
GET OUT!
Winter is unoffically over, even if we happen to get a few more frigid days. Meteorologists view the first day of spring as March 1, while the astonomical spring doesn’t kick off until March 20.
Either way, this is a great time of year to get out and do stuff. Walk! Rake! Bike! Pickleball! Plant!
Why now, specifically?
If spring is here, 99-degree weather can’t be far behind. Not to mention 99-percent

Kids playing outside in 2026
humidity.
It’s possible that some reading this are members of that strange “the-hotter-thebetter” tribe. For you, there’s no rush.
Of course, most of us have tons of practice being outside. As kids during vacations and on weekends back in the day, we couldn’t wait to get outside to play, all day every day until dark. Yes, every day. We climbed trees, played in the woods, rode our bikes everywhere, got up impromptu baseball and football games, pretended to be cowboys and Indians or soldiers in battle or astronauts. We built forts in the backyard, tried to dig our way to China, picked hot apples from trees in neighbors’ yards in summertime, explored empty houses (whether new construction or vacant and “haunted”), and when the sun went down we played hide-and-seek, caught lightning bugs and sometimes camped out all night in our own backyards — but always got scared and were inside, snug in our beds long before midnight.
We did all of this without much parental supervision. Kidnappers were as rare as they are today, but parents then knew that.
Please see GET OUT page 3
EVERYBODY HAS A STORY
Our oldest daughter, Olivia, caught measles. At the time she was seven years old. As the illness took its usual course I can remember reading to her often in bed and not feeling particularly alarmed about it. Then one morning, when she was well on the road to recovery, I was sitting on her bed showing her how to fashion little
animals out of colored pipe-cleaners, and when it came to her turn to make one herself, I noticed that her fingers and her mind were not working together and she couldn’t do anything.
“Are you feeling all right?” I asked her.
“I feel all sleepy,” she said.
DRESS FOR SUCCESS








PARENTHOOD
by Dr. Warren Umansky, PhD
You have just replaced the children’s tablets for the fourth time. They get into fights over who is playing which games or watching which videos. You wish they would be as passionate about school or going to the store with you or going outside to play. Their grades are not good. They rush through homework and won’t get off their games to eat or get ready for bed without a battle. What should you do?
A. They are kids and they should be doing the things they love. Furthermore, most jobs will be in the videogame/computer industry when they are older. They’ll be fine.
B. Set a timer for how long they can be on their tablets. That should take care of the problem.
C. Take the tablets away whenever they fight. Let them know they can have them back when they can use them peacefully.
D. Make electronics disappear at least during the school week. Make it a family rule that will not change.
If you answered:
A. Playing videogames and watching videos will not be careers at any time in the future. Being a gamer as a career means your child has a special combination of skills, personality, and something to offer that will attract thousands of viewers. Game developers, on the other hand, must know computer coding and computer language that is a whole different set of advanced skills than playing games and watching videos. And since their “play” involves constant fights, it doesn’t sound like fun and certainly interferes with what they should be doing to be productive.
B. Setting a timer might work, but if conflicts are still happening, school performance stays poor, and your children are not contributing to the family, that will be your signal that it isn’t working.
C. You likely are going to be accused of being mean. But, if you let them know that it’s their responsibility to show that they can follow your rules for using the tablets, this approach might help them learn more responsibility. It is important that you include in your rules getting homework completed neatly and correctly first, finishing chores, responding quickly when it is time to eat and get ready for bed, and treating their siblings and you with respect.
D. This is the very best approach. Speak to some of your friends or co-workers who have tried this approach. They will say that home life has never been so good. After two days of “detoxing” from their electronics habit, the children will have no reason to rush through school work. They will be more willing to go outdoors to play. They will read more, do crafts more, build Legos more, get along with each other better.
Electronics are toxic for children. They interfere with doing good schoolwork. They are a source of conflicts at home. They interfere with sleep, and they keep the children from engaging in healthier and more productive activities (riding bikes, shooting baskets, doing puzzles, reading, doing crafts). Try Option D. You will be amazed and pleased!

Dr. Umansky has a behavioral health practice for children in Augusta
THOUGHTS
THOUGHTS
ABOUT THOUGHTS
50 PARANOIA VS DELUSION:
“I KNOW THEY’RE TALKING ABOUT ME”
Editor’s note: Written by local mental healthcare professionals, this series explores how people may think and act when affected by common and lesser-known mental health conditions.
Angela is a 38-year-old office manager who recently began feeling uneasy at work.
The feelings were subtle at first. She noticed two coworkers whispering and laughing. She assumed it was about her. Soon, she began replaying conversations in her head, scanning for hidden meanings.
Whenever an email response was short, she interpreted it as intentional hostility.
Over time, her suspicions intensified. She became convinced her supervisor was monitoring her calls. She stopped eating in the breakroom. She avoided meetings.
When her sister gently suggested that the situation might not be what she feared, Angela became frustrated. “You don’t see what I see,” she said. “They’re trying to push me out.”
Angela’s experience illustrates a spectrum many people don’t realize exists — the difference between paranoia and delusion.
What Is Paranoia?
Paranoia involves heightened suspicion or mistrust of others, often without sufficient evidence.
At milder levels, paranoid thoughts can occur during
Understanding the Spectrum Paranoia and delusions are not identical — but they can exist along a continuum.
FEATURE PARANOIA DELUSION
Flexibility Some openness to Fixed and other explanations unshakeable
Insight Partial or fluctuating Typically absent
Intensity Ranges from mild Firm conviction suspicion to severe despite evidence mistrust
Functional May cause strain Often causes Impact or anxiety significant impairment
Not all suspicious thoughts indicate psychosis. But when beliefs become rigid, all-consuming, and disconnected from shared reality, clinical evaluation is needed.
stress, sleep deprivation, or major life transitions. A person may question others’ motives or feel unusually sensitive to criticism. Importantly, reality testing is usually intact — meaning the individual can consider alternative explanations when presented calmly and rationally.
Paranoia becomes clinically concerning when it is persistent, distressing, and interferes with functioning.
What Is a Delusion?
A delusion is a fixed, false belief that remains unchanged despite clear evidence to the contrary.
Delusions are not simply strong opinions. They are rigid beliefs that are not culturally or socially supported and that resist logical discussion.
Common types include:
• Persecutory delusions (believing one is being harmed, followed, or conspired against)
• Grandiose delusions (believing one has special powers or identity)
• Referential delusions (believing neutral events contain special personal meaning)
• Somatic delusions (false beliefs about bodily illness or defects)
Delusions are typically associated with psychotic disorders but can also occur in severe mood disorders or medical conditions.
Signs
and Symptoms
Emotional Features
• Anxiety or fearfulness
• Irritability
• Social withdrawal
• Heightened vigilance
Cognitive Patterns
• Interpreting neutral events as threatening
• Jumping to conclusions with limited evidence
• Difficulty considering alternative viewpoints
• Rigid or fixed false beliefs
Behavioral Patterns
• Avoiding perceived threats
• Checking behaviors or excessive reassurance-seeking
• Confronting others based on suspicions
Please see THOUGHTS page 3
• Isolation from work or family
Functional Impact
• Occupational decline
• Relationship conflict
• Increased risk of depression or substance misuse
• Escalation to crisis if untreated
What Causes Paranoia or Delusions?
Multiple factors may contribute:
• Severe stress or trauma
• Sleep deprivation
• Substance use (especially stimulants or cannabis at high potency)
• Mood disorders such as bipolar disorder or major depression with psychotic features
• Psychotic disorders such as schizophrenia
• Medical or neurological conditions affecting brain function
In many cases, vulnerability reflects a combination of biological predisposition and environmental stressors.
These symptoms are not character flaws. They reflect changes in how the brain processes threat, meaning, and interpretation.
Common Misconceptions
“If someone is paranoid, they’re dangerous.”
Most individuals experiencing paranoia are more fearful than threatening. Risk increases primarily when fear escalates to desperation or self-protection behaviors.
“You can just reason someone out of a delusion.”
Direct confrontation often strengthens the belief. Treatment focuses on building trust
and gently improving insight over time.
“Paranoia always means schizophrenia.”
Paranoid thoughts can occur in anxiety disorders, trauma-related conditions, depression, and during acute stress — not only in psychotic disorders.
“They’re just being dramatic.”
The distress is real. Even when beliefs are inaccurate, the emotional experience is authentic and often overwhelming.
Treatment
Treatment depends on severity and underlying cause.
Psychotherapy
Cognitive Behavioral Therapy (CBT) helps individuals examine thought patterns and consider alternative interpretations.
Trauma-focused therapies may reduce hypervigilance when paranoia stems from past harm.
Medication
Antipsychotic medications may be indicated when delusions are present or when paranoia significantly impairs functioning. Mood stabilizers or antidepressants may be used when symptoms are part of a mood disorder.
Lifestyle Stabilization
• Sleep restoration
• Reduction of substance use
• Stress management
• Structured daily routine
Family Education
Loved ones benefit from learning how to


respond calmly, avoid power struggles, and encourage professional support.
Prognosis
With early intervention, many individuals experience significant improvement.
Mild paranoid thinking related to stress may resolve fully with therapy and stabilization. Delusional symptoms often require longer-term treatment but can become manageable, allowing individuals to return to work, relationships, and meaningful daily life.
Left untreated, rigid false beliefs can become more entrenched and impair functioning. Early support improves outcomes and reduces crisis risk.
Understanding the distinction between suspicion and psychosis allows families and providers to intervene earlier — before mistrust becomes isolation.
About Us
IPS (Integrated Psychiatric Solutions) provides inpatient and outpatient mental health services, with or without a referral, to help patients and their families progress through the care journey. To make an appointment, call 706-204-1366 or visit integratedpsych.care.
Parents today seem to think something evil is lurking around every corner, and will sometimes call police if they spot a child alone in a park or walking down a quiet neighborhood street.
An article by James Campbell in the Los Angeles Times a few years ago cited a study showing that many children today “spend less than 30 minutes per week playing outside,” but average as much as seven hours a day glued to TV screens, tablets, smart phones and video games. Yikes.
It’s not hard to imagine that those statistics are worse today than they were a few years ago.
We adults, meanwhile, those former outside kids, spend 93 percent of our lives inside buildings or vehicles, said a study cited by Campbell.
Granted, we have had the “it’s too cold” excuse for months, but seven or eight straight months of pleasant weather are looming on the horizon. This is a great time to establish some heathful active habits that don’t involve a screen, a recliner, or a remote.
Let’s get out! And stay out!
www.AugustaRx.com

www.Facebook.com/AugustaRx
Who is this?
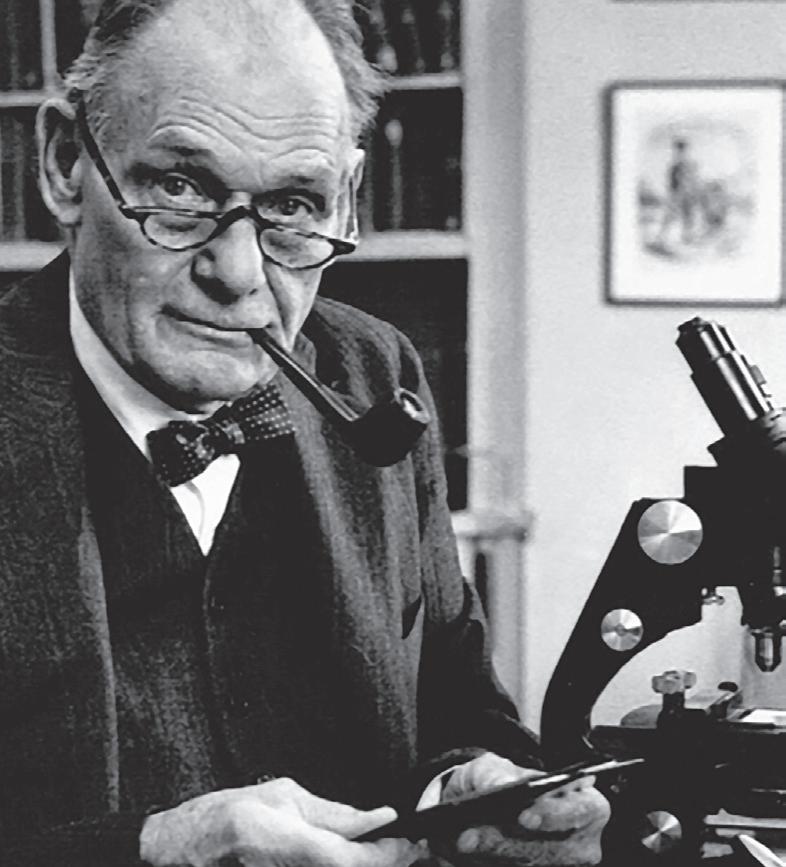
Should we light a candle for the days when doctors could smoke a pipe while carrying out their duties? You know what — let’s not.
But it was what it was, as the picture above shows. As you can clearly see, that’s John F. Enders puffing away near his microscope. He took quite a convoluted to get to this page.
He was born in 1897 in West Hartford, Connecticut into a somewhat prominent family. His grandfather John was the founder of Aetna Life Insurance Co., and his father John was the president of Hartford National Bank, whose financial clients included Mark Twain. When he (John) died, he left our John $19 million.
What would he do with that kind of money?
After high school he went to Yale, where he majored in English with the goal of becoming an English teacher. However, World War I interrupted his studies, and he went off to war as a Navy pilot. By the time he returned, he had changed his career plans. As he pursued his degree at Harvard he worked in real estate, even though he graduated with a Masters in English. While he worked on his thesis for his English Ph.D., one of his roommates was an instructor in Harvard’s department of bacteriology and immunology. Enders would just hang out with his friend in the lab and watch him work.
Through this acquaintance, Enders met the head of the department, Hans Zinsser. That was a turning point, because Zinsser was not only a scientist; he was a lover of literature amd had even published poetry in The Atlantic Monthly. John Ender had found his career path. It wasn’t English. It wasn’t business or real estate. It was bacteriology and immunology.
Within less that a decade after getting his Ph.D., Enders was running an infectious disease lab at Boston Children’s Hospital. Within another decade Enders and two colleagues successfully grew poliovirus in cultured cells, enabling mass production of the polio vaccine.
For this accomplishment, Enders and his two collaborators won the 1954 Nobel Prize.
That same year Enders and another colleague did something similar with the measles virus. By isolating the it, a measles vaccine could finally be produced and tested, and when Enders was hailed for that accomplishment in a September 1961 article in The New York Times, he immediately wrote the paper to correct the story: credit for the discovery belonged to an entire team, not to him alone. The letter marked a stark contrast from Jonas Salk, who that same year failed to credit the researchers upon whose work the “Salk” vaccine was based.
John Franklin Enders, who has been called “The Father of Modern Vaccines,” died at age 88 in Connecticut.

ADVENTURES IN
Middle Age
BY J.B. COLLUM
I was proud of myself Saturday night.
There I was at Chili’s, executing what I believed to be a masterclass in parking precision. I had dropped Lorie off at the door — as is our long-standing marital peace treaty — and circled back to find a spot. This arrangement works beautifully. She gets chivalry. I avoid the impossible task of locating the exact parking space she would have chosen herself — odds roughly equivalent to the Atlanta Falcons winning the next Super Bowl and me winning the lottery (which I don’t even play)
I found an edge spot. Tight but workable. Checked my mirrors. Used the backup camera. Parked flawlessly. Then I stepped out of the truck.
Friends… I was parked at an angle that suggested either:
• I completely lost all depth perception, or
• The Earth’s magnetic poles had shifted during my parking attempt.
If you use all available technology and still get out of your vehicle wondering how you managed to park like you were fleeing a crime scene… you might be middle-aged.
Now let’s talk about the wings. It was late. Too late for dairy. But Chili’s boneless wings with blue cheese dressing were calling my name. And when I say I use blue cheese, I don’t mean a polite dip. I mean those wings receive the full spa treatment. Deep immersion. Full coverage. Blue cheese baptism.
The servers there know me. They bring extra dressing automatically. Extra drinks, too. When I’m eating I consume my drinks the way I imagine a resurrected 4,000-year-old mummy would if he was discovering sugary carbonated drinks for the first time.
What followed on the drive home was… pressure. Not atmospheric. Not emotional. Digestive.
Despite the cold, Lorie had her window down. I’ll let you figure out why.
We developed what can only be described as a tactical extraction plan for when we reached the driveway:
1. She exits the vehicle at low speed.
2. Sprints to unlock the door.
3. Secures the hallway.
4. Clears the master bathroom.
5. Leaves all doors open and ensures no obstacles in my path.
This is not romance. This is coordinated middle-aged survival. It is something that you arrive at after decades of marriage and lots of practice.
If you have to strategize bathroom access like a military operation because you chose dairy after 8 p.m.… you might be middle-aged.
Then Sunday morning arrived. I had a sore throat, sniffles, dry cough, headache. The unmistakable feeling that my immune system had decided to clock out early.
I suspect it was COVID, but I never got it

officially confirmed. What I did confirm is that illnesses hit differently now. They don’t slow you down. They take you down.
I had a doctor’s appointment Tuesday and figured I’d keep it. I was dragging, but I’d already done the paperwork online — which apparently counts for nothing.
I arrived 13 minutes late. Thirteen. The front desk lady winced and said, “Let me make sure your PA will still see you.”
Apparently this particular PA runs on something more precise than Swiss rail schedules — and with less grace.
I was informed that I would need to reschedule. I will not share with you the words that passed through my mind. I will say I was proud they did not pass my lips.
If you remember a time when doctors ran hours late for you — but now you are the one penalized for being 13 minutes late… you might be middle-aged.
I briefly considered going to another one of their clinics since they already have all my information and I could just switch to another caregiver — maybe one that actually cared
But as I passed Bojangles, my stomach reminded me I had been fasting for blood work, so I made an executive decision.
Biscuit therapy. It’s a thing. Trust me. If you don’t believe me, try it. After that, I attempted to head toward another one of their clinics as I had been planning before the Bojangles sign enticed me — but halfway there, fatigue overtook ambition. I rerouted home.
I went straight to bed. slept from that moment until approximately yesterday morning. At some point, I attempted to watch television. I started shows. I started YouTube videos. I finished none of them. That’s my life now.
If you routinely fall asleep watching something you were genuinely excited to watch… you might be middle-aged.
If getting sick now requires three days of hydration, sleep, and negotiations with your own body… you might be middle-aged.
If dairy after dark is a calculated risk with known consequences… you might be middle-aged.
And if you still think you nailed that parking job — until you open the door and reality corrects you — well…
Welcome to the club.
The good news? We survive. We adapt. We hydrate. We strategize.
And sometimes we even park straight. Until next time — stay chivalrous, avoid late-night dairy, always have a bathroom extraction plan, and maybe get a really good air freshener for the car.


J.B. Collum is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com

Special Forces
Parenting
Last weekend, we attended an all-day assembly in Orangeburg, South Carolina. It was a full day of meaningful, faith-building information. To adults, it’s encouraging and uplifting. To an eight-year-old — especially our special needs granddaughter, Freyja — it probably feels like a very long day of being told to sit still and be quiet. I can understand how frustrating that must be for her.
At home, we celebrate every sound she makes. As we’ve chronicled in this column, Freyja hasn’t learned to speak yet, and there is no guarantee she ever will, but she is trying. She sings along as best she can with movies. She makes sounds, and we parrot them back to show her we hear her. Every attempt matters.
But an auditorium with nearly 2,000 people sitting quietly with their Bibles? That’s a very different environment. There is singing. The music is probably a welcome break for her. But mostly, it’s sitting.
Listening. Waiting. With only a midday lunch break to stretch.
These events have always been tough with Freyja. We’ve tried just about every strategy we could think of. When she gets too loud or fidgety, one of us takes her to the lobby, where there’s a beautiful waterfall. If that’s not enough, sometimes we step outside. This time, though, it rained nearly all day.
Before we went, I asked the family to keep the day in their prayers. I also asked that we all make a conscious effort not to react at the first sign of trouble — to be patient, steady, calm. We agreed.
And would you believe it? It worked. She only had to be taken out briefly twice — and both times it was for a diaper change. She even slept through part of the program,

which we were perfectly fine with.
I’ve come to believe that children mirror the emotional posture of the adults around them. They read our faces. They sense our tension. They respond to our body language. Because we made a deliberate, prayerful effort not to be reactive, I believe it showed — in our posture, in our expressions, in our steadiness when she made small noises.
And something else stood out.
The people around us weren’t bothered. They were kind. Supportive. Several even spoke with us before the program or during lunch about Freyja and her condition. We felt warmth. We felt understanding.
That’s a beautiful thing.
I truly believe most people are ready to help and ready to understand — especially when they see parents doing their best.
It feels different from when I was a kid. Back then, one little noise in a quiet setting and you expected to be scooped up and marched out immediately. You were already bracing for a spanking. Heads would turn. Some kids looked at you with pity. A few sweet grandmothers might smile kindly. But some adults — usually the ones without children — wore that irritated smirk, as if justice was about to be served.
Maybe that’s just my dramatic childhood memory talking.
But I do think, in many ways, things have changed for the better.
During intermission, we even met another family with a special needs child. We stood there talking about shared experiences — the challenges, the small victories, the learning curve. It was encouraging to connect with someone who truly understood.
In July, we’re attending a three-day event similar to this one. We’re hopeful. If it goes well for three straight days, wonderful. If it doesn’t, we’re prepared.
We’ll be staying at a camping resort with a lazy river and multiple pools. Our plan is to let her expend her energy each evening so she’ll rest more during the day. And if needed, there’s an online option. One of us can stay back at the camper for a quieter day or take her to the pool while the other attends.
That’s what Special Forces Parenting looks like sometimes — planning for success, preparing for Plan B. As the old military saying goes, no plan ever survives first contact with the enemy.
We are grateful for whatever progress comes. And there is progress. We see it — and that is a very good feeling.
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
This disgraced physician, Cecil B. Jacobson, belongs in a category all by himself; we have never profiled a doctor like him before; he holds a unique place on the pages of disgraceful medicine.
Exhibit #1: unlike every other person to appear on this side of this page, he didn’t kill anybody, not a single person.
Exhibit #2: he fathered up to 75 children.
Exhibit #3: he was born and died (in 2021) in Utah.

All of the above statements are true. We threw in Exhibit #3 to possibly throw you off the scent.
“So he practiced polygamy?” you might have thought. Unfortunately, the truth is far more disturbing.
Born in 1936, Jacobson in the 1960s was Chief of the Reproductive Genetics Unit at George Washington University Medical School and we have to say, even then the weirdness was already starting to show: he claimed to have impregnated a male baboon, and to have implanted his own sperm into the abdominal cavity of a female baboon (a pregnancy he said he terminated in its 4th month).
Fast forward a couple of decades and the 1980s found Jacobson operating a reproductive genetics center in Fairfax County, Virginia, specializing in treating women who had trouble conceiving and/or carrying to full term.
A couple of patterns developed in this practice. Many patients were injected with a fertility drug, and the results were good: Jacobson would confirm that they were pregnant, and he performed ultrasounds to show mothers their growing fetus. Alas, about the third month, Jacobson would often deliver the sad news that the fetus had died.
Although some of his patients did conceive and deliver healthy full-term babies, there were enough first trimester deaths to invite questions. A TV station got the probes started, discovering that most of the women had never been pregnant; Jacobson merely said they were; the “fetuses” shown in ultrasounds were just other nearby body parts.
Jacobson’s clinic also offered artificial insemination for infertile women by carefully screened anonymous donors. As it turned out, the donors weren’t anonymous at all; they were Dr. Jacobson. Investigators could never find a shred of evidence that any sperm donor donation program affiliated with the clinic existed, but they did find through DNA testing that at least 15 of his patients unknowingly delivered Jacobson’s children, and he is suspected of fathering up to 75 others without the knowledge or consent of the mothers.
PUBLIC HEALTH: BROADER THAN YOU THINK
Part 2 of a series
Public health is multi-dimensional and dynamic, revolving around the health and safety of populations and communities. Public health is far-reaching and rooted in studying health trends, applying best-practices for patient care, and offering services throughout urban and rural settings to respond to and meet our communities’ health needs.
Core public health functions include preventing disease; promoting health; fostering access to care; ensuring environmental safety; developing policy such as laws and safety standards aimed at saving lives; and reducing injuries.
Public health involves researching, collecting, and analyzing data to determine health and disease trends, identify risks, and propose solutions. We also measure and measure the results and effectiveness of interventions and programs.
You benefit daily
Even if you have never entered a County Public Health Department,
you benefit from public health services, whether you realize it or not. Public health is working ‘behind the scenes’ when you eat in a restaurant (food handling and preparation inspections), dip into public, club, or aquatic center swimming pools (testing water quality), experience a natural disaster (Hurricane Helene), get a tattoo or body piercing, or a when a disease outbreak like measles, salmonella, influenza or other communicable diseases strike your community.
The A to Z’s of public health range from Adolescent health, Baby and infant care, reproductive health, sports physicals, vaccines, and wellness checks to controlling the Zika Virus. Educating, building awareness, and informing the public are also central to delivering the ABC’s of public health, but for most of us, sifting
through the info avalanche can seem daunting.
Puzzled by the plethora of public health information?
With misinformation swirling around the internet, getting reliable public health and safety information can be confusing. Use these three “Who, What, Where” tips for learning about the accuracy, credibility, and reliability of public health info.
1. WHO: Know the source of your health information. Is the originator of the information credible? Public health professionals turn to unbiased epidemiology, research-based articles, and large studies that review the published literature to date.

Public health relies on many resources for the clearest, data driven recommendations for care.
We look closely at CDC information, but especially at other evidence-based
sources such as the American Medical Association (ama-assn. org), American Academy of Pediatrics (aap.org), the American Academy of Family Physicians (aafp.org; familydoctor.org) and the American Public Health Association (apha. org). Evidence-based care and recommendations are always the goal.
2. WHAT: What’s the evidence? Is the information a primary source of published research? How representative is the study population reflected in the data? Are sources cited? How recent is the information?
To help answer these questions, look to resources such as the Public Health Institute (PHI) (phi. org) which aims to strengthen public health work and build community programs using dependable data.
3. WHERE: Where can I access reliable public health information?
If web-surfing, go to established, reliable, and trusted organizations. The Mayo Clinic (mayoclinic.org) and the Cleve-
Please see PUBLIC HEALTH page 9
S I C K O F W A I T I N G ? S I C K O F W A I T I N G ?


TRYTHISDISH
CAESAR STEAK SANDWICHES
These sandwiches hit the perfect balance between meat and vegetable intake.
Ingredients
• 1 pound boneless beef top sirloin or top round; cut ¾ inch thick or flank steak
• ½ cup prepared non-creamy Caesar dressing
• 2 cups coarsely chopped romaine lettuce
• ¼ cup shredded Parmesan cheese
• 4 hoagie rolls (6-inches long each), split, toasted
Directions
Cut the beef steak lengthwise in half, then crosswise into 1/8 to ¼-inch thick strips. Reserve 2 tablespoons dressing. Pour remaining dressing in a medium bowl. Add beef; toss to coat. Cover and marinate in refrigerator from 30 minutes to 2 hours.
Remove beef from marinade; discard marinade. Heat a large nonstick skillet over medium-high heat until hot. Add ½ of beef; stir-fry 1 to 2 minutes or until outside surface of beef is no longer pink. (Do not overcook.). Remove from skillet; keep warm. Repeat with remaining beef.

Toss lettuce with reserved dressing and 2 tablespoons cheese in medium bowl. Divide evenly over bottom of each roll. Top with beef; sprinkle with remaining cheese. Close sandwiches and enjoy!
Nutrition Breakdown: Calories 632, Fat 21g, (6g saturated, 6g monounsaturated), Cholesterol 45mg, Sodium 800mg, Carbohydrate 70g, Fiber 4.2g
Protein 38g.
Recipe provided by: “Beef It’s What’s for Dinner”. For more information see: www.beefitswhatsfordinner.com
Kim’s note: This recipe is high in carbohydrate due to the hoagie roll. To make more room for the delicious fillings and decrease carbohydrate scrape out some of the inside of the hoagie roll.





For external use only. May be habit-forming. Take regularly; do not discontinue use unless advised by a physician. Product not child resistant. Do not chew or crush. Not to be taken by mouth. May be taken (read) on an empty stomach, or with food. May be taken one hour before or after meals. And at any other time. Product may not be gargled. Do not drive a motor vehicle or operate heavy machinery while reading. Tell your doctor if you are pregnant. Use in conditions of adequate light. Store in a cool dry place. Not to be used as a personal flotation device. Dispose of properly. Overeating, poor diet, cigarette smoking and excessive drinking may alter the effectiveness of this product. Do not use near spark or flame. Not dishwasher safe.
CAUTION: If you become too salubrious, please read fewer articles.


I WAS THINKING
by Pat Tante
WHAT SHALL I DO WITH JUNE? (PART III)
Editor’s note: In Parts I & II, Pat and June, traveling by urn (June that is, not Pat), have been racking up frequent flyer miles in a quest for a suitable final resting place for June. Thwarted by bad weather in the tropics, the pair is headed back to Augusta
During the flight I perused several magazines that I had bought at the airport. One article caught my eye. “Send Your Loved One Into Space.” A company is offering memorial spaceflights. Who knew? Your loved one could orbit the earth for $5,000, spend eternity on the lunar surface for $12,500 (who would guess that lunar property was so expensive) or be sent on a spaceflight and return to earth as a shooting star! Wow! For $1,000 this seemed more reasonably priced, plus you could have a DVD made of the return and accompanying memorial service (extra). Other options were available “depending on where you’re going and how much of you is going.” It was not cheap for an out-of-this-world experience.
I pondered this all the way home. I tried to send June a thought wave so that she could consider these fantastic options.
Upon arriving home, I placed June and her chocolate tin back in the sunny window and during the next weeks pictured myself organizing the send-off: mailing invitations, selecting an appropriate outfit, and calling a caterer. Yes, by all means, a caterer. I had planned for my own memorial service to include wine and snacks while my friends and family circled my Keepsake Cremation Urn.
I called Ned and asked if he had $5,000 so June could orbit the earth



and we could see her pass by on clear nights. Although he had given me June, he had not given me an inheritance along with her.
He was quite taken aback and said that I was really over-thinking where to put June and that she would probably be just as happy scattered in the local botanical garden. Probably under cover of darkness I was thinking. I could see myself traipsing fawn-like through the flowers fertilizing the beds with June. I hung up, disappointed that my wonderful plans had come to naught. I’m sure June was moping too.
I spoke to some friends at dinner one evening. What would they want if they were June? Gloria said that she would just park on the mantel in her son’s house as a reminder of his inattention and selfishness. She would stare down at her ungrateful grandchildren who never acknowledged a present or a card.
Lucy said that she didn’t care what they did with her – just shove her into a ditch and leave. I looked expectantly at Jack for his take. He said that cremation had never been his choice. He had told his kids that he wanted to be eaten by wolves or maybe sharks — good for the planet and good for the animals.


We all pondered this for a few minutes and tabled that discussion for another day. Well, at least we had plenty to talk about even if no one came up with anything worthwhile for June. I’ll bet they could hardly get to sleep that night. I had opened up a new avenue of worry.
Several days later, I was attending a small dinner party. The hostess was wearing a lovely heart-shaped pendant around her neck. I told her how unusual I thought it was. Oh, thank you, she said, it is a very special treasure because it contains the ashes of my dear mother. She will always be close to my heart. I muttered something like “how sweet” and fled to the living room. Cremation jewelry was not an option for me.
Days after the dinner party, a friend who had heard me discussing my predicament called. She said she had been reading a magazine in her doctor’s office and came across what she thought was a very intriguing advertisement. Entitled “Rest in Vinyl,” the article explained that you could press your loved one’s ashes into a record album – with music!
Will June spend eternity spinning at 33 RPM? Tune in next time for the exciting conclusion!



PUBLIC HEALTH
... from page 6
land Clinic’s Health Library (my.clevelandclinic.org/ health) are my “go to” sources for personal health information. A Consumer Health Information guide covers health and medical topics in lay language (https://libguides.mssm.edu/consumer-health-information) as does the familydoctor.org A-Z Health index.
For broader public health perspectives, I rely on well-respected medical and public health professions’ groups mentioned earlier, as well as organizations combatting health-related misinformation such as the Public Health Communications Collaborative (PHCC) (publichealthcollaborative.org). PHCC addresses a host of health topics and offers education and training that helps public health professionals and others become critical consumers of health information. PHCC provides resources, messaging, and learning opportunities to identify and counter misinformation. The Trust for America’s Health (tfah.org) delivers webinar briefings. The AMA offers a free subscription for timely position statements and news releases (https://fsso.ama-assn. org/sign-up). Our Canadian neighbors share a helpful tip sheet to evaluate health websites at cda-amc.ca/sites/default/files/pdf/CADTH_credible_websites_onepager.pdf.
Tip of the iceberg
The next time you buy a coffee, eat at your favorite food truck, decide to get a tattoo, or hear a news story about young children suffering from new cases of preventable measles, remember that a team of committed nurses, doctors, data clerks, epidemiologists, sanitation inspectors, IT specialists, and health educators at your county public health departments are working diligently to keep you healthy, safe, and well informed.
About the Author: Christine O’Meara, MA, MPH is a national, NC, and GA award-winning public and community health professional with 40 years’ experience, currently working as a grants specialist with the GA DPH East Central Health District.









CRASH COURSE

More Americans have died on US roads since 200 0 than in World Wars I & II combined
It might not be commonplace, but there are probably people out there who read the subheading of this series (above, where it says more Americans have died on our roads just since 2000 than died in two world wars) and think, “that’s not so bad. It could certainly be worse.”
Well, if 10 million people died every year, even that could be worse. 11 million could die, for example.
If you’re wondering, the real fatality numbers for WWI & II deaths are roughly 535,000.
Vehicle crashes are one of the worst chronic causes of death in this and pretty much every country. Compared to other means of travel, it’s practically suicidal to drive. For example, many years there are zero fatal commercial aviation crashes. Even in a bad year, the number of fatal incidents would typically be in the single digits.
are vehicle sizes. Some older pickup trucks, like the old Chevy S-10, look like toys compared to today’s huge trucks. Larger vehicles pose a greater risk for pedestrians and the occupants of other cars.
Keep in mind also that roadway improvements always lag behind traffic volume. Most roads were designed for less traffic and lower speeds than they are being used for today.
South Carolina: You have work to do.
Rail travel, believe it or not, results in hundreds of deaths each year in the US, and boating accidents can add up in a bad year to around a thousand deaths.
All of those pale in comparison to the 35,000 to 45,000 people who die every year behind the wheel.
That’s why we sometimes feel here at Medical Examiner World Headquarters in Augusta that our subheading, as sobering as it might be, actually makes the problem seem less serious than it really is.
Consider: the world wars comparison, looks only at the twenty-something years since the turn of the century. Care to take a guess what the all-time grand total of traffic fatalities in the US might be?
It’s a shocking number: 3,996,709. That figure is from data compiled by the National Highway Traffic Safety Administration (NHTSA) for the years 1899 (26 deaths) through 2023 (40,990 deaths, which represents a drop from 42,514 in 2022 and 43,230 in 2021).
Why are traffic deaths so difficult to bring under control? After all, cars are much safer than they used to be, and roadway design incorporates many safety features not employed decades ago.
Several factors contribute to fatality numbers staying high, chief among them: more drivers, more cars on the road, and more miles driven. Added to that, unsafe driving behaviors like distracted driving are on the increase, and so
TELL A
Even so, it’s amazing how 40,000 or more annual deaths can slide under the radar almost unnoticed. The wartime casualties were concentrated in a relatively short time frame. That made them more shocking and more newsworthy. By comparison, highway deaths drone on at horrible levels year after year and just become part of the background noise. Plus they’re sprinkled here and there across the entire nation, one or two at a time across millions of trips and billions of miles traveled. They rarely receive national attention, and often not much coverage even in local news.
So it’s easy to miss significant traffic trends and developments. For example, many Medical Examiner drivers probably don’t know that they live in the most deadly state in the entire US.
That dubious distinction belongs to South Carolina. Per billion miles driven, it has the highest death rate of any state, 20.8. By comparison, Georgia’s rate is 14.9 deaths per billion miles. The national average is 13.7. Massachusetts gets the gold star with a rate of 7.1 deaths per billion miles driven.
The Palmetto State is pretty bad by other measures too. Per capita, it suffers more than 23 deaths per 100,000 people and an even 30 deaths per 100,000 drivers. For comparison, the national averages are 12.9 and 18.4, respectively. (Georgia’s rates are 16.7 and 23.4) All figures in the above two paragraphs are from 2021 fatality statistics.
If it all seems dreary and deadly, that’s probably because it is. Traffic safety experts had been slightly encouraged by a mini-trend of slow improvements in highway safety, but recent numbers have burst that bubble. In fact, a 2020-2021 surge in fatalities marked the largest percentage increase in the history of FARS, the Federal Analysis Reporting System.
They say the most important safety component in any car is the nut behind the wheel. Safe driving is largely up to you and me.
OLIVIA
... from page 1
In an hour, she was unconscious. In twelve hours she was dead.
The measles had turned into a terrible thing called measles encephalitis and there was nothing the doctors could do to save her. That was twenty-four years ago in 1962, but even now, if a child with measles happens to develop the same deadly reaction from measles as Olivia did, there would still be nothing the doctors could do to help her.
On the other hand, there is today something that parents can do to make sure that this sort of tragedy does not happen to a child of theirs. They can insist that their child is immunized against measles. I was unable to do that for Olivia in 1962 because in those days a reliable measles vaccine had not been discovered. Today a good and safe vaccine is available to every family and all you have to do is to ask your doctor to administer it.
It is not yet generally accepted that measles can be a dangerous illness. Believe me, it is. In my opinion, parents who now refuse to have their children immunized are putting the lives of those children at risk. In America, where measles immunization is compulsory, measles like smallpox, has been virtually wiped out.
Here in Britain, because so many parents refuse, either out of obstinacy or ignorance or fear, to allow their children to be immunized, we still have a hundred thousand cases of measles every year. Out of those, more than 10,000 will suffer side effects of one kind or another. At least 10,000 will develop ear or chest infections. About 20 will die.
LET THAT SINK IN.
Every year around 20 children will die in Britain from measles.
So what about the risks that your children will run from being immunized?
They are almost non-existent. Listen to this. In a district of around 300,000 people, there will be only one child every 250 years who will develop serious side effects from measles immunization! That is about a million to one chance. I should think there would be more chance of your child choking to death on a chocolate bar than of becoming seriously ill from a measles immunization.
So what on earth are you worrying about? It really is almost a crime to allow your child to go unimmunized.
Editor’s note: The open letter above, “Measles: A Dangerous Illness,” was written by children’s author Roald Dahl (Charlie and the Chocolate Factory, Matilda, The BFG, James and the Giant Peach, and The Twits, among others) in 1986 out of concern over the high and ongoing incidence of measles in the UK. The measles vaccine was approved in the UK in 1968, too late for his daughter, who died in 1962 from measles complications. Despite the vaccine’s availability, by the late 1980s there were still more than 80,000 cases of measles each year in the UK. That number seemed too high and absolutely unnecessary to Dahl (illustrated on page 1), who wrote the letter to encourage parents to get their children vaccinated.













Examiners
Looks like you got a new travel mug. Yeah, it’s kind of a pain.


Wherever I go, whatever I’m doing, I have to carry this mug around. What do you mean?
ACROSS
1. Easy stride
5. Short note
9. Breath sounds
14. Part of the eye
15. Saharan
16. Chicago film critic
17. Almost tailless rodent
18. Home of a noted medical school
19. Robust (Scottish)
20. 1969 bestseller (ending with “-Five”)
23. Character in The Matrix
24. Bottom-row key
25. His donkey spoke
29. A woman, in old movies
31. Just a little drink
34. Unwraps
35. Alpha follower
36. Main ingredient in some casseroles
37. Eye specialist
40. Swing around
41. Threaten, as a crisis
42. Locations
43. Lead-in for 56-D
44. Macon county
45. 2-point football play
46. Tavern
47. There’s a big one in Columbia County
48. Mathematical operation
56. Augusta ________
57. A month of the Jewish calendar
58. Sports award
59. Bladder liquid
60. Sea eagle
61. On the sheltered side
62. Noted apostle
63. No longer living
64. Monthly expense
by Dan Pearson
That is the craziest thing ever. Why?
CAPTION THIS
Check out our new reader contest on p. 11 Write your most appropriate, clever, or funny caption to the photo shown for a chance to win whatever cool swag we eventually decide to give away! Email your entry to Dan@AugustaRx.com
DEADLINE TO ENTER: 5:00 PM FRIDAY, FEB. 27, 2026 Have fun!
E X A M I N E R
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
1. They can be cyanotic
2. Spoken; verbal
3. Size of type
4. Jacob’s twin
5. He’s in Allstate commercials
6. Muse of lyric poetry
7. 1,760 yards
8. River in central Europe
9. A job for Hakky
10. Approximately 11. Optical device
12. Scottish Gaelic
13. Pigpen
21. Grind teeth together
22. Brightest star in the Aries constellation
25. Uplift
26. Singer Fiona
27. Tiny island west of Kauai
28. Poker stake
29. Send troops home at war’s end (in brief)
30. It comes from a Greek word meaning indivisible
31. Connected series of rooms
32. A map within a map
33. Nashville’s Cline
35. Early Steve McQueen movie (with The)
36. Week-ending abbreviation
38. Person used as one’s excuse
39. He founded al-Qaeda
44. Local high school
45. _______ Heart
46. Flying vehicle
47. Princess of Wales, 1981-1996
48. Female horse
49. Single entity
50. Piper adjective
51. Small harplike stringed instrument
52. It can precede gas
53. Small piece of land surrounded by water
54. Nasty type of fracture
55. No to Boris
56. It often follows 43-A
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
words to solve the puzzle above. All the listed letters following #1 are the first letters of the various words; the letters following #2 are the second letters of each word, and so on. Try solving words with letter clues or numbers with minimal choices listed. A sample is shown. Solution on page 14


ATHEBESTMEDICINE

ha... ha...
woman was found guilty before a judge in traffic court. She asked the judge for leniency in recognition of her community service.
“What type of community service do you perform?” asked the judge.
“I’m a school teacher,” she replied.
“Very well,” said the judge. “In consideration for your service I hereby waive your fine — on one condition.”
“Sure judge,” she said gratefully. “Anything you say.”
Gesturing toward a table at one side of the courtroom, he said, “I want you to sit down over there are write ‘I will not run red lights’ 500 times.”
Moe: The dermatologist told my dad he needs to start using sunscreen, but my dad absolutely refuses.
Joe: Why on earth does he object to that?
Moe: He’s a staunch Republican.
Joe: What’s that got to do with it?
Moe: The label says “apply liberally.”
Moe: I think somebody should create a recipe book for people who can’t cook.
Joe: Why don’t you do it?
Moe: You know what? I think I will.
Joe: I have an idea for your first recipe.
Moe: Tell me!
Joe: “How to Order Pizza.”
Moe: Math makes no sense.
Joe: Why do you say that?
Moe: Let me give you an example. Let’s say I cut a cake into three big pieces. Each piece would be 0.333 percent of the cake, right?
Joe: Right.
Moe: So if I multiply that number by three, I get 0.999. So what happened to the rest of the cake? Where’s the .0001?
Joe: On the knife, Einstein.
Moe: This recipe calls for 5 potatoes cubed.
Joe: Whoa! 125 potatoes? That sounds like a typo if you ask me.
Moe: I feel so bad for my neighbor.
Joe: Why?
Moe: They’re having a hard time right now and two days ago their water was cut off.
Joe: Isn’t there something you can do?
Moe: This morning I sent them a Get Well card.
Because try as they might, no one can stare at their phone all day.
Staring at my phone all day has certainly had no fffect on ME!

By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME
ADDRESS
CITY STATE ZIP
Choose six months for $26 ____ or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397

Dear Advice Doctor,
Advice Doctor

Whatever idea anyone might have of the ideal boss, mine is the polar opposite. He is mean, unforgiving, selfish and arrogant. He walks around all day every day with a chip on his shoulder against the whole world. I’m not sure there’s any advice you can offer that will change things, but that’s not really my question anyway. What I want to know is: how does someone like him get to be in management?
— One of the abused
Dear One,
I truly feel for you, and I offer my sympathies that this is something you have to deal with every day. As you suggest, maybe there isn’t a lot you can do, so let’s focus on him.
My immediate question is, why is he like this? What is so bad in his life that he is angry at the world all day every day?
I think I know the answer.
Your letter mentions that he has a chip on his shoulder all the time. That could be the problem right there. Being the boss can be stressful, and bone spurs form in the shoulder when the joint is exposed to chronic stress, from inflammation, and from general degeneration in the shoulder joint.
You don’t mention his age, but often as we get older cartilage in the shoulder (and elsewhere) becomes thinner, making movement less smooth. The body responds by generating extra bone (called osteophytes) to re-stabilize the joint. The same bone-building process can come from repetitive motion, chronic inflammation from bursitis, rotator cuff irritation, etc., or from old injuries.
The shoulder joint can be particularly susceptible to bone spurs, and the result is pain, stiffness, and grinding or clicking sensations, among others.
Your boss should see a doctor and get some relief. And it wouldn’t be just for him. It sounds like the whole office would benefit.
I hope this answers your question. Thanks for writing!
Do you have a question for The Advice Doctor about health, life, love, personal relationships, career, raising children, or any other important topic? Send it to Dan@AugustaRx.com. Replies will be provided only in the Examiner.





PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC Augusta Acupuncture Clinic 4141 Columbia Road 706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC

DERMATOLOGY
Evans Chiropractic Health Center

Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net

DENTISTRY
Jason H. Lee, DMD 116 Davis Road Augusta 30907
706-860-4048 Floss ‘em or lose ‘em!


Georgia Dermatology & Skin Cancer Center 2283 Wrightsboro Rd. (at Johns Road) Augusta 30904 706-733-3373 www.GaDerm.com


DEVELOPMENTAL PEDIATRICS
Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901
706-396-0600 www.augustadevelopmentalspecialists.com

Steppingstones to Recovery 2610 Commons Blvd. Augusta 30909 706-733-1935



Home Care Personal Care|Skilled Nursing|Companion 706-426-5967 www.zenahomecare.com

Parks Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com PHARMACY









MOVE-Lp(a) study
A clinical research study for people who have or are at risk for heart disease or stroke and have high Lp(a) levels

MOVE-Lp(a) is a clinical research study from Eli Lilly and Company. The MOVE-Lp(a) study will test if an investigational medicine safely lowers Lp(a) levels and reduces the risk for heart disease or stroke.
Can I join the study?
Yes, you may be able to join the study if you:
• are at least 18 years of age
• have a high level of Lp(a) in your blood
• already have heart disease or have had a stroke or are at risk for a first heart attack or stroke
visit
or scan the QR code

Lipoprotein(a) is also known as Lp(a). Lp(a) is an important risk factor for heart disease and is largely determined by your genes.
Lp(a) carries cholesterol (a type of fat) in the blood. If you have a high level of Lp(a), you may have a higher risk for heart disease or stroke. You may have a high level of Lp(a) even if you have a healthy lifestyle or are taking other medicine for your cholesterol.

CALL
Masters of Clinical Research 1232 Augusta West Parkway Augusta, GA 30909 Tel: (706) 210-8890