The Aestheticians Journal Digital October'2025 Issue
Emerging Regenerative Therapies for Hair Loss: Exosomes, PRP and GFC
Hyaluronic Acid
Lip Boosters in Lip
Rejuvenation: Mechanisms, Techniques and Clinical Outcomes
Comprehensive Multimodal Management of Acne Vulgaris for Optimized Aesthetic Outcomes
Chemical Peel for Hyperpigmentation Part-I
Autologous Biofillers in Aesthetic
Dermatology: From Volume Restoration to Tissue Regeneration in Scar Management
EXECUTIVE
EDITOR & PUBLISHER
Dom Daniel CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
Printed, Published, Edited and Owned by Dom Daniel Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of October -2025
Advancing Aesthetic Dermatology: From Lip Rejuvenation to Regenerative Therapies
The field of aesthetic dermatology is evolving rapidly, bridging medical science with cosmetic enhancement. From minimally invasive procedures to advanced regenerative therapies, the goal is not only to enhance appearance but also to improve skin health and function. Innovations such as Chemical peels, lasers, autologous biofillers, and regenerative modalities empower clinicians to deliver personalized, safe, and effective care. Mastering both the art and science of these interventions is vital for optimal outcomes. We proudly present the October edition of The Aestheticians Journal, featuring insightful articles on these advancements.
This issue opens with an in-depth review of emerging regenerative therapies for hair loss, including exosomes, PRP, and GFC. We also spotlight hyaluronic acid lip boosters in lip rejuvenation, examining the mechanisms, techniques, and clinical outcomes that establish them as a cornerstone of modern lip enhancement. In addition, a comprehensive article on the multimodal management of acne vulgaris offers strategies to optimize both therapeutic and aesthetic outcomes.
Alongside chemical peels for hyperpigmentation, we also feature autologous biofillers, highlighting their emerging role in volume restoration and tissue regeneration, with particular promise in scar management.
We hope this issue provides you with valuable clinical insights and practical knowledge to enrich your practice and patient care.
Hope you have a great read!
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher
Dr. Karthini Baba, MD (Dermatology)
Dr. Irfana Patil, MBBS, DNB, DVL
Dr. Nirali Modi, MD (Dermatology)
Dr. Dipak Patel, MD,
Dr. Arunima Singh, MBBS, MD (Dermatology, Venereology and
Dr. Radhika Agarwal, MBBS, DNB, DVL
Editorial Board
Dr. Karthini Baba
MD (Dermatology)
Founder & Consultant Dermatologist
Skin Sanctum Hyderabad
Dr. Irfana Patil
MBBS, DNB, DVL
Consultant Cosmetic Dermatologist
Owner and Founder
Forever Young Skin and Hair Clinic
Kolhapur, Maharashtra
Dr. Nirali Modi
MD (Dermatology)
Dermatologist & Cosmetologist
Sparsh Skin Clinic
Godhra, Gujarat
Dr. Arunima Singh
MBBS, MD (Dermatology, Venereology and Leprosy)
Consultant Dermatologist
Agra, Uttar Pradesh
Dr. Dipak Patel
MD, DVD
Aesthetic Dermatologist & Cosmetologist
Neel Aesthetics
Surat
Dr. Radhika Agarwal
MBBS, DNB, DVL
Consultant Dermatologist
Agra, Uttar Pradesh
Emerging Regenerative Therapies for Hair Loss: Exosomes, PRP and GFC
Dr. Karthini Baba
MD (Dermatology)
Founder & Consultant Dermatologist
Skin Sanctum
Hyderabad
Introduction
Hair loss is a common dermatologic concern in both men and women, with a significant impact on self-esteem, social confidence, and quality of life. Causes are multifactorial, including genetic, hormonal, nutritional, systemic, drugrelated, stress-induced, and cosmetic factors. Androgenetic alopecia (AGA) is the most prevalent form. In men (male androgenetic alopecia, MAA), it manifests as receding hairline and crown thinning, progressing through miniaturization of terminal hairs into vellus hairs in a predictable pattern, with prevalence increasing with age. In women (female pattern hair loss, FPHL), it presents as diffuse thinning over the crown and frontal scalp with preservation of the frontal hairline. While DHTdriven follicular miniaturization is central, many women lack hyperandrogenism, suggesting additional genetic and androgen-independent mechanisms. Variants in androgen and estrogen receptors may also influence disease risk and treatment response. Current FDA-
approved treatments include minoxidil and finasteride, which can slow progression but have limitations such as delayed results, side effects, the need for long-term use, and high relapse rates upon discontinuation. Hair transplantation is effective but invasive, costly, and limited by donor availability. These challenges have shifted focus toward biologic and regenerative therapies, which hold promise for safer, more durable outcomes.1,2,3,4 Regenerative treatments can serve two important roles in the management of hair loss. For individuals who prefer not to use medications such as minoxidil or finasteride, these therapies provide an effective alternative option. At the same time, for those who are already on minoxidil and finasteride, regenerative approaches can act as complementary treatments, adding value by enhancing overall results and improving treatment outcomes.
One of the most exciting developments is the use of exosomes. These nanosized extracellular vesicles are
secreted by cells and carry proteins, nucleic acids, and lipids, enabling intercellular communication. Exosomes participate in vital processes such as wound healing, immune regulation, and tissue regeneration. In dermatology, they have been studied for photoaging, wound repair, atopic dermatitis, and more recently for hair growth. Exosomes derived from dermal papilla cells or mesenchymal stem cells can stimulate follicular activity, enhance angiogenesis, and promote regeneration of miniaturized follicles, making them an attractive therapeutic option for alopecia. Another biologic therapy that has gained significant traction is platelet-rich plasma (PRP). PRP is derived from the patient’s own blood and is rich in growth factors such as vascular endothelial growth factor (VEGF), plateletderived growth factor (PDGF), insulin-like growth factor (IGF), and transforming growth factor-β (TGF-β).1,4,5,6 Along similar lines, Growth Factor Concentrate (GFC) represents a more standardized method of preparing PRP. The process involves pre-set tubes, optimized spin protocols, and controlled processing times, ensuring consistency and reproducibility in the final product. Unlike PRP, which can vary depending on technique and operator, GFC minimizes variability and yields a concentrated, ready-to-use preparation of growth factors.
Many exosome products on the market are lab-grown or plant-derived, including those from flowers or other nonhuman sources. These are not considered true regenerative
treatments. True regenerative therapies are autologous exosomes, derived from the patient’s own body, harnessing their natural growth factors and signaling molecules to promote tissue repair and hair follicle regeneration.
Here, we summarize recent progress in the use of exosomes, PRP and GFC for hair growth, highlighting their biological mechanisms, therapeutic potential in the management of alopecia. We also present illustrative cases demonstrating excellent clinical outcomes, further supporting the promise of these regenerative approaches in real-world practice.
Diagnosis and Evaluation
Androgenetic alopecia (AGA) is the most common form of hair loss, presenting gradually after puberty. In men, it manifests as bitemporal recession and vertex thinning, while in women, it appears as diffuse thinning over the crown with frontal hairline preservation. Diagnosis is primarily clinical, aided by the Norwood-Hamilton scale in men and the Ludwig scale in women. Examination focuses on hair density, distribution, and miniaturization. A detailed history is essential to rule out mimickers such as chronic telogen effluvium. In women with signs of androgen excess, biochemical and imaging tests are warranted and metabolic syndrome screening is advisable.2,7
Dermoscopy (trichoscopy) is a valuable noninvasive tool for diagnosing androgenetic alopecia (AGA), enabling visualization of follicular changes such as hair shaft miniaturization, peripilar brown halos and
variation in shaft diameter. It also helps differentiate AGA from mimickers like diffuse alopecia areata, which shows tapered “exclamation point” hairs and fractured shafts. Although AGA is primarily a clinical diagnosis, a detailed history is crucial to exclude other causes, including onset and progression of hair loss, family history, systemic illnesses, stress, nutrition and medications. In women, telogen effluvium may unmask or exacerbate AGA, while earlyonset AGA in men is linked to metabolic abnormalities. Laboratory tests are reserved for uncertain cases or suspected contributing factors. Psychiatric assessment may be indicated, as hair loss can impact quality of life and cause depression or anxiety. Scalp biopsy is rarely needed, showing follicular miniaturization and increased telogen hairs.7
Relevant investigations for patients with hair loss include:
• Thyroid function tests
• Complete blood count (CBC)
• Iron profile: serum iron, ferritin and total iron-binding capacity (TIBC)
• Vitamin B12 levels
• Syphilis serology (if clinically indicated)
• In female pattern hair loss: hormonal profile including serum testosterone, DHEAS, and prolactin
Emerging Regenerative Treatment Modalities
When discussing true regenerative treatments, exosomes can be broadly categorized into two types. The first are those derived from an individual’s Adiposederived stem cells (ADSCs),
which harness the regenerative potential of stem cells to promote repair and rejuvenation. The second type is platelet-rich plasma (PRP), which utilizes the patient’s own platelets to release growth factors and stimulate tissue regeneration. Both approaches represent key pillars of regenerative medicine in aesthetic and hair restoration therapies.8,9 Central to these therapies are exosomes— nanosized extracellular vesicles (50–150 nm) secreted by cells that carry proteins, nucleic acids, and lipids. Acting as biological messengers, exosomes regulate intercellular communication and influence processes such as immune modulation, angiogenesis, tissue regeneration, and even disease progression. Their presence in biological fluids also makes them potential biomarkers for diagnosis through liquid biopsy. In regenerative dermatology, exosomes are increasingly recognized for their ability to promote hair growth by stimulating dermal papilla cells, enhancing angiogenesis, and activating pathways involved in follicular regeneration. Among exosome sources, stem cell–derived exosomes, particularly from ADSCs, have shown remarkable promise. ADSCExos facilitate hair growth by modulating the dermal papilla cell (DPC) cycle, promoting DPC proliferation, and rejuvenating the follicular microenvironment. They can also be engineered or photoactivated to boost proangiogenic and regenerative properties, offering innovative therapeutic potential for alopecia.1,8,9,10,11,12 PRP has already demonstrated encouraging clinical outcomes
in androgenetic alopecia (AGA). Recent advances have introduced PRP-derived exosomes (PRP-Exos), which encapsulate plateletderived growth factors within vesicles, enhancing efficacy, extending shelf stability, and improving clinical convenience. By combining the regenerative benefits of both PRP and exosomes, PRP-Exos represent a next-generation therapy for hair restoration.1,4,5,6
In comparison, PRP-derived exosomes (PRP-Exos) are effective but relatively less potent. They primarily encapsulate plateletderived growth factors, offering regenerative benefits with greater convenience and stability than traditional PRP, but their spectrum of action is narrower than ADSC-Exos.
PRP is an autologous concentrate prepared from centrifuged blood, enriched with platelets and growth factors such as PDGF, VEGF, TGF-β, and bFGF. These bioactive molecules play a crucial role in stimulating angiogenesis, collagen synthesis, and tissue repair, making PRP a widely used tool in regenerative medicine and aesthetics. Its therapeutic potential in hair loss is well-established, with growing clinical evidence supporting its role in androgenetic alopecia (AGA) and other hair disorders. A major challenge, however, lies in the variability of preparation protocols, which can impact consistency and clinical efficacy. Efforts to optimize PRP have included pre-incubation, dilution techniques, and supplementation with cryoprecipitates, all of which enhance its angiogenic and regenerative activity. More recently, photobiomodulation (low-level laser/light therapy) has been investigated as a method to “activate” PRP, enabling a more sustained and controlled release of growth factors. This combination approach holds promise for superior follicular regeneration and improved treatment outcomes.13,14,15,16 When injected into the scalp, PRP stimulates follicular stem cells, promotes cellular proliferation, and enhances angiogenesis. These effects collectively prolong the anagen (growth) phase of the hair cycle, supporting thicker, healthier hair regrowth.1,4,5,6
Patient 1
Before treatment
Before treatment
After 6 months of GFC treatment
After 6 months of GFC treatment
Before treatment
After 6 months of PRP treatment
Patient 2
Patient 3
Patient 4
Discussion
Androgenetic alopecia (AGA) remains one of the most common yet therapeutically challenging conditions encountered in dermatological practice. Conventional modalities such as topical and oral medications require long-term adherence and are often limited by variable efficacy and side effects, while surgical options are restricted to selected candidates. In this context, regenerative therapies—particularly platelet-rich plasma (PRP), exosomes, and autologous growth factor concentrate—have emerged as promising alternatives. PRP, prepared from autologous blood, exerts its effects through concentrated platelets and associated growth factors that stimulate angiogenesis, stem cell activation, and follicular proliferation. It has shown efficacy in both male and female pattern hair loss, as well as in alopecia areata. However, heterogeneity in preparation protocols, dosing, and frequency of sessions necessitates standardization before PRP can be universally adopted as a first-line regenerative therapy. Exosomes, extracellular vesicles critical to intercellular communication and tissue regeneration, represent a novel therapeutic frontier. Their role in hair follicle morphogenesis and modulation of the follicular microenvironment positions them as a compelling candidate for hair restoration. Preliminary evidence suggests favorable outcomes even after a single session, highlighting their potential for durable efficacy with minimal intervention. Nevertheless, their novelty underscores the need for larger controlled studies to validate safety, dosing, and long-term outcomes. GFC therapy, a modification of PRP technology, offers a concentrated pool of key bioactive molecules including platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), and insulin-like growth factor-1 (IGF-1). These growth factors synergistically promote angiogenesis, stem cell proliferation, follicular regeneration, and tissue repair. Mechanistically, PDGF facilitates hair canal formation, VEGF enhances perifollicular angiogenesis, EGF supports outer root sheath cell proliferation and shaft growth, and IGF-1 promotes
follicular proliferation and cycling. Improvements in hair pull test scores and high levels of patient satisfaction further reinforce the therapeutic promise of GFC. Adverse events were mild and transient, consisting mainly of pain at injection sites, erythema, and transient scalp irritation—findings consistent with prior literature. Overall, patient satisfaction is a critical outcome, given the psychosocial burden of alopecia. In this study, 80% of patients reported being highly satisfied with their results, aligning with prior reports documenting satisfaction rates exceeding 70%. However, limitations include small sample sizes and short follow-up durations. Larger randomized controlled trials with standardized protocols and extended follow-up are essential to validate efficacy, optimize treatment regimens, and integrate these therapies into evidence-based, individualized management strategies for androgenetic alopecia.6,17,18
Conclusion
In conclusion, hair loss— particularly androgenetic alopecia—remains a widespread and psychologically distressing condition. While conventional therapies are helpful, they are limited in effectiveness and tolerability. Regenerative approaches such as exosomes, PRP, PRP-Exos represent a new frontier in alopecia management. By directly harnessing the body’s own regenerative capacity, these biologic therapies hold promise not only for halting hair loss but also for achieving meaningful follicular regeneration, thereby restoring both hair and confidence. Exosomes, PRP
After 6 months of GFC treatment
Before treatment
Patient 5
represent three promising regenerative strategies for hair restoration. While PRP remains a widely used and cost-effective option, GFC offers a more standardized and potent formulation. Exosomes, as next-generation biologics, provide a futuristic approach by directly modulating cellular pathways for follicular regeneration. Together,
References
1. Cheng, Ming et al. “The Roles of Exosomes in Regulating Hair Follicle Growth.” Clinical, cosmetic and investigational dermatology vol. 17 16031612. 5 Jul. 2024, doi:10.2147/CCID. S465963
2. Singal A, Sonthalia S, Verma P. Female pattern hair loss. Indian J Dermatol Venereol Leprol 2013;79:626-640
3. Asfour L, Cranwell W, Sinclair R. Male Androgenetic Alopecia. [Updated 2023 Jan 25]. In: Feingold KR, Ahmed SF, Anawalt B, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi. nlm.nih.gov/books/NBK278957/
4. Gokce N, Basgoz N, Kenanoglu S, Akalin H, Ozkul Y, Ergoren MC, Beccari T, Bertelli M, Dundar M. An overview of the genetic aspects of hair loss and its connection with nutrition. J Prev Med Hyg 2022;63(suppl.3):E228-E238. https://doi.org/10.15167/2421-4248/ jpmh2022.63.2S3.2765
5. Lu, Changpei et al. “Platelet-rich plasmaderived exosomes stimulate hair follicle growth through activation of the Wnt/βCatenin signaling pathway.” Regenerative therapy vol. 29 435-446. 17 Apr. 2025, doi:10.1016/j.reth.2025.04.003
6. Bhargava, Aksha et al. “Revitalizing Hair Growth: A New Regimen Utilizing Growth Factor Concentrate for Hair Loss Treatment.” Cureus vol. 16,6 e63354. 28 Jun. 2024, doi:10.7759/cureus.63354
7. Ho CH, Sood T, Zito PM. Androgenetic Alopecia. [Updated 2024 Jan 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/ books/NBK430924/
8. Feng, Heting et al. “Adipose-derived stem cell exosomes: mechanisms and therapeutic potentials in wound healing.” Biomarker research vol. 13,1 88. 20 Jun. 2025, doi:10.1186/s40364-025-00801-2
9. Li, Yanqiao, Wang, Guangxing, Wang, Qian, Zhang, Yun, Cui, Lei, Huang, Xin, Exosomes Secreted from Adipose-Derived Stem Cells Are a Potential Treatment Agent for Immune-Mediated Alopecia, Journal of Immunology Research, 2022, 7471246, 14 pages, 2022. https://doi. org/10.1155/2022/7471246
10. Mahmood, Anarkali et al. “Exosome secretion kinetics are controlled by temperature.” Biophysical journal vol. 122,7 (2023): 1301-1314. doi:10.1016/j. bpj.2023.02.025
11. Yang, K., Li, D., Wang, M. et al. Exposure to blue light stimulates the proangiogenic capability of exosomes derived from human umbilical cord mesenchymal stem cells. Stem Cell Res Ther 10, 358 (2019). https:// doi.org/10.1186/s13287-019-1472-x
12. Kalluri, Raghu, and Valerie S LeBleu. “The biology, function, and biomedical applications of exosomes.” Science (New York, N.Y.) vol. 367,6478 (2020): eaau6977. doi:10.1126/science.aau6977
these therapies mark a paradigm shift in alopecia management, moving from symptomatic treatment to true biologically driven scalp rejuvenation.
13. Irmak, Gülseren et al. “Sustained release of growth factors from photoactivated platelet rich plasma (PRP).” European journal of pharmaceutics and biopharmaceutics : official journal of Arbeitsgemeinschaft fur Pharmazeutische Verfahrenstechnik e.V vol. 148 (2020): 67-76. doi:10.1016/j. ejpb.2019.11.011
14. Etulain, J., Mena, H.A., Meiss, R.P. et al. An optimised protocol for plateletrich plasma preparation to improve its angiogenic and regenerative properties. Sci Rep 8, 1513 (2018). https://doi. org/10.1038/s41598-018-19419-6
15. Wu, Jiuping et al. “Platelet-rich plasma-derived extracellular vesicles: A superior alternative in regenerative medicine?.” Cell proliferation vol. 54,12 (2021): e13123. doi:10.1111/cpr.13123
16. Pinto, Hernán et al. “The Effect of Photobiomodulation on Human Mesenchymal Cells: A Literature Review.” Aesthetic plastic surgery vol. 45,4 (2021): 1826-1842. doi:10.1007/s00266-02102173-y
17. Hassan L, et al. (2024). Compare the Efficacy of PRP Intervention VS Exosomes for Hair loss, a Case Series Study. Dermis. 4(3):19
18. Singh N, Reddy M, Jajapuram G. Growth factor concentrate therapy for management of hair loss: a prospective, real-world study. Int J Res Dermatol 2023;9:27-31.
Hyaluronic Acid Lip Boosters in Lip Rejuvenation: Mechanisms, Techniques and Clinical Outcomes
Dr. Irfana Patil
MBBS, DNB, DVL
Consultant Cosmetic Dermatologist
Owner and Founder
Forever Young Skin and Hair Clinic
Kolhapur, Maharashtra
Introduction
Lip aesthetics play a crucial role in facial harmony and overall attractiveness, as the lips serve as a focal point of the face, significantly influencing emotional expression, communication, and the perception of beauty. The structure, proportions, and contour of the lips contribute to overall facial balance, making them a key consideration in both medical and aesthetic practices.1 Anatomically, the lips consist of several distinct regions. The cutaneous zone (external surface) is the outermost layer, covered by thin, pigmented skin that lacks sebaceous and sweat glands. The vermillion border acts as a transitional zone between the skin and the mucosal surface, defining the lip contour. The vermillion itself is a highly vascularized, pinkish-red portion of the lips. The upper vermillion features the Cupid’s bow, a prominent aesthetic landmark, while the lower lip is typically fuller, contributing to overall
balance and proportion. The philtrum is a vertical groove extending from the base of the nose to the upper lip, which gradually diminishes in prominence with aging, affecting lip definition. The oral commissures, where the upper and lower lips meet laterally, play a key role in facial expressions and impact the perception of youthfulness. Lip movement is primarily controlled by the orbicularis oris, a circular muscle responsible for lip motion, while other muscles, including the zygomaticus major and minor, levator anguli oris, and depressor anguli oris, contribute to facial expressions such as smiling, frowning, and pursing the lips. The vascular supply to the lips is primarily derived from the facial and infraorbital arteries, while venous drainage occurs through the facial veins, ensuring adequate circulation, hydration, and overall lip health.2
The ideal lip proportions have long been guided by aesthetic principles, such as the golden
ratio, which suggests an optimal upper-to-lower lip ratio of approximately 1:1.6. However, lip morphology can vary significantly due to genetic factors and natural aging processes. Over time, factors such as aging, environmental exposure, lifestyle choices, and genetics can all impact lip aesthetics.2 As we age, changes like volume loss, thinning of fat and collagen, flattening of the Cupid’s bow, elongation of the philtrum, deepening of smoker’s lines and descent of the oral commissures contribute to a more fatigued or aged appearance. Additionally, sun exposure, smoking, and hormonal changes further exacerbate these effects, leading to a less expressive and diminished look. These changes can affect an individual’s selfesteem, often creating a desire to restore a youthful appearance. As a result, lip augmentation becomes a necessary option for enhancing lip volume, definition, and overall facial harmony.1
The natural positioning and dynamic motion of the lips contribute to perceived youthfulness and emotional expressiveness. Over time, aging leads to notable changes in lip morphology, including volume loss, diminished vermillion definition, increased perioral rhytides (fine lines and wrinkles), and a downturn in oral commissures. These changes contribute to an aged or fatigued appearance, prompting many individuals to seek aesthetic interventions for lip enhancement.2
Case report
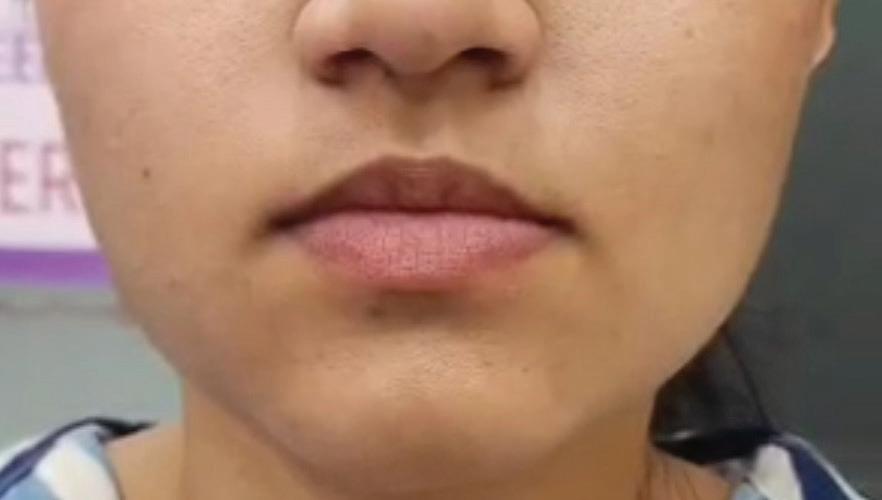
A 25-year-old female patient
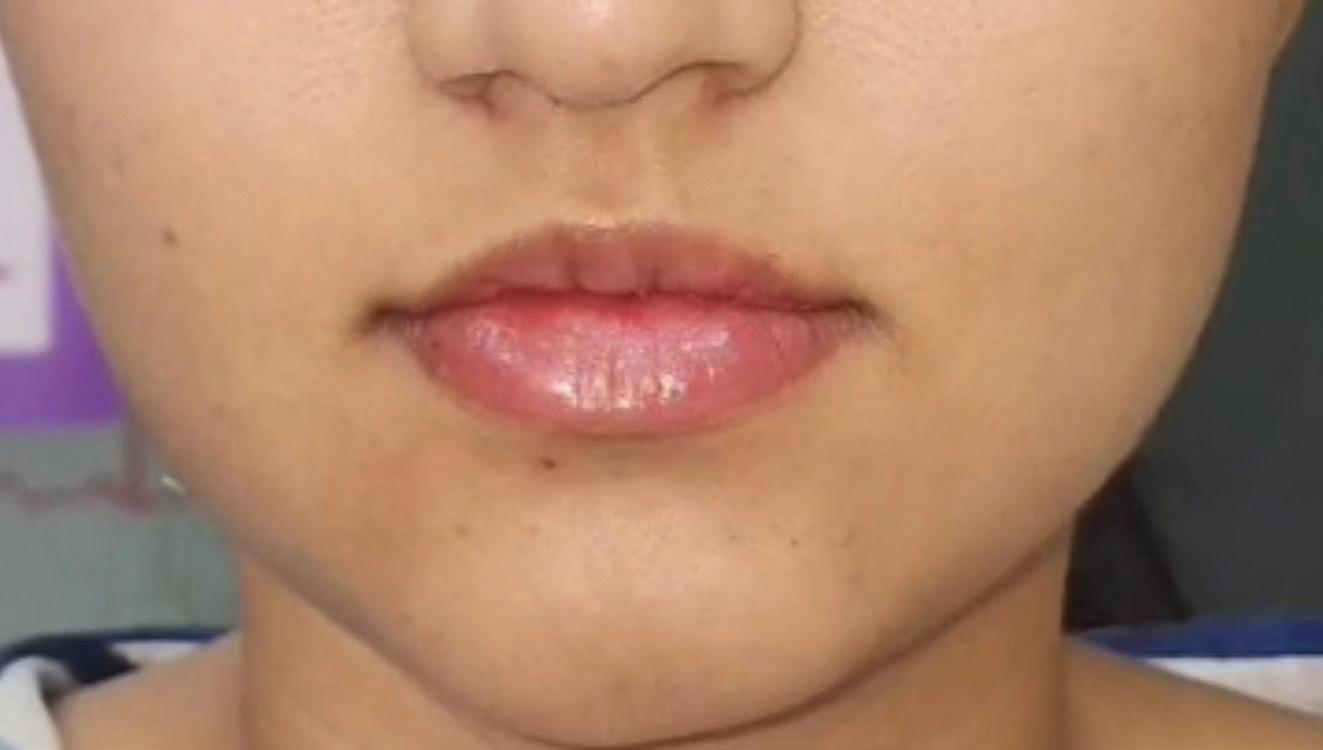
presented with dry, dehydrated lips despite regular use of lip balms that failed to deliver lasting hydration. Patient just wanted lip hydration without augmentation in lip volume. The treatment opted was lip skin boosters, advanced hyaluronic acid injections designed to deeply hydrate and rejuvenate the lips from within. The procedure was performed using microinjections of stabilized hyaluronic acid, aiming to restore moisture, smooth fine lines, and enhance the lips' natural glow without adding unnecessary volume. Within a short period, the patient experienced significant improvement in lip hydration, texture, and radiance. The patient's lips remained well-hydrated and supple, with fine lines visibly reduced. The treatment was well tolerated with no adverse effects, demonstrating the effectiveness of lip skin boosters in providing long-lasting lip hydration and rejuvenation, without affecting the lip shape volume.
Before treatment
After treatment
1: Hyaluronic acid lip booster demonstrates effective treatment for lip hydration and smoother lip texture
Discussion
Collagen-based fillers, once widely used for lip augmentation, have declined in popularity with the advent of hyaluronic acid (HA) fillers but remain valuable for their natural feel, immediate results,
Hyaluronic
Figure
and ability to enhance volume, contour, and hydration. Derived from bovine, porcine, human, or bioengineered sources, they provide structural support, degrade naturally, and may stimulate endogenous collagen production. In contrast, polymethylmethacrylate (PMMA) is a synthetic, biocompatible polymer offering semipermanent results. Composed of microspheres in a gel carrier, PMMA provides immediate volume, with collagen gradually forming around the spheres for lasting effects. Both options serve distinct purposes in delivering customized lip enhancement outcomes.3,4
Hyaluronic acid (HA), a naturally occurring glycosaminoglycan composed of alternating d-glucuronic acid and N-acetyld-glucosamine residues, exerts its mechanism of action by attracting and retaining water molecules due to its anionic properties. This ability to bind water contributes to the volumizing effect and enhanced hydration of the skin. When injected into the submucosa of the lips, HA fillers integrate with the surrounding tissue, providing structural support, improving tissue elasticity, and restoring lost volume. The cross-linked structure of the HA gel ensures prolonged stability within the tissue, leading to long-lasting enhancement of lip volume, definition and contour. Hyaluronic acid (HA) fillers, extensively used for lip augmentation, are valued for their soft, gel-like texture and versatility. The viscosity and structure of HA gels can be tailored to create either a softer, skin-like consistency or
a firmer formulation for greater support.5,6,7
The primary aim of fillers is to enhance lip volume, shape, definition, and symmetry, while also improving contour. Because of their cross-linked structure, dermal fillers retain their form and typically last 6–12 months, depending on the product used, the treatment area, and the patient’s metabolism.
Lip boosters contain non–crosslinked hyaluronic acid and may be combined with other ingredients aimed at improving hydration, smoothness, and texture. The goal is not to significantly increase lip volume but rather to provide deep hydration and subtle enhancement. Lip boosters tend to offer more temporary results compared to fillers, often requiring multiple sessions for optimal effect.
Techniques and Considerations
Treatment begins with a thorough patient consultation, including medical history review, anatomical assessment, and clarification of aesthetic goals. The lips are then cleansed and disinfected, and local anesthesia—topical or injectable—is administered for comfort.5, 6, 7
The procedure itself is minimally invasive, typically lasting 15 to 30 minutes, making it a convenient option for individuals seeking immediate results. Following the injections, an ice pack is applied to reduce swelling and bruising, and patients are instructed to avoid touching or manipulating the treated area for atleast 48 hours. Additionally, patients are advised to refrain
from strenuous physical activity during this time to ensure optimal healing.5,6 A follow-up appointment is scheduled to assess the final results, and touch-ups are considered if necessary.7
Lip boosters are injected intradermally rather than into deeper tissues, as with traditional fillers. The procedure often uses a fine needle (e.g., 32G) or a cannula, with injections spaced approximately 0.5–1 cm apart. Common techniques include:
• Microinjections – small boluses (0.05–0.1 ml) deposited superficially for even hydration.
• Linear Threading – product placed parallel to the vermillion border for subtle definition.
• Retrograde Linear Threading – product deposited during needle or cannula withdrawal for smooth distribution.
• 4-Point Technique – injections at key anatomical landmarks (e.g., cupid’s bow and lower lip tubercles) for balanced hydration.
A typical session uses 1–1.5 ml of product, with 2–3 sessions spaced 2–6 weeks apart recommended for best results. Maintenance treatments are generally performed every 5–8 months.
Benefits and Limitations
The primary benefits of lip boosters include intense hydration, improved lip texture, increased elasticity, and a subtle plumping effect without altering natural proportions. They are particularly well-suited for patients seeking a refreshed, healthy lip appearance rather than a noticeable volume
Hyaluronic
increase. However, the main limitations are their shorter duration, need for repeat treatments, and the risk of affecting pre-existing filler if used in previously augmented lips.
Conclusion
Lip boosters are most beneficial for clients whose primary concern is hydration rather than volume. They are ideal for individuals suffering from dry, cracked, or sore lips, as well as those who want to improve lip smoothness and elasticity without altering the shape or size. They may also be suitable after lip filler dissolution, particularly if the client’s natural hyaluronic acid has been depleted or if the lip tissue has been compromised (e.g., pockets after migration or lumps). In such cases, boosters can aid in tissue repair
References
1. Piccinin MA, Zito PM. Anatomy, Head and Neck, Lips. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 5, 2023.
2. Kar M, Muluk NB, Bafaqeeh SA, Cingi C. Is it possible to define the ideal lips? Acta Otorhinolaryngol Ital. 2018; 38(1):67-72. Doi: 10.14639/0392-100X-1511.
nodules of the lips: Clinical presentation and management by intralesional neodymium:YAG laser therapy. Dermatol Ther. 2019; 32(1):e12755. doi:10.1111/ dth.12755.
7. Walker K, Basehore BM, Goyal A, Zito PM. Hyaluronic Acid. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 3, 2023. Hyaluronic Acid Lip Boosters in
3. Rostan E. Collagen fillers. Facial Plast Surg Clin North Am. 2007; 15(1):55-VI. doi:10.1016/j.fsc.2006.11.001.
4. Goldman A, Wollina U. Polymethylmethacrylate-induced
5. Díaz-Aguayo I, Urdiales-Gálvez F, Benítez PA, et al. Aesthetic management of lips and perioral region with Hylacross® and Vycross® hyaluronic-acid based fillers: A document of recommendations. J Cosmet Dermatol. 2024; 23(9):2843-2856. doi:10.1111/jocd.16358.
6. Nikolis A, Bertucci V, Solish N, Lane V, Nogueira A. An Objective, Quantitative
and restoration. However, lip boosters are not a replacement for fillers. Using them in clients who expect volumetric enhancement may lead to disappointment. Additionally, they should be avoided in clients who already have a substantial amount of dermal filler in the lips, as the hydration effect can disperse the filler (similar to a saline flush), potentially causing lumps or migration.
Assessment of Flexible Hyaluronic Acid Fillers in Lip and Perioral Enhancement. Dermatol Surg. 2021; 47(5):e168-e173. doi:10.1097/DSS.0000000000002917.
Emerging Treatment Demonstrates Efficacy in Acne Scar Management
Acne vulgaris remains a prevalent inflammatory dermatosis, frequently resulting in atrophic scarring that poses significant therapeutic and psychosocial challenges. Current treatment modalities—such as microneedling and laser therapies—offer variable efficacy depending on scar morphology and patient skin type, with no universally accepted standard of care. A recent investigation assessed the efficacy of a novel combination therapy integrating autologous fibroblast transplantation with platelet-rich plasma (PRP) injections, compared to PRP monotherapy, in the management of atrophic acne scars. While both groups demonstrated clinical improvement, the combination therapy yielded superior outcomes, including enhanced dermal thickness, reduced scar volume, improved skin elasticity, and restoration of barrier function. The autologous nature of fibroblast therapy reduces immunogenic risk and may provide more sustained dermal remodelling compared to temporary fillers. No serious adverse effects were reported, and patient-reported outcomes indicated high levels of satisfaction. Although initial results are encouraging, the authors underscore the need for larger, controlled studies to validate clinical efficacy, refine treatment protocols, and assess long-term safety. This approach, pending further evidence, may represent a promising advancement in the treatment of acne scarring.
Advancing Phage PA6 as a Therapeutic Strategy for Acne Vulgaris
Acne vulgaris, a prevalent inflammatory skin disorder driven largely by Cutibacterium acnes, continues to pose therapeutic challenges, particularly in the face of rising antibiotic resistance. With traditional treatments increasingly limited by microbial resistance, bacteriophage therapy has emerged as a promising alternative. Bacteriophages are viruses that specifically target and lyse bacteria, offering precision in microbial control. Phage PA6, a lytic bacteriophage identified for its specificity against Cutibacterium acnes, has shown potential due to its ability to target and destroy the bacterium without affecting the surrounding microbiota. However, challenges remain, including limited phage diversity due to the genetic homogeneity of C. acnes, difficulties in penetrating the biofilm environment of hair follicles, and restricted in vivo accessibility via topical application. Despite these hurdles, bacteriophage-based treatments have demonstrated success in other dermatologic infections, such as those caused by Staphylococcus aureus, highlighting their potential broader utility. With further research and clinical validation, phage therapy could offer a highly targeted, resistance-free approach to managing acne and other dermatological conditions, and may extend its applications into cosmetic and antimicrobial preservation sectors.
Low-Level Light Therapy Shows Expanding Promise in the Treatment of Alopecia
Low-level light therapy (LLLT) is increasingly emerging as a clinically relevant, non-invasive treatment option for various forms of alopecia, with recent data supporting its efficacy particularly in androgenetic alopecia and early promise in scarring alopecias such as central centrifugal cicatricial alopecia (CCCA) and lichen planopilaris. A recent comprehensive review evaluated the current landscape of LLLT, emphasizing its role as an adjunct or alternative to conventional pharmacologic treatments like minoxidil and finasteride. The therapy functions by utilizing targeted wavelengths of light to stimulate follicular repair, extend the anagen growth phase, and enhance perifollicular microcirculation. With growing accessibility through dual-wavelength LED caps and at-home devices, LLLT offers a patient-friendly modality that demonstrates improved hair density, reduced shedding and potential immune-modulatory effects, particularly in cases of telogen effluvium and alopecia areata. The review synthesized existing literature and categorized findings across various alopecia subtypes. Notably, case reports within the scarring alopecia subset described visible regrowth and decreased inflammation, highlighting a new therapeutic avenue for traditionally refractory conditions. While LLLT has demonstrated a favorable safety profile and high compliance rates, the authors emphasized the need for further large-scale studies to define standardized treatment protocols, optimal dosimetry and long-term efficacy. Given the current evidence, clinicians are encouraged to consider integrating LLLT into individualized treatment regimens for patients seeking non-systemic options or those unresponsive to conventional therapies.
Efficacy of Medium to Deep Chemical Peels in the Management of Refractory Melasma
Recent clinical evidence highlights the safety and therapeutic efficacy of medium to deep chemical peels, particularly phenol–croton oil and trichloroacetic acid (TCA)-based formulations, in the management of refractory melasma among women with diverse Fitzpatrick skin types. A segmented application technique was utilized for enhanced procedural control and optimized healing, involving either phenol with croton oil or a two-step regimen of glycolic acid followed by TCA with croton oil. Post-procedural care included a protective chemical mask containing lidocaine and nystatin under a plastic barrier, followed by a regenerative topical regimen with collagenase, chloramphenicol and petroleum jelly to support wound healing and dermal remodeling. Objective assessments using digital image analysis and subjective evaluations by dermatology experts demonstrated significant improvement in pigmentation, skin tone uniformity, texture, and overall skin luminosity. Most treated areas showed a marked reduction in melasma severity, with improved border definition and decreased pigment density. Healing was achieved uneventfully in most cases, with transient erythema and post-inflammatory hyperpigmentation being the most commonly reported adverse effects; one case of allergic reaction was noted during the recovery phase. These findings confirm that individualized medium to deep peels, when combined with appropriate post-care, represent a safe, effective and clinically durable therapeutic option for managing recalcitrant melasma.
Comprehensive Multimodal Management of Acne Vulgaris for Optimized Aesthetic Outcomes
Dr. Nirali Modi
MD (Dermatology)
Dermatologist & Cosmetologist
Sparsh Skin Clinic
Godhra, Gujarat
Introduction
Acne vulgaris is a chronic inflammatory disorder of the pilosebaceous unit, predominantly affecting adolescents and young adults, with prevalence estimates ranging from 35% to over 90%. Onset typically occurs between 7 and 12 years of age, with spontaneous resolution by the third decade in most cases; however, persistence or adultonset acne is not uncommon. Adolescent acne demonstrates a higher prevalence in males, whereas post-adolescent acne is more frequently observed in females. Clinically, acne is characterized by polymorphic lesions including open and closed comedones, inflammatory papules, pustules, nodules, and cysts, primarily distributed over the face, upper chest, back, and upper arms. The condition is graded in severity from Grade 1, marked by predominantly comedonal lesions, to Grade 4, characterized by extensive nodulocystic involvement
and marked inflammation. Notable variants include acne conglobata, characterized by extensive nodulocystic lesions with interconnected comedones predominantly in young males; acne fulminans, an acute ulcerative form often accompanied by systemic symptoms; Acne excoriée, often seen in young females, is associated with compulsive picking or manipulation of lesions, while infantile acne is attributed to temporary elevations in androgen levels during early infancy. Acne may also be associated with syndromic entities such as SAPHO and PAPA syndromes, which involve multisystem inflammation.1, 2
The pathogenesis of acne vulgaris is multifactorial, arising from the interplay of four core mechanisms: excess sebum production, follicular hyperkeratinization, colonization by Cutibacterium acnes (formerly Propionibacterium acnes), and inflammation. Sebaceous
gland hyperactivity is driven by elevated androgen levels or heightened sensitivity of sebocytes to circulating androgens. Simultaneously, abnormal keratinization within the follicular infundibulum results in obstruction and comedone formation. The occluded follicular milieu promotes proliferation of C. acnes, which triggers inflammatory cascades via proinflammatory mediators and activation of innate immune pathways. Notably, inflammation is now recognized to occur even in clinically non-inflamed lesions, emphasizing acne as a chronic inflammatory disorder. Multiple endogenous and exogenous factors modulate disease severity. Well-known pharmacologic triggers include systemic corticosteroids, lithium, and anticonvulsants such as phenytoin, while oilbased cosmetics and occlusive skincare products aggravate lesions in predisposed individuals. Ultraviolet exposure may provide temporary benefit but often exacerbates inflammation and induces flareups. Endocrinopathies such as polycystic ovary syndrome, congenital adrenal hyperplasia, and pregnancy-related hormonal changes frequently worsen acne, with up to 70% of women reporting premenstrual flares due to periductal edema and heightened sebaceous activity. Dietary influences are increasingly recognized, with high glycemic index foods and dairy products linked to elevated insulin and insulinlike growth factor 1 (IGF1) levels. IGF-1 promotes sebaceous gland proliferation and keratinocyte growth,
perpetuating acne lesions. Environmental exposures, including tobacco smoke and atmospheric pollutants, enhance oxidative stress and cutaneous inflammation. Additionally, repetitive mechanical trauma— such as over-cleansing, abrasive scrubbing, or harsh soaps—damages the skin barrier and perpetuates inflammation. Collectively, these diverse influences highlight the complex pathophysiology of acne vulgaris. Understanding its multifaceted mechanisms underscores the need for tailored, multimodal treatment strategies to achieve optimal and sustained clinical outcomes.2,3
We present a series of cases with moderate to severe acne, including comedonal lesions and post-acne atrophic scarring, managed through a comprehensive multimodal therapeutic regimen. The protocol incorporated an anti-acne cocktail, salicylic acid chemical peels, hydradermabrasion, fractional CO₂ laser, and microneedling radiofrequency (MNRF), with treatment plans individualized according to skin type and clinical severity. One patient demonstrated marked improvement in comedonal and inflammatory lesions, along with enhanced skin texture, within three months of initiating therapy. Another patient exhibited appreciable improvement in acne activity and scar remodeling at the six-month follow-up. This combination-based approach was clinically effective in simultaneously addressing active acne, comedonal lesions, and atrophic scars. The
outcomes underscore the value of personalized, multimodal strategies in optimizing therapeutic results and improving long-term skin quality.
Diagnosis
Acne vulgaris is mainly diagnosed through clinical evaluation, with standardized scoring systems aiding in assessing severity, guiding treatment choices, and tracking outcomes. Among these, the Global Acne Grading System (GAGS) is frequently applied, as it considers both the type of lesions and their distribution across different body sites. Complementary scales such as the Investigator Global Assessment (IGA) and the Leeds Revised Acne Grading System provide consistency in clinical evaluation. Lesion counting—documenting.......... comedones, papules, pustules, and nodules in defined regions—is particularly useful in clinical trials and during followup assessments. Advances in multimodal digital imaging, including cross-polarized light, ultraviolet fluorescence, and three-dimensional mapping, allow detailed lesion visualization and objective quantification. Laboratory testing is recommended in patients with features of hyperandrogenism— such as hirsutism, menstrual irregularities, or refractory acne—particularly in females. Relevant investigations include serum testosterone, androstenedione, DHEA, DHEAS, LH, and FSH, aiding in the detection of polycystic ovary syndrome or other androgen-excess disorders.4 Dermoscopy has emerged as a valuable non-invasive tool,
enhancing the visualization of follicular plugging, perifollicular erythema, and telangiectasia.5 Microbiological studies, though not routine, may be employed to identify Cutibacterium acnes or detect secondary infections, supporting targeted antimicrobial therapy.6 Skin biopsy is rarely required but can assist in atypical, severe, or recalcitrant cases by demonstrating follicular inflammation, rupture, and dermal changes.7 Sebumetry, which quantifies sebum excretion, provides additional insight into seborrhea—a major pathogenic factor in acne— and is particularly relevant in research and therapeutic monitoring.8
Accurate application of these diagnostic modalities strengthens clinical decisionmaking, ensuring effective evaluation and optimal management of acne vulgaris.
Treatment
Acne treatment is tailored to severity and lesion type, addressing abnormal keratinization, microbial colonization, inflammatory processes, and sebaceous activity.
Anti-acne cocktail agents offer a synergistic approach targeting key factors in acne pathogenesis, including abnormal keratinization, microbial proliferation, inflammation, and sebum production. Common agents include benzoyl peroxide, topical antibiotics, retinoids, azelaic acid, and dapsone, formulated in various vehicles for tailored treatment based on lesion type and location. Benzoyl
peroxide disrupts comedones, reduces inflammation, and kills C. acnes, with low resistance risk, making it effective alone or combined. Topical antibiotics like clindamycin provide antimicrobial and antiinflammatory benefits, enhanced when used with benzoyl peroxide. Retinoids (adapalene, tazarotene, tretinoin) normalize keratinocyte differentiation, reduce microcomedones, and inflammation—adapalene being more tolerable, tazarotene more potent. Fixed combinations improve adherence and outcomes. Azelaic acid is a safe, welltolerated agent effective against hyperpigmentation, suitable in pregnancy.6 Topical dapsone offers anti-inflammatory and antibacterial effects, particularly for adult females. Together, these agents form a personalized, evidencebased, and safe acne treatment strategy.9
Salicylic acid, a lipid-soluble beta hydroxy acid, is widely used in superficial chemical peels for its comedolytic, keratolytic, anti-inflammatory, and antibacterial effects. At 20–30% concentrations and pH 3–4, it effectively clears comedones, reduces sebum, and improves acne and skin texture. Other agents, including alpha hydroxy acids like glycolic and lactic acid, complement BHAs by enhancing exfoliation, promoting epidermal turnover, and improving skin tone. Glycolic acid offers deeper exfoliation, while lactic acid provides gentler resurfacing with moisturizing benefits.6, 9
A non-invasive................... hydradermabrasion procedure
integrates precise mechanical exfoliation, vacuum-assisted pore cleansing, and concurrent delivery of specialized topical formulations. Utilizing proprietary vortex technology, it facilitates the removal of keratinized epithelium, sebaceous material, and follicular occlusions contributing to acne lesion formation. By targeting key pathogenic factors such as follicular hyperkeratinization, sebum retention, and microbial colonization, the treatment offers a multifactorial therapeutic approach. It is welltolerated and serves as an effective adjunct in managing acne vulgaris, especially in patients with comedonal and inflammatory lesions.10, 11
Carbon dioxide (CO₂) laser therapy, emitting at 10,600 nm, is an effective modality for both active acne and atrophic acne scars. Through selective photothermolysis, it enables precise ablation and controlled dermal coagulation, reducing sebaceous activity and inflammation. Fractional CO₂ laser induces neocollagenesis and dermal remodeling, improving scar depth and skin texture with minimal damage to surrounding tissue. Other energy-based devices also aid in acne and scar treatment: KTP and pulsed dye lasers target vascular lesions; diode and erbium glass lasers reduce sebum and remodel collagen. IPL treats acne and pigmentation. RF microneedling boosts collagen, while blue/ red light and photodynamic therapy offer antimicrobial and sebosuppressive effects. Treatment can be tailored to acne severity, scarring, and skin
type.12, 13
Microneedling radiofrequency (MNRF) is a minimally invasive procedure used to treat acne and atrophic acne scarring. It delivers controlled radiofrequency energy via microneedles into the dermis, inducing neocollagenesis and dermal remodeling to improve scar texture. MNRF also reduces sebaceous gland activity and bacterial colonization, decreasing inflammation and sebum production. By sparing the epidermis, it minimizes downtime and decreases the incidence of post-inflammatory hyperpigmentation, making it suitable for various skin types. MNRF is an effective and safe option in tailored acne management.14
Cryotherapy for acne uses controlled cold to destroy overactive
Result
Patient 1
Aesthetic Outcomes
sebaceous glands, reduce inflammation, and suppress acne-causing bacteria, promoting faster lesion resolution with minimal surrounding skin damage.15 Effective acne management relies on a personalized, multimodal strategy combining pharmacologic and procedural treatments to target multiple pathogenic factors and improve outcomes.
Before Treatment
After 3 months of treatment
Multimodal Management of Acne Vulgaris for Optimized
Patient 2
Patient 3
After 3 months of treatment
Patient 4
Patient 5
Discussion
Acne vulgaris is the most common dermatological disorder worldwide, and its rising incidence poses growing challenges for clinicians and public health systems. Beyond visible lesions, acne profoundly impacts psychosocial wellbeing, contributing to low selfesteem, social withdrawal, anxiety, and depression. These psychological consequences highlight the importance of early recognition and effective management to improve both skin health and quality of life. Diagnosis of acne vulgaris is primarily clinical, yet accurate differentiation from acneiform and non-acneiform mimickers is essential, especially in atypical, treatment-resistant, or adultonset cases. Careful evaluation of lesion morphology, distribution, demographics, and systemic associations forms the cornerstone of diagnostic accuracy. Infectious mimics include bacterial folliculitis and Malassezia folliculitis, which present as monomorphic pustules without comedones, often pruritic. Acne keloidalis nuchae, common in individuals with coarse or curly hair, manifests as chronic papules and keloid-like plaques on the nape. Non-inflammatory mimics such as milia, syringomas, and sebaceous hyperplasia present as uniform papules with distinct clinical clues. Rare conditions like nevus comedonicus, characterized by grouped dilated follicular openings in a congenital or dermatomal
pattern, may resemble acne. Other considerations include papulopustular rosacea (centrofacial erythema, telangiectasia, absence of comedones) and keratosis pilaris (keratotic papules on extensor surfaces). Nodulocystic mimics such as eruptive vellus hair cysts and steatocystoma multiplex also resemble severe acne but are non-inflammatory and unresponsive to standard therapies. Drug-induced acneiform eruptions are another diagnostic challenge. They present as sudden-onset, monomorphic papules and pustules without comedones, often on the trunk or upper arms. Causative agents include corticosteroids, anabolic steroids, lithium, isoniazid, halogenated compounds, and targeted therapies like EGFR and VEGF inhibitors. Improvement after discontinuation strongly supports the diagnosis. In refractory cases, syndromic conditions such as Birt–Hogg–Dubé, Cowden, or Muir–Torre syndromes should be considered due to associations with follicular tumors, sebaceous neoplasms, and internal malignancies. Complications of acne include post-inflammatory hyperpigmentation, particularly in darker skin types, and hypopigmentation after severe inflammation. Scarring is common and distressing, with atrophic (ice pick, boxcar, rolling) and hypertrophic or keloidal variants significantly affecting quality of life. Rare sequelae such as Morbihan
disease and dystrophic calcinosis cutis have also been reported. Although the prognosis of acne vulgaris is generally favorable with early and sustained treatment, it often follows a chronic, relapsing course. Adultonset acne—particularly in women—is increasingly prevalent due to hormonal, cosmetic, and lifestyle factors. Management requires a multimodal, individualized approach combining topical and systemic agents, procedural interventions, and adjunctive therapies. Emerging evidence on diet, particularly high glycemic index foods and dairy, further supports lifestyle modification as part of comprehensive care.1,2,3
Conclusion
Acne vulgaris affects both males and females, with males often experiencing more severe androgen-driven inflammatory lesions, while females commonly present with persistent adult acne influenced by hormonal changes. The condition significantly impacts patients' well-being and can lead to social withdrawal. A multimodal approach with treatments such as anti-acne cocktail, salicylic acid chemical peels, hydradermabrasion, CO₂ laser, and microneedling radiofrequency (MNRF) shows efficacy in managing acne. Advances in targeted biologics, hormonal therapies, and novel topicals have further enhanced treatment outcomes.
References
1. Sutaria AH, Masood S, Saleh HM, Schlessinger J. Acne Vulgaris. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 17, 2023.
2. Vasam M, Korutla S, Bohara RA. Acne vulgaris: A review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023; 36:101578. Published 2023 Nov 23. doi:10.1016/j.bbrep.2023.101578.
3. Ayer J, Burrows N. Acne: more than skin deep. Postgrad Med J. 2006; 82(970):500506. doi:10.1136/pgmj.2006.045377.
4. Bae IH, Kwak JH, Na CH, Kim MS, Shin BS, Choi H. A Comprehensive Review of the Acne Grading Scale in 2023. Ann Dermatol. 2024; 36(2):65-73. doi:10.5021/ad.23.094
5. Alma A, Sticchi A, Chello C, et al. Dermoscopy, Reflectance Confocal Microscopy and Optical Coherence Tomography Features of Acne: A Systematic Review. J Clin Med. 2022; 11(7):1783. Published 2022 Mar 24. Doi: 10.3390/jcm11071783.
6. Xu DT, Chen Q, Yang JY, et al. A noteworthy issue: microbiome data
variation depending on sampling methods in skin microecology studies in acne vulgaris patients. Front Immunol. 2025; 16:1566786. Published 2025 Jun 9. doi:10.3389/fimmu.2025.1566786.
7. Korfitis C, Gregoriou S, Antoniou C, Katsambas AD, Rigopoulos D. Skin biopsy in the context of dermatological diagnosis: a retrospective cohort study. Dermatol Res Pract. 2014; 2014:734906. doi:10.1155/2014/734906.
8. Liu Y, Jiang W, Tang Y, et al. An optimal method for quantifying the facial sebum level and characterizing facial sebum features. Skin Res Technol. 2023; 29(9):e13454. doi:10.1111/srt.13454
9. Bozzo P, Chua-Gocheco A, Einarson A. Safety of skin care products during pregnancy. Can FAM Physician. 2011; 57(6):665-667.
10. Storgard R, Mauricio-Lee J, Mauricio T, Zaiac M, Karnik J. Efficacy and Tolerability of HydraFacial Clarifying Treatment Series in the Treatment of Active Acne Vulgaris. J Clin Aesthet Dermatol. 2022; 15(12):42-46.
11. Razi S, Truong TM, Khan S, Sanabria B, Rao B. Hydradermabrasion through the lens
of Line-Field Confocal Optical Coherence Tomography. Skin Res Technol. 2024; 30(4):e13684. doi:10.1111/srt.13684.
12. Jih MH, Kimyai-Asadi A. Laser treatment of acne vulgaris. Semin Plast Surg. 2007; 21(3):167-174. Doi: 10.1055/s-2007-991185.
13. Pall A, Pall S. An Innovative Approach of Treating Acne Scars Using Bipolar Rotational Stamping and Monopolar Criss-cross Technique with Insulated Microneedling Radiofrequency in Asians. J Cutan Aesthet Surg. 2021; 14(2):191202. doi:10.4103/JCAS.JCAS_89_19.
14. Oge' LK, Broussard A, Marshall MD. Acne Vulgaris: Diagnosis and Treatment. Am FAM Physician. 2019; 100(8):475484.
15. Hong JY, Kim KR, Kim HJ, Seok J, Park KY. Targeted precision cryotherapy for acne vulgaris. Skin Res Technol. 2024; 30(9):e70045. doi:10.1111/srt.70045.
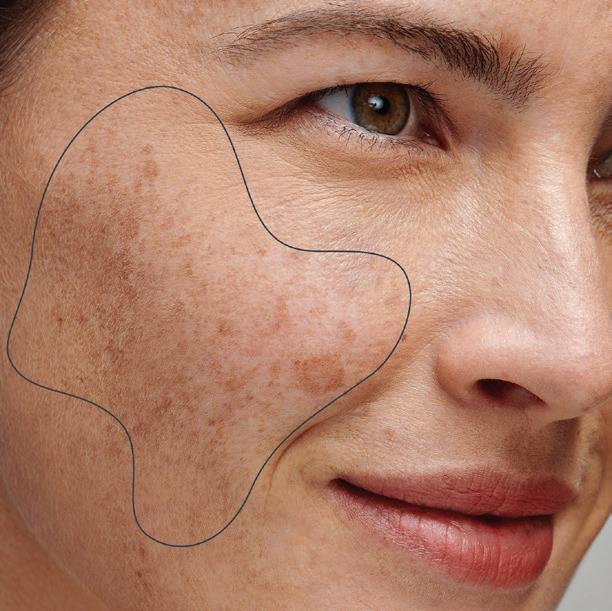
Chemical Peel for Hyperpigmentation Part-I
Dr. Dipak Patel
MD, DVD
Aesthetic Dermatologist & Cosmetologist
Neel Aesthetics
Surat Introduction
Chemical peeling is defined as the application of a chemical agent to the skin, resulting in the controlled destruction of either a portion or the entirety of the epidermis, with or without involvement of the dermis. This procedure induces exfoliation, facilitates the removal of superficial lesions, and promotes the regeneration of new epidermal and dermal tissues. Chemical peeling is routinely performed in an outpatient setting for both aesthetic enhancement and the treatment of various specific dermatological conditions.1
History of chemical peel
The practice of skin exfoliation to improve texture, enhance smoothness, and elevate aesthetic appearance has historical precedent dating back to ancient civilizations. Historical records suggest that Cleopatra utilized sour milk, recognized for its lactic acid content, while women in France historically employed old wine, which contains tartaric acid, to
enhance the appearance of the skin.1
Mechanism
The mechanism underlying chemical peeling involves the replacement of epidermal and partial dermal tissue through several key processes. Regeneration and remodelling occur as the application of chemical agents stimulates a healing response, leading to the formation of new tissue. During this process, elimination of damaged cells and superficial lesions enhances skin clarity and texture. Additionally, controlled destruction of specific skin layers is achieved through the targeted application of chemical agents, facilitating deeper skin rejuvenation. Finally, a regulated inflammatory response is initiated, which plays a critical role in promoting the healing process and subsequent tissue regeneration.1, 2
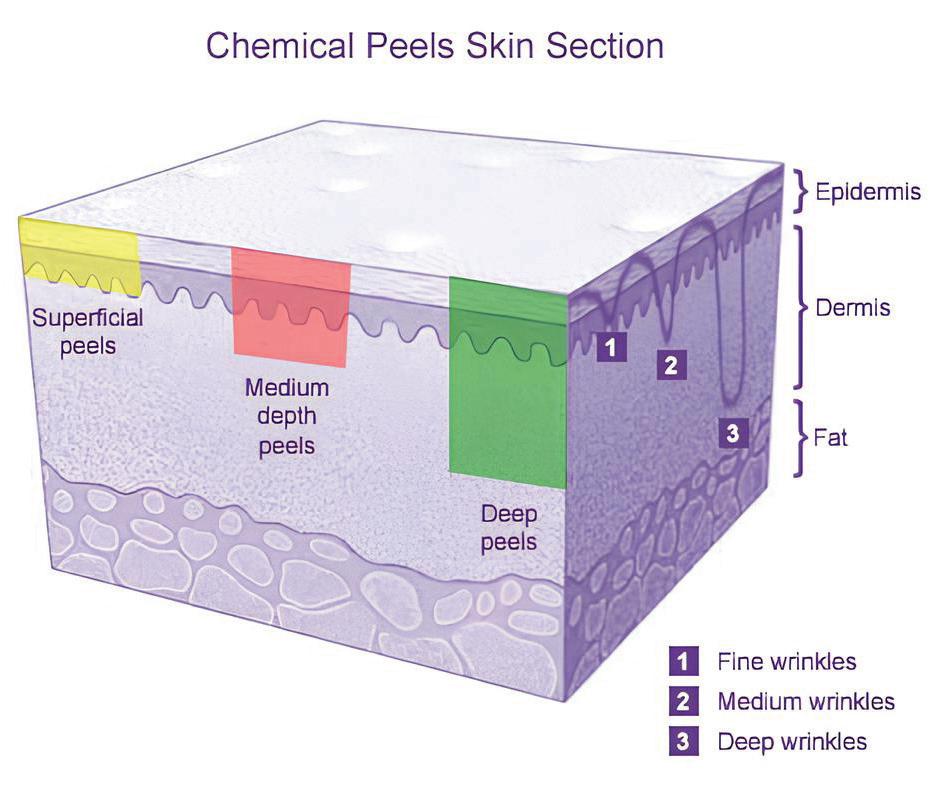
Classification of Peeling : Depth of Injury
Chemical peels are classified based on the depth of tissue injury they induce, which
includes three main categories:1,2
Superficial Peeling (Light Peel) targets the stratum granulosum and the papillary dermis, affecting the outermost layers of the skin.
Medium Depth Peeling (Medium Peel) penetrates the upper reticular dermis, resulting in a more pronounced effect than superficial peels.
Deep Peeling (Deep Peel) which reaches the mid-reticular dermis, causes significant tissue injury and necessitates a longer recovery period.
Indications
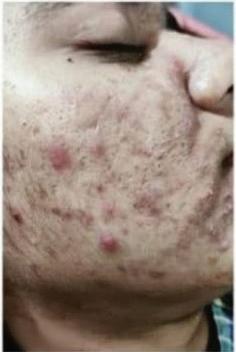
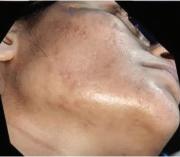
For dermatological treatments targeting pigmentation, melasma, and solar lentigines, varying concentrations of acids are commonly applied. Postinflammatory hyperpigmentation and melasma are treated with salicylic (35%), glycolic (5070%), pyruvic (40-60%), trichloroacetic (15-25%), or Jessner's Solution. Solar lentigo and actinic keratosis may require stronger acids like trichloroacetic (>25%), pyruvic (50-70%), or phenol (6080%). Under-eye pigmentation is managed with azelaic and lower glycolic acid (20%). Rosacea and acne vulgaris involve salicylic (1535%) and pyruvic (40-60%), often with Jessner’s Solution or Unna's Paste for acne. For acne scars and photoaging, deeper treatments use trichloroacetic (25-50%) or phenol (45-88%), with severe cases utilizing glycolic (70%) and trichloroacetic (35%) or phenol (88%).
Contraindications for chemical peel procedures include the presence of unrealistic or noncompliant patients, active infections such as herpes simplex or bacterial infections, and active dermatoses, including rosacea, atopic dermatitis, and psoriasis. Additional contraindications comprise open wounds, the use of photosensitizing medications, known allergies to the components of the peel, as well as pregnancy and lactation. Patients with impaired healing or skin atrophy are also advised against undergoing such treatments due to the increased risk of adverse effects.3
Patient Selection
When selecting the appropriate chemical peel for a patient, it is essential to take a comprehensive history, including any history of recurrent herpes infections, use of photosensitizing drugs, tendencies toward postinflammatory hyperpigmentation, and previous scarring. Counsel the patient on the necessity of serial applications, outlining the expected short-term and longterm results while setting rational expectations for treatment outcomes. Additionally, obtain informed written consent that details the procedure and potential complications, ensuring the patient understands the risks involved. Finally, document the condition through photographic evidence to track progress and outcomes effectively.3
Pre peel care
Medium- and long-term preparation of the skin prior to chemical peeling is crucial for enhancing and achieving uniform penetration of the peel. This preparatory phase stimulates keratinocyte regeneration and accelerates the healing process while reducing the risk of postinflammatory pigmentation. Pre-peel priming of the patient's skin with agents such as sunscreens, hydroquinone, glycolic acid, azelaic acid, arbutin, licorice extract, and tretinoin is recommended for a duration of 2 to 4 weeks. Specifically, glycolic acid at concentrations of 10-15% and tretinoin serve as penetration enhancers; however, these agents should be discontinued 3 to 5 days prior to the procedure to optimize outcomes and minimize adverse effects.3
Equipment
The necessary equipment for performing a chemical peel includes a glass cup or beaker to contain the selected chemical agent, a headband or cap to secure the patient's hair away from the treatment area, and gloves to maintain proper hygiene during the procedure. Additional supplies consist of cotton-tipped applicators or swab sticks for precise application, cotton gauze pieces for absorption, and a fan to provide cooling for the patient during the procedure. A timer is also essential, particularly for monitoring the duration of alpha-hydroxy acid peels to ensure optimal efficacy and safety.3
Procedure
The patient should be positioned supine, with a headband and apron for comfort and protection. Cotton plugs are placed in the ears, and the eyes remain closed during the procedure. The skin is degreased with spirit, acetone, or a pre-peel cleanser for optimal adhesion of the chemical agent. Sensitive areas, such as the angle of the mouth, perinasal region, and inner canthus, are protected with petroleum jelly. The peel is prepared in a bowl or beaker and applied to the treatment area while monitoring for the desired endpoint. Once reached, the peel is neutralized, and postpeel care instructions are reinforced to ensure proper recovery and optimal results.3
Post peel care
During the post-peel period, patients may experience edema, erythema, and desquamation, with duration varying by peel depth: 1 to 3 days for superficial peels and 5 to 10 days for deeper peels. Mild soap or a non-soap cleanser is recommended for cleansing the skin. In cases of crusting, a topical antibacterial ointment should be applied to mitigate the risk of bacterial infection. Cold compresses or calamine lotion may be utilized to soothe the skin. Patients should be advised to use broad-spectrum sunscreens and
Figure 2: Equipment for chemical peel procedure
Chemical Peel for Hyperpigmentation
only bland moisturizers until the peeling process is complete, while avoiding any peeling
References
1. Rendon MI, Berson DS, Cohen JL, Roberts WE, Starker I, Wang B. Evidence and considerations in the application of chemical peels in skin disorders and aesthetic resurfacing. J Clin Aesthet Dermatol. 2010 Jul; 3(7):32-43. PMID: 20725555; PMCID: PMC2921757.
or scratching of the skin. Although analgesics are generally not necessary, they may be recommended to manage any burning sensations experienced during recovery.3
2. Krueger L, Saizan A, Stein JA, Elbuluk N. Dermoscopy of acquired pigmentary disorders: a comprehensive review. Int J Dermatol. 2022 Jan; 61(1):7-19. doi: 10.1111/ijd.15741. Epub 2021 Jul 7. PMID: 34235719.
3. O'Connor AA, Lowe PM, Shumack S, Lim AC. Chemical peels: A review of current practice. Australas J Dermatol. 2018 Aug; 59(3):171-181. doi: 10.1111/ajd.12715. Epub 2017 Oct 24. PMID: 29064096.
Dual-Wavelength Low-Level Laser Therapy Linked to Increased Photosensitivity Risk in Patients with Darker Skin
A recent retrospective cohort study has brought to light a significant clinical concern regarding the safety of dual-wavelength low-level laser therapy in patients with darker skin tones. The investigation encompassed a diverse patient population, stratified by self-reported skin color, and revealed that individuals with higher melanin content are disproportionately susceptible to photosensitivity reactions and thermal burns when subjected to combined red and near-infrared laser irradiation. The data demonstrated a marked increase in both the frequency and severity of adverse events in this group, independent of confounding factors such as age, sex, concurrent medications or total laser energy administered. This heightened risk is mechanistically linked to the photothermal properties of melanin, which absorbs laser energy leading to elevated local tissue temperatures and subsequent injury. These findings underscore the imperative for Dermatologists and laser practitioners to adopt skin pigmentation-aware protocols, emphasizing the need for power modulation or the consideration of single-wavelength devices to mitigate thermal risks in patients with skin of color. Moreover, this study advocates for further research to elucidate the complex interactions between melanin and laser energy, aspiring to optimize therapeutic safety and efficacy across heterogeneous populations. The incorporation of such tailored strategies promises to refine clinical guidelines and enhance the translational application of photobiomodulation therapies in Dermatologic practice.
Isotretinoin Remains the Gold Standard for Severe Acne: Insights on Mechanism, Efficacy, and Management
Isotretinoin is a potent oral retinoid primarily indicated for the management of severe nodular acne that is refractory to conventional therapies, including systemic antibiotics. It exerts therapeutic effects through multifaceted mechanisms impacting the major pathogenic factors in acne. These include marked reduction of sebaceous gland size and sebum production, normalization of follicular keratinization to prevent comedogenesis, and modulation of Cutibacterium acnes colonization within the pilosebaceous unit. In addition to these effects, isotretinoin possesses significant anti-inflammatory properties, reducing the expression of pro-inflammatory cytokines such as IL-8, IL-36 and TWEAK, which contribute to inflammatory lesion formation and progression. The drug influences cellular differentiation, survival, and apoptosis within sebocytes, further contributing to decreased gland activity and inflammation. Due to its teratogenic potential and systemic side effects, isotretinoin therapy is closely monitored under risk management programs to ensure patient safety. Its efficacy in inducing long-term remission or significant improvement has positioned isotretinoin as a cornerstone in acne management, especially for patients with severe, treatment-resistant disease or those at risk for scarring. Ongoing research continues to elucidate the precise molecular and immunomodulatory actions of isotretinoin to optimize therapeutic protocols and minimize adverse effects.
Autologous Biofillers in Aesthetic Dermatology:
From Volume Restoration to Tissue
Regeneration in Scar Management
Dr. Arunima Singh
MBBS, MD (Dermatology, Venereology and Leprosy)
Consultant Dermatologist
Agra, Uttar Pradesh
Dr. Radhika Agarwal
MBBS, DNB, DVL
Consultant Dermatologist
Agra, Uttar Pradesh
Introduction
The evolution of dermal fillers over the past century reflects remarkable progress in both materials and clinical practice. Early fillers such as paraffin and liquid silicone were abandoned due to complications, leading to the introduction of bovine collagen in the 1960s. While collagen offered improved outcomes, its use was limited by immunogenicity and short duration of effect. The 1990s heralded hyaluronic acid (HA) fillers, which remain widely used owing to their superior safety and biocompatibility. The 2000s saw the development of longer-lasting options, including cross-linked HA,
calcium hydroxyapatite, and poly-L-lactic acid, enabling enhanced volumetric correction and durability. The 2010s emphasized minimally invasive and regenerative approaches, notably fat grafting and biostimulatory fillers. In the 2020s, integration of autologous therapies such as PRP and PPP-based biofillers highlights a shift toward patient-specific, regenerative strategies.1
Biofillers, defined as injectable dermal fillers derived from biological sources, specifically the patient’s own blood, have gained significant traction in aesthetic dermatology due to their ability to restore volume,
reduce wrinkles, and rejuvenate the skin. These agents are valued for their safety, natural origin, and capacity to stimulate collagen synthesis. Clinically, biofillers are utilized for a wide range of indications, including tear trough correction, nasolabial folds, marionette lines, as well as the treatment and rejuvenation of acne scars, post-surgical, post traumatic, and other depressed scars. Biofillers serve as dynamic, bioactive matrices that support tissue regeneration. These biologically derived materials are rich in endogenous growth factors, including plateletderived growth factor (PDGF), transforming growth factor-beta (TGF-β), epidermal growth factor (EGF), and vascular endothelial growth factor (VEGF). PDGF significantly contributes to the activation and migration of fibroblasts, processes that are crucial for the synthesis of key structural proteins like collagen and elastin. Meanwhile, TGF-β enhances the production of type I collagen, helping to maintain the skin’s structural integrity and elasticity. EGF enhances keratinocyte proliferation, facilitating epidermal regeneration and improving skin texture, and VEGF induces angiogenesis, ensuring adequate oxygen and nutrient supply to support tissue repair. Together, these growth factors synergistically promote neocollagenesis, angiogenesis, and extracellular matrix remodeling, leading to volume restoration and improved skin quality. Additionally, biofillers serve as scaffolds that support mesenchymal stem cell recruitment, resulting in sustained improvements in
skin firmness and elasticity. In contrast to synthetic fillers, biofillers offer the dual benefits of immediate volumization and biological regeneration.2, 3
Thermally activated PPP gel exemplifies the dual modality of biofillers by offering both immediate volumetric correction and long-term regenerative effects. Beyond soft tissue augmentation, it stimulates mesenchymal stem cell recruitment and type I collagen synthesis, progressively restoring dermal architecture and improving skin texture over time. Biofillers have also demonstrated utility in scar management by preventing refibrosis and supporting dermal remodeling. Their efficacy is further enhanced when combined with subcision or energy-based modalities such as fractional CO₂ laser and microneedling, which synergistically promote epithelial regeneration, reduce post-inflammatory erythema, and improve dyschromia through growth factor receptor modulation and suppression of pro-inflammatory mediators. For facial rejuvenation, the integration of autologous biofillers necessitates continuous evaluation using standardized diagnostic tools. The Wrinkle Assessment Scale and Global Aesthetic Improvement Scale (GAIS) remain fundamental for measuring wrinkle severity and global aesthetic outcomes. In patients undergoing scar rejuvenation, Goodman and Baron’s qualitative and quantitative scar grading systems provide an objective framework for assessing
baseline severity and treatment response. Advanced diagnostic technologies such as highresolution ultrasonography and three-dimensional imaging systems further refine evaluation by enabling precise tracking of soft tissue regeneration, elasticity, and symmetry over time. Regular follow-up appointments are indispensable not only for monitoring the filler’s duration of effect and early detection of adverse events but also for tailoring future interventions according to tissue response and patient expectations. Together, these approaches underscore the evolving role of biofillers as both corrective and regenerative tools in aesthetic dermatology.2,3
Here we present a series of three cases involving patients with atrophic facial scars of varying etiologies, including post-acne and post-traumatic scars, treated with autologous biofillers prepared from the patients’ own blood. The biofillers were administered through intradermal injections to the scarred regions, aiming to provide both immediate volumetric correction and longterm regenerative benefits. All patients demonstrated noticeable improvement in scar depth, skin texture, and overall contour, with no adverse effects reported. This series highlights the potential of biofillers as a safe and effective regenerative option in the aesthetic management of facial scarring.
Preparation and Injection Protocol
Following informed written consent, 10 mL of the patient’s venous blood is collected under aseptic conditions and mixed
with 1 mL of anticoagulant acid citrate dextrose. A twostep centrifugation protocol is implemented to separate the blood components. The first centrifugation is carried out at 3500 revolutions per minute (RPM) for 8 minutes. The resulting plasma layer is carefully aspirated and subjected to a second centrifugation at 1500 RPM for 5 minutes. The upper two-thirds of the supernatant, which consists of plateletpoor plasma (PPP), is carefully aspirated using a tuberculin or 2 mL syringe. The remaining lower third, enriched with platelets and classified as platelet-rich plasma (PRP), is drawn into 1 mL insulin syringes and can be utilized for optional intradermal rejuvenation treatments.4, 5
The process of preparing PPP gel involves transforming the platelet-poor plasma into a functional autologous filler by applying controlled heat, which induces its structural activation. To initiate this process, calcium gluconate is added to the PPP in a ratio of 0.1 mL per 1 mL of plasma, serving as an activator. The PPP-calcium mixture is then incubated in a hot water bath or metal container initially heated between 60°C and 100°C, with the temperature gradually reduced to 98°C over 3 to 5 minutes. This is immediately followed by immersion in a cold water bath, beginning at 7°C and slowly increasing to 10°C over the next 10 minutes. A digital thermometer is consistently employed during the procedure to maintain accurate temperature regulation. This method of thermal cycling facilitates the polymerization and gelation of plasma proteins,
resulting in the formation of a viscous, plasma gel that is suitable for soft tissue augmentation.4, 5
Prior to injection, a topical anesthetic cream containing 2.5% lidocaine and 2.5% prilocaine is applied to the target treatment areas and left in place for approximately 45 minutes, if required, to enhance patient comfort. After removal of the anesthetic, in cases where skin rejuvenation is desired, the previously isolated PRP can be injected intradermally at multiple sites across the forehead, cheeks, and chin using 1 mL insulin syringes. The activated PPP gel is injected into the deep dermal layer using a tuberculin syringe fitted with either a 25-gauge or 27-gauge sharp needle, or alternatively, a blunt-tip microcannula measuring 50 mm or 38 mm in length, depending on the treatment area and specific clinical considerations. All injections are performed with careful consideration of vascular anatomy to avoid inadvertent vascular injury. After the injection, the treated region is softly massaged to promote uniform gel dispersion and achieve a seamless contour.4, 5
Post-Treatment Care and Follow-Up
Post-procedural care includes advising patients to avoid massaging or applying pressure to the treated areas for at least one week. Engaging in intense exercise or vigorous physical exertion is discouraged for a period of 24 to 48 hours. The application of makeup and topical skincare products should be withheld for the first 24 hours, and sun exposure should be minimized with the use of appropriate sunscreen if necessary. Cold compresses may be applied intermittently to reduce swelling or bruising. Follow-up appointments are scheduled to assess the aesthetic outcomes and identify any possible adverse effects.4, 5
Clinical outcomes have demonstrated favorable patient satisfaction, particularly in cases involving post acne scars and post traumatic scars. The Global Aesthetic Improvement Scale (GAIS) has been applied to systematically evaluate and verify improvements in visual appearance. While volumetric effects gradually reduce over a twomonth period, the stability of outcomes tends to be greater in structural correction cases as compared to treatments for atrophic scars.4, 5
Figure 1: Biofiller injection
Clinical outcome
Patient 1
Discussion
The approach to soft tissue augmentation in dermatologic and aesthetic practice is increasingly evolving from static volume replacement to dynamic tissue regeneration. Biofillers, derived from plasma components, represent a novel and biologically active category of dermal fillers that extend beyond conventional volume correction. Unlike traditional synthetic fillers, which primarily serve as passive space-occupying agents, biofillers possess intrinsic regenerative properties due to their rich composition of endogenous growth mediators and their ability to form a supportive, fibrin-based matrix within the dermal and subdermal layers.2, 5, 6
In response to the limitations of conventional fillers, biofillers have emerged as regenerative, patient-specific alternatives that offer superior biocompatibility and eliminate the risk of hypersensitivity reactions. These biofillers are produced through controlled heating of platelet-poor plasma, inducing polymerization and gelation of plasma proteins to form a cohesive, viscoelastic matrix with both structural integrity and biological functionality. Upon injection, the biofiller serves not only as a volumetric scaffold but also as a reservoir for the sustained release of bioactive cytokines and chemotactic factors. This bioactivity promotes fibroblast chemotaxis and proliferation, enhances dermal fibroplasia, and stimulates neocollagenesis and elastogenesis, thereby improving dermal density and tensile strength. Furthermore, the angiogenic effects contribute to enhanced microcirculation and tissue oxygenation, which are essential for long-term dermal regeneration and restoration of cutaneous vitality.2, 5, 6
The viscoelastic properties of biofillers enable precise placement within both superficial and deep dermal layers, supporting a wide range of aesthetic applications such as midface contouring, periorbital hollow correction, and fine wrinkle filling. While meticulous injection technique and thorough knowledge of facial anatomy are essential to minimize complications, most adverse effects are mild, transient, and typically include erythema, edema, or
Patient 2
Patient 3
tenderness at the injection site. These biofillers support tissue regeneration by progressively releasing natural growth factors at the injection site, thereby stimulating ongoing collagen production and longterm dermal restructuring. The growing integration of biofillers into aesthetic practice signifies a pivotal shift toward regenerative and personalized dermatologic therapies. In addition to enhancing appearance, biofillers have shown significant therapeutic value in areas such as tissue reconstruction, scar
References
1. Amiri R, Khalili M, Iranmanesh B, Ahramiyanpour N, Karvar M, Aflatoonian M. The innovative application of autologous biofillers in aesthetic dermatology. Ital J Dermatol Venerol. 2023; 158(4):321-327. doi:10.23736/S2784-8671.23.07485-6.
2. Gupta S, Borde Bisht P, Kannan C. BioFiller: An Effective Facial Rejuvenation Tool-Easy on Pocket. J Cutan Aesthet Surg. 2020; 13(3):243-246. doi:10.4103/ JCAS.JCAS_172_19
3. Bhatt M, Jamale V, Kale M, Hussain AA, Nikam BP. Monotherapy of Biofiller for Atrophic Acne Scars: A Prospective
remodeling, and the treatment of chronic wounds, positioning them as multifunctional agents in holistic clinical practice. This lowrisk, minimally invasive procedure is generally well accepted by patients, requires little recovery time, and provides a natural and biocompatible substitute for synthetic fillers making it an attractive choice for those seeking reliable and biologically driven treatment options for tissue regeneration.2, 5, 6
Conclusion
Biofillers are emerging as a valuable biologic option in aesthetic and regenerative dermatology, offering volumizing effects along with stimulation of collagen synthesis and tissue regeneration. Their biocompatibility, safety profile and ability to promote natural tissue remodeling make them a viable alternative to synthetic fillers. As interest in personalized and minimally invasive treatments grows, biofillers hold significant promise for both cosmetic and therapeutic applications, although further research is needed to standardize protocols and confirm long-term outcomes.
4. Nethaji B, Bhardwaj S, Deora MS, Vaishampayan S, Patra A, Sharma M, et al. The efficacy, safety, and application of platelet-poor plasma gel as an autologous dermal filler for esthetic enhancements and facial rejuvenation – A pilot study. CosmoDerma. 2025; 5:42. doi: 10.25259/ CSDM_221_2024.
5. Cheng H, Li J, Zhao Y, Xia X, Li Y. In Vivo Assessment of Plasma Gel: Regenerative Potential and Limitations as a Filler. J
6. Dashore, Shuken. Understanding the Structure and Function of Platelet-Poor Plasma Biofiller, an Electron Microscopic and Fourier Transform Infrared Spectroscopy (FTIR)-Based Analysis. Indian Dermatology Online Journal 15(3): p 534-536, May–Jun 2024. | DOI: 10.4103/idoj.idoj_376_23.
Obstructive Sleep Apnea and Skin Conditions: Emerging Associations and Clinical Considerations
Dermatological conditions such as atopic dermatitis and impaired wound healing have been increasingly linked to obstructive sleep apnea (OSA), a disorder defined by repetitive upper airway obstruction during sleep causing intermittent hypoxia and systemic inflammation. Studies indicate that patients with newly diagnosed OSA are at increased risk of developing atopic dermatitis, with this risk being more pronounced in male and younger populations, implicating age and sex as key factors in susceptibility. OSA impact on wound healing is also notable, with delayed recovery observed in both surgical and chronic wounds, attributed to oxidative stress, endothelial dysfunction and persistent systemic inflammation. Additionally, the continuous positive airway pressure (CPAP) therapy frequently prescribed for OSA can lead to skin complications such as dermatitis due to friction, pressure, moisture, or material sensitivities, especially when masks are poorly fitted. While further research is needed to establish definitive causality, these findings emphasize the importance of recognizing skin manifestations in patients with OSA, advocating for integrated care approaches involving both dermatologists and sleep medicine specialists to address the complex interaction between respiratory and dermatologic health.
Breakthrough IL-2 Pathway Agonist Shows Promising Advances in Treating Moderate to Severe Atopic Dermatitis
A novel IL-2 pathway agonist that selectively expands regulatory T cells offers a promising new approach for the treatment of moderate to severe atopic dermatitis by addressing the underlying immune dysregulation central to the disease's pathophysiology. Atopic dermatitis involves an imbalance in immune signaling, characterized by overactivation of Th2 cells and elevated levels of cytokines such as IL-4, IL-13 and IL31, which contribute to skin barrier dysfunction, inflammation and pruritus. This IL-2 agonist works by stimulating regulatory T cells, which play a critical role in maintaining immune tolerance and modulating excessive inflammation. Clinical benefits include marked reductions in skin lesions, itch intensity and extent of affected skin, alongside improvements in sleep quality and pain control, which collectively enhance patients' quality of life. The treatment supports long-term disease control by restoring immune homeostasis rather than merely suppressing inflammatory pathways. It has demonstrated a favorable safety profile, with mostly mild and manageable adverse effects reported. This therapeutic strategy represents a significant advancement by targeting the root cause of immune dysregulation, providing hope for more durable and effective management of inflammatory skin conditions refractory to conventional therapies.