PUBLISHED IN THE INTEREST OF OUR MEMBERS AND THEIR PATIENTS
President’s Message
FACS President, Pennsylvania Academy of Otolaryngology –Head and Neck Surgery
Welcome to the Winter issue of Soundings! It is both an honor and a privilege to address you in my first message as President of the Pennsylvania Academy of Otolaryngology – Head and Neck Surgery, a role I assumed at our annual meeting this past June. I want to begin by expressing my deep appreciation to our immediate past president, Dr. Jessyka Lighthall whose leadership and dedication strengthened
our Academy’s academic mission and voice in political advocacy. Through her partnership with our lobbyist, Philip Dunn, she was able to promote issues important to Pennsylvania Otolaryngologists and expand our presence in Harrisburg. We are continuing that important work— ensuring that the interests of our patients and our specialty are well represented in Harrisburg and beyond.
Last years’ annual PAO-HNS scientific meeting took place in Hershey, Pennsylvania. It was a great success and lead by program chairs Dr. Sandra Stinnett and Dr. Neerav Goyal. The meeting coordinators, chairs, and program committee provided an excellent line up of speakers and panels from across the state as well as other disciplines discussing current management of otolaryngologic pathology in pediatrics and adults.
As we build on the foundation set by our past leaders, our focus this term expands to education, collaboration, and member engagement. The Academy is committed to serving as a dynamic resource not only for practicing otolaryngologists, but also for residents, fellows, and the advanced practice providers who are integral to patient care across the state. We are
actively working to foster growth within the society by creating new opportunities for involvement and strengthening connections among our members. This includes exploring partnerships with regional and national APP societies to provide highquality educational content tailored to their professional needs. At the same time, we are broadening our social media presence and evaluating new online educational platforms to better disseminate clinical updates, highlight Academy initiatives, and increase access to learning for clinicians across Pennsylvania. Through these efforts, we aim to cultivate a more engaged, informed, and connected community.
Our strength as a specialty depends on connection—among colleagues, across disciplines, and between generations of clinicians. I invite each of you to participate in these efforts, share your ideas, and help shape the future of our Academy. Together, we can ensure that Otolaryngology in Pennsylvania continues to thrive and lead.
Warm regards,
Colin
Huntley, MD FACS President, Pennsylvania Academy of Otolaryngology –Head and Neck Surgery
Colin Huntley, MD
President Colin T. Huntley, MD Jefferson University—Otolaryngology Head & Neck Surgery
President-Elect Pamela C. Roehm, MD, PhD St. Luke’s University Health Network, Lehigh Valley, PA
Secretary-Treasurer Neerav Goyal, MD, MPH Penn State Health Milton S. Hershey Medical Center - Otolaryngology - Head & Neck Surgery
Administrative Office 400 Winding Creek Blvd. Mechanicsburg, PA 17050-1885 833-770-1544 855-918-3611 (fax)
Visit our website at www.otopa.org
Soundings accepts classified advertisements; however, there is no guarantee that they will be published. All submissions are subject to review. The advertisement should be of interest/ pertain to otolaryngologists, their practice, and health care in Pennsylvania. Submissions that are self-promotional or commercial in nature will not be accepted. Publication of advertising does not imply endorsement of the products advertised or the statements contained in such advertising by Soundings or the PAO-HNS. The opinions expressed in this newsletter do not necessarily reflect the opinion of PAO-HNS.
Evidence-Based Management and Advanced Treatment Options for Bell’s Palsy in Pennsylvania
F. Jeffrey Lorenz, MD, Jessyka G. Lighthall, MD, FACS Penn State Department of Otolaryngology-Head and Neck Surgery
Introduction
Bell's palsy, or idiopathic facial paralysis, affects approximately 15 to 30 per 100,000 people annually and represents the most common cause of acute unilateral facial nerve paralysis.1 While the majority of patients experience spontaneous recovery, 20 percent or more develop persistent facial weakness or synkinesis that significantly impacts quality of life.2 The otolaryngologist plays a crucial role not only in the acute diagnosis and management of Bell's palsy, but also in recognizing when cases require advanced intervention and appropriately referring patients to specialized facial nerve centers.
Evidence-Based Diagnosis and Management in the Acute Setting
Bell's palsy is a diagnosis of exclusion, requiring careful history and physical examination to rule out alternative etiologies of facial paralysis. The clinical presentation should demonstrate rapid onset of symptoms within 72 hours with involvement of both the upper and lower divisions of the facial nerve, without evidence of other cranial neuropathies.3 The history and examination must exclude features suggestive of Ramsay Hunt syndrome, such as vesicles, otalgia, or hearing loss,4 as well as structural lesions suggested by gradual onset or the presence of a parotid mass. Given that Pennsylvania is endemic for Lyme disease, serologic testing with Lyme antibody titers should be obtained especially in Summer months, as early identification and treatment of Lyme-associated facial palsy with appropriate antibiotic therapy is essential.5 However, other laboratory testing is unnecessary. In patients with classic features of Bell’s palsy, no imaging
is warranted. In cases with atypical features such as slow progression without any recovery, imaging with CT/MRI may be warranted to exclude alternative diagnoses.
For the acute treatment of Bell's palsy, corticosteroids should be initiated within 72 hours of symptom onset.3 The standard regimen consists of prednisone 50-60 mg daily for 10 days, with or without a taper. The addition of antiviral therapy with acyclovir or valacyclovir may be offered, though randomized controlled trials have not demonstrated statistically significant benefit over corticosteroids alone.6,7 Eye protection with artificial tears, lubricating ointment, and nighttime taping or moisture chambers is essential to prevent exposure keratopathy in patients with incomplete eye closure. Coordination with ophthalmology should occur when indicated.
When Bell's Palsy Does Not Resolve
For the patients who fail to recover adequate facial function within 3 to 6 months, several additional treatment modalities are available. A significant complication of incomplete recovery is the development of synkinesis, which occurs when aberrant reinnervation of the facial nerve leads to involuntary muscle movements coupled with voluntary ones.8 Onset of synkinesis and hypertonicity typically occurs 4-6 months after initial episode of paralysis. Common examples include eye closure when smiling (oralocular synkinesis), platysma contraction with eye closure, or chin dimpling during blinking. Patients may also experience facial tightness, hypertonicity, and asymmetry at rest. These sequelae can be as distressing as the initial paralysis and significantly impact social interactions and quality of life.9 Advanced interventions for these patients generally fall into three categories, which include neuromuscular retraining, chemodenervation, and surgical reconstruction. Notably, transcutaneous
electrical stimulation is NOT recommended for nerve recovery and may be associated with increased synkinesis, though further research is needed to definitively establish this relationship.
Neuromuscular Retraining
Physical therapy with specialized neuromuscular retraining has emerged as an effective treatment for synkinesis and persistent asymmetry. This therapy focuses on restoring symmetry at rest, controlling synkinetic movements, and improving voluntary movement patterns through mirror feedback and specific exercises.10
Chemodenervation
Botulinum toxin injection has become a mainstay for managing nonflaccid facial paralysis. Injection of the affected side can reduce synkinetic movements and spasm, while contralateral injection can improve symmetry at rest and with animation.11 Patients require ongoing treatment every 3 to 4 months for optimal results.
Surgical Options
For patients with persistent severe paralysis, surgical management may be indicated. The available options can be categorized as static procedures, dynamic reanimation techniques, or selective neurectomy and myectomy. Static procedures include upper eyelid weight placement for lagophthalmos, brow lift, lower lid tightening, and facial sling procedures to improve oral commissure position.12 For patients who develop severe synkinesis, selective neurectomy and/or myectomies may be considered as more permanent solutions to reduce synkinetic movements.13 For patients with paralysis without recovery, nerve transfer procedures offer the best opportunity for restoring voluntary facial movement when performed within 12-18 months of onset, before irreversible muscle atrophy develops. These procedures, such as masseteric to facial or hypoglossal to facial nerve transfer, redirect an intact
Evidence-Based Management
and
Advanced Treatment
Options for Bell’s Palsy in Pennsylvania
Evidence-Based Management and Advanced Treatment Options for Bell’s Palsy in Pennsylvania
motor nerve to reinnervate the paralyzed facial muscles.14,15 Often, these procedures are combined to optimize outcomes. When paralysis persists beyond 18 to 24 months and the denervated facial muscles have undergone irreversible atrophy, free functional muscle transfer using gracilis or other muscle provides an alternative option for smile reanimation.16
nerve to reinnervate the paralyzed facial muscles.14,15 Often, these procedures are combined to optimize outcomes. When paralysis persists beyond 18 to 24 months and the denervated facial muscles have undergone irreversible atrophy, free functional muscle transfer using gracilis or other muscle provides an alternative option for smile reanimation.16
Table 1: Advanced Treatment Options for Bell's Palsy Patients who Fail to Recover Spontaneously or Develop Complications Treatment
Neuromuscular Retraining Exercises
Asymmetry, synkinesis
Table 1: Advanced Treatment Options for Bell's Palsy Patients who Fail to Recover Spontaneously or Develop Complications
Anecdotally associated with N/A - Avoid use RECOMMENDED increased synkinesis for nerve recovery
Evidence-Based Management and Advanced Treatment Options for Bell’s Palsy in Pennsylvania
Facial Nerve Specialty Centers in Pennsylvania
Pennsylvania has several centers offering comprehensive facial nerve care. Penn State Health Hershey Medical Center, the University of Pittsburgh Medical Center, Thomas Jefferson University Hospital, and Penn Medicine all provide multidisciplinary treatment options ranging from neuromuscular retraining and botulinum toxin therapy to advanced surgical reconstruction including nerve transfers and free functional muscle transfer for facial reanimation.
Role of the Comprehensive Otolaryngologist
The comprehensive otolaryngologist often serves as the essential first point of contact for Bell's palsy patients and has several key responsibilities in their care. Accurate diagnosis is paramount, and the physician must ensure that facial paralysis is truly idiopathic while excluding other etiologies. Timely treatment with corticosteroids within 72 hours of symptom onset can significantly improve outcomes. Patient education regarding eye protection is critical to prevent corneal complications. Finally, appropriate referral to specialized centers is essential when patients require advanced interventions. Patients who show minimal improvement or develop significant synkinesis should be referred to a facial nerve specialist for evaluation of advanced treatment options. Early recognition of these patients and timely referral can optimize their long-term functional and aesthetic outcomes.
Conclusion
While most Bell's palsy patients recover with conservative management, approximately one in five will have persistent deficits requiring specialized intervention. The comprehensive otolaryngologist plays a vital role in both acute management and recognizing when advanced treatments are needed. Facial nerve centers throughout
Pennsylvania offer comprehensive multidisciplinary care for these complex patients. By understanding the full spectrum of available treatments and maintaining a low threshold for specialty referral, otolaryngologists can optimize outcomes and ensure they receive the care necessary to restore both function and quality of life.
References:
1. Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002;(549):430. http://www.ncbi.nlm.nih.gov/ pubmed/12482166
2. Holland NJ, Bernstein JM. Bell’s palsy. BMJ Clin Evid. 2014;2014. http://www.ncbi.nlm. nih.gov/pubmed/24717284
3. Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell’s palsy. Otolaryngol Head Neck Surg. 2013;149(3 Suppl):S1-27. doi:10.1177/0194599813505967
4. Zainine R, Sellami M, Charfeddine A, Beltaief N, Sahtout S, Besbes G. Ramsay Hunt syndrome. Eur Ann Otorhinolaryngol Head Neck Dis. 2012;129(1):22-25. doi:10.1016/j.anorl.2011.08.003
5. Clark JR, Carlson RD, Pachner AR, Sasaki CT, Steere AC. Facial paralysis in lyme disease. Laryngoscope. 1985;95(11):13411345. doi:10.1288/00005537198511000-00009
6. Engström M, Berg T, Stjernquist-Desatnik A, et al. Prednisolone and valaciclovir in Bell’s palsy: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2008;7(11):993-1000. doi:10.1016/S1474-4422(08)70221-7
7. Sullivan FM, Swan IRC, Donnan PT, et al. Early Treatment with Prednisolone or Acyclovir in Bell’s Palsy. N Engl J Med. 2007;357(16):1598-1607. doi:10.1056/ NEJMoa072006
8. Husseman J, Mehta R. Management of Synkinesis. Facial Plast Surg. 2008;24(2):242-249. doi:10.1055/s-2008-1075840
9. Lorenz FJ, Schopper HK, Lighthall JG. Chemodenervation is Associated With Reduced Mental Health Disorders in Patients With Synkinesis. Otolaryngol Neck Surg. Published online August 15, 2024. doi:10.1002/ohn.936
10. Diels HJ. Facial Neuromuscular Retraining for Synkinesis. In: Management of Post-Facial Paralysis Synkinesis. Elsevier; 2022:75-90. doi:10.1016/B978-0-32367331-0.00009-9
11. Hetzler L, MacDowell S, Diels J, VandeWater T, Azzizadeh B. Chemodenervation Algorithm: Functional and Aesthetic Considerations for Facial Harmony in Patients with Post-Facial Paralysis Synkinesis. Facial Plast Surg Aesthetic Med. 2023;25(6):512-518. doi:10.1089/fpsam.2022.0206
12. Ibrahim A, Rabie A, Kim P, et al. Static Treatment Modalities in Facial Paralysis: A Review. J Reconstr Microsurg. 2013;29(04):223-232. doi:10.1055/s-0032-1333317
13. Dimovska EOF, Jensson D. Myectomies and Neurectomies in the Management of Hyperkinetic Asymmetries and Synkinesis in Facial Palsy. In: Facial Palsy. Springer International Publishing; 2021:319-328. doi:10.1007/978-3-030-50784-8_30
14. Klebuc MJA. Facial Reanimation Using the Masseter-to-Facial Nerve Transfer. Plast Reconstr Surg. 2011;127(5):1909-1915. doi:10.1097/PRS.0b013e31820e9138
15. Hamdi OA, Jones MK, Ziegler J, Basu A, Oyer SL. Hypoglossal Nerve Transfer for Facial Nerve Paralysis: A Systematic Review and Meta-Analysis. Facial Plast Surg Aesthetic Med. 2024;26(2):219-227. doi:10.1089/fpsam.2023.0144
16. Lindsay RW, Bhama P, Weinberg J, Hadlock TA. The Success of Free Gracilis Muscle Transfer to Restore Smile in Patients With Nonflaccid Facial Paralysis. Ann Plast Surg. 2014;73(2):177-182. doi:10.1097/ SAP.0b013e3182a0df04
From Invitation to Invoice: A Cautionary Tale in Academic Publishing
F. Jeffrey Lorenz, MD, Jessyka G. Lighthall, MD, FACS Penn State Department of Otolaryngology-Head and Neck Surgery
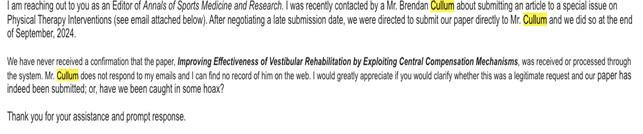
Unsolicited invitations to submit manuscripts have become a routine feature of academic life. The email we received looked like dozens before it, referencing a special issue of a respectable sounding journal (named something strikingly similar to an established journal) with a guest editor. It praised our work and extended an invitation to submit a review article due to our expertise in the topic (Figure 1).
Upon completion of the manuscript, we were directed to submit the manuscript directly to the guest editor rather than through a conventional editorial management system. Following submission, the expected markers of legitimate editorial handling did not materialize. There was no automated confirmation of receipt of the manuscript, no communication regarding peer review, and no indication of the editorial decisionmaking process. Repeated follow-up emails went unanswered. Concerned, a senior coauthor contacted an individual she knew who was listed as an editor for the journal to verify the legitimacy of the process. The response was unequivocal: the named individual stated they were not affiliated with the journal and could not confirm its legitimacy (Figure 2). This
explicit denial of editorial association is notable, as false or unverifiable editorial board membership is a defining characteristic of predatory journals.
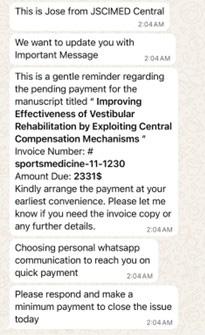
Weeks later, a payment demand was issued for over $2,000, referencing an invoice number and the manuscript title. The message emphasized urgency and suggested that a minimum payment be made immediately to “close the issue”. This demand was not preceded by any formal acceptance letter, peer-review feedback, or disclosure of publication fees at the time of submission. Even more striking, the payment request was delivered via WhatsApp, with the sender stating that this platform was chosen to facilitate rapid payment (Figure 3).
Figure 1. Initial unsolicited email invitation requesting direct submission to a guest editor.
Figure 2. Email correspondence documenting denial of editorial affiliation by a named editor.
From Invitation to Invoice: A Cautionary Tale in Academic Publishing
Figure 3. Initial unsolicited email invitation requesting direct submission to a guest editor.
References
1. Shamseer L, Moher D, Maduekwe O, Turner L, Barbour V, Burch R, Clark J, Galipeau J, Roberts J, Shea BJ. Potential predatory and legitimate biomedical journals: can you tell the difference? A cross-sectional comparison. BMC Med. 2017 Mar 16;15(1):28. doi: 10.1186/ s12916-017-0785-9. PMID: 28298236; PMCID: PMC5353955.
2. Laccourreye O, Rubin F, Maisonneuve H. “Predatory” journals threatening the scientific medical press. Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135(1):37–39. doi:10.1016/j. anorl.2017.08.003. PMID: 28916412.
3. Piccirillo JF, Chandra R, Fisher EW, et al. Open Access—Is There a Predator at the Door? JAMA Otolaryngol Head Neck Surg. 2018;144(4):289–290. doi:10.1001/jamaoto.2018.0026
4. Cobey KD, Grudniewicz A, Lalu MM, Rice DB, Raffoul H, Moher D. Knowledge and motivations of researchers publishing in presumed predatory journals: a survey. BMJ Open. 2019 Mar 23;9(3):e026516. doi: 10.1136/bmjopen-2018-026516. PMID: 30904874; PMCID: PMC6475169.
5. Mercier E, Tardif PA, Moore L, Le Sage N, Cameron PA. Invitations received from potential predatory publishers and fraudulent conferences: a 12-month early-career researcher experience. Postgrad Med J. 2018 Feb;94(1108):104-108. doi: 10.1136/ postgradmedj-2017-135097. Epub 2017 Sep 14. PMID: 28912190; PMCID: PMC5800329.
Ellie Goldenberg Award Nominations
The Goldenberg Family and the Pennsylvania Academy of Otolaryngology – Head and Neck Surgery are now accepting nominations for The Ellie Goldenberg Award. Established by the Goldenberg Family, The Ellie Goldenberg Award is a tribute to Ellie’s legacy of hard work, dedication, and kindness.
Previous recipients include: Kasra Zai, MD and Nicole Molin, MD (2023) Cheng Ma, MD (2024) Annie Moroco, MC (2025)
To be eligible, the nominee must be an Otolaryngology resident within the Commonwealth of Pennsylvania who demonstrates:
• a strong work ethic • diligence • initiative
and kindness
Submission requirements include a statement of support and a letter from their program director (PDF or DOC).
The award will be presented at the PAO-HNS Annual Meeting dinner on Friday, June 12, 2026 at the Lancaster Mariott at Penn Square. To nominate a deserving resident, please visit our website. You will be prompted to log in or create an account).
Submissions will be accepted until April 6th
Questions can be directed to info@otopa.org
Log in to the member portal at https://pao-hns.joynportal.com/portal/#login or scan the QR code to pay today.
Member benefits include Soundings Newsletter, Legislative Representation, Discounted Meeting Registration and more!
Group Dues Discounts
If you’re part of a large organization, contact us about group dues. Discounts are available to otolaryngologists in a group practice when two or more qualifying physicians are PAO-HNS members:
n 2–10 members:10% discount
n 11–20 members: 20% discount
n 21+ members: 30% discount
Renew today and continue enjoying the benefits of PAO-HNS membership!
BOG Update Winter 2026
Karen A. Rizzo, MD FACS
Lancaster ENT, LLC
Past Chair AAO/BOG
Director Private Practice/AAOHNS
Since the completion of the annual Academy meeting in Indianapolis in October 2025, the American Academy of Otolaryngology Head & Neck surgery has been busy advocating for issues impacting the way we practice medicine. It has supported legislation giving physicians an inflationary payment update. The Academy along with 14 other physician groups sent a letter to Congress supporting HR 6160, the Strengthening Medicare for Patients and Providers Act, which would provide an annual inflationary update to Medicare physician payment tied to the Medicare economic index. Medicare’s persistent yearly payment cuts fail to keep pace with inflation and threaten practice stability making it more difficult to recruit staff, keep clinics financially solvent, and maintain access for Medicare patients. The letter warned that these pressures can force practices to limit Medicare participation, consolidate, or close. The Academy also urged congressional action on prior authorization reform where it joined the AMA and 124 other national medical specialty societies and state medical associations in a letter urging House and Senate leadership to take immediate
action on the Improving Seniors Timely Access to Care Act of 2025 citing multiple studies documenting the negative impact of prior authorization requirements on patient care.
For the first time in six years CMS has finalized an increase to the Medicare conversion factor for 2026. There was however a decrease to work RVU's called the efficiency adjustment of 2.5% for nearly all non time based codes. Codes exempt from this policy include E/M codes, new codes for 2026, and Medicare telehealth codes. Changes to practice expense methodology for services performed in hospital settings was also finalized. For otolaryngologists CMS estimates a -12% impact on total allowed charges in facility settings. In contrast non facility settings can anticipate a 3% increase.
For more information on these changes I refer you to the AAO website under Bulletin (entnet.org). For the first time ever the American Academy of Otolaryngology Head and Neck surgery 2026 OTO forum will be held in Louisville KY which is a welcoming destination that blends sports heritage, modern flair, and great hospitality. There will be two days dedicated to elevating the business of
medicine and strengthening the collective voice of the otolaryngology community at this meeting. Great opportunities to get updated on best practices, reimbursement strategies, networking, and advocacy updates will be available. All are urged to attend whether in private practice, hospital based employment, or academic institutions.
The annual meeting for the Academy for 2026 will be held in Los Angeles CA from October 17th to 20th. This is an opportunity to educate, collaborate, and get more engaged in political advocacy with the Academy. You're encouraged also to donate to the ENT PAC. Supporting the ENT PAC ensures physicians not policymakers, without clinical experience, help shape the laws that affect patient care and the sustainability of ENT practices.
Lastly the new leadership of the Board of Governors involves Dr. Steve Cragle from St. Cloud, MN who is chair, and Dr. Eileen Rayner from Duke University chair elect. The new president of the American Academy of Otolaryngology Head & Neck Surgery is Dr. Eugene Brown from Charleston ENT and Allergy and president-elect is Dr. Daniel Chelius from Houston.
A Remembrance of Max Ronis, MD
Max Ronis, the longest serving Chairperson of our Temple Department, died last year. Max was born during the Great Depression in Southwest Philadelphia in the shadow of the GE switch gear plant. His uncles were butchers in Kensington. His father, BJ worked as a pharmacist while studying medicine at Temple and later made house calls as a general practitioner. His mother was a recent immigrant from Ukraine, so Max spoke mostly Yiddish until he went to public school.
At the start of the Second World War, Max’s father joined the Army medical corps and 13-year-old Max moved with his family to Walla Walla, Washington. It was a strange and wonderful place for a city boy. He fished for steelhead trout in the town’s stream and joined
the Future Farmers of America. When the Army relocated the family to Van Nuys California, Max learned to drive a tractor, slop pigs and raise bamboo for musical instrument reeds. Eventually, he drove the family home across America at age 16 on an agricultural driver’s license.
At the end of the war the family returned to SW Philly and BJ re-opened his general practice while studying ENT at the Graduate Hospital. Max (everyone called him Lee then) finished public school at Bartram High. When he started college at Muhlenberg, Max felt ill-prepared. ‘My roommate had this funny sliding ruler to do math. I was better at wood and metal shop.’ After a few years of struggle, he found his way to Temple Medical School, graduating in 1956. Max met his future wife Mary during medical school. They married in 1954 and raised three girls on a resident’s salary.
David Myers, the chairman of ENT at Temple welcomed Max to the residency. Myers was a generous teacher and Max learned quickly. Once, after a particularly bloody tonsillectomy Myers sighed, “There are some things you just don’t get any better at” – which Max frequently quoted later on.
By then BJ had an established ENT practice in Center City and had learned otology skills visiting Julius Lempert in New York and John Shea in Memphis. Max joined him after residency and learned
to use the newly developed operating microscope to do tympanoplasties and stapedectomies. Max and his father developed a set of ear instruments that still bears the Ronis name.
BJ succeeded David Myers as department chair and eventually Max succeeded his father. Max was perhaps the last part-time Temple chairperson. He maintained the Spruce Street private practice in his family home while also seeing patients and operating at TUH. This did not diminish his achievements at Temple. Max trained over 60 residents, expanded the Department to seven faculty, built a multi-million-dollar tinnitus research laboratory, and served as a Vice President of the Triological Society. Max fought to establish our Department’s place in head and neck surgery at Temple and to build our Pediatric ENT presence at St. Christopher’s.
Max continued to operate into his 70s and to see patients at Spruce Street well into his 80s. When interviewed years later about his achievements he said while all three pillars of academics were important, there was nothing for him like teaching. He inspired 3 decades of medical students to pursue Otolaryngology as a specialty. Max trained scores of residents, not only in the skills of the ENT, but through his energy, humor, and kindness, he taught them to be better doctors.
We miss Max.
Annual Meeting Recap
First Place Oral Presentation
Yash Satyendra Dixit, University of Pennsylvania
The Effect of Route of Breathing on Pharyngeal Collapsibility in Patients with Obstructive Sleep Apnea: A Pilot Study
Second Place Oral Presentation
Pallavi Kulkarni, MD, Penn State
Genomic Structural Variation of Anaplastic Thyroid Cancer Using Optical Genome Mapping
First Place Poster Presentation
Christopher Tseng, MD, Penn State
Exploring the Impact of Obesity on Thyroid Pathology in the DUOX2Y1200H Murine Model of Thyroid Cancer
Second Place Poster Presentation
Mimi Kim, BS, University of Pennsylvania
Long-Term Quality of Life Outcomes in Pediatric Surgical Otitis Media Management
Jeopardy Winner—University of Pittsburgh Medical Center Team Members:
Allison Rolling, MD
Nanki Hura, MD
Shivam Patel, MD
Philip Dunn
As for legislation, in July of this year the Pennsylvania House of Representatives passed HB 80 which would authorize Pennsylvania to join an Audiology and Speech Language Pathology Compact. Although 36 states have passed enabling measures to enter into the compact, PAO has consistently opposed the arrangement citing conditions that:
• do not provide adequate oversight of Audiology and SpeechLanguage Pathology providers,
• do not set criteria for the education and training of providers,
• do not establish vetting of credentials and professional behavior, and
• do not establish clear processes for transparency regarding disciplinary and/or legal actions against providers from outside the Commonwealth, which then essentially replacing PA Pennsylvania laws and licensing regulations.
PAO-HNS is also strongly concerned that:
• there is currently no acceptable or well-documented process for ensuring patient safety,
• no rules and bylaws have been created for review by states considering entering the Compact, and
• a data system for documentation and communication between compact states has yet to be implemented.
Legislative Update
The legislation is now in the Senate Consumer Protection and Professional Licensure Committee. PAO has sent a letter to the Chairman of this committee expressing PAO’s concerns and meetings are being planned to discuss our position in the coming weeks.
Additionally, On Sepetember 23 of 2025, the PA Hearing Health Association and the PA Audiology Association met with state officials from the Department of Human Services to discuss potential changes to Act 262 of 1976, known as the Hearing Aid Sales Registration Act. This statute was last substantially amended in 1998. Among the proposed changes put forth by PHHA was language that would allow hearing aid fitters to do cerumen removal. Although PAO was not present at the meeting, Dr. Huntley provided a letter expressing PAO’s opposition to this practice. In the letter, the following points were presented:
• Lack of Standardized Training and Certification: The proposal fails to establish a uniform, accredited training program or certification process specific to cerumen management. While there are general references to training requirements, they are vague and lack detail regarding required hours, clinical supervision, and competency verification.
• Absence of Oversight and Regulation: There is no clear provision for state-level oversight, clinical supervision, or ongoing quality assurance related to cerumen removal. Without appropriate regulation, there is a substantial risk or harm to patients undergoing these procedures outside of medical settings.
• Continuing Education Deficiencies: There are no enforceable requirements for continuing education specific to cerumen management. This is particularly concerning given the dynamic nature of best practices and safety protocols in otologic care.
• Misalignment with Scope of Practice: The proposal permits hearing aid specialists to perform clinical assessments and interventions – including otoscopy, auditory testing, and cerumen management – that overlap significantly with the scope of practice traditionally and safely performed by licensed medical professionals, specifically Otolaryngologists and they designated advanced practice providers.
• Public Health and Liability Concerns: Allowing non-accredited or supervised professionals to conduct procedures on the external auditory canal without appropriate training, medical backup, or malpractice accountability creates unacceptable risk to public safety. Even within medical practices, cerumen removal can result in complications that require prompt diagnosis and treatment by a physician.
There has been no bill introduced for PHHA’s proposals but we must remain vigilant to present our opposition if and when a measure might emerge.
Thank You To Our Exhibitors:
Acclarent—Integra LifeSciences
Acera Surgical
Align ENT + Allergy
Atos Medical
Axogen
Cochlear
Cuesta Medical Solutions
ENT and Allergy Associates, LLP
Everis Medical
Fuel Medical Group
Grace Medical Inc.
GSK
Inspire Medical Systems, Inc.
J&J MedTech
Karl Storz
LivaNova
Medtronic ENT
Merck & Co.
Naveris
Penn Medicine
Sanofi / Regeneron
Smith+Nephew
Stryker ENT
Vertex Pharmaceuticals
A S pecial Thank You To…
Industry Symposium Sponsor
Sanofi/Regeneron
Open Table Discussion and Networking with Residents
ENT and Allergy Associates, LLP
Women in Otolaryngology Sponsor
Stryker
HOW TO GET INVOLVED!
As a member of the Pennsylvania Academy of Otolaryngology – Head and Neck Surgery (PAO-HNS), there are several ways you can actively engage and contribute to the field of otolaryngology in Pennsylvania
1. Participate in Annual Meetings and Events
PAO-HNS hosts an Annual Scientific Meeting, which serves as a platform for members to present research, attend educational sessions, and network with peers. Engaging in these events can enhance your professional development and keep you updated on the latest advancements in the field.
2. Serve on Committees and Executive Council
Members have the opportunity to serve on various committees or the Executive contributing to the governance and strategic direction of the organization. This involvement allows you to play a pivotal role in shaping the future of otolaryngology practice within the state.
3. Engage in Advocacy Efforts
PAO-HNS is dedicated to advocating for the interests of otolaryngologists and their patients. By participating in advocacy initiatives, you can help influence healthcare policies and regulations that impact the practice of otolaryngology in Pennsylvania.
4. Contribute to Educational Resources
Members can contribute to the development of educational materials and resources, aiding in the dissemination of knowledge and best practices within the otolaryngology community. This can include authoring articles, assisting with editing our newsletter, Soundings, or participating in educational workshops. Bring your ideas and energy!
5. Mentor Emerging Professionals
Experienced members are encouraged to mentor medical students, residents, and fellows-in-training. Through mentorship, you can provide guidance, share experiences, and support the professional growth of the next generation of otolaryngologists.
6. Share Your Givebacks and Commitment
The Pennsylvania Academy of Otolaryngology – Head and Neck Surgery proudly supports the individual projects and community initiatives our members pursue, both locally and globally. Whether you are involved in community service, patient education, medical missions, or other outreach efforts, we want to hear from you. Your stories inspire others and highlight the many ways otolaryngologists make a meaningful impact beyond the clinic. We invite you to share your experiences so we can help celebrate and amplify your work. For more information on how to get involved, you can visit the PAO-HNS website or contact them directly at info@otopa.org or 833-770-1544.
President
Colin T. Huntley, MD
Associate Professor, Jefferson University, Otolaryngology— Head & Neck Surgery
Immediate Past President
Jessyka G. Lighthall, MD, FACS
Chief, Division of Facial Plastic and Reconstructive Surgery
Director, Facial Nerve Disorders Clinic
Medical Director, Esteem Penn State Health
Cosmetic Associates Fellowship Director, Facial Plastic and Reconstructive Surgery
Associate Professor, Department of Otolaryngology-Head & Neck Surgery and Department of Surgery
Penn State College of Medicine
The Pennsylvania Academy of Otolaryngology—Head & Neck Surgery
2023-2025
Jessyka G. Lighthall, MD, FACS
2021-2023 David M. Cognetti, MD, FACS 2019-2021 Johnathan D McGinn, MD 2017-2019 Ahmed M.S. Soliman, MD
2015-2017 Jeffrey P. Simons, MD, FACS 2013-2015 David Goldenberg, MD, FACS 2011-2013 Jason Newman, MD, FACS 2009-2011 Scott M. Gayner, MD
2007-2009 Robert L. Ferris, MD, PhD, FACS
2005-2007 Robert T. Sataloff, MD, FACS
2003-2005 Edmund A. Pribitkin, MD, FACS
2001-2003 Karen A. Rizzo, MD, FACS
1999-2000 J. David Cunningham, MD, FACS
1998-1999 Carl L. Reams, MD
1997-1998 Phillip K. Pellitteri, DO, FACS
1996-1997 Barry E. Hirsch, MD
1995-1996 Alan M. Miller, MD, FACS
1994-1995 Ernest L. McKenna, Jr., MD, FACS
1993-1994 Frank I. Marlowe, MD, FACS
1992-1993 Thomas L. Kennedy, MD, FACS
1991-1992 G. William Jaquiss, MD
1990-1991 Louis D. Lowry, MD, FACS
President-Elect
Pamela C. Roehm, MD, PhD
St. Luke’s University Health Network, Lehigh Valley, PA
Division of Otolaryngology— Head and Neck Surgery
Secretary Treasurer
Neerav Goyal, MD, MPH, FACS
Professor, Department of Public Health Sciences
Penn State Cancer Institute
Cosmetic Associates Fellowship Director, Facial Plastic and Reconstructive Surgery Associate Professor, Department of Otolaryngology-Head & Neck Surgery and Department of Surgery
Penn State College of Medicine
PAST PRESIDENTS
Pennsylvania Academy of Ophthalmology and Otolaryngology (1943 – 1990)
1989 Helen F. Krause, M.D.
1988 Dorothy C. Scott, M.D.
1987 Webb Hersperger, M.D.
1986 Edward A. Jaeger, M.D.
1985 Donald P. Vrabec, M.D.
1984 James L. Curtis, M.D.
1983 George H. Conner, M.D.
1982 George J. Gerneth, M.D.
1981 Donald B. Kamerer, M.D.
1980 Jerome Dersh, M.D.
1979 Eugene B. Rex, M.D.
1978 William C. Frayer, M.D.
1977 Silvio H. DeBlasio, M.D.
1976 Paul A. Cox, M.D.
1975 Louis E. Silcox, M.D.
1974 Robert D. Mulberger, M.D.
1973 James M. Cole, M.D.
1972 C. William Weisser, M.D.
1971 Joseph P. Atkins, M.D.
1970 Robert J. Beitel, Jr., M.D.
1969 H. Ford Clark, M.D.
1968 Harold G. Scheie, M.D.
1967 John T. Dickinson, M.D.
1966 Benjamin F. Souders, M.D.
1965 Merril B. Hayes, M.D.
1964 Glen G. Gibson, M.D.
1963 Raymond E. Jordan, M.D.
1962 Robert E. Shoemaker, M.D.
1961 Norbert E. Alberstadt, M.D.
1961 Benjamin H. Shuster, M.D.
1960 John Knox Covey, M.D.
1959 Paul C. Craig, M.D.
1958 Murray F. McCaslin, M.D.
1957 J. Floyd Buzzard, M.D.
1956 Chevalier L. Jackson, M.D.
1955 William T. Hunt, Jr., M.D.
1954 James H. Delaney, M.D.
1953 Paul McCloskey, M.D.
1952 Samuel T. Buckman, M.D.
1951 Matthew S. Ersner, M.D.
1950 Jay G. Linn, Sr., M.D.
1949 Daniel S. DeStio, M.D.
1948 James J. Monahan, M.D.
1947 Gilbert L. Daily, M.D.
1946 Thomas F. Furlong, Jr., M.D.
1945 Lewis T. Buckman, M.D.
1944 Lewis T. Buckman, M.D.
1943 James E. Landis, M.D.
400 Winding Creek Blvd.
Mechanicsburg, PA 17050-1885
BENEFITS OF MEMBERSHIP
Soundings Newsletter
Members receive hard copies of Soundings, the PAO-HNS member newsletter
Legislative Representation
Representation in the state legislature via our own lobbyist
Direct Input with Medicare
Representation on the Novitas Solutions Carrier Advisory Committee (CAC), which has input into local Medicare reimbursement policy
Specialty Events Listings
Members may post their specialty events at no cost
Priority Review for ENT Journals
Priority review for possible publication in ENT Journal, the official journal of the PAO-HNS
National Representation
Representation on the American Academy of Otolaryngology-Head Neck and Neck Surgery's Board of Governors
Discounted Registration for Annual Science Meeting
Discounted registration to our annual Scientific Meeting featuring CME-approved educational seminars focused on current otolaryngology topics and family-oriented social functions