22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: info@residerm.com
TEL: + 91 22 2345 1404
Printed, Published, Edited and Owned by Dom Daniel Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“Residerm ” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of March 2026
SHAPING COMPETENT RESIDENTS: LEARNING, REFLECTION AND HOLISTIC CARE
Beginning residency in dermatology is both exhilarating and demanding. The breadth of clinical presentations, evolving therapeutic modalities, and growing aesthetic landscape can feel challenging at first. With this in mind, RESIDERM is committed to creating a supportive academic platform that nurtures curiosity, sharpens clinical reasoning, and builds confidence among young dermatologists. Our aim is not only to simplify complex concepts but also to cultivate thoughtful clinicians who positively influence their institutions and the larger healthcare community.
In this issue, we present thought-provoking contributions from experienced faculty members whose perspectives are rooted in years of academic and clinical excellence. Their guidance is intended to strengthen foundational knowledge while encouraging reflective practice.
This issue features insightful case discussions addressing both the psychosocial and therapeutic aspects of pigmentary disorders. Impact of Quality of Life in Patients with Facial Melanosis at a Tertiary Care Center highlights the significant emotional and social burden of facial hyperpigmentation. Meanwhile, Successful Treatment of Recalcitrant Facial Melasma Using Combined Tranexamic Acid, Hydroquinone, Q-Switched Nd:YAG Laser, and Glycolic Acid Peel demonstrates an effective multimodal strategy for resistant melasma, emphasizing individualized, evidence-based management.
These articles underscore the multifaceted nature of pigmentary disorders. We hope this edition inspires your learning journey and encourage you to contribute your research and clinical experiences to future issues.
We look forward to your contributions for the next edition.
Hope you have a great read!
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher
Impact of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
Dr. Ruttoo Polra
Senior Resident (2024)
Department of Dermatology, NAMO Medical College, Ahmedabad
Dr. Dhruv Patel
MBBS, MD (Skin &VD)
Consultant Dermatologist, Gandhinagar
Dr. Jinal Tandel
MBBS, MD
Consultant Dermatologist, Valsad
Dr. Dharmesh Parmar
MBBS, MD
Class I Officer, General Hospital Siddhpur, Gujarat
Ms. Jaishree Ganjiwale
Assistant Professor (Bio-statistician)
Department of Community Medicine
Pramukhswami Medical College, Shree Krishna Hospital
Bhaikaka University, Karamsad, Gujarat
Dr. Pragya A Nair
MD (Dermatology)
Professor
Department of Dermatology
Pramukhswami Medical College, Shree Krishna Hospital
Bhaikaka University, Karamsad, Gujarat
Herpes Zoster in Adolescence: Clinical Presentation, Diagnostic Approach and Therapeutic Management — A Case-Based Review
Dr. Atul Singhania
MBBS, DVD
Skin Specialist, Venereologist , Leprologist, and Cosmetologist
Shreekrupa Skin and Hair Care Clinic
Akola, Maharashtra
Impact of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
Impact of Quality of Life in Patients with Facial
Melanosis at Tertiary Care Center
Dr. Ruttoo Polra
Senior Resident
Department of Dermatology
NAMO Medical College
Ahmedabad
Dr. Dhruv Patel
MBBS, MD (Skin &VD)
Consultant Dermatologist
Gandhinagar
Dr. Jinal Tandel
MBBS, MD
Consultant Dermatologist
Valsad
Dr. Dharmesh Parmar
MBBS, MD
Class I Officer, General Hospital
Siddhpur, Gujarat
Ms. Jaishree Ganjiwale
Assistant Professor (Bio-statistician)
Department of Community Medicine
Pramukhswami Medical College, Shree Krishna Hospital
Bhaikaka University, Karamsad, Gujarat
Dr. Pragya A Nair
MD (Dermatology)
Professor
Department of Dermatology
Pramukhswami Medical College, Shree Krishna Hospital
Bhaikaka University, Karamsad, Gujarat
Abstract
Introduction: The measurement of the impact of skin diseases on patient’s quality of life is important as virtually all aspects of patient’s lives can be affected by skin disease. Pigmentary disorders over face are associated with significant social, psychological and cosmetic challenges because of their visibility on exposed areas of the body and the stigma associated.
Aim: To study the pattern of facial pigmentary disorders and their impact
on quality of life.
Material & methods:
The study was carried out during August 2019 to July 2020 in the department of dermatology. Patients of either sex, more than 12 years of age and with any type of facial pigmentation (hyper & hypopigmentation) were included in the study and were given the DLQI questionnaire to measure the impact of these facial melanoses on the quality of their lives. The sum of these scores is then calculated as the total DLQI score. The descriptive statistics has been used to describe the categorical data. Quality of life was presented by mean (SD) QOL.
Result: Total 161 patients with facial melanosis were evaluated of which 103 (63.98%) were females and maximum 98 (60.87%) were in 19-40 years of age group. Melasma was the most common condition with 70 (43.5%) cases followed by postinflammatory pigmentation with 15 (9.3%) cases. Maximum 80 (49.68%) patients are categorised as a small affected DLQI group. Out of total 10 questions, question 2 (How embarrassed or selfconscious have you been because of your skin?) had
Impact of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
maximum mean score of 1.02.
Conclusion: DLQI is an assessment tool that can be used to measure the physical, psychological and social burden of dermatological disorder and can be an important tool to assess the response to various therapeutic modalities.
Limitations
Correlation of DLQI with duration of disease or severity of disease was not assessed.
Key words- DLQI, facial melanosis, melasma, PIP, POP
Introduction
The measurement of the impact of skin diseases on patient’s quality of life (QOL) is important for clinical, therapeutic and health service research, political purposes and to inform clinical decisions. Various measurement techniques include general health, disease specific and dermatology specific questionnaires. The Dermatology Life Quality Index (DLQI) is a simple, practical, and selfadministered questionnaire, which assess the impact of skin disease on quality of life.[1]
In a study of 2000 patients, pigmentary disorders were the third most common skin disorder with post inflammatory pigmentation as most frequent followed by melasma.[2]
Facial melanoses includes conditions like Melasma, Riehl’s melanosis, lichen planus pigmentosus, Postinflammatory ......... pigmentation (PIP), Periorbital pigmentation (POP), Erythromelanosis peribuccale pigmentaire of Brocq (EPP), Poikiloderma of Civatte, Erythromelanosis follicularis and Nevus of Ota. Treatment of facial melanoses is not only challenging but requires therapy to maintain remission.
Pigmentary disorders over face are associated with significant social, psychological and cosmetic challenges because of their visibility on exposed areas of the body and the stigma associated with it.[3] In India, 20–30% of 40–65 years old women present with facial melasma, and 70% of patients with history of acne develop postinflammatory pigmentation before 35 years of age.[4] The overall prevalence of periorbital pigmentation in Indian women is 50% which
Impact of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
increases with age, thus pigmentary disorders are a major concern in India and has a great psychosocial impact on quality of life. [5] As disease’s impact on quality of life provide a good measure of health status and there are very few studies that too of individual disease,[6,7] we took the study to find the pattern of facial pigmentary disorders and their impact on quality of life.
Material & methods
Present study was carried out during August 2019 to July 2020 in the department of dermatology, venereology and leprosy at a tertiary care centre, after approval from institutional ethic committee. Patients of either sex, more than 16 years of age and with hyper or hypopigmentation were included in the study. Patients with pigmentation over other parts of body or having any other chronic diseases were excluded from the study. Demographic details were collected in a proforma. Cutaneous examination was done. Diagnosis was made, on the basis of history, clinical examination or dermoscopy if required.
Participants were given the DLQI questionnaire to measure the impact of
facial melanoses on the quality of their lives. It is a health quality of life scale comprised of 10 items which focus on 6 dimensions: “symptoms,” “daily activities,” “leisure,” “work,” “personal relationships,” and “treatment.” The scoring of each question is as follows: Very much scored 3, A lot scored 2, A little scored 1, Not at all scored 0, Not relevant scored 0 covering the last one week of the patient’s life. The total score is calculated by adding the score of each question and ranges from a minimum of “0” to a maximum of “30,” with higher scores representing greater impairment of quality of life.[1] The interpretation of the DLQI score was done as: 0–1=No effect on patient’s life, 2–5 = Small effect, 6–10 = Moderate effect, 11–20 = Very large effect, 21–30 = Extremely large effect.
DLQI is designed for use in adults, i.e over the age of 16. It is self-explanatory and can be simply handed to the patient who is asked to fill it in without the need for detailed explanation and is completed in one or two minutes.
Questionnaire was translated in vernacular language and it was
validated before the start of study.
The descriptive statistics has been used to describe the categorical data. Age group wise and gender wise frequency and percentage were calculated for the related exposures found. Quality of life of the facial melanosis patients were presented by mean (SD) QOL.
Results
Total 161 patients with facial melanosis were evaluated of which 103 (63.98%) were females and maximum 98 (60.87%) were in 1940 years of age group followed by 41-60 years of age group, consisting of 55 patients (34.16%). Mean SD (DLQI) in males was 3.21 while in females it was 5.50. Maximum 80 (49.68%) patients are categorised as a small affected DLQI group followed by 51 (31.68%) patients as a moderate affected DLQI group. Among 19-40 years of age group 46 had small effect and 34 had moderate affected DLQI. Twenty-two patients (13.66%) were not affected, while a small portion of study group, comprised of 8 patients (4.96%) were very largely affected in 19-40 years of age group. [Table:1]
Impact of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
Table 1: Gender and age wise DLQI Score distribution and comparison
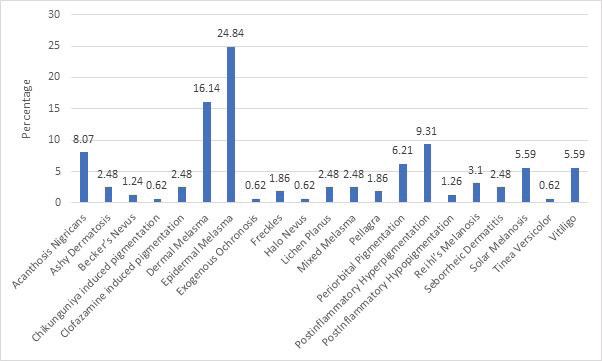
Epidermal melasma was the most common facial melanosis with 40 (24.84%) cases followed by dermal melasma 26 (16.14%), PIP 15 (9.31%), acanthosis nigricans 13 (8.07%) and POP with 10(6.21%) cases. [Figure-1]
Figure 1: Distribution of various facial melanosis
Impact of Quality of Life in Patients with Facial
at Tertiary Care Center
PIP had mean score of 7.07 ± 2.8 with 11 cases having moderate effect on DLQI followed by epidermal melasma having mean score of 5 ± 3.5 with 15 cases who had moderate effect on DLQI and dermal melasma with 4.69 ± 4.4mean score. [Table -2]
Table 2: DLQI in common facial dermatosis
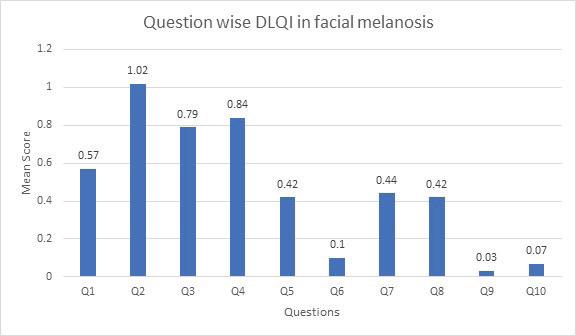
Out of total 10 questions, question 2 had maximum mean score of 1.02 followed by question 4 and 3 respectively with mean score of 0.84 and 0.79, while question 9 had minimum mean score of 0.03. [Figure-2]
Figure 2: Question wise DLQI in common facial melanosis
Impact of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
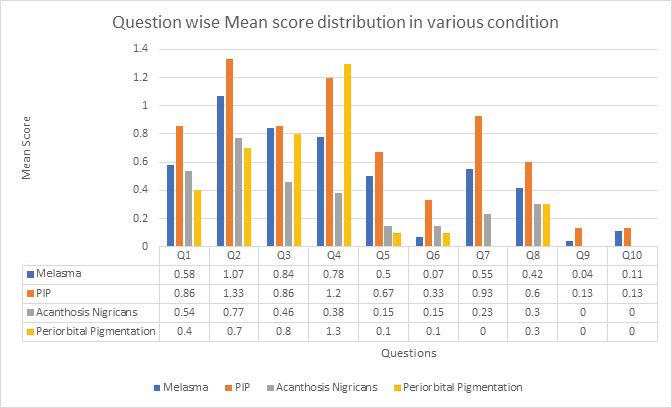
In patients diagnosed with Melasma, Q2, (How embarrassed or self-conscious have you been because of your skin?) had maximum score with mean score of 1.07 while Q9, (How much has your skin caused any sexual difficulties?) had minimum score with mean score of 0.04. In PIP and Acanthosis Nigricans, Q2 had maximum score with mean score of 1.33 and 0.77 respectively and Q9 and Q10 (How much of a problem has the treatment for your skin been, for example by making your home messy, or by taking up time?) had minimum score with mean score of 0.13 and 0 respectively. [Figure-3]
Discussion
In present study of 161 patients, 43.5% had melasma, 9.3% had PIP followed by 8.04% of acanthosis nigricans. Halo nevus, tinea versicolor, ochronosis and chikunguniya induced pigmentation was seen in 0.62% cases, as we included both hypo and hyperpigmentory conditions in our study. In study by Amatya B et al also most
common facial melanosis was melasma with 43% patients followed by acne induced hyperpigmentation with 18%, while conditions least commonly observed were Hori’s naevus, verrucous epidermal naevus, ochronosis andperibuccal pigmentation of Brocq.[8]
Females were more with 63.9% like in study by Amatya B et al where
78.56% females were affected. Maximum patients (60.87%) were in 19-40 years of age group similar to study by Amatya B et al where (71.3%) belonged to the age group 16–35 years.[8] The mean age of the participants was 32.7 ± 12.3 years with a range of 67 years (16–83 years).
Mean SD (DLQI) in males was 3.21 while it was 5.50 in females. Maximum 49.68%
Figure 3: Question wise mean score distribution in various facial melanosis
Impact of Quality of Life in Patients with Facial Melanosis
at Tertiary Care Center
patients were categorised as a small affected DLQI group of which 46 patients were in 19-40 years of age group followed by 31.68% patients as a moderate affected DLQI group of which 34 are in same age group. Total 13.66% were not affected, while a small portion of study group, 4.96% were very largely affected in 1940 years of age group.
A healthy face plays important role in selfconfidence particularly during adolescent age group, thus in our study quality of life was affected more commonly in that age group. We could not find any study which showed association of age group and effect of DLQI in facial melanosis.
The skin diseases have an impact on QOL of the patient owing to their high visibility. Patients with skin conditions on the face are at risk of having depression and can suffer from feelings of loneliness and isolation.[6]
Patients with pigmentary disorders are more affected by depression than patients with acne, acne scars, and rosacea.[7]
Facial melanoses includes many overlapping clinical conditions, thus patients experience
severe consequences on self-concept. Various studies done individually regarding quality of life in pigmentary disorders such as melasma, vitiligo, lentigo, post inflammatory hyperpigmentation, ......... and idiopathic guttate hypomelanosis have shown a significant negative impact on a person’s health-related quality of life.[9]
Mean DLQI score was maximum (7.07±2.8) in PIP followed by mixed and epidermal melasma with 7±0.8 and 5±3.5 respectively. In Raveendra et al study, QOL in facial melanosis was done by using Skindex-16 score. Skindex-16 score contain 16 question related to patient’s symptoms, social and emotional status. Mean Skindex-16 score was 23.25 ± 19.10.[10] Skindex cores of pigmentation due to melasma was less than conditions like acanthosis nigricans, Nevus of Ota, PIH and post-Chikangunya pigmentation.
In Taylor et al study of patients with diagnosed pigmentary disorders, using quality of life assessment questionnaire, majority (53%) patients were not at all bothered by the skin’s appearance, 47.3% felt self-conscious about
their skin to some degree, 21.8% felt others focused on their skin, 32.7% felt unattractive because of their skin, 32.7% put effort into hiding pigmentary changes, and 23.6% felt their skin affected their activities.[11] In our study maximum patients felt embarrassed and selfconscious about their skin with mean score of 1.02, followed by 0.79 where patients felt that their skin has affected their outdoor activities like shopping and social activities.
An analysis based on individual questions revealed that the second question recorded the highest mean score (1.96 ± 0.78) while the ninth recorded the lowest (0.05 ± 0.22)in study by Amatya B et al [8] while in our study also second question had mean score of 1.02 while 9th question has lowest mean of 0.03 .Question 2 had maximum mean score of 1.07and 1.33 in melasma and PIP, in comparison to other conditions like AN and POP where mean score was 0.7.Questions related with symptoms and any problem with partners or any sexual difficulties were not much affected in our study with 0.57, 0.42 and 0.03 mean scores respectively. The explanation behind it is possibility of questions
related with leisure activity and sexual difficulties may not be suitable for Indian population particularly living in rural areas.
In another study of healthrelated quality of life in patients with primary cutaneous amyloidosis, cosmetic disfigurement and severe pruritus dramatically affected patient’s quality of life which led to psychosocial stress and the impairment of emotional functioning.[12] Strong impact of primary cutaneous amyloidosis was seen on patients’ quality of life both for dermatologyspecific (using the DLQI) and for general health perceptions (using the SF36).
Most of the facial dermatosis has gradual progression without spontaneous improvement. Treatment options are limited and often not effective, which may have contribute to the higher impairment on quality of life. It is possible that with long duration of pigmentation, the effect on quality of life is more.
Several studies have focused on specific pigmentary disorders like melasma, vitiligo and their psychosocial and cosmetic
Impact
of Quality of Life in Patients with Facial Melanosis at Tertiary Care Center
challenges,[8] because of their visibility on exposed areas of the body and because of the stigma associated with pigmentary alteration in Nepal and the Indian subcontinent.[13,14 ]
Facial melanoses decreases the QOL but the extent and severity of facial pigmentation and the decrease in the QOL does not appear to be proportional. In the study by Balakrishnan et al. they found that the extent or the type of facial blemish did not influence the HRQOL but the mere presence of the facial blemish reduced the HRQOL.[1] We could not do the correlation between severity of facial melanosis with QOL.
Conclusion
Study of quality of life can be used in the evaluation of patients presenting with facial pigmentation as it is an important tool to assess the response to various therapeutic modalities, thus planning and allocating resources for the prevention and management can be planned.
Limitations
Correlation of DLQI with duration of disease or severity of disease was not assessed.
References
1. Finlay A, Khan G. Dermatology life quality index [DLQI]: a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–216.
2. Halder RM, Grimes PE, McLaurin CI, Kress MA, Kenney JA Jr. Incidence of common dermatoses in a predominantly black dermatologic practice. Cutis 1983;32:388-90.
3. Akay A, Pekcanlar A, Bozdag KE, Altintas L, Karaman A. Assessment of depression in subjects with psoriasis vulgaris and lichen planus. J Eur Acad Dermatol Venereol 2002;16:34752.
4. Hourblin V, Nouveau S, Roy N, de Lacharrière O. Skin complexion and pigmentary disorders in facial skin of 1204 women in 4 Indian cities. Indian J Dermatol Venereol Leprol. 2014;80:395–401.
5. Shenoi SD, Prabhu S. Role of cultural factors in the biopsychosocial model of psychosomatic skin diseases: An Indian perspective. Clin Dermatol 2013;31:62 5
6. Balakrishnan R, McMichael AJ, Hu JY, Camacho FT, Shew KR, Bouloc A, et al. Correlates of health-related quality of life in women with severe facial blemishes. Int J Dermatol 2006;45:111-5.
7. Seite S, Deshayes P, Dréno B, Misery L, Reygagne P, Saiag P, et al. Interest of corrective makeup
Impact of Quality of Life in Patients with Facial Melanosis
at Tertiary Care Center
in the management of patients in dermatology. Clin Cosmet Investig Dermatol 2012;5:123-8.
8. Amatya B , Jha AK and Shrestha SFrequency of different types of facial melanoses referring to the Department of Dermatology and Venereology, Nepal Medical College and Teaching Hospital in 2019, and assessment of their effect on health-related quality of life. BMC Dermatology (2020) 20:4
9. Amatya B, Pokhrel DB. Assessment and comparison of quality of life in patients with melasma and vitiligo. Kathmandu Univ Med J. 2019;66:114–118.
10. Raveendra L, Sidappa H, Shree S. A study of quality of life in patients with facial melanoses. Indian Dermatol Online J 2020;11:154-7
11. Taylor A, Pawaskar M, Taylor SL, Balkrishnan R, Feldman SR. Prevalence of pigmentary disorders and their impact on quality of life: a prospective cohort study. J Cosmet Dermatol. 2000;7:164-168.
12. Fang S, Shen X, Chen AJ, Li S, Shan K. Health related quality of life in patient with primary cutaneous amyloidosis. PLoS One. 2015; 10: e0120623.
13. Parsad D, Dogra S, Kanwar AJ. Quality of life in patients with vitiligo. Health Qual Life Outcomes. 2003;1:58.
Dermatology life quality index score in vitiligo and its impact on the treatment outcome. Br J Dermatol. 2003;148:373–4.
Herpes Zoster in Adolescence:
Clinical Presentation, Diagnostic Approach and Therapeutic Management — A Case-Based Review
Dr. Atul Singhania
MBBS, DVD
Skin Specialist, Venereologist, Leprologist and Cosmetologist
Shreekrupa Skin and Hair Care Clinic
Akola, Maharashtra Introduction
Herpes Zoster occurs throughout the year without any seasonal variation. Herpes zoster, commonly known as shingles, is a viral infection caused by reactivation of the varicellazoster virus (VZV), which remains dormant in the sensory dorsal root ganglia after a primary varicella infection or vaccination. Reactivation results in a painful, unilateral vesicular eruption confined to a single dermatome. The disease typically progresses through three phases. The preeruptive phase is marked by prodromal symptoms such as localized pain, burning, or abnormal skin sensations in the
affected dermatome, often accompanied by headache, malaise, and photophobia. These symptoms usually precede the rash by 48–72 hours. The acute eruptive phase begins with erythematous papules that rapidly evolve into clusters of fluid-filled vesicles on an inflamed base. Few patients may have acute segmental pain without ever developing skin eruptions (Zoster Sine herpte). The vesicles may rupture, ulcerate, and crust over, and patients remain contagious until complete crusting occurs. Pain during this stage can be severe and may persist for 2–4 weeks. The chronic phase is characterized by postherpetic neuralgia
(PHN), defined as persistent neuropathic pain lasting beyond four weeks after rash onset. PHN may present with paresthesias, dysesthesias, and shocklike sensations and can persist for months or longer. A hallmark of herpes zoster is the synchronous evolution of lesions from macules to vesicles and crusts. The rash most commonly affects the thoracic region or face and may leave postinflammatory pigmentation. Complications include Ramsay Hunt syndrome due to facial nerve involvement, herpes zoster ophthalmicus indicated by Hutchinson’s sign, and delayed cerebral arteritis, which may increase stroke risk.1
Herpes zoster, or shingles, originates from reactivation of the varicella-zoster virus (VZV) following a primary varicella (chickenpox) infection. During the initial infection, VZV enters through the respiratory mucosa or conjunctiva, spreads hematogenously, and produces the characteristic generalized vesicular rash. After recovery, the virus establishes lifelong latency within the sensory dorsal root and cranial nerve ganglia, particularly in the thoracic, lumbar, and cervical regions, where
it persists in a dormant, non-replicative state within neurons. Reactivation occurs when cell-mediated immunity declines, especially VZV-specific memory T-cell responses. This reduction may result from aging, psychological stress, immunosuppressive medications, HIV infection, malignancy, organ transplantation, or chronic systemic diseases such as diabetes. When immune surveillance weakens, the latent virus resumes replication within the affected ganglion. Newly formed virions travel centrifugally along sensory nerve fibers to the skin of the corresponding dermatome. Viral replication within nerves and ganglia causes inflammation and neuronal damage, producing prodromal pain, burning, or numbness that may precede visible skin changes. As the virus reaches the dermis and epidermis, localized inflammation gives rise to erythematous maculopapular lesions that rapidly evolve into clusters of fluid-filled vesicles containing infectious viral particles. These vesicles may rupture and subsequently crust over, marking the late stage of infection and a reduction in contagiousness. This sequence of neural and cutaneous events
underlies the characteristic dermatomal rash and neuropathic pain seen in herpes zoster.2
Approximately 95% of adults are seropositive for VZV, indicating a substantial risk of herpes zoster. Complications of herpes zoster include post-herpetic neuralgia, which is associated with neuronal sensitization and deafferentiation. Involvement of thoracic, lumbar, cervical, and occasionally sacral dermatomes is typical, while extensive disease can affect the lungs, central nervous system, mucous membranes, liver, cardiovascular system, bladder, skeletal system, blood vessels, and gastrointestinal tract, with severe complications such as disseminated disease potentially leading to fatal outcomes. The progression of this infection through its distinct phases and its potential to affect various organ systems underscore the importance of effective management and prevention strategies, particularly in vulnerable populations.2
Case Report
A 13-year-old male presented with complaints of severe pain, burning sensation, and itching over the right side of the abdomen Herpes Zoster
Herpes Zoster in Adolescence:
for 4 days. Dermatological examination revealed grouped erythematous papules and vesicles distributed unilaterally along the T9–T10 dermatomes on the right abdominal wall. The lesions were clustered, did not cross the midline, and were consistent with a dermatomal pattern. Based on clinical findings, a diagnosis of herpes zoster was confirmed. The patient was started on oral acyclovir 400 mg four times daily for 5 days. Supportive therapy included amoxicillin with potassium clavulanate for 7 days to prevent secondary bacterial infection, tramadol with paracetamol for pain control, ranitidine for gastric protection, and amitriptyline 10 mg at bedtime for neuropathic pain. A multivitamin and multimineral syrup was prescribed as an adjunct. Topical management consisted of calamine and aloe vera gel lotion to soothe the lesions. Baseline investigations, including hemoglobin, total and differential leukocyte counts, SGPT, serum creatinine, and urine routine and microscopy, were advised. Follow-up after 2 weeks, the patient reported complete resolution of pain and skin lesions, with only mild residual post-inflammatory changes. No complications or adverse drug reactions were noted. The overall outcome was favorable, indicating effective early intervention and good immune recovery.
Before treatment
After treatment
Figure 1: Complete resolution of herpes zoster lesions with mild residual post-inflammatory changes
Diagnosis
Diagnostic evaluation of herpes zoster includes several laboratory techniques that confirm the presence of varicella-zoster virus (VZV), especially in atypical or
complicated presentations. Viral culture is a traditional gold standard method in which vesicular fluid is inoculated onto cell cultures such as human fibroblasts. When VZV is present, characteristic cytopathic effects including cell rounding, syncytia formation, and cell destruction are observed. This method is highly specific and helps differentiate VZV from other herpesviruses such as herpes simplex virus.3 Polymerase chain reaction (PCR) is currently the most sensitive and specific technique for detecting VZV DNA. It involves extraction and amplification of viral DNA using VZV-specific primers. A positive result confirms infection, while quantitative PCR (qPCR) allows measurement of viral load and helps assess disease severity.4 Quantitative PCR is particularly valuable in atypical herpes zoster and can be performed on vesicular fluid, crusts, blood, or cerebrospinal fluid (CSF).5 Serological testing assesses the immune response by detecting VZV-specific IgM and IgG antibodies. IgM positivity indicates recent infection or reactivation, whereas IgG reflects prior
Herpes Zoster in Adolescence:
exposure. These antibodies are typically measured using ELISA or indirect immunofluorescence......... assays.3 A Tzanck smear is a rapid diagnostic method in which cells scraped from a vesicle are microscopically examined for multinucleated giant cells and intranuclear inclusions. Electron microscopy can directly visualize viral particles, providing confirmatory evidence. Direct immunofluorescence assay (DFA) detects VZV antigens in lesion samples using fluorescent antibodies, enabling rapid and specific diagnosis.6 Skin biopsy with histopathological and immunohistochemical........ analysis demonstrates characteristic ballooning degeneration and multinucleated giant cells.7 Non-invasive saliva PCR testing may detect VZV DNA, though sensitivity is lower. In suspected neurological cases, CSF PCR confirms central nervous system involvement.8
Treatment
Antiviral drugs for herpes zoster inhibit viral DNA synthesis. Acyclovir, a guanine analog, is activated by viral thymidine kinase and converted to its triphosphate form, which inhibits viral DNA
polymerase and causes premature chain termination, reducing disease severity when administered early.9
Amitriptyline, a tricyclic antidepressant, is used in herpes zoster to manage postherpetic neuralgia. It inhibits reuptake of serotonin and norepinephrine, enhancing descending inhibitory pain pathways and reducing pain perception. Its additional anticholinergic effects further modulate pain signaling. Through these combined actions, amitriptyline effectively alleviates neuropathic pain, and early initiation has been shown to significantly reduce the severity and persistence of postherpetic neuralgia.9
Tramadol is used in herpes zoster to relieve moderate to severe pain. It acts through a dual mechanism by weakly binding to μ-opioid receptors and inhibiting serotonin and norepinephrine reuptake. This combination enhances descending inhibitory pain pathways, effectively reducing pain when conventional analgesics are insufficient.10
Paracetamol is used in the treatment of herpes zoster infection to manage mild to moderate pain and reduce fever. It is commonly
employed for symptomatic relief, often in conjunction with other medications, but it does not address the underlying viral infection or inflammation directly.11
The combination of amoxicillin and clavulanic acid simplifies treatment regimens, making it easier for patients to adhere to their antibiotic therapy. By effectively treating secondary infections and complications associated with herpes zoster, this combination helps prevent further health issues and promotes overall recovery. Ranitidine is used to manage gastrointestinal side effects, such as acidrelated discomfort or ulcers that can occur with other medications used in herpes zoster treatment. It reduces stomach acid production to improve overall comfort.12
Valacyclovir, a prodrug of acyclovir, is converted to its active form and inhibits viral DNA polymerase with improved bioavailability, providing effective symptom relief when given early. Famciclovir, metabolized to penciclovir, similarly inhibits viral DNA polymerase and reduces pain and lesion duration, especially in severe cases. Topical penciclovir limits viral replication locally. Foscarnet directly inhibits
Herpes
viral DNA polymerase by binding its pyrophosphate site and is reserved for resistant VZV infections in immunocompromised patients. Brivudin, a VZVselective nucleoside analogue, causes premature DNA chain termination and offers convenient once-daily dosing.9
In herpes zoster management, oxycodone relieves severe pain through μ-opioid receptor binding in the CNS. Gabapentin reduces neuropathic pain by modulating voltagegated calcium channels. Corticosteroids suppress inflammation but should be combined with antivirals. Topical aspirin and NSAIDs such as naproxen, diclofenac, and ibuprofen reduce pain and inflammation, while dipyrone helps control severe pain and fever. Strong opioids are reserved for refractory pain. Lidocaine patches and topical capsaicin provide localized analgesia. Interferons enhance antiviral immune responses and are mainly used in complicated or immunocompromised cases.10, 13
The live attenuated zoster vaccine contains a weakened virus that stimulates immunity and is recommended for
adults ≥60 years, reducing shingles incidence and severity, though protection wanes over time. The recombinant adjuvanted glycoprotein E vaccine is a non-live, two-dose formulation recommended for adults ≥50 years, offering higher and longer-lasting protection against shingles and postherpetic neuralgia. Supportive therapy with multivitamins aids immune function and healing. Topical calamine and aloe vera soothe itching and inflammation, dry lesions, and promote skin recovery, improving patient comfort during herpes zoster treatment.14
Overall, a multidisciplinary approach that encompasses these supportive measures can significantly enhance the effectiveness of treatment and improve quality of life for individuals with herpes zoster.
Discussion
The varicella-zoster virus (VZV), a member of the Herpesviridae family, is an enveloped virus measuring approximately 180–200 nm in diameter. Unlike many enveloped viruses that bud from the plasma membrane, VZV buds from the nuclear membrane of infected cells. It contains an icosahedral capsid enclosing a double-
stranded linear DNA genome associated with viral proteins. The fully sequenced VZV genome comprises about 124,884 base pairs and includes 71 open reading frames encoding 67 proteins, of which only a subset has been fully characterized. VZV replication follows the typical herpesvirus pattern. The virus attaches to host cells through specific receptors and delivers its capsid into the cytoplasm, after which the viral genome enters the nucleus. Immediate early genes are transcribed first, followed by early genes that regulate viral DNA replication. Subsequent expression of late genes produces structural proteins required for virion assembly. These proteins migrate to the nucleus, where capsid assembly and DNA encapsidation occur, forming mature virions. Epidemiological studies indicate that VZV reactivation is more frequent in females than males, particularly in older populations. Incidence rates are higher in Caucasians compared with nonCaucasians, with geriatric data reporting 3.4% in Caucasians versus 1.4% in African Americans. Trauma to specific dermatomes may act as a trigger by
Herpes Zoster in Adolescence: Clinical Presentation, Diagnostic
stimulating affected nerves, although zoster does not consistently develop at injury sites. Genetic susceptibility also contributes; variations in the interleukin-10 gene and a positive family history have been associated with increased risk of reactivation. Compared with primary varicella, herpes zoster lesions are generally less contagious.13
Postherpetic neuralgia (PHN) is defined as pain that persists for more than 30 days after resolution of the herpes zoster rash and is the most common and debilitating complication in immunocompetent patients. Its incidence and duration increase markedly with age. PHN affects approximately 8%–70% of herpes zoster patients, with fewer than 1% of individuals under 40 years developing PHN compared with about 18% of those older than 75 years. Each advancing decade of life is associated with a proportional rise in risk. In addition to persistent pain, patients may experience hyperesthesia, characterized by increased sensitivity to light touch. Despite damage to sensory nerve fibers, preserved thermal sensation is believed to contribute to the persistence and severity of pain. Clinically, PHN is
considered a continuum distinct from acute zoster pain: acute pain is often sharp and stabbing, whereas PHN is typically described as burning and chronic. Major risk factors include advanced age, severe acute rash, intense prodromal symptoms, and female sex. The coexistence of these factors significantly increases the probability of developing PHN.9
The quality of life (QOL) for patients with herpes zoster can be significantly impaired by both acute pain and the chronic pain of PHN. Acute zoster pain can reduce QOL to levels comparable to serious chronic conditions like diabetes, cardiovascular diseases, and depression. Patients with persistent PHN face ongoing physical, psychological, functional, and social challenges. Elderly patients are particularly vulnerable to physical impairment from fatigue, anorexia, and insomnia, which can impede their ability to perform daily activities such as bathing, dressing, cooking, and shopping. Therefore, prompt and effective management of herpes zoster is crucial to mitigating these impacts on QOL.9
Conclusion
Herpes zoster remains a
major health issue due to its severe pain, complications, and impact on quality of life, especially in older and immunocompromised individuals. Effective management requires early diagnosis and comprehensive care to address acute symptoms and prevent long-term issues like postherpetic neuralgia (PHN). Challenges include variable disease presentation, high PHN incidence in the elderly, and complex cases in immunocompromised........ patients. The effectiveness of preventive measures, such as vaccination, and the rising incidence of herpes zoster in vaccinated individuals underscore the need for continued research. Future studies should focus on improving preventive strategies, understanding PHN pathophysiology, and developing new treatments to reduce the impact of herpes zoster and its complications.
References
1. Nair PA, Patel BC. Herpes Zoster. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 4, 2023.
2. Koshy E, Mengting L, Kumar H, Jianbo W. Epidemiology, treatment and prevention of herpes zoster: A comprehensive
Herpes Zoster in Adolescence:
review. Indian J Dermatol Venereol Leprol. 2018;84(3):251262. doi:10.4103/ijdvl. IJDVL_1021_16.
3. Opstelten W, van Loon AM, Schuller M, et al. Clinical diagnosis of herpes zoster in family practice. Ann Fam Med. 2007;5(4):305309. doi:10.1370/afm.707.
4. Frisch S, Guo AM. Diagnostic methods and management strategies of herpes simplex and herpes zoster infections. Clin Geriatr Med. 2013; 29(2):501-526. doi:10.1016/j.cger.2013.01.003.
5. de Jong MD, Weel JF, van Oers MH, Boom R, Wertheim-van Dillen PM. Molecular diagnosis of visceral herpes zoster. Lancet. 2001;357(9274):21012102. doi:10.1016/s01406736(00)05199-0
6. Schmidt NJ, Gallo D, Devlin V, Woodie JD, Emmons RW. Direct immunofluorescence staining for detection of herpes simplex and varicella-zoster virus antigens in vesicular lesions and certain tissue specimens. J Clin Microbiol. 1980;12(5):651-655. doi:10.1128/jcm.12.5.651655.1980.
7. Annunziato PW, Lungu O, Panagiotidis C, et al. Varicellazoster virus proteins in skin lesions: implications for a novel role of ORF29p in chickenpox. J Virol. 2000;74(4):2005-2010. doi:10.1128/jvi.74.4.20052010.2000.
8. Kelley A. Herpes zoster: A
primary care approach to diagnosis and treatment. JAAPA. 2022; 35(12):13-18. doi:10.1097/01. JAA.0000892712.73041.ae
9. Cohen KR, Salbu RL, Frank J, Israel I. Presentation and management of herpes zoster (shingles) in the geriatric population. P T. 2013; 38(4):217227.
10. Valladales-Restrepo LF, Velasquez-Quimara S, MachadoAlba JE. Pharmacological Treatment of Herpes Zoster and Factors Associated with Its Recurrence. Antibiotics (Basel). 2023; 12(4):757. Published 2023 Apr 14. Doi: 10.3390/ antibiotics12040757.
11. Mikaeloff Y, Kezouh A, Suissa S. Nonsteroidal anti-inflammatory drug use and the risk of severe skin and soft tissue complications in patients with varicella or zoster disease [published correction appears in Br J Clin Pharmacol. 2010 Jun;69(6):722]. Br J Clin Pharmacol. 2008; 65(2):203209. doi:10.1111/j.13652125.2007.02997.x
12. Banno F, Riccelli T, Banno M. Simultaneous parotitis and ipsilateral herpes zoster ophthalmicus: coincidence?. BMJ Case Rep. 2019;12(3):e228897. Published 2019 Mar 20. doi:10.1136/bcr-2018-228897
13. Nikkels AF, Piérard GE. Recognition and treatment of shingles. Drugs. 1994; 48(4):528548. Doi: 10.2165/00003495199448040-00004.
14. Patil A, Goldust M, Wollina U. Herpes zoster: A Review of Clinical Manifestations and Management. Viruses. 2022; 14(2):192. Published 2022 Jan 19. Doi: 10.3390/v14020192.
OBSERVERSHIP IN AESTHETICS
3-Nights, 4-Days Program Highlights*
2 Half-days
Package to be announced shortly
Inclusions:
2 Half-days
Observership in Aesthetic Procedures
Lectures by DHA Certified Faculty with upto 6 DHA@CME Credits# CME Credits# with
* 3-Nights 4-Days Stay, in a 4-STAR Hotel with breakfast and dinner, Lunch at Academy/Aesthetic Centre, To and fro - Hotel to Academy/Aesthetic Centre SIC◊
Exclusions:
Air fare to Dubai and back , airport transfer, Sight seeing etc.
@ DHA- Dubai Health Authority
# Proposed s/t confirmation
◊ SIC- Seat in Coach
Interested Drs kindly call for further details: +91