





BY MALACHI SHEAHAN III, MD
INTERVIEWER: “Good morning, nice to meet you. Are you going to get pregnant?”
While this may seem like a shocking way to begin a conversation, some version of this dialog occurs in many surgical residency interviews. According to research presented at the 2021 Society for Clinical Surgery Symposium by Arash Fereydooni, MD, and colleagues, more than one-third of vascular applicants in the 2020 Match were asked about marital status and family planning. Females experienced a significantly higher proportion of these inquiries than their male counterparts. Speak with a few female surgeons, and it becomes clear that bias in interviews extends far beyond training. As a specialty, our answer to this issue can’t be “try to stop asking sexist questions.” Don’t worry though—as usual, I have a solution. And you (as usual?) will probably hate it. The answer? Stop interviewing
I have heard the resistance already. You are a chief, chair, program director, or some other thing of great significance. You have been interviewing candidates for decades. You have an unwavering confidence in your ability to spend 20 minutes with someone and “feel them out.” Well, no one else has told you this, so I will. Stop. You are not just bad at interviewing, but you are actively terrible. A literal lottery would produce better results. How do I know this? Because you are human.
A few years ago, the University of Texas Medical School at Houston increased its enrollment from 150 to 200 students. The expansion was authorized late in the application cycle, so the class had to be filled with 50 students who most schools had already rejected, often based on low interview scores. Over the next four years, there was no difference in performance between the last 50 students and the 150 picked first. The interviews had failed

to select better candidates. A 2012 study by Jason Dana and Robyn Dawes asked participants to predict students’ GPA for the upcoming year. The participants were given the students’ background information, including previous semesters’ GPA. They then conducted interviews with half of the students. While instructed that a student’s academic record is the best predictor of future performance, the participants often let their interview impressions outweigh these data. As a result, they were much worse at predicting future GPAs among those they interviewed.
Through these and many other studies, science has found that humans have a persistent, irrational confidence in their interviewing ability. In most cases, this misplaced conviction significantly hinders the process of selecting the best applicant. Renowned psychologist Scott Highhouse calls this “the greatest failure of industrial and organizational psychology.”
Most surgeons would point to the interview process as an integral tool for selecting applicants who will be the best fit with their culture. That is because we have a misunderstanding of the most critical components of work culture. We want to hire doctors who will work hard and succeed, and are also easy to get along with. So as a proxy for developing this rubric, we tend to hire people just like ourselves. After all, what is your model for success? Most
likely yourself or some other archetype you associate with achievement. If you were a collegiate lacrosse player, you tend to value this characteristic in others. This process leads us to limit the potential paradigms for success. Interviewing tends to exclude outliers, to reject exceptionalism. Would you find the young doctor from the University of Baghdad who will become aortic disease titan Hazim Safi, MD? More likely you wouldn’t even interview him.
Organizational psychologists know that effective work cultures are not built on cohesive personalities. They are formed with congruent values. A department developed with doctors who value collaboration and learning will always outperform one with a great lacrosse team. Our current interview system, however, is poorly designed to identify core values. Most applicants already have set answers for our values-based questions. We think we are interviewing medical students, but, in reality, we are interviewing their publicists.
Interview scenario: The interviewer asks, “What is your greatest weakness?”
Applicant: “I think it’s that I care too much. I will never rest until I get the job done. I will stay single-minded on a task at all costs. I guess what I’m saying is that if you hire me, I will literally murder your enemies.”
In medicine, most of us conduct what are called unstructured interviews. The interviewer is free to explore random details they find relevant. Have you ever lived in the South? What are your hobbies? If you were a tree, what kind of tree would you be? (Obviously the type of tree that would murder your enemies!) The problem with unstructured interviews is that the interviewer rates them highly for perceived effectiveness, but, in reality,
“Most surgeons would point to the interview process as an integral tool for selecting applicants who will be the best fit with their culture. That is because we have a misunderstanding of the most critical components of work culture”
continued on page 7
VASCULAR SPECIALIST
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD, Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Marie Drudi, MD
Executive Director SVS Kenneth M. Slaw, PhD
Director of Membership, Marketing and Communications Tara J. Spiess CAE
Managing Editor SVS Beth Bales
Marketing & Membership Specialist Anna Vecchio
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA Publishing. Content for the News From SVS is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA Publishing will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein.
The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018.
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com.
For missing issue claims, e-mail subscriptions@bibamedical.com.
Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA Publishing.
Printed by Vomela Commercial Group
© Copyright 2021 by the Society for Vascular Surgery
Published by BIBA Publishing, which is a subsidiary of BIBA Medical Ltd.
Publisher Roger Greenhalgh
Content Director Urmila Kerslake
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution
Jocelyn Hudson, Will Date and Jamie Bell
Design Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
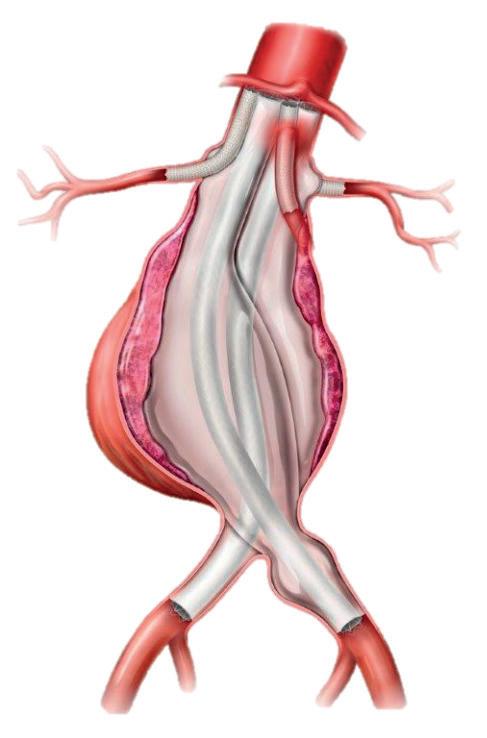
Radiopaque marker band
Radiopaque Marker Bands for accurate placement and visualization
Occlusion membrane
Occlusion membrane supports rapid occlusion and limits recanalization
Distal nitinol fiber segment
Distal nitinol fiber segment designed to limit migration and promote thrombus formation


Proximal nitinol fiber segment
Proximal nitinol fiber segment designed to stabilize the membrane and promote thrombus formation
Radiopaque marker band
Radiopaque marker band
BY BETH BALES
Vascular surgeons could see a significant cut in reimbursement if the proposed Medicare Physician Fee Schedule is made final. The Society for Vascular Surgery (SVS) plans to work to stave off the decreases through advocacy, continued work with the 12-member Surgical Care Coalition, working with members of Congress and grassroots action from members.
THE CENTERS FOR MEDICARE AND MEDICAID Services (CMS) released the rule—cutting the Medicare conversion factor for calendar year 2022 by 3.75%—in
mid-July. The conversion factor is the basic starting point for calculating Medicare payments. CMS is reinstating the cut that Congress prevented in late 2020, and, without action from Congress, surgeons face significant payment cuts in 2022.
Preliminary study of the proposal indicates only interventional radiologists face larger reimbursement cuts than vascular surgeons. Because of changes in reimbursement for practice expenses, in fact, those vascular surgeons who practice in community settings could be facing a severe cut that could be end up being larger than 20%.
“Vascular surgeons not only provide surgical care when indicated, but a tremendous amount of pre- and post-surgery medical management and long-term care— often for the rest of patients’ lives, for millions of seniors covered primarily by Medicare,” said SVS President Ali AbuRahma, MD.
“If these cuts proceed, the elderly population in this country will face an enormous crisis of access to quality care—not only surgical care, but support in decisionmaking and lifelong medical management for optimal vascular health.”
The Medicare program’s budget-neutral rules are
BY BETH BALES AND BRYAN KAY
Following a year like no other comes a Vascular Annual Meeting (VAM) like no other—sort of.
THIS YEAR, THE KEY DATE ON THE vascular conference calendar features a seemingly unprecedented double header: a Presidential Address tandem. After the cancellation of the 2020 VAM in the wake of the COVID-19 pandemic, then serving Society for Vascular Surgery (SVS) President Kim Hodgson, MD, was unable to deliver the customary presidential send-off talk. In its stead, this year VAM (Aug. 18–21; San Diego) will feature addresses from both immediate past presidents. Ronald L. Dalman, MD, who recently handed over the SVS presidency to Ali AbuRahma, MD, and Hodgson, who served as president from 2019–2020, will take to the podium on separate days with talks that reflect on 75 years of SVS history and look ahead to where the vascular surgical specialty is headed. Yet, as Dalman points out, the incidence of two addresses at one SVS conference is not without precedent. Some 18 years ago, before the SVS merged with the American Association for Vascular Surgery (AAVS), the joint annual meeting held between the two societies included addresses from their respective presidents. His predecessor brings this broad sweep of societal history right up to the
SVS of today and pressing clinical matters currently on the leadership agenda. “If you build it, he will come,” intones the mysterious voice in the classic baseball movie Field of Dreams. But Hodgson has a slightly different take on this with respect to some important SVS initiatives. His voice would proclaim: “We built them. It’s up to you to use them.”
He’s referring to the latest additions to the SVS portfolio of Quality Improvement tools, the just-completed Appropriateness Use Criteria (AUC) on Intermittent Claudication, and the remotely monitored SVS Supervised Exercise Therapy (SVS SET) app and Vascular Center Verification and Quality Improvement Program, both nearing the end of their pilot phases.
“These are tools the SVS has developed to help members distinguish themselves from the less scrupulous actors in the space, in the case of the verification program, and to improve the outcomes and care of our patients,” Hodgson says. He was giving a preview of the Presidential Address he will deliver Thursday, Aug. 19, at VAM. “Membership now has to stand up and embrace these things and participate.”
driving many of these cuts. The SVS applauded the CMS effort to update the clinical labor rates after 20 years (i.e., nurses, technologists).
However, the burden of the “pay-for” is disproportionately distributed within the Medicare fee schedule, the Society said. The SVS believes CMS should hold harmless specialized services performed in the office-based setting when implementing the muchneeded update to clinical labor rates.
Surgical care cuts harm patients by threatening access to critical treatments and procedures. For SVS members, whose patients primarily are Medicare patients, this threat is at the heart of their worry over the CMS proposed rule.
More information will be available in the coming weeks and months, and SVS members are urged to follow this issue closely.
“While it is true that the magnitude of the cuts will differ based on an individual's practice venue and pattern, we are all vascular surgeons,” said Matthew Sideman, MD, chair of the SVS Policy and Advocacy Council. “Cut one of us and we all feel the pain. My mission, as council chair, is that we fight for all vascular surgeons. We must all stand united to overturn this unfair policy.”
SVS is developing a verification program for vascular surgery practices, in both the outpatient and inpatient settings. “Outside people are coming in, looking at your program, reviewing it, talking with you, interviewing your staff. It’s active quality improvement, not passive,” he said. Of special importance is a focus on defining quality and appropriateness of care for all vascular surgeons across practice settings, but with some emphasis on practitioners working in an OBL (outpatientbased lab). OBLs as a site of service are extremely important to the future of vascular surgery. However, they are relatively unregulated for quality and appropriateness and so more open to the potential for outlier practice behavior, Hodgson added. He stressed neither he, nor the SVS, are “antiOBL—we are pro-quality and appropriateness. If we don’t set up standards and assess ourselves, someone else surely will do it for us.” Currently, the SVS is “in the final stage of the piloting—with six practices included—to evaluate the relevance of our standards,” he says. Hodgson also lauds SVS SET, the app that employs coaches plus tracking via phones to supervise patients with peripheral artery disease in their walking therapy, as a substitute for SET done in a medical setting. Challenges remain, including
“We built this. Now it’s up to our members” — Kim Hodgson
insurer reimbursement, but preliminary results are promising, says Hodgson. The app is another tool members can use to deliver top-notch patient care, he adds. “We built this. Now it’s up to our members.”
Meanwhile, Dalman is set to use his address, set for Friday Aug. 20, to touch on the three-quartercentury-long legacy of the SVS and its antecedents.
“Having two presidential addresses this year honors our history” — Ronald L. Dalman
“As the 75th president, I will celebrate what the SVS has accomplished since our founding in 1946, as well as anticipating the challenges that lie ahead,” he says. “A robust and effective SVS is essential for the health and sustainability of the specialty of vascular surgery.” His time at the podium, he explains, will outline what is going to be required to keep the SVS going strong for another 75 years.
Dalman opened his presidency at the 2020 VAM digital replacement, SVS ONLINE, with a Crawford Forum focused on the existential questions in the specialty. Dalman elaborates on the broad context of the SVS. “Prior to the merger of the AAVS and SVS in 2003, the combined AAVS/SVS meeting, as VAM was then called, always included two presidential lectures,” he says. “Having two presidential addresses this year honors our history as well as acknowledging the unfortunate cancellation of VAM 2020 in Toronto.”
BY BETH BALES
On the heels of a worldwide pandemic that has helped expose deep disparities in healthcare, the Society for Vascular Surgery (SVS) has published a response—and a promise—in the form of the 2021 diversity supplement, summarizing what Society members have learned and how to move forward.
The supplement, “Creating Success in Comprehensive Vascular Surgical Care Through Diversity, Equity and Inclusion,” is an addition to the August edition of the Journal of Vascular Surgery (JVS). Bernadette Aulivola, MD, Dawn Coleman, MD, and Joseph Mills, MD, are guest editors for the supplement, available at vascular.org/ DEIsupplement.
“The SVS is deeply committed to understanding inequities related to gender, race, ethnicity, age and sexual orientation, and developing strategies to make meaningful changes,” said Aulivola. She served as chair of the SVS Diversity, Equity and Inclusion (DEI) Task Force, created in 2019. The task force has since segued into an SVS committee led by Vincent Rowe, MD, and charged, in part, with assuring implementation of the task force recommendations.
“Scientific and anecdotal research has shown us that many vascular surgeons are working tirelessly to address disparities within healthcare, but new approaches are essential in making continued progress,” Aulivola said. “Publications like this supplement serve to enhance our understanding of the current status of diversity-related issues in the field of vascular surgery. The focused efforts of the SVS DEI Committee will assure that we become a stronger specialty that is better equipped to care for a diverse patient population.”
said Dalman. The articles cover a variety of topic areas, promoting equity and inclusion opportunities in the SVS and in its members’ workplaces, he said.
More than a year in the making, the DEI supplement covers 16 topic areas. These include not only those that would be expected in a document such as this, like a review of healthcare disparities in vascular surgery; mentorship; inclusion and retention opportunities and challenges; and pay disparities. But it also explores the unexpected, including a study into bias and letters of recommendation. Awareness of bias has been building steadily within the SVS for more than a decade, and so have challenges to it. This forward motion culminated in 2019 in the creation of the DEI Task Force, said Dalman. The group presented its findings and recommendations to the SVS Executive Board in July 2020. The Board accepted the report and recommendations, and began an implementation plan, “underscoring our commitment to evolutionary change in both the structure and the function of the SVS,” Dalman added.
continued from page 4
they are among the worst predictors of job performance. Our overconfidence in our expertise and experience leads us to cling to this broken system. Unstructured interviews are not only ineffective, they are also a perfect environment for our implicit biases to run amok. Many of these biases focus on women. They will need to leave early to take care of their children. They will take an extended maternity leave. They will get married and not care about surgery anymore. Gender norms are powerful. Men who brag about their accomplishments are seen as confident, while in women this characteristic is seen as cockiness. Therefore women tend to downplay their achievements. Prior to conducting a skills course, I have the trainees complete a self-assessment regarding their ability to perform various procedures. One rated their confidence in performing an open thoracoabdominal aneurysm repair as “extreme.” The surprise was not to learn that the trainee was a male but rather that he was an intern. Extreme indeed.
applicant’s CV so the score can provide an independent data point. Each answer should be scored immediately and independently to eliminate a potential halo effect when one attribute of the applicant (either an answer or a personal characteristic) is viewed so favorably by the interviewer that all of their other scores are artificially buoyed. The pitchfork effect is the opposite, such as a student from Alabama may experience with me during football season.
Structured interviews allow for qualitative assessments over time. Which questions best predicted job performance? If likability is really important to you, then grade it. This is obviously open to bias, but if given a numeric score, it becomes controllable. Other best practices include avoiding panel interviews and group assessments which are subject to the dominant personality problem. Do you really want all of your hires to mirror the most overbearing and irritating doctor in your group? Finally, use the scores. Sure, it’s shady math, but at least it’s math? According to psychologists, the best predictors of future job performance are work sample tests. These assessments require applicants to perform physical or psychological tasks similar to those they would experience on the job. So an aspiring sales executive might be given 20 minutes to design an ad campaign. Work sample
“A diverse vascular surgery workforce yields cognitive diversity”
The supplement’s summary of “what we have learned and how to move forward is the measure of the moment,” said Ronald L. Dalman, MD, president during the document’s creation.
— Dawn Coleman
The measurement’s precedent, he said in the introduction to the supplement, lies in the 2010 JVS diversity supplement. Unlike the 2021 version, that publication focused primarily on vascular health outcome disparities among underrepresented minority populations. “This year’s update turns that focus inward, to challenges within the profession itself,”
“A diverse vascular surgery workforce yields cognitive diversity, which is essential to deliver higher quality healthcare to our collective patients,” said Coleman. “Diversity, supplemented with equity and inclusion, yield a superior creative culture that will optimize the specialty of vascular surgery.” She added that “this critical culture change will empower vascular surgeons to be the best and most effective version of themselves for their patients, their learners and their peers and [it] ultimately will enhance patient care, personal and professional growth, and workforce recruitment and retention.”
The new supplement “dramatically advances” on its 2010 predecessor, said Dalman. “Our task now is to implement the structural changes necessary to ensure the future of the SVS and the wellness and professional success of our evolving membership,” he said.
A study by Jessi L. Smith and Meghan Huntoon at Montana State University examined womens’ unease with selfpromotion. They asked two groups of female students to write an essay describing their accomplishments to earn a scholarship. A black box was placed in the room with each group. The box was unexplained to the control group, but the others were told it was a subliminal noise generator that can’t be heard but may cause mild discomfort. The box itself was empty, of course, because there is no such thing as a subliminal noise generator. The group that was warned about possible discomfort performed significantly better on their essay scores. It seems that women may experience distress with selfpromotion, but this can be overcome if acknowledged and explained, even by something that does not exist.
Over the past several years, I have conducted a semi-qualitative analysis of my own interview “instincts.” Not of my trainees; that is too small a sample size. When I travel to different institutions or meetings, I try to take stock of the progress of vascular residents I did not take. Particularly of those who did not impress me. The results were sobering enough that I stopped interviewing applicants altogether. Instead, I let them interview me. To their credit, they have all managed not to ask me about my family and marital plans.
If I can’t convince you to turn your hiring process into some megamillions-type lottery carnival, there are some alternatives rooted in science.
Structured interviews allow each candidate to face the same questions, in the same order, in the same amount of time. The interviewer should be blind to the
“It is time to reform our process for selecting surgical trainees and faculty. Questions about marriage and children are not only Match violations, they are also a defiance of federal laws”
tests also help to eliminate age, gender and appearance biases. Research in developing these tools for surgery is desperately needed. Technical skill assessments might seem like a logical place to start. But after 14 years of experience testing trainee surgical proficiency, I would caution against using this metric to predict future ability among novices. The scatterplot of technical skill during the first year of residency is mostly noise, but it sharpens inexorably to competence as training and experience proceed. If we really consider ourselves master teachers, shouldn’t we be fighting over the true disasters anyway? I’ll take the hard worker who can’t tie a knot over the lazy prodigy any day.
It is time to reform our process for selecting surgical trainees and faculty. Questions about marriage and children are not only Match violations, they are also a defiance of federal laws. If we can’t even conduct interviews without committing actual crimes, it’s probably time to move on.
MALACHI SHEAHAN III is the Claude C. Craighead Jr. professor and chair in the division of vascular and endovascular surgery at Louisiana State University Health Sciences Center in New Orleans.
BY BRYAN KAY
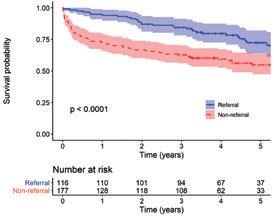
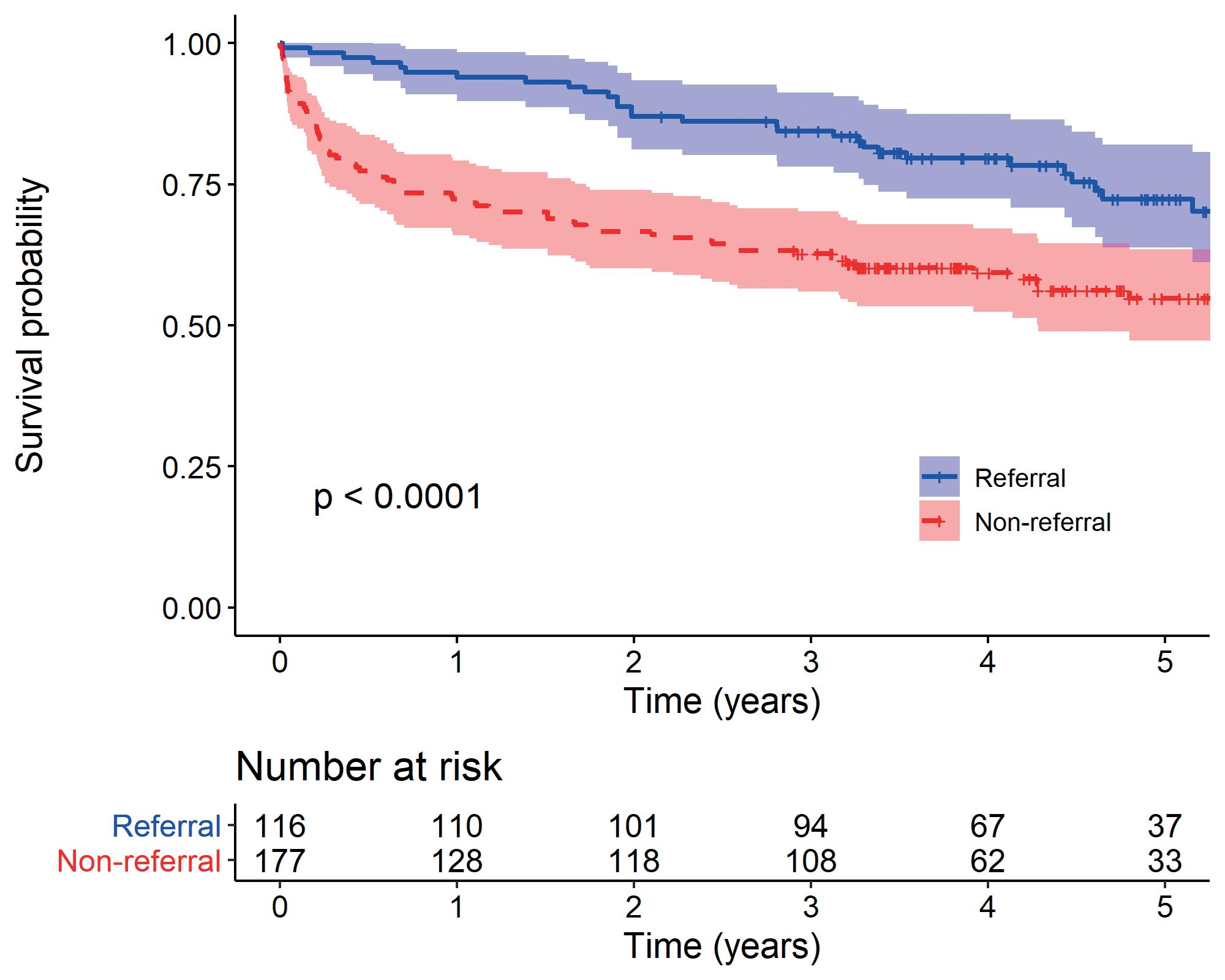
Prosthetic referral was an independent predictor of long-term survival among patients who had undergone lowerextremity amputation, new findings set to be published in the Journal of Vascular Surgery will reveal.
Asingle-center retrospective study by William Shutze, MD, a vascular surgeon at Texas Vascular Associates in Dallas, and colleagues found factors associated with decreased survival were increasing age, higher American Society of Anesthesiologists (ASA) class, Black race, and body mass index (BMI), and that prosthetic referral was linked with improved survival with a hazard ratio (HR) of 0.73 vs. 0.55 for non-referral. Prosthesis-referred patients were approximately 50% less likely to experience mortality (propensity-score adjusted HR 0.54).
Shutze explained he was motivated to drill into data concerned with which patients were being referred for prosthetics and those who were not—as well as where survival fits into this conundrum—after identifying a hole in the vascular literature.
“We had developed in-house prosthetics delivery—and that gave us the ability to capture all of the information on the clinical side and the prosthetics side, as well as to know who was actually crossing over,” he told Vascular Specialist
“Whereas, traditionally, for patients who are having an amputation, the prosthetics piece is outsourced. After doing this for about five years, I realized that the prosthetics side of the care for our vascular patients is not really well studied in the vascular world. There are other specialties where it’s looked at a little more closely, and I relied on those for our background research to get a better understanding. In the vascular world it was kind of a black box.”
Shutze and colleagues also sought to establish reasons why the patients were not referred for prosthetics.
“Vascular surgery would automatically assume that somebody who is being referred for prosthetics is going to be healthier than somebody who is not,” he said. “That may not be the case. There may be other barriers like ability to pay; there could be unconscious bias. So we did this analysis to get a better understanding of these factors. What type of patients will face barriers to referral and what is the survival after a lower-extremity amputation— and how does the prosthetics piece fit into that?”
The study included 293 patients who underwent amputation between January 1, 2010, to June 30, 2017, excluding patients who had amputations below the ankle or hip disarticulation. The cohort bore a mean age of 66, with 53% classed as white, 32% Black, and 15% as other. The average BMI was 27. The most common comorbidities were diabetes and hypertension—present in the majority.
A significant number (158) were classified as ASA IV or V. Approximately half (51%) of the patients were current
or former smokers and almost half (51%) were on a statin medication. The majority of the patients had a below-theknee amputation (BKA)—71.6%. Twenty-one patients, or 7.2%, developed an amputation stump complication significant enough to require a revision, Shutze and colleagues discovered.
They established that prosthetic referral occurred among 42% of their cohort. Significant differences were observed between patients referred vs. those not referred in age, sex, hyperlipidemia, ASA class, postoperative ambulatory status, need for surgical revision, and amputation level.
“The multivariate model identified age >70 years, female sex, diabetes, ASA score of IV or V, postoperative ambulatory status and current smoking status as significantly associated with failure to refer for prosthetic fitting,” they write in their paper. “Patients having a BKA, BMI 25–30, history of previous arterial procedure or revision were more likely to be referred for prosthetics.”
One-year survival was 81.2% overall—86.7% in the BKA subgroup and 67.5% among above-the-knee amputation (AKA) patients. In terms of five-year survival, the overall figure was 61.7%, with 64.7% and 53.8% in the BKA and AKA subgroups, respectively. Survival was statistically significantly lower among patients undergoing AKA than BKA, Shutze et al revealed.
“Our study was the first to connect long-term survival to the ASA score,” Shutze elaborated. “And we also found that BMI had an effect on survival as well. The prosthetic piece was surprising: We took what appeared to be similar patients and found that if the only difference was prosthetics referral, getting a prosthetics referral was associated with long-term survival.
“Some studies in the past have said that if you get a prescription for your prosthesis, that counts as a referral, but the patient may never go. For us, the patients actually had to be fitted with a temporary prosthesis. So they had
“After doing this for about five years, I realized that the prosthetics side of the care for our vascular patients is not really well studied in the vascular world” — William Shutze
to complete the mission, follow up with our prosthetist, get evaluated, and then sign on to get the prosthesis. That independently was associated with better long-term survival.
“This raises a lot of questions. Why would just having a prosthesis independently be predictive of better long-term survival? It’s something that we’re not capturing. Perhaps frailty, or perhaps there are some biases. There may be some benefits to prosthetic fitting—even with a temporary one—that has effects we might not even think of. Now the patients might have better mobility, and so can get in to see the doctor easier. Their overall healthcare is better. Maybe there are some psycho-emotional factors. With patients who have a prosthetic—do they do better on the anxietydepression scores? This opens up all kinds of interesting avenues that we can go down to try to understand this better.”
Shutze elaborated on potential barriers to prosthetics referral. “We found some areas that are independent of each other: older patients, females, higher ASA scores and people who smoke. Some of these areas make you wonder: Since these are independent, is there some bias in our referral practice? Maybe we have some unconscious bias against certain people.”
Shutze and colleagues identified two areas for further research in their JVS paper.
“The first one is to determine whether the factors identified as associated with non-referral are markers for patient characteristics that make them clinically unsuitable for prosthetic fitting, or if they are symptoms of unconscious bias or of a patient’s access to care which would need to be addressed through the development and implementation of standardized referral criteria and/or systemic changes to eliminate financial, geographical, or physical barriers to prosthetic referral and fitting,” they write.
“The second one is to validate the prosthetic referral-survival benefit for variables that were not captured in this study and may have impacted the findings.”
William Shutze
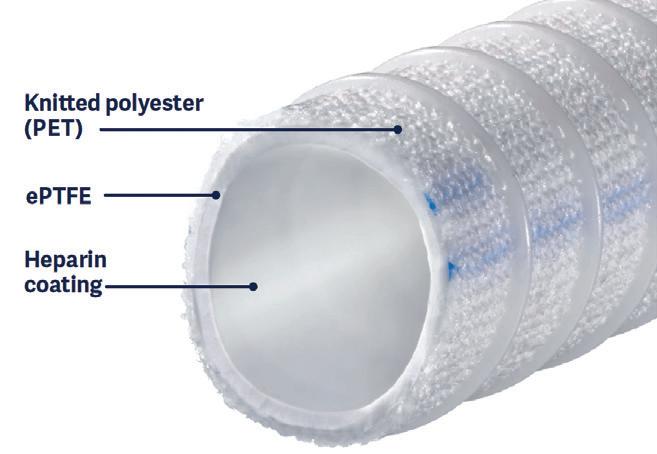
Alan Lumsden, MD, Jean Panneton, MD, and Hiranya Rajasinghe, MD, detail the hemostatic and minimally thrombogenic benefits of the Fusion Bioline vascular graft.
WITH A HEPARIN-BONDED luminal vessel surface of minimally thrombotic polytetrafluoroethylene (PTFE) and an outer surface of highly thrombogenic polyethylene terephthalate (PET), Getinge’s Fusion Bioline expanded-PTFE vascular graft has demonstrated remarkable benefits in time-tohemostasis compared with standard PTFE grafts for peripheral bypasses, according to Alan Lumsden, MD, medical director at Houston Methodist DeBakey Heart and Vascular Center at The Methodist Hospital in Houston. Lumsden brings perspective drawn from twin vantage points. When he arrived in Houston to practice vascular surgery, he first worked under the cardiovascular colossus and medical device pioneer Michael DeBakey, MD, who, Lumsden points out, was the first to use a Dacron, or polyethylene terephthalate (PET), graft. Lumsden was also a lead investigator in the randomized controlled trial (RCT) comparing the safety and efficacy between Fusion Bioline and standard ePTFE grafts for femoropopliteal bypasses, known as the FINEST trial. The RCT probed durability and effects on suture hole
“If you compare the Fusion Bioline with the non-Fusion grafts, there was a highly significant difference”
— Alan Lumsden

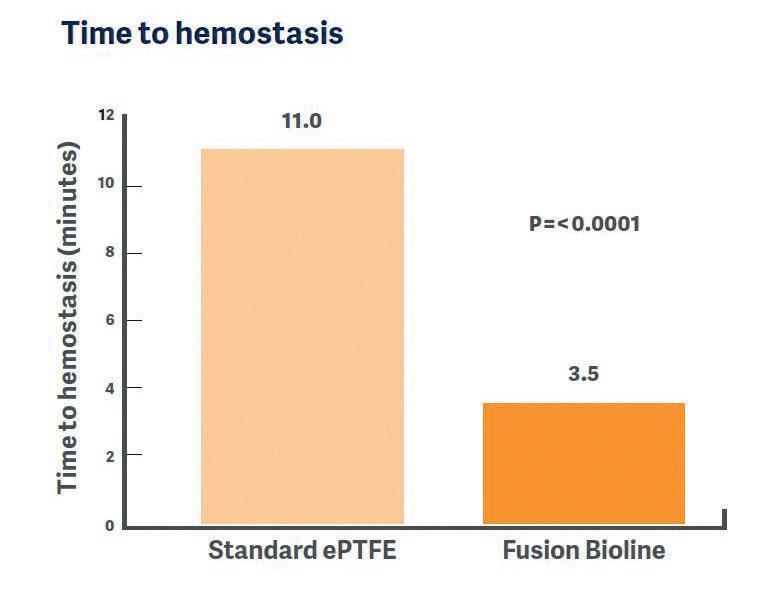
the non-Fusion grafts, there was a highly significant difference between the two. That’s the major point of interest for physicians.”
Jean Panneton, MD, professor of surgery, chief in the Division of Vascular Surgery at Eastern Virginia Medical School in Norfolk, Virginia, and a FINEST trial co-investigator, has routinely used the Fusion Bioline graft since it first cleared Food and Drug Administration 510(k) in 2013. Panneton points out the graft’s high safety profile, saying, “In some ways, it’s probably the most technologically advanced vascular graft that we have because it combines three different characteristics.”

Namely: The inner bioline coating of albumin and heparin, which helps prevent clotting.
agents, but I would say the biggest benefit is this: When you’re suturing surgical anastomoses, the use of vascular sutures pass through this graft nicely in a manner that resembles more of a autogenous graft and less of a prosthetic graft,” he says. “In the alternative grafts that we have had available to use prior to Fusion Bioline, we would simply reverse the coagulation that we give for the procedure, most commonly heparin, so we would reverse that with protamine and perhaps supplement with hemostatic agents on the site of the anastomosis to aid in reducing the amount of bleeding. So clearly, in the case of Fusion Bioline, there is less of a need, or sometimes, in fact, no need for either of that.”
bleeding. “With the Fusion Bioline graft, platelets and red cells see minimally thrombogenic PTFE on the luminal surface, while on the outer surface they see highly thrombogenic PET,” explains Lumsden. “The question was: Could that help the suture hole bleeding? Would this compromise the durability of these grafts? That was what the FINEST trial was really all about. We were not so much trying to show that the Fusion Bioline graft had more durability than an equivalent heparin-bonded PTFE graft, but that it was at least equivalent in durability. And, number two—does it decrease the amount of needle hole bleeding? It turns out that there is equivalence in terms of the durability and there’s a marked decrease
in the amount of bleeding.” Relevant results from the trial showed a primary patency rate at six months of 86.4% for the group implanted with a Fusion Bioline graft, compared with 70% for patients treated with a standard ePTFE graft (95% confidence interval [CI], 2.7–29.9; p=0.006). At 12 months, the patency rates were 76.5% and 67.0%, respectively (95% CI, -4.8–23.0; p=0.05).
“When you compare Fusion Bioline to some of the stents put in, they perform remarkably well,” comments Lumsden.
In terms of heparin elution, he explains the healing process after graft implantation. “Some healing occurs at the peri-anastomotic area—in other words where you actually sew the graft onto the native artery,” he says. “That is the area where grafts can thrombose, and the idea is that when you put these grafts in, this is where they are probably most susceptible to thrombosis. This is why you want the heparin bonding to be maintained—and most of that heparin is on there for a long time. The neat thing about this graft is that on the luminal surface you have an anticoagulant—heparin—bonded to a minimally thrombotic PTFE. With both of those things you would worry about needle-hole bleeding. And that’s the other nice thing about the Fusion Bioline: On the external surface, you’ve got prothrombotic activity.”
Key data from the FINEST trial demonstrated mean time to hemostasis of bleeding at the suture hole was 3.5 minutes in the Fusion Bioline group of patients and 11 minutes in the standard ePTFE group (p<0.0001).
Lumsden recalls using a stopwatch as an objective means of measurement. “Essentially, you sew the anastomosis, you release the flow, and you measure the time to hemostasis—and that’s done with a stopwatch,” he says. “I’ve been in rooms where this can go on for 35–40 minutes. So that’s really very good. And if you compare the Fusion Bioline with
Ultimately, Panneton views the intraoperative of “much less anastomotic bleeding as opposed to a pure PTFE graft” as a chief benefit of Fusion Bioline: “If you have less anastomotic bleeding, you waste less time to achieve hemostasis, and you also end up using less hemostatic agent to try to help you get that hemostatic anastomosis.”
Ordinarily, Panneton would use smaller PTFE needles to obviate suture hole bleeding—or if operating in the neck he routinely deploys bio-glue—but he says using a bioline graft versus a pure PTFE graft “is another way to try to diminish the problem.” He points to the benefit provided by saving on operating room (OR) time. “OR time is precious because, one, it’s hard to have enough operating time as OR time is a precious commodity, and, two, for a hospital OR time is expensive, so every minute counts.”
Panneton adds that the time to hemostasis working with the Fusion Bioline graft, as reported in the FINEST trial, was three times faster than a pure PTFE graft. “In some situations, you’re saving maybe 10 or 15 minutes of time. The other thing that was noted was half-
“If you have less anastomotic bleeding, you waste less time to achieve hemostasis and you also end up using less hemostatic agent...”
— Jean Panneton
usage of hemostatic agent compared to the pure PTFE grafts.”
Hiranya Rajasinghe, MD, a vascular and endovascular surgeon at The Vascular Group of Naples, Florida, lauds the technical benefits of Fusion Bioline grafts.
“We’ve certainly observed that there’s less suture line bleeding and pursuant to that less need for topical hemostatic
Typically, Rajasinghe noted, his team waits anywhere from 7 to 11 minutes during which no other part of the procedure can proceed until hemostasis is achieved. “The advantage of, for example, the Fusion Bioline product by comparison is that you would perform the surgical anastomosis, and, if things go right, there’s no surgical bleeding, and all the other remaining steps of the operation can flow seamlessly.”



BY BETH BALES
The Society for Vascular Surgery (SVS) 2021 Vascular Annual Meeting (VAM) in San Diego (Aug. 18–21) starts in mere days. For those who face travel or other restrictions and cannot attend in person, the SVS has a technical alternative: livestreaming.
Atotal of 17 sessions will be livestreamed during the meeting. This includes all six plenary sessions, several international events and many special events. Physicians can earn a total of 15 Continuing Medical Education (CME) credits via the streaming option. Cost for students, Candidate members-intraining and residents range from $25 to $165. International physicians pay $292; SVS Candidate members pay $354; SVS members pay $475 and non-member physicians pay $623. Register at vascular. org/RegisterVAM21. The full selection of streamed events, in calendar order, and all at Pacific Daylight Time, are as follows:
WEDNESDAY, AUG. 18
n The William J. von Liebig Forum (Plenary 1), 8 to 9:30 a.m.
n Plenary 2, 9:45 to 10:45 a.m.
n The Crawford Forum, 10:45 a.m. to 12:15 p.m.
n International Forum, 1 to 3 p.m.
n International Fast Talk, 3 to 4 p.m.
THURSDAY, AUG. 19
n Plenary 3, 8 to 9:30 a.m.
n Awards Ceremony, 9:30 to 9:45 a.m.
n Roy Greenberg Distinguished Lecture, 9:45 to 10:15 a.m.
n Presidential Introduction and Address (by Kim Hodgson, MD, president in 2019–20), 10:45 a.m. to 12 p.m.
n International Chapter Forum, 1:30 to 3 p.m.
FRIDAY, AUG. 20
n Plenary 4, 8 to 9:30 a.m.
n Special Session: Diversity, Equity and Inclusion, 10 to 11 a.m.
n Presidential Introduction and Address (by Ronald L. Dalman, MD, president in 2020–21), 11 a.m. to 12:15 p.m.
n International Young Surgeon Competition, 1:30 to 3 p.m.
SATURDAY, AUG. 21
n Plenary 5, 8 to 9:30 a.m.
n John Homans Lecture, 9:30 to 10 a.m.
n Plenary 6, 10:30 a.m. to 12 p.m.
Annually, VAM offers two lectures, named in honor of vascular giants Roy Greenberg, MD, and John Homans, MD. These are among the streamed sessions listed above, so even those at home can view the presentations.
The Roy Greenberg Distinguished Lecture will see Elsie Gyang Ross, MD, of Stanford University Hospital and Clinics in Stanford, California, present “Oh the places we will go: How artificial intelligence will transform the practice of vascular surgery.”
Ross is an assistant professor of surgery and medicine at Stanford. She completed a two-year post-doctoral fellowship in biomedical informatics during residency,
and her current research focuses on using machine learning and electronic health records for early disease identification, precision medicine and evaluating opportunities to engage in patient education beyond the clinic.
James C. Stanley, MD, of the University of Michigan Medical Center in Ann Arbor, Michigan, will present the John Homans Lecture. His topic is “Renal artery occlusive disease, renin-angiotensinaldosterone, inflammation and refractory arterial hypertension: A half-century’s perspective.”
Stanley is professor emeritus of surgery at Michigan. He has an extensive clinical practice in arterial reconstructions and a long-standing research interest in molecular and cellular biology of arterial diseases.
For a full roundup of the VAM schedule, visit vascular.org/Planner21.
Visit SVS Booth in the Exhibit Hall Headshots, help and giveaways will all be available at the SVS Booth in the Exhibit Hall during VAM. Be sure to save time in your schedule to not just peruse the exhibits and visit with vendors—plus have lunch, enjoy coffee breaks and watch “Vascular Live” presentations—but also stop by and talk with staff. The SVS Booth is No. 227, towards the back of the Exhibit Hall right across from the Vascular Live presentation area.

At the booth, you can:
n Participate in the Exhibit Hall Scavenger Hunt
n Get a professional headshot, from 10 a.m. to 2 p.m. Thursday and Friday. SVS reserves the right to keep copies of the photos for use in SVS publications
n Sign up for SVSConnect, our online community, download the SVSConnect app or update your profile (import that new headshot, for example)
n Update your SVS membership information
n Get some SVS swag!
Visitors also can pay their membership dues, plus learn about the Society’s educational offerings and programs; the SVS Foundation’s mission and initiatives; the Vascular Quality Initiative (VQI) and the SVS Political Action Committee; and inquire about the Journal of Vascular Surgery (JVS) publications (maybe JVS editors will have some JVS-branded socks to distribute!).
The SVS Booth is also one of the several stops on the aforementioned SVS Scavenger Hunt. Using the SVS VAM mobile app, just scan the QR code in the SVS Booth and answer the membership-related question that appears. Participants receive 10 points for each correct answer.
Prizes are: $3,000 ticket voucher for American Airlines; $1,500 Amazon gift card; and a $500 Apple gift card. Winners’ names will be available in the VAM registration area on Saturday.
host this dinner, to welcome our women colleagues and hear others impart some words of wisdom on challenges—and successes—that will come along the way for them,” said Reed. “And we will also be able to remember and honor our great friend, Robyn Macsata, who left us way too soon.”
Starting a vascular surgery integrated program or fellowship can be a daunting process; a number of misconceptions about required case volume, program affiliations and required number of faculty members exist.
The SVS and the Association of Program Directors in Vascular Surgery (APDVS) have a number of initiatives in place to help.
SVS members Malachi Sheahan III, MD, and Jeffrey Jim, MD, will host “How to start a vascular training program.”
The informative session will be from 9 to 10 a.m. on Friday, Aug. 20. It is planned to be interactive, with experienced program directors offering participants useful information and practice advice.

This year’s Women’s Leadership Dinner will include a tribute to the late Robyn Macsata, MD, a member and Distinguished Fellow of the SVS. Macsata died suddenly on May 21.
The dinner will be held from 7:45 to 9:30 p.m. on Thursday, Aug. 19, in the Balboa/Mission Hills Room in the Marriott Marquis San Diego Marina Hotel. SVS Secretary Amy Reed, MD, and Past President Julie Ann Freischlag, MD, are hosts.
Cost is $80 each. Interested women are asked to register in advance, if possible. Registration is available through the VAM registration site (vascular.org/ RegisterVAM21).
Reed will present the tribute to Macsata, who was chief of vascular surgery at the George Washington University Department of Surgery, Washington, D.C. Three panels, aimed at women at various stages of their careers will follow, with panelists each offering a particular suggestion for success, as well as a challenge for women at each stage of their careers. Audience members will be able to ask questions. All women recipients of this year’s SVS Foundation awards also will be honored.
“Dr. Freischlag and I are delighted to
be presented all four days. SVS opens the submission process to the entire membership, seeking the widest range of topics of interest to its members, who work in a variety of practice settings. Those submitting topics should provide the educational value of a session, a short outline of the program topic, session goals and target audience, among other information.
The Society recognizes the effort and
commitment required to develop VAM programs. This process is intended to elicit preliminary proposals without a great expenditure of time up front, and feedback will be provided for those selected for further development.
Submission proposals are expected to be due toward the end of September.
A link to the submission form will be available at vascular.org/VAM.
BY BETH BALES
The Society for Vascular Surgery (SVS) is pleased to present to its members the 2021-22 officers and the Strategic Board of Directors.
The officer lineup was finalized during the first virtual Annual Business Meeting for 2021 in midJune during which Joseph Mills, MD, was announced as the new Society vice president.
Check the VAM Planner (vascular.org/ Planner21) for more information.
Meanwhile, after VAM concludes, there will be enduring opportunities to view missed content through recordings of various sessions and presentations.
Approximately six to eight weeks after VAM ends on Aug. 21, SVS OnDemand will host the meeting’s educational content.
The videos and recordings will be available free to VAM 2021 registrants. Those who were unable to participate in the meeting will be able to purchase the sessions; special discount pricing will be available for members. It’s the perfect way for VAM attendees to review a session at their own pace, or catch up on something they missed on-site, and for non-attendees to take advantage of all the programming that was presented. Keep your eyes on vascular.org/education for information on VAM21 offerings.
SVS already planning VAM 2022
Preventing complications. Imaging. Limb salvage, wound complications, leadership. Mesenteric artery revascularization and conducting clinical trials. Vascular access and kidney disease. Malpractice. Vascular surgeons encounter situations daily that vex or perplex them. If you’ve ever thought that a particular situation would be perfect for examination at a session at VAM, now is your chance.
Shortly after VAM 2021 ends, the SVS will begin soliciting ideas and proposals from the entire membership for invited sessions for VAM 2022. That meeting will be June 15 to 18, 2022, in Boston. Educational programming will
Officers are President Ali AbuRahma, MD (elected 2019); President-elect Michael Dalsing, MD (elected 2020); Vice President Mills (elected 2021); Secretary Amy Reed, MD (third of three-year term; elected 2019); Treasurer Keith Calligaro, MD (year two of three-year term; elected 2020); and Immediate Past President: Ronald Dalman, MD (elected 2018).
Attendees heard reports from officers and also witnessed the transition of the SVS presidency from Dalman to AbuRahma. The traditional “passing of the gavel” will occur Aug. 21, at the Annual Business Meeting during the Vascular Annual Meeting (VAM).
Acknowledging a term defined by the pandemic, Dalman said that despite that challenge, SVS stayed focused on top member priorities. He thanked the Executive Board, which met much more frequently than usual because of COVID-19, and all committee and council members and chairs.
“We play the hand with the cards we are dealt,” said Dalman, referring to the pandemic. “We made tremendous progress on your behalf. It was truly a privilege and honor to steer us through rocky seas.”
AbuRahma talked briefly as well. “I am extremely honored and humbled to serve as president of your Society for this coming year, to advance our society and our specialty.”
He thanked Dalman for an “outstanding job” during a difficult year. “You have the ship sailing in the right direction, without tipping over,” he said. “All of us appreciate what you have done this past year.”
The Strategic Board of Directors includes all officers and the following representatives:
n Clinical Practice Council Chair, William Shutze, MD
n Education Council Chair, Linda Harris, MD
n Patient Safety Organization/VQI Governing Council, Fred Weaver, MD
n Policy and Advocacy Council Chair, Matthew Sideman, MD
n Quality Council Chair, Thomas L. Forbes, MD
n Research Council Chair, Raul Guzman, MD
n Program Committee Chair, Andres Schanzer, MD
n American Venous Forum, Joann Lohr, MD
n Association of Program Directors in Vascular Surgery, Jason Lee, MD
n Canadian Society for Vascular Surgery, April Boyd, MD
n Eastern Vascular Society, Palma Shaw, MD
n Midwestern Vascular Surgery Society, Sean Lyden, MD
n New England Society for Vascular Surgery, Patricia Furey, MD
n Society for Clinical Vascular Surgery, William Quinones-Baldrich, MD
n Southern Association for Vascular Surgery, Michael Freeman, MD
n Vascular and Endovascular Surgery Society, Murray Shames, MD
n Vascular Surgery Board, C. Keith Ozaki, MD
n Western Vascular Society, Ahmed Abou-Zamzam, MD
n SVS Executive Director, Kenneth M. Slaw, PhD
BY YAZAN DUWAYRI, MD, AND J. SHEPPARD MONDY III, MD
The Society for Vascular Surgery (SVS) has released an updated clinical practice guideline accompanied by an implementation document on the management of patients with extracranial carotid artery disease. Since prevention of stroke related to carotid disease is of major interest to vascular surgeons, the documents aim to use the existing clinical evidence to ensure that patients with atherosclerotic occlusive disease in the carotid arteries receive appropriate treatment and care.
THE CLINICAL SIGNIFICANCE OF CAROTID artery stenosis is mainly related to its prevalence and its potential to cause stroke, defined as partial or global loss of brain neurologic function from blood supply
interruption, or transient ischemic attack (TIA), defined in a similar manner but with symptom resolution in less than 24 hours. Vascular surgeons offer all therapeutic options for the disease entity, including medical therapy optimization, surgical removal of carotid plaque in carotid endarterectomy (CEA) procedures, or carotid artery stenting (CAS).
Extensive research has resulted in the development of evidence to guide treating physicians towards the appropriate type and timing of intervention depending on the degree of carotid disease, the presence of neurological symptoms, and the patient’s comorbidities.
Since publication of the SVS’s previous update of the clinical practice guidelines for carotid disease in 2011, several pivotal studies comparing CEA and CAS have been published. In addition, the literature has demonstrated a confirmation of the need for optimization of medical therapy. Therefore, the updated SVS guideline provides graded recommendations that address five relevant questions: The role of surgical therapy over medical therapy alone in asymptomatic low-risk patients; the role of CEA vs. CAS in symptomatic low-risk patients; the optimal timing of interventions after acute stroke; screening for carotid artery stenosis in asymptomatic
“These guideline recommendations address the latest technology in the management of carotid disease” — Ali AbuRahma


patients; and the sequence of carotid and coronary interventions in patients undergoing intervention for diseases in both vascular territories.
According to SVS President Ali AbuRahma, MD, chair of the guideline writing group, “These guideline recommendations address the latest technology in the management of carotid disease, such as transcarotid artery stenting with flow reversal and how its outcomes compare to transfemoral stenting and the gold-standard, carotid endarterectomy.”
The writing group, composed of experts in carotid artery disease, also identified additional topics that needed to be addressed in more detail. These topics are addressed in a separate implementation document published in the Journal of Vascular Surgery. This companion document includes details about therapeutic decision-making, perioperative management, medical therapy, other cerebrovascular conditions, and practice management. It is intended to make the guideline more practical and helpful to clinicians, and provides implementation details to facilitate adoption and operationalization of the guideline recommendations.
“The advantage of two documents is having quick access to evidence-based recommendations in the clinical practice guideline, while also having the implementation document, which comprehensively addresses every aspect of the management of carotid disease and stroke prevention,” said AbuRahma.
The guidelines provide much needed guidance to vascular surgeons and interventionalists who treat patients with the disease. The ultimate treatment goal should be to decrease the incidence of disabling stroke from this condition.
BY COLLEEN P. FLANAGAN, MD, AND WARREN J. GASPER, MD
In May 1945, President Harry Truman appointed Gen. Omar Bradley to lead what is now the United States Department of Veteran Affairs, with Paul Howley, MD, as chief medical director and orthopedic surgeon Paul Magnuson, MD, as his aide.1,2 Colloquially, most people call it simply the VA, for Veterans Administration.
MAGNUSON’S VISION WAS that each VA hospital should be closely affiliated with a medical school.2 This idea served three important purposes: to give veterans the best access to cutting-edge therapies, to bring federal research dollars into universities, and to establish comprehensive and replicable training programs for U.S. medical school graduates.1,3 With the passage of Public Law 293, the VA Department of Medicine and Surgery was created and the marriage between academic medicine and the VA was born.
instrumental and beneficial for surgical training across subspecialties.4-7
In 2020, the Society for Vascular Surgery (SVS) VA Vascular Surgeons Committee surveyed vascular surgeons practicing within the VA system about their work environment, including their role in surgical education. The vast majority (89%) of surgeons endorsed working in a facility affiliated with an academic medical center; most (76%) practice in a complex/ high-acuity hospital environment; and 52% have regular access to a hybrid room. Importantly, 42% of respondents work with integrated (0+5) vascular surgery residents, and 54% work with vascular surgery fellows.

Today, more than 70% of U.S.-trained physicians will have received at least a part of their training at a VA medical center, and 154 VA facilities are affiliated with 149
allopathic and osteopathic medical schools.1,3 With a population that skews toward older and medically complex patients, this experience has been
The Society for Vascular Surgery (SVS) Vascular Quality Initiative (VQI) has created “My PAD,” a pilot program for collecting patient-reported outcomes (PROs) from patients undergoing endovascular treatment for peripheral arterial disease (PAD). Traditional outcomes such as patency and reintervention may not fully capture the quality of care or the experience of PAD patients. It is important to learn and measure the patient’s perspective, according to the VQI.
VQI LAUNCHED THE MY PAD PILOT IN APRIL. IT INCLUDES SEVERAL SVS VQI centers that participate in the Peripheral Vascular Intervention Registry. The pilot will collect center workflow data and seeks to improve PRO collection in the least burdensome manner by leveraging technology, such as smartphones and tablets.

The SVS VQI will enroll a variety of practice types, from universityto community-based practices in rural and urban settings. This will serve as a foundation for future SVS VQI patient-reported outcome programs.
The data will be collected from patients undergoing peripheral vascular interventions for claudication or chronic limb-threatening ischemia (CLTI). Centers will collect VascuQoL-6 and EuroQol 5D5L (estimated completion time is less than 10 to 15 minutes) at three points: preprocedure, one month and 12 months post-procedure.
The VQI is exploring the introduction of patient advisor groups this fall in order to gain patient perspectives on PAD treatment.—Caroline Morgan and Carrie Bosela For more information, visit VQI@M2S.com.
procedures and patient stories encountered by vascular trainees will no doubt play an integral role in the development of the next generation of specialists.
1. Burns R., Lafave B., Clinard K. VA: The Human Cost of War. Public Broadcasting Service. 2017. Accessed June 1, 2021.
2. Guernsey, J.M. The Veterans Administration and Surgical Education in the United States. Arch Surg. 1989;124(4):407.
3. Dell'Italia L.J. Impact of VA Research on Health Care for All: Contributions Over Nine Decades and Counting. Circ Res. 2017 Jun 23;121(1):16–18.
4. Poteet S., Tarpley M., Tarpley J.L., Pearson A.S. Veterans Affairs general surgery service: The last bastion of integrated specialty care. Am J Surg. 2011 Nov;202(5):507–10.
The VA’s commitment to clinical training is coupled to programs for resident and fellow professional development. The one-year Chief Resident in Quality and Patient Safety (CRQS) and two-year VA Quality Scholars (VAQS) programs provide comprehensive training in quality improvement and patient safety.
For those with broader interests in non-biologic sciences, healthcare research and health policy, the two-year National Clinician Scholars Program (NCSP), in collaboration with the Robert Wood Johnson Foundation, is available. Given that more than half of VA vascular surgeons are involved with training future vascular surgeons, and the VA’s training opportunities for healthcare research, the many vascular pathologies,
5. Bakaeen F.G., Stephens E.H., Chu D., Holman W.L., Vaporciyan A.A., Merrill W.H., Grover F.L. Perceptions regarding cardiothoracic surgical training at Veterans Affairs hospitals. J Thorac Cardiovasc Surg. 2011 May;141(5):1107-13.
6. Lanigan A., Spaw M., Donaghe C., Brennan J. The impact of the Veteran's Affairs Medical System on an otolaryngology residency training program. Mil Med 2018 Nov 1;183(11–12):e671-e675.
7. Ravin A.G., Gottlieb N.B., Wang H.T., et al: Effect of the Veterans Affairs Medical System on plastic surgery residency training. Plast Reconstr Surg. 2006; 117(2): 656–60
COLLEEN P. FLANAGAN is a second-year vascular surgery resident at the University of California, San Francisco. WARREN J. GASPER is a member of the VA Vascular Surgeons Committee.
LimFlow system a ‘cost-effective and high-value alternative’ to traditional therapies
Percutaneous deep vein arterialization (pDVA) with the LimFlow system offers a cost-effective and high-value alternative to traditional therapies or amputation, according to a recent study published in the Journal of Critical Limb Ischemia.
PETER SCHNEIDER, MD, PROFESSOR of surgery at the University of California San Francisco and co-author of the published article, said: “The costeffectiveness analysis builds on recently published 12-month data from the PROMISE I study by showing that pDVA with the LimFlow system can be a highvalue therapy alternative to the status quo for no-option chronic limb-threatening ischemia (CLTI) patients.
“This research highlights the health economic benefits of reducing amputations and the need to offer patients a better alternative worldwide.”
The findings highlighted significant and promising data from cost-effectiveness analysis comparing pDVA with the LimFlow system to the current treatment for no-option CLTI patients, according to the study authors.
The status quo was defined by a
meta-analysis conducted by the Yale Cardiovascular Research Group on nooption patient outcomes from other reputable studies ranging from 2006 to 2018, which is pending publication in the Journal of Critical Limb Ischemia
The comparative analysis demonstrates that expected outcome improvements with pDVA justify its incremental costs and qualifies it as a “high-value” therapy per established willingness-to-pay thresholds.
Dan Rose, CEO of LimFlow, added: “Avoiding major amputation is a key treatment goal in CLTI due to its associated high costs, loss of functional status and quality of life, and high mortality. The analysis using data from PROMISE I demonstrates our technology can provide significant clinical and healtheconomic value to patients and healthcare providers who are drastically underserved by the status quo.”—VS News

Go deep with Vein Global –Venous education to advance your skills

If you haven’t attended an International Vein Congress (IVC) meeting, you’ve missed out on some of the most exciting innovations in treating venous disease. The good news is that you can still get access to all the great content presented at the IVC meeting, plus a whole lot more.
Education
Abstract • Procedure Videos • Case Studies • Slide Presentations Research
Video Interviews • Literature • Premarket Testing • Regulatory and Finance Practice
Expert Opinion on Patient Care • Office Management • Profiles of Industry Partners
Vein Global is a resource dedicated to those that are committed to staying connected with not only current, but future trends in venous practice and patient care.
Make Vein Global your source for year-round venous education. Subscribe today.
VeinGlobal.com

2022 International Vein Congress
Stay tuned for more information!
IVCmiami.com

BY URMILA KERSLAKE
“There appears to be heightened risk of major amputation after use of paclitaxel-coated balloons [PCBs] in the peripheral arteries,” findings from a systematic review and meta-analysis of randomized controlled trials (RCTs) published in the European Journal of Vascular and Endovascular Surgery (EJVES) last month suggest. However, the authors clarify that the level of evidence is graded moderate, not high, due to scarce events in some studies.
FURTHERMORE, LEADING PHYSICIANS PROPOSE that the methodology used needs to be carefully considered and scrutinized before these conclusions are accepted.
Clarifying at the outset that he is not an expert on statistical methodology, globally recognized leader in the development of new, less-invasive procedures, Barry T. Katzen, MD, founder and medical director of Miami Cardiac & Vascular Institute and the president of the CLI Global Society, tells Vascular Specialist: “As a physician engaged in multidisciplinary limb salvage with a view to improving quality of life by preventing amputations and death due to critical limb ischemia, the conclusions from this meta-analysis are of concern, of course, and need to be taken seriously.
“However, I have, in parallel, questions about the complex methodologies used in this paper to arrive at a finding that prospective RCTs have not demonstrated. From a practical point of view, before accepting the conclusion regarding the risk of paclitaxel DCB [drugcoated balloon] use, there needs to be a significant discussion and analysis of the methodologies employed in this paper. This needs to be undertaken by appropriate statistical experts before these findings change practice, if they do so at all.”
This latest meta-analysis, authored by Konstantinos Katsanos, MD, of Patras University Hospital, Rion, Greece, and colleagues with co-authors from France, Germany, Finland and The Netherlands, drills down on the longterm risk of major amputation alone associated with use of PCBs in the lower limbs. The findings point to a significantly higher long-term risk of major limb loss using these devices in the femoropopliteal and/or infrapopliteal arteries.
Anna Maria Belli, MD, a former consultant radiologist and professor of interventional radiology at St. George’s Hospital and Medical School in London, England, a past president of the Cardiovascular and Interventional
87 41 2,216 1,544
Radiological Society of Europe (CIRSE) and proponent of evidence-based trials, comments: “It is essential that we have publications such as this interrogating data on new technologies in an unbiased way. There is a natural tendency to believe new technologies will provide better results than old ones. It is only by pooling results from published trials that enough numbers are amassed to detect trends that might be missed by individual trials. Katsanos and colleagues are to be commended for highlighting the increased risk of amputation with PCBs and, as they say, this now needs to be confirmed or refuted by further investigations.”
Commenting on the publication in EJVES, Younes Jahangiri, MD, statistical editor of the Journal of Vascular and Interventional Radiology (JVIR), says: “The manuscript has used a robust search strategy and meta-analysis techniques. Nevertheless, there are a considerable number of back-calculations and imputations that have been performed for data generation, which might not necessarily fit with real-world data. Additionally, exclusion of studies with no events in both arms, especially if the studies were of high quality and adequate follow-up, might have led to overestimation of the crude risk in both groups
“Although the meta-analysis itself suggests an alarming signal in a heavily computational way, confirmation of accuracy and adequacy of the signal would still require real-world targeted data” — Younes Jahangiri
Endologix announced the company’s ChEVAS (chimney endovascular aneurysm sealing) system has been granted a Breakthrough Device designation from the Food and Drug Administration (FDA).
CHEVAS IS CURRENTLY BEING evaluated through the ChEVAS ONE investigational device exemption (IDE) clinical study that is approved to enroll approximately 120 patients at up to 50
clinical sites worldwide. The national principal investigators of the ChEVAS ONE study are Francis Caputo, MD, of the Cleveland Clinic Foundation, Cleveland, Ohio; William Jordan, MD, of
and potentially to the statistical significance of betweengroup differences. Although the meta-analysis itself suggests an alarming signal in a heavily computational way, confirmation of accuracy and adequacy of the signal would still require real-world targeted data.”
87 major amputations in 2,216 limbs in the paclitaxel arm (4% crude risk)
The harm signals suggested for paclitaxel devices from previous meta-analyses have not been substantiated by a wealth of real-world datasets that have shown no long-term safety concerns, and instead suggested increased benefits with the use of paclitaxelcoated devices. Importantly, an interim mortality analysis of the SWEDEPAD registry did not confirm a heightened mortality risk in cases of paclitaxel treatment, as noted in the EJVES paper.
41 major amputations in 1,544 limbs in the control arm (2.7% crude risk)
As reported in EJVES, the investigators performed a literature search last updated on Feb. 20, 2021, to analyze 21 RCTs with 3,760 lower limbs treated nearly equally for intermittent claudication (52%) and chronic limb-threatening ischemia (CLTI; 48%).
The median follow-up period was two years. Authors report 87 major amputations in 2,216 limbs in the paclitaxel arm (4% crude risk) compared with 41 major amputations in the 1,544 limbs in the control arm (2.7% crude risk). The risk of major amputation was significantly higher for paclitaxel-coated balloons with a hazard ratio (HR) of 1.66 (95% CI 1.14–2.42; p=0.008, one-stage stratified Cox model). The observed amputation risk played out equally across femoropopliteal (p=0.055) and infrapopliteal (p=0.055) arteries. The number needed to harm was 35 for CLTI. In this systematic review and meta-analysis, the authors suggest the summary effect demonstrated a 66% higher relative risk of major amputation in the limbs treated with PCBs, and call for further investigations. Further, Katsanos and colleagues write that there was good evidence of a significant non-linear dose relationship with accelerated risk per cumulative paclitaxel dose (chi square model p=0.007). The results were also stable across sensitivity analyses (clarified as pertaining to different models and subgroups, based on anatomy and clinical indication, and excluding unpublished trials).
Ziv Haskal, MD, of the University of Virginia, Charlottesville, the former editor (2011–2020) of the JVIR tells Vascular Specialist: “Dr. Katsanos and the research team stand, again, to shake up the PCB planet with a suggested finding of worse amputation—the same goal paclitaxel was intended to make better, and with a dosedependent effect. Unsurprisingly, it is a rigorous and clearheaded analysis. But there are interpolations, intercalations and imputations, likely to bring out critics with force. This may be a curtain raiser, but the main play is yet to unfold.”
Emory University School of Medicine, Atlanta; Joseph Lombardi, MD, of Cooper University Health Care, Camden, New Jersey; and William Quinones-Baldrich, MD, of UCLA, Los Angeles.
“The aneurysm sac sealing technology featured in the ChEVAS system is designed to reduce endoleaks, including gutter endoleaks, that are reported after endovascular treatment of complex aneurysms,” said James
McKinsey, MD, of The Icahn School of Medicine at Mount Sinai, New York, the leading enroller in the ChEVAS ONE IDE study. “Our initial clinical results of this therapy have been promising in a challenging group of patients.” McKinsey will present his initial experience with ChEVAS at the Eastern Vascular Society Annual Meeting (Sept. 23–26; Charleston, South Carolina).—VS News
The ChEVAS system






Specialised source of news and education in the field of renal disease management
Breaking news, in-depth analysis, and leading opinion from key industry figures
Steered by globally-renowned physicians to monitor the latest innovations and controversies alike in the kidney care field
Industry updates and real-time event coverage via social media, videos and more on print and digital platforms
Visit www.renalinterventions.net and click ‘Subscriptions’ for complimentary print subscription* and e-newsletter subscription**
*Available for US and EU readers only **Available worldwide

While a surgeon’s expertise is key to patient outcomes, coding and documenting the procedures are key to the surgeon’s payment and reimbursement.
And, when it comes to billing and coding, a twist of an adage applies: What you don’t know can definitely hurt you financially.
One solution? Make plans today to attend the 2021 SVS Billing and Coding Reimbursement Workshop. This year’s iteration is set for Sunday and Monday, Dec. 5 and 6, at the OLC
Education and Conference Center in Rosemont, Illinois. The building is minutes from O’Hare International Airport and houses the Society for Vascular Surgery (SVS) headquarters office, located at 9400 W. Higgins Road, Suite 100.
The workshop kicks off with an optional workshop, “E&M (Evaluation and Management) Coding for Vascular Surgeons,” from 8 a.m. to 12 p.m. on Dec. 5. Faculty is Teri Romano, BSN, a coding and reimbursement specialist with KarenZupko & Associates and longtime SVS consultant for the Coding and Reimbursement Workshop.
The main workshop will be held from 1 to 5 p.m. Dec. 5, and from 7:30 a.m. to 4:15 p.m. Dec. 6. Romano will be joined by SVS members and longtime coding course faculty Sean P. Roddy, MD, Sunita Srivastava, MD, and Robert M. Zwolak, MD.
Registration will open in early September. For more information, visit vascular.org/Coding21.— Beth Bales
The Sixth Annual University of California Los Angeles (UCLA)-Society for Vascular Surgery (SVS) Symposium returns as a live course for 2021 from Oct. 1 to 3 at the Beverly Hilton in Beverly Hills, California.
The October dates are a change from the typical August timeframe. Registration is now open.
The three-day course, “A comprehensive review and update of what’s new in vascular and endovascular surgery,” offers an in-depth review of the specialty for those preparing to take the Vascular Surgery Board (VSB) examinations, as well as providing the basic didactic education for vascular residents and fellows in training.
The division of vascular and endovascular surgery at UCLA and the SVS offer the course jointly.— Beth Bales
More information—including the course description, faculty, agenda, objectives, accreditation and more—is available at vascular.org/Symposium21.
Apply for SVS Membership by Sept. 1: The third deadline of 2021 to apply for Society for Vascular Surgery (SVS) membership is Sept. 1.
Be a part of the premiere organization representing vascular surgeons and allied health professions, and reap the substantial benefits SVS offers.
These include discounts on meetings, the SVSConnect online community; camaraderie; the new Branding Toolkit and other practice tools; publications (including the Journal of Vascular Surgery, free for Active and Associate members, online access for International members and highly reduced rates for Affiliate and Senior members); mentorship and other career advancement efforts; research and other grants; advocacy in Washington, D.C., and more. Visit vascular.org/JoinSVS.
Claim CMEs by Sept. 24: The deadline for claiming Continuing Medical Education (CME) or Maintenance of Certification (MOC) self-assessment credits from the 2021 Vascular Annual Meeting (VAM) is Sept. 24.
The SVS designates this live course for 35.25 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation.
Full credit is not available for attendance at two sessions occurring simultaneously.
Multiple sessions also permit earning of MOC credits, with 16 available.
Those claiming credits must complete a course evaluation first. This feedback provides SVS with important information to help organizers of future annual meetings make programming decisions. The 2021 VAM Planner (vascular.org/Planner21) and mobile app both include a link to credits and certificates; this link will be live after the first plenary session on Aug. 18.—Beth Bales
The SVS Executive Board has approved the 2021–22 SVS Foundation Board appointments, as recommended by the Foundation Board.
MELINA KIBBE, MD, has been named the 17th dean of the University of Virginia School of Medicine and chief of the Health Affairs Office for UVA Health in Charlottesville, Virginia. She will start Sept. 15.
Kibbe is currently the Colin G. Thomas Jr. Distinguished Professor and chair of the Department of Surgery at the University of North Carolina at Chapel Hill, North Carolina.
JAMES BLACK, MD, and MUSSA, MD, received the “Hero with a Heart Award” in June from the Marfan Foundation, which works to save lives and improve the quality of life for individuals with Marfan syndrome.
Black is with Johns Hopkins Hospital and Mussa is with the Zucker School of Medicine at Northwell Health in New York. The two were the medical honorees for 2021.—Beth Bales
Continuing for an additional one-year term of office are Richard Lynn, MD, and William Shutze, MD, and joining the board for a three-year term is Ulka Sachdev-Ost, MD. Kim Hodgson, MD, has transitioned off the board in his role as the SVS Immediate Past President and Edith Tzeng, MD, has transitioned off in her role as the chair of the SVS Research Council.
Foundation Board of Directors:
Chair Peter F. Lawrence, MD, enters the second year of a three-year term. Other members of the SVS Foundation Board of Directors are: SVS President Ali AbuRahma, MD; Keith Calligaro, MD; Ronald L. Dalman, MD; Matthew Eagleton, MD; Joseph Hart, MD; Nasim Hedayati, MD; Raul Guzman, MD; Lynn; Sachdev-Ost; Shutze; Martin Sylvain, MBA; and James Neupert.

Sylvain and Neupert are the non-surgeon board members; this broadening and diversification of the board began in 2020 with the restructuring of the Foundation, explained Lawrence. The SVS thanks Tzeng and Hodgson for their service to the SVS Foundation.
SVS Foundation Development Committee: The SVS Foundation Development Committe is made up of Chair Peter Nelson, MD; Vice Chair Thomas L. Forbes, MD; Lawrence; and members Lisa Bennett, MD, Peter Brant-Zawadzki, MD, Luke Brewster, MD, Rocco Ciocca, MD, Ryan Nolte, MD, Tzeng, and Chandu Vemuri, MD.— Beth Bales

BY MADELINE DILLS, MD
In this month’s column for trainees: Taking to the podium for the first time

The COVID-19 pandemic left many of us missing social interaction and hungry for a change of scenery. As someone who had never been to a vascular surgery conference, I was already eagerly anticipating the Society for Clinical Vascular Surgery (SCVS) meeting in 2020 when it was canceled. Fortunately, the vaccine made the 2021 SCVS meeting possible and so my excitement and enthusiasm to attend were doubled. Though I wasn’t quite sure what to expect, any nervousness to present was quickly overcome by the prospect of spending time with my fellow trainees in Miami.
I HAVE NEVER BEEN ONE TO SHY away from public speaking, but as a second-year resident, the thought of a room full of attending surgeons was a little daunting. I watched as even my seemingly infallible chief residents were nervous to perform. After about 100 times practicing in front of the hotel mirror, and cautiously observing others’ presentation styles, my time at the podium arrived.
Once I took the stage, however, my nerves faded. The once daunting task of effectively and succinctly presenting my points morphed into a chance to discuss a topic near to my heart with a room of
people who were also passionate about the topic. My research focused on what attracts medical students to vascular surgery and how we can continue to
After about 100 times practicing in front of the hotel mirror, and cautiously observing others’ presentation styles, my time at the podium arrived
A pair of breakfast sessions aimed at medical students—and potential future vascular surgeons—will form part of the Vascular Annual Meeting (VAM) Aug. 19.
pique interest in a specialty that can be underrepresented in medical school curricula. As someone who passionately, although somewhat biasedly, believes we are in one of the best fields of medicine, I want more people to know about it. I also want to attract the best of the best amongst medical students. It was a huge resource to have an audience who are not only educated in the subject, but also share the same passions. At the conclusion of my presentation, I stepped away thankful that I had many brilliant surgical minds contributing to the discussion and offering new insight.
As a runner, I always prefer to run with someone else. Running with a partner challenges my competitive nature to push harder and faster. Having someone to talk with also takes my mind away from any physical pain. This concept that working alongside someone increases performance rang true as I attended sessions at SCVS. The interview trail was the first place I took note of the fact that vascular surgeons know each other well. This factor confirmed my career choice— and increased my fervor to match. Rewitnessing the interconnectedness at SCVS reminded me why vascular surgery is so special.
THE MEDICAL STUDENT PROGRAM
Breakfasts take place simultaneously from 6:30 to 8 a.m. (Pacific time), with one aimed at first- and second-year students (MS1–2), and the other at those in their third or fourth years (MS3–4).
The session targeting MS1–2 attendees focuses on providing an introduction to vascular surgery for those who have an interest in pursuing the specialty as a career. It features such topics as “Vascular Surgery 101,” “How vascular surgery differs from other specialties,” and “How to get more exposure to vascular surgery.”
The session for MS3–4 participants is designed for those medical students planning to apply for vascular surgery residency. It covers the application process
As researchers and surgeons, we can challenge one another to improve and increase the quality of patient care. As friends, we can support one another, which combats the evergrowing challenge of burnout. Complacency and inertia are a surgeon’s worst enemies. Attending the conference and listening to the work other vascular surgeons are conducting challenged me to ask more questions about my own clinical decisions. It pushed my mind to ask, “Where can we take this next?” All the while, I knew I was developing connections with individuals who could help me answer that question.
My final takeaway from attending a vascular scientific meeting is the importance of fostering these relationships in person. After a year of social distancing and virtual substitutes for education and meetings, we may ask why we should spend valuable time to travel to a meeting.
While the SCVS did an excellent job of accommodating the challenges of hosting a meeting during a pandemic when many individuals faced travel restrictions, the hybrid format did highlight the importance of physical presence. Being in the room at the same time as the presenter allowed for more meaningful discussions to take place.
We could bounce ideas off one another, and the entire group could participate. Obviously, in-person attendance also made it easier to meet new people and connect. One of the many reasons I chose our specialty is the type of person it attracts: hardworking, compassionate and smart. It is an honor to have my fellow vascular surgeons as colleagues. I will certainly leap at the opportunity to attend the next conference and continue to interact and bond with my peers.
MADELINE DILLS is a third-year integrated vascular surgery resident in the Louisiana State University (LSU) division of vascular surgery in New Orleans.
and how to successfully match. Both sessions will include leadership welcomes, with Society for Vascular Surgery (SVS) President-elect Michael C. Dalsing, MD, performing the address for MS1–2s, and outgoing President Ronald L. Dalman, MD, opening proceedings for MS3–4s.
The former session is being moderated by Cassius Iyad Ochoa Chaar, MD, from Yale University School of Medicine, New Haven, Connecticut, and Nii-Kabu Kabutey, MD, from the University of California Irvine, with the latter hosted by Benjamin Pearce, MD, from the University of Alabama at Birmingham, and Dawn Coleman, MD, from the University of Michigan Medical Center, Ann Arbor, Michigan.—Bryan Kay
BY BRYAN KAY
A new study aiming to establish whether a series of mindfulness and physical interventions can help reduce stress and burnout among physicians who treat highacuity patients has started recruitment at the University of Pittsburgh Medical Center (UPMC) in Pennsylvania.
Led by Rabih Chaer, MD, chief of vascular surgery at UPMC Presbyterian, the research is being conducted with grant funding from the UPMC Physician THRIVE program, and is double-pronged. One cohort of participants will be made up of practitioners from specialties working with high-acuity patients— the likes of vascular surgeons, cardiac surgeons and cardiologists. The other is comprised of providers who care for those who have contracted COVID-19, including nurses. Chaer has personal experience of the effects of burnout, recently telling Pitt Med, a quarterly publication of the University of Pittsburgh, how running had helped him overcome its ravages and how he had been prompted to look for ways to help colleagues. In a recent interview
INDICATIONS FOR USE
with Vascular Specialist, he explained that the genesis of the study was rooted in establishing road-tested methods providers could use to alleviate stress. “For physicians who deal with complex patients, with high-acuity patients, there is a stressful component to the job,” he says. “Parts of this are the stress of the complex situations, so more of a mental stress. And other parts are physical stress, either because you are wearing loupes, your neck is bent, you are wearing a lead apron, or because cases can be long.”
The interventions being tested cover emotional, mental and physical stressors. Questionnaires will be disseminated, but the research team will also objectively measure stress by collecting samples of hair to measure cortisol levels. “Hair cortisol level is a marker of chronic stress, meaning we will have to wait about three months or so before we test it in order to see a difference,” explains Chaer.
The first intervention involves mindfulness, with routines centered on providing short breathing and selfawareness exercises that can be carried out between patients or cases. Physical interventions focus on the neck and upper shoulders, and the lower back—the areas typically affected through the use of lead aprons and loupes. They involve short yoga-like exercises put to video that providers can use to incorporate into their schedule. Experts from the fields of psychology, exercise and physical therapy helped develop the interventions.
“The eventual goal is that if this pans out to be useful, and the people who take part are compliant—we will be seeking their feedback to see if they like it—then maybe this can become part of an institutional protocol that can be made available to everyone. We can say, ‘We tested this, it works, you might want to consider it.’ It can potentially be endorsed by the institution as an intervention that can reduce stress and improve wellness.”
Chaer and colleagues expect tangible findings from the study to be available in about six months.
The IN.PACT™ AV Paclitaxel-coated PTA Balloon Catheter is indicated for percutaneous transluminal angioplasty, after appropriate vessel preparation, for the treatment of obstructive lesions up to 100 mm in length in the native arteriovenous dialysis fistulae with reference vessel diameters of 4 to 12 mm.
CONTRAINDICATIONS
The IN.PACT AV DCB is contraindicated for use in the following anatomy and patient types:
Coronary arteries, renal arteries, and supra-aortic/cerebrovascular arteries
Patients who cannot receive recommended antiplatelet and/or anticoagulant therapy
Patients judged to have a lesion that prevents complete inflation of an angioplasty balloon or proper placement of the delivery system
Patients with known allergies or sensitivities to paclitaxel
Women who are breastfeeding, pregnant, or are intending to become pregnant, or men intending to father children.
It is unknown whether paclitaxel will be excreted in human milk and whether there is a potential for adverse reaction in nursing infants from paclitaxel exposure
WARNINGS
A signal for increased risk of late mortality has been identified following the use of paclitaxel-coated balloons and paclitaxel-eluting stents for femoropopliteal arterial disease beginning approximately 2-3 years post-treatment compared with the use of non-drug coated devices. There is uncertainty regarding the magnitude and mechanism for the increased late mortality risk, including the impact of repeat paclitaxel-coated device exposure. Inadequate information is available to evaluate the potential mortality risk associated with the use of paclitaxel-coated devices for the treatment of other diseases/conditions, including this device indicated for use in arteriovenous dialysis fistulae. Physicians should discuss this late mortality signal and the benefits and risks of available treatment options for their specific disease/condition with their patients.
Use the product prior to the Use-by date specified on the package.
Contents are supplied sterile. Do not use the product if the inner packaging is damaged or opened.
Do not use air or any gaseous medium to inflate the balloon. Use only the recommended inflation medium (equal parts contrast medium and saline solution).
Do not move the guidewire during inflation of the IN.PACT AV DCB.
Do not exceed the rated burst pressure (RBP). The RBP is based on the results of in vitro testing. Use of pressures higher than RBP may result in a ruptured balloon with possible intimal damage and dissection.
The safety of using multiple IN.PACT AV DCBs with a total drug dosage exceeding 15,105 μg paclitaxel has not been evaluated clinically.
PRECAUTIONS
This product should only be used by physicians trained in percutaneous transluminal angioplasty (PTA).
Assess risks and benefits before treating patients with a history of severe reaction to contrast agents. Identify allergic reactions to contrast media and antiplatelet therapy before treatment and consider alternatives for appropriate management prior to the procedure.
medtronic.com/avDCB
UC202104335a EN ©2020 Medtronic. All Rights Reserved. Medtronic, Medtronic logo, and Further, Together are trademarks of Medtronic. All other brands are trademarks of a Medtronic company. For distribution in the USA only. 09/2020

“The idea is to have a short enough intervention for physicians to be able to carry them out in a short amount of time—between patients or between cases” —Rabih Chaer
This product is not intended for the expansion or delivery of a stent.
Do not use the IN.PACT AV DCB for pre-dilatation or for post-dilatation.
This product is designed for single patient use only. Do not reuse, reprocess, or resterilize this product. Reuse, reprocessing, or resterilization may compromise the structural integrity of the device and/or create a risk of contamination of the device, which could result in patient injury, illness, or death.
The use of this product carries the risks associated with percutaneous transluminal angioplasty, including thrombosis, vascular complications, and/or bleeding events
The safety and effectiveness of the IN.PACT AV DCB used in conjunction with other drug-eluting stents or drug-coated balloons in the same procedure has not been evaluated.
The extent of the patient’s exposure to the drug coating is directly related to the number of balloons used. Refer to the Instructions for Use (IFU) for details regarding the use of multiple balloons and paclitaxel content. Appropriate vessel preparation, as determined by the physician to achieve residual stenosis of ≤ 30%, is required prior to use of the IN.PACT AV DCB. Vessel preparation of the target lesion using high-pressure PTA for pre-dilatation was studied in the IN.PACT AV Access clinical study. Other methods of vessel preparation, such as atherectomy, have not been studied clinically with IN.PACT AV DCB.
POTENTIAL ADVERSE EFFECTS
Potential adverse effects which may be associated with balloon catheterization may include, but are not limited to, the following: abrupt vessel closure, allergic reaction, arrhythmias, arterial or venous aneurysm, arterial or venous thrombosis, death, dissection, embolization, hematoma, hemorrhage, hypotension/hypertension, infection, ischemia or infarction of tissue/organ, loss of permanent access, pain, perforation or rupture of the artery or vein, pseudoaneurysm, restenosis of the dilated vessel, shock, stroke, vessel spasms or recoil.
Potential complications of peripheral balloon catheterization include, but are not limited to, the following: balloon rupture, detachment of a component of the balloon and/or catheter system, failure of the balloon to perform as intended, failure to cross the lesion. These complications may result in adverse effects.
Although systemic effects are not anticipated, potential adverse effects not captured above that may be unique to the paclitaxel drug coating include, but are not limited to, the following: allergic/immunologic reaction, alopecia, anemia, gastrointestinal symptoms, hematologic dyscrasia (including leucopenia, neutropenia, thrombocytopenia), hepatic enzyme changes, histologic changes in vessel wall, including inflammation, cellular damage, or necrosis, myalgia/arthralgia, myelosuppression, peripheral neuropathy.
Refer to the Physicians’ Desk Reference for more information on the potential adverse effects observed with paclitaxel. There may be other potential adverse effects that are unforeseen at this time.
Please reference appropriate product Instructions for Use for a detailed list of indications, warnings, precautions and potential adverse effects. This content is available electronically at www.manuals.medtronic.com.
CAUTION Federal law (USA) restricts this device to sale by or on the order of a physician.
56% FEWER REINTERVENTIONS THAN PTA1 ACCESS CIRCUIT PRIMARY PATENCY *1 TARGET LESION PRIMARY PATENCY*1 78% 86%
LEARN MORE: medtronic.com/avDCB
*The largest global, randomized, AV fistula drug-coated balloon study conducted, with subjects from Japan, New Zealand, and the United States.
†In an AV DCB study.
1 Lookstein RA, et al. Drug-Coated Balloons for Dysfunctional Dialysis Arteriovenous Fistulas. N Engl J Med. 2020;383:733-42. DOI: 10.1056/ NEJMoa1914617. Highlighted results reported at both 180 and 210 days.
IN.PACT AV DCB can reduce the need for AV fistula reinterventions. This could help enable longer periods of uninterrupted dialysis, and positively impact patients’ lives. The unmatched results are produced by a unique drug dose and formulation only found in the IN.PACT AV DCB.1