2 Guest editorial Less vain, more vein: Perceptions of venous disease
6 Stroke VEITH 2023 plays host to lively debate over CMS decision to expand coverage of carotid artery stenting
11 Comment & Analysis
Christopher White rebuts recent editorial, ‘Sex, lies and carotid stents’
15 Smoking SVS members pitch in to help their patients kick the habit
www.vascularspecialistonline.com
CHANGING COURSE?
The natural history of tibial claudication comes under scrutiny as interventions for ‘relatively benign’ disease trend upward
By Bryan Kay
n the end, reflected Michael S. Conte, MD, “it’s not the evidence.” The leading vascular surgeon and peripheral arterial disease (PAD) expert made the bold statement during the recent 2023 VEITHsymposium (Nov. 14–18) as he pointedly asked a room full of colleagues: what is behind the trend that appears to show tibial interventions for intermittent claudication are growing?
The question of whether or not the practice carries a reasonable risk or, rather, if the risks “exceed the benefits” has long lingered, the chief of vascular and endovascular surgery at the University of California San Francisco (UCSF) told the New York City gathering.
Ultimately, the preponderance of the data, Conte said, suggests the latter.
So what of those reasons behind the recent trend? Conte, finding his rhythm, first turned to datasets outlining pattern of use.
Vascular Quality Initiative (VQI) data from 2003–2018 demonstrated that about 11% of claudication interventions involved infrapopliteal arteries, with isolated infrapopliteal interventions or combined interventions associated with a higher risk for major amputation compared to femoropopliteal interventions alone, he said. “This finding was particularly true in patients with diabetes,” Conte added.
Then to some of the factors potentially responsible: One research group looked at the influence of a competitive marketplace and found that working in an area with high market competition seemed to be associated with a higher rate of using tibial interventions—particularly atherectomy—for claudication patients. “I guess, if you have a lot of competition around you, you may be prone to be more aggressive in the patients that you treat; these data seem to imply that competition
GUEST EDITORIAL
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | Professor HansHenning Eckstein, MD | John F. Eidt, MD
| Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor Christopher Audu, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Managing Editor SVS Beth Bales
Manager of Marketing
Kristin Spencer Communications Specialist
Marlén Gomez
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Content Director Urmila Kerslake
Head of Global News Sean Langer
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell, Éva Malpass and George Barker
Design Terry Hawes and Wes Mitchell
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America 155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
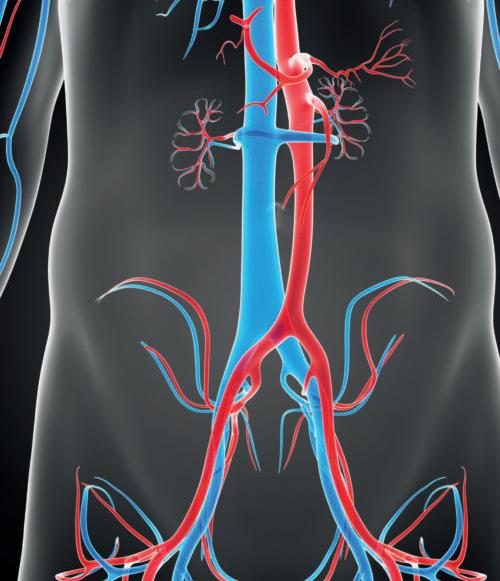
Less vain and more vein: Evaluating the perceptions of venous disease amongst the vascular surgery community
By Sarah Wells, MS, Eric Pillado, MD, and Laura M. Drudi, MD
Our biases permeate the fabric of our very being, as they weave their way into our training and practice. It is clear that complex aortic work is definitely in vogue and “in,” and, well... treating veins gets a bad rap. While training, our staff perpetually complained about not only treating venous disease but not having the patience to sit and listen to these “complex” patients. Current vascular surgery training paradigms focus significantly on arterial disease, and training programs rarely focus on venous disease management as part of the core curriculum. It comes as no surprise that if those teaching the next generation of vascular specialists are not enthusiastic or motivated and possibly even deterring the pursuit of treating venous disease, the next generation will face similar sentiments. It is clear that not all vascular systems are created equal, but why?
The management of venous disease is imperative, as it has been reported to be twice as prevalent as coronary heart disease and five times more prevalent than peripheral arterial disease (PAD). More than 25 million adults in the U.S. suffer from chronic venous insufficiency, with more than 6 million having advanced venous disease.2
Further, venous disease cost of care is estimated to range from $3 to $10 billion annually.2,4 However, there seems to be a discrepancy in its perceived importance among vascular surgery specialists.
surgeons must navigate in a similar way as they do with arterial diseases.
It cannot go unsaid that vascular surgery is a maledominated specialization and that, interestingly enough, the perception that venous diseases are of less importance stemmed mainly from younger female respondents. It is difficult to disseminate clearly why this may be the case, but the survey data suggest that this disparity in perception paves the way for a key new body of research. An in-depth analysis of existing and potentially inherent gender-based values as drivers for framing systemic perceptions in vascular surgery could be a valuable step in reducing gender bias within the field.
$3-10bn
Cost of venous care annually
It has been proposed that there exists a lack of adequate, specific and practical training throughout the academic curriculum presented to future vascular surgeons, which has led to the view that venous pathology, compared to arterial conditions, is of secondary nature.
In addition to this, themes such as less technical challenge, lower morbidity/mortality risk, ease of lifestyle, less institutional support for research or clinical programs, and fewer funding opportunities were highlighted as reasons for the existence of this perception in a survey on the topic Furthermore, the terms “ego” and “prestige” were mentioned when describing rationales for arterial work being more important than those in the field of venous disease.1
Vascular surgeons continue to be the largest provider for venous disease care in both medical and surgical specialties.3 More than 17% of all medical and surgical venous care providers do not have active board certification. Therefore, it behooves our specialty to uphold best practices in venous disease and continue to better understand the venous disease population. Our versatility in open and endovenous surgical management provides our specialty the skillset to care for venous disease when compared to other specialties.
Another important and complex layer involved in this perception of venous and arterial work differing in value is gender bias and disparity. There is a significant lack of literature in venous disease compared to arterial disease regarding healthcare disparities.
Racial/ethnic, gender and socioeconomic disparities impact venous disease similarly to arterial disease, driving how we approach our patients’ care. Chronic venous insufficiency can involve a difficult disease pattern superimposed with various risk factors that vascular
The scarce exposure of trainees to the array of levels of venous interventions that exist seems to have driven and deeply embedded this perception that venous work is less of a challenge, and, in turn, of less interest to vascular specialists
Above all, the scarce exposure of trainees to the array of levels of venous interventions that exist seems to have driven and deeply embedded this perception that venous work is less of a challenge, and, in turn, of less interest to vascular specialists. As vascular surgery residents and fellows have reported feeling deficient in venous training, this is logically a root cause in the lack of value it has been historically attributed.
One could argue it is ironic, as venous diseases pathologies are often complex, even more so than arterial ones, yet lack of attention to this nature during training is a recurring theme. A shift in this perception, however, is necessary. Potential avenues for improving such a deficit could include various mandates with regard to trainee exposure to venous pathologies and interventions, as well as the inclusion of continuing education initiatives, similar to that of advanced aortic training and formal limb salvage. Addressing and reducing the gender bias in existing perceptions may also pave the way for a more equitable view of both venous and arterial work.
References
1. Kiguchi MM, Drudi LM, Jazaeri O, Smeds MR, Aulivola B, MacCallum K, et al. Exploring the perception of venous disease within vascular surgery. JVS: Venous and Lymphatic Disorders, 2023:11(5);1063–1069.
2. Kim, Young, et al. Defining the human and healthcare costs of chronic venous insufficiency. Seminars in Vascular Surgery, vol. 34, no. 1, Mar. 2021, pp. 59–64. DOI.org (Crossref), https://doi.org/10.1053/j.semvascsurg.2021.02.007.
3. Gabel, Josh, et al. Who is treating venous disease in America today? Journal of Vascular Surgery: Venous and Lymphatic Disorders, vol. 7, no. 4, July 2019, pp. 610–14. DOI.org (Crossref), https://doi.org/10.1016/j. jvsv.2019.03.009.
4. O’Banion, Leigh Ann, et al. A review of the current literature of ethnic, gender and socioeconomic disparities in venous disease. Journal of Vascular Surgery: Venous and Lymphatic Disorders, vol. 11, no. 4, July 2023, pp. 682–87. DOI.org (Crossref), https://doi.org/10.1016/j.jvsv.2023.03.006.
SARAH WELLS is a clinical research assistant at Centre Hospitalier de l’Université de Montréal (CHUM) in Montreal, Canada; ERIC PILLADO is an integrated vascular surgery resident at Northwestern Medicine in Chicago; and LAURA M. DRUDI is an assistant professor of surgery at CHUM.
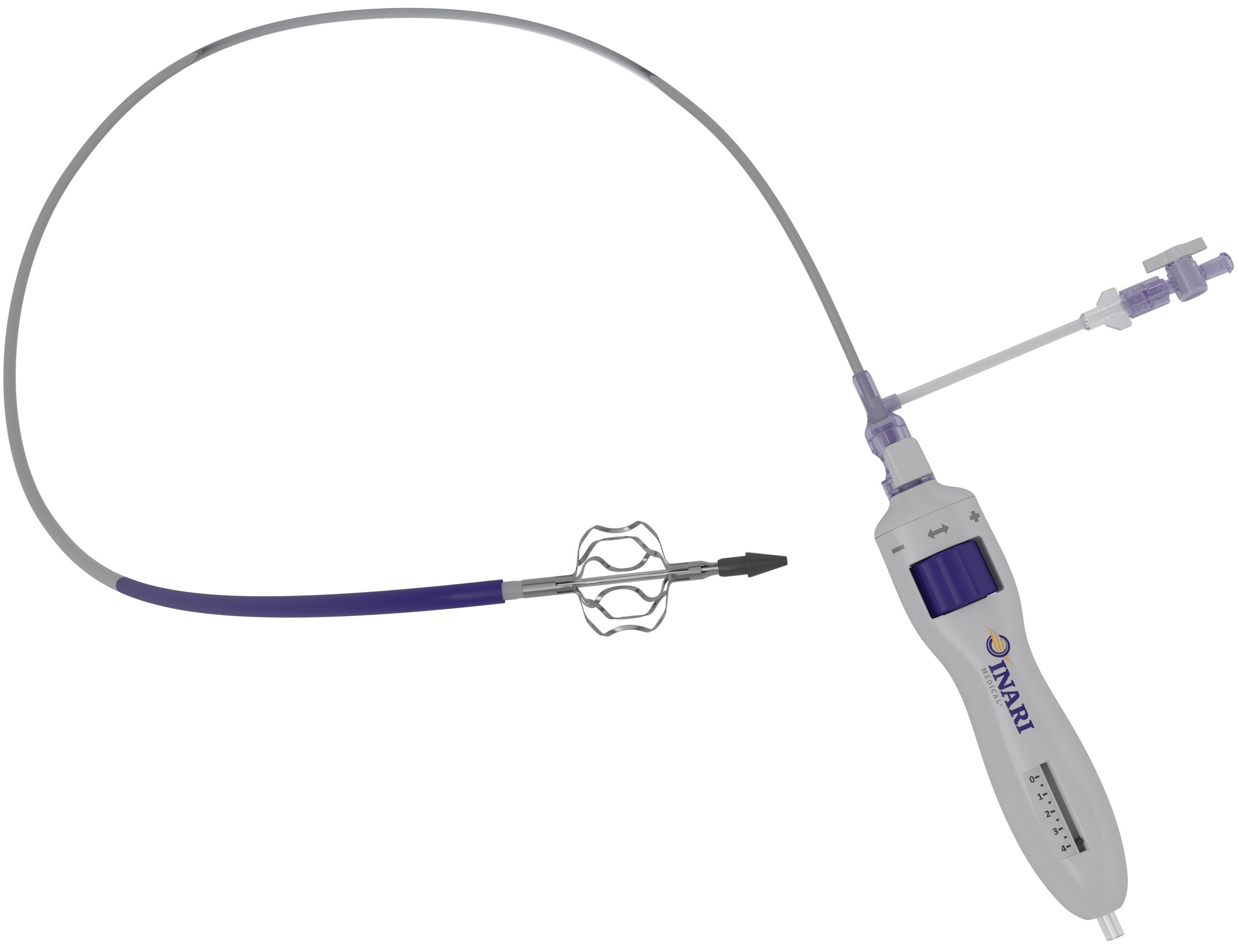
RevCore™ Thrombectomy Catheter
Right Size, Every Time
Expandable element to treat vessels 6 - 20 mm in diameter
Complete Control
Accurate and immediate torque response in targeted segment
FROM THE COVER CHANGING COURSE: THE NATURAL
HISTORY OF TIBIAL CLAUDICATION COMES UNDER SCRUTINY
continued from page 1
in the area affects the utilization of tibial interventions in claudicants,” Conte said.
He moved onto Medicare data from 2017–2019. “Now you can see the numbers are a little bit different: 28% of all claudication interventions involved infrapopliteal arteries, and of these more than a third were isolated infrapopliteal and about a third were multiple tibial arteries,” Conte continued. “This pattern was more prevalent in patients who are Black, Hispanic and who had kidney disease.” He delved deeper, pointing to evidence showing that the providers who were associated with higher use were more likely to be early-career interventionalists or surgeons, in the western half of the U.S., in higher volume practices, more often based at ambulatory surgery centers (ASCs) or office-based labs (OBLs), and more commonly interventionalists versus vascular surgeons.
Conte then turned to recent VQI-VISION (Vascular Implant Surveillance and Interventional Outcomes Network) data on patients who received infrapopliteal interventions, presented at last year’s VAM.
“You can see looking downstream that the risk of conversion to chronic limb-threatening ischemia [CLTI] was significantly higher among patients who underwent tibial interventions versus patients who had isolated femoropopliteal interventions for claudication—and the risk of needing repeat interventions was significantly higher, suggesting that patients getting these procedures are being placed at greater risk for deterioration of their disease and multiple additional procedures,” he explained.
As the data pile up, and many have questioned the wisdom of such interventions, Conte asked: “Are we really doing the right thing?”
“This alarming trend, from 11% to more recently
SVS RECEIVES CMSS GRANT TO ADVANCE DIAGNOSTIC EXCELLENCE SCREENING
T
he SVS has received a $100,000 grant from the Council of Medical Specialty Societies (CMSS) to promote diagnostic excellence across the medical field.
The CMSS, a coalition of 53 specialty societies representing over 800,000 physicians, has recognized the importance of enhancing capabilities in healthcare and has committed resources to support innovative projects in this area. The SVS proposal, “Advancing diagnosis and staging for early detection and treatment of peripheral arterial disease [PAD] to prevent amputation,” is one of 11 grant recipients.
The grant plays a significant role in the SVS’ commitment to improving patient care, said SVS Director of Clinical Guidelines and Quality Practice Reva Bhushan, PhD, who helped secure the grant.
“Vascular surgeons and their care teams play a key role in screening and managing PAD patients. This
around 30% of peripheral vascular interventions in the U.S. involving a tibial artery for claudication, suggests we may be at risk of changing the natural history of a relatively benign disease,” he summarized.
Conte went further. A systematic review that looked at 11 studies covering current conservative management and intervention, and 16 studies probing peripheral vascular interventions or open surgery for claudication “found that there were consistently higher rates of major amputation or repeat intervention associated with revascularization, and particularly with tibial interventions,” he said.
What of the guidelines and appropriate use criteria (AUC) in the arena of treatment for intermittent claudication? It’s a mixed bag, said Conte. While the Society for Vascular Surgery (SVS) guidelines from 2015 recommend against endovascular therapies for isolated infrapopliteal disease for claudication “because it is of unproven benefit and possibly harmful,” other bodies, such as the Society for Cardiovascular Angiography & Interventions (SCAI), suggest that “this practice may be occasionally or rarely appropriate,” Conte said.
The recent SVS AUC for intermittent claudication, a multispecialty collaboration, saw unanimous agreement that the risks outweighed the benefits regarding revascularization for infrapopliteal disease, he added.
So, to Conte’s original question: what explains the increasing use of tibial interventions for claudication? “It certainly is not the evidence that it is helping people, because the evidence is simply not there to support this concept of full revascularization for claudication, with
grant will allow the SVS to promote the use of diagnostic, staging and quality-of-life tools for patient assessment to prevent chronic limb-threatening ischemia [CLTI] and amputation,” said Bhushan.
CMSS projects focus on three categories of conditions known to cause a disproportionate share of preventable harm due to suboptimal diagnosis: cancer, cardiovascular disease and infection.
The grant program, administered by CMSS and funded by the Gordon and Betty Moore Foundation and The John A. Hartford Foundation, assists medical specialty societies in promoting analytical excellence for clinicians and patients. “Diagnostic excellence is fundamental to the health and well-being of all people, especially older adults who often have multiple chronic conditions complicated by frailty,” said Terry Fulmer, PhD, RN, president of The John A. Hartford Foundation.
“With the generous support of our funders, 20 specialties are actively engaging their members in diagnostic excellence,” said CMSS CEO Helen Burstin, MD, MPH.
“The legacy of the CMSS grant program will be greater awareness, attention and action to prevent avoidable diagnostic harm across medicine.”—Marlén Gomez
treatment of every lesion in sight on the angiogram,” Conte elaborated.
The data suggests other practice-level factors may be at play, he reflected: economic incentives and the current reimbursement framework; elevated use in ASCs and OBLs; strong associations with atherectomy; higher use among certain types of providers; meetings where live
“This trend, from 11% to more recently around 30% of peripheral vascular interventions in the U.S. involving a tibial artery for claudication, suggests we may be at risk of changing the natural history of a relatively benign disease”
MICHAEL CONTE
case demonstrations focus on technical elements of the interventions rather than their appropriateness.
“I guess that some providers believe that the short-term risk of these interventions is low, and the downstream harms are not tangible at the time, so they have convinced themselves they may be providing a benefit,” Conte concluded.
“That’s certainly not a basis for evidence-based practice, and with growing signals of harm, the vascular community needs to address the overuse and misuse of interventions that will erode the public trust.”
CAREER
SVS urges active participation on compensation survey
THE SVS ENCOURAGES MEMBERS to participate in a compensation survey, a collaboration with Phairify, that aims to provide vascular surgeons with tailored insights into compensation, practice and productivity data relevant to their specialty and practice situations, helping them make informed career decisions.
The SVS seeks a 20% response rate from its members to ensure the survey’s scientific validity.
of compensation and practice trends within our specialty. Your participation is key to the success of this initiative,” he said.
Phairify, a web-based data collection and visualization platform, offers free access to SVS members. Members can complete an anonymous 15-minute survey that allows them to filter and access compensation, productivity and practice data specific to the specialty. The survey provides members with a better understanding of their compensation and productivity through data comparisons with their peers.
Keith Calligaro
“Ensuring a robust response rate from SVS members is crucial for the scientific credibility of the compensation survey,” said Keith Calligaro, MD, chair of the SVS Compensation/Phairify Committee that developed the survey. “The data obtained will not only benefit individual vascular surgeons, but will also contribute to a comprehensive understanding
20%
response rate required
Members can participate by visiting vascular.org/CompensationStudy2023
“Over the last few years, many SVS members have noted that when vascular surgeons apply for a job somewhere—whether after completing a fellowship or a mid-career move—they are not sure what to expect in terms of financial compensation. This survey will help in terms of dealing with future employers, what to expect and maybe even what to ask for,” Calligaro previously stated when assessing the importance of the survey.—Marlén Gomez
Michael Conte
Risks may include: abrupt or subacute closure, pseudo-aneurysm, thrombosis, allergic reaction to device materials or procedural medications, arterial injury (such as dissection, perforation, or rupture), embolism, hematoma, and hemorrhage. Indications, contraindications, warnings, and instructions for use can be found in the product labeling supplied with each device.
CAUTION: Federal (USA) law restricts this product for sale by or on the order of a physician.
1 Medtronic data on file, Final Study Report The Chocolate BAR CLR782.
‘There is no reliable way to measure carotid stenosis—methods have changed and tend to overestimate the degree of narrowing’
The recent move to expand Medicare coverage of carotid stenting formed the basis of a recent debate over the wisdom of the decision taken by CMS. Two heavyweights in the stroke arena went head-tohead, sparring over whether the decision should have been taken at all.
By Bryan Kay
Two luminaries in the field of stroke prevention weighed in on opposite sides of a still-raging debate over whether the recent decision by the Centers for Medicare & Medicaid Services (CMS) to expand Medicare coverage for carotid artery stenting (CAS) was the right move to make amid conflicting opinion on what the weight of the scientific evidence says on carotid revascularization interventions.
Thomas Brott, MD, a professor of neurology at the Mayo Clinic in Jacksonville, Florida, and a principal investigator of the ongoing and keenly followed CREST-2 (Carotid Revascularization Endarterectomy vs. Stenting Trial-2) study, and Anne Abbott, MD, a neurologist at Central Clinical School, Monash University, in Melbourne, Australia, took up opposing positions during the 2023 VEITHsymposium back-and-forth in New York City (Nov. 14–18).
Brott took up that position that, “Since TCAR [transcarotid artery revascularization] already has it, reimbursement for transfemoral and transbrachial carotid stenting should be expanded to include asymptomatic patients.” Abbott pushed back strongly, arguing, “There should be no reimbursement for CAS or TCAR in asymptomatic or symptomatic [patients].”
Brott took issue with recent published writings from Abbott in which she stated that stenting near the transaortic root causes more procedural stroke, death and heart attacks than does carotid endarterectomy (CEA); that there is no randomized trial evidence of patient benefit from any carotid procedure compared with current standards of non-invasive care alone; that crucially needed trials such as CREST-2 to assess procedural efficacy will be exceedingly difficult if not impossible to complete; and that the CMS funding changes “will open the floodgates.”
Regarding Abbott’s point on unfavorable outcomes in stenting vs. CEA near the transaortic root, “where she emphasizes randomized trial evidence,” Brott contended that “that’s not true for CREST; that’s not true for ACST-2 [Asymptomatic Carotid Surgery Trial-2]; it’s not true for ACT-1 [Asymptomatic Carotid Stenosis]; and it’s not true for the combined analysis of CREST and ACT-1—all randomized trials.”
the medical arm is actually the experimental arm in CREST-2.” Brott also addressed Abbott’s statement that crucially needed trials will be difficult, if not impossible, to complete. “CEA enrollment in CREST-2 is complete,” he argued. “With CAS enrollment, we have only got about 80 or so patients to go.” Finally, he focused on Abbott’s claim over the CMS funding changes and increased usage. “Atherosclerosis is getting less and less common,” he retorted. “We are seeing fewer and fewer patients. We don’t know what is going to happen, but the changes in medical care are decreasing the numbers of patients with asymptomatic carotid stenosis.”
Stepping up to the VEITH 2023 debate podium after Brott, Abbott hit back, standing behind her recent writings with which Brott took issue. “In a major coup for bad medicine, U.S. Medicare has just announced it finds coverage for carotid stenting is reasonable and necessary for beneficiaries with symptomatic carotid stenosis of at least 50%, or asymptomatic stenosis of at least 70%,” she told the gathering. “This is greatly expanded coverage, including to average-surgical-risk patients. Further CMS—or third-party—accreditation or certification are no longer required. Facilities will now be responsible for their own procedural standards and training. Formal shared decision-making with beneficiaries has been encouraged. Facility oversight committees are encouraged to apply published guidelines.”
“Guidelines worldwide are outdated and encourage procedural overuse. Procedural outcomes are highly dependent on operator expertise, and removal of externally applied standards will encourage harm”
ANNE ABBOTT
Brott turned to Abbott’s assertion of no randomized trial evidence of patient benefit from any carotid procedure compared to current standards of non-invasive care. “These are 70-year-old patients on average, and you can see here 10-year ipsilateral stroke [rates],” he said, pointing to a slide illustrating relevant data. “Six percent in CREST, 6% in ACST-2. Remember, these patients came in with risk factors for stroke, high-grade stenosis, and that is 0.6% per year in this patient population. In the United States, for a random population in that age group, any stroke is 0.6% per year. This is an achievement.”
Brott continued: “What about current standards of non-invasive care? With people that have high-grade carotid stenosis and all the attendant risks of that disease, we do not know. And that is why
She called the move “a major breach of U.S. Medicare’s duty of care to the public—and there are many reasons for this.” First, Abbott said stenting “does cause more harm” than CEA. “In randomized trials, stenting caused more 30-day periprocedural stroke, death and heart attack in symptomatic patients, and in a meta-analysis of randomized trials stenting caused more 30-day periprocedural stroke and death in asymptomatic patients,” she continued. “Stenting was worse with risk-factor long-term stroke rates, and registry stroke shows similar, if not worse, results with stenting compared to endarterectomy.”
Furthermore, Abbott argued that “there is no reliable way to measure carotid stenosis—methods have changed and tend to overestimate the degree of narrowing. Guidelines worldwide are outdated and encourage procedural overuse. Procedural outcomes are highly dependent on operator expertise, and removal of externally applied standards will encourage harm.”
Abbott also addressed the case of TCAR. “It has not been compared to endarterectomy,” she said, “and its efficacy has not been assessed and compared to non-invasive care alone, so there is no procedural indication and, in fact, there is no current procedural benefit for any carotid artery so-called revascularization procedure compared to current standards, particularly of best practice non-invasive care alone.”
At the debate conclusion, the VEITH 2023 audience overwhelming voted to back the arguments put forward by Abbott.
RESEARCHERS REPORT 30-DAY OUTCOME DATA FOR PAIR OF INVESTIGATIONAL CAROTID STENTING SYSTEMS
Thirty-day results from two trials assessing the performance of investigational carotid artery stenting systems—the Neuroguard and the CGuard—were recently presented at VIVA 2023.
Stenting with the CGuard embolic protection carotid stent system (InspireMD) in patients with carotid artery stenosis and at high risk for carotid endarterectomy (CEA) had a death (all-cause mortality), any stroke or myocardial infarction rate of 0.95%, from procedure through 30 days of follow-up, reported D. Christopher Metzger, MD, an interventional cardiologist at OhioHealth in Columbus, Ohio, at the Las Vegas meeting (Oct. 30–Nov. 2).
The C-GUARDIANS U.S. investigational device exemption (IDE) pivotal trial looked at 316 patients from July 2021–June 2023 who were prospectively enrolled in the singlearm study performed at 24 sites in the U.S. and Europe. The primary endpoint was a composite of either: incidence of major adverse events including death (all-cause mortality), any stroke or myocardial infarction through 30 days post-index procedure; or ipsilateral stroke from day 31 to day 365 post-procedure.
InspireMD anticipates reporting primary endpoint results from C-GUARDIANS—which the company stated may support a premarket approval (PMA) application to the Food and Drug Administration (FDA)— in the second half of 2024.
In the PERFORMANCE II prospective, multicenter study evaluating the safety and effectiveness of the Neuroguard (Contego Medical) integrated embolic protection (IEP) system, meanwhile, the 30-day stroke rate was 1.31% in the intention-to-treat analysis and 0.98% in a per-protocol analysis, with no major strokes or contralateral strokes, and all patients returning to baseline neurologically within 30 days, William Gray, MD, the system chief of cardiovascular disease at Main Line Health in Philadelphia, reported at VIVA 2023.
The PERFORMANCE II single-arm study is assessing the device among 305 patients at 40 clinical sites in the U.S. and Europe. At one-year followup (all stroke within 30 days, and ipsilateral stroke between day 31 and 12 months), the reported stroke rate was 1.68% in the intention-to-treat analysis and 1.35% in a per-protocol analysis, Gray said. No major strokes or neurological deaths occurred, he added.
In addition to the PERFORMANCE II trial—in which stents were placed via either transfemoral or transradial access—the PERFORMANCE III study is currently enrolling patients to evaluate the same stent placed via transcarotid access, Contego Medical reported. Bryan Kay
Clinical Confidence
iCast covered stent system
• First to market balloon expandable covered stent
• 6 Fr and 7 Fr compatible on all sizes
• Backed by years of real-world evidence in di cult lesions1
• Proven primary patency at 5 years2
1. Mwipatayi BP, Ouriel K, Anwari T, et al. A systematic review of covered balloon-expandable stents for treating aortoiliac occlusive disease. J Vasc Surg. 2020;72(4):1473-1486.e2. doi:10.1016/j.jvs.2020.01.084
2. Mwipatayi BP, Sharma S, Daneshmand A, et al. Durability of the balloon-expandable covered versus bare-metal stents in the Covered versus Balloon Expandable Stent Trial (COBEST) for the treatment of aortoiliac occlusive disease. J Vasc Surg. 2016;64(1):83-94.e1. doi:10.1016/j.jvs.2016.02.064
MACHINE LEARNING
UC San Diego surgeon-scientist secures NIH funding aimed at using AI models to predict PAD in diverse patient populations
By Bryan Kay
TEN YEARS AGO, ELSIE GYANG ROSS, MD, WAS a postdoctoral student with a background in computer science and an interest in healthcare policy. At that point, the ubiquity of artificial intelligence (AI) was still some way off, and the notion of AI intervening in one of the most costly endeavors on the healthcare map might’ve been seen as something of a pipe dream.
Not for Ross.
Even back then, the now associate professor of surgery at the University of California San Diego (UC San Diego) saw potential for AI to make an impact on care for patients with peripheral arterial disease (PAD).
Now, she is a little closer to realizing work already a decade in the making thanks to coveted funding secured through the National Institutes of Health (NIH) Research Project Grant Program (R01).
The award, worth more than $3 million over five years, will be used to build a powerful AI model inside the electronic medical record (EMR) to help identify patients
at risk of PAD and predict their outcomes. A randomized controlled trial (RCT), too, is planned to establish whether or not AI can improve practice.
“Ten years ago, I was a resident and I was looking around at the healthcare system. I had a background in health policy, and I realized that the American healthcare system was very broken,” Ross recalls. “But how do we fix that? I initially thought maybe through some policy research, but, ultimately, because I had a background in computer science, I thought giving clinicians information at their fingertips would help them make better decisions—from more of a grassroots perspective we can improve healthcare that way.”
rithms and models that could identify these patients and eventually predict their outcomes and maybe one day help us make treatment decisions for them.
$3m
over 5 years
At the root, Ross explains, is the vascular patient—a neglected figure in the wider sphere of the cardiovascular space. These patients tend to be lower income, have less education and less wealth, she says. “So they have less access to resources, less access to primary care doctors. And we find that patients with PAD are often undiagnosed until they have a severe problem.”
At that point of understanding, Ross set about putting the strands of her education, training and experience together into a cohesive research plan.
“So putting that altogether, how do we improve care, potentially reduce the cost of care and improve access for our patients who are underserved? I wanted to build algo-
“We are going to do a randomized study to see if AI can actually move the needle forward for PAD”
ELSIE GYANG ROSS
MEMBERSHIP BYLAWS REFERENDUM APPROVED BY SVS VOTING MEMBERS
The voting members of the SVS have approved amendments to the Society bylaws following a referendum that closed on Nov. 20. The proposed changes were focused on two areas: adjustments to membership privileges for earlycareer members and adjustments to the composition of the SVS Executive Board.
A total of 453 voting members participated, exceeding by a factor of three the quorum requirement of 150 votes (5% of voting members). A two-thirds majority of those voting is required for ratification of bylaw changes.
On the question of changes regarding early-career membership, the referendum passed with 92.72%. On Executive Board composition, it passed with 81.24%.
“The approval of these amendments reflect the ongoing interest and commitment of our members to advancing the SVS and ensuring that our membership and governance structures align with the evolving needs of our dynamic medical community,” said SVS President Joseph Mills, MD.
The voting, which began on Nov. 6,
asked members to consider and ratify proposed amendments that had been formally approved by the SVS Strategic Board of Directors.
The amendments are aimed at accelerating engagement of early-career vascular surgeons within the SVS and fostering diversity of perspective.
The bylaw changes go into effect immediately regarding early-career membership revisions.
For Executive Board composition, the changes will begin to apply for 2024–2025, which will include potential expansion of the number of candidates in officer elections from the current two, to a maximum of four; and expansion of the appointed members of the board from three to five, and making each position “at-large,” selected on the basis of merit, qualifications and identified gaps in expertise on the Executive Board.
A review of the changes is available at vascular.org/2023BylawsRef. For answers to any questions regarding the referendum, email governance@ vascularsociety.org. Marlén Gomez
“I started off working with small datasets while I was a postdoctoral fellow,” Ross relates. “When I finished my residency and gained a faculty position at a university, I then decided to build models inside our electronic health records so that, again, it would be at our fingertips. It was 10 years in the making, building these things, evaluating them and seeing the best path forward. The funding is a game changer because it is over $3 million over five years to build a powerful AI model that can that can predict PAD in diverse patient populations—so not just at one hospital, but across the country.
“We want to see if these models, when we put them in the clinician’s hands, will actually change care. We are going to do a randomized study to see if AI can actually move the needle forward for PAD.”
Ross, as an early-career surgeon-scientist, has managed to pull off the rare feat of attaining R01 funding from the NIH before the ago of 40. She puts this down, primarily, to perseverance and mentorship.
“I’m very focused,” she says. “I think the focus on starting work on something that began 10 years ago is how you get to this point early on. I have had great mentorship up to this point. My mentors took an approach of kind of just advising me and letting me take the reins of where I wanted to drive the research, which was really helpful. I’ve had a very supportive environment. And it’s just the right time. It’s kind of lucky to have been working on something 10 years ago that now everyone is talking about with ChatGPT and Alexa, and all this other stuff. The timing worked out, along with all the hard work that went into it.”
Nominations open for 2024 SVS Excellence in Community Practice Award LEADERSHIP
By Marlén Gomez
THE SVS IS CALLING FOR nominations for its Excellence in Community Practice Award, which recognizes outstanding leadership within the community by a practicing vascular surgeon who has made sustained contributions to patient care and community well-being.
Patricia Furey, MD, one of last year’s recipients, highlighted the inspiration it provides.
wouldn’t even think of nominating themselves,” she said.
Nominees must have a minimum of 20 years as a practicing vascular surgeon, with at least five years as an SVS member to qualify.
The selection process considers evidence of the nominee’s impact on vascular care and community health, such as leadership in a community-based practice.
The 2024 nomination period is now open, with nominations due by Feb. 1, 2024. Any SVS member can nominate a candidate by submitting a nomination form and supporting documentation. Selfnominations are also accepted. Nominations will be carefully reviewed by the SVS Community Practice Section, which will determine the award recipient.
“This award is extremely important for many of us who are in community practice, so I was very pleased to receive the award and very grateful, and I think it’s inspiring because we have a lot of wonderful community surgeons that
Robert Molnar, MD, a 2022 award recipient, underscored the importance of recognizing community practice surgeons, who constitute nearly 50% of the SVS membership, he said.
To make inquiries or to obtain more information on the award and nominations, visit vascular.org/ CommunityPracticeAward
Elsie Gyang Ross
Patricia Furey is pictured alongside Robert Molnar
YAO FAMILY AND SVS FOUNDATION ESTABLISH JAMES S.T.
YAO RESIDENT RESEARCH AWARD
In a tribute to the late James S.T. Yao, MD, PhD, a luminary in the field of vascular surgery, the Yao family and the SVS Foundation announced the renaming of the Resident Research Award to the James S.T. Yao Resident Research Award.
By Marlén Gomez
THE RENAMING OF THE AWARD serves as a testament to Yao’s unwavering commitment to the advancement of vascular surgery, said Yao’s wife, Louise. The contribution from Louise and their three children—Kathy, a surgeon; John, a musician; and Pauline, a museum curator—ensures that his legacy continues to inspire future generations. Yao resided in Wilmette, Illi -
nois, and had a longtime association with Northwestern University.
“He was a great believer in research and writing papers,” reminisced Louise. “I see other people like him and my daughter, who is also in medicine and has many of those traits.”
The award supports emerging medical professionals exploring vascular disease biology and innovative translational therapies. It recognizes unpublished, original scientific work in manuscript form that demonstrates publication quality. The recipient presents the research in a plenary session at the SVS Vascular Annual Meeting (VAM).
“The Resident Research Award was my first opportunity to present the work of our team to a large audience, including many of my heroes, including Dr. Yao, from papers I had read,” said Luke Brewster, MD, a 2005 recipient of the award.
Louise recalled her husband’s regard for the Foundation and how “he thought so highly of this organization and the things they did to help young people get into the field.”
Yao, known as Jimmy, passed away on Dec. 20, 2022. His career began with his medical education at the National Taiwan University Medical School in Taipei. He continued his journey with a surgical residency at Cook County Hospital in Chicago and earned a doctorate in London, England. From 1988–2007, he served as the Magerstadt Professor of Surgery and chief of vascular surgery at Northwestern University.
His work led to the development of the ankle-brachial index (ABI), a quick and simple test for peripheral arterial disease that is now standard practice. His contributions included formalizing protocols for noninvasive vascular studies and founding the Society for Noninvasive Vascular Technology in 1977.
Throughout his career, Yao wrote 200 textbook chapters and 50 academic books. He established the first blood flow laboratory in Chicago, initiated a vascular fellowship training program and held various leadership positions in vascular surgery organizations, including serving as SVS president in 1993.
“[Dr. Yao] wrote over 300 manuscripts; he probably influenced every aspect of vascular surgery based on their case series,” said Michael C. Dalsing, MD, SVS Foundation chair and one of Yao’s former trainees. “But with all his success, he never forgot who he
was—truthful, dedicated, humble and intellectually fearless.”
Through his leadership in the SVS History Project Work Group, Yao demonstrated his commitment to preserving the history of vascular surgery by conducting interviews with more than 85 prominent figures in the field. In 2007, he received the SVS Lifetime Achievement Award.
The recipient of the resident award renamed in his honor receives a $5,000 award and a one-year subscription to the Journal of Vascular Surgery
“The award deals with research that looks at the basic mechanisms of how vascular disease pathophysiology presents, or an innovative spin on treatment and how it sets the basis of how we look at disease or vascular health. It’s an innovative process, which is always very important if science is going to move forward,” said Dalsing.
For more information on the award, visit vascular.org/YaoRRA. Submissions for 2024 are due Jan. 10, 2024.
“The award deals with research that looks at the basic mechanisms of how vascular disease pathophysiology presents or an innovative spin on treatment and how it sets the basis of how we look at disease or vascular health”
This Multi-modality therapy combines noncontact cyclical Compression with Oxygen and Humidification, is easily added to your care plan, and is self-administered by the patient at home over their dressings, including CCD or UNNA boot, improving compliance and access to care for all.
MICHAEL DALSING
James S.T. Yao
COMMENT& ANALYSIS CORNER STITCH
ON THE VAST ARRAY OF MEETINGS AND CONFERENCES
Christopher Audu, MD, surveys the 2024 meeting landscape, highlighting prime opportunities for trainees to showcase their research.
IT IS ABSTRACT SUBMISSION SEASON, and this month I wanted to highlight a few national meetings that are “trainee friendly” for getting your work presented as a podium talk or poster presentation. This list is not exhaustive but hopefully gets you thinking about applying.
■ Vascular and Endovascular Surgical Society (VESS)
We did a deep exposé on this organization in the December 2020 issue. A premier vascular meeting, the VESS winter conference is always in January and always at a ski resort, making it very popular. There is programming for trainees from the medical student, to the resident and fellow level. In addition, there is always great science presented. A very welcoming society, if you miss the winter conference, watch out for the spring edition—that’s always paired with the SVS Vascular Annual Meeting (VAM).
■ Society for Clinical Vascular Surgery (SCVS)
This is another society that has programming for students, residents and fellows. The meeting is usually in the late winter/
early spring—in March—and is usually somewhere warm. Be on the lookout for the SCVS Top Gun Competition, where you can go head-to-head with your colleagues in friendly battle.
Don’t be fooled by the name, this is a meeting of vascular minds that invites faculty from all over the country to participate. Usually in Seattle, and hosted by the University of Washington, this meeting also has a friendly competition where programs can send a team to compete in a variety of vascular simulations. In addition, it is a great place to present some newer work.
■ Academic Surgical Congress (ASC)
This meeting is not exclusively focused on vascular surgery, but it does accept papers discussing vascular conditions. This is a great conference for students and trainees to get on for podium presentations. The meeting usually is in close temporal proximity to VESS—in February.
■ American Venous Forum (AVF)
Have you done work looking at venous pathology? This is the premier national meeting to present your work either in talk or poster format. The AVF is usually at a resort and often seeks trainee input. While there is no dedicated trainee programming, the organizers actively seek out trainee involvement.
■ Charing Cross (CX) International Symposium
This is an international meeting, set in London, England, and is usually in April. It’s a unique-style symposium that focuses on controversies in vascular surgical management in an effort to develop a consensus. While not entirely exclusive to vascular surgeons, it serves as a great meeting to hear the latest and reconsider what may be dogma based on practice patterns at your institution.
■ Vascular Research Initiatives Conference (VRIC) and Vascular Discovery (AHA)
This is a gathering for anyone conducting basic science vascular research. VRIC is often the day before the American Heart Association (AHA) Vascular Discovery meeting,
“Be on the lookout for the SCVS Top Gun Competition, where you can go head-to-head with your colleagues in friendly battle”
and usually in April or May. It’s a wonderful opportunity to present groundbreaking work in a friendly environment. There is a poster competition and select abstracts will be recognized and awarded. For the budding basic scientist-vascular surgeon, this is a must-attend meeting that will allow you to meet other like-minded surgeon-scientists.
■ Vascular Annual Meeting (VAM)
This is always a big hit, and is the premier vascular surgery meeting in the U.S. With excellent programming aimed at medical students, residents/fellows, and a general audience, this meeting provides ample opportunity to learn, network and gain exposure to current practices in vascular surgery. As a trainee, if there’s only one meeting you can make, this one is probably it.
In addition to those listed above, there are a number of other meetings and conferences that are great for educational and learning purposes, although the talks at these are usually in the form of invited lectures given by attendings rather than through abstract submission. These include, but are not limited to, VIVA (Vascular Interventional Advances), The VEINS (Venous Endovascular Interventional Strategies), VEITHsymposium and the Strandness Symposium.
In the end, these are all opportunities to meet and re-meet expert vascular surgeons as we progress on this journey towards becoming competent vascular surgeons ourselves. I look forward to seeing you on a podium somewhere as you share your awesome work!
CHRISTOPHER AUDU is the Vascular Specialist resident/fellow editor.
How SVS members can contribute to actively support advocacy efforts GOVERNMENT GRAND ROUNDS
By Andrew Kenney
WHILE ADVOCACY CONSISTENTLY MAINTAINS a top spot among the list of priorities for SVS members, there remains a degree of uncertainty among many in the vascular surgery community regarding how to actively support SVS advocacy-related programs, the spectrum of available activities, and methods for measuring success throughout the process.
In response to this need, the SVS advocacy team introduced a new column dedicated to shedding light on the actions of Congress and regulatory agencies and their direct implications on vascular surgery. The Government Grand Rounds series was designed to address these uncertainties, aiming to propel the SVS towards its objective of fostering a robust culture of engagement across the entirety of our SVS membership.
Through the series, the emphasis was placed on highlighting the significance of the various tools we can utilize across our advocacy efforts. Looking back at that advocacy toolkit, we see the importance of advocacy from a multitude of perspectives.
Protect: Advocacy in vascular surgery aims to protect patient access to necessary procedures.
Engage: Engaging with the full range of healthcare policymakers and professionals is pivotal in advocating for vascular surgery.
Educate: Vascular surgery advocacy focuses on educating decision makers about the importance of the vascular surgical specialty.
Serve: Advocacy in vascular surgery is about serving the community by ensuring access to quality care and resources for vascular health.
Advance: Advocacy initiatives in vascular surgery strive to advance and enhance patient outcomes and overall vascular care.
Reform: Advocates in vascular surgery work to reform healthcare policies to ensure equitable access to vascular treatments and procedures.
Promote: Vascular surgery advocacy seeks to promote awareness of the vascular specialty.
Amplify: Advocacy in vascular surgery amplifies the voices
of medical professionals and patients, advocating for better resources and understanding.
Build: Vascular surgery advocacy aims to build collaborative networks among medical practitioners to improve standards and innovation in the field.
Change: Advocacy efforts in vascular surgery are committed to driving systemic changes that improve patient care, treatment options and overall vascular health outcomes.
Government Grand Rounds will continue into next year, to serve as a vehicle to drive the SVS towards its primary goal: cultivating that vibrant culture of engagement throughout its extensive membership. This strategic initiative aimed to not only resolve doubts but to galvanize participation, uniting members under a common cause of advancing vascular surgery.
For more information about how the SVS advocacy programs help protect vascular surgeons and the patients you serve, visit vascular.org/advocacy
ANDREW KENNEY is a member of the SVS advocacy staff.
Those who live in glass houses… CAS REBUTTAL
Christopher J. White, MD, responds to a recent editorial by Malachi Sheahan III, MD, that took a critical look at the decision by the Centers for Medicare & Medicaid Services (CMS) to expand coverage for carotid artery stenting (CAS).
I’m grateful for the opportunity extended by Dr. Sheahan to respond to his very entertaining, and acerbic commentary in “Sex, lies, and carotid stents.” While I don’t agree with much of the opinion expressed, I enjoyed reading his well-done piece. Allow me to offer some constructive criticism, correct some misstatements and clarify my rationale for supporting the recent CMS decision to reimburse for CAS on par with carotid endarterectomy (CEA).
First, in our spirited debates over optimal approaches to managing carotid artery disease, we must assume our surgical colleagues have good intentions and sincerely want to offer their patients the best opportunity for good clinical outcomes. Alas, some vascular surgeons appear to be influenced by an ulterior, self-serving motive designed to protect their “turf.” Thus, the goal of achieving the best patient outcome, the “raison d’etre” of our profession, becomes collateral damage.
In many areas of medicine, there are clinical conditions treated by multiple specialties from different training pathways and backgrounds. It is generally accepted that multispecialty teams are the best solution to turf battles, offering better perspective and more balanced patient guidance than that of individual specialties who are siloed in their views. Carotid artery disease is but one example of a condition managed by clinicians from multiple disciplines: the neurosciences (neurology and neurosurgery); radiology; surgery (general and vascular); and cardiology. The Multispecialty Carotid Alliance (MSCA), so vilified by Dr. Sheahan, is made up of a diverse group of physicians with representation from
CODING
WHY SHOULD SVS MEMBERS RESPOND WHEN THEY RECEIVE AN INVITATION TO COMPLETE AN RUC SURVEY?
By Wayne Causey, MD
The SVS is an active participant in the American Medical Association (AMA)/ Specialty Society Relative Value Scale Update Committee (RUC) process. A very important component of the RUC process is the RUC survey.
each of these specialty groups (many of whom have held leadership positions within their various specialty societies), and along with many others supported the decision by CMS to reimburse for carotid stenting. The rationale for the MSCA’s support for carotid stenting reimbursement is detailed in a letter to CMS.1 The simple contrast of a multispecialty group (which, by the way, included vascular surgeons) supporting carotid stent reimbursement versus the single specialty of vascular surgery (represented by the SVS) in opposition is revealing. Which group would have the patient’s best interest in mind versus protecting their specialty’s turf?
The most blatant misstatement made by Dr. Sheahan was asserting a lack of training and preparation of interventional cardiologists to manage patients with carotid artery disease. In February 2023, the most recent advanced training statement on interventional cardiology was published with multiple mentions of “carotid” and “cerebrovascular” management in a very detailed and robust training document.2 This begs the question: why single out cardiologists when specialists from the neurosciences and radiology are also very much engaged in managing patients with carotid artery disease? Are their respective training programs up to par? Isn’t the best solution a multidisciplinary approach, not one dictated by a single specialty represented by the SVS?
Dr. Sheahan’s failure to discuss transcarotid artery revascularization (TCAR)—included in the CMS coverage decision for stenting—is telling. TCAR was developed and championed by vascular surgeons and is rarely if ever performed by cardiologists. Yet, Dr. Sheahan’s concern for high-quality care failed to mention the glaring gaps in evidence regarding the efficacy of TCAR versus alternative procedures. With the earliest publications of this technique dating back to 2004,
“The most blatant misstatement made by Dr. Sheahan was asserting a lack of training and preparation of interventional cardiologists to manage patients with carotid artery disease”
The rules related to conducting an RUC survey are governed by the RUC. The specialty societies conduct the surveys, analyze the data and use those data to advocate for fair physician work relative value units (RVUs).
RUC surveys are conducted when new CPT (Current Procedural Terminology) codes are approved by the AMA’s CPT Editorial Panel or when the Centers for Medicare & Medicaid Services (CMS) and/ or the AMA RUC identify a service as potentially misvalued.
RUC surveys are completed online and must be completed independently without coaching or assistance, with the exception of clarification from specialty society staff.
An RUC survey of physician work solicits information about: physician time
there are now 20 years of experience with this procedure. Yet, as of today, no prospective randomized trials have been performed. In stark contrast, carotid stenting is one of the most studied clinical procedures of all time, with dozens of randomized trials supporting its use. Yet, vascular surgeons happily offer their patients TCAR without any comparative evidence of benefit. For shame! It appears that the occupants of vascular surgery’s “glass house” have started a rock-throwing fight. Finally, my rationale for supporting CMS reimbursement for carotid stenting is to allow a flexible, informed and individualized approach. Of those patients with carotid artery disease likely to benefit from revascularization, some will be better served with surgery, some better treated with carotid stenting, and many who are candidates for either procedure and should be offered an informed choice.
Remember, the National Institutes of Health (NIH) has determined that there is equipoise for carotid surgery and carotid stenting. In sponsoring CREST-2, a randomized clinical trial, they adopted a parallel-arm approach comparing carotid surgery with medical therapy to medical therapy alone, and carotid stenting plus medical therapy to medical therapy alone. Patients are enrolled in this trial by investigators who discuss treatment options with the patient. The patient, with physician counsel, is allowed to choose either the surgery arm or the stent arm. Sounds like a great example of patient-centered care. I rest my case.
Thank you, Dr. Sheahan, for the opportunity to participate in this discussion.
2. Bass TA, Abbott JD, Mahmud E, et.al. 2023 ACC/AHA/ SCAI advanced training statement on interventional cardiology (coronary, peripheral vascular, and structural heart interventions): A report of the ACC Competency Management Committee. J Am Coll Cardiol. 2023;81: 1386–1438.
CHRITSTOPHER J. WHITE is the medical director of the Centers of Excellence and Service Lines at Ochsner Health in New Orleans, Louisiana.
required to perform the service; mental effort and judgment; technical skill and physical effort; and psychological stress.
Respondents are asked to indicate whether the typical patient described in their survey is their typical patient for that procedure. However, regardless of whether the patient described is the respondent’s typical patient, the respondent should complete the survey based on the described typical patient. Demographic information about the person completing the survey is collected to assist with data analysis. The survey includes a reference service list of codes for currently performed procedures and their corresponding RVUs. Respondents will estimate how much time it takes to perform the surveyed procedure and the
number and level of postoperative visits. Respondents will be asked to compare the mental effort and judgment, technical skill or physical effort, and psychological stress of the surveyed code to the reference procedure.
In the final step, respondents are asked to estimate a relative physician work RVU for the surveyed procedure based on responses to all the previous questions. Members, your voice needs to be heard. Next time you receive an invitation in your email to complete an RUC survey, please take the time to complete it. Contact SVSAdvocacy@vascularsociety.org with questions.
WAYNE CAUSEY is a member of the SVS Coding Committee.
Christopher J. White
Specialty representation at all levels of a healthcare organization is ‘increasingly important’ in value-based systems
By Bryan Kay
A 14-YEAR EFFORT TO ACHIEVE DEPARTMENTAL status for vascular surgery at a large healthcare system in Southern California resulted in significant gains for the specialty within the organizational apparatus, according to an administrative case report on an effort finalized last year.
Jeffrey Hsu, MD, the regional chief of vascular surgery at Kaiser Permanente Southern California, charted the course of departmentalization at his institution amid resistance from general surgery and organization-level bylaw changes necessary to define a transition process during a 2023 VEITHsymposium (Nov. 14–18) session in New York City. The process originated after a general consensus was reached among the healthcare system’s vascular surgeons in 2008 that they needed their own department due to issues around inadequate representation for the specialty, lack of administrative control over vascular surgery resources, and “a
general sense of recognition and identity for the specialty,” Hsu told attendees.
After changes to the Kaiser Permanente bylaws were defined and approved, it became apparent vascular surgery met all the criteria required to become a department.
“In 2016, vascular surgery was granted divisional status by the executive leadership,” explained Hsu. “However, operationally this had little effect, and the majority of vascular surgery chiefs wanted to continue to pursue department status. In 2017, vascular surgeons in our organization collectively decided to transition from a division to a department. Through a lengthy process of negotiations and discussions, we were finally able to achieve unanimity. In 2021, we were able to gain the support of the general surgery department to proceed.”
clerkships and appointed vascular surgery preceptors.” Surgical residents are given increased exposure and longer rotations in vascular surgery, and vascular surgery chiefs are now invited to all surgical leadership meetings, both regionally and locally, Hsu added.
“This report demonstrates that departmentalization of vascular surgery is possible in a large healthcare organization,” he concluded.
“So I ask our colleagues who take leadership positions in your organizations who are faced with mounting administrative challenges—it is my hope that you will consider departmentalization as a viable option.”
Finally, in 2022, the Kaiser Permanente board of directors “unanimously voted to form the department of vascular surgery,” added Hsu.
The stakes couldn’t be higher, he observed.
“It stands to reason that specialty representation at all levels of healthcare organizations will become increasingly important as we move toward value-based systems, increased administration and more corporate control of healthcare,” Hsu said. “Vascular surgery’s place in the organizational structure is an important factor to consider.”
He listed the benefits witnessed in the year since the department was formed. Surgical service line operations now include vascular surgery decision-making, Hsu said. Collegiality with general surgery “remains strong and unharmed,” and “the medical school has established vascular surgery
“It
stands to reason that specialty representation at all levels of healthcare organizations will become increasingly important as we move toward valuebased systems, increased administration and more corporate control of healthcare”
JEFFREY HSU
Jeffrey Hsu addresses VEITH 2023
INTRAVENOUS ANESTHESIA DELIVERY DURING VARICOSE VEIN
TREATMENT PROVES SAFE AND REDUCES PAIN SCORES, RESEARCHER REPORTS
By Bryan Kay
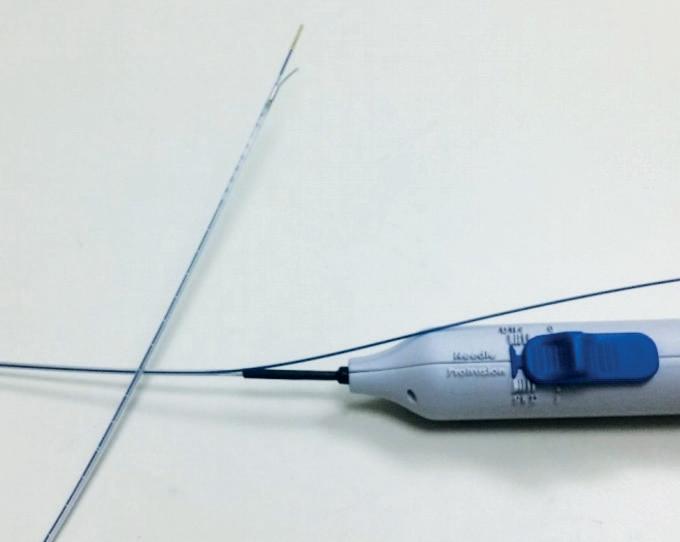
Anew intravenous anesthesia delivery technique used during endothermal ablation for varicose veins demonstrated comparatively low pain scores according to first-in-human (FIH) data recently presented at the 2023 VEITHsymposium.
The investigational Solutio catheter, which contains both a bent needle for tumescence deployment through the vessel wall into the perivascular space and endothermic fiber for ablation treatment, produced a median score of 5 (0–24) on the visual analogue scale (VAS) in nine consecutive patients in Sweden, Michael
Åkesson, MD, an interventional radiologist and developer of the device, told the New York City gathering (Nov. 14–18).
He hailed the catheter as a safe and feasible solution resulting in a single puncture as opposed to several.
Traditionally, Åkesson observed, patients find the anesthesia part of the ablation treatment process unpleasant, with VAS pain scores often varying from 20–60.
Results from the FIH study showed two “mild” device deficiencies and no serious adverse events. Patients—eight women and one man—underwent treatment
The Solutio catheter
PCPs
Overcoming barriers to a successful wound care program
PROPER INTEGRATION OF PRIMARY care physicians (PCPs) in the multidisciplinary care of vascular wounds is going to play an increasingly important role as the popularity of the team approach spreads.
by a single vascular surgeon. They were recorded as having a great saphenous vein median length of 41cm. “The subject with the 24 VAS score reported that the pain came from the puncture site area in the lower leg,” Åkesson told VEITH 2023.
“The surgeon suspected this was caused by a dissection while accessing the vein. He generally considered the catheter to be safe and easy to use, but with a short learning curve. Two minor device-related defects were reported—low flow rate in the long needle and catheter with high friction while pushing the needle out of the catheter. Both problems will be resolved with the prototype.”
During the four-week follow-up period following treatment, no serious adverse events emerged and no signs of bleeding were reported, Åkesson added.
“I think the key is making sure we get to the patients early,” said Vincent Rowe, MD, chief of vascular surgery at the University of California Los Angeles (UCLA) in Los Angeles, in an interview with Vascular Specialist during VIVA 2023 (Oct. 30–Nov. 2), in Las Vegas.
“We need to provide education so patients can understand how they can prevent these wounds, but we also need to educate the PCPs,” he said.
“Do we keep these patients in our care for a while, or do we send them back and hope that nothing else happens again? Those are going to be some of the keys in how we manage these patients.”
Rowe had just given a talk on patient-specific decisions and how to determine appropriate timing, resources and management of wounds.—Jocelyn Hudson
PACLITAXEL
NEED FOR ‘CLEAR, WELL-DEFINED GUIDELINES’ IN PATIENT SELECTION FOR SURGICAL IMPLANTATION OF BAROREFLEX ACTIVATION THERAPY DEVICES IDENTIFIED VASCULAR ASSIST TRANSCEND
THE EMERGENCE OF A BAROREFLEX activation therapy device for heart failure patients is drawing in the assistance of the open surgical expertise of vascular surgeons in the arena of the carotid bulb— and drawing attention to a need for “clear and well-defined guidelines.”
Discussion was stirred after the delivery of a case experience from the University of Miami, Florida, during the Eastern Vascular Society annual meeting (Sept. 7–9) in Washington, D.C., in which presenter Christopher Chow, MD, a vascular surgery resident at the institution, raised the possibility of a randomized controlled trial comparing the Barostim device (CVRx) to a sham therapy.
Chow described the University of Miami experience working with his institution’s heart failure-cardiology team who identify patients who would benefit.
He reported successful intraoperative therapy among all patients treated, many of whom returned home the same day. “Patients by and large tolerate the procedure without significant complications,” he said. “Discomfort associated with device activity is actually a common complaint, known as extraneous stimulations. It’s been described as stimulations of the nerves around the
carotid bulb.” They can take the form of headaches and a painful buzzing sensation in the chest, Chow added.
The baroreflex activation therapy device is an implantable pulse generator designed to deliver continuous electrical stimulation to carotid baroreceptors through a lead sewn into the adventitia of the carotid bulb, with a subsequent increase in parasympathetic outflow and a reduction in symptoms of heart failure, Chow said.
“There have been some early studies that it may be beneficial,” Chow said. “The implantation of the device is very neatly suited for the skillset of vascular surgeons. It requires a small carotid cutdown at the carotid bulb through ultrasound identification and then sewing of the lead onto the adventitia of the bulb.”
But Chow emphasized a need for clearer guidelines.
“Further research is definitely needed, such a randomized controlled trial—we would suggest a sham device therapy,” he said. “Vascular surgeons are very keen on generating this data. We should continue working with heart and cardiovascular teams to find the best practice guidelines for Barostim therapy.”
Under audience questioning, Chow
underscored the point: “In general, I would say there is really no clear and well-defined guidelines about who would actually benefit from this therapy, and that is actually one of the aims of this discussion—to try to foster that conversation,” he said.
The baroreflex activation technology is relatively new but is gaining traction, Chow observed, with work already starting on a percutaneous approach. “You can imagine what that may imply for future carotid interventions,” he added.—Bryan Kay
Baroreflex activation therapy
“Patients by and large tolerate the [baroreflex] procedure without significant complications
CHRISTOPHER CHOW
36-month data ‘continue to demonstrate safe and effective performance’
PETER SCHNEIDER, MD, PROFESSOR of vascular and endovascular surgery at the University of California San Francisco (UCSF) in San Francisco, recently presented 36-month data from the TRANSCEND clinical trial at the 2023 VEITHsymposium (Nov. 14–18) in New York City.
The TRANSCEND trial is a prospective, multicenter, single-blind randomized controlled trial to assess the safety and efficacy of the SurVeil (Surmodics).drugcoated balloon (DCB) versus the IN.PACT Admiral DCB (Medtronic) for treatment of superficial femoral and proximal popliteal artery lesions.
A total of 446 patients were randomized to either the low-dose paclitaxel (2.0µg/ mm2) SurVeil DCB (n=222) or the highdose (3.5µg/mm2) paclitaxel IN.PACT Admiral DCB (n=224) at 65 sites in the U.S., Australia, Austria, Belgium, Czech Republic, Germany, Italy, Latvia and New Zealand.
The SurVeil DCB continues to show similar outcomes at 36 months—showing statistically comparability vs. the IN.PACT Admiral DCB, VEITH 2023 attendees heard.—Jocelyn Hudson
SMOKING
SVS members pitch in to help patients kick the habit
By Beth Bales
SVS MEMBERS ARE TAKING ADVANTAGE OF THE new Smoking Cessation Toolkit and resources from Vascular Quality Initiative (VQI), adding them to existing programs and giving new life to their quest to get their patients to kick the nicotine habit and improve their health.
The SVS Patient Safety Organization (PSO) launched the national smoking cessation initiative, CAN-DO (Choosing Against Combustible Nicotine Despite Obstacles) in June during the VQI Annual Meeting held in conjunction with SVS’ Vascular Annual Meeting.
CAN-DO includes several components to increase smoking rates: physician and patient toolkits; including smoking cessation variables in the SVS PSO VQI’s arterial registries; and updating information on smoking cessation on the SVS website.
Toolkit elements that physicians and surgeons may find useful include:
◆ A quick guide to treatment options
◆ Information on counseling via text messaging
◆ Use of smartphone apps and web-based services
◆ Resource documents
◆ Information on quit lines
◆ Patient-facing information doctors can distribute
◆ Billable smoking cessation codes
The patient toolkit, meanwhile, includes links to many resources on quitting smoking.
“As vascular surgeons, we are tasked with helping our patients navigate through some of their most challenging and life-changing moments in their lives,” said Gary Lemmon, MD, associate medical director for the SVS PSO. “It is up to us to advise them as to their best chance of success and quality-of-life improvement. Smoking cessation assistance is integral to that success.”
Cassius Iyad Ochoa Chaar, MD, an associate professor of surgery at Yale University in New Haven, Connecticut; Yale postdoctoral research fellow Dana Alameddine, MD; and Peter Henke, MD, the section chair of vascular surgery at University of Michigan Health in Ann Arbor, Michigan, all are taking advantage of the toolkit to help strengthen their existing “quit smoking” messaging.
“This extensive toolkit is very, very helpful and user-friendly,” said Chaar. “We can incorporate the various phrases and strategies included and get all our providers to engage with them. If someone doesn’t want to prescribe medications, he or she can incorporate other elements VQI wants to encourage, such as counseling and nicotine replacement therapy.”
Their experiences with predecessor programs and, after reviewing the resources included in the new VQI initiative, led them to stress how an upcoming major inpatient surgery and its recovery provide a great opportunity to deliver the “quit smoking” message. Patients by and large will have to quit smoking while in the hospital, plus multidisciplinary teams are available who can reinforce the message from different angles. They also emphasized the importance of “systemizing” the effort by making sure it is part of the hospital system. “If you have to opt out, rather than opt in, that’s helpful,” said Henke. “Statewide, in Michigan, it became part of the discharge summary.”
The surgeons also noted how smoking cessation requires the emphasis the toolkit and initiative have created. The group also stressed that the tools in the toolkit are easily adoptable to different practices and physicians. Surgery and recovery provide an optimal time to deliver the “quit smoking” message, said Chaar.
“We can basically reinforce the message on a daily basis – and we do that,” he continued. The patients also become “plugged into” the hospital smoking cessation program. Prior research shows that a lack of connection can impede patient follow-up, but inpatients receive both that link and that follow-up. “We’re able to sometimes provide them with medications, and we’ve given them nicotine patches in the hospital, so when they leave, we give them their best shot at stopping.”
Said Henke: “Surgery, particularly an aneurysm or bypass or similar major operation, is a major life event. They’ve had to quit smoking while they’re in the hospital—for weeks of hospitalization—so if they’ve stopped and then they’re smoking sporadically, perhaps you can transition them to a nicotine patch and varenicline. They have a higher quit rate as well, as compared to a patient who may have a one-day procedure.”
Chaar said the anti-smoking effort stretches across all medical teams that deal with smokers. “At every hospital we deliver the same message about smoking but from different angles,” he said. For example, cardiologists can point to cardiac disease, neurologists about strokes, and vascular surgeons about the many diseases smoking worsens. Oncologists can speak to the different cancers that can result.”
Yale physicians and providers are incorporating suggested thought phrases and incorporating the elements VQI wants to capture regarding counseling and treatment for patients into electronic health records, Chaar said.
“They’ve had to quit smoking while they’re in the hospital—for weeks of hospitalization—so if they’ve stopped and then they’re smoking sporadically, perhaps you can transition them to a nicotine patch and varenicline”
PETER HENKE
“So, we’re able to be early adopters and we can track this in our own institution and our health system, and also contribute to the nationwide initiative as well,” he said.
Yale has been very active in the smoking cessation movement, said Chaar. “It’s terrible for people with vascular disease and we’ve been trying to look at novel ways to help them quit.”
Michigan has been active too. “We were early adopters of this,” said Henke, who practices in that state. Michigan’s statewide quality collaborative created a cessation intervention initiative several years ago, in the wake of the VAPOR clinical trial results that covered the feasibility and pilot efficacy of a brief smoking cessation intervention delivered by vascular surgeons. The trial concluded that “implementation of a brief, surgeon-delivered smoking cessation intervention is feasible for patients with peripheral arterial disease. A larger trial will be necessary to determine whether this is effective for smoking cessation.”
YES, SMOKERS DO QUIT!
Do patients actually quit smoking after receiving help? The data—and SVS members—say “yes.”
Several years prior to the Vascular Quality Initiative’s national smoking cessation project, Yale University’s Division of Vascular Surgery and Endovascular Therapy received a Quality Improvement Project grant from the Vascular Study Group of New England.
“We got disrupted by COVID like everything else,” said Cassius Iyad Ochoa Chaar, MD. However, they were able to enroll 48 inpatients in an intensive direct smoking cessation program, with follow-up at three months and one year.
Patients had smoked an average 40 years. Multidisciplinary teams gave presentations specific to their specialties, and patients then received four weeks of nicotine replacement therapy.
Physicians followed up with the patients at the two time points, when the patients were enrolled in an outpatient smoking cessation program. Forty-four percent had stopped smoking at three months, while 51% had stopped at one year. Sixty-one percent had reduced the number of cigarettes smoked, said Dana Alameddine, MD.
Both Yale and the state of Michigan have long had smoking cessation programs.
All three doctors emphasized that a major surgical episode is a great time to provide information and tools. It’s important to attempt to tie the anti-smoking effort to a patient’s particular procedures, said Alameddine. “It would be a teachable moment for patients to motivate them to quit, or at least reduce the rates of smoking,” she said. Previous studies have shown that major procedures are more associated with a higher rate of smoking cessation than minor outpatient procedures, she added.
Some patients are skeptical or unaware of smoking’s effects, said Chaar. “It’s important to convey the message and confirm the unequivocal link between smoking and health outcomes, including the lowered life expectancy,” he said. It’s equally important to stress that the minute someone stops smoking, life expectancy goes up, Chaar added.
Conveying information without judgment is crucial as well, he stressed.—Beth Bales
The state added a fairly robust set of resources following the VAPOR trial. The new VQI toolkit, Henke said, adds impetus and heft to the state’s efforts. The initiative included nicotine replacement therapy, a referral to the telephone quit-line, and physician-delivered advice along the lines of “Smoking is harmful, it’s important to quit and how can we help you accomplish that?”
The quit-line has proved fairly successful, he said, noting that referrals to such help lines are part of the VQI toolkit.
Smoking cessation needs such emphasis engendered by the toolkit and initiative, Henke said, adding he hopes VQI and SVS leadership make this a top priority.
“Vascular surgeons almost more so than those in another field, see the ramifications and results of smoking,” he said. “We see amputations, death, aneurysm growth—all so smoking-related. We’re really at the front lines of this public health program.”
“The tools in the toolkit are easily adoptable,” he said. “And this is a super important message. It’s not as headline-striking as a new device, but it decreases amputation and death, heart attacks and strokes. It’s a no-brainer in one sense. But it’s hard to keep it in the forefront, when other topics grab headlines.”
The toolkit, pointed out Chaar, includes not only phrases and strategies physicians can use to help their patients stop smoking, but also information on the billing component of delivering such advice and resources. “That’s important for physicians’ and surgeons’ practices,” he said.
More information is available at www.vqi.org/qualityimprovement/quality-improvement-tools
DIVERSITY
VAM TRAVEL SCHOLARSHIPS OPEN DOORS FOR UNDERREPRESENTED MEDICAL STUDENTS
By Marlén Gomez
THE SVS RESIDENT AND STUDENT Outreach Committee (RSOC) is accepting applications through Jan. 8, 2024, for the Diversity Medical Student Travel Scholarship. The award aims to provide aspiring vascular surgeons from underrepresented racial and ethnic minorities with the opportunity to attend the 2024 Vascular Annual Meeting (VAM) in Chicago.
Scholarship recipients will receive financial assistance for travel expenses and complimentary registration for VAM. In addition to scientific sessions, VAM will offer medical student sessions, a mock interview session, a Residency Fair, SVS Connect@VAM and the VAM Mentoring Program.
Carlo Angello Sánchez Montaño, MD, a previous scholarship recipient, shared his experience as the only Mexican resident from his program to receive the award for VAM 2023. He emphasized the significance of the opportunity, expressing his gratitude for the chance to connect with professionals and participate in the Vascular Health Step Challenge at VAM.
Applicants currently enrolled as medical or pre-med students must have an active SVS account before submitting their applications. Although not eligible for the monetary travel award, local applicants are encouraged to apply for complimentary registration by selecting “local student/resident” on the application form.
“My advice to future applicants is never to surrender, do your best, be a good person and pursue what you’re passionate about. If you don’t get selected the first time, don’t lose faith,” said Sánchez Montaño.
Learn more at vascular.org/DiversityVAMTravel
VAM 2024 also includes the General Surgery Resident/Medical Student VAM Travel Scholarship for aspiring vascular surgeons. This scholarship includes a financial award for travel expenses and complimentary VAM registration for medical and pre-med students, as well as general surgery residents. Local applicants can apply for complimentary registration. Learn more at vascular.org/VAMtravelscholarship
Meanwhile, several SVS and SVS Foundation Awards and Scholarships are now available for 2024.
SVS awards
James S.T. Yao Resident Research Award: Apply by Jan. 10, 2024: This award motivates early-career physicians to pursue research in vascular disease and translational therapies. The recipient receives $5,000, a one-year complimentary subscription to the Journal of Vascular Surgery and the opportunity to present his or her research at VAM (vascular.org/YaoRRA).
SOOVC Presentation Award and SOOVC Research Seed Grant: Apply by Jan. 15, 2024 for two SVS Section on Outpatient and Office Vascular Care (SOOVC) opportunities to engage in clinical research within office-based labs (OBLs) or ambulatory surgery centers (ASCs).
The SOOVC Presentation Award ( vascular.org/SOOVCPresentationAward ) recognizes three outstanding projects, offering recipients the chance to present their research and receive recognition. Additionally, the SOOVC Research Seed Grant (vascular.org/SOOVCResearchGrant) provides three grants of $10,000 each, renewable for a second year, to support data analysis for actionable insights, quality improvement and patient care.
Excellence in Community Practice Award: Apply by Feb. 1, 2024 for this award (vascular.org/CommunityPracticeAward), which honors a practicing vascular surgeon
who has demonstrated exceptional leadership within their community.
Lifetime Achievement Award and Medal for Innovation in Vascular Surgery: Nominate by March 1, 2024 for these honors. The Lifetime Achievement Award (vascular.org/LifetimeAward) is the highest accolade bestowed by the SVS. It recognizes an individual’s outstanding and sustained contributions to the profession and the Society, and exemplary professional practice and leadership.
The Medal for Innovation in Vascular Surgery honors individuals whose transformative contributions have had a profound impact on the practice or science of vascular surgery.
SVS Foundation awards
Apply by March 1, 2024 for the SVS Foundation Clinical Research Seed Grant ( vascular.org/clinicalresearchgrant ) to encourage clinical investigation in vascular disease. There is a Feb. 1, 2024, deadline for the Student Research Fellowship (vascular.org/studentfellowship), which supports laboratory and clinical vascular research by undergraduate and medical school students.
Trainees should apply by Jan. 10, 2024, for the Vascular Research Initiatives Conference (VRIC) Trainee Award can receive this award (vascular.org/VRICtraineeaward). VRIC fosters collaboration and encourages interest in research among aspiring academic vascular surgeons.
Clinical topics and special sessions set to take center stage at annual meeting
With the 2024 Vascular Annual Meeting (VAM) just six months away, the gathering’s 25-session education program is taking shape. By
Beth Bales
SOME 21 SESSIONS WILL BE AUGMENTED WITH AN additional four developed by SVS special membership sections—Community Practice, the Subsection on Outpatient and Office Vascular Care (SOOVC), Women’s and Young Surgeons—for a total of 25 spread across all four days of VAM. The educational program sessions take place as breakfast or lunch sessions and afternoon concurrent sessions.
VAM will be June 19–22, 2024, at McCormick Place in Chicago.
Fifteen of the 21 sessions are focused on clinical topics and six will cover such issues as leadership, resident training, practice management, and finance and business, said William Robinson, MD, Chair of the SVS Postgraduate Education Committee (PGEC), which manages and oversees the Educational Program.
The PGEC selected the 21 topics out of a record 90 proposals submitted not only from SVS members at large, but also sister vascular organizations and societies, a variety of SVS councils and committees, and even the Food and Drug Administration (FDA), he said.
JVS-VL TO BE OPENACCESS BEGINNING IN JANUARY PEER REVIEW
The Journal of Vascular Surgery: Venous and Lymphatic Disorders (JVS-VL) will move from a subscription model to one of open access— freely available online—on Jan. 1, 2024. JVS-VL is the journal for both the SVS and the American Venous Forum (AVF) and is celebrating its 10th year of publication. By Beth Bales
“Balance and addressing current needs are key to the program. We aim to cover all major components of vascular surgery practice, while at the same time making sure we address topic areas with current controversy and important innovation,” Robinson said of the blinded selection process. Crucial areas include dialysis access, venous treatment innovations, open and endovascular options for arterial reconstruction, thoracic outlet syndrome, visceral artery aneurysms and challenging surgical scenarios, amongst a host of topics, he added.
Some sessions will highlight important new developments, including one focused on carotid disease management within the context of the Centers for Medicare & Medicaid Services’ (CMS) decision in October to expand coverage for carotid artery stenting. Yet another session will highlight the changes to resident training and surgeon certification brought on by the adoption of Entrustable Professional Activities (EPAs).
Robinson said that the PGEC is encouraging and supporting where possible, and based on attendee feedback, audience interaction and case-based presentations in the sessions, which are either 60 or 90 minutes long.
Robinson also said PGEC remains focused on taking ad-
“I believe we have the makings of a very high-impact educational program for our members and all vascular specialists interested in the cutting edge of vascular disease management and important practice and education issues”
WILLIAM ROBINSON
vantage of the depth and breadth of talent, plus the diversity of perspectives, within the SVS. In developing the overall education program, the PGEC limits the number of instances an individual member can take on a speaker or moderator role to two, thereby tapping as many members as possible for participation in the program.
As is typical, the SVS is partnering with other organizations for some sessions, including the American Venous Forum (AVF) for the session on the latest innovations in venous disease, the American Pediatric Surgical Association (APSA) for a session on pediatric vascular issues, and the European Society for Vascular Surgery (ESVS) for a presentation on the differences between SVS and ESVS guidelines. The FDA is a partner for 2024 for a session entitled “Regulatory Overview of Vascular Devices: From an Idea to Clinical Implementation.”
More details on all of these sessions will be provided in the months and weeks leading up to VAM, said Robinson. “Overall, I believe we have the makings of very high-impact educational program for our members and all vascular specialists interested in the cutting edge of vascular disease management and important practice and education issues.”
Learn more about VAM 2024 at vascular.org/VAM.
JVS-VL had already changed to electroniconly as of January 2023, as only 3.3% of AVF and SVS subscribers had a print subscription.
“I think this reflects changing habits and demographic changes,” Bush said of the move. “It’s about people’s choices and how they interact with the literature. And it’s environmentally friendly.”
“Open access removes restrictions and the science is available to everyone, not just those behind a privileged paywall,” she said. “Anyone with internet service can access the science.”
critically, improve manuscripts and then make them available to the public.”
Authors will see both advantages and disadvantages, said Bush. Articles will be disseminated much more rapidly to the public and the science community. “As soon as an article is reviewed and accepted, after copyediting, it’s available to anyone around the globe,” Bush said. “We are accelerating the pace at which knowledge is available and, hopefully, positively influence citation behavior.”
T he change is part of the larger overall adjustment to eliminating paywalls in scientific journals and making research accessible to all, said JVS-VL Editor-in-Chief Ruth L. Bush, MD, JD. Publishers make such decisions in part based on the number of print subscriptions versus electronic ones, as well as submission volume and impact factor.
Bush and other editors have been accepting articles that will be part of the new open-access system since midAugust. The final non-open-access articles were published in November’s JVS-VL
Under the new model
Readers will have immediate access to cutting-edge research from around the country and the world. Reviewers will see no change, continuing to “read articles
However, under open access, authors pay an article processing charge, which, Bush acknowledged, may anger or concern some prospective contributors and could be a major barrier.
“However, we have in place various ways to help with the processing fee,” Bush said. “Reach out and ask.” Readers are asked to email cgreen@vascular. society.org for more information.
In addition, many academic institutions have so-called “transformative agreements” with Elsevier, publisher of
the JVS publications, to cover the charge. Her own institution in Texas covers a portion of the charges, as do many others, Bush said.
SVS members receive a 20% discount on the fee, and both the SVS and the AVF will subsidize the processing charge for authors of manuscripts accepted for the 2024 AVF annual meeting’s plenary sessions. Bush also pointed out that a fee split between five or six co-authors, even if it’s a total fee of $1,600, reduces the per-person fee to a more manageable level.
Open access also means the ability to reach out to people from other countries to be able to publish their work. “We’ll be more global,” said Bush.
JVS-VL is already truly a global journal, and a top-tier one for publications dedicated to venous and lymphatic disorders, she said. In 2022, 25% of articles came from China, and 35% from the U.S, with the balance from around the world.
“Whether the move is positive or negative, it’s where we are,” said Bush. “I am someone who fully believes, if we want our science to be appreciated, then everyone should have access to it.”
Learn more about open access, fees and more at www.jvsvenous.org
William Robinson
SOCIETY BRIEFS
Compiled by Marlén Gomez
VRIC, VAM abstract submissions open for 2024
ABSTRACT SUBMISSIONS ARE NOW open for two of the major SVS scientific meetings on the 2024 calendar of events: the Vascular Research Initiatives Conference (VRIC) and the Vascular Annual Meeting (VAM).
VRIC will be held in Chicago on May 15, 2024, in conjunction with the American Heart Association’s Vascular Discovery meeting, “From Genes to Medicine,” Scientific Sessions, from May 15–18, 2024. Visit vascular.org/VRIC24
VAM abstracts may be submitted from Nov. 15–Jan. 10, 2024. The meeting is open to individuals at all career levels, offering a diverse array of content areas.
For more information and to submit, visit vascular.org/VAM24Abstracts
SVS EXECUTIVE DIRECTOR ELECTED TO EXECUTIVE COUNCIL OF COUNCIL OF MEDICAL SPECIALTY SOCIETIES
SVS EXECUTIVE DIRECTOR KENNETH M. SLAW, PhD, was appointed to the Executive Council of the Council of Medical Specialty Societies (CMSS). This body comprises 53 board-certified medical specialties, representing over 800,000 specialty physicians across the U.S.
“I am proud and honored to do all I can to accelerate the movement of specialty societies and CMSS to face a litany of future challenges,” said Slaw. “Vascular health and healthcare spans the lifespan, and interacts with dozens of other medical specialty physicians and societies. Serving CMSS will tighten these important relationships for the SVS and help improve care for patients. The SVS will have a front-row seat and active role in addressing the future of healthcare.”
As a collaborative body, the CMSS has effectively brought together various medical specialty societies to address common issues, challenges and national initiatives, added Slaw. CMSS has established cross-society policies for ethics, relations with industry, diversity, equity and inclusion (DEI), and takes formal advocacy positions when essential to foster and protect specialty medicine.
The CMSS mission is to “advance the expertise and collective voice of specialty societies in support of physicians and the patients they serve.” The vision emphasizes collaboration and states that “specialty societies can advance healthcare for patients and physicians by working together.”
Staff executives in specialty societies meet across numerous professional peer groups to share best practices and optimize education, marketing, communications, governance, legal, industry relations, registries and quality initiatives.
SVS Foundation’s ‘Celebration of Science’ campaign inspires support for vascular health advancements
THE SVS FOUNDATION HAS launched its “Celebration of Science” campaign, an end-of-year giving initiative to recognize the achievements of healthcare heroes while driving crucial funding.
The campaign will spotlight the Foundation’s mission to fund vascular health. Leaders hope to raise $60,000 by Dec. 31 to ensure continued support for ground-breaking work in vascular disease.
A standout feature is a Giving Tuesday match, sponsored by longstanding partners at Gore, which took place on Nov. 28.
“The overall campaign serves as a rallying call for supporters to contribute,” said SVS Foundation Chair Michael C. Dalsing, MD.
To contribute to “Celebration of Science,” visit vascular.org/Donate.
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson and Will Date
Randomized trial set to elucidate value of image fusion technology for aortic repair
AN ONGOING UK NATIONAL INSTITUTE FOR Health and Care Research (NIHR)-funded randomized controlled trial (RCT) seeks to illuminate the value of an image fusion guidance technology for endovascular aortic repair. In a presentation on the trial at this year’s VEITHsymposium (Nov. 14–18) in New York City, Rachel Clough, MD, a consultant vascular surgeon at King’s College London in London, England, outlined the issue at hand. While endovascular devices are available to treat complex aortic disease using a combination of branches and fenestrations, she said, challenges arise when positioning these devices in three-dimensional spaces. “We currently use high-contrast and high-spatial resolution CT [computed tomography] angiography to both plan these procedures and to design these custom-made devices,” Clough said. Until recently, however, she noted that there was “no direct link” between these preoperative image data and intraoperative two-dimensional fluoroscopy images. To remedy this, Clough detailed that a new technology— Cydar Maps (Cydar Medical) image fusion guidance—was designed in order to accurately and in real time automatically overlay preoperative CT, volume-rendered aortas onto intra-
operative fluoroscopy data.
The presenter noted that Cydar Maps is now a cloudbased product that incorporates three phases—planning, navigation and review. The benefits of a cloud-based system, Clough relayed, include the fact that it is always updated, enables remote planning and review of cases, and provides a platform for sharing data with other organizations or device companies.
Furthermore, Clough said, the technology has the benefit of being able to aggregate data in an effort to develop data-driven clinical decision support. “During the planning, navigation and review phases, the data are pooled and then analytics can be used to try to predict outcomes,” the presenter explained. She continued that a particular patient could be matched to similar previous patients, and not just necessarily in one center, but across multiple centers, after which predictions of outcomes based on different device type usage could be provided.
Data-wise, Clough shared that the technology has been demonstrated in independent case-control series in both the United Kingdom and the U.S. to result in reduced radiation and procedure times in both standard and complex endovascular repair. In fenestrated cases, she added, it has also been shown to reduce the amount of iodinated contrast agent used. The presenter further noted a sustained reduction in radiation exposure for the operator after just 10 cases.
Integration into healthcare systems, however, will require further data. “We
VOYAGER PAD analyses shed light on use of rivaroxaban in high-risk patient populations
NEW ANALYSES FROM THE VOYAGER PAD clinical trial in both high-risk and fragile patients and those with and without comorbid coronary artery disease (CAD) were presented at the American Heart Association (AHA) 2023 Scientific Sessions (Nov. 11–13) in Philadelphia.
The randomized, double blind VOYAGER PAD trial enrolled more than 6,500 patients in 34 countries who had peripheral arterial disease (PAD) and had undergone lower-extremity revascularization.
Patients were randomly assigned to receive either rivaroxaban (Xarelto, Janssen) or a placebo in addition to daily aspirin. The research team previously reported that VOYAGER PAD met its primary endpoint, with a 15% statistically significant reduction in the risk of a first major adverse limb or cardiovascular event (MALE or MACE) seen in patients who received rivaroxaban compared with those who received the placebo.
Fragile patients with PAD can be at a heightened risk for MALE, defined as a composite of acute limb ischemia (ALI) and major amputation. In the first of the two analyses presented by Mario Enrico Canonico, MD, from the University of Colorado Anschutz Medical Campus in Aurora, Colorado, fragile patients were
defined as being older than 75 years, weighing less than 50kg, or having a baseline estimated glomerular filtration rate (eGFR) less than 50 mL/min/1.732.
Rivaroxaban plus aspirin (2.5mg twice daily plus aspirin 100 mg once daily) was shown to be effective in reducing the occurrence of MALE in both fragile and non-fragile patients, compared to aspirin alone. In fragile patients treated with rivaroxaban plus aspirin, 6.2% of patients experienced a MALE compared to 10.3% of patients treated with placebo. In non-fragile patients, 7.9% of patients treated with rivaroxaban plus aspirin experienced a MALE compared to 9.7% of patients treated with placebo.
The second analysis examined the role of rivaroxaban plus aspirin on myocardial infarction (MI) in patients with PAD with and without concomitant CAD.
In this analysis, 14.1% of patients with PAD and CAD treated with rivaroxaban plus aspirin experienced a MACE versus 17.6% of patients treated with placebo (aspirin alone). In patients with PAD only, 11% of patients treated with rivaroxaban plus aspirin experienced a MACE versus 9.8% of patients treated with placebo. Overall, rivaroxaban plus aspirin showed a consistent benefit in reducing MACE in patients with and without CAD.
need to demonstrate that [Cydar Maps] provides similar operator benefit and similar or lower overall costs compared to comparators, as the UK is a value-based healthcare system,” Clough stated. She noted that the UK National Institute of Health and Care Excellence (NICE) has a digital evidence framework that requires a high-quality randomized trial for any technology designed to guide treatment.
Against this backdrop, Clough and Tom Carrell (co-creator of Cydar Maps) applied for funding to NIHR for an RCT to investigate the technology’s value. The funding was granted, and the investigators subsequently set up a prospective, multicenter, two-arm RCT recruiting patients with thoracoabdominal aortic aneurysm (TAAA) and AAA at 10 UK sites.
“[The trial] is designed to capture real-world practice, so it is deliberately relatively simple,” Clough commented. A quality-of-life questionnaire (the 10-question EQ5D) is really the only additional element needed for the trial, she added.
“We are pleased that, on the whole, sites are recruiting patients well [for the Cydar Maps randomized controlled trial]”
RACHEL CLOUGH
Clough continued that patients will be randomized in a 1:1 fashion, with the aim being to recruit a total of 340 patients. Clinical, technical and cost-effectiveness data will be collected to evaluate the technology.
The presenter closed with a progress report, detailing that 213 patients—just over 60% of the cases required—have been enrolled so far. “We are pleased that, on the whole, sites are recruiting patients well,” she remarked, noting that around 80% of all eligible patients that are screened are being recruited into the trial.
GORE® TAG® Conformable Thoracic Stent Graft with ACTIVE CONTROL System
INDICATIONS FOR USE IN THE U.S.: The GORE® TAG® Conformable Thoracic Stent Graft is intended for endovascular repair of all lesions of the descending thoracic aorta, including: isolated lesions in patients who have appropriate anatomy, including: adequate iliac/femoral access; aortic inner diameter in the range of 16-42 mm; ≥ 20 mm non-aneurysmal aorta proximal and distal to the lesion. Type B dissections in patients who have appropriate anatomy, including: adequate iliac/femoral access; ≥ 20 mm landing zone proximal to the primary entry tear; proximal extent of the landing zone must not be dissected, diameter at proximal extent of proximal landing zone in the range of 16-42 mm.
CONTRAINDICATIONS: Patients with known sensitivities or allergies to the device materials; patients who have a condition that threatens to infect the graft. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
Products listed may not be available in all markets.
GORE, Together, improving life, ACTIVE CONTROL, TAG and designs are trademarks of W. L. Gore & Associates. 2023 W. L. Gore & Associates, Inc. 231254052-EN NOVEMBER 2023
Your smarts. Your skills. Your relentless pursuit of what’s possible. They’re all part of what makes TEVAR triumphant. As we commemorate the 25th anniversary of the GORE® TAG® Device family,* we’re celebrating everyone who has helped to make this foundational procedure possible. From the first device to future development, we are TEVAR.