Murrumbidgee Primary Health Network (MPHN) acknowledge and pay our respect to the traditional owners of the lands on which MPHN operates: the Wiradjuri, Nari Nari, Wemba Wemba, Perepa Perepa, Yorta Yorta, Ngunnawal, Nagrigo, Bangerang and Yitha Yitha Nations. We recognise our communities are made up of many Aboriginal and Torres Strait Islander peoples descended from additional mobs and clans who also call the Murrumbidgee region home. We pay our respects to elders past, present and future and recognise these lands have always been places of traditional healing and medicine, and this plays a role in shaping future health services.
Introduction
Murrumbidgee Primary Health Network’s (MPHN) vision is “Well People, Resilient Communities across the Murrumbidgee”.
The Needs Assessment and Annual Planning Guide supports MPHN to identify priority health needs and conduct annual planning across the Murrumbidgee region through commissioning of services, integration and collaboration activity.
This document focuses on the processes of conducting a needs assessment and development of Activity Work Plans through the process of planning. Separate documents detail the process of procurement, commissioning and monitoring and evaluation.
As part of the Health Needs Assessment process, MPHN seeks to understand the health needs in the areas of:
• Vulnerable populations who experience socio economic disadvantage
• Aboriginal and Torres Strait Islander people
• Maternal Child and Youth
• Older Persons
• Population Health
We continue to work with partner service providers including the Murrumbidgee Local Health District, Aboriginal Medical Services, Aged Care Services and other local providers to implement integrated/coordinated models of care, including the development of Health Pathways.
To assist in the identification of opportunities to improve primary healthcare across the Murrumbidgee we have established four Clinical Councils and a Community Advisory Committee. These committees are an important part of the MPHN governance infrastructure and play a significant role in supporting the delivery of best practice healthcare. They also provide advice about population health planning and the commissioning of services.
Governance
Clinical Councils
Clinical leadership is important in shaping health service delivery and improving the effectiveness of healthcare outcomes. There are four clinical councils across the region to reflect the diversity of healthcare needs across the region. Membership of the clinical council includes a broad range of clinicians working in these local areas including: GPs; allied and mental health professionals and nurses and pharmacists. All four clinical councils are chaired by a GP from that local area.
The clinical councils are based in four geographical sectors and include the following Local Government Areas:
Border: Berrigan, Edward River, Federation, Greater Hume Shire, Lockhart and Murray River
Western: Carrathool, Griffith, Hay, Lachlan, Leeton, Murrumbidgee, and Narrandera
BORDER
WESTERN
RIVERINA
WAGGA WAGGA
The four Clinical Council GP Chairs make recommendations to the Board. This may include recommendations regarding:
• Clinical issues that are unique to the needs of the region
• Opportunities to improve the efficiency and effectiveness of medical and healthcare services
• Population health planning
• Commissioning of programs and services that support local and national priorities.
Community Advisory Committee
MPHNs Community Advisory Committee (CAC) is informed by 33 Local Health Advisory Committees (LHACs) from across the Murrumbidgee region. Membership of the CAC includes four LHAC Chairs, one drawn from each of the four geographical sectors
Edward River
Murray River
Berrigan Federation Greater Hume
Lockhart Wagga Wagga
Snowy Valleys
Cootamundra -Gundagai Regional
Hilltops Junee
Coolamon Temora Bland
Lachlan (part)
Carrathool
Hay
Murrumbidgee Gri th
Leeton
Narrandera
WESTERN NSW
MURRAY
GIPPSLAND
Influencing principles Commonwealth PHN program guidelines
MPHN’s Health Needs Assessment and Commissioning Framework are underpinned by the Commonwealth Primary Health Network Program Guidelines. The stated objectives of these guidelines are:
• Increasing the efficiency and effectiveness of medical services for patients, particularly those at risk of poor health outcomes
• Improving coordination of care to ensure patients receive the right care in the right place at the right time.
The guidelines suggest PHNs will achieve these objectives by:
• Understanding the health care needs of their PHN communities through analysis and planning. PHNs will know what services are available and help to identify and address service gaps where needed, including in rural and remote areas, while getting value for money.
• Providing practice support services so that GPs are better placed to provide care to patients subsidised through the Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS), and help patients to avoid having to go to emergency departments or being admitted to hospital for conditions that can be effectively managed outside of hospitals.
• Supporting general practices in attaining the highest standards in safety and quality through showcasing and disseminating research and evidence of best practice. This includes collecting and reporting data to support continuous improvement.
• Assisting general practices in understanding and making meaningful use of eHealth systems, in order to streamline the flow of relevant patient information across the local health provider community.
• Working with other funders of services and purchasing or commissioning health and medical/clinical services for local groups most in need, including, for example, patients with complex chronic conditions or mental illness.1
Throughout all stages of our commissioning framework, we consider the four elements of the Quadruple Aim.2 These measures – across population health, consumer experience, value for money and provider experience – provide guidance in making decisions and prioritising solutions that deliver outcomes for all those involved in the health system.
Figure 1. Quadruple aim
Population health
• Improving health outcomes
• Ensuring equitable access to services
• Delivering quality health and care
• Reducing the burden of disease
Value for money
• Improving the cost effectiveness of service delivery
• Rationalising the ratio of primary and acute care funding
• Increasing efficiency in service delivery
Consumer experience
• Reducing waiting times for services
• Improving access to services
• Meeting consumer and carer needs
• Focusing on the consumer experience of the service
Provider experience
• Increasing clinician and staff satisfaction
• Promoting teamwork and integrated care
• Promoting leadership in best practice
• Promoting a culture of continuous quality improvement
2 Berwick DM, Nolan TW, Whittington J. (Insitute for Healthcare Improvement) 2008. The Triple Aim: care, health, and cost. Health Affairs 27:3, 759-769; Bodenheimer T, Sinsky C 2014. From Triple to Quadruple Aim: Care of the Patient Requires Care of the Provider. Annals of Family Medicine 12:6, 573-576.
Underpinning principles
Principles for commissioning
The following principles have been developed to guide our approach to commissioning. They are consistent with and support our overarching organisational vision, values and strategic goals, and should be considered together with our commitment to supporting vulnerable populations.
Through our commissioning approach, we will:
Listen to our communities, including those who haven’t traditionally been given a voice in shaping health services, and engage meaningfully to understand their needs and co-design solutions with communities.
See the whole person and put them at the centre of their care, recognising the impacts of a person’s circumstances on their health needs at all stages of life.
Improve access to health care across our region by removing barriers and increasing the equity of services, including in relation to their location, cost and appropriateness.
Develop new solutions and initiatives that are based on evidence, flexible to local settings, and deliver value for money.
Collaborate with existing and new partners to deliver a seamless experience for consumers and carers across the health journey, without duplicating effort.
Invest in our providers to build local capabilities and support local workforce development.
Partner with our providers to understand whether initiatives are making a difference, to share successes, and to learn from and continuously improve what we do together.
Ensure commissioning and procurement is fair, accountable, transparent and impartial.
Social disadvantage principles
MPHN’s needs assessment process is heavily influenced by the social disadvantage principles of the organisation. The eight principles are listed below with a description of the role for the health needs assessment where it is most applicable.
Addressing inequality
We will work to address inequality through raising awareness and increase access through developing the capacity and capability of our staff and our providers.
Evidence and consultation
Through our Health Needs Assessment (HNA) process we consult with health professionals, Government Agencies, Local Councils, Community based organisations and community members to better understand the health and social needs of our population. We will identify, quantify and geographically locate areas of social disadvantage. The HNA process includes a systematic analysis of data and information on demographic, health and service usage across the region and more importantly consultation with community members and health care professionals. This approach will inform planning to address identified needs in particular for those with social disadvantage.
Identification of vulnerable populations
We will ensure through our HNA and HNA Live process we identify vulnerable populations such as Aboriginal and Torres Strait Islanders, Culturally and Linguistically Diverse, Lesbian, Gay, Bisexual, Transgender and/or Intersex, homeless people, mentally unwell people, elderly isolated people, veterans and those exiting the justice system. We will work to ensure that the above people are not marginalised and excluded from accessing services.
Local responses
Through our work with local communities we will identify local and emerging issues associated with social disadvantage and address specific local needs through co-design.
Integrated care across the sectors
We will commit to ‘wrap-around’ care and support ensuring that a person is at the centre of their care and through commissioning will encourage innovative programs across the health and social sectors.
The early years response
We will foster cooperative relationships to ensure that all children across the region have access to the buildingblocks of a self-defining and self- fulfilling life.
Policy Level
We will collaborate with other organisations to establish broad inter-sectoral support to advocate for public policies that address current socio-environmental issues that have impact upon the health of individuals and communities in our region.
Sustainability
We will create viable and sustainable programs that address the needs and aspirations of our communities.
Planning principles
The following principles have been developed to guide our approach to planning. They are consistent with and support our overarching organisational vision, values and strategic goals, and should be considered together with our commitment to supporting vulnerable populations.
Through our planning approach, we will ensure:
Equality
Providing services across the Murrumbidgee region so that every person has the same equal ability to access them.
Equity
Providing services across the Murrumbidgee region so that people from vulnerable populations such as those with low socioeconomic disadvantage can access them. For commissioned services we will target services to people who normally face barriers to accessing them. This may be due to physical, financial or other barriers.
Why we undertake health needs assessment
MPHN has adopted the commissioning model developed by the Australian Government Department of Health. This model is a continual and iterative cycle.
The first phase of the cycle is strategic planning, including assessing the health needs of the community and prioritising them through annual Activity Work Plans. In the second phase, procuring services, initiatives are designed and contracted, working closely with providers. The final phase, monitoring and evaluation, encompasses performance management and evaluation to inform continuous improvement and learning.
At all points throughout the cycle, stakeholder input through consultation, engagement and co-design is crucial.
While this model provides a useful way to communicate our approach to commissioning, in reality it is more complex. Multiple initiatives are often happening at the same time, requiring careful planning, coordination and prioritisation across all of our activities.
MPHN undertakes a health needs assessment to meet its commitment to the Commonwealth Department of Health and to inform development of services and programs in primary care throughout the Murrumbidgee region. Figure 2 depicts the role of needs assessment in strategic planning as part of the Commonwealth’s Commissioning Framework.
Source: Australian Department of Health 2015
Figure 2. The Commonwealth PHN Commissioning Framework
Definition
According to the World Health Organisation, the definition of health needs is “objectively determined deficiencies in health that require health care, from promotion to palliation”. There are three types of needs, perceived health needs; the need for health services as experienced by the individual. Professionally defined health needs; the need for health services as recognized by health professionals and scientifically confirmed health needs; the need confirmed by objective measures of biological, anthropometric or psychological factors, expert opinion or the passage of time.
Health planning is the orderly process of defining health problems, identifying unmet needs and surveying the resources to meet them, establishing priority goals that are realistic and feasible, and projecting administrative action, concerned not only with the adequacy, efficacy and efficiency of health services but also with those factors of ecology and of social and individual behaviour that affect the health of the individual and the community.3
Further in defining health problems is the term needs assessment. A needs assessment is a systematic method of identifying unmet health and healthcare needs of a population and making changes to meet these unmet needs. It involves an epidemiological and qualitative approach to determining priorities which incorporates clinical and cost effectiveness and patients’ perspectives. This approach must balance clinical, ethical, and economic considerations of need—that is, what will be done, what can be done, and what can be afforded.4
“This approach must balance clinical, ethical, and economic considerations of need—that is, what will be done, what can be done, and what can be afforded.”
Commonealth key priority areas
• The PHN objective of efficiency and effectiveness of medical services for patients, particularly those at risk of poor health outcomes
• The PHN objective of opportunities to improve coordination
• The seven key priorities for targeted work: mental health, Aboriginal and Torres Strait Islander health, population health, health workforce, eHealth, aged care and alcohol and other drugs
• The four headline indicators which include; mental health treatment rates, cancer screening rates, childhood immunisation rates and potentially preventable hospitalisations
4 Wright J, Williams R, Wilkinson JR. Development and importance of health needs assessment. BMJ 1998: 316: 1310-1313. Also see Katterl R et al. Regionally-based needs assessment in Australian primary health care. PHCRIS 2011.
Needs assessment process
MPHN uses a supply and demand approach to determine gaps in service which results in identification, prioritisation and planning of strategies or programs to address the gaps identified. Planned commissioned services and programs in response to the identified health needs provide service utilisation data which informs effectiveness and efficiency of services and programs and which feeds back into the continuous review of health needs and gaps in service provision.
A formal approach to reviewing the Health Needs Assessments is undertaken annually, however it is reviewed and updated continuously. The Health Needs Assessment is the precursor to PHN Annual Activity Work Plans which include other factors such as cost, capacity and timing.
Four steps of needs assessment and planning
There are four steps in the process of health needs assessment and planning. This framework details this activity (see figure 3).
Step 1 Planning needs assessment
Step 2 Identifying health needs
Step 3 Identifying service needs
Step 4 Prioritisation and activity work plans
• Define Population(s)
• Define Objectives
• Identify Partners and Collaborators
• Identify resources needed
• Identify risks
• Create population profile
• Create health status and health behaviour profiles
• Gather other data including feedback and consultation data
• Use MPHN decision making Tool to consider impact at regional level
• Use MPHN LGA data prioritisation Tool to consider impact at local government area level
• Review service use across the region
• Undertake service delivery mapping
• Review internal data sources from commissioned service providers
• Triangulate profiles and other data and information
• Create final list of priorities for MPHN
• Identify options for commissioned services or programs to address identified priorities
• Endorsement of the Needs Assessment
• Plan development of Activity Work Plans for identified priorities
• Develop Activity Work Plans
Figure 3. Four steps in Health Needs Assessment and Activity Work Plans
Step 1 Planning Needs Assessment
Define population(s)
For the purpose of this document the population of interest includes all towns of the Murrumbidgee region. There are no limitations on specific populations or age groups, however service mapping concentrates on detailed mapping of primary care and superficial mapping of acute health care services.
The Commonwealth recommendation for geographic analysis is to use the Australian Statistical Geography Standard (ASGS) basis of sub-regions using SA 3 level as a building block. Demographic data can also be analysed at SA 2 level where possible. ASGS includes the Indigenous Urban Centres and Localities and the Remoteness Area classifications.
Local Government Areas (LGAs) are an ABS approximation of officially gazetted LGAs as defined by each State and Territory (S/T) Local Government Department. Local Health Districts use LGAs as a basis for planning acute sector health services.
Depending on data, MPHN will use SA levels to report and compare data where available. Individual profiles within the MPHN will utilise LGAs given the strong relationship with the Local Health District and its use of LGAs for health service system planning. MPHN will consider when completing its health needs assessment areas that include potential issues with cross-border flows with adjacent PHN regions, in particular the Murray PHN in the border area of the MPHN.
Define objectives
The objective of the health needs assessment for the MPHN is to deliver an evidence based, prioritised list of health needs reflecting community consultation for the primary care sector. Further the identified health needs will result in options prioritised to deliver quality commissioned services and programs that address identified health needs. Lastly an objective of the health needs assessment framework is to ensure that services and programs are able to be monitored and evaluated to further inform new iterations of the next health needs assessment.
Identify partners and collaborators
Consultation with the community and its representative groups, health professionals, providers, funders and other stakeholders is undertaken to inform the health needs assessment on gaps in service provision and to validate the proposed approaches to service delivery in response to the identified gaps.
Consultation will take a systematic approach and will include but not be limited to the following groups;
• Community Advisory Council, Clinical Councils, Local Health Advisory Committees
• Local Health District encompassing hospitals and community health
• Consortia, including; Aboriginal Health Consortium, Aged Care Consortium, Mental Health and Drug and Alcohol Consortium
• General practice, allied health professionals and non-Government agencies
• Representatives of housing, education and justice sectors, and local councils
• Population Health Needs Assessment Special Interest groups
Figure 4 below demonstrates the relationships and potential interactions of these key stakeholders.
Figure 4. Relationships and interactions of key stakeholder groups
Commissioners, including partners such as Local Health Districts, local councils, and other government agencies with a role in service delivery
Communities and consumers, including those with lived experience, consumers, carers and the broader local community
Providers, including existing and potential providers, general practices and clinicians, other medical experts and providers in related sectors
Identify resources needed
MPHN has access to appropriate qualified and experienced staff in data analytics and population health planning.
Additional resources include:
• Access to data and information such as national, state and local data and information gathered within the MPHN such as commissioned service evaluation data, including general practice data
• Support to map services
• Access to target populations for consultations such as health professionals and community members
• Access to the Data Analytics Platform (DAP) designed to capture visual representation of internal MPHN data for monitoring and the Population Health Analytics (PHA) Tool which assists with determining impact of relevant publicly available data
Identify risks
The process of health needs assessment is not without risk. Risk identification prior to commencement will allow for risk mitigation strategies to ensure minimisation or complete removal. Risk identification is undertaken in accordance with the Risk Management Framework, through the organisation’s risk management software Folio.
Step 2 Identifying health needs
Create population profile(s)
Using data from external sources, we develop population profiles that include geographic and demographic information. The Commonwealth recommendation is to derive data from ABS Census or Estimates of Resident Population. Characteristics such as ethnicity, location, gender, age, socioeconomic status etc. will be collected and may identify issues or inequities specific to these.
Using demographic and health data a profile for the Murrumbidgee region will be developed taking into account the prioritisation of health issues through use of the Population Health Analytics Tool. For the entire MPHN region data will be compared to National and State averages to determine magnitude of the issue locally.
Within the MPHN there are 21 local government areas. Data that represents the total MPHN region and the 21 LGAs will be collated to develop a representative profile. Data for LGAs and subregions will be assessed using the Population Health Analytics Tool to determine areas with higher impacts denoting higher need for intervention.
Create health status and health behaviour profiles
Using data from external sources, MPHN will develop population profiles that include health status and health behaviour profiles. Additionally, data from internal sources such as general practice data will be analysed allowing for triangulation of the data issue locally.
According to the Commonwealth recommendations, health status and health behaviours can include:
Health status
• deaths (mortality rates and life expectancy measures)
• health conditions (prevalence of disease, disorder, injury or trauma or other healthrelated states)
• human functions (alterations to body structure or function [impairment], activity limitations and restrictions on participation)
• wellbeing (measures of physical, mental and social wellbeing of individuals).
Health behaviours
• attitudes, beliefs, knowledge and behaviours such as patterns of eating, physical activity, smoking and alcohol consumption, and participation in cancer screening programs.
• According to the Commonwealth recommendations health needs assessments will consider chronic disease, the burden of communicable disease and injury. The Australian Institute of Health and Welfare (AIHW) provide examples of chronic diseases that include;
• cardiovascular conditions (such as coronary heart disease and stroke)
• cancers (such as lung, breast and colorectal cancer)
• many mental disorders (such as depression)
• diabetes
• many respiratory diseases (including asthma and COPD)
• musculoskeletal diseases (arthritis and osteoporosis)
• chronic kidney disease
• oral diseases.
Gather other data including feedback and consultation data
MPHN has several other mechanisms to gather information that informs the health needs assessment. These include both feedback and consultations.
Community and provider feedback
MPHN has two feedback mechanisms for recording health needs assessment data through a continuum branded HNA Live, including a community feedback survey and HNA mini community feedback. HNA Community Feedback allows consumers and healthcare professionals of the region to let MPHN know in real time their concerns about emerging health issues through completing two questions. MPHN also have a community feedback survey that gathers more targeted information about community perceptions of and use of health services in their communities.
Data for specific populations or LGA’s is sought by promotion of a month-long activity of feedback. Twitter, Facebook and MPHN newsletters are used to promote the feature or LGA(s) of the month to encourage the community to provide feedback. In addition, promotion of the feedback mechanisms occurs through the Local Health Advisory Committees (LHACs).
General feedback is also sought through feedback on the MPHN website. In addition to the above, MPHN register community members, both general community and health care professionals to be contacted in the future in relation to specific topics that require further input from the community. Posters and postcards have also been delivered throughout the region to prominent health places that the community visit to encourage feedback, such as general practice waiting rooms.
Feedback is acknowledged to the community via the HNA Community Feedback website to ensure the community are confident we are listening, individual acknowledgement is provided if requested.
Informal consultation
Informal consultations occur with LHACs and their chairs at regular meetings. Primary Care Engagement Officers (PCEOs) and other relevant MPHN staff of the MPHN attend LHAC meetings and LHAC Chair teleconferences regularly. LHAC Chairs also are members of the MPHN Board Community Advisory Committee, who receive feedback from MPHN staff relating to the Health Needs Assessment and have influence over activities to gather further feedback.
Consultation with key stakeholders and partners is undertaken informally as part of scheduled meetings, specific to health needs assessment or opportunities arising throughout meetings. MPHN actively work with the Murrumbidgee Local Health District and key general practice partners such as the Rural Doctors Network.
Formal consultation – Population health
MPHN will undertake formal consultation with both health care professionals (clinicians) and the community. Consultations will be held in each of the four sectors of the MPHN, Border, Riverina, Wagga Wagga and Western. The consultation methodology may use a focus group approach. Separate focus groups would be conducted for community and clinicians (see table 1 for examples of target groups for consultation). Focus groups seek information for non-specific population identification of needs.
Facilitation of the focus groups will be undertaken by the MPHN. Focus group participants will be recruited by a number of methods, listed below:
• Invitation letter sent directly to clinicians (may be emailed or posted)
• Invitation delivered through MPHN newsletters (utilising internal mailing lists)
• Invitation through social media, for example Facebook and Twitter
• Invitation through LHACs, Consortiums and other stakeholder groups
• Invitation delivered by PCEOs when undertaking a general practice visit
Table 1. Examples of Clinicians and community to be targeted for focus groups
Clinicians
Clinical Council members
Local Health District representatives
General Practice
Allied Health groups (ie Pharmacy, Podiatrists, Physiotherapists, Occupational Therapists, Speech Pathologists, Diabetes Educators, Respiratory Educators)
Formal consultation – Specific lifespan population groups
MPHN presents its data using a lifespan population grouping approach. Lifespan population groups are supported in some instances by Consortiums which MPHN are members of. Consortiums include the Murrumbidgee Aboriginal Health Consortium, the Youth Reference Group, the Shared Care Antenatal Group, the Mental Health Drug and Alcohol Alliance, the Local Response Group and the Aged Care Consortium.
Where MPHN has access to specific lifespan groups and consortiums, the HNA process will include an invitation to members to participate in a short survey of needs for the group they represent and an opportunity to disseminate invitations to focus groups described above. For specific populations where other naturally occurring groups of people occur, such as playgroups for the maternal and child lifespan group, short surveys will be offered to them. People who register for the MPHN feedback website will also be sent the same short survey to gain insight into their opinions on health needs.
Conversations on the Couch
Conversations on the Couch is the MPHN mechanism for annual consulting with communities within the Murrumbidgee region. Consultations inform the health needs assessment and service planning. Consultations occur in each town with a population greater than 1,000 people to ask them about their views on health services, their perceived need for health services locally and what services they need for now and the future. Consultations are conducted in high visibility venues for general public, ie coffee shops. Conversations on the Couch will target specific groups from time to time, for example engaging with Aboriginal and Torres Strait Islander people through a similar approach of “yarning”.
Community led planning
MPHN have commenced hosting in collaboration with the Murrumbidgee Local Health District, community based forums in targeted communities to increase understanding at a town level of health needs and are working with the community to prioritise and undertake health service planning that meets their unique needs. No more than two communities will be involved in this intensive approach at any given time.
Prioritisation and decision making
In order to ensure that the MPHN address identified needs in a structured and transparent manner a decision making tree approach will employ algorithms related to set criteria to rank in order of importance the health or social needs and their impacts on the region.
There are two major components of prioritisation in MPHN. To order the impact of health or social needs identified and to order the location where services would best be placed for relevant population groups based on the socio-demographic profiles of the 21 LGAs across the region. This ranking process ensures that commissioned services developed to address the health needs identified are located in the areas of most need across the MPHN.
Decision making – Health or social needs
Criteria for the prioritisation of health or social needs includes the following variables:
• Burden of disease, measured by the prevalence and/or incidence of health status and health behaviours – number and proportion of people affected
• Severity of the above, measured by either mortality or morbidity or both
• Increased burden of disease associated with specific vulnerable populations
• Comparison of above with both State and National averages for the same status and behaviours
• Community and Clinician concern about the health need
• Availability of an effective intervention, measured by access to services including aspects of both equity and equality. Equity being the ability to access an affordable service and equality being the ability to physically access a service
A further consideration where information is available would the cost effectiveness of an intervention where a costs/ benefits analysis has been undertaken. It is anticipated that this last criteria is likely to be unavailable the majority of the time so will be considered outside the scope of the algorithm.
The Population Health Analytics Tool is constantly being developed and additional aspects, such as the time series trend data, may be added to the Tool as it matures.
MPHN Population Health Analytics Tool
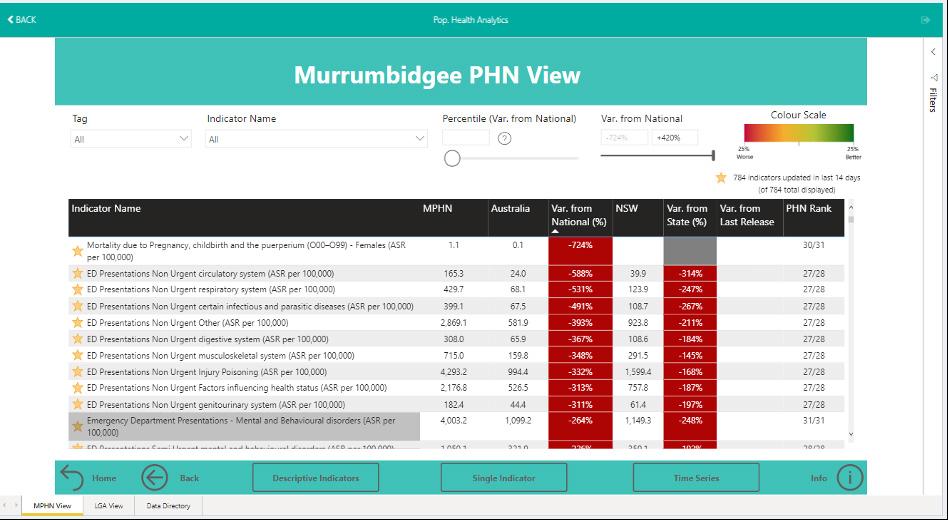
MPHN has developed its Population Health Analytics Tool to identify and visualise the areas of most need based on higher impact of health status, health behaviours or demographic profiles that identify vulnerable populations.
Data is ingested into the Tool for the 31 PHN’s across Australia to determine how we fare in relation to them and a rank score is determined. Data is ordered by PHN dependent on whether a lower or higher score is relevant. For example having less infant deaths is desirable so the ascending order would be by lower values, the higher the MPHN value is the worse the issue is. Having more people exercising is desirable so this variable would be sorted by higher values. Ranking remains static in that a rank of one is always considered better than a ranking of 31 considered to be worse. In the MPHN view in the Tool in addition to the rank score the variance to the National average and the State average is displayed if available. The Tool preferentially sorts indicators by most significant variance to Nation.
Quality of the ingested data and information relating to the Tool are contained within the Tool.
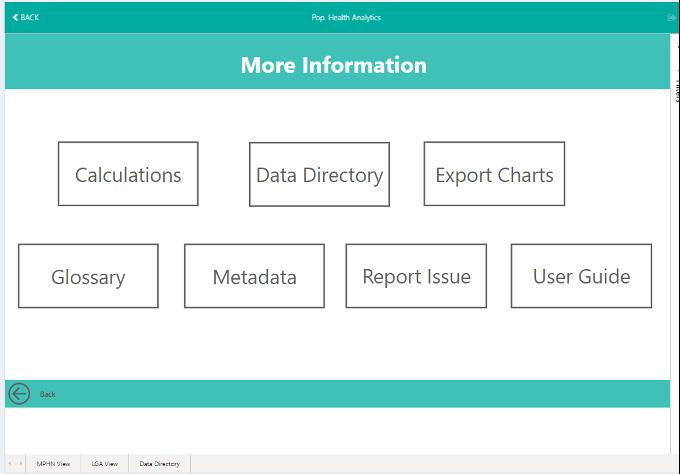
Figure 5. MPHN Population Health Analytics Tool – More information
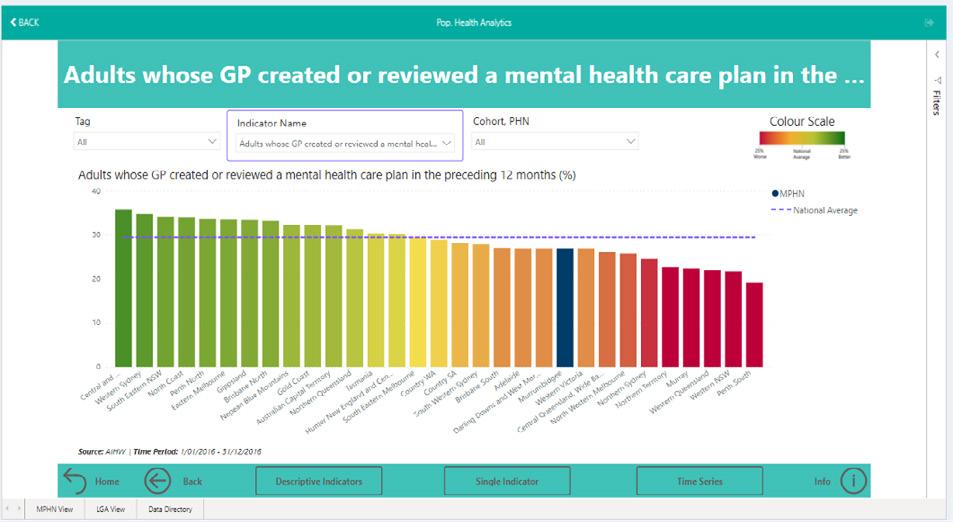
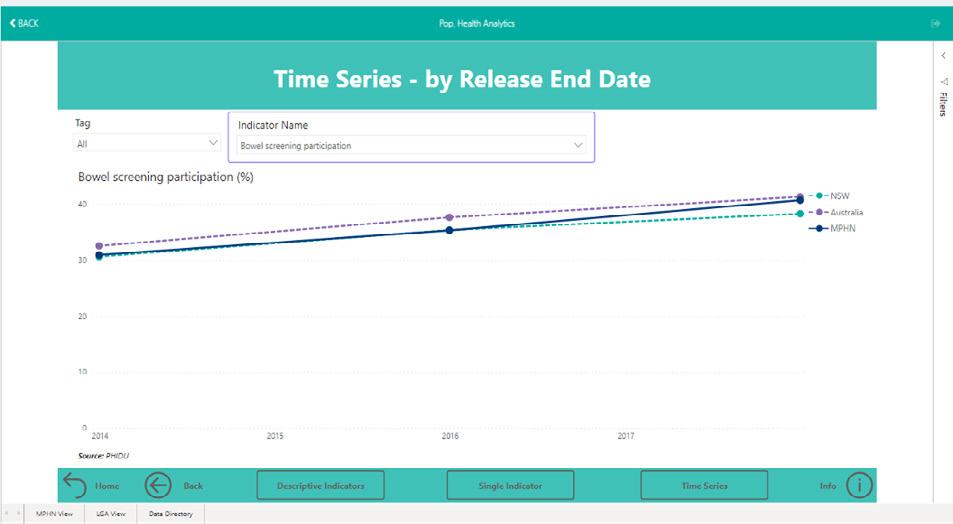
In the MPHN view visually each indicator is graphed in relation to all other PHNs with a National average line to demonstrate where MPHN sits in relation to the Nation. Most recently MPHN has added time series graphing to the Tool and refinement of including trend data is planned for a future iteration of the Tool.
Figure 7. MPHN Population Health Analytics Tool – MPHN view – Single indicator
Figure
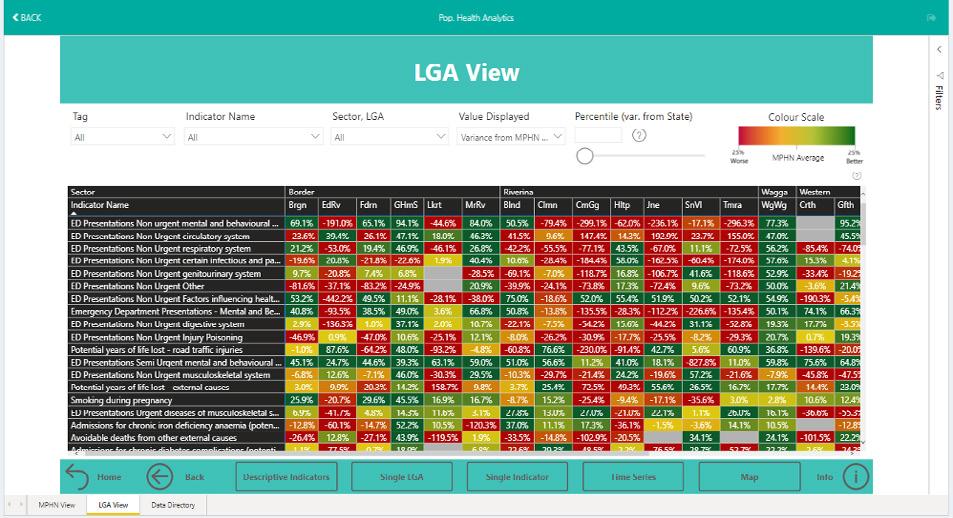
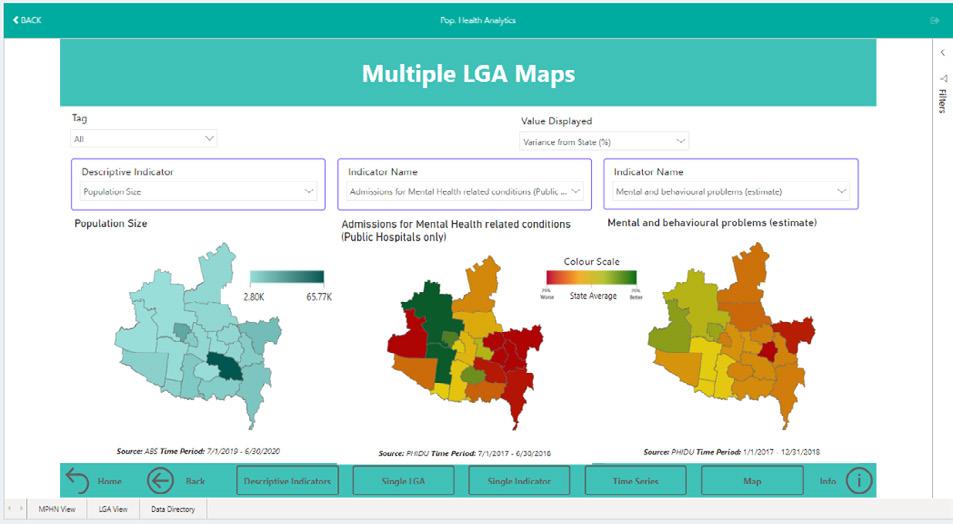
Whilst the above allows MPHN to determine which health conditions or demographic variables are of concern against a National profile with local and state considerations it does not detail at a local area within the PHN where services should be improved. MPHN has a varied profile including regional and more remote communities with specific health and social needs. MPHN use the table below to provide evidence of location need. The MPHN LGA view demonstrates each LGA and the variance from the MPHN average or the State average. Single indicators can be viewed visually to determine where they sit in MPHN in relation to each other. Single LGAs can be viewed for all relevant indicators and there is a map feature for additional comparisons.
Figure
Figure 9. MPHN Population Health Analytics Tool – LGA view
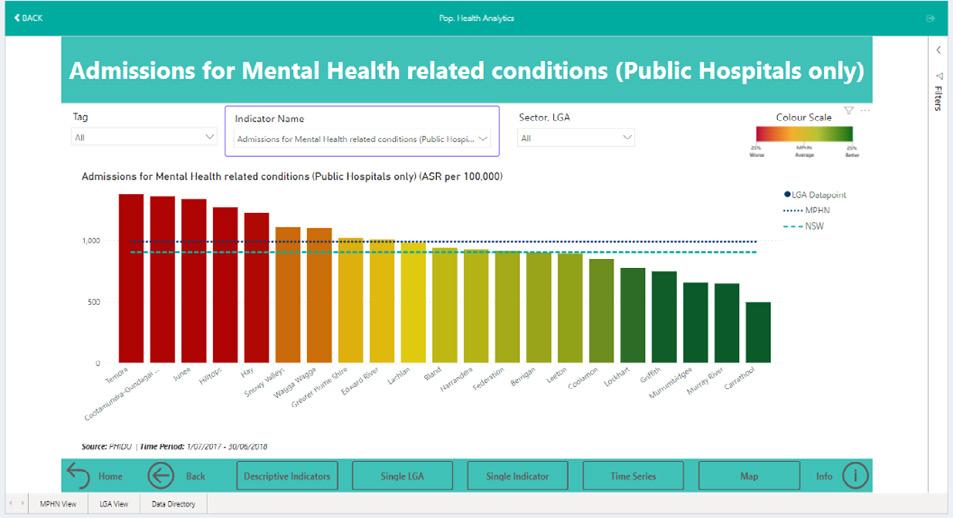
Figure 10. MPHN Population Health Analytics Tool – LGA view – Single indicator
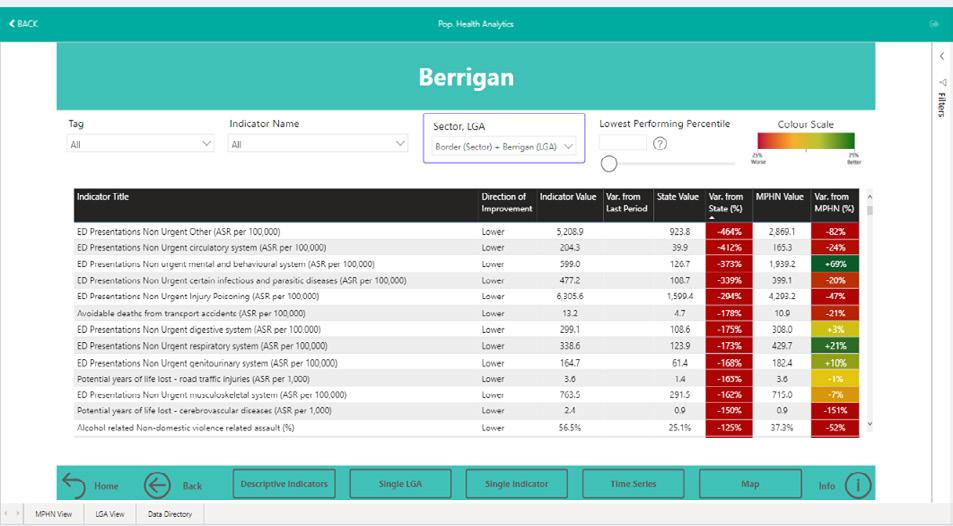
Figure 11. MPHN Population Health Analytics Tool – LGA view – Single LGA
Once collection of evidence of health needs has been completed, information can be populated to the Commonwealth template exampled below in table 2. Table 2 provides an example from the Commonwealth that identifies the key issues and a description of the evidence. The description of the evidence will include reference to the source of the information to allow validation if required.
Table 2. Outcomes of the health needs analysis
This table illustrates how findings of the health needs analysis can be summarised.
Identified Need
Key Issue
e.g. Health status Poor self-assessed health status in (specific locations)
e.g. Chronic disease Lifestyle and risk factors impact on the development of (identified) chronic diseases
Description of Evidence
NHPA analysis of ABS Patient Experience Survey 2013–14. Variation within PHN obtained through consultations. Utilisation of hospitals and general practices.
Variations between population groups and locations. Evidence from community consultations on diet, smoking, drug and alcohol use, physical activity and health determinants.
Hospitalisations for chronic diseases.
Step 3
Identifying service needs
Review service use across the region
MPHN will utilise gold standard data sets that provide data on services delivered such as MBS and PBS items. Hospital and emergency department data will be sourced and confirmed by local health district data experts. General practice data will be used to confirm findings of nationally available public data such as MBS and PBS data.
Undertake service delivery mapping
MPHN will review and update its CRM service database which informs the availability of services throughout the region across all health disciplines. This process is a continual process undertaken by the Primary Care Engagement Officers who regularly interact with the community and health care professionals.
Annually MPHN will conduct a census audit of general practice which updates all general practice workforce data and service availability. Simultaneously this census will collect data that informs the continuous professional development required in general practice that is provided by MPHN as part of its workforce strategy.
Desktop reviews along with special projects to supplement information as required will also be considered as part of this element of the health needs assessment. Recommendations from the Commonwealth in relation to health workforce could include:
• Number and distribution by type, such as GPs, allied health, pharmacy, specialist services such as psychiatry, community health services etc.
• Characteristics such as full or part time, public versus private, qualified but not working in health care etc., advanced skills; and relationships between professional groups.
Further the Commonwealth recommendations for service mapping include identifying and documenting a range of services available and will consider aspects such as:
• Location – physical location include outreach, hours of opening
• Utilisation – including MBS and PBS data, a range of hospital data, such as use of Emergency Departments and Potentially Preventable Hospitalisations, other measures of occasion of service
• Accessibility – including financial and cultural barriers and access to specialists and secondary referred services, access to services after hours
• Responsiveness – such as wait times
• Capability – such as skills and competence
• Acceptability – such as cultural sensitivity, patient experience of and satisfaction with the quality of care
• Quality – such as practice accreditation and PIP enrollment.
The AIHW defines effectiveness as how well the outputs of a service achieve the stated objectives of that service. Indicators to measure this cover characteristics such as access, quality and appropriateness, including issues such as cultural competency of services for Indigenous and CALD communities. Horizontal equity is exhibited when services are equally accessible to everyone in the community with a similar level of need, and vertical equity is exhibited when it accounts for the special needs of certain groups in the community and adjusts aspects of service delivery to suit these needs.
MPHN will take the above recommendations and definitions into account when mapping services and programs across the sector. It is noted that the sophistication of service mapping techniques will increase over time.
Review internal data sources from commissioned services data
MPHN will utilise its Data Analytics Platform to analyse data from services that have been commissioned. Data for Mental Health, Alcohol and Other Drugs, Allied Health, Integrated Chronic Care, Integrated Team Care, After Hours and any other relevant data sets collected by the MPHN and analysed in its DAP will be used to confirm service use across the region.
Once collection of service availability has been completed, information can be populated to the Commonwealth template exampled below in table 3.
Table 3. Outcomes of the service needs analysis
This table illustrates how findings of the service needs analysis can be summarised.
Identified Need Key Issue
e.g. Service coordination
e.g. Mental health
Lack of easily understood and accessible referral pathways across settings and providers
Lack of child and adolescent psychiatry services in specific locations.
Description of Evidence
Proportion of GPs, community based medical specialists and allied health providers with secure messaging systems. Discharge information, analysis of directory and eligibility criteria for services, awareness of services from consultations with consumers and health professionals.
Identified through consultation with mental health workers and school counsellors.
Data on available psychiatric sessions per capita, waiting list for assessment and caseload information.
Step 4
Prioritisation and activity work plans
Triangulate profiles and other data and information
Once all data has been collected, both quantitative and qualitative, on health need (= demand), and service availability (= supply), priorities can be developed. It is important to note that service gaps will be identified when the number and amount of services used has been compiled in relation to the number of services that are required. Health needs, service needs and service gaps will form the basis of priorities for action.
It should be noted that not all data is publicly available. Where data informs the HNA and is able to be used for planning but is not able to be published the data will be suppressed.
Outcomes of the health needs analysis
Create final list of priorities for MPHN
Annually the Commonwealth, as an indicator expects submission of a Health Needs Assessment culminating in a list of identified health needs and potential options to address those needs.
Prior to submission to the Commonwealth the last important actions for the compiled priority list is to validate the results with key stakeholders. Key stakeholders would include identified staff from the Murrumbidgee Local Health District as a major partner in the process. Refinement of the list will occur based on validation feedback.
Identify options for commissioned services or programs to address identified priorities
An example of the Commonwealth recommendations for the final step of the Health Needs Assessment is the creation of the opportunities, priorities and options table. This table provides the basis for future work in the Activity Work Plans that guide activity for the following 12 months. An example of this table is provided below (see table 4).
Table 4. Opportunities, priorities and options
This table illustrates how PHNs can summarise the priorities arising from the Needs Assessment and options for how they will be addressed.
Opportunities and priorities
Aboriginal and Torres Strait Islander
Increase respect and reduce racism and discrimination Aboriginal and Torres Strait Islander Health Appropriate care (including cultural safety)
HSI230.1 Collaboration with the Aboriginal population
The purpose of the Murrumbidgee Aboriginal Health Consortium is to work together and with the community to coordinate action that improves the wellbeing of Aboriginal and Torres Strait Islander people living in the Murrumbidgee region.
AOD407 Aboriginal and Torres Strait Islander employment initiative
Support Aboriginal and Torres Strait Islander people whose substance use is impacting their ability to gain or maintain employment or participate in education.
Endorsement of the needs assessment
Once validation has been completed the Health Needs Assessment will be detailed to the Clinical Councils and the Community Advisory Committee of the MPHN. Once endorsed the MPHN Board will consider its recommendations and approve submission to the Commonwealth or request amendments. Once submitted and during the process of waiting for Commonwealth approval, planning for services for the next 12 months will commence. This planning is detailed below.
Planning
Importance of planning
The delivery of health services occurs in an ever changing environment with increasing community expectations, government priorities and technological advances. Limited health budgets combined with increasing pressures and demands result in the essential need to ensure that services are well planned and have the capability to respond to evolving changes in order to meet community needs. The ageing population and the increasing prevalence of chronic diseases through the region are factors that influence the pressure on the health system.
Understanding the current situation and demand for services and taking into account the future demand for service is an important element of planning. Resources available for commissioning of health services are limited. Identification and prioritisation of health needs and service issues identified through the needs assessment process support resources being directed towards the areas of greatest need.
Other aspects of planning that are important include
• Ensuring needs of particular populations such as Aboriginal and Torres Strait Islander peoples and Culturally and Linguistically diverse are met
• Ensuring that services are coordinated, reducing duplication
• Ensuring equity in service delivery by commissioning accessible services
• Improving population health outcomes
• Provision of quality services
• Provision of culturally appropriate services
• Considering service efficiency cost effectiveness and viability, and
• Providing safe and sustainable services.
Development of activity work plans
Once we have identified needs, we work to identify priorities and options for commissioned services. We collaborate with consumers, communities, clinicians and other stakeholders through co-design to prioritise needs, and find solutions.
Annual planning is driven by our needs assessment, but is also informed by other factors that need to be considered like cost, capacity and timing. The key output of the Strategic Planning phase is Activity Work Plans, which set out our agreed priorities and initiatives to address them.
We’re committed to collaborating with existing and new partners to deliver a seamless experience for consumers and carers across the health journey, without duplicating efforts. This means working closely with partners throughout the planning phase to identify how we can better work together and coordinate our responses.
Activity Work Plan development could include options and priorities that:
• May be considered and supported by PHN flexible funding
• May be undertaken using program specific funding
• May be led or undertaken by another agency.
Activity Work Plans have a prescribed template from the Commonwealth and have guidelines for each of the major schedules that are consulted during the development phase.
Key information for each activity
The Commonwealth Activity Work Plan template includes the following variables.
Table 5. Activity Work Plan – Activity template
Variable Notes
Title for activity
Activity title
Existing, Modified or New activity
Program Key Priority Area
Including unique reference numbering
Drop down list
If activity is existing or modified, provide the relevant reference/s from previous Activity Work Plan/ and page number
Drop down list
7 Commonwealth priorities
Needs Assessment Priority As identified in the Priorities, Options and Opportunities Section of the Needs Assessment, provide the number, title and page reference for the priority that this activity is addressing
Aim of Activity
Description of activity
Target population cohort
Indigenous specific
Coverage
Consultation
Collaboration
Activity milestone details (duration (dates for activity (planning procurement) and service delivery
Commissioning method and approach to market
Decommissioning
Planned expenditure & Funding sources
Describe what this activity will aim to achieve, and how it will address the identified need
The description of the activity should include both the strategy and outcome to be achieved
How the activity and/or services will be delivered
Specific population ie youth, older people, general population
Drop down list (Yes/No)
If yes, briefly describe how this activity will engage with the Indigenous sector
Describe where the activity will be provided
Where area covered is not the whole PHN region, provide the statistical area as defined in the Australian Bureau of Statistics (ABS), or LGA
Provide details of stakeholder engagement and consultation activities to support this activity
List and describe the role of each stakeholder that will be involved in designing and/or implementing the activity, including stakeholders such as Local Health Networks, state/ territory governments, or other relevant support services
Provide the anticipated activity start and completion dates (including the planning and procurement cycle)
If applicable, provide anticipated service delivery start and completion dates (excluding the planning and procurement cycle)
Set of three questions dealing with approach
Including approach, co-design, joint commissioning, previous history
Drop down list (Yes/No)
If yes, provide a description of the proposed decommissioning process and any potential implications
Table indicates funding sources across years and relevant to the particular schedule
Activity Work Plans are created in PPERS in accordance with the Commonwealth guiding documents. Plans and budgets will be developed for priority areas considering the appropriate schedule for each of the below funding streams
• Core and flexible funding (including health system improvement, flexible and corporate governance)
• Primary Mental Health (Including Empowering our communities and Aged Care)
• Alcohol and Other Drugs (National Ice Action Strategy (NIAS)
• Integrated Team Care
• After Hours
• National Psychosocial Measure
• Other specific projects, such as Greater Choice at Home Palliative Care and Bushfire response
The Activity Work Plan process is detailed in figure 13 to follow.
Annual planning process
Figure 13. MPHN Activity Work Plan Process Development stage
November 20XX
Needs assessment with priority list of needs to be addressed circulated to all participants; Responsible: Planning; Purpose: Ensure that all priority needs are covered by planned activity
December 20XX
Review of existing AWP contracts (5-6 month interim review of contract, including compliance with funding and KPI activity);
Responsible: Portfolio Managers and Managers; Purpose: Relevance of contracts ongoing
December 20XX
Interim allocation of priority areas in AWP budgets; Responsible: Planning; Purpose: Consider Commonwealth instructions, provide indicative amounts for each priority area
Meeting 1: December 20XX
Review meeting
Responsible: All participants;
Purpose: Form first draft of AWP taking into account needs, existing activity, opportunities for new activity; Outcome: Planning will develop draft plan and budget (PPERS), and additional working budget
Meeting 2: December 20XX
Responsible: All participants; Purpose: Provide final draft of plan for ratification prior to submission to Executive and Board for approval
Consultation stage
Community Advisory Committee and Clinical Councils
January 20XX
Consultation:
Responsible: Clinical Council Community Advisory Committee; Purpose: Review consultation results and development of activities to meet needs; Outcome: Comments included and endorsement of penultimate plan
Submission stage
January 20XX
Executive Review: Responsible: Executive
Purpose: Review penultimate final draft of plan and budget Outcome: Planning will finalise penultimate plan and budget
January 20XX
Board Review: Responsible: CEO and Board Purpose: Review final draft of plan and budget Outcome: Planning will finalise plan and budget
February 20XX
Upload to Commonwealth (PPERS): Responsible: Planning Purpose: Ensure that plan and budget are entered for submission to the Commonwealth
Approval stage
Conditional – Respond to Commonwealth requests and submit response
In full – Remove $ values and PDF form for lodging on PHN website. Distribute link to staff Finance Manager update finance system budget Finance Manager updates working budget and records contracts as approved (MayJune 20XX and as required throughout 12 months cycle)
Timeframes
The diagram below provides a high level overview of the timing of our commissioning activities. It has been designed to align with submission of required deliverables to the Department of Health, and shows the changing focus of our commissioning activities each quarter. In reality, however, all of our commissioning activities are ongoing throughout the year.
Strategic planning
Procuring services Monitoring and evaluation
Stakeholder engagement
Health needs assessment products
Overall Regional summary including at a glance profile and outlining high impact population and health conditions and behaviours. This summary will take a social determinant, person centered approach to specific population’s which is aimed at the consumer. The summary includes the Commonwealth template populated with health and service needs and priorities and potential options.
LGA level reports that describe the population and the needs of that population in order to address the deficits using a social determinants approach (ie inclusion of housing, education, health etc) at the local level.
Including in both the Regional summary and the LGA level reports are databooks with all the facts and justifications that support the identification of the existing high impact profiles above.
Data sources
Data will be sourced from both internal and external sources including but not limited to:
Geographic, demographic & health status and health behaviours –LGA level
• Australian Bureau of Statistics (ABS) Census and Census-derived data on demographics, including the Socio Economic Indices for Areas (SEIFA) and profiles of health including the National Health Survey, the National Nutrition and Physical Activity Survey and the National Health Measures Survey, the National Aboriginal and Torres Strait Islander Health Survey, the National Aboriginal and Torres Strait Islander Nutrition and Physical Activity Survey, and the National Aboriginal and Torres Strait Islander Health Measures Survey
• Australian Institute of Health and Welfare (AIHW) and National Health Performance Authority (NHPA) datasets and publications, including the METeOR metadata registry
• Information on the PHIDU website, such as the Social Health Atlas of Australia
• Information on Indigenous data from a range of sources
• NSW Cancer Institute
• The Australian Childhood Immunisation Register
• State and Territory Health Department data
• Local Government data
• Child Education and development data
Service data – LGA level
• Medicare Benefits Schedule (MBS), Pharmaceutical Benefits Scheme (PBS) and Practice Incentives Program (PIP) data
• Data from Local Hospital Networks or equivalents (including acute and community care services)
• Aged care data (both residential and community based) such as Commonwealth Home Support Program, or Department of Veterans Affairs (DVA) data
• Mental health data such as the National Mental Health Service Planning Framework database
• The National Notifiable Diseases Surveillance System
• Resources from the Royal Australian College of General Practitioners (RACGP)
• Data from practices through clinical audit Tools
• Health workforce data
• National Health Services Directory (NHSD) and Healthdirect