Dr Matt Doane Avant member

GPs are asking for a voice at the table and a greater role in preventative and posthospital healthcare.
It’s no secret that primary care plays an important role in keeping people well and out of hospital, and that healthcare cannot exist in silos.
Last year WA public hospitals were under significant pressure. It was labelled a crisis by representative bodies.
The state government is hoping to avoid the same pressure this winter, but that cannot be achieved without change.
As part of the solution the RACGP WA Faculty has called for a Chief GP Advisor to be appointed in the state. The person in this role would help bridge the gap between primary and secondary care, strengthen clinical governance across primary care and work with the state government to make healthcare more efficient.
GPs are asking for a voice at the table and a greater role in preventative and post-hospital healthcare.
But will such a role ever exist? In this edition we look at what a Chief GP Advisor in WA would look like and whether the role would work in WA.
While the RACGP continues to push for the role, the state government says it already meets regularly with GP representatives, such as the College, and has general practitioners employed within its clinical leadership teams to ensure their expertise were “embedded within core decisionmaking structures”.
Wading through the weeds of the response, it doesn’t look likely WA will have a Chief GP Advisor any time soon.
What do you think – do we need a Chief GP Advisor in WA? Email editor@mforum.com.au
SYNDICATION AND REPRODUCTION Contributors should be aware the publisher asserts the right to syndicate material appearing in Medical Forum on the mforum.com.au website. Contributors who wish to reproduce any material as it appears in Medical Forum must contact the publisher for copyright permission.
DISCLAIMER Medical Forum is published by Medforum Pty Ltd (Publisher) as an independent publication for health professionals in Western Australia. Neither the Publisher nor its personnel are medical practitioners, and do not give medical advice, treatment, cures or diagnoses. Nothing in Medical Forum is intended to be medical advice or a substitute for consulting a medical practitioner. You should seek immediate medical attention if you believe you may be suffering from a medical condition. The support of all advertisers, sponsors and contributors is welcome. To the maximum extent permitted by law, neither the Publisher nor any of its personnel will have any liability for the information or advice contained in Medical Forum. The statements or opinions expressed in the magazine reflect the views of the authors and do not represent the opinions, views or policies of Medical Forum or the Publisher. Readers should independently verify information or advice. Publication of an advertisement or clinical column does not imply endorsement by the Publisher or its contributors for the promoted product, service or treatment.
Advertisers are responsible for ensuring that advertisements comply with Commonwealth, State and Territory laws. It is the responsibility of the advertiser to ensure that advertisements comply with the Competition and Consumer Act 2010 (Cth) as amended. All advertisements are accepted for publication on the condition that the advertiser indemnifies the Publisher and its personnel against all actions, suits, claims, loss or damages resulting from anything published on behalf of the advertiser.
EDITORIAL POLICY This publication protects and maintains its editorial independence from all sponsors or advertisers. Medical Forum has no professional involvement with advertisers other than as publisher of promotional material. Medical Forum cannot and does not endorse any products.




We’ve got another round of wine to giveaway this month, this time from Margaret River’s Vasse Felix.
Read our Master of Wine’s review of the winery on page 53 for more on these iconic wines.
Or if you’d fancy something other than wine, we’ve got movie tickets and a book up for grabs.
To enter, scan the QR code on this page or go to mforum.com.au and hit the competitions tab.
PUBLISHERS
Alice Miles – Director Fonda Grapsas – Director
Tony Jones – Director
EDITORIAL TEAM
Managing Editor
Andrea Downey 0437 909 904 andrea@mforum.com.au
Clinical Editor
Dr Joe Kosterich 0417 998 697 joe@mforum.com.au
Graphic Design Studio Scotts hello@studioscotts.com.au
ADVERTISING
Advertising Manager
Bryan Pettit 0439 866 336 bryan@mforum.com.au
Advertising Account Manager and Clinical Services Directory
Rita Murphy 08 9203 5222 rita@mforum.com.au
CONTACT MEDICAL FORUM
Suite 3/8 Howlett Street, North Perth WA 6006
Phone: 08 9203 5222 Fax: 08 6154 6488 Email: info@mforum.com.au www.mforum.com.au


















Doctor John Rosser Davies’ five decades of service to his community has been recognised.
The Manjimup doctor arrived in the South West town in 1978 as a temporary locum and has been there ever since.
Dr Davies received a WA Rural Health Long Service Award from Rural Health West.
His career, which began in the United Kingdom in 1972, spans obstetrics, anaesthetics, surgery, emergency medicine and aged care.
Relocating to Australia in January 1978, he filled locum positions in Wyndham, Exmouth, Port Hedland, Esperance, Adelaide, Sydney, Caloundra, Mooloolaba and Longreach before arriving in Manjimup.
“The work was mainly in the hospital, the mandatory service provision needing archetypal GP skills such as obstetrics, caesarean section, anaesthetics, appendicectomy, emergency work and anything else one could do safely,” Dr Davies said.
“The job utilised all my medical knowledge and quickly needed me to learn new skills.”
As Manjimup’s only obstetrician for the past 19 years, he has delivered more than 1000 babies, often caring for those same children as adults later on.
He is known for having pioneered homebased palliative care in the area long before it became widely practised in Australia.
According to Rural Health West Dr Davies is the only rural doctor in WA to have provided surgical, anaesthetic and obstetric services concurrently.
Eighty-eight GP clinics in WA have moved from being a mixed billing practice to fully bulk billing since federal government incentives began in November.
The federal Department of Health released figures showing the number of fully bulk billing clinics in each state prior to the Bulk Billing Incentive Program beginning and up to January 31, 2026.
The data showed that 1269 previously mixed billing practices across Australia were now registered as Medicare Bulk Billing Practices – a 16% increase on data released in December.
Previous data released during Senate Estimates in December showed 1092 previously mixed billing practices had signed up to the incentive program in the first month.

He has mentored more than 80 medical students and is a long-standing faculty member and co-convenor at the UWA Clinical Training and Evaluation Centre. Dr Davies is still practising in the community. His care has extended beyond hospital walls having been associated with the Asthma Foundation and many locals would know him from providing road safety education and delivering antenatal and first-aid education in the community.
Prior to the incentive program just over 77% of GP clinics across the country were fully bulk billing. In the past three months, this rose by 4.3% to 81.4%.
So far more than $61 million in incentives have been paid out since January. However, a breakdown of payments state by state was not provided.
A simple SMS reminder could improve vaccination of children by 6%, according to new research.
The Kids Research Institute Australia carried out the research, which saw the AuTOMATIC trial send more than 20,000 text messages to parents between 2021 and 2024. Some 10,000 parents took part in the trial.
The results, published in the Lancet Regional Health, described how
sending a text message ‘nudge’ reminding parents of upcoming vaccinations could potentially see an additional 35,000 children nation-wide receive their 18-month and four-year-old vaccines on time.
Professor Tom Snelling, Head of Infectious Disease Implementation at the Wesfarmers Centre of Vaccines and Infectious Diseases, said about 20% of Australian children were usually late in receiving critical vaccinations.
“We understand that family lives are very busy, so we partnered with 20 general practice clinics across Australia to see if simple text message reminders could be an effective tool for prompting parents to book in for their child’s vaccinations.
“The SMS reminders came directly from the GP clinics, and I believe this played an important role in the successful outcome as parents
A suite of new private facilities has officially been opened at Joondalup Health Campus.
While ministers welcomed the addition of new beds and surgical facilities, concerns were raised about the future of private maternity services at the hospital following the departure of two obstetricians.
Federal Health Minister Mark Butler was in Perth to attend the opening of the $166 million upgrades alongside Premier Roger Cook on February 18. The work has boosted medical bed numbers by 30, while another 22 surgical beds have been added in addition to six operating suites, including two which are shared public/private, two day procedure suites, a day surgery admissions unit, and expanded back-of-house facilities.
The upgrades also provide scope for another 30 beds – referred to as ‘shell beds’ – to be fitted out and brought online in the future.

respond positively to a trusted, credible source of information.
“These results also suggest potential for using SMS reminders to improve health behaviours for other GP-led public health programs, like reminding people to undergo blood pressure checks or cancer screening.”
Specialist fees set to be public Specialists may soon have to make their fees public after legislation to require disclosure was introduced to Federal Parliament.
The government has put forward a Bill to allow it to publish
However, the opening of the new facilities comes as news that two obstetricians are departing from the hospital’s private maternity services this year.
Dr Kim Jones is understood to have moved her services to St John of God (SJOG) Hospital Subiaco, while Dr Nicola English confirmed to Medical Forum she would be finishing within Joondalup when her current cohort of patients had delivered their babies at the end of July 2026.
The state’s private maternity services have been under increasing pressure in recent years, with some units closing and others losing staff.
A spokesperson for Ramsay Health Care, which runs the private facilities at Joondalup, told told Medical Forum new obstetricians would soon be taking up roles at the Campus.
“We are committed to continuing to provide high quality private maternity services for the local community in Joondalup and surrounding areas,” they said.

details about what individual medical specialists charge for particular services on its Medical Costs Finder website, which was launched in 2019 by the Liberal/National government.
However just six of 6300 specialist doctors across the country had chosen to voluntarily display their fee information by the end of 2022.
According to Health Minister Mark Butler that number has since risen to 88 individual doctors.
The government also proposes to publish Medicare, hospital and insurer billing data already collected, on the Medical
Costs Finder in an effort to improve transparency.
AMA (WA) President Dr Kyle Hoath told Medical Forum other drivers of rising out-of-pocket costs should not be overlooked.
“We have endured decades of inadequate Medicare indexation and increasingly restrictive private health insurance policies characterised by rising premiums and benefits which do not keep pace with wage growth and inflation,” he said.
By Dr Jing Liu, Radiologist
Breast cancer is not only the most common cancer for women in Australia, but also the second leading cause of death.
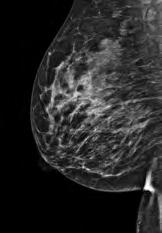
While conventional mammography remains the cornerstone of breast imaging its sensitivity is limited, particularly in dense breasts.
Contrast-enhanced mammography (CEM) is an emerging breast imaging modality that combines anatomical and functional assessment, offering increased sensitivity and diagnostic certainty.
What is contrast-enhanced mammography?
CEM involves performing digital mammography following intravenous administration of iodinated contrast – the same contrast agent used for CT, therefore the same contraindications apply.
Dual-energy exposures generate subtraction images that demonstrate areas of contrast uptake, due to increased vascularity.
The low energy exposures are the same as conventional digital mammography. Both standard 2D mammograms and tomosynthesis can be performed as part of contrast-enhanced mammography.
Radiation dose for CEM is approximately 25-30% more than conventional digital mammography. This is similar to obtaining one additional conventional mammogram view, or around two months of natural background radiation.
CEM may be particularly beneficial for:
• Dense breast tissue (BI-RADS categories C and D), limiting conventional mammographic sensitivity
• Surveillance of intermediate and high-risk patients (e.g. previous history of breast cancer or strong family history)
• Evaluation of the symptomatic breast (e.g. palpable lump)
• Assessment of disease extent in known breast cancer to identify multifocal or contralateral disease for treatment planning
• Assessment of response to neoadjuvant chemotherapy
It can also be an alternative to breast MRI for patients who have:
• Increased lifetime risk of breast cancer but do not qualify for MBS-funded breast MRI
• Severe claustrophobia
• Non-MRI-compatible devices
CEM compared with other breast imaging modalities
Total examination for CEM takes around 15 minutes, compared to 30-45 minutes for a breast MRI.
It is performed in a familiar digital mammogram machine, rather than face down in an MRI machine

where positioning and noise may trigger claustrophobia.
CEM comes at a significantly lower cost than breast MRI, and is often more accessible.
For women with dense breasts, conventional digital mammography sensitivity for lesion detection can be as low as 60-70%, whereas sensitivity of CEM in dense breasts is 95-97%, similar to breast MRI.
Dr Liu is a MBChB FRANZCR Radiologist, recently completing a sub-specialised Breast Radiology Fellowship at SKG. Educational Activities
0.5 0.5 hours Reviewing Performance hours Activity


Billions of dollars of additional funding is on the way for West Australian public hospitals – but will it be enough?
State, territory and the federal governments have agreed on public hospital funding deals after two years of negotiations.
West Australian public hospitals will see an additional $2.4 billion in funding from the Commonwealth across the next five years.
The deal is in addition to what had already been budgeted and comes as the Commonwealth strives to meet its commitment to increase the proportion of health funding it provides to states and territories.
But the AMA (WA) said the agreement must be “the floor, not the ceiling” for hospital funding reform.
Following tense negotiations – which saw Prime Minister Anthony Albanese write to state health ministers telling them to rein in hospital spending – the Commonwealth announced an extra $25 billion would go to public hospitals across Australia over the next five years.
This would bring the total federal funding for public hospitals to more
than $219.6 billion for the period from mid-2026 to mid-2031.
The Commonwealth agreed the share of funding it provides public hospitals would grow to 45% within 10 years from July 2025, reaching 42.5% before 2030.
AMA (WA)
President Dr Kyle Hoath said given WA public hospitals were under unprecedented pressure with emergency departments, elective surgery and workforce capacity all overstretched, this agreement must be the starting point for hospital reform.

He said WA hospitals faced unique pressures, including rapid population growth and workforce shortages, especially in regional and outer-metropolitan areas.
“Our clinicians are seeing long ED wait times, ambulance ramping and elective surgery backlogs,” he said.
“Workforce must be central – funding alone won’t fix hospitals without staff.
“WA needs more doctors, nurses and allied health professionals, and better retention of senior clinicians, with safe staffing levels to reduce burnout.
“The AMA (WA) will be watching closely to ensure funding supports front-line clinical care and is not absorbed by administrative growth or short-term fixes.”
WA Health Minister Meredith Hammat said the agreement provided certainty to WA and all states on critical health funding matters.
“It is an acknowledgement by the Commonwealth of the challenges facing Western Australia’s health system, particularly the increasing number of older patients who’ve been medically cleared for discharge but are unable to leave hospital due to a lack of aged care packages and placements.”

Hundreds of West Australian women having a hysterectomy are set to benefit from a novel surgical technique which reduces pain and hospital stays.
By Cathy O’Leary
While hysterectomy rates have declined worldwide in the past two decades, the numbers have remained relatively stable in Australia, with more than 30,000 women undergoing the surgery each year.
With the most common form being a total hysterectomy, involving the removal of the uterus as well as the cervix which connects it to the vagina, it remains a major surgery for women requiring weeks of recovery.
But now a newer technique being used in the public and private health sectors in Western Australia is making hysterectomy less invasive and offering a shorter healing process.
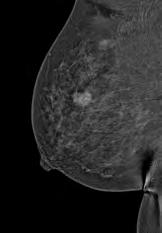
Known as vNOTES, vaginal natural orifice transluminal endoscopic surgery is an advanced technique for performing a vaginal hysterectomy that combines the benefits of both traditional vaginal and laparoscopic surgery.
Used increasingly around the world, including Australia, the surgery is designed to leave no visible scarring and help the patient recover faster.
Surgeons do not make incisions in the abdomen – everything is done through the natural orifice (the vagina), using an airtight device that creates a seal that allows them to expand the abdomen so they can see the structures they want to cut and remove.
The surgery is designed to be performed quicker, leave no visible scarring and can often reduce the recovery time compared to abdominal surgery.
According to the Royal Australian and New Zealand College of Obstetricians and Gynaecologists, the method by which a hysterectomy is performed needs to be based on factors including the size of the uterus, whether there is scarring in the pelvis or cervix from previous surgery and whether the uterus can be manoeuvred through the vagina.
There are three broad techniques used:
• vaginal hysterectomy, where the uterus and cervix are removed via the vagina
• abdominal surgery, using an incision in the abdominal wall
• laparoscopic hysterectomy where keyhole incisions are made into the abdominal wall to allow a camera and instruments, and this can also include laparoscopic assisted vaginal hysterectomy.
RANZCOG describes vNOTES as “an emerging approach to gynaecological surgery”, including hysterectomy, using laparoscopic surgery performed through an incision in the vagina to avoid abdominal skin incisions.
Until recently, the technique has only been available in WA in limited scope in the private hospital system. The technique was first used at Hollywood Private Hospital, led by gynaecologist Dr Robyn Leake who performed the first vNOTES laparoscopic vaginal surgery in 2022.
But in a recent breakthrough for women’s health, a handful of female patients at Armadale Health Service (AHS) have become some of the first in a public hospital to have a hysterectomy without external incisions.
Rather than face an extended recovery, they can leave hospital the same day, without scarring, pain or immobility.
Four women at AHS had undergone hysterectomies using vNOTES by mid-October 2025, with another 20 patients expected to be suitable for the surgery in the following six months.
AHS gynaecologists Dr Basil Lyngdoh and Dr Lachlan Baxter performed the vNOTES surgery,
which allowed them to surgically enter through the patient’s vagina to remove the uterus, cervix and fallopian tubes, instead of making laparoscopic cuts in the stomach.
After 20 years of performing endoscopic procedures the traditional way, Dr Lyngdoh learned about the new procedure at a medical conference overseas and then travelled to Europe in June 2025 to work with Belgian doctor Jan Baekelandt, widely regarded as the “master” of the technique.
Both Dr Lyngdoh and Dr Baxter then attended a workshop with Dr Leake at Hollywood to learn from her experiences in carrying out the surgery in the private sector.
Dr Sangeeta Malla Bhat, Head of Obstetrics and Gynaecology at AHS, which currently performs about 80 hysterectomies a year, said vNOTES was a relatively new procedure.
Dr Lyngdoh told Medical Forum that he first heard about vNOTES in 2024, when it was discussed at many conferences he attended.
“I met the pioneer in vNOTES who works in Belgium, who showed the different complex surgeries that can be done using it, but initially we were keen to bring it here for hysterectomy for a benign condition,” he said.
“At the time it was already being done in the private sector in WA,
so it was something I wanted to bring to our public health system.
“It’s good surgery in the right patient because it’s faster and has better outcomes, and decreases the burden on the public health system because we can convert a major surgery like hysterectomy into a day surgery. That’s definitely a win-win for everyone.”
Dr Lyngdoh said that while women who have conventional laparoscopic hysterectomy could also leave hospital on the same day, they faced more abdominal pain.
The new technique gave surgeons magnified visibility of the reproductive organs, due to the specialist equipment used.
“We make no cuts in the abdomen, and we do everything through the vagina,” he said.
“We put an airtight device that creates a seal so we can expand the abdomen, and this allows us to see the structures we want to cut and remove.”
Dr Baxter said it was exciting to perform different techniques with new technology which result in improved outcomes for the patient and hospital alike.
Vaginal natural orifice transluminal endoscopic surgery (vNOTES) hysterectomy is a minimally invasive surgical approach for removing the uterus through the vagina, using a specialised port to provide endoscopic viewing and access without abdominal incisions.
It uses a single vaginal incision, but with the addition of an endoscope, to allow for viewing of the peritoneal cavity and surrounding structures, making it easier to access organs that are typically reached via laparoscopy.
Endoscopic instruments are used to cut and ligate the uterine ligaments and vessels. Once the uterus is free, it is removed through the vaginal canal, and the vaginal incision is then closed. This can lead to benefits like reduced operative time, potential for a complete exploration of the peritoneal cavity, and the ability to remove tissue without fragmentation by using a containment bag. Continued on page

Join Medical Forum and colleagues for an informative day on common presentations in general practice.
Hear from local WA specialists on topics including HRT considerations, lipid management, red eye presentations, acute upper limb, handling Ahpra complaints, vaccinations in older adults, cardiac murmur and more.
Claim RACGP CPD time while you learn.
Date: May 9 Where: Pan Pacific, Perth
Masterclass that provides GPs and other healthcare professionals with a case-based, practical update on metabolic and endocrine presentations commonly encountered in general practice. The program integrates contemporary evidence with real-world clinical scenarios, focusing on decision making in complicated diabetes, re-conceptualising metabolic risk, managing endocrine incidental findings, and assessing fatigue through a hormonal lens.
6.5 hours RACGP approved CPD.
Date: March 21, 9am-3pm
Where: Boulevard Centre, Floreat

Speakers: Dr Chloe Nettlefold, Dr Paul Maggiore, Dr Kevin Chung
Topics: Cardiometabolic risk, Arrhythmia management, Valvular heart disease
Date: March 11, 6.30pm
Where: UWA Uniclub



Speakers: Dr Sebastian Leathersich, Dr Roma Poplawski, Dr Melanie Walls
Date: April 29, 6pm
Where: Akoya Suites, 58 Southside Drive, Hillarys
RSVP: TBC

ADHD in WA: the current landscape, overview of the WA ADHD Training Program, technology and AI tools, practical guidance for GPs on ADHD care, non-pharmacological management.
Date: March 28, 8.30am-5pm
Where: Beaumonde on the Point, East Perth
A 12-month program that combines educational content and practical experiences to maximise impact and professional growth. The program blends hands-on experience with structured learning to ensure healthcare professionals are well-prepared to manage the complexities of Parkinson’s care.
Register your interest email Yasmin Naglazas: yasminnaglazas @parkinsonswa.org.au
General practice is evolving rapidly, from accreditation reforms and privacy legislation updates to the integration of AI and digital tools. The Practice manager Forum will explore how to navigate these changes.
Date: March 27, 9am-3pm
Where: Four Points by Sheraton, Perth
Continued from page 9
The vNOTES surgery was less time consuming than a traditional hysterectomy by about 40 minutes.
“Armadale Hospital was the first hospital in the WA’s public health to start sending home hysterectomy patients the same day,” he told Medical Forum.
“And now vNOTES complements that by bridging the advances of vaginal surgery, which in our speciality is a dying art, as well as the convenience and surgical visibility of laparoscopic surgery into a procedure that offers significant recovery benefits to the patient.”
Dr Baxter said women with large uteri could have vNOTES hysterectomy, but the biggest exclusion area was probably women with significant pelvic adhesions or endometriosis because it was not technically feasible for those patients.
“For the vast majority of women having hysterectomy for benign indications they would be eligible for a vNOTES procedure,” he said.
“We are upfront with patients about the newness of the technique, and
the pros and cons, but it can be offered to patients as an alternative to a conventional laparoscopy, with some advantages, and most women are very excited to avail themselves of that.
“Obviously, there are also significant bed pressures in all parts of the health system, and being able to offer patients a safe ability to return home sooner has advantages for the patient in terms of their recovery and also for the health system and public health dollar.”
Dr Lyngdoh said the science showed that internal cuts healed faster.
“When you have laparoscopic surgery and the incision is on the abdomen, that is exposed, so by making an incision at the point of a natural orifice, then it will heal faster,” he said.
“We’re trying to bring this surgery to different forms, such as women who want to have permanent contraception. We initially had to go through the abdomen but now we can offer it through the vagina, so that’s another win for women.
“The patients who’ve had the surgery with us so far have been very happy with the procedure.”
Dr Baxter said that while the recovery time for hysterectomy was still several weeks, vNOTES had some clear benefits for patients, as well as for members of the surgical team.
“It’s another option in our armamentarium, just as we offer vaginal hysterectomy, laparoscopic and open hysterectomy – it provides us with a different tool to allow good patient care,” he said.
“It requires less head down and lower intrabdominal pressures, which has significant advances for our anaesthetic colleagues, and then we see that postoperatively in the patient recovery with less pain, less requirement for opioid analgesia and earlier mobilisation – all of which affect the earlier return to home.”
Dr Baxter said that while AHS had not offered vNOTES for other gynaecological surgery so far, he expected that would change in coming months, and other public hospitals in WA were likely to adopt vNOTES as a hysterectomy surgical option.

Assured but humble about his abilities, Associate Professor Raj Mohan takes the difficult cases and the ones others won’t touch in the world of gynaecological cancers.
By Ara Jansen
Associate Professor Raj Mohan is comfortable in his own skin and his abilities. He says it has taken working and learning in numerous countries and several direction changes to get there.
It’s one reason why, as a gynaecologist and gynaecologic oncologist, he’s given some of the toughest and most tricky surgical cases.
He won’t accept any accolades for talent or ability but gently asserts that: “God gave me this talent. He gave it to me to put to good use. I believe any talent I have has been given to me to use wisely and to try my best.”
Growing up in Malaysia, a young Raj thought about being an accountant or the exciting travelling life of a pilot. Instead, Raj’s dad – the manager of a medical lab – foresaw that medicine was his son’s future.
On starting medical school, Raj settled on general surgery, but as he grew to learn, life had other plans for him. Yes, he’s still doing surgery, but in the field of gynaecologic oncology.
“General surgery was my focus,” says Raj of those early years. “Every young doctor wants to be a surgeon. When I went into general medicine I worked with a physician who was very inspiring and motivating.”
If the universe has a way of sending us messages, he got one on a shift. After reading a book on shoulder dystocia, he fell asleep. After waking in the morning and starting rounds he was called to help a screaming woman who was experiencing shoulder dystocia during her delivery.
“I’d read about exactly that the night before, so I told everyone to stand back. I did what I’d read, the baby was delivered safely. I became a bit of a hero in delivering this baby.
“While I was a senior registrar I just kept getting more and more responsibility. My whole life changed that night and so did my direction.
“Once I found what I was good at, things really started to roll. How many people go to work and really enjoy what they do?

I wasn’t going to be happy with a general doctor’s life. I met a gynaecologic oncologist and I liked his attitude, his aura and surgical skills and that convinced me to move to gynaecologic oncology.
“My path went that way and I think destiny was calling me.”
When working in the UK after his initial studies in Malaysia, Raj did both obstetrics and gynaecology. Since moving to Australia more than two decades ago he spends most of his time in gynaecologic oncology.

“I was a lot more interested in gynaecologic oncology than in obstetrics in that I thought I could be better at it. In certain countries, like the UK and here, they don’t have many gynaecologic oncologists.
“This has allowed me to do more advanced surgery. If it’s a simple gynae issue, I tend to send them back to their doctor.”
Raj, now 56, began his career in London, completing his obstetrics and gynaecology training in 2003 and earning Membership of the Royal College of Obstetrics and Gynaecology. He worked as a specialist for six years before moving to Australia, where he gained his Fellowship in 2010 and later a subspecialist certification in gynaecologic oncology.
Raj continued his learning to include a Master of Clinical Trials and Research at the University of Sydney.
These international training and academic achievements now underpin the leadership in gynaecological cancer care across Western Australia.
By the time he arrived in Perth, he’d moved eight times in 10 years, including working in the UK, Sarawak, Kuala Lumpur and on the east coast of Australia. At that point his wife Elaine said if he made another move, he’d be doing it alone.
Continued on page 15


Because there’s more to menopause than hot flushes.1–7
For her.
Medicine co-pack containing one pack of Estrogel® (estradiol hemihydrate) plus one pack of Prometrium® (micronised progesterone) for women with a uterus
The Estrogel® in Estrogel®Pro targets the underlying cause of menopause symptoms – her hormones8,9
Changes in hormone levels can result in a range of symptoms, and their type and severity can vary Estrogel Pro combines body-identical estrogen with micronised progesterone for women with a uterus, offering a regimen that addresses estrogen deficiency.9,10 With flexible dosing, it supports personalised symptom management so you can tailor treatment to each patient’s needs.9,10
When the body changes, life shouldn’t
PBS Information: EstrogelPro, Estrogel & Prometrium are listed on the PBS. Refer to the PBS for more details.
Please review the Product Information which includes the full indications and safety information before prescribing, accessible at besins-healthcare.com.au/PI or 1800 BESINS (237 467), or by scanning the QR code:
INDICATIONS: Estrogel is a Hormone Replacement Therapy (HRT) for estrogen deficiency symptoms in postmenopausal women and for prevention of osteoporosis in postmenopausal women at high risk of future fractures who are intolerant of, or contraindicated for, other medicinal products approved for the prevention of osteoporosis.9 Prometrium is for adjunctive use with an estrogen in postmenopausal women with an intact uterus.10
CONTRAINDICATIONS: Estrogel is contraindicated in women with previous or current VTE and active or recent thromboembolic disease. Estrogel should not be used in women with current or a history of breast cancer.9 Prometrium is contraindicated in patients with undiagnosed vaginal bleeding; mammary or genital tract carcinoma; thromboembolic disorders; thrombophlebitis and cerebral haemorrhage.10
SAFETY INFORMATION: Common Estrogel AEs include, but are not limited to, headache, nausea, abdominal pain, breast swelling/pain, and breast enlargement.9 Common Prometrium AEs include, but are not limited to, altered periods/shortening of the cycle, amenorrhoea, intercurrent bleeding/breakthrough bleeding.10 A proper risk/benefit analysis should be undertaken for each patient before commencing treatment with Menopausal Hormone Therapy.
References: 1. Saljoughian M. US Pharm 2018;43(1):13–16. 2. MedlinePlus [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2020 June 24]. Aging changes in the breast; [reviewed 2022 July 21]. Available at: https://medlineplus.gov/ency/article/003999.htm (Accessed January 2026). 3. Zagaria MAE. US Pharm 2011;36(9):22–26. 4. Fenton A. J Mid-life Health 2021;12:187–192. 5. Prabakaran S, et al. Ther Adv Endocrin Metab 2021;12:1–11. 6. Bhatnagar A, Kekatpure AL. Cureus 2022;14(9):e29367. 7. MedlinePlus [Internet]. Jacobson (MD): National Library of Medicine (US); [updated 2020 June 24]. Aging changes in the female reproductive system; [reviewed 2022 November 10]. Available at: https:// medlineplus.gov/ency/ article/004016.htm (Accessed January 2026). 8. Jean Hailes. Menopause fact sheet. Available from: https://www.jeanhailes.org. au/resources/menopause (Accessed January 2026). 9. Estrogel® (estradiol hemihydrate) Product Information, updated 18 December 2023. 10. Prometrium® (micronised progesterone) Product Information, updated 1 Feb 2022. Estrogel® and Prometrium® are registered trademarks of Besins Healthcare. Besins Healthcare Australia Pty Ltd ABN 68 164 882 062. Suite 5.02, 12 Help Street, Chatswood NSW 2067. For medical information call 1800 BESINS (237 467). www.besins-healthcare.com.au EPR-EST-PRM-2656 January 2026
Continued from page 13

In December last year, Raj was named St John of God Murdoch Hospital’s Doctor of the Year for 2025.
SJOG Murdoch Hospital described Raj as a doctor admired for his kind and gentle nature, humility and dedication. Actively involved in gynaecological cancer research and clinical trials he’s also committed to supporting the next generation of specialists through his teaching roles at the University of Notre Dame Fremantle and the University of Western Australia.
“He is a kind and deeply compassionate clinician who consistently places patient care first and is known for his unwavering support of his friends, colleagues and anyone in need. A gentleman in every sense,” says SJOG Murdoch Hospital chief executive Ben Irish.
What keeps Raj in gynaecologic oncology is a passion for the mix of surgery and general gynaecology.
“It suits my need to be a surgeon,” he says. “That’s what moves me forward – I’m always learning. Of course, it’s great when you can make a difference and cure cancer and the patient survives.
“Even if you can’t cure a cancer and the patient is going to die, it’s about giving them the care they need, some quality of life and time to put their affairs in order. Yes, it can be depressing but you retain that compassion and desire to help.
“One of my favourite things is doing the radical surgeries; doing the stuff other people are not able to do. I’m happy to be in this stage of my life – I’m more confident in what I do because of the all the learning and knowledge I have now.
“But that comes from a lot of experience. In my younger years I was always concerned about things. In the last four to five years, I’ve settled into myself so much more, and with a sense of comfort.
“Now I’m excited for the next phase of things around robotic surgeries, which takes our work to a whole new level.”
Raj laughs easily and smiles often. He learnt the hard way that sometimes you have to keep that sun inside, after early on in his career being told that delivering bad news to a patient with his naturally cheerful disposition wasn’t the best way.
“I really do enjoy what I do and I have become a bit of a workaholic. My wife is so incredibly understanding. At one point during my overseas studies I wanted to give up and she reminded me that I could do it and it meant the world.
“It’s good I have such support from her and the kids but I do need to learn to have a bit of work-life balance.”
Raj and Elaine met in Malaysia, when she worked at a local bank and he was a customer. Married in 2001, they have three sons who are 19, 20 and 22.
While sometimes he can be operating until late into the night, Raj likes to spend what spare time he has with family, playing tennis and visiting family and friends in Malaysia. He uses conferences as an opportunity to travel and tack on a few days of leisure once business is done. Trying to create that balance, the goal is to take at least three to four holidays a year.
Raj’s guilty pleasure is sitting down to watch television, usually something not very serious so he can switch off for a while.
Emeritus Professor Bryant Stokes is being remembered as a champion of excellence in clinical practice and medical research and a pillar of the WA medical community.

Professor Stokes – affectionately known to his colleagues as Bars –passed away in February.
He was a member of the first graduating class of medical students at UWA in 1959 and went on to become a leader in the healthcare field in Australia for more than five decades.
Professor Stokes served as Director General of the WA Department of Health from 2013 to 2015, was Chief Medical Officer for WA from 1995 to 2000 and was elected President of AMA (WA) in 1982.
As Acting Commissioner of Health in 2000, he supported publication of healthcare
outcomes and adverse events, along with associated learnings and recommendations.
He also served as Chair of the Bryant Stokes Neurological Research Fund (previously the Neurotrauma Research Program) for over 20 years and held the role of Clinical Professor of Neurosurgery at UWA, Consultant Neurosurgeon at several of WA’s metropolitan hospitals and Professor of Anatomy at Notre Dame University.
In a statement WA Health said Professor Stokes would be remembered for his thoughtful leadership, his generosity of spirit

and his enduring passion for improving health outcomes for the people of Western Australia.
“He led with clarity, humility and a deep sense of responsibility. Those of us who serve in senior leadership roles across WA Health recognise the high standard he set – one grounded in service, stewardship and unwavering commitment to the health of West Australians.
“Professor Stokes’ influence on research was equally profound. As Chair of the Neurotrauma Research Program for more than two decades, he helped shape the direction of neuroscience and trauma research in Western Australia.
“The annual Bryant Stokes Oration, delivered as part of the Royal Perth Hospital Research Foundation awards program, stands as a testament to his leadership and the deep respect he earned from colleagues across the profession. His lifelong contribution to medicine was further recognised through the Australian Medical Association’s Hippocrates Award.
“WA Health is stronger for his service, and his legacy will continue to guide and inspire our work for many years to come.”
Professor Stokes made significant contributions to professional organisations during his career, including the Royal Australasian College of Surgeons, and as inaugural chair of the Royal Perth Hospital Medical Research Foundation
and Deputy Chair of the Medical Research Foundation of WA.
He was a former Director of the Perron Institute Board.
Perron Institute chief executive Steve Arnott said the organisation owes an enormous debt of gratitude to Professor Stokes.
“As a champion of excellence in clinical practice and medical research, his vision was to see WA develop and achieve recognition as a world-class centre in the neurosciences field, and as part of this, he played a huge role in the planning and development of the Ralph and Patricia Sarich Neuroscience Institute building at the QEII Medical Centre,” he said.
In 2001 Professor Stokes was made a Member of the General Division of the Order of Australia for his services to medicine and in 2008 he was invested to the Sovereign Order of St John of Jerusalem “Knights Hospitaller”.
More recently, his outstanding contribution to Australian healthcare was recognised by
“He led with clarity, humility and a deep sense of responsibility. Those of us who serve in senior leadership roles across WA Health recognise the high standard he set – one grounded in service, stewardship and unwavering commitment to the health of West Australians.”
his appointment as an Officer in the General Division (AO) of the Order of Australia in the 2020 Queen’s Birthday Honours List.
AMA (WA) said Professor Stokes was held in the highest regard by his colleagues, his patients, his friends and his family.
“He was a man of principle and compassion, a man who treated all patients as if they were his own family – and a man who made things happen.”
Medical Forum Clinical Editor Dr Joe Kosterich, who trained under Professor Stokes early in
his career, said: “If you wanted the best neurosurgeon - it was him. It was daunting for an intern in their second rotation to be on his ward, as I was at the old Shenton Park Hospital Neurosurgical rehab ward.
“He was always polite to all, a brilliant clinician and eager to teach. There have been few careers in medicine in WA as distinguished and impactful.”
A funeral for Professor Stokes was held at St Georges Cathedral in Perth on February 21, attended by friends, family and WA health leaders.


GPs have long been sounding the alarm on poor collaboration between primary and secondary care resulting in increased pressure on hospitals. Would a Chief GP Advisor in WA help?
By Aleisha Orr
The Western Australian branch of the RACGP has called on the state government to appoint a Chief GP Advisor in an effort to improve primary and secondary care collaboration and reduce pressure on hospitals, but how exactly would this work?
Last year in the midst of what the AMA (WA) described as a crisis in WA hospitals, the RACGP put forward a proposal for the state government to implement a number of changes to break down healthcare silos, improve patient outcomes, and reduce hospital admissions.
When taking the proposal to the steps of Parliament in October, RACGP Vice President and WA Chair Dr Ramya Raman said appointing a Chief GP Advisor could improve the way the healthcare system operated.
“Appointing a Chief GP Advisor would help the WA government identify local opportunities to make our health system more effective, efficient, and patientcentred,” she said.
“Our healthcare system can work better; it’s just a matter of putting systems in place.”
Dr Raman said the RACGP had discussed the creation of such a role with the state government in the past, but this marked the first public call for the role.
Speaking to Medical Forum, Dr Raman said there was a need for such a role in the public service, separate to the role of stakeholders such as the RACGP.
“The most important part of this role would be to strengthen clinical governance and safety across general practice,” she said
“We speak a lot about the role of general practice in keeping patients out of hospitals because of ambulance ramping and the number of patients we are seeing presenting to hospitals.
“But we’ve also got to think about how to better understand general practice and to have improved integration between hospital, community care and general practice.”
On a smaller scale, hospital liaison GPs (HLGPs) exist within each hospital with the intent of helping non-GP health professionals better understand how general practice works.
The aim is to create a conduit between what happens in hospitals and the GPs who will see these patients during their recovery and ongoing care.
“If we take a step back, we don’t have someone looking at the strategic purpose of how general practice integrates with the health system,” Dr Raman said.
She said a Chief GP Advisor would not only play a role in strengthening clinical governance and safety across general practice, and better integration between hospitals, community care and general practice, but they would also improve accessibility and enhance GP workforce supply and development across the state.
“They could provide clinical leadership and strategic advice to WA Health and also help coordinate some of the primary care initiatives.”

Dr Raman said while siloed approaches to healthcare resulted in a lack of integration, collaboration, and coordination ultimately leading to poorer health outcomes, input from a Chief GP Advisor could create a more person-centred health system and improve outcomes.
She envisioned such a role to be a high-level strategic position that could be offered to a practising GP taking it as a part-time role.
Having a working GP in the role would ensure they are across the reality of general practice from a health system and process point of view.
Dr Raman said while the ACT and Victoria had both created roles for Chief GP Advisors, she understood the role in Victoria was no longer filled.
Professor Lena Sanci took up the inaugural role of Chief GP Advisor in Victoria in June 2023.
A spokesperson for Victoria’s Department of Health confirmed her term concluded in December 2024.
“The time-limited role supported the department’s work to strengthen primary care, including informing Victoria’s advocacy to the Commonwealth on key reforms in the primary care sector,” they said.
“Professor Sanci continues to provide advice to the department through her ongoing participation in advisory groups.”
The ACT created two similar roles in February of 2024, the territory’s Chief GP and the Primary Care Advisor.
The two roles are both currently held by Dr Melanie Dorrington.
In these roles, Dr Dorrington leads the Office of General Practice and Primary Care (OGPPC) where she provides policy input and advice to all teams within ACT Health and Community Services Directorate, particularly when those policies affect general practice and primary care.
According to a spokesperson for the ACT Health Department, the role ensures that general practice is represented in the development of local and national policy as well as providing a crucial link between community general practice and the broader public health system.
“The Office of General Practice and Primary Care connects policy with general practice and primary care, including through research and education, to strengthen the health system in the ACT, specifically to primary and community care,” they said.
The Chief GP explored challenges and improvements in the whole health system to ensure that the primary care needs of the population were considered.


Our podcasts bring you the latest updates and key insights into new treatment options available.
Join our clinical editor Dr Joe Kosterich in conversation with WA specialists to learn more about developments to improve patient outcomes. Our podcasts are now CPD verified. Look for the CPD logo to complete your self-reflection and claim your time.
Learn more about:
Minimally invasive breast surgery with Dr Saud Hamza
Bridging the treatment gap in osteoarthritis with Dr Arash Taheri
Is it pelvic venous congestion? With Dr Marek Garbowski
Aortic stenosis: managing low-risk patients with Dr Gerald Yong
Rethinking radiation oncology with A/Prof Yvonne Zissiadis & Celia Byatt

Listen on your favourite podcast platform – scan the QR code to follow us!
“She works collaboratively with diverse stakeholders including other parts of the Health and Community Services Directorate, Canberra Health Services, the Capital Health Network, local GP and primary care practices, other jurisdictional and Federal Government GP leaders (where they exist), and relevant professional bodies including the RACGP.”
The two roles were also responsible for working to improve attraction and retention of the GP workforce in the ACT and the OGPPC has links to the Australian National University’s Academic Unit of General Practice.
Will WA follow suit?
Medical Forum put questions to WA Health Minister Meredith Hammat on whether the government was considering creating a Chief GP advisor position, or a similar high level strategic role for a practising GP to provide clinical leadership and strategic advice around health system integration.
WA Health did not directly address whether there were plans for the role, but a spokesperson said the department has a range of established mechanisms through which general practice expertise informs policy design, implementation, and system integration.
“The government meets regularly with valued stakeholders like RACGP to ensure West Australians have access to the healthcare they need, when and where they need it,” the spokesperson said.
“The Office of the Chief Medical Officer (OCMO) meets regularly with RACGP, Australian College of Rural and Remote Medicine (ACRRM), WA Primary Health Alliance and Rural Health West to discuss areas of mutual interest.”
They said the department also engages directly with general practice through these peak bodies for structured, representative clinical advice across a range of initiatives.
“The department has a fiveyear grant agreement with the WA Faculty of the RACGP that
enables it to engage with general practice on clinical matters, policy development, service configuration, planning and advocacy.”
The spokesperson went on to say general practitioners were employed within senior clinical leadership and advisory roles in the department which ensured GP expertise were “embedded within core decision-making structures”.
“This includes the current Acting Chief Medical Officer,
who is a registered GP and Fellow of ACRRM, and medical advisors with general practice backgrounds working across policy, safety, quality, and system reform portfolios.
“This distributed leadership model allows GP perspectives to be integrated across multiple portfolios and reforms, rather than relying on a single position to represent the breadth and diversity of general practice.”
A spokesperson for the ACT Health Department said the Chief GP and the GP Policy Advisor work together on general practice and primary care policy, research and education, and on joint programs including workforce initiatives and the development and evaluation of innovative models of care.
They said the roles provide advocacy and expert advice to the Minister for Health to ensure GP voices and primary care perspectives are represented in health policy, governance and funding.
“They work to bring a whole-of-health system approach to work that is occurring, based on the role of GPs as health advocates for their patients and community, and leaders in team and multidisciplinary care.”
In 2025 the OGPPC supported the establishment of a professional development and wellbeing fund for GPs and general practice staff.
The fund is currently being co-designed with the sector to determine funding priorities to support GP attraction and retention, wellbeing and professional development. This includes for GP registrars.
The ACT’s Chief GP and the GP Policy Advisor have also been involved in work on expanding scope of practice for GPs for ADHD care.
“They also work with teams on maternity shared care, and broader maternity work, pharmacy prescribing and scope of practice, nurse prescribing and scope of practice, clinical system governance, child screening and programs, voluntary assisted dying, opioid maintenance therapy prescribing, mental health care and service planning, and workforce,” the spokesperson said.
The Chief GP is the chair of the ACT’s Primary Care Emergency Response Committee, for which she works closely with Capital Health Network (CHN), the ACT’s Primary Health Network.
“Her involvement, alongside that of the chief executive of CHN, demonstrates the understanding in the ACT that being prepared for, and considering prevention and response to emergencies, requires participation of all aspects of the health system.”
AI has the potential to transform medical research and reduce the time doctors spend on repetitive tasks, but can it replace a doctor?
By Aleisha Orr

Two recent developments within health-related AI have seen some medical professionals expressing concern about how much authority the technology should be given; these have covered prescription writing and online health advice.
An investigation by The Guardian highlighted the potential dangers posed by AI generated health advice.
The publication found that Google’s AI Overviews, which use generative AI to provide information on a question or topic, were providing false and misleading health information.
The investigation uncovered incorrect advice being provided to pancreatic cancer patients, incorrect details about liver disease and certain cancers specific to women.
Experts who weighed in said such information could increase the risk of patients dying, make people wrongly think they were healthy, or dismiss genuine symptoms.
While the search engine recently removed some of these health summaries, WA Data Science Innovation Hub Director Alex Jenkins said risks with AI health advice remained.
He said while AI technology had evolved significantly in recent years, it had the same potential risks as previous online searches relating to health.
“This is the natural evolution of ‘Doctor Google’, except now the information sounds even more authoritative,” he said.

“AI is increasingly helpful for health information, however the public needs to understand it can’t be trusted 100%.
“Governments need to consider special safeguards for health information provided by AI, as corporations won’t regulate themselves on this.

“Another risk is an increasing number of people will trust AI with their private medical information and health records, without knowing the risks to their data.”
In January ChatGPT launched ChatGPT Health, offering members of the public information about their health and wellbeing.
Users are able to connect medical records and wellness apps to help inform the AI chatbots responses.
“You can now securely connect medical records and wellness apps – like Apple Health, Function, and MyFitnessPal – so ChatGPT can help you understand recent test results, prepare for appointments with your doctor, get advice on how to approach your diet and workout routine, or understand the tradeoffs of different insurance options based on your healthcare patterns,” the company said in a statement. “ChatGPT Health is designed to support, not replace, medical care. It is not intended for diagnosis or treatment.”
However, experts from around the world have raised concerns relating to privacy and misinformation.
It comes at the same time an artificial intelligence platform is, for the first time, legally able to participate in clinical decisions for prescription renewals.
The company behind the technology, Doctronic, told The BMJ that a pilot program using AI would decide if patients in the US state of Utah should have their prescriptions renewed for treatment for chronic conditions.
The first 250 prescriptions for each drug category will be overseen by a doctor, then after that one in every 10 prescriptions will be randomly sampled for a safety check.
The Utah Department of Commerce’s Office of Artificial Intelligence Policy released a statement announcing the pilot which began in December 2025, describing it as “a major milestone to demonstrate how AI can improve access to care and health outcomes”.
According to the department, prescription renewals accounted for about 80% of all medication activity in the state.
“The pilot would test how autonomous AI can help close gaps in access, reduce delays that lead to medication lapses, and improve outcomes for millions of people managing chronic conditions,” it said in a statement.
However, the head of the American Medical Association, Dr John Whyte, has raised a number of concerns about risks to patients and doctors without proper human oversight.
Doctronic co-founder Dr Adam Oskowitz said medication noncompliance was one of the largest drivers of poor health outcomes and preventable healthcare costs, responsible for billions of dollars’ worth of avoidable medical expenses each year.
“Improving access to medication renewals will directly impact this by improving medication compliance and reducing unnecessary emergency room visits,” he said.
The pilot will track medication refill timeliness and adherence, patient access and satisfaction, safety outcomes, workflow efficiency, and cost impacts.
An Australian Medical Association (AMA) report on artificial intelligence in healthcare released in August maintains the final decision on patient care should always be made by a human.
The AMA acknowledged that over the past decade, AI has gained significant momentum in healthcare, promising to transform the medical industry and the way health providers interact with their patients.
It noted that AI was already being used to streamline some medical tasks. However, it stated significant system changes needed to take place and be continuously updated to keep pace with the technology.
“It is crucial to consider the roles of doctors and other healthcare professionals, as well as the current medical system, to ensure they are adequately equipped to keep pace with the rapid advancements in AI.”
Generative AI was raised in the Safe and Responsible Artificial Intelligence (AI) in Health Care –Legislation and Regulation Review last year as an area that potentially required special treatment.
The creation of specific governance and regulation were suggested to manage uncontrolled inputs and outputs, as well as training on large datasets containing errors and bias.
Advanced Pharmacy Australia stated there could be a major risk from disinformation from AI tools not intended for healthcare due to the lack of guardrails.
“Large language models are easily and readily available, provide misinformed advice and recommendations for managing diseases/conditions/ ailments with no oversight of output,” it said in a statement.
A federal Department of Health spokesperson said the legislation review took a broad approach in considering the potential impact of AI on the regulation of healthcare in Australia.
It also considered the potential role for non-regulatory initiatives in supporting the safe and responsible adoption of AI technologies.
Continued on page 25
Body identical MHT providing relief from vulvovaginal symptoms associated with estrogen decline including:1,2†
Vulvovaginal Atrophy (VVA)
Dyspareunia due to VVA
Pruritus vulvae

choice 1 mg/g OVESTIN cream 0.5 mg OVESTIN ovula MHT = menopause hormone therapy † Refer to Product Information for additional indications



Intravaginal estriol cream or pessaries are the recommended treatment for symptoms of vulvovaginal atrophy.3
Intravaginal treatment with estrogen is not associated with an increased risk of cardiovascular disease or venous thromboembolism, or of developing breast-cancer.3
Before prescribing, please review the Product Information available by scanning this QR code or calling 1300 659 646.
PBS Information: OVESTIN Cream and OVESTIN Ovula are listed on the PBS as an estrogen.

References: 1. Ovestin Cream PI. 2. Ovestin Ovula PI. 3. Intravaginal therapy for menopausal symptoms [published 2020 Dec]. In: Therapeutic Guidelines Limited; Melbourne: accessed Feb 2026 https://www.tg.org.au.
Aspen Pharmacare Australia Pty Ltd, St Leonards, NSW 2065
Trademarks are owned by or licensed to the Aspen Group of companies. © 2026 Aspen Group of companies or its licensor. All rights reserved. Prepared: Feb 2026 AU-EST-02-26-00001
In Australia the TGA regulates software, including software with artificial intelligence when the intended use of the product meets the definition of a medical device. This is inclusive of products that are intended to support diagnosis, treatment and monitoring of a disease or condition.
“The TGA routinely monitors the market for newly released products that may meet the definition of a medical device and assesses all available information to confirm compliance with Australian regulations,” the department’s spokesperson said.
“AI is increasingly helpful for health information, however the public needs to understand it can’t be trusted 100%.”
services like 1800Medicare and Healthdirect, and online resources where the information has been verified for accuracy.”
It also warned of the potential privacy implications of entering sensitive health data into generative AI products – something doctors may want to remind their patients who come to them with health advice from AI products.
“All aspects of patient care, including recommendations about appropriate treatment and interpretation of PBS eligibility and access via the PBS, are the responsibility of the treating doctor,” the spokesperson said.
“Software that recommends treatment, including prescribing of medicines, would generally be a medical device and require TGA approval for supply.”
“For a medicine to be subsidised through the PBS, it must be prescribed by a doctor, dentist, optometrist, midwife or nurse practitioner, who is approved to prescribe PBS medicines under the Act and who holds a valid PBS prescriber number.” Continued from page 23
The department acknowledged the importance of consumers seeking medical information from reputable sources.
“Reputable sources include medical professionals and organisations,
While the department regulates the Pharmaceutical Benefits Scheme (PBS), prescribing of medicines is regulated by states and territories individually, not the TGA.
The department did not clarify whether it had considered incorporating AI into represcribing in Australia in a similar way to the Utah trial.
Hear from WA specialists on common presentations in General Practice including:
• Lipid Management
• Panel discussing HRT considerations
• Vaccinations for older adults
• Peripheral Vascular disease
• The acute red eye
• Upper limb presentations
• Handling Aphra complaints
• Decoding the Murmur: A Practical Guide for GPs



The largest intake of new GP registrars in Western Australia has begun their on-the-job specialised training.
A total of 251 new GP registrars are participating in the Commonwealth-funded Australian General Practice Training (AGPT) Program with the RACGP.
This year’s cohort is 28% bigger than the 2025 cohort. More than half of these future GPs and Rural Generalists (130) will spend the full three years of their training in regional, rural, or remote WA on a rural training pathway, a 68.8% increase on 2025.
The other 121 GP Registrars on a general pathway will train across Perth, with at least 12 months in an outer metropolitan, rural,
or non-capital city region, or an Aboriginal and Torres Strait Islander health training post.
RACGP Vice President and WA
Chair Dr Ramya Raman said the state’s growing cohort showcased the appeal of WA’s diverse training environments and the profession’s strong local reputation.
“People throughout the state will soon have better access to a GP who knows them and is a part of their community,” she said.
“That’s an incredibly valuable outcome for communities throughout the state, and it’s
something we need sustained investment in to support.”
Dr Raman said more GPs would ease pressure on WA’s hospital system.
“Wider access to the continuous care GPs provide means better preventive health outcomes, and care provided by GPs after unplanned hospital visits significantly reduces the chance a patient is readmitted,” she said.
Dr Raman said the growth in the number of GPs training in regional and remote WA was especially welcome news.

Roberta Dumbrava has now entered her third year of AGPT training and hopes to return to rural practice.
Ms Dumbrava was born in Romania and lived in a number of towns in Australia before settling in Bunbury. She finished her studies at UWA and worked at Sir Charles Gairdner Hospital for three years.
She then returned to Bunbury to work in ED, paediatrics, and eventually general practice. She is currently with Southern Clinic Como while also serving as the RACGP’s Registrar Medical Educator, helping to ensure that training materials and support meet registrars’ needs.
“I feel a deep sense of pride for what I do, I feel really connected to my community. In general practice you really feel like you’re improving the quality of your patients’ lives,” she said.
“When I was younger, we lived in a few small towns, and we couldn’t see a specialist. The GPs were a godsend. They were a person we all trusted as a family. I know how important it is to have a doctor who understands your needs and can tailor their care to the community.
“So that’s my end goal, is to go back somewhere rural. Give back to those communities. Become the jack of all trades.”
Among them is Dr Prasanna Henegama. He worked as a medical doctor in Sri Lanka specialising in emergency medicine for 15 years before undertaking training in Australia.
After a rewarding training experience in KalgoorlieBoulder, Dr Henegama decided to change medical pathways but stay in the outback city.
He said while rural medicine could be challenging, it was also engaging and rewarding, and he planned to spend his career in rural Australia.
“You might end up with fewer facilities than you have access to in a metro setting, but at the same time I notice there are a lot of acute cases coming in and I think that’s something my experience from Sri Lanka can help with – maybe more than if I was in a metropolitan area,” Dr Henegama said.
“In a rural setting you aren’t always seeing a huge number of patients, so those you see you will meet again. As you work with them you can see them becoming well, and when they express their gratitude it’s like getting an immediate reward. It’s very satisfying.
“It makes you feel more a part of the community, working so closely with people and their families.”
Dr Henegama has just begun his first year of Rural Generalist training with Bega Garnbirringu Health Services.

Many West Australians cannot access timely diagnosis and treatment for ADHD, but a GP training program aims to change that, writes Professor David Coghill and Dr Sean Stevens

Western Australia faces a significant healthcare access crisis. With 14,000 children on the Child Development Service waiting list and no public adult ADHD service, many West Australians cannot access timely diagnosis and treatment for one of the most common neurodevelopmental conditions.
In our combined experience – spanning international ADHD research and three decades of general practice – this represents one of the most pressing access issues confronting our health system.
The WA ADHD GP Training Program was developed to address this inequity by equipping GPs with the skills to assess, diagnose, and initiate treatment for ADHD within appropriate clinical governance frameworks.
With 65 participants now enrolled across two cohorts, this government-funded initiative represents the most comprehensive GP ADHD training program in Australia. Is the training robust?
Some commentary has questioned whether this GP training in ADHD assessment is sufficiently robust. We welcome this scrutiny – it reflects appropriate concern for
diagnostic accuracy. However, it is important to understand what this program entails.
The program comprises several integrated components.
Participants must first complete two foundational online modules covering ADHD identification and pharmacological management.
These RACGP-developed modules serve as prerequisites for entry, not the training itself. The substantive clinical education occurs through six 90-minute interactive peer group learning sessions, cofacilitated by paediatricians and psychiatrists in collaboration with the Australasian ADHD Professionals Association (AADPA).
Before addressing treatment options these sessions place major emphasis on comprehensive assessment methodology, differential diagnosis, comorbidities and, critically, the assessment of functional impairment – the cornerstone of accurate ADHD diagnosis.
Beyond formal sessions, participants engage in an asynchronous clinical discussion forum alongside experienced paediatricians and psychiatrists, allowing real-time consultation on de-identified cases.


Importantly, during training, GPs cannot independently initiate or titrate stimulant medications. Instead, they are encouraged to form mentoring relationships with local non-GP specialists, work up patients thoroughly, refer for diagnostic confirmation, and then engage in case conferences to learn directly from experienced clinicians’ approaches to diagnosis and management.
The program explicitly defines cases that remain outside GP scope, requiring referral to non-GP specialists.
These exclusion criteria, developed through detailed consultation with local paediatricians and psychiatrists, include children under 10 years, complex comorbidities such as psychosis, bipolar disorder, or substance use disorder, significant intellectual disability, high-risk cases involving self-harm, and atypical medication responses.
This ensures appropriate patient safety boundaries.
Concerns have been raised about the potential for rapid assessment clinics and inappropriate stimulant prescribing.
The program incorporates robust safeguards against this happening with WA GPs.
Participating GPs will have an initial cap of 50 patients on stimulants under their care, with any increase requiring justification to WA Health, such as working within a rural community with poor access to ADHD care.
This ensures prescribing remains appropriate to each GP’s context.
It is worth placing current concerns in context. Epidemiological research consistently demonstrates that ADHD prevalence has remained
stable at approximately 5-7% of children and around 3% of adults.
What has changed is recognition. While there are legitimate concerns about potential misdiagnosis and over prescribing, this reflects broader system issues rather than GP practice specifically.
Simultaneously, significant underrecognition persists, particularly in remote communities, culturally and linguistically diverse populations, Aboriginal and Torres Strait Islander communities, and those with limited financial resources.
The program has deliberately prioritised recruitment from GPs working in these areas to address these inequities.
ED: If you would like to become a mentor, paediatricians and psychiatrists are encouraged to contact wa.faculty@racgp.org.au.
Professor David Coghill is Chair of Australasian ADHD Professionals Association and Dr Sean Stevens is a Perth GP and Chair of the RACGP WA ADHD Working Group.
More than 400 GPs have applied to take part in training to allow them to diagnose and prescribe for ADHD, despite only 65 places being available.
Participating GPs have been split into three cohorts, with the first of those groups beginning training at the end of October 2025.
The second cohort began training in February and the third are set to begin later in 2026.
Upon completing the training GPs will be able to assess ADHD in patients aged 10 and older. Under recent changes to WA’s prescribing regulations they will also be able to prescribe stimulant medications.
It is hoped the program would ease pressure on specialists such as paediatricians and psychiatrists by helping more people access early diagnosis and treatment.
The WA government was the first Australian jurisdiction to announce a comprehensive program for ADHD diagnosis and management by specialist GPs, with other states following suit in recent months.
Dr Roma Poplawski is a highly trained Obstetrician and Gynaecologist who specialises in fertility, recurrent miscarriage, and early pregnancy complications. She is passionate about supporting women and couples through early pregnancy –particularly during times of uncertainty or loss. Dr Roma specialises in:
Gynecological endocrinology
Menstrual disorders
Perimenopause/ Menopause
Early pregnancy
Fertility/Fertility preservation
Concept Fertility and Day Hospital prides itself on a leading team of fertility specialists, gynaecologists, scientists and nurses, as well as its state-of-the-art laboratories and day hospital. Delivering the latest advances in fertility technology and women’s health, Concept’s priority is to ensure patients receive the highest-level of quality care, whatever their treatment journey entails.
Dr Poplawski obtained her medical degree in Poland and completed all her postgraduate training, including specialist training in Obstetrics and Gynaecology, in Manchester in the United Kingdom. She is also a Consultant Obstetrician and Gynaecologist at King Edward Memorial Hospital where she is serving as the Early Pregnancy Lead.

By Prof Andrew Briggs and Prof Helen Slater, Faculty of Health Sciences, Curtin University
Chronic musculoskeletal conditions, which can start in childhood and increase in prevalence over the life course, are often difficult to treat.
They can also impose a substantial burden on the health and wellbeing of individuals, families, communities and health systems. A unifying characteristic of chronic musculoskeletal conditions is persisting, and frequently disabling, pain.
The 2022 Australian National Health Survey estimated that around 7.3 million Australians (29%) lived with a chronic musculoskeletal condition. Other estimates suggest a prevalence of one in five experience chronic musculoskeletal pain, such as low back pain.
This likely underestimates the true prevalence of musculoskeletal conditions due to poor surveillance for a range of conditions.
Burden in WA
A recent modelling study commissioned by Arthritis and Osteoporosis WA, and undertaken in partnership between Monash University, Curtin University and HelloJP consulting provides contemporary and reliable burden estimates for WA.
The report used prevalence and
cost data from the ABS and Australian Institute of Health and Welfare (AIHW) to model current and future numbers of West Australians living with arthritis, long-term back problems and osteoporosis, and the direct costs of managing these conditions.
The number of West Australians living with arthritis is projected to increase by 41% to 609,858 (an additional 177,874 people relative to 2025) by 2045.
Local health system expenditure for osteoarthritis, rheumatoid arthritis and long-term back problems are conservatively forecast to exceed $2.25 billion in 2045 ($1.03 billion in 2025).
Implications for service delivery
These forecasts highlight the need for strengthening our health system and service delivery models.
The WA Sustainable Health Review provides a guiding framework for strengthening the health system agnostic to health condition, while National Strategic Action Plans (NSAPs) for Arthritis and Pain Management outline targeted reform agendas.
Forward-planning considering life course, equity, accessibility and affordability of care is
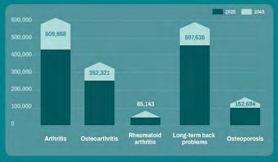


particularly relevant for groups disproportionately affected, including older and younger West Australians, females and people who experience disparities in accessing care (e.g. people in rural and remote locations and Aboriginal and Torres Strait Islander people).
Critically, Aboriginal people experience chronic musculoskeletal conditions at a similar or higher prevalence rate than nonAboriginal people, yet are less likely to access care, while services are not designed as culturally sensitive.
The Staying Moving, Staying Strong initiative contributes to addressing these gaps for arthritis care in Aboriginal people.
How can we meet challenges?
Musculoskeletal conditions will become an increasingly prominent driver of chronic disease burden and health care utilisation in WA, demanding a health workforce with a shared understanding and with joint capabilities in managing musculoskeletal health and associated pain care across health care settings and disciplines.
The current workforce volume, distribution and capabilities will not meet future demand. The future musculoskeletal health
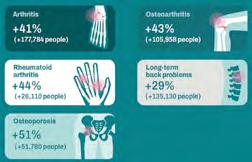
and pain care clinician will need not only discipline and diseasespecific competencies, but also capabilities that reflect models of interdisciplinary practice.
In response to the NSAPs, national consortia funded by the Australian Government developed digital training programs for building interdisciplinary workforce capability in arthritis and pain care. Expertise from WA contributed to the development of both
the Arthritis Training, Learning and Upskilling (ATLAS) and Open Pain Education Network (OPEN) platforms. Both platforms are structured as flexible, modular learning environments. ATLAS provides curated learning pathways or a ‘build your own’ option, while OPEN offers 15 training modules.
Developed in WA, and supported by WA Health, the painHEALTH and youngpainhealth digital platforms were co-created with people with lived experience to
Holistic and personcentred pain assessment and management from a biopsychosocial perspective
Enabling supportive selfmanagement knowledge and skills in patients
Effective communication and empathy
Understanding of the building blocks of healthy ageing (e.g. physical and mental functions, supporting functional ability and ageing in place, and enabling meaningful social participation).
provide credible, practical, and evidence-based information and resources to support consumers in their self-management.
ED: Author competing interests – the authors contributed to the development of the ATLAS and OPEN platforms.
Resources
www.arthritiswa.org.au/its-time-to-act www.arthritisaustralia.com.au/ managing-arthritis/staying-movingstaying-strong www.atlasarthritis.com.au www.openpaintraining.com www.painhealth.com.au www.youngpainhealth.com.au
0.5 0.5


Medical Forum is now an approved RACGP CPD provider for general practitioners, offering EA, RP and MO modules

Look for the RACGP CPD logo on Medical Forum content to complete your annual CPD hours.
Scan the QR code in the magazine or follow the links on our website to complete the activity requirements.
Your hours will be automatically added to your RACGP CPD home seven days after completion.

DR MAREK GARBOWSKI

Complete four hours of CPD, including MO, with our Pelvic Venous Congestion podcast. Learn when to consider the diagnosis and how to manage it.

Each country has a different system, but the issues in primary care seem universal. Increased pressure to do more in less time for less money with a decreasing tolerance for any outcome that is not perfect.
There is a wonderful quote from economist Milton Friedman: “One of the great mistakes is to judge policies and programs by their intentions rather than their results.”
Regular readers know my fondness for Sensible Medicine on Substack. Recently there was a guest post by Bobby Scott MD, a practising family physician and associate professor at Wake Forest University School of Medicine, about protecting primary care doctors.
Each country has a different system, but the issues in primary care seem universal. Increased pressure to do more in less time for less money with a decreasing tolerance for any outcome that is not perfect.
Riding alongside this, in Australia at least, is a reluctance to move ‘up the food chain’ by delegating tasks which can be done by others – think pharmacists and nurse practitioners.
Scott floated an idea which I think has merit, that is to delegate routine chronic disease management where the situation is stable.
He notes: “Physicians would still be responsible for the patient’s overall care, yet the maintenance logistics are managed by other professionals. Care would only be escalated to the physician when certain criteria are met or when the team’s clinical judgment deems it necessary.”
Sound a bit like the ill-fated Health Care Homes?
But that was nearly a decade ago. Technology has advanced since then, especially monitoring apps and telehealth.
There is also a point which may be part of the underlying reason for burnout – nobody can be everything to everyone all the time. Similar themes are emerging in specialty practice too – there are the beginnings of a split between obstetrics and gynaecology with some choosing only one.
Doctors are a valuable resource in society. A system that fails us fails the patients we serve.





By Dr Rae Watson-Jones, Obstetrician & Gynaecologist
Ovarian cysts are a common finding on ultrasounds of the female pelvis. Although the term sparks fear and anxiety, the vast majority of ovarian cysts are benign, and many do not require surgery.
A thorough history, combined with an analysis of the ultrasound findings, can often diagnose the cyst type, allay anxiety and help with decision-making about the next steps, even before referral to a gynaecologist.
A basic classification of ovarian cysts is simple versus complex.
A simple cyst on ultrasound has thin walls, is filled with fluid and is highly likely to be benign.
A complex cyst may have the following ultrasound features:
• septations (1 or multiple)
• solid areas
• papillary projections (an irregular-appearing wall)
• internal vascularity.
Complex cysts may or may not be malignant.
If ultrasound is equivocal, MRI is excellent at characterising the gynaecological organs, especially in relation to surrounding structures. Remember though, there is no
Doctor:
“Your ultrasound shows you have a cyst on the ovary.”
Patient:
“Oh no… what does that mean?”
Medicare rebate for a pelvic MRI so this can be expensive if done outside a public hospital.
clinical features
What is the age of the person?
Premenopause ovarian cancer is rare. Even when cysts have a complex appearance, the cysts are still more likely to be a common, benign type of cyst rather than a malignancy.
Tumour markers should still be performed but should be expanded to include the “premenopausal” tumour markers, including bhcg, alpha-feto protein (AFP), lactate dehydrogenase (LDH).
What are the associated symptoms?
Clinical features that are more suspicious include symptoms such as pain (may be acute onset or chronic), a large cyst

(palpable per abdomen), rapid growth, other systemic symptoms (nausea, vomiting, fevers, altered bowel habit, altered behaviour).
Common complex cysts in premenopausal people include:
Haemorrhagic cysts: these arise from follicular cysts that at ovulation have caused bleeding into the cyst. Although it is physiological for a follicular cyst to rupture, if the cyst was unusually large or there was a reasonable amount of bleeding, this can result in sudden onset and severe lower abdominal pain, to the extent where presentation to the emergency department is required. The pain is usually associated with nausea, vomiting and physical weakness and can take days or weeks to resolve. On ultrasound, the appearance is of “mixed echogenicity”.
Conservative management with analgesia is usually appropriate for haemorrhagic cysts except where there is a large haemoperitoneum or there is clinical suspicion of ovarian torsion.
Endometrioma: colloquially known as “chocolate cysts”, these arise from endometrial deposits on the ovaries which have become
Key messages
• Ovarian cysts are common and most are benign
• Clinical features provide a clue to diagnosis
• Ultrasound is inexpensive and provides key information for characterising a cyst.
encapsulated. Even though they are associated with endometriosis, they are commonly asymptomatic. They may be bilateral. On ultrasound, they have a typical heterogenous “ground glass” appearance.
Dermoid cysts or mature cystic teratomas: these arise from remnant stem cells within the ovarian stroma. Usually fascinating to gynaecologists but repulsive to others, they can contain any number of human tissues including fat, hair, teeth, bone, cartilage, nerve cells, thyroid tissue.
This is what gives them the complex appearance on ultrasound. Dermoid cysts can be small
and stable or slow growing. Some can grow very large and be an incidental finding, for example at an early pregnancy ultrasound or rapidly growing.
Or they can present with ovarian torsion. There are some characteristic features on ultrasound that lead radiologists to label it with certainty. However, tumour markers should always be done to exclude a malignant germ cell tumour.
In this group any complex ovarian cysts are assumed to be malignant unless proven otherwise.
Suspicious features include solid components, internal vascularity and an irregular shape. Unless completely simple, if a postmenopausal woman is found to have an ovarian cyst, tumour markers should be performed. This includes Ca 125, CEA and CA 19.9.
There are also several systems that can be used to stratify the risk of an ovarian cyst.
These include:
• IOTA simple rules consist of assessing the features of the cyst against five criteria that are likely benign and five criteria that are likely malignant
• O-RADS (Ovarian reporting adnexal and data system) is another reporting system to risk stratify an adnexal mass based on its ultrasound features. Radiologists are usually happy to review the images and provide this score if requested
• Risk of Malignancy Index (RMI). This involves calculating a score consisting of the cyst features, patient menopausal status and Ca125 value.
0.5 0.5

Alcohol and drug clinical assessment and pathway navigation. Brighter patient outcomes with Lumera.
Complement your care with clinical insight, personalised treatment plans and immediate availability.
Led by Clinical Nurse Specialist to AOD care is confidential and free of judgement
Why refer to Lumera?
• Excellence in clinical assessment
• 20+ years in ethical AOD care
• Collaborative approach.
• Personalised treatment plans
• Seamless referral process.
• Flexible consult options.
• No waitlists.

We work with you to enable the best possible recover y pathway for your patients. lumerapathways.au mylumera
By Dr Simone Altaf, General Practitioner
Pelvic pain in women is one of the most common, yet complex presentations encountered in clinical practice.
It affects millions of women worldwide, contributing to significant reduction in quality of life and often results in repeated healthcare visits.
Understanding the nature of pelvic pain, the many diverse causes and the evidence-based approaches to management is essential for supporting patients.
Defining pelvic pain
Pelvic pain refers to discomfort perceived in the lower abdomen or pelvis. It may be acute, being present for minutes, or chronic, persisting for at least six months.
Chronic pain is particularly challenging as it often involves multiple overlapping conditions –gynaecological, gastrointestinal, urological, musculoskeletal and psychological.
Pelvic pain is not simply a symptom, it is a multi-dimensional experience influenced by biological, psychological and social factors. Effective management requires acknowledging this complexity.
Common causes of pelvic pain
Gynaecological causes
Endometriosis: one of the most frequent causes of chronic pelvic pain. Ectopic endometrial tissue triggers inflammation, scarring and adhesions leading to dysmenorrhoea, dyspareunia and chronic pain.
Adenomyosis: endometrial tissue within the myometrium causing heavy periods and pelvic pressure.
Pelvic inflammatory disease: acute infection of the upper genital tract, often presenting with fever, tenderness and abnormal discharge.
Ovarian cysts or torsion: can cause acute, severe pain requiring urgent assessment.


Fibroids: particularly submucosal or degenerating fibroids may contribute to pain.
Ectopic pregnancy: acute pelvic pain with positive pregnancy test, urgent attention required.
Urological causes
Interstitial cystitis which is characterised by urinary urgency, frequency and supra pubic pain. Recurrent urinary tract infections can also cause pelvic discomfort.
Gastrointestinal causes
Irritable bowel syndrome frequently overlaps with gynaecological pain, with symptoms fluctuating with stress and diet. Inflammatory bowel disease may also present with abdominal pain, diarrhoea systemic symptoms
Musculoskeletal and neuropathic causes
Pelvic floor myalgia: overactivity or spasm of the pelvic floor muscles leading to deep pelvic pain.
Nerve entrapment: pudendal neuralgia or ilioinguinal nerve irritation can cause burning or shooting pain.
Lower back or hip pain: pain may radiate into the pelvis
Psychosocial factors
Other factors such as stress and anxiety, past trauma, central sensitisation and social and environmental stressors can have an impact on pelvic pain.
Approach to assessment
A thorough assessment is essential taking into account patient history, pain mapping and management.
History:
• Onset, duration and pattern of pain
• Menstrual cycle relation to pain
• Sexual, urinary and bowel symptoms
• Past surgeries or infections
• Impact on daily living
Pain mapping and validated questionnaires can help clarify the nature and severity of symptoms.
Physical examination:
• Abdominal and pelvic examination to assess tone, tenderness and organ mobility
• Muscular assessment if indicated
Investigations:
• Pelvic ultrasound
• Bloods if suspected infections
• STI screening
• Cervical screening if indicated
• Pregnancy test if history indicates
• Urine sample if indicated
• MRI for complex cases or suspected deep endometriosis (if suspect this referral to specialist required)
Medical management:
Analgesia: NSAIDs for inflammatory pain, paracetamol as adjunct.
Hormonal therapies: combined oral contraceptive pill, progestogen dominant oral pill, ius or GnRH analogues for endometriosis related pain.
Neuropathic pain agents: antidepressants or anticonvulsants.
Antibiotics should be considered for infections.
Surgical management:
• Endometriosis resection
However, surgery is not a cure, and repeated procedures may make the pain worse through scarring.
Physiotherapy:
Pelvic floor dysfunction is frequently seen in these women and physiotherapy can reduce muscle spasm, improve pelvic alignment, teach relaxation and strengthening exercises and address dyspareunia.
This is often one of the most effective interventions for chronic pelvic pain.
Psychological support
Cognitive behavioural therapy, reduction in stress and painfocused counselling can help women develop coping strategies and reduce pain.
Lifestyle and self-management such as regular exercise, heat therapy, dietary advice for IBS, sleep optimisation, stress reduction may help.
multidisciplinary clinics can provide a more holistic approach to care.
Pelvic pain in women is a multifaceted condition requiring thoughtful, compassionate and comprehensive approach.
Effective management hinges on recognising the interplay of biological, psychological and social factors, avoiding unnecessary interventions and empowering women with knowledge and support.
By working collaboratively across disciplines, clinicians can significantly improve outcomes and helping women improve their quality of life.
0.5 0.5



By Dr Anthony Chau, Neurosurgeon, Joondalup & Subiaco
Cauda equina syndrome (CES) is a rare but important surgical emergency caused by pathology –most commonly a compressive disc herniation – of multiple lumbosacral nerve roots.
Difficulties in diagnosis can be related to the heterogeneity of its presentation, and the multitude of definitions in the published literature. Additionally, the challenge in general practice is recognising the possibility of CES amongst the high volume of patients presenting with common back pain and lumbar radiculopathy. CES occurs in only 0.1% of lumbar disc prolapses.
CES is best thought of as a clinical entity occurring across a broad spectrum.
CESI (incomplete CES): on one end of the spectrum exists symptoms of back pain and sciatica with at least some form of early micturition dysfunction, broadly including straining micturition or impaired sensation of urinary flow; in my experience, some symptoms can be hard to differentiate from prostatic or pelvic floor dysfunction, so it is the context in which these symptoms occur or change which is paramount.
CESR (CES with retention): on the far end, executive control of bladder and/or bowel function has been lost leading to retention (500ml urine or more) and/or overflow. Often at this late stage, there will be accompanying symptoms of saddle anaesthesia, sexual dysfunction, bilateral sciatica and motor paralysis (not uncommonly asymmetric).
The implications for delayed diagnosis or treatment include potentially mitigable lifelong patient disability, and medicolegal ramifications.
In general practice, the most important factor is an awareness that CES can present in a multitude of ways and in varying combinations, and that


symptoms alone (regardless of the presence or absence of physical examination findings such as anal tone or saddle paraesthesia) are sufficient to warrant emergency referral for an urgent MRI.
Whilst the incidence of CES in the community is one in 200,000, this rises to one in five when clinical suspicion is present.
In the hospital, the spinal team checks for any upper motor neuron signs as, occasionally, thoracic cord compression or conus medullaris syndrome may mimic
CES (frequently the whole spine will be screened with a sagittal crosssection MRI at the same time).
If the diagnosis of a large lumbar disc herniation is confirmed, surgery takes place within hours to maximise the chance of neurologic recovery.
Evidence suggests that the severity of preoperative neurologic dysfunction is the most significant determinant of final prognosis, with other factors such as onset and duration of symptoms also playing a role.
A 30-year-old woman with no medical history presented to emergency with three weeks of back pain, severe left sciatica and foot weakness, inability to mobilise, two weeks of intermittent urinary incontinence, and one day of faecal incontinence.

On examination she was unable to rise out of bed due to severe pain, with bilateral positive straight leg raise, diffuse 2/5 weakness of the left foot (ankle plantar, dorsiflexion, inversion and eversion) which was additionally insensate, and absent ankle reflexes bilaterally.
Rectal examination demonstrated saddle anaesthesia, poor anal tone but intact sphincter contraction, and a post attempted-void residual of 500ml, leading to bladder catheterisation.
Urgent MRI demonstrated a large left-sided L5/S1 disc herniation causing complete compression of the cauda equina nerve roots within the spinal canal (Figure 1a).
Management and treatment
The patient proceeded immediately to theatre, where a minimally invasive left L5/S1 microdiscectomy was performed (scan the QR code for a video demonstration of this type of operation).
Intraoperatively, large soft disc fragments were removed, and bilateral neural decompression was achieved.
Postoperatively, she reported immediate and complete relief of sciatica. She remained an inpatient for three days, undergoing physiotherapy and a successful trial of void. She was discharged independently ambulant with no analgesic requirements.
Key messages
• CES is a pathological syndrome affecting multiple lumbosacral nerve roots. The most common cause is a large lumbar herniated disc
• CES is a spectrum with urinary dysfunction a key component. The most useful classification is incomplete CES (CESI) and CES with urinary retention (CESR)
• Acute awareness of possible CES amongst routine presentations of back pain and sciatica is essential. Typically, the presence of any new sphincter, saddle or sexual symptoms, or progressive neurology, in this population should trigger some level of suspicion.

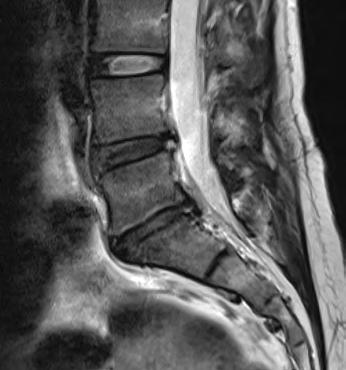

What is your area of practice?
I am a Consultant Obstetrician and Gynaecologist with a special interest in fertility, recurrent miscarriage, and early pregnancy complications. Supporting women and couples through early pregnancy – particularly during times of uncertainty or loss – is a central focus of my clinical practice.
I am currently the Early Pregnancy Lead at King Edward Memorial Hospital, where I am actively involved in the assessment and management of early pregnancy complications and pregnancy loss, as well as service development and clinical leadership within this field.
My work in this role allows me to combine evidencebased medicine with compassionate, patient-centred care at a critical time in patients’ lives.
In addition to early pregnancy and fertility care, I have a strong interest in gynaecological endocrinology, including menstrual disorders, perimenopause and menopause. I enjoy caring for women across all stages of life and supporting them through hormonal transitions with clear information, practical management strategies, and individualised care plans.
Where did you train?
I obtained my medical degree in Poland and completed all my postgraduate training, including specialist training in Obstetrics and Gynaecology, in Manchester in the United Kingdom. Training within the NHS provided extensive exposure to complex obstetric and gynaecological care, multidisciplinary teamwork, and high clinical standards.
My procedural practice is guided by safety, precision, and patient comfort, with clear communication at every stage.
I relocated to Perth three years ago and currently work as a Consultant Obstetrician and Gynaecologist at King Edward Memorial Hospital. This role enables me to remain closely involved in tertiary-level care while also offering personalised private care informed by current best practice and international training experience.
What procedural services do you offer?
I provide a comprehensive range of obstetric and gynaecological procedures, including early pregnancy ultrasound, medical and surgical management of miscarriage, inpatient and outpatient hysteroscopy, diagnostic laparoscopy and sterilisation procedures. I also perform IUD insertions, colposcopy, fertilityrelated procedures including egg retrievals and embryo transfers, and other core gynaecological procedures.
My procedural practice is guided by safety, precision, and patient comfort, with clear communication at every stage.
How is your service different?
My practice is holistic and strongly patient-centred. I place great importance on listening, clear explanation, and shared decision-making. Each patient’s care is tailored to their medical needs, personal circumstances, and priorities.
By combining public hospital leadership experience with private practice care, I aim to provide a service that is clinically rigorous, compassionate, and supportive – particularly for patients navigating fertility challenges, early pregnancy complications, or hormonal change.

By Saud Hamza, Oncoplastic Breast Surgeon, Fiona Stanley Hospital
Minimally invasive breast surgery (MIBS) had become attractive for carefully selected women with pathogenic genes mutation and for women with multifocal/multicentric breast cancer such as laparoscopic and robotic nipple sparing mastectomy with immediate breast implant reconstruction.
This new and innovative surgical technique was the result of advances in surgical equipment technology, which offers several potential benefits for patients undergoing breast cancer riskreducing breast surgeries.
The advantages
Precision and Accuracy:
Robotic and laparoscopic 3D lens systems provide surgeons with enhanced precision and accuracy during breast surgery.
Robotic arms are controlled by the surgeon, allowing for precise movements and manoeuvres.
Minimally invasive approach: The surgeries are performed using minimal access technique, which involve smaller incisions compared to traditional open surgery.
Minimally invasive procedures can result in less scarring, reduced pain, and faster recovery times, and less tissue trauma and blood loss.
Improved visualisation: MIBS typically incorporate high-definition cameras that provide surgeons with improved visualisation of the surgical planes. This enhanced view allows for better identification of critical structures, such as nerves and blood vessels, reducing risk of complications.
Customisation and personalisation: MIBS offer a high degree of customisation and personalisation for each patient’s unique anatomy and surgical needs.
Surgeons can plan and execute procedures with great precision, tailoring the surgery to the individual patient’s specific circumstances.


This can result in better outcomes and increased patient satisfaction.
The precision and minimally invasive nature of MIBS can contribute to a reduced risk of complications. By minimising tissue trauma, nerve damage, and blood loss, robotic and laparoscopicassisted techniques may lower the risk of post-operative complications such as infection, haematoma, or seroma formation.
Improved outcomes
Multiple meta-analyses show reduced blood loss and shorter hospital stays with robotic breast surgery (RBS) MIBS compared to traditional methods. These included:
Quicker recovery time: Patients often experience shorter hospital stays and faster recovery times.
Minimally invasive techniques and smaller incisions result in less post-operative pain and discomfort, allowing patients to return to normal activities sooner.
Cosmetic benefits: It can help preserve the natural shape and appearance of the breast, particularly in procedures such as nipple-sparing mastectomies.
This preservation of breast aesthetics can have significant psychological benefits for patients, improving body image and selfesteem following surgery.
A meta-analysis showed excellent cosmetic outcomes and high
patient satisfaction with RBS for nipple-sparing mastectomies.
Overall, while robotic/endoscopic breast surgery offers several potential advantages in terms of precision, minimally invasive techniques, and improved outcomes, its costeffectiveness compared to traditional surgical approaches is complex and multifaceted.
An in-depth review of the different medical technologies used in MIBS will help to better understand the economic implications, and its role in breast risk reduction and therapeutic surgery.
As technology continues to advance, and surgeons and theatre teams gain experience, MIBS techniques are likely to become increasingly prevalent in breast surgery, further improving outcomes and patient experience.
Author competing interests – the author has received in-kind support from Device Technology and 3D Laparoscopic Lenses

By Dr David Blacker, Neurologist, Nedlands


Lifestyle interventions are increasingly recognised as critically important in symptom management and possibly disease modification for Parkinson’s disease (PD).
During the last year, several key publications have addressed this topic.
A Lancet Neurology review summarised the literature on physical activity, nutrition and stress. Exercise is regarded as the intervention most likely to be proven to have a beneficial impact on the course of PD.
At least four phase two clinical studies have demonstrated stabilisation of progression or improvement, using different forms of high intensity aerobic exercise compared with moderate exercise or standard care.
A large phase three study of treadmill walking is underway. Data is accumulating on the optimal dose and form of exercise for PD and is nicely summarised in guidelines by the Parkinson’s Foundation (USA) in conjunction with the American College of Sports Medicine.
Ideally, an expertly supervised program includes activities from four domains: aerobic, strength training, balance/agility/ multi-tasking and stretching.
It also provides recommendations on suitable forms of exercise, frequency, duration and intensity. A further nuance to this is to distribute the proportions of these domains in relation to an individual’s stage of PD.
For example, early on, high intensity aerobic and strength training might be emphasised. At later stages, balance and agility might receive more attention. The beneficial effects of group training and socialisation are also important. Exercise should be combined with medication, and best undertaken while in the “on-state”
Attention to nutrition in relation to the energy expenditure and protein requirements due to exercise is also important. Fatigue, weight loss and injury may be the consequence
of overtraining with enthusiastic unsupervised exercise programs.
Nutrition and diet are gaining prominence in the management of PD. There is now considerable long-term observational data on PD and dietary habits, in relation to risk, age of onset and progression.
Favourable factors include a mainly plant based diet, consumption of coffee, fish and possibly wine.
Unfavourable foods include red meat, dairy products, sugar and highly processed foods. Consumption of ultra-processed foods has recently been shown to be associated with increased risk of prodromal PD symptoms. There are very few interventional randomised controlled trials of diet in PD.
The Mediterranean diet has been shown to have benefits in markers of cognition in PD compared with controls. A model comparing the Mediterranean diet with the MIND and PRO PD 21 diets has been proposed.
An important issue related to diet is the potential for food contamination by toxins (particularly pesticides).
Unfortunately, some of the foods most likely to be beneficial, such as blueberries are also at risk of having pesticide residues. Herbicides such as paraquat, glyphosate and insecticides like organochlorine have been linked to PD.
Released in mid-2025, a landmark book, The Parkinson’s Plan, by neurologists Ray Dorsey and Michael Okun highlights 25 practical steps to potentially decrease personal and population risk of PD.
Their number one recommendation is to wash fruit and vegetables, even if it organically grown. The second is to change diet as suggested above. More than half of their recommendations involve lifestyle.
The central theme is recognising that environmental toxins are likely to be the major factor behind the startling increase in PD over the past three decades, and that changing the way we live may play a key role in slowing this.
Stress has been shown to impact on PD pathology in animal models and to increase motor symptoms in humans.
Approximately half of all people with PD will experience anxiety or depression. Stress reducing strategies such as mindfulness and yoga has been shown in a randomised trial to be beneficial for PD symptoms.
The combination of multiple lifestyle interventions has the potential for a synergistic effect, with the possibility of creating a positive feedback loop.
For example, dietary change may affect gastrointestinal microbiome and bowel habits, allowing for better absorption of medications, which may allow for more effective exercise and the associated benefits.
The key message is that lifestyle interventions are showing great promise for symptom management and possibly disease modification in PD.
Hear from WA specialists on common presentations in General Practice including:
• Lipid Management
• Panel discussing HRT considerations
• Vaccinations for older adults
• Peripheral Vascular disease
• The acute red eye
• Upper limb presentations
• Handling Aphra complaints
• Decoding the Murmur: A Practical Guide for GPs
Further studies of specific interventions are needed to build the evidence base. Packaging lifestyle interventions together to create a holistic care plan would seem ideal.
From my own perspective as a person living with PD, I have found new data on quantifying the optimum level of exercise to be very helpful to guide my level of training.
I have also undertaken dietary changes on the basis of the observational data. While I feel like they have been beneficial, it would be very encouraging and incentivising to have firm interventional data to support this.
Author competing interests - nil
0.5 0.5
By Dr Reza Feizerfan, Pain Specialist, Nedlands & Murdoch
Following a thorough pain assessment, developing a comprehensive management plan is essential for reducing suffering, enhancing quality of life, and improving function and independence.
Pain management plans should address the physical, psychological, and social aspects of pain. This holistic approach ensures that all factors contributing to the patient’s pain are considered, leading to more effective outcomes.
When managing pain in older adults, it is crucial to account for physiological changes, including altered pharmacokinetics and declining liver and kidney function.
For example, a patient who has been on a stable dose of pregabalin for many years may require a dose adjustment if their kidney function declines.
Healthcare providers must balance the need for effective pain relief with the potential risks of adding to an already complex medication regimen.
This requires frequent medication reviews and careful consideration of non-pharmacological treatment options. The Beers Criteria, published by the American Geriatrics Society, serves as a valuable reference in this regard.
Paracetamol is one of the safest analgesics for older adults. Although drug interactions are possible, they are relatively rare. A key consideration is dose adjustment for individuals with body weight under 50kg (15mg/kg/dose).
Non-Steroidal Anti-inflammatory Drugs (NSAIDs) should be used sparingly and with extreme caution in this population. Both the American and British Geriatric Societies recommend minimising or avoiding NSAIDs and COX-2 selective inhibitors in older adults due to their


potential to cause kidney failure, gastrointestinal bleeding, and cardiovascular toxicity.
If NSAIDs are required, they should be prescribed for the shortest possible duration at the lowest effective dose, with close and regular monitoring.
Opioids can have profound adverse effects even at low doses in older adults. Side effects such as respiratory depression, sedation, falls, cognitive impairment, and constipation may occur even after a single dose.
The risk of interactions with other centrally acting medications should also be considered. When prescribing opioids, it is essential to start with a lower-than-normal dose, especially in opioid-naïve patients, and to allow longer dosing intervals with slow upward titration.
Starting with immediaterelease formulations can help guide appropriate dosing for slow-release versions.
Gabapentinoids are effective for managing neuropathic pain but
are primarily excreted through the kidneys, requiring dose adjustments and longer intervals in patients with impaired renal function.
For instance, in patients on renal dialysis, a single dose of pregabalin after dialysis may suffice, as the drug will remain in the system until the next dialysis session.
Antidepressants (serotoninnoradrenaline reuptake inhibitorsSNRIs and tricyclic antidepressants - TCAs) are commonly used for neuropathic pain.
However, they can cause significant side effects, including drowsiness, falls, cardiac conduction issues, nausea, vomiting, postural hypotension, electrolyte imbalances, and cognitive impairment. TCAs are associated with more side effects in older adults than SNRIs.
Benzodiazepines are rarely recommended for pain management. When combined with other centrally acting drugs, they can significantly increase the risk of morbidity and mortality.
• Prescribing medications needs careful consideration
• Allied health input is invaluable
• Injections for pain management can work very well with less side effects in older adults.
Adjuncts to pain management may include medications like low-dose naltrexone or memantine, topical treatments, or over-the-counter options such as turmeric, fish oil, palmitoylethanolamide (PEA), and transcutaneous electrical nerve stimulation (TENS) therapy.
These can complement pharmacological pain management strategies while minimising the need for higher-risk medications.
Numerous studies underscore
Exercise programs tailored specifically for older adults can improve strength, flexibility, and balance, and thereby reduce musculoskeletal pain and enhance overall function.
Cognitive-behavioural therapy (CBT) is also highly effective in helping patients address the psychological aspects of chronic pain, reducing dependence on medications and improving their quality of life.
Injections in older adults tend to have fewer side effects compared to pharmacological treatments. Procedures such as facet joint injections, radiofrequency ablation (rhizotomy), epidural, and nerve root sleeve injections, when carefully selected for appropriate cases, can greatly enhance a multidisciplinary care approach. These interventions can reduce the need for long-term
Ultimately, when treating chronic pain in older adults, several non-pain-related factors must be considered before developing a management plan. Pharmacological options should be chosen with caution, augmented by incorporating physical therapy, psychological support, and patient education.
The role of interventional techniques, such as injections, should not be overlooked. Injections can be highly effective in alleviating pain, with less side effects compared to medications in older adults.
0.5 0.5


By Dr Rodrigo Carlessi, Senior Research Fellow, Curtin University
Hepatocellular carcinoma (HCC) is the most common form of liver cancer and carries a high disease burden.
Liver cancer (primarily HCC) is among the fastest-growing causes of cancer-related death in Australia. Approximately twothirds of patients experience recurrence within five years of curative-intent therapy.
The standard follow-up for HCC survivors relies heavily on imaging and serum tumour markers, but each has significant limitations. Post-treatment surveillance typically involves periodic imaging (MRI or CT scans) and checking alpha-fetoprotein (AFP) levels.
Small tumours – especially under 2cm – can evade detection. Many patients develop recurrences that grow for months before becoming visible on scans.
Serum AFP, while historically used for HCC surveillance, has wellknown performance gaps. Many early-stage HCCs do not produce a significant AFP rise, yielding poor sensitivity for detecting recurrence.
There is need for more sensitive, accessible tools to monitor for HCC returning after treatment.
The Liver-TRACE innovation
Liver-TRACE (a methylation-based liquid biopsy assay that detects traces of cancer DNA in the bloodstream) is a new precision health initiative from WA aimed at addressing these surveillance gaps.
It looks for tumour-derived genetic “signatures” in a patient’s blood – essentially a blood test to flag microscopic cancer recurrence before it’s visible on a scan.
The assay requires only a small volume of plasma, meaning it could be performed easily and even serially in resourcelimited settings – an important consideration for remote clinics.
This makes Liver-TRACE a highly scalable innovation, potentially


enabling more frequent surveillance than is feasible with MRI/CT alone.
While still experimental, early results for Liver-TRACE have been promising. In a pilot study, the research team found that the assay could detect residual ctDNA shortly after curative surgery even when post-operative MRI showed no remaining disease.
In other words, the blood test signalled microscopic cancer presence that imaging had missed – hinting at the ability to identify very early recurrence. These preliminary findings suggest the blood test may outperform our conventional tools (AFP and scans) in sensitivity, particularly for low-volume disease.
Indeed, the developers note that Liver-TRACE can detect tumour
fractions in blood as low as ~0.1–1%, considered of very high sensitivity for liquid-biopsy assays.
With these encouraging data, the Liver-TRACE project was recently awarded nearly $500,000 through the WA Future Health Research and Innovation (FHRI) Seed Innovation Fund program to expand into a larger trial.
A state-wide prospective clinical validation study is commencing recruitment in early 2026 to rigorously evaluate the test’s performance in routine follow-up of HCC patients.
The next step is to assess the test’s effectiveness in a larger group of patients. Importantly, during this phase, the assay will be offered in a research setting – it is not yet available for routine clinical use outside of clinical trials.
• Liquid biopsy tests (detecting circulating tumor DNA) for HCC surveillance are under development. These assays aim to catch early microscopic recurrence that traditional imaging or AFP might miss
• Consider referral of eligible HCC patients into clinical trials evaluating ctDNA-based monitoring (such as the Liver-TRACE study) once these become available
• Precision oncology approaches like methylation-based blood tests may augment or enhance standard HCC follow-up, particularly for patients in rural and remote settings.
If validated, how might a tool like Liver-TRACE fit into HCC management?
Potentially, it could complement the existing surveillance schedule by providing a quick, minimally invasive check for molecular relapse between imaging appointments.
For example, rather than waiting 3-6 months for the next scan, a clinician could use periodic ctDNA tests to “scan” the blood for early tumour signals.
A positive result might prompt earlier confirmatory imaging or intervention, whereas a negative result could reassure when imaging is delayed. This could be especially impactful in remote or underserviced regions of WA where access to MRI or specialist follow-up is limited.
A blood sample can be taken locally and sent to a central lab, enabling patients in rural areas to benefit from high-end genomic surveillance without frequent travel.
From a broader perspective, LiverTRACE exemplifies the ongoing shift toward precision oncology and personalised post-treatment care. It aligns with the trend of using liquid biopsies to monitor cancer in real-time, which could transform follow-up paradigms for HCC and other cancers.
Clinicians should keep an eye on clinical trial opportunities –patients who have had curative treatment for HCC may be eligible for studies like the LiverTRACE validation, which could offer additional surveillance on top of standard care.
Ultimately, while we must stress that ctDNA surveillance is not yet an established routine, its development signals where liver cancer care is heading.
Detecting recurrence earlier means a better chance to re-treat and potentially prolong survival, and innovations like Liver-TRACE are paving the way for more proactive, personalised cancer follow-up.
Author competing interests – the author is involved in the research described
“My period pain is totally normal.”

Soprano Jessica Blunt says opera mirrors some of the greatest themes about what it means to be human. Love, loss and sacrifice feature in West Australian Opera’s new production of La traviata.
By Ara Jansen

In an opera every singer brings their own experience and unique voice to a role, which makes no two performances the same.
For soprano Jessica Blunt, her debut lead role as Violetta for West Australian Opera’s La traviata this month will be as unique as she is.
“My version of a character is never going to be like someone else’s,” says Jessica. “I have to understand my character and see how they speak to me. It mixes with how I see life, and I can add my colour and interpretation.
“That’s what is so exciting about opera – how unique it can be. A singer will bring their own taste and flavour, their own emotions and life experience. I draw from my life experiences to see what might be similar to what Violetta is experiencing.”
Being a glamorous courtesan falling in love with an idealistic aristocrat isn’t everyone’s experience, but love, loss or dating someone your parents hate stand as fairly universal.
Considered one of the great love stories, in La traviata courtesan Violetta and aristocrat Alfredo have a society-defying passion which ultimately destroys them. Alfredo’s father demands Violetta leave her man to
protect the family’s honour and she agrees to make the ultimate sacrifice.
“At its core opera has those huge themes of humanity and so much of what we experience as human beings –versions of love, sacrifice and death. Violetta reminds us to make the most of the time we have, try and live the best lives we can and find joy and meaning in that.”
Part of Jessica’s preparation for the part is digging into Violetta’s emotions so she is not only able to sing the words in Italian but give them the right weight, emotion and level of sincerity.
“I have a bit of a process when I start working on a new role. I always start with the language, because in opera, the story and text are really important while the music serves as the drama. I start with what I am singing and thinking and I have to understand every word.
“I studied Italian and I can carry on a conversation – I’ve prioritised learning the languages I will be singing in. I want to be as real as possible and make sure I know why she is saying what she is saying and what has led her to this point.”
Jessica has synesthesia which gives her an added sensory layer that she says enhances her musical perception, memorisation and performance.

This neurological phenomenon allows a singer to see the colour of a pitch, feel the texture of a harmony or map an entire aria in their mind’s eye. This also means her scores are annotated in all the colours of the rainbow.
We have a bumper round of competitions for you this month, from films to wine.
We have one copy of David Whish-Wilson’s new book O’Keefe to giveaway. Follow the main character as he works on the wharves of Fremantle to investigate the Mexican cartel meth which is flooding the streets.

Or if you’d rather watch a film, we have 10 double passes to Project Hail Mary
And we’re continuing with our popular wine giveaways. This month you can win a selection of wines from Margaret River’s well-known Vasse Felix winery.
Read our Master of Wine’s review on page 53.
To enter, use the QR code on this page or go to mforum.com.au and hit the competitions tab.
In any opera, there are a lot of balls for a performer to juggle –singing, acting and sometimes dancing, much like their musical theatre counterparts.
Let’s not forget too, for the female characters, the added strain of a

heavy costume, requiring strength and aerobic fitness to simultaneous sing, move and carry the dress.
“You need to do plenty of exercise and have lots of stamina to prepare yourself for carrying a heavy costume around for three hours and still be able to sing strongly.
“Singing opera is a full body exercise and you’re likely doing it for three hours non-stop and about seven times in two weeks, as well as feeling all the feelings of the story while connecting with the audience and the people on stage with you. It’s an incredibly athletic job.”
La traviata is at His Majesty’s Theatre from March 14–28

An unexpected sighting of an old friend in a crime documentary set David Whish-Wilson on the road to his new book, O’Keefe.
During a night of insomnia author David Whish-Wilson went down an online video rabbit hole. He emerged having seen an old friend and the idea for his latest novel.
While watching a documentary about the 2021 death of well-known Dutch investigative journalist Peter de Vries, David spied an old friend in a crowd outside de Vries’ Amsterdam home, where mourners were gathering.
Having not talked to the man for decades, they reconnected, discussed the dead journalist and David started having ideas of what his fictional character Paul Cutler might do next.
By Ara Jansen
This led to the Fremantle resident’s twelfth crime novel, O’Keefe. In it, undercover operative Paul Cutler takes on a new identity as Paul O’Keefe. He’s a security guard working on the wharves at Fremantle to investigate the Mexican cartel meth which is flooding the streets.
O’Keefe discovers a world of offthe-books operations which has little to do with security and a lot to do with who has control over the port’s drug smuggling operations.
The de Vries documentary inspired the author to look at drug transport routes around the world and how they might end up off the coast and at WA ports. Then he started
to think about what O’Keefe might get up to in a fictional story with real practicalities.
“Drug smuggling is a rapidly evolving situation and a lot of information is online,” says David. “This happens all over the world and there’s a lot of information online going all the way back to growers through to transport information.”
Part of the attraction of writing for David is the opportunity to use his imagination and create something that doesn’t yet exist. He likes to create something with his mind, turn it into a narrative and gets great pleasure from making things with his hands.
He also makes jewellery, knives and whiskey.
“Writing is like my meditation. I go into a completely different mental state and writing is a great pleasure. It’s definitely something I feel a strong pull to do. I start to feel a nagging sense of frustration if I don’t write for a while and a need to get into that state.”
Originally David thought his previous book Cutler would be a standalone, but once he started thinking about his latest book he realised there was more to the character that he wanted to know and was intrigued by him playing such a high stakes game, where one wrong move could be fatal.
“O’Keefe is the same person playing a different role. He’s very chameleon-like and can move across different groups and see how far he can push it. He’s also figuring it out as he goes along.
“He’s surrounded by people who if they find out who he is, he would be in trouble.”
Set largely around Fremantle, David enjoys writing about the city he loves and knows so well. It allows him to use both true details and let his imagination run wild – and a reason he also loves reading other people’s novels set in Western Australia.
“In a place like Perth, there’s always what’s happening on the surface – the beautiful beaches, clear skies – and a story like this
is a good vehicle for the stories happening underneath that.”
O’Keefe is out now through Fremantle Press. Medical Forum has a copy of O’Keefe to giveaway, head to our competitions section to find out more.



The Peoples Economist
MON 2 MAR
Gary Stevenson, former Citibank trader turned bestselling author of the The Trading Game and global voice on inequality, comes to Australia for the very first time.
The Crofty & Ant Show
MON 9 MAR
Fresh from the Melbourne Grand Prix the day before, Crofty and Ant will share all the latest insights about the teams and drivers, giving us a glimpse of what to expect from the rest of the thrilling 2026 Formula 1® race calendar.




Seventh Wonder
SAT 7 MAR
This world-class performance, brings together a star-studded band and a 16-piece string symphony orchestra to create an unparalleled tribute to Fleetwood Mac’s music.
An Intimate Evening With Celtic Thunder
TUE 24 MAR
Featuring a carefully curated setlist of their greatest hits, this show will showcase the powerful harmonies, soaring ballads, and electrifying performances that have made Celtic Thunder a household name.


The Australian Beach Boys
SUN 8 MAR
Australia’s original, and number one award winning Tribute Show to the iconic Beach Boys.
Rockaria
FRI 27 MAR
The ELO Experience – a tribute to the unforgettable sound of “Jeff Lynne’s The Electric Light Orchestra. The iconic English rock band from Birmingham.

At Humphrey Homes, every home we design and build begins with listening. We take the time to understand your vision, your lifestyle and your budget - then shape that insight into thoughtful spaces that are beautifully crafted. By seamlessly integrating architecture, interior design and construction, we make creating your forever home harmonious, effortless and deeply personal.
To start the conversation, call Dean Humphrey on 9284 5444.

It was in 1967 that Perth Cardiologist Dr Tom Cullity planted vines on his Vasse Felix property in Cowaramup, Margaret River region – one of the first to plant vines in the now internationally known region.
Vasse Felix has been blessed by a procession of fine winemakers. Cullity employed Cumbrian cheesemaker and self-taught winemaker David Gregg, with their first vintage in 1972.
I was lucky to work the 1987 vintage with David and witnessed his prowess. He later became owner, with his hard work setting the benchmark and creating the wine styles that have made Vasse Felix famous.
He sold to the Holmes a Court family in 1987 but continued for some years as their viticulturist/winemaker. Follow on winemakers Clive Otto and currently Virginia Willcock have pursued quality to an even higher level.
As well as the home Estate they own several other properties within the region totalling over 230 hectares of vines. Their focus has been on the most premium Margaret River varieties – Chardonnay and Cabernet Sauvignon.
Wines are released in several quality levels. The Filius range is the entry level wine, followed by the premium range of greater quality and longevity. Then there are the super-premium Heytesbury Chardonnay and Tom Cullity Cabernet Sauvignon Malbec.
But it must be said having tasted the Filius wines that all are of very good quality.
Vasse Felix Filius 2025 Margaret River Sauvignon Blanc, RRP $28
Attractive limpid light gold colour with a green tinge. Bright, clean, penetrating aromas without being overstated, displaying lemon pith and grapefruit. The palate has flavours of peach and green apple. This wine is drinking very nicely now.
Vasse Felix Filius 2025 Margaret River Chardonnay, RRP $ 30
Very good entry level Chardonnay and good value. Palate focused and linear with citrus and grapefruit. Wonderful lively acidity. Oak just comes through adding a little textural weight.A very pleasing early drinking style that will also drink well for another two to three years.
Vasse Felix 2024 Margaret River Chardonnay, RRP $ 46
The premium level Chardonnay from the 2024 dry, warm, early vintage but has not compromised the fruit quality in this wine. Nectarine and citrus flavours with roasted cashew from oak, alongside complex flavours of white peach and Nashi pear.
More intense and complex than the Filius, will drink well for a few years.
Vasse Felix Filius 2023 Margaret River Shiraz, RRP $28
Plush fruit across the palate. Oak in the background indicative of maturation in aged oak. Fruit characters of ripe satsuma, plum, blueberry, black pepper and allspice. Tannins fine grained and supple. The pepper and spice characters in this wine suggest that fruit was sourced from the cooler more southerly areas of Margaret River.

Good current drinking. Has the integrity and structure to cellar for another five to seven years.
Vasse Felix Filius 2013 Margaret River Cabernet Sauvignon, RRP $ 30
A great value entry level Cab Sav. The addition of some Malbec has added a savory supple edge. Nose is fruit driven, leafy with varietal blackcurrant. Palate shows blackberry, dark plum and dried herbs. Fine grippy tannins. Made for current drinking but will reward for another three to five years.
Vasse Felix 2023 Margaret River Cabernet Sauvignon, RRP $56
This premium wine is richer, deeper and more intense than the Filius. For me, it is what Margaret River is all about.
The deep ruby red colour suggests this wine is youthful. Nose shows classic Margaret River cassis. It is oaky and complex. Wonderful flavours of blackcurrant and black olive follow on the palate. Intense fruit with layers of quality oak, fine acidity and supple tannins all beautifully integrating.
If this wine is premium, then I can’t wait to get my hands on a bottle of the super-premium Tom Cullity. A great wine that will give pleasure for 12 to 15 years.