Malachi Sheahan III, MD, on 'Marriage and other things I'm probably doing wrong'
6 Interview
14 Society briefs Legislation targets stability amid Medicare cuts In this issue:
Jean Panneton, MD, discusses the aortic surgery landscape and the state of training
POSITIVE ONEYEAR DATA FOR NEW VENOUS VALVE PORTENDS PROMISING FUTURE IN
CHRONIC VENOUS INSUFFICIENCY TREATMENT
SAVVE trial principal investigators discuss results showing 98.4% VenoValve device patency, 85% clinically meaningful benefit and an 80% rate of ulcer size reduction at 12 months.
By Bryan Kay
12 Corner Stitch Resident unionization: Could it be a step toward equity in healthcare training?
VASCULAR TRAINEES BETTER PREPARED FOR OPEN AORTIC PRACTICE THAN COMMONLY REPORTED, NEW STUDY SHOWS
By Bryan Kay
CURRENT GRADUATES FROM both vascular surgery residency and fellowship programs are well prepared for surgical practice in aortic disease whether they are performing open repair or endovascular therapy, contrasting with research indicating that trainees are entering the workforce with inadequate experience of open aortic repair. That is the main finding of a new study set to be presented at the 2025 annual meeting of the Southern Association for Vascular Surgery (SAVS) in St. Thomas, the U.S. Virgin Islands (Jan. 22–25).
The analysis of Accreditation Council for Graduate Medical Education (ACGME) reports from 2013–2023 adds a counterweight to the increasingly accepted wisdom that current vascular fellows are graduating with less than five open abdominal aortic aneurysm (AAA) repairs on their docket when they complete training, according to senior author Young Kim, MD, an assistant professor of surgery at Duke University School of Medicine in Durham, North Carolina.
Crucially, Kim highlighted that trainee experience was robust across the breadth of open aortic cases, not only those which involve aneurysm repair.
“An open aorta is an open aorta, whether it is for occlusive disease or an infected aorta,” he tells Vascular Specialist
“There are a lot of very similar principles between the different types of aortic operations, but the well-cited study quoting the five-open-aortas statistic pertained only to open AAA repairs, and that was back in 2014, and looked at Medicare beneficiaries.”
Young and colleagues found
See page 6
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS
| Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Manager of Marketing
Kristin Spencer
Communications Specialist
Marlén Gomez
SVS Consultant
Beth Bales
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Global Sales Director Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America 155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. | The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. | Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. | Printed by Ironmark |
Marriage and other things I’m probably doing wrong
By Malachi Sheahan III, MD
Imet my wife, Claudie, at the Harvard Medical School vascular re search lab. This was not a romantic environment by most standards (depending, I suppose, on your Many of the researchers were gen eral surgery residents invigorated by this temporary reprieve from the horrors of their (pre-80-hour work week) training programs.
My friend Evan Deutsch pinned a map of Oslo above his desk, letting the other poseurs know who was destined for greatness. But, as the kids say, we were all NPCs (nonplayer characters) living in Claudie’s story. She would roll in around noon, latte in hand, opining on her selfdiagnosed insomnia. I once considered suggesting that she would fall asleep more easily if she simply woke up earlier. It was never my sense, however, that she was seeking enlightenment.
Everyone knew not to book the conference room over lunch, as that was Claudie’s time to spread out the current issue of the Boston Globe carefully consider the new shoe offerings at Filene’s. My predominant feeling towards Claudie during this time was jealousy. As the clinical fellow, I had minimal time in the lab and needed to focus on boring database research. Claudie, however, had the prize project: a study of the effects of stem cells on intimal hyperplasia. But this was 2003, and we had not learned how to make those pesky stem cells stick to the endothelium. With her research time dwindling, Claudie needed to get a few projects to the finish line. So, as PubMed can attest, our relationship began studying minor amputations and bypasses in transplant patients. Who needs romance?
spurred my interest in looking at the data behind surgeon marriages. Matt was preparing a talk on the topic and asked if we had any insight or advice. Matt also made the mistake of asking for a picture of the two of us, not knowing that my wife guards these with the determination of a North Korean press secretary. After reviewing her photo selections, it appears Claudie’s criteria are that she is wearing something she likes, and I look like the cover of The Complete Idiot’s Guide to Looking Like a Doofus
Surgeons marrying surgeons is a relatively recent occurrence. Halstead’s original residents were required to be single males. Like Catholic priests, they were bonded to their vocation. Marriage between surgeons has become much more common as more women enter the surgical workforce. According to census data, about 25% of physicians are married to another doctor. The divorce rate among these pairings is around 25%, which trails the 35% seen in the general population.
A 1997 study of Johns Hopkins graduates found the specialties with the highest rates of divorce were psychiatry (50%!) and surgery (33%).
A 2008 American College of Surgeons (ACS) survey found that surgeons in dual-physician relationships experienced a higher incidence of career and work-home conflicts. This led to more depressive symptoms and a lower mental quality
Among U.S. medical school surgery faculty, 40% of women and 29% of men have an academic physician partner. These couples are generally more productive, with higher numbers of publications and more leadership positions. They are also seen as more stable with longer tenure, likely because leaving would require finding two new opportunities.
On average, female physicians interrupt their careers for 8.5 months for child rearing, while, for men, it is less than four weeks. Unsurprisingly, male physicians have significantly more children than females.
Female doctors who marry other physicians report working fewer hours and having more children. The tradeoff appears to be that they earn less money and are more likely to report that their family life substantially limited their professional life. In the end, though, female physicians married to other doctors do not report less success in achieving their career goals.
The prospect of marrying another physician was terrifying. How would this all work? At the time, there weren’t even many women in vascular surgery, never mind married couples. Claudie never seemed hesitant, though. I thought, well, she is incredibly bright and seems always to have a plan; she must have thought this through. Well reader, she had not. Twenty years later, it has been a life of complications. A life of extremes. And, primarily due to my chosen spouse, a life of insane, unforced financial peril. But despite my decades of experience, I am definitively not an expert in physician marriages. My insight is more akin to one of my patients with a 9.5cm aneurysm. I don’t really know what is happening, but it’s probably going to kill me.
A few months ago, my friend and SVS President Matt Eagleton
I have spent a good portion of the last decade studying the effects of burnout on surgeons. At the beginning of our careers, most of us perseverate over life choices such as where to live, what type of employment to seek, and when to have children. I am now convinced that the two most important decisions are your spouse and your work partners. Nail both choices and the rest tend to sort themselves out.
Surgeon-surgeon marriages will continue to grow in popularity as we change the demographics of our workforce. For now, though, the data is relatively limited. So, for the next issue, I have assembled an all-star team of married surgeons to offer advice, guidance and safety tips. Until then, please enjoy your holidays, and thank you for all of the interaction this year (even the haters!).
MALACHI SHEAHAN III is Vascular Specialist medical editor.
Claudie and Malachi Sheahan
HOW PHYSICIAN ASSISTANTS HELP VASCULAR SURGERY TEAMS PROVIDE ‘CONTINUITY OF CARE’
By Bryan Kay
THE KEY ROLE PLAYED BY PHYSICIAN ASSISTANTS (PAs) as part of vascular surgery teams in the U.S. came into focus during the Vascular Societies’ Annual Scientific Meeting in Brighton, England.
Julie Ann Freischlag, MD, the former Society for Vascular Surgery (SVS) president and current CEO of Atrium Health Wake Forest Baptist in Winston-Salem, North Carolina, outlined how the integration of PAs had positively impacted vascular practice over the course of the last couple of decades during a President’s Symposium session on multi-professional teams.
have helped across a number of fronts, with impacts made across areas such as patient length of stay and the length of time residents spend in the operating room (OR).
Freischlag provided attendees with a rundown of lessons learned during her career—from the point at which PAs were not part of the picture of vascular surgical practice, through the advent of the 80-hour work week limit for residents in training and their subsequent incorporation into the heart of surgical services and research.
For Freischlag, PAs entered the scene while she was practicing at Johns Hopkins in Washington, D.C., where an early PA surgical program was developed and rolled out.
Fast forward 20 years, and now at Wake Forest, she said PAs
By Beth Bales
FIVE PROMINENT VASCULAR
surgeons have been named “at-large” members of the SVS Executive Board (EB), which has been newly restructured and expanded to increase diversity of perspective and better meet the Society’s evolving needs.
They are Chelsea Dorsey, MD, Yazan Duwayri, MD, Katherine Gallagher, MD, Vikram Kashyap, MD, and Robert Molnar, MD. All are involved SVS members, leading education or policy initiatives, serving as committee or section members and chairs, and performing other roles.
The expansion is the result of a bylaws referendum in 2023 that received strong support from the membership to change the board’s structure and composition. The new at-large positions expand the Executive Board from nine to 11 members and replace three “designated” positions.
“This completes an initiative begun by the Executive Board in 2019 to examine the governance structure of the SVS and make adjustments to meet the changing and growing needs of our members and the Society,” said SVS President Matthew Eagleton, MD.
An open call for nominations resulted in 45 applications that were reviewed by the SVS Nominating Committee.
At present, Freischlag pointed out, some 3% of PAs work in general surgery, with about 18.7% operating in the surgical subspecialties. “When I moved from Hopkins to UC Davis and I was doing my first case—involving a thoracic outlet—my PA was talking to my really young partner about how to assemble the retractor and how to take care of that patient,” she reflected. “PAs who have worked with me on thoracic outlet can assess and treat and take care of postoperative patients as well as I can.”
She highlighted how she sees much more “continuity of care,” with improvements seen in care coordination and patients’ ability to navigate the healthcare system. “We do simulation in virtual encounters, working through scenarios together, so not only do the patients go through what they do when they get to the hospital but we do all this before they even show up so they are used to many different types of people around the bed, around the OR table,” Freischlag added.
The committee then presented its recommendations to the Executive Board for consideration and final approval. Considerations included, among others, merit and achievement, qualifications, proficiencies, and gaps in expertise on the EB as identified by the SVS’ Strategic Board of Directors.
Chelsea Dorsey
Dorsey is an associate professor in the Section of Vascular Surgery and Endovascular Therapy at the University of Chicago Medicine. She serves as associate dean for medical student academic advising and advancement at the Pritzker School of Medicine and as vice chair in the Department of Surgery.
Her research interests include workforce diversity in surgery, augmentation of inclusive practices in the surgical environment and optimizing academic resources for diverse learners in the undergraduate medical education space.
Yazan Duwayri
Duwayri is a professor of surgery at Emory University School of Medicine and is codirector of the Emory Aortic Center. He leads his institution’s participation in several aortic device trials as the site principal investigator. Since April, he has been the chief for the Division of Vascular Surgery and Endovascular Therapy at Emory Healthcare.
To be able to safely and efficiently perform their roles in vascular surgery teams, PAs must satisfy heavy requirements that include 2,000 hours of supervised clinical practice. Freischlag also zeroed in on another dimension where their impact is felt: in the context of social determinants of health and health equity. She used an example from her own time as a resident to illustrate the PA effect, explaining how, while working at the VA, “we used to double book patients because many didn’t show up and we didn’t understand that it was mainly because of their social determinants.” Now, as PAs help patients navigate often labyrinthine health systems and with their ability to attend, those issues are being better tackled. “PAs, NPs [nurse practitioners], all of us need to know those impediments to care,” Freischlag noted.
Ultimately, she said, how PAs fit into vascular surgery teams might differ but “continuity throughout the perioperative period decreases complications and increases patient satisfaction, and that’s what is so important.”
“Continuity throughout the perioperative period decreases complications and increases patient satisfaction, and that’s what is so important”
JULIE ANN FREISCHLAG
His current research focus is outcomes and quality improvement in vascular surgery. He has held national leadership positions in the SVS, including as a member of the executive council of the SVS Patient Safety Organization. He also served as medical director of the Southeastern Vascular Study Group (SEVSG), which is dedicated to tracking outcomes and improving the quality of vascular surgical interventions.
Katherine Gallagher
Gallagher is professor of surgery, professor of microbiology and immunology and vice chair of basic and translational science in the Department of Surgery at the University of Michigan. She is an expert in the molecular pathogenesis of wound repair and has contributed substantially to the understanding of epigenetics in immune cells associated with tissue repair, cardiovascular diseases, sepsis and, most recently, COVID-19. Her research has been supported by multiple grants. In addition to memberships in several associations, Gallagher is a mentor to junior faculty and trainees in medical research and has trained many postdoctoral residents to be the next generation of scientists.
Vikram Kashyap Kashyap is the endowed chair of the Frederik Meijer Heart and Vascular Institute and the vice president for Cardiovascular Health
at Corewell Health in Grand Rapids, Michigan. He formerly worked at the Cleveland Clinic for nearly 20 years, including as chief of the Division of Vascular Surgery and Endovascular Therapy and the co-director of the Vascular Center of the Harrington Heart & Vascular Institute at University Hospitals Cleveland Medical Center, Cleveland, Ohio.
He is principal investigator of several clinical studies of new vascular stents, grafts and prostheses. He leads a national trial on transcarotid artery revascularization (TCAR).
Robert Molnar
Molnar is based in Flint, Michigan, and is a member of the Michigan Vascular Center, one of the oldest private practice vascular surgery groups in the U.S.
Molnar is past chair of the SVS Clinical Practice Section and SVS Subsection of Outpatient and Office Vascular Care (SOOVC), a clinical professor in the Michigan State University Department of Surgery, associate program director of the University of Michigan Health-Sparrow general surgery residency, chair of the Department of Surgery and director of surgical education at McLaren Regional Medical Center, and faculty member of the McLaren vascular fellowship program.
Molnar has been active in clinical research, including being local principal investigator in more than 70 national clinical trials conducted at his facility.
Julie Ann Freischlag
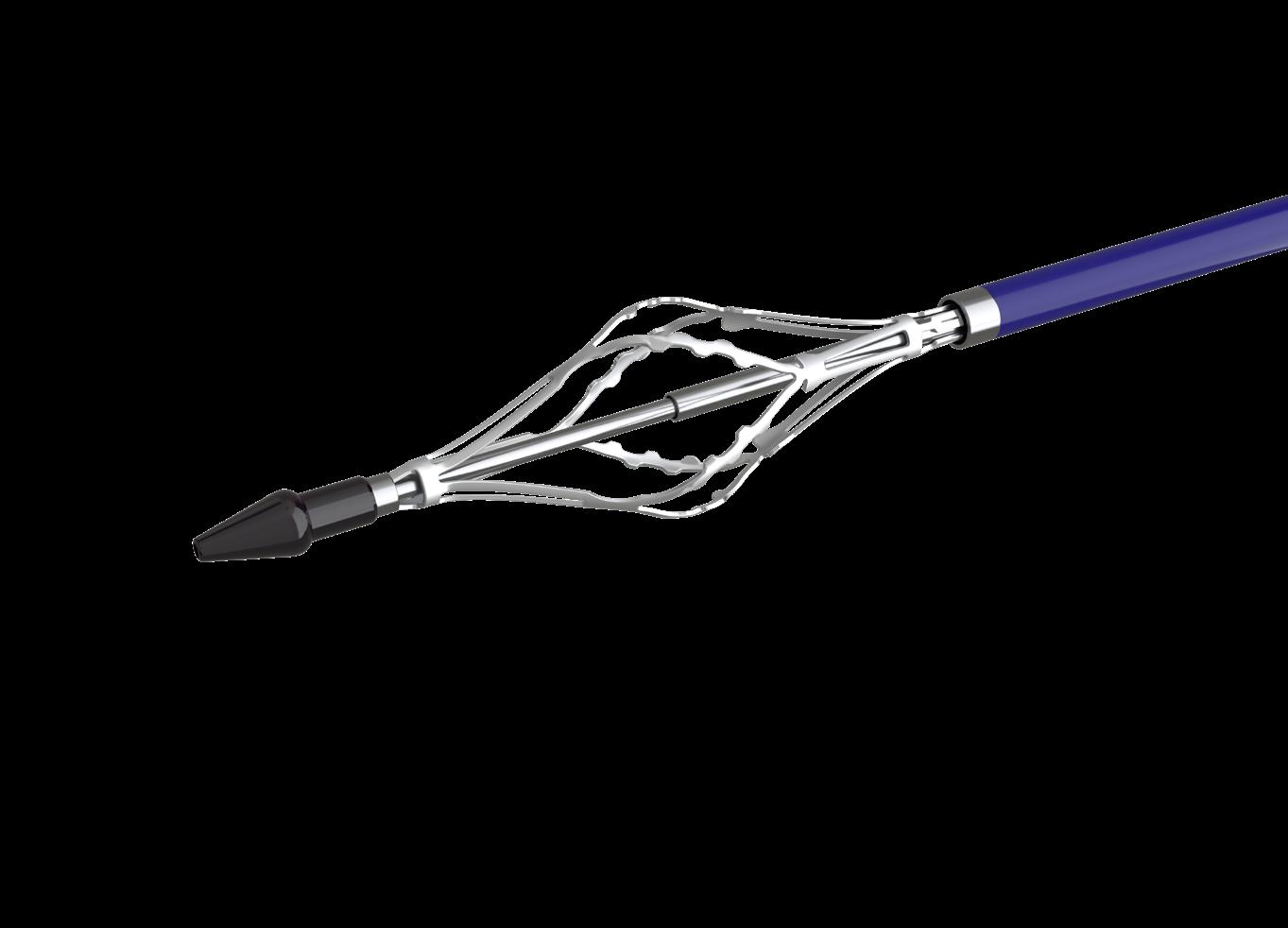
VenaCore
Thrombectomy Catheter TM
Designed to Address Challenging Venous Occlusions
Dynamic Control
Quick compress handle lever for element collapse and expansion Indications
Engage. Separate. Remove. Modified off-axis edge design for in-line vessel treatment of venous occlusions
How the RevCore and VenaCore thrombectomy catheters combine to broaden treatment approach among advanced deep vein thrombosis patients previously limited to few options
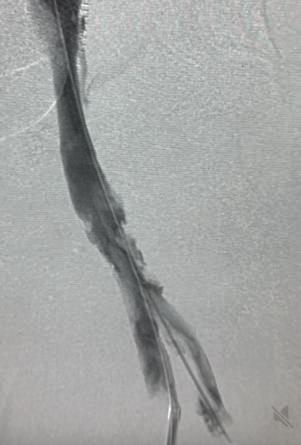
For Joseph M. Liechty, MD, a vascular surgeon with Texas Vascular Associates in Plano, Texas, the emergence of the RevCoreTM and VenaCoreTM devices (Inari Medical) have helped broaden his treatment strategies for advanced venous disease patients in whom options were previously limited. Liechty, who operates in the Dallas-Fort Worth (DFW) metroplex, sees a significant number of patients living with the long-term sequalae of deep vein thrombosis (DVT), especially those with symptoms of post-thrombotic syndrome (PTS).
Here, he describes how he has harnessed the RevCore thrombectomy catheter to tackle in-stent thrombosis and the VenaCore thrombectomy catheter to address challenging venous occlusions, as he builds a venous practice that reaches beyond best medical therapy with a limited suite of interventional tools. These new thrombectomy devices, Liechty explains, have helped him reach a community in need of alternatives with enduring results.
Can you describe how your venous practice has evolved since you started to see patients in the DFW metroplex?
Venous patients make up about 30% of all the cases I do now, with acute referrals coming from emergency departments (EDs) and hospitalists from multiple healthcare systems in the area, and from outpatient clinics dealing with more chronic DVT and symptomatic venous obstructions. When I first came here, I did a lot of ED and intensive care unit talks and I visited primary care, wound care, hematology/oncology and cardiology practices. I did a lot of promotion, case sharing, and awareness work because the technology was so new. There has been a long-standing paradigm of treating venous disease extremely conservatively that is not easy to change. Something that has been helpful when speaking to colleagues is to have trials and data to show them, as well as case presentations.
In what ways have RevCore and VenaCore grown your practice?
Prior to the introduction of RevCore, there was a certain period in which a thrombectomy needed to be done before the clot in the stent became impossible to remove and would require a new stent to be placed inside the old one. The only real option was to go in with some kind of aspiration tool
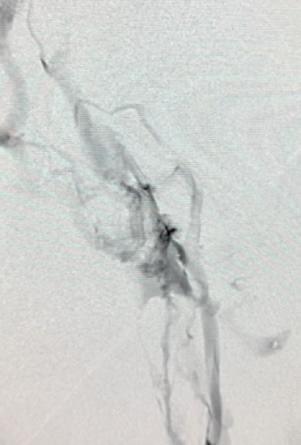
1. Pre-procedural venogram. 2. Venogram taken post-procedure 3. A representation of the clot removed. 4. The RevCore (top) and VenaCore (bottom) devices used
tients who have problems for which they have been told there aren’t any good solutions. In the vascular world, DVT is different because the disease process skews toward a younger population compared to arterial disease. We can improve the quality of life for people who are still trying to work and support a family, for example.
to remove the thrombus or use thrombolytics; however, neither of these options were consistently effective in cases where the thrombus had been present for perhaps a couple of weeks, and so it was a pressing matter to get the thrombectomy done as soon as possible. With the RevCore device, that sense of urgency has been removed. We have the liberty to go in a little bit later. More importantly, if a patient should present late with a thrombosed stent, we don’t have to say, “There is nothing we can do.”
Additionally, prior to RevCore, if you couldn’t get the clot out when it was fresh, you didn’t really have any other choice than to place another stent. RevCore gave us an option to remove thrombus of varying chronicity from an existing stent and hopefully limit the need to place another.
What has been your experience offering patients treatment with the RevCore and VenaCore devices when previously they couldn’t get an interventional option?
We have had a lot of success. We haven’t had many cases where there has been thrombus that has been resistant to these devices. I have found VenaCore to be especially useful in the common femoral vein, where perhaps there would be concern for having to stent across the infrainguinal ligament, even though this is well-tolerated when I’ve done it.
For clotted stents, the only option was to aspirate whatever could be removed, perform balloon angioplasty, and then possibly place more stents, leading to patients with a couple of layers of stents if they had experienced more than one clotting episode. RevCore allows you to clean out stents, which has decreased my need to re-stent.
What would you tell your peers about building an advanced venous practice?
There are a lot of upsides. We deal with pa-
Advanced venous cases require considerable planning in terms of anatomy, thrombus distribution, pre-existing stents and/or filters, and available access points, as well as which devices are available. We have seen very grateful patients for whom previously there wasn’t anything we could do other than offer compression stockings and anticoagulation.
If you are just starting out with these devices, perhaps an ideal patient might be one who has a unilateral problem and no thrombotic history. For more advanced cases, I favor general anesthesia because these cases can take a few hours, and having multiple access sites could be uncomfortable for an awake patient.
Can you break down how RevCore fits into your surveillance of patients who have had a stent placed?
I schedule regular surveillance on all the iliac vein stents I implant—I routinely follow up with these patients at four weeks, three months, nine months and then annually— and occasionally we’ll see stents that appear to be occluding, developing a lining on the inside that narrows the flow lumen.
There is a subset of patients whose stents will eventually go on to occlude and they remain asymptomatic. This is probably because they have managed to develop collaterals that are sufficient during that time. But I also have patients who have a stent that is starting to occlude, and they are beginning to have swelling and pain in their leg. Those are the patients who don’t have collaterals yet, or maybe they are always going to be dependent on their stent. These are the patients on whom I would intervene early. Essentially, my strategy is based more on how the patient feels and how the leg looks rather than whether there is some narrowing on ultrasound. That shouldn’t be the deciding factor.
Case report
A man in his late 60s with a left iliac vein stent and revision two years prior was referred for consultation. The patient dis -
continued his anticoagulation two months before he was referred for consultation for severe left leg swelling. Duplex ultrasound confirmed a reoccluded left iliac venous stent. The decision was made to intervene with mechanical thrombectomy.
Procedural overview
Access was obtained in the superficial femoral vein and right internal jugular (IJ) vein under ultrasound guidance. A venogram demonstrated significant thrombus in the common femoral vein, profunda and extending into the external iliac vein. A .035” guidewire was inserted into the femoral vein and externalized through the access sheath. A ProtrieveTM sheath (Inari Medical) was inserted over the wire into the right IJ vein and advanced into the inferior vena cava. Next, the Triever20 catheter (Inari Medical) was inserted over the wire and directed to the profunda and common femoral vein. Aspiration with the Triever20 removed acute and sub-acute thrombus. Organized material could not be removed with aspiration. RevCore was then inserted over the wire into the occluded stent. Multiple clockwise and counterclockwise turns in conjunction with scrubbing the element within the stent resulted in successful clearance of nonacute thrombus. VenaCore was then introduced through the Protrieve sheath to clear the common femoral vein. Completion venogram demonstrated brisk cephalad flow. Total procedure time was 90 minutes.
DISCLOSURE: Joseph M. Liechty is a paid consultant of Inari Medical. All views and opinions expressed here by Liechty are his own and do not represent those of Inari Medical.
Indications For Use: The RevCore Thrombectomy Catheter is indicated for (1) The non-surgical removal of thrombi and emboli from blood vessels. (2) Injection, infusion, and/or aspiration of contrast media and other fluids into or from a blood vessel. The RevCore Thrombectomy Catheter is intended for use in the peripheral vasculature. The VenaCore Thrombectomy Catheter is indicated for (1) The non-surgical removal of thrombi and emboli from blood vessels. (2) Injection, infusion, and/or aspiration of contrast media and other fluids into or from a blood vessel. The VenaCore Thrombectomy Catheter is intended for use in the peripheral vasculature. The Protrieve Sheath is indicated for use as a conduit for the insertion of endovascular devices into the vasculature while minimizing blood loss associated with such insertions. Triever Catheters are indicated for (1) The non-surgical removal of emboli and thrombi from blood vessels (2) Injection, infusion, and/ or aspiration of contrast media and other fluids into or from a blood vessel. Triever Catheters are intended for use in the peripheral vasculature and for the treatment of pulmonary embolism. Triever Catheters are also intended for use in treating clot in transit in the right atrium, but not in conjunction with FlowTriever Catheters.
Caution: Federal (USA) law restricts these devices to sale by or on the order of a physician.
Review complete Instructions for Use, Indications for Use, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the product.
For all non-Inari products, please refer to complete manufacturer Instructions for Use/ Intended Purpose for complete indications for use, contraindications, warnings and precautions.
All copyrights and trademarks are property of their respective owners.
Inari Medical 6001 Oak Canyon, Suite 100, Irvine, CA 92618
FROM THE COVER VASCULAR TRAINEES BETTER PREPARED FOR OPEN AORTIC PRACTICE THAN COMMONLY REPORTED, NEW STUDY SHOWS
continued from page 1
that over the 11-year period of their analysis, the mean aortic case volume among graduating vascular surgery fellows and residents were 118.8 and 130.5, respectively.
The open aortic experience comprised 32.9 cases among fellows, including 17.5 aneurysm repairs and 15.5 operations for aortic occlusive disease, with a <1% decline in open aortic operations.
Endovascular aortic volume among fellows included 85.8 total cases, which increased by 1.5 each year. These included 42.2 endovascular aneurysm repairs (EVARs), 15.8 thoracic EVARs (TEVARs), and 27.8 aortoiliac angioplasty and/or stenting operations.
Among graduating residents, open aortic experience comprised 36.1 cases, including 18.3 aneurysm repairs and 17.7 operations for aortic occlusive disease, with no decline in open aortic operations. Residents’ endovascular aortic case volume included 94.4 total cases, which increased by three annually. These included 46.5 EVARs, 15.8 TEVARs, and 32.1 aortoiliac angioplasty and/or stenting operations.
“Having personally graduated from fellowship three years ago, and speaking with many other co-fellows and fellows in training at the moment, we all know this intrinsically to be not true for ourselves—that we graduate prepared for surgical practice in open AAA repairs,” Kim explains.
“I’m not sure how that speaks to the national trends, but it is hard to hear that as somebody who recently has gone through training, having other people tell me that we are not prepared for surgical practice in open AAA repairs. That was the impetus for taking a look at the data. Specifically, we wanted to look at the ACGME case logs because these are self-reported cases by each of the trainees during their training, so reliable in that regard.”
The types of open repairs included in the analysis ranged from infrarenal, suprarenal, thoracoabdominal and thoracic aneurysms, to aortoiliac bypasses and aortofemoral bypasses or resections for occlusive disease.
“Open aortic case volume for both residents and fellows was somewhere between 30 and 40 by the time of graduation,” Kim says. “That number didn’t really change much over the years, which really speaks to the consistency and reliability of the data for total open aortic case volume, so it’s not as if this data is unreliable.”
Still, as trainees enter practice, Kim adds, “the most important thing is having a supportive senior partner because, though you may have done a number of aortic cases during training, it is really only during the first few aortic cases you do in practice when the training wheels come off.”
INTERVIEW
The endovascular revolution and open aortic training:
‘It’s not necessarily a crisis but it could become one’
By Bryan Kay
JEAN PANNETON, MD, CONSIDERS HIMSELF WHAT HE terms a “blue-collar” vascular surgeon as much as one engaged in academic practice and the necessity of helping contribute to the next generation of vascular surgeons. He operates. And he operates a lot. But he is also a professor of surgery, and a program director in charge of turning out vascular trainees so important to the future of the specialty. For him, the rigors of both silos, brisk practice and academia, coalesce in his everyday working life—and they also underpin the thrust of the message he was trying to send in a recent turn at the lectern as well as in this interview. “Blue refers to the fact you have to take care of business, take care of patients,” Panneton, a vascular surgeon with Sentara Vascular Specialists and chief of vascular surgery at Eastern Virginia Medical School in Norfolk, Virginia, tells Vascular Specialist. “Because when you work in a non-academic center per se, and non-university hospitals, some of these places are very busy, high volume, so that is where that statement comes from.” When he used the phrase as he delivered the Robert R. Linton Lecture at the 2024 annual meeting of the New England Society for Vascular Surgery (NESVS) in Portland, Maine (Oct. 25–27), he got a few laughs, but a seriousness underpinned it. “The changing landscape of aortic surgery” was the title. The message was twofold: the shift in volume from open surgery to endovascular therapy and the new language and complications that have come with it, alongside the impact this evolution has had on the open surgical skills with which graduating trainees emerge from residency and fellowship.
“With endovascular therapy comes an increased need for reintervention and the concept of new types of complication—endoleaks for example, graft migration too,” he says. “These never existed before. And how has this shift affected training? Nowadays, a lot of the recent graduates are not comfortable with open aortic surgery.”
a formal way of measuring knowledge transfer and aortic care skill acquisition outside of the standard structures of ACGME programs and American Board of Surgery (ABS) exams, scalable solutions remain to be developed.
On the other hand, there is the other side of that training deficit, the endovascular revolution, the one for which Panneton had to learn a new language and new way of doing things, and it has tracked his 35-year career. The new language signposted those new complications but, importantly, came along with reduced mortality and morbidity. “One of the exciting things of this move toward endo has definitely been the evolving technology that has gone hand in hand with that shift,” he says. “Over 30 years of implanting endografts, from gen-one devices to the next-gen devices, has been phenomenal. Industry has done a fantastic job of trying to improve devices year after year. We started with simple EVAR [endovascular aneurysm repair], to now being able to do fenestrated or branched repairs for TAAA [thoracoabdominal aortic aneurysm] and endovascular repair of aortic arch pathology as well.”
Complex problems and devices to match brought with them not only issues related to complications but others like repair complexity, high costs and the need for additional devices such as bridging stents. Thus, Panneton says, the necessity of simple solutions and devices endures. He points to in situ laser fenestration, for example, which “can be done in a very simple, effective manner, and those devices have a smaller delivery profile than more complex devices. The operations tend to be quicker, and with less manipulation.” On the topic of in situ fenestration, Panneton’s group has a paper due at the 2025 annual meeting of the Southern Association for Vascular Surgery (SAVS) in St. Thomas, the U.S. Virgin Islands (Jan. 22–25), in which they look at a 15-year experience of the technique in zone 2 thoracic EVAR (TEVAR). The paper will report “a very, very low stroke rate,” Panneton says. “It’s also very durable.” His first patient received the procedure in August 2009, with that subject representative of quite a few others among the cohort, he adds: an intact fenestration, patent vessel and no fenestration-related complications.
“Nowadays, a lot of the recent graduates are not comfortable with open aortic surgery”
Nationwide, there is a growing realization of the issue and the need to address it—regionalized aortic care, an aortic fellowship, simulation, trainees rotating to high-volume centers are among the remedies circulating— but Panneton is not sure scalable solutions to remedy the deficit are close. “For now, it’s not necessarily a crisis but it could become one,” he says. “Because when you look at the median age of currently practicing vascular surgeons, and how a lot of them have significant open aortic skills, in the next 10 to 15 years, a lot of those surgeons will end up retiring. It’s crucial that before this wave of vascular surgeons with open aortic skills retire that they transmit the skills to the younger generation. Some of those surgeons do not work in a place where there is a formal ACGME [Accreditation Council for Graduate Medical Education] training program. One way for these skills to be transferred might be for trainees to continue to look, wherever they end up after completing training, at their job as an apprenticeship mode, where junior surgeons can really be tagged to more senior surgeons who can share some of that experience with open aortic surgery to junior partners.” Still, Panneton adds, absent
JEAN PANNETON
Alongside complexity sit an aging patient population, increasing prevalence of vascular disease, and, therefore, a need for more vascular surgeons. Up come those training questions again: Panneton sees a need for an increase in the number of vascular surgery training programs. While the level has been steadily increasing, he notes, it “is not increasing fast enough. What’s predicted is a deficit in vascular surgeons. There is also a generational shift, with the newer generation not necessarily looking at working as a surgeon in the same way we previous generations looked at it.” Which is to say, work-life balance has taken root, further shaping the face of the workforce and needs of the workplace, Panneton observes. Running in tandem are increased demands on vascular surgeons—the expansion of peripheral arterial disease (PAD) treatment, pulmonary embolism response teams (PERTs), wound care, and, an area previously the preserve of cardiac surgery, the aortic arch. “When a hospital has a TAVR [transaortic valve replacement] program, they cannot exist without vascular surgeons,” he continues. “We get called a few times per week for structural heart. There has been an increase in the demand for vascular surgeons because the work has diversified even more.” As a result, another evolution plays out. “Vascular surgery is evolving like general surgery,” Panneton reasons. “In the past, general surgeons took care of everything. But now, there are general surgeons who do only trauma, or oncology surgery, or colorectal surgery. We are seeing that start to happen with vascular surgery. Some only do vein procedures, because they tend to be elective, which is a much more controlled thing. Some do wound care or work in a limb salvage clinic. There are some, like me, who you might consider an aortic surgeon, as the majority of my practice is aortic stuff. That is one way for the workforce to deal with the demands of practice in the future.”
Yet, the training imperatives of aortic surgery remain, adds Panneton. “That is the most high-risk and most likely to be the one to require additional training, as opposed to other ‘sub-specialties’ within vascular surgery, which are not quite the same level of complexity and risk.”
continued from page 1
F
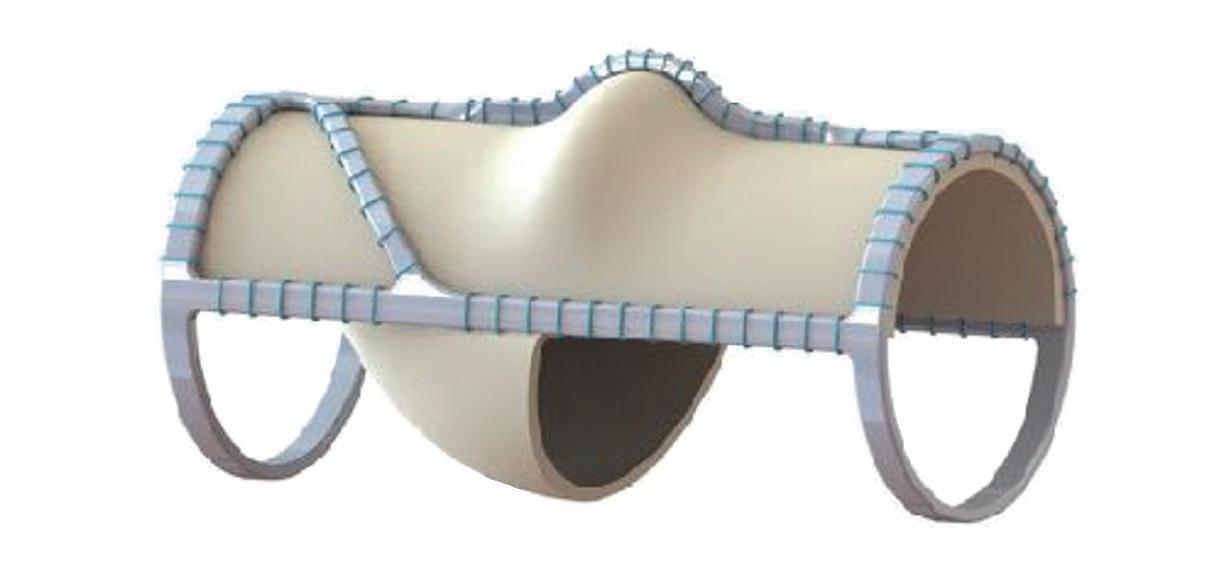
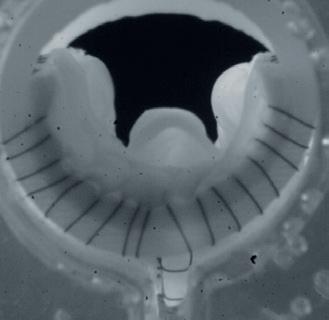
resh from delivering positive one-year data from the Surgical Antireflux Venous Valve Endoprosthesis (SAVVE) pivotal trial at the 2024 VEITHsymposium in New York City (Nov. 19–23), site principal investigators Matthew Smeds, MD, and Raghu Motaganahalli, MD, are both ebullient about what the results might mean about the future for patients with chronic venous insufficiency (CVI) and venous ulcerations.
The data show that 85% of patients surgically implanted with a bioprosthetic VenoValve (enVVeno Medical) reached the one-year milestone having achieved a clinically meaningful benefit of a three-or-more point improvement in revised Venous Clinical Severity Score (rVCSS); a 7.91 point average improvement in rVCSS; a clinically meaningful benefit across all CEAP (Clinical, Etiological, Anatomical and Pathophysiological) classes of patients enrolled (C4b–C6); 97% target vein patency at one year; and significant resolution in venous ulcerations.
“It is the first device we have had to treat deep venous insufficiency in years,” says Smeds, a professor of surgery and the former division chief of vascular and endovascular surgery at Saint Louis University in Saint Louis, Missouri. “These patients are typically relegated to compression therapy alone. There is no really great surgical options for this issue.”
Motaganahalli describes the novel device as representing a “gamechanger” given how previous attempts at developing a surgical option for the CVI patient population failed to take hold. “The procedure does not have a steep learning curve; technically, this is a procedure that can be accomplished by any trained vascular surgeon. It is not technically demanding,” he says. “Before, these were technically demanding operations: if you really look at the historical data from internal valvuloplasty or the external valvuloplasty, vein valve reconstruction, vein valve transplant, they were effective in a few select centers and a few select hands but that result was not reproducible at multiple centers.”
Smeds zeroes in on the topline result of 98.4% device patency and considers how there were nine device occlusions over the year. “However, eight of them recanalized,” he explains. “I had some patients that thrombosed the device. Interestingly, in one of them I sucked out the thrombus via mechanical thrombectomy and then it occluded a few weeks later. I thought that device was never going to be functional, but, within a month or two, the device recanalized and the patient had decreased reflux below the device and she was healing her ulcer.” Though these thromboses were each marked down as a device “failure,” Smeds continues, the fact eight reopened and many were then functional were pleasant surprises. “I think you see that in the natural history of people with DVTs [deep vein thromboses] to begin with,” he explains.
Elsewhere among the data, he picks out the trial’s inability to pinpoint a direct relationship between reflux and ulcer healing, and the role of compression therapy compliance as intriguing propositions. “We cannot find a direct one-to-one ratio in terms of if you have a really high decrease in reflux, then you get a really high ulcer healing rate,” Smeds says. “So, there are certainly more complex things going on at a patient-topatient level with the device as far as who is benefiting from it.
“We also looked at whether there was full compliance for compression therapy—whether that increased or decreased over the length of the trial—and there was a slight decrease in its use, which demonstrates that the device is doing something to aid in the ulcer healing and the symptom improvement, because it wasn’t necessarily due to an increase in compression.”
For Motaganahalli, chief of vascular surgery and program director at Indiana University in Indianapolis, ulceration reduction data were stark. In those who had their ulcers for less than three months, the SAVVE trial demonstrated that there was 100% resolution—“complete healing,” he says. “Most of the patients who had an ulcer more than a year or so, even then 60% of them showed full resolution of the ulcer. The average area of the ulcer, especially in those who had a longer duration of ulcer, those patients had an average ulceration of 20.6cm2 at baseline and that reduced to 12.3cm2.”
Motaganahalli sees a promising future: “The oneyear data tells you that it provides a sustained benefit
DIALYSIS ACCESS
WAVE TRIAL AVG COHORT ALSO BENEFITS WITH WRAPSODY AT SIX MONTHS
Newly released six-month results from the single-arm arteriovenous graft (AVG) cohort in the WAVE (Wrapsody arteriovenous access efficacy) trial showed target lesion and access circuit primary patency rates of nearly 82% and 68.8%, respectively. By Bryan
Kay
THE LATEST DATA ON THE Wrapsody cell-permeable endoprothesis (Merit Medical) for treatment of stenosis or occlusion within the dialysis access outflow circuit were revealed during the final day of VEITH 2024 by co-principal investigator Mahmood K. Razavi, MD, from St. Joseph Heart and Vascular Center in Orange, California. “In light of the historically low patency rates for AVG patients, the positive results from the AV graft arm of the WAVE trial are very encouraging for physicians who manage these patients,” he said.
The WAVE trial was designed to evaluate the efficacy and safety of the WRAPSODY endovascular stent graft across two cohorts: up to 244 AV fistula patients randomized 1:1 to either the Wrapsody device or percutaneous transluminal angioplasty, and the AVG cohort.
covered stents (efficacy: 60%; safety: 89%). Efficacy of the Wrapsody device was 81.4%—21.4 percentage points higher than the performance goal (p<0.0001).
The proportion of graft patients who were free from an adverse event was higher than the safety performance (95.4% vs. 89.0%, p=0.0162). “As you well know,” Razavi told VEITH 2024, “these types of numbers are somewhat unusual in this patient population, having this kind of patency.”
The historical controls were based on three prior stent graft studies, he explained, with patency ranging between 50–71% at six months.
The graft arm enrolled 112 patients across 43 international sites. Primary efficacy and safety endpoints were assessed by comparing actual rates for the device to performance goals for
“The patency results from the WAVE trial are the highest that I have seen to date and are expected to meaningfully improve patients’ quality of life and vascular access survival,” said WAVE trial investigator Leonardo Harduin, MD, a vascular surgeon at University of Rio de Janeiro State in Rio de Janeiro, Brazil. “These results will probably have a positive impact on costs related to the care of these patients.”
The device is mandated investigational in the U.S.
When RCTs are essential for novel vascular
AS A PART OF A VEITH 2024 DEBATE, Robert E Lee, MD, a medical officer recently retired from the Food and Drug Administration (FDA), presented an argument in favor of when the use of randomized controlled trials (RCTs) for the regulation and approval of novel vascular access devices becomes important.
“Randomization,” he stated, “helps assure that participants in both treatment groups are similar in the distribution of prognostic factors. This minimizes bias in statistical comparisons of patient outcomes when looking at both effectiveness and safety.”
“RCTs yield the highest level of evidence to establish causal associations in clinical research,” he said, so that there is no need for statistical sleight of hand with propensity scoring or other complex methodology to understand if a new therapy is more effective. George Barker
Mahmood K Razavi
Raghu Motaganahalli
Matthew Smeds
of symptomatic improvement for patients with CVI. The VenoValve is a safe and effective treatment for patients with CVI due to deep valvular incompetency. It’s not only effective, but effective across the whole spectrum of CEAP classification: for C4b through C5 and C6. The benefits were seen within the first three months and sustained through the one-year observation.”
Motaganahalli also lingered on the significance of the improvement in average rVCSS among the trial cohort: the 7.91 score recorded at 12 months came amid a Food and Drug Administration (FDA) mandate for a more than 3-point advance in rVCSS. “Here, more than 85% of the patients had more than 3-point improvement,” Motaganahalli notes.
still “Pandora’s box as far as putting devices and valves in there,” he says. Further, in the SAVVE trial, each patient was implanted with only one replacement valve. Smeds considers the questions of whether more than one device should be fitted in patients to further decrease reflux; whether in patients with duplicate incompetent systems both should receive a VenoValve; and whether the location of the replacement valves should be modified. “There are a lot of unknown questions that will hopefully begin to be answered once this becomes FDA approved,” he adds.
“There are a lot of unknown questions that will hopefully begin to be answered once this becomes FDA approved” MATTHEW SMEDS
On the eve of the VEITHsymposium, enVVeno Medical announced it had submitted an application with the FDA seeking approval to market the VenoValve based on the data Smeds and Motaganahalli presented. The company is also developing a next-generation, non-surgical transcatheter-based replacement valve called enVVe. It is expected to be ready for its own pivotal trial during the middle of 2025.
Smeds is excited by the portent of what might be to come as development proceeds. The venous system is
AV FISTULA
Motaganahalli believes some might query the cost of the device once it enters the market but sees the potential impact on the heavy costs associated with wound care for venous ulcers as a boon. “If you look at the cost of treating ulcerations, several billions of dollars are spent annually,” he says. “With appropriate patient selection, the device can do wonders. We have 2.5 million potential patients with CVI in the U.S., with close to around 40% missing workdays, $3 billion in direct medical costs, $30,000 per patient in terms of the annual cost of ulcer treatment, with the potential for 20–40% of these patients to have a recurrence. This makes the device a very attractive option.”
NOVEL BIOABSORBABLE PERIVASCULAR WRAP AIMS TO REDUCE AVF FAILURE
Ellen Dillavou, MD, division chief of vascular surgery at WakeMed Heart Center in Raleigh, North Carolina, primary investigator (PI) for the VenoStent trial, presented new data about the SelfWrap (VenoStent) bioabsorbable perivascular wrap, outlining how the novel device can, she says, improve arteriovenous fistula (AVF) maturation and patency.
According to data published in the Journal of the American Society of Nephrology (JASN) and American Journal of Kidney Disease (AJKD), annually, 5 million patient lives are put at risk by 60% one-year failure rates of AVFs and arteriovenous grafts (AVGs), as well as 20% one-year failure rates of vein grafts in bypass grafting, she said.
One solution, Dillavou argued, is the SelfWrap device. Receiving its Food and Drug Administration (FDA) Breakthrough Device designation in May 2022, followed by investigational
device exemption (IDE) approval in May 2023, this vascular wrap made of bioabsorbable polymers uses an artery-like mechanical support to help veins first “behave” and then “become” like an artery. It also regulates flow—which Dillavou stated will “impart hemodynamic benefits.”
“In every large animal model which tested AVFs, AVGs and bypass grafts over five years and three different centers, the advanced materials approach that ‘arterializes’ veins significantly reduces neointimal hyperplasia,” said Dillivou.
The SelfWrap trial’s objective was to demonstrate feasibility and evaluate the safety and performance of the SelfWrap device by enrolling 20 participants in a single-center, prospective, single-arm study, with follow-up obtained at six months up to 60 months. The primary endpoint was a high patency rate. Three SelfWrap sizes were employed,
PATIENT SAFETY
Venous VQI celebrates decade milestone
By Jocelyn Hudson
DURING THE VEITHSYMPOSIUM, MARC PASSMAN, MD, reflected on the achievements of the Society for Vascular Surgery (SVS) Vascular Quality Initiative (VQI) venous arm, in collaboration with the American Venous Forum (AVF), since its inception 10 years ago.
Passman, who is professor of surgery in the Division of Vascular and Endovascular Therapy at the University of Alabama at Birmingham and chair of the VQI Venous Quality Council (VQC), shared that a total of 1,302,849 procedures have been captured by the VQI as a whole as of Nov. 1, 2024.
Regarding venous interventions, Passman specified that there are currently three venous modules in the VQI, with varicose vein, inferior vena cava (IVC) filter, and venous stent procedures comprising 70,097, 19,793 and 305 of the November 2024 total, respectively.
Passman first highlighted data from the VQI IVC filter registry. Initiated in 2014, the presenter shared that 50 centers were subscribed to the registry as of November 2024. He noted that this has decreased by 16 from a peak in July 2017 of 66 centers subscribed.
Participation in the varicose vein registry shows a similar trend, Passman highlighted. Following its inception in 2015, the number of centers subscribed peaked at 45 in May 2021 ahead of falling by 13 to 32 centers as per the latest figures.
The venous stent registry was the most recent of the three venous modules to be established. Passman reported that the number of centers subscribed has been on an upwards trajectory since data capture began in 2020 and currently stands at 10.
Providing an update on the newest of the venous VQI registries, Passman noted that there has been a recent revision of the original data fields. Specifically, he shared that less-needed registry variables have been removed and highlighted efforts to decrease registry data entry burden. Passman also detailed that the development of registry reporting measures is now underway, as well as a drive to increase site recruitment.
with selection based on vein size. A total of 13 patents (65%) were given brachiocephalic fistulas (BCFs), two received basilic vein transpositions (BVTs), and five were given radiocephalic fistulas (RCFs).
Dillavou reported that there were no adverse events probably or definitely related to the device through 36 months, as well as no device deficiencies nor adverse device effects.The SelfWrap device had a high maturation rate, she reported. Functional maturation was 95%, compared to the <58% expected, and unassisted maturation was 90% for SelfWrap, compared to 33%. Further, SelfWrap saw 89.5% of catheters removed at nine months, 94% of which were unassisted, compared to ~27% at nine months for untreated AVFs. Dillavou noted that, should the results translate to the ongoing IDE study, they would prove impactful in the space.—George Barker
Passman shared that a VQI best practices dashboard has been introduced across the board to summarize each center’s results, and provide comparison to national VQI benchmarks
Passman stated that a venous VQI research advisory council (RAC), chaired by Nicholas Osborne, MD, of the University of Michigan, was set up in 2020. The presenter noted that submission of venous RAC proposals is increasing, and encouraged centers not enrolled in a venous VQI module but are interested in research projects to connect with a venous VQI registry partner.
He also highlighted several publications to have emerged from the venous VQI registries over the past 10 years, including on the impact of COVID-19 on the varicose vein and IVC filter registries and on the use of telemedicine for the management of patients with varicose veins, among various other topics.
Passman lauded 10 years of achievement since the first venous VQI registry was initiated: the improvement of long-term outcomes through standardization, the availability of evidence-based outcomes analysis, and the use of data to define best clinical practices. In addition, Passman underscored the introduction of regional and national benchmarks that have the potential to monitor safety and efficacy.
SYMPOSIUM FEATURES
• Comprehensive and Practical Programming
• Practice Management Essentials
• Clinical Case Reviews
• New Methods, Early Results, Clinical Trials and Innovation
• International Call for Abstracts and E-Poster Presentations
• Latin Session in Collaboration with CADECI
• Extensive Exhibition Hall
• Social Networking Events
LIVE
PATIENT SESSIONS
• Live Patient Consultations, Examinations
• Ultrasound Protocols
• Interactive Discussions on The Evaluation, Diagnosis, Treatment and Follow Up of The Patients
Novel sirolimus-eluting scaffold system
demonstrates ‘potential
to address Achilles' heel’ of currently available endovascular treatment options
By Bryan Kay
Ongoing studies of the Efemoral vascular scaffold system (EVSS)—previously described as a potential new paradigm in the treatment of long occlusive lesions—show that the device continues to show promise, according to investigators.
The latest animal study assessed the subacute response to implantation of the novel, sirolimus-eluting bioresorbable system in 10 arteries of five female mini-swine, finding that it provided effective scaffolding of the treated artery, achieved near-complete reendothelialization within 30 days and “generated only a modest vascular proliferative response.” The data were revealed at the 2024 Midwestern Vascular Surgical Society (MVSS) annual meeting in Chicago (Sept. 12–14).
Clinical data from the ongoing first-in-human trial of the device, EFEMORAL I, are due to be presented at the 2025 Charing Cross (CX) International Symposium in London, England (April 23–25). Here, Rym El Khoury, MD, a vascular surgeon at NorthShore-Endeavor Health in Chicago, the first-named author on the latest animal study, takes stock of the progress made with the EVSS (Efemoral Medical) to date.
Can you tell us about the latest animal data presented at MVSS 2024 and how this contrasts with that from MVSS in 2021? In 2021, we presented an acute animal study of a novel bioresorbable vascular scaffold system. This investigational device consisting of multiple, serial, short, balloon-expandable scaffolds was implanted in a validated large animal model of
SVS FOUNDATION GETS MOVING ON PADRELATED GRANT DISPARITIES
By Beth Bales
ALL THOSE STEPS LOGGED DURING the SVS Foundation’s exercise challenge in September will help the Foundation—and researchers—take new steps to unlock new treatments for peripheral artery disease (PAD).
The foundation’s Vascular Health Step Challenge, during National PAD Awareness Month, raised money and heightened awareness of the disease process. Foundation members decided to use the funds for a new grant under the Vascular Care for the Underserved (VC4U) program, “intended to support innovative pilot projects that address the unique challenges faced by underserved populations affected by PAD, with an emphasis on improving diagnosis, treatment and patient education.”
Members of both the SVS and the Society for Vascular Nursing (SVN) will be eligible to apply for the $20,000 grant.
percutaneous femoropopliteal arterial intervention. The animal’s hindlimb was bent in a physiologic and supra-physiologic position to assess arterial deformation and preservation of arterial lumen diameter after device implantation. We found that the inter-scaffold spaces allowed for unencumbered arterial motion in an environment that exceeded the mechanical requirements of the human superficial femoral and popliteal arteries. We also demonstrated that the copolymer of poly-L-lactic acid (PLLA) scaffold was able to deform with hindlimb extreme flexion. The hypothesis that long segments of human arteries can be effectively treated with this new paradigm was thus tested. In order to address the periprocedural arterial injury and
“At 30 days, all treated arteries exhibited modest inflammation, near-complete endothelialization, modest neointimtal reaction, and ubiquitous fibrin”
RYM EL KHOURY
Details, including the application process and deadlines, are under development and will be announced shortly, once completed.
Foundation Chair Joseph Mills, who directed a previous VC4U pilot project, is excited the program will fund a grant specifically earmarked for PAD and underserved populations. “All vascular surgeons understand the disproportionate effect of PAD on people with poor healthcare access,” he said. “If we can reach and educate people earlier, we can hopefully start with minimally invasive therapy such as medical management, lifestyle modifications and exercise therapy to reduce limb complications and amputation.”
Foundation Executive Board members also released updates on two existing projects: “PAD in west and southwest Philadelphia: Providing education and screening and investigating barriers to care,” from Julia Glaser, MD, and “UMass homeless foot and diabetes screening outreach program,” from Tammy Nguyen, MD.
neointimal hyperplasia that hinders durability, we spray-coated this investigational device with a known antineoplastic agent—sirolimus—and implanted it in a similar model. The purpose of this study was to assess the subacute response to its implantation. At 30 days, all treated arteries exhibited modest inflammation, near-complete endothelialization, modest neointimtal reaction, and ubiquitous fibrin. This novel sirolimus-eluting PLLA-based scaffold demonstrates the potential to address the Achilles’ heel of currently available endovascular treatment options.
Can you update us on how the first-inhuman trial is progressing?
EFEMORAL I is a multicenter international trial currently enrolling in Australia and New Zealand. To date, 28 patients have been treated with the investigational device, with follow-up data up to three years in the first human subjects. In April 2024, Dr. Andrew Holden, the principal investigator for this first-in-human trial, presented the early results at CX, including the first transcutaneous ultrasound demonstrating device resorption between the first and second year. The clinical data are scheduled to be presented at the next CX meeting in 2025 as Dr. Holden presents EFEMORAL I’s results for the first time.
The device has been adapted for belowthe-knee interventions. How is this development progressing?
The Efemoral system presents the advantages of treating long-segment tibial disease with a single device; prolonged drug elution to limit neointimal hyperplasia; disappearing from the artery within the first two years; and promoting positive remodeling. In May 2024, the Food and Drug Administration granted Efemoral a Breakthrough Device designation for the treatment of de novo or restenotic lesions of the infrapopliteal arteries in patients with chronic limb-threatening ischemia (CLTI). Pre-clinical studies assessing drug transfer and vascular response to the tibial device are underway.
Glaser, an assistant professor of clinical surgery at Penn Medicine, conducted two health fairs to screen attendees for abdominal aortic aneurysms (AAAs), carotid disease and PAD, as well as for PAD risk factors. She now is undertaking the second part of her grant, to conduct a qualitative study to determine factors that cause patients with chronic limb-threatening ischemia (CLTI) to delay seeking care.
The successful outreach fairs screened approximately 90 patients on various health measures. Patients received the results, guidance on care and encouragement to share the results with a primary care physician.
In the interview study, Glaser is targeting people who needed amputations for vascular disease. Her grant is being extended partially as a result of her maternity leave this year. Study enrollment has been slower than anticipated, “which is actually a good thing—we are doing fewer amputations for vascular disease,” said her colleague, Sarah Harrison Benchimol. Nguyen, from the University of Massachusetts and an assistant professor
at UMass Chan Medical School, aims to increase access to comprehensive diabetic foot care in order to prevent, diagnose, and treat diabetes-related foot ulcers among homeless people.
In an update presented earlier this year, Nguyen reported her team has partnered with two community centers— one in a rural area and one in an urban community—to provide comprehensive and multidisciplinary diabetic foot care. For its next event, Nguyen anticipates recruiting pulmonologists and thoracic surgeons as well.
Results from her first event prompted the team to modify outreach site selections to better identify at-risk populations and to serve more homeless participants. The participation number increased by almost 50 % between her first and second events. Finally, with a goal to ensure followup by enrolling eligible patients in a state-sponsored free medical insurance program, the team identified 12 high-risk patients from the two most recent mobile clinics and arranged appropriate follow-up care for them.
To learn more about VC4U, visit vascular. org/Vascular-Care-for-the-Underserved.
Joseph Mills
Rym El Khoury
COMMENT& ANALYSIS
Resident unionization: Could it be a step toward equity in healthcare training?
By Saranya Sundaram, MD
IN THE COMPLEX LANDSCAPE OF HEALTHCARE, medical residents are vital players, balancing the demands of rigorous training while providing invaluable patient care. However, despite their significant contributions, residents often face challenging working conditions, long hours, and inadequate support systems. Recent movements towards unionization among medical residents reflect a collective effort to advocate for better working conditions, equitable treatment, and mental wellbeing.
Unionizing offers medical residents a platform to voice their concerns and negotiate as a unified group. This is particularly essential in an environment where individual residents may feel powerless against institutional practices. This is most pronounced within the surgical community, where the responsibilities/work hours expected of residents remain greatly disproportionate to the amount of residents available to perform those duties. In a study published in JAMA this year, the most commonly reported benefit from unionization was “increased salary stipends and/or housing stipends,” which suggest unions have been successful in securing ade-
quate compensation for hours worked.1
One of the most pressing concerns driving the push for unionization is the issue of burnout and stress among residents. The demanding hours, often exceeding the legally mandated limits, coupled with high-stakes responsibilities, can lead to detrimental physical and emotional effects. Studies indicate that burnout among medical residents can lead to decreased patient safety and negatively impact the quality of care provided. Examples of benefits that unions have fought for include the right for pregnant residents to reject 24-hour shifts at the University of Washington and increased salaries for “hurricane shifts” at the University of Miami.2
common. Concerns regarding potential disruptions in the training process or pushback against institutional structures can arise.
Moreover, unionization can enhance the overall experience of residency programs. A union can advocate for better educational opportunities, improved mentorship, and access to training resources that are crucial for professional development. When residents are part of a union, they can push for a more structured and supportive training environment that prioritizes learning and personal growth. Unions can also negotiate for more competitive compensation packages, as well as better benefits, including health insurance and housing stipends.3 This financial support is essential, particularly in high-cost living areas, where many residents struggle to make ends meet while fulfilling their demanding roles. Additionally, organizing as a union empowers residents to participate in broader conversations about healthcare reform. A resident union can serve as a powerful voice at the policymaking table, advocating for reforms that improve not only the residency experience but also patient care standards and healthcare accessibility.
Resistance to unionization from institutional leaders is
However, successful unionization efforts have demonstrated that collaboration between administration and residents can result in improved conditions without compromising the educational integrity of residency programs. Balancing the needs of residents with the goals of healthcare institutions is crucial to fostering a beneficial partnership. Though this may not necessarily require formal unionization at every institution, it begs the question of whether we are doing enough to provide residents with adequate agency to determine appropriate workplace conditions.
Allowing for unionization, when appropriate, could be a step toward a more equitable and supportive environment in healthcare, ultimately benefiting residents, patients and the broader healthcare system alike.
References
1. Foote DC, Rosenblatt AE, Amortegui D, et al. Experiences With Unionization Among General Surgery Resident Physicians, Faculty, and Staff. JAMA Netw Open 2024;7(7):e2421676.
2. Stacy Weiner. Thousands of medical residents are unionizing. Here’s what that means for doctors, hospitals, and the patients they serve. AAMC News. June 7, 2022
3. Hendrix JM, Burgart AM, Baker EB, Wolman RL, Kras JF. Physician Unionization: Opportunities and Challenges for Anesthesiologists in the United States. Anesth Analg. 2024 Aug 1;139(2):432–438
SARANYA SUNDARAM is Vascular Specialist’s resident/ fellow editor.
Saranya Sundaram
STUDY REPORTS LACK OF EVIDENCE TO SUPPORT THEORY THAT HOSPITAL INTEGRATION IMPROVES VALUE OF HEALTHCARE
By Bryan Kay
A SYSTEMATIC REVIEW OF U.S. literature focused on analyzing the effects of mergers and acquisitions on healthcare suggests that there is a lack of evidence to support the theory that integration is an effective strategy for improving the value of care delivery, according to the study authors.
“In the last 30 years, consolidation of healthcare systems in the United States has accelerated through mergers and acquisitions,” Bhagwan Satiani, MD, and colleagues write in the Journal of the American College of Surgeons (JACS). “We completed a systematic literature review on integration to determine if its reputation for enhancing the value of healthcare by reducing price and cost/spending and improving overall quality of care is justified.”
The authors found that, in papers published from 1990–2024, neither horizontal integration (joining two or more hospitals) nor vertical integration (the merging of physicians and hospitals) has been found to result in “consistent and significant improvements
in price, cost/spending, or quality associated with healthcare delivery.”
The authors screened 1,297 articles and identified 37 that met inclusion criteria. Results from any form of integration were mixed, they reported. Thirteen of 14 studies (93%) about price reported price increases. Thirteen of 16 (81%) about cost/spending showed cost increases or no change. Twenty of 26 studies (77%) about quality showed reductions or no change from integration.
“This finding represents an opportunity for healthcare leaders, including surgeons, to better define value in their efforts to im prove quality while balancing the financial stability of the healthcare industry with a focus on benefiting the patient,” Satiani and colleagues conclude.
Satiani, professor of surgery emeritus at The Ohio State University College of Medicine, Columbus, Ohio, and a Vascular Specialist associate ed itor, writes frequently for this publication on the topics of hospital administration and
how healthcare is delivered.
In a column published in the July edition entitled “Beyond private equity: A new sheriff in town,” Satiani explored the entrance of insurance companies into the physician practice acquisition market.
“When hospitals—which have integrated horizontally, vertically and every which way to consolidate and hire thousands of physicians— complain about the insurance companies buying physician practices, we better pay attention,” he wrote.
physician practices that are dominant in certain markets is their poor record related to passing on any savings to employers and ultimately patients.”
In the article, Satiani pondered what might be ahead “It is possible we may have three or four vertically and horizontally integrated for-profit juggernauts serving the entire healthcare supply chain or a single payor system,” he considered.
“Insurers like UnitedHealth Group now employ not only more physicians than the health systems, but they also own data analytic centers, accountable care organizations, office-based labs (OBLs), pharmacy benefit managers, urgent care centers, nursing homes, behavioral and mental health centers, and nursing schools.
“A recent example is the large acquisition of Wisconsin-based ProHealth Care, armed with 800 employees to manage the revenue cycle, information technology and data analytics. The strategy is to build out the back office to support the workers. Amazon-like, isn’t it? A particular concern with insurer-owned
“It is like the Wild West and Dodge City right now. Is it possible for physicians to ‘get outta Dodge’ and escape from this scenario? Is it possible that we will see a repeat of the hospital acquisitions of the 1980s and the accompanying financial disaster?”
“This finding represents an opportunity for healthcare leaders, including surgeons, to better define value in their efforts to improve quality”
BHAGWAN SATIANI
Journal of the American College of Surgeons
Bhagwan Satiani
SOCIETY BRIEFS
Compiled by Marlén Gomez and Beth Bales
Past SAVC Award recipients reflect on impact
WITH NOMINATION DEADLINES NOW past, Section on Ambulatory Vascular Care (SAVC) award season is upon us, and past recipients of the Society for Vascular Surgery (SVS) awards reflect on how the recognition has shaped their careers and advanced vascular care in their communities.
This year marks the inaugural awards cycle for SAVC, which was formed in 2024 by merging the Section on Outpatient and Office Vascular Care (SOOVC) and the Community Practice Section (CPS).
Enrico Ascher, MD, a previous recipient of the Excellence in Community Practice Award, said the recognition highlighted his dedication to building the first vascular institute in Brooklyn, New York. “I can’t tell you how proud and humbled I am by this very special recognition,” Ascher said.
Chong Li, MD, who received the Research Seed Grant from the former SOOVC, credited the award with enabling him to pursue groundbreaking research.
“I am honored and thankful for having received the SOOVC Research Grant to realize my proposal of finding the adequate and safe dosage of heparin during outpatient arterial and venous interventions,” Li said.
Olga Bakayev, MD (pictured, center), a recipient of the Presentation Award, described the recognition as a reflection of her team’s dedication to advancing knowledge in vascular care.
The 2025 award recipients will be announced at the 2025 Vascular Annual Meeting (VAM), scheduled for June 4–7, in New Orleans.
For more information about the SAVC awards or to apply, visit vascular.org/SAVC
Year-end giving campaign
THE SVS FOUNDATION CLOSED THE year rallying support for its year-end giving campaign, building on the momentum of Giving Tuesday to fund research that transforms lives.
Giving Tuesday, held Dec. 3, had a $20,000 match from W. L. Gore Associates, Inc., with every donation going further to fuel groundbreaking research, patient education and innovative programs. The foundation celebrated a historic milestone in 2024 with the inaugural James S.T. Yao Resident Research Award. Visit give.vascular.org
LEGISLATION TARGETS STABILITY FOR PHYSICIANS AMID MEDICARE CUTS
PHYSICIANS ARE FACING A FIFTH CONSECUTIVE YEAR OF MEDICARE
payment reductions due to policy adjustments and budget neutrality requirements in the Medicare Physician Fee Schedule. To address the issue, the SVS, in collaboration with congressional leaders and other physician organizations, advocates for a sustainable solution to protect medical practices and ensure patient access to care.
The push for reform has led to the introduction of the Medicare Patient Access and Practice Stabilization Act of 2024 (H.R. 10073). The bipartisan bill proposes a twopart solution: eliminating the scheduled payment cuts and providing an additional adjustment equal to 50% of the Medicare Economic Index (MEI). Together, these measures would deliver a 4.73% positive payment update for physicians in 2025.
The legislation follows months of advocacy, including a “Dear Colleague” letter signed by 233 members of Congress urging action to stabilize physician payment structures. The letter underscores the need for reforms to ensure physicians can deliver high-quality care to Medicare beneficiaries without financial hardship.
With H.R. 10073 now introduced, the SVS is urging its members to take action. Physicians are encouraged to reach out to lawmakers and advocate for two key steps: cosponsoring H.R. 10073, the Medicare Patient Access and Practice Stabilization Act, and pressuring congressional leaders to include the legislation in year-end policy negotiations.
If passed, H.R. 10073 could signal a significant shift in Medicare reimbursement policy, ensuring payment structures align with inflation and the realities of modern practice, providing stability for physicians and patients alike.
SVS members can send alerts to legislators through the SVS Grassroots Advocacy Center or by visiting vascular.org/Grassroots
SVS launches 2025 awards
THE SVS AND SVS FOUNDATION have opened applications for a variety of prestigious awards and scholarships for 2025, offering opportunities for medical students, residents, researchers and vascular surgeons to advance their careers and foster innovation in vascular surgery.
SVS Awards
SVS General Surgery Resident/ Medical Student Vascular Annual Meeting Travel Scholarship
Deadline: Jan. 6, at 4 p.m. EST
Apply at vascular.org/travelscholarship. International Scholars Program Deadline: Jan. 15
Apply at vascular.org/ internationalscholarsprogram. Lifetime Achievement Award and Medal for Innovation in Vascular
Smokers CAN-DO it
JUST 18 MONTHS AFTER ITS creation, the SVS Vascular Quality Initiative (VQI) Smoking Cessation Initiative is in full swing, with posters to be available this month and a year-long webinar series on quitting smoking to start in January 2025.
VQI introduced CAN-DO (Choosing Against combustible Nicotine Despite Obstacles) at the 2023 Vascular Annual Meeting (VAM). The SVS website now includes an updated patient section called “Your Vascular Health.” Its “Healthy Living” section includes a major focus on quitting smoking. A printable poster on smoking cessation is now available. In addition, SVS VQI Director of Quality Betsy Wymer obtained her Certified Tobacco Treatment Specialist Certification. A webinar series will be based on the education she received during that training course, with the first session set for 1 p.m. CST on Jan. 28, 2025.
Visit www.vqi.org or vascular.org/ VQI for more information.
Renew Membership Today
DUES FOR 2025 FALL DEC. 31, which means SVS members have time to fit that into their calendars before we usher in the New Year.
Members in good standing will continue to receive their Journal of Vascular Surgery peer-reviewed publication and keep utilizing items such as practice management resources and the online SVSConnect community.
To renew, visit vascular.org/invoices
VAM 2025 abstracts
Surgery
Nomination Deadline: March 1
Apply at vascular.org/ medalofinnovation.
SVS Foundation Awards
James S.T. Yao Resident Research Award
Deadline: Jan. 8
Apply at vascular.org/YaoRRA. Student Research Fellowship Deadline: Feb. 1
Apply at vascular.org/ studentresearchfellowship. Clinical Research Seed Grant Deadline: March 1, 2025
Apply at vascular.org/ clinicalresearchgrant.
Visit vascular.org for full details on each award and its application process
VASCULAR SURGEON-SCIENTISTS are invited to submit research abstracts for the 2025 Vascular Annual Meeting (VAM) in New Orleans (June 4–7). The submission period, which began Nov. 6, closes Wednesday, Jan. 8, 2025. In 2024, nearly 800 abstracts were submitted, with more than 400 included in the program.
Broad submission categories for VAM 2025 include aortic disease, basic research, cerebrovascular disease, complications, dialysis access, healthcare disparities, peripheral arterial disease, vascular trauma and more.
For submission guidelines, visit vascular. org/VAM25Program
CLINICAL&DEVICENEWS
Compiled
by
Jocelyn Hudson and Bryan Kay
In search of the ‘holy grail’: New analysis brings aneurysm rupture prediction closer, but more data needed
Arupture prediction-based algorithm is set to enhance patient selection for abdominal aortic aneurysm (AAA) repair. This is according to Randy Moore, MD, a vascular surgeon at the University of Calgary in Calgary, Canada, who, at the 2024 VEITHsymposium (Nov. 19–23) in New York City reported that the ViTAA system (ViTAA Medical) can predict rupture risk independent of aneurysm size and post-endovascular aneurysm repair (EVAR) neck behavior.
Before sharing the results of a retrospective analysis of computed tomography (CT) factors determining AAA wall weakness and strength in AAAs, Moore—who is chief medical officer for ViTAA Medical—began his presentation by outlining an unsuccessful case that highlighted for him an unmet need in vascular surgery. Showing a CT scan, the presenter recalled: “Fifteen years ago, this patient died on my operating table. He wasn’t supposed to die; his aneurysm was small, and I was following guidelines.”
Moore noted that cases such as this are not unique. “In fact,” he said, “a number of large database studies with thousands of patients have demonstrated that up to 12% of patients may have a rupture below size threshold.” Despite this, Moore highlighted that there are investigators who are suggesting the size thresholds for repair can safely be increased due to a low overall risk of rupture.
Moore’s explanation for this “confusion” is the “absolute reliance on AAA size to risk stratify.” In his VEITHsymposium presentation, it was Moore’s aim to suggest to the audience that this firm trust in aneurysm size “remains fundamentally flawed.” “We really need to analyze the aortic wall,” he said. “That’s the key.”
Other investigators have tried to analyze the aortic wall using traditional finite element analyses and stress-based indices, Moore shared, before noting that several publications in the engineering space have underscored the deficits of such strategies. “You’re not taking into account the actual intrinsic patient wall characteristics,” the presenter stated. “In other words, the same stress or force applied to two aortas is going to give you two different clinical outcomes based on the tissue characteristics.”
Carotid stenting: First patient enrolled in CGUARDIANS II pivotal study INSPIREMD ANNOUNCED THAT THE FIRST patient has been enrolled in the company’s CGUARDIANS II clinical trial evaluating its CGuard Prime carotid stent system in patients undergoing carotid artery stenting (CAS) via the transcarotid artery revascularization (TCAR) approach. The patient was enrolled by Patrick Muck, MD, chief of vascular surgery at Good Samaritan Hospital, part of the TriHealth System in Cincinnati, Ohio. Muck serves as both the site principal investigator as well as a co-lead investigator of the CGUARDIANS II study. CGUARDIANS II is a prospective,
“We took a different tack,” Moore told the VEITHsymposium audience. Over the past decade, the presenter recounted that he and a team of engineers have processed over 200 aortic specimens. The aim has been “to develop technology that precisely takes into account the integral strength of the aortic wall,” Moore shared.
The presenter explained that, based on a cardiac-gated scan that allows a clinician to track the motion of the aortic wall, data are uploaded to the cloud where a combination of algorithms assess the intraluminal thrombus thickness, time-averaged wall shear stress with computational fluid dynamics and a peak strain module, all of which are then combined as an output called a regional aortic weakness (RAW) map.
“These maps allow you for the first time to virtually assess the mechanical properties of the aortic wall, not based on population data but based on the individual patient sitting in front of you in the clinic,” Moore elaborated. “We now have an AAA wall analysis that includes wall tissue strength characteristics irrespective of size.”
On use of the technology so far, Moore reported that it has played a role in analyzing landing zones for EVAR and has demonstrated that implanting a stent into a weak infrarenal aortic neck is more likely to result in a type 1 endoleak. “That’s not a surprise,” Moore commented, “but now we can actually measure that.”
The technology can also be used for surveillance, Moore continued. He explained that this is due to its ability to analyze peak strain post-EVAR and to point out “which endoleaks actually need to be treated, and which can be safely ignored.”
Furthermore, Moore shared that the technology is being used with artificial intelligence (AI) algorithms to predict rapid growth, which he describes as a “surrogate marker for negative outcomes.” These data were shared at the 2023 VEITHsymposium.
The “holy grail,” however, is rupture prediction. Moore detailed that he and his team previously published on the ability to identify the site of aortic rupture, but that the more recent aim had been to complete a study looking at the risk of rupture and the ability to predict rupture using the ViTAA technology. “This was a very difficult study to complete,” the presenter remarked, citing specifically the challenge of finding patients with images prior to rupture.
Moore detailed that he and colleagues retrospectively
multicenter, single-arm pivotal study that aims to enroll a minimum of 50 evaluable patients. The objective is to evaluate acute device success and technical success of the CGuard Prime when used in conjunction with a Food and Drug Administration (FDA)cleared TCAR neuroprotection system in patients at high risk for adverse events from carotid endarterectomy.
FEVAR: First-in-human implantation of BeFlared bridging stent BENTLEY REPORTED THE SUCCESSFUL first-in-human implantation of its recently CE-certified BeFlared stent graft system, which the company states is the world’s first dedicated bridging stent for fenestrated endovascular
reviewed 38 patients with rupture and matched them in terms of size, age and demographics to 38 non-ruptured patients before conducting a ViTAA analysis. “We wanted to make sure we included patients who had a range of aneurysm sizes to reflect real-world practice—roughly 4.6cm all the way up to 12cm,” he said. The team then completed a traditional analysis using finite element and stressbased indices, finding no statistical difference between ruptured and nonruptured patients. With the ViTAA analysis, however, Moore reported that the team was able to identify a “highly predictive” tool and one that “provides the clinician with an at-a-glance interpretation of aortic wall risk with an accuracy of 92%, a sensitivity for rupture prediction of 100%, specificity of 83% and an area under the curve of 86%.”
“Our AAA wall analysis based on tissue strength and strain allows for patient-specific wall maps that will eventually allow us to more precisely inform patient care,” Moore concluded. “We have a rupture prediction algorithm that will enhance patient selection for repair so that patients like mine 15 years ago will no longer die unnecessarily.”
In Moore’s closing statement, he outlined the longer-term goal of “no longer seeing exclusive reliance on aortic size to determine patient care.”
Data collection ‘absolutely crucial’
In discussion time following Moore’s presentation, Rao Vallabhaneni, MD, a professor of vascular surgery at the University of Liverpool in Liverpool, England, commented on the potential limitations of the 38-patient sample size of the study.
“The difficulty is the great heterogeneity within one person’s aneurysm from different areas of the same aneurysm and between patients,” Vallabhaneni began. “It is such highly heterogenous tissue that I don’t think your sampling is enough to develop a reliable tool.”
While acknowledging Vallabhaneni’s concern, Moore stressed that “the proof is in the pudding.” “With a limited number of 38 ruptured patients, we showed a sensitivity of 100% in terms of rupture prediction,” he reiterated.
However, Moore closed his reply by agreeing with Vallabhaneni that data accumulation is “absolutely critical,” going on to share that he and his team have initiated a series of prospective registries they hope will answer further questions about the technology.
aneurysm repair (FEVAR).
The procedure was performed by Stéphan Haulon, MD, a vascular surgeon at the Hôpital Marie Lannelongue in Paris, France.
“I am happy to report that the BeFlared met all our expectations regarding ease of use during the intervention, duration and matching the requirements of the patient’s anatomy,” Haulon said. “The recent certification of the BeFlared marks a milestone in the endovascular treatment of aortic aneurysms as it allows [us] to shorten procedure times and therefore reduce X-ray exposure to patients and operation staff significantly. This ‘two-in-one’ device creates a new standard for bridging stents in FEVAR procedures. The BeFlared is a gamechanger as it makes these interventions safer, faster and enables better outcomes for the patients.” he added.
The BeFlared will be officially launched at Leipzig Interventional Course (LINC 2025; Jan. 28–30) in Leipzig, Germany.
Microbot Medical announces FDA submission for commercialization of Liberty endovascular robotic system MICROBOT MEDICAL RECENTLY announced that it has submitted a 510(k) premarket notification to the Food and Drug Administration (FDA) for its Liberty endovascular robotic system.
A company press release details that Liberty is the world’s first single-use, fully disposable robotic system for endovascular procedures. The 510(k) submission follows the successful completion of a multicenter, single-arm trial to evaluate the performance and safety of Liberty in human subjects undergoing peripheral vascular interventions.