










Welcome to the inaugural e-issue of The Ventilator. For the first time in MSA history, we are no longer mailing a print version. This format mirrors the modern evolution of our specialty, our membership and the world around us. While technology is undeniable, however, so too are our human connections. This issue retains the tradition of the print versions before it, continuing to remind that we stand stronger together — in service of our specialty, our patients and our communities. Enjoy the read and please send us your feedback. Don’t forget to save the date for another first ever event: GLAM 2026 — celebrating our collective strength in the Great Lakes region. Another step in MSA’s commitment to navigate our landscape with strategic advocacy and member services/ connections to support careers at all stages. See you in the Windy City!
Warmly, Neeju Ravikant, MS, MD
PRESIDENT
Matthew Dellaquila, MD, MBA, FASA
PRESIDENT-ELECT
David Salama, DO, MBA, FASA
SECRETARY-TREASURER
Paul Polyak, MD, FASA, FASE
IMMEDIATE PAST PRESIDENT
Michael Lewis, MD, FASA
MANAGING EDITOR
Neeju Ravikant, MS, MD
FOR ADVERTISING CONTACT
Hillary Walilko, CAE
Phone: 517.346.5088
Fax: 517.371.1170
Email: walilko.h@gcsionline.com

AMatthew Dellaquila, MD, MBA, FASA President, Michigan Socity of Anesthesiologists
Together, we are advancing a vision of anesthesiology that is not only strong today but secure for tomorrow.
s we approach the end of the year, I’ve been reflecting on what makes both our specialty and our society resilient. Michigan anesthesiologists face the same national pressures — staffing shortages, reimbursement challenges, and ongoing debates over scope of practice. My predecessor, Dr. Michael Lewis, often reminded us of the saying, “May you live in interesting times,” a phrase that feels especially fitting now. Since stepping into the role of MSA President in midSeptember, I’ve experienced just how “interesting” these times are. On Sept. 11, West Michigan Anesthesia and MSA members, including myself, held a joint press conference on truth and transparency in anesthesiology, which drew statewide media attention in the days that followed. Soon after, the Michigan College of Emergency Physicians released a statement suggesting emergency physicians were qualified to deliver general anesthetics — an assertion we strongly challenge and continue to work with our national colleagues on strategies to address.
Alongside this, MSA continues to support several key pieces of legislation and offer CME programs with nationally recognized speakers. Your membership has never been more vital, and I am deeply grateful for your continued support and commitment to strengthening our society.
If you have a lot of passion and want to take a stronger role in what MSA does and what the society can offer in the future, join a committee! Run for an elected spot! We need you to be engaged now more than ever. Practice Management, Vanguard, Medical
Students and Residents, Government Affairs, and Communications are all seeking passionate members to get more involved in our committees. Our society is only as strong as the engagement of its members, so if you’d like to learn more, contact us (admin@mymsahq.org) to get more involved.
This fall, I am proud to share highlights of the progress we have made together:
Earlier this year, our public awareness campaign brought anesthesiology into the public eye with a billboard and digital ads in West Michigan. These efforts reminded patients and policymakers that anesthesiologists are the physicians uniquely trained to safeguard them during their most vulnerable moments.
We have also stepped forward to address scope of practice challenges directly. Reports from across the state have raised concerns about the substitution of non-anesthesiologist providers in roles that demand our expertise. While we value all members of the care team, MSA has consistently affirmed that patient safety is best protected when anesthesiologists lead anesthesia care. We will continue to work tirelessly on this troubling development and are committed to ensuring the practice of anesthesiology is led by an anesthesiologist.

One of the most exciting developments has been the launch and growth of our Vanguard Committee. Designed to bring early-career anesthesiologists into the heart of MSA’s work, the committee is already building momentum. Our Vanguard members bring fresh ideas, new perspectives, and an eagerness to ensure that anesthesiology in Michigan thrives for decades to come. Their energy is contagious, and I have no doubt they will become some of our most effective advocates and leaders.
Equally exciting is the soon-to-be-revamped Medical Student Section of MSA. For years, we have seen growing interest among medical students in understanding the role anesthesiologists play — not just in the operating room, but across the continuum of care. This new section will provide mentorship, educational opportunities, and a formal voice for medical students within MSA. By investing in this next generation, we are building the pipeline of leaders who will carry our specialty forward.
Education has always been at the heart of MSA’s mission. This year, we worked with the Michigan State Medical Society (MSMS) to ensure the Specialty Network Access Fund was distributed to eligible programs when members sounded the alarm on late disbursements. By allocating funds fairly and effectively, MSA is helping advance the shared goal of ensuring access to care and assuring the future viability of anesthesiology.
In parallel, we are also investing in the professional infrastructure that our members need. One of the most significant developments is the rejuvenation of the MSA Practice Management Committee. This committee, formed with leaders from both private practice and academic medicine, will serve as a hub for information, strategy, and shared problem-solving. Topics such as contracting, payer negotiations, and workforce dynamics are increasingly critical to the viability of anesthesia practices in Michigan. By formalizing a venue for these discussions, we are equipping our members to succeed in a rapidly changing environment.
Even as we take on these new initiatives, we have much to celebrate. Our 2025 Annual Conference in Grand Rapids was a resounding success, bringing together anesthesiologists, residents, and trainees from across the state. The engagement and exchange of ideas affirmed that MSA is a true community, united by shared purposes.
We also participated in the ASA Day of Contributing (DoC), once again demonstrating that anesthesiologists are committed not only to patient care, but also to the communities we live in. Michigan ranked 4th in the total amount of money raised and 3rd in the number of donors nationally. From volunteerism to philanthropy, MSA members showed the depth of compassion that defines our profession. Looking ahead, I am especially excited for the Great Lakes Anesthesia Meeting in downtown Chicago. This gathering is quickly becoming one of the premier regional events in anesthesiology, and Michigan anesthesiologists are at the center of its success. I hope many of you will join us for what promises to be an inspiring and energizing meeting.
MSA has been recognized by national leadership at ASA multiple times — winning a national award for our advocacy, being awarded grants to support our work, and being recognized in the ASA Monitor. Our leaders have been elected to ASA executive council positions, sit on the board of directors, and have been invited to join thought leader committees. Very few of us entered MSA this way. It’s the mentorship, experiences, and fellowship that have led to that success — and what awaits you when you’re ready to jump in!
The coming months will not be without challenges. Questions of scope, reimbursement, and workforce are not going away. But if the past year has proven anything, it is that anesthesiologists in Michigan are ready — ready to innovate, ready to advocate, and ready to protect both our patients and our profession.
The work of MSA is not done by any one individual. It is carried by the collective efforts of every member — whether you attended a conference, mentored a student, wrote to a legislator, or simply renewed your membership. Together, we are advancing a vision of anesthesiology that is not only strong today but secure for tomorrow.
I also want to close on a note of personal gratitude. I stand on the shoulders of giants, and it’s only through them that our society functions as well as it does. Drs. Lewis, Neeju Ravikant, Roy Soto, John LaGorio, and Tom George have all provided counsel to me on these issues, and we are all indebted to them. Many of the structures they built and the foresight they had are still serving us well today. It’s through that foundation we can work towards a better future for our society. I’d also be remiss if I didn’t thank my other fellow officers, Drs. David Salama and Paul Polyak for their hard work and steadfast support as we navigate the future.
MSA and anesthesiologists who practice at Corewell Health West sounded the alarm on Sept. 11 with a joint press conference about a growing trend in healthcare: removing board-certified anesthesiologists from surgeries and procedures and replacing them with doctors whose primary training is in other specialties or other providers.
“I have seen Corewell West replace anesthesiologists with emergency medicine and intensive care unit doctors, particularly for endoscopy procedures like colonoscopies, and they are not always informing patients,” said Dr. Kathryn Wladischkin, an anesthesiologist and president of West Michigan Anesthesia (WMA). “While my physician colleagues are highly trained doctors, they lack the expertise that uniquely qualifies anesthesiologists to manage challenges to a patient’s airway and other complications that could occur during or after anesthesia.”
During the press conference, MSA warned patients about the dangers that come with this change and encouraged them to ask questions about the medical professionals administering their anesthesia during surgery and procedures.
“Anesthesiologists are the physicians in charge of keeping patients safe when they are under anesthesia, and if a
patient flatlines, has a seizure, heart attack or stroke during surgery, it’s the anesthesiologist who leads the team to save the patient’s life,” said Dr. Matt Dellaquila, MSA president. “Every patient should ask clearly: ‘Will a board-certified anesthesiologist be part of my care team?’ That question can protect lives.”
To amplify this message, MSA launched a billboard and digital campaign in West Michigan reminding patients of their right to transparency.
“Any attempt by hospitals and healthcare providers to remove anesthesiologists from overseeing the delivery of anesthesia puts a patient’s life at additional, unnecessary risk,” said Dr. David Salama, MSA president-elect. “Patients have a right to expect the very best healthcare provider to oversee their care while under anesthesia, and they have the right to know exactly who is providing their care and what qualifications their providers have. Transparency is essential to trust, and trust is essential to safety.”
MSA also warned against the misconception that removing anesthesiologists reduces costs. In most cases, patients are billed the same rate for anesthesia services regardless of who leads the team.

John LaGorio, MD, MBA, FASA Director, Michigan Socity of Anesthesiologists
More than 10,000 anesthesiologists gathered for the world’s largest meeting of anesthesia professionals at the annual American Society of Anesthesiologists (ASA) meeting Oct. 10-15. Bringing together clinicians, thought leaders, and researchers, ANESTHESIOLOGY 2025 offered a robust platform for advancing our field through education, networking, and cutting-edge innovations. Key themes included leveraging data-driven insights, navigating emerging technologies, enhancing patient safety, and addressing critical practice management issues. Here are a few highlights.

Keynote: The keynote was delivered by Dr. Lucy Kalanithi, widow of neurosurgeon Dr. Paul Kalanithi, author of the memoir When Breath Becomes Air. Her address offered a powerful reflection on her husband's life and legacy, urging attendees to find deeper meaning and empathy in patient care. This set a tone of humanism that resonated throughout the meeting.
Rovenstine Memorial Lecture:
Michigan’s own Dr. Sachin Kheterpal took center stage to deliver this year’s installment of the prestigious lecture. “Anesthesiologists as Leaders in a Data Driven World” highlighted the increasing importance of leveraging data and technology for clinical excellence. His insights provided a roadmap for anesthesiologists to take a leading role in a healthcare landscape shaped by large-scale datasets.
Severinghaus Lecture: Focusing on the human element of medicine, Dr. Joyce Wahr’s talk, “It's Not Your Fault! The Cognitive Basis of Error,”
explored the psychological factors behind medical errors. By examining the cognitive underpinnings of mistakes, she provided a crucial perspective on ways to improve patient safety culture and foster a more empathetic environment for practitioners.

This year’s educational opportunity was expansive, featuring hundreds of sessions and workshops across 11 clinical tracks, including dedicated content on:
Perioperative Medicine: Much focus was placed on optimizing patient care throughout the surgical process, with sessions exploring topics like risk assessment, perioperative medication management, and enhanced recovery after surgery (ERAS). Several sessions reviewed new guidance in care for geriatric patients and cardiac evaluation.
The role of artificial intelligence and new technologies were prominent themes. Attendees explored potential applications, from improving practice efficiency to enhancing patient monitoring.
Point-of-Care
(POCUS): Hands-on workshops and numerous sessions explored the expanding utility of POCUS for diagnostic and procedural applications in the perioperative setting.
Recognizing the demands on modern anesthesiologists, the program included a strong emphasis on practice management, business strategies, and physician wellness.
Leadership and Advocacy: Sessions focused on management strategies and advocacy, empowering attendees to become leaders within their institutions and on Capitol Hill.
Acknowledging the ongoing challenges facing the profession, the meeting addressed topics related to workforce shortages and strategies for practice sustainability.
In addition to the above, the annual meeting serves as the venue for the governance activities of the Society. This year’s delegation consisted of roughly two dozen elected Michigan delegates, alternates, and directors representing Michigan’s voice to the direction and activities of the ASA. This includes operational topics as well as approval of guidance and statement documents that help to establish common platforms of care within the field of anesthesiology. These efforts help us all to work with our colleagues and partner facilities to provide the best anesthesia care as is currently known.

ANESTHESIOLOGY 2025’s success underscores the value of in-person connection, while the virtual options ensure that its educational reach extends far beyond the convention center. As attendees return to their practices, they carry with them new knowledge, strengthened professional networks, and a renewed sense of purpose, ensuring that the specialty continues to thrive and innovate. If you missed this year’s meeting — no worries — ANESTHESIOLOGY 2025 OnDemand is available, which contains more than 200 recorded lectures and other content from the meeting, including CME credit.
Finally, please mark your calendars to consider joining us next year for ANESTHESIOLOGY 2026 in San Diego, California, Oct. 16-20. I look forward to seeing you there. I heard it will be sunny and 75 degrees!

Paul Polyak, MD, FASA, FASE Chair, CME Committee
The Michigan Society of Anesthesiologists had a one-of-a-kind meeting in Grand Rapids this Sept. 12-14. Anesthesiologists from across the state along with residents and medical students were in attendance to socialize, make connections, present their research, and partake in the educational offerings.
The conference kicked off with a fun-filled reception at the Ashton Lounge sponsored by West Michigan Anesthesia. Saturday started with an informative session on perioperative ICD management by Scott Strekenbach, MD, from Massachusetts General Hospital, followed by workforce updates by Ronald L. Hart, MD, FASA, ASA’s immediate past-president. The day continued with practical tips on managing discomfort during a caesarean section by Melanie L. Darke, MD, from Henry Ford St. John Hospital. Bassam Kadry, MD, from Standford University School of Medicine, gave a thought-provoking talk on how we can adapt to a changing world. Consolidating systems, payer cuts, and AI were all discussed during this riveting session. Subsequently, Kentan Chopra, MD, from Henry Ford Health, provided a summary on the most recent guidelines for the management of perioperative nausea and vomiting.
Resident and medical student poster sessions were an opportunity for learners to showcase their work,


and they came out in force. Eighty residents and students attended the conference this year. Roy Soto, MD, FASA, from Corewell Health, NorthStar Anesthesia, put together our first Resident Jeopardy, which was a big hit with the participants and the audience. The day concluded with a fantastic dinner featuring a live jazz band.
The conference concluded on Sunday with the whole morning dedicated to point of care ultrasound (POCUS) skills. Models and instructors were available to teach cardiac, lung, gastric, and FAST exams. The session was led by Eric Reilly, DO, from Corewell Health, NorthStar Anesthesia, with John Mitchell, MD, from Henry Ford Health, Michigan State University College of Human Medicine, who helped participants experience virtual reality learning.
Join us next year as we break new ground by joining three other state societies for the first Great Lakes Anesthesiology Meeting in Chicago, Aug. 29-30. It will be GLAMorous!


Las Vegas, NV JAN

TERIC REILLY, DO Chair, Committee on Governmental Affairs
Despite our victories, the field of anesthesiology faces great change.
hank you to those who have donated their time, energy, and money towards our legislative endeavors over the past year. Thanks to a strong MSAPAC fundraising year and widespread engagement from MSA members, we have rallied support for our causes from politicians at both the national and state levels. It’s commonplace for lawmakers to remark, “We love our anesthesiologists,” during our meetings. Below are some of our 2025 key accomplishments and ongoing efforts as we remain committed to protecting your patients and your practice.
• Defeated dangerous Tort Law reform which would have inflated costs of malpractice insurance (HB 6085).
• Secured bipartisan congressional sponsorship for the recently introduced bill supporting Certified Anesthesiologist Assistant Licensure in Michigan (HB 4832, SB 428).

• Continue to battle the dangerous bill which could expand nurse practitioner scope of practice (HB 4399, SB 268).
• Working alongside other state medical societies to promote Truth and Transparency legislation to ensure patients know exactly who is providing care in clinical settings.
Despite our victories, the field of anesthesiology faces great change. In Michigan, we’ve seen widespread funding cuts, licensure battles, and shifts in anesthesia care models. Nationally, those same themes are compounded with commercial insurer battles, Medicare rates, and the No Surprises Act. As your Governmental Affairs team, we will continue to anticipate and legislatively manage such changes to

best support our profession and our patients. Our abilities depend on the strength of both ASAPAC and MSAPAC
If able, please consider donating to the ASAPAC and MSAPAC. If you are unable to make a financial donation, consider donating your time. We are always looking for driven MSA members to engage with state and national lawmakers at various fundraisers and conferences, such as the ASA Legislative Conference in Washington, D.C. Change is inevitable. With your help, we can steer it properly.

We are nearly halfway through the 103rd Michigan Legislature, and the split control of government has proven to be a significant obstacle in advancing legislative priorities. Democrats maintain control of the Michigan Senate while Republicans hold the majority in the Michigan House.
Upon taking control, House leadership under Speaker Matt Hall expanded the authority of the Oversight Committee, granting it broad subpoena power over matters ranging from child welfare and public health to economic development spending. In contrast, the Senate made transparency its first priority, passing legislation to bring the Governor’s office and the Legislature under the Freedom of Information Act (FOIA), which has long been considered a symbolic reform target in Lansing.
Despite these early moves, overall legislative productivity has been low, with only a limited number of bills enacted to date. Earlier this year, lawmakers were forced to prioritize a fix to minimum wage and paid sick leave statutes following a court decision, adjusting implementation timelines to avoid disruption for employers.
The tone of the session continues to reflect a pushand-pull between aggressive oversight and entrenched policy gridlock. The House has positioned itself as an accountability check on the executive branch, while the Senate has focused on structural reforms tied to transparency and public access.
The split government also led to a drawn-out Fiscal Year (FY) 2025–26 budget process. Lawmakers were forced to adopt a temporary continuing resolution on the evening of Oct. 1 to avert a government shutdown. Negotiations
centered heavily on a long-term road funding framework, a shared priority of both Gov. Whitmer and House Republicans. A final agreement was reached in the early morning hours of Oct. 3, dedicating $1.85 billion in ongoing revenue specifically for road improvements.
Importantly, $3 million for general anesthesia in dental procedures was restored in the final budget after the House initially attempted to eliminate it. This continues the Medicaid reimbursement support structure from previous cycles, maintaining minimum reimbursement rates of $1,495 for services in ambulatory surgical centers and $2,300 for outpatient hospital settings.
We continue to push back against the expansion of nurse practitioner scope of practice under Senate Bill 268 and House Bill 4399, in partnership with other specialty medical organizations. These bills have not yet moved out of committee in their respective chambers, and that’s the way we would like it to remain. Advancing “Truth and Transparency” and securing licensure for Certified Anesthesiologist Assistants (HB 4832, SB 428) remain top priorities. We have secured bipartisan support for the licensure legislation and are actively working to secure committee hearings in both chambers this fall. A “Truth and Transparency” bill is expected to be introduced in the House in the coming weeks, and we are prepared to offer our full support.
Looking ahead, the extent to which legislative leaders are willing to engage in genuine bipartisan negotiation will determine whether this session ends as one of the most gridlocked in Michigan’s history, or whether meaningful policy gains can still be achieved.
John Ghanem, MD, and Jack Dillon, MBA, MSHR Practice Management Committee Co-chairs
Across Michigan, anesthesiology practices are confronting a period of rapid transition. Traditional hospital employment models are under financial stress, independent practices face growing payer consolidation, and anesthesiaspecific reimbursement remains one of the most undervalued in healthcare. Despite these pressures, Michigan’s anesthesiologists have continued to demonstrate resilience, creativity, and leadership — innovating new structures that preserve both clinical excellence and professional autonomy.


MSA has an essential role to play in this evolution. Practice management is no longer just a matter of billing and compliance — it is the foundation of stability, equity, and practice sustainability. From private practices to large academic departments, governance models that empower our teams and align incentives are emerging as the defining factor in longterm success. Transparent governance, physician-led decision-making, and strong communication channels have proven to create cohesive, adaptive organizations capable of navigating payer and health system challenges.
Reimbursement advocacy remains equally critical. Michigan’s anesthesia groups are uniquely affected by regional payers, whose conversion factors lag behind national averages, despite rising clinical costs.
Addressing these inequities requires data-driven negotiation. MSA’s platform should amplify this effort by supporting members with access to data, contract education, and collaborative discussions with payers and policymakers.
The path forward depends on collaboration. Whether in hospital-based departments, office-based practices, or emerging hybrid models, anesthesiologists must shape the future of their profession rather than react to it. Through education, advocacy, and shared experience, MSA can help ensure that every anesthesiologist in the state — regardless of practice type — has the tools to thrive in a changing healthcare environment.

MS2, Oakland University William Beaumont School of Medicine
Midazolam, a short-acting benzodiazepine, has long been used for anxiolysis and amnesia in the perioperative setting. However, its use in elderly patients warrants careful reconsideration. Numerous studies have highlighted the increased sensitivity of older adults to benzodiazepines. Aging significantly alters the pharmacodynamics and pharmacokinetics of sedative agents like midazolam. Reduced hepatic and renal clearance can prolong drug half-life and increase the accumulation of active metabolites. Additionally, age-related changes in body composition — such as increased fat-to-lean mass ratio and decreased total body water — expand the volume of distribution for lipophilic drugs, leading to prolonged sedation. Compounding this, diminished neuroplasticity and altered GABA receptor sensitivity in the aging brain heighten susceptibility to cognitive impairment, delirium, and paradoxical agitation. These factors underscore the importance of dose reduction and careful monitoring in elderly patients.
The American Geriatrics Society’s Beers Criteria lists benzodiazepines as potentially inappropriate medications for older adults due to their association with cognitive impairment, falls, and fractures. Midazolam, in particular, has been implicated in delayed emergence and increased PACU length of stay in elderly surgical patients. A 2020 study in Anesthesia & Analgesia found that benzodiazepine use in patients over 65 was independently associated with higher rates of postoperative delirium and unplanned ICU admissions.
Further reinforcing these concerns, the STOPBenzo trial (Sedation and Delirium Prevention with Benzodiazepine Avoidance) demonstrated that avoiding benzodiazepines in older surgical patients significantly reduced the incidence of
Aging significantly alters the pharmacodynamics and pharmacokinetics of sedative agents like midazolam
postoperative delirium and improved early recovery metrics. This multicenter, randomized trial adds high-quality evidence to the growing consensus that benzodiazepines should be minimized or avoided in this population whenever possible.
Despite these concerns, internal data from our institution reveal that midazolam is used 7% more frequently in elderly patients compared to peer surgical hospitals. This discrepancy suggests an opportunity for improvement in our prescribing practices. While anxiolysis remains an important goal, alternative strategies such as verbal reassurance, regional anesthesia, or low-dose dexmedetomidine may offer safer options with fewer adverse effects.
We encourage all providers to critically assess the necessity of midazolam in elderly patients and consider age-appropriate alternatives. When benzodiazepines are deemed necessary, dose reduction and close monitoring are essential. By aligning our practice with current evidence and national benchmarks, we can enhance patient safety and improve outcomes for our older surgical population.
1. American Geriatrics Society Beers Criteria Update Expert Panel. J Am Geriatr Soc. 2019.
2. Deiner S, Silverstein JH. “Postoperative delirium and cognitive dysfunction.” Br J Anaesth. 2009.
3. Neufeld KJ et al. “Benzodiazepines and risk of delirium.” Anesth Analg. 2020.
4. Neuman MD, Feng R, Shukla AS, et al. Strategies to Limit Benzodiazepine Use in Anesthesia for Older Adults: A Randomized Clinical Trial. JAMA Netw Open. 2024.
Membership Committee Co-chairs
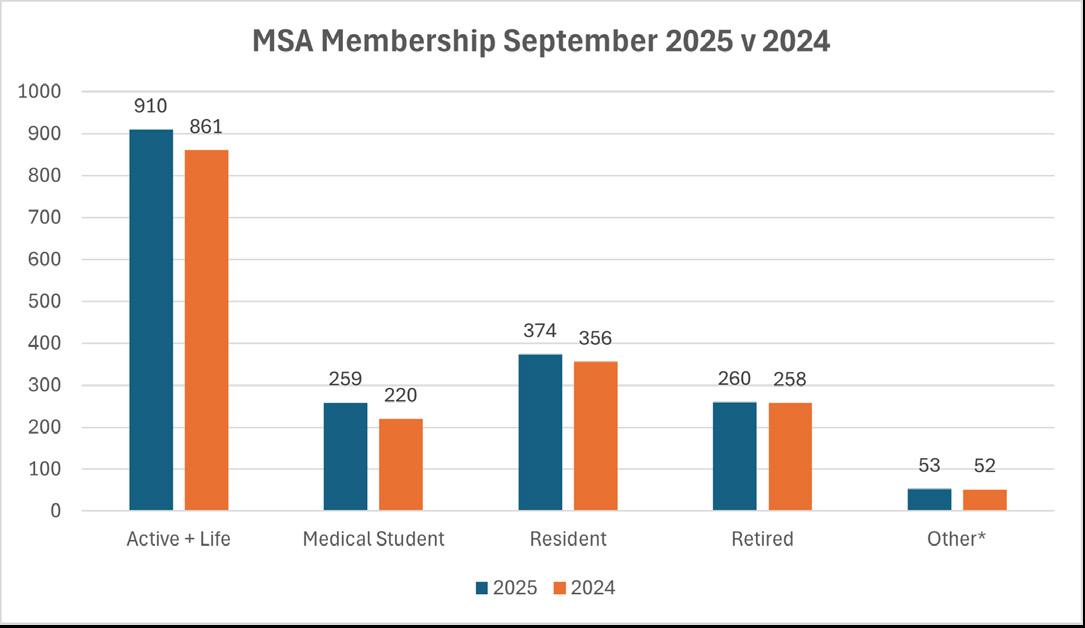
As we enter the final quarter of 2025, the Michigan Society of Anesthesiologists (MSA) is pleased to share encouraging updates on membership growth and engagement. Despite the challenges of a rapidly changing practice environment, our organization continues to see strong renewal activity and steady gains across multiple segments.
• Active renewals are 5% higher in 2025 when compared to the same period last year
• All categories of membership have increased compared to this time last year
MSA’s membership has already surpassed this year’s goal of 900 active members, with steady growth particularly among residents, medical students, and early-career physicians.
• Early-career physicians continue to be one of our strongest growth areas, reflecting successful engagement with new graduates.
• Residents and medical students together represent more than 600 members, an important future pipeline for active membership.
• Retired members remain a key part of our society, contributing experience, continuity, and mentorship.
The ASA 2025 membership survey provides valuable context:
• Satisfaction: A majority of MSA members report being satisfied or extremely satisfied with the society and its offerings
• MSA members report the following offerings to be the most valuable:
• Advocacy
• Education
• Networking
With our 2025 membership goal already surpassed, the focus turns to The Thousand Strong Campaign. Over the next two years, we hope to surpass the 1,000-member threshold. This goal will help strengthen our voices at the state and national level, as well as improve our value and offerings to individual members. We hope to achieve this goal by focusing on member retention and satisfaction while continuing to enhance member offerings.
MSA’s strength lies in its diverse membership base, spanning students to retirees. We invite all MSA members to participate in The Thousand Strong Campaign by encouraging colleagues to join and sharing the value you receive from MSA. Together, we have a stronger voice for both our patients and our profession.
After earning her medical degree from Wayne State University and completing her residency at Vanderbilt University Medical Center, Dr. Jamie Pendy knew one thing for certain: Michigan was calling her home. In July 2023, she and her husband answered that call — leaving the bustle of Nashville for the tight-knit community and outdoor paradise of Michigan’s Upper Peninsula.
Now an anesthesiologist at UP Health SystemMarquette, the region’s largest hospital and only Level II trauma center, Dr. Pendy has found that rural medicine brings both immense rewards and profound responsibility.
“We’re taking care of our community,” she said. “Our patients are our neighbors. There’s a strong sense of community investment and connection here.”
As the medical hub for the Upper Peninsula, UPHSMarquette receives transfers from hospitals across hundreds of miles. While it doesn’t have all the resources of a large tertiary center, it delivers highacuity care for some of Michigan’s sickest patients. In this environment, physician leadership is crucial.
“Despite being relatively small, the hospital handles many complex cases,” Dr. Pendy noted. “Our patients value receiving care locally, and we take pride in providing high-quality, safe care here in Marquette.”
In rural healthcare, the temptation can be to substitute non-physician providers in the name of cost savings or access. However, this approach can have the opposite effect, leading to fragmented care, more patient transfers, and higher downstream costs. The team-based approach to anesthesia plays a crucial role in preventing these inefficiencies, ensuring that patients receive the right care, in the right setting, the first time.
Rural hospitals face inherent challenges: recruiting specialists, maintaining coverage, and containing costs while serving wide geographic areas.
“Access to subspecialists can be limited,” Dr. Pendy said. “That makes it vital for physicians to captain the care team and make sound, evidencebased decisions that optimize outcomes and conserve scarce resources.”
As a rural medicine physician, Dr. Pendy often encounters patients with minimal prior engagement with the healthcare system. “The preoperative workup can be somewhat limited,” she said. “One of our roles is to perform a comprehensive evaluation to make sure patients are optimized and that no additional workup is needed before surgery.”
This reality has reinforced her appreciation for the collaborative, community-focused approach at UP Health System-Marquette, where the whole team works to optimize patient outcomes with the available resources.
For Dr. Pendy and her husband, a hospitalist at the same institution, life in Marquette has proven deeply fulfilling — both professionally and personally. The supportive community, the autonomy of rural practice, and the proximity to nature have made the UP an ideal place to practice medicine and raise their daughter.
“It’s very different from where we used to live and work,” Dr. Pendy reflected, “but it’s hard for us to imagine being anywhere else.” Pendy
MD MSAPAC Co-chairs
As 2025 comes to a close and we approach the holiday season, we would like to take a moment to share what the Michigan Society of Anesthesiologists Political Action Committee (MSAPAC) has accomplished this year on your behalf. Every day, MSAPAC works to represent anesthesiologists across Michigan by listening to your concerns, engaging with lawmakers, and advocating for policies that protect patients and strengthen physician-led care — both locally and nationally.
MSAPAC is a member-funded organization, and the progress we’ve made this year has been possible only through your continued support and participation. From advocacy events to direct engagement with legislators, your contributions have made a meaningful difference for our specialty and our patients.

We began the year with strong momentum during our annual Day of Contributing on March 31. More than 170 Michiganders donated that day, and more than 700 supporters contributed throughout the year to advance anesthesiology advocacy on both state and national levels. We are especially proud of the Corewell Health Royal Oak and Henry Ford Health St. John residency programs, which achieved 100% resident participation — an effort recognized nationally at the 2025 ASA Anesthesiology Annual Conference.

At the state level, MSAPAC maintained an active presence in Lansing, monitoring and responding to legislative proposals that could impact anesthesiology practice. We worked diligently to prevent measures that expand scope of practice without appropriate training, countered abusive insurance practices, and promoted policies that safeguard patient safety. Collaboration with partners like the Michigan State Medical Society continues to strengthen our shared mission of advancing physician-led, high-quality patient care.
Nationally, through our partnership with ASAPAC, we have supported ongoing initiatives addressing title misappropriation, abusive insurance practices, and scope creep—issues that have significant longterm implications for our profession. These efforts
help ensure that anesthesiologists remain the recognized leaders in perioperative medicine and patient safety.
Another key focus of MSAPAC’s advocacy this year has been patient awareness. We launched initiatives through local media and billboard campaigns emphasizing that every patient deserves to have a qualified anesthesiologist caring for them during procedures and surgeries. By empowering patients with knowledge about who provides their anesthesia care, we reinforce transparency, safety, and trust in the healthcare system.
As co-chairs of the MSAPAC, we want to express our sincere gratitude to everyone who contributed, attended events, or supported advocacy efforts this year. Your engagement —whether through donations, participation, or outreach — directly strengthens our collective voice. We also want to thank the residents who joined us for this year’s ice cream events at Corewell Health Royal Oak and Henry Ford St. John; your enthusiasm inspires us to continue this important work.
Looking ahead to 2026, we anticipate new legislative challenges that will directly affect anesthesiology practice across Michigan. MSAPAC will remain steadfast in advocating for safe, physician-led anesthesia care and ensuring that your professional interests are represented at every level.
We encourage you to stay involved. Please continue to donate, participate, and reach out to the MSA and ASA PACs with your ideas and concerns. Together, we can ensure that anesthesiologists’ voices remain strong in shaping the future of healthcare in Michigan.
Anesthesiology of Marquette MSA Vanguard Committee
The Michigan Society of Anesthesiologists is proud to announce the creation of the Medical Student Section. The goal of this new section is to attract future anesthesiologists to MSA, expand their involvement in organized medicine, and help shape student-centered initiatives within MSA.
In recent years, there has been a marked increase in medical students’ interest in anesthesiology and engagement in MSA. In fact, more than 50 medical students attended the 2025 Annual Conference in Grand Rapids. Many of these students also presented posters. In response to this enthusiasm, the Vanguard Committee has collaborated with a few dedicated medical students to create a space within the MSA specifically focused on student members.
MSA's Medical Student Section will work to increase opportunities for mentorship, research, and advocacy, providing students with the tools and networking necessary to thrive in the field of anesthesiology.
MSA has been actively reaching out to medical students across Michigan to better understand their interests and goals and how it can best support them on their educational and professional journeys.
Stay tuned for more upcoming events, leadership opportunities, and other ways to get involved!
Wissam Maroun, MD and Arun Marimuthu-Kala, MD
Henry Ford Hospital, Department of Anesthesiology, Pain Management & Perioperative Medicine
Anesthesiologists become intubation experts incidentally — after all, these tricky procedures are not at the top of the list on the anesthesiologist’s job description. But the anesthesiologist’s ability to safely intubate patients within a range of critical care sites outside the operating room is, in fact, a critically important element of the profession. In emergent situations, such as in the intensive care unit (ICU), physicians may need to perform difficult intubations; however, in these critical situations, an anesthesiologist with more experience in securing a wide range of airways may have a higher likelihood of first pass success.
Studies of airway management in critical care environments have revealed the difficulty of intubation under emergent conditions and the need for specialized expertise:
• One study found that the ICU involved more challenging intubation conditions and that first pass intubation success rates were lower in the ICU than in the operating room.1
• A Mayo Clinic study showed an almost 90% first pass intubation success rate for anesthesia specialists in the ICU.2
• The international INTUBE study found that anesthesia as the primary specialty of the intubator was independently associated with a higher firstpass success rate. In this cohort, the overall first pass success rate was almost 80%. Notably, use of video laryngoscopy and neuromuscular blockade further improved success rates.3
But importantly, the INTUBE study also observed substantial rates of peri-intubation adverse events in critically ill patients:3
• About 45% of patients experienced at least one major adverse peri-intubation event.
• Cardiovascular instability was observed in 43% of patients.
• Severe hypoxemia was observed in 9% of patients.
• Cardiac arrest was observed in 3% of patients.
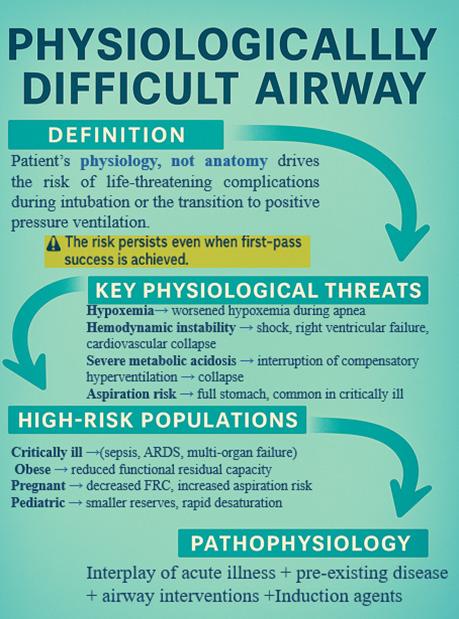
So, the question arises: If the first-pass intubation rates were high, why did so many patients have peri-intubation complications? The answer is simple: Critically ill patients in the ICU who require airway interventions often have what is called a “Difficult Airway.” They are “difficult” not in the traditional sense of involving challenging anatomy, such as subglottic stenosis or airway tumors, but rather “difficult” due to underlying physiological conditions that create a high-risk environment for airway manipulation, such as hypoxemia, metabolic dysfunction, or hemodynamic instability (Figure 1).
Overall, patients with physiologically difficult airways have a higher risk of life-threatening complications during intubation or transition to positive pressure ventilation.4-6 Essentially, it is in these situations where the difficult can become deadly, which highlights a key role for anesthesiologists in not only securing difficult airways but also in providing comprehensive physiological management. Thus, a recent Delphi study conducted by an international committee of experts proposed recommendations for tracheal intubation in critically ill adults with a physiologically difficult airway (Figure 2).6
Altogether, these guidelines can be encapsulated in 3 essential actions:
1. Do no harm: Do not use induction agents that might cause hemodynamic collapse, individualize drugs according to patients’ needs, and decrease aspiration risk by using rapid sequence induction or gentle mask ventilation.
2. Be prepared: Check the room environment, have a checklist, ensure the video laryngoscope is ready, adjust the bed position before starting, and have proper preoxygenation.
3. Take a multidisciplinary approach: Having at least two people managing the airway is crucial so that important steps are not overlooked. Plan beforehand with the ICU team, who may be more familiar with the patient. Treat and monitor the patient rather than focusing solely on endotracheal tube insertion.
In essence, remember that the path from difficult to deadly can be fast when intubating “physiologically difficult airways.” The Golden Rule remains: Avoid crashing the airway by preparing, collaborating, and avoiding potential harms.
1. Comparison of Tracheal Intubation Conditions in Operating Room and Intensive Care Unit: A Prospective, Observational Study. Taboada M, Doldan P, Calvo A, et al. Anesthesiology. 2018;129(2):321-328. doi:10.1097/ ALN.0000000000002269.
2. Practice of Intubation of the Critically Ill at Mayo Clinic. Smischney NJ, Seisa MO, Heise KJ, et al. Journal of Intensive Care Medicine. 2017;:885066617691495. doi:10.1177/0885066617691495.
3. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. Russotto V, Myatra SN, Laffey JG, et al. JAMA. 2021;325(12):1164-1172. doi:10.1001/jama.2021.1727.
4. The Physiologically Difficult Airway: An Emerging Concept. Myatra SN, Divatia JV, Brewster DJ. Current Opinion in Anaesthesiology. 2022;35(2):115-121. doi:10.1097/ACO.0000000000001102.
5. Management of the Difficult Airway. Heidegger T. The New England Journal of Medicine. 2021;384(19):1836-1847. doi:10.1056/NEJMra1916801.
6. Tracheal Intubation in Critically Ill Adults With a Physiologically Difficult Airway. An International Delphi Study. Karamchandani K, Nasa P, Jarzebowski M, et al. Intensive Care Medicine. 2024;50(10):1563-1579. doi:10.1007/s00134-024-07578-2.
7. Shenson, Jared A., and C. Kwang Sung. “Transoral Laryngeal Microsurgery for Supraglottic Airway Obstruction in Thyroid Goiter.” Otolaryngology Case Reports 10 (March 2019): 17–19.

Figure 2: Summary of recommendations for intubating patients with “physiologically difficult airways.”

This video of a pre-operative flexible nasolaryngoscopy demonstrates severe narrowing of the nasopharynx, oropharynx, hypopharynx, and supraglottis with lateral wall compression, extensive edema and polypoid changes of the larynx, and redundant arytenoid mucosa.7

Nitrous oxide pipelines were introduced into U.S. hospitals in the 1960s as anesthesia services became more prevalent, and the need for a consistent supply of medical gases became apparent. Nitrous oxide became the only anesthetic gas to be incorporated into building architecture and has remained there ever since. However, as anesthetic practice has evolved, the clinical use of nitrous oxide continues to decrease, owing to clinical concerns such as the increased risk of postoperative nausea and vomiting, potential increased cardiovascular risk, atelectasis, and gas expansion of closed spaces.1, 2 Contemporary alternatives are now plentiful, with the continued growth of regional anesthetic techniques, total intravenous anesthesia, and multimodal analgesia throughout anesthetic practice.
As anesthetic practice has evolved, so has our ability to measure the volume of anesthetic gases used through the minute-by-minute anesthesia records of our electronic medical records. When comparing the volume of nitrous oxide delivered during patient care to the volume of nitrous oxide purchased annually by a hospital, one can calculate a leak rate for nitrous oxide.
Across multiple continents, countries, and hospitals, we know that 80-95% of nitrous oxide that is centrally supplied is lost to leakage before it can even reach an anesthesia
Mary Jarzebowski, MD
Henry Ford Health, Jackson MSA Vanguard Committee
80-95% of piped NO is lost to leakage
300x more potent than CO2 Stays in the atmosphere 100+ years
(7.5x3.75)
machine.3 This leakage presents both an occupational hazard (chronic nitrous oxide exposure has been linked to myelosuppression, neurotoxicity, and infertility1) and an environmental hazard. Nitrous oxide is 300 times more potent as a greenhouse gas than carbon dioxide, persisting in the atmosphere for more than 100 years.3 Given the innate environmental impact of nitrous oxide, reducing the unnecessary leak presents a unique opportunity to reduce emissions with minimal change to workflow or patient care.
Leaking nitrous oxide pipelines present a unique opportunity for anesthesiologists to lead hospitals toward efficient practices by reducing financial waste associated with leaked nitrous oxide while simultaneously improving the environmental sustainability of anesthetic practice. A simple switch to delivering nitrous oxide via E-cylinders connected to anesthesia machines offers an easy solution for all anesthesia groups, even those regularly using nitrous oxide at major pediatric hospitals. The American Society of Anesthesiologists issued a practice statement in 2024 to support decommissioning nitrous oxide pipelines4, with many hospitals now following suit. Converting to E-cylinders reduced nitrous oxide use by 97.6% at one quaternary care hospital in the U.S., almost entirely attributed to the reduced leakage fraction.3
fiscally responsible practice. Notably, both Michigan Medicine and Henry Ford Health are building large new hospitals with new operating rooms. One major change in the blueprints? The new hospitals won’t have nitrous oxide pipelines.
Across multiple continents, countries, and hospitals, we know that 80-95% of nitrous oxide that is centrally supplied is lost to leakage before it can even reach an anesthesia
The physical decommissioning of the nitrous oxide pipeline is a simple process and can be done by medical gas companies. The large tanks in the central supply are removed, and the pipeline is purged of remaining nitrous oxide gas. The manifolds and pipeline alarms are decommissioned. In each operating room, the existing nitrous oxide ports are replaced with flat wall plates to prevent anyone from inadvertently accessing the empty pipeline (Figure 1). Work in each operating room takes approximately 15 minutes. Both Michigan Medicine and Henry Ford Jackson Hospital were able to complete the work to their facility in one night, minimizing disruption to the daily operating room workflow. Ongoing E-cylinder changes have been infrequent, with most operating rooms needing to replace empty cylinders every three to four months.
Two major health systems in Michigan, Henry Ford Health and Michigan Medicine, have committed to decommissioning nitrous oxide pipelines from all facilities. Michigan Medicine has implemented the change at its major hospitals and is continuing to work toward eliminating it at smaller ambulatory sites. Henry Ford Health has decommissioned the nitrous oxide pipeline at two of its hospitals, working toward its other sites by the end of 2026. The working groups at both health systems were led by the Departments of Anesthesiology, demonstrating the commitment of anesthesiologists to environmentally sustainable and
Although converting to nitrous oxide E-cylinders at the point of care is a simple and effective solution, there are several considerations for hospitals wishing to make the change.
1. Is anyone else using the piped nitrous oxide?
Some facilities have piped nitrous oxide supplying dental clinics, procedural areas, and labor and delivery rooms. Involving all stakeholders at the initial stages is crucial to ensuring a smooth decommissioning process. Each hospital must have an annual medical gas report, which will


Ceiling medical gas panel before and after nitrous oxide pipeline decommissioning.
show all end ports of the nitrous oxide pipeline in the building.
2. Are your anesthesia machines set up to hold nitrous oxide E-cylinders?
Some anesthesia machines are designed to hold nitrous oxide E-cylinders. However, some brands and models require retrofitting to hold an E-cylinder, which can be an expensive endeavor (up to $2,000 per machine). This reduces the cost effectiveness of the proposal.
3. Are your anesthesia providers ready to use E-cylinders?
Consider having educational sessions and creating standard workflows for checking cylinder pressures and changing cylinders.
Decommissioning nitrous oxide pipelines presents a unique opportunity for anesthesiologists to lead hospitals toward prioritizing efficient and costeffective healthcare that also reduces environmental impact. Anesthesiology groups across Michigan should consider changing their practice toward
delivering nitrous oxide via E-cylinders at the point of care, a practice supported by the American Society of Anesthesiologists.
1. Gropper, M. A., Eriksson, L. I., Fleisher, L. A., Cohen, N. H., Leslie, K., & Johnson-Akeju, O. (Eds.). (2025). Inhaled anesthetic uptake, distribution, metabolism, and toxicity. In Miller’s Anesthesia (10th ed., Vol. 1, pp. [page range]). Elsevier.
2. Kampman JM, Plasmans KYQ, Hermanides J, Hollmann MW, Repping S, Sperna Weiland NH. Influence of nitrous oxide added to general anaesthesia on postoperative mortality and morbidity: a systematic review and meta-analysis. Br J Anaesth. 2024 Dec;133(6):1419-1426. doi: 10.1016/j. bja.2024.02.011. Epub 2024 Mar 11. PMID: 38471989.
3. Chesebro BB, Gandhi S. Mitigating the systemic loss of nitrous oxide: a narrative review and data-driven practice analysis. Br J Anaesth. 2024 Dec;133(6):1413-1418. doi: 10.1016/j.bja.2024.08.028. Epub 2024 Sep 24. PMID: 39322471.
4. American Society of Anesthesiologists. (2024, October 23). Statement on deactivating central piped nitrous oxide to mitigate avoidable health care pollution. https://www.asahq.org/standards-and-practice-parameters/ statement-on-deactivating-central-piped-nitrous-oxide-to-mitigateavoidable-health-care-pollution
Abstract Title
"Cleared for Anesthesia:" the Challenges of Anesthetizing a 4.9kg Infant for Direct Laryngoscopy, Bronchoscopy, and Auditory Brainstem Response Testing, following Congenital Heart Disease Repair
"Vitamin B12 Deficiency and Pulmonary Emboli due to Chronic Recreational Nitrous Oxide Abuse"
A Calculated Approach: Neuraxial Anesthesia in a High-Risk Parturient with Aortic Stenosis
A Case of an Anterior Mediastinal Mass and Cardiac Tamponade: Anesthetic Considerations
A Case of Ventricular Fibrillation After Undergoing General Anesthesia
A Heated Encounter in the MRI Suite: Unmasking Malignant Hyperthermia in a Sepsis-Confounded Case
A Novel Platform to Centralize Preparation of Surgical Patients: PATO
A Perilous Perioperative Passage: Managing Anesthetic Challenges in a Patient with Polysubstance Disorder
A Review of Intraoperative and Postoperative Complications Associated with Shockwave Lithotripsy
A Shocking Airway: Airway Management and Anesthetic Considerations in a High-Voltage Electrical Injury
A Tight Spot: Managing Tracheostomy Dislodgment in a Stented Airway
A Wet Tap’s Echo: Neurologic Drama After Epidural Bolus
ACGME Trends in Race/Ethnicity and Gender Makeup in Obstetric Anesthesiology Fellows from 2012-2024
Acute Reverse Takotsubo Cardiomyopathy Triggered by Neuraxial and General Anesthesia in a Parturient: A Case of Sudden Cardiogenic Collapse
Adoption and Pattern of Use of End-Tidal Control at a Large Pediatric Hospital
AI-Assisted Self-Diagnosis: Navigating Patient Anxiety and Clinical Accuracy
Airway Lasering with Precision: Juggling Systemic Pulmonary Hypertension and Multiple Cardiac Arrests from Airway Collapse
Airway Management in Bilateral Lung Transplant Patient with Mounier-Kuhn Syndrome
An Ultrasound-Guided Approach to Neuraxial Anesthesia in a Patient with Down Syndrome and Complex Anatomy
An Unusual Presentation of Propofol Induced Uric-Aciduria
Analysis of Use and Outcomes of GE Healthcare End Tidal Control Across a Major US Academic Health System
Analyzing the Effects of Quality Improvement Initiatives on Environmental Sustainability in Anesthesia
Anesthetic Challenges in Spine Surgery for a Patient with a Complex Fontan Physiology
Anesthetic Challenges in the Management of Maternal Trauma: Case of Gunshot Wound During Pregnancy.
Anesthetic Considerations in a High Risk Parturient with Myelomeningocele, Transaminitis, and Urosepsis undergoing Emergent Surgery
Anesthetic Management and Airway Challenges in High-Risk Burn Patients
Primary Author/ Michigan Author
Institution
Rija Awan BS et al. University of Michigan
Ho Young Curiel-Moon BS et al. Michigan State University COM
Adam Kapp BS et al. Michigan State University CHM
Jill Carter DO et al. McLaren Flint
Hira Ali BS et al. Michigan State University CHM
Bryan Roberts DO et al. Wayne State University
Kristin Konja DO et al. Henry Ford Health
Kush Patel MS et al.
Michael Balce MD et al.
Spencer Kitchen MD et al.
Central Michigan University
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Dhanush Bathala DO et al. Henry Ford Health
Muhammad Shahyan Baber Ali MD et al. Detroit Medical Center
Shikha Lakhani BS, Dhanush Bathala DO et al.
The University of Toledo, Henry ford Health
Marshall Balderston DO et al. Detroit Medical Center
Allie Thompson MPH et al. University of Michigan
Grace Li BS et al.
Oakland University William Beaumont School of Medicine
Nicole Dobija MD et al. University of Michigan
Arun Muthukumar Marimuthu Kala MD et al. Henry Ford Health
Stephanie Stevens MD et al. Detroit Medical Center
Alexander Gomez Student et al. Michigan State University CHM
Douglas Colquhoun MBChB et al. University of Michigan
Armaan Patel BS et al. University of Michigan
May Rhee BS et al. University of Michigan
Arun Muthukumar Marimuthu Kala MD et al. Henry Ford Health
Maxwell Sievers MD et al. University of Michigan
Hannah Lee BS et al. Wayne State University
Abstract Title
Anesthetic Management and Challenges in a Patient with a BMI over 90
Anesthetic Management and Considerations in High - Risk Cardiac Surgery with Multivalve Disease and Right Heart Failure
Anesthetic Management in the Excision of a Cardiac Paraganglioma: A Medically Challenging Case
Anesthetic Management of a Multidisciplinary Surgical Patient with Fascioscapulohumeral Muscular Dystrophy
Anesthetic Management of an Elderly Patient with Idiopathic Pulmonary Fibrosis Undergoing Spinal Surgery
Anesthetic Management of Cavo-atrial Rupture During Intra Cardiac Device Lead Extraction
Anesthetic Management of Pediatric Congenital Cardiac Patient Undergoing Posterior Spine Fusion
Anesthetic Strategy in Jaundiced Patients: The Influence of Underlying Etiology
Anterior Mitral Valve Leaflet Myxoma: A Rare Case with Stroke-Like Presentation and Concurrent Coronary Artery Disease
Artificial Intelligence and Machine Learning in Pediatric Anesthesia: A Systematic Review
Artificial Intelligence and Machine Learning in Postoperative Geriatric Anesthesia: A Systematic Review
Avoiding Sudden Death: A Review of at Risk Populations and Perioperative Treatment for Severe Hypertrophic Cardiomyopathy
Awake, Aware, and Paralyzed: Lessons from a Hidden Enzyme Deficiency
Balancing Identity and Safety: Inclusive and Accurate Preoperative Assessments for Transgender Patients
Bilateral Hemotympanum Following Complicated Cardiopulmonary Bypass Procedure, a Case Report
Breathing for Two: Anesthetic Management of Severe Subglottic Stenosis in Pregnancy
Can Frailty Index Factors Predict Postoperative Dispositional Outcomes in Cardiac Surgery?
Cardiac Arrest from High Spinal Anesthesia During Cesarean Section in a Patient with Sickle Cell Disease: A Case Review
Coexisting Acute Ischemic Stroke, Hyperviscosity Syndrome, and Multiple Myeloma in a Patient with Septic Shock
Considerations for management of a medialization thyroplasty in a patient with dolichoectasia
Continuous and non-invasive blood pressure monitoring in patients undergoing surgery
Critical Care Management of Pan-Resistant Acinetobacter Osteomyelitis Requiring Novel Antibiotic Therapy
Crucial Change of ECMO Strategy Prompted by New Intraoperative TEE findings
Difficult Airway Management in a Patient With Head and Neck Radiotherapy
Disparities in Representation of Regional Anesthesiology and Acute Pain Medicine Fellows
Disparities in Research Engagement Among Medical Students: Implications for Diversity in Anesthesia and Surgery
Dorsal Root Ganglion Stimulation for Refractory Chronic Pelvic Pain
Primary Author/ Michigan Author
Elizabeth Giaimo DO et al.
Institution
Corewell Health William Beaumont Hospital
Cooper Laurain MD et al. Henry Ford Health
Sevar Yaldo et al. Henry Ford Health
Rebecca Rush DO et al. Henry Ford Health
Sarah Kadado BS et al.
Corewell Health William Beaumont Hospital
Nirmeen Chouaib DO et al. Henry Ford Health
John Raupp BA et al.
Revati Rashingkar BS et al.
Frass Ahmed BS et al.
Aditya Shah BS et al.
Christya Haddad BS et al.
Michael Balce MD et al.
University of Michigan
Corewell Health William Beaumont Hospital
Michigan State University CHM
Central Michigan University
Central Michigan University
Corewell Health William Beaumont Hospital
Marshall Balderston DO et al. Detroit Medical Center
Nidhi Navaratna BA et al.
Corewell Health William Beaumont Hospital
Rachna Jayaprakash MB et al. Henry Ford Health
Joshua Jones MD et al.
Mark Whitton BS et al.
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Ahmad Hadri DO et al. Wayne State University
Jonathan Ong MD, Nikhil Aggarwal BS et al.
Pratik S. Vadlamudi et al.
Sophia Lin PhD [] Daniel Molitor BS, Carlos Guerra Londono MD et al.
Nidhi Navaratna BA et al.
LewisGale Medical Center, Oakland University
University of Michigan
Vena Vitals, Henry Ford Health
Oakland University William Beaumont School of Medicine
Brianna Grimes MD et al. Detroit Medical Center
Abdul Ansari DO et al. Michigan State University
Swamroop Nandwani BS [] Dhanush Bathala DO et al.
Sahil Dhandi BA, Suhas Nagappala, BA et al.
The University of Toledo, Henry Ford Health
University of Southern California, Wayne State University
Jason Comeau MD et al. Pain Clinic of Michigan
Abstract Title
Double Lung Transplant Complicated by Bronchial Dehiscence: A Complex Case Requiring Coordinated Multidisciplinary Management
Double Trouble: Difficult Airway in Turner Syndrome with Substernal Goiter
Emergent Airway Management in the Setting of Severe Facial Trauma
Emergent Fasciotomy for Radial Artery Dissection and Compartment Syndrome Following PCI
Endoscopic endonasal, bifrontal craniotomy for resection of recurrent meningioma
Epidural Anesthetic Management of a Parturient with Von Willebrand Disease Type 1C
Epinephrine induced coronary artery spasm
Estimations of Optimal Intraoperative Treatment Strategies for Reducing Cardiac Surgery-Associated Acute Kidney Injury
Ethical Considerations and Management of Patients Refusing Blood Products in Trauma
Examining Student Perspectives on Medical Device Education
Exparel Interscalene Block & Respiratory Failure
Exploring the Relationship Between Body Mass Index and Postoperative Nausea and Vomiting: A Single-Institution Analysis
Eye See a Problem Here: Expeditious Diagnosis and Treatment of Orbital Compartment Syndrome during Orbital Surgery following a Retrobulbar Block
Fight or Flight: A Perioperative Balancing Act in Pheochromocytoma
FLUID MITIGATION AT JOHN D. DINGELL VA MEDICAL CENTER DUETO HURRICANE HELENE: IS IT IMPACTING THE HEMODYNAMICS OF THE PATIENT?
Food Impaction Secondary to Subcarinal Lymph Node Compression in a Patient with High PD-L1 Expressing NSCLC : A Unique Case of Aggressive Disease Despite Immunotherapy
From Circuit to Scalpel: Managing VV-ECMO Dependence in Emergent Double Valve Repair
From TOLAC to Total Abdominal Hysterectomy: Perioperative Challenges in a Case of Severe Postpartum Hemorrhage
Geographic Trends and Disparities in Opioid Overdose Mortality Among Elderly Adults in the United States
Glass Half Empty: Acute Upper Gastrointestinal Bleed During Pediatric Liver Transplant
Help or Harm? The Impact of Opioid Prescribing Guidelines on Opioid-Exposed Patients
Hemodynamic Instability After Endovascular AAA Repair: A Case Report
Holding Pressure: Navigating Urologic Urgency in Cardiogenic Instability
Homemade Single Lung CPAP During Device Shortage
Honeycombing through Airway Challenges in a Patient with Severe Pulmonary Fibrosis
Hypertensive Crisis and Respiratory Failure After Supraclavicular Nerve Block
Primary Author/ Michigan Author
Institution
Fares Alghanem MD et al. Henry Ford Health
Yuya Takahashi MD Henry Ford Health
Angelica Alexopoulos BS et al.
Oakland University William Beaumont School of Medicine
Maitreyi Narayan MD et al. University of Michigan
Zachary Osborn DO et al. Henry Ford Health
Travis Bell BS et al. Michigan State University CHM
Rachael Fakolujo MD et al. Henry Ford Health
Michael Mathis MD et al. University of Michigan
Oakland University
Mazen Zamzam et al.
William Beaumont School of Medicine
John Raupp BS et al. University of Michigan
Samantha Alexander MD et al. Corewell Health William Beaumont Hospital
Nidhi Navaratna BA et al.
Christina Thomas BS et al.
Oakland University William Beaumont School of Medicine
Oakland University William Beaumont School of Medicine
Radwa Koujane MD et al. University of Michigan
Rachel Semaan DO et al.
Detroit Medical Center / Wayne State University
Vidushan Sabanathan et al. Henry Ford Health
Oakland University
Madison McClune BS et al.
Maya Jaradi BS et al.
Swamroop Nandwani BS, Dhanush Bathala DO et al.
William Beaumont School of Medicine
Oakland University William Beaumont School of Medicine
The University of Toledo, Henry Ford Health
Riha Hagalwadi BS et al. University of Michigan
Jessica Yen BS et al. University of Michigan
Nasim Shakibai DO et al.
Corewell Health William Beaumont Hospital
Radwa Koujane MD et al. University of Michigan
Jackson Stevens DO et al.
Neehar Haryadi BS et al.
Corewell Health William Beaumont Hospital
Central Michigan University
Laura Mendez Pino MD et al. Henry Ford Health
Abstract Title
Hypothermic Fibrillatory Arrest: A Case Report
Improving Operating Room Fire Safety Through Targeted Training: A Quality Improvement Initiative
Incarcerated Gravid Uterus in an Incisional Ventral Hernia: Anesthetic Implications
Intraoperative ECG Changes Associated With IV Lacosamide During Awake Craniotomy
Intraoperative Infusion of Sub-hypnotic Propofol As Prevention for PONV: A Systematic Review
Intraoperative Management of Adult Congenital Heart Disease: A Multidisciplinary Approach to Managing Severe Right Heart Failure and Pulmonary Hypertension
Intraoperative Shock Liver during a Trisegmentectomy
Intraoperative TEE Detection of Aortic Mechanical Valve Placement in Mitral Position During MVR
Intraprocedural Considerations for Complex Lumbar Medial Branch Block
Ischemic Stroke in the Setting of Post OP Management of Aortic Dissection Repair
Life Threatening Anaphylaxis After SpaceOAR Hydrogel Administration
Light the Way: Light Wand Intubation in a Challenging Airway
Management of agitation, analgesia, and sedation in an intubated SICU patient
Management of Malignant Hyperthermia and Pseudocholinesterase Deficiency in Trauma
Management of Nutrition and Fluid Losses in the Setting of High Output Duodenostomy
Management of Postpartum Hemorrhage in a Parturient with Oligodendroglioma, Chronic Immune Thrombocytopenia and Preeclampsia, a Case Report
Managing Hyponatremia in a Liver-Kidney Transplant Patient During a Nationwide IV Fluid Shortage: A Perioperative Challenge
Managing the Unexpected: Ruptured Splenic Artery Aneurysm in a Pregnant Patient
Mast Cell Activation Syndrome
Medical Error and Anesthesiology: Using Theater to Teach Bioethics and Patient Safety in Medical Education
Medical Tourism and the Division in Anesthesia Surgical Clearance
Methylene Blue with a Pinch of Garlic: Novel Dual Therapy in Hepatopulmonary Syndrome
Mid-Humeral Nerve Block: Unlocking Regional Anesthesia in Traumatic Forearm Injuries.
Minimally Invasive Management Options for Thoracic Outlet Syndrome
Minimizing Withdrawal with Prolonged Pediatric Sedation in the Setting of the ICU
Primary Author/ Michigan Author
Nasim Shakibai DO et al.
Mustafa Hasnain MD et al.
Taylor Lonjin DO, Arunthevaraja Karuppiah MD
Alexis Lonjin, BS
Institution
Corewell Health William Beaumont Hospital
Detroit Medical Center / Wayne State University
Virginia Commonwealth University, Oakland University William Beaumont School of Medicine
Laura Mendez Pino MD et al. Henry Ford Health
Jackson Stevens DO et al.
Corewell Health William Beaumont Hospital
Syed Tariq-Un Nabi MD et al. Detroit Medical Center
Adebukola Owolabi MD [] Arun
Muthukumar M K MD et al.
Anderson Cancer Center, Henry Ford Health
Nupur Kumar DO et al. Henry Ford Health
Gareema Agarwal MS et al. University of Michigan
Sebastian Iniguez BS et al. University of Michigan
Anuja Nikam DO et al. Detroit Medical Center
Marshall Balderston DO Detroit Medical Center
Ellanya Kallabat MD et al.
Mazen Zamzam BS et al.
Jazmine Skala-Wade MD et al.
Corewell Health William Beaumont Hospital
Oakland University William Beaumont School of Medicine
Corewell Health William Beaumont Hospital
Ijeoma Ndupu MD et al. Henry Ford Health
Rania Fardous MD et al.
Maya Jaradi BS et al.
Mohamad Alkhatib MD
Jade Ayers MS et al.
Sama Ramo et al.
Corewell Health William Beaumont Hospital
Oakland University William Beaumont School of Medicine
Wayne State University / Detroit Medical Center
Oakland University William Beaumont School of Medicine
Oakland University
William Beaumont School of Medicine
Yaman Dalati DO et al. Henry Ford Health
Alexander Schreck BS et al.
Angelica Alexopoulos BS et al.
Jazmine Skala-Wade MD et al.
Michigan State University CHM
Oakland University
William Beaumont School of Medicine
Corewell Health William Beaumont Hospital
Abstract Title
Mitral Paravalvular Leak Closure Via Left Anterolateral Thoracotomy
Mobitz Type 1 Heart Block After a Cesarean Section with Spinal Anesthesia: A Case Study
Nausea and Vomiting After General Anesthesia: A Case of Unmet Expectations
Navigating Anesthetic Challenges in Epidermolysis Bullosa: A Unique Approach To Patient Management
Navigating Ethical and Legal Complexities in End-of-Life Decision Making: The Role of Guardianship in Patient Care
Navigating Hemodynamic Lability: Anesthesia for Bilateral Pheochromocytoma in MEN 2B
Noble Gas Post-Conditioning against Ischemia/Reperfusion Injury in Rat Isolated Hearts
Off-Pump Coronary Artery Bypass Graft Revision with Sternal Sparing Technique
Oops, I did it Again: Intentional Ingestion of a Stylet in a Patient with History of Foreign Body Swallowing
Optimizing Anesthesia Care in Post-Polio Syndrome
Optimizing Trauma Resuscitation: A Case Report on Thromboelastography Guided Management of a Massive Transfusion Scenario
Pacing and Pressure - Anesthesia for HOCM and Dual Devices in Transsphenoidal Surgery
Parkinsonian Symptoms and Delayed Emergence as a Predictor for Cognitive Impairment: A Case Report
Patient Preferences for Hemodynamic Monitoring Information: A Survey-Based Study in the US and UK
Patients Can Have Do-Not-Resuscitate Orders in the Operating Room: Results from an Ethics Simulation
Pediatric Airway Management: Surgical Removal of a Wooden Skewer from the Oral Cavity
Pediatric Recessive Dystrophic Epidermolysis Bullosa
Pelvic Pain Perplexity: A Case of Post-Zoster Sacral Plexopathy
Perioperative Challenges in Myasthenia Gravis: A Case of Liver Transplantation
Perioperative Challenges of Abdominal Compartment Syndrome in Complex Hernia Repair
Perioperative Considerations of a Myasthenia Gravis Patient with Epidural Metastasis and Prior Pneumonectomy: A Case Report
Perioperative Fluid Management in Central Arginine Vasopressin Deficiency
Perioperative Management of Combined Liver-Kidney Transplantation Requiring Massive Transfusion
Perioperative Management of Multinodular Goiter
Perioperative Management of Pheochromocytoma Resection in a Patient with Hypertrophic Cardiomyopathy and Left Ventricular Outflow Tract Obstruction
Primary Author/ Michigan Author
Institution
Farah Aboufakhr MD et al. Corewell Health William Beaumont Hospital
Gabrielle Gappy BS et al.
Hashim Aslam BS et al.
Oakland University William Beaumont School of Medicine
Oakland University William Beaumont School of Medicine
Paige Pieczarka MD et al. Henry Ford Health
John A. Pardington Jr, BS et al. Michigan State University CHM
Itzel Lopez-Hinojosa MD et al. University of Michigan
Matthias Riess MD, Symone D. Caruthers et al.
TVHS VA Medical Center, Andrews University
Michael Debeau MD et al. McLaren Flint
Deepti Sanku BS et al.
Jakob Amcheslavsky BS et al.
Theodore Schiff BS et al.
Nitin Venkatesh MD et al.
William Nguyen BS Mohammed Shium BA, Sarah Kadado et al.
Central Michigan University
Central Michigan University
Detroit Medical Center / Wayne State University
Trinity Health Oakland
NYU Grossman, Oakland University William Beaumont School of Medicine
Wael Saasouh MD et al. Wayne State University
Michael Balce MD et al.
Anna Jahshan-Abdalla MD et al.
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Maedeh Marzoughi BS et al. University of Michigan
Amanda Herrera MD et al.
Revati Rashingkar BS et al.
Vivian Chang MD et al.
Farah Aboufakhr MD et al.
Jack Dryden BA et al.
Austin Johnson BS et al.
Nikhil Aggarwal BA et al.
Caleb Weissman BSc et al.
Corewell Health William Beaumont Hospital
Oakland University William Beaumont School of Medicine
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Oakland University William Beaumont School of Medicine
Michigan State University CHM
Click on Abstract Title to view poster abstract
Abstract Title
Perioperative Management Pitfalls: Vasopressor Extravasation in Septic Shock
Perioperative Multidisciplinary Planning for Recurrent Ascending Aortic Pseudoaneurysm Repair in a Patient with Extensive Cardiac Surgical History: A Case Report
Perioperative Risks of Cannabis Use: Aspiration During Elective Surgery
Peripartum Management of Pulmonary Alveolar Proteinosis in Pregnancy: An Interdisciplinary Approach
Physician Opioid Prescribing Attitudes in Michigan: An Exploratory Pilot Study of Age-Gender Interactions and the AwarenessUncertainty Paradox
Post Esophagectomy Tracheostomy Failure
Post-Partum Aortic Dissection
POUNCE syndrome after accidental ingestion of methadone in a unsupervised 2-year-old
Practice Patterns of midazolam administration in patients undergoing cardiac-related non-operating room procedures: A multi-center study
Practice Variation in Intraoperative Hemodynamic Management for Left Ventricular Assist Device Implantation: A Multicenter Observational Analysis
Pregnancy-Induced Narcolepsy: A Case Study
Preoperative Fasting Status and Retained Gastric Content in Patients Receiving Glucagon-Like Peptide Type 1 Receptor Agonists: A Retrospective Study
Pulmonary Hypertension in a Parturient Complicated by Right Ventricular Failure
Pulmonary Hypertension: A Challenging Extubation
Pump Removed, Problems Remain: Navigating Intrathecal Pain Pump Removal and Opioid Conversion Challenges
Recognizing and Managing Perioperative Stroke in Postoperative Cardiac Cases
Repair of Atrial Septal Defect and Tricuspid Valve Complicated by Bilateral Hemotympanum, a Case Report
Serotonin Syndrome in the Operating Room Following Use of Fentanyl in a Patient on a Monoamine Oxidase Inhibitor
Severe Hypercarbia s/p Sedation in a Patient with Severe Pulmonary Hypertension
Severe Postoperative Negative Pressure Pulmonary Edema (NPPE) Following Adenoidectomy Requiring ECMO: A Fatal Case
Severe Tracheal Stenosis Following Intubation in an Asthmatic Patient
Severe Vitamin C Deficiency as a Potential Contributor to Recurrent Cardiac Tamponade, Mediastinal Hemorrhage, and Multisystem Complications in a Post-Operative Cardiac Surgery Patient
SGLT2 Induced Euglycemic DKA in the setting of Emergent Surgery
Silent Triggers: Simultaneous Laryngospasm and Bronchospasm in a Toddler Caused by Secondhand Vaping, a Case Report
Simultaneous Off-Pump Coronary Artery Bypass and Liver Transplantation in a High-Risk Cirrhotic Patient With Multivessel Coronary Disease
Primary Author/ Michigan Author
Nelson Jones BS et al.
Mustafa Hasnain MD et al.
Grace Li BS et al.
Institution
Corewell Health William Beaumont Hospital
Detroit Medical Center / Wayne State University
Oakland University William Beaumont School of Medicine
Jessica Yen BS et al. University of Michigan
Deepti Sanku BS et al. Central Michigan University
Mercylia Untono et al. Wayne State University
Patrick Thrasher MD et al.
Eitan Scher MD
Corewell Health William Beaumont Hospital
McLaren Flint
Lisa Rong MD [] Allison Janda MD et al. Weill Cornell Medicine, University of Michigan
Jonathan Herrera MD et al. University of Michigan
Gabrielle Gappy BS et al.
Laura Mendez Pino MD et al.
Darshan Rola DO
Patrick Thrasher MD et al.
Spencer Kitchen MD et al.
Jade Ayers MS et al.
Ted Frederic DO
Frass Ahmed BS et al.
Victoria Schomer DO et al.
Harsh Patel BS et al.
Oakland University William Beaumont School of Medicine
Henry Ford Health
Henry Ford Health
Corewell Health William Beaumont Hospital
Corewell Health William Beaumont Hospital
Oakland University William Beaumont School of Medicine
Henry Ford Health
Michigan State University CHM
Corewell Health William Beaumont Hospital
Michigan State University COM
Cara Marolt MD et al. Henry Ford Health
Avery Heo BS et al.
University of Michigan
Kaab Husain BSc et al. Henry Ford Health
Ijeoma Ndupu MD et al. Henry Ford Health
Simon Zetuna MD et al. Henry Ford Health
Click on Abstract Title to view poster abstract
Abstract Title
Socioeconomic Status and Anesthesia Choice in Same-Day Total Joint Arthroplasty Cases
Successful Bronchial Blocker for R. Lobectomy After Failed Double Lumen Tube
Sudden Onset of Severe Headache in a Parturient
Sugammadex and Sudden Collapse: Cardiac Arrest Complicated by Takotsubo Cardiomyopathy
Sugammadex Utilization: A Systems Based Practice & Health System Analysis
Temperature Matters: Rocuronium Storage Conditions and Incomplete Neuromuscular Blockade in a Complex Pancreaticoduodenectomy
The Bullae Challenge: Anesthetic Considerations in the Face of Vanishing Lungs
The Effect of Abdominal Insufflation on Transversus Abdominis Plane (TAP) Block Efficacy in Laparoscopic Gynecologic Surgery
The effect of dexmedetomidine as an adjunct to transversus abdominis plane block in adults undergoing abdominal nonobstetric surgery under general anesthesia A systematic review and meta-analysis
The Quality Outcomes Committee: An Innovation for Patient Safety Indicator Validation at Henry Ford Hospital
The Silent Threat: A Fatal Case of Intraoperative Massive Pulmonary Embolism
Tug of War: A Multidisciplinary Approach to a Retained Epidural Catheter After Delivery
Tumor Embolism as an Intraoperative Complication of Nephrectomy for Wilms Tumor
Under Pressure: Extremity Blood Pressure Discordance in Peripheral Vascular Disease
Understanding Post-Operative Seizure Predictors: A MultiCondition Review of Risk Factors and Clinical Outcomes
Primary Author/ Michigan Author
Institution
Phillip McKegg DO et al. Henry Ford HealthStJohn
Ronald Te DO et al. Detroit Medical Center
Victoria Schomer DO et al.
Corewell Health William Beaumont Hospital
Kristin Konja et al. Henry Ford Health
Samantha Alexander MD et al.
Hashim Aslam BS et al.
Corewell Health William Beaumont Hospital
Oakland University William Beaumont School of Medicine
Amanda Herrera MD et al. Corewell Health William Beaumont Hospital
Hussein Bazzi BS et al. Wayne State University
Juan Jose Guerra Londono MD et al. Henry Ford Health
Chineze Mbanugo MD et al. Henry Ford Health
Isaac Kim MD Henry Ford Health
Joshua Jones MD et al.
Corewell Health William Beaumont Hospital
Aditya Bhagirath DO McLaren Flint
Aruna Jain BS et al.
Osama Hassan BA, Akshar Patel MD et al.
Unknown splenic artery aneurysm rupture after cesarean delivery Elizabeth Giaimo DO et al.
Unmasking an Atypical Presentation of Anaphylaxis - the sugammadex reaction
Unusual Abdominal Wall Complication Following Bilateral TAP Block: A Case Report
Uvular Necrosis After Spine Surgery
Venovenous ECMO: A Life-Saving Intervention in a Young Asthmatic Patient
VV ECMO for Management of Septic Shock-Induced ARDS and Air Leak Syndromes
When Mimicry Holds the Key: Navigating Anesthesia in a Nonverbal Autistic Child with a Mysterious Neuromuscular Disorder
When the Tap Turns Critical: Hemorrhagic Shock Following Paracentesis for Decompensated Cirrhosis
When Two Emergencies Collide: Managing Vasoplegia in a Preeclamptic Patient with a Type A Aortic Dissection
When You Don’t Trust Your Gut: A Case of Pneumatosis Intestinalis in a Complex Geriatric Patient
Ali Tanvir MBBS, Nirmeen Chouaib DO et al.
Michigan State University CHM
Northwestern University Feinberg School of Medicine, University of Michigan
Corewell Health William Beaumont Hospital
Mayo Hospital, Henry Ford Hospital
Ajay Pius MD et al. Henry Ford Health
Stephanie Boldt MD et al. McLaren Flint
Nidhi Navaratna et al.
Joon Sung BS et al.
Tristan Attisha BS et al.
Oakland University William Beaumont School of Medicine
Oakland University William Beaumont School of Medicine
Oakland University William Beaumont School of Medicine
Vivian Chang MD et al. Corewell Health William Beaumont Hospital
Chineze Mbanugo MD et al. Henry Ford Health
Madison McClune BS et al.
Oakland University William Beaumont School of Medicine
120 N. Washington Sq., Suite 110A
Lansing, MI 48933
Phone: 517.346.5088

https://mymsahq.org/for-members/msa-pac/