Health, Place & Retrofit: Findings and recommendations for change
HEALTH, PLACE, AND RETROFIT:
FINDINGS AND RECOMMENDATIONS FOR CHANGE
Understanding the Nuance of Place in Retrofit.....................................................................................
Health and Retrofit: The Promise and the Pitfall....................................................................................
Using Community Health Impact Assessments (CHIAs).......................................................................
Practice,
Collaborator:
Strategic Partner:
Research Contributor: Dr. Kate Simpson
With appreciation for the innovators whose time and interviews allowed us to create the Innovator Profiles: HACT, Social Value Portal, UKGBC, Leeds Beckett University, Retrometer, Edinburgh Climate Change Institute. With thanks to our survey respondents and to all who participated in our workshops. With special thanks to The Portland Inn Project.
Title image, and images on page 7 are credited to Angela Grabowska & Paul Stringer
A tonal difference may be noticeable across the paper. This is intentional and reflects the deep collaboration that was involved in the production of the paper.
INTRODUCTION
The quality of the UK’s housing stock has a direct and growing impact on health, well-being, and inequality. Cold, damp, overheating, and poorly ventilated homes contribute to physical illness, mental stress, and insecurity, yet retrofit policy and delivery often focus narrowly on technical performance and energy metrics.
This paper argues that retrofit must be understood as a place-based, health-shaping intervention, not only a building upgrade. Homes sit within wider social, economic, and environmental systems, and the outcomes of retrofit are shaped as much by lived experience, local context, and delivery practice as by materials and specifications.
Drawing on evidence, practice, and emerging innovation, this paper explores how integrating community-led health insight with robust measurement of building performance can improve retrofit outcomes. It sets out why tools such as Community Health Impact Assessments (CHIAs) and measured performance approaches are needed to complement existing policy instruments, and how they can support more effective, equitable, and accountable retrofit at scale.
MEASURING OUTCOMES & IMPACT EVALUATION (MO+IE) PROJECT BACKGROUND AND METHODOLOGY
This paper forms part of a wider project of work led by the National Retrofit Hub and supported by Impact on Urban Health, Arup, and TrustMark, focused on strengthening how retrofit outcomes are defined, measured, and used to inform policy and delivery. The Measuring Outcomes and Impact Evaluation (MO+IE) project adopted a mixed-methods methodology structured around four interlinked work packages. Together, these enabled an assessment of current retrofit outcome measurement, active engagement with sector stakeholders, analysis of emerging best practice, and the co-creation and testing of future-focused policy and delivery approaches.
The project itself emerged following the publication of the NRH State of the Nation Review of retrofit delivery. A recurring theme had arisen in that research around the need for broader outcomes measurement in retrofit programme design as well as a need for stronger evaluation of retrofit programmes currently in operation. This led to the research question “How can broader outcome measurement accelerate retrofit delivery and be designed to drive better policy, funding, and delivery decisions - particularly to maximise co-benefits like health and equity in a fiscally constrained environment?”
A Three Horizons model provided the overarching analytical structure, linking current practice (Horizon 1), near-term delivery innovation (Horizon 2), and long-term systemic change (Horizon 3). Key outputs include evidence reviews, current retrofit programme measurement baselining, stakeholder insights, innovator profiles, and within this document, recommendations to support outcome-driven retrofit delivery.
A series of Future Visioning workshops were held to draw out recommendations based on the research carried out across the project. A novel approach, these were carried out to remind us that we as an industry are working towards improving the conditions of our collective communities. Future positive lived outcome scenarios were used to enable stakeholders to imagine and visualise what is possible. These fed into the practice, delivery, and policy recommendations at the end of this paper.
AUDIENCES
This is not an academic paper, but a practical overview informed by emerging innovations and stakeholder perspectives. It sets out opportunities and challenges for future work and investigation by showing how:
- success in retrofit must be defined more broadly - measured performance must complement modelled assumptions - communities must be supported to shape and assess outcomes
WHO SHOULD USE THIS REPORT?
• Central Government Departments (e.g., DESNZ, Cabinet Office) and Ofgem to inform and develop multi-generational and cross-sectoral policy and funding design.
• Combined Authorities and Devolved Governments for regional policy development and implementation.
• Local Authorities and Housing Associations for planning and prioritising retrofit programmes.
• Delivery Partners and Grant Administrators to design schemes that both reward verified outcomes and require community codesign.
• Communities to navigate methods of creating data led agency to engage with all of the above.
• Consultants in their advice to all of the above.
EXECUTIVE SUMMARY
Poor housing remains a major driver of ill health and inequality across the UK, yet retrofit success is still largely defined through narrow technical metrics that fail to reflect lived experience. Retrofit policy and assessment frameworks often prioritise compliance and modelled performance, overlooking how health impacts are shaped by place, tenure, and long-standing structural inequities. As a result, there is a persistent gap between technical performance and the outcomes that matter most to households and communities.
The MO+IE project points to clear shifts that are now needed across policy and delivery.
First, success in retrofit must be defined more broadly. Carbon reduction and bill savings remain vital, but they are not sufficient on their own. Health, comfort, and lived experience must be valued as core outcomes, not secondary benefits.
Second, measured performance must complement modelled assumptions. Post-intervention monitoring, including approaches that draw on real-world data, is essential to understanding whether retrofit is actually improving homes in practice. Without this, policymakers and delivery partners are effectively flying blind.
Third, communities must be supported to shape and assess outcomes. Tools such as Community Health Impact Assessments (CHIAs) offer a practical way to centre lived experience, surface local realities, and ensure that interventions respond to the specific identities and needs of places. This is not about consultation for its own sake, but about improving decision-making and accountability.
Together, these shifts move retrofit away from technical compliance towards outcomes that improve health, reduce inequality, and strengthen places.
RETROFITTING AS A NATIONAL MISSION
Retrofitting the UK’s housing stock is often described as a national mission, one that requires urgency, scale, and ambition1. Climate change is already driving the UK into a new era of climate-related health risks as made clear in the latest National Emergency Briefing2, and we cannot afford retrofit failures. As the UK Health Security Agency warns of escalating heat stress3, damp, mould and poor air quality, and both the CCC4 and IPCC5 underline the accelerating pace of climate extremes, badly designed or poorly delivered retrofit is no longer just a wasted investment, it is a direct threat to human health. Every retrofit decision made today must protect indoor environmental quality as much as it tries to cut carbon, for example, or we risk locking millions of people into homes and communities that are thermally volatile, unsafe, and unhealthy.
“Future heat will risk the health and lives of vulnerable people. Heat-related deaths already occur in the thousands each year but could rise several times over to exceed 10,000 in an average year by 2050.”
- CCC
“Regional changes in the intensity and frequency of climate extremes generally scale with global warming… The number of hot days and hot nights and the length, frequency, and/or intensity of warm spells or heatwaves will increase over most land areas (virtually certain).”
- IPCC
The path toward meaningful and lasting decarbonisation in our built environment remains clouded by structural and methodological limitations. Firstly, policies developed to increase retrofit delivery tend to rely on highly standardised, one-size-fits-all approaches, designed to reach broad populations but often failing to reflect the complexities of local context. In turn, these broad policies miss the diversity of lived experience, building typologies, and environmental conditions that shape how retrofit interventions land, let alone what might genuinely be needed in a place. A policy delivered successfully in one place may struggle in the next because people, homes, and needs differ more than national frameworks currently acknowledge.
A second, equally significant challenge is performance measurement. Much of the evidence base for retrofit relies on results built on modelled averages rather than granular, real-world performance data. This makes it difficult to predict outcomes reliably and exposes policymakers, investors, and communities to risk6. Over the last decade, several national schemes have shown the consequences of poor data and a complex quality assurance system7. Delivery falls short; homes do not perform as expected, trust fades, and money is wasted.
“An estimated 22,000–23,000 homes with external wall insulation - 98% of installations - have major issues requiring remediation.” - NAO Report
“...clear failures in the design and set-up of ECO and in the consumer protection system have led to poor-quality installations, as well as suspected fraud.” - NAO Press Release
RETROFITTING AS A NATIONAL MISSION
These issues point to a systemic gap - the absence of an integrated, place-sensitive feedback loop that connects policy design, delivery, and real-world outcomes (especially health and equity), grounded in robust, ongoing measurement. The contrasting experiences of Kirklees Warm Zones and Fishwick in Preston (see appendix) illustrate this gap. Kirklees Warm Zones demonstrated how areabased, inclusive delivery can improve uptake, thermal comfort, and well-being. By contrast, Fishwick highlights the risks of rushed installation, poor workmanship, and lack of local sensitivity, which led to severe housing and health impacts. Without accurate and relevant measurement before work starts, during delivery and after completion, the sector is left with only part of the picture. Outcomes remain uncertain, and it becomes harder to understand what is happening in different places and for different households. For an investment landscape that requires long-term confidence, this lack of clarity is untenable8 .
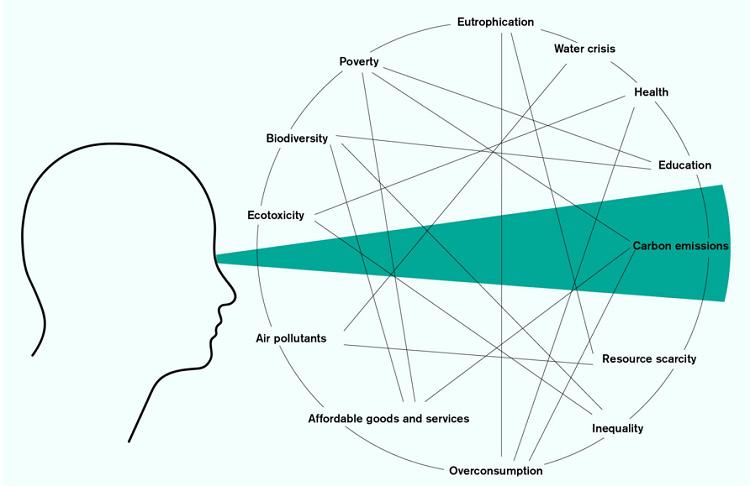
Thirdly, there is a deeper narrative problem at the heart of this. Retrofit is still presented largely through carbon reductions, energy efficiency, and bill savings. These do not always feel compelling for people, especially in a context where energy costs continue to rise. Carbon is abstract. It cannot be felt or seen, and it is hard to connect to daily life when the cost of living, financial insecurity, social tensions, and family pressures are far more immediate.
Energy efficiency retrofit in practice can be disruptive without any apparent tangible benefit and delivered to troubling degrees of quality. Relief from any short-term bill savings is quickly eroded by the next wave of energy prices rising. This, combined with other known barriers, means the public’s appetite for retrofit has often been lukewarm. What does resonate are the tangible outcomes: decent, resilient, comfortable, healthy homes and neighbourhoods for people and their loved ones9. When framed through the lens of housing quality, well-being, and fairness, retrofit becomes not simply a technical intervention but a social one, something that improves lives as well as climate profiles.
Figure 1 - Carbon Tunnel Syndrome10
RETROFITTING AS A NATIONAL MISSION
CHANGING THE NARRATIVE
The challenge of retrofit sits within a number of growing health crises. Homes, which are largely held as places of sanctuary, can become active stressors on people’s lives. Living standards and behaviours have changed since most of the U.K’s housing stock was built, and the damaging impacts of air and noise pollution are now better understood. Additionally, there is growing awareness that the neighbourhoods and urban environments we live in have an impact on our health; where inequitable access to goods, services and resources adds pressure for many communities. It is well understood that housing and health are closely linked across all aspects of our environment.
Health, equity, and retrofit are therefore deeply interconnected. Improving homes can meaningfully improve lives12, but only when interventions are carefully attuned to the realities of place. Just as a doctor would not prescribe treatment without first conducting a triage, practitioners should not be designing retrofit interventions without a structured assessment of local need, vulnerability, and opportunity.
The aim of this paper is to explore these intertwined gaps: the absence of robust tools for targeting and quantifying the wider impacts, particularly health and equity implications, of housing interventions, and the lack of consistent performance measurement across retrofit activities. We argue that integrating processes such as building performance evaluation methodologies and deeper understanding of place data, such as CHIAs, can equip local authorities, policymakers, communities, and delivery partners with structured insight into both the real condition of our building stock and begin to account for the nuances of place in programme delivery.
Figure 2 - Photographs from CIVIC SQUARE’s ‘Retrofit House’11
RETROFITTING AS A NATIONAL MISSION
Better outcomes measurement must be embedded throughout the retrofit process, from baseline assessment of both buildings and communities, to post-installation performance monitoring. Together, health-focused impact assessment and rigorous performance measurements help provide credible data that drives uptake and attracts further investment. They can ensure that retrofit delivers not only on carbon, but on all the outcomes that matter to people: safe, resilient, equitable homes and strong communities.
SUMMARY
• National policies can miss local reality. Broad approaches overlook how people actually live and how homes behave in different contexts.
• Over reliance on modelled averages instead of real performance data increases risk for policymakers and residents.
• Carbon and energy efficiency do not motivate most people. Comfort, safety and well-being do.
• Housing quality and health are deeply linked, so retrofit must respond to local needs and vulnerabilities.
• Better tools such as CHIAs, combined with stronger performance measurement, help us design retrofit that works for people and place.
RETROFIT TARGETS AND PROGRESS
HOW RETROFIT SUCCESS IS CURRENTLY MEASURED
At present, the Energy Performance Certificate (EPC) is the primary national policy tool used to assess retrofit outcomes in the UK. It was designed to support benchmarking at scale, not to provide an accurate picture of performance at the household level. Its use has long been debated, including through a recent consultation on its reform, to which the National Retrofit Hub responded, proposing a roadmap towards change in The Future of Energy Performance Certificates: A Roadmap for Change, a comprehensive report advocating essential updates to EPCs.
Bearing such limitations in mind, it is important to first understand how each of the major retrofit delivery programmes measure success. As an earlier output of the Measuring Outcomes & Impact Evaluation (MO+IE) project, the NRH published a summary document baselining what is currently being measured in retrofit programmes, and what is not. Most of the insights presented are drawn from policy documents and project specifications rather than exhaustive practical delivery experiences. One of its key findings was the gap between what is intended to be measured and what is visible in practice. It highlighted the missed opportunity when broader outcomes are not identified or tracked, and the risk of not systematically measuring the energy efficiency improvements of retrofit programme investments.
IMPROVING RETROFIT MEASUREMENT AND EVIDENCE
So how can we do better? This gap between intended and realised outcomes is the challenge addressed by BS 40101:2022, the voluntary British Standard for the Building Performance Evaluation (BPE) of occupied and operational buildings. BS 40101 sets out a structured approach to assessing how buildings actually perform in use, drawing on measured energy data, environmental monitoring, observation, and user experience. Unlike EPCs, which are predictive and standardised for benchmarking, the intention of BS 40101 is to focus on real-world performance and lived outcomes, providing a framework for evaluating whether retrofit investments are delivering their intended benefits in practice.
Researchers previously recommended using monitored energy data to complement EPCs13 . Subsequently, the SMETERS project (Smart Meter Enabled Thermal Efficiency Ratings) explored whether smart meter data, combined with optional sensors and heating controls, could be used to estimate building heat loss more accurately and efficiently. The Heat Transfer Coefficient (HTC) indicates building heat loss and is typically predicted by EPC calculation methods, or measured by time-intensive co-heating tests. The project found that using smart meter data to calculate heat loss has clear potential, offering more robust results and better understood error characteristics than EPC derived estimates, while being less intrusive and potentially more cost effective. Read more about this in our report Data and technology: strengthening our understanding for better retrofit outcomes
Additionally, a Metered Energy Savings (MES) approach could also be more broadly adopted, such as Retrometer14. The MES approach looks at the actual metered energy use, both gas and electricity, after the retrofit, and compares it to how much energy would have been consumed in that home during the post-retrofit period, had there not been a retrofit. In addition, RetroMeter values the multiple benefits arising from retrofits so that they can be assigned to various stakeholders and attract different types of capital. More details of this approach are published in the NRH Innovator Profile document
RETROFIT TARGETS AND PROGRESS
While energy performance matters, other environmental conditions such as relative humidity, air quality, noise, and light impact our health. These factors are influenced by housing upgrades at the household level15 and by transport, climate resilience, and biodiversity interventions at the neighbourhood level. However, both in the UK and internationally, success of energy efficiency retrofit beyond operational energy is rarely captured. The Build Upon Framework15 is one such practical tool that can assist in such cases. It enables local authorities, cities and organisations to measure the full benefits of building retrofit — not only energy savings, but also social and economic impacts.16
Such approaches align closely with the principles set out in BS 40101. It emphasises the use of monitored data and transparent comparators to understand building performance in operation. By encouraging the use of in-use measurements rather than relying solely on design-stage predictions, the standard provides a consistent evaluative context within which methods like HTC estimation and Metered Energy Savings can be interpreted and compared.”
Advances in technology now make it quicker and cheaper to monitor variables such as air temperature, airborne pollutants, noise and light, making the measurement of such indicators more readily available. Some pioneering policy schemes have begun to reflect this, such as Optimise Retrofit Programme in Wales17. The programme includes a specification for monitoring operational energy, relative humidity, temperature and CO² as an indicator of air quality and ventilation; however the success of this is still to be more widely evaluated in practice.
TOWARDS CONSISTENT MEASUREMENT OF WIDER OUTCOMES
The National Audit Office reports on energy efficiency retrofit schemes have called for better monitoring of outcomes, clarity in standards and success criteria across the four audits relating to schemes of the time, dated 200918, 201619, 202120 and 202521. Unfortunately, these requests have never been fully addressed, and the cost of remediation, resulting from poor quality installations, could now be in the billions, for known cases.
UK decision-makers recognise this major gap in monitoring the health impacts of climate policies, including housing retrofit. Despite guidance such as the Green Book, departments and local authorities often lack the capacity to carry out robust health impact assessments, leaving little evidence linking retrofit to outcomes like reduced asthma or fewer hospital admissions. Using the Green Book, a previous study showed that 79% of the benefits of climate action across six UK urban regions are social22 - such as improved air quality, increased physical activity, and better home comfort - highlighting the benefit of and need for systematic, place-specific monitoring.
This raises the question of whether an overarching monitoring framework is needed to introduce a standardised way of measuring wider outcomes, helping to build consensus and trust across the sector. Our Innovator Profiles publication sought to identify existing frameworks and methodologies that could be readily adopted for this purpose.
These innovations provide a strong foundation on which to build, drawing on existing models that could be scaled up and applied to larger programmes. Testing these approaches at scale would help generate the data needed to demonstrate how greater value can be achieved when retrofit investment is used more effectively.
RETROFIT TARGETS AND PROGRESS
SUMMARY
• EPCs remain the primary policy tool for assessing retrofit outcomes, but they were designed for benchmarking at scale, not for measuring household level performance or lived outcomes. See NRH’s work on EPC Reform.
• Measured performance approaches, including monitored energy data and SMETER technologies & Metered Energy Savings, could offer better baselining and more reliable insight into whether retrofit is delivering real improvements in building performance.
• Environmental conditions such as temperature, air quality, noise, and light have a direct impact on health, yet are rarely captured in retrofit evaluation. See NRH report on SMETERHTC and our Innovator Profiles.
• Repeated National Audit Office findings highlight the consequences of weak outcome monitoring and unclear success criteria across retrofit programmes, and subsequent costly remediation.
• Existing frameworks and past programmes demonstrate that broader, health-led evaluation is possible and can reveal significant social and economic value.
• Without integrated measurement of material performance and health outcomes, the true benefits of retrofit remain hidden, and the risks of poor delivery persist.
UNDERSTANDING THE NUANCE OF PLACE IN RETROFIT
To design retrofit strategies that genuinely improve lives, we must begin with a clear and grounded understanding of place. Too often, place is treated as a purely geographic term, a pin on a map or an administrative boundary. But places are far more complex23. They carry the imprint of historical, environmental, and social inequities as well as the architectural and policy decisions that have shaped their built environment over decades. When retrofit is planned without this deeper understanding, interventions risk being technically correct yet socially ineffective.
Housing stock does not emerge by accident; its condition and typology also reflect decades of planning policy, historic land ownership, investment, neglect, and local responses to environmental pressures24. These forces determine not only how buildings perform today but also how people experience them, whether homes feel safe, comfortable, and dignified. In this way, the nature of the built environment becomes inseparable from the nature of the community that inhabits it.
Such structural determinants shape both population health and retrofit readiness. In 2023-2024 approximately 3.6 million households were living in non-decent homes, about 14% of all households in England25. Non-decent homes are those that fail the statutory Decent Homes Standard. Communities that have experienced repeated cycles of failed or inconsistent interventions, austerity, or inaction over environmental pollution often exhibit lower trust in institutions and reduced capacity to engage with retrofit programmes26,27
Feedback from retrofit delivery stakeholder workshops throughout the MO+IE project included:
“Many programs lack dedicated funding for evaluation, making it difficult to measure outcomes effectively. The constraints of grant deadlines often lead to rushed implementations without adequate baseline data.”
Meanwhile, buildings in such areas may face compounding issues with damp, overcrowding, poor ventilation, or outdated construction, that require specifically considered rather than pre-determined measures-focused solutions. When these buildings interact with areas high in air, noise, light, and heat pollution, the home becomes a health risk. Identifying these interlinked determinants is essential for designing retrofit pathways that support rather than overwhelm local systems.
Understanding the nuance of place requires blending quantitative data with qualitative insight. Numbers provide critical baseline information: housing stock condition, energy performance data, health indicators, environmental exposures, and demographic patterns. But such data alone cannot explain how people navigate their homes, how communities perceive risk, or why some groups engage readily with retrofit while others do not. Qualitative evidence, including community narratives, cultural context, intergenerational memory, local identity, and levels of trust fill this critical gap. When these forms of knowledge are held together, they create a richer picture of place, allowing for interventions that respond to real conditions rather than assumed ones.
The work of Centric Lab offers an especially valuable lens for this deeper understanding. Their research emphasises that environmental context shapes both neurobiological and social health. They also argue that “upgrading cities from merely places of commerce to habitats that can support human health will require a biological approach to urban planning”28, highlighting how the human stress response system (called the HPA Axis) is a key pathway linking internal human biology with the external environment. In other words, place is not just something people live in; it is something that actively interacts with their regulatory systems, influencing health, agency, and resilience.
UNDERSTANDING THE NUANCE OF PLACE IN RETROFIT
The work of Centric Lab builds on a history of sociological and scientific work linking habitats to health outcomes. In 1899 in America, W.E.B.Du Bois29 put forward how the outcomes for African-American communities reflected the neighbourhoods they were forced to live in. Later in the 21st Century the American academic and neuroscientist, Robert Sapolsky30, brings to light the toxic relationship between psycho-social stress (a life event or situation that creates stress) and notions of genuine ”free will”, where life events, stress exposure, social environment, determine behaviour rather than free will. This framing reinforces why retrofit must be approached as both a technical and a social-health endeavour.
Ultimately, to develop approaches to retrofit effectively, policymakers and practitioners must move beyond generic solutions and toward a place-attuned model, one that sees buildings within their social ecosystems and recognises that meaningful change depends on understanding people and place as fundamentally interconnected.
SUMMARY
• Place is shaped by people, history, buildings and local systems, not just geography.
• Neighbourhoods reflect historic inequities, local decision making, and environmental pressures.
• Building performance data does not capture trust, culture, behaviour, agency, or lived experience.
• The built environment interacts with our human biology and affects health, agency, and resilience.
• Retrofit must be tuned to local conditions, not just standardised assumptions
HEALTH AND RETROFIT: THE PROMISE AND THE PITFALL
Retrofit is often introduced as a technical intervention, as an upgrade, an optimisation, a series of measures applied to a building so it performs better. But when we look closely at what people need from their homes, it becomes clear that retrofit sits squarely within the domain of health and wellbeing. Not just the absence of illness, but the conditions that allow people to live well, feel safe, and exercise agency over their daily lives31. The potential here is vast. Yet so too are the risks when retrofit is offered or delivered without a deep understanding of the starting conditions of homes, residents, and neighbourhoods.
The promise of retrofit as a practice to improve health is an appealing one. Better indoor air quality, improved thermal comfort, more affordable energy use, even housing stability and quality, each of these is directly tied to healthier bodies and minds32. Under the right conditions, retrofit can reduce exposure to pollutants and stressors that quietly undermine health every day. But it is also important to understand where in the system retrofit plays its part in ensuring positive health outcomes.
To situate retrofit within this broader system, it is useful to distinguish between key health concepts that describe how health is shaped, measured, and experienced:
Determinants of Health:
The factors in your life and environment that affect your health.
Health indicators:
Clues or signs that show the current state of health in a person or community.
Health metrics:
The actual numbers or measurements used to track and compare health.
Health outcomes:
The results or effects of health factors and care on a person’s or community’s health.
The potential health outcomes should not be taken at face value alone. We talk often about mould, damp, and cold, and whilst it might be desirable to claim that once those issues are fixed, health outcomes will naturally improve, health doesn’t respond to environmental change in a simplistic one-step cause-and-effect. Just as light pollution disrupts our melatonin production which in turn cascades into sleep disorders and mood impacts, exposure to damp and mould triggers a biological stress response. It can activate inflammation, impair breathing, disturb sleep, and heighten vulnerability to chronic conditions33. These environmental exposures accumulate; they nudge the body into a state of constant alert. So, the removal of mould, damp, and cold conditions, though crucial, and may have an immediate impact on well-being, are unlikely to have an immediately measurable longer term health impact. The key extra ingredients are time, and approaching health and retrofit in a systemic, ecological manner that reflects the wider determinants of health people live within, over time.
The environmental pressures and determinants of health that people live in act as early warning signs of future health problems. They shape how resilient or vulnerable someone is to illness34. Retrofit can reduce these pressures by eliminating sources of stress and building agency, but only if it’s based on understanding what people are actually exposed to and how those exposures affect their everyday lives.
HEALTH AND RETROFIT: THE PROMISE AND THE PITFALL
It is crucial that the narrative of retrofit as a practice to improve health is robust because this represents a significant lever in increasing the perception of the value of retrofit. Many people lack choice in the measures applied to their homes or the subsequent removal of products installed badly that are causing unsafe living conditions. Agency is a fundamental driver of health outcomes.
The pitfall emerges when retrofit is delivered without this contextual sensitivity. For instance, the Fishwick programme’s failed external wall insulation created damp, mould, and unsafe living conditions, exacerbating health risks rather than alleviating them (see appendix). Too often, programmes begin with assumptions about buildings that are only partially understood: standardised archetypes, incomplete condition surveys, or generic models that flatten the diversity of homes into a manageable dataset. There is talk of resident engagement, but much of it stops at consultation rather than cultivating genuine agency35. And while building archetypes receive attention, neighbourhood archetypes that take into account the layered social, environmental, and infrastructural conditions that shape health are rarely considered. The result is a retrofit system that can unintentionally cause harm.
SUMMARY
• Retrofit has real potential to improve health through better air quality, warmth and comfort.
• Health improvements take time because health is ecological, requiring a systemic approach, and long-term stress affects the body in complex ways.
• If retrofit is based on assumptions rather than real conditions, it can create new risks.
• Residents need genuine influence over design and delivery, not surface-level engagement.
• A place-led approach supports safer, more effective and more equitable outcomes, long term.
• Agency is a fundamental driver of health outcomes.
USING COMMUNITY HEALTH IMPACT ASSESSMENTS (CHIAs)
This chapter describes the detail of CHIAs as one such solution to overcome the pitfalls and to consider how to account for place as set out in the previous chapters.
Community Health Impact Assessments (CHIAs) offer a practical and justice-led framework for understanding how retrofit interacts with place, health, and lived experience. In simple terms, it is when the community defines the criteria around what makes up their health and well-being based on their interactions with the systems around them36. CHIAs help surface local insight that standard policy tools often miss, making them useful for shaping more responsive and effective retrofit planning. Kirklees Warm Zones demonstrates how understanding and responding to local needs without means testing or administrative barriers can support equity and well-being (see appendix).
Unlike traditional Environmental or Social Impact Assessments, which often rely on technocratic, top-down metrics and secondary quantitative data, CHIAs invert the process: they are built by the community, grounded in lived experience, and designed to inform future interventions such as retrofit programmes. This shift matters because conventional Health Impact Assessments can miss nuance, depend on incomplete datasets, and exclude the people most affected by change. A CHIA, by contrast, acts as an ethical tool aligned with the World Health Organisation’s (WHO) values of democracy, equity, sustainable development, and the ethical use of evidence by centring residents’ own criteria for health and well-being37
Crucially, CHIAs surface the real conditions behind health data, conditions that are often flattened or hidden in large datasets. Communities articulate how stress, insecurity, mould, overcrowding, pollution exposure, or isolation are produced through specific interactions with the built, social, economic, and political environments around them.
These qualitative insights can reveal pathways of harm, adding to experiences of overwhelm and chronic stress. The experiences of environmental stressors, or behavioural patterns shaped by poor building and urban design, are insights that would otherwise remain invisible to external stakeholders. Through this process, CHIAs create place-based datasets that reflect how determinants of health are experienced locally and how they intersect.
For retrofit, the benefits are significant. Firstly, CHIAs can reveal hidden risks and opportunities before interventions take place. They illuminate not only the physical condition of the housing stock, but also the relational systems that shape outcomes, including landlord decision making, overcrowding, informal care networks, community activity, and everyday household routines. These factors often determine whether retrofit improves lives or deepens existing inequities.
Secondly, they allow retrofit strategies to be tailored to real conditions. Communities may identify heat stress from solar gain, unsafe green spaces, noise exposure, or a lack of communal areas as critical determinants of health, prompting solutions that combine technical retrofit with nature-based, social, or governance interventions.
Thirdly, CHIAs strengthen trust, agency, and social capital by validating lived experience and disrupting patterns of institutional gaslighting that many communities face.
USING COMMUNITY HEALTH IMPACT ASSESSMENTS (CHIAs)
A simple example shows what this looks like in practice. Imagine a neighbourhood about to undergo a large scale retrofit of its ageing terraced homes. The technical surveys focus, quite rightly, on insulation levels and heat loss. But a CHIA reveals a wider set of issues that would otherwise be missed.
Residents talk about constant traffic noise, anxiety about long construction periods, fears of temporary relocation becoming permanent, and the importance of informal childcare networks that rely on neighbours being close by. They also point out that existing ventilation systems make damp worse, because real kitchen and bathroom use does not match the assumptions built into standard designs.
When these insights are taken seriously, the retrofit programme changes. Ventilation strategies are adjusted to reflect how homes are actually used. Construction is phased to reduce disruption and avoid breaking informal support networks. Community led oversight is built into delivery. Less obvious but meaningful additions, such as green wall noise buffers or improved shared spaces, are included. The result is a retrofit programme that is materially effective, socially rooted, and health-producing.
CHIAs create space for communities to explain how they experience impacts on their health, in their own words. They allow multiple perspectives on the environments people live in to sit alongside one another, rather than being reduced to a single narrative.
When developed in partnership with public health teams and local healthcare services, these insights can directly inform “Health in All Policies” approaches38, grounding them in lived experience rather than abstract objectives. When facilitated well, CHIAs can also unlock imagination and hope, reflecting the diversity of cultures, histories, and knowledge within a community. Crucially, this work goes beyond technical assessment. It strengthens the social fabric of a place, builds on existing community assets, and supports solutions that are shaped with communities rather than imposed on them.
Ultimately, CHIAs reposition retrofit as more than a technical upgrade. They show that healthier homes emerge when communities define what health means for them, when retrofit engages with the ecological determinants of well-being, and when place-based insight becomes the foundation for transformative, equitable change.
USING COMMUNITY HEALTH IMPACT ASSESSMENTS (CHIAs)
SUMMARY
The use of CHIAs can:
• Identify who benefits and who might be left behind.
• Identify additional or replacement interventions in retrofit programmes that improve health outcomes.
• Ensure participatory processes that give voice to underrepresented groups.
• Build trust by showing transparency and responsiveness in decision-making.
• Communities help identify the meaningful and experience-led health-based criteria that can be measured and tracked over time.
• Be key places of interaction between public health departments and local communities.
• Become practical spaces of the development of social capital.
PRACTICE, DELIVERY & POLICY RECOMMENDATIONS
Integrating place-based health insights into policy and practice ensures that retrofit interventions are tailored to the needs of local populations and deliver measurable benefits across multiple dimensions. At the same time, stronger approaches to measuring building performance are essential to confirm whether retrofit capital investment is achieving real, lasting improvements in the built environment. This requires moving beyond assumed compliance or modelled performance. Instead, it means monitoring real indoor conditions, including temperature stability, ventilation, humidity, and heat retention, and linking these material outcomes to health, comfort, and well-being.
Together, approaches such as Community Health Impact Assessments (CHIAs), measured performance methods, and the innovations highlighted in our Innovator Profiles point towards a more integrated, place led model of retrofit delivery.
The following set out practical steps for improving retrofit practices and a series of policy recommendations.
* In these recommendations, the term communities refers to community and civil society organisations. These organisations can take many forms, but they share a common purpose: representing the voices of, and acting as intermediaries for, groups of people with shared interests or characteristics. Such organisations include, but are not limited to, community energy groups, faith and justice groups, residents’ associations, arts organisations, and sports or social clubs.
PRACTICE AND DELIVERY RECOMMENDATIONS
For local authorities:
• Use devolved governance to coordinate place-based, health-led retrofit strategies.
• Embed CHIA type methods into retrofit planning, feasibility, and evaluation.
• Combine health data (public health, housing quality) with social insight (community engagement, local knowledge).
• Strengthen collaboration across departments, particularly housing, public health, environment, and planning.
• Build local retrofit ecosystems that connect housing providers, public health teams, community organisations, and local supply chains.
• Use measured performance data to assess whether retrofit programmes are delivering stable, healthy indoor environments in practice, not just on paper.
PRACTICE, DELIVERY & POLICY RECOMMENDATIONS
For policymakers:
• Acknowledge that structural inequities (racial, economic, geographic) shape exposure to poor housing and health outcomes and limit opportunities.
• Develop government-backed longitudinal studies combining NHS, housing, energy, and social data to track indoor environments, occupancy patterns, governance models, and long-term impacts on health, education, and work.
• Standardise data sharing and interoperability across housing, health, and energy systems with clear governance and safeguards building upon existing frameworks.
For delivery partners:
• Engage communities early; co-produce decisions to build trust and agency.
• Advocate for community-led research methods to build local data profiles of communities’ lived experiences.
• Use CHIA findings to inform communication, design, sequencing of work, and resident support.
• Combine technical monitoring with qualitative insight to understand how buildings are used in practice and how interventions land in everyday life.
For communities:
• Working with trusted allies can make a difference. Community organisations, health teams, charities, or local advocates can help create safer ways to gather experiences and carry them into decision making spaces.
• Help define what “good” looks like. Community Health Impact Assessments can be a useful way to set local priorities and describe the outcomes that matter most to residents.
• Advocate for how homes are used. Simple details about cooking, heating, ventilation, and family life can highlight issues that technical surveys often miss.
• Sharing lived experience works best when it feels safe and supported. This might involve group discussions, facilitated research, or anonymised insight, rather than individuals speaking out in formal settings.
PRACTICE, DELIVERY & POLICY RECOMMENDATIONS
Through a range of projects and programmes, the National Retrofit Hub has developed a number of policy recommendations that support and align with the findings of the MO+IE project. Before setting out the specific policy recommendations arising from MO+IE, we first highlight related recommendations from across our other work.
These include:
1. Our work on Building Logbooks which called for the establishment of a national Building Logbook system as a legally required record of works, warranties, and guarantees, transferable between owners and capable of holding additional and interoperable datasets.
2. Our proposals for EPC Reform so that they better reflect actual energy use, building condition, and retrofit readiness, supporting more appropriate interventions to support health, comfort, and social outcomes.
3. Our work on the Minimum Energy Efficiency Standard we recommend addressing power dynamics directly, recognising for example, that post retrofit rent increases represent a social injustice that requires political intervention.
Furthermore, there are a number of overarching recommendations that could help support the sector at large, including the following:
• Create trusted provider frameworks, managed at local authority level, to improve quality, accountability, and market confidence.
• Support replicable, community based retrofit models, backed by local authorities, including mechanisms such as neighbourhood care and repair or retrofit panels.
POLICY RECOMMENDATIONS
Finance and governance
• Design funding mechanisms that embed contextual data and evidence, not just technical metrics.
• Develop a joined-up national cross sectoral strategy to address housing quality, linking health, housing, and energy policy rather than treating mould, cold, overheating, overcrowding, and poor ventilation as separate issues.
• Shift from individual building models towards place-based design, linking retrofit with resilience, public realm improvements, health outcomes, and insurance considerations.
PRACTICE, DELIVERY & POLICY RECOMMENDATIONS
Data and evidence
• Build towards a national system for post-intervention monitoring and health impact assessment, drawing on measured performance methods such as SMETER-HTC to assess real world outcomes.
• Mandate or incentivise place-based health assessments, including CHIAs, in retrofit programmes.
Knowledge and capacity
• Introduce targeted placement programmes, such as the Innovate UK Net Zero Living Programme, to embed retrofit and co-design expertise within local government and public sector teams, addressing persistent capacity gaps.
Partnerships and civil society
• Recognise third-sector organisations as core retrofit delivery partners whose work with vulnerable communities can support retrofit outcomes.
• Embed community anchor organisations in retrofit design and delivery to align programmes with local social, economic, and health priorities.
CONCLUSION: RETROFIT AS A FOUNDATION FOR HEALTHIER FUTURES
This paper has argued that retrofit will fall short of its potential if it continues to be treated primarily as a technical or property level intervention. While standards, funding, and delivery mechanisms matter, they are not sufficient on their own. What determines success in practice is how retrofit interacts with people’s lives, health, and the places they live.
The home is meant to be a place of restoration, of care, and of safety. Across the chapters, we have shown that housing conditions shape health in direct and cumulative ways, and that these impacts are unevenly distributed. Poor quality homes, insecurity, and exposure to environmental stressors are not experienced in isolation. They are shaped by place, by policy, and by long-standing structural inequities. Yet many existing policy tools flatten this reality, relying on abstract metrics, incomplete data, or assumptions about how homes are used.
A central theme of this paper is the need to rebalance retrofit policy towards outcomes that matter. Community Health Impact Assessments offer one way of doing this, by grounding decision making in lived experience and surfacing local realities that would otherwise remain invisible. Measured performance methods, including the use of sensor data, provide the material evidence needed to test whether interventions are actually delivering building performance improvements - or the conditions of healthier and more resilient homes. Together, these approaches shift the focus from assumed success to demonstrated impact.
The paper also highlights the importance of place-based thinking. Homes do not sit outside their social, economic, and environmental contexts. Retrofit outcomes are shaped by neighbourhood conditions, informal support networks, local capacity, and delivery ecosystems. Local authorities are therefore critical actors, not just as commissioners, but as coordinators of health led, place-based strategies that link housing, public health, community organisations, and supply chains.
At a national level, there is a clear need for greater policy integration. Housing quality, health, energy, and climate objectives are deeply connected, yet they are often addressed through fragmented strategies and narrow success measures. Expanding how success is defined, improving postintervention monitoring, and valuing contextual insight alongside technical performance are essential steps if retrofit is to reduce inequality rather than reinforce it.
Ultimately, this paper calls for a shift in how retrofit is understood and governed. From delivery to outcomes. From individual properties to places. From technical compliance to lived experience and health. Making this shift does not mean abandoning standards or data. It means using them differently, in service of homes that are safer, healthier, and more secure for the people who live in them.
If retrofit is to meet the scale of the challenge ahead, it must be designed not just to improve buildings, but to improve lives.
i) Case Study: Kirklees Warm Zones
Kirklees Warm Zones (2007–2010) was a pioneering area-based fuel poverty and energy efficiency initiative in West Yorkshire, unique for its cross-tenure model offering free loft and cavity wall insulation to all households in the borough, regardless of tenure, without means-testing. This approach removed administrative barriers and stigma associated with targeted schemes, enabling widespread uptake and social inclusion across different housing types.39
The programme was funded through blended funding, combining local council investment with external resources from energy company obligations (such as Scottish Power’s CERT contributions) and other grant streams. This blend reduced upfront costs for households and maximised scale and delivery efficiency.40 An Ulster University impact assessment highlighted that this inclusive, area-wide delivery improved thermal comfort and was likely to have positive effects on well-being and mental health, as residents experienced warmer homes and reduced fuel poverty stress.41
Kirklees Warm Zones demonstrated the value of an area-based, place-sensitive approach to delivery, and while impacts on comfort and well-being were identified through post-programme evaluation, the initiative also highlights the opportunity for future schemes to embed an ongoing, integrated feedback loop linking policy design, delivery, and real-world health and equity outcomes.
ii) Fishwick, Preston, Lancashire
The failed external wall insulation at Fishwick, and the subsequent misery of the people living in affected houses, is still regularly cited within the energy efficiency retrofit community as a cautionary tale of what can go wrong when good installation practice and a sense of care are lacking.42
“The work was part of the Community Energy Saving Programme (CESP), which aimed to improve energy efficiency in homes in the most deprived areas of the UK.
In 2013, 387 small, terraced houses in Fishwick built in 1900 had energy-efficiency measures installed as part of the programme. The main measures included solid wall insulation, with the installed external wall insulation expected to contribute almost half the total calculated savings.
The work was rushed due to existing installation targets and potential fines, resulting in a large portion being completed during the spring, increasing the risk of wet masonry. Many homes were in poor condition before the work, and there was a shortage of skilled labour.
A study found that the combination of poor workmanship, rushed deadlines, lack of previous maintenance and repair, and suboptimal weather conditions left residents in substandard conditions due to the retrofit work. The homes experienced severe issues with dampness, interior surface deterioration, black mould, and florid fungal growth. Plaster, furniture, and belongings were damaged in some cases, and some ceilings collapsed. Moisture retention within the external wall insulation led to humid and uncomfortable living conditions that had a detrimental impact on residents’ health (Selincourt, 2018).”43
The Fishwick case exposes the consequences of a systemic failure to integrate place-sensitive feedback between policy intent, delivery practice, and post-installation health and housing outcomes, with no robust mechanism to detect harm early or recalibrate the programme in response to emerging risks.
National Energy Action (NEA) implemented the Warm and Safe Homes in Fishwick project, addressing the consequences of failed insulation installations in Fishwick through resident engagement, property repairs, and support services.
REFERENCES
1. NRH, Improving Health and Housing Outcomes in the Private Rental Sector, https:// nationalretrofithub.org.uk/uk-must-commmit-to-a-10-year-retrofit-workforce-strategy-new-reporturges/, 2025
2. National Emergency Briefing, https://www.nebriefing.org/, 2025
3. UKHSA - 2023–2024 Health Effects of Climate Change (HECC) report, https://www.gov.uk/ guidance/health-effects-of-climate-change-hecc-report, 2024
4. CCC, Progress in adapting to climate change: 2025 report to Parliament, https://www.theccc.org.uk/ publication/progress-in-adapting-to-climate-change-2025/, 2025
6. Bhorkar et al, Improving survey-based data collection for more effective domestic retrofit evaluations, https://www.tandfonline.com/doi/ epdf/10.1080/09613218.2025.2540848?needAccess=true, 2025
7. National Audit Office, Energy Efficient Installations under the Energy Company Obligation, https://www.nao.org.uk/reports/energy-efficiency-installations-under-the-energy-companyobligation/?nab=1, 2025
8. NRH, State of the Nation, https://nationalretrofithub.org.uk/resource/retrofit-delivery-state-of-thenation-review/, 2024
10. Newham Borough Council, Just Transition Plan, https://www2.local.gov.uk/case-studies/ newham-councils-just-transition-plan, 2024
11. The Guardian, ‘It’s about quality of life’: Can Birmingham’s Retrofit House help fix the UK’s terrible housing?, https://www.theguardian.com/artanddesign/2025/nov/17/birmingham-retrofit-house-inladywood, 2025
12. NEPC, “Healthy, safe, sustainable buildings – maximising benefits in building retrofit“ https://nepc. raeng.org.uk/healthy-buildings?utm, 2024
13. Lomas et al, A domestic operational rating for UK homes: Concept, formulation and application, https://www.sciencedirect.com/science/article/pii/S0378778819308990, 2019
15. Crawley et al, Quantifying the measurement error on England and Wales EPC ratings, https://www. creds.ac.uk/publications/quantifying-the-measurement-error-on-england-and-wales-epc-ratings/, 2019
REFERENCES
16. Hanna, R., Simpson, K., Camacho McCluskey, K. and Gross, R. Accelerating energy efficiency retrofits in owner-occupied homes: An international review of good practice policies, The UK Energy Research Centre, https://ukerc.ac.uk/publications/accelerating-energy-efficiency-retrofits-in-owneroccupied-homes/ , 2025
18. NAO, The Warm Front Scheme, https://www.nao.org.uk/reports/the-warm-front-scheme/, 2009
19. NAO, Green Homes Grant Voucher Scheme, https://www.nao.org.uk/reports/green-homes-grant/, 2021
20. NAO, Green Deal and Energy Company Obligation, https://www.nao.org.uk/reports/green-dealand-energy-company-obligation/, 2016
21. NAO, Energy efficiency installations under the Energy Company Obligation, https://www.nao.org. uk/reports/energy-efficiency-installations-under-the-energy-company-obligation/,2025
22. Sudmant et al, Climate policy as social policy? A comprehensive assessment of the economic impact of climate action in the UK, https://www.research.ed.ac.uk/en/publications/climate-policy-associal-policy-a-comprehensive-assessment-of-the/, 2025
23. NRH, Place Based Retrofit: National Retrofit Hub Unveils New Project, https://nationalretrofithub. org.uk/place-based-retrofit-national-retrofit-hub-unveils-new-project/, 2025
24. Nelson et al, Housing inequalities: The space-time geography of housing policies, https://www. sciencedirect.com/science/article/pii/S0264275123005395, 2024
25. MHCLG, English Housing Survey 2023 to 2024: drivers and impacts of housing quality, https:// www.gov.uk/government/statistics/english-housing-survey-2023-to-2024-drivers-and-impacts-ofhousing-quality/english-housing-survey-2023-to-2024-drivers-and-impacts-of-housing-quality, 2025
26. Citizen’s Advice, Building Support, https://assets.ctfassets.net/ mfz4nbgura3g/2HIBTHUBNdh3KXJ2CekxJs/3a438fb481b8c6018c915a0f615af9b1/Building_Support__ Improving_consumers-_experiences_of_energy_efficiency_schemes.pdf, 2025
27. Wright, KJ, Resilient communities: Experiences of risk and resilience in a time of austerity, https:// eprints.whiterose.ac.uk/id/eprint/100549/3/Revised_resilience_risk.pdf, 2016
28. The Centric Lab, Place & Health, https://www.thecentriclab.com/research-archive/place-andhealth
29. DuBois, W.E.B, The Philadelphia Negro: A social study, https://www.jstor.org/stable/j.ctt3fhpfb, 1996
30. Sapolsky, R. M, Determined: A Science of Life Without Free Will, Penguin Press, 2023
31. WHO, Constitution of the World Health Organization, https://www.who.int/docs/default-source/ documents/publications/basic-documents-constitution-of-who.pdf, 2006
REFERENCES
32. East Sussex Director of Public Health, Health and Housing 2019/20, https://www.eastsussexjsna. org.uk/resources/annual-public-health-report-2019-20-health-and-housing/, 2020
33. The Centric Lab, Place & Health, https://www.thecentriclab.com/research-archive/place-andhealth
34. The Centric Lab, An Ecological Definition of Health Through the Stress Response, https://www. thecentriclab.com/research-archive/an-ecological-definition-of-health-through-the-stressresponse
35. Middlemiss, Davis, et al, Rethinking retrofit: Relational insights for the design of residential energy efficiency policy, https://ukerc.ac.uk/publications/rethinking-retrofit-relational-insights-for-the-designof-residential-energy-efficiency-policy/, 2025
36. Centric Lab, Community Health Impact Assesment Toolkit, https://www.thecentriclab.com/chia/ community-health-impact-assessment-toolkit, 2025
37. WHO, Health Impact Assessment, https://www.who.int/health-topics/health-impactassessment#tab=tab_1
38. LGA & Public Health England, Local well-being, local growth, https://assets.publishing.service.gov. uk/media/5a806d9840f0b62302693733/Health_in_All_Policies_overview_paper.pdf, 2016
39. Memorandum submitted by Kirklees Council, Kirklees Energy Services and Kirklees Warm Zone (EEFP 47), https://publications.parliament.uk/pa/cm200809/cmselect/cmenvfru/37/9011412.htm?utm_, 2009
41. University of Ulster, “Kirklees Warm Zone - The project and its impacts on well-being”, https://pure. ulster.ac.uk/ws/files/11261680/KIRKLEES_PROJECT_and_COST_BENEFIT_REPORT.pdf , 2011
42. National Energy Action, Warm and Safe Homes in Fishwick, https://www.nea.org.uk/wp-content/ uploads/2025/06/Rebuilding-Trust-Learnings-from-Fishwick.pdf, 2025
43. Historic England, When Retrofit Goes Wrong, https://historicengland.org.uk/research/heritagecounts/heritage-and-environment/introduction-to-retrofitting/when-retrofit-goes-wrong/, 2024