

Making waves
SONOGRAPHY RESEARCH
Contributors
Matt Adams, AFASA

Matt trained as a clinical vascular scientist in the UK, where he worked with the vascular studies team at the Royal Free Hospital. After 5 busy years scanning, helping with teaching and assisting in research conducted by the University College London, Matt made the move to Australia in early 2017, where he is now in charge of the Camperdown Vascular Lab in Sydney.
Julie
Archbold

A general sonographer with over 25 years of clinical experience, Julie has been involved in all areas of ultrasound education, including training postgraduate students, delivering ultrasound undergraduate lectures at Monash University, and providing mentorship and support to clinical supervisors and tutors. Completing a Certificate IV in Training and Assessment in 2017, Julie has a keen interest in the support and training of clinical supervisors and training program accountability and is passionate about supporting training processes for the next generation of sonographers. Julie was the recipient of the Sonographer of the Year – Victoria, awarded in 2019. She is a member of the ASA Board and serves on the ASA SIG Clinical Supervision Committee.
Deborah Carmody, AFASA

Deb Carmody holds a Master of Medical Sonography from the University of South Australia. She has been actively engaged in advancing musculoskeletal ultrasound practice, serving on the ASA’s MSK SIG, and previously chairing the committee. Deb is also the head of ultrasound marketing for Asia-Pacific and Japan at Siemens Healthineers, based in Brisbane, where she focuses on education, innovation, and supporting the sonography community.
Heath Edwards, FASA

Heath is a general sonographer with a subspeciality in vascular ultrasound. He practises clinically with Queensland Vascular Diagnostics and at the Royal Brisbane and Women’s Hospital. Additionally, he serves as a sessional tutor at Central Queensland University, chairs the ASA Vascular Special Interest Group, and is a fellow of the ASA. Heath has a strong interest in correlating ultrasound findings with patient symptoms to support accurate diagnosis and management.
Emma Jardine, AFASA

Emma is a senior sonographer working in Victoria. She has a passion for professional growth and believes that investing in ongoing education and training will benefit individual sonographers, contribute to better patient outcomes and overall healthcare experience.
Assoc Prof Michelle Fenech, FASA

Assoc Prof Michelle Fenech is a sonographer, teaching scholar and active researcher based at Central Queensland University (Brisbane campus) where she is the head of course of post graduate medical sonography studies. She is the chair of the ASA MSK Special Interest Group (SIG) and a member of the ASA Research SIG and has a keen interest in anatomy and musculoskeletal sonographic imaging and is involved in researching and teaching these topics. She holds a principal teaching fellowship with AdvanceHE and HERDSA fellowship (Higher Education Research and Development Society of Australasia). Michelle is passionate about the sonographic profession and key professional issues including developing a strong sonographer professional identity, models of sonographer training, extended scope of practice, and the development sonographer career framework.
Fiona Hilditch

Fiona is a dedicated healthcare professional with 16 years of radiology experience in radiation therapy, mammography, breast ultrasound, and cancer support. For the past 9 years, she has worked in 2 leading tertiary breast imaging clinics in Brisbane. Passionate about women’s imaging, she has built strong expertise in breast imaging and oncology-related radiology. Fiona is committed to patient-centred care, quality assurance, training, and best practices. She thrives in multidisciplinary teams, working to improve departmental systems and processes. Her goal is to help create advanced radiology departments known for high quality imaging and compassionate, skilled teams.
Contributors
Sara Kernick

Sara Kernick is currently the chief sonographer at the Royal Children’s Hospital in Melbourne, where she has worked for over 20 years after returning home from working at Great Ormond Street Hospital for Children in London.
Since returning, she has tried her hand at many varied roles in sonography, including women’s imaging and corporate applications, but the call of paediatric sonography is all too compelling. Her hot topics are paediatric hip, liver transplantation and sonographer education.
Ilona Lavender, FASA

Ilona Lavender, FASA, is the lead clinical educator of imaging at Monash Health. She has served as a tutor sonographer for several years, building a strong foundation in clinical education, mentoring, and leadership.
Ilona is deeply passionate about teaching and education, with a strong focus on fostering collaboration among healthcare professionals to enhance learning outcomes and improve patient care. She is currently interested in the integration of AI and simulation into healthcare education, recognising their potential to transform clinical practice and outcomes.
Ilona has performed numerous audits and presented frequently over the years.
She has served on multiple committees, including the SIG for Paediatrics and the Clinical Supervisors Committee. Additionally, Ilona is an associate lecturer at Monash University, where she specialises in obstetric imaging.
Ling Lee, AFASA

Ling Lee AFASA is a clinical sonographer specialising in maternal-fetal medicine and women’s health. Following a rewarding period as a clinical educator for rural and regional sonographers, she has returned to active clinical practice, bringing extensive expertise from both public tertiary and private settings to frontline patient care. Ling remains committed to the profession’s advancement through her ongoing research, which applies a socialpsychological lens to improve support for future sonographers. A dedicated volunteer and mentor, she views research and service as essential pillars of clinical practice, ensuring the continued growth and excellence of the sonography profession.
Glenda McLean, FASA

Glenda McLean, FASA, is a sonographer with a specialist interest in neonatal intensive care ultrasound, particularly cranial imaging. She is a PhD candidate at Monash University, investigating cranial ultrasound screening protocols in preterm neonates.
Glenda was the imaging research and knowledge translation lead at Monash Health and Peninsula Health until 2025, and has held senior clinical and teaching roles, including in the Master of Medical Ultrasound program at Monash University. She has presented nationally and internationally and currently serves on the Editorial Boards of Sonography (Australasian Sonographers Association) and Ultrasound (British Medical Ultrasound Society).
Amber Mohacsy

Amber is a sonographer working in private practice in Victoria. Amber is a passionate advocate for women’s health.
Donna Napier, FASA

Donna Napier, FASA, is a radiographer/ sonographer and the acting sonography section manager at Tweed Valley Hospital in northern NSW, with over 24 years of industry experience. She holds a Master in Medical Sonography and is a Fellow of the Australasian Sonographers Association (FASA). Donna has a strong passion for education and is an advocate for expanding the sonographer’s scope of practice. She is a frequent conference presenter and author of multiple ultrasound publications. Donna has a keen interest in emergency ultrasound applications and, more recently, in the use of ultrasound to improve men’s health outcomes.
Kim Prince

Kim is a lecturer in the echocardiography course at Central Queensland University and a professional development manager at ASA, and brings nearly 2 decades of clinical experience in cardiac sonography.
Kim is passionate about fostering excellence in echocardiography education, teaching both undergraduate students and qualified sonographers. Her career spans clinical practice in public and private sectors across Australia and internationally, providing her with a broad perspective on patient care and imaging standards.
Kim has served as an examiner for the Diploma of Medical Ultrasound (DMU) and previously tutored in the postgraduate echocardiography course at QUT. Kim is particularly interested in the integration of emerging technologies – such as strain imaging, artificial intelligence, and advanced sonographic modalities into clinical practice and education.
Contributors
Dr Jacqueline Roots

Dr Jacqui Roots is a research sonographer and lecturer at QUT, as well as a sonographer at the Herston Imaging Research Facility in Brisbane. Jacqui’s PhD was titled ‘Shear wave elastography to assess the change in stiffness of muscles in the acute stage post-stroke’. She is currently involved in numerous research projects with a focus on musculoskeletal imaging and biomechanics, as well as artificial intelligence and CMUT technology.
Louise Smith

Louise Smith is a clinical nurse consultant and cardiac sonographer specialising in critical care echocardiography at Nepean Hospital’s Intensive Care Unit and Cardiac Diagnostic Department. She integrates expertise in echocardiography and intensive care nursing to optimise care for critically ill patients. Louise is an accredited assessor for basic echocardiography with the College of Intensive Care Medicine and a clinical supervisor for cardiac sonography students. Passionate about education and leadership, she empowers healthcare professionals and students across multidisciplinary teams through teaching, research, and mentorship, fostering clinical excellence and advancing knowledge locally, nationally, and internationally.
Christopher Thomas

Christopher Thomas graduated from The University of Queensland in 1997 with a Bachelor of Applied Science in Human Movement Studies and completed a Master of Scientific Studies specialising in cardiac physiology and rehabilitation. He manages and is the senior cardiac sonographer at Queensland Echocardiography, a standalone and fully accredited echocardiography imaging service – the first of its kind in Queensland. In addition to presenting original research at the World Congress of Cardiology in 2002, Christopher has been involved in numerous research initiatives associated with emerging technologies, including ASD/VSD closure devices, ventricular assist devices, and transcatheter heart valve replacements and interventions.
Keith VanHaltren

Keith VanHaltren is currently the ultrasound supervisor at the Monash Children’s Hospital in Melbourne and a sessional lecturer in paediatric ultrasound at Monash University. He is passionate about paediatric ultrasound and has a particular interest in neonatal cranial ultrasound. Keith has been employed at Monash Health for the past 10 years, where he has enjoyed working in the tertiary paediatric, fetal diagnostic and vascular services. Keith has presented at numerous local, state and national conferences and has been involved in several peer-reviewed publications in international journals.
Jane Wardle

Jane Wardle is a dedicated educator and senior lecturer at CQUniversity. With a clinical background in radiography and sonography, she has extensive experience in healthcare and academic leadership. Jane is passionate about advancing sonographer education with self-compassion and reflective practice, emphasising patientcentred care, and fostering critical thinking in her students. A lifelong learner, Jane is about to complete a Master of Educational Neuroscience, combining her interests in teaching and the science of learning to enhance student outcomes, which in turn impacts patient outcomes.
Marilyn Zelesco, AFASA

Marilyn Zelesco, AFASA, is a Western Australian-trained diagnostic radiographer who gained a postgraduate ultrasound qualification in 1991. Marilyn completed her Master in Ultrasound through the Royal Melbourne Institute of Technology in 2007.
Marilyn has received professional awards from the Australian Institute of Radiography, the Australasian Sonographers Association and the Australian Society for Ultrasound in Medicine.
Marilyn is the lead sonographer at the Fiona Stanley Hospital in Perth. Marilyn has an interest in hepatic, bowel and male reproductive tract ultrasound, elastography, CEUS, renal transplants, research, education and sonography in Indigenous healthcare.

CLINICAL SUPERVISORS
What makes a good clinical practice experience in radiography and sonography? An exploration of qualified clinical staff and student perceptions 6
CLINICAL SUPERVISORS
Body painting, ultrasound, clinical examination, and peer teaching: A student-centered approach to enhance musculoskeletal anatomy learning 8
VASCULAR
New 3-dimensional volumetric ultrasound method for accurate quantification of atherosclerotic plaque volume 9
VASCULAR
Ultrasound characteristics and risk factors of female patients with pelvic varicose veins and concomitant chronic pelvic pain 10
MSK
Comparative study between MRI and ultrasound in articular affection of rheumatoid arthritis 11
MSK
High-resolution ultrasound of clinically relevant sensory nerves of the arm and the forearm 12
HEALTH AND WELLBEING
Improving the process of second trimester singleton morphology sonography examinations. A survey of Australian and New Zealand sonographers 13
HEALTH AND WELLBEING Emotion and feedback influence the learning landscape in sonography 14
WOMEN’S HEALTH
Value of automated breast ultrasound in screening: Standalone and as a supplemental to digital breast tomosynthesis 15
WOMEN’S HEALTH
Transvaginal ultrasound for detecting parametrial involvement in suspected deep pelvic endometriosis: updated meta-analysis 17
PAEDIATRIC
Non-visualization of the ovaries on pediatric transabdominal ultrasound with a nondistended bladder: Can adnexal torsion be excluded? 18
PAEDIATRIC
Ultrasound as the first line investigation for midgut malrotation: a UK tertiary centre experience 19
RESEARCH
Participatory Action Research-Dadirri-Ganma, using Yarning: methodology co-design with Aboriginal community members 20
RESEARCH
Facilitators and barriers to undertaking research into the practice and delivery of clinical ultrasound: A qualitative investigation 22
GENERAL
Ultrasound measurement of perirenal adipose tissue indicates cardiovascular disease, but standardisation is needed: A systematic review 23
GENERAL
Ancillary US of the bowel: Endovaginal US, contrast-enhanced US, and elastography 24
CARDIAC
Recommendations for the evaluation of left ventricular diastolic function by echocardiography and for heart failure with preserved ejection fraction diagnosis: An update from the American Society of Echocardiography 25
CARDIAC
Strain reversus sign: Diagnostic role and correlation with cardiac magnetic resonance findings in constrictive pericarditis 27
EMERGING TECHNOLOGIES
Offline ultrasound–MRI fusion imaging for assessment of normal fetal brain development 29
© Australasian Sonographers Association 2026. Disclaimer: The information in this publication is current when published and is general in nature; it does not constitute professional advice. Any views expressed are those of the author and may not reflect ASA’s views. ASA does not endorse any product or service identified in this publication. You use this information at your sole risk and ASA is not responsible for any errors or for any consequences arising from that use. Please visit www.sonographers.org for the full version of the Australasian Sonographers Association publication disclaimer.
What makes a good clinical practice experience in radiography
and sonography? An exploration of qualified clinical staff and student perceptions
Why the study was performed
The study was performed to have a better understanding of what makes a high quality clinical practice experience in medical imaging, from radiography student, sonography student and qualified clinical staff perspectives.
The article’s key features were:
• to explore the factors that influence student learning and satisfaction during clinical placement
• to identify the common challenges as well as the positive factors that both educators and learners experience
• to explore future improvement in clinical education – this includes effective, supportive clinical placements.
How the study was performed
A structured interview approach was used in this study, where participants could share their personal experiences. Participants were recruited through Invitational Theory across clinical placement sites affiliated with one UK university and its students. A total of 25 participants took part in the study – 15 students and 10 qualified clinical staff – drawn from a range of clinical settings to capture diverse perspectives. The data was analysed thematically, identifying recurring patterns and themes related to both barriers to learning and factors that supported effective clinical education.
What the study found
Thematic analysis revealed four key themes that influenced the clinical practice experience in radiography and sonography.
1. Favourable and unfavourable traits
• several students identified specific qualities in clinical staff that had a positive impact
on their learning. Key attributes considered essential for effective supervision included being approachable, supportive, friendly, patient, and caring.
• student quote: ‘… one of the most important things is for them to be approachable … We want to feel comfortable and confident asking them for help …’
2. Creating an optimal learning environment
• students noted that certain clinical staff promoted an environment that supported and encouraged learning.
• student quote: ‘He takes out the time from his day just that he’ll sit down and will go over everything …, he goes beyond that so if there’s something I don’t understand he’ll explain and then he’ll be like you need to go home, revise, go over this topic and then come back to me tomorrow.’
3. Challenges
• qualified staff cited time pressures and workload as key challenges to providing effective student support.
• qualified quote: ‘Having an opportunity to have some time with them so that you can let them know what you expect from them and vice versa, what they expect. You want to ask questions but they’re busy. They are always busy. It’s almost impossible even to sit down at the end of the three weeks.’
4. Considerations for clinical education
• students emphasised the importance of supervisor training for a successful learning experience. They noted gaps in training, with some supervisors lacking understanding of the clinical practice document or not prioritising student support.
• student quote: ‘I don’t think anything’s been put in place. I feel there should be stuff to put in place, train the staff members for different students.’
CLINICAL SUPERVISORS
Reviewer: Ilona Lavender, FASA
Authors: Khine R, Harrison G, Flinton D. Radiography. 2024; 30, (1): 66-72
Open Access: Yes
Read the full article here
‘The relationship with the student is key – if they feel supported, they will thrive.’
What makes a good clinical practice experience in radiography and sonography? An exploration of qualified clinical staff and student perceptions (continued)
Perceptions of an optimal clinical practice experience can be understood through the lens of the five ‘P’ domains of Invitational Theory, which offer a framework for creating supportive and inclusive learning environments.
1. People – The attitudes and behaviours of individuals, particularly clinical educators and peers, play a key role in shaping the learning experience.
2. Places – The physical and emotional environment of the clinical setting influences how safe, supported, and engaged students feel.
3. Policies – Institutional and departmental policies impact the structure, expectations and consistency of clinical education.
4. Programs – The design and delivery of educational programs, including supervision models and learning opportunities, affect student development.
5. Processes – Day-to-day interactions, feedback mechanisms, and communication strategies contribute to a student’s ability to learn and grow.
Relevance to clinical practice
The findings of this study are highly relevant to sonographers, as they highlight the critical role of supportive supervision, structured learning environments, and effective communication in shaping student development.
By understanding what contributes to a positive clinical experience, educators and departments can implement targeted strategies to enhance student engagement, confidence, and competence – ultimately improving workforce readiness and patient care outcomes.
Body painting, ultrasound, clinical examination, and peer teaching: A student-centered approach to enhance musculoskeletal anatomy learning
Why the study was performed
The study was introduced to secondyear medical students to assess whether incorporating ultrasound, body painting and clinical examination of upper and lower limb anatomy in addition to peer teaching would enhance current approaches to anatomical learning of deep and superficial musculoskeletal structures. The aim was to explore how these learning methods were accepted by students and how they affected their understanding of applied anatomy.
How the study was performed
The course curriculum was developed to create an environment where students were motivated and engaged with learning processes through teaching lectures, group peer presentations and practical sessions. Teams of three to four students rotated through stations utilising body painting, ultrasound and clinical examination of limb joints. Ultrasound was performed on the opposite limb during painting to reinforce anatomical relationships. These stations utilised self-directed and team-based learning with the supervision of a teaching surgeon. The practical sessions were enhanced by team presentations prepared during the sessions and a reflective diary to foster self-reflection and promote deeper learning. A final exam included both description and drawing of anatomy. Students were invited to complete an anonymous questionnaire combining Likert-type scale and free-text questions to ascertain their perception of the activities and how they perceived the activities impacted their learning of anatomy.
What the study found
Students reported high engagement, with most finding the course helpful and that it was well perceived. Prior knowledge of anatomy was considered beneficial, but most would recommend the course to younger students. The importance of learning anatomy without the ‘sectioning’ that is present in anatomical textbooks and anatomy lab specimens was thought to be particularly useful. The body painting promoted a transfer of knowledge from 2D structures to a 3D understanding and was thought to enhance deeper learning. Ultrasound was appreciated as the most useful task in the understanding of anatomy; however, it was considered the most difficult due to the lack of experience.
Relevance to clinical practice
Effective knowledge building requires a combination of traditional teaching with student-centred and peer learning to enhance learning outcomes. The hands-on methods in this study, which combined team-based learning with body painting, ultrasound and clinical examination, could be a valuable integration to either university coursework or clinical placements for ultrasound students. Developing presentation skills through peer teaching increases confidence and fosters professional growth with benefits to the wider sonography community. Emerging teaching approaches that complement historical methods are part of a continuing need to adjust learning processes to benefit individual and generational learning needs. This dynamic and collaborative approach, supported by a reflective diary, has the potential to enhance engagement, deepen anatomical knowledge and improve clinical application when scanning.
CLINICAL SUPERVISORS
Reviewer: Julie Archbold
Authors & Journal: Bilella A, Eppler E, Link K, Filgueira L. Anat Sci Educ. 2024; 17: 157–172
Open Access: Yes
Read the full article here
‘Learning is considered as a social process embedded within a social context as students and teachers work together to build knowledge.’
New 3-dimensional volumetric ultrasound method for accurate quantification of atherosclerotic plaque volume
Why the study was performed
Using ultrasound to generate 3D images is not a new technology, and regrettably, there remains no regular clinical use of 3D techniques within vascular ultrasound in Australia. The aim of this study was to test the accuracy of a new 3D matrix transducer that utilises an electronic sweep during image acquisition. The main benefit of this transducer is that it has a smaller footprint, which allows for superior imaging at angular surfaces and in small fields of view while also allowing it to be manipulated more easily during ultrasound exploration.
How the study was performed
This study was split up into two parts: ex vivo and in vivo.
The ex vivo arm of the study used excised segments of porcine femoral and carotid arteries placed into a phantom to test the accuracy of the 3D matrix probe with electronic sweep for quantifying plaque volume. The pigs had upregulation of specific liver enzymes, allowing arterial stenoses that resemble those found in humans to be generated when fed a high cholesterol diet. Histological samples were placed in a phantom because they are located quite deep in the adult pig, which would limit ultrasound interrogation in vivo. 3D volume assessment was then carried out on 49 phantoms, which consisted of 23 carotid and 26 femoral arteries.
The in vivo part of the study tested the accuracy of the 3D matrix probe with electronic sweep against an already validated 3D matrix probe that uses a mechanical sweep. Both probes were used to look at the femoral and carotid territories of 20 cardiovascular diseasefree individuals.
What the study found
When compared directly against histology samples, 3D volume quantification utilising the electronic sweep demonstrated a systematic bias in slightly overestimating plaque volume, which was more marked when analysing larger lesions. Despite this, 3D volume assessment was overall deemed excellent.
Agreement between the 2 types on 3D volume measurement tested in the in vivo part of the study was statistically excellent, as were rates on both inter- and intra-observer reliability.
Relevance to clinical practice
The vascular subspeciality of ultrasound has largely not adopted any 3D techniques despite rapid advancement in both hardware and software over the past decade. This study further proves the accuracy of 3D ultrasound when it comes to measuring arterial plaque volume, which may represent a new paradigm in assessing plaque burden.
The combination of the continuous data type associated with plaque volume measurement, paired with the relative ease of use that 3D ultrasound offers, may represent a particularly powerful tool when it comes to screening for cardiovascular risk.
VASCULAR
Reviewer: Matt Adams, AFASA
Authors & Journal: Lópes-Melgar B, Mass V, Nogales P, Sánchez-González J, et al. J Am Coll Cardiol Img. 2022; 15 (6) 1124–1135
Open Access: Yes
Read the full article here
‘Three dimensional vascular ultrasound (3DVUS) using new matrix transducer technology, together with improved 3D plaque quantification software, simplifies the accurate volume measurement of early (small) and intermediateadvanced plaques located in carotid and femoral arteries.’
Ultrasound characteristics and risk factors of female patients with pelvic varicose veins and concomitant chronic pelvic pain
Why the study was performed
Pelvic venous disorders (PeVDs) are being more frequently linked to patients suffering from chronic pelvic pain, which is defined as pain lasting greater than six months. This study was performed to investigate the ultrasound characteristics of patients with chronic pelvic pain, pelvic varicose veins and subsequent peVD.
How the study was performed
The study was performed retrospectively, with the clinical and ultrasound data collected from female patients diagnosed with pelvic varicose veins between December 2017 and October 2022 from a single hospital site.
The inclusion criteria required the patient to be 18 years old or greater, have a previous transvaginal ultrasound that suggested greater than 4 mm unilateral or bilateral parauterine and perivaginal vein diameters, and the voluntary completion of the Chronic Pelvic Pain Assessment Form.
The assessment form collected a range of general data, including age, height, body mass index, age of menarche, number of pregnancies and deliveries and an assessment of menstrual flow using a menstrual blood loss chart. The physical examination recorded the presence or absence of pelvic and lower limb varicose veins to determine the location and nature of the patient’s pain.
The patients were then categorised into two separate groups. The patients with pelvic varicose veins (PVV) and chronic pelvic pain (CPP) were referred to as the CPP group. The patients with PVV not combined with CPP were referred to as the non-CPP group.
The patients then undertook a transvaginal pelvic ultrasound performed
by the gynaecology team, followed by a transabdominal ultrasound performed by the vascular group to assess the renal, ovarian and iliac veins in multiple postural states.
What the study found
The study assessed a total of 236 female patients diagnosed with PVV. This included 89 patients in the CPP group and 147 patients in the non-CPP group.
The results showed that the patients in the CPP group had a wider diameter of the left ovarian vein (LOV), a higher positive rate of LOV incompetence, and a higher rate of left internal iliac vein incompetence. There was, however, no statistically significant difference in the degree of left common iliac vein compression and the nutcracker phenomenon between the two groups.
The multifactorial logistic regression analysis showed that LOV reflux, low BMI, increased menstrual flow and concomitant varicose veins are all independent risk factors for concurrent CPP in patients with PVV.
Relevance to clinical practice
Chronic pelvic pain is a debilitating affliction that affects women across the world. Pelvic venous disorders are being increasingly linked to CPP, with imaging and literature evolving rapidly in this space. This study depicts the need for ultrasound to provide a dynamic assessment of the anatomy to best understand the postural haemodynamic changes in these patients with PeVD. This will improve the diagnostic accuracy of imaging in forming a diagnosis for these patients with CPP, as well as provide improved information leading to correct treatment and management pathways. This study reiterated that LOV incompetence is still the cornerstone PeVD causing CPP in women.
VASCULAR
Reviewer: Heath Edwards, FASA
Authors & Journal: Zheng B, Liu G, Liu Y. J Vasc Surg Venous Lymphat Disord. 2025; 13(2): 102165
Open Access: Yes
Read the full article here
‘Left ovarian vein incompetence is still the cornerstone pelvic venous disorder causing chronic pelvic pain in women.’
Comparative study between MRI and ultrasound in articular affection of rheumatoid arthritis
Why the study was performed
Rheumatoid arthritis (RA) is the most common inflammatory disorder, impacting roughly 1% of the global population. There is no definitive test for diagnosing RA – rather, there are clinical signs, rheumatoid factor (RF), radiographic changes, inflammation markers (ESR, CRP), and anti-cyclic citrullinated peptide (antiCCP) antibodies. While this approach can lead to early treatment, it may also result in unnecessary therapy for some patients. Thus, developing more accurate diagnostic methods for early joint symptoms is crucial. Early diagnosis of RA is challenging, and this study aimed to compare the diagnostic accuracy of musculoskeletal ultrasound to MRI.
How the study was performed
This was a prospective comparative accuracy study from the Ain Shams University Hospital in Egypt between February 2022 and February 2023. There were 20 participants were selected with clinically and laboratory-confirmed RA, who underwent ultrasound and MRI examinations. Patients were excluded if they had evidence of radiographic joint destruction or if they had known contraindications to MRI.
What the study found
MRI and ultrasound are valuable tools in assessing RA, offering early identification of inflammation such as synovitis and tenosynovitis, with greater sensitivity than clinical examination or X-ray. Ultrasound detected synovitis in all patients, compared to only 85% with MRI, and identified tenosynovitis in 95%.
Relevance to clinical practice
This study found that ultrasound is highly effective for detecting synovitis and tenosynovitis, often outperforming MRI in early inflammatory changes. Access to MRI is not always an option; however, ultrasound is accessible, cost-effective and can detect vascularity using power Doppler, making it a practical tool for diagnosing RA, and complementing the clinical diagnosis.
Reviewer: Deborah Carmody, AFASA
Authors & Journal: Gamal N, Shalaby MH, Abdul Majeed M, Fadel IY. Rom J Rheumatol. 2025; 34(1)
Open Access: Yes
Read the full article here
‘Both ultrasound (US) and magnetic resonance imaging (MRI) successfully detect synovitis, tenosynovitis, bone erosions, and joint effusion.’ MSK
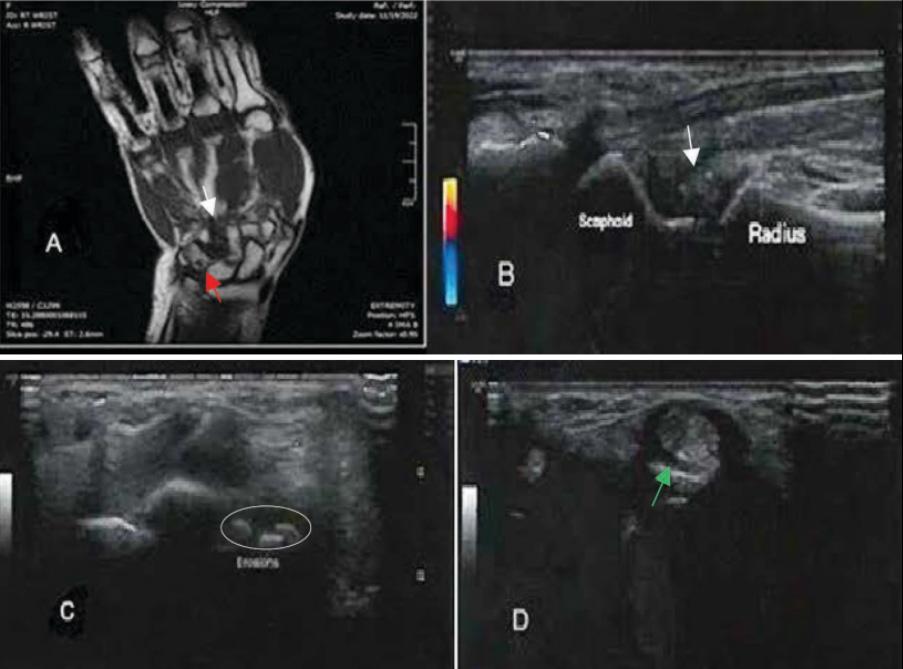
Figure 3. A 51-year-old female patient with positive rheumatoid factor. (A) Coronal T1-weighted MRI shows mild intercarpal synovial thickening (white arrow) and carpal cortical erosion (red arrow). (B) Power Doppler ultrasound (PDUS) clearly shows wrist joint synovial thickening between the radius and scaphoid (white arrows) with no detectable Doppler activity. (C) Transverse ultrasound (US) of the carpal bones shows tiny cortical bony erosions (white circle). (D) Ultrasound image shows tenosynovitis of the extensor tendon in wrist compartment III (green arrow).
Ro J Rheumatol. 2025; 34(1) pg 30
High-resolution ultrasound of clinically relevant sensory nerves of the arm and the forearm
Reviewer: Assoc Prof Michelle Fenech, FASA
Authors & Journal: Zaottini F, Picasso R, Pistoia F, Macciò M, Marcenaro G, Miguel M, Spingardi O, Barendrecht EJ, Gandikota G and Martinoli C. J Ultrasound Med. 2025; 44: 22092228
Open Access: Yes
Read the full article here
Why the review was performed
Cutaneous nerve disorders can cause sensory alterations, including pain. In the arm and forearm, they are often overlooked clinically and subsequently diagnosed late. With improvement in ultrasound spatial resolution, with very high frequency transducers (> 24 MHz), the cutaneous nerves of the upper limb are now discernible. However, as the cutaneous neural anatomy and the sonographic technique to image the cutaneous nerves of the arm and forearm are not well appreciated, sonographic imaging of these nerves is not commonly conducted. This review outlines the anatomy of cutaneous nerves of the arm and forearm and the sonographic technique to image them to allow identification and reporting of any associated cutaneous neural pathology.
What the review described
The medial cutaneous nerve of the arm (MCNA) arises from the medial cord of the brachial plexus, courses anterior to the subscapularis muscle, and descends along the medial arm between the long and medial heads of triceps initially. More distally in the arm, the MCNA overlies the medial head of the triceps and sits posterior to the ulnar nerve. At the medial epicondyle, the MCNA variably gives rise to up to five terminal branches.
The MCNF most commonly originates from the medial cord of the brachial plexus and can share a common trunk with the MCNA. The MCNF courses along the medial arm in close relationship with the basilic vein, superficial to the brachial artery and median nerve. At
the distal third of the upper arm, the MCNF bifurcates into anterior and posterior branches.
The lateral cutaneous nerve of the forearm (LCNF) is a continuation of the musculocutaneous nerve (MCN), which arises from the lateral cord of the brachial plexus. The MCN courses between the biceps brachii and brachialis muscles and gives off motor branches to these muscles. The LCNF continues distally after these branches have been given off and courses laterally to the biceps muscle. At the elbow crease, the LCNF sits between the cephalic vein and the distal biceps brachii tendon.
The posterior cutaneous nerve of the forearm (PCNF) arises from the radial nerve and follows it in the spiral groove of the posterior humerus. In the mid to distal upper arm (10cm superior to the elbow), the PCNF pierces the lateral intermuscular septum and, distal to this, diverges away from the radial nerve. The PCNF becomes superficial proximal to the elbow and courses anterior to the lateral epicondyle, travelling to the radial side of the forearm.
Relevance to clinical practice
The cutaneous nerves of the arm and forearm can encounter traumatic injuries, compressive syndromes and be affected by tumours, diffuse neuropathies and infectious diseases. They are often in the field of view of sonographic imaging of the arm and forearm. Knowledge of the anatomy and location of the cutaneous nerves of the arm and forearm relative to other structures can allow them to be sonographically located, appreciated, and associated pathology or injury detected.
‘Ultrasound should be considered as a first level diagnostic modality in cases of suspected neuropathies of the medial cutaneous nerve of the arm (MCNA), medial cutaneous nerve of the forearm (MCNF), posterior cutaneous nerve of the forearm (PCNF), and the lateral cutaneous nerve of the forearm (LCNF).’
Improving the process of second trimester singleton morphology sonography examinations. A survey of Australian and New Zealand sonographers
Why the study was performed
Second trimester morphology scans play an important role in prenatal care, providing detailed assessments of fetal development and helping to identify structural anomalies. However, these examinations are often lengthy, technically demanding, and prone to variation in scanning technique and reporting practices. Recognising these challenges, Milanese et al. undertook a study to investigate the factors contributing to prolonged scan times and workflow inefficiencies in singleton second trimester morphology assessments. The research aimed to capture the perspectives of Australasian sonographers, identifying the key obstacles they face during these appointments and exploring practical strategies to enhance the scanning process and overall clinical experience.
How the study was performed
To gather insights into the challenges, the research team developed a targeted survey for sonographers across Australia and New Zealand. The questionnaire aimed to capture the perceptions of practitioners who routinely perform these examinations, focusing on factors that contribute to appointment complexity and opportunities for process improvement. Before distribution, the survey was piloted with three practising sonographers to ensure face validity. It was then disseminated through the Australasian Sonographers Association to all currently practising sonographers and student sonographers who had commenced clinical placements, ensuring broad representation across experience levels and clinical settings.
What the study found
The survey gathered responses from 697 sonographers; over half (53.9%) reported having 60-minute appointment slots for these examinations, and 23.4% allocated 40 minutes. Sonographers identified a range of factors that made these appointments challenging. These were categorised into five key themes: modifiable patient-related factors, nonmodifiable patient-related factors, modifiable scan-related factors, non-modifiable scanrelated factors, and modifiable clinic-related factors, as outlined in Table 1.
Table 1: Factors contributing to challenging appointments Category Challenges encountered
Modifiable patient-related factors
Non-modifiable patient-related factors
Modifiable scanrelated factors
Non-modifiable scan-related factors
Modifiable clinicrelated factors
HEALTH AND WELLBEING
Reviewer:
Emma Jardine, AFASA
Authors & Journal: Milanese S, Farley A, Lamb K, Perry R. Sonography. 2025; 12(4): 489-495.
Open Access: Yes
Read the full article here
These included issues such as late arrivals, language barriers, distractions (e.g. children in the room), and inadequate patient preparation. While these factors may not be entirely preventable, their impact can be mitigated through better planning and communication.
These encompassed maternal body habitus, fetal position, placental location, and gestational age, elements that cannot be changed but significantly influence scan complexity and duration.
These included administrative inefficiencies, unclear protocols, and the need for transvaginal scans. Improvements in workflow and clearer expectations could help address these.
These involved the detection of abnormalities, complex pathologies, or the need for additional imaging or referrals, factors that extend scan time.
These included the quality of ultrasound equipment, staffing levels, and the presence of students requiring supervision.
Importantly, over half the respondents felt that current appointment times negatively impacted scan quality, particularly during complex cases. In response, the authors advocate for a review of appointment scheduling practices. They recommend that any future redesign be grounded in a user-driven and cooperative approach to ensure the process is clinically effective, practically useful, and supportive of both scan quality and sonographer wellbeing. To address these challenges, several practical improvements were suggested by the authors, as noted in Table 2.
Table 2: Suggested improvements to address appointment challenges
‘Reviewing and optimising scheduling practices may enhance healthcare quality and support better work-life balance for sonographers.’
Solutions for identified challenges Strategy to enhance appointment efficiency
Flexible appointment scheduling Triaging patients based on complexity (e.g. high BMI, language needs, previous surgeries) and allowing longer appointments for more complex cases.
Enhanced patient preparation Encouraging punctuality, discouraging the attendance of unsupervised children, and ensuring patients understand the importance of the scan and what to expect.
Protocol and workflow review Allocating time for non-scanning tasks such as reviewing referrals, obtaining consent, and completing reports. Incorporating evolving best practices, such as routine cervical length assessment via transvaginal ultrasound, was also recommended.
Relevance to clinical practice
In busy clinical environments, particularly those with staffing pressures or high patient volumes, re-evaluating how appointment times are scheduled is important. By incorporating the perspectives of end users, such as sonographers, this process can lead to the delivery of high quality ultrasound services while supporting the wellbeing and sustainability of the sonography workforce.
Emotion and feedback influence the learning landscape in sonography
HEALTH AND WELLBEING
Reviewer: Jane Wardle
Authors & Journal: Oomans D, White A, Thomas S, Robinson C, Clarke J. Health Educ Pract. 2025; 8(1)
Open Access: Yes
Read the full article here
Why the study was performed
The study was conducted to address a noticeable gap in the sonography education literature – specifically, the under representation of the affective domain (emotion, empathy, communication) in peer learning contexts. While much is known about cognitive and psychomotor skill development in medical imaging, less is understood about how emotions and feedback shape learning experiences, particularly for complex tasks like arteriovenous fistula (AVF) ultrasound examinations. As sonographers must continually adapt to emerging technologies and techniques, understanding how emotional states and feedback influence skill acquisition becomes critical for improving both educational practices and patient care outcomes.
How the study was performed
The research synthesised data from two previous studies: a national survey and semi-structured interviews with Australian sonographers. Fifty sonographers completed the survey, and 16 participated in interviews. Recruitment occurred via the Australasian Sonographers Association. The survey explored initial learning methods, confidence, and perceived competence, while interviews examined experiences within the learning landscape, feedback reception, and emotional responses. Interviews were transcribed and analysed thematically using NVivo software, with triangulation between survey and interview data to ensure validity.
What the study found
Three major themes emerged: the impact of the learning landscape, the role of feedback, and the interplay between confidence and
competence. The learning landscape was categorised as well-supported, limited support, or ‘sink or swim’. Participants who received structured, ongoing support reported positive attitudes and higher confidence, whereas those with minimal or no support often expressed negative feelings and lower perceived competence. Feedback was identified as either extrinsic (from supervisors) or intrinsic (self-initiated). While proactive feedback seeking correlated with improved performance and reflective practice, many participants reported feedback as infrequent, evaluative rather than developmental, or absent altogether. Alarmingly, some sonographers equated increased case numbers with skill mastery, despite limited understanding of AVF physiology, highlighting risks of overconfidence and compromised patient care.
Relevance to clinical practice
The findings underscore the critical role of emotional support and structured feedback in sonography education. A positive learning environment reduces cognitive and emotional load, fostering deeper learning and professional growth. Conversely, inadequate support and poor feedback practices can perpetuate negative attitudes, hinder skill acquisition, and jeopardise patient outcomes. For clinical supervisors, the study advocates adopting scaffolding strategies, promoting feedback literacy, and encouraging reflective practice. Organisations must prioritise resources for supervisor training and feedback culture, recognising that effective supervision is integral to maintaining high standards of person-centred care. Ultimately, this research highlights that technical competence alone is insufficient; emotional resilience and constructive feedback are essential for safe, high quality sonographic practice.
‘The learning landscape significantly influences how learners perceive taught skills and process acquired knowledge. The importance of pedagogical support and resources for both peers and learners, in the areas of the affective domain and feedback literacy, is imperative in peer learning situations to optimise the learning experience.’
Value of automated breast ultrasound in screening: Standalone and as a supplemental to digital breast tomosynthesis
Reviewer: Fiona Hilditch
Authors & Journal: Aribal E, Seker ME, Guldogan N and Yilmaz E. Int J Cancer. 2024; 155(8): 1466-1475.
Open Access: Yes
Read the full article here
Why the study was performed
The study aimed to evaluate automated breast ultrasound (ABUS) as a screening tool for women with dense breasts (BI-RADS B–D), where 2D mammography and even digital breast tomosynthesis (DBT) have reduced sensitivity. ABUS may overcome these limitations by being less affected by density, standardised, and capable of detecting cancers missed by other modalities. The objectives were to:
1. assess ABUS as both a standalone and supplemental screening method
2. compare its diagnostic performance –detection rates, sensitivity, specificity, and recall rates – with DBT
3. determine whether ABUS could enhance or replace mammography-based screening, particularly for dense breasts or limitedresource settings.
How the study was performed
This prospective screening study included 3,466 women aged ≥ 39 years (mean age 50) at a breast imaging clinic in Istanbul (November 2018 to December 2020).
Participants attended opportunistic screening via physician referral, hospital check-ups, or insurance programs. Exclusion criteria were breast symptoms, pregnancy, lactation, prior surgery or implants, recent mammogram (< 12 months), refusal of either test, or ACR A (fatty) breasts.
Screening Procedures:
• DBT: 3D MLO with 2D synthetic MLO and CC views (GE Senographe Pristina Machine)
• ABUS: GE Invenia system, performed by trained technicians with ≥ 3 projections per breast (AP, LAT, MED).
Image interpretation: DBT images were double-read; ABUS was read independently by a blinded radiologist. BI-RADS (5th ed.) guided categorisation, with consensus on final results. True-positive 2D mammograms were retrospectively reviewed by two radiologists for detectability comparison.
Risk and staging: Breast cancer risk estimated using the NCI Breast Cancer Risk Assessment Tool (5-year and lifetime risk) and AJCC guidelines used for cancer staging.
What the study found
1. participants: 3,466 women (mean age 50 +/- 8.6 years), with 31 cancers detected
2. ABUS detected the same number of cancers as DBT – both had a cancer detection rate of 7.5 per 1000 women screened
3. when ABUS and DBT were combined, the cancer detection rate increased slightly to 8.4 per 1000, detecting one extra cancer per 1000 women
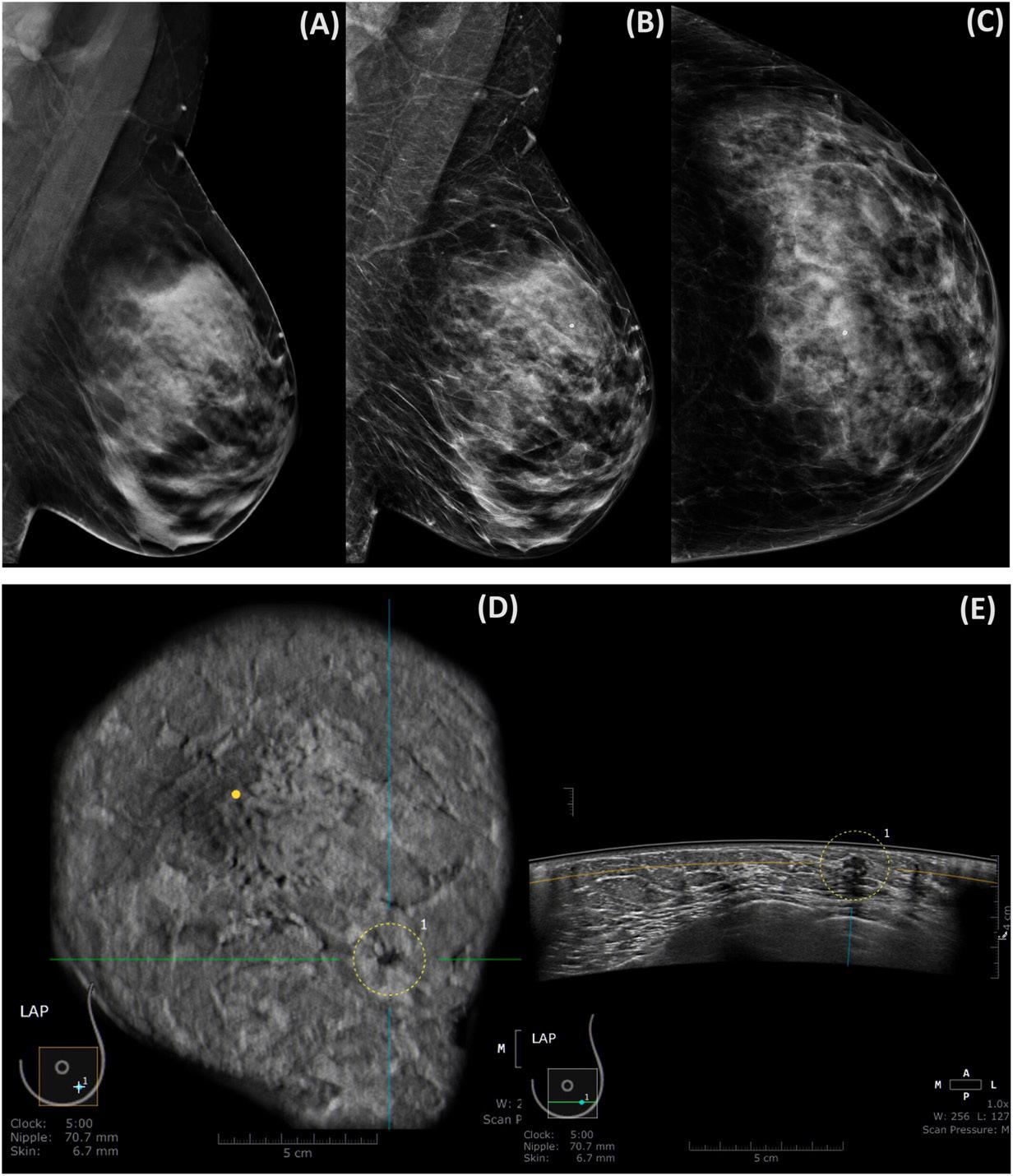
4. ABUS identified 12.5% more invasive cancers than DBT, suggesting it may detect more clinically important tumours (example imaging below)
5. sensitivity was the same for DBT and ABUS (84%), but highest when combined (94%)
6. specificity was highest for DBT (95%) and lower for ABUS (88%) and combined (86%)
7. the recall rate (false positives) was higher for ABUS (12.4%) and highest for the combined approach (14.9%), compared with DBT alone (6%).
‘Automated breast ultrasound (ABUS) is as effective as digital breast tomosynthesis (DBT) in detecting breast cancers and finds more invasive breast cancers in women with dense breast tissue, offering an effective supplemental or alternative screening tool despite the slightly higher recall rates.’
Value of automated breast ultrasound in screening: Standalone and as a supplemental to digital breast tomosynthesis (continued)
Limitations of the study
This single-centre study in a dedicated breast clinic may limit generalisability, though results align with multicentre studies. The opportunistic screening design may not fully represent a population-based program, but evidence suggests similar effectiveness. The imaging protocol used one-view DBT plus a 2D mammography view (hybrid DBT) rather than full two-view DBT, which could affect detection and recall rates, although prior research supports single-view DBT efficacy.
Relevance to clinical practice
This study is highly relevant to breast cancer screening in women with dense breasts, where mammography sensitivity is reduced. ABUS performs comparably to DBT and is particularly effective in detecting invasive cancers missed by DBT, supporting its use as a supplemental tool. Combining ABUS with DBT or 2D mammography increases cancer detection but also recall rates, suggesting selective use in dense breasts. With no ionising radiation, standardised imaging, and suitability for resource-limited settings, ABUS offers a practical, cost-effective option for personalised screening based on breast density, risk, and access to technology.
Figure 1. 50-year-old woman with BI-RAD C-type breast tissue. (A) LMLO DBT slice capturing a potential section of the MLO, providing insight into the location where the mass might be present. (B, C) 2D mammogram of the left breast. (B) 2D synthetic LMLO view. (C) 2D LCC view. No evidence of breast cancer is (A, B and C). (D) Coronal ABUS image. (E) Transverse ABUS image. A spiculated irregular mass with a hypoechoic pattern at 5:00 is seen. Histopathology of the lesion showed invasive cancer. Int J Cancer. 2024; 155(8) pg 1470
Transvaginal ultrasound for detecting parametrial involvement in suspected deep pelvic endometriosis: updated meta-analysis
Why the study was performed
The study was performed to provide an understanding of the current sensitivity and specificity of transvaginal ultrasound (TVS) performance for the detection of lateral parametrial involvement of suspected deep pelvic endometriosis. Parametrial involvement occurs in one in five women with deep endometriosis. TVS assessment of the parametrium has previously been underutilised but is important as it can cause more severe pain, voiding issues, constipation, and urethral obstruction, leading to silent functional loss of the kidney.
How the study was performed
A literature search for scans that assessed TVS against laparoscopy or histology. An exclusion protocol was run, and then studies were combined with previous meta-analysis data (6728 women total). Specificity and sensitivity were then calculated, and the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool was used to check the quality of each of the included studies.
What the study found
Subgroup analysis. Sensitivity and specificity: 85% (95% CI) and 98% (95% CI) for the left parametrium; 84% (95% CI) and 97% (95% CI) for the right.
Relevance to clinical practice
This article is encouraging, showing that the development of sonography in this area has been improving our detection of parametrial endometriosis. This is important due to patient symptoms, validating patient experience and surgical planning. It is bringing awareness to a fast-evolving area of ultrasound. It also provides evidence for why a defined scan protocol should be used, as this seems to be why our detection rates are improving when compared to the previous meta-analysis. Reference 12 contains instructions on how to perform this assessment.
WOMEN’S HEALTH
Reviewer: Amber Mohacsy
Authors & Journal: Alcázar J, Montoya C, Candau C, Catalan C, Orozco R, et al. Ultrasound Obstet Gynecol. 2025; 67: 7-14.
Open Access: Yes
Read the full article here
‘The diagnostic performance of TVS for detecting parametrial involvement in women with suspected deep pelvic endometriosis is better than that reported previously. This may be attributable to the use of a standardised TVS scanning technique and improved knowledge of pelvic ultrasound anatomy.’
Non-visualization of the ovaries on pediatric transabdominal ultrasound with a non-distended bladder: Can adnexal torsion be excluded?
Why the study was performed
Acute pelvic/lower abdominal pain is a common presentation to emergency departments. Bladder filling is the standard for the assessment of the pelvic organs in female children and adolescents (or those born with a uterus and ovaries) to rule out ovarian/adnexal torsion. This can often be a challenge and is time-consuming. Often, the patient is dehydrated from vomiting/anorexia and requires high volumes of water orally or intravenously. This article presents the potential efficacy and outcomes of visualisation of these organs without bladder filling.
How the study was performed
Retrospective analysis of 341 female patients aged between 1 and 19 years of age between January 2013 and July 2018 referred for transabdominal ultrasound (TA US) scans to rule out adnexal torsion and/or appendicitis. They were scanned with no bladder filling preparation and then filled and rescanned. Ovarian volumes, ratio of volume of larger ovary to smaller and the time between scans were documented. Diagnostic performance was assessed using sensitivity and specificity, and predictive values.
What the study found
• 9/341 had surgically proven adnexal torsion and a preoperative TA US with a nondistended bladder
° 8 out of the 9 girls who had surgically proven adnexal torsion – the torted ovary was identified with a non-distended bladder
• the NPV and PPV for exclusion of adnexal torsion with non-distended bladder were 1.0 and 0.8, respectively
• the specificity and sensitivity were 99.4% and 88.9%
• limited subgroup analysis of pre- and postmenarchal differences noted.
Relevance to clinical practice
This study addresses a practical challenge in paediatric imaging – the delay and discomfort of bladder filling. The authors proffer that in the post-menarchal patient, non-visualisation of the ovary correlates with the absence of torsion. Rapid diagnosis of adnexal torsion enables timely intervention or discharge, improving patient outcomes and reducing emergency department strain. Potential audit, review and adjustment of the current departmental protocol to non-visualisation of ovaries could be considered.
PAEDIATRIC
Reviewer: Sara Kernick
Authors & Journal: Shapira-Zaltsberg G, Fleming NA, Karwowska A, Perez Trejo ME, Guillot G, Miller E. Pediatr Radiol. 2019; 49(10): 1313-1319
Open Access: No
Read the full article here
‘Non-visualization
of the ovaries with a non-distended bladder on transabdominal US study can help exclude clinically suspected adnexal torsion, alleviating the need for bladder filling and prolonging the wait time in the emergency department.’
‘Inclusion
of nonvisualization of the ovaries as one of the features in a predictive score for adnexal torsion should be considered.’
Ultrasound as the first-line investigation for midgut malrotation: a UK tertiary centre experience
PAEDIATRIC
Reviewer: Keith VanHaltren
Authors & Journal: Meshaka R, Leung G, Easty M, Giuliani S, Loukogeorgakis S, Perucca G, Watson TA. Clin Radiol. 2024; 79(2): 150–159
Open Access: Yes
Read the full article here
Why the study was performed
The study presented the experience of a tertiary paediatric radiology department in transitioning from the traditional upper gastrointestinal (GI) fluoroscopy study to an ultrasound-first pathway in the diagnostic investigation for suspected midgut malrotation and volvulus in neonates (< 1 year) presenting with bilious vomiting.
How the study was performed
A 22-month retrospective audit was undertaken of all patients with bilious vomiting or suspected malrotation and volvulus who underwent the new ultrasound-first imaging pathway. The operators performing the ultrasound studies included both radiologists as well as paediatric sonographers who had been provided the appropriate training to perform the examination.
The ultrasound assessment included two important components: (i) assessment of the mesenteric vessels orientation from their origin to the distal-most aspect of the mesentery, and (ii) following the course of the duodenum from the pylorus to the duodenojejunal flexure, thus ensuring a normal retroperitoneal course of the third part of the duodenum (D3). Duodenal assessment was facilitated by the instillation of a bolus of sterile water via the nasogastric tube.
The new imaging pathway was determined by the radiology department in collaboration with the paediatric surgical team. The ultrasound ideally is to be performed first, with the outcome of the scan determining the subsequent imaging or management pathway for the patient. The three pertinent sonographic outcomes and their management pathway included:
(1) positive for volvulus and/or malrotation (whirlpool sign or D3 doesn’t cross midline): referral made back to the surgical team for operative management
(2) confidently negative (no volvulus and normal retroperitoneal third part of duodenum
(D3) and total length of mesenteric vessels visualised): the surgical team had the option of managing conservatively or requesting an upper GI study for further confirmation of normality
(3) indeterminate (D3 or mesenteric vessels not traced confidently, hence malrotation could not be ruled out): radiology offered an upper GI study.
What the study found
There were 101 patients in the audit period, with 63/101 (62%) having both ultrasound and upper GI studies, while 31/101 (31%) had ultrasound only, with the authors noting increasing proportions of patients having ultrasound only after the first year of transition. 76/101 (75%) had normal midgut appearances, while 8/101 (8%) had midgut malrotation, three of whom had a surgically confirmed volvulus. Six of the eight abnormal cases were detected correctly on ultrasound. Importantly, ultrasound identification and assessment of D3 was shown to demonstrate improvement over the transition period. 15/101 (15%) of cases had alternative management, changing diagnoses detected on ultrasound (ileocolic intussusception, choledochal cyst and massive haematocolpos), which would not have been otherwise diagnosed on upper GI studies alone.
Relevance to clinical practice
Transition to ultrasound as the first diagnostic test for midgut malrotation can be done safely and effectively with a rigorous protocol and management pathway clearly established from the outset. The benefits to neonates include a reduction in the use of upper GI studies needing radiation and contrast, the practicality of the scan being performed at the bedside, as well as the ability for the ultrasound to detect alternative diagnoses beyond the duodenal loop.
‘Transition to ultrasound as the first diagnostic test for midgut malrotation can be done safely and effectively.’
Participatory Action Research-DadirriGanma, using Yarning: methodology co-design
with Aboriginal community members
Why the study was performed
The study was performed to develop an appropriate methodology for the Aboriginal arm of the South Australian multiphase PAR project, ‘Stopping the Run Around’: Comorbidity Action in the North (CAN) project. The overall CAN project aimed to make recommendations for improving local mental health and alcohol and other drugs (MH-AOD) comorbidity services for people aged 12 and over.
The specific goal of this study was to codesign a Western methodology, participatory action research (PAR), with Indigenous concepts of Yarning (talking together/ consultation), Dadirri (deep listening), and Ganma (knowledge sharing). The aim was to adopt a suitable research design in Aboriginal health by fostering mutual and trustworthy partnerships between Indigenous and nonIndigenous researchers and stakeholders.
How the study was performed
The research was conducted by an international PhD student (the main author and a registered nurse by profession) in collaboration with a supervisor and multiple stakeholders, including an Aboriginal Elder
mentor and co-researcher (Aunty Coral Wilson, ACW), the Aboriginal Working Party (AWP – 10 local Aboriginal people), Aboriginal community members, health professionals and consumers, non-Indigenous service providers in the CAN project.
Given the involvement of the Aboriginal community, ethical approval was gained from an Aboriginal-specific ethics committee, the government health department, and nongovernment MH-AOD organisations, a process that was time-consuming, complex, and took 18 months to accomplish.
The study utilised the co-designed PARDadirri-Ganma using Yarning methodology over four phases with Indigenous concepts incorporated throughout (Figure 1 of the original article):
1. look and listen (incorporating Yarning)
2. think and reflect (incorporating Dadirri and Ganma)
3. collaborate, consult and plan (incorporating Dadirri and Ganma)
4. take action (incorporating Dadirri and Ganma).
The study included interviews, focus groups, and a final workshop with local Aboriginal participants.
Reviewer: Ling Lee, AFASA
Authors & Journal: Sharmil H, Kelly J, Bowden M, Galletly C, Cairney I, Wilson C, et al. Int J Equity Health. 2021; 20: 160
Open Access: Yes
Read the full article here
‘Mindfulness in adopting an appropriate methodology and considering specific ethical requirements when working with Indigenous communities.’
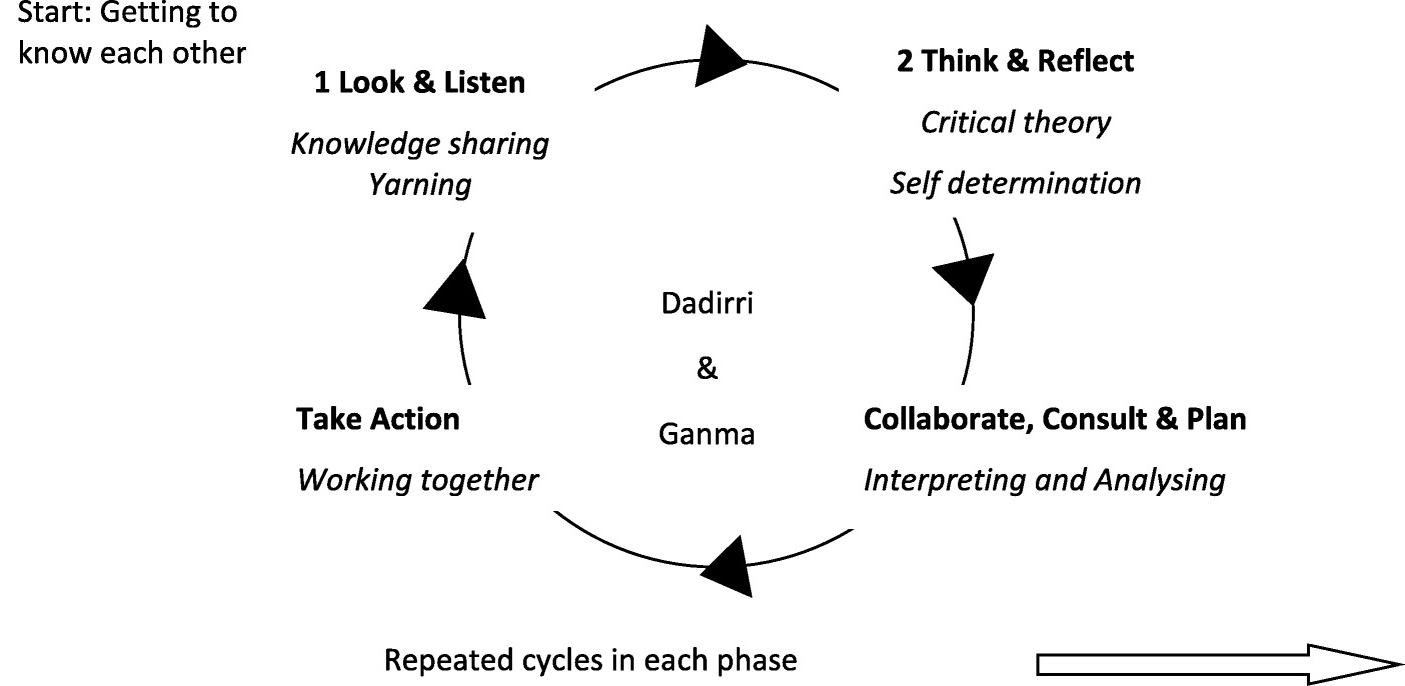
Figure 1. PAR inquiry cycle incorporating DADIRRI and GANMA. Int J Equity Health 2021; 20: 160
Participatory Action Research-Dadirri-Ganma, using Yarning: methodology co-design with Aboriginal community members
(continued)
What the study found
The PAR-Dadirri-Ganma, utilising the Yarning methodology, was a key component in successfully running the Aboriginal arm of the CAN project. The PAR-Dadirri-Ganma, using the Yarning methodology, successfully cultivated a trustworthy and mutually beneficial partnership among multiple stakeholders to address healthcare issues related to MHAOD comorbidity. The main author discovered that transparent communication, two-way knowledge sharing, and decision-making are vital for building trust when working with the Aboriginal community, where distrust of Western research is a known barrier. Significantly, the study identified corresponding components between Dadirri (Listening, Reflecting, Reciprocity, Re-listening) and the PAR cycle (Listening, Thinking, Acting, Reacting) (Figure 2 of the original article). One major outcome was that the recommendations regarding MH-AOD comorbidity care were being considered by the South Australian Parliament.
Relevance to clinical practice
This paper shares the experience and findings to benefit other research students and community members conducting future research projects in similar settings (involving Aboriginal communities in healthcare settings). It emphasises the importance of adopting an appropriate methodology and ethical considerations when working with Indigenous communities and how to cultivate a mutual, trustworthy partnership to achieve desirable outcomes that benefit the communities being served.
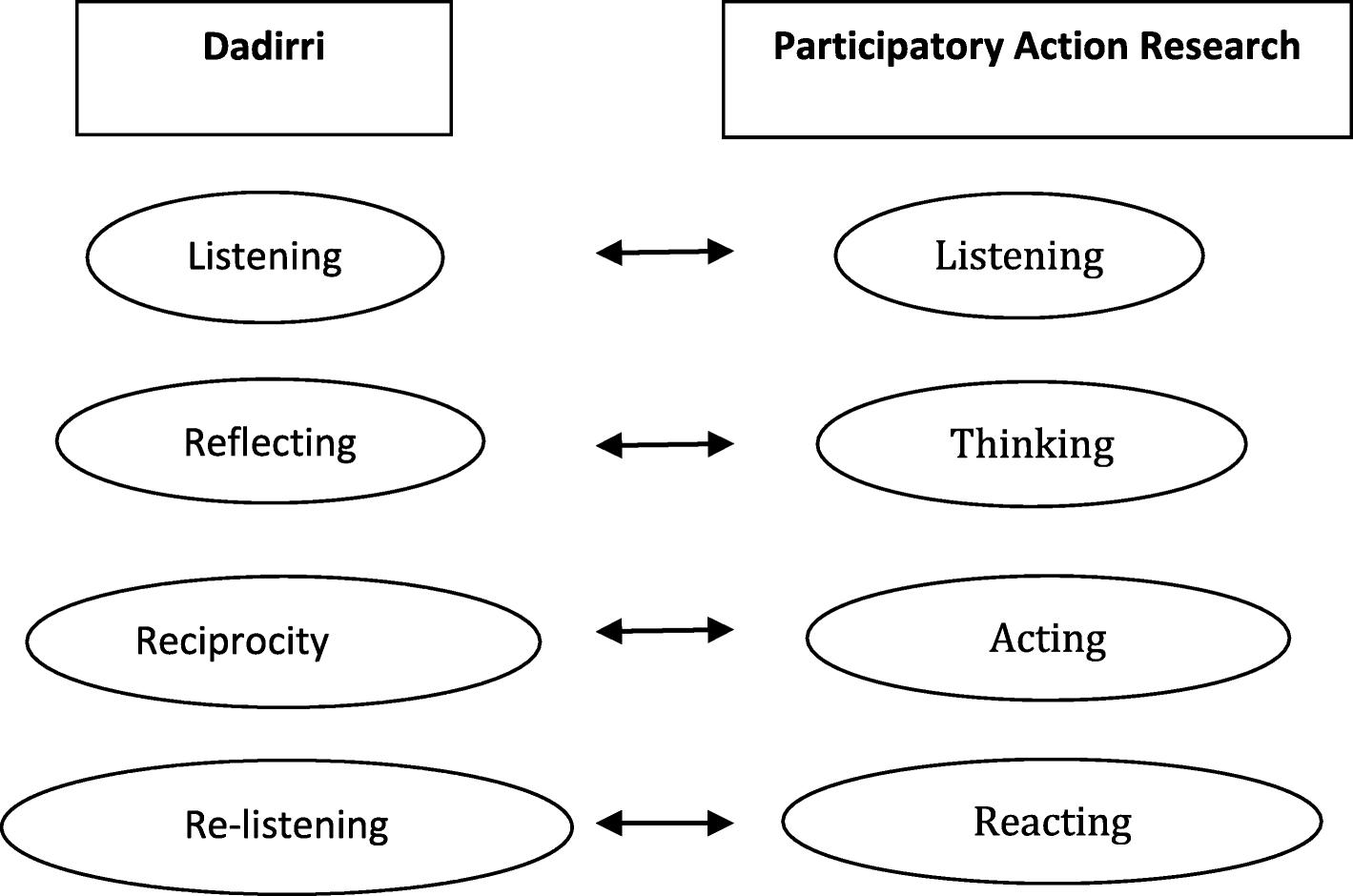
Figure 2. Components of Dadirri discovered by Hepsibah. S, and the PAR cycle. Francis Jebaraj H. Stopping the Run-around: Addressing Aboriginal community people’s mental health and alcohol and drug co morbidity service needs in the Salisbury and Playford local government areas of South Australia Australia University of Adelaide. 2015; pg 346
Facilitators and barriers to undertaking research into the practice and delivery of clinical ultrasound: A qualitative investigation
Why the study was performed
The study aimed to understand the facilitators and barriers to conducting ultrasound research by professionals from multiple disciplines who use clinical ultrasound.
How the study was performed
A qualitative study employed semi-structured qualitative video-platform interviews, which were analysed using reflexive thematic analysis. Participants were recruited via advertisements on social media platform X (formerly known as Twitter) in the United Kingdom, and relevant organisations were tagged (e.g. British Medical Ultrasound Society, Society and College of Radiographers). Current and prospective researchers interested in undertaking ultrasound research were recruited.
Interviews were recorded and automatic transcripts generated and analysed using reflexive thematic analysis.
What the study found
Twelve participants from a range of disciplines participated in the study. Five themes were identified. Facilitators and barriers to undertaking clinical research:
• research is a challenging path
• interpersonal networks fuel research
• research requires resources
• data collection is challenging
• scientific curiosity.
These themes support previous studies into research barriers and facilitators in clinical professions. This study found that the key facilitators are internal (self-motivation, and to improve career skills) while the barriers are external (lack of time, funding and support). This is useful for the non-sonographer groups as well as sonographers and midwives who use ultrasound.
Relevance to clinical practice
Organisations can increase the likelihood of research activity by ultrasound practitioners by providing allocated research time and social support networks.
RESEARCH
Reviewer: Glenda McLean, FASA
Authors & Journal: Al-Ghunaim T, Harrison G, Kaur E, Arezina J, Carr R, Johnson J. Radiography. 2024; 30(5): 1391–1397
Open Access: Yes
Read the full article here
‘Increase the likelihood of research activity by providing allocated research time.’
Ultrasound measurement of perirenal adipose tissue indicates cardiovascular disease, but
A
standardisation is needed:
systematic review
Why the review was undertaken
In light of the global obesity crisis, this review was undertaken to evaluate ultrasound-derived thickness measurement of perirenal adipose tissue (PRAT) as a prognostic indicator of cardiovascular disease (CVD). Central to this, the review investigates current techniques with which this measurement is derived and assesses the reproducibility and accuracy of the results. Current methods of obesity risk assessment, including waist measurement and BMI calculation, are non-specific in differentiating the amount of PRAT (the type of visceral fat that may have a higher association with cardiovascular and renal disease) from other visceral fat deposits and/or normal biological tissue. PRAT thickness is most accurately reflected in vivo by radiology, at present CT and MRI being the gold standard. This article suggests that ultrasound may be a more attractive option in obtaining PRAT measurement, with multifactorial reasoning including portability, ease of access, affordability and the lack of non-ionising radiation.
How the review was performed
This systematic review evaluates the current ultrasound PRAT measurement techniques for the prediction of CVD. Clinical studies published between 2010 and 2013 were included in the analysis to assess the accuracy of this measurement when compared to CT and MRI, as well as its reliability and predictive capability, considering variations in how the measurement is undertaken.
What the review found
PRAT is anatomically located between the renal capsule and rigid Gerota’s fascia and is contiguous with the perivascular renal sinus fat. With little capacity to expand, Gerota’s fascia is responsible for PRAT, imposing a mechanical compressive effect that results in both local
and systemic repercussions. Compression of encapsulated PRAT is thought to contribute to localised renal damage, whereby compression of renal vessels may directly result in heightened systemic vascular resistance.
An interesting point of discussion within the article focuses on PRAT being considered a complex endocrine organ. Its composition of adipocytes, nerve endings, vascular networks and inflammatory cells contributes to metabolic activity associated with the development of CVD, chronic renal disease (CRD), hypertension, atherosclerosis and tumour progression. The development of CVD relative to PRAT is associated with its overproduction of fatty acids, which initiate chronic systemic inflammation, promote endothelial dysfunction and instigate the formation of atherosclerosis.
The systematic review confirms that ultrasound-derived PRAT thickness measurements are predictive of CVD risk factors, being comparable to CT and MRI findings. Twenty different measurement techniques were used across the 21 evaluated studies, however, and suggests a need for standardisation before clinical implementation, to ensure reproducibility and reliability.
Relevance to clinical practice
Given the clinical potential of using ultrasound-derived PRAT measurement as a risk assessment for CVD and metabolic dysfunction, the addition of this to a routine abdominal examination could have lifesaving potential. Considering the large volume of abdominal ultrasound examinations already undertaken in Australia, the addition of PRAT measurement would not be onerous and could facilitate interventions that may reduce patient morbidity and mortality. This is especially significant for regional patients who may experience limitations or challenges when accessing the currently favoured modalities of CT and MRI. For this to be confidently utilised in clinical practice, however, more research is required to obtain standardisation in ultrasound measurement technique.
GENERAL
Reviewer: Donna Napier, FASA
Authors & Journal: Baumann VJ, Banati R, Clarke JL. Australas J Ultrasound Med. 2024; 28(1):e12407
Open Access: Yes
Read the full article here
‘Considering the large volume of abdominal ultrasound examinations already undertaken in Australia, the addition of PRAT measurement would not be onerous and could facilitate interventions that may reduce patient morbidity and mortality.’
Ancillary US of the bowel: Endovaginal US, contrast-enhanced US, and elastography
Reviewer: Marilyn Zelesco, AFASA
Authors & Journal: Wajahat N, Merrill CD, Medellin A, Wilson SR. Radiographics. 2025; 45(9): e240149
Open Access: Yes
Read the full article here
Why the article was published
Sonography provides high resolution, dynamic, real-time scanning of the bowel. Although its major application is in the assessment of patients with inflammatory bowel disease (IBD), other pathologic conditions, both benign and malignant, are amenable to and greatly benefit from ultrasound study. The use of colour Doppler further demonstrates vascular detail while still being non-invasive. This is of particular use in pregnant women, paediatric patients and those patients who are unable to undergo CT or MRI. Nonetheless, standard B-mode and colour Doppler imaging have limitations in bowel sonography – usually due to gas and associated artefacts. Colour Doppler often loses sensitivity at increased depth and is unable to visualise flow at the capillary level. B-mode ultrasound may be of excellent resolution, but it is unable to reflect the biomechanical properties of the normal or pathological gut. This article was published to assess the role of ancillary ultrasound techniques in gut imaging –endovaginal sonography (EVS), contrastenhanced ultrasound (CEUS), and shear wave elastography (SWE).
How the study was performed
The authors systematically addressed the fundamentals of bowel ultrasound in IBD –discussing normal bowel wall appearances (5-layer tubular structure), normal bowel wall thickness (3 mm), presence of hyperaemia, and demonstration of associated inflammatory fat. These independent factors are collectively called the ‘Ultrasound Global Assessment (USGA)’ and relate to the sonographic grading of disease as inactive, mild, moderate or severe. The authors systematically examined the role of each of the ancillary techniques that can lead to missed or incompletely assessed diagnoses of bowel disease.
What the study found
The review found that when compared to conventional ultrasound, the three ancillary techniques – EVS, CEUS and SWE – provide increasing evidence for the use of sonography in bowel assessment. Specifically, EVS allows assessment of deep bowel structures such as the distal small bowel loops and sigmoid colon, or in some women, the terminal ileum and appendix may also only be visualised by EVS. The proximity of the high frequency probe to the bowel produces higher resolution images that can reveal subtle or otherwise unseen morphologic features such as localised perforations, fistulas, ulcerations, and masses. Movement and pressure from the probe can also localise pathologic findings and sources of pain.
CEUS allows a real-time view of blood flow to the capillary level as a reflection of inflammatory or neoplastic blood flow. For IBD, it may contribute at the time of diagnosis, at surveillance, and for response to therapy. CEUS is also known for its exceptional ability to depict peri-enteric inflammatory masses and to differentiate an avascular abscess from a vascular phlegmon.
In the bowel, SWE has some obvious technical limitations, including peristalsis, gas artefact, luminal content, and mobility, that cannot always be controlled. Although SWE values have not been validated for bowel imaging, in the current literature, there is some emerging evidence that SWE may be reliable in the assessment of bowel stiffness and particularly in the characterisation of strictures as inflammatory or chronic.
‘Bowel evaluation is an often overlooked but integral part of all abdominopelvic sonography.’
Recommendations for the evaluation of left ventricular diastolic function by echocardiography and for heart failure with preserved ejection fraction diagnosis: An update from the American Society of Echocardiography
Why the study was performed
The American Society of Echocardiography (ASE) has released updated guidelines for the evaluation of left ventricular (LV) diastolic function, replacing the 2016 ASE/EACVI recommendations. Over the past nine years, technological advances such as the integration of left atrial (LA) strain have expanded diagnostic capabilities. The new guidelines aim to improve accuracy in assessing LV filling pressures and diastolic dysfunction, particularly in patients with heart failure with preserved ejection fraction (HFpEF). A major goal is to reduce the rate of indeterminate cases seen with the previous approach. Accurate evaluation of LV diastolic function is essential for guiding therapy, and the update emphasises that this assessment should be routine in comprehensive echocardiograms, especially for patients with dyspnoea or suspected heart failure.
How the study was performed and what the study found
The updated guideline was developed by a multidisciplinary panel through a systematic review of recent studies validating new algorithms and imaging modalities, including LA strain. Findings highlight that accurate diastolic assessment requires an integrated approach using multiple echocardiographic parameters rather than relying on single measurements. The panel also recognised the need for tailored guidance for special populations such as HFpEF patients.
Relevance to clinical practice
The 2025 guidelines recommend a broader range of measurements – mitral inflow, tissue Doppler and LA strain for evaluating diastolic function and LV filling pressures. New algorithms incorporate age-specific reference ranges and exercise stress echocardiography criteria, aiming to reduce indeterminate cases. Specialised protocols are provided for complex populations, including those with atrial fibrillation, pulmonary hypertension, mitral annular calcification, post-heart transplant and post-transcatheter edge-to-edge repair (TEER) patients.
A key strength of the update is clearer guidance on image acquisition, interpretation and reporting – promoting evidence-based consistency.
Key additions to the standard echocardiography assessment: IVRT – reflects LV relaxation and inversely relates to LA pressure
LAVi – a supplemental measure of chronic diastolic burden and assists with LA pressure estimation
LARS – strongly correlates with the diastolic dysfunction and is inversely related to LV filling pressure; the lower the LARS, the higher the LVFP
GLS – a more sensitive marker of systolic performance than EF; reduced GLS is a criterion for HFpEF and is recommended. Initial measurement steps when assessing diastology with echocardiography are demonstrated in the flow chart below and then incorporated into the grading algorithm to determine grade and filling pressures.
Reviewers: Kim Prince and Christopher Thomas
Authors & Journal: Nagueh SF, Sanborn DY, Oh JK, Anderson B, Billick K, Derumeaux G, et al. J Am Soc Echocardiogr (JASE). 2025; 38(7): 537-569
Open Access: Yes
Read the full article here
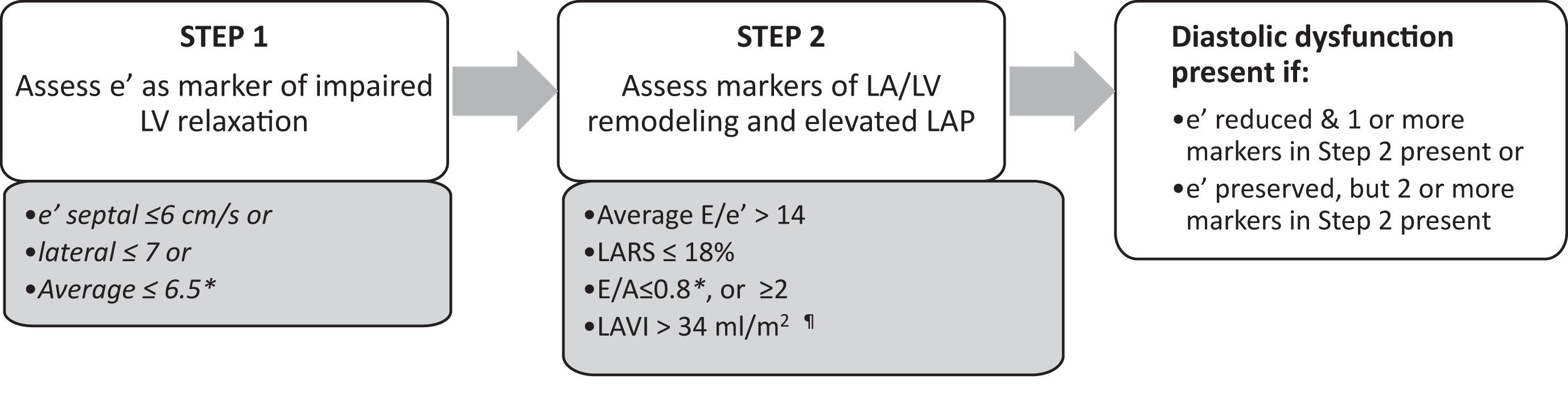
Figure 2. Steps for diagnosing LV diastolic dysfunction. J Am Soc Echocardiogr 2025; 38:(7) pg 553
Recommendations for the evaluation of left ventricular diastolic function by echocardiography and for heart failure with preserved ejection fraction diagnosis: An update from the American Society of Echocardiography (continued)
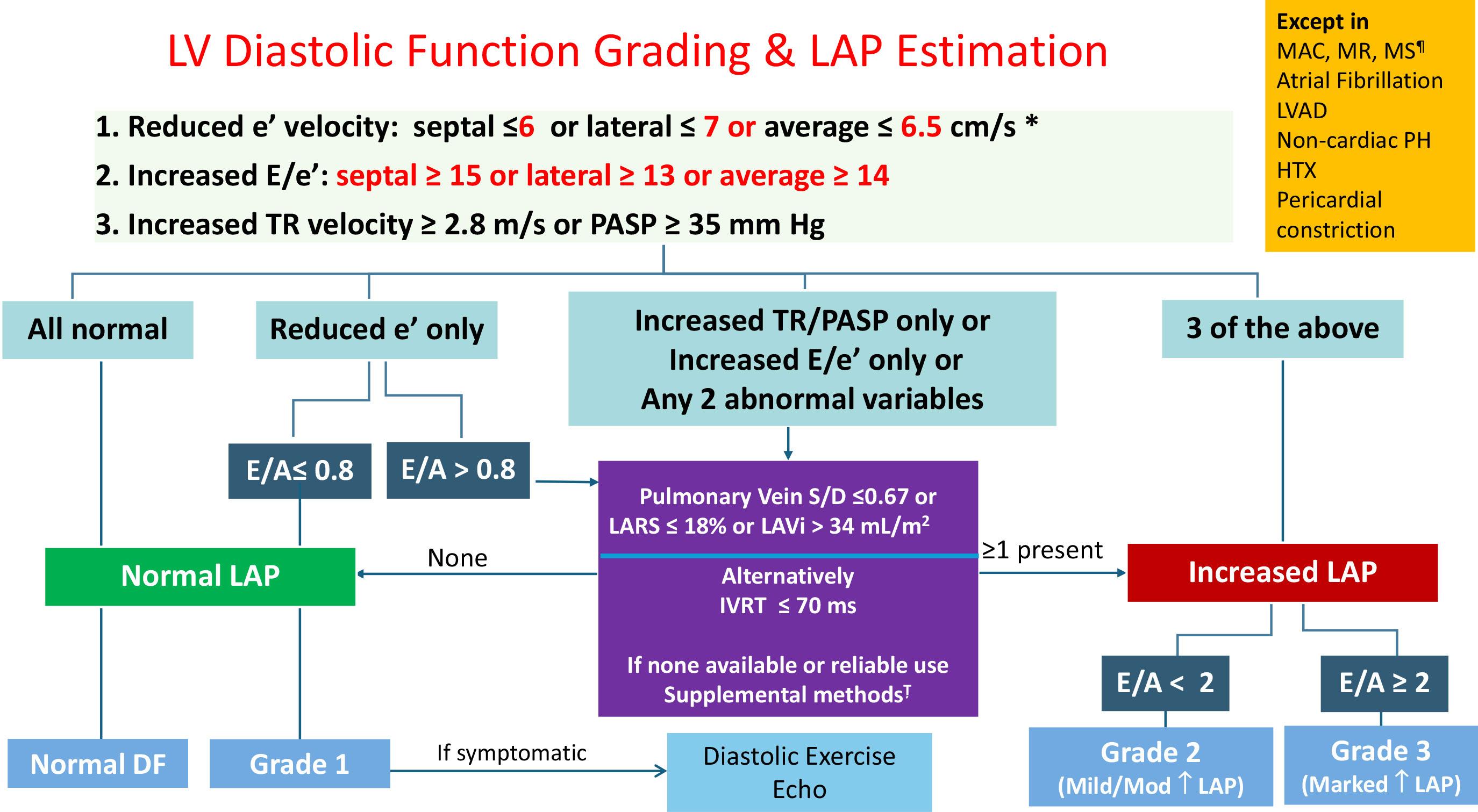
Figure 3. Algorithm for estimation of mean LAP for patients in sinus rhythm and who do not have severe primary MR, any degree of mitral stenosis (MS), or moderate or severe MAC. The algorithm should also not be applied to patients in atrial fibrillation, heart transplant (HTX) recipients, noncardiac PH, pericardial constriction, or LV assist device (LVAD).
*For annular e’ velocity, age-adjusted lower limits of normal values shown in Table 6 can be applied in place of the values shown in this figure. The algorithm should also not be applied to patients with mitral valve repair, mitral valve replacement, or mitral-TEER. DF, Diastolic function; Ț, PR end-diastolic velocity ≥ 2 m/s, PA diastolic pressure ≥ 16 mm Hg, mitral inflow L-wave velocity ≥ 50 cm/s, Ar-A duration > 30 ms, and/or a decrease in mitral E/A ratio of ≥ 50% with Valsalva maneuver. J Am Soc Echocardiogr 2025; 38:(7) pg 554
The 2025 ASE guidelines represent a significant advancement in diastolic function assessment. By integrating new imaging modalities, refining algorithms and standardising protocols, they enhance diagnostic accuracy and reduce indeterminate classifications. For sonographers, the update requires adopting a broader set of measurements, applying age-specific reference ranges, and incorporating stress testing when appropriate. Consistent reporting – including diastolic grade and LV filling pressures – is now essential. These changes support cardiac sonographers in delivering accurate, evidencebased evaluations that improve patient care and standardise practice.
‘The primary goal of this update is to simplify the approach and thus increase the utility of the guidelines in daily clinical practice.’
Strain reversus sign: Diagnostic role and correlation with cardiac magnetic resonance findings in constrictive pericarditis
Why the study was performed
Constrictive pericarditis (CP) is a rare but clinically significant condition characterised by impaired diastolic filling due to a rigid, thickened pericardium. Non-invasive imaging modalities, such as echocardiography (echo), serve as essential first-line diagnostic tools; however, when echo findings are inconclusive, cardiac magnetic resonance (CMR) and computed tomography (CT) provide complementary anatomical information.
Accurate diagnosis is crucial because CP is potentially reversible through surgical pericardiectomy, unlike restrictive cardiomyopathy. However, diagnosing CP remains challenging and often relies on multimodality imaging. Traditional echocardiographic criteria, such as the Mayo Clinic criteria, have limitations in sensitivity and specificity, which can create diagnostic uncertainty.
A new echocardiographic marker, strain reversus (SR), has been identified in CP; it is characterised by a reversal of the normal longitudinal strain gradient, where septal strain exceeds lateral wall strain. This pattern indicates altered ventricular mechanics caused by pericardial constriction. The study aimed to:
1. evaluate the prevalence of SR among patients with pericardial disease
2. assess the diagnostic value of SR for CP
3. explore the correlation of SR with pericardial involvement on CMR.
How the study was performed
Acute and chronic pericarditis were defined according to the 2015 European Society of Cardiology guidelines. This single-centre retrospective cohort study screened and evaluated 385 patients for pericardial disease. Of these, 85 patients (mean age 57 ± 17 years; 32.8% female) with suspected pericardial
disease underwent both echo and CMR. CP was confirmed by right heart catheterisation, which served as the reference standard.
Patients were categorised into two groups: 24 with CP and 61 with non-constrictive pericarditis (NCP).
All standard echo parameters were measured for each patient, including twodimensional, Doppler, colour Doppler and tissue deformation (TDI). Longitudinal strain (LS) echocardiography was used to identify SR with the Mayo Clinic criteria. CMR and late gadolinium enhancement (LGE) investigated the pericardium, pericardial thickness, oedema, and the presence of pericardial effusion. Echo was performed within two days of patient admission, and subsequent CMR within five days.
What the study found
• prevalence: SR was present in 91% of CP patients versus 25% of NCP (P < .001)
• diagnostic Value: Adding SR to Mayo criteria improved diagnostic accuracy:
° C-statistic increased from 0.82 to 0.92 (P = .004)
° net reclassification improvement index: 0.198
• CMR Correlation: SR was significantly associated with:
° pericardial thickening (OR 2.30; P = .001)
° LGE (OR 1.55; P = .036)
SR was not associated with pericardial oedema.
• LV LS for the diagnosis of CP
° SR had the best sensitivity, qualitative assessment 0.92, and specificity 0.75, while SR ratio had an increase in specificity 0.92 and sensitivity 0.79, quantitative assessment.
Statistical analysis evaluated SR prevalence, its incremental diagnostic performance when added to Mayo criteria, and its association with CMR findings.
Reviewer: Louise Smith
Authors & Journal: Fazzari F, Cannata F, Tassetti L, Garattini D, Pensotti F, Milanese R, et al. J Am Soc Echocardiogr. 2025; 38(9): 832–42
Open Access: No
Read the full article here
Strain reversus sign: Diagnostic role and correlation with cardiac magnetic resonance findings in constrictive pericarditis (continued)
HIGHLIGHTS
• SR is a typical strain pattern described in patients with CP.
• SR shows reduced LV free wall strain with septal sparing on the bull’s-eye plot.
• SR increases the diagnostic accuracy of the Mayo Clinic criteria.
• SR is strongly correlated with invasive diagnosis of CP.
• SR is associated with pericardial thickening and pericardial LGE observed on CMR.
Relevance to clinical practice
SR is a non-invasive parameter that strengthens diagnostic confidence when used alongside the Mayo Clinic criteria. Its strong correlation with CMR underscores its pathophysiological relevance. Early detection of CP through SR can aid clinical diagnosis, enabling timely intervention and improving patient outcomes.
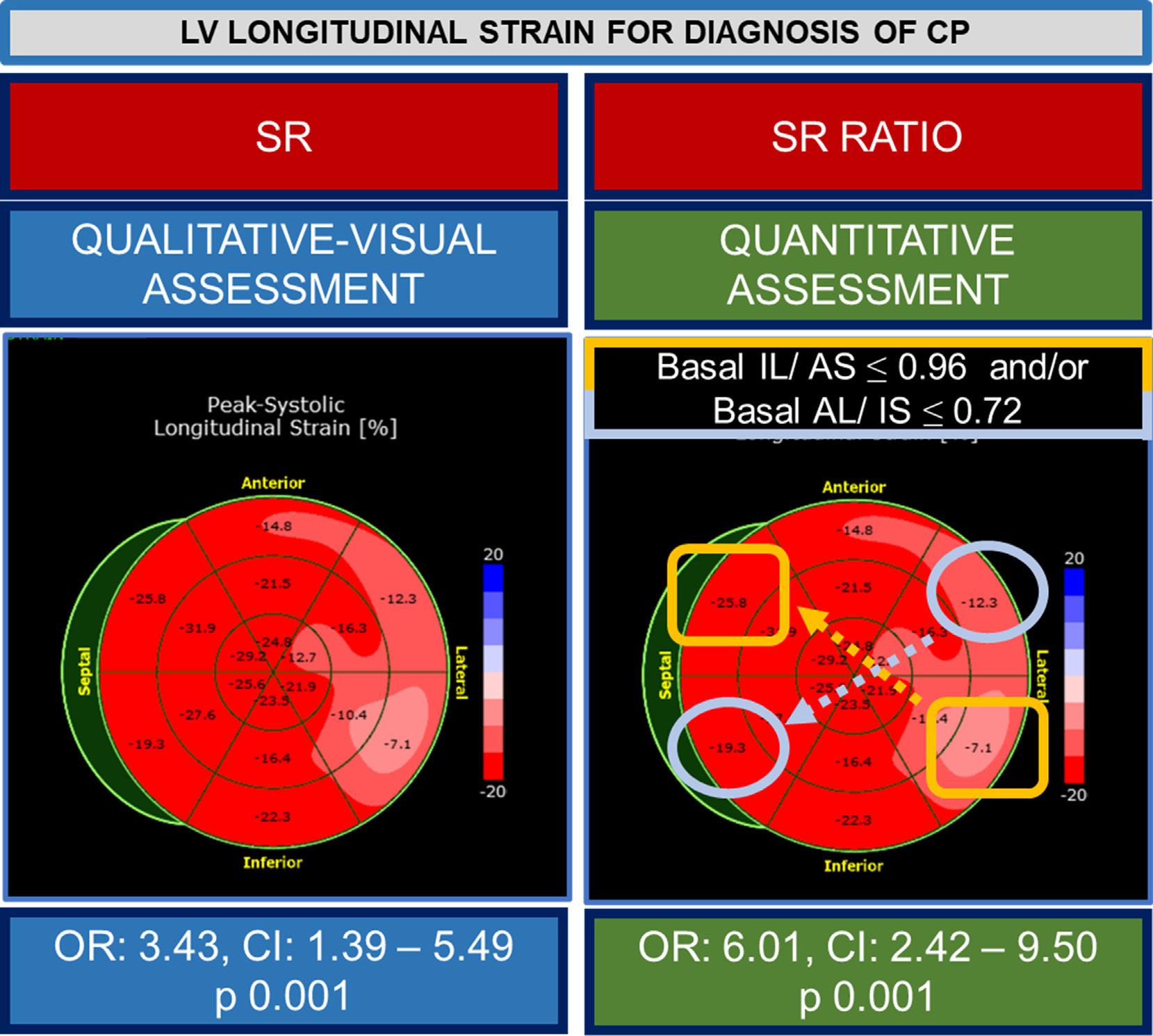
LV
for diagnosis of CP.
is visually assessed on the bull’s-eye plot as an area of normal (red) LS of the interventricular septum (IVS) and impaired LS of the lateral wall (light red to pink). (Right) SR ratio is a quantitative evaluation of the septal-to-lateral diagnosis on multivariate models (lower boxes). J Am Soc Echocardiogr. 2025; 38 (9) pg 838
‘When constrictive pericarditis is suspected, the bull’s-eye plot can be quickly evaluated, given the excellent accuracy of strain reversus in confirming or excluding CP. In case of uncertainty, SR ratio should be further assessed by calculating the basal IL/AS and AL/ IS ratios.’
Figure 1.
LS
(Left) SR
Offline ultrasound–MRI fusion imaging for assessment of normal fetal brain development
Why the study was performed
This exploratory research fused 3D ultrasound (3D-US) of the fetal brain with magnetic resonance imaging (MRI) to investigate the feasibility of such a novel technique, and then to determine the success rate in evaluating the brain structures in the 3D reconstruction.
How the study was performed
The study recruited women with a healthy singleton pregnancy between 16 and 36 weeks’ gestation at a Paris hospital. The 3D-US acquisitions of the fetal brain were collected in axial, sagittal and coronal planes using a curvilinear or transvaginal transducer (if necessary) on a GE Voluson E10 ultrasound machine. The acquisitions were also completed with microvascularisation imaging in Doppler mode in each plane. The women underwent an MRI examination afterwards using a GE Optima MR450W 1.5-Tesla MRI scanner. Afterwards, the DICOM data from the 3D-US and MRI were merged using GE 4D View Fusion software. A minimum of 3 anatomical landmarks inside the brain were used to register the volume datasets together, with additional landmarks included if the superimposition needed to be improved. The 3D-US, MRI and US-MRI fusions were reviewed by two fetal sonographers and a neuroradiologist.
What the study found
The analysis included 113 women with a mean gestational age of 25+3 weeks and a mean maternal age of 34 years. The 3D-US reconstructions were assessed for quality. All three planes of the fetal brain reached quality criteria in 87.6% (99/113) of pregnancies overall. 3D-US of specific planes was usable in
97.3% (110/113) of sagittal acquisitions, 87.6% (99/113) of coronal acquisitions, and 100% of axial acquisitions. For MRI acquisitions, all three planes of a fetal brain were quality in 97.3% of cases. Fetal movement resulted in the failure of the MRI acquisition in the remainder of cases (2/113).
The fusion of the US and the MRI together was usable in all three planes in 85/99 cases, with later gestational ages having less success. The average time to fuse and superimpose the images from the two modalities was three minutes in each plane. A complete evaluation of the fetal brain was possible in 9.4% (8/85) cases for 3D-US, 74.1% for MRI, and 87.1% (74/85) for the US-MRI fused datasets.
Different anatomical landmarks had different rates of successful identification. In the 3D-US images, the sylvian fissures, CSP, corpus callosum, and choroid plexus were some of the anatomies that were identified successfully in 100% of cases. The infratentorial spaces were visualised with the lowest level of success at only 7.64% of cases. In the US-MRI fusion images, all structures were successfully identified in 100% of cases.
Relevance to clinical practice
While fusion of US and MRI imaging resulted in a higher rate of visualisation in the fetal brain, this novel application of imaging technologies is still being explored. When fetal brain abnormalities are detected on US, fusion application has the potential to be performed to confirm the location of the abnormality. This application may be most beneficial for remote locations and educational purposes. The authors do note that this paper did not explore the anatomical detail provided, nor whether any diagnostic information was gained from the fusion.
EMERGING TECHNOLOGIES
Reviewer: Dr Jacqueline Roots
Authors & Journal: Codaccioni C, Arthuis C, Deloison B, Bault JP, et al. Ultrasound Obstet Gynecol. 2025; 66(4): P509–517.
Open Access: Yes
Read the full article here
‘Fusion imaging is a technique that merges two examinations, from the same or from different imaging modalities. Ultrasound (US)–MRI fusion imaging has the potential to fill in information missing from each modality to provide complementary information through the fusion of the two examinations.’