SVS is working to effect change in the 2019 CMS Medicare fee schedule rules.
Tracking 90day vascular surgery outcomes: The coming new normal?
BY MARK S. LESNEY MDEDGE NEWS FROM SURGERY
The Centers for Medicare & Medicaid Services is test driving a new quality measurement model that pushes hospital readmissions measures out from 30 to 90 days.
Previous research has identified vascular surgery as having twice as high rates of 90-day readmissions, compared with 30-day readmissions (Am J Manag Care. 2014;20[9]:e432-e438), and this could prove problematic in light of the CMS pilot project currently underway, according to Donald E. Fry, MD, of MPA Healthcare Solutions,
16
Physician burnout impacts patients negatively as well.
Vascular programs without NIVL curriculum leave trainees wanting
Dr. Daisy Chou
BY KARI OAKES MDEDGE NEWS REPORTING FROM MIDWESTERN VASCULAR 2018
ST. LOUIS – Many vascular surgery trainees felt unprepared to take the Registered Physician in Vascular Interpretation (RPVI) exam, according to a recent survey. However, trainees in a program without a structured noninvasive vascular laboratory (NIVL) curriculum felt particularly unprepared, said Daisy Chou, MD.
“There is wide variation in NIVL experience amongst
vascular surgery training programs,” noted Dr. Chou, a vascular surgery fellow at the Ohio State University, Columbus. She presented survey results at the annual meeting of the Midwestern Vascular Surgical Society. The survey constructed by Dr. Chou and her colleagues went out to trainees in both 0+5 and 5+2 vascular surgery training programs in September 2017, in 114 unique programs.
Eventually, trainees from just over half of the programs responded (n = 61 programs, 53.5%), said Dr.
Trainees · page 7
Vascular Nurses Get SVS Affiliate Member Discount
Vascular Nurses Week was Sept. 9-15. SVS is inviting Society for Vascular Nursing members to join the SVS as affiliate members. Applicants will receive a 50% discount through Dec. 1. Email CVs and the completed membership form (available at https://vascular.org) to membership@vascularsociety.org
Continued on page 7
For appropriate patients with DVT/PE
Choose ELIQUIS from the START
DVT: deep vein thrombosis; PE: pulmonary embolism.
INDICATIONS
ELIQUIS is indicated for the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and to reduce the risk of recurrent DVT and PE following initial therapy.
IMPORTANT SAFETY INFORMATION
WARNING: (A) PREMATURE DISCONTINUATION OF ELIQUIS INCREASES THE RISK OF THROMBOTIC EVENTS, (B)SPINAL/EPIDURAL HEMATOMA
(A)Premature discontinuation of any oral anticoagulant, including ELIQUIS, increases the risk of thrombotic events. If anticoagulation with ELIQUIS is discontinued for a reason other than pathological bleeding or completion of a course of therapy, consider coverage with another anticoagulant.
(B)Epidural or spinal hematomas may occur in patients treated with ELIQUIS who are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis. Consider these risks when scheduling patients for spinal procedures. Factors that can increase the risk of developing epidural or spinal hematomas in these patients include:
CONTRAINDICATIONS
• use of indwelling epidural catheters
• concomitant use of other drugs that affect hemostasis, such as nonsteroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors, other anticoagulants
• a history of traumatic or repeated epidural or spinal punctures
• a history of spinal deformity or spinal surgery
• optimal timing between the administration of ELIQUIS and neuraxial procedures is not known
• Active pathological bleeding
• Severe hypersensitivity reaction to ELIQUIS (e.g., anaphylactic reactions)
WARNINGS AND PRECAUTIONS
• Increased Risk of Thrombotic Events after Premature Discontinuation: Premature discontinuation of any oral anticoagulant, including ELIQUIS, in the absence of adequate alternative anticoagulation increases the risk of thrombotic events. An increased rate of stroke was observed during the transition from ELIQUIS to warfarin in clinical trials in atrial fibrillation patients. If ELIQUIS is discontinued for a reason other than pathological bleeding or completion of a course of therapy, consider coverage with another anticoagulant.
• Bleeding Risk: ELIQUIS increases the risk of bleeding and can cause serious, potentially fatal, bleeding.
Monitor patients frequently for signs and symptoms of neurological impairment. If neurological compromise is noted, urgent treatment is necessary.
Consider the benefits and risks before neuraxial intervention in patients anticoagulated or to be anticoagulated.
– Concomitant use of drugs affecting hemostasis increases the risk of bleeding, including aspirin and other antiplatelet agents, other anticoagulants, heparin, thrombolytic agents, SSRIs, SNRIs, and NSAIDs.
– Advise patients of signs and symptoms of blood loss and to report them immediately or go to an emergency room. Discontinue ELIQUIS in patients with active pathological hemorrhage.
– The anticoagulant effect of apixaban can be expected to persist for at least 24 hours after the last dose (i.e., about two half-lives). An agent to reverse the anti-factor Xa activity of apixaban is available. Please visit www.andexxa.com for more information on availability of a reversal agent.
• Spinal/Epidural Anesthesia or Puncture: Patients treated with ELIQUIS undergoing spinal/epidural anesthesia or puncture may develop an epidural or spinal hematoma which can result in long-term or permanent paralysis. The risk of these events may be increased by the postoperative use of indwelling epidural catheters or the concomitant use of medicinal products affecting hemostasis. Indwelling epidural or intrathecal catheters should not be removed earlier than 24 hours after the last administration of ELIQUIS.
ELIQUIS for initial DVT/PE treatment*—
And for appropriate patients, continue on a low dose† to reduce the risk of recurrent DVT/PE following initial therapy1
*Initial therapy: 10 mg, orally twice daily for the first 7 days. After 7 days, 5 mg orally twice daily.
† Extended therapy: 2.5 mg, orally twice daily. Please see full dosing information in the Prescribing Information.
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
WARNINGS AND PRECAUTIONS (cont’d)
The next dose of ELIQUIS should not be administered earlier than 5 hours after the removal of the catheter. The risk may also be increased by traumatic or repeated epidural or spinal puncture. If traumatic puncture occurs, delay the administration of ELIQUIS for 48 hours. Monitor patients frequently and if neurological compromise is noted, urgent diagnosis and treatment is necessary. Physicians should consider the potential benefit versus the risk of neuraxial intervention in ELIQUIS patients.
DRUG INTERACTIONS
• Prosthetic Heart Valves: The safety and efficacy of ELIQUIS have not been studied in patients with prosthetic heart valves and is not recommended in these patients.
• Acute PE in Hemodynamically Unstable Patients or Patients who Require Thrombolysis or Pulmonary Embolectomy: Initiation of ELIQUIS is not recommended as an alternative to unfractionated heparin for the initial treatment of patients with PE who present with hemodynamic instability or who may receive thrombolysis or pulmonary embolectomy.
ADVERSE REACTIONS
• The most common and most serious adverse reactions reported with ELIQUIS were related to bleeding.
TEMPORARY INTERRUPTION FOR SURGERY AND OTHER INTERVENTIONS
• ELIQUIS should be discontinued at least 48 hours prior to elective surgery or invasive procedures with a moderate or high risk of unacceptable or clinically significant bleeding. ELIQUIS should be discontinued at least 24 hours prior to elective surgery or invasive procedures with a low risk of bleeding or where the bleeding would be noncritical in location and easily controlled. Bridging anticoagulation during the 24 to 48 hours after stopping ELIQUIS and prior to the intervention is not generally required. ELIQUIS should be restarted after the surgical or other procedures as soon as adequate hemostasis has been established.
Clarithromycin
• Inhibitors
Combined P-gp and Strong CYP3A4 Inhibitors: of P-glycoprotein (P-gp) and cytochrome P450 3A4 (CYP3A4) increase exposure to apixaban and increase the risk of bleeding. For patients receiving ELIQUIS doses of 5 mg or 10 mg twice daily, reduce the dose of ELIQUIS by 50% when ELIQUIS is coadministered with drugs that are combined P-gp and strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, or ritonavir). In patients already taking 2.5 mg twice daily, avoid coadministration of ELIQUIS with combined P-gp and strong CYP3A4 inhibitors.
Although clarithromycin is a combined P-gp and strong CYP3A4 inhibitor, pharmacokinetic data suggest that no dose adjustment is necessary with concomitant administration with ELIQUIS.
• Combined P-gp and Strong CYP3A4 Inducers: Avoid concomitant use of ELIQUIS with combined P-gp and strong CYP3A4 inducers (e.g., rifampin, carbamazepine, phenytoin, St. John’s wort) because such drugs will decrease exposure to apixaban.
• Anticoagulants and Antiplatelet Agents: Coadministration of antiplatelet agents, fibrinolytics, heparin, aspirin, and chronic NSAID use increases the risk of bleeding. APPRAISE-2, a placebo-controlled clinical trial of apixaban in high-risk post-acute coronary syndrome patients treated with aspirin or the combination of aspirin and clopidogrel, was terminated early due to a higher rate of bleeding with apixaban compared to placebo.
PREGNANCY CATEGORY B
• There are no adequate and well-controlled studies of ELIQUIS in pregnant women. Treatment is likely to increase the risk of hemorrhage during pregnancy and delivery. ELIQUIS should be used during pregnancy only if the potential benefit outweighs the potential risk to the mother and fetus.
Reference: 1. ELIQUIS® Package Insert. Bristol-Myers Squibb Company, Princeton, NJ, and Pfizer Inc, New York, NY.
Please see Brief Summary of Full Prescribing Information, including Boxed WARNINGS, on adjacent pages.
ELIQUIS® (apixaban) tablets, for oral use
Brief Summary of Prescribing Information. For complete prescribing information consult official package insert.
WARNING: (A) PREMATURE DISCONTINUATION OF ELIQUIS INCREASES THE RISK OF THROMBOTIC EVENTS (B) SPINAL/EPIDURAL HEMATOMA
(A) PREMATURE DISCONTINUATION OF ELIQUIS INCREASES THE RISK OF THROMBOTIC EVENTS
Premature discontinuation of any oral anticoagulant, including ELIQUIS, increases the risk of thrombotic events. If anticoagulation with ELIQUIS is discontinued for a reason other than pathological bleeding or completion of a course of therapy, consider coverage with another anticoagulant [see Dosage and Administration, Warnings and Precautions, and Clinical Studies (14.1) in full Prescribing Information]
(B) SPINAL/EPIDURAL HEMATOMA
Epidural or spinal hematomas may occur in patients treated with ELIQUIS who are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis. Consider these risks when scheduling patients for spinal procedures. Factors that can increase the risk of developing epidural or spinal hematomas in these patients include:
• use of indwelling epidural catheters
• concomitant use of other drugs that affect hemostasis, such as nonsteroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors, other anticoagulants
• a history of traumatic or repeated epidural or spinal punctures
• a history of spinal deformity or spinal surgery
• optimal timing between the administration of ELIQUIS and neuraxial procedures is not known [see Warnings and Precautions]
Monitor patients frequently for signs and symptoms of neurological impairment. If neurological compromise is noted, urgent treatment is necessary [see Warnings and Precautions].
Consider the benefits and risks before neuraxial intervention in patients anticoagulated or to be anticoagulated [see Warnings and Precautions].
INDICATIONS AND USAGE
Reduction of Risk of Stroke and Systemic Embolism in Nonvalvular Atrial Fibrillation— ELIQUIS® (apixaban) is indicated to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation.
Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery— ELIQUIS is indicated for the prophylaxis of deep vein thrombosis (DVT), which may lead to pulmonary embolism (PE), in patients who have undergone hip or knee replacement surgery.
Treatment of Deep Vein Thrombosis—ELIQUIS is indicated for the treatment of DVT.
Treatment of Pulmonary Embolism—ELIQUIS is indicated for the treatment of PE.
Reduction in the Risk of Recurrence of DVT and PE—ELIQUIS is indicated to reduce the risk of recurrent DVT and PE following initial therapy.
DOSAGE AND ADMINISTRATION (Selected information)
Temporary Interruption for Surgery and Other Interventions
ELIQUIS should be discontinued at least 48 hours prior to elective surgery or invasive procedures with a moderate or high risk of unacceptable or clinically significant bleeding [see Warnings and Precautions]. ELIQUIS should be discontinued at least 24 hours prior to elective surgery or invasive procedures with a low risk of bleeding or where the bleeding would be non-critical in location and easily controlled. Bridging anticoagulation during the 24 to 48 hours after stopping ELIQUIS and prior to the intervention is not generally required. ELIQUIS should be restarted after the surgical or other procedures as soon as adequate hemostasis has been established. (For complete Dosage and Administration section, see full Prescribing Information.)
CONTRAINDICATIONS
ELIQUIS is contraindicated in patients with the following conditions:
• Active pathological bleeding [see Warnings and Precautions and Adverse Reactions]
• Severe hypersensitivity reaction to ELIQUIS (e.g., anaphylactic reactions) [see Adverse Reactions]
WARNINGS AND PRECAUTIONS
Increased Risk of Thrombotic Events after Premature Discontinuation
Premature discontinuation of any oral anticoagulant, including ELIQUIS, in the absence of adequate alternative anticoagulation increases the risk of thrombotic events. An increased rate of stroke was observed during the transition from ELIQUIS to warfarin in clinical trials in atrial fibrillation patients. If ELIQUIS is discontinued for a reason other than pathological bleeding or completion of a course of therapy, consider coverage with another anticoagulant [see Dosage and Administration (2.4) and Clinical Studies (14.1) in full Prescribing Information].
Bleeding
ELIQUIS increases the risk of bleeding and can cause serious, potentially fatal, bleeding [see Dosage and Administration (2.1) in full Prescribing Information and Adverse Reactions].
Concomitant use of drugs affecting hemostasis increases the risk of bleeding. These include aspirin and other antiplatelet agents, other anticoagulants, heparin, thrombolytic agents, selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, and nonsteroidal anti-inflammatory drugs (NSAIDs) [see Drug Interactions]
Advise patients of signs and symptoms of blood loss and to report them immediately or go to an emergency room. Discontinue ELIQUIS in patients with active pathological hemorrhage. Reversal ofAnticoagulant Effect
An agent to reverse the anti-factor Xa activity of apixaban is available. The pharmacodynamic effect of ELIQUIS can be expected to persist for at least 24 hours after the last dose, i.e., for about two drug half-lives. Prothrombin complex concentrate (PCC), activated prothrombin complex concentrate or recombinant factor VIIa may be considered, but have not been evaluated in clinical studies [see Clinical Pharmacology (12.2) in full Prescribing Information] When PCCs are used, monitoring for the anticoagulation effect of apixaban using a clotting test (PT, INR, or aPTT) or anti-factor Xa (FXa) activity is not useful and is not recommended. Activated oral charcoal reduces absorption of apixaban, thereby lowering apixaban plasma concentration [see Overdosage]
Hemodialysis does not appear to have a substantial impact on apixaban exposure [see Clinical Pharmacology (12.3) in full Prescribing Information]. Protamine sulfate and vitamin K are not expected to affect the anticoagulant activity of apixaban. There is no experience with antifibrinolytic agents (tranexamic acid, aminocaproic acid) in individuals receiving apixaban. There is no experience with systemic hemostatics (desmopressin and aprotinin) in individuals receiving apixaban, and they are not expected to be effective as a reversal agent.
Spinal/Epidural Anesthesia or Puncture
When neuraxial anesthesia (spinal/epidural anesthesia) or spinal/epidural puncture is employed, patients treated with antithrombotic agents for prevention of thromboembolic complications are at risk of developing an epidural or spinal hematoma which can result in long-term or permanent paralysis.
The risk of these events may be increased by the postoperative use of indwelling epidural catheters or the concomitant use of medicinal products affecting hemostasis.Indwelling epidural or intrathecal catheters should not be removed earlier than 24 hours after the last administration of ELIQUIS. The next dose of ELIQUIS should not be administered earlier than 5 hours after the removal of the catheter. The risk may also be increased by traumatic or repeated epidural or spinal puncture. If traumatic puncture occurs, delay the administration of ELIQUIS for 48 hours. Monitor patients frequently for signs and symptoms of neurological impairment (e.g., numbness or weakness of the legs, or bowel or bladder dysfunction). If neurological compromise is noted, urgent diagnosis and treatment is necessary.Prior to neuraxial intervention the physician should consider the potential benefit versus the risk in anticoagulated patients or in patients to be anticoagulated for thromboprophylaxis.
Patients with Prosthetic Heart Valves
The safety and efficacy of ELIQUIS (apixaban) have not been studied in patients with prosthetic heart valves.Therefore, use of ELIQUIS is not recommended in these patients.
Acute PE in Hemodynamically Unstable Patients or Patients who Require Thrombolysis or Pulmonary Embolectomy
Initiation of ELIQUIS is not recommended as an alternative to unfractionated heparin for the initial treatment of patients with PE who present with hemodynamic instability or who may receive thrombolysis or pulmonary embolectomy.
ADVERSE REACTIONS
The following serious adverse reactions are discussed in greater detail in other sections of the prescribing information.
• Increased risk of thrombotic events after premature discontinuation [see Warnings and Precautions]
• Bleeding [see Warnings and Precautions]
• Spinal/epidural anesthesia or puncture [see Warnings and Precautions]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Reduction of Risk of Stroke and Systemic Embolism in Patients with Nonvalvular Atrial Fibrillation
The safety of ELIQUIS was evaluated in the ARISTOTLE and AVERROES studies [see Clinical Studies (14) in full Prescribing Information], including 11,284 patients exposed to ELIQUIS 5 mg twice daily and 602 patients exposed to ELIQUIS 2.5 mg twice daily. The duration of ELIQUIS exposure was ≥12 months for 9375 patients and ≥24 months for 3369 patients in the two studies.InARISTOTLE,the mean duration of exposure was 89 weeks (>15,000 patient-years).In AVERROES, the mean duration of exposure was approximately 59 weeks (>3000 patient-years). The most common reason for treatment discontinuation in both studies was for bleedingrelated adverse reactions; in ARISTOTLE this occurred in 1.7% and 2.5% of patients treated with ELIQUIS and warfarin, respectively, and in AVERROES, in 1.5% and 1.3% on ELIQUIS and aspirin, respectively.
Bleeding in Patients with Nonvalvular Atrial Fibrillation in ARISTOTLE and AVERROES
Tables 1 and 2 show the number of patients experiencing major bleeding during the treatment period and the bleeding rate (percentage of subjects with at least one bleeding event per 100 patient-years) in ARISTOTLE and AVERROES.
Table 1: Bleeding Events in Patients with Nonvalvular Atrial Fibrillation in ARISTOTLE* ELIQUIS N=9088 n (per
In ARISTOTLE, the results for major bleeding were generally consistent across most major subgroups including age, weight, CHADS2 score (a scale from 0 to 6 used to estimate risk of stroke, with higher scores predicting greater risk), prior warfarin use, geographic region, and aspirin use at randomization (Figure 1). Subjects treated with apixaban with diabetes bled more (3.0% per year) than did subjects without diabetes (1.9% per year).
Table 2: Bleeding Events in Patients with Nonvalvular Atrial Fibrillation in AVERROES ELIQUIS (apixaban) N=2798
Events associated with each endpoint were counted once per subject, but subjects may have contributed events to multiple endpoints.
Other Adverse Reactions
Hypersensitivity reactions (including drug hypersensitivity, such as skin rash, and anaphylactic reactions, such as allergic edema) and syncope were reported in <1% of patients receiving ELIQUIS.
Prophylaxis of DeepVeinThrombosis Following Hip or Knee Replacement Surgery
The safety of ELIQUIS has been evaluated in 1 Phase II and 3 Phase III studies including 5924 patients exposed to ELIQUIS 2.5 mg twice daily undergoing major orthopedic surgery of the lower limbs (elective hip replacement or elective knee replacement) treated for up to 38 days. In total, 11% of the patients treated with ELIQUIS 2.5 mg twice daily experienced adverse reactions.
Bleeding results during the treatment period in the Phase III studies are shown in Table 3. Bleeding was assessed in each study beginning with the first dose of double-blind study drug. Table 3: Bleeding During the Treatment Period in Patients Undergoing Elective Hip or Knee Replacement Surgery
Bleeding Endpoint*
* Bleeding events within each subcategory were counted once per subject, but subjects may have contributed events to multiple endpoints. Bleeding events were counted during treatment or within 2 days of stopping study treatment (on-treatment period).
† Defined as clinically overt bleeding accompanied by one or more of the following: a decrease in hemoglobin of ≥2 g/dL, a transfusion of 2 or more units of packed red blood cells, bleeding at a critical site: intracranial, intraspinal, intraocular, pericardial, intra-articular, intramuscular with compartment syndrome, retroperitoneal or with fatal outcome.
‡ Intracranial bleed includes intracerebral, intraventricular, subdural, and subarachnoid bleeding. Any type of hemorrhagic stroke was adjudicated and counted as an intracranial major bleed.
§ On-treatment analysis based on the safety population, compared to ITT analysis presented in Section 14.
¶ GI bleed includes upper GI, lower GI, and rectal bleeding.
** Fatal bleeding is an adjudicated death with the primary cause of death as intracranial bleeding or non-intracranial bleeding during the on-treatment period.
* All bleeding criteria included surgical site bleeding.
† Includes 13 subjects with major bleeding events that occurred before the first dose of apixaban (administered 12 to 24 hours post-surgery).
‡ Includes 5 subjects with major bleeding events that occurred before the first dose of apixaban (administered 12 to 24 hours post-surgery).
§ Intracranial, intraspinal, intraocular, pericardial, an operated joint requiring re-operation or intervention, intramuscular with compartment syndrome, or retroperitoneal. Bleeding into an operated joint requiring re-operation or intervention was present in all patients with this category of bleeding. Events and event rates include one enoxaparin-treated patient in ADVANCE-1 who also had intracranial hemorrhage.
Figure 1: Major Bleeding Hazard Ratios by Baseline Characteristics – ARISTOTLE Study Apixaban Better Warfarin Better
Adverse reactions occurring in ≥1% of patients undergoing hip or knee replacement surgery in the 1 Phase II study and the 3 Phase III studies are listed inTable 4.
Table 4: Adverse Reactions Occurring in ≥1% of Patients in Either Group
Undergoing Hip or Knee Replacement Surgery
ELIQUIS (apixaban), n (%) 2.5 mg po bid N=5924 Enoxaparin, n (%) 40 mg sc qd or 30 mg sc q12h N=5904
Nausea 153 (2.6) 159 (2.7)
Anemia (including postoperative and hemorrhagic anemia, and respective laboratory parameters)
Contusion
Hemorrhage (including hematoma, and vaginal and urethral hemorrhage)
Treatment of DVT and PE and Reduction in the Risk of Recurrence of DVT or PE
The safety of ELIQUIS has been evaluated in the AMPLIFY and AMPLIFY-EXT studies, including 2676 patients exposed to ELIQUIS 10 mg twice daily, 3359 patients exposed to ELIQUIS 5 mg twice daily,and 840 patients exposed to ELIQUIS 2.5 mg twice daily.
Common adverse reactions (≥1%) were gingival bleeding, epistaxis, contusion, hematuria, rectal hemorrhage,hematoma,menorrhagia,and hemoptysis.
AMPLIFY Study
The mean duration of exposure to ELIQUIS was 154 days and to enoxaparin/warfarin was 152 days in the AMPLIFY study. Adverse reactions related to bleeding occurred in 417 (15.6%) ELIQUIS-treated patients compared to 661 (24.6%) enoxaparin/warfarin-treated patients. The discontinuation rate due to bleeding events was 0.7% in the ELIQUIS-treated patients compared to 1.7% in enoxaparin/warfarin-treated patients in theAMPLIFY study.
In the AMPLIFY study, ELIQUIS was statistically superior to enoxaparin/warfarin in the primary safety endpoint of major bleeding (relative risk 0.31,95% CI [0.17,0.55],P-value <0.0001).
Bleeding results from theAMPLIFY study are summarized inTable 5.
Table 5: Bleeding Results in the AMPLIFY Study
ELIQUIS N=2676 n (%)
Enoxaparin/Warfarin N=2689 n (%) Relative Risk (95% CI)
Major 15 (0.6) 49 (1.8) 0.31 (0.17, 0.55) p<0.0001
CRNM* 103 (3.9) 215 (8.0)
Major + CRNM 115 (4.3) 261 (9.7)
Minor 313 (11.7) 505 (18.8)
All 402 (15.0) 676 (25.1)
* CRNM = clinically relevant nonmajor bleeding.
Events associated with each endpoint were counted once per subject, but subjects may have contributed events to multiple endpoints.
Adverse reactions occurring in ≥1% of patients in theAMPLIFY study are listed inTable 6.
Table 6: Adverse Reactions Occurring in ≥1% of Patients Treated for DVT and PE in the AMPLIFY Study
ELIQUIS N=2676 n (%)
Enoxaparin/Warfarin N=2689 n (%)
Epistaxis 77 (2.9) 146 (5.4)
Contusion 49 (1.8) 97 (3.6)
Hematuria 46 (1.7) 102 (3.8)
Menorrhagia 38 (1.4) 30 (1.1)
Hematoma 35 (1.3) 76 (2.8)
Hemoptysis 32 (1.2) 31 (1.2)
Rectal hemorrhage 26 (1.0) 39 (1.5)
Gingival bleeding 26 (1.0) 50 (1.9)
AMPLIFY-EXT Study
The mean duration of exposure to ELIQUIS was approximately 330 days and to placebo was 312 days in the AMPLIFY-EXT study. Adverse reactions related to bleeding occurred in 219 (13.3%) ELIQUIS-treated patients compared to 72 (8.7%) placebo-treated patients. The discontinuation rate due to bleeding events was approximately 1% in the ELIQUIS-treated patients compared to 0.4% in those patients in the placebo group in theAMPLIFY-EXT study.
Bleeding results from theAMPLIFY-EXT study are summarized inTable 7.
OtherAdverse Reactions
Less common adverse reactions in ELIQUIS-treated patients in the AMPLIFY or AMPLIFY-EXT
studies occurring at a frequency of ≥0.1% to <1%:
Blood and lymphatic system disorders: hemorrhagic anemia
General disorders and administration-site conditions: injection-site hematoma, vessel puncture-site hematoma
DRUG INTERACTIONS
Apixaban is a substrate of both CYP3A4 and P-gp. Inhibitors of CYP3A4 and P-gp increase exposure to apixaban and increase the risk of bleeding. Inducers of CYP3A4 and P-gp decrease exposure to apixaban and increase the risk of stroke and other thromboembolic events.
Combined P-gp and Strong CYP3A4 Inhibitors
For patients receiving ELIQUIS 5 mg or 10 mg twice daily, the dose of ELIQUIS should be decreased by 50% when coadministered with drugs that are combined P-gp and strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, ritonavir) [see Dosage and Administration (2.5) and Clinical Pharmacology (12.3) in full Prescribing Information]
For patients receiving ELIQUIS at a dose of 2.5 mg twice daily, avoid coadministration with combined P-gp and strong CYP3A4 inhibitors [see Dosage and Administration (2.5) and Clinical Pharmacology (12.3) in full Prescribing Information]
Clarithromycin
Although clarithromycin is a combined P-gp and strong CYP3A4 inhibitor, pharmacokinetic data suggest that no dose adjustment is necessary with concomitant administration with ELIQUIS [see Clinical Pharmacology (12.3) in full Prescribing Information].
Combined P-gp and Strong CYP3A4 Inducers
Avoid concomitant use of ELIQUIS with combined P-gp and strong CYP3A4 inducers (e.g., rifampin,carbamazepine,phenytoin,St.John’swort)becausesuchdrugswilldecreaseexposure to apixaban [see Clinical Pharmacology (12.3) in full Prescribing Information].
Anticoagulants and Antiplatelet Agents
Coadministration of antiplatelet agents, fibrinolytics, heparin, aspirin, and chronic NSAID use increases the risk of bleeding.
APPRAISE-2, a placebo-controlled clinical trial of apixaban in high-risk, post-acute coronary syndrome patients treated with aspirin or the combination of aspirin and clopidogrel, was terminated early due to a higher rate of bleeding with apixaban compared to placebo. The rate of ISTH major bleeding was 2.8% per year with apixaban versus 0.6% per year with placebo in patients receiving single antiplatelet therapy and was 5.9% per year with apixaban versus 2.5% per year with placebo in those receiving dual antiplatelet therapy.
In ARISTOTLE, concomitant use of aspirin increased the bleeding risk on ELIQUIS from 1.8% per year to 3.4% per year and concomitant use of aspirin and warfarin increased the bleeding risk from 2.7% per year to 4.6% per year. In this clinical trial, there was limited (2.3%) use of dual antiplatelet therapy with ELIQUIS.
USE IN SPECIFIC POPULATIONS
Pregnancy
Pregnancy Category B
There are no adequate and well-controlled studies of ELIQUIS in pregnant women. Treatment is likely to increase the risk of hemorrhage during pregnancy and delivery. ELIQUIS should be used during pregnancy only if the potential benefit outweighs the potential risk to the mother and fetus.
Treatment of pregnant rats, rabbits, and mice after implantation until the end of gestation resulted in fetal exposure to apixaban, but was not associated with increased risk for fetal malformations or toxicity. No maternal or fetal deaths were attributed to bleeding. Increased incidence of maternal bleeding was observed in mice, rats, and rabbits at maternal exposures that were 19, 4, and 1 times, respectively, the human exposure of unbound drug, based on area under plasma-concentration time curve (AUC) comparisons at the maximum recommended human dose (MRHD) of 10 mg (5 mg twice daily).
Labor and Delivery
Safety and effectiveness of ELIQUIS during labor and delivery have not been studied in clinical trials. Consider the risks of bleeding and of stroke in using ELIQUIS in this setting [see Warnings and Precautions]
Treatment of pregnant rats from implantation (gestation Day 7) to weaning (lactation Day 21) with apixaban at a dose of 1000 mg/kg (about 5 times the human exposure based on unbound apixaban) did not result in death of offspring or death of mother rats during labor in association with uterine bleeding. However, increased incidence of maternal bleeding, primarily during gestation, occurred at apixaban doses of ≥25 mg/kg, a dose corresponding to ≥1.3 times the human exposure.
Nursing Mothers
It is unknown whether apixaban or its metabolites are excreted in human milk. Rats excrete apixaban in milk (12% of the maternal dose).
Women should be instructed either to discontinue breastfeeding or to discontinue ELIQUIS (apixaban) therapy,taking into account the importance of the drug to the mother.
Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
Geriatric Use
Of the total subjects in the ARISTOTLE and AVERROES clinical studies, >69% were 65 years of age and older, and >31% were 75 years of age and older. In the ADVANCE-1, ADVANCE-2, and ADVANCE-3 clinical studies, 50% of subjects were 65 years of age and older, while 16% were 75 years of age and older. In the AMPLIFY and AMPLIFY-EXT clinical studies, >32% of subjects were 65 years of age and older and >13% were 75 years of age and older. No clinically significant differences in safety or effectiveness were observed when comparing subjects in different age groups.
Renal Impairment
Reduction of Risk of Stroke and Systemic Embolism in Patients with Nonvalvular Atrial Fibrillation
The recommended dose is 2.5 mg twice daily in patients with at least two of the following characteristics [see Dosage and Administration (2.1) in full Prescribing Information]:
• age greater than or equal to 80 years
• body weight less than or equal to 60 kg
• serum creatinine greater than or equal to 1.5 mg/dL
Patients with End-Stage Renal Disease on Dialysis
Clinical efficacy and safety studies with ELIQUIS did not enroll patients with end-stage renal disease (ESRD) on dialysis. In patients with ESRD maintained on intermittent hemodialysis, administration of ELIQUIS at the usually recommended dose [see Dosage and Administration (2.1) in full Prescribing Information] will result in concentrations of apixaban and pharmacodynamic activity similar to those observed in the ARISTOTLE study [see Clinical Pharmacology (12.3) in full Prescribing Information].Itisnotknownwhethertheseconcentrations will lead to similar stroke reduction and bleeding risk in patients with ESRD on dialysis as was seen inARISTOTLE.
Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery, and Treatment of DVT and PE and Reduction in the Risk of Recurrence of DVT and PE
No dose adjustment is recommended for patients with renal impairment, including those with ESRD on dialysis [see Dosage and Administration (2.1) in full Prescribing Information]. Clinical efficacy and safety studies with ELIQUIS did not enroll patients with ESRD on dialysis or patients with a CrCl <15 mL/min; therefore,dosing recommendations are based on pharmacokinetic and pharmacodynamic (anti-FXa activity) data in subjects with ESRD maintained on dialysis [see Clinical Pharmacology (12.3) in full Prescribing Information].
Hepatic Impairment
No dose adjustment is required in patients with mild hepatic impairment (Child-Pugh class A). Because patients with moderate hepatic impairment (Child-Pugh class B) may have intrinsic coagulation abnormalities and there is limited clinical experience with ELIQUIS in these patients, dosing recommendations cannot be provided [see Clinical Pharmacology (12.2) in full Prescribing Information]. ELIQUIS is not recommended in patients with severe hepatic impairment(Child-PughclassC) [seeClinicalPharmacology(12.2)infullPrescribingInformation].
OVERDOSAGE
Overdose of ELIQUIS increases the risk of bleeding [see Warnings and Precautions]
In controlled clinical trials, orally administered apixaban in healthy subjects at doses up to 50 mg daily for 3 to 7 days (25 mg twice daily for 7 days or 50 mg once daily for 3 days) had no clinically relevant adverse effects.
In healthy subjects, administration of activated charcoal 2 and 6 hours after ingestion of a 20-mg dose of apixaban reduced mean apixaban AUC by 50% and 27%, respectively. Thus, administration of activated charcoal may be useful in the management of apixaban overdose or accidental ingestion. An agent to reverse the anti-factor Xa activity of apixaban is available.
PATIENT COUNSELING INFORMATION
Advise patients to read the FDA-approved patient labeling (Medication Guide).
Advise patients of the following:
• Not to discontinue ELIQUIS without talking to their physician first.
• That it might take longer than usual for bleeding to stop, and they may bruise or bleed more easily when treated with ELIQUIS. Advise patients about how to recognize bleeding or symptoms of hypovolemia and of the urgent need to report any unusual bleeding to their physician.
• To tell their physicians and dentists they are taking ELIQUIS, and/or any other product known to affect bleeding (including nonprescription products, such as aspirin or NSAIDs), before any surgery or medical or dental procedure is scheduled and before any new drug is taken.
• If the patient is having neuraxial anesthesia or spinal puncture, inform the patient to watch for signs and symptoms of spinal or epidural hematomas [see Warnings and Precautions]. If any of these symptoms occur,advise the patient to seek emergent medical attention.
• To tell their physicians if they are pregnant or plan to become pregnant or are breastfeeding or intend to breastfeed during treatment with ELIQUIS [see Use in Specific Populations].
• How to take ELIQUIS if they cannot swallow, or require a nasogastric tube [see Dosage and Administration (2.6) in full Prescribing Information]
• What to do if a dose is missed [see Dosage and Administration (2.2) in full Prescribing Information]
Marketed by: Bristol-Myers Squibb Company Princeton,New Jersey 08543 USA and Pfizer Inc NewYork,NewYork 10017 USA
GUEST EDITORIAL: We need to reassess our primitive understanding of the venous system
BY JEAN BISMUTH, MD
If one includes the entire spectrum of venous disease, it is a more common pathology than peripheral arterial disease. The financial impact of venous disease is substantial. Why, then, has it taken so long to generate enthusiasm for venous disease of the femorocaval and subclaviocaval segments? For years, the endovascular management of venous disease used technology and techniques borrowed from the arterial space; although results were encouraging, it is clear that they varied widely and continue to do so. Management of these vascular beds is very reminiscent of the barrage of devices we have thrown at the superficial femoral artery.
In peripheral arterial disease, there have been much education and research focused on understanding atherosclerosis and its interaction with arterial devices. However, the paucity of investigation and enlightenment in the venous domain is evident when a literature search is performed. Certainly there are data from Comerota et al. showing an increased amount of collagen in the walls of chronically diseased veins. While this is a reasonable start, there are not sufficient data on which to build an entire treatment paradigm. Just like peripheral arterial disease, venous pathology presents in a continuum. Without an in-depth appreciation of the variability of those presentations, it is difficult to envision targeted therapies.
Although vendors have recently engaged in the development of venous-specific devices, it is in great part grounded in expert opinion rather than in hard data. The Medicare Evidence Development & Coverage Advisory Committee has made it known that we need more evidence on the efficacy
Dr. Bismuth is an associate professor of surgery and associate program director, Houston Methodist Hospital.
our group’s opinion, these considerations are elemental in determining the next steps in the research paradigm. What determines the remodeling of a vein, with or without intervention? How does a stent influence remodeling? Not surprisingly there are numerous questions that remain unanswered.
VASCULAR SPECIALIST Medical Editor Malachi Sheahan III, MD
Associate Medical Editors Mark A. Adelman MD, Bernadette Aulivola, MD, O. William Brown, MD, Elliot L. Chaikof, MD, PhD, Carlo Dall’Olmo, MD, Alan M. Dietzek, MD, RPVI, FACS, Professor Hans-Henning Eckstein, MD, John F. Eidt, MD, Robert Fitridge, MD, Dennis R. Gable, MD, Linda Harris, MD, Krishna Jain, MD, Larry Kraiss, MD, Joann Lohr, MD, James McKinsey, MD, Joseph Mills, MD, Erica L. Mitchell, MD, MEd, FACS, Leila Mureebe, MD, Frank Pomposelli, MD, David Rigberg, MD, Clifford Sales, MD, Bhagwan Satiani, MD., Larry Scher, MD, Marc Schermerhorn, MD, Murray L. Shames, MD, Niten Singh, MD, Frank J. Veith, MD, Robert Eugene Zierler, MD
Resident/Fellow Editor Laura Drudi, MD.
Executive Director SVS Kenneth M. Slaw, PhD.
Interim Director of Membership, Marketing and Communications
Angela Taylor
Managing Editor SVS Beth Bales
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of health care policy. Content for Vascular Specialist is provided by Frontline Medical Communications Inc. Content for the News From the Society is provided by the Society for Vascular Surgery.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and Frontline Medical Communications Inc. will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein.
of all venous procedures. Peter Gloviczki, MD, former president of the Society for Vascuar Surgery, put it succinctly in an issue of Venous News: “We need to focus on venous research and never forget that whoever owns research owns the disease. We must continue innovation and collaboration, with other venous specialties and with industry.” Truth be told, there doesn’t seem to be much fascination with comprehension of the disease, but there appears to be an enormous drive from a variety of specialties to do procedures.
In July 2015, Gerard O’Sullivan, MD, wrote of a multidisciplinary group in Europe established to develop some standardization in venous stenting guidelines. He describes a “need for consistent guidelines for preoperative imaging, follow-up, anticoagulation duration and type, stent diameter, length into the inferior vena cava and lower end in relation to the internal iliac vein/external iliac vein.” I concur, that this would be utopic. I have not come across such guidelines to date.
Current basic science research focuses on pathologic considerations of venous thrombosis, including the consequences related to mechanical behavior of the venous wall in those conditions. In
POSTMASTER Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 10255 W Higgins Road, Suite 280, Rosemont, IL 60018-9914.
RECIPIENT: To change your address, contact Subscription Services at 1-800-430-5450. For paid subscriptions, single issue purchases, and missing issue claims, call Customer Service at 1-833-836-2705 or e-mail custsvc.vasc@fulcoinc.com.
The Society for Vascular Surgery headquarters is located at 633 N. St. Clair St., 22th Floor, Chicago, IL 60611. Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by Frontline Medical Communications Inc., 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609. Phone 973-206-3434, fax 973-206-9378
Subscription price is $230.00 per year.
National Account Manager Valerie Bednarz, 973-206-8954, cell 973-907-0230, vbednarz@mdedge.com
Digital Account Manager Rey Valdivia 973-206-8094 rvaldivia@mdedge.com
Scan this QR Code to visit vascularspecialistonline.com
Translational investigation has provided insight into innovative ways to use computed tomography and magnetic resonance imaging. The ability to stage venous disease noninvasively could have a profound impact on how and why we manage the pathology. Additionally, knowing what the pathology looks like and potentially behaves like has the potential to promote more appropriate therapies. Intravascular ultrasound (IVUS) is well described by users and essential to the management of venous disease as it allows us to visualize and appreciate the pathology being treated in real time.
IVUS, though, is primarily used in the context of delivering a therapeutic tool as well as being invasive. Until recently, we have not been able to bring the power of cross-sectional imaging into the operative space. Our group has published on the use of multimodal imaging techniques such as magnetic resonance venography and fluoroscopic image fusion, which can potentially guide future interventions and optimize therapeutic decision making. Ultimately, we believe that diseased veins behave differently than arteries do. Therefore, managing veins with tools meant for another space is likely not ideal. Many venous interventions use arterial devices that are not optimized for venous pathologies and underline the fact that we need to continue to develop tools specifically designed for the venous space. The ATTRACT (Acute Venous Thrombosis: Thrombus Removal
In affiliation with Global Academy for Medical Education, LLC
President David J. Small, MBA
NIVL curriculum
Trainees from page 1
Chou. Using responses from individual trainees, the authors grouped programs into one of two categories: those whose trainees felt well prepared for the RPVI, and those whose trainees felt unprepared for the RPVI.
In addition to a yes/no question about preparedness, the survey also asked whether training programs had a structured curriculum; respondents were asked to identify specific NIVL-related training activities. The survey asked about individual didactic components, as well as whether the trainee spent individual time with
Of the 32 programs with trainees who reported taking the RPVI exam, 18 had trainees who felt unprepared.
an attending physician and hands-on time with vascular technologists. Respondents were asked about the amount of time, measured in half days per week, spent in the vascular laboratory.
Finally, the survey asked whether trainees took a pre-RPVI exam review course, and whether they passed the RPVI exam on their first attempt.
Overall, 34 of the programs with respondents (55.7%) had structured curricula; the same number included lectures. Twenty programs (32.8%) provided video content, and 29 (47.5%) used textbooks. Just 18 programs (29.5%) assigned articles. One-on-one time spent with an attending physician and focused on NIVL techniques was reported for 32 programs (52.5%). More programs (n = 37; 60.7%) provided trainees hands-on experience with
vascular technologists.
Most programs (n = 32; 52.5%) had trainees spending less than one–half day per week in the vascular laboratory, according to survey respondents.
In terms of preparedness, respondents for over half of the programs did not respond to the question asking whether they felt prepared for the RPVI, presumably because they had not yet taken the exam. This, acknowledged Dr. Chou, was a significant limitation of the survey. There was a timing problem: Trainees were surveyed at the start of the 2017-2018 academic year, but the RPVI exam isn’t usually taken until the end of the final year of training, with review courses taken not long before that.
Of the 32 programs with trainees who reported taking the RPVI exam, 18 had trainees who felt unprepared, and 14 program had trainees who felt well prepared. About a quarter of programs (n = 15; 24.6%) had trainees who took a review course prior to taking the exam.
Dr. Chou and her colleagues then examined the survey responses another way, seeing what differentiated the programs whose trainees felt well prepared from those with trainees who felt unprepared.
Statistically, the clear standout was whether the program had a structured curriculum: The 14 programs with a structured curriculum all had students who reported feeling well prepared. Just one-third of the 18 programs with unprepared students had a structured curriculum, which was a significant difference (P = .0001).
Also, programs that assigned articles and those that gave formal lectures were more likely to have students who felt prepared to sit for the RPVI exam (P = .002 and .004, respectively). A higher number of programs that gave trainees hands-on time with vascular technologists had
Venous
continued from page 6
With Adjunctive Catheter-Directed Thrombolysis) trial has been extremely impactful in the treatment paradigm of venous thrombosis. Although the results remain heavily debated and, on some level, contested, it is a critical trial and should – in many ways – serve as an example of the good research being
executed in venous disease. A quote many have attributed to Albert Einstein says: “The one who follows the crowd will usually go no further than the crowd. Those who walk alone are likely to find themselves in places no one has ever been before.” We have an opportunity to be more enlightened with respect to
trainees who felt prepared, but the difference wasn’t quite statistically significant (P = .05).
Having taken a review course prior to the exam was associated with feeling well prepared (P = .03).
Dr. Chou and her colleagues performed a logistic regression analysis to arrive at the educational components associated with the highest odds for trainees feeling well prepared. Lectures and articles came out on top in this analysis (odds ratios for feeling well prepared, 15.88 and 15.97, respectively). Hands-on time with vascular technologists had an odds ratio of 5.12 for feeling prepared.
Taking a review course boosted preparedness as well, with an odds ratio of 11.85 for feeling well prepared for the RPVI exam. This created a bit of a conundrum for the investigators, said Dr. Chou: “All well-prepared programs had a structured NIVL curriculum, but most of their trainees still took an RPVI review course, so it’s unclear if the structured curriculum or the review course is responsible for trainees feeling well prepared for the RPVI exam,” she said.
An important caveat to the analysis of survey results, said Dr. Chou, is that “It’s unknown how these results will translate into pass rates.
“Vascular surgery leadership should not leave NIVL education to review courses,” said Dr. Chou. The ultimate goal, she said, should be to achieve expertise in the service of providing better patient care. To this end, Dr. Chou and her coauthors recommend that a structured NIVL curriculum be incorporated into vascular surgery training, and that the program include time spent with vascular technologists, a formal lecture-based component, and structured reading, as is provided by a journal club.
Dr. Chou reported no conflicts of interest, and no external sources of funding. ■ koakes@mdedge.com
central venous therapies; let’s not act like lemmings and follow one another off the cliff. ■
References
Comerota AJ et al. 2015 May. Thromb Res. 135(5):882-7.
Vedantham S et al. 2017 Dec 7. N Engl J Med. 377(23):2240-52.
O’Sullivan G 2015 Jul. Endovascular Today.14;7:60-2.
Gloviczki P 2017 Apr. Venous News.1:8.
NEWS Briefs
October Is Psoriasis Awareness Month
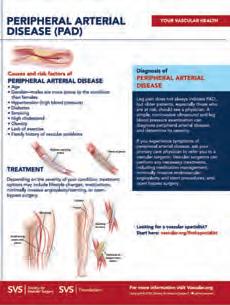
Psoriasis is a chronic systemic inflammatory condition, most notably characterized by skin lesions. But vascular surgeons are well aware that the disease presents a heightened risk for noncardiac vascular diseases, including carotid, peripheral artery, and chronic kidney disease, as well as metabolic co-morbidities such as type 2 diabetes mellitus, and metabolic syndrome. Check out the National Psoriasis Foundation for more info (www. psoriasis.org).
In Memoriam
William Long, MD, who was Tallahassee’s first board-certified peripheral vascular surgeon, died on Aug. 29, 2018. In 1970, he began his career as a general surgeon in Tallahassee after completing the peripheral vascular surgery program at Emory University. After a year, he limited his practice to peripheral vascular surgery and subsequently formed Vascular Associates of Tallahassee.
Upcoming Meetings
(Check https://vascular.org/meetings for details)
2018 Pacific Northwest Vascular Society Annual Meeting
The Pacific Northwest Vascular Society includes physicians interested in vascular disease from the Alaska, Washington, Oregon, Idaho, Montana and British Columbia, Alberta, and Saskatchewan. It will be held Nov. 1-2, 2018 at The Edgewater Hotel, 2411 Alaskan Way, Seattle. The PNVS is recognized as an official regional vascular society by the SVS
2018 Texas Society for Vascular and Endovascular Surgery Annual Meeting
The Texas Society for Vascular and Endovascular Surgery will hold its annual meeting at the Marriott Marquis Houston on Nov. 2-3. The TSVES represents the vascular surgeons of Texas and is recognized as an official regional vascular society by the SVS.
The new normal?
Outcomes from page 1
Chicago, and his colleagues.
They performed a study that found a high level of adverse outcomes for common vascular procedures and that there was a significant variability in risk-adjusted outcomes among best- and poorest-performing hospitals in all major vascular procedures, indicating that a large opportunity exists for improvement in results.
Medicare’s value-based care Readmissions Reduction Model developed financial penalties for hospitals that fail to achieve acceptable performance scores, and in doing so shifted some of the financial risks of care to the providers based on a 30-day readmission model. In contrast, the pilot Bundled Payments for Care Improvement (BPCI) Advanced Program, which the CMS plans to launch this month, will follow a 90-day period of postoperative care as its duration of financial accountability.
“While BPCI Advanced, has, until now, focused upon orthopedics, cardiovascular procedures, and high-volume medical admissions areas, it is anticipated that vascular surgery will be included in the future,” according to the investigators. Therefore, the researchers performed an in-depth analysis to examine the 90-day outcomes of common vascular surgeries across hospitals as a prelude to the vascular surgery field having to potentially confront this new CMS model (Surgery 2018 Jun 22 doi: 10.1016/j.surg.2018.03.025).
Dr. Fry and his colleagues used the Medicare Limited Data Set for 2012-2014 to follow the outcomes of major vascular surgery beginning with the inpatient stay and on through 90 days of postoperative care. A pool of more than 500 aggregated and individual candidate risk factors, including age and sex, was used in model development, based upon data from 359 hospitals with 10,815 patients in the Medicare Limited Data Set.
The researchers examined the risk-adjusted outcomes of four major groupings of vascular surgery procedures: elective open aortic; open peripheral vascular procedures; endovascular
DR. FRY
aortic; and percutaneous angioplasty procedures. They found that the total adverse-outcome (AO) rate was 27.8% for open aortic procedures, 31.5% for open peripheral vascular procedures, 19.6% for endovascular aortic procedures, and 36.4% for percutaneous angioplasty procedures. The difference in risk-adjusted AO rates between the best- and the poorest- performing deciles was 32.2% for open aortic procedures, 29.5% for open peripheral vascular procedures, 21.5% for endovascular aortic procedures, and 37.1% for percutaneous angioplasty procedures.
The model determined significant risk factors (P less than .001) for inpatient death (including malnutrition, intestinal ischemia, supplemental oxygen, and age greater than or equal to 85 years); prolonged length of stay (including supplemental oxygen, peritoneal adhesions, and chronic obstructive lung disease); 90-day postdischarge death (including heart failure, chronic infection, psychosis, and primary head/neck cancer); and 90-day postdischarge readmission (malnutrition, chronic
First readmissions during days 31-90 following discharge were almost as common as those occurring during the initial 30 days. PAD AND CLAUDICATION
obstructive lung disease, upper aerodigestive tract cancer, and skin ulceration) for these procedures. For all cases, the total 90-day postdischarge mortality rate exceeded the inpatient death rate, and readmissions were the major driver of the total AO. They found that 22% of all patients readmitted across the entire 90-day interval had not seen a physician for follow-up after discharge. This “begs the question of whether more frequent physician or physician-extender follow-up can reduce this AO,” according to Dr. Fry and his colleagues. “Importantly, first readmissions during days 31-90 following discharge were almost as common as those occurring during the initial 30 days. Over 20% of total readmissions were subsequently repeat events during the 90-day interval,” they added.
They also found that the variability in risk-adjusted outcomes among the best and poorest performing hospitals was over 20% in all of the major vascular procedures and indicates a large opportunity for improvement in results.
“Understanding variables associated with higher risk can be used as a decision support tool to identify which patients will need increased vigilance to avoid AOs. Identification of very high risk may become a consideration in the assessment of the appropriateness of the surgical intervention. If providers know their outcomes and those outcomes are benchmarked against the whole population of hospitals, then clinical performance can be improved by specific care redesign initiatives,” the researchers concluded.
Dr. Fry is executive vice president of MPA Healthcare Solutions, which funded the research. ■ mlesney@mdedge.com
SOURCE: Fry DE et al. Surgery. 2018 Jun 22. doi: 10.1016/j.surg.2018.03.025.
Using WIfI as a predictive tool for amputation risk
WIfI is a promising tool to identify chronic limb-threatening ischemia (CTLI) presentations most likely to benefit from revascularization, according to Jessica M. Mayor, MD, and her colleagues, and could be used to better inform patients, guide decision making, and risk-adjust quality and outcomes assessments.
Dr. Mayor, of the Baylor College of Medicine, Houston, presented their research study to quantify which CLTI patients most benefit from revascularization by comparing the predicted to observed 1-year major lower-extremity amputation (LEA) risk stratified by WIfI Clinical Stage at the Vascular Annual Meeting.
The Society of Vascular Surgery (SVS) Wound Ischemia Foot Infection (WIfI) classification was intended to predict 1-year major LEA risk without revascularization, and identify which CLTI patients benefit most from revascularization.
Dr. Mayor and her colleagues retrospectively reviewed composite multi-institutional cohort data
from centers that had previously validated WIfI. They compiled Individual WIfI component grades, corresponding WIfI clinical stages, and observed LEA rate for each presentation. Multivariable linear regression analysis was performed to quantify which WIfI score component(s) best predicted amputation.
They collated data from 10 centers, and from a total population of 2,878 limbs at risk, they examined the subset of pa-tients undergoing revascularization as their study base (1,654 limbs; 169 LEAs). Of 64 potential WIfI grade combinations, 12 were never reported and were excluded from analysis. Stratifying by the original WIfI stages, the observed LEA rate after revascularization was: Stage 1, 6.8% (8/118); Stage 2, 3.8%; Stage 3, 6.0%; Stage 4, 18.8%.
They used cluster analysis to identify four clusters with the following 1-year LEA rates: Cluster 1, 4.4%; Cluster 2, 14.8%; Cluster 3, 28.1%; Cluster 4, 51.2%. The analysis showed that the revascularization ben-
efit was greatest in limbs with small to moderate wounds, moderate to severe ischemia, and moderate-severe foot infection (W2 I2 FI3; W1 I3 FI2).
Initially, for WIfI clinical stage 4, these presentations behaved as lower-risk Cluster 2 after revascularization. Multiple linear regression revealed wound grade most strongly predicted LEA (P less than .001). Ischemia (P = .001) and infection (P = .003) were similarly associated with LEA risk. Interaction terms between each component of WIfI score were not statistically significant.
“Our results show that wound severity is most strongly associated with LEA risk and that ischemic and infectious grades confer additive, but not synergistic risk,” according to Dr. Mayor.
“Future cluster analyses comparing specific WIfI presentations treated with and without revascularization may quantify the benefit of revascularization for a given WIfI presentation and further refine the risk-stratification provided by WIfI,” she and her colleagues concluded. ■
EXPERIENCE THE DIFFERENCE IN
BELOW THE KNEE PROCEDURES
Choose the distinctive performance of our balloon dilatation catheters
Engineered to provide best-in-class PUSHABILITY* with a small profile for accessing target lesions1
Complete support for complex BTK cases
PINNACLE® DESTINATION®
Guiding Sheath NAVICROSS® Support Catheters
*Tested against select leading competitors
Demonstrated excellence in CROSSABILITY with a low deflation time1
GLIDEWIRE ADVANTAGE® Peripheral Guidewires
GLIDEWIRE® GOLD Hydrophilic Coated Guidewire
When RX tested against Boston Scientific Sterling™ Monorail™ and OTW tested against Bard Ultraverse® 0.018" RX ONLY. Refer to the product labels and package inserts for complete warnings, precautions, potential complications, and instructions for use. Reference: 1. Data
SVS Submits Comments Seeking Changes in CMS Proposed Rules for 2019
In an effort to alter specific policies in the Centers for Medicare and Medicaid Services’ (CMS) CY 2019 Medicare Fee Schedule Proposed Rules, Society for Vascular Surgery leaders have submitted a 20-page comment letter with recommendations to CMS.
CMS released the combined Medicare Physician Fee Schedule (PFS) /Quality Payment Program (QPP) proposed rule in July. Comments were due in mid-September; the final rule is expected on or around November 1, 2018.
These rules affect payment policies and reimbursements for procedures performed by physicians and healthcare providers across the country.
SVS, with other societies, urges the CMS to delay implementing the E/M proposal.
Another important element for vascular surgeons is CMS’ recommended repricing on both the vascular ultrasound room (EL016) and the general ultrasound room (EL015). Pricing for both would decrease dramatically: 57 percent, from $466,492 to $199,449 for the vascular ultrasound room and 65 percent, from $369,945 to $130,252 for the general ultrasound room.
Regarding the combined Medicare Physician Fee Schedule (PFS) /Quality Payment Program (QPP) proposed rules, of particular importance to vascular surgeons are proposals to combine and flatten payments for Evaluation and Management (E&M) codes and a proposal to reprice the cost of the practice expense direct inputs. If finalized, this would result in substantial cuts to vascular labs and other vascular procedures.
At the same time, SVS supports a number of the CMS proposals, including efforts to reduce paperwork and increase time spent on patient care.
CMS proposes a single rate for E/M office visits for levels 2 through 5 services. As a result, “the Indirect Cost Indices change significantly for some specialties,” SVS wrote, including a possible 10 percent loss for vascular surgery. “This is not a sound policy,” SVS leaders said.
These two equipment inputs are among 2,107 items currently used as direct practice expense inputs for which CMS proposes to update pricing for CY 2019, with a four-year transition given the impact to the fee schedule. SVS and other agencies question the validity of the pricing, all performed by a CMS contractor. They question several aspects of the pricing process and urge CMS to delay any pricing changes for 2019.
SVS calls the approach to repricing “careless” and one that “does not accurately account for all typical ultrasound room components.” Should CMS insist on pricing changes, SVS leaders said they have provided enough information to request maintaining current pricing for both ultrasound rooms and then refer repricing of the two rooms to an American Medical Association subcommittee.
Quality Payment Program Comments
The SVS also commented on several proposed changes for Year 3 of the Quality Payment Program (QPP):
The Benefits of Belonging
Membership in the Society for Vascular Surgery is a valuable resource at all stages of your career. You receive:
Community and professional standing
• A professional home for all those involved with circulatory diseases, from those researching the how and why, to those delivering top-quality care
• The prestige of being part of the largest professional association in the world representing vascular surgeons
• Branding initiatives to target vascular specialists as the experts for the care of circulatory diseases
Publications to keep you in the know
• Peer-reviewed research, science and surgical techniques via the Jour-
nal of Vascular Surgery (free for active members, online only for international members; affiliate and senior members pay highly reduced rate)
• Important SVS news, via the electronic newsletter, Pulse; and the monthly Vascular Specialist publication (U.S. only)
Education and networking with thought leaders, at exclusive member pricing
• At meetings: Vascular Annual Meeting, the Vascular Research Initiatives Conference and the Coding & Reimbursement Workshop
• Through educational products including the Vascular Education and Self-Assessment Program
Practice management resources
• Thoroughly researched, evi-
• Seeking a single 12-month determination period for participants in the Merit-Based Incentive Payment System, not a proposed 24-month assessment period.
• Not expanding the low-volume threshold criterion for several reasons, including that expansion impacts the availability of bonus payments.
• Urging CMS to move ahead with specialtyspecific subgroups within a larger multi-practice group, to further the goal of quality care.
• Asking CMS to consider 2019 a field-testing year, holding SVS members harmless from episode-cost measure results, particularly because of physician difficulties in getting access to field-testing reports.
• Opposing a blanket requirement that all physicians use electronic health records technology certified to the 2015 edition.
• Urging a better process for approval for Advanced Alternative Payment Models for specialists. (SVS is working to develop an advanced APM for vascular surgeons.)
The letter, which contains many more suggestions and details, was submitted by President Dr. Michel Makaroun and Drs. Sean Roddy, Matthew Sideman, Megan Tracci and Karen Wood, chairs, respectively, of the Policy and Advocacy Council, plus Coding and Reimbursement, Government Relations and the Quality and Performance Measures committees. See the full letter at vsweb.org/PFScomments18D
SVS also submitted comments later in September on other CMS proposed rules, including the CY 2019 Hospital Outpatient Prospective Payment System. Read those comments at vsweb.org/ HOPPScomments18 ■
dence-based clinical practice guidelines and reporting standards to facilitate exemplary patient care
• Consensus documents
• Patient care and awareness brochures
• The popular Find a Specialist referral service (active members only)
• Information on the Medicare Quality Payment Program
• The SVS Patient Safety Organization’s Vascular Quality Initiative
Career advancement and the chance to shape the future of vascular surgery, through
• Mentorship
• Leadership opportunities, such as service on councils and committees
• Scholarships
Research grants
• For promising vascular surgeons at every stage of their careers
A voice in Washington, D.C.
• Advocacy in decisions that affect members’ lives and livelihoods
Other benefits to enhance your professional career
• The SVS Job Board
• Financial services products available at member discounts through the Affinity Program of Expanded Benefits, including:
Disability coverage designed with the vascular surgery subspecialty in mind; many vascular surgeons aren’t adequately covered
– The Kai-Zen program of accelerated retirement funding. ■
YOUR SVS
Dues Statements Distributed Membership dues statements for 2019 were sent to all members at the beginning of October. Members should pay their dues by Dec. 31 to ensure they continue to receive all the benefits of SVS membership. The pluses are numerous and outlined on page 10.
Visit vascular.org/invoices or call the SVS Membership Department, 312-334-2313, to pay dues.
Donate to SVS Foundation While Paying Dues; Read Foundation Annual Report
While paying their dues, members also can make a donation to the SVS Foundation, which has expanded its mission to include not only funding crucial vascular research but also disease prevention, patient education and public awareness of circulatory disorders.
As part of the expansion, the Foundation has just completed patient education materials on nine topics (see story on page 12), all of which members can download. It co-sponsored a screening for abdominal aortic aneurysms at the Veterans of Foreign Wars annual convention in July. In June, three members received the first Community Awareness and Prevention Grants for projects aimed squarely at improving community health.
These and other accomplishments are highlighted in the just-released SVS Foundation Annual Report, “Because …” Read and/or download it at vsweb.org/
SVSF_Annual_Report_2018.
To pay dues and donate: log on to vascular.org/invoices to locate the owed dues and simply add the donation amount at “Please consider making a gift to the following funds.” The donation will be added; simply check out and pay the invoice.
Final 2018 Membership
Deadline is Dec. 1
Dec. 1 is the final deadline in 2018 to apply to become part of the world’s premier vascular care organization.
The Society for Vascular Surgery switched to a quarterly application system this year, with deadlines on March 1, June 1, Sept. 1 and Dec. 1. This provides four chances to join the Society, which supports excellence and innovation in vascular health through education, advocacy, research and public awareness, and many perks of membership, outlined on the bottom of the previous page.
Visit vsweb.org/JoinSVS for more information and an application. Email questions to membership@vascularsociety.org
Claim VAM 2018
Credits by Dec. 31
Credits from the 2018 Vascular Annual Meeting must be claimed by Dec. 31. To do so, visit vsweb.org/ClaimCME and follow the directions to list sessions, provide evaluations, take exams and generate credit certificates. ■
Please Give, Because Every Gift Matters
A letter from the SVS
Foundation Chair
Because …
That’s the simple – yet multifaceted — theme for our SVS Foundation Annual Report (just released and available at vsweb.org/ SVSF_Annual_Report_ 2018) and for our annual Giving Campaign.
The word resonates. It links the “why” with the “how” and also reflects the busy and productive past few years.
For example, after expanding our mission last year to include disease prevention and patient awareness and education, we have awarded our first Community Awareness and Prevention Grants.
We launched this grant because prevention and public awareness are critical in the fight against circulatory disease and because our community-based practitioners are in the front lines of this battle every day. We highlighted the three projects and SVS project administrators in August’s Vascular Specialist and in the report.
This grant is just one of the new 2018 Foundation initiatives we began to support the enhanced core mission. For example: To optimize the vascular health and well-being of patients and the public through support of research that leads to discovery of knowledge and innovative strategies,
Submit Research to VAM Starting Nov. 12
R
esearch to shed new light on PAD, long-term survival after EVAR, diving into whether vascular surgeons are hurting themselves while operating: at their core, abstracts such as these — presented at earlier Vascular Annual Meetings — all include data and insights important to vascular surgeons.
Though the 2019 VAM is still months away, the time to submit abstracts for possible inclusion in the meeting is approaching rapidly. Abstract guidelines are expected to be available the week of Oct. 29, and researchers can submit abstracts in less than
a month, starting Nov. 12. Abstract submissions will close Jan. 16, 2019.
The meeting will be held June 12-15, 2019, at the Gaylord National Resort & Convention Center in National Harbor, Md., outside Washington, D.C. Scientific sessions will be held June 13 through 15 and exhibits will be open June 13 and 14. Housing and registration will open in early March.
Authors may submit their research – including videos – in several categories.
The selection committee will choose abstracts
as well as education and programs, to prevent and treat circulatory disease.
• … Because patient education is critical to helping prevent circulatory diseases and provide help at early stages, we created brochures and other patient education materials on nine common issues, including PAD, smoking and carotid artery disease.
• ... Because some mid-career surgeon-scientists face an unanticipated loss of national grant money for a funding cycle, we launched a new Bridge Grant program to sustain critical research projects.
I hope you’ll read the annual report, which contains articles and information about what we do, how much money we raise and where it goes, why people give and the profound differences we can make in our research labs and in our communities.
The SVS Foundation touches every SVS member, from our academicians searching for solutions to our surgeons in private practice saving patients’ lives and limbs. We all share the same goal: improving patient care. And because we must do more, we need your help. Please give today to support our expanded objectives. Because … every gift matters.
Give at vsweb.org/Give ■ – R. Clement Darling III, MD
for different program types: scientific sessions, the Vascular and Endovascular Surgery Society (VESS) sessions, International Forum, International Fast Talk, Poster Competition and Interactive Poster Competition.
Submission categories include: aortic disease; cerebrovascular (including Great Vessels); complications; dialysis access; educational/training credentialing; peripheral arterial disease; practice management; renal/visceral disease; vascular laboratory and imaging; vascular medicine; vascular trauma: aortic, arterial, venous; venous disease; and basic research (poster competition only).
See the guidelines at vsweb.org/Guidelines19 and learn more about VAM at vsweb.org/ VAM19. ■
DR. DARLING
SVS Announces Award for Community Service Honoree Will be Community-Based Practitioner
The Society for Vascular Surgery emphasizes not only education and research, but also public awareness.
Now, through the justannounced Excellence in Community Service Award, the Society plans to honor a member who has made not only contributions to the profession but to the community as well.
Applications for this new honor are due Feb. 1, 2019. The recipient will be announced and recognized at the 2019 Vascular Annual Meeting in June.
“We want to honor a vascular surgeon working in the community who also is a community leader, a philanthropist, someone who contributes outside of
the operating room,” said Daniel McDevitt, MD, chair of the SVS Community Practice Committee. The committee developed and will oversee the award.
Nominees must have practiced vascular surgery for at least 20 years and been an SVS member for at least five. They also must present evidence of impact on vascular care or community health, such as:
• Leadership in a community-based practice
• Implementation of services or innovations to advance community health
• Partnerships or collaborations with community organizations
• Contributions that elevate the stature of the vascular surgery specialty in the community
Dr. McDevitt stressed that the award isn’t particularly geared to members who have already received multiple professional awards. “He or she has a civic presence and exhibited a lifetime of commitment to our profession and the community,” he said. “There’s no real vehicle for recognizing such a person right now except for
the accolades of family and friends.”
Members may nominate a candidate — including him or herself — by submitting the nomination form and supporting documents. All materials are due by Feb. 1. Required are:
• The Nomination Form
• The nominees’ curriculum vitae (either abbreviates or full)
• Description of the nominee’s significant work and impact in a community-practice setting (one page)
• Three letters of recommendation, at least one of which must be from an SVS member.
The SVS Community Practice Committee will review the nominations and select the recipient. Though nominees will be sought every year, the award may not be presented each year.
Nomination materials, all in PDF format, should be mailed to vascular@vascularsociety.org. Learn more at vsweb.org/CommunityService, email the address above or call 800-258-7188. ■
First of 9 Patient Education Fliers Available
Due to popular demand, the SVS Foundation has developed a new set of patient education fliers. The first one – on Peripheral Arterial Disease – is now available, and was released to coincide with PAD Awareness Month in September.
All members are welcome to download and start using the PAD flier, which has a writable area for your name, clinic name and address.
More fliers are coming soon on:
• What is a vascular surgeon?
• Carotid artery disease
• Abdominal aortic aneurysms
• Varicose veins
• Cholesterol/nutrition
• Smoking
• Diabetes
• Physical activity
All will have updated SVS branding and were written and edited by task force members Drs. Tej Singh and Benjamin Pearce.
“Our goal is to provide handouts on key vascular health topics that surgeons can share with primary care physicians and patients,” said Dr. R. Clement Darling III, Foundation chair. “This aligns with our expanded mission of providing materials and tools for community health and education.”
Members do not need to order the fliers and wait for them to arrive in the mail, he noted. The materials are free to download and print immediately with personal office information.
Members may download either an easy-share flier version to print in their offices or email to a patient at vsweb.org/PADflier, or a high-
Education: Submit Your Abstracts for VRIC ‘19
The Society for Vascular Surgery will begin accepting abstracts Oct. 30 for the 2019 Vascular Research Initiatives Conference. VRIC, which focuses on emerging vascular science, will be held May 13, 2019, in Boston.
Abstract submission closes Jan. 15, 2019.
Besides abstract presentations, VRIC also will feature the Alexander W. Clowes Distinguished Lecture, a Trans-
lational Panel that will discuss “Arterial Calcification,” reception and posters. As in the past, VRIC will be held in conjunction with the American Heart Association’s Scientific Sessions, which will take place May 14 to 16, 2019.
Visit vsweb.org/VRIC19 for more information. ■
er-quality one to email to a local print shop at vsweb.org/PAD_flier_for_printing. Members should be sure to add their contact information in the writable area. ■
From JVS, JVS-VL
From JVS: Results of a new study suggest that medical therapy alone is insufficient protection against strokes for patients with significant carotid stenosis.
The study, in the November Journal of Vascular Surgery, studied stroke patients admitted with a radiographically confirmed infarct ipsilateral to a documented carotid artery stenosis of equal to or greater than 50 percent. Researchers said that even patients receiving both antiplatelet and
lipid-lowering medical therapy are still at risk for a carotid-mediated stroke. Read more at vsweb.org/ JVS-StrokeStenosis
From JVS-VL: A large, image-based study of patients with iliofemoral deep venous thrombosis furthers understanding of the relationship between iliac vein compression and DVT. The article from November’s JVS: Venous and Lymphatic Disorders, is open source through Dec. 31 at vsweb.org/ JVSVL-IliacVein. ■
Opioids don’t treat pain better than ibuprofen after venous ablation surgery
BY KARI OAKES
MDEDGE NEWS
ST. LOUIS – Compared with ibuprofen, opioid pain medication offered little benefit for pain control after venous ablation surgery, in the experience of one surgical center.
Sharing study results at a poster session at the annual meeting of the Midwestern Vascular Surgery Society, Jana Sacco, MD, and her colleagues found that patients who received opioid prescriptions after venous ablations did not have significantly different postsurgical pain than did those who received ibuprofen alone.
The study, conducted against the national backdrop of greater scrutiny of postsurgical opioid prescribing, was the first to look at post–venous ablation pain management strategies, said Dr. Sacco, a resident physician at Henry Ford Hospital, Detroit. Venous ablation surgery can improve quality of life for patients with varicose veins, but best practices for managing postprocedure discomfort had not been clear; some patients re-
ceive opioid pain medications, while others are directed to use ibuprofen as needed for pain control.
The retrospective, single-center study assessed pre- and postoperative pain for patients undergoing venous ablation procedures over a 2-year period, said Dr. Sacco.
Patients who were prescribed opioids were compared with patients who were simply asked to take ibuprofen for pain control.
Comparing preoperative to postoperative pain scores, Dr. Sacco and her colleagues defined a change of 2-3 points on a 0-10 Likert scale as “good” improvement; a change of 1 point was defined as “mild” improvement, and no change or worsening was defined as no improvement.
Of the 268 patients for whom postoperative follow-up data were available, 142 received opioid prescriptions, while 126 did not.
Across the entire group of patients studied, those who had moderate to severe preoperative pain had significant improvement in pain after their procedures.
Whether patients received opioid pain medication after their venous
ablation was not correlated with the degree of improvement in postprocedure pain scores. Of those who saw no improvement, 30 patients (45%) received opioids and 36 (55%) did not.
Of the 89 patients who saw mild postprocedure improvement in pain, 35 (40%) were not discharged on opioids, and of 65 patients who had good improvement in postprocedure pain, 44% were not discharged on opioids (P = .7 for difference across groups).
When Dr. Sacco and her fellow researchers examined such patient characteristics as sex, race, body mass index, smoking status, and CEAP venous severity classification, they did not see any significant differences in pain scores. Similarly, neither the type of procedure (radiofrequency or laser ablation) nor information on whether compression treatment was used was associated with a difference in pain scores.
Dr. Sacco and her coauthors noted that the study was limited by its retrospective nature and the fact that patients were all drawn from a single institution. Additionally, the investigators were only able to ascertain whether opioids had been prescribed, not whether – or how much – medication was actually taken by patients.
“Most patients report an improvement in symptoms after undergoing vein ablation procedures,” reported Dr. Sacco and her colleagues, and most patients also do well with nonopioid pain control regimens. “Overprescribing opioids exposes patients to the risk of narcotic overdose and chronic opioid use and should be used with caution for patients undergoing vein ablation surgery,” they wrote.
Dr. Sacco reported no outside sources of funding and no conflicts of interest. ■
koakes@mdedge.com
The SVS will accept abstracts for the 2019 Vascular Annual Meeting beginning November 12, 2018
June 12–15, 2019 vsweb.org/VAM19
at vsweb.org/2019abstracts
Risk factors for postop cardiac events differ between vascular and general surgery
BY MARK S. LESNEY
MDEDGE NEWS FROM ANNALS OF MEDICINE AND SURGERY
Predictive risk factors for cardiac events (CEs) after general and vascular surgery differed significantly, according to a large retrospective study. However, there was no significant difference seen in the overall incidence of CEs between the two types of surgery, reported Derrick Acheampong, MD, and his colleagues at the Icahn School of Medicine at Mount Sinai, New York.
They performed a retrospective data analysis of 8,441 adult patients at their large urban teaching hospital; these patients had undergone general or vascular surgery during 2013-2016 and, in the analysis, were grouped by whether they experienced postoperative CEs.
Univariate and multivariate analyses identified predictors of postoperative CE and the association of CEs with adverse postoperative outcomes. CEs were defined as myocardial infarction or cardiac arrest within the 30-day postoperative period.
A total of 157 patients (1.9%) experienced CEs after major general and vascular surgery, with no significant difference in incidence between the two types of surgery (P = .44), according to their report, published online in the Annals of Medicine
and Surgery. CE-associated mortality among this group was high, at 55.4%.
The occurrence of a CE following surgery in both groups was significantly associated with increased mortality, as well as pulmonary, renal, and neurological complications, in addition to systemic sepsis, postoperative red blood cell transfusion, unplanned return to the operating room, and prolonged hospitalization, according to the researchers.
However, predictors of CEs risk between vascular and general surgery were significantly different.
For general surgery, American Society of Anesthesiologists (ASA) status greater than 3, dependent functional status, acute renal failure or dialysis, weight loss, creatinine greater than 1.2 mg/dL, international normalized ratio (INR) greater than 1.5, and partial thromboplastin time (PTT) less than 35 seconds were all unique independent predictors of postoperative CEs.
For vascular surgery, the unique significant predictors of postoperative CEs were age greater than 65 years, emergency surgery, diabetes, congestive heart failure, systemic sepsis, and operative time greater than 240 minutes.
The only common predictive risk factors for postoperative CEs for the two forms of surgery were hematocrit less than 34% and ventilator dependence.
“The present study corroborates reported studies that recommend separate predictive CE risk indices and risk stratification among different surgical specialties. Predictors for CE greatly differed between general and vascular surgery patients in our patient population,” the authors stated.
They concluded with the hope that their study “provides useful information to surgeons and allows for the necessary resources to be focused on identified at-risk patients to improve surgical outcomes.”
Dr. Acheampong and his colleagues reported having no disclosures. ■ mlesney@mdedge.com
SOURCE: Acheampong D et al. Ann Med Surg. 2018. doi: 10.1016/j. amsu.2018.08.001.
u A companion app for off-line use (Apple only)
u Syncing between the app and desktop version
u Expanded bookmarking and annotation
u Easier navigation
u Simplified tracking of CME/MOC certificates
u Surgeons who need to meet CME/MOC requirements
u Surgeons preparing for qualifying, certification and recertification vascular surgery exams
u Residents and fellows preparing for ABSITE and VSITE exams
Physician burnout may jeopardize patient care
BY JEFF CRAVEN MDEDGE NEWS FROM JAMA INTERNAL MEDICINE
Physicians experiencing burnout are twice as likely to be associated with patient safety issues and deliver a lower quality of care from low professionalism and are three times as likely to be rated poorly among patients because of depersonalization of care, according to recent research published in JAMA Internal Medicine.
“The primary conclusion of this review is that physician burnout might jeopardize patient care,” Maria Panagioti, PhD, from the National Institute for Health Research (NIHR) School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre at the University of Manchester (England) and her colleagues wrote in their study. “Physician wellness and quality of patient care are critical [as are] complementary dimensions of health care organization efficiency.”
Dr. Panagioti and her colleagues performed a search of the MEDLINE, EMBASE, CINAHL, and PsycInfo databases and found 47 eligible studies on the topics of physician burnout and patient care, which altogether included data from a pooled cohort of 42,473 physicians. The physicians were median 38 years old, with 44.7% of studies looking
at physicians in residency or early career (up to 5 years post residency) and 55.3% of studies examining experienced physicians. The meta-analysis also evaluated physicians in a hospital setting (63.8%), in primary care (13.8%), and across various different health care settings (8.5%).
The researchers found physicians with burnout were significantly associated with higher rates of patient safety issues (odds ratio, 1.96; 95% confidence interval, 1.59-2.40), reduced patient satisfaction (OR, 2.28; 95% CI, 1.42-3.68), and lower quality of care (OR, 2.31; 95% CI, 1.87-2.85). System-reported instances of patient safety issues and low professionalism were not statistically significant, but the subgroup differences did reach statistical significance (Cohen Q, 8.14; P = .007).
Among residents and physicians in their early career, there was a greater association between burnout and low professionalism (OR, 3.39; 95% CI, 2.38-4.40), compared with physicians in the middle or later in their career (OR, 1.73; 95% CI, 1.46-2.01; Cohen Q, 7.27; P = .003).
“Investments in organizational strategies to jointly monitor and improve physician wellness and patient care outcomes are needed,” Dr. Panagioti and her colleagues wrote in the study. “Interventions aimed at improving the culture of health care organizations, as well as interven-
SVS PAC: A Unified Voice for Vascular Surgery in Congress
The Society for Vascular Surgery® (SVS) Political Action Committee (PAC) is the only PAC that provides a unified voice for vascular surgeons. Your support is critical to the future of your practice and profession.
The SVS PAC is an independent committee formed to raise funds used to make contributions to the campaigns of United States House of Representatives and Senate candidates who support high quality diagnosis and care for vascular disease patients and solutions to physician reimbursement challenges. Contributions from corporate accounts and SVS members who are not US citizens or do not have green cards are not permitted. Remember, 100% of your SVS PAC contribution goes directly to candidates.
With your $1,000 contribution, receive an invitation to an exclusive SVS PAC reception during the Vascular Annual Meeting and proudly wear a gold PAC pin in recognition of your donation.
tions focused on individual physicians but supported and funded by health care organizations, are beneficial.”
Researchers noted the study quality was low to moderate. Variation in outcomes across studies, heterogeneity among studies, potential selection bias by excluding gray literature, and the inability to establish causal links from findings because of the cross-sectional nature of the studies analyzed were potential limitations in the study, they reported.
Because of a lack of funding for research into burnout and the immediate need for change based on the effect it has on patient care seen in Panagioti et al., the question of how to address physician burnout should be answered with quality improvement programs aimed at making immediate changes in health care settings, Mark Linzer, MD, of the Hennepin Healthcare Systems in Minneapolis, wrote in a related editorial.
“Resonating with these concepts, I propose that, for the burnout prevention and wellness field, we encourage quality improvement projects of high standards: multiple sites, concurrent control groups, longitudinal design, and blinding when feasible, with assessment of outcomes and costs,” he wrote. “These studies can point us toward what we will evaluate in larger trials and allow a Burnout continued on page 17
PAC Donation Form
SVS
continued from page 16
place for the rapidly developing information base to be viewed and thus become part of the developing science of work conditions, burnout reduction, and the anticipated result on quality and safety.”
There are research questions that have yet to be answered on this topic, he added, such as to what extent do factors like workflow redesign, use and upkeep of electronic medical records, and chaotic workplaces affect burnout.
Further, regulatory environments may play a role, and it is still not known whether reducing burnout among physicians will also reduce burnout among staff. Future studies should also look at how burnout affects trainees and female physicians, he suggested.
“The link between burnout and adverse patient outcomes is stronger, thanks to the work of Panagioti and colleagues,” Dr. Linzer said.
“With close to half of U.S. physicians experiencing symptoms of burnout, more work is needed to understand how to reduce it and what we can expect from doing so,” she added.
The study was funded by the United Kingdom NIHR School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre. The authors and commenters reported no relevant conflicts of interest. ■
SOURCE: Panagioti M et al. JAMA Intern Med. 2018 Sept 4. doi: 10.1001/ jamainternmed.2018.3713.
PERSPECTIVE
What’s your bottom line?
The importance of leadership for organizational success seems obvious to me. It is my opinion that leaders shape culture and cultural changes impact the bottom line. I ask you, what is your bottom line? More specifically, what is the bottom line required to effect urgent change to the threat of (vascular) surgeon burnout? If not simply for the threatened well-being of our friends and colleagues, or for the risk of lost revenue, surgeon recruitment and retention, I urge you all to consider the immediate threat to patient safety and satisfaction.
Dawn M. Coleman, MD is Program Director, Integrated Vascular Surgery Residency Program and Fellowship. University of Michigan, Ann Arbor.
Dr. Panagioti and colleagues performed a meta-analysis of 47 quantitative observational studies that included 42,473 physicians across hospital settings in an effort to examine whether physician burnout impacts core domains of health care delivery. The authors identified physician burnout as associated with an increased risk of patient safety incidents, poorer quality of care due to low professionalism, and reduced patient satisfaction, while recognizing the study limitations of high study
TRAUMA
Seven-years of vascular injury from war in Afghanistan assessed
BY MARK S. LESNEY MDEDGE NEWS FROM THE VASCULAR ANNUAL MEETING
BOSTON – At this year’s Vascular Annual Meeting, Major Jigarkumar A. Patel, MD, reported on a study that he and his colleagues did to examine the scope of vascular injury during seven years of the war in Afghanistan, including characterization of anatomic injury patterns, mechanisms of injury, and methods of acute management.
heterogeneity and only low to moderate study quality. Interestingly, residents and early-career physicians were at greater risk.
The authors conclude that “physician burnout may jeopardize patient care and that the reversal of this risk must be viewed as a fundamental health care policy goal across the globe.” Moreover, “health care organizations are encouraged to invest in efforts to improve physician wellness, particularly for early-career physicians.”
Whatever your bottom line, there appears to be an opportunity to more concisely capture the outcome of burnout on the performance of health care organizations that carefully considers patients care quality and safety outcomes. Larger scale, high-quality studies are desperately needed that reconcile systemic threats to physician wellness (i.e., inefficient workflow, excessive record-keeping, the EMR and regulatory compliance) with quality improvement. Perhaps this will drive real change.
higher than that reported in previous wars,” said Dr. Patel. “Noncompressible torso hemorrhage remains the primary cause of battlefield fatality.”
“Vascular injury is a leading cause of death and disability in military and civilian trauma, and the rate of vascular injury in modern combat is
He and his colleagues from Walter Reed National Military Medical Center, Bethesda, Md., used the Department of Defense Trauma Registry to identify U.S. military service members who sustained a battle-related vascular injury and survived to be treated at a surgical facility in Afghanistan between Jan. 1, 2009, and Dec. 31, 2015. All battle-related injuries (nonreturn to duty) were used as a denominator to establish the injury rate. Mechanism and anatomic distribution of injury,
Afghanistan continued on page 19
DR. PATEL
VTE unchanged by postdischarge rivaroxaban
BY WILL PASS REPORTING FROM THE ESC CONGRESS 2018
For patients hospitalized for medical illness, giving rivaroxaban after discharge does not significantly reduce the risk of venous thromboembolism, reported Alex C. Spyropoulos, MD, of Hofstra University in Hempstead, N.Y., and his colleagues.
Previous research suggested that the risk of major bleeding from rivaroxaban outweighed its benefits; however, major bleeding was uncommon in the MARINER trial. “Patients who are hospitalized for acute medical illnesses, such as heart failure, respiratory insufficiency, stroke, and infectious or inflammatory diseases, are at increased
TERUMO
risk for venous thromboembolism,” they wrote in the New England Journal of Medicine. The results were also presented at the annual congress of the European Society of Cardiology.
Although the increased risk of thromboembolism continues for at least 6 weeks after hospitalization, postdischarge anticoagulants, such as rivaroxaban, are controversial.
“Studies of extended thromboprophylaxis have shown either excess major bleeding or a benefit that is based mainly on reducing the risk of asymptomatic deep-vein thrombosis,” the investigators wrote.
The double-blind MARINER study involved 12,019 patients who were hospitalized for medical illness and had an increased risk of venous thrombo-
embolism. Hospitalization lasted 3-10 consecutive days. Patients were randomized to receive either 10 mg of rivaroxaban daily (n = 6,007) or placebo (n = 6,012) for 45 days after discharge. Patients with renal impairment had a reduced dose of 7.5 mg rivaroxaban. Efficacy was similar in both groups. Symptomatic or fatal venous thromboembolism occurred in 50 patients (0.83%) in the rivaroxaban group, compared with 66 patients (1.10%) in the placebo group (P = .14). These findings suggest that rivaroxaban provides a minor and insignificant benefit.
Although major bleeding was slightly more common in patients receiving rivaroxaban, compared with patients receiving placebo (0.28% vs. 0.15%), the researchers suggested
ADVERTISING
that, in large populations, the marginal benefit of rivaroxaban might outweigh the increased bleeding risk. Still, the authors noted that “the usefulness of extended thromboprophylaxis remains uncertain.”
“Future studies should more accurately identify deaths caused by thrombotic mechanisms and focus on the patients who are at highest risk and who may benefit from anticoagulant prophylaxis,” they wrote.
Funding was provided by Janssen Research and Development. Most of the study authors reported fees or grants from Janssen. ■
SOURCE: Spyropoulos AC et al. N Engl J Med. 2018 Aug 26. doi: 10.1056/NEJMoa1805090.
INDUSTRY INFO SPONSORED PRODUCTS AND INDUSTRY NEWS
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES – INTRODUCING RADIAL TO PERIPHERAL (R2P™) by TERUMO From the leaders in radial access, Radial to Peripheral (R2PTM) is the first and only portfolio of longer-length radial devices specifically designed for peripheral procedures, including Above-the-Knee (ATK) and PAD/CLI vascular interventions.
With the introduction of R2P™, TERUMO continues to advance procedural solutions, enabling physicians to utilize a comprehensive radial to peripheral approach to perform more peripheral procedures for more patients:
• Optimize entry site management with Slender Technology™
• Enable the potential for quicker ambulation, improved patient comfort, and satisfaction
• May increase cath lab efficiencies and decrease overall costs per procedure
o Coming in 2018—contact a TERUMO representative for availability
Indications
The MISAGO® RX Self-expanding Peripheral Stent is indicated to improve luminal diameter in symptomatic patients with de novo or restenotic lesions or occlusions of the Superficial Femoral Artery (SFA) and/or proximal popliteal
artery with reference vessel diameters ranging from 4 to 7 mm and lesion length up to 150 mm.
Important Safety Information
Do not use this device in pregnant patients or patients who may be pregnant, patients who exhibit angiographic evidence of severe thrombus in the target vessel or lesion site before/ after undergoing Percutaneous Transluminal Angioplasty (PTA) procedure, patients with contraindication to antiplatelet and/or anticoagulation therapy, patients with known allergy to nickel-titanium alloy, gold or contrast media, vessels in which there may be a residual stenosis of 50% diameter or larger in the target vessel after the planned intervention, a lesion that is within an aneurysm or an aneurysm with a proximal or distal segment to the lesion, a lesion through which a guide wire cannot pass. This device should only be used by a physician who is familiar with, and well trained in, Percutaneous Transluminal Angioplasty (PTA) techniques and stent implantation.
• TR BAND® Radial Compression Device o Regular 24 cm and Long 29 cm
Discover what’s next in peripheral intervention--learn more at www.terumois.com/r2p
RX ONLY. Refer to the product labels and package insert for complete warnings, precautions, potential complications, and instructions for use.
Senior vascular residents, firstyear vascular fellows and distinguished faculty from both regional and national training programs came together for a hands-on skills course on Sept. 13-15 at Weill Cornell Medicine for the 3rd Annual Big Apple Bootcamp.
The event was sponsored by the Division of Vascular and Endovascular Surgery at NewYork-Presbyterian Hospital/Weill Cornell Medicine and endorsed by the New York Society for Vascular Surgery. The event, which was held in SAIL (Skills Acquisition and Innovation Laboratory), was led by Darren Schneider, MD, Chief of Vascular and Endovascular Surgery and Sharif Ellozy, MD, Associate Professor of Clinical Surgery, Division of Vascular and Endovascular Surgery, in the role of Bootcamp Director.
The vascular skills course provided a thought-provoking and fast-paced exchange of ideas and surgical technique by renowned faculty from regional and national training programs. The goal of the course was to provide participants with a foundation for success in their training and beyond.
Over the two-day course, trainees participated in open surgical simula-
Afghanistan
continued from page 17
as well as the acute management strategies of revascularization, ligation, and use of endovascular techniques were defined, according to Dr. Patel.
Compared to their previous study from 2002 to 2009, the current results over the past 7 years show an apparent increase in the rate of vascular injury from 12% to 17%. They found 3,900 service members who sustained a battle-related injury, of whom 685 patients (17.6%) had 1,105 vascular injuries (1.6 vascular injuries per patient). Extremity trauma accounted for the majority of vascular injuries (72%), followed by the torso (17%) and cervical (11%) regions. Lower-extremity vascular injury was the most prevalent anatomic location (45%).
tion using both cadavers and models, endovascular simulation using multiple platforms, planning workshops, arterial closure workshops, and hands-on device deployment.
Overall, Big Apple Bootcamp proved to be a memorable and enjoyable learning experience for all. ■
The cause of the injuries were explosion with fragment penetration (70%) and gunshot wounds (30%).
Open repair was performed in 60% of cases, whereas ligation was the initial management strategy in 38%. Diagnostic angiography was used in 374 cases and endovascular techniques as a form of definitive repair were used in 24 cases (3%). Overall mortality of the vascular injury cohort was 5%.
“Our study showed that open reconstruction is performed in half of cases, with diagnostic angiography being common and endovascular repair now used in nearly 10% of cases. This means that proficiency with open and endovascular methods of vascular injury management remains a critical need for the U.S. military and will require partnership with civilian institutions to attain and maintain,” Dr. Patel and his colleagues concluded. ■
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis is indicated for the treatment of de novo or restenotic lesions found in iliac arteries with reference vessel diameters ranging from 5 mm – 13 mm and lesion lengths up to 110 mm, including lesions at the aortic bifurcation.
CONTRAINDICATIONS: Do not use the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at goremedical.com for a complete description of all contraindications, warnings, precautions and adverse events.
Participants learned and had fun at the 2018 Big Apple Bootcamp, a hands-on skills course featuring renowned faculty from regional and national training programs.