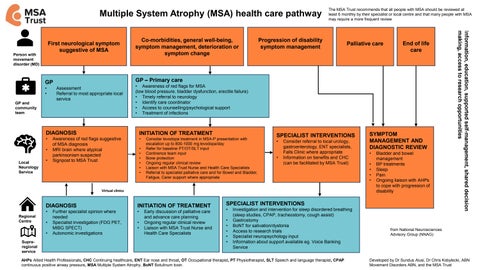

Multiple System Atrophy (MSA) health care pathway
First neurological symptom suggestive of MSA
GP
• Assessment
• Referral to most appropriate local service
Co-morbidities, general well-being, symptom management, deterioration or symptom change
– Primary care
Progression of disability symptom management
The MSA Trust recommends that all people with MSA should be reviewed at least 6 monthly by their specialist or local centre and that many people with MSA may require a more frequent review
Palliative care
End of life care
• Treatment of infections Person with movement
• Awareness of red flags for MSA (low blood pressure, bladder dysfunction, erectile failure)
• Timely referral to neurology
• Identify care coordinator
• Access to counselling/psychological support
DIAGNOSIS
• Awareness of red flags suggestive of MSA diagnosis
• MRI brain where atypical parkinsonism suspected
• Signpost to MSA Trust
INITIATION OF TREATMENT
• Consider levodopa treatment in MSA-P presentation with escalation up to 800-1000 mg levodopa/day
• Refer for baseline PT/OT/SLT input
• Continence team input
• Bone protection
• Ongoing regular clinical review
• Liaison with MSA Trust Nurse and Health Care Specialists
• Referral to specialist palliative care and for Bowel and Bladder, Fatigue, Carer support where appropriate
SPECIALIST INTERVENTIONS
• Consider referral to local urology, gastroenterology, ENT specialists, Falls Clinic where appropriate
• Information on benefits and CHC (can be facilitated by MSA Trust)
SYMPTOM
MANAGEMENT AND DIAGNOSTIC REVIEW
• Bladder and bowel management
• BP treatments
• Sleep
• Pain
• Ongoing liaison with AHPs to cope with progression of disability
DIAGNOSIS
• Further specialist opinion where needed
• Specialist investigation (FDG PET, MIBG SPECT)
• Autonomic investigations
INITIATION OF TREATMENT
• Early discussion of palliative care and advance care planning
• Ongoing regular clinical review
• Liaison with MSA Trust Nurse and Health Care Specialists
SPECIALIST INTERVENTIONS
• Investigation and intervention for sleep disordered breathing (sleep studies, CPAP, tracheostomy, cough assist)
• Gastrostomy
• BoNT for salivation/dystonia
• Access to research trials
• Specialist neuropsychology input
• Information about support available eg. Voice Banking Service
disorder (MD) GP and community team