



For the most vulnerable in society cutting back to save money can often come at the cost of essentials like food… or healthcare.
I’m willing to bet everyone has thought about their finances in some way, shape or form in recent weeks.
With interest rate rises and the price of fuel hitting our pockets, the cost of living is once again front and centre of headlines.
Most people will be cutting back in some way to keep their bank accounts happy, but for the most vulnerable in society that can often come at the cost of essentials like food… or healthcare.
There has been a greater focus on the affordability of healthcare in recent months, but is it enough?
The federal government has introduced bulk billing incentives – which from initial data seem to be having some impact – and it has made moves to change prescribing practices to make it easier for patients to access some medicines, although it should be noted GPs are cautious about this.
In a bid to make care more affordable for the most vulnerable, the RACGP and 20 other patient bodies have called on the federal government to increase Medicare rebates for longer GP consultations.
The College has long been calling for a 40% increase to Medicare rebates for these appointments, which it says will allow patients with complex needs to have their care met without it hitting their wallet.
But on the flip side, there is a conversation to be had on whether attributing a dollar value to consultation minutes will actually make care more affordable, or will it just mean more people can spend longer with already time-poor GPs?
What do you think? Email editor@mforum.com.au
SYNDICATION AND REPRODUCTION Contributors should be aware the publisher asserts the right to syndicate material appearing in Medical Forum on the mforum.com.au website. Contributors who wish to reproduce any material as it appears in Medical Forum must contact the publisher for copyright permission.
DISCLAIMER Medical Forum is published by Medforum Pty Ltd (Publisher) as an independent publication for health professionals in Western Australia. Neither the Publisher nor its personnel are medical practitioners, and do not give medical advice, treatment, cures or diagnoses. Nothing in Medical Forum is intended to be medical advice or a substitute for consulting a medical practitioner. You should seek immediate medical attention if you believe you may be suffering from a medical condition. The support of all advertisers, sponsors and contributors is welcome. To the maximum extent permitted by law, neither the Publisher nor any of its personnel will have any liability for the information or advice contained in Medical Forum. The statements or opinions expressed in the magazine reflect the views of the authors and do not represent the opinions, views or policies of Medical Forum or the Publisher. Readers should independently verify information or advice. Publication of an advertisement or clinical column does not imply endorsement by the Publisher or its contributors for the promoted product, service or treatment.
Advertisers are responsible for ensuring that advertisements comply with Commonwealth, State and Territory laws. It is the responsibility of the advertiser to ensure that advertisements comply with the Competition and Consumer Act 2010 (Cth) as amended. All advertisements are accepted for publication on the condition that the advertiser indemnifies the Publisher and its personnel against all actions, suits, claims, loss or damages resulting from anything published on behalf of the advertiser.
EDITORIAL POLICY This publication protects and maintains its editorial independence from all sponsors or advertisers. Medical Forum has no professional involvement with advertisers other than as publisher of promotional material. Medical Forum cannot and does not endorse any products.





We’ve got another round of wine to giveaway this month, this time from Frankland Estate
Read our Master of Wine’s review of the winery on page 43 for more on these iconic wines.
Medical Forum readers can also get 15% off their first purchase of a dozen Frankland Estate wines with the code MEDF15.
Or if you’d fancy something other than wine, we’ve got another book up for grabs.
To enter, scan the QR code on this page or go to mforum.com.au and hit the competitions tab.
PUBLISHERS
Alice Miles – Director Fonda Grapsas – Director
Tony Jones – Director
EDITORIAL TEAM
Managing Editor
Andrea Downey 0437 909 904 andrea@mforum.com.au
Clinical Editor
Dr Joe Kosterich 0417 998 697 joe@mforum.com.au
Graphic Design Studio Scotts hello@studioscotts.com.au
ADVERTISING
Advertising Manager
Bryan Pettit 0439 866 336 bryan@mforum.com.au
Advertising Account Manager and Clinical Services Directory
Rita Murphy 08 9203 5222 rita@mforum.com.au
CONTACT MEDICAL FORUM
Suite 3/8 Howlett Street, North Perth WA 6006
Phone: 08 9203 5222 Fax: 08 6154 6488 Email: info@mforum.com.au www.mforum.com.au












A GP who transformed youth healthcare and another who provides on-call and after-hours cover for obstetrics and anaesthetics have been recognised in the 2026 WA Rural Health Excellence Awards.
This year’s recipients span nearly every region of WA, highlighting the depth of expertise, commitment and compassion that underpin rural healthcare.
Dr Sarah Youngson was named Community Health Professional of the Year. The GP was recognised for transforming youth health in the Warren Blackwood region.
For more than a decade, she has delivered inclusive, holistic care that extends beyond the clinic.
She was involved in the creation of a program to streamline consultations and reduce waiting times, called the Kids Colab program, founded Blackwood Youth Action and chairs the BridgetownGreenbushes Suicide Prevention Network.
In 2024, she secured funding for a GP in Schools initiative at Manjimup Senior High School, improving access and reducing stigma around mental health and LGBTQIA+ inclusion.
In other awards, Dr Richard Taylor was recognised as General Practitioner of the
The full list of winners:
Aboriginal Health Professional of the Year: Vernon Dann (Kimberley)
Allied Health Professional of the Year: Kathryn Braysich (Midwest)
Clinical Leader of the Year: Kim Tracey (South West)
Community Health Professional of the Year: Sarah Youngson (South West)
Doctors are warning of a risk to women’s health amid a “dangerous” decision by the federal government to allow pharmacists to prescribe the oral contraceptive pill.
From January 2027 a pilot program will allow concession holders to access contraceptives and treatments for uncomplicated UTIs prescribed by qualified pharmacists, without a doctor’s prescription.


Year for his work advancing rural healthcare through leadership, teaching and advocacy.
He has served the Geraldton and Midwest communities for more than a decade and provides consistent on-call and after-hours cover for obstetrics and anaesthetics, responding to urgent and complex cases to support local maternity and surgical services.
Rural Health West chief executive Professor Catherine Elliott said the awards highlighted the critical role rural health professionals play in community wellbeing.
“Their work strengthens communities, inspires colleagues, and highlights the vital role rural healthcare plays in building healthier, more connected regions across our state,” she said.
General Practitioner of the Year: Richard Taylor (Midwest)
Health Team of the Year: WACHS Older Person Complex Care Team (South West)
Nurse or Midwife of the Year: Jane Darlington (Kimberley)
Specialist (non-GP) of the Year: Jacinta Cover (South West)
Young Professional of the Year: Rosalie Gent (Goldfields)
WA Country Health Service Intern of the Year: Celia Wong (Midwest)
WA Country Health Service
Resident Medical Officer of the Year: Catherine Daly (South West)
Chairs’ Award: WACHS Older Person Complex Care Team (South West)
RACGP Vice President and WA
Chair Dr Ramya Raman said the decision represents a serious failure of health policy that puts women’s health and safety at risk.
Dr Raman said that while hormonal contraception is safe and commonly used, it should not be prescribed casually.
“It carries well established risks, including increased risk of stroke and blood clots, particularly
during periods of hormonal change, the very times when women need comprehensive medical assessment, not fragmented care,” she added.
“Allowing pharmacists to prescribe the pill sends a dangerous public health message to Australian women, that this is a simple, riskfree medication when it is not.”
National President of the Pharmacy Guild of Australia Professor
An Australian-first surgery carried out in Perth has enabled a patient with suspected lung cancer to have biopsies taken, cancer confirmed and then removed all in one operation, under one anaesthetic.
The ground-breaking procedure was carried out at Sir Charles Gairdner Hospital earlier this year.
Respiratory medicine consultant
Dr Dhaval Thakkar led the surgery, detecting the cancer deep in the lungs, before carrying out precision tissue sampling and then highlighting the cancer with a glowing marker for a thoracic surgeon to easily locate.
Thoracic surgeon Dr Miguel Mesa-Guzman followed with keyhole surgery that led to the patient waking up cancer-free.
Dr Thakker said while the surgery involved a lot of planning, it improved hospital efficiency as it replaced what would have been multiple procedures. Instead, the entire surgery was carried out in just five hours.
He said the hospital’s bronchoscopy robot equipment allowed greater access to lesions or nodules on the lungs and mapped out defined pathways.
Trent Twomey welcomed the news as recognition of the vital role pharmacists play as the “most accessible frontline primary healthcare providers”.
“Women deserve expert care where and when they need it — and community pharmacists are uniquely placed to provide it safely and locally,” he said.
Registered nurses may soon be able prescribe medicines under the Pharmaceutical Benefits Scheme (PBS).
A Senate Committee has recommended the passage of the Health Legislation Amendment (Prescribing of Pharmaceutical

“We are usually constrained as to whether the airway reaches the lesion, but the robotic system helps us get to those difficult to reach parts of the lungs,” Dr Thakker said.
He said his team had pathologists right at the bedside to carry out the biopsy process.
“They can tell us if it looks like normal lung or whether it could be inflammatory or could be cancer,” Dr Thakker said.
He said it was an exciting surgery to be part of and was proof that the public hospital system in Australia could take on complex procedures.
Benefits) Bill 2025, which would allow designated registered nurses to prescribe medicines as of July.
However, the RACGP WA branch is concerned that allowing registered nurses to prescribe medicines under the PBS may affect patient outcomes, fragment care, put patients at risk of misdiagnosis and potentially delay necessary treatment.
Dr Ramya Raman said a GP-led model of care was preferred.
“Prescribing is a complex clinical task. For the safety of patients, it should occur within a coordinated, GP - led care model that prevents fragmentation and ensures appropriate oversight of high - risk medicines,” she said.

“This includes strong clinical governance, clear prescribing agreements, shared care records, and ongoing GP collaboration to ensure safe, continuous care for patients.”
The Australian College of Nursing (ACN) welcomed the recommendation.
ACN chief executive Adjunct Professor Kathryn Zeitz said:
“Designated registered nurse prescribing will strengthen the health system by easing workforce pressures and building the longterm capacity and sustainability our communities urgently need.
“Nurses operate across most healthcare settings, and this means their patients will be able to access prescriptions in a timely and equitable way.”
The endoscopy team at St John of God Hospital Murdoch has made a small change that drastically cut plastic waste and use of toxic chemicals.
Plastic waste makes up about a third of the general waste produced by hospitals in Australia, and due to infection prevention concerns, much of it is incinerated.
This includes the histopathology pots used for holding samples taken during endoscopy procedures.
But one simple change has helped address this. Head of Gastroenterology and Endoscopy
Dr Oliver Waters said most samples during these procedures were just a few millimetres, yet hospitals used 70ml pots.
Dr Waters and Clinical Nurse Carla Hazelgrave led the team’s move to smaller 25ml pots.
“It makes no sense having a 2mm specimen floating in a 70ml pot, it’s the equivalent of keeping and transporting a human-sized sample in an Olympic swimming pool-sized pot,” he said.
Medical colleges across Australia have called for ethical billing practices and fee transparency to tackle disparities in access to specialist care.
The Council of Presidents of Medical Colleges has warned patients are increasingly concerned about access to specialist care, including out of pocket expenses and unexpected bills. It launched a national professionalism framework on ethical billing and fee transparency in March.
The framework establishes shared expectations for ethical billing, fee transparency and informed financial consent.

“Samples are separated into different pots according to patient procedure and anatomical location of the tissue sampled. It is common that at the end of a list between 10 and 30 individual pots are used.”
The team use around 41,000 pots each year and transitioning to smaller pots has helped save an estimated 26 kilograms of
It sets out several key principles that should be followed, including:
• Plain-language disclosure of all costs
• Genuine informed financial consent as a prerequisite to treatment
• Compassionate billing that accounts for patients’ circumstances.
It also sets out an explicit expectation that specialists consistently uphold these principles in their practice.
CPMC Chair Associate Professor Kerin Fielding said: “Patients deserve clear information about the cost of their care and the
plastic and over 700 litres of formalin from being incinerated each year, just at Murdoch.
“By reducing their size, we’re cutting down on waste, lowering our exposure to formalin, and proving that sustainability and high-quality care can go hand in hand,” Dr Waters said.
confidence that billing practices are fair, transparent and respectful.
“This framework reinforces that informed financial consent is not complete unless patients have had a genuine opportunity to understand the financial implications of their care, including available alternatives.”
Billing practices that exploit vulnerabilities, obscure costs, or include undisclosed fees are inconsistent with professional standards and should not form part of contemporary specialist practice, the Council said.

The RACGP and 20 peak patient bodies have called on the federal government to increase Medicare rebates for longer GP consultations to reduce out of pocket costs for patients.
The RACGP, along with groups including Palliative Care Australia, Parkinson’s Australia, Sexual and Reproductive Health Australia and Dementia Australia, delivered an open letter to Parliament House in Canberra last month.
“Currently, the per minute value of patient Medicare rebates decreases the more time a patient spends with their specialist GP. That means, for many people, the sicker you are, the more you pay out of pocket,” the letter stated.
RACGP President Dr Michael Wright said properly funding longer consultations was vital for patients with chronic disease, mental health concerns, and complex health needs.

He pointed to the positive flow-on effects it would have, including improving diagnosis times,
making care more affordable, and reducing pressure on already stretched hospitals.
“The RACGP has long called for a 40% increase to Medicare rebates for Level C and Level D consultations, and with average GP appointment times getting to 20 minutes in 2025 this funding is well overdue,” he said.
“The health needs of our communities are becoming more complex, with many people experiencing one or more longterm health conditions, so the care GPs provide requires more time, space, and empathy.
“When people can’t afford longer GP appointments, complications and other health issues develop. People get sicker and need expensive hospital care.”
The letter quoted analysis that showed increasing Medicare rebates for long GP appointments would deliver more than $338.9 million in annual healthcare system savings.
Australian Patient Advocacy Alliance chief executive Deidre Mackechnie said that poorly managed chronic or complex disease had a significant impact on the health system, contributing to “the overloaded system we see now”.
“We also see the impact on the lives of people living with a chronic condition: reduced ability to care for family or to work, often not being able to work at all, or to participate in social activities,” she said.
“Inadequate management of a chronic condition can result in disease progression to the point of disability, including the need to access the NDIS.
“Longer consultations with the GP will contribute to better management and consequently better outcomes so that people living with a chronic condition are living their best life and we enjoy a healthcare system that works for all.”
How long is too long to be playing video games? While children may enjoy playing games, there comes a point where it becomes bad for their health.

By Aleisha Orr
An increasing number of primary and high school aged children are presenting in GP clinics with issues related to excessive gaming.
While playing games itself is not a direct risk to children’s health, spending too much time on the console was found to be impacting sleep, diet and overall activity levels, leading to an increased risk of longer-term health conditions later in life.
WA research and a Perth GP have warned there comes a point when health professionals may need to intervene.
Research from Curtin University, published in Nutrition, surveyed 317 students from five Australian universities with a median age of 20 years old.
Participants were split into three groups depending on the self-reported amount of time spent playing video games.
Low gamers were those who spent zero to five hours per week gaming, moderate five to 10 hours, and high gamers more than 10 hours.
The team found that while low and moderate gamers reported similar health outcomes, results worsened dramatically once gaming exceeded 10 hours a week.
Professor Mario Siervo, from the Curtin School of Population Health, said the findings suggested excessive gaming was the key issue, rather than gaming itself.
“What stood out was students gaming up to 10 hours a week all looked very similar in terms of diet, sleep and body weight,” Professor Siervo said.
“The real differences emerged in those gaming more than 10 hours a week, who showed clear divergence from the rest of the sample.”


The study found a decline in diet quality once gaming exceeded 10 hours per week. Obesity was more prevalent in the high gamers’ group, compared to low and moderate gamers.
High gamers had a median body mass index of 26, compared to the healthy range of around 22 for low and moderate gamers.
“Each additional hour of gaming per week was linked to a decline in diet quality, even after accounting for stress, physical activity and other lifestyle factors,” Professor Siervo said.
Gaming hours also showed a significant link to sleep disruption. All groups reported generally poor sleep quality, but moderate and high gamers scored worse.
“This study doesn’t prove gaming causes these issues, but it shows a clear pattern that excessive gaming may be linked to an increase in health risk factors,” Professor Siervo said.
“Our data suggests low and moderate gaming is generally fine, but excessive gaming may crowd out healthy habits such as eating a balanced diet, sleeping properly and staying active.”
The study concluded that excessive gaming may contribute to adverse health outcomes. It recommended targeting excessive or high gaming levels and promoting healthy lifestyle habits in university to prevent bad health habits following students into adulthood.
While the study focused on university students, Perth GP Dr Andrew Leech warned similar patterns were emerging in primary and high school students.

A rise in gaming disorder and related problems among children and young adults was noted during the COVID-19 pandemic, typically showing up as presentations in emergency departments and youth and adult mental health and medical wards.
To combat the issue, an Australianfirst gaming disorder clinic has been operating within Fiona Stanley Hospital’s Addiction Prevention and Treatment Service since 2022.
Dr Leech, director of The Garden Family Medical Clinic, said health and wellbeing problems related to gaming addiction and unhealthy social media use had become more prominent in the past 10 years.
“This reflects a fast-evolving digital landscape that healthcare providers need to engage with more actively in clinical conversations,” he said.
“While gaming and social media are now a normal part of young people’s lives, the intensity, accessibility and design of these platforms have changed significantly over the past decade, and this has clinical implications.”
Dr Leech said gaming use seems more prevalent in boys from mid-primary school through to high school.
He noted there was also a strong association between problematic gaming and young people who were neurodivergent, socially isolated, or experiencing anxiety or low mood, and that unhealthy gaming use often presented indirectly in GP clinics.
“For some, gaming becomes an escape in a world that
otherwise feels overwhelming or unsafe,” Dr Leech said.
“Families rarely book an appointment specifically for gaming or social media.
“Instead, we see sleep disturbance, irritability, emotional dysregulation, school refusal, declining academic performance, anxiety, low mood, or family conflict.
“I also see adults who struggle to disengage from gaming, sometimes at the expense of sleep, mood and daytime functioning.
“This is the tip of the iceberg – what is going on under the surface is what we really need to consider, not only the amount of screentime and what games are being played but also screening for mental health and developmental conditions.”
Dr Leech encouraged GPs to consider that parents were sometimes unaware of the extent of their child’s gaming or online activity, particularly when devices were used in bedrooms or with headsets.
“In busy households, this can be easy to miss and screens can unintentionally become a coping tool or ‘digital babysitter’.”
He said some children described spending many hours gaming without eating, drinking water, or going outside.
“Some speak very casually about violent content within games, which raises concerns about emotional desensitisation and developmental appropriateness,” he said.
“The interactive and social nature of modern games, often played online with voice chat, also increases exposure to risks such as inappropriate content, pornography, and contact with strangers posing as peers.”
In more severe cases, Dr Leech had worked with families who had made attempts to limit or remove devices only for their child to become distressed or aggressive.
He said such behavioural responses could resemble withdrawal, which reflected the powerful reward-based design of many gaming platforms. Continued on page 11



Because of the risks associated with high levels of gaming, and the likelihood that will be seen in GP clinics, Dr Leech called for better training and upskilling in the area.
“There has been very little formal training for primary care clinicians in recognising and managing problematic gaming or social media use,” he said.
“We need better frameworks to guide assessment and support. This includes understanding popular games and platforms, how algorithms work, and the specific risks for vulnerable young people.”
Clinicians can play an important role in normalising discussions, validating parental concerns, and supporting families with practical, evidence-based strategies. In his practice, Dr Leech goes beyond asking about total screen time.
“I ask about what is being played or watched, who the child is interacting with, and what type of content their feeds are promoting.
“This is particularly important in mental health presentations. I have seen cases where social media algorithms appear to reinforce distress, such as repeated exposure to dark, violent or suicidal content in adolescents already struggling emotionally.”
The goal does not have to be around prohibition of games and devices, but rather about balance.
“The challenge is helping families set developmentally appropriate boundaries that are realistic and sustainable, balanced with time outdoors and participating in other activities without a screen.”
He urged doctors to encourage early conversations, clear expectations, consistent routines, and adults modelling healthy screen use themselves.
A 12-year-old boy presented to his GP with escalating behavioural difficulties centred on technology use, with a background of Autism Spectrum Disorder (ASD), combinedtype ADHD, Pathological Demand Avoidance (PDA), Generalised Anxiety Disorder and intellectual disability.
Gaming disorder is increasingly recognised in this population and research confirms that boys with both ASD and ADHD carry significantly elevated risk for problematic video game use.
From a GP perspective, the central challenge was coordinating an already complex background while supporting his family and keeping him engaged at school.
It became more obvious when he started refusing to go to school simply because the drawcard of gaming was far too strong, and his parents were struggling to motivate him enough to attend. When there is a lot going on like this, it is easy to miss issues such as screentime until much later in the journey.
This child would spend the entire weekend gaming, only stopping for a few hours to sleep. He would need prompting to eat his meals and it would often turn into an argument.
In this case, any amount of screen restriction, or even stopping screen use, consistently led to severe dysregulation including aggression, physical violence toward parents, property destruction, and complete breakdown of family functioning. His parents described a fundamentally different child on versus off the device.
Management required genuine multidisciplinary coordination and maintaining regular bookings to check in and support the family. In this situation, there needs to be a family focussed approach, rather than simply managing the child. He was already seeing a developmental paediatrician, and we remained connected via phone calls or emails to try and develop the best medication combination. This turned out to be a higher dose of stimulant for his ADHD (lisdexamfetamine, dexamfetamine) to help treat his very impulsive behaviour.
It was important to involve an occupational therapist who could see him in his home environment and work through some simple changes including speaking with the school to enforce that he cannot bring his school laptop home.
His parents were referred to a psychologist for parenting support as they were struggling at both ends of the boundary setting, give in and he could spend all night gaming, be too tough and they would be at risk of violence and a dysregulated child.
This illustrates a common example in that gaming disorders and neurodevelopmental conditions are often linked. The GP role is vital in maintaining a therapeutic relationship, coordinating the team, supporting overwhelmed carers, and advocating for additional measures in his environment including at school.

This case study was provided by Dr Andrew Leech.

Being diagnosed with Parkinson’s Disease forced Clinical Professor David Blacker to change direction and form a different outlook on life.
By Ara Jansen
After the shock of being diagnosed with Parkinson’s Disease, Clinical Professor David Blacker AM decided he wasn’t going to live in fear of what might happen but instead thrive firmly in the present and live his most satisfying life.
The neurologist was diagnosed in 2018 and decided he would do all he could to slow down any progression. He also pivoted his career to focus on research and advocacy.
“I do know a bit about the brain,” he says in an amused way while alluding to his decades of work.
These days that workload looks a lot lighter, though some would argue he’s still pretty busy making noise about and supporting people with Parkinson’s. He’s also taking care of his health by keeping up an active lifestyle which includes boxing and yoga.
He previously used running to keep fit and maintain a healthy body weight, including completing six marathons. After developing dystonia in his right leg, David struggled to run even short distances, so he searched for other activities to keep fit.
Through mutual connections, David met former champion boxer Rai Fazio and started training with him. Fazio’s PD Fighters is a boxing therapy program the pair codesigned to empower people with Parkinson’s to reclaim strength, balance, co-ordination and fitness. There are now eight classes a week in Leederville and the pair are working to also move south of the river.
“Particularly for balance, I’ve found it amazingly helpful,” David said.
After prostate cancer surgery and a retinal detachment derailed his health in 2023, David used his knowledge from exercise-based therapy to get his fitness back.
His wife Kirsten, a midwife and yoga teacher, collaborated with an exercise physiologist to build a recovery program. Between walking, yoga and regular boxing classes he’s covering aerobic activity, strength training, balance, agility and multitasking.
“I started doing yoga about 12 years ago as a way to try and help me relax and handle the stress of work. I was pretty crap at it. Then Kirsten did her teacher training
and we now have a Friday class as part of a program for people with Parkinson’s.
“I think it has kept me in better shape than I otherwise would have been.
“There’s a paradigm with Parkinson’s that you always get worse and that can be a selffulfilling prophecy. Lifestyle changes, including diet, exercise and stress reduction can really make a difference. Keeping positive and active is the key.”
David’s Newly Diagnosed Parkinson’s Clinic at the Perron Institute is an “opportunity to really shape the course of the disease”, especially during the shock in the first few weeks post diagnosis.
“We connect them with the right people and show them how to avoid getting bad information. We have a group of Parkinson’s buddies who we link to the newly diagnosed, which has been very successful.”
David says his diagnosis has created opportunities in his personal and professional lives he’d never imagined.

Born in Bunbury and after spending time in Kambalda and the small Wheatbelt town of Pingaring, David’s family – his dad was a teacher – moved to Perth when he was about 11.
“There were about 40 kids in the Pingaring school. At the end of the day, all the farm kids got on the bus to go home and it was just my brother and me and there’s only so much cricket you can play with your brother.
“But I did have free rein of the school library, that encouraged a voracious appetite for reading, filling up on information and creating a sense of curiosity.
“That was probably part of the influence on going into medicine. I remember reading about the Wright Brothers and the inventor of the rocket, Robert Goddard.”
Young David was also an avid bone collector, roaming about looking for dead animals, often not getting home until after dark, just in time for dinner.
David’s Scottish granddad Jim worked on the mines in Kalgoorlie and died of lung disease. Seeing him needing oxygen, David remembers thinking “there should be more research done about this”.
“When I got to Perth I was reading a lot. Somewhere along the line I got interested in the brain and the mind and vividly remember reading Sigmund Freud’s book. The interpretation of dreams, I found absolutely fascinating.”
A scholarship to Wesley College exposed him to a whole raft of new people he might not have otherwise met. In high school a friend’s dad had a stroke and David remembers asking a lot of questions about him and his condition.
“I felt like I was learning a lot before I got to uni. There was an expectation that if you had the marks you would do law or medicine at UWA. Unlike today, the world didn’t seem much bigger than that, so in my era that’s what you did.”
David started at UWA in 1986. His undergraduate years were great, he sailed through them, found a whole new group of friends and played a lot of golf.


Our podcasts bring you the latest updates and key insights into new treatment options available.
Join our clinical editor Dr Joe Kosterich in conversation with WA specialists to learn more about developments to improve patient outcomes. Our podcasts are now CPD verified. Look for the CPD logo to complete your self-reflection and claim your time.
Learn more about:
Fertility investigations in general practice with Dr Johannah Scaffidi
Minimally invasive breast surgery with Dr Saud Hamza
Bridging the treatment gap in osteoarthritis with Dr Arash Taheri
Is it pelvic venous congestion? With Dr Marek Garbowski
Aortic stenosis: managing low-risk patients with Dr Gerald Yong
Listen on your favourite podcast platform – scan the QR code to follow us!
By his fourth year of medicine, David had already been exposed to a lot of different options but continued to carry a fascination for the brain and the mind. He initially thought that might lead him to psychiatry.
Time in general surgery saw him exposed to the early stages of laparoscopic surgery and some of the first laparoscopic gall bladder operations in the state – his job was to hold the camera. He moved into neurosurgery and that’s “when things got really interesting” for David.
“I was doing 100-120 hours a week, doing rounds with the registrars and being on the ward looking after some really sick patients. The other half of my time was in the theatre with surgeons, where I got to see a living, breathing brain.
“That was amazing. I did two rotations in neurosurgery.”
Since graduating in 1991, David’s almost four-decade career has included two years at the famed Mayo Clinic and helping lead a revolution in the care of acute stroke in hospital.
He has also been instrumental in shaping clinical care, education and advocacy in the neurological space – and now with Parkinson’s.
Known for his compassion, David has made lasting contributions to neurological care, including serving as former head of department of neurology at Sir Charles Gairdner Hospital.
He retired as Medical Director and clinic neurologist at the Perron Institute last year but has taken on the role of Research Advisor and maintains his Newly Diagnosed Parkinson’s Clinic, delivered in partnership with Parkinson’s WA at the Institute. He remains a Clinical Professor at UWA.
In 2023 David was made a Member of the Order of Australia (AM) in the King’s Birthday Honours for services to medicine and neurological research.
In August last year, Parkinson’s WA named David their first Honorary Medical Director, in recognition of his involvement with the group over many years and in supporting the development of their clinical, wellness and outreach programs, which help deliver person-centred care across the state.
For almost a decade he has been involved with Argenica Therapeutics, a company developing novel neuroprotective therapeutics to reduce brain damage after stroke and other devastating brain injuries.
Last year, David released a book called My Fight with Parkinson’s Putting his story down on paper and sharing it was inspired after re-reading actor and vocal Parkinson’s advocate Michael J. Fox’s No Time Like the Future.
It was the first time David had read the book as someone with Parkinson’s, not simply as a neurologist.
“Having to slow down because of Parkinson’s was also what inspired me to write the book. Since it has

come out, I have really enjoyed talking about it. There are 22 Parkinson’s support groups in WA, with 16 in Perth and I think I have visited about two thirds of them. I talk about the book and how to live well.
“I try to offer people guidance and that shared experience for people to know that other people are going through the same thing and it’s not just me.
“I’m also really interested in how diagnoses are framed. There’s a lot we can do differently, rather than focus on the negatives. You need to have hope, not a doctor with a careless phrase or two. That happens and it’s a big worry to me.
“People with Parkinson’s are twoand-a-half times more likely to be a suicide risk after diagnosis. Doctors have to be very mindful of how they talk to people.”
In May, David and Kirsten are heading to the World Parkinson Congress in Arizona. They are looking forward to seeing friends and colleagues they have made at previous events. It’s highly possible David will be out on the local greens too, enjoying some golf.
April is Parkinson’s Awareness Month and World Parkinson’s Day is April 11.
My Fight with Parkinson’s is available in bookstores. David will donate $5 to Parkinson’s WA for each copy sold through the charity’s website.

One year ago Western Australia’s gun laws were reformed requiring a greater input from GPs. How are the changes playing out?
By Aleisha Orr
One year ago WA’s gun laws were reformed to bring in a requirement for a health assessment to carry a firearm.
As of March 31, 2025 people seeking a firearms licence were required to undergo a health assessment with a GP, and existing licence holders to be assessed every five years in an effort to protect public safety.
The assessment is made up of two parts, a self-assessment completed by the applicant and a medical assessment completed by the GP. At the time, concerns were raised about the additional workload for GPs and the potential to disrupt the doctor-patient relationship.
Since WA’s legislation was passed even greater attention has been directed at gun laws across the country.
With other jurisdictions looking closer at their gun laws, the Australian College of Rural and Remote Medicine (ACRRM) has developed a position paper on the role of rural generalists in assessing suitability for having a firearms permit.
The College’s director Dr Alice Fitzgerald told Medical Forum that as more states and territories were looking at bringing in health assessments for firearms permits, there was a need for ACRRM to have a national response to ensure consistency.
Dr Fitzgerald, who works in a rural clinic in Kununurra, said there had been less assessments taking place in her clinic than she had expected.
“It has been noted that there are 40,000 licensed firearms owners requiring a firearms health assessment across the state,” she said.
“Speaking from my own experience working in a rural clinic, the number of assessments carried out has been lower than might have been expected given my rural location.”
Dr Fitzgerald said the assessments provided an important opportunity for a thorough clinical review — in some cases, one that may not have been undertaken for some time — and reinforced the role rural doctors play as an early point of contact for people who may need additional support.
“The assessments open the door to broader conversations about mental health, wellbeing and safety — and rural doctors are well placed to have those discussions because of the trust built over time,” she said. However, she said patient understanding of the process varied.
While GPs are not obliged to carry out the assessments, rural and remote clinics were already under significant workforce pressure and adding additional assessments only increased workloads, particularly in areas where support services were limited.
“This is one of the reasons ACRRM believes governments need to engage directly with rural doctors and communities before making changes that affect weapon licensing requirements,” Dr Fitzgerald said.
“Some clinicians are also seeking clearer guidance, appropriate training, and reassurance around medico-legal responsibilities and personal safety.”

Police does not receive medical information as part of the health assessment, only whether the applicant meets or does not meet the firearm authority requirements.

GPs are no stranger to patients Googling their symptoms, but AI brings a whole new challenge when it comes to health advice, writes Alex Jenkins.
Many GPs will be long used to patients arriving not only with a list of symptoms they’ve searched online, but also a firm belief they’ve already found the answer to their health concern.
What’s changed in recent years is the online ‘answer’ now arrives in a calm, polished paragraph that sounds like it was written by a clinician.
Patients are using AI tools and AI-enhanced search to selfdiagnose, interpret test results and weigh treatment options before they step into your clinic.
The opportunity – and challenge – for a general practitioner is to respond in a way that keeps the patient engaged, informed and safe.
In early January 2026, it was reported Google had removed some AI-generated health summaries from search results after concerns were raised about misleading information –including on the interpretation of liver function tests.
AI tools don’t ‘reason’ clinically: they generate plausible language based on patterns in data. This means they can be useful for explaining concepts but unreliable at interpreting an individual patient, especially when context is missing. This could include age, sex, comorbidities, medications, symptom duration, red flags and what exactly the patient means when they say they feel ‘dizzy’ or ‘tightness’.
Patients are increasingly coming in with symptoms, a diagnosis and even a proposed treatment plan drafted by a chatbot.
The problem isn’t just occasional factual errors – it’s that the output can be confident, tidy and persuasive, even when it’s incomplete or misapplied.
How to approach an ‘AI diagnosis’
If a patient mentions they used AI for their research, a curious, non-judgemental approach usually works better than trying to shut it down.
Two quick questions can save time and improve rapport:
“What exactly did you ask the AI — and what did you tell it about you?”
You’ll quickly see if the prompt was vague, missing key symptoms, or based on incorrect assumptions.
“What worries you most about what it said?”

This gets to the anxiety underneath and helps you address the real concern.
From there, you can reposition the AI output as a starting point, not a clinical verdict.
The under-discussed risk: patient data security
One of the biggest shifts is not just what patients ask AI, but what they upload into it.
People are increasingly entering highly sensitive information –sometimes complete medical histories or screenshots of results – into chatbots.
AI can be useful for patients when it’s used for general health education. For example, explaining medical terms in plain language or helping them draft questions to bring to their GP.
For people living in remote and rural Australia, AI tools can help people prepare for appointments and recognise when to seek care.
At its best, AI can be used to make the appointment more productive, rather than to compete with the GP’s advice.
However, AI is not a useful or appropriate tool for diagnosing, interpreting results in isolation or deciding on treatment.
At worst, it can also give patients false confidence to delay a review of potential red flags.
If a patient does this, here are some ways to explain the above, without running the risk of shaming the patient.
1. Validate
“I can see why you’d look this up – it’s stressful when you’re not sure what’s going on.”
2. Reframe
“AI can be great for explaining terms and helping you think of questions, but it can’t examine you or see your full history, so it’s not reliable for diagnosing or deciding treatment.”
3. Safety-net
“Let’s use what you found as a starting point; I’ll help you work out what fits your situation and what we need to rule out today.”

This is a growing privacy risk: patients may share private medical information with companies, including overseas providers, without understanding where the data might go, how it may be stored or what happens if there is a breach.
If a patient is determined to use AI to help explain a report, you should encourage de-identification such as removing their name, date of birth and address, and remind them the safest place to
review personal results is still in a clinical setting where privacy protections are in place.
The future: Safer AI will sit closer to the clinic
The safest future model is not patients alone with a chatbot, but clinician-governed tools sitting within trusted systems where advice is constrained and sources are clearer.
This patient-facing AI could be linked to a clinical setting,
so the doctor can review what the tool is advising patients.
There is no doubt patients will keep using Dr Google, so the goal for GPs is to discourage them away from that behaviour without shaming them in the process.
If doctors stay curious, remain informed, correct misinformation kindly and set clear boundaries around self-diagnosis and privacy, AI can become a tool that improves health literacy rather than undermines it.
ED: Alex Jenkins is the Director of WA Data Science and Innovation Hub, member of the WA Health AI Oversight Committee and sits on the Western Australian State Government AI Advisory Board.
1543343
0.5 0.5 hours

As International Women’s Day was celebrated, RACGP Vice President and WA Chair Ramya Raman reflects on the role of GPs in tackling a pervasive women’s health issue.
As International Women’s Day was celebrated last month, we’re reminded that it’s an important moment to recognise, yet it’s also a moment to reflect on persistent challenges affecting women’s safety and wellbeing.
Among the most pressing is family and domestic violence (FDV), including intimate partner violence (IPV) an issue that presents frequently, though often quietly, in general practice.
For many victim-survivors, their GP may be the first professional they disclose violence to. This makes primary care a critical setting for identification, early intervention and support.
Spotting the signs
Peta, a 56-year-old mother of five, attends for recurrent headaches and insomnia. Over the past year she has presented several times with anxiety and abdominal pain.
Her partner accompanies her to most appointments. This happens for over a year until she comes on her own for an appointment. She breaks down in the consult – tells me that she is trapped in a relationship that is suffocating. Her finances are blocked; she is being monitored and made to feel like she is a burden to her family and to the world.
Take a minute and reflect on this, how would you respond? What would you do? How do you manage this consultation?
Unfortunately, this is not an uncommon occurrence in our communities and in a general practice consultation.
Family and domestic violence remains a major public health issue. According to the Australian Institute of Health and Welfare (AIHW):
• 1 in 4 women (23%) have experienced physical or sexual violence by an intimate partner since the age of 15
• Around 1 in 14 men (7%) have experienced similar violence
• Emotional abuse from a partner affects 23% of women and 14% of men.
Domestic violence is also associated with severe outcomes. On average in Australia one woman is killed by an intimate partner every eight days, highlighting the ongoing lethality of abusive relationships.
Beyond immediate injury, exposure to violence has profound health consequences. FDV is associated with depression, post-traumatic stress disorder, chronic pain, substance misuse and reproductive health complications.
Importantly, violence against women contributes more death,
When a patient discloses violence, the GP response can significantly influence whether they seek further help.
Listen and validate
Acknowledge the patient’s experience. Simple statements such as “I’m glad you told me” or “This is not your fault” can be powerful.
Assess immediate safety
If there is risk of imminent harm, urgent safety planning or emergency support may be required.
Document carefully
Clinical documentation should include:
• the patient’s description of events
• observed injuries
• behavioural observations

disability and illness for women aged 25-44 than any other preventable risk factor in Australia.
Research suggests more than one in five women who disclose domestic violence tell their GP first. This places general practitioners at the frontline of identification and support.
The clinical signs
Patients experiencing IPV may not present with an explicit disclosure of violence. Instead, clinicians should be alert to possible indicators such as:
• anxiety, depression or PTSD
• chronic pain or medically unexplained symptoms
• repeated injuries or delayed presentations
• sleep disturbance
• substance misuse
These records may later become important medico-legal evidence.
Provide referral pathways
Patients should be offered information about support services such as 1800RESPECT — Australia’s 24-hour national domestic, family and sexual violence counselling service.
Local crisis services, social workers and specialist FDV organisations should also be part of a GP’s referral network.
Provide ongoing care
Many patients are not ready to leave a violent relationship immediately. Maintaining ongoing GP care provides continuity, support and monitoring.
• reproductive health issues
• controlling partner behaviour during consultations
Recognising these patterns can prompt sensitive enquiry. Routine universal screening remains debated internationally, but many guidelines support casefinding; asking about safety when clinical indicators are present.
Validated screening tools can support these conversations, including:
HITS (Hurt, Insult, Threaten, Scream)
A short four-question tool asking how often a partner:
• physically hurts you
• insults or talks down to you
• threatens you with harm
• screams or curses at you
WAST (Woman Abuse Screening Tool)
A brief questionnaire assessing tension and conflict within relationships.
Partner Violence Screen (PVS)
Three questions focusing on safety and physical violence.
These tools are simple and practical to use in primary care settings. Importantly, screening should occur in private, without partners present.
Disclosure initiatives
One barrier to identifying domestic violence is that patients often struggle to disclose abuse directly. Programs designed to facilitate disclosure sometimes referred to as ‘safe to tell’ initiatives encourage victim-survivors to speak up in safe environments, including healthcare settings.
These programs aim to reduce stigma associated with disclosure, encourage earlier help-seeking, and ensure professionals respond appropriately.
GP education initiatives such as the Safer Families Toolkit provide practical guidance on identifying and responding to domestic violence in clinical practice.
Engaging men in prevention
While women are disproportionately affected by severe intimate partner violence, preventing violence requires engaging men as part of the solution.
Most men do not perpetrate violence, but they play a critical role in shaping social norms around gender equality and respectful relationships.
Healthcare professionals can contribute by promoting healthy relationships, supporting men’s mental health, addressing substance misuse and behavioural risk factors.
The question that may change a patient’s life is often simple: “Are you safe at home?”
For some patients, that question opens the door to safety, support and the first step toward a life free from violence.
0.5 0.5




WA is not unique in struggling to attract doctors to rural areas, but it is unique in its size and distance between towns.
Back in 2000 the federal government committed $500 million to “improve regional health and increase GP numbers in the bush” as part of its Rural Health Strategy.
It was a key health policy, aiming to double the number of doctors working in regional areas over four years.
So how is WA doing in 2026?
A survey by the West Australian Local Government Association showed that 41 shires had together spent $9.5m to obtain and support GP services.
Health is not a local government responsibility and any money spent on attracting a GP is money not spent on core council responsibilities – think roads and local infrastructure.
WA is not unique in struggling to attract doctors to rural areas, but it is unique in its size and distance between towns.
One Nation MP Barnaby Joyce has floated the idea of forcing GPs to work remotely before being granted a Medicare provider number. This is a twist on the moratoriums faced by international medical graduates and won’t work.
Back in the day teachers and police had to start their careers in the bush before being “promoted” back to the city. Could a twist on this work?
A quarter of the way into the 21st century we are not advanced from its start. All ideas are welcome.





By A/Prof Davinder Hans, Psychiatrist, Nedlands
Antidepressants remain among the most commonly prescribed medications.
While long-term use often occurs in the context of complex mental health issues and physical and social comorbidities, there is considerable potential for structured re-evaluation and timely discontinuation when medications are no longer needed.
This is because, for some patients, continuing medication may provide no clear, evidence-based benefit.
Discontinuing antidepressants is complex and requires careful, collaborative discussions between clinicians and patients. These are more likely if clinicians proactively discuss deprescribing.
While some need ongoing therapy, studies show up to 50% of long-term prescriptions over five years lack current indication, and clinicians might consider supervised cessation. About one-third of those on antidepressants for over two years lack a clear reason to continue.
Prolonged and unnecessary treatment is not harmless. Continued exposure increases the risk of cumulative adverse effects, such as emotional blunting, weight gain, and sexual side effects. While these effects may be overlooked during routine reviews, they can affect patients’ quality of life and long-term adherence.
When to deprescribe
A key aspect of deprescribing is recognising the reality of antidepressant withdrawal. Withdrawal symptoms are common and clinically significant.
Over half of people trying to stop antidepressants experience withdrawal effects. It is not unusual for withdrawal to persist for several weeks or months; about 40% of individuals report symptoms lasting at least six weeks, and 15% say effects continue for 12 weeks or more.


The clinical presentation of withdrawal is broad. Typical reactions include increased anxiety, flu-like symptoms, insomnia, nausea, sensory disturbances and hyperarousal.
Patients may report dizziness, electric shock-like sensations or “brain zaps”, diarrhoea, headaches, muscle spasms, tremors, agitation, confusion, malaise, sweating and irritability. Given this range, anticipatory guidance and careful monitoring are essential when planning dose reductions.
Withdrawal or relapse?
An important implication of the higher incidence and longer duration of withdrawal than historically acknowledged is the risk of misdiagnosis. Withdrawal may be mistaken for relapse or treatment failure, prompting antidepressant reinstatement or dose escalation.
A commonly cited distinction is that withdrawal begins within days of cessation and resolves quickly if the medication is restarted, whereas relapse tends to emerge later.
However, this distinction is unreliable in antidepressants with longer half-lives. Fluoxetine, for example, may produce delayed withdrawal symptoms weeks after cessation, confounding the above assumption about temporal proximity.
Withdrawal may also be a misinterpretation of covert non-adherence or perceived as an emerging bipolar disorder when agitation is interpreted as hypomania.
It might also be incorrectly seen as a side effect of a newly prescribed antidepressant during the switching process. These misinterpretations can only be clarified with meticulous, patient-centred reviews and discussions about medication.
Understanding relative withdrawal risk is therefore central to safe deprescribing. Antidepressants associated with the highest potential risk of withdrawal include desvenlafaxine, paroxetine, duloxetine, mirtazapine, and venlafaxine.
Key messages
• Routinely reviewing long-term antidepressant use is part of good prescribing practice
• Recognise that antidepressant withdrawal is common, can be prolonged, and may be misdiagnosed as relapse or treatment failure
• Deprescribing requires shared decision-making and individualised tapering strategies tailored to the specific medication and the patient’s response.
Those with medium potential risk include amitriptyline, clomipramine, escitalopram, citalopram, sertraline and fluoxetine. In general, agents with shorter half-lives are associated with greater withdrawal risk, although individual patient variability remains considerable.
In antidepressant deprescribing, a tapering strategy is essential. Proportional tapering, which involves decreasing the dose by a
percentage of the current amount, is commonly used. For example, reducing 20mg by 25% results in a 5mg decrease to 15mg.
Hyperbolic tapering refines this approach by slowing reductions even further as doses fall, particularly once approximately half the original dose has been reached.
In higher discontinuation risk antidepressants, and/or for patients who may be sensitive to withdrawal effects, the final 50% of the dose reduction may need to be made with particularly slow steps, sometimes requiring compounded or liquid formulations to allow for very small adjustments.
Evidence suggests that underestimation of withdrawal incidence, severity and duration may partly explain longerterm antidepressant use. When withdrawal is misdiagnosed as relapse, treatment resistance or emergent bipolarity, medication is often reinstated or intensified, reinforcing long-term use.
Deprescribing antidepressants, therefore, requires more than a reduction schedule. It requires
reassessment of ongoing indications, shared decisionmaking, education on withdrawal, and tapering strategies tailored to pharmacokinetics and patient experience.
In patient-centred care, routine review of long-term antidepressant use should be standard practice. Raising the possibility of discontinuation, when clinically appropriate, may reduce unnecessary medication exposure while maintaining patient safety and therapeutic alliance.

Join us for our annual GP Urology Masterclassan in person conference offering interactive learning and RACGP CPD accredited activities.
Proudly delivered by PUC specialist urologists and guest speakers, designed specifically for general practitioners. This masterclass continues our commitment to giving back to GPs through gold-standard, practical education focused on what you need to know in everyday clinical practice.
Places are limited so book now to avoid disappointment. events@perthurologyclinic.com.au
This comprehensive program will cover all major aspects of urological care, providing up-to-date insights, clear clinical guidance, and practical take-home messages relevant to primary care.
By Professor Blossom Stephan, Chair of Dementia for Dementia Australia
Dementia is now the leading cause of death in Australia. It is not a normal part of ageing, there is currently no cure, and it has profound impacts on the individual, those closest to them, their healthcare providers and communities.
There are an estimated 446,500 Australians currently living with dementia, including more than 43,400 people in WA. Without action, these numbers are projected to more than double by 2065.
There is an urgent need for a preventative-focused approach that enables earlier intervention and reduces the incidence of new cases.
GPs are uniquely placed to engage their patients in conversations about brain health and to lead dementia risk reduction and prevention efforts.
As the primary entry point to the healthcare system, they are central to early risk identification and to translating evidencebased strategies into personalised prevention practices.
Although age, sex and genetic susceptibility are non-modifiable determinants of dementia risk, evidence suggests that a substantial proportion of dementia cases in later life may be prevented or delayed through the effective management of modifiable risk factors.
A 2024 Lancet Commission on the prevention, treatment and care of dementia identified 14 modifiable risk factors from early life through to older age, that together account for approximately 45% of dementia cases globally.
These factors include less education in early life, hearing loss, high LDL cholesterol, depression, traumatic brain injury, low physical activity, diabetes, smoking, high blood pressure, obesity, excessive alcohol use in


midlife, air pollution, vision loss and social isolation in later life
Despite the growing evidence base on modifiable risk factors, and the substantial populationlevel impact that reducing prevalence could achieve, prevention is rarely discussed by GPs and their patients.
Further, global evidence indicates that public understanding of dementia and its preventability remains limited, with many people continuing to view dementia as an inevitable consequence of ageing, rather than as a preventable condition.
It is important to recognise that dementia is complex. People who develop dementia have not simply caused it through modifiable risk factors.
However, increasing awareness of the things people may be able to influence, and supporting individuals to address them, can meaningfully reduce populationlevel risk and contribute to improved brain health across a patient’s lifespan.
Dementia prevention should begin as early as possible, but early mid-life represents a critical window linked to a range of cardio-metabolic and psychosocial changes that can influence later life brain health.
For eligible patients, the 45-49year health assessment provides a structured opportunity to assess brain health, identify modifiable risk factors, and initiate risk reduction discussions and risk management planning.
Routine assessments of heart health, mood, vision and hearing also provide opportunities to assess risk, reinforce prevention messages and support the implementation of strategies that promote brain health.
Preventative actions that reduce dementia risk align closely with well-established principles and policies that support overall chronic disease prevention.
1. Physical activity
Living a sedentary lifestyle increases dementia risk. Regular physical activity such as aerobic exercise (e.g., walking, swimming) and strengthbased training can lead to improved general health, including brain health.
2. Healthy behaviours
Dietary patterns such as the Mediterranean diet, the MIND (Mediterranean and DASH [Dietary Approach to Stop Hypertension] Intervention for Neurodegenerative Delay) diet or traditional dietary patterns, such as the Japanese or Nordic diets, are associated with improved brain health and reduced dementia risk.
Emphasising a high intake of vegetables, fruit, wholegrains, legumes, fish and healthy fats, for example olive oil, along with reduced salt intake support both cardiovascular and cognitive health.
Dementia stats at a glance
The number of deaths caused by dementia has risen by 39% over the past decade.
Limited alcohol intake and quitting smoking may also reduce dementia risk.
3. Hearing care
Regular hearing testing, avoiding loud noise, wearing hearing protection and ensuring aids are used when needed can play an important role in reducing risk.
4. Head injury prevention
Helmet use, fall-prevention strategies and safe participation in sports can help protect the brain across all ages.
5. Social and cognitive engagement
Maintaining meaningful social connection, volunteering, joining community activities and learning new skills can build reserve, supporting cognitive health and wellbeing as we age.
9.4% 68.2% 62.4% 39%
More than two-thirds (68.2%) of deaths were people aged over 75 years, compared to 66.1% some 10 years ago.
GPs may find free online risk assessment tools, such as CogDRisk, useful for supporting discussions about personalised risk profiles and identifying areas where targeted risk reduction and prevention may be beneficial.
Free online courses, such as the Preventing Dementia Massive Open Online Course (MOOC), taught by the Wicking Dementia Centre, provide clear evidence-based guidance on modifiable risk factors and preventative strategies.
BrainTrack, a free app developed by Dementia Australia, can help individuals monitor and understand changes in their cognition over time and may also support conversations about brain health with their GP.
Latest data show dementia accounted for 9.4% of total deaths in Australia.
62.4% of people who died from dementia in 2024 were women.
GPs play a central role in communicating prevention information. It is, however, important to recognise that social determinants (e.g. education, income, environment and access to services) significantly influence an individual’s ability to make and sustain behavioural changes.
By reducing stigma and raising awareness of modifiable risk factors, GPs can support patients in developing personalised risk reduction plans.
ED: Professor Blossom Stephan is also the Director of the Dementia Centre of Excellence, Curtin University.
For more information or to access resources to support patient discussions, contact Dementia Australia through the National Dementia Helpline on 1800 100 500 or visit dementia.org.au.
Resources
www.cogdrisk.neura.edu.au www.mooc.utas.edu.au/course/20282/ Preventing_Dementia__2026 www.dementia.org.au/braintrack
Saturday 9th May, Pan Pacific Perth



The Niggling Shoulder
Dr Taro Okamoto Coastal Orthopaedics

From Door to Disposition: Patient Pathways in the Emergency Department
Dr Tracy Bhar Fiona Stanley Hospital

Sorting the Serious from the Simple: Acute Red Eye for GPs
Dr Xia Ni South Street Ophthalmology
From Claudication to Critical Limb Ischaemia: What Every GP Must Know
Dr Stefan Ponosh Ponosh Vascular
Latest in Lipids: Updates and Optimising Lipids in Primary Care
Dr Stephen Gordon Western Cardiology

Beyond Sugar: Navigating the Cardiometabolic Overlap in General Practice
Dr Michael Hancock Living Diabetes & Endocrinology
Join us for a day of clinical education designed by your colleagues. Up to 22 hours of CPD if you complete all the activities.
6.5 6.5 9


The Modern Menopause Consult: Evidence-Based Management for GPs
Dr Lauren Neppe Fertility North

Vaccinations in older adults
Clinical Prof Michaela Lucas
Sir Charles Gardiner Hospital


Decoding the Murmur: A Practical Guide for GPs
Dr Gerald Yong iSave Heart Clinic
Claims and complaints insights for General Practitioners Nicola Kent and Tessa Flynn Avant Law
For Regional attendees or those who wish to take advantage of a city stay, the Pan Pacific is offering a discounted rate. Please email alice@mforum.com.au for booking link.

Complimentary CPD event. Places are limited. Scan the QR code to register today.

fellowship training in Hip and Knee Reconstruction at the Nuffield Orthopaedic Centre, University of Oxford in the UK, followed by further fellowship training at the Perth Orthopaedic Sports Medicine Centre in 2011.
In 2013, I was selected for the prestigious John N. Insall Travelling Fellowship, involving visits to leading knee surgery centres across North America. I practised as an orthopaedic surgeon in Victoria, British Columbia for 15 years, with a focus on arthroplasty and trauma, while also holding an academic appointment as a Clinical Assistant Professor with the University of British Columbia.
I hold public appointments at Rockingham and Peel Hospitals and am fully accredited by the Royal Australasian College of Surgeons.
My private practice is based at St John of God Murdoch Hospital as part of Murdoch Orthopaedic Clinic.
What services do you offer?
My practice focuses on hip and knee replacement surgery, including primary, complex, and revision procedures, as well as knee arthroscopy.
I provide comprehensive care from initial consultation and surgical planning through to post-operative rehabilitation and long-term follow-up, with an emphasis on achieving safe and durable outcomes.

A central component of my practice is careful patient selection and pre-operative optimisation, ensuring patients are appropriately prepared for surgery by addressing medical comorbidities, functional status, and individual risk factors. This approach is particularly important in more complex cases, where thoughtful planning can significantly influence outcomes.
How has your experience influenced your practice?
My work with the Canadian Alpine Ski Team, involvement in medical coverage for the Vancouver 2010 Winter Olympic Games, and time spent working with the Whistler Blackcomb Ski Patrol exposed me to a wide range of acute orthopaedic presentations and multidisciplinary team environments.
These roles required efficient assessment, clear communication, and an emphasis on patient safety in settings where conditions were often unpredictable.
This experience has reinforced the importance of preparation, planning, and teamwork in both orthopaedic trauma care and elective joint replacement surgery.
While the clinical context is different, the principles of anticipating risk, coordinating care, and making considered decisions translate directly across these settings.

What do you see as the future of hip and knee surgery?
I see the future of hip and knee surgery as increasingly focused on optimising the entire patient pathway, including patient selection, pre-operative optimisation, and enhanced recovery pathways, rather than the operation alone.
While advances in surgical technique and implant design continue, outcomes are increasingly influenced by coordinated peri-operative care and thoughtful planning.
Technology such as computer-assisted planning and robotic-assisted surgery will continue to play a role in improving accuracy and consistency when used appropriately.
By Bella Fedele, Dietician
The Better Health Coaching Service is a free, WA Department of Health commissioned telephone-based health coaching service designed to support adults in WA to prevent or better manage chronic health conditions through guided sustainable lifestyle change.
The service complements primary care by providing personalised, evidence-based health coaching that addresses behavioural risk factors commonly associated with chronic disease.
The service is available statewide and is intended to reduce barriers to care for patients who may benefit from additional support beyond brief GP consultations.
The service supports adults to improve health behaviours linked to chronic disease prevention and management, including:
• Healthier food choices and nutrition habits
• Increasing physical activity
• Stress management and mental wellbeing
• Improving sleep quality
• Reducing alcohol consumption
• Smoking cessation
• Building social connection and routine
• Self-management of chronic conditions such as diabetes, cardiovascular disease, cancer and related comorbidities.
Participants receive up to 10 individual health coaching sessions, each approximately 30 minutes, delivered via telephone to use within a 6-month period.
Appointments are scheduled on patient preference or clinical need.
Coaching is provided by tertiaryqualified health professionals with backgrounds in dietetics, exercise physiology and health psychology, and trained in behaviour change, motivational interviewing, and chronic disease prevention.
Who is suitable?
The service is appropriate for adults who:
• Are 18 years or older living in WA
• Are seeking support to prevent or manage chronic disease
• Would benefit from structured lifestyle behaviour change support
• May face barriers to in-person programs (e.g. time, transport, rural location, mobility, confidence or language).
Patients do not require a formal diagnosis to participate. The service is suitable for individuals who are at risk of developing chronic disease, newly diagnosed and needing lifestyle support, or living with established chronic conditions.
Where English is a second language free interpreting services are available.
This service is particularly beneficial for patients who require regular accountability, goal setting, and problem-solving support.
What patients can expect
Patients enrolled can expect a person-centred, collaborative approach focused on achievable and meaningful change.
Key components include:
• Individualised goal setting aligned with patient priorities and readiness to change
• Problem-solving strategies to address barriers such as time constraints, motivation, stress or confidence
• Support to build sustainable habits, rather than shortterm behaviour change
• Access to practical resources, including factsheets, tools and healthy recipes
• Ongoing encouragement, reflection and accountability over the 6-month period.

Health coaches work alongside patients to identify realistic actions that fit within their daily lives, reinforcing autonomy and self-efficacy.
The service is designed to complement, not replace, existing primary care. With patient consent, regular progress updates are shared with referring GPs, including information on patient engagement, goals and progress over time.
This supports continuity of care and enables GPs to reinforce lifestyle changes during routine consultations, aligning coaching support with broader chronic disease management and preventive care plans.
Referrals to the service can be made by GPs, practice nurses, allied health professionals, Aboriginal health practitioners and community health workers.
Referral options are online or self-registration at www. betterhealthcoaching.com.au/wa or by phone on 1300 822 953.
Patients can also self-refer at no cost. Patients do not require a Medicare card to access the service.
Author competing interests – the author works for Better Health Company, which delivers the Better Health Coaching Service.
ED: Bella Fedele is Head of Service Design at Better Health Company.
0.5

By Dr Sheldon Moniz, Orthopaedic Surgeon, Murdoch
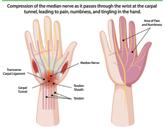
Upper limb compressive neuropathies are a frequent cause of pain, paraesthesia and weakness. Although carpal tunnel syndrome is the most recognised condition, a spectrum of central, proximal, and distal nerve compressions can present with overlapping clinical features.
Accurate localisation is critical, as delayed recognition – particularly in the presence of motor involvement – can result in permanent deficit.
Carpal tunnel syndrome
Carpal tunnel syndrome is the most common compressive neuropathy. Patients typically report nocturnal numbness or tingling affecting the thumb, index, middle and radial half of the ring finger.
Symptoms often wake patients at night and may improve with shaking the hand.
Functional complaints include dropping objects, reduced grip strength and fine motor difficulty. In advanced cases, numbness becomes constant and thenar weakness or wasting may develop.
Phalen’s and Tinel’s signs are supportive but not diagnostic alone. Risk factors include diabetes, pregnancy, inflammatory arthritis and repetitive wrist loading.

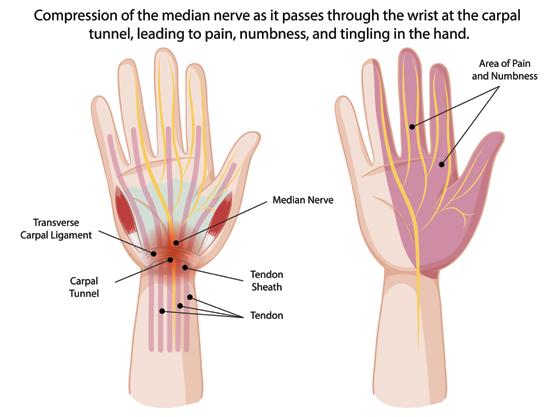
Initial management involves night splinting and corticosteroid injection. Nerve conduction studies are useful when symptoms are atypical. Persistent symptoms beyond 6-12 weeks, progressive sensory loss or any motor involvement warrant surgical assessment.
Cubital tunnel syndrome is the second most common neuropathy and is often under-recognised. Patients describe numbness
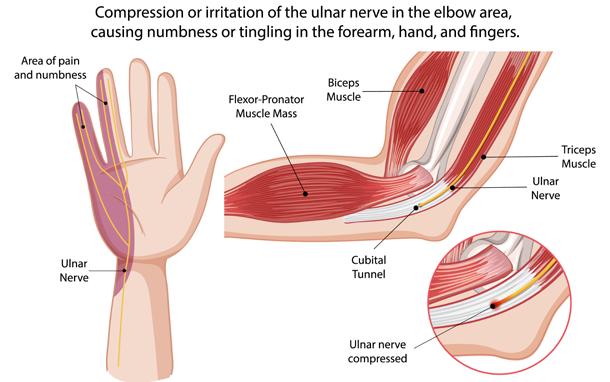
or tingling in the ring and little fingers, frequently exacerbated by prolonged elbow flexion (e.g. phone use or sleeping with elbows bent).
As compression progresses, hand clumsiness, intrinsic weakness and reduced grip strength may develop.
Examination may reveal reduced sensation in the ulnar distribution, positive Tinel’s at the elbow and weakness of interossei. Froment’s sign may indicate adductor pollicis weakness. Advanced cases show intrinsic wasting or early clawing.
Motor involvement should prompt early referral, as prolonged compression risks irreversible intrinsic muscle loss.
Ulnar nerve compression at the wrist is less common and often related to ganglia, hook of hamate fractures or repetitive trauma such as cycling.
A distinguishing feature from cubital tunnel syndrome is sparing of dorsal ulnar hand sensation. Depending on the level of compression, symptoms may be sensory, motor or mixed.
Persistent symptoms or suspicion of a space-occupying lesion warrant imaging and referral.
Radial tunnel syndrome is an uncommon cause of lateral forearm pain and is frequently confused with lateral epicondylitis.
Patients report deep, aching pain distal to the lateral epicondyle, exacerbated by resisted supination or middle finger extension. Objective motor weakness and sensory loss are typically absent.
Diagnosis is clinical and often one of exclusion. Referral is appropriate when symptoms persist despite conservative treatment.
Proximal median nerve compression beneath the lacertus fibrosus is increasingly recognised but frequently overlooked.
Patients may report forearm fatigue, reduced grip endurance or pinch weakness without classic symptoms. Nerve conduction studies are often normal.
Examination may demonstrate weakness of flexor pollicis longus or flexor digitorum profundus to the index finger, with tenderness over the proximal forearm.

This condition should be considered in patients with persistent median symptoms despite carpal tunnel treatment or inconclusive investigations. Central causes: cervical radiculopathy and myelopathy
Peripheral neuropathy must be distinguished from cervical pathology. Dermatomal patterns, associated neck pain, bilateral symptoms or upper motor neuron signs raise suspicion of cervical radiculopathy, brachial neuritis or myelopathy.
Red flags include gait disturbance, hyperreflexia and progressive weakness. These findings require urgent spinal referral.
A structured assessment improves localisation:
• Determine distribution; median, ulnar or dermatomal
• Identify provoking factors; wrist flexion (CTS), elbow flexion (cubital tunnel), gripping fatigue (lacertus)
• Assess motor involvement; EPB wasting (median), intrinsic muscle wasting (ulnar)
• Screen for red flags; bilateral symptoms or upper motor neuron signs suggest central pathology
• Refer appropriately; persistent symptoms beyond six weeks, motor deficit or diagnostic uncertainty justify specialist review.
Upper limb compressive neuropathies are highly treatable when accurately diagnosed. A systematic clinical approach enables timely intervention and optimises patient outcomes.

CTEC’s Cutting Edge workshops cover a comprehensive range of medical and surgical skills for the General Practitioner and Rural Generalist. Learn from expert faculty in our large-scale surgical training lab at The University of Western Australia.
The Cutting Edge: Managing Skin and Soft Tissue Injuries Workshop
Convenor: Dr Olga Ward
Co-Convenor: Dr Denis Carragher
Faculty: Ms Tania Girschik, Dr Dhruva Ramachandran, Dr John Rosser-Davies
Date: Friday 12 June, 8.00am
Where: CTEC, The University of Western Australia Entrance No. 2 Hackett Drive, Crawley

Scan to read more about the workshop and register
The Cutting Edge: Introductory Wound Suturing Workshop
Convenor: Dr Nikki Damen
Co-Convenor: Dr Denis Carragher
Faculty: Dr Simon Kusel, Dr Yvonne Pinto, Dr Dhruva Ramachandran
Date: Thursday 18 June, 8.00am
Where: CTEC, The University of Western Australia Entrance No. 2 Hackett Drive, Crawley

Scan to read more about the workshop and register
The Cutting Edge: Proceduralist Obstetrics and Gynaecological Skills Workshop
Convenor: Dr Olga Ward
Faculty: Dr Su Hamid, Dr John Rosser-Davies
Date: Thursday 15 October & Friday 16 October, 7.45am
Where: CTEC, The University of Western Australia Entrance No. 2 Hackett Drive, Crawley

Scan to read more about the workshop and register
By A/Prof Kaushalendra Rathore, Cardiothoracic Surgeon, Nedlands
Post cardiac surgery readmissions are a significant issue, typically ranging from 10-15%.
Various studies and national data suggest a substantial number of readmissions occurred at a hospital different to the operating hospital and non-referring GP clinics.
This eventually leads to a notable rise in morbidity and mortality risk after cardiac surgery.
Coronary artery bypass grafting (CABG)
Fortunately, country-wide decline in acute coronary syndrome (ACS) cases has been reported over the last two decades, and mortality rates have improved by refining diagnostic and therapeutic pathways.
Further, stratification by the types of ACS presentations show that the proportion of non-STsegment elevation myocardial infarction (NSTEMI) patients increased, whereas the number of ST-segment elevation myocardial infarction (STEMI) patients proportionally decreased over time.
Nearly two thirds of these cases with ACS undergo coronary angiogram and out of this 5060% require emergency stenting. Often these patients present with multiple co-morbidities.
All these changes in coronary artery disease management are leaving high-risk, complex, diffusely diseased patients with previous percutaneous coronary intervention (PCI) on dual antiplatelet therapy, chronic atrial fibrillation (AF) on anticoagulation, combined valve surgery and elderly patient for CABG surgery, which in turn increases incidence of post-operative complications including readmissions.
Surprisingly, even with a worsening patient cohort, contemporary mortality rates following CABG surgery are reducing.


In a recent NSW study, the most frequently reported underlying causes of 30-day readmissions were infection and sepsis, cardiac arrythmia, congestive heart failure, respiratory complications and pleural effusion. Among preoperative characteristics, older adults, females, weight loss, preoperative immunosuppression, atrial fibrillation (AF), NYHA Class III or more, high serum creatinine, anticoagulant use or dialysis, and comorbidities were found to be statistically significant.
A recently published Australian series reported outcomes in 80,883 patients of surgical aortic valve replacement (AVR). As the population is ageing, the proportion of mechanical AVR implantation is reducing (39% to 9%).
Highest readmissions rates happen in the first 60 days after surgery. The most common cardiovascular cause of readmission was arrhythmia, followed by heart failure and valve-related dysfunction (residual regurgitation/ stenosis, endocarditis, thrombosis, and mechanical complications).
There was a similar percentage of surgical valve procedure–related readmissions (wound pain of noncardiac origin, respiratory tract infection, and pleural effusion). Patients with a higher comorbidity profile and urgent surgery were more likely to have an unplanned readmission. Often heart valve cases are discharged with fluid overload, infections in the early stages, mild pleural and pericardial effusions, and arrhythmias like AF. They can present to the GP with worsening of symptoms and may require readmission.
• Readmissions after cardiothoracic surgery increases morbidity and treatment cost
• Often these patients will present to primary care with post-op complications
• Be alert for infections, fluid overload and arrythmias and refer back promptly when needed.
The volume of surgical AVR procedures has increased after the introduction of trans aortic valve implantation (TAVI). The main reasons are the ageing population with increasing degenerative aortic valve disease, a previous underuse of surgical AVR because of late referrals – 30 to 40% of aortic valve patients do not undergo a valve procedure – and the availability of a TAVI program might increase referrals.
TAVI procedures are refining and indications are expanding with a 52% annual increase in numbers from 2014.
Although TAVI is less invasive compared to SAVR, the rate of rehospitalisation for heart failure/ valve-related causes was similar between both. About 30% of all 90-day readmissions following TAVI were due to cardiovascular conditions, with congestive heart failure being the most frequent principal diagnosis.
Mitral regurgitation (MR) accounts for most mitral pathology in Australia. The prevalence of primary MR (intrinsic valvular disease, infection) has increased by 70% over the past two decades, with secondary MR (left ventricular dysfunction, ischemic MR) also increasing.
Mitral stenosis, predominantly caused by rheumatic disease, has a much lower prevalence in Australia.
Mital valve repair is the procedure of choice for symptomatic MV dysfunction due to superior long-term survival outcomes and lower risks of infection and stroke compared with MV replacement (bioprosthetic and mechanical MV replacement).
Bioprosthetic MV repair is increasing, while use of a mechanical valve is reducing. MV repair remains underutilised due to the low volume of cases referred per surgeon in Australia.
Use of bioprosthetic valves has significantly reduced early readmissions but risk of developing heart failure, pericardial or pleural collection, sepsis and arrythmia are also reasons for representations after mitral valve surgery.
Often these patients present to non-index periphery hospitals and GPs, impacting continuity of care and delaying management. These cases should be managed as team and when required an early primary specialist such as a cardiologist, cardiac surgeon, infectious disease physician and rehabilitation team must be involved.
By Dr Frances Theunissen and Dr Dev Nathani, Perron Institute
The rapidly evolving field of precision medicine and how it is reshaping the understanding and treatment of motor neurone disease (MND) was explored in a recent review led by WA researchers in collaboration with Kings College London.
Amyotrophic lateral sclerosis (ALS), the most common form of MND, is a life-limiting neurodegenerative disease, with the median survival being 2-4 years from disease onset.
Current available treatment options are limited with just two medications in Australia approved by the Therapeutics Goods Administration (TGA) and listed on the Pharmaceutical Benefits Scheme (PBS): Riluzole and Edaravone.
Both medications are associated with a modest benefit in terms of disease modification, hence the crucial need for higher efficacy treatments.
ALS is a heterogeneous disorder with patients exhibiting variable clinical features (i.e. site of onset, age at onset, cognitive and behavioural changes) and survival duration.
This phenotypic heterogeneity is underpinned by the interplay between the complex underlying genetic architecture consisting of rare pathogenic variants, structural variants, changes in the non-coding genome, epigenetics, and the contribution of environmental/lifestyle factors.
Conventionally, 10–15% of ALS cases are considered ‘familial’ with Mendelian inheritance, which is often complicated by incomplete penetrance (not every person with the genotype developing the disease), while the remaining 85% of cases are considered ‘sporadic’ (no prior family history).
Although these classifications are still commonly used, with the emergence of gene targeted treatment for ALS (Tofersen for


SOD1-ALS; under TGA review and not on PBS), we anticipate that genetic testing will become a standard practice for all ALS patients and knowledge of genetic variant status will increasingly influence treatment decisions.
the genes say
Over 50 genes have now been associated with ALS, with variants in C9orf72, SOD1, FUS and TARDBP being most common, while other disease-causing variants are relatively uncommon, each representing <1% of cases. For most apparent ‘sporadic’ cases, a clear genetic basis has not yet been identified.
Genetic testing practices differ between countries, with no formal consensus among specialists. While many clinics offer genetic testing, this was historically reserved for patients <40 years and/or a clear family history of ALS/FTD.
However, studies of comprehensive genetic testing in patients with sporadic ALS have identified potentially relevant variants in up to 17% of cases.
Importantly, in one study, genotyping of ALS patients
(both familial and sporadic) demonstrated that 21% of patients harboured a pathogenic variant, with 15% meeting the inclusion criteria for ALS gene therapies in clinical trial at the time.
With the emergence and increased accuracy of longread sequencing technology, it is now evident that all ALS patients should be offered whole-genome sequencing and that the current gaps in our understanding will continue to be filled as the genomes of ALS patients from varying ethnicities are sequenced and studied.
ALS genetic architecture differs between ethnic populations and global efforts to establish improved, and populationspecific reference genomes will assist in the understanding of genetic drivers of disease in each specific patient group.
This will not only enable a better understanding of the drivers of disease but will also allow the design of population-specific treatments that encompass a true precision medicine approach.
The ability to mine large data sets with bioinformatics tools has transformed the processing of both clinical and patient omics data and has also led to the improved stratification of ALS patient subgroups based on transcriptomic signatures highlighting distinct underlying disease mechanisms.
While there is still much to uncover regarding how these pathophysiological sub-classifications may change over the course of the disease, this is a large step forward and will allow for targeted therapies to be designed and applied to the most relevant subgroups of patients.
To offer more targeted treatments for ALS patients, precision medicine principles must be applied throughout all phases of drug development. A comprehensive patient profiling approach will be key to ensure the right drug is tested in the right patient and may eventually influence treatment choices in the clinic.
Leveraging these latest advancements in the field, the effective translation of therapies for ALS patients will be achieved one patient sub-group at a time.
Key messages
• With the emergence of antisense oligonucleotide technologies, additional gene targeted therapies will soon enter the market for MND/AL
• Leveraging omics data and machine learning methodologies will improve our understanding of both ALS phenotype and the underlying molecular heterogeneity between ALS patients, enhancing patient stratification into specific sub-groups
• Comprehensive patient profiling through the collection of full omics data will be critical to define responder populations.
Author competing interests – Dr Theunissen is the FightMND Early Career Research Fellow at The University of Notre Dame Australia and provides consultancy services to Black Swan Biotech, a precision medicine development company specialising in antisense oligonucleotide development. The review was published in Molecular Neurodegeneration.




A spinal cord injury not only influenced Dr Olivia Ong’s specialty, but she became a more compassionate doctor because of it.
By Ara Jansen
Dr Olivia Ong would probably have been a very different doctor if she hadn’t become a patient.
In 2008, a car accident outside the hospital where she was working left the rehabilitation specialist trainee with a catastrophic spinal cord injury. While it’s not an experience she would wish on anyone, decades later she can admit it has probably been the making of her.
Back on My Feet is Olivia’s memoir of her journey from doctor to 28-year-old patient and the rebirth of a different kind of doctor.
Against the odds and what the first doctors declared, during three painful years of rehabilitation Olivia regained the ability to walk and returned to medicine.
Decades later, she specialises in rehabilitation and pain management and has particular empathy for what her patients are experiencing. Based in Melbourne, the physician entrepreneur is known as the Heart-Centred Doctor.
Leveraging her experiences of resilience and burnout, she’s also a life and business coach for doctors, and a speaker and media commentator who shares the tips and tools which changed her life.
“I partially wrote this book as a love letter to my younger self and to the people who stood by me all the way,” says Olivia.
One of those people is her husband John, who she describes as a quiet man who doesn’t talk much.
Actions speak louder than words and he very much embodies that, being her biggest support.
The couple met at church and celebrated their 20th wedding anniversary this year. His constancy and their shared faith helped Olivia through many dark nights during recovery.
“Faith is a real thing for me. In the early days of growing up it’s probably more knowledge and an intellectual understanding of who God is. Until you have been through a terrible thing, then you really have to lean in and figure out what faith is to you.
“Faith is in the unseen and believing in small things and then the big things that come later.”
The radical awakening and imposed exploration of selfcompassion showed Olivia that while doctors know plenty, they are not always great at connecting with or listening to patients.
Being a patient taught her that hearing and understanding someone’s story and circumstances are just as important as their physical issue. She believes the characteristics you want in a doctor are competence, compassion, being comfortable with vulnerability and being an active listener.
Oliva had wanted to write Back on My Feet for a long time, but waiting has allowed for the perspective which might not have been present had her younger self written it closer to the accident.
“I’ve been interested in writing this book for a long time, but really life got in the way.
After my rehab I wanted to concentrate on establishing my spinal practice and then waited until my two kids were older.
“I really wanted to share a message for patients with persistent pain that recovery is often misunderstood and it’s often more complex, like in my case. It not only involved the physical, but accepting the grief and my new identity.
“Going from a doctor to a patient was a huge challenge, but I adapted. I hope this book helps someone feel less alone and gives them permission to be more human.
“It would have been too depressing to have written this book in the early days of my recovery. There was a lot of grief that came up in the beginning, in the early stages of my injury, and I didn’t really know what this kind of grief was. I grieved my mobility. I grieved my independence.
“In healthcare we have this illusion that we’re all a little untouchable. I’ve learned that despair, grief and gratitude can co-exist. Writing this book helped me honour that grief.”
That writing was both therapeutic and re-traumatising as Olivia also went through old photos and had conversations with people to jog her memory of her recovery.
“I remember everything. Writing the book forced me to re-engage with the moment of my accident; I remember the smell and the trees. I had clinically processed it and at the same time not fully processed the experience.
“I think there was some shame around that. Healing is never linear. Writing helped me transform that into a narrative and give trauma some kind of structure and helped me integrate it into my personality. The whole exercise gave me the space to do that.”
Olivia and John have two children aged five and 10. They are not closer in age because Olivia made a hard choice which faces many women in medicine – exams for further qualifications or children.

She figured out how to do both –have one child, then work towards her exams and have a second child after she passed them.
One of the aspects of her healing which helped Olivia immeasurably was having a team who believed in her and her desire to walk again. She picked a new rehab team when her original doctor told her she would just have to get used to life in a wheelchair. She now walks with two canes and spent two years at San Diego’s Project Walk where she learnt to walk again, inspired she says by American optimism.
Back on My Feet is out now through ABC Books.


Finally, workplaces are getting a much-deserved performance review for bad corporate language in the new show by Wankernomics at Perth Comedy Festival.
When James Schloeffel finally let his young son attend his Wankernomics show, the lad came armed with a pen and notepad. He then proceeded to dutifully tote up all the sweary and rude words and dad was later made to pay up for the swear jar back at home.
“There was no way around it,” says James. “He knew exactly how many there were.” The night cost the Melbourne comedian $24 – his son is not getting invited back in a hurry.
James – Chief Disruptor and Strategy Optimisation Evangelist –along with Customer Engagement Jedi Charles Firth are back as your favourite workplace tossers in the new Wankernomics comedy show.
By Ara Jansen
The pair have had sold-out runs in Australia, the Edinburgh Fringe and in the UK over the last few years and are back sharing their subtle, obvious and obnoxious observations of less than OK workplace behaviour.
It all started with a run at Adelaide Fringe a few years ago when the pair realised they had stumbled onto something, because who hasn’t complained about the people in their workplace – or let a buzzword tragically fall from their lips in a meeting so they feel included.
“We thought initially the idea might appeal to corporate groups but quickly realised it had a broader appeal. People were coming up to us after the show and saying how it mirrored their work life – how
they had to sit through stupid and useless meetings or other things that impacted their world.”
It was an idea James had been sitting with for a long time, especially with the advent of all those annoying and ultimately useless buzzwords and phrases which have found their way into workplace speak.
Prime contenders include “let’s circle back”, “move the needle”, “take this offline”, “deep dive”, “cross functional” and “bandwidth”.
As comedians the pair have known each other for a decade, Charles being a longtime political satirist, including being a founding member of The Chaser, while James is behind The Shovel
Creating Wankernomics was a chance for them to work together and turn their smart snark on the modern workplace – and like an office place virus, letting it spread across the land.
“While the word wanker doesn’t translate exactly in every country, here we get a pretty clear idea of what someone is talking about. Words I hate include symbiotic and stakeholders, it’s a cover for someone who is important but probably doesn’t actually exist,” James said.
“Another one is ‘socialise a document’ – which means can you email it.”
Wankernomics ’ return to town is part of the upcoming Perth Comedy Festival, where the duo will explain how corporate ‘bullshittery’ is taking over the world – and your life.
They’ll be joining a line-up of new faces and returning favourites, including Malaysian doctorturned-comedian Dr Jason Leong and UK-born Aussie resident nurse Georgie Carroll.
“It’s a ridiculous title but I think people will relate to it. I worked in marketing for a while and worked as a copywriter and what I wanted to do was help corporations get rid of jargon and help them write clearly and in a way that makes sense. Now I’m trying
to do that on stage and we’re having lots of fun doing it.”
Perth Comedy Festival runs from April 20 to May 17 in venues around Perth. Tickets and info from www.perthcomedyfestival.com
This month we have another round of competitions for you, whether you want to enjoy a glass on wine or get comfy with a book.
We have two copies of Dr Olivia Ong’s book Back On My Feet: From doctor to patient to give away.
We also have a case of Frankland Estate wines for one lucky reader. Read our Master of Wine’s review on page 43.
Medical Forum readers can also get 15% off their first purchase of a dozen Frankland Estate wines with the code MEDF15.
To enter, use the QR code on this page or go

Disney’s The Little Mermaid
4 12 APR
Dive into a magical kingdom where Ariel, a curious young mermaid, dreams of life above the waves. Featuring unforgettable songs including Under the Sea, Kiss the Girl and Part of Your World.

Colin Mochrie and Asad Mecci Star in HYPROV
SUN 26 APR
HYPROV is the smash-hit comedy show that blends hypnosis and improv for a one-of-a-kind night out.


David O’Doherty FRI 24 APR
A new opus from the hairy Enya, the Ryanair Bublé, the nine-volt battery powered Beethoven. Talking, songs, talking during songs, talking while walking around – it’s got the lot.


The Perth Comedy Festival Gala
29 APR, 6 & 13 MAY
The Perth Comedy Festival Gala brings together a dazzling line-up of the Festival’s funniest international stars, Australian legends and next-big-things for spectacular night of comedy.

Jenny Tian FRI 24 APR
Join Jenny as she unpacks one of her most character defining relationships in her signature style of storytelling.

Jimmy Rees THU 30 APR
Thanks to his on-point social observations, Jimmy is a bonafide comedic viral sensation. Nothing and no-one is safe in this hilarious and chaotic show.

At Humphrey Homes, every home we design and build begins with listening. We take the time to understand your vision, your lifestyle and your budget - then shape that insight into thoughtful spaces that are beautifully crafted. By seamlessly integrating architecture, interior design and construction, we make creating your forever home harmonious, effortless and deeply personal.
To start the conversation, call Dean Humphrey on 9284 5444.

Frankland Estate vineyard and winery is located in the Frankland River subregion of Australia’s most vast wine region, the Lower Great Southern – a region that, in my opinion, produces Australia’s best cool climate Shiraz and some of our greatest Rieslings.
The property was established by the late Barrie Smith and Judi Cullum in 1988. I witnessed the energy and fervour with which they approached the project in those first years when all of us in the region were learning the ropes of vine and wine.
They laid the foundations for the family business, the 35 hectares of vineyard and the winery now run by brother and sister Hunter and Elizabeth Smith, alongside Elizabeth’s husband, Brian Kent who has led the winemaking since 2010.
Organic Certification was achieved in 2009. The wines are marketed in several quality levels. The Estate wines are varietal Riesling, Chardonnay, Cabernet Sauvignon and Shiraz.
The Isolation Ridge Wines, from the original plantings, are of premium quality and represent quintessential expressions of their site. The high premium wines are Olmo’s reward and in exceptional years the Smith Cullum Riesling and Syrah wines.
Frankland Estate is remote, but well worth the visit.
Medical Forum readers can also get 15% off their first purchase of a dozen Frankland Estate wines with the code MEDF15.
Frankland Estate Isolation Ridge
2024 Riesling, RRP $60
From a warm, dry, low yielding vintage resulting in plenty of fruit flavour. Vibrant floral and lime aromas. Palate shows the regional lemon citrus flavours against a ‘slaty’ iron flint background.
Pristine, linear and pure. A touch of textural complexity from a small portion of barrel ferment will add to this wine’s longevity. A 10-year wine.
Frankland Estate Isolation Ridge
2024 Chardonnay, RRP $60
Shows a complex ‘mealy’ aroma which I love. Hazelnut and mango skin, flavours of stone fruits/ white peach. Textural but with a mineral backbone. Malolactic fermentation has been blocked giving a core of firm acidity that will give a few years ageing. Only 50 dozen bottles produced.
Frankland River Isolation
Ridge 2023 Syrah, RRP $60
Great cool climate Syrah (Shiraz) from a coolish vintage. Aromas of white pepper, violets and plum have been lifted by the addition of 2% Viognier. Palate displays
blackcurrant, wild herbs and cinnamon. Maturation mainly in older larger format French oak adds a savory austere edge. An 8-10-year wine.
Frankland Estate Isolation Ridge 2023 Mourvedre, RRP $60
This variety emanates from Southern France, particularly Bandol, and is usually a blending variety. A fascinating wine. Perfumed aromas with rose petal and potpourri. Sweet fruited on palate, displays blueberry. Nice punchy tannins. Amazing ripeness for this late-ripening variety in a cool vintage. Only 110 dozen produced.

A tribute to Prof. Harold Olmo, the Californian viticulturist who in 1955 identified this region’s potential for full bodied red wines. A blend of 90% Cabernet Franc, 7.5% Cab Sav and 2.5% Mourvedre, there were 350 cases produced.
The aim of this wine is for an “elegant, harmonious, mediumbodied blend”, certainly achieved in this example. The Cab Franc certainly dominates, with its lifted perfumed aromas, and grassy, blackcurrant leaf, raspberry and red fruit characters. A terrific wine with a 12-year future.
Frankland Estate 2023 Smith Cullum Syrah, RRP $125
Produced in only the very best vintages from carefully selected parcels of the highest quality fruit – a wine to recognise the founding partners.
The concentration of this wine accentuates all the Shiraz characters with layers of flavour.
The quality parameters – intensity, complexity, length and finish – all well and truly met. A 15-year wine. Reviewer’s Pick




