Directors, The American Association of Orthodontists Foundation
Dr. John Carter, Leawood, KS
Dr. Neal Kravitz, Chantilly, VA
Editor
Dr. Jim Vaden, Cookeville, TN
ON THE COVER:
Top left: Dr. Eric Nease
Top right: Dr. Matt Ng
Center: Dia de los Muertos Happy Hour
Bottom left: Committee on Annual Meeting Planning
Bottom right: SSO Members
Presidents’ Message
Dr. Christie Ellis | Dr. Preston Miller
June 3, 2025 marked the first birthday of the SSO, and what a year it has been.
Our first year highlights included a smooth transition to combine operations of the SAO and SWSO as well as a profitable annual session in Orlando.
Our leaders are united in the goal of continuing to build a strong constituency that reflects the shared vision that we are truly stronger together. SSO is moving forward and leading the effort to strengthen the constituency model with the goal of improved organizational support for our components, increased opportunities for our member volunteers, leadership training for our future leaders and unforgettable must-attend annual sessions in exciting cities.
We are thankful for the opportunity to lead the SSO during this next year and must give thanks to the people who play critical roles in supporting us in our job. Our Executive Committee –Don Balhoff, Kyle Shannon, Jeremy Albert and Chopper Synder volunteer countless hours and wear too many leadership hats to list. They are dedicated servants of the SSO, consummate professionals and good friends. The future of the SSO is in good hands.
The SSO covers 15 states, each of which has its state related professional concerns. Each state in the SSO is represented on our Board of Directors by a Component Director. It would be impossible to be aware of what is happening without boots on the ground, and we are thankful for the help of our Component Directors for fulfilling that important role. Because of these men and women, the SSO is aware of state-level issues that impact Medicaid reimbursement and specialty licensure as well as other critical issues that are important to our membership.
Thanks also goes to the members of CAMPJim Martin (2026 Chair), Theresa Coleman, Kalynn Naglieri, Eric Park, Prem Premaraj, Kyla Swearingen and Don Wilcoxon. These members ensure that our annual session is a fun, can’t miss meeting. They are the “hosts and hostesses with the mostest”. The SSO is fortunate to have so many creative “event planners” who also double as orthodontists.
The SSO AAO Board of Trustees, Dr. Richard Williams, Dr. Steve Robirds, Dr. Enrique Cruz and Dr. India Collier attend our meetings and serve as mentors, trusted colleagues and voices of experience and wisdom. Their understanding of the inner workings of the SSO serve us well within the AAO. While the SSO is united in its effort, it is recognized as two separate entities by the AAO in order to ensure fair representation for our membership. Dr. Williams is the SAO Trustee and Dr. Robirds is the SWSO Trustee. Dr. Cruz and Dr. Collier are Trustees at Large. We are so thankful for their leadership.
There is not enough space in this newsletter to thank the many, many volunteers who serve on Councils, on Committees, in academic institutions, and in so many other positions within our specialty. Our organization would not be what it is without you and we THANK YOU for your time and service.
Finally, we would be remiss if we did not give recognition and thanks to ZuBu, our Executive Director team – Lissette Zuknick, Kelsey Bulnes and Jaclyn Whiddon – for keeping the SSO organized, on task and prepared.
This coming year we are excited to continue the process of building the future of the SSO. Challenges lie ahead, but we are confident that the SSO is well positioned to handle the inevitable headwinds. We ask that, as members, you support the SSO by getting involved. Consider volunteering to join a Leadership Development Class, contribute to the PAC, volunteer at our annual session or simply read your newsletter and stay up to date with SSO news.
Highlights from the SSO meeting in San Antonio, Texas – Yee-haw!!
One of the things we are most excited about happens next Fall. We can’t wait for all SSO members and their staffs to celebrate with us in Nashville on Oct 15-17, 2026. Not only will we have great CE for you and your team, our venue is within walking distance to Broadway. Our Friday night celebration will be at Luke Combs Category 10 Honky Tonk! This exciting venue will be closed to the public. Expect to line dance on the dance floor, sample some beverages and hear some great live music!
While the SSO is still quite young with most of its future still to be written. We are the old timers who have reached the final year on the SSO Executive Board. We have been blessed by all the former leaders who have held this position and we look forward to continuing to build on their efforts. It is a privilege and we are honored to serve as your SSO Co-presidents.
Dr. Christie Ellis
Dr. Preston Miller
Trustees’ Report
This report was written by Dr. Steve Robirds, SWSO Trustee, in consultation with Dr. India Collier, Trustee at Large, Dr. Enrique Cruz, Trustee at Large, and Dr. Richard A. Williams, SAO Trustee.
As I write this, we have returned from an exciting SSO meeting in San Antonio! Over 1,000 people attended.
All attendees enjoyed excellent lectures, an exhibit hall filled with the latest in technology and equipment, a fun round of golf at a course built inside an old rock quarry, and a fitting finish by having Sea World all to ourselves for one fun night of food, shows, and, of course, roller coasters (I personally rode 4 different ones)!!
The weather in San Antonio was perfect. Under a clear blue sky, lows were in the 60’s and highs in the low 80’s. A special thanks goes out to CAMP (Committee on Annual Meeting Planning) for all of the hard work and dedication that made this meeting great. Our Executive Management Team, ZuBu, kept all meetings and activities on time with no disruptions. This team is amazing. All SSO members should feel so good about the team. They keep us moving forward as we grow and continue to find the best ways to serve each of you, our members. Next year’s annual session will be in Nashville in mid-October, so put it on your calendar!
Special thanks goes out to Drs. Eric Nease and Matthew Ng for their strong leadership as our co-Presidents this past year. They kept us moving forward and accepted each challenge with the energy and intelligence necessary to oversee an organization of which we can all be proud. Our new co-Presidents are Drs. Christie Ellis and Preston Miller. I can promise you they have hit the ground running along with your SSO Board. There is always a lot to do, and with ZuBu ready to carry out the actions of the Board, all of you will continue to see the SSO provide the member benefits that keep our practices and specialty strong.
At the national level, your AAO Board of Trustees met in St. Louis for our quarterly board meeting. As always, there were a myriad of topics to discuss. Steve Siegel is now over half way through his Presidency. We will close out his Presidency at the May 2026 Orlando Annual Session. As always, it will be an action packed meeting with one night dedicated to the AAO at a Universal Studio Amusement Park! Also, the Winter Conference is set for January 23-25 at the JW Marriott in Phoenix, Arizona. The topic this year is “The Sagittal Dimension: Approach to Non-Surgical Cl II and CL III Correction “. Last year was close to a sell-out, so get your reservation in now!
One thing we can point to with pride is that the SSO has not one, not two, not even three, but four Trustees! Dr. Williams, myself, and two Trusteesat-Large – Drs. Enrique Cruz and India Collier. This is truly remarkable and it provides a strong voice from our part of the country at the Trustee level. If there is anything that needs the help of a Trustee, do not hesitate to reach out!
Dr. Steve Robirds
One-Minute Task:
Make sure you are receiving emails
from SSO
The SSO is updating its email address to ssoevents@ssortho.org.
Since combining the operations of the SAO and SWSO, we have used the SAO email address. During the first part of 2026 we will switch to the new SSO address for sending monthly eNews, Annual Session information, and special announcements.
WHAT TO DO:
Please scan the QR code to ensure you are subscribed. You must use the email address attached to your AAO Membership
Reasons you may not be receiving emails:
• New email sorting features may segment messages away from your Primary inbox. Sorting helps declutter your inbox, but you have to be intentional about looking for newsletters to which you are subscribed (often on an Updates tab).
• If your email system “bounced” an email from us in the past, your address was automatically unsubscribed. Be sure to scan the QR code to opt back in to our newsletters, using the email address attached to your AAO Membership.
Make sure you don’t miss a thing:
• Add our new email address ssoevents@ssortho.org and saoevents@saortho.org to your address book.
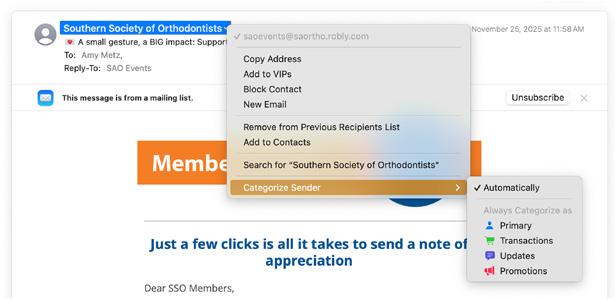
• Change the way your email system categorizes the sender, moving these two email addresses to your Primary tab. Every email client is different (Apple, Microsoft, etc.), but start investigating yours by right-clicking on the email address for options.
Apple Mail automatically sorts incoming emails into the following category segments:
Primary: Contains personal and time-sensitive messages. Only emails in this category are counted towards your unread count.
Transactions: Includes confirmations, receipts, and shipping notices.
Updates: Collects newsletters, social updates, and other news.
Promotions: Gathers emails with coupons and sales.
This feature helps declutter your inbox by separating personal messages from receipts, newsletters, and sales emails. You can also manually categorize a sender by using the “Categorize Sender” option, which applies to both current and future emails from that address.
How to utilize category segments when sending/ viewing emails:
Manually Categorize a Sender:
Right-click (or Control-click on Mac) a message, select “Categorize Sender,” and choose a category to apply it to all future messages from that sender.
View All Mail:
You can see all your messages by switching to the “All Mail” view, which is typically done by tapping the current category again or swiping left on the categories.
Fundraising Goal $1,800,000
FOR THE FUTURE
The future of orthodontics depends on our commitment to invest in the best educators. The AAO Foundation has launched For the Future – a campaign to invest in fellowships that will advance our specialty by helping educators. The Full-Time Faculty Fellowship is a two-year, $30,000 fellowship designed to supplement the salaries of young educators who are dedicated to orthodontic academics. In concert with AAO, and following the House of Delegates’ unanimous support to create this
powerful opportunity, this fellowship is our way of ensuring that the future is led by the most qualified and passionate individuals. Contributions will be matched dollar-for-dollar to create a fund to award three fellowships (awarded for two years) every year. To learn more about leadership opportunities, please call Brett Schott at the Foundation office: 314.292.6546 or bschott@aaortho.org
FRED A. GARRETT RESIDENT EDUCATION PROGRAM RETURNS
The AAO Foundation recognizes the importance of residents having the opportunity to experience an AAO Annual Session, and we support them through this program by offering a $300 incentive for first-time, and $100 for second-time resident attendees, to offset expenses to attend the conference.
Visit aaofoundation.net/residents to see the qualifications.
CLASSES FOR ORTHODONTIC RESIDENT EMPOWERMENT (CORE)
The AAO Foundation is proud to offer residents a complimentary six-module virtual course on business fundamentals that is led by Dr. Bill Layman. Use the QR code to register to gain access and complete it at your own pace.
GIVE THE GIFT OF A SMILE – VOLUNTEER WITH GIFTED SMILES TODAY!
Every day, orthodontists transform lives through confident, healthy smiles — and the AAO Foundation’s Gifted Smiles program offers a way to extend that impact even farther. By volunteering, you can provide essential orthodontic care to children who otherwise couldn’t afford treatment, restoring not only their smiles but their confidence and opportunities. The program makes it easy to get involved. It connects you with pre-screened patients in your area and offers administrative support every step of the way. A few hours of your time can make a lifelong difference — because a smile is one of the most powerful gifts you can give.
AAO FOUNDATION BREAKFAST
Register to attend the AAO Foundation Breakfast in Orlando when you register for AAO Annual Session. The Foundation will present the Eugene & Pauline Blair, Distinguished Service Award to:
Dr. Richard Williams
FOUNDATION STAFF
Brett Schott, Vice President | bschott@aaortho.org
Mindy Copp, Sr. Specialist, Marketing & Development | mcopp@aaortho.org
George Reinarman, Jr., Program Specialist | greinarman@aaortho.org
Tabitha Smith, Program Administration, Gifted Smiles | tsmith@aaortho.org
ABO Update
The American Board of Orthodontics Directors’ Report
Dr. Onur Kadioglu | Dr. Timothy Tremont
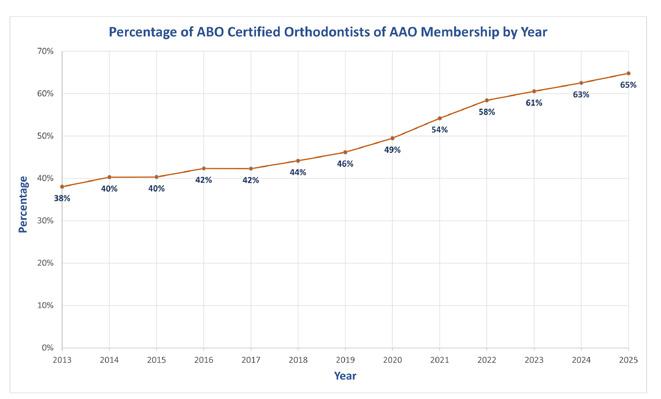
Currently, over 5,000 graduates of CODA accredited graduate orthodontic programs are Certified by The American Board of Orthodontics. This accounts for approximately 65% of the AAO active membership.
One of the ABO’s strategic objectives is to increase the number of board-certified orthodontists by promoting the value of certification and recertification. The ABO has seen consistent growth in certification over the past twelve years. This growth aligns us with our mission “to elevate the quality of orthodontic care for the public”.
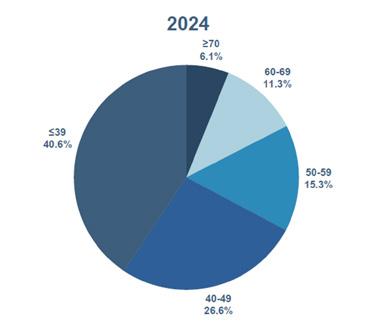
Demographics by Age Range
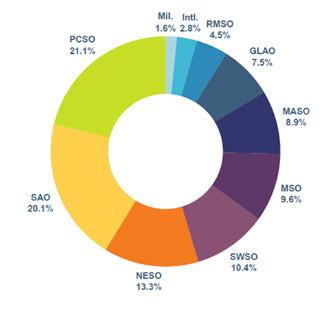
Percent of Total ABO-Board Certified by Constituent Organization
Volunteer Opportunities
The American Board of Orthodontics welcomes every certified orthodontist’s unique perspectives and strengths through a variety of leadership and professional growth opportunities. These opportunities will enable volunteers to make meaningful contributions to the specialty while advancing their own development.
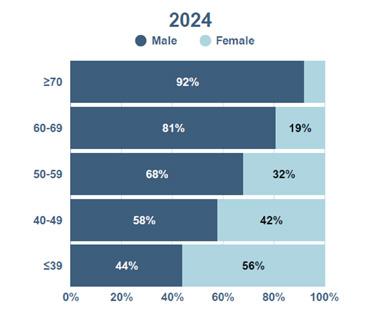
Gender by Age Range
If you are interested in exploring these opportunities within the ABO, please complete the Volunteer Interest Form located on your Dashboard by logging into your ABO (roc-p) account. There will be openings to serve on the standard-setting panel and to serve as an ambassador. If you are interested in assisting as an examiner or as a future director for the ABO, please get in touch with your constituent Director.
ABO Director
According to The American Board of Orthodontics (ABO) Bylaws, each constituency is responsible for submitting a list of nominees to fill the ABO Director vacancy for their region when the current Director’s term ends. For example, the Middle Atlantic Society of Orthodontists (MASO) is currently selecting nominees to succeed Dr. Roberto Hernandez-Orsini upon completion of his presidential year.
ABO Board Certified
Credential Standardization
The ABO is pleased to introduce a standardized way for certified orthodontists to display their board certification status.
Recommended Order of Credentials
A standardized order of credential display ensures that patients, colleagues, and regulatory organizations can easily understand an orthodontic specialist’s qualifications. This order promotes clarity and consistency in professional identification and aligns with best practices in the health sciences fields.
Example: John Smith, DDS, MS, ABO-Board Certified
More info can be found on the ABO’s Across the Board blog page, as well as in the ABO Brand Standards and Marks Usage Guidelines.
In the dental profession, the recommended order of listing credentials is:
1. abbreviated dental degree(s) (e.g., DDS, DMD, or equivalent);
2. and any other earned and/or attained advanced academic degrees (e.g., MS, MSD, PhD, etc.);
3. board certification, as long as such use and indication are in accordance with any applicable Ethics Code (e.g., ABO-Board Certified)
4. fellowships and memberships
2025-2026 ABO Directors
All ABO Marks may not be used in any way that explicitly states or implicitly suggests that a board-certified orthodontist is superior in skill, ability, or quality of care when compared to a non-board-certified orthodontist. This is outlined in detail in the ABO Marks Usage Guidelines.
Marketing Update
ABO Marketing has developed and released a new Resource Guide and launched a new ABO Storefront. The Resource Guide was mailed to all active ABO-Board Certified Orthodontists in September. To access the new storefront, log in to your ABO account and click ABO Storefront.
The new ABO Storefront features are listed below:
Complimentary Downloads
ABO logo(s) and Seal(s), Sample Press Releases, Website Content, Social Media Graphics, It Takes a Specialist Video, Board Certification Process Pathway Graphic, ABO Brand Standards and Marks Usage Guidelines
Thank you for the opportunity to serve as your directors for The American Board.
Respectfully submitted by,
Dr. Onur Kadioglu kadioglu@americanboardortho.com
Dr. Timothy Tremont tremont@americanboardortho.com
AAO Political Action Committee Report
Dr. Ed C. Davis | Dr. Jeff Genecov
Advocacy is still going strong and the SSO is doing its part.
Although the SSO is leading the nation in AAOPAC donations, we continue to need your help. At the recent SSO Annual Session we initiated a campaign to increase the number of SSO donors. Dr. Steve Robirds, AAO Trustee and Dr. Ed Davis, AAOPAC Chair, managed an effort to increase the number of new SSO donors with the “100 for $100 campaign”. At the meeting, we reached over half the goal Elsewhere, the advocacy team has been working to inform Congress of problems associated with direct-to-consumer orthodontic treatment. During the MASO meeting, an AAO delegation met with FDA leadership and Congressional staff on Capitol Hill to discuss data from the MAUDE database and to present a petition from over 1,700 orthodontists who attested to concerns about treatment with Direct To Consumer plans. On the student loan front, the AAO is working with organized dental coalitions to push a reimagined REDI ACT, one that will allow students to defer interest
on medical or dental loans. On a state level, the Advocacy team has been tirelessly working to push state legislation, especially in many SSO components, that requires in-person exams and radiographs prior to the initiation of orthodontic treatment.
We are continuing to attempt to increase the number of SSO members who contribute to advocacy by serving as AAOPAC state captains and CALs (Component Advocacy Liaisons). The more members who are part of the National Advocacy Network, the more we “have a say” on what Washington’s policies and our individual state’s policies will be. Please consider becoming a member of the National Advocacy Network. Email Dr. Davis at ybender@bellsouth.net or Dr. Genecov at jgenecov@icloud.com or your state captain so you can be enrolled to join the fight.
Please consider joining us at the Advocacy Conference in Washington DC, March 17-18, 2026. For a minimum $250 donation to the AAOPAC you will receive an invitation to the conference. Your hotel and a $400 stipend to help defray travel costs will be funded. This is an exciting conference that always energizes members to become better advocates for our specialty. You will meet with orthodontists and residents from around the country and visit with members of Congress. You will learn about what is being done to protect our specialty from unnecessary regulations. As chairman of the AAOPAC, I would appreciate your support and attendance. See you there!
Presented by Dr. Edward Davis, on behalf of both contributors.
Learning, Laughter and Lone Star Memories
Our members are the heartbeat of this association. Each year, we honor those who have gone above and beyond—champions who strengthen our organization, advance our specialty, and support the next generation of orthodontists.
AWARDS
2025 Award Winners
As we celebrate the 2025 Award Winners, we invite you to nominate a colleague for the 2026 Awards. Please scan the QR code to access our website and complete the nominations before February 21, 2026
Orthodontic Legend Award
Dr. Rolf “Buzz”
Behrents
Dr. Behrents has had a distinguished career in orthodontics. He has served as Department Chair at The University of Tennessee, Texas A&M Baylor College of Dentistry and St. Louis University. His contributions to research and education have been recognized with multiple prestigious awards, including the Dewel Award (twice), the AAO’s Milo Hellman Research Award (twice), the Louise Ada Jarabak Memorial International Teaching and Research Award, and the Albert H. Ketcham Award.
Dr. Behrents served for twelve years as Editor in Chief, American Journal of Orthodontics and Dentofacial Orthopedics. He “retired” from this important position in May 2025. In addition to his academic and clinical achievements, he has held numerous volunteer leadership positions, made extensive editorial contributions, and delivered numerous presentations. He has had a remarkable career and has made an incredible impact on the specialty of orthodontics.
Sharon Hunt Emerging Leader
Award
Dr. Christian Johnson
Dr. Christian Johnson completed the SAO Leadership Program in 2019. This training served as a launching pad for her continued involvement in organized dentistry. Following the program, she spent two years as a director on the executive committee of the Georgia Association of Orthodontists before transitioning into her current role as the component director from Georgia to the SSO.
At the AAO level, Dr. Johnson served for two years on the Special Committee on Inclusion and Engagement and contributed to the
Practice Transition Project of the Council on Orthodontic Practice. Dedicated to fostering future leaders, she is a member of the SSO Leadership Development Program Committee.
Outside of orthodontics, Dr. Johnson is the president of a local dental study club, volunteers with the Junior League of Atlanta, and has participated in several pediatric dental mission trips to Guatemala.
Dr. Enrique Cruz
Born in Oaxaca, Mexico, Dr. Cruz received his DDS degree the from Universidad Nacional Autonoma de Mexico where he also was trained in oral surgery. He eventually moved to the United States where he completed a six-year dual residency in orthodontics and periodontics at Indiana University School of Dentistry. While at Indiana, he met and married Dr. Mahya Farnia who was also doing a residency in orthodontics. Their children are Enrique, Rosha, and Neela.
He is the CEO and Co-Founder of Sonrisas Orthodontics & Periodontics and Co-Founder of the Sonrisas Training Center where he and his team focus on building not just beautiful smiles but stronger teams, leaders, and communities. If you haven’t had a chance to watch his reels with Mahya and their staff, you have truly missed out! In fact, Dr. Cruz
has built a powerful social media presence with over two million followers who use his platform to educate, empower, and inspire a new generation of dental professionals! To Enrique, today’s dentistry is more than just treatment plans it’s about relationships, culture, and impact.
Beyond his practice, Dr. Cruz is a Past President of the Texas Association of Orthodontists and is currently a Trustee-at-Large for the American Association of Orthodontists. He also teaches part-time at the University of Texas Health Science Center in San Antonio.
He often says that patients may come for the treatment, but they stay because of how you make them feel. That same philosophy drives his leadership, his teaching and the work he does every day at Sonrisas and beyond.
Oren Oliver Distinguished Service Award
Dr. Tim Trulove
Dr. Trulove’s journey began at the University of Alabama where he earned his undergraduate degree before moving on to the University of Alabama School of Dentistry. Demonstrating both dedication and academic excellence, he continued his education by completing a master’s degree in orthodontics at the University of Iowa.
Throughout his career, Dr. Trulove has been shaped by the wisdom and guidance of renowned mentors including Dr. John Casko, Dr. David Sarver, Dr. Jim Vaden, and his first orthodontic partner, Dr. Grady Price. Their influence has instilled in him a profound commitment to service within the orthodontic specialty.
Dr. Trulove’s passion for elevating the specialty is reflected not only in his distinguished private practice, established in Montgomery, Alabama
in 1989, but also in the many leadership roles he has undertaken. The pinnacle of his service is marked by his selection as Director of The American Board of Orthodontics, where he represented the Southern Association of Orthodontists with integrity and vision.
His academic achievements include induction into the Alpha Lambda Delta Honor Society and Omicron Kappa Upsilon Honor Society, as well as being Certified by The American Board of Orthodontics—a testament to his commitment to lifelong learning and excellence.
Dr. Trulove’s career is a shining example of leadership, mentorship, and service. His legacy is not only defined by his achievements but also by the countless lives he has touched—patients, students, and colleagues alike. His unwavering dedication, exemplary service, and inspiring leadership set the standard for all of us.
Claude R. Stephens Jr, DDS, MS, is a native of Bonham, Texas. He is the son of a career Army medic and travelled the world with his family as an “Army Brat”. Married to his childhood sweetheart at the ripe old age of 20, he and his wife Valerie will soon celebrate 47 years together.
Dr. Stephens, affectionately known as “Rick” by his friends, graduated from Austin College in 1977. Because Austin College is a liberal arts college, his degree is an unusual Bachelor of
Dr. Claude Rick Stephens Martin Dewey Memorial Award
Arts in Biology instead of the more common Bachelor of Science. He likes to tell people he is a biological artist with a specialty in dentistry. He is a graduate of The Baylor College of Dentistry. After graduation he joined the Navy and was assigned to Recruit Training Command, Orlando, Florida. Following three years in the Navy, he attended orthodontic residency training at The Ohio State University. During that time, he continued his military career as a Naval Reserve officer. He moved back to Texas upon graduation and started a private practice in orthodontics.
He continued his reserve military affiliation for a total of 32 years at which time he retired with the rank of Captain, US Navy. In 1989 he was awarded the Navy Dental Corps’ highest recognition, The Admiral Vaughn Award, and received the Navy Commendation Medal. In 1991, while serving as Battalion Dental Officer with Reserve Naval Mobile Construction Battalion 22, his battalion was mobilized to serve in Operation Desert Storm. Because it was such a short conflict, he jokingly says they ran out of war before he got past Fort Worth, Texas on his way to Iraq.
Dr. Stephens has been committed to organized dentistry throughout his 40 years in dentistry. He is a member of the American Dental Association and the American Association of Orthodontists. He has served as President of the Texas Dental Association’s 6th District on three different occasions and has been a delegate to the Texas Dental Association for the past five years. He served as Editor of the Southwest Society of Orthodontists Newsletter which led to his serving as Editor of the ICD District 15 Newsletter. He continues to serve the specialty as an Associate Clinical Professor in Orthodontics at the University of Texas Dental Branch, Houston and Texas A&M University Health Science Center, Dallas.
As a member of the First Baptist Church of Lancaster, Texas he has developed an affiliation with Orphan Outreach. Each non-covid year since 1996 he has travelled to Liepaja, Latvia to minister to children at the Christian Day Center supported by Orphan Outreach. He says he is easing into retirement and has recently sold the bigger of his two practices and looks forward to working just two days a week.
Texas-Sized Smiles in San Antonio
Leadership Development Program
We are excited to introduce you to the 2026 Leadership Development Class! The purpose of this program is to provide members with tools and resources to enhance their leadership skills.
Updates from our State Associations
Component Meeting Dates
We encourage all members to attend your state meeting! These gatherings offer an excellent opportunity to network with fellow Southern Society of Orthodontists members, engage in discussions about issues facing local orthodontists, and take advantage of valuable continuing education sessions. Save the date for your 2026 State meeting:
Alabama
Arkansas
Florida
Georgia
Kansas
Kentucky
Louisiana
Mississippi
North Carolina
Oklahoma
South Carolina
Tennessee
Texas
Virginia
West Virginia
February 6, 2026
To Be Announced
March 5-7, 2026
February 20 - 21, 2026
To be announced
August 21, 2026
April 18, 2026
February 7, 2026
January 30-31, 2026
March 6, 2026
March 6, 2026
February 13, 2026
February 27, 2026
February 27 - 28, 2026
July 18, 2026
Southern Society of Orthodontists Director & Delegates Update
The Southern Society of Orthodontists is excited to introduce the following new Directors and Delegates:
Component Directors
Dr. Celeste Block - Louisiana
Dr. Kelly Goeckner - North Carolina
Dr. Jay Joshi - Kansas
Dr. Danielle Robb - Virginia
Dr. Trecy Watson - South Carolina
We extend our heartfelt gratitude to the outgoing Directors and Delegates for their dedicated service. The SSO deeply appreciates the invaluable contributions of all our volunteers!
SAO Delegates
Dr. William Bates - Alabama
Dr. Angie McNeight | Alternate - Florida
Dr. Tyler Rathburn - Georgia
Dr. Eser Tufekci - Virginia
Outgoing Component Directors
Dr. JK Dillehay - Kansas
Dr. Brian Hamby - South Carolina
Dr. George Sabol - Virgina
Dr. Rob Selden - North Carolina
Dr. Corbin Turpin - Louisiana
SWSO Delegates
Dr. Chris Cramer | Alternate - Texas
Dr. Christine Ellis | Alternate - Texas
Outgoing SAO Delegates:
Dr. Eric Nease - South Carolina
Dr. Chopper Snyder - Virginia
Arkansas Association of Orthodontists Annual Meeting
Kansas Association of Orthodontists Annual Meeting
Kentucky Association of Orthodontists Annual Meeting
2026 Leadership Class
Tennessee
Pardeep Kaur Virginia
Leadership Development Program Committee
PART 8 IN A SERIES
Parliamentary Pearls
Dr. Jeff L. Rickabaugh
Incidental Motions: Part II
This column in the previous SSO NEWS introduced Incidental Motions and 2 of the 9 motions in that category were discussed. Those were Point of Order and the Motion to Suspend the Rules.
As mentioned previously, Incidental Motions do not relate directly to the Main motion, but relate instead to matters arising from the conduct of the meeting. Incidental motions may interrupt business and may, if necessary, interrupt the Speaker. These Incidental motions are to be disposed of prior to the business from which they arose.
MOTION TO APPEAL
This motion allows at least two members who disagree with the presiding officer’s ruling to challenge that ruling and have the assembly decide, by vote, whether the presiding officer’s ruling is to be sustained (agreed upon or upheld) or to be reversed. If the ruling of the chair or presiding officer is sustained, this ruling becomes the decision of the assembly. Likewise, if the ruling is not sustained, the decision is reversed. This reversal overturns the ruling and becomes the decision of the assembly.
Any decision of a presiding officer that involves judgement is subject to appeal. However, statements of fact that provide information or rulings on unambiguous provisions of bylaws are not subject to appeal. An appeal is permissible immediately after the presiding officer’s ruling has been stated. It is too late to appeal if any other business has intervened.
When a member wishes to challenge/appeal the ruling of the presiding officer, they must quickly arise and state “I appeal the ruling of the chair (or Speaker or Presiding Officer) “to which there must be a second. The presiding officer then announces “the ruling of the chair has been appealed and seconded”. At which point the presiding officer states his/her reasons for the ruling and calls on the member appealing the
decision. Subsequently, the member states the reason(s) for the appeal. Following this, a vote is taken. The vote requires a simple majority of the assembly to vote yes and sustain or uphold the presiding officer’s ruling; while a no vote overturns the ruling. This appeal is only for the presiding officer’s ruling and is not germane whatsoever to the business of the main motion on the floor.
Rules for an Appeal:
• Can interrupt the Presiding Officer to confirm the lawfulness of the ruling before a vote or next order of business
• Requires a second
• Cannot be amended
• Debatable only on the ruling, not on the motion
• Requires a majority vote or uphold or overturn the Presiding Officer’s ruling
• An appeal is not recorded in the minutes.
INQUIRIES; PARLIAMENTARY OR FACTUAL
An Inquiry allows a member to ask the presiding officer a question that relates to procedure in connection with the pending motion (Parliamentary Inquiry); or to request substantive information or facts about the pending motion or the meaning or effect of the pending question (Factual Inquiry).
Any member has the right to inquire at any time during the processing of a motion provided a vote has not begun on the motion. The inquiry does not need a second, it is simply a request to obtain clarity in order for the members to make an informed decision. The presiding officer assists in obtaining the information requested whether related to procedural matters or specific facts of the pending motion. At the AAO House of Delegates, the Speaker can ask the professional Parliamentarian for assistance with a complex procedural issue or request factual information from a Council Chair, AAO Trustee, an AAO staff member or the maker of the motion on the floor.
An Inquiry is not debatable, requires no second since it is a request, and there is no vote. No entry of inquires are necessary for the minutes.
Rules for an Inquiry
• Can interrupt the Presiding Officer or Speaker if it requires an immediate answer
• Requires no second, it is simply a request
• Not debatable nor amendable
• Requires no vote
• Inquiry can be withdrawn
• Can be recorded in minutes if the inquires add clarity
REQUEST TO WITHDRAW A MOTION
A request to withdraw a motion allows the member who has proposed a motion to remove it or request it be removed from consideration by the assembly. If the request to withdraw is granted, the motion is withdrawn from further consideration.
Typically, when a motion has been moved, it has been restated to the assembly by the presiding officer. The motion now becomes the property of the assembly or House. However, if the proposer requests the motion be withdrawn before the presiding officer restates the motion, the presiding officer can simply state “the motion has been withdrawn”. Otherwise, the presiding officer has to request the assembly to allow the motion to be withdrawn. The presiding officer states “the maker of the motion asks permission to withdraw the motion”. A vote by general consent or a majority vote is necessary from the assembly to withdraw the motion.
Rules to Withdraw a Motion:
• Can interrupt the Presiding Officer or Speaker
• Requires no second, it is a request
• Motion to withdraw is not debatable nor amendable
• Must be decided immediately
• Motion to withdraw is granted by the Presiding Officer before motion becomes property of the Assembly
• After motion is restated by Presiding Officer or Speaker, it becomes the property of the Assembly and a majority vote is required to allow the motion to be withdrawn
• Motions withdrawn before the presiding officer restates the motion are not included in the minutes whereas a motion that has been restated is to be included in the minutes. A statement that the motion was withdrawn should accompany this entry.
Dr. Jeff L. Rickabaugh
References:
American Institute of Parliamentarians
Standard Code of Parliamentary Procedure 2nd Edition, 2023
Cannon’s Rules of Order, 1992
How Would YOU Treat This Patient?
A healthy 6 ½ year girl was referred to me by my orthodontic assistant, a friend of this little girl’s mom. The mother reported no family history of Class III growth, not grandparents, aunts or uncles, or siblings, on either her side or the father’s side. This was perplexing, as it was this patient’s most obvious problem. Orthodontic records were obtained for a thorough understanding of the dental and skeletal characteristics, consideration of potential treatment solutions, and the timing of such treatment.
Dr. Timothy Shaughnessy
The panoramic radiograph (Figure 3) confirms a favorable difference in size between the primary second molars and permanent second premolars. Although a cursory evaluation of maxillary arch length does not appear to be as good as the available space in the mandible, expansion of the maxilla will obviously be required and generate more space.
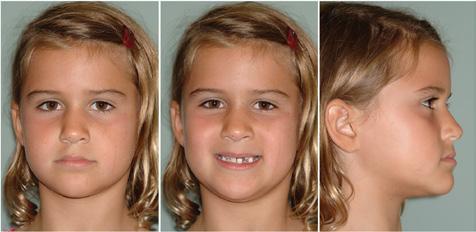
The INITIAL facial photographs (Figure 1) reveal a mild Class III profile with a hint of mandibular prognathism. The maxilla appears normal. Upon smiling, the mandibular incisors are displayed and hide the maxillary incisors because of the negative overjet and dental deep bite. The midlines are coincident and ‘on’ with the face.
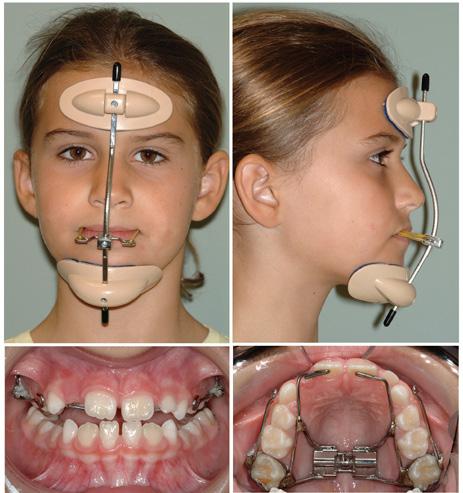
The INITIAL intraoral photographs (Figure 2) show a transverse discrepancy between the maxillary and mandibular posterior teeth. The anteroposterior molar relationship is super Class I. The canine relationship is solid Class I, with space mesial to the mandibular primary canines. Clinical manipulation of the mandible to centric relation placed the primary canines in initial contact, followed by an anterior and vertical functional shift to maximum intercuspation. The overjet between the incisors was negative however, in both centric relation and centric occlusion. Arch length appears adequate in both the maxilla and mandible.
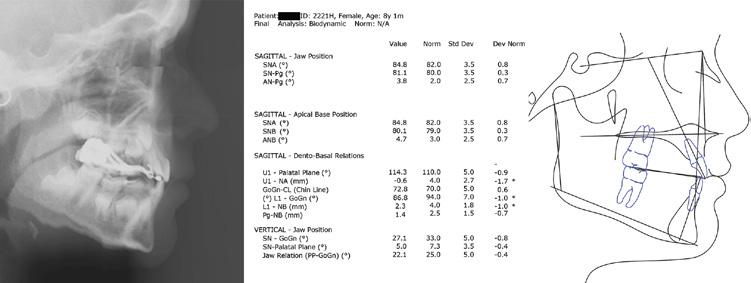
The cephalometric radiograph and analysis (Figure 4a and Figure 4b) confirm a mild Class III skeletal relationship (ANB 1). The erupting maxillary incisors are retroclined and the mandibular incisors are proclined, contributing to the negative overjet.
How would YOU treat this patient?
Treatment Planning
Evaluation of the INITIAL records make it clear that this is not a Class III skeleton with dentoalveolar compensation. This makes the prognosis better because normalization of incisor position helps, rather than hurts. Maxillary orthopedic expansion is required as part of any treatment plan. When should interceptive treatment be initiated? Which of the following options would YOU choose, if any?
Figure 1
Figure 3
Figure 4a and 4b
Figure 2
Option 1:
Maxillary 3-way sagittal appliance designed to both widen the transverse dimension and lengthen the anteroposterior dimension. More specifically, advancement of the anterior teeth is preferable to distalization of the molars. This removable appliance therapy depends on cooperation wearing the appliance and compliance with turning of the central jack screw.
Option 2:
Any number of appliances in the category which includes the Carriere Motion Appliance for Class III correction, utilizing the maxillary arch for anchorage, along with Class III elastics to the device connecting the mandibular molar and canine. With this option, the expansion of the maxilla is typically deferred until after anteroposterior correction. The mandibular primary canines are suitable for use in this young patient.
Option 3:
Plan to expand the maxilla with a fixed appliance, designed in a way to advance the permanent incisors, when combined with a reverse pull facemask.
Option 4:
No treatment now, as this patient will A) likely require surgical correction when growth has ceased, or B) treatment now will make no difference in the eventual outcome.
The Treatment Plan Chosen
Option 4 was not selected for a variety of reasons. The cephalometric analysis revealed a significant dental component to the negative overjet relationship and a mild skeletal Class III. Had there been a larger skeletal Class III discrepancy reflected in the posterior occlusion, combined with Class III dental compensation, the prognosis for conservative correction would be worse. In addition, the absence of a family history of Class III growth improved the prognosis. Establishing positive overjet now if possible, and removing any functional shift component, could eliminate a factor which might contribute to a worsening of the Class III relationship.
Options 1 and 2 target the dentition exclusively, however, there is a Class III skeletal component that cannot be attributed entirely to a functional shift. Option 1 is heavily dependent on patient cooperation and my preference is to expand with a fixed appliance whenever possible. Some unwanted maxillary molar distalization could also occur, a reciprocal side effect of advancing the anterior teeth. Option 2 distinctly separates transverse correction from the anteroposterior, arguably decreasing efficiency and potentially increasing treatment time.
Option 3 was selected because it targeted both the dental and skeletal components of this patient’s Class III discrepancy. Correction of the transverse and anteroposterior planes of space occur together like Option 1. Cooperation is required with this option also. However, at least some of the appliance therapy is fixed. In retrospect, it would have been possible to combine Option 3 with an Option 2 style appliance.
Initiation of treatment was judiciously delayed for several months (age 7), until both of the maxillary central incisors erupted sufficiently for fixed appliance fabrication. Expansion of the maxilla began immediately by turning the device 1/4 turn every other day. Initial expansion of 5mm was accomplished in 6 weeks. The expander was tied off with a steel ligature to prevent any change but permit further expansion as needed. A reverse pull facemask was delivered at this time. 1/2”, 14 oz. elastics were provided for traction between the hooks of the appliance and the facemask. These initial elastics generated approximately 350 grams of force. The patient was instructed to wear the facemask all the time except at school. PROGRESS photographs (Figure 5) were obtained one month later, and the elastic strength was increased to 5/16”, 14 oz., generating approximately 600 grams of force.
PROGRESS photographs (Figure 6) were again obtained six weeks later. They showed the development of a positive overjet. Over the next six months, wear time was gradually reduced to sleeping hours only. It was necessary to cut the expander arm to permit eruption of the maxillary right lateral incisor during this time.
Figure 5 - Appliance design courtesy of SSO Member Dr. Stuart Loos
Figure 6
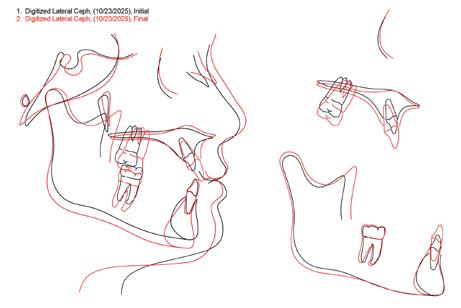
Photographs (Figure 7) were obtained at the age of 8 after one year of treatment. A lateral cephalogram, its tracing and the cephalometric values (Figure 8a and Figure 8b) were also obtained at the same time. The pre-treatment/posttreatment superimposition (Figure 9) reveals that correction occurred both dentally and skeletally. The maxilla and maxillary dentition moved slightly forward. The additional extrusion of the maxillary molar resulted in bite opening and downward and backward jaw rotation. Fortunately, this is something this patient could tolerate. Bottom line, it is better to open the bite in a patient who is Class III and deep than Class III and open.
Photographs (Figure 10) obtained at age 10, two years later, show that the overjet correction remained stable. I completed comprehensive orthodontic treatment on this patient’s older sister four years later. So, at age 14, I know with certainty that the patient described in this case report remained stable through adolescence. The family never chose to do any additional orthodontic treatment.
YOU may have treated this patient differently, or chosen not to provide interceptive treatment. There will always be acceptable differences of opinion regarding treatment, based on experience, personal preferences, and bias, among other reasons. This is the ART of orthodontics. We may not always agree. The SCIENCE of orthodontics is the diagnosis, and here there should be general agreement. The purpose of this case report is to illustrate one way to treat this patient and provide the rationale for such treatment.