and one-year mortality in the cases of extent 1–3 and 5 aneurysms were 7.3% (VQI) vs. 2.6% (ARC), and 16.3% vs. 13.1%, respectively.
“The appearance of our Kaplan Meier survival curves mostly mirror our findings at 30 days and one year, with a significant drop off in the perioperative period for the VQI group, but a significant difference in survival was noted in both groups,” Heslin added.
“Patients repaired in the IDE studies have better perioperative and one-year survival compared to patients treated off label or entered in a real-world registry, regardless of extent” Ryan Heslin
Commenting on the idiosyncracies two registries, Heslin explained that though the patient populations studied are similar in terms of pathology, “the conditions under which they are studied are quite different.” He continued: “The VQI represents real-world practice using off-label techniques, including physician-modified grafts [PMEGs] and parallelstenting techniques. This dataset allows us to evaluate endovascular techniques outside of clinical trial settings, and thus is much more representative of the general population.
“The U.S. ARC is a group of investigators with physiciansponsored IDEs that has access to endovascular repair using custom-built or off-the-shelf medical devices. This allows us to evaluate the outcomes of endovascular repair in a clinical
Aortic Research Consortium ‘pushes the envelope’ on F/BEVAR
BY JOCELYN HUDSON
The U.S. investigational device exemption (IDE) Aortic Research Consortium (ARC) has produced the strongest data so far on the use of fenestrated/branched endovascular aneurysm repair (F/ BEVAR), Andres Schanzer, MD, professor and chief of vascular surgery at the University of Massachusetts Medical School in Worcester, Massachusetts, claimed at the Critical Issues in Aortic Endografting 2021 meeting (Dec. 17–18) in Paris, France. As a result of the group’s work, “more patients are getting better care, by more providers, using F/BEVAR devices,” he said, summarizing a slew of data unveiled since 2018.
The primary objective of the ARC, first conceived of in 2018, is to evaluate custom-made fenestrated and branched endovascular devices for the treatment of patients with complex abdominal, thoracoabdominal and arch aneurysms, Schanzer detailed. He noted that, currently, the literature includes primarily iterative, single-center reports, the findings of which “may be limited due to the potential for a type 1 error secondary to limited statistical power.” According to Schanzer, ARC medical director, that is about to change,
as the consortium includes prospective, physician-sponsored data from across 10 U.S. sites and is independently monitored and Food and Drug Administration (FDA) audited. Referencing an email he sent to investigators when initiating this effort in early 2018, Schanzer wrote: “If we are able to pull this off and figure out a way to aggregate our data in a relatively seamless way and work together as a team of investigators, I believe we have the potential to make a much more significant impact than multiple iterative, single-center reports.”
trial setting. It is important to know these patients are highly selected for and studies are under heavy scrutiny from multiple avenues.” Heslin pointed out that the researchers had elected to study Crawford extent 4 aneurysms separately from extents 1–3 and 5 mostly because of overall volume, their lack of a thoracic component, and differences in overall management.
Notable differences among extent 4 patients in the U.S. ARC population included the fact they were more often Caucasian, male and in possession of a history of coronary artery disease (CAD), he said. The VQI equivalent patients more commonly had a history of chronic obstructive pulmonary disease (COPD) and diabetes. Those with extent 1–3 and 5 aneurysms in the ARC dataset were more likely to be older by about a year, Caucasian, and have a history of CAD. Their VQI counterparts were more likely to have a history of congestive heart failure and COPD. “It is important to note that maximal aneurysm diameter did not vary across the VQI or ARC datasets in any Crawford extent,” said Heslin. He conceded certain limitations to the study. “We did not evaluate risk-adjusted mortality,” he began. “While patients overall had similar comorbidities, disease-specific death was not used to compare overall survival. We believe that risk adjusting this type of analysis removes the clinical decisionmaking that is critical in these elective procedures in complex aneurysms. Additionally, we did not evaluate long-term mortality after one year. We believe that 30-day mortality likely represents procedural success in patient selection, and one-year mortality is indicative more specifically of patient selection.
“Although reintervention and device or aortic failures may impact longer-term survival, this is likely more impacted by patient factors such as age and comorbidities, as well as unmeasured outcomes such as cancer-related deaths. In summary, in both the ARC and VQI cohorts, more extensive
Key datasets highlight growing pool of evidence
Members of the U.S. F/BEVAR ARC have presented data on behalf of the consortium at several key conferences since 2018.
The datasets started off small, Schanzer relayed. At the Society for Vascular Surgery (SVS) 2018 Vascular Annual Meeting (VAM) in Boston, for example, Emanuel R. Tenorio, MD, a postdoctoral researcher at the University of Texas Health Science Center at Houston in Houston, Texas, presented outcomes of endovascular repair of post-dissection and degenerative thoracoabdominal aortic aneurysms (TAAAs) using fenestrated and branched stent grafts. The study,
which incorporated 240 patients, showed F/BEVAR to be safe and effective, with similar outcomes in patients with postdissection and degenerative TAAAs, and also that patients with post-dissection had more type II endoleak during follow-up.
Tenorio stressed that larger clinical experience and longer follow-up was needed to better evaluate differences in mortality, spinal cord injury, target vessel instability and secondary interventions.
At the same meeting, Schanzer recounted, Darren B. Schneider, MD, chief of vascular surgery and endovascular therapy at the University of Pennsylvania, Philadelphia, presented target artery outcomes after branched and fenestrated
Andres Schanzer
aneurysms, extents 1, 2, 3 and 5, have poorer survival at 30 days and one year. Survival at 30 days and one year was statistically better for ARC patients in both groups.”
The challenges faced in repairing TAAAs with endovascular devices has bred brisk surgeon activity in the arena, Heslin commented. “Limitations of endovascular repair have largely been challenges related to the inclusion of aortic branches, thus patients needed to be anatomically suitable for optimal repair,” he said. “This problem has inspired numerous and creative ways that vascular surgeons have continued to approach thoracoabdominal aneurysm repair, including PMEGs, parallel-stenting grafts and other techniques, and most-recently custom or purpose-built endografts designed to specifically match patient anatomy.”
That’s where the IDE trials come in.
Concluding, Heslin highlighted that the IDE trial patients studied had better perioperative and one-year survival compared to patients treated off label or entered in a real-world registry, regardless of extent.
“The reasons for these differences require further analysis and remain unclear,” he said. “A couple of things they could be related to would be differences in devices or device durability, differences in device comorbidity profiles, the intangible surgeon and patient psychosocial factors related to when, whether and how to repair these aneurysms, as well as volume-related outcomes. All of these IDE centers have dedicated teams of research coordinators and nurses. These include dedicated resources and additional infrastructure that help manage those patients. This allows for a more programmatic approach to each patient, which likely contributes to better outcomes.”
Designated discussant Michol A. Cooper, MD, an assistant professor in the division of vascular surgery and endovascular therapy at the University of Florida College of Medicine in Gainesville, Florida, asked for further comment on the survival curves, saying: “Although the overall mortality for the VQI is greater for patients in both groups, based on the Kaplan Meier curves, the
endovascular repair of pararenal aortic aneurysms and TAAAs in 661 patients.
Schneider summarized that the selective use of fenestrations and directional branches for visceral artery incorporation is durable, that the risk of target artery instability is higher for renal versus mesenteric arteries, and that greater TAAA extent is associated with increased target instability.
Future efforts, he informed the VAM 2018 audience, should focus on improving renal artery patency and reducing interventions.
Later that same year, Schanzer recalled that Carlos H. Timaran, MD, the Sam H. Phillips, Jr. MD Distinguished Chair in Surgery at University of Texas Southwestern, Dallas, Texas, gave evidence on the expanded use of preloaded branches and fenestrated endografts for endovascular repair of complex aortic aneurysms.
Speaking at the 32nd European Society for Vascular Surgery (ESVS) Annual Meeting in Valencia, Spain, Timaran presented data on 564 patients, concluding that the expanded use of preloaded catheters and wires of fenestrations and directional branches for target artery incorporation is associated with even higher technical success and lower early mortality.
Schanzer then looked back to the 2019 VAM in National Harbor, Maryland, where he presented results of F/BEVAR after failed infrarenal EVAR in 893 patients. He noted that F/BEVAR was safe and effective in patients with prior failed EVAR, with
majority of the difference appears to be in the initial postoperative period, after which the mortality curves parallel each other.”
Heslin pondered several possibilities associated with a “really high” relative risk of perioperative mortality. “We discussed patient selection and procedural success previously, which we believe certainly could play a role. Additionally, it could be related to a high-volume center. You could have staff and nurses and dedicated teams, like there is in the IDEs, that are much more comfortable managing the complications that may arise. So, successfully managing these perioperative complications may additionally lead to decreased perioperative mortality as well.”
The data also prompted Murray Shames, MD, chief of vascular surgery at the University of South Florida (USF) Health Morsani College of Medicine in Tampa, Florida, to ask Heslin whether “industry has a responsibility to expand access if it is shown that [these] devices are better than what is being done in the real world.” The rest of the world has access to such devices, he said. “Europe has devices, Asia has devices, Australia has devices, and we are still limited to [the IDE] sites.”
U.S. ARC investigator and session moderator Beck stepped in, arguing that responsibility also falls upon the FDA to expand access. “These things are going to be expanded,” he said. “It is just going to take time. Unfortunately, we may be talking about five or 10 years down the road before these things are available.”
Shames said his institution has two IDE trials of its own—one involving purpose-built and the other PMEG devices. Beck reasoned that PMEG IDEs “would be really interesting to study in addition to the VQI data, which are non-IDE PMEG devices, essentially.” David Minion, MD, a professor of surgery at the University of Kentucky in Lexington, Kentucky, added that specialists faced a reproducibility crisis. “Seventy percent of all studies are not reproducible.” He wondered whether the right question was being asked: “Is it getting more access to more centers? How do we deal with that crisis of being able to compare these things?”—Bryan Kay
nearly identical outcomes as compared to patients without prior EVAR, while differences in procedural metrics indicated higher level of technical challenge when performing F/BEVAR in patients with prior failed EVAR.
The speaker concluded that F/BEVAR, at high-volume centers, is a viable option for the treatment of EVAR failure that compared favorably to historical reports of open conversion.
“More patients are getting better care, by more providers, using F/BEVAR devices”
Andres Schanzer
At the 33rd ESVS Annual Meeting in Hamburg, Germany, in 2019, Fernando Motta, MD, a vascular surgeon at the University of North Carolina, Chapel Hill, North Carolina, informed the audience that F/BEVAR is a safe and effective option for octogenarians in training complex aortic aneurysms compared to nonoctogenarians, Schanzer detailed, outlining data from 893 patients.
Finally, Schanzer gave an overview of the largest U.S. IDE Consortium dataset so far—a study on sex-related outcomes after F/BEVAR for TAAAs involving 1,681 patients. Announcing the findings during ESVS Month in 2020, Matthew P. Sweet, MD, a vascular surgeon at the University of
Washington, Seattle, revealed that women experienced higher rates of technical failure for extensive aneurysms, non-home discharge and postoperative sac expansion.
A turning point for fenestrated and branched procedures
Addressing the Critical Issues audience, Schanzer summarized that the U.S. F/ BEVAR ARC is the largest dataset of fenestrated and branched procedures in the world. The consortium involves a core group of investigators “committed to improving patient care and pushing the envelope on endovascular therapies from the aortic valve to the common femoral artery,” he said
The consortium is “an engine for exchange of ideas and promotion of F/BEVAR technologies,” the speaker continued, emphasizing his hope that the group’s work will have an impact not just in the U.S. but across the globe.
On a more practical level, Schanzer said, the consortium “offers infrastructure and a more agile regulatory pathway for testing emerging technologies to obtain preliminary data,” and also represents a departure from the heretofore single-center reports.
The project provides a framework in which to conduct randomized trials, Schanzer stressed, noting that the trajectory of F/BEVAR technologies has reached an “inflection point.”
Larger studies will henceforth reveal the direction of travel in this developing field, he added.
More proximal landing zone produces better outcomes for TEVAR of acute TBAD, study finds
A review evaluating the results of thoracic endovascular aortic repair (TEVAR) following acute type B aortic dissection (TBAD) suggests most patients have less than 2cm of proximal healthy descending thoracic aorta. In patients treated for complicated acute TBAD, zone 2 TEVAR is associated with a lower need for aortic reintervention and aortic-related adverse events than zone 3 TEVAR, researchers behind the study found.
Further, patients may benefit from a more aggressive proximal landing zone with similar perioperative morbidity when zone 2 TEVAR is done with left subclavian artery revascularization, according to senior author Jean Panneton, MD, chief of vascular surgery at Eastern Virginia Medical School in Norfolk, Virginia. The study was recently published in the Journal of Vascular Surgery (JVS). “TEVAR for the treatment of complicated acute TBAD has been shown to have favorable outcomes compared to both open aortic repair and medical therapy,” he said. However, the optimal approach—including timing, coverage length and landing zone—has yet to be fully elucidated, he added. Panneton and colleagues performed a retrospective chart review, from a single center, of adult patients who underwent TEVAR for complicated acute TBAD within six weeks of diagnosis from January 2008–December 2018.
“The proximity of the primary tear to the origin of the left subclavian artery can make it difficult to achieve a secure 2cm landing zone of healthy aorta without coverage of one of the aortic arch branch vessels. Notably, 90% of our study patients had a less than 2cm proximal landing zone,” said Panneton. “Factors which may contribute to the better outcomes observed for the zone 2 patients may include a landing zone that is further away from the aortic pathology and is more optimal in terms of seal given it is less curved than in zone 3. Additionally, our low rate of retrograde dissection may be related to avoiding proximal endograft oversizing (>10%) and post-deployment balloon molding.” Many technical details must be considered to achieve excellent outcomes in this difficult patient population, said JVS editors.—Paul DiMuzio, MD
Vital signs
continued from page 1
expense-per-case, vascular surgery nursing labor expenses per-patient-day and total nursing expense per-relativevalue-unit (RVU), uncovering what lead author and Ochsner senior staff surgeon Clayton Brinster, MD, described as “a disturbing story of increasing total nursing expenses.” He pointed to a top line increase over the last nine months of 67% per month in total nursing expenses in the institution’s vascular surgery units. As most health systems operate at slim (0 to +3%) to negative net financial margins, “this is a staggering increase,” Brinster stated. The results were derived from seven cohorts corresponding to three-month periods dating to the start of the pandemic in March 2020 through November 2021, and compared with the 14-month period preceding the COVID-19 outbreak. The findings build on data, delivered a year ago, showing that the Ochsner vascular division recorded three-month sustained decreases in operative and outpatient clinical volume, as well as a “severe” financial loss, during the initial stages of the pandemic. Delivering the group’s findings at the 2022 Southern Association for Vascular Surgery (SAVS) annual meeting in Manalapan, Florida (Jan. 19–22), Brinster told attendees traditional determinants of surgical net revenue—such as total cases per month, RVU per month, and Centers for Medicare and Medicaid Services (CMS) case mix index—showed no significant difference when the post-COVID cohorts were compared with the pre-COVID era. Yet, he informed the gathering, they observed a “consistent erosion of vascular surgery margins,” despite consistencies in revenue generation. As the team delved deeper into the data, standardizing against a per-case basis, “we saw a
similarly disturbing trend, with an increase of about 75% per vascular surgery case—that’s the increase in nursing costs alone,” Brinster said. System-wide, nursing labor costs in 2021 increased about 200%, or $104 million more than the 2020 number, he noted. “Don’t forget, 2020 was a pandemic year with elevated nursing costs as well.”
Brinster and colleagues went further. The pandemic inevitably will lead to about 80 million Americans either becoming uninsured or seeing their health insurance status altered, resulting in shifts in the insurance payor mix and associated distribution, Brinster explained. This, in turn, directly impacts reimbursement, net revenue and profit margin, he said. “When we looked at our own vascular surgery payor mix, we saw some shifts during the course of the pandemic: the equivalent increase in the more profitable commercial payor is about +5% on average, and the more costly lowerreimbursing Medicaid payor is about +5%. This likely will offset, but just looking at +5 and +5 does not show the whole picture, so we wanted to take it a step further in terms of standardizing our clinical cost data.”
“When you consider that nurses incur a disproportionately high COVID exposure risk, that means subsequent quarantines and recoveries, requiring the use of mandatory sick time,” he said. “That then leads to decreased available labor, increased agency usage and increased costs.”
Summing up, Brinster said the pandemic had intensified “an evolving nursing labor crisis that has been going on for decades,” with the results from the Ochsner study demonstrating a “severe erosion of vascular surgery profit margin in the presence of dramatically escalating nursing labor costs, despite consistent revenue generation present throughout the pandemic.” Tackling the problem represents a mammoth task, he said. The government has taken action, pledging to invest $1.5 billion in an attempt to combat the nursing crisis. “The educational debt of over 22,000 nurses and nurses assistants will be absolved in exchange for a commitment to work in critically underserved areas affected by the pandemic.”
“Investments should really be focused on nursing education, training and recruitment—and established permanently”
Clayton Brinster
This led Brinster et al to scrutinize total nursing expense per RVU, which he described as “perhaps the most accurate standardized measure of variation of clinical expenses over time.”
In this analysis, they demonstrated “a dramatic 55% conglomerate increase” during the COVID era. The RVU dimension also served the purpose of making the data generalizable beyond Ochsner and capable of application across the country, he said. Overall, pandemic peaks in the COVID positivity rate in New Orleans was closely followed by spikes in nursing labor costs that were “almost proportional to the degree of positivity,” Brinster observed.
Elsewhere, Brinster said, the 2022 Medicare Physician Fee Schedule will support physician practices that rely very heavily on nursing support staff, medical assistants and other clinical staff covered by Medicare, with rates for registered nurses increasing by 67%.
Ultimately, the plans seem “stopgap”at both the national and individual health system levels, he argued. The longterm remedy requires institutional, state and national programs to alleviate the workforce and financial crises, Brinster said. “As we struggle to recover from the ongoing pandemic, investments should really be focused on nursing education, training and recruitment—and established permanently,” he concluded.
New data adds to body of evidence highlighting ‘importance’ of vascular surgery in trauma center setting
BY BRYAN KAY
Another study has emerged showing vascular surgery’s heavy intraoperative consult activity in a level 1 trauma center setting, lending further fuel to the “vascular firefighter” analogy.
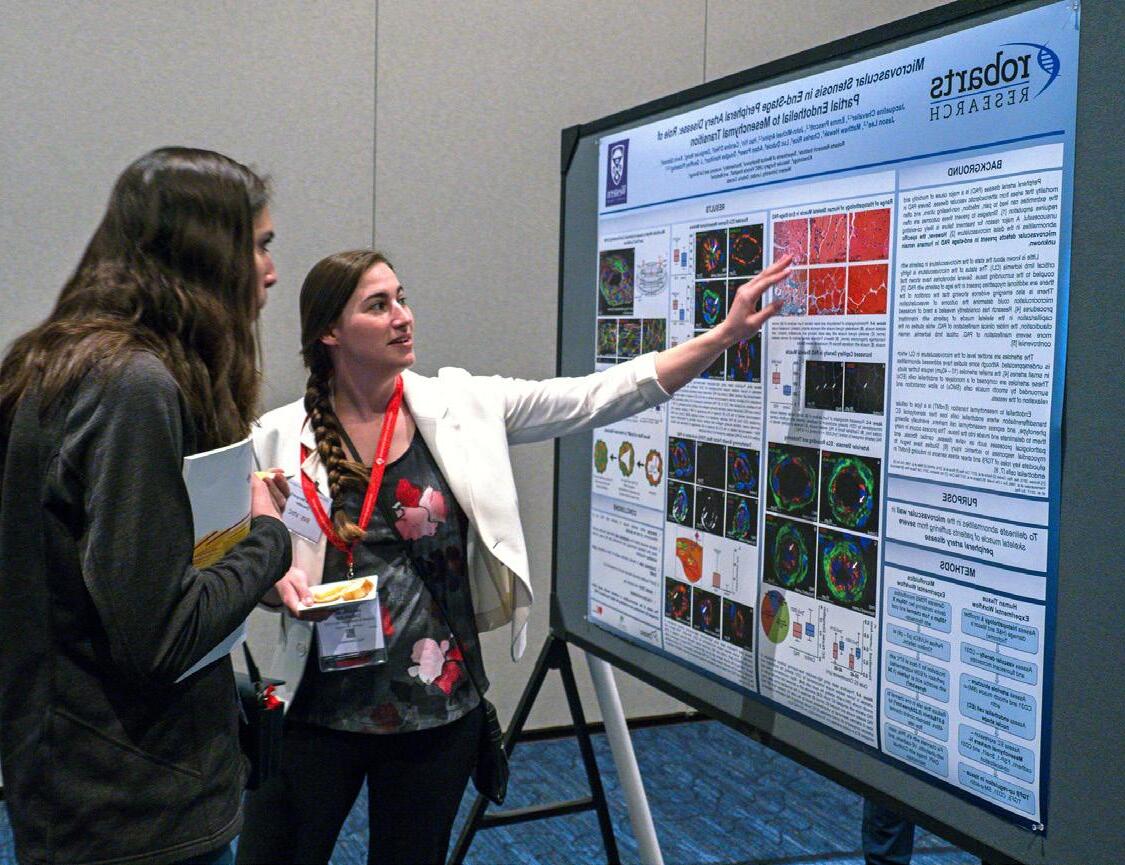
Aresearch team that included fourth-year medical student Abigail Hatcher, MS, of Emory University School of Medicine, Atlanta, and study lead Jaime BenarrochGampel, MD, assistant professor of vascular surgery, found that vascular surgery was consulted at a higher rate in both emergent and immediate operative trauma cases than any other surgical subspecialty at Atlanta’s Grady Hospital over a five-year period from 2015–2019.
Hatcher and colleagues noted that the retrospective analysis showed vascular consults ahead of orthopedic surgery and neurosurgery, both of which—unlike vascular surgery—are required in order for an institution to attain American College of Surgeons (ACS) level 1 trauma center certification.
Overall, vascular surgery was the only surgical group to see a statistically significant upward trend in intraoperative consultation over the period, whereas the other top surgical subspecialties did not experience any statistically significant change, Hatcher revealed. On multivariate analysis, she continued, “immediate trauma operations, younger patients, and those who presented with a severe injury severity score were independently associated with intraoperative vascular surgery consultation.”
The results were presented at the 2022 Southern Association for Vascular Surgery (SAVS) annual meeting in Manalapan, Florida (Jan. 19–22) by Hatcher, who told delegates the team hopes to expand the study by recruiting other level 1 trauma centers regionally and nationally in order to more broadly analyze consultation rates of surgical subspecialties. “We propose an assessment of the financial impact of vascular surgery’s contribution in trauma centers, and the adequacy of on-call coverage by vascular surgeons,” said Hatcher, who plans to enter general surgery residency on completion of her medical degree. “We recommend a reevaluation of not only ACS but regional and local guidelines and polices to reflect our findings and the importance of vascular surgery in the trauma setting.”
Study development
Speaking to Vascular Specialist after presenting the data, Hatcher and Benarroch-Gampel described how their coming together, mentee with mentor, got the research project rolling.
Hatcher’s background interest in healthcare policy and BenarrochGampel’s robust experience of vascular surgery’s need at the coalface of a level 1 trauma center seeded the endeavor.
“We work incredibly well with our trauma peers here, and we get along incredibly well, and I have seen how much we assist them when they need us,” explained Benarroch-Gampel.
“That brought us to the question: vascular surgeons in one of the busiest trauma hospitals in the nation, though we are pretty involved with them, how come we’re not what we call part of the table?
The ACS guidelines for level 1 trauma certification does not require vascular surgery—why not?”
That’s when the team decided they needed to compare vascular surgery’s trauma consult rate with the other surgical subspecialties. As they sifted through the data, they discovered that of 2,265 patients identified, 221 required vascular consultation, which compared with 507 across the other surgical subspecialties combined. Hatcher, Benarroch-Gampel and colleagues further found that in addition to vascular surgery recording the highest rate of intraoperative consultation overall, it also saw the highest rate among consultations on cases classed as “immediate,” or patients taken to the operating room in under 60 mins.
“Abigail did a really good job finding the data because after I saw what it told us, I said, ‘Wow, we actually come out with more than the required subspecialties in emergent cases,’” said Benarroch-Gampel. “And I call them emergent because if you have six hours to fix a problem, you can just send the patient somewhere. But if you have to fix the problem in hours, you better have the
way to fix the problem in hours.”
Armed with such evidence of vascular surgery’s import in the level 1 trauma setting, the researchers continue to mull over how best the certification anomaly might be rectified. “It takes buyin from not only other vascular surgeons and programs across the country— because this is a nationwide guideline that we’re addressing—but also the individual hospitals and the trauma teams that you’re assisting,” said Hatcher. “It’s not something that is going to happen overnight, but it is an appropriate change to start talking about and working towards.”
In the meantime, it is imperative that vascular surgery continue to provide a high level of assistance in trauma cases when called upon, Benarroch-Gampel said. There are signs of promise, added Hatcher, who noted major changes to the ACS guidelines in the past, suggesting further updates of this nature “are not out of the realm of possibilities.”
Important cog in healthcare wheel
The Society for Vascular Surgery (SVS) last year published a document chronicling the value of the modern vascular surgeon to the healthcare system. The report from the SVS Valuation Work Group highlighted the unique mix of medical, open surgical and endovascular skills vascular surgeons provide, along with the critical role they play in a safe operating room
Extent of vascular consults vs. other specialties in certain settings
- Immediate trauma operations: 65.6% vs. 38.1%
- Penetrating trauma cases: 73.3% vs. 47.9%
- Cases at night: 60.6% vs. 51.9%
environment. Benarroch-Gampel said the Atlanta studies represents yet another example that can be used to show how important vascular surgeons are to healthcare systems. “In many cases, we are called the firefighters,” he elaborated. “The value we provide should be highlighted. And the value we provide should be appreciated. Here, it is. We just need to be sure that nationwide this is something where people understand what vascular surgeons provide.”
Benarroch-Gampel said his group previously published data showing that they had seen a rise in their vascular trauma workload—from about 12% to nearly 80%—with good results. “As a society, we need to support that; we need to show that in the vascular trauma field, we are providing a good job compared to other specialties.”
The sresearch team’s attention now turns to getting their latest data published, but Hatcher disclosed that the SAVS meeting room has already yielded interest from senior vascular surgeons about chipping in with data from their own institutions. “They said, ‘We would love to offer our data over the same time period, or a similar time period,’ to see if this is something that they think they’re already experiencing, but they also want to prove, and contribute to a wider dataset.” For Benarroch-Gampel, the question beckons: Are these results isolated to the Atlanta data, or are they occurring across the country? “I personally believe this is nationwide, and not just in one place,” he said. “This is one of the busiest places, with one of the most well-trained trauma surgeon teams, and we still come in and assist when needed.”
Abigail Hatcher Jamie BenarrochGampel
Sex discordance and postoperative outcomes:
We should be vigilant of a real disparity
BY KAREN WOO, MD
in health outcomes
The recent JAMA Surgery publication “Association of surgeon-patient sex concordance with postoperative outcomes” is a population-based, retrospective cohort study of more than 1 million patients that concluded “sex discordance between surgeons and patients negatively affected outcomes following common procedures.”1 Furthermore, the finding is driven by “worse outcomes among female patients treated by male surgeons.”
My initial reaction upon reading these conclusions was: “How can this be possible?”
The scientist in me was certain I could find something(s) in the methodology that could easily explain how they got these seemingly outrageous findings. Thus, I set off to meticulously review the article.
The authors used the Ontario Health Insurance Plan database, derived from the single government payer for Ontario, Canada. The strength of this dataset is that it is representative of the population of Ontario, more so than most administrative databases available in the U.S., such as Medicare claims, which all have some limitation in the population captured. The authors linked the database to four other databases that provided follow-up data for hospitalizations, emergency department visits, patient demographic information and surgeon level data. This looked like about as strong a dataset as you could get in the world of “big data.”
The investigators then imposed a number of inclusion criteria that I won’t bore you with. Suffice it to say, I was satisfied that they carefully considered situations that could represent data entry errors (e.g. date of death preceded date of surgery) or could skew the data (e.g. multiple surgical procedures in the same day and sex-specific procedures). These cases were excluded, leaving the authors with 1,320,108 unique patients—an impressive sample size.
Well, what about the statistical methods? I thought surely I could find something to pick apart there. The methods described in detail the sophisticated statistics used (multivariable generalized estimating equation with an independent correlation structure and clustering on the procedure performed). The investigators appeared to have accounted for all the covariates and potential confounders they could in their statistical modeling with the available data. I found myself commending the authors for their appropriate, rigorous and robust statistical approach.
“Big data” analyses such as this are often criticized for being “fishing expeditions,” where the investigators do not start out with a hypothesis
and then perform hundreds of comparisons looking for anything that might be statistically significant and then assign it meaning. Wallis and colleagues were careful to indicate throughout the manuscript that this was not a “fishing expedition.” They presented the preliminary data to support their explicitly stated hypothesis which was that “sex discordance between surgeons and patients may contribute to differences in postoperative outcomes, with worse outcomes in female patients treated by male surgeons.” They carefully outlined the “pre-planned” stratified and subgroup analyses in the methods.
The primary outcome was a composite of death, readmission or major complication (e.g. acute renal failure, stroke, myocardial infarction) within 30 days
‘Big data’ analyses such as this are often criticized for being ‘fishing expeditions’
after surgery. The composite outcome rate was 14.9%. Sex discordance between patient and surgeon was independently associated with a 7% increase in the likelihood of the primary outcome. Analyses stratified by physician, patient and hospital factors demonstrated that this effect largely persisted in the stratified analyses. Further, among female patients, those treated by a male surgeon were 15% more likely to experience the primary outcome compared to those treated by a female surgeon. In contrast, among male patients, those treated by a female surgeon were no more likely to experience the primary outcome compared to those treated by a male surgeon.
Poking holes in the way the study was executed was proving to be difficult. Certainly, the study suffered from the limitations that are inherent to all administrative data studies, namely lack of granularity, which in this case, as the authors acknowledge, included the inability to distinguish between sex and gender.
The authors also
Karen Woo
acknowledged that case complexity could contribute to the findings if male surgeons perform more highrisk cases. The authors did perform an analysis of low- vs high-risk cases, and found that the association of discordance with the primary outcome was robust to this analysis. However, low-risk was defined as appendectomy, cholecystectomy and carpal tunnel release. All other operations were defined as high-risk. Relevant to vascular surgery, femoropopliteal bypass and abdominal aortic aneurysm (AAA) repair were categorized as high risk. Clearly, within each of those operations, there are complexities such as redo bypass, or short angulated AAA neck, that cannot be captured by administrative data.
Nevertheless, my mind shifted to thinking, “Maybe they have something here.” The only thing these kinds of “big data” analyses can do is demonstrate an association. It is simply not possible to prove causality using a retrospective cohort study design. In a retrospective study, it is entirely possible for two variables to be associated with each other without one causing the other. That said, the investigators did a good enough job with this study for me to believe the observed association in this dataset was real. The obvious next question was “What is the underlying cause?” The authors speculated in the discussion that these findings may be a result of the way sex discordance between surgeon and patient may “adversely affect the physician-patient relationship.” There are abundant data, although largely in medical specialties, to demonstrate that the physician-patient relationship and communication can influence long-term health outcomes.2,3
This study generated a wide range of reactions on social media, with everything from “Of course women surgeons do a better job than men” to “This study is a lie.” Once we’ve processed our visceral reactions, as clinicians that prioritize our patients’ well-being above all else, we should be concerned that these results may represent a real disparity in health outcomes. The data scientists among us can and should do more work to investigate whether this association holds true in other populations. However, as surgeons, and even data scientists, we are poorly trained and poorly equipped to properly investigate whether the patient-surgeon relationship is the driver of these findings. We need to partner with those who have appropriate expertise, such as sociologists, to rigorously study this issue. In the meantime, this study reminds us that what all of us can do now, regardless of whether the findings are valid, is strive to treat each of our patients equally with the utmost compassion, respect, and diligence.
Study highlights
Christopher J. D. Wallis, MD, an assistant professor of urology at the University of Toronto in Canada, and colleagues found that sex discordance between the patient population and the 2,937 surgeons in the study was associated with “a small but statistically significant increased likelihood of adverse postoperative outcomes.” This, the authors noted, “was driven by worse outcomes for female patients treated by male physicians without a corresponding association among male patients treated by female physicians.”
References
1. Wallis CJD, Jerath A, Coburn N, et al. Association of surgeon-patient sex concordance with postoperative outcomes. JAMA Surgery. 2021;doi:10.1001/ jamasurg.2021.6339.
2. Coelho KR, Galan C. Physician cross-cultural nonverbal communication skills, patient satisfaction and health outcomes in the physician-patient relationship. International Journal of Family Medicine. 2012;2012.
3. Street RL, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician–patient communication to health outcomes. Patient Education and Counseling. 2009/03/01/ 2009;74(3):295–301. doi:https://doi.org/10.1016/j.pec.2008.11.015.
KAREN WOO is associate professor of surgery at the University of California, Los Angeles (UCLA). She is also associate director of the Vascular Low Frequency Disease Consortium.
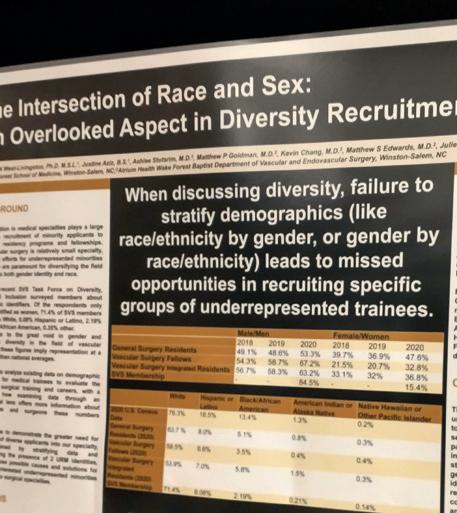
Trainee pipeline: ‘Recruiting more women without knowing the race/ ethnicity of those women only tells part of the story’
Failure to stratify gender by race or ethnicity, or vice versa, leads to missed opportunities in the recruitment of underrepresented members of the potential vascular surgery trainee pool.
THAT WAS ONE OF THE messages delivered in a poster presentation at the Southern Association for Vascular Surgery (SAVS) annual meeting in Manalapan, Florida (Jan. 19–22). Among integrated vascular surgery residents in the U.S. and Canada in 2020, 63.2% identified as male, 53.9% as white, 7% Hispanic, 5.8% Black, 1.5% American Indian or Alaska Native, and 0.3% Native Hawaiian or other Pacific Islander, according to a research team that included first author Lauren N. West Livingston, PhD, and senior author Gabriela A. Velazquez, MD, of Wake Forest School of Medicine in Winston-Salem, North Carolina. Similarly, the analysis found that among vascular surgery fellows, 67.2% were male, 59.5% were white, 6.6% Hispanic, 3.5% Black, 0.4% American Indian or Alaska native, and 0.4% Native
Diversity
dos and don’ts:
Hawaiian or other Pacific Islander. Livingston and colleagues used data drawn from the Association of American Medical Colleges compared with data on the sex/gender and race/ ethnicity of practicing vascular surgeons.
The researchers said the analysis demonstrated that minorities continued to be underrepresented in medicine but that the data were limited by training paradigm and did not examine results with an “intersectional lens.”
Analyzing the data in this way, they said, would have allowed further stratification of the figures by combination of race and gender, or the subgroups within certain racial/ethnic identities. “For example, recruiting more women without knowing the race/ethnicity of those women only tells part of the story,” the investigators said.—Bryan Kay
Academic writing in the DEI space
BY JOCELYN HUDSON AND AARON KUDHAIL
It’s been almost 18 months since the Journal of Vascular Surgery (JVS) implemented changes aimed in part at diversifying involvement with the publication and addressing how papers on social determinants of health are written and reviewed.
Part of that process was the recruitment of a diversity editor. With more than a year under her belt in the role, Ulka Sachdev-Ost, MD, sat down with Vascular Specialist for a video interview during which she outlined milestones reached and how the journey has evolved so far.
She also had some tips for authors looking to write and report better academic papers in the arena of diversity, equity and inclusion (DEI) and healthcare disparities for publication in JVS and beyond.
Copious resources exist, she said, not least from Elsevier, the publisher of JVS, which has produced webinars covering
Atherectomy use during index intervention for claudication ‘is associated with higher’ reintervention rates vs. other technologies
Atherectomy use during index peripheral vascular interventions in claudicants is associated with higher reintervention rates when compared to other technologies, a newly unveiled study by Caitlin Hicks, MD, et al at Johns Hopkins Hospital in Baltimore, Maryland, shows.
intervention compared to “first quartile” atherectomy users—with those in quartiles 1–3 being termed “inlier” physicians and those in quartile 4 “outliers.”
DEI-related academic writing, and she encouraged authors to make full use of them. Further guidelines are planned by the JVS team on how to report on sex and gender, and social determinants of health, Sachdev-Ost added.
“These can help authors navigate some of the wording when you’re going to talk about women vs. females, and how to make that distinction in research, because it’s different when you’re talking about humans vs. whether you’re talking about animal research; how to incorporate socioeconomic and racial differences in your reporting, and what might be some of the best ways to make sure some of the appropriate stakeholders are included, or at least addressed in the correct way in the research,” she explained.
Look out for the full video interview with Ulka Sachdev-Ost at vascularspecialistonline.com.
“These can help authors navigate some of the wording when you’re going to talk about women vs. females”
Ulka Sachdev-Ost
The researchers found that 48.9% of those who received an index atherectomy procedure later underwent reintervention, but just 29.8% of patients who did not undergo atherectomy did so. Some 59.7% of the study group—drawn from 2019 Medicare data on more than 15,000 patients intervened upon for claudication—received index atherectomy, with the patient pool followed through June 2021. Comparing reintervention between groups stratified by index procedure, Hicks et al revealed that 85.7% of patients undergoing a first-known intervention with atherectomy also received a reintervention using the same procedure. This compared with just 30.9% among those whose initial intervention was carried out using a different technology. The data were delivered by Qinqwen Kawaji, MD, a general surgery resident, at the 2022 Southern Association for Vascular Surgery (SAVS) annual meeting in Manalapan, Florida (Jan. 19–22).
Compared to vascular surgeons, cardiologists, radiologists, CT surgeons and those from other specialties were also associated with higher risk for reintervention, the research team said. Other significant physician characteristics included male sex and high volume peripheral vascular intervention practice, Kawaji added. “Previously, physicians working at OBLs [office-based labs] have come under scrutiny for atherectomy use. In our adjusted model, we did not find an association between site of service and reintervention.”
Reintervention: atherectomy vs. non-atherectomy
Probing physician side characteristics, the research team also found the estimated 2.5-year cumulative incidence for firsttime reintervention was 60% among practitioners deemed high atherectomy users vs. 42.4% in those found to be standard atherectomy users (p<0.001).
After adjusting for all patient characteristics, atherectomy continued to be associated with a 33% higher risk for reintervention, Kawaji told SAVS attendees. “Other characteristics associated with reintervention include Black race, diabetes and urban residence,” she said.
Meanwhile, patients treated initially by high atherectomy user physicians were associated with a 49% increased risk for
Kawaji concluded: “Index femoropopliteal atherectomy for claudication is associated with high reintervention rates, and high atherectomy physician users and nonvascular surgeons perform more peripheral vascular reinterventions than their peers. Because of the limitations of our study, we were unable to elucidate whether or not the high reintervention rates were related to atherectomy device failure or physician practice patterns. Our study suggests that appropriateness for atherectomy use in initial peripheral vascular reintervention for claudication needs critical reevaluation.”
The analysis builds on previous findings by Hicks and colleagues in recent years. Last year, her group reported on a study of physician practice patterns using the same Medicare dataset in which they found that some 420 physicians, or 25.8%, performed atherectomy in 87.5%-plus of their index femoropopliteal disease intervention cases. Another 133 physicians (8.2%) performed atherectomy in 100% of their cases. They also demonstrated that high users of atherectomy were more frequently cardiologists or radiologists, and less frequently vascular surgeons.—Bryan Kay
Medtronic recalls HawkOne
Medtronic has recalled 95,110 HawkOne directional atherectomy system devices distributed in the United States between Jan. 22, 2018, and Oct. 4, 2021, the Food and Drug Administration (FDA) has announced.
The FDA has identified the recall as Class I—the most serious type. So far, there have been 163 complaints, 55 injuries and no deaths reported in relation to the device issue, the FDA reported. HawkOne consists of a catheter and cutter driver, and is used during procedures intended to remove blockage from peripheral arteries. The recall was made “due to the risk of the guidewire within the catheter moving downward or prolapsing when force is applied during use,” according to the FDA.—Bryan Kay
Combating the problem of spin, or overinterpretation, in RCTs
BY BRYAN KAY
The presence of spin, or overinterpretation, in scientific papers that ultimately demonstrate statistically insignificant findings had been gnawing away at Thomas Forbes, MD, for quite some time.
THE PRACTICE, THE UNIVERSITY OF TORONTO vascular chair reflects, is by no means unique to vascular surgery but would often spring to the forefront of his mind as he pored over randomized controlled trials (RCTs) comparing endovascular aneurysm repair (EVAR) to open repair, and carotid stenting to endarterectomy (CEA).
In the case of EVAR vs. open repair, he recalls, he would see trial researchers with nonsignificant studies declare the former “no better” than the latter. “So, the new kid on the block is no better than the gold standard,” he says. “By saying no better, that has a negative connotation.” On the other hand, he would see authors involved with carotid stenting trials write that the new kid on the block—in this case, stenting—was “just as good as” the gold-standard CEA. “Whereas,” Forbes says, “statistically there was no
medical students and a cardiothoracic resident, he set about probing its extent in an analysis of abdominal aortic aneurysm (AAA) and carotid stenosis RCTs.
What they found was that a large proportion of statistically nonsignificant RCTs yielded interpretations that were inconsistent with their results, disseminating them in a poster presentation at the 2022 Vascular Annual Meeting (VAM) in San Diego and again at last year’s annual meeting of the Canadian Society for Vascular Surgery (CSVS). They identified spin in nine abstracts and 13 main texts among 18 AAA articles, and seven abstracts and 10 main texts across 13 carotid stenosis studies. In reality, Forbes says, whether findings have a positive or negative connotation should be left to the interpretation of the reader. “As a reader, I should say, ‘With the new treatment, should I be disappointed that it is no better, or should I be happy that it’s just as good?’”
In their analysis, the researchers also looked at whether overinterpretation might be related to the publishing journal’s impact factor, the source of trial funding, and where exactly in the paper the spin occurred. No significant association was detected in terms of funding source, and increasing journal impact
“Try not to become a salesman for your science. Let it speak for itself” Thomas Forbes
factor was associated with a statistically significant lower likelihood of spin in the study title or abstract conclusion, the team reported. As for location, overinterpretation was “very common” in discussion sections, says Forbes. “But I think, more importantly, it was also quite prevalent in the titles as well as the abstract conclusions. Why I say that’s very important is I think readers of the scientific literature are deluged with massive amounts of information. And I’m sure most of us, if we’re honest, in our everyday practice, there’s very few papers that we read from front to back. There’s maybe a bit more where we actually read the entire abstract, and there’s maybe a bit more where we actually just read the conclusion of the abstract. So, spin, or overinterpretation of findings, in abstract conclusions and in titles has much more impact than the spin that occurs buried in the paper.”
It is incumbent on peer reviewers and editors to hold authors accountable for their wording so that overreach does not occur. “As an associate editor of the Journal of Vascular Surgery myself, that’s one of the big things that we go back and say to the authors,” Forbes explains. “We say, ‘Look, you had a negative finding. Don’t give that negative or positive connotation. Just say you were unable to find a change.’” Words matter, Forbes points out.
“Try not to become a salesman for your science. Let it speak for itself.”
Thomas Forbes
Novel use of TCAR to treat complex brachiocephalic disease shown to be effective, researchers report
BY BRYAN KAY
A “unique” case series of patients undergoing transcarotid artery revascularization (TCAR) in which the system was put to novel use for proximal intervention or incorporated in a hybrid approach to complex brachiocephalic disease demonstrated it to be effective in “providing safe, comprehensive treatment solutions,” the 2022 Vascular and Endovascular Surgery Society (VESS) winter annual meeting (Jan. 27–29) in Snowmass, Colorado, heard.
VIRAJ PANDIT, MBBS, DELIVERED the findings on behalf of a University of Oklahoma (OU), Tulsa, team of researchers led by vascular chief Peter R. Nelson, MD, informing delegates that a total of 94 patients underwent TCAR, with 8.5% (n=10) undergoing combined procedures. They found that two patients
VAM 2022: More science, discussion, streaming
BY BETH BALES
had concomitant common carotid artery stenosis, four patients had subclavian artery stenosis and one had an occluded contralateral internal carotid artery. None in the combined group had postoperative complications—stroke, myocardial infarction or cranial nerve injury—and all were discharged home on postoperative
With abstract selection finished this month and the lineup of many other sessions in place, organizers are excited about the offerings of the 2022 Vascular Annual Meeting (VAM).
VAM 2022 will be held June 15–18 at the Hynes Convention Center in Boston. Educational programming will be held all four days and exhibits will be open June 16–17. The Society for Vascular Surgery (SVS) Foundation “Cheers to 75 Years” Gala, celebrating the Society’s 75 years of treating patients with vascular disease, will be June 17. Registration and housing are expected to open in earlyto mid-March.
Andres Schanzer, MD, chairs the SVS Program Committee, which oversees overall VAM programming. He offered several innovations for the 2022 meeting, most made in response to participant feedback of previous iterations of VAM.
VAM 2022 will include two additional podium-based plenary sessions, and eight overall. “This allows us to offer more science in the program and the opportunity to highlight more of our talented investigators,” said Schanzer.
There will be more discussion. This is a change based on overwhelming feedback from members who find the discussion period following abstract presentations very valuable, said Schanzer. Thus, the discussion period for
day one, Pandit added. TCAR experience is expanding for the treatment internal carotid artery stenosis, but its applicability in patients with more complex brachiocephalic disease has not been described, the researchers reasoned as they set out to analyze the series.
Viraj Pandit
In that vein, they explored their experience with TCAR used in combination with other cerebrovascular interventions, including retrograde common carotid artery stenting and carotid-subclavian bypass. “This unique case series of patients undergoing TCAR in association with other cerebrovascular interventions demonstrated successful outcomes,” Pandit—formerly a vascular surgery fellow at OU Health and now a surgeon with VA in Fresno, California, and colleagues concluded.
Speaking to Vascular Specialist, senior author Nelson elaborated: “This paper probably falls between a traditional patient series and a technical note. Compared to traditional literature, this approach seems applicable to the new technology. It doesn’t require endarterectomy to accomplish the
same combination of treatment. We can do it through the less invasive approach of a TCAR. The technical aspects are more or less how to maneuver the delivery system and how to engage the flow protection system that we’ve come to adopt with TCAR.” Some of that older literature “suggests that doing tandem lesions had
“This is obviously a small number of patients, but we’ve seen no increase in complications and arguably similar or less complications in this small group”
Peter R. Nelson
increased complication rates—and we’ve not seen that,” Nelson explained. “This is obviously a small number of patients, but we’ve seen no increase in complications and arguably similar or less complications in this small group,” he added.
the three-minute rapid-paced presentations has been extended from three to four minutes. “We hope this will allow for even richer discussion and exchange of ideas,” he added.
Two sessions will offer innovative formats, including visual abstracts and content shaped by social media as opposed to more standard didactic presentations followed by questions and answers.
“Members told us that livestreaming in 2021 was really valuable for those who couldn’t attend VAM in person so we have added more,” said Schanzer. “For 2022, we will again offer livestreaming of the morning sessions, which generally are plenaries, and we have added one full afternoon track on each day. We will also be livestreaming all of the international sessions in order to reach those who are unable to travel from abroad.”
"This will be a great opportunity to get back together, enjoy each other’s company and also support the important mission of the SVS Foundation” Andres Schanzer
SVS
Recording practices are being altered this year; Schanzer said the goal is to have all content available to VAM registrants rapidly. “We are shooting for an aspirational goal of having all video content of all presentations available on Monday, June 20, 48 hours after close of the meeting,” he said.
SVS members have been celebrating the Society’s creation in 1946 since the 2021 VAM in San Diego. Festivities will culminate in the SVS Foundation Gala on the evening of Friday, June 17.
“We hoping it’s going to be the biggest and best VAM we’ve ever had,” Schanzer added.
For more information about VAM, including the meetings and conferences of the Vascular Quality Initiative and the Society for Vascular Nursing, visit vascular.org/VAM.
President Ali AbuRahma speaks during VAM 2021 in San Diego
VAM 2022 will offer innovative formats
BY BETH BALES
The Society for Vascular Surgery (SVS) Postgraduate Education Committee is breaking up the format in favor of change and innovation for two sessions at this year’s Vascular Annual Meeting (VAM). These in-person-only events will involve both networking and social media.
Endovation: Endovascular Innovation for Urgent and Emergency Complex Aortic Disorders, 3–4:30 p.m., Wednesday, June 15
With “Endovation,” this concurrent session gets into the spirit of innovation, as its title suggests. It will bring together experts in “creative but understudied techniques” for complex aortic repair to discuss drawbacks, regulatory issues and best practices for those who are either considering or currently performing, off-label techniques in urgent and emergency settings.
“Endovation” starts with didactic podium presentations on various facets of the repairs, pre-recorded video
presentations of challenging aortic cases involving nontraditional surgical solutions, and a panel discussion.
The audience will be part of the conversation for discussion of the challenging cases. “Cases Under the Stars” encourages mingling and vascular conversation in a reception-type setting with light refreshments and beverages. Organizers may turn to social media to solicit the case-based content.
JVS Special Session, 1:30–2:30 p.m., Thursday, June 16
This special session highlighting the Journal of Vascular Surgery (JVS) publications will be an Audible Bleeding podcast using ESPN’s “Pardon the Interruption” program format.
As envisioned, panelists will cover a handful of provocative, entertaining topics. JVS editors will work with the SVS Social Media Subcommittee to solicit, via social media, interesting questions and topic ideas in advance of VAM. Audience involvement is key, said Paul DiMuzio, MD, assistant editor for social media for all JVS publications. He likened the informal give-and-take to “discussion around a workplace water cooler.”
The audience has the chance to pose any question they wish to those involved with the Journal of Vascular Surgery, at all levels of involvement in the publication process, DiMuzio said. Topics will be sought fairly close to the meeting itself, to ensure “the questions will be fresh
75th anniversary Gala tickets go on sale on Feb. 22
How will you help the Society for Vascular Surgery (SVS) celebrate “Cheers to 75 Years?”
MAYBE IT’S OFFERING AN ADVENTURE IN THE wilderness, on a mountain or secluded location. Perhaps it’s providing the chance to stay in a house by the ocean or obtain a case of high-end wines put together by a connoisseur.
The committee overseeing this year’s SVS Foundation Gala, “Cheers to 75 Years,” is seeking contributions for both the live and silent auctions that are a big part of the fun during the Gala.
This year’s Gala, to be held Friday, June 17, during the 2022 Vascular Annual Meeting (VAM) celebrates the 75th anniversary of the founding of SVS in 1946. The celebration began in San Diego during the 2021 VAM and will end with the last tune spun by the DJ in June.
and topical,” said session organizer Gale Tang, MD. For example, in terms of diversity, equity and inclusion (DEI) issues, a member could seek to ask how the “be careful what you post in social media” article of 2020—which prompted a firestorm of criticism and plenty of social media posts of female doctors in swim attire—could possibly have made it through the review process.
Another member may want an answer as to whether published papers are even relevant in the era of social media/YouTube videos and sound bites.
The session will include a podcast with Imani McElroy, MD, one of Audible Bleeding’s regular personnel as a comoderator. It also will feature a short interview with Peter Gloviczki, MD, JVS editor-in-chief, while Peter Lawrence, MD, senior editor, will be on the panel answering questions. Gloviczki and Lawrence are completing their five-year terms at the head of the JVS publications.
Tang hopes participants will come away with “a better idea of what is involved with putting together the premier vascular surgery journal and how they can get involved with JVS at any career level.”
VAM takes place June 15–18, at the Hynes Convention Center in Boston. Registration and housing opens early to mid-March; educational offerings and plenary sessions take place across all four days; and exhibits are open June 16–17. Meanwhile, the SVS Foundation “Cheers to 75 Years” Gala is June 17.
Visit vascular.org/VAM for more information.
awareness programs and patient education efforts, among other initiatives. Dress is semi-formal, with black-tie attire optional. Everyone, no matter where in the world they are on June 17 can participate in the Silent Auction. All they need is an internet connection to be able to view the items and to place a bid. Notifications will even let participants know when someone has upped the ante on a particular offering. Bidding for Silent Auction items will open several days before the Gala itself.
The 2019 “Vascular Spectacular Gala” in National Harbor, Maryland, was a huge hit. Tickets sold out within weeks and guests enjoyed dinner, entertainment and spirited bidding, and then danced the night away.
“You know how we surgeons are,” said Ronald Dalman, MD, Gala Committee chair. “If they’re not competing with each other to put together the most elaborative and imaginative adventure possible, they’re preparing for the competition to outbid each other. We expect some great items to be offered.”
Festivities begin at 6:30 p.m. at the Sheraton Boston Hotel, the VAM headquarters hotel. The evening starts with a reception, followed by dinner, entertainment, the live auction, raise the paddle event and dancing. Tickets—sales open Feb. 22—are $500 each or $5,000 for a table of 10. VIP tables and sponsorship packages are available now for purchase at vascular.org/Gala22Tickets.
All proceeds will benefit the SVS Foundation, to fund ongoing research into the causes and treatments of vascular disease, public
Venita Chandra, MD, and Matthew Eagleton, MD, are the Gala Committee cochairs.
While all contributions are welcome, the sub-committee handling ticket sales and auction items is particularly interested in sporting events and skyboxes, sports memorabilia, travel and timeshares, food, entertainment, wine and high-end liquors, artwork, activities such as golf, chef classes, jewelry and educational experiences.
Beth Bales
To donate, email Catherine Lampi at SVSFoundation@vascularsociety. org. For information on the gala visit vascular.org/Gala22Tickets.
GALA AT A GLANCE
n SVS Foundation “Cheers to 75 Years” Gala
n 6:30 p.m. Friday, June 17
n Sheraton Boston Hotel Grand Ballroom (the VAM 2022 Headquarters Hotel)
n Reception, which will be followed by dinner, entertainment, live auction and dancing
n Tickets: $500 each or $5,000 for a table for 10
n Ticket availability: Beginning Feb. 22
n Information and tickets: Vascular.org/ Gala22Tickets; you cab also scan the QR code below
n Email: SVSFoundation@ vascular.org
SVS PAC: A voice for vascular surgeons on Capitol Hill
BY SHAHRAM AARABI, MD, YAZAN DUWAYRI, MD
As everyone turned the page on 2021 and entered 2022 with a new hope for a return to normalcy, vascular surgeons continue to be at the forefront of the fight to combat the COVID-19 pandemic.
OUR DAYS, AND NIGHTS, ARE taxing as we handle the challenging vascular manifestations of COVID-19, the life- and limb-threatening consequences of delayed medical care for chronic vascular conditions, the limited hospital bed capacity and the healthcare workforce shortages.
The resulting burnout, diminishing financial reimbursements and sluggish growth in the vascular surgery workforce necessitate a further push for vascular surgery’s seat at the legislative table as healthcare policies are developed that impact our patients and us.
In 2021, the Society for Vascular Surgery
n Advocacy for relief from regulatory burdens such as prior authorization
n Awareness about physician wellness issues
n Resolution of workforce attrition issues
Overall, the SVS PAC continues to grow in a positive direction, with 254 unique members (6% of the SVS membership).
Despite this growth, the SVS PAC lags other specialty societies in the amount and percentage of contributing members—a crucial metric to open the doors for our advocacy efforts in Congress. The SVS PAC aims to increase the percentage to 10% of the SVS membership as unique members of the PAC by the end of this election
physician payment cuts including a delay in resuming the 2% Medicare sequester for three months (Jan. 1–March 31), followed by a reduction to 1% for three
Time to pay 2022 dues
Members, have any of you perhaps missed your most recent issue of the Journal of Vascular Surgery (JVS)?
If so, it could be because your 2022 Society for Vascular Surgery (SVS) dues have not yet been paid up.
As of Dec. 31, 2021, members with unpaid dues are no longer considered in good standing and thus unable to receive benefits such as a free or heavily discounted subscription to JVS Membership suspensions and loss of all remaining benefits will begin in midFebruary.
Enjoy all the benefits that SVS membership has to offer and remit those 2022 dues today.
– Beth Bales
To register, visit vascular.org/Invoices.
any additional PAY-GO cuts through 2022; and a one-year increase over the Conversion Factor of 3% (0.75% less than the expired conversion factor “patch” provided for 2021). However, the clinical labor update went into effect on Jan. 1, as year one of four.
These Medicare reimbursement results represent partial success of tremendous advocacy efforts, by the SVS PAC and other healthcare organizations. But, we still need your help as we continue to work on the clinical labor updates and its impact on office-based vascular surgery procedures.
Congress must hear your voice and the SVS PAC needs your continued support to do so. Please continue to contact your elected representatives and to contribute to the SVS PAC for 2022.
Vascular surgeons deserve representation equal to our role in the fight for a healthier society.
Shahram Aarabi
Yazan Duwayri
Office-based laboratory setting proves 'safe' for iliac vein stenting
A retrospective study of 1,223 iliac vein cases performed in three office-based laboratories (OBLs) demonstrated a major complication rate of 0.41%, suggesting these procedures are safe and well-tolerated in this setting, the authors say.
ACCORDING TO CORRESPONDING
researcher Levan Sulakvelidze, BS, from the Center for Vascular Medicine in Greenbelt, Maryland, “Because OBLs are not regulated to the same degree as inpatient facilities or ambulatory centers, questions have been raised regarding patient safety and outcomes in this environment.
“The safety profile of iliac vein stenting in the OBL setting has not been thoroughly evaluated. The purpose of
the present study was to evaluate the complication rate and safety profile of this procedure when performed in an OBL.”
As reported in the January 2022 issue of the Journal of Vascular Surgery: Venous and Lymphatic Disorders, Sulakvelidze, senior author Peter Pappas, MD, part of the leadership at the Center for Vascular Medicine, and colleagues reviewed prospectively collected data from
FDA issues guidance documents for including patient perspectives in medical device studies
The Food and Drug Administration (FDA) has issued two final guidances providing recommendations for including patient perspectives in medical device clinical studies.
AS PER AN FDA PRESS RELEASE, THE finalized version of the first of these two guidance documents, entitled “Patient Engagement in the Design and Conduct of Medical Device Clinical Studies,” features key points including:
n Describing how device developers, sponsors and industry can voluntarily use patient engagement to improve clinical study design and conduct
n Providing examples of approaches to consider when device developers, sponsors and industry wish to incorporate patient advisor input in clinical studies
n Describing which patient engagement activities are generally not considered by the FDA to constitute an activity subject to the FDA’s regulations regarding Institutional Review Boards (IRBs)
n Clarifying how sponsors can receive feedback from the FDA on plans to voluntarily include patient advisors’ input on their clinical study through the Q-submission process
The second of these two newly issued guidances, entitled “Principles for selecting, developing, modifying, and adapting patient-reported outcome instruments for use in medical device evaluation,” intends to describe principles that may be considered for instruments that capture and measure patient-reported outcomes; provide recommendations about the importance of ensuring these instruments are fit-for-purpose; and outline best practices for selecting, developing, modifying, or adapting a patient-reported outcome instrument for use in medical device evaluation.—Jamie Bell
1,104 patients who underwent a total of 1,223 iliac vein stents in OBL centers. Three patient groups were studied based on presentation: lower-extremity symptoms (305), pelvic symptoms (91) and, a combination of the two (827).
Trained nursing personnel, under the supervision of the attending interventionalist, administered conscious sedation to all patients. Typical dosing involved midazolam (1mg) and fentanyl (50µg). Excluded from this setting were patients with significant cardiac/ pulmonary risk, history of severe airway issues, morbid obesity and complex venous lesions (e.g., inferior vena cava [IVC] obstruction).
There were no mortalities and no complications related to the sedation rendered. The total complication rate was 7.8%, including five major complications (0.4%) and 90 minor complications.
Sulakvelidze comments: “In the study, because most of the complications were considered minor, including suspected over-
VRIC input in 2021 helped strengthen research, says award-winner
BY BETH BALES
THE SOCIETY FOR VASCULAR
Surgery (SVS) Vascular Research Initiatives Conference (VRIC) in 2021 helped Sriganesh (Sri) Sharma, MD, better understand his own work.
During the free-wheeling discussion following his presentation, “I got a lot of meaningful input into my research,” he said. “I was introduced to perspectives of my own research that I hadn’t thought of before.”
Under the mentorship of Andrea Obi, MD, at the University of Michigan, Sharma studied the intersection of inflammation and coagulation as it pertains to COVID-19 patients, with a goal of creating a therapy that would protect COVID-positive patients from blood clots. The timing was fortuitous; Sharma joined Obi’s lab with an interest in immunology, including the immunology of blood-clotting.
“The pandemic had just started,” he said. “It seemed like a very compelling question without many answers.”
The abstract on his research was not only selected for presentation at VRIC 2021 (held during the 2021 Vascular Annual Meeting) it also was judged as one of the top four among trainees, earning him and three researchers the SVS
reported hematomas, we have presented strong evidence that demonstrates iliac stenting performed in the OBL setting is safe. Given these promising results, we recommend all OBLs become Joint Commission [formerly the Joint Commission on Accreditation of Health Care Organizations, or JCAHO]-certified and include quality assurance efforts to maximize patient safety.”—Bryan Kay
“Because OBLs are not regulated to the same degree as in-patient facilities or ambulatory centers, questions have been raised regarding patient safety and outcomes in this environment”
Levan Sulakvelidze
Foundation VRIC Trainee Travel Award. (His conclusions: “The coronavirus infection inflammatory state induces MLL1 and urokinase expression in bone marrow derived Mφs and circulating Mφs. MLL1urokinase regulation contributes to the hyperfibrinolytic phenotype seen in critically ill patients with COVID19 and represents a potential immunotarget to curb fibrinolysis.”)
VRIC draws from throughout the field of vascular biology and the
“I love that the presentations are from different fields in vascular biology and from people at different levels of training”
Sriganesh (Sri) Sharma
conference is well-known for the robust and instructive discussion following presentations. “It’s a fantastic venue,” said Sharma. “I love that the presentations are from different fields in vascular biology and from people at different levels of training.”
“It’s a diverse crowd with diverse
perspectives,” Obi agreed. And because of that, plus the almost ubiquitous problem of blood clots from across almost all specialties and fields, Sharma said.
He has continued his work with Obi, with a manuscript set for publication, and he hopes his findings since a year ago, with much more now known, are selected for presentation this year.
“This is a fascinating subject to study. I thought it would be a flash in the pan when I started,” Sharma said. “But what we found is incredibly interesting and we want to learn more about it.”
Where the goal was once to create a therapy protecting COVID patients, the two now see broader applications.
“We’ve known for 30 years that these innate immune cells are involved in thrombosis” said Obi. “But to date, no one has come up with an immune therapy to target it.”
Those experiencing clots typically are put on blood thinners, but the side effect of bleeding can be problematic and sometimes lifethreatening.
“Maybe we can get rid of the clotting propensity without putting a patient on thinners,” said Obi.
“That’s what Sri is studying.”
Coincidentally, given Sharma’s work in immunology, this year’s conference theme is “Translational Immunology and Cardiovascular Disease.” Sharma will feel at home. VRIC 2022 will be held Wednesday, May 11, in Seattle. Registration has opened. Visit vascular.org/VRIC22 to register and for more information.
Corner Stitch
Diversity efforts while in training: Is it just another box to check?
BY CHRISTOPHER AUDU, MD
2020 was a herald year. It ushered in a global pandemic and a reckoning with issues of diversity, equity and inclusion (DEI) in our workspaces. Vascular surgery, by nature of the diseases we encounter and our longitudinal relationship with our patients, have been front and center in both the clinical and social effects of the pandemic. Resultingly, we have been at the cutting edge of surgical treatment for COVID sequelae, and have the opportunity to be at the center of effective diversity efforts. However, the plethora of DEI efforts sometimes seems overwhelming, superficial or forced; and to the vascular trainee—you!—it can be another item to check off our evergrowing competency list.
SO HOW DO WE BEGIN TO ENGAGE diversity, equity and inclusion efforts as a trainee in a meaningful way? If you’re like me, your plate is already full. There is no easy answer here, but from talking with colleagues who are also navigating this, and from taking notes from our colleagues in other specialties, here are a few simple ideas on how to approach this as a trainee.
Listening to our patients to really hear them
Clinical medicine trains us to listen for buzz words, symptoms and pattern recognition. We learn much about pathophysiology. However, what we are not taught is how our patients experience the disease that we are tasked with helping them through. To get at this important and critical communication point, we must listen to what our patients are telling us and what is not being said. Ask open-ended questions without judgement. Acknowledge their reality. If appropriate, verbalize the obvious emotion. Listen. Don’t rush to fill the silence void. Patients know you’re busy, and most want to respect your time, but what active listening does is communicate that their perspective is valued and heard. To our minoritized patients, many of whom have been explicitly or implicitly told that their opinions, experiences and expressions don’t matter, this simple act is
cultural norms. As surgical trainees, who are often tired and running on caffeine, it can be easy to revert to how we see the world and assume that everyone sees it that way as well. It can be easy to revert to common stereotypes and tropes when that consult page comes in at the end of your call shift, or when you have to explain instructions to a difficult patient after you’ve just endured a negative evaluation, or when you finally get to see a patient who has “been lost to follow-up” or has “no-showed” clinic appointments. This is not fair to the patient—nor to you, as a surgeon. We must seek to know our biases (there are several online tools for this), and then inwardly reflect on them. This is easier said than done but the effort to do it will pay off, especially when communicating with our minoritized patients and/or anyone who doesn’t share the same heritage and upbringing as you. And this brings me to my next point.
Sitting with discomfort and learning
own performances when we hit negative feedback, I advocate that we sit with our discomfort and use it to propel us to grow.
Recruiting talent
much appreciated—even if you eventually have to relay bad news regarding their disease diagnosis and prognosis. Everybody desires to be truly heard, and not summarily dismissed or ignored. When you acknowledge the patient experience of their disease, both trainee and patient grow towards a common health goal.
Checking our implicit biases during patient care
We all have biases based on our individual experiences, expectations, upbringing and
Sometimes, our biases show up when we least expect it. A situation may make us uncomfortable, unpleasant or upset—and we can’t put a precise finger on why. I love these moments, personally, because they reveal deeply held convictions, thoughts or experiences that beckon us to examine them thoughtfully. Other times, our biases are pointed out to us by our seniors, peers or friends. These are all opportunities for self-reflection, a resetting of our priorities, and if needed, personal education. Just as we strive to improve technically and in clinical judgement as our training goes on, and we constantly evaluate our
Apply for VAM travel scholarships by March 9
Everybody desires to be truly heard, and not summarily dismissed or ignored
Medical students and general surgery residents have until March 9 to apply for Society for Vascular Surgery (SVS) travel scholarships that enable attendance at the 2022 Vascular Annual Meeting (VAM) in Boston this June.
THE SCHOLARSHIPS ARE THE SVS GENERAL SURGERY Resident/Medical Student VAM Travel Scholarship and the SVS Diversity Medical Student VAM Travel Scholarship. Each provides not only a travel award to underwrite expenses to attend VAM, but also complimentary meeting registration, a mentorship program, mock interview practice session
There is a linear relationship between being a trainee and increasing responsibility. One year you’re the medical student, and in a few short years, you become the chief. No matter where you are on this journey, you have the power to positively influence someone else, especially those who are historically underrepresented in our profession. These don’t have to be grandiose efforts. It can be as simple as giving positive feedback when someone does something right; or letting your junior know that you value them and their work; or helping someone navigate the hidden curriculum at your institution; or encouraging that student who is on the fence to seriously consider vascular surgery, letting them know that they belong. There is no doubt that having a surgeon who shares your experience and culture (and maybe even language) goes a long way in building a positive therapeutic alliance, and we should recruit as much talent to our team as possible. This list is by no means exhaustive. Rather, I write this to show that engaging in meaningful DEI efforts as a trainee doesn’t need big budgets or lofty programs to be impactful, but can begin with a kind word, a listening ear and a reflective attitude. To our minoritized patients, colleagues and juniors, these are what make a difference in the day-to-day grind that is vascular surgery. May we be up to the task of becoming competent, confident and compassionate surgeons.
and a dedicated educational and networking program. Diversity scholarship winners also will participate in the Meet the Leaders Luncheon and Leadership Development Program graduation with members of the SVS Leadership Development and Resident and Student Outreach committees and mentors.
Students who live in the Boston area will not receive the travel award portion of the scholarship. Students and residents may apply to each scholarship program but are eligible to receive only one award per year. Priority will be given to those who have not previously received any type of SVS travel scholarship, are not presenting an abstract/poster at the meeting, and have not already matched into a training program. VAM 2022 will be held June 15–18 in Boston. Scholarship notifications will occur in mid-April.—Beth Bales
More information is available at vascular.org/VAMTravel1 and vascular.org/VAMTravelDiversity.
Guidelines recognize potential role for earlier endovascular treatment of uncomplicated TBAD
BY WILL DATE
Newly published clinical practice guidelines aim to act as “guard rails” to determine the treatment options and best practices for managing patients with type B aortic dissection (TBAD). An important update in the document is the potential for earlier endovascular treatment in patients with uncomplicated TBAD at higher risk of progressive disease.
THE GUIDELINES, PRODUCED JOINTLY BY THE Society of Thoracic Surgeons (STS) and the American Association for Thoracic Surgery (AATS) were published online in the Annals of Thoracic Surgery and the Journal of Thoracic and Cardiovascular Surgery. The new document offers evidence-based recommendations that include employing a “stepwise approach” to the evaluation and treatment of patients with uncomplicated TBAD, followed by close clinical surveillance.
“There has been an explosion of information in the form of research reports of varying quality regarding the treatment of type B dissection over the past decade,” said author G. Chad Hughes, MD, from the division of cardiovascular and thoracic surgery at Duke University Medical Center in Durham, North Carolina.
According to the guidelines, aggressive medical therapy is the first step and considered the gold standard for managing patients with uncomplicated TBAD, while open surgery should be reserved for complicated cases. Importantly, the guidelines recognize advances in less invasive treatment options for the disease, including the new role of earlier endovascular treatment such as thoracic endovascular aortic repair (TEVAR). They suggest that surgeons now may be able to identify subsets of patients with uncomplicated TBAD who have a higher risk of progressive disease and treat them earlier with TEVAR—before progression develops. But this advisory remains secondary to medical management.
“There has been an explosion of information in the form of research reports” G. Chad Hughes
PAD skills course postponed to October
Because of the surge in COVID-19 pandemic cases, the Society for Vascular Surgery (SVS) has postponed the planned SVS Complex Vascular Intervention Skills Course (formerly known as the Peripheral Arterial Disease Workshop) set for February to Oct. 23–24 in Rosemont, Illinois. The decision followed careful monitoring by SVS of the pandemic and the recent surge in cases. The decision was not made lightly; the top priority for the Society is the health and safety of SVS members and other learners. Those who registered for the course, which will include hands-on skills training on Oct. 24, should check the email used for registration for refund and other important information.— Beth Bales
For information on the course and/or the postponement may contact the SVS education team at education@ vascularsociety.org or visit vascular.org/ PADCourse22.
Community practice award deadline extended
The Society for Vascular Surgery (SVS) has extended the deadline to nominate an SVS member for the prestigious Excellence in Community Practice Award. Applications now are being accepted through March 31 for this award, formerly known as the Excellence in Community Service Award. The honor is exclusively for those who practice in the community setting, including members in office-based labs (OBLs). Selection recognizes an individual’s sustained contributions to patients and their community, as well as exemplary professional practice and leadership.
To be considered, applicants must be community practitioners and have been in practice as a vascular surgeon for at least 20 years, been an SVS member for at least five years, and show evidence of impact on vascular care or community health. Learn more at vascular.org/CommunityServiceAward.—Beth Bales
Europe: ESVS publishes 2022 guidelines on management of chronic venous disease
The European Society for Vascular Surgery (ESVS) has released 2022 clinical practice guidelines on the management of chronic venous disease (CVD) of the lower limb to update its 2015 recommendations. The document, authored by Marianne De Maeseneer, MD, a venous specialist at Erasmus Medical Centre in Rotterdam, The Netherlands, and colleagues, was published online ahead of print in the European Journal of Vascular and Endovascular Surgery (EJVES).
The focus of the new guidelines is related to pathology of the superficial,
From the SVS journals
The Journal of Vascular Surgery Cases, Innovations and Techniques has been growing rapidly, publishing an estimated 33% more articles this year than two years ago, according to JVS editors Peter Lawrence, MD, and Peter Gloviczki, MD. “In 2021, we modified the name of the journal to reflect its increased scope, which will now accept articles on all areas of innovation, including practice, education, outcome assessment and procedural technique as well.” See vsweb. org/JVSCITtransformation.
What’s the role of diet in managing PAD? JVS-Vascular Science discusses this topic in “Nutrition in the management of peripheral arterial disease: Should we pay more attention to what our patients eat?” See vsweb.org/ JVSnutritionandPAD.—Beth Bales
perforating and deep veins of the lower limb, as well as to abdominal and pelvic venous pathology.
Compared with the 2015 version of the guidelines, the authors communicate that the global structure of the document has been modified considerably in an attempt to make it more practical and user friendly.
In addition, they write that special subsections on management strategy with accompanying flowcharts have been added to the different chapters.
There are several new chapters in the 2022 document, addressing the management of patients with venous leg ulcers and of patients with varicose veins, related to underlying pelvic venous disorders, special patient characteristics and their potential influence on management strategy, and gaps in evidence and future perspectives.
De Maeseneer et al detail that five recommendations have been upgraded in the 2022 guidelines, with three downgraded.—Jocelyn Hudson
March 1 awards deadline nears
The deadline is March 1 for several awards and honors from the Society for Vascular Surgery (SVS) and the SVS Foundation. They include the SVS Lifetime Achievement Award, the Medal for Innovation in Vascular Surgery, the Distinguished Fellow Designation, as well as SVS Foundation Clinical Research Seed Grants (writes Beth Bales).
n Lifetime Achievement Award: This is the highest honor the SVS bestows on an individual member. This recognizes an individual’s outstanding and sustained contributions to the profession and the SVS, as well as their exemplary professional practice and leadership. The most recent recipient was Robert Smith, MD, of Georgia (in 2020), who received his honor at the 2021 Vascular Annual Meeting (VAM) in San Diego n Medal for Innovation in Vascular Surgery: This honors an individual whose contribution has had a transformative impact on the practice or science of the vascular surgical specialty. The most recent recipient was venous surgery pioneer Robert Kistner, MD, in 2019 n Distinguished Fellow designation: This designation goes to Active, International or Senior members who are vascular surgeons and who have made substantial contributions in two of the three categories of research, service and education. Visit vsweb.org/DistinguishedFellow for more information
n Clinical Research Seed Grants: These awards provide $25,000 in direct support for clinical pilot projects that have the potential to become larger studies funded by industry or government sources
For more information on the awards, visit vascular.org/SVSAwards or vascular.org/ FoundationAwards.
In memoriam Pinkus H. Szuchmacher, MD, of Manhasset, New York, died Aug. 8, 2021. Szuchmacher emigrated from Brazil in 1965 and spent 50 years in practice as a vascular surgeon— as well as training residents—in New York City. He was 81.