
AcousticsinNeonatalCare:
DesigningaQuieterAcousticalEnvironment
By JasmineVargas
ChristopherNoroña
JesusJacquezSicaeros
RC4870HealthcarePlanningDesign
ProfessorHenryDeJesus
FinalPaper
Date:12/8/25
TableofContents
Introduction
Background/Overview
- AcousticsinaHospital
Importance
TypicalStrategies
- Materials
- WallAssemblies
CaseStudies
- LucilePackardChildren’sHospital
HMCWallStrategies
- NICUBuiltProject
HealthcareWorkerInterview
- JenaEidschunInterview
DesignMethods
- SandySmithandJunGangInterview
Conclusion
Introduction:
ThesisStatement:
TherearemanydifferentwaystodampenacousticalsoundsinNICUstopromote comfortfornewborns.InNeonatalIntensiveCareUnits(NICUs),soundplaysamajorrolein howinfantsgrowandhealintheirearlystagesoflife.Becausetheseroomsarehighlysensitive spaces,thedesignofeventhesmallestobjectcanchangeconstructionchoicesofwhatmaterials areneeded,andcreateamajorimpact.Somecommonsoundsthatarecreatedinclude mechanicalsystems,corridors,orstaffmovement,whichmayseemminorbutcancausefatigue, sleepdisruption,andstressinanewborn,potentiallyslowingtheirrecovery.Understandingallof theseissues,theacousticaldesignbecomesanessentialpartofcreatingasupportive environment.Thisstudyexploreshowwallassemblies,materials,construction,anddesign strategiescanallhelpreducenoiselevelsandcreateapeacefulspacethatsupportscomfortfor patients,visitors,andstaff.
Background/Overview
AcousticsinHospitals:
Inordertounderstandwhatstandardsareneededforanewborn'shealthrecovery, hospitalsrelyonstrictacousticalstandardsthatlimithowsoundtravelsbetweenspaces.Inmost facilities,acousticdesignfocusesoncontrollingairborneandstructuralnoisethatpasses betweenpatientrooms,corridors,andserviceareas.Forthisreason,inthe California Building Code (CBC),partitionsthatseparatepatientroomsmustachieveaminimumSound TransmissionClass(STC)of50,andceilingsinNICUsarerequiredtohaveaNoiseReduction Coefficient(NRC)ofatleast0.90toabsorbsoundefficiently.Theserequirementsreflecthow
importantbuildingcodesaretocomfortandrecoveryincreatingstandardsfordesigngoals.The rigorandimportanceplacedonthesestandardsshowhowintentionalandintegralacousticsare inhealthcaredesign.
Importance
ofAcoustics/ItsEffectsonPatients,Staff,&Visitors:


Evenwiththesestandards,hospitalsmanagehowtocontainnoisefluctuationsthataffect patienthealth.Forexample,newborns,havinghighorunpredictablesoundlevels,areanissue becausetheycancreateirregularheartrates,breathingchanges,anddropsinoxygensaturation. Duetotheunexpectedchanges,NICUDesignStandardsrecommendusingmaterialsandwall assembliesthathelpcreatecalm,privateenvironments.Meanwhile,inHealthcareDesign Magazine,theytalkabouthowhospitalssuchasGolisanoChildren’sHospitalandPhoenix Children’sHospitalusedouble-studpartitions,resilientflooring,andabsorptiveceilingpanelsto meetthesegoals.Theseareimportantforourstudybecausetheywillhelpusunderstandwhat challengestheyhadandwhatresultsareusefulforbeingabletoreducenoisepollution,andalso keepthepatientsfromfeelingvibrationsfromthesurroundings.
TypicalStrategies:
Materials:
Healthcarearchitecturerequiresveryspecificstandardstobemetforpatientcomfort,but evenmoresowheninfantsareinvolved.Infantsaresusceptibletoalotofenvironmentalfactors thatcanleadtopoorrecoveryrates.Becauseofthis,healthcaredesignersusematerialsthatare durable,hygienic,andacousticallybalancedforallpatients.Acrosshospitalsandclinics, designersselectvariousassembliesandmaterialsthatmeetvariousstandards,butmost importantly,theyachievethedesirednoisemanagementandmufflenoisevibrationlevelthat supportspatientrecoveryandalsohelpswithstaffperformance.Forexample,onematerialused iscleanableacousticwallpanelsthataretypicallyusedinpatientandstaffareas.Thesepanels typicallyfeatureafiberglassormineralfibercorewithawashablesurface.Theseachievea NoiseReductionCoefficient(NRC)ofabout0.75-1.0+.Thismeansthatthesepanelscan absorb75-100percentofsoundwavesinthespeechfrequencyrangeof250-2000Hz.
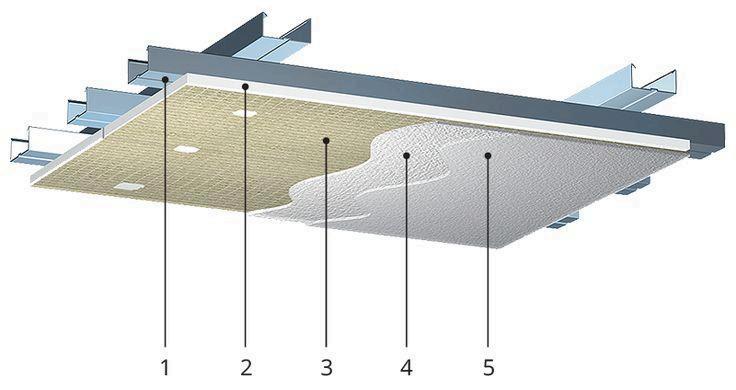
Inmoresound-sensitiveenvironmentslikeNICUs,monolithicplastersystemsareused. Theseplastersystemsprovideaseamless,joint-freesurfacethatreachesanNRCvalueof 0.55-0.85.TheNRCvaluedependsonthethicknessandbackingofthepanels.Theseplaster systemsaremainlyaimedatwallacousticcontrol.Ceilingshaveotherstandardsthattheymust meet.Ceilingsoftenincorporatehigh-NRCtileswithwashableandantimicrobialfinishesthat reachNRCValuesof0.80-0.90.
WallAssemblies:
Thesematerials,whenpairedwithwallabsorption,reducereverberationsandimprove speechclaritybetweencaregiversandfamily ForSoundIsolationbetweenpatientrooms,
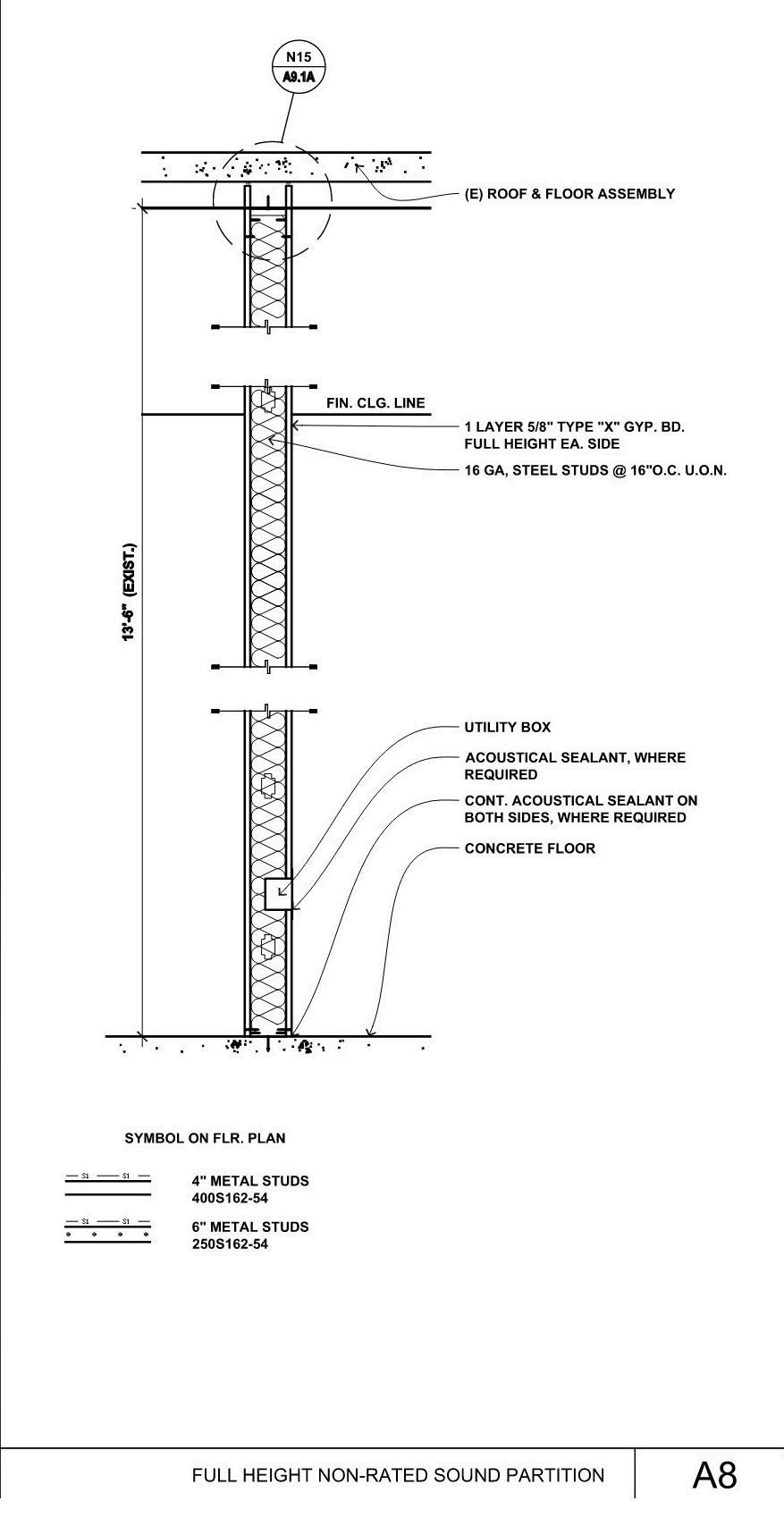
includingNICUs,wallassembliesaredesignedtoachieveSoundTransmissionClass(STC) ratingsof50-60decibels(dB).Thesesoundratingsaretypicallyachievedthroughdoublestud orstaggeredstudframing,alongwithmultiplelayersofTypeXGypsumBoardandhigh-density mineralwoolinsulation.AccordingtotheNRCResearchCenter,theyfoundthatthese assembliescanblockover50decibelsofairbornenoisewhentheyareproperlysealed.While wallfinishesareimportantforabuseandmoistureresistance,theycontributeverylittletothe overallsoundabsorptionofawallassembly.Wallfinishessuchasgypsumbordersfinishedwith epoxyorhigh-performancepaintprovideabout0.05-0.10NRC.
CaseStudy:

OnestrongexampleofhowhospitalshandleacousticsisLucilePackardChildren’s Hospital,wherethedesignteamusedPyrokStarSilenttomeetbothperformanceandhygiene goalsintheNICU.StarSilentisaseamlessacousticplastersystemmadefromrecycledglass beadsthatattachesdirectlytotheframing,lettingthecavitybehinditaddtotheabsorption, especiallyinthelowerfrequencyranges.Thepanelscomeinthicknessesof3/8",5/8",and1",
withNRCratingsrangingfromabout0.55upto0.85dependingontheassembly Thissystem providedthehospitalwithreliablesoundcontrolwhilealsocreatingacontinuous,cleanable surfacethatsupportsinfectioncontrolandstilldeliversamodern,smoothlook.
WhiletypicalNICUwallassembliesfollowpredictableacousticstrategies,their constructioncanvarysignificantlyoncetheseprinciplesareappliedtoanactualproject.
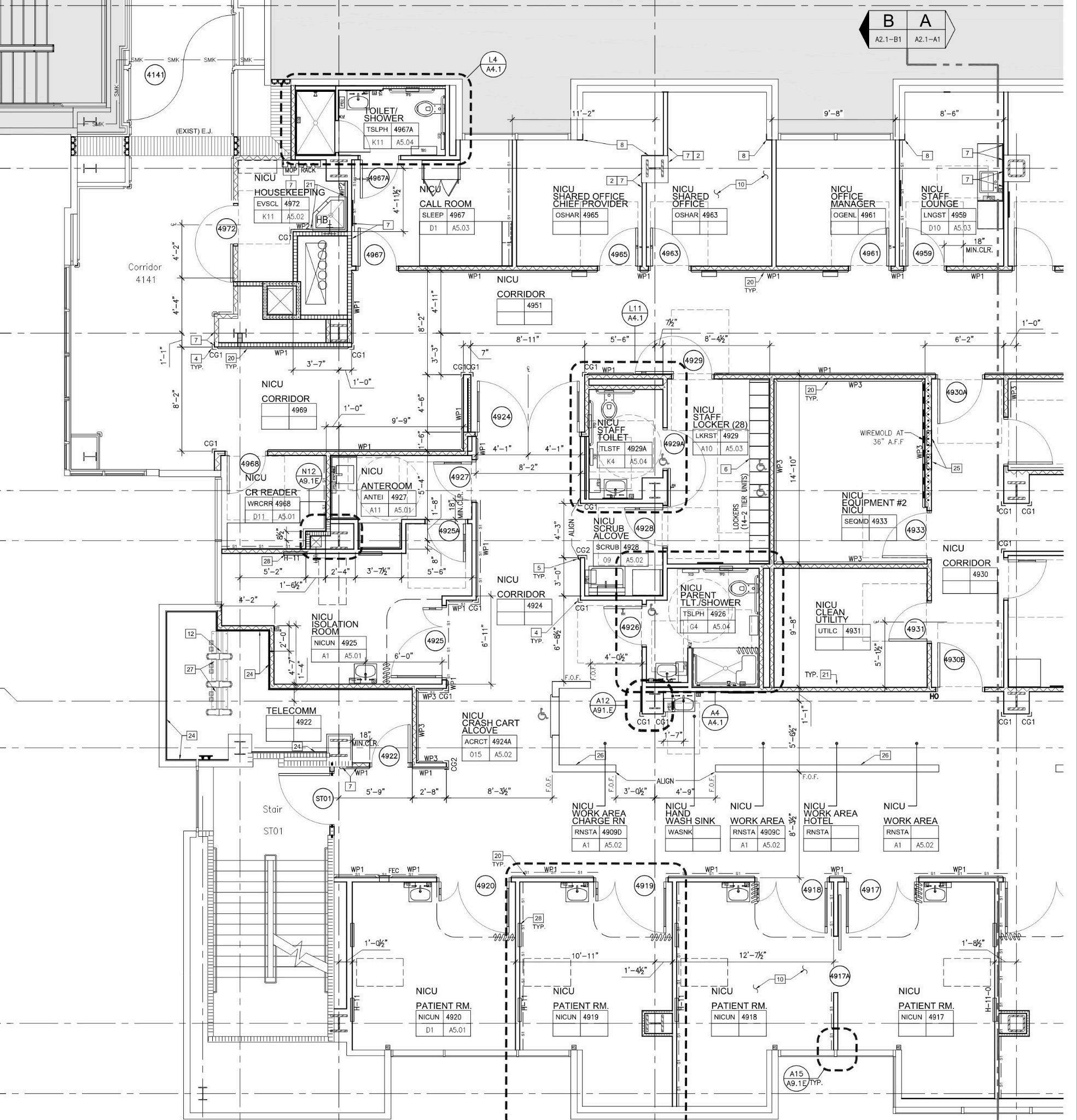
Tobetterunderstandhowtheseapproachesareadaptedinpractice,ourgroupconsultedthe HealthcareStudioprofessor,JimmyMacias,whoisalsoadesigneratHMCArchitects.He providedwalldetailsandfloorplansfromaNICUrenovationhisfirmcompleted.Thedrawings includepatientroomsaswellasadjacentstaffspacessuchaslounges,restrooms,andoffices, offeringaclearviewofhowacousticsareaddressedacrossdifferentprogrammaticconditions. Whatbecomesimmediatelyapparentinthesedocumentsisthatthewallassembliesarenot uniformthroughout;instead,theyarestrategicallyvariedtosupportspecificacousticneeds.This levelofprecisionreflectsthecarefulattentionrequiredtoprotectthesoundenvironmentina NICU.Beyondtheassembliesthemselves,theplanlayoutalsoreinforcesacousticgoalsby separatinglouderstaffareasfromsensitivepatientzones.Together,theseplansanddetails illustratehowacousticperformanceisachievedthroughacombinationofthoughtful constructionandprogrammaticorganizationinhealthcaredesign.
Nurse/HealthcareWorkerInterview:
WeconductedaninterviewwithJenaEidschun,aProgramManagerIIatStanfordHealth Care,andwereabletodiscusshowmuchnoiseaffectsdailycareintheseunits.Mrs.Eidschun describedworkingintheNICUasbothdemandingandrewardingbecauseoftheconstantneed tosupportfragilenewborns,neonates,andtheirfamilies.Sheexplainedthatnoiseisamajorpart ofthejobsincealarms,equipment,andcommunicationcreatealoudenvironmentthatishardto control.Mrs.Eidschunsaidthatnoisecanimpactinfantsbyaffectingtheir“physiological stability,comfort,andsleep,”whichshowshowimportantitistomanagesoundlevelsinsidethe unit.Evenwithstaffbeingcareful,theamountofactivitymakesitdifficulttocreateacalm spaceforeachinfant.
Mrs.Eidschunalsotalkedabouthowlayoutsshapetheacousticalenvironment.Theysaid that“modernsingle-familyrooms”workbetterthanolderopenbayunitsbecausetheyreduce soundexposureandgivefamiliesmoreprivacy Openbayswouldallowforallthesoundsof conversationsandequipmentnoisestotravelacrosstheroom.Mrs.Eidschunalsosharedthatthe olderNICUwheretheyworkedhadanopenbaylayoutandfelt“lessinviting,”whilethenewer hospitalhadsingle-familyroomsthatcreatedaquieterandmorecomfortableenvironmentfor thestaffandthefamilies.Apartfromtherebeingsingle-familyrooms,shealsosaidthathospitals oftenhave“dedicatedquietrooms”sofamiliesandstaffcantalkprivatelywithoutdisturbing infants.
DesignchoicesalsoplayabigroleinhowquiettheNICUfeels.Mrs.Eidschunexplained thatthenewerhospitalusedbettermaterialsandnewerconstructionmethodsthathelpedlower noiselevels.Theysaidthatthenewunithad“quieterenvironmentsandfamilyareas”becauseof improvedwallsystemsandacousticfinishes.Theyexplainedthatdurable,cleanablesurfacesare requiredduetoallthedifferenttypesofsituationsthatcouldhappen,butthecombinationof thickerwalls,acousticceilings,andmovingloudequipmentawayfromthebedsidehelpedmake thespacecalmerforinfants.
Apartfrommateriality,Mrs.Eidschunalsosharedsomeofthestrategiestheyhaveseen usedtomanagenoise.Theseincluded“staffandparenteducation,”whichmeanstoestablish scheduled“quiettimes,”anddoingroundsawayfrompatientbedsand“silencingalarmsif possible”.Also,repositioningequipmentorinstallingquietdoorshashelpedreduceoverallnoise levels,whichhavebeenusefulassetstomodernNICUs.Furthermore,fromtheirpointofview, toomuchsound“negativelyimpactsthehealthofaneonate,”sobothdesignstrategiesanddaily routinesneedtoworktogethertosupportinfanthealingandreducestressforfamiliesandstaff.
DesignMethods:
InthepursuitofproperacousticsinNeonatalunits,therearemanyfactorsthatmustbe takenintoaccount.Mostfundamentalistheunitlayout.ThefirstNICUintheUS,establishedby Yale'sDr.LouisGluck,setaprecedentforanopenbaylayout,wheremultipleinfantswouldbe groupedintoalargeopenplannurseryandstaffworkcouldbecentralized, increasingthe efficiencyofthecare.Atthispointinmedicalhistory,thebenefitsofthisconfigurationfar outweighedanycons,butasmedicinegrewmoreadvanced,thislayout'sflawsbecamemore pronounced.
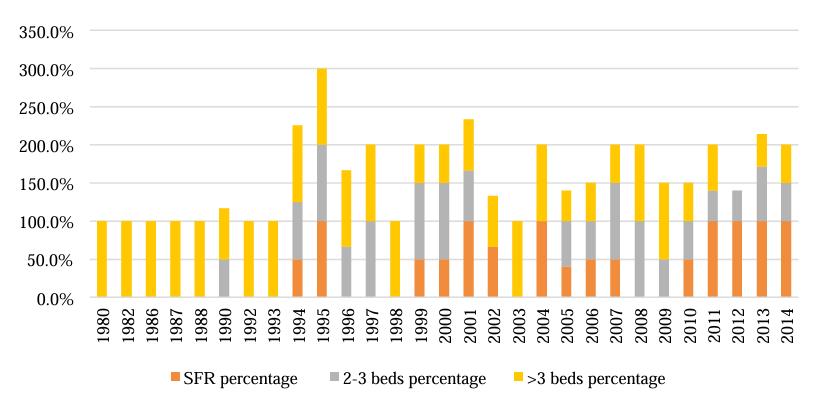
AstudyconductedbytheAIAAcademicArchitectureforHealthtrackedthe implementationofdifferentNICUlayoutsinhospitalsfrom1980to2014.Before1993, open-baystylenurserieswerethenorm,butsmalleroccupancyroomsbegantoincreasein popularitysoonafter Theimplementationofunitswith2-3bedsperroomandsingle-family roomswithonlyoneoccupantbecamemoredesirableformanyreasons.Inmodern-dayNICUs, moreindividualizedcareispreferable;thus,thesesmallerenvironmentsallowformore
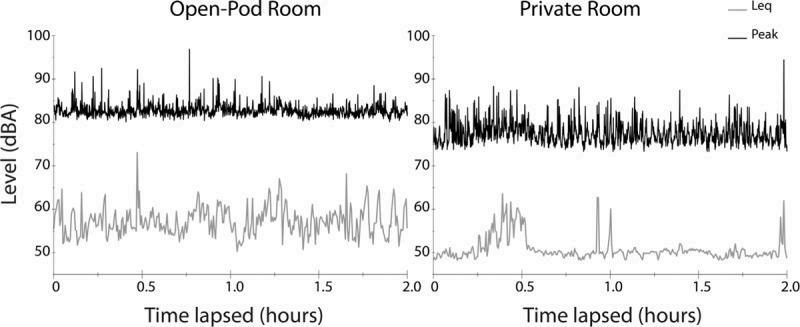
personalizedattention.WhilenottheprimarypurposeoftheSFRs,thisunittypedoeshavesome benefittotheacousticalexperienceinNICUs,allowingformoreseparationofnoisyday-to-day staffoperations,patientbedareas,andvisitorspaces.WashingtonUniversitySchoolofMedicine conductedastudyontheacousticsofanopen-podroom(whichhouses5baysforpatientbeds) versusaprivateroom.Thestudyfoundthatvolumepeakswerebothmorefrequentandhigher onaverageintheopen-podroom.However,theoverallnoiseaveragesinbothlayoutsstill exceededtherecommendedlevels,sowhilethisapproachdoeshelpinimprovingtheacoustical environment,otherinterventionsarestillneeded.
ManystudieshavebeenconductedtorecordnoiselevelsinNICUs,oneofwhichwas donebyJohnsHopkinsBayviewMedicalCenter.Afterfindingthattheydidnotmeetthe requiredstandards,theytrackedwhatexactlytheproblemareaswereinanefforttoachievemore appropriatenoiselevels.Muchofthisexcessivenoisecamefromstaffrounds,conversations, phonecalls,andnoisyequipment.IntermsoftheNICUdesign,theyfeltthattherewerenot enoughbuffersintheroomtohelpdecreasesoundtransmissionandechoes,andtooclose
proximitybetweenbedsandstaffworkstations.ThisparticularNICUhasanopenbaylayout, andnursesoftencitethisdesignaspectofthefacilityasanobstacletoreducingnoiselevelsthat theyhavelittleabilitytoremedy
InsituationsofpreexistingNICUs,manycan’tchangethelayoutoftheunits,likein JohnsHopkins'case.However,loweringnoiselevelsisstillachievable;manyotherstrategies haveproveneffectiveinthisendeavorandshouldbeusedinconjunctionwitheachother.After firstassessingwhattheproblemareasareinanyparticularNICU,theimplementationofbarriers toisolatenoisesourcesisaneasystart.Manynon-criticalalarmsandmonitoringsystemscanbe switchedtovisualmodelsratherthanthetypicalauditorytypes.Thisimplementationalsohelps preventalarmfatigueinthenursingstaff.Someofthemostsuccessfuldecreasesinnoiselevels comefromthemorehumanaspect,alertingstaffwhenthenoisebeginstocreepintotheharmful range.
Inadditiontotheseinterventions,afewmorethatcameupoftenwhileresearchingwere theuseof“quietzones”orspecifiedroomsandspacesawayfromthepatientareasthatallowfor conversationsbetweenvisitorsandstaff,aswellasamongthemselves.Propersignageisalsoan importantimplementationinmostoftheseinstances,denotingwherepeopleshouldbemore mindfulandwhereitisappropriatetotalkatnormallevels.Thisisinadditiontoeducatingstaff andvisitors,whetherthroughsigns,pamphlets,ornotices,aboutthedangersofelevatednoise levelsinNICUsandtobemoremindfuloftheirvolume.Theimplementationofmorethanone ofthesestrategieshelpsimprovetheiroveralleffectivenessinreducingnoiselevelsbybuilding offeachother’simpacts.
Manyofthesefindingsandconclusionswereechoedinaninterviewconductedwith Sanford“Sandy”SmithandJunGang,aretireddesigneratHoagMemorialHospitalanda
designerfromHenselPhelps,respectively Whilecitingapaperonthetopic,Sandyreiterated that“single-familyroomsinNICUs,whileshowingsomeimprovementsinoutcomesfor prematureinfants,havenotachievedasignificantreductioninnoiselevels”andstatedthat “muchofthechallengerelatesdirectlytotheaudiblealarmsthataresopervasiveinthe healthcareenvironment”.Shebroughtupadditionalinterventions,suchassound-absorbing materialsbeingusedonwallsandceilings.Junbroughtupthatthecleanabilityofthematerial wasalsocrucialtoconsider,pointingtowardstheCaliforniaBuildingCode,Title24,Chapter12, Table1224.4.11“AcceptableCeilingandCarpetLocations”.Junalsoaddedthatinadditionto theequipment,staffnoisewasanotherpervasiveacousticissue;inhisexperience,“theytendto beabitloudattimes”.Overall,theconsensusseemedtobethatamultitudeofapproacheswere necessary.Junbelievedthatinadditiontothedesignoflayouts,openvsclosedconcept,there needstobeamindfulstrategyinroomplacementandspatialadjacenciesto“minimisenoisenot onlyfromotherpatients,butfromstaffaswell”.
Otheraspectsofdesignthatwerebroughtupinthisdiscussionincludedisolatingnoise sourcesandincludingmorevisualalarmmonitoringsystems,whichwereapproachesthatJohns Hopkinsimplementedtogreateffect.Alongwithafinalsuggestiontoimplementcolor-coded visualalarmsystemsforlegibility.Whilesomeoftheseinterventionsinisolationonlyoffera littleimpactontheacousticenvironment,Junbelievesthat“anythingtohelpthestaffand familiescanbebeneficial”.
Conclusions:
Tosummarizeourfindings,designingforacousticsinNeonatalIntensiveCareUnits (NICUs)isultimatelyaboutprotectingthephysiologicalandemotionalwell-beingofthemost vulnerablepatients.Acrossbuildingcodes,materialperformance,andwallassemblystrategies,
theresearchshowsthatacousticaldesignmustbebothtechnicallypreciseanddeeplyresponsive toclinicalrealities.CasestudieslikeLucilePackardChildren’sHospitaldemonstratehow innovativesystemslikeseamlessacousticplastermeetbothhygieneandsound-controlneeds, whileinterviewswithhealthcareworkersanddesignersrevealhownoisechallengespersist throughalarms,equipment,staffingpatterns,andunitlayouts.Theshifttowardsingle-family roomsimprovesprivacyandreducescross-unitnoise,yetstudiesshowthatlayoutalonecannot solveacousticproblemswithoutthoughtfulmaterialselection,strategicadjacencies,andongoing staffpractices.Together,thefindingsemphasizethatreducingsoundinNICUsrequiresalayered approach:high-performanceassemblies,cleanableacousticsurfaces,carefulplanning,visual alarmsystems,andeducationforfamiliesandstaff.Whenthesedesigndecisionsworkin combination,theycreatecalmer,saferenvironmentsthatsupporthealing,reducestress,and enhancetheoverallqualityofneonatalcare.
References: AcousticsinNeonatalCare
“Sound Plan: Achieve Optimal Healthcare Acoustics ” Healthcare Design Magazine,EmeraldX, ASoundPlan:HowToAchieveOptimalHealthcareAcoustics-HCDMagazine
“BestInterior/TenantImprovement:PhoenixChildren’sHospitalNICUBuild-Out” Engineering
News-Record,2024,BestInterior/TenantImprovement PhoenixChildren’sHospitalNICU
Build-out|EngineeringNews-Record
California Building Code,Title24,Part2,Chapter12:“InteriorEnvironment.”UpCodes,Chapter12
InteriorEnvironment:CaliforniaBuildingCode2022(Vol1&2)|UpCodes
“Standard 29: Acoustic Environment.” NICU Design Standards,UniversityofNotreDame,NICU Standard28:AcousticEnvironment
“Standard 21: Wall Surfaces.” NICU Design Standards,UniversityofNotreDame,NICUStandard20:
WallSurfaces
Baca,KellyA.“Noise Reduction in the Neonatal Intensive Care Unit: Promoting Neuroprotection and a Healing Environment.”NeonatalIntensiveCare/Pediatrics, JohnsHopkinsBayviewMedical Center,2023.Noisereductionintheneonatalintensivecareunit
Song,Yilin,andMardelleMShepley.“Neonatal Intensive Care Unit (NICU) Room Type Design
Trends.”AIAAcademyofArchitectureforHealth,2015.AAH 2015