

6
Vascular groups send special letter to HHS.

13 News From SVS
Set your sights on VAM at National Harbor, Md. The program will be a great one.

6
Vascular groups send special letter to HHS.
Set your sights on VAM at National Harbor, Md. The program will be a great one.
BY JEFF CRAVEN MDEDGE NEWS
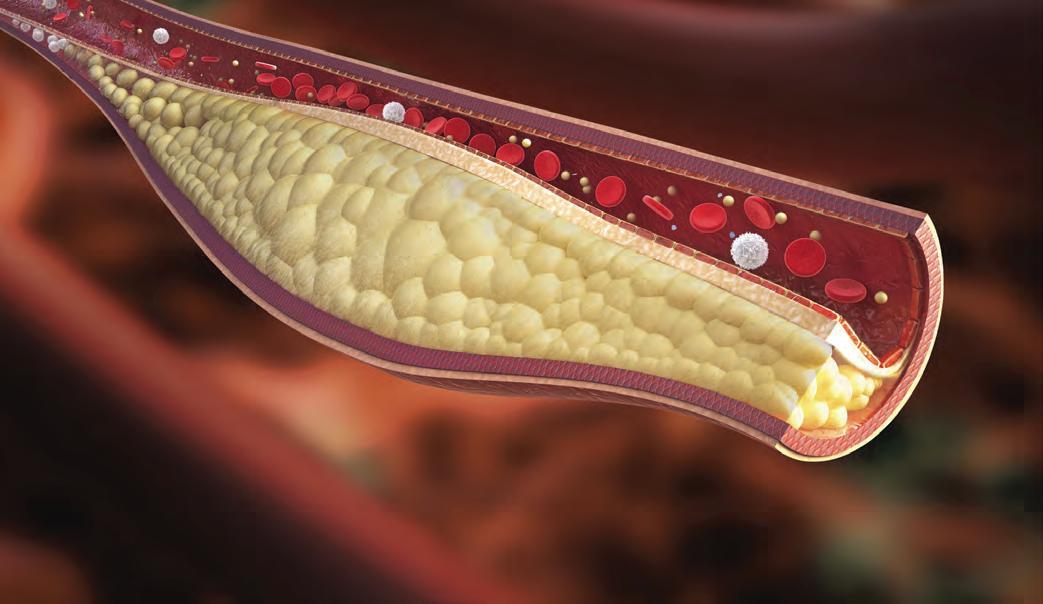
The Food and Drug Administration has issued a letter alerting health care providers that it is aware of and examining recent data on an increase in long-term mortality rates for patients receiving paclitaxel-coated balloons and paclitaxel-eluting stents for treatment of peripheral artery disease.
“Currently, the FDA believes that the benefits continue to outweigh the risks for approved paclitaxel-coated balloons and paclitaxel-eluting stents when used in accordance with their indications for use,” William Maisel, MD, MPH, chief medical officer of the Center for Devices and Radiological Health at the FDA, wrote in a letter to

16
Check out our new SVS members.
BY MICHELE G. SULLIVAN
MDEDGE NEWS
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Newly released criteria aim to advise clinicians about the most appropriate interventions for managing peripheral artery disease.
The report, published in the Journal of the American College of Cardiology, drew on the expertise of a broad panel of experts, including representatives from
the American Heart Association, the Society for Cardiovascular Angiography and Interventions, the Society of Interventional Radiology, the Society for Vascular Medicine, and the Society for Vascular Surgery.
“Improvements in the diagnosis of peripheral artery disease (PAD) have led to an increasing number of treatment and revascularization methods, especially endovascular interventions,” wrote Steven R. Bailey, MD, who headed the multidisciplinary writing committee. “As new and increasingly sophisticated devices are devel-
Gilbert Upchurch Jr., MD, elected SAVS President
Dr. Upchurch, of the University of Florida Heart Health and Vascular Hospital, Gainesville, was elected 2019 president of the Southern Association for Vascular Surgery at their 43rd Annual Meeting held in Boca Raton, Fla., Jan 23-26, succeeding Matthew S. Edwards, MD, of Wake Forest Baptist Health, Winston-Salem, N.C.
Column Continued on page 19
BY MALACHI G. SHEAHAN III, MD MEDICAL EDITOR, VASCULAR SPECIALIST
T
January 25, 2019
Seema Verma, Administrator Centers for Medicare & Medicaid Services Department of Health & Human Services
Don Rucker, MD, National Coordinator for Health Information Technology Office of the National Coordinator for Health Information Technology
U.S. Department of Health & Human Services

hrough the 21st-Century Cures Act, Congress directed the Department of Health & Human Services (HHS) to establish a goal, develop a strategy, and provide recommendations to reduce EHR-related burdens that affect care delivery. HHS has now submitted a draft titled “Strategy on Reducing Regulatory and Administrative Burden Relating to the Use of Health IT and EHRs.” A call for comments from the public and medical community was issued. The response from the Society for Vascular Surgery is documented at right. The work of the SVS Wellness Task Force shaped the content of this letter. Your remarks and responses to the surveys and focus groups have been heard and are now directing action. At press, the presidents of the Association of Program Directors in Vascular Surgery, the Society for Clinical Vascular Surgery, the Vascular and Endovascular Surgical Society, and all five major regional vascular societies have endorsed the letter. This document represents a clear and definitive specialty-wide call for change.
VASCULAR SPECIALIST Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD., Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Drudi, MD.
Executive Director SVS Kenneth M. Slaw, PhD.
Interim Director of Membership, Marketing and Communications
Angela Taylor
Managing Editor SVS Beth Bales
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of health care policy. Content for Vascular Specialist is provided by Frontline Medical Communications Inc. Content for the News From the Society is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and Frontline Medical Communications Inc. will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein.
Dear Administrator Verma and Dr. Rucker,
On behalf of the undersigned organizations, we would like to thank you for the efforts of the Centers for Medicare and Medicaid Services (CMS) and the Office of the National Coordinator for Health Information Technology (ONC) to address the burden regarding the use of health IT and EHRs in a physician’s practice. However, there is still much work to be done, and the Society for Vascular Surgery (SVS) in concert with eight of our fellow societies have developed a set of recommendations regarding future steps that CMS and ONC could take to further address the regulatory and administrative burden of health IT and EHRs. Together our groups represent the majority of vascular surgeons in the United States. Today, we take this opportunity to reach out to you with one voice, on these recommendations to address this significant disruption throughout our specialty.
While systems of medical records have been
POSTMASTER Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 10255 W Higgins Road, Suite 280, Rosemont, IL 60018-9914.
RECIPIENT: To change your address, contact Subscription Services at 1-800-430-5450. For paid subscriptions, single issue purchases, and missing issue claims, call Customer Service at 1-833-836-2705 or e-mail custsvc.vasc@fulcoinc.com.
The Society for Vascular Surgery headquarters is located at 633 N. St. Clair St., 22th Floor, Chicago, IL 60611. Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by Frontline Medical Communications Inc., 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609. Phone 973-206-3434, fax 973-206-9378
Subscription price is $230.00 per year.
National Account Manager Valerie Bednarz, 973-206-8954, cell 973-907-0230, vbednarz@mdedge.com
Digital Account Manager Amanda Smith, (973) 206-2321, asmith@mdedge.com
Classified Sales Representative Drew Endy, 215-657-2319, cell 267-481-0133, dendy@mdedge.com
Senior Director of Classified Sales Tim LePella, 484-921-5001, cell 610-506-3474, tlapella@mdedge.com
Advertising Offices 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609 973-206-3434, fax 973-206-9378
©Copyright 2019, by the Society for Vascular Surgery


Scan this QR Code to visit vascularspecialistonline.com
in place for a very long time, only recently have they become the source of widespread physician dissatisfaction. This phenomenon coincides with the mass integration of electronic-based health records over the past decade. Paper-based charts could be completed almost passively, usually during interactions with the patient. Computer-based systems often require the physician to literally turn their back on the patient to complete the documentation in real time. Many physicians eschew this practice in favor of performing the record keeping at some later point in time, after completion of the patient encounter. Multiple studies have confirmed the increased documentation burdens placed on physicians via Electronic Health Record (EHR) integration. This additional time often occurs after regular work hours and comes at the expense of time spent with families, time spent on leisure activities, and even sleep. The result is emotional exhaustion, an essential component of physician burnout.
In 2018, active SVS members were surveyed anonymously using a validated burnout assessment embedded in a questionnaire that also captured demographic and practice-related characteristics. The survey was personalized for the specialty and did allow for free-text. We specifically analyzed emotional exhaustion, a critical dimension of burnout. Responses from 872 practicing vascular surgeons were analyzed. Overall, 30% of respondents met criteria for burnout, 37% screened positive for symptoms of depression in the past month,
Letter continued on page 12
FRONTLINE MEDICAL COMMUNICATIONS SOCIETY PARTNERS
Director, FMC Society Partners Mark Branca
Editor in Chief Mary Jo M. Dales
Executive Editors Denise Fulton, Kathy Scarbeck
Managing Editor Mark S. Lesney
Creative Director Louise A. Koenig
Director, Production/Manufacturing Rebecca Slebodnik
Letters to the Editor: VascularSpecialist@vascularsociety.org
Editorial Offices: 2275 Research Blvd, Suite 400, Rockville, MD 20850, 240221-2400, fax 240-221-2548
Corporate
President/CEO Alan J. Imhoff
CFO Douglas E. Grose
SVP, Finance Steven J. Resnick
VP, Operations Jim Chicca
VP, Sales Mike Guire
VP, Society Partners Mark Branca
VP, Editor in Chief Mary Jo M. Dales
VP, Editorial Director, Clinical Content Karen Clemments
Chief Digital Officer Lee Schweizer
VP, Digital Content & Strategy Amy Pfeiffer
President, Custom Solutions JoAnn Wahl
VP, Custom Solutions Wendy Raupers
VP, Marketing & Customer Advocacy Jim McDonough
VP, Human Resources & Facility Operations Carolyn Caccavelli
Data Management Director Mike Fritz
Circulation Director Jared Sonners
Corporate Director, Research & Comms. Lori Raskin
Director, Custom Programs Patrick Finnegan
In affiliation with Global Academy for Medical Education, LLC
President David J. Small, MBA
FDA from page 1
health care providers.
PERSPECTIVE by Dr. Peter A. Schneider
AThe FDA letter was in response to a recent systematic review of paclitaxel-coated balloons and stents recently published in the Journal of the American Heart Association. Konstantinos Katsanos, MD, PhD, from Patras University Hospital in Rion, Greece, and colleagues performed the systematic review and meta-analysis of 28 randomized controlled trials with 4,663 patients who received paclitaxel-coated devices in the femoral and/or popliteal arteries and found similar 1-year risk of all-cause patient mortality (2.3%; risk ratio, 1.08; 95% confidence interval, 0.721.61).

recently published meta-analysis concluded that “There is increased risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery of the lower limbs.”1 The study was an analysis of summary-level data from 28 published or presented trials (4,663 patients) that evaluated the use of drug-coated balloons (DCB) or drug-eluting stents (DES) for the treatment of femoral-popliteal occlusive disease. Mortality was similar at 1 year but was significantly increased at 2 years for paclitaxel versus control (7.2% versus 3.8%), and there was an even larger differential at 5 years (14.7% versus 8.1%). On face value, this is worrisome.
present for the length of patient’s follow-up after a single time balloon inflation many years before? These trials were powered to evaluate 1-year patency, not longer-term mortality. We have to take the data for what they are; a signal that we have work to do to better understand if there is any increased risk to our patients.

The FDA told health care providers to continue surveillance of these patients per standard of care.
However, there was an increased risk of all-cause mortality for patients with paclitaxel-coated devices at 2 years (7.2% vs. 3.8%; RR, 1.68; 95% CI, 1.15-2.47) and at 5 years (14.7% vs. 8.1%; RR, 1.93; 95% CI, 1.27-2.93), compared with control groups.
The number needed to harm at 2 years was 29 patients (95% CI, 1959) and 14 patients (95% CI, 9-32) at 5 years. Their meta regression analysis found a significant link between paclitaxel exposure and absolute risk of death.
“Actual causes for this serious late side effect remain unknown, and further investigations with longer-term follow-up are urgently warranted,” Dr. Katsanos and colleagues wrote in their review.
The FDA told health care providers of patients with paclitaxel-coated balloons and paclitaxel-eluting stents to continue surveillance of these patients per standard of care, to discuss the risks and benefits of
The use of summary-level data to perform meta-analysis is a legitimate form of scientific inquiry. However, this method is typically used to generate hypotheses, which must be subsequently confirmed and is not intended to be used as a definitive answer.
The advantages of summary level data are clear; it is readily available and it permits use of larger patient cohorts than would otherwise be possible, which may identify a signal that is not otherwise apparent. There are some disadvantages of using summary level data that can result in bias and possibly incorrect conclusions.
Assumptions have to be made: that the analyzed trials are similar enough to each other to be comparable; that the delivery of paclitaxel was uniform; that censored patients were handled in a certain way in all the studies. The actual dose of paclitaxel cannot be calculated. Missing data must be imputed, since some studies report percentages, rather than numbers of events.
Is it scientifically valid to include studies of DCB and DES in the same meta-analysis, given the dramatic difference in the mechanism of paclitaxel delivery? Is it reasonable to make the assumption that paclitaxel remains
PAD treatment options with patients, and to report any adverse or suspected adverse events to MedWatch.
The FDA said they are currently evaluating the long-term data on
The conclusion of the meta-analysis focuses on the long-term mortality risk. Only three studies extend to five years; 2 DCB studies and one DES study.2-4 In all three of these studies, longer-term mortality was higher for paclitaxel devices than control. Is this finding a coincidence or a missed safety signal? Because there are only three studies, idiosyncratic features of any of these trials will have an outsized effect on the results of the meta-analysis. Among the DCB trials for example, the IN.PACT SFA Trial randomized DCB to PTA in a 2:1 manner (104 patients in the PTA group), and the subsequent mortality rate for the PTA group in the first three years was the lowest ever reported in a trial of peripheral vascular patients (0%, 0.9%, and 1.9%, respectively).2 The Thunder Trial only randomized 54 patients to PTA and the initial design was for a two-year follow up.
Dr Schneider is Chief Medical Officer for Intact Vascular; has received modest royalties from Cook Medical; and has served as a noncompensated advisor for Medtronic, Abbott Vascular, and Cardinal. He has published articles regarding the IN.PACT SFA trial2 and has an upcoming article in discussing this topic further, which will be reported on in next month’s Vascular Specialist.
cause. Mortality rates for all of the DCB and DES trials are within the range of that demonstrated in other vascular device trials. No particular mechanistic relationship between paclitaxel and mortality has been proposed.
DCB and DES have resulted in a substantial improvement in patency for patients that require femoral-popliteal revascularization and have appeared until now to possess an acceptable safety profile.
Beneficial results have been confirmed in numerous trials performed by a myriad of investigators, using a variety of devices over a broad geography. The benefits are substantial, but if there is a safety signal with paclitaxel, we need to understand its magnitude urgently.
Because this is an important issue for our patients and because of a deep desire to do no harm, it cannot be summarily rejected and we owe it aggressive due diligence. Is this a statistical aberration or an important safety signal that must guide subsequent clinical practice? In my opinion, it is not appropriate to draw a firm conclusion at this time.
When the patients were subsequently followed up at five years, 48% of the PTA group was lost to follow-up.3 No one could have anticipated that these seemingly small things could weight a meta-analysis in a particular direction many years later. In studies that fully evaluated the causes of mortality, there does not appear to be any clustering of the deaths as to any particular
paclitaxel-coated products to determine whether the devices carry an increased risk of death or other long-term risks, and noted there were several paclitaxel-coated balloons or paclitaxel-eluting stents that
The mortality risk will be better understood when we have a patient-level data with calculated drug doses and adjudicated mortality from a variety of trials.
References
1. J Am Heart Assoc. 2018;7:e011245.
2. Circ Cardiovasc Interv 2018;11:e005891.
3. JACC Cardiovasc Interv 2015;8:102-8.
4. Circulation. 2016;133:1472-83.
have either been approved or are under study in the United States. ■
SOURCE: Katsanos K et al. J Am Heart Assoc. 2018. doi: 10.1161/ JAHA.118.011245.
PAD from page 1
oped, the medical community needs to understand how best to incorporate these technologies into daily clinical decision making and care, and how to choose between new and more established methods. This project was initiated to respond to this need and to ensure the effective use of peripheral artery revascularization.”
The document is not intended to cover every possible clinical scenario that could employ these interventions, wrote Dr. Bailey, who is the Janey Briscoe Distinguished Chair in Cardiology at the University of Texas, San Antonio, and his coauthors. “Rather, the goal is to provide generalized guidance into the use of these devices and techniques, while understanding that each clinical situation is unique, with physicians using their best judgment and the available evidence base to craft the most beneficial approach for the patient. In all cases, it is assumed that guideline-directed medical therapy should be applied first.”
The panel identified 45 scenarios in key clinical areas in which PAD interventions – either surgical or endovascular procedures – might be employed as first-line therapy. These included renal artery stenosis, lower extremity disease, critical limb ischemia, and asymptomatic artery disease. The report also discussed options for endovascular interventions, and secondary treatment options for lower extremity disease. The panel graded the value of interventions as appropriate, may be appropriate, or rarely appropriate.
“The scenarios in this document are arranged according to the clinical decision points confronting vascular practitioners in everyday clinical practice,” the panel wrote. “These include the presence or absence of symptoms, presence or absence of limb-threatening disease, severity and anatomical location of the culprit lesion, recurrent or de novo disease, the advantage of endovascular or surgical revascularization, and the expected durability of clinical benefit after an intervention.”
Renal artery stenting Recommendations in this category were largely based on the CORAL (Cardiovascular Outcomes in Renal Atherosclerotic Lesions) study, which recommends best medical therapy as the initial treatment for a newly diagnosed patient. (N Engl J Med 2014;370:13-22).
The optimal medical approach is
generally thought to be three antihypertensive medications, one of which should be a diuretic. Primary stenting can be considered for patients with an accelerating decline in renal function and bilateral or solitary significant renal artery stenosis, or moderate stenosis with translesional gradients that exceed threshold measurements. In patients with stable renal function and unilateral significant stenosis, intensifying medical therapy is appropriate. Stenting is rarely appropriate in patients with small, nonviable kidneys.
Lower extremity disease
Recommendations for lower extremity revascularization in patients with claudication are based largely on the 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease. For patients with PAD and intermittent claudication, medical therapy and exercise are the first-line treatments. Revascularization should be considered only when this option fails. The appropriateness of inter-
"The scenarios in this document are arranged according to the clinical decision points confronting vascular practitioners in everyday clinical practice."
vention depends on the location and length of the lesion.
Intensification of medical therapy or endovascular treatment are appropriate for patients with aortoiliac, superficial femoral artery, and popliteal artery lesions; surgery also may be appropriate here. Medical therapy is appropriate for lesions located below the knee, as well; endovascular approaches also may be appropriate. Surgery for these lesions is rarely appropriate.
Critical limb ischemia
Medical therapy is generally not considered for these patients. But regardless of the lesion location, the panel found either endovascular or surgical treatment appropriate. Indeed, revascularization is the only viable treatment for these patients.
“Revascularization, whether endovascular or surgical, is critical for the reduction of high morbidity and mortality rates associated with limb loss. Mortality rates have been reported to be as high as 20% within 6 months of diagnosis and exceeding 50% after 5 years in patients left untreated. Furthermore, this degree of PAD is commonly associated with excessive cardiovascular events, often surpassing mortality rates associated with even symptomatic coronary artery disease.”
Asymptomatic artery disease
The recommendations in this category address the need to gain arterial access for potentially life-saving cardiovascular procedures. There are no published data in this area, so the recommendations are all based on expert opinion.
To gain access for coronary interventions, endovascular treatment and surgery are both appropriate. For hemodynamic support and large vascular or valvular interventions, endovascular approaches are appropriate, and surgical approaches may be appropriate.
Options for endovascular treatment when deemed appropriate or may be appropriate Since there is no standardized treatment when an intervention is deemed appropriate, the potential procedures are organized by general lesion location (above or below the inguinal ligament and below the knee), and by lesion length. The recommendations cover the most commonly used endovascular treatment modalities.
“Of note, the use of atherectomy in the iliac artery has been rated Rarely Appropriate in all clinical scenarios,” the team noted. “This rating derives from an absence of data supporting the use of this technology, compared with balloon angioplasty and stenting. Similarly, the use of atherectomy in the superficial femoral and popliteal arteries and belowthe-knee vessels also received a lower score, again because of the lack of comparative data relative to technologies with prospectively collected data. The evidence base to judge intervention below the knees is not as developed as other lower-extremity locations, which results in more frequent use of the May Be Appropriate category. The rating panel felt that below-the-knee atherectomy once again lacked comparative evidence to support general use.”
There are some exceptions, “favoring atherectomy include severe calcification and undilatable lesions; however, other technologies had a
better evidence base for routine revascularization in most settings.”
Secondary treatment options
This section addresses options for very specific situations, including in-stent restenosis, venous bypass graft failure, and prosthetic bypass graft failure.
“It is recognized that the need for revascularization of a failing conduit, graft, or stent is a marker of adverse outcomes for all of the reparative modalities employed,” the panel wrote. “Literature comparing treatment modalities for in-stent stenosis, venous graft failures, and arterial graft failures is very limited. Therefore, the recommendations primarily reflect consensus based upon current clinical practice.”
The modality choice should probably depend more upon surgeon preference and clinical experience, rather than a blanket recommendation. In general, the panel felt that surgical revascularizations are rarely appropriate for in-stent stenosis, especially if the patient is asymptomatic.
The panel felt that endovascular approaches are generally appropriate for focal stenoses in patients with prior surgical grafts and bioprosthetic material, but in patients with diffused stenosis or thrombosed grafts, both endovascular and surgical approaches were graded as may be appropriate.
“The specific type of therapy [device or surgical procedure] is at the discretion of the clinician, dictated by the clinical scenario plus physician and facility experience.”
Dr. Bailey had no financial disclosures; however, some members of the panel did disclose relationships with device manufacturers and pharmaceutical companies. ■
msullivan@mdedge.com
SOURCE: Bailey SR et al. J Am Coll Cardiol. 2018 Dec 17.

BY M. ALEXANDER OTTO MDEDGE NEWS REPORTING FROM THE 2018 ACS CLINICAL CONGRESS
BOSTON – The higher the comorbidity burden, the greater the likelihood that osteomyelitis will lead to amputation within 2 years, according to a review of 1,186 patients at the University of Michigan, Ann Arbor.
The limb amputation incidence was 7.2% over 2 years in patients with no comorbidities, 21.4% among patients with heart failure, 36.1% in patients with diabetes, and 36.7% among those with peripheral vascular disease (PVD).
The 2-year incidence marched steadily upward with combined comorbidities to 47.4% in patients with diabetes and heart failure; 64.5% in patients with diabetes and PVD; and 75.0% in patients with diabetes, heart failure, and PVD.
“What this means is that looking at diabetes versus no diabetes alone is not sufficient to gauge the risk of amputation. We have to look at the patient’s comorbidity profile as a whole,” said lead investigator Toby Keeney-Bonthrone, a medical student.
“The question is if some patients would benefit from [an earlier,] more prophylactic amputation,” he said at the annual clinical congress of the American College of Surgeons.
“We often find ourselves reacting to osteomyelitis as it progresses. I think patients deserve a better deal than that. They deserve for us to think one or two steps ahead,” he added.
The team reviewed adult patients from 2004 to 2015 who were followed for at least 2 years after diagnosis; 610 had diabetes, a known risk factor for osteomyelitis and amputation, and 576 did not.
Comorbidities were considerably more common in the diabetes group, including PVD and heart failure, but also chronic obstructive pulmonary disease, previous heart attack, prior amputation, and especially renal disease. The 2-year amputation incidence was also higher in the diabetes group (43.1% vs. 12.3%), as was 2-year mortality (22.3% vs. 15.5%).
Odds ratios for lower limb amputation climbed in a stepwise fashion on multivariate analysis, from almost a 100% increase in men and in black patients to a 158% increase among patients with past amputations; a 206% increase with PVD; a 256%
increase in patients with type 2 diabetes, and a 349% increase among patients with type 1 diabetes.
The work was funded by the NIH. The investigators reported no relevant disclosures. ■
aotto@mdedge.com
SOURCE: Keeney-Bonthrone T et al. J Am Coll Surg. 2018 Oct;227(4), S105.
13 SCIENTIFIC SESSIONS: June 13–15, 2019 / EXHIBITS: June 13–14, 2019
NUMEROUS OPPORTUNITIES TO NETWORK WITH COLLEAGUES & LEADERS
SVS WILL HOST THE VASCULAR SPECTACULAR GALA FRIDAY EVENING TO BENEFIT THE SVS FOUNDATION.
c CUTTING-EDGE RESEARCH
c TECHNICAL & EDUCATIONAL EXHIBITS
c SESSIONS FOR THE ENTIRE VASCULAR TEAM, WITH
• MORE ‘ASK THE EXPERT’ SESSIONS
• MORE CHANCES TO INTERACT WITH PRESENTERS

ALL EVENTS HOSTED AT THE GAYLORD NATIONAL RESORT & CONVENTION CENTER, NATIONAL HARBOR, MD. JUST OUTSIDE WASHINGTON, D.C.
HOUSING & REGISTRATION OPEN IN EARLY MARCH
BY DONALD L. ZIMMERMAN, PHD
Burnout among vascular surgeons and other physicians is a serious national epidemic that needs immediate attention by senior policy makers and health care leaders. Not only is maintaining an appropriate supply of fully qualified surgeons important to the medical demands of our country, the underlying causes of physician burnout clearly point to increased personal pain and suffering within the physician community.
While it is quite clear that a serious response to physician burnout requires immediate action, the most pressing and urgent question for senior leadership is exactly what can be done to best address the causes of this epidemic.
This commentary reflects an approach and strategy for building an effective response to physician burnout deeply rooted in the broad discipline of health care management theory and research. Our understanding of the problem starts with the simple and common observation that our thoughts about our job are deeply embedded in the conditions and “lived reality” of doing our job. We can see this link in everyday conversations when they quickly turn to detailed complaints about all things work related.
Listening to people complain about their jobs can sometimes sound like unfounded “whining.” But if we dig deeper into such complaints, we can start to see some common elements giving credence to such grievances. For example, if we step back a little from our current preoccupations and look at the history of work over the last 100 years or so, we can see the outline of a long and generally progressive arc of change aimed at improving the conditions for making a living.
This arc of change has allowed us to stop complaining so much about the risk of losing life and limb from industrial accidents because those complaints helped to create new laws that imposed strict regulations, making the conditions of working with big machines much safer. From the 40-hour week, paid vacations, and tenure to workplace discrimination, harassment, and abuse, there are many examples of how complaining about the conditions of one’s job has led to major changes in how people work together in an organization.
Coming back to the present, the big, clamoring machines that caused many to complain years ago have now been replaced by the clicking and hum of computers used by knowledge-based workers. But while the tools, physical environment, workforce, and other key characteristics of what people do for a living change over time, serious complaints about job conditions remain important sources of information about how to make those conditions job safer and healthier.
The importance of complaining One of the primary goals of every health care organization should be to consciously create safe and healthy working conditions for physicians and everyone else involved in the daily production of health care services.

Dr. Zimmerman is a professor of health care management at the University of New Orleans.
At present, there is considerable interest in developing new programs for addressing physician burnout by using therapeutic interventions. This approach is focused on mediating the severity of an unhealthy workplace by helping physicians better cope with personal frustrations and other psychological difficulties related to their job.
Personal counseling, yoga at noon, and other tools for building personal resilience can certainly improve coping skills but fundamentally miss the point for addressing the underlying causes for burnout.
The problem here is that a reliance on therapeutic interventions alone can mask and reflect the cause of the problem from their source in the conditions of the workplace back onto the physicians who must do their job under those conditions. This is roughly equivalent to providing therapeutic counseling to a factory worker who loses an arm to a machine in an industrial accident with no mention or effort to fix the dangerous machine that workers were loudly complaining about before the accident.
In order to develop an effective response to burnout, attention needs to be given to the specific content of what physicians are complaining about as existential threats to their personal health and safety in the environment in which they do their work as physicians.
A clear-eyed assessment of the real-life structures and processes that define how the work of physicians is routinely carried out every day is needed in every modern health care organization. Such
an assessment is not a call for simply “whining” about everyday annoyances and bothers that are encountered as part of most people’s jobs. Rather, a thoughtful cataloging of what physicians are complaining about is required.
This examination needs to carefully listen to complaints to better understand two highly related factors. First: What do vascular surgeons and other physicians “want to do” in order to be personally “satisfied” with their job? And second: How does the organization (structure) and established “flow” (processes) of their given work environment encourage, help, hinder, or prevent them from being satisfied as a regular part of being a physician?
Such an assessment of complaints will not be easy. Important methodological considerations will need to be made to make conceptual and measurable distinctions between complaints about major threats to physician health that are part of the current work environment and ongoing and rapid changes affecting the overall profession of medicine. For example, new and ongoing developments in medical technology, health informatics, generational shifts in the attributes of the workforce, evolution of state and federal policy, shifting patient and epidemiological profiles, and other major trends will continue to affect the workplace of physicians. Such changes are part of the current dynamics of the workplace of physicians and may be major components of the conditions of work that are generating complaints and contributing to burnout.
Viewing physician complaints as important tools for improving the working conditions of physician does not mean that such changes can be stopped. More directly, it means that physician complaints can become a critical part in the policy debate and management discussion about what changes in the physician workplace need to change to eliminate burnout.
From a health care management perspective, physicians should take the lead and keep complaining. It is an essential window for senior leadership to see exactly what needs to be done to create a safer and healthier workplace for physicians to be physicians. ■



EXPERIENCE THE DIFFERENCE IN



























Choose the distinctive performance of our balloon dilatation catheters
Engineered to provide best-in-class PUSHABILITY* with a small profile for accessing target lesions1
Complete support for complex BTK cases
PINNACLE® DESTINATION®

Demonstrated excellence in CROSSABILITY with a low deflation time1
Guiding Sheath NAVICROSS® Support Catheters GLIDEWIRE ADVANTAGE® Peripheral Guidewires GLIDEWIRE® GOLD Hydrophilic Coated Guidewire
*Tested against select leading competitors


When RX tested against Boston Scientific Sterling™ Monorail™ and OTW tested against Bard Ultraverse® 0.018" RX ONLY. Refer to the product labels and package inserts for complete warnings, precautions, potential complications, and instructions for use. Reference: 1. Data on file. ©2018 Terumo Medical Corporation. All
continued from page 6
and 8% reported thoughts of taking their own life during the last 12 months. Factors significantly associated with burnout included clinical work hours, on-call frequency, electronic medical record (EMR)/documentation requirements, perceived conflict between work and personal responsibilities, and physical pain. What was more compelling, perhaps, was that nearly 80% of the free text comments expanded on frustrations of the EHR.
Similarly, Wellness Focus Groups were conducted at the 2018 Vascular Annual Meeting of the Society for Vascular Surgery. Participants identified several themes that produced additional stress and negatively impacted quality of life. Again, the EHR was identified as one of the most significant stressors. Simply put, we are a specialty in crisis with rates of burnout and suicidal ideation that far surpass the general population. The integration of EHR has significantly, and perhaps principally, contributed to these issues.
The proprietary EHR vendors helped to defeat the Stark bill (HR 6898) and pass the Health Information Technology for Economic and Clinical Health Act (HITECH). HITECH essentially mandated EHR implementation. The vendors then marketed themselves to hospital administrators, often based on billing efficacy. Usability remained unmeasured. If EHRs had been designed to maintain or improve the physician experience, this would have been a priority. To this
day, there have been no standards placed on the “usability” of EHR platforms. While proprietary EHR vendors have generated billions in profits, there is little evidence of any significant investment in finding methods to reduce the burden they place on physicians, much less improving the work life of doctors, a vital component of the Quadruple Aim system to improve health care.
While we agree with many of the principles advanced by the 21st-Century Cures Act, we feel there must be a greater sense of urgency. The effects of EHR implementation have created a public health crisis. As a surgical subspecialty, vascular surgery is facing a dire workforce shortage. According to reports prepared for the Association of American Medical Colleges, there are no current projections under which the demand for vascular surgeons can be met by 2030. EHR burdens are producing widespread burnout in our existing workforce, leading to decreased productivity, substance abuse, and early retirement. Urgent reform is needed. The major EHR vendors have shown little interest in addressing the impact their technology has had on physician burnout. As such we need actionable goals and strict deadlines for implementation. It is time to hold the major EHR vendors accountable for their contributions to the deficiencies of our current system.
1. Usability of EHR systems remains unmeasured. Metrics, measures, and standards must be developed immediately to improve the physician experience and decrease time spent on EHR documentation. These actions must be performed
with full physician collaboration including vascular surgeons who remain at particular risk to EMR related emotional exhaustion.
2. To better integrate EHRs, all systems should be required to have a standardized import/ export function.
3. Prescription Monitoring Programs should be integrated into all EHRs.
4. Vascular surgeons should be able to document patient encounters according to their practice. The focused history, problem list, review of systems, physical exam should be specialty specific. These guidelines and requirements should be set in coordination with the Society for Vascular Surgery.
5. Each EHR vendor should be required to continuously consult clinicians from all essential medical and surgical specialties. This could be achieved by either submitting to each major clinical society or by nationally (or each state/region) developing a team of clinicians with representatives from each specialty to review new EHRs. This team should include not only practicing physicians but also residents, physician assistants and nurse practitioners who also regularly interact with the EHR.
6. Health insurance agencies should be required to facilitate automatic authorization through communication with EHRs.
7. Effective and efficient physician training and support for EHR use must become standard and not related to the specific “support package” purchased by the health care organization.
8. Quality measures must be universal across all payers.
Thank you for your review, we enthusiastically offer our assistance in any manner required. ■

Deadlines are Coming Up for SVS and SVS Foundation Honors, Awards & Scholarships
DEADLINE: FEBRUARY 27, 2019
• SVS General Surgery Resident/Medical Student Vascular Annual Meeting Travel Scholarship
• SVS Diversity Medical Student Vascular Annual Meeting Travel Scholarship
DEADLINE: MARCH 1, 2019
• SVS Lifetime Achievement Award
• SVS Medal for Innovation in Vascular Surgery
• SVS Distinguished Fellows Designation
• SVS Women’s Leadership Training Grant
• SVS Foundation Clinical Research Seed Grants
• SVS Foundation Community Awareness and Prevention Project Grant
• SVS Foundation E.J. Wylie Traveling Fellowship Visit: vsweb.org/Awards
Session by session, time slot by time slot, the 2019 Vascular Annual Meeting is coming together.
“Dr. (Vik) Kashyap and his Postgraduate Education Committee have finished selecting breakfast sessions and postgraduate courses, and the members are well on the way to finalizing workshops and concurrent sessions,” said Dr. Matthew Eagleton. He chairs the Program Committee, which oversees all the programming of the Vascular Annual Meeting.
Also selected, said Dr. Eagleton, are topics for most of the “Ask the Expert” sessions. These debuted in 2018 and were so popular that in some instances hopeful participants had to be turned away; additional sessions are slated for this year. “Attendees continue to tell us that they like the small-group setting and the chance to talk with the presenters,” Dr. Eagleton said.
“Particularly with the non-research-related events, we can respond both to feedback from the previous year and the suggestions and proposals for the current year in selecting subjects,” said Dr. Eagleton. “That helps us build a VAM program of interest to a wide range of participants.”

For example, the “Advanced Tools for Vascular Surgeon Wellness” breakfast session will tackle surgeon wellness and avoiding burnout. Those topics are so relevant and significant that SVS has a task force addressing them, said Dr. Eagleton.
Other requests for 2019 include:
• Scheduling workshops throughout VAM. This year’s workshops will on Thursday and Friday afternoons, instead of holding them all on Wednesday.
• The latest on issues vascular surgeons face frequently. “There’s a great demand for information on hemodialysis, for example, this year
and every year,” said Dr. Eagleton. “We’re responding with a breakfast session and other programming.”
• Programming specifically for Fellows.
• Career setting-specific gatherings. “The needs of our academic and hospital-based surgeons are different from those in private practice, and surgeons at the beginning of their careers face different challenges than those established practitioners face,” Dr. Eagleton said. “We need to, and will, meet a host of different needs, including career paths, practice management, even exit strategies.”
As for research, abstracts and vid-
June 12-15, at the Gaylord National Resort & Convention Center, National Harbor, Md., outside Washington, D.C.
Registration and housing open in early March.
Postgraduate Sessions: June 12
Scientific Sessions: June 13-15
Exhibits: June 13-14
Vascular Spectacular Gala: June 14
Visit vsweb.org/VAM19
eos were to be selected by the end of February for podium presentations: scientific sessions, the two VESS sessions, International Forum and International Fast Talk, plus the Poster Competition and the Interactive Poster Session.
“With each additional component identified and slotted, all of us involved with creating this year’s meeting are getting more excited,” said Dr. Eagleton. “It’s going to be a great, informative meeting. No matter what stage of career, from trainee to seasoned veteran, we’ll offer sessions of interest and value.
“Don’t miss it.” ■
Dr. Catherine Go had the opportunity last year to present her research at VRIC, answer questions about her work and talk collaboratively with others during the conference.
After her positive experience, she encourages other young researchers to attend this year’s Vascular Research Initiatives Conference with an eye toward submitting an abstract in 2020. (Abstract submissions are closed for this year’s VRIC, May 13, in Boston.)
Dr. Go, an integrated vascular surgery resident at the University of Pittsburgh Medical Center, was awarded an SVS Foundation VRIC Trainee Travel Scholarship to present at 2018 VRIC. She also received the SVS Foundation’s Student Research Fellowship in 2013. Her VRIC presentation was on “Retrograde Hemorrhage and Ischemic Injury after REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) in a Porcine Model of Uncontrolled Aortic Injury.”
She found that by “occluding the aorta, endovascular balloons lead to spinal cord ischemia and organ malperfusion.” This was a smaller
What: The 2019 VRIC: “Hard Science: Calcification and Vascular Solutions.”
When: Monday, May 13, at the Marriott Copley Square Hotel in Boston. VRIC is held the day before and in the same location as the American Heart Association’s Vascular Discoveries sessions.
Cost: Member, $275; nonmember, $300; resident/student/candidate (both member and nonmember): $150.
Highlights: Cecilia Giachelli, PhD, Professor and Chair, Department of Bioengineering at

part of a larger project to compare the REBOA balloon to a retrievable self-expanding “rescue” stent that she and her fellow researchers envi-
University of Washington, will present the 2019 Alexander W. Clowes Distinguished Lecture, “New Concepts in Regulation and Bioengineered Therapies for Vascular and Valvular Calcification.” This year’s Translational Session is “Hard Science: Calcification and Vascular Solutions.”
Abstract sessions: Aortopathies and novel vascular devices; vascular regeneration, stem cells and wound healing; mechanisms and advanced therapies for venous disease; atherosclerosis, arterial injury and diabetes.
sion using in aortic trauma patients.
“This was one my first experiences as a presenting author,” said Dr. Go. Mentor Dr. Bryan Tillman was invaluable to her success, she said. “He’s been very supportive, but also gives me the independence and confidence to answer discussion questions myself up at the podium, and that
Purchase tickets today for “Vascular Spectacular,” the elegant evening planned for Friday, June 14, at the Vascular Annual Meeting to benefit the SVS Foundation.
The ticket/donation website (vam19gala. givesmart) is now open. Members and friends may purchase their tickets there for the gala and, later, not only arrange to donate items for the Live Auction and Silent Auction but also peruse the listings to see if anything tickles their fancy. Bidding is expected to open sometime in May.
Attendees will enjoy cocktails and dinner, headliner entertainment, both Live and Silent auctions and an evening of conversation and fun with friends and colleagues. All proceeds will benefit
continued from page 13
allows me to showcase my contribution to the project.”
Mentorship is vitally important, said Dr. Tillman. Mentoring “promising clinicians, such as Dr. Go, in research is an essential foundation for future advances in the care of our patients,” he said. “The VRIC has been instrumental in promoting young talent in our vascular community, as well as to provide a forum to discuss issues that are both timely and unique to the field of vascular surgery.”
She enjoyed all parts of VRIC. “It’s a great place to collaborate with others,” she said, adding she especially enjoyed the people who approached her to discuss their own REBOA experiences. And because the engineering department at UPMC is integral to her research team, she liked hearing about other researchers’ partnerships.
The annual Translational Panel discussion – last year’s was “The Road to Entrepreneurship” – also stood out, she said. “That was a nice break: we discussed basic science and research, and then talked about translating that to the hospital or industry.” This year’s topic is “Hard Science: Calcification and Vascular Solutions” – identical to the VRIC meeting theme – with time for audience input into the crippling disease.
As for this year, Dr. Go continues her research and hopes to continue her presentations. She has submitted an abstract for VRIC – and also for the Vascular Annual Meeting in June. ■
the SVS Foundation and the community initiatives, research, scholarships, grants and disaster relief it helps fund. Tickets to the Vascular Spectacular are $250, $150 of which is a tax-deductible donation to the SVS Foundation.
Anyone can register to participate in the Silent Auction via the website, vam19gala.givesmart com. When bidding opens, bids will be updated in real time and high bidders will be notified when their bids are topped. “This lets all of our members, colleagues and friends be part of the excitement of ‘Vascular Spectacular,’ “ said Cynthia Shortell, MD, gala co-chair with Benjamin Starnes, MD. “While we at VAM will be on the East Coast, anyone – on the West Coast or an-
other part of the world – can still participate in the Silent Auction.”
Silent Auction bidding will end during the evening. Because of the rapid pace of live auctions, only those present can participate in that. “But anyone who wants to can view the items ahead of time, and arrange bidding with a friend,” Dr. Shortell advised. “You might come away with something remarkable.”
Both co-chairs are excited about the evening. “It will bring people together on the final evening of VAM to not only have a wonderful time but also to showcase and benefit the important work of the SVS Foundation,” said Dr. Shortell. “It’s going to be spectacular.” ■
Young Erben, MD, has fully embraced SVS membership, joining an SVS committee and actively taking advantage of the benefits SVS offers.
March 1 is the first quarterly membership application for 2019. Dr. Erben urges all who are eligible to apply and enjoy the boost that membership can provide a career. For example:
“The most important thing is the fact that we get to see and interact with a lot of colleagues,” said Dr. Erben, who became an Active member in 2018. “We recognize each other; we’re constantly communicating with each other. It helps to know there are fellow members, who are devoted to the field and are part of the community.”
The ability to encourage younger people and get them engaged: Dr. Erben is a member of the Resident and Student Outreach Committee, which participates in the student/resident/fellowship activities during the Vascular Annual Meeting. Committee members assist with the simulation activities and in the forums that help coach students on interviewing and other career development necessities.
This work is important, she said. “We’re encouraging young people, helping to disseminate information and get them engaged early on.”
Mentorship and applications: Most members would cite mentorship as an important factor in

going into the field of vascular surgery, she said. “It’s crucial. The right mentorship attracts students and gets them to be engaged, active members of the community, and that’s what keeps our Society running and advancing the science in vascular care,” she said.
Her mentors all are SVS members, she said. “They encourage their residents to go into vascular surgery,” she said. “As a resident, you want to emulate these members – you know your mentors are good people and excellent members developing guidelines for the care of our patients. You WANT to become a member and be a positive contributor to the field.”
Scholarships, plus leadership and training opportunities, such as the Women’s Leadership Training Grant: Dr. Erben applied last summer for and received an SVS Foundation Research Career Development Travel Award. “The beauty of being a member is that
you get all of these opportunities to improve yourself and get better,” she said. Being a practicing vascular surgeon means constant continuing education. “These opportunities are available to all members,” said Dr. Erben. “It’s silly not to take advantage of them.”
She’s considering the Women’s Leadership Training Grant, believing it important not only to encourage women to go into vascular surgery and also take on leadership roles. “If a woman sees only males, they think, ‘This is not for me.’ They don’t see role models they can relate to,” she said “SVS is actively encouraging our women to take on leadership roles.
“It’s an amazing opportunity,” she added.
Take advantage of all SVS has to offer. Visit vsweb.org/Join for more information. Deadlines for 2019 are March 1, June 1, Sept. 1 and Dec. 1. ■


Patients 75 years and older may present a myriad of challenges. CEA may not be the best option. With thousands of real world patients studied, TCAR has shown to be a safe and clinically effective alternative to CEA.
Other patients who could benefit from carotid revascularization through robust reverse flow include:*
• AGE ≥75
• CONGESTIVE HEART FAILURE
• ≥2 DISEASED CORONARIES WITH ≥70% STENOSIS
• SEVERE PULMONARY DISEASE
• SURGICALLY INACCESSIBLE LESION
• PRIOR HEAD/NECK SURGERY
• RESTENOSIS POST CEA
• IRRADIATED NECK
• CONTRALATERAL OCCLUSION
• BILATERAL STENOSIS REQUIRING TREATMENT
• SEVERE TANDEM LESIONS
*Reimbursement eligible criteria for the TCAR Procedure per the Medicare National Coverage Determination (20.7) on PTA including CAS
Please visit
for instructions for use and to learn more about TCAR
The Society for Vascular Surgery welcomes the following new members, who joined in 2018.
Active Members
Jessica Secor, MD; Dunlap, IL
Michael Madigan, MD; Pittsburgh, PA
Daniel Alterman, MD, RPVI; Muskegon, MI
Luis Antonio Lopez Galarza, MD; Manati, PR
William B. Harris, DO; Fort Sam Houston, TX
Charles Bailey, MD; Brandon, FL
Kevin Brown, MD; Bethesda, MD
Christopher Busken, MD; San Antonio, TX
Jonathan Cardella, MD; New Haven, CT
Sherry Cavanagh, MD, RPVI; Flint, MI
Jason Chapman, MD; Macon, GA
Allan Conway, MD; New York, NY
Ajay Dhadwal, MBBS; Jersey City, NJ
Young Erben, MD; New Haven, CT
Edgar Galinanes, MD; Miami, FL
Matthew Goldman, MD; Winston Salem, NC
Claire Griffin, MD; Salt Lake City, UT
Angela Gucwa, MD; Lanham, MD
George Hipp, MD; Vestavia, AL
Kamran Jafree, MD; Dayton, OH
Mila Ju, MD, MS; Allentown, PA
Vijay Kamath, MD,; Brown Mills, NJ
Sarah Koch, MD; Tacoma, WA
Jared Kray, DO; Cedar Rapids, IA
Lidie Lajoie, MD; Washington, DC
Chandler Long, MD; Durham, NC
Sarah Lucas, MD; Memphis, TN
Greg Magee, MD, MSc; Los Angeles, CA
Megan March, MD; Daytona Beach, FL
Katherine McGinigle, MD, MPH; Chapel Hill, NC
R Michael Patton, MD; Wilmington, NC
Shardul Nagre, MD; Kingsport, TN
Zachary Osborne, MD; Urbana, IL
Eugene Palchik, MD; Syracuse, NY
Karen Quirk, MD; Oxnard, CA
Elena Rinehardt, MD; Bellevue, WA
Adam Ring, MD; Saint Louis, MO
Melanie Rose, MD; Mobile, AL
Michael Rosenbaum, MD; Cleveland, OH
Hossain Said-Mahmoudian, MD; Salisbury, MD
Noah Scherrer, MD; Lousiville, KY
Mark Song, MD; Brooklyn, NY
Emily Spangler, MD; Birmingham, AL
Michael Stephen Williams, Jr., MD; St. Louis, MO
Jordan Stern, MD; Mountain View, CA
Joseph Stinson, MD; Tupelo, MS
Scott Sundick, MD; Springfield, NJ
Pedro Teixeira, MD; Austin, TX
Axel Thors, DO, RPVI; Overland Park, KS
Ellis Tinsley, MD, Wilmington, NC
Samuel Tyagi, MD; Lexington, KY
Joshua Unger, MD; Miami Beach, FL
Matthew W. Lawrence DO; Philadelphia, PA
Douglas W Jones, MD; Boston, MA
Marlin Wayne Causey, MD; San Francisco, CA
Jonathan Wilson, DO; North Kansas City, MO
Affiliate Members, PA Section
Lauren Alstot, PA-C; Clackamas, OR
Jo Ann Eisinger, PA; Lake Success, NY
Eric Barth, PA-C; St. Paul, MN
Ashley Bays PA-C; Kalamazoo, MI
Bryon Brown, PA-C; Charleston, SC
Chrystal Buchanan, PA-C; Tacoma, WA
Jennifer Czarniak, PA-C, MHP; Mash-
pee, MA
Rachel Dresher Gurr, PA-C; Murray, UT
Sarah Finke-Fyffe, PA-C; Northfield, IL
Daniel Forsberg, PA-C, MPH; Roslyn, NY
Rocelious Goodson III, PA-C; Royal Oak, MI
Jill Gulliford, PA-C, MPH; Fairfield, CT
Peggy Hall-Curci, PA-C; Nashville, TN
Stacy Henderson, PA-C; Danbury, CT
Christina Hopps, PA-C; Grand Rapids, MI
Kierney Jackson, PA-C; Athens, GA
Samantha Jones, PA-C; Hattiesburg, MS
Jessica Kinnell, PA-C; Detroit, MI
David Lund, PA-C; Salt Lake City, UT
Brittany Macdonald, PA-C; Denver, CO
Keri Minton, PA-C; Atlanta, GA
Sarah Montanez, PA-C; Denver, CO
Sherri Morrison, PA-C; Champaign, IL
Sebastien Nantermet, PA-C; Wynnewood, PA
Benson Phillip, PA-C; Bronx, NY
Madelena Pimentel, PA; Salt Lake City, UT
Ruth Pinkerton, PA-C; Dallas, TX
Laura Prince, PA-C; Salt Lake City, UT
Steven Savoy, PA-C; Tupelo, MS
Angel Segura, PA; Walnut Creek, CA
Anna Singur, PA-C; Tacoma, WA
Robert Skasko, PA-C; Wilkes-Barre, PA
Kimberly Skinner, PA-C; Charlotte, NC
Illiana Suero, PA-C; Salt Lake City, UT
Iris Swiderski, PA-C; Middletown, NY
SVS is accepting nominations and applications through March 1 for its three highest honors, to be recognized at the 2019 Vascular Annual Meeting in June.
The SVS Lifetime Achievement Award recognizes an individual’s outstanding and sustained contributions to the profession and SVS as well as exemplary professional practice and leadership.
The SVS Medal for Innovation in Vascular Surgery honors individuals whose contributions have transformed the practice or science of vascular surgery.
The Distinguished Fellow Designation recognizes members who have provided sustained contributions to vascular surgery through research, teaching, clinical and/or creative accomplishments.
Annsley Troxell, PA-C; Beaufort, SC
Emose Voltaire-Piou, PA; Boston, MA
Amanda Waugh, PA-C; Colorado Springs, CO
Cheryl Weinstein-Shama, RPA-C; Brooklyn, NY
Affiliate Members
Kenneth Becht, APRN; Louisville, KY
Emmie Butterworth, CRNFA; Henrico, VA
Louie Garcia, NP; Torrance, CA
Aubrey Harman, ARNP; Orlando, FL
Ansley Holland, APRN; Tulsa, OK
Tina Mathew, APRN; Maywood, IL
Pierre McKenzie, CNP; Albuquerque, NM
Melissa McPhail, NP; Macon, GA
Jacquelyn Paige, MSN, RN, AGACNP-BC; Altadena, CA
Catherine Ratliff, PhD, GNP-BC, CWOCN, CFCN; Charlottesville, VI
Shelby Rogers, DNP, FNP-C; Memphis, TN
Lily Toy, NP; Burlingame, CA
International Members
Alexandre Bueno Silva, MD; Rio Grande do Sul, Brazil
Manuel Doblas, MD; Toledo, Spain
Dale Maharaj, MD; Port of Spain, Trinidad
Juan Paolini, MD; Buenos Aires, Argentina
Juan Pardo, MD; Buenos Aires, Argentina
Felipe Trajano de Barao, PhD; Sao Paulo, Brazil
Kak Khee Yeung, MD, PhD; Amsterdam, Netherlands
Associate Member
Brent Haverstock, MD; Birmingham, AL
A number of SVS and SVS Foundation awards also carry March 1 application dates. They are: the SVS Women’s Leadership Training Grant and the SVS Foundation Community Awareness and Prevention Project Grant, E.J. Wylie Traveling Fellowship and Clinical Research Seed Grant.
Visit vsweb.org/Awards for more award information. ■
From JVS: Researchers believe metformin, a commonly used prescribed oral hypoglycemic agent, may limit enlargement of abdominal aortic aneurysms, after analyzing patients of diabetic patients who are being treated in the U.S. Department of Veterans Affairs. The findings, outlined in an opensource article in the March Journal of Vascular Surgery, support holding clinical trials to test the drug’s effectiveness in limiting progression of early AAA disease. Read more through April 30 at vsweb.org/ JVSVL-EVToveruse.
From JVS-VL: A recent retrospective study showed that vascular surgeons accounted for 22.6 percent of specialists performing endovenous therapy among Medicare patients from 201214. However, the largest percentage of providers (29.7 percent) was comprised of non-surgical specialties or specialists not generally associated with vascular procedures. The study, according to the article in the March JVS-Vascular and Lymphatic Disorders, “raises the question of financially driven, potentially inappropriate utilization of EVT.” Read more free through April 30 at vsweb.org/JVS-Metformin. ■

Michael Daniel Sulkin, 79, Dec. 20, 2018. Dr. Sulkin founded one of the largest vascular surgery practices in Maryland and enjoyed a distinguished medical career in surgery that spanned 40-plus years. He was a constant advocate of innovative procedures and techniques to enhance patient care.
Do you know of an SVS member who has passed away? Please let us know at communications@ vascularsociety.org. ■
T
he SVS’ Affinity Program of expanded benefits can help members protect their businesses, practices, families and future.
SVS launched the portfolio of financial and practice surgeons two years ago, providing members pre-vetted products and services. Members get a special discount on nearly every one of them.
Most SVS members tend to concentrate on three particular offerings: medical malpractice insurance, dis-
ability insurance and the retirement accelerator program.
Medical Malpractice Insurance: The Affinity Program offers professional liability insurance with a 5% discount through MedPro; the company said its claims team wins 90 percent of all physician malpractice trials. In addition, MedPro will not settle any case without the physician’s consent, offers free tail coverage for physicians at retirement Benefits continued on page 18



Connected that is, via SVSConnect, the Society for Vascular Surgery’s new online members-only community. There, members can post discussions, respond to others’ questions, collaborate and expand their professional networks.
SVSConnect opened in December and has enjoyed many robust conversations since then, on topics ranging from burnout, electronic health records, to

insurance company issues and many practice-oriented questions, such as those on imaging.
To be part of SVSConnect, visit vsweb.org/SVSConnect ■
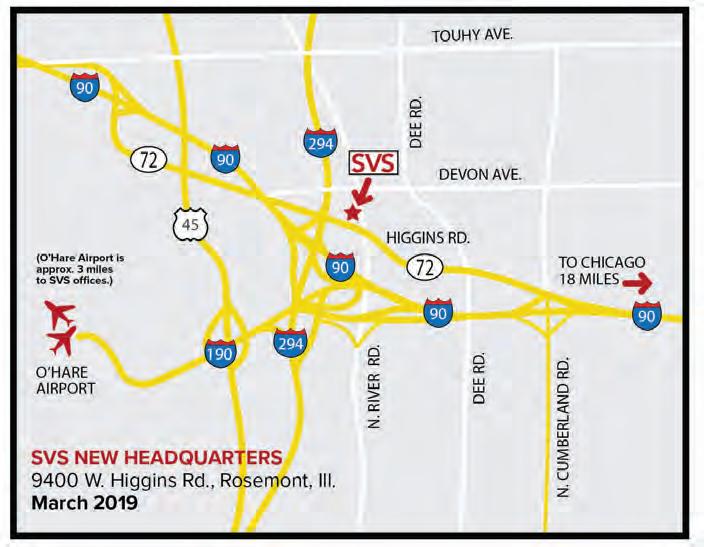
By the end of this month, the Society for Vascular Surgery will be working out of its new headquarters in Rosemont, Ill., just minutes from O’Hare International Airport.
The SVS Foundation and the SVS Patient Safety Organization share SVS’ workspace. The Society also provides management services for the Association of Program Directors in Vascular Surgery, the Society for Vascular Nursing and the Delaware Vascular Society.
The new space is nearly twice the size of the current main office in Chicago. It has room for expansion and additional programming to meet the future needs of vascular surgeons, including ongoing training. Its location near O’Hare is convenient for meeting attendees and will eliminate the need to rent meeting room
continued from page 17
Note Our New Address, as of Feb. 22
9400 W. Higgins Road Suite 315 Rosemont, Ill., 60018
space near the airport, as has been routine for many years.
The new headquarters also includes access to a surgical simulation center where surgeons can hone their skills on the latest endovascular procedures and maintain their open surgery skills.
SVS will show off its new headquarters in photos in the March Vascular Specialist, as well as in Pulse and on the SVS website. Be sure to check out our new look! We’re proud of our new space and can’t wait for members to see it as well. ■
after just one year of insurance and is addressing emerging issues such as cyber liability and optional coverage for billing errors and omissions.
Disability Insurance: More than one disability income protection program is available. Critical factors to consider include: whether benefits are
Coming soon to SVSConnect
The SVSConnect mobile app, bringing SVSConnect to phones and tablets “Mentor Match”capability Additional discussion groups
taxed or not, recognition of medical specialties and subspecialties, plan portability and renewability and whether rates are locked in at enrollment. The tax-free benefits have no offsets from other income and enrollees are protected as a vascular surgeon. Discounts apply for members.
Retirement Protection: Kai-Zen essentially accelerates retirement income, with participant funding complete in five years. The unique product combines financing and life insurance, with funds

growing tax-deferred. The policy repays the loan at the end of 15 years and is the ONLY collateral for the loan. The plan uses a life policy which has a zero percent floor, meaning contributions are protected, and it is portable unlike a 457 plan. The plan has money available for long-term care and death benefits.
Other products address needs across the spectrum. For individuals, offerings include high net-worth life insurance, identity theft protection insurance, dental and vision care discounts, international medical insurance, student loan consolidation and high-limit disability income protection.
Offerings for practices include help with payroll, 401K programs and workers’ compensation insurance; payment processing; business overhead expense insurance; guarantee issue life and disability insurance for employees; business cybercrime protection; simplified issue life insurance; guarantee issue to group practices; and employee dental and vision care discounts.
For more information, visit vsweb.org/AffinityProgram, call 312-291-4472 or email Mark Blocker, SVS program representative, at mark@ nationalaffinity.net ■
BY BIANCA NOGRADY MDEDGE NEWS
FROM JAHA: JOURNAL OF THE AMERICAN HEART ASSOCIATION
Women who have a healthier lifestyle during the menopausal transition could significantly reduce their risk of cardiovascular disease, new research suggests.
Because women experience a steeper increase in CVD risk during and after the menopausal transition, researchers analyzed data from the Study of Women’s Health Across the Nation (SWAN), a prospective longitudinal cohort study of 1,143 women aged 42-52 years. The report is in JAHA: Journal of the American Heart Association.
The analysis revealed that women with the highest average Healthy Lifestyle Score – a composite score of dietary quality, levels of physical activity, and smoking – over 10 years of follow-up had a 0.024-mm smaller common carotid artery intima-media thickness and 0.16-mm smaller adventitial diameter, compared to those with the lowest average score. This was after adjustment for confounders and physiological risk factors such as ethnicity, age, menopausal status, body mass index, and cholesterol levels.
“Smoking, unhealthy diet, and lack of physical activity are three wellknown modifiable behavioral risk factors for CVD,” wrote Dongqing Wang of the University of Michigan, Ann Arbor, and his coauthors. “Even
Audible Bleeding Podcast

after adjusting for the lifestyle-related physiological risk factors, the adherence to a healthy lifestyle composed of abstinence from smoking, healthy diet, and regular engagement in physical activity is inversely associated with atherosclerosis in midlife women.”
Women with higher average health lifestyle score also had lower levels of carotid plaque after adjustment for confounding factors, but this was no longer significant after adjustment for physiological risk factors.
The authors analyzed the three components of the healthy lifestyle score separately, and found that not smoking was strongly and significantly associated with lower scores for all three measures of subclinical atherosclerosis. Women who never smoked across the duration of the study had
Audible Bleeding is a new podcast from the Vascular Surgery Fellowship Program at New York Presbyterian – Cornell / Columbia. Recent episodes have featured Frank Veith, Thomas Forbes, and Vascular Specialist Medical Editor Malachi Sheahan. Available through Apple, Spotify, and Google. www.audiblebleeding.com.
Upcoming Meetings
Charing Cross Symposium
The Charing Cross Symposium will be held Apr. 15-18, 2019, in London. The symposium assembles a
a 49% lower odds of having a high carotid plaque index compared with women who smoked at some point during the follow-up period.
The analysis showed an inverse association between average Alternate Healthy Eating Index score – a measure of diet quality – and smaller common carotid artery adventitial diameter, although after adjustment for BMI this association was no longer statistically significant. Likewise, the association between dietary quality and intima-media thickness was only marginally significant and lost that significance after adjustment for BMI.
Long-term physical activity was only marginally significantly associated with common carotid artery intima-media thickness, but this was not
world-class faculty to address key issues in vascular and endovascular treatment and to challenge the available evidence in order to reach a consensus after discussion with an expert audience.
The Congress is being held at the Lowes Miami Beach hotel, Miami Beach, Fla., on Apr. 25-27, 2019. This CME event covers the treatment of superficial and deep venous disease, including topics from sclerotherapy optimization to managing thrombophilias and discussing clot bursting strategies.
significant after adjustment for physiological risk factors. No association was found between physical activity and common carotid artery adventitial diameter or carotid plaque.
The authors said that 1.7% of the study population managed to stay in the top category for all three components of healthy lifestyle at all three follow-up time points in the study.
“The low prevalence of a healthy lifestyle in midlife women highlights the potential for lifestyle interventions aimed at this vulnerable population,” they wrote.
In particular, they highlighted abstinence from smoking as having the strongest impact on all three measures of subclinical atherosclerosis, which is known to affect women more than men. However, the outcomes from diet and physical activity weren’t so strong: The authors suggested that BMI could partly mediate the effects of healthier diet and greater levels of physical activity.
One strength of the study was its ethnically diverse population, which included African American, Chinese, and Hispanic women in addition to non-Hispanic white women. However, the study was not powered to examine the impacts ethnicity may have had on outcomes, the researchers wrote.
The Study of Women’s Health Across the Nation is supported by the National Institutes of Health. No conflicts of interest were declared.
SOURCE: Wang D et al. J Am Heart Assoc. 2018 Nov 28. doi: 10.1161/ JAHA.118.010405.
LESIONS ACROSS THE ELBOW
Thrombosed AV grafts
Complex iliac lesions
In-stent restenosis of the SFA
PTA failures of AV graft lesions
Long SFA lesions
Chronic total SFA occlusions





Physicians are achieving durable outcomes across the elbow with fewer reinterventions in rapidly failing AV access circuits. See the NEW case study at goremedical.com/viabahn/elbow
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® Endoprosthesis is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery de novo and restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 –7.5 mm, in superficial femoral artery in-stent restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 6.5 mm, and in iliac artery lesions up to 80 mm in length with reference vessel diameters ranging from 4.0 – 12 mm. The GORE® VIABAHN® Endoprosthesis is also indicated for the treatment of stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous (AV) access grafts.
CONTRAINDICATIONS: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is contraindicated for noncompliant lesions where full expansion of an angioplasty balloon catheter was not achieved during pre-dilatation, or where lesions cannot be dilated sufficiently to allow passage of the delivery system. Do not use the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface in patients with known hypersensitivity to heparin, including those patients who have had a previous incidence of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at goremedical.com for a complete description of all warnings, precautions and adverse events. Only
Images courtesy of Minneapolis Vascular Physicians. Used with permission. W. L. Gore & Associates, Inc. | Flagstaff, AZ 86004 | goremedical.com Products listed may not be available in all markets.
®, VIABAHN®, and designs are trademarks of W. L. Gore & Associates. © 2018 W. L. Gore & Associates, Inc. AX1547-EN1 DECEMBER 2018