Dental Repair Technician 100300 Series (1 Week In-Person)
ONLINE & HANDS-ON PROGRAMS
Customization Options Available
Biomed to Imaging (B2I)
Biomedical Imaging & Information Systems (BIIS)
Medical Device Integration (MDI)
Medical Equipment Technician 100-300 Series
Radiological Safety
MRI Safety
Biomedical Information Systems
Analyzing & Design
Linear Accelerators - Beginner through Intermediate
INTEREST-FREE PAYMENT PLANS AVAILABLE.
PROFESSIONAL OF THE MONTH
Adam Vorpagel, CBET
BY K. RICHARD DOUGLAS
One of the great things about the HTM profession is that there is real opportunity for advancement if that is a biomed’s goal. It is possible to go from an intern to a system director.
Just ask Adam Vorpagel, CBET, system director of clinical engineering at Munson Healthcare.
“Coming out of high school, wasn’t entirely sure which career path I wanted to pursue. My mother was a NICU nurse at the time, and she mentioned that there were people in the hospital whose job was to fix and maintain the medical equipment their team relied on. I’d always enjoyed taking
things apart, figuring out how they worked, and fixing them, so that immediately caught my attention,” Vorpagel says.
He remembers that the more he researched the HTM/ biomed field, the more he realized it aligned perfectly with his interests, technical problemsolving with a purpose.
“That combination is what ultimately drew me into the profession,” Vorpagel says.
The decision to enter biomed led Vorpagel to enter the biomedical engineering technology associates’ program at Schoolcraft College.
“I started out as a biomed tech intern, worked my way up through the ranks holding positions as a BMET I, BMET II, BMET III, lead tech/coordinator and I am currently the system director for clinical engineering for Munson Healthcare,” Vorpagel says.
Munson Healthcare is northern Michigan’s largest and
leading healthcare system. It is based in Traverse City; a tourist destination and home to nearly 16,000 residents. The system serves patients across the entire region. Prior to entering leadership, Vorpagel’s primary area of focus and specialty was patient monitoring.
GETTING PATIENT MONITORING RIGHT
There are few projects that biomeds and HTM leadership can engage in with a more impactful benefit to patients than cutting edge patient monitoring. This also reduces stress for clinicians.
“One of the most challenging and impactful projects I am currently working on is the standardization of patient monitoring across all hospitals and care sites in our system. Prior to this work, our environment included multiple legacy platforms, inconsistent alarm workflows and fragmented connectivity models. As part of this initiative, we are implementing an enterprisewide conversion to Philips patient monitoring, establishing a standard, scalable platform that brings consistency, interoperability and long-term stability to our entire clinical monitoring environment,” Vorpagel says.
Some of the challenges that this initiative has presented include a highly fragmented technology landscape with more than a dozen monitor models across the enterprise, each with different integration workflows, alarm behaviors and data formats.
Vorpagel says another is “complex cross-department workflows: critical care, procedural areas, emergency departments and med/surg units all had unique expectations for monitoring, requiring careful alignment
BIOMETRICS
FAVORITE BOOK:
“Extreme Ownership” by Jocko Willink
FAVORITE MOVIE:
Does anyone have just one? don’t think I have a single favorite. I honestly am more into binge watching shows when time allows.
FAVORITE FOOD:
Polish food! Pierogies and kielbasa with sauerkraut
HIDDEN TALENT:
My team members probably disagree sometimes; but I like to think I am a pretty talented multi-tasker.
FAVORITE PART OF BEING A BIOMED?
My favorite part of being a biomed is the fulfillment that comes from helping others.
WHY DO YOU READ TECHNATION?
Keep up with industry trends and new technologies
of clinical needs.”
He also lists a couple of other challenges uncovered during this project.
“Interoperability inconsistencies: variations in how monitors interfaced with middleware, networks, and downstream systems created reliability and data quality issues and deployment logistics: coordinating replacements and go lives across multiple hospitals with minimal disruption to patient care requires a highly structured rollout strategy,” he says.
Vorpagel’s approach to the HTM profession has been consistent since he entered the field.
“At my core, I am driven by a sense of responsibility. If a device is in a patient’s room, it should work every time, integrate seamlessly, and support clinicians without adding burden, and above all, it must be safe for both patients and the staff who rely on it every day,” he says.
“That mindset has guided me from my earliest days in the field to this current systemwide leadership role,” Vorpagel adds.
In his free time, Vorpagel says he enjoys anything outdoors.
“I love to fish, hunt, hike and camp,” he says. He also says that he is happily married to his wife of five years.
The couple has two children, ages 3 and 1. Vorpagel knew that HTM was the right career from early on and he has embraced a philosophy and approach that has served him, clinicians and patients well over a successful career.
DEPARTMENT OF THE MONTH
University of Miami Health System Clinical Engineering Department
BY K. RICHARD DOUGLAS
Large healthcare systems require a large HTM presence to keep the medical equipment inventory up to peak performance standards and to take on big projects.
The University of Miami Health System Clinical Engineering Department fits that description
The department includes 53 full-time employees. Executive Director of Clinical Engineering and Facilities Regulatory Quality & Compliance Anthony McCabe, CPSO, CBCP, CBCLA, CCRP, CHSP, CLSO/M, LSSBB, CHTM, PMP, CHFM, leads a talented team.
Leadership members include Director of Clinical Engineering-Biomed Carlos Rivera; Director of Clinical Engineering-Imaging & IoMT Enrique Ortega, MBA, MSHI, MEM, PMP; Manager of Clinical Engineering-Quality Beatriz Hernandez, MBA, CHSP; Manager of Clinical EngineeringImaging Mayra Becerra, BAS, CBET; Manager of Clinical Engineering-Biomed Robert Kershaw Jr. and Manager of Clinical Engineering-Biomed Jorge Correa.
“The clinical engineering department supports a large academic health system across South Florida, encompassing acute care hospitals, specialty hospitals, ambulatory centers, research facilities and outpatient clinics,” McCabe says.
He says that the core inpatient footprint includes approximately 634-licensed beds across several facilities.
“This includes UHealth Tower, the system’s flagship acute care hospital with approximately 538-licensed beds, as well as dedicated inpatient capacity at Sylvester Comprehensive Cancer Center and Bascom Palmer Eye Institute, which support highly specialized oncology and ophthalmology care,” McCabe says.
Beyond this large inpatient environment, McCabe adds that the department provides support for more than 120 satellite and outpatient sites across the region, including large ambulatory centers such as UHealth SoLé Mia, specialty clinics and research locations.
“These environments range from high-acuity settings like operating rooms, ICUs, cath and electrophysiology labs to high-volume outpatient and procedural spaces with diverse technology needs,” he says.
Supporting this breadth of care delivery requires a flexible, risk-based clinical engineering model that scales across inpatient, outpatient and specialty settings while maintaining consistent standards for safety, reliability and regulatory compliance.
McCabe says that the facilities span five counties in southern Florida with over 40,000 assets that the CE team is responsible for maintaining. He says that the members of the CE team are
cross-trained and the department uses a balanced approach that combines specialization with cross-functional coverage.
BRINGING VALUE AND SHAPING GROWTH
Aligning with a standard and equipping a new facility are just a couple of the major projects from the CE team’s calendar over the past year and a half.
“One major special project has been the department’s pursuit of ISO 13485 certification, applying a medical device quality management system within an in-house clinical engineering operation. This effort required formalizing and standardizing processes across the full equipment life cycle, including procurement support, acceptance testing, maintenance, corrective actions, change management and documentation control,” McCabe says.
He says that the team aligned daily HTM operations with ISO 13485 requirements while continuing to support clinical operations, emphasizing risk-based decision-making, traceability and continuous improvement.
“Achieving this certification represents a significant shift in how the department governs quality and demonstrates that an internal clinical engineering program can operate with the same rigor and accountability expected of medical device manufacturers and service organizations,” McCabe says.
He says that over the past year, the department has been deeply involved in several large-scale, high-impact projects that significantly expanded the size and complexity of the medical device environment.
“At the beginning of 2025, we supported the opening of the Kenneth C. Griffin Cancer Research Building, a 12-story, 244,000-square-foot, state-of-the-art facility on UHealth’s downtown Miami campus. Supporting a National Cancer Institute-designated center required close coordination with research teams, facilities, IT and vendors to ensure highly specialized equipment was installed, tested, documented and placed into service under strict regulatory and operational requirements,” McCabe says.
He says that the project demanded a high level of planning around infrastructure readiness, device integration and longterm maintainability in a research-intensive environment.
“We also completed our portion of the opening of UHealth SoLé Mia, a new seven-story, 370,000-squarefoot ambulatory care center in North Miami. As the largest ambulatory facility in UHealth’s network to date, SoLé Mia added approximately 3,000 new medical devices to the clinical engineering inventory. The team managed largevolume device onboarding, acceptance testing, CMMS integration and go-live support while working alongside
clinical leaders to align equipment deployment with new care models and workflows,” McCabe says.
He explains that SoLé Mia brings together nationally recognized specialty programs under one roof, including the Sylvester Comprehensive Cancer Center, Bascom Palmer Eye Institute, Desai Sethi Urology Institute and a unique collaboration with the Hospital for Special Surgery (HSS).
“Supporting this level of specialty care required careful coordination across diverse technologies ranging from imaging and surgical platforms to outpatient diagnostics and procedural equipment,” McCabe adds.
The department has also proven that it can think outside the box as they have shown with their approach to cybersecurity.
“As more equipment became network connected, we quickly realized that traditional IT patching approaches did not always work for FDA-regulated medical devices. Instead of treating this as an IT problem alone, our team built a risk-based process that brought clinical engineering, IT and vendors to the table,” McCabe says.
He says that the team prioritized devices based on patient risk, worked with manufacturers on approved mitigations and partnered with IT on network controls when patches were not immediately available.
“This allowed us to reduce risk without disrupting clinical operations,” McCabe adds.
Away from the workplace, the department is actively involved in professional association leadership and standards development.
McCabe and Beatriz Hernandez participate in the Association for the Advancement of Medical Instrumentation (AAMI) standards committees focused on quality, contributing to the development and interpretation of industry best practices.
McCabe also serves as an alternate member on the NFPA 1660 Technical Committee, supporting the Standard for Emergency, Continuity, and Crisis Management: Preparedness, Response, and Recovery.
“In addition, Mayra Becerra serves as chairwoman of the South Florida Association for Medical Instrumentation (SFAMI) and as the SFAMI chapter representative for the Florida Biomedical Society (FBS). Through these leadership roles, the department supports professional development, regional collaboration and knowledge sharing across the HTM community,” McCabe says.
With many projects to support, and with their involvement in capital planning and budget management, this is an HTM department that is prepared to take on the big demands of a major health system and deliver the goods.
NEXT GEN POWERED BY YP AT MD
Raphael Torres
Medical Equipment Repair
Technician (MERT) Raphael Torres is truly part of the next generation of HTM. Torres is a college student while also learning on the job at University Hospitals in Ohio.
“Biomeds that don’t have the experience or qualifications to become an ISE (Imaging Service Engineer) 1 can do on-the-job training, learn from the DI team while getting their in-house background learning, as well as going to school to train and gain experience,” is how HTM Imaging Director Josh Nice, with University Hospitals Academic Market & Sodexo USA, explained the MERT position.
TechNation Editor John Wallace quizzed Torres to find out more about how he found HTM as a promising career field.
Q: WHERE DID YOU GROW UP?
A: Dominican Republic
Q: WHERE DID YOU RECEIVE YOUR HTM TRAINING/ EDUCATION?
A: University Hospitals and RSTI
Q: HOW DID YOU FIRST DISCOVER HTM?
A: Edgar Ortega introduced me to the field. I’m grateful for him.
Q: WHY DID YOU CHOOSE TO GET INTO THIS FIELD?
A: You get the satisfaction of engineering with meaning. It’s not just about fixing machines, it’s about ensuring safety, reliability and trust in healthcare systems.
Q: WHAT DO YOU LIKE MOST ABOUT YOUR POSITION?
A: What like most is that every day is different, there’s always a new problem to solve, which keeps the job interesting and motivates me to keep learning.
Q: WHAT INTERESTS YOU THE MOST ABOUT HTM?
A: What I enjoy the most about HTM is solving technical problems and helping people at the same time.
Q: WHAT HAS BEEN YOUR GREATEST ACCOMPLISHMENT IN YOUR FIELD THUS FAR?
A: My greatest accomplishments have been keeping customers happy through fast problem resolution and strong communication.
Q: WHAT GOALS DO YOU HAVE FOR YOURSELF IN THE NEXT 5 YEARS?
A: My goal in the next five years is to grow technically, improve my leadership and communication skills, and contribute at a higher level within HTM.
FUN FACTS
FAVORITE HOBBY: Skiing
FAVORITE SHOW OR MOVIE: Cars
FAVORITE MEAL: Steak with white rice WHAT
B SHIFTING GEARS
MX (Bicycle Motocross) is a versatile, action-packed sport that originated during the 1960s. It includes racing, freestyle, flatland, BMX park and dirt jump events. The riders often engage in maneuvers like spins, grind and flips. The focus is on speed and agility. Riders can be found at skate parks, dirt trails and on city streets.
As would be expected, a BMX bike needs to be durable as well as offer control and maneuverability. They generally are outfitted with 20-inch wheels. Riders need to have the athletic abilities that allow the endurance, bike handling and speed required to be competitive in the sport.
One experienced BMX rider comes out of the biomed ranks. Dustin Arp, CBET, is a network of care supervisor, anesthesia specialist at Children’s Hospital Colorado.
“I have been riding BMX for 28 years. It has brought me all across the U.S. and to different countries in search of exciting new things to ride. I also film and create videos of my friends riding and have produced three full-length BMX videos,” Arp says.
Arp credits his older brother for his introduction to BMX.
“He had a BMX bike growing up. He also had a subscription to a BMX magazine called BMX PLUS. My exposure to the magazine and him having a bike really sparked my interest,” he says.
Arp not only rides BMX but has captured the sport on video.
“Filming a full-length BMX video is a lot of work but very rewarding. It’s basically a compilation of all the best tricks my friends and I film over the course of two to four years compiled into one video. Most of the clips are filmed in and around the Denver metro area. Multiple road trips are also taken during the filming of the video to keep things fresh and ride new spots,” Arp says.
He says that the best part of any video project is the premiere when the video is done.
“It’s always amazing gathering everyone together in one place to watch the end project. It’s awesome to have a period in time documented that we can all look back on and remember. I think the overall message from these videos is to just get out there with your friends and have fun and create something,” Arp says.
After nearly three decades of practicing the sport, Arp has had to adjust some of the surfaces he rides on the most to compensate for wear-and-tear.
“For the first 25 years, I was always riding street; jumping off obstacles and grinding down rails. As of lately, my body can’t take that abuse anymore so I have transitioned into riding dirt jumps and skateparks. Riding those types of terrain, when executed correctly, is a lot less impact on my body,” he says.
Participating in BMX has also meant travel and interesting experiences.
“My first international riding trip was to Barcelona, Spain. That was an incredible experience I will never forget. The architecture is really different than it is here in the U.S., which made for some amazing spots to ride. In 2023, took a riding trip to Copenhagen, Denmark. That city is the most bike-friendly city in the world. Multiple bikes lanes on every street made it very easy to get around. Incredible spots also. There really is no better way to explore a city than there is on a bike. You really can get a true feel for a city and really get up in it,” Arp adds.
TAKING THE ADVENTURE OFF ROAD
His BMX adventures aren’t Arp’s only passion. He is also into
off-roading and camping. The off-roading involves a modified truck.
“This is a new endeavor I started four years ago when I bought my truck. I’m lucky to live in Colorado because we arguably have the best trails in the U.S. The adventures consist of picking an area to explore and go get lost. Always on the hunt for the best camp spots, fishing holes and amazing views I can find,” he says.
Arp says that the adventures also consist of exploring the many abandoned mining towns along the trails as most of the trails are old mining roads.
“Most the roads I drive on are very remote. I come across a lot of wildlife such as bear, moose, deer, mountain goats and big horn sheep,” he says.
What modifications has he made to his truck?
“Full suspension upgrade, big tires with beadlock wheels, armor, regear, steal front bumper with winch, rear steal bumper with swing out spare tire carrier, and I built a drawer system in the back bed to accommodate all my camping gear. It’s better to have it and not need it then to need it and not have it,” Arp says. Some of Arp’s favorite destinations for off-roading and camping include the San Juan Mountains, Moab, southern Utah, White Pocket Arizona and the Black Hills in South Dakota. For those considering either getting into BMX or off-roading, what advice does Arp have?
“For BMX, I would start with getting a bike. After that just get out and cruise. Hit the streets or skatepark and have fun with it and progress at your own pace. You really have to put time in on the bike to get good at it and feel comfortable. For off-roading, would start with any 4x4 vehicle,” he says.
After that, he says to download an app called onX Offroad. The app shows you all the trails in your area and rates them by difficulty.
“Then find some trails and get out there and explore. Then, slowly modify your rig as needed for whatever types of terrain you choose to tackle,” Arp adds.
On the job, Arp is a certified advanced technician at the Children’s Hospital Colorado in Aurora, Colorado.
“I take care of all the ICUs. I also take care of all the anesthesia preventative maintenance work. I just hit my 20th year of doing biomed last summer,” he says.
There is never a dull moment with this experienced biomed; dialed in for a BMX ride or an off-road adventure.
K. RICHARD DOUGLAS
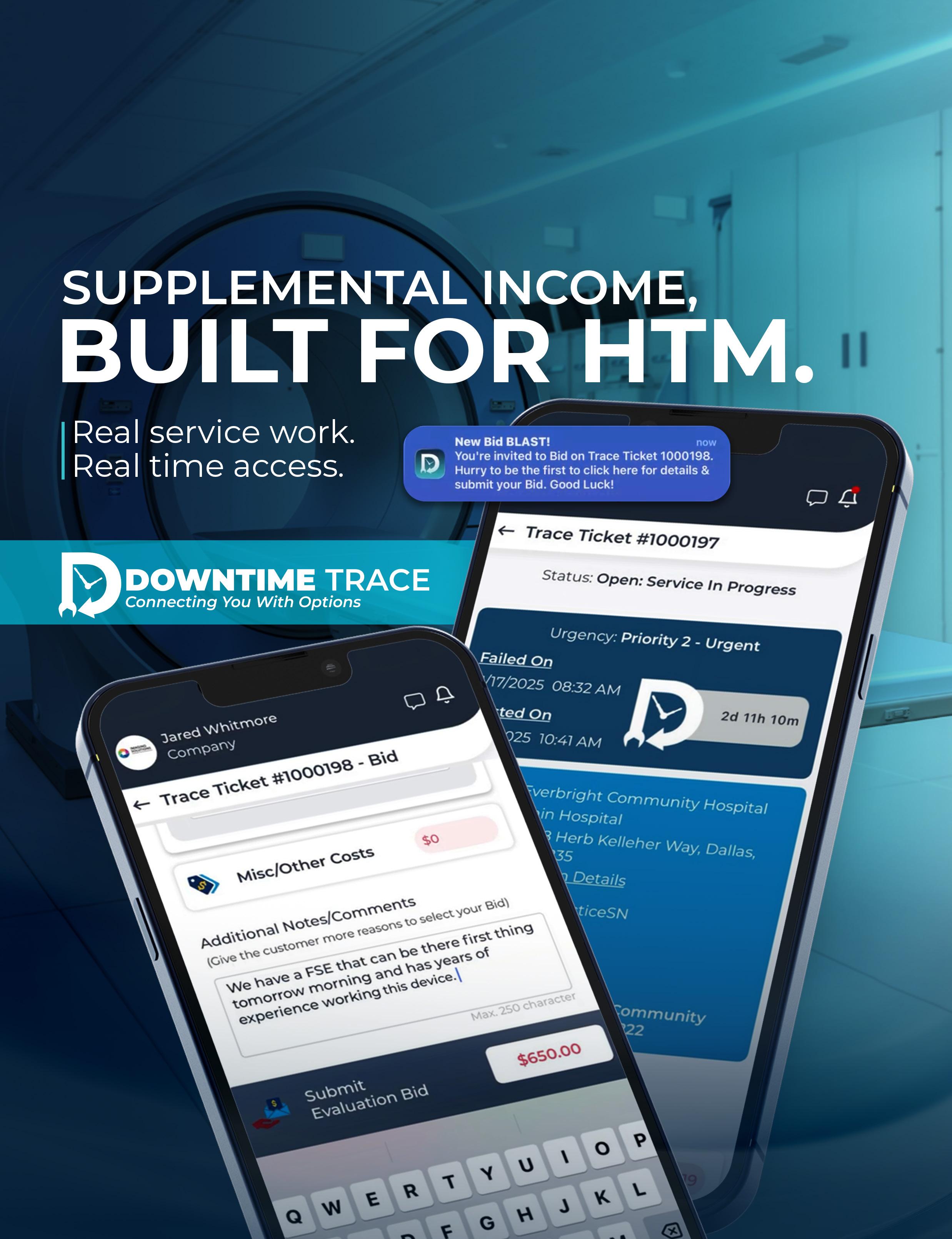
Turn your skill set into supplemental income — on your terms.
For gig technicians earning on the side, and ISOs looking to win work beyond their current network.
Downtime Trace was built for the Biomedical/HTM community that deserves a faster, clearer way to access work.
Founded in 2023 by brothers Danny and Jason Mobley, Downtime Trace came from a real, familiar problem: qualified technicians are out there, ready to help, but it has been hard to access facility requests directly. Jason felt that firsthand while working as a biomed department manager and still picking up side hustles at night to make ends meet. The hospital he worked for paid premium after-hours rates to outside vendors for repairs he could have done himself.
At the same time, Jason was delivering pizzas after hours, and the hospital was working with the OEM. That gap sparked the idea: what if medical equipment service work moved the way the rest of the world already moves?
Downtime Trace is a mobile app that works as a service marketplace for medical equipment maintenance and repair. It is designed to connect service providers with work based on their expertise and availability.
For gig technicians, it’s a clean path to extra income on their terms: create a profile that highlights make/ model competency, receive instant notifications on service opportunities that match what they are qualified to
support, and choose which jobs to bid on based on scope, timing and payout.
No contracts. No gatekeepers. Just service requests matched to their skill set.
For ISOs, it is a way to expand beyond their current network by gaining real visibility into demand and responding quickly with standardized bids, without relying on word-of-mouth, long vendor cycles or cold calls.
The app puts competition in the open. When a service provider places a bid on a “Trace Ticket” in Downtime Trace, the customer who submitted the request can compare the hourly rate, reviews left by other customers and the timeline for when the service provider can arrive. Customers love the control and side-by-side comparison, and service providers love the opportunity to compete for work they did not previously have access to.
Downtime Trace makes reputation part of the workflow. Every service event is reviewed, which means feedback is consistent and performance becomes visible over time. Strong work does not get buried in private relationships or scattered across email threads. It becomes a track record that helps service providers stand out and win future work. That is especially meaningful for independent technicians. Building credibility as a solo tech has traditionally depended on private networks. Downtime Trace provides a place to build a public reputation through completed jobs, verified certifications and mandatory reviews.
Downtime Trace was also built for flexibility. Service providers can set their service area and adjust it based on where they want to work. If a technician or ISO is open to travel, they can expand coverage. If they are traveling for a period of time and want to earn supplemental income, their service area can move with them so they can see opportunities in the region they are visiting and decide whether a job is worth bidding on.
The result is practical. Downtime Trace gives service providers more access to work, more control over what they take on, clearer expectations during service events, and faster payment, so they can spend less time chasing logistics and more time doing the work they are qualified to do. Which leads to the ultimate outcome, limiting interruptions for patient care across the country. Service providers can sign up at DowntimeTrace.com. A Downtime Trace team member will guide onboarding from start to finish.
The following Q&A provided by the Downtime Trace team answers the most frequent questions they hear from service providers.
Q:
HOW DOES DOWNTIME TRACE WORK?
A: Downtime Trace connects service providers to medical equipment maintenance and repair opportunities through a simple, app-based workflow.
1. Create a service provider profile: Service providers build a profile that highlights experience, make/model competency and supporting details such as photos and videos, technical scoring and relevant background.
2. Get matched to relevant opportunities: When a facility submits a service request, the platform matches that “Trace Ticket” to vetted service providers who are qualified for the make/model in need of service.
3. Receive the Trace Ticket notification: Matched service providers receive the request and can review key details before responding, including scope, timing preferences and other information included by the customer.
4. Submit a bid in a standard format: Service providers respond through a real-time bid process. Bids are submitted in a standard format that includes:
• What the provider believes is the likely problem and solution
• When the provider can begin service (estimated onsite arrival time)
• How much the provider will charge
5. The customer compares and selects: Customers view bids side by side and can compare service provider options using the details that matter most: competency, responsiveness, availability, price and performance history reflected through ratings and reviews.
6. Complete the service event and close out: Once selected, service is performed and the service event is documented through the platform, so the full experience is tracked from start to finish.
7. Get reviewed and get paid: Each service event requires a review, which helps service providers build a visible track record over time. Downtime Trace also serves as the trusted, single point of payment for service events. Approved payments are distributed to service providers and parts suppliers within days, not weeks or months.
CORPORATE PROFILE
Q: HOW DOES DOWNTIME TRACE WORK FOR INDEPENDENT TECHNICIANS VERSUS ISOS?
A: Downtime Trace supports both independent technicians and ISOs within the same standardized workflow, but the impact looks different depending on how they operate. For independent technicians, the platform provides direct access to service requests that match their make/model competency and availability, allowing them to bid on work without relying on private networks or vendor contracts. It creates a structured way to build a visible reputation through completed service events and required reviews, while also enabling payment within days of approval rather than weeks or months.
For ISOs, Downtime Trace serves as a scalable channel to expand beyond their existing network. ISOs can respond to demand with standardized bids, coordinate technicians and manage documentation across multiple service events within one system. The platform provides visibility into opportunity, performance and payment in a centralized format, helping ISOs compete more efficiently and operate with clearer expectations.
Q: HOW CAN A SINGLE STANDARD MAKE SERVICE WORK EASIER?
A: When a healthcare provider chooses Downtime Trace over older methods for ordering and tracking service, it signals a preference for a single, consistent standard. That consistency reduces complexity for both sides of the service event. Instead of navigating different vendor policies, workflows and communication styles for every service relationship, facilities can manage service requests within one platform and measure outcomes using the same set of expectations.
For service providers, a single standard helps reduce the friction that often slows down service events. Clearer service requests, a standardized bidding format and consistent expectations for communication create a smoother experience from the initial request through completion. It also creates clearer performance signals over time. Providers can be evaluated using measurable factors such as response time, downtime and uptime impact, performance against repair estimates, ratings and reviews, and financial information tied to completed work.
Q: WHAT IS ON THE HORIZON FOR THE COMPANY?
A: Downtime Trace has launched, and the focus now is building a healthy marketplace that supports both sides of the service ecosystem. The company is especially excited for independent technicians and ISOs who are gaining increased access to opportunities, supplemental income potential and flexibility, including the ability to choose which jobs they want to bid on.
A healthy Downtime Trace creates more income and freedom for service providers while helping facilities reduce inefficiency, improve equipment uptime and lower spend on device-related issues. The long-term goal is to continue modernizing how medical equipment service is requested, sourced, tracked and paid for by creating a platform that makes service events more transparent, more measurable and easier to manage.
Q: IS THERE ANYTHING ELSE READERS SHOULD KNOW?
A: The best solutions often feel simple. Downtime Trace is a practical step toward the future of service operations, and it reflects a shift that is already happening across industries: technology is making it easier to connect supply and demand, standardize communication and measure outcomes.
The team feels a strong sense of accountability to the service providers and healthcare organizations who rely on these systems. Building a new standard will require patience and adoption from the industry, but the model is designed to work because it aligns incentives. Service providers gain clearer access to opportunity and a more portable reputation. Facilities gain more control, more transparency and better visibility into service performance.
Q:
HOW CAN PEOPLE GET MORE INFORMATION?
A: Service providers can sign up at DowntimeTrace.com.
A Downtime Trace team member supports onboarding from start to finish. For more detail on the platform and how service providers interface with it, visit Downtime Trace on YouTube (@DowntimeTrace), where the team has created commercials and videos that walk through the concept, the workflow and the experience on both sides of a service event.
Join Downtime Trace and Transform Equipment Maintenance!
Whether you’re managing healthcare operations or providing essential repair services, Downtime Trace streamlines, simplifies, and strengthens your workflow.
NEWS & NOTES
Updates from the HTM Industry
IMED BIOMEDICAL REMAINS FOCUSED ON ISO 9001:2015 & 13485:2016 CERTIFICATION
iMed Biomedical was founded on a bedrock of core values that define it as an organization, as well as how it does business. iMed Biomedical previously announced its ISO 9001:2015 and 13485:2016 certification. As part of the ISO certification process, iMed Biomedical engaged in a rigorous audit of its product and service quality requirements.
The FDA conducted market research on third-party service organizations in the equipment repair industry. They concluded that there is not enough information to determine if non-OEM organizations would negatively or positively impact patient safety or quality of care. Lastly, they recommended these companies obtain an ISO certification to improve consistency of services and reduce liability. iMed Biomedical’s dedication to the quality of the services and products it provides is illustrated by its dual certification. What does this mean moving forward?
“We continue implementing the ISO standard and keep looking for ways to improve. As a team, we will constantly look for opportunities to build and support the industry with products that are dependable yet coupled with innovation and creativity,” iMed Biomedical website states.
“Over the past seven years, the iMed Biomedical has demonstrated a sustained commitment to quality, accountability and innovation through the successful maintenance of our ISO 9001:2015-certified quality management system. From the outset, our approach to quality has been intentional, rigorous and designed to support both operational excellence and long-term growth,” iMed Biomedical Quality Management Director Russender Powell said.
When iMed Biomedical first pursued ISO certification, it made the deliberate decision to pursue both ISO 9001:2015 and ISO 13485 simultaneously, she added.
“Achieving dual certification within a nine-month
timeframe placed our team and systems under a rigorous test, requiring disciplined process development, comprehensive documentation and a deep alignment with the highest international quality and regulatory standards,” Powell said. “This effort resulted in the successful dual management of ISO 9001:2015 and ISO 13485 for three consecutive years, during which time we established a mature, highly effective quality management system with no outstanding major or minor corrective actions.”
Since that initial certification milestone, iMed Biomedical has continued to demonstrate consistency and excellence through stellar annual surveillance audits.
“Our most recent audit included a distinct recognition for outstanding use of risk analysis and opportunity identification, reflecting how deeply risk-based thinking is embedded into our operations,” Powell shared. “Rather than treating risk management as a compliance exercise, we use it as a strategic tool to strengthen processes, anticipate challenges and drive innovation across the organization.”
“This sustained performance speaks directly to the strength of our team and the leadership of our Quality Management Director Russender Powell, who brings over 14 years of patient care experience and extensive expertise in healthcare facility regulations. This clinical and regulatory perspective ensures that quality decisions remain grounded in real-world healthcare impact, safety and reliability,” a company spokesperson said.
“As part of our continued quality journey, iMed Biomedical is planning to reactivate ISO 13485 certification to further align with medical device-specific quality and risk management requirements. This next phase reflects our commitment to regulatory readiness, patient safety, and providing healthcare organizations with dependable, compliant and forward-thinking equipment service solutions,” Powell said.
INTELAS LAUNCHES TEAMCHAMPS
Intelas, Compass Healthcare’s signature healthcare technology management (HTM) brand, has launched TeamCHAMPS, a new mobile experience designed to simplify medical equipment service and strengthen day-to-day communication.
TeamCHAMPS connects hospital clinicians, administrators and HTM technicians through a shared, real-time workflow that supports faster request submission, clearer status visibility and more consistent coordination from request to resolution. This launch reinforces Intelas’ focus on unifying HTM through a connected technology ecosystem that replaces fragmented tools with one streamlined operational experience.
“HTM plays a critical role in the patient experience, and every minute of equipment downtime creates a ripple effect across a hospital,” said Jim Cheek, president of Intelas. “We developed TeamCHAMPS to bring clarity and confidence to the equipment life cycle. By connecting the nurse at the bedside with the technician in the field on a single, intuitive platform, we are helping our partners minimize clinical disruption, improve asset performance and empower care teams to focus on what they do best: patient care.”
TeamCHAMPS is designed to reduce equipment downtime and give time back to patient-facing caregivers. Instead of tracking down phone numbers or logging into desktop systems, clinical staff can use TeamCHAMPS to instantly report an issue by scanning an equipment barcode and
describing the problem — eliminating manual entry and follow-up. The request is automatically routed to an Intelas technician, creating a work order complete with the device’s location, history and AI-driven service guidance. The application, which is part of Intelas’ broader TechCONNECT platform, uses AI to analyze the reported issue against historical data, manufacturer manuals and previous resolutions for similar problems. This provides the responding technician with a recommended repair path and parts list before they even arrive, dramatically increasing the likelihood of a first-trip resolution.
“The future of HTM is about moving from a reactive, service-centric function to a proactive, data-driven discipline,” said Dan Miles, vice president of information technology at Intelas. “TechCONNECT is more than a work order tool. It’s part of a connected ecosystem that enhances our technicians’ expertise with AI-powered insights and empowers clinical staff with real-time visibility. By unifying people, data and processes, we are building a more resilient, transparent and reliable healthcare environment.”
TechCONNECT connects the people requesting service with the teams delivering it, making it easier to submit requests, monitor status in real time and support technicians with the right information at the point of service. The result is a smarter, more predictable service model where devices are restored to service faster, technicians work more efficiently, and care teams have a seamless experience.
ARMY EYES MEDICAL MAINTENANCE PROGRAM EXPANSION
FORT DETRICK, Md. U.S. Army Medical Logistics Command is continuing to boost medical equipment readiness, reduce downtime and increase overall enterprise visibility through its Forward Repair Activity-Medical, or FRA-M, program.
Over the first 12 months of operation, technicians at the first FRA-M site at Fort Bragg completed over 1,600 maintenance service requirements for units on or near the North Carolina installation.
In total, the program has bridged a gap for more than 1,200 units without organic biomedical equipment specialists and ensured over 17,000 medical devices received required sustainment-level maintenance.
The FRA-M name is a rebrand from the program initially launched in October 2024 – known as Home-Station Medical Maintenance Support, or HMMS. The change better aligns medical with naming conventions used by other Army sustainment commodities, such as communications and weapons systems, which utilize Forward Repair Activities for maintenance needs.
“The first year has gone very well,” said Alfred Zamora, deputy director of the FRA-M program under AMLC’s Medical Maintenance Management Division, or M3D. “One of the things we quickly learned during setup was the importance of coordinating with the organizations on the installation, simply so they’d know that we’re there and what capabilities we can provide.”
The Fort Bragg FRA-M site is staffed with four technicians ready to provide regular maintenance and repair services for medical devices to units without organic 68A biomedical equipment specialists. Similar setups are planned for additional sites set to come online over the next few years.
Zamora said the next site is planned for Fort Campbell, Kentucky, expected to open in a temporary space before moving into its renovated, permanent location by early summer.
Additional FRA-M sites are planned at Fort Benning in Georgia, Fort Hood in Texas, Fort Carson in Colorado and Joint Base Lewis-
McChord in Washington, along with AMLC’s Medical Maintenance Operations Divisions, or MMODs, in Pennsylvania, Utah and California.
AMLC, a major subordinate command to U.S. Army Communications-Electronics Command, delivers integrated medical logistics that enables Army and Joint Force readiness from the strategic support area to the tactical edge.
The FRA-M program is one of the first major improvements put in place under an AMLC-led effort called Medical Logistics in Campaigning, or MiC, which aims to integrate medical logistics and equipment services into the wider Army sustainment enterprise, ensuring medical capabilities remain aligned with warfighter requirements.
The establishment of FRA-M at home stations, specifically, will have a significant impact on operational readiness and support capacity, Zamora said.
“FRA- M closes a longstanding gap in Class VIII medical maintenance by delivering targeted, on-site support where it was previously unavailable,” he said.
Before the FRA-M sites, units without maintainers in their ranks had to coordinate with their local medical treatment facilities, or MTFs, for support or ship equipment back to one of the MMODs, taking equipment out of service for extended periods of time.
Additionally, the MTFs, now a function under the Defense Health Agency, used different information systems that “didn’t talk” to the Global Combat Support System-Army, the Army’s sustainment system of record.
“When work was processed, the hospital techs weren’t in the Army system, so the information about the equipment was never put into G-Army,” Zamora said, “so some historical records about our equipment weren’t accurate.”
“Having a fixed-base operation through our FRA-M sites simplifies the process for the units, saving time and money, all while improving visibility for commanders and total readiness of the force.”
GE HEALTHCARE LAUNCHES READYFIX SOLUTION
GE HealthCare has announced the United States launch of ReadyFix, a remote fleet management solution designed to help healthcare systems support device uptime. ReadyFix will seamlessly integrate with GE HealthCare’s MAC VU360 resting ECG workstations, which are designed to deliver high-quality ECG readings that help clinicians make faster, more confident cardiac care decisions. When paired with ReadyFix, healthcare systems can leverage real-time data for remote device diagnosis and repair, supporting optimized MAC VU360 performance and continuity of cardiac care.
With an average of 10 to 15 connected devices per bed, the biomedical engineering team may be responsible for managing thousands of medical devices in their hospital – making it increasingly difficult to keep up with day-to-day maintenance and repairs. In fact, a recent survey found the majority of biomedical engineers (56%) describe their workload as “heavy” or “excessive.” At the same time, the U.S. Bureau of Labor Statistics projects more than 7,300 openings for biomedical equipment technicians over the next decade, yet only about 400 new graduates enter the field each year, widening the gap between demand and available support.
“Remote fleet management tools provide us with the
clarity, structure and real - time insights needed to stay ahead of equipment issues and maintain a high standard of reliability across the hospital,” said Tony Williams, director of biomedical engineering at Baptist Hospital in Pensacola.
“These tools elevate the way our biomedical engineering team supports patient care equipment.”
The introduction of ReadyFix expands GE HealthCare’s growing portfolio of DeviceReady remote fleet management solutions, designed to help biomedical engineers navigate the complexity of managing medical devices.
NEW TALENT JOINS AIS NUCLEAR MEDICINE TEAM
AIS has announced the addition of Chris Sheets and Andrew Long to the AIS team. Both joined AIS earlier this year as nuclear medicine field service engineers and “are already making valuable contributions to our growing service organization,” according to CEO Grant Norris. Chris Sheets joins AIS as a senior field service engineer, bringing extensive experience in nuclear medicine. He previously worked as an in-house equipment service engineer with Absolute Imaging Solutions in Stokesdale, North Carolina, where he supported nuclear medicine systems for more than six years. He also spent time with Carestream as a field service engineer supporting portable X-ray systems. Based in Wilmington, North Carolina, he strengthens AIS’s Southeast coverage and adds depth and expertise to its nuclear medicine service team.
Andrew Long joins AIS as a field service engineer based
REFURBISHED CAPITAL MEDICAL EQUIPMENT
HTM Week is set for May 17-23 this year and TechNation has announced a new contest. The TechNation HTM Week Contest sponsored by AllParts invites HTM professionals to share their “Most Satisfying Repair: That one fix that felt like winning a trophy.” Each weekday of HTM Week TechNation will present one lucky winner with a gift card. Find out all
TechNation is the primary monthly magazine and ultimate resource guide for over 12,000 medical
AllParts is a leading provider of OEM replacement parts, and Philips parts, operating out of two state-ofthe-art facilities in Nashville, Tennessee, totaling 160,000 square feet. It proudly supports all major Imaging OEMs and modalities. As an ISO 13485:2016 certified company, AllParts maintains a rigorous QMS, ensuring industry-leading warranty rates across all modalities. Find out more at allpartsmedical.com/
MEDWRENCH DELIVERS ‘PMS FOR PIZZA’
MedWrench recently shared its new HTM Week contest for 2026. The contest, which is sponsored by FSI, is titled “PMs for Pizza.” HTM professionals are invited to submit their best preventative maintenance tip for a chance to win. Five winners will be selected each weekday of HTM Week. Each winner will earn a pizza party for their HTM department.
MedWrench.com is a leading online community and resource for medical equipment service professionals. It connects HTM teams with trusted service providers, OEMs, and industry experts through articles, service directories, live forums, and more.
More than 1,000 hospital departments trust FSI for its easy-to-use CMMS – built for, and by, healthcare professionals. FSI offers a truly cloud-based CMMS, with built-in industry standards and best practices for the entire HTM team. Find out more at fsiservices.com/
Find out more about the PMs for Pizza contest at MedWrench.com.
WELCOME TO THE TECHNATION COMMUNITY!
Q: WHAT PRODUCT, SERVICE OR SOLUTIONS DOES YOUR COMPANY PROVIDE TO THE INDUSTRY?
TechMaster® Carts designs and manufactures premium, modular mobile workstations for healthcare technology management (HTM), clinical engineering, IT, and facilities teams. Our carts support medical equipment maintenance, deployment, parts organization, and mobile service workflows - helping technicians work more efficiently and keep critical equipment in service.
Q: TELL US WHAT DIFFERENTIATES YOUR ORGANIZATION FROM THE COMPETITION?
TechMaster® Carts are purpose-built specifically for healthcare environments - not repurposed industrial carts. Our modular platform allows departments to configure carts to their exact workflow, while premium construction, ergonomic design, and hospitalready durability deliver long-term performance and measurable productivity gains.
Q: WHY DID YOU CHOOSE TECHNATION FOR ADVERTISING?
RIBBON CUTTING
TechNation connects directly with the HTM and clinical engineering professionals who rely on efficient tools to support patient care. Its targeted audience and trusted industry presence make it the ideal platform to showcase solutions that improve technician productivity and equipment uptime.
Since 1979, Befour Inc. has been engineering, manufacturing,and testing the finest professional scale products on the market –and one of the select few companies that can say its products are made in the USA.
In addition to making scales under the Befour name, it has been an original equipment manufacturer (OEM) for several of the bestknown brands of scales who marketed Befour designs under their trade names. Every day, tens of thousands of individuals have their weight measured, not even realizing that the very scale they stood on was designed and manufactured by Befour Inc.
Befour scales are used across the healthcare field in hospitals, physicians’ offices and nursing homes. They are also the chosen scales of commercial gyms, professional sports teams, police departments, fire stations, schools, universities and the United States Armed Forces.
Befour Inc. President Kariann Thon recently shared more information about the company and how it can help healthcare technology management professionals.
Q: WHAT ARE SOME OF THE SERVICES AND PRODUCTS YOU OFFER?
A: Befour has been designing and manufacturing precision digital scales for over 45 years. Our scales are specifically designed to weigh patients, with a product line ranging from pediatric scales with 1 gram accuracy all the way up to bariatric wheelchair scales with a 1,000-pound weight capacity. One of Befour’s most popular scale lines is our stand-on measurement stations, which utilize our exclusive Opti-Height technology for the most accurate, safest and fastest way to measure a patient’s weight and height. We’ve also added to our existing ADA-compliant scale options an ADA-compliant
wheelchair scale (MX480D-ADA) and also introduced a wall-mount wheelchair scale (MX440D).
Q: HOW DOES YOUR COMPANY STAND OUT IN THE MEDICAL EQUIPMENT FIELD?
A: Befour scales are USA-made and built to last decades in high-use, demanding environments. All scales are safety-listed to the most current medical device electrical standards and most competitive scale companies can’t make that claim. In addition, our scales include cost-saving features such as exceptional battery life, 3-year warranty and technical support for the life of the scale. These scales are incredibly easy to own and operate, while also providing the most accurate weight measurements.
Q: DO YOU HAVE ANY GOALS YOU WOULD LIKE TO ACHIEVE IN THE NEAR FUTURE?
A: Historically, Befour has put all our resources into engineering and manufacturing incredible scales that surpass the competition in every way, resulting in a complete line of competitively priced healthcare scales we are proud to stand behind. Now, our dual focus is furthering the Befour brand and ensuring those in healthcare are aware of who we are and why our scales can create a patient-positive, cost-saving difference within your facility.
Q: IS THERE ANYTHING ELSE YOU WOULD LIKE TECHNATION READERS TO KNOW?
A: If your facility uses patient scales in any capacity, Befour is a proven brand that should be considered prior to your next purchase.
You can visit us at befour.com - but if you really want to learn what sets Befour apart from all other scale brands – check out befour.com/fast-facts!
Joe Paese
National Sales Manager TechMaster® Carts
AAMI UPDATE
Five Major Trends Shaping Medical Device Software
BY DAVID NELSON
The medical devices industry is witnessing one of the fastest growth spurts in software innovation in years. That uptick has played a core role in enabling new developments in diagnostic technologies, clinical workflows, patient communication and product outcomes. This article discusses five key trends that are re-orientating how medical device software is developed and maintained.
1. CLINICAL INTELLIGENCE POWERED BY AI AND MACHINE LEARNING
Artificial Intelligence (AI) and Machine Learning (ML) are revolutionizing medical device software, particularly with Software as a Medical Device (SaMD). There are AI algorithms that can process complicated medical data –including imaging, physiological signals and patient histories – with the level of accuracy that expert doctors and physicians can achieve. These types of medical device software facilitate early identification of disease, risk stratification and patient-specific therapy planning.
Regulatory strategies, such as the FDA’s PCCP (Predetermined Change Control Plan), make managing updates more feasible by not requiring repeated full approvals. Modernizing the regulatory process has been key to meeting the increased demand created by these advancing technologies.
Key Takeaway: AI and ML technologies are revolutionizing clinical decision-making and providing improved patient outcomes.
2. CYBERSECURITY: PROTECTING CONNECTED DEVICE DATA
With medical devices increasingly integrated with cloud services, hospital networks and consumer endpoints, cybersecurity has become a critical concern. Recent security incidents and ransomware attacks have raised the issue of insecure devices, so manufacturers are needing to apply robust security measures, including scanning trust architectures, advanced encryption
techniques, constant vulnerability scanning and AI-driven threat detection are becoming the standard for medical device software.
Regulations require comprehensive security planning throughout the device life cycle, including secure update procedures and documented incident response plans.
Key Takeaway: Proactive cybersecurity is essential for regulatory compliance, patient safety, and maintaining trust with healthcare professionals.
3. INTEROPERABILITY: SEAMLESS DATA EXCHANGE
Medical device software must be integrated with electronic health records (EHRs), telehealth systems, analytics solutions and population health systems. Interoperability standards such as Fast Healthcare Interoperability Resources [FHIR] and open APIs are facilitating real time data exchange between multi-level systems. This connectivity allows for continual care –such as tracking EHRs with a monitor that can automatically update them, monitoring the state of equipment notifications that can set off clinical workflows, or using imaging data that can improve AI diagnostics. Strong interoperability minimizes human errors and can facilitate personalized medicine.
Key Takeaway: Easily exchanged data is crucial to efficient clinical action and patient care.
4. CLOUD-NATIVE SOLUTIONS AND REMOTE MONITORING
Cloud computing is revolutionizing medical device software with scalable storage of data, real time analytics and centralization of device management. Cloud-native platforms are specifically well-suited for imaging, remote patient monitoring and healthcare analytics.
Healthcare facilities can centralize massive amounts of data, conduct advanced analytics with populations and remotely update equipment.
streamlining clinical documentation and decision support. Applications include summarizing diagnostic information, generating clinical notes from device readings, and producing natural-language descriptions of imaging or sensor data.
These solutions alleviate administrative burdens, standardize reporting and allow clinicians to focus on complex care decisions. While still new in regulated medical software, generative AI is shifting clinical intelligence from purely human-driven to machineassisted processes.
Key Takeaway: Generative AI has the potential to revolutionize clinical documentation and decision support, improving workflow efficiency and patient communication.
The future of medical device software is defined by intelligence, connectivity, security and integration. Secure, interoperable, cloud-enabled and AI-driven devices are not merely technological advancements, they are essential for improving patient outcomes, streamlining workflows and enabling personalized medicine. As regulatory environments evolve and technical capabilities mature, software will remain the engine of innovation in the medical device landscape.
– David Nelson is the associate director of software at Boston Scientific. Opinions and speculation are his own, and do not reflect the position of AAMI, Boston Scientific or TechNation.
5. GENERATIVE AI: ENHANCING CLINICAL WORKFLOWS
Generative AI is emerging as a powerful tool for
ECRI UPDATE
Why Hospital Supply Chains Are Always in ‘Urgent Mode’ & How Leaders Take Back Control
Most healthcare supply chain challenges do not begin with a strategy conversation. They begin with an email, a hallway exchange or a last-minute request marked urgent. A clinician needs a different product. A device fails unexpectedly. A recall hits without warning. A shortage forces a workaround. By the time supply chain is engaged, the expectation is often clear: move fast.
Over time, this constant urgency becomes normalized. But when everything is urgent, leaders lose the ability to distinguish true clinical need from systemic breakdowns –driving higher costs, greater risk and increased friction. High-performing supply chain leaders approach this problem differently. They do not eliminate urgency; they control how demand enters the system, often without formal authority and within highly matrixed clinical environments. They rely on influence, evidence and relationships – not mandate – to bring structure to chaos.
REALITY OF CLINICIAN-DRIVEN DEMAND
Clinicians are not trying to create chaos. Most requests are rooted in legitimate concerns, including:
• patient safety
• clinical effectiveness
• workflow efficiency
• past negative experiences with products or equipment In practice, these requests frequently surface through informal channels – outside of established value analysis or prioritization workflows that are already stretched thin. The challenge is that demand often arrives without context, without prioritization and without a shared framework for evaluation. Supply chain teams are left to react – balancing speed, safety, cost and relationships in real time. When this becomes the default operating mode,
organizations experience:
• decision fatigue
• inconsistent outcomes
• strained supply chain-clinician relationships
• missed opportunities for standardization
These dynamics are consistent across organizations, though the scale and formality of processes may vary between community hospitals and large, integrated delivery systems.
WHY EVERYTHING FEELS URGENT
Several common triggers repeatedly push demand into crisis mode:
• product recalls and safety alerts requiring immediate action
• equipment failures or end-of-life assets identified too late
• supply shortages or backorders forcing rapid substitutions
• preference changes driven by new hires, new techniques or vendor influence
• budget pressure colliding with unplanned requests
None of these scenarios are unusual. What separates more mature organizations is not whether these events occur, but how early – and how clearly – they are framed before decisions are forced.
COST OF REACTING INSTEAD OF FRAMING THE PROBLEM
When prioritization is informal or inconsistent, urgency drives decisions instead of strategy. The consequences are tangible:
• higher total cost due to rushed purchasing or limited negotiating leverage
• increased variation that undermines standardization efforts
• safety risk introduced through poorly evaluated substitutions
• friction between supply chain, clinicians and finance
• a perception that supply chain “slows things down,” even when protecting value
In these moments, supply chain is often blamed for delays that are actually the result of upstream ambiguity. In contrast, leaders who pause long enough to frame the problem regain control without sacrificing speed – and reduce the likelihood that the same issue resurfaces again as another “urgent” request.
HOW LEADERS INTRODUCE STRUCTURE WITHOUT SLOWING CARE
Effective supply chain leaders do not block demand; they shape it in ways that preserve speed while reducing noise. The goal is not to add bureaucracy, but to introduce enough structure to protect downstream decisions – often within existing value analysis or governance structures rather than creating new ones.
1. Establish Clear Intake Expectations (Without Creating Red Tape)
Not every request requires a committee, but every request requires the same minimum context.
High-performing teams define a short, consistent intake standard that answers:
• What problem is being experienced at the point of care?
• What risk or impact is driving the request today?
• What happens if this decision is delayed 30, 60 or 90 days? They also clarify:
• Who must be involved early (e.g., clinical, safety, finance) versus who can be consulted later
• What qualifies for an expedited path (e.g., recalls, patient safety risk, equipment failure)
This approach reduces back-and-forth, shortens evaluation time and prevents supply chain teams from having to “reinterview” stakeholders after the fact – particularly when requests move quickly outside normal workflows.
2. Explicitly Separate Urgent, Time-Sensitive & Important
One of the most effective – and simplest – changes that leaders make is naming urgency with precision.
Rather than debating whether something is urgent, they introduce a shared language:
• Urgent: Immediate patient safety or operational risk
• Time-sensitive: Requires resolution within a defined window
• Important: A valid request that benefits from full evaluation
This shift reframes conversations from emotion-driven escalation to risk-based prioritization and helps clinicians understand why some requests move faster than others –even when supply chain does not control final clinical decisions.
3. Reframe the Ask Before Evaluating the Solution
Experienced leaders resist starting with product comparisons. Instead, they pause long enough to align on the problem –often within value analysis discussions that are already under time pressure.
They consistently ask:
• What outcome are we trying to improve or protect?
• What risk are we trying to reduce or avoid?
• What would success look like 6 months after implementation?
By anchoring discussions in outcomes and risk – not brand or preference – leaders reduce downstream conflict and create space for evidence-based options without slowing momentum.
4. Make Prioritization Decisions Visible and Defensible
When prioritization occurs behind closed doors, frustration grows – even when decisions are reasonable.
Leading organizations:
• Document why requests are prioritized, deferred or redirected
• Communicate decisions in plain language, not policy terms
• Tie decisions back to safety, access or organizational goals This transparency builds trust and consistency. Even when the answer is “not now,” stakeholders understand the rationale and are less likely to bypass the process or reintroduce the request through informal channels.
5. Close the Loop So the Same Urgency Does Not Reappear
Structure only works if learning feeds forward.
Strong leaders ask:
• Why did this issue surface as urgent?
• Was this preventable with earlier visibility or monitoring?
• What should change so the next request enters earlier – and with less disruption?
Over time, this reduces repeat fire drills and shifts supply chain from crisis response to proactive stewardship, even in environments where resources and authority are limited. Leaders who introduce structure at the front end do not slow care; they protect it – by ensuring that speed is applied where it truly matters and discipline is applied where it delivers the most value.
THE PAYOFF OF CONTROLLING THE FRONT END
Leaders who take control of how demand enters the system see measurable benefits:
• fewer downstream surprises
• stronger clinician alignment
• more defensible, evidence-based decisions
• reduced variation and value leakage
• lower risk exposure over time
Most importantly, they shift supply chain from a reactive problem solver to a strategic partner – without losing responsiveness.
LOOKING AHEAD
Demand pressure never disappears in healthcare. But when leaders manage how requests enter the system, they protect every decision that follows – evaluation, contracting, utilization and risk management.
For more information, visit ecri.org
BIOMED
BY CLAIRE WILSON
Life is a series of peaks and valleys. Moments that rise and fall the way an ocean tide flows with the Earth. We often choose to forget how much progress we have made, always looking to what still needs to be understood to reach the next milestone. The past reminds us; disappointments and accomplishments are equally beneficial to our careers. Negative results are motivation to reach a higher level of opportunity.
The recent changes in my life have taught me the peace of being in the moment. To not have to plan every step of my life in advance. The opportunities that did not expect were
the ones that carried me the farthest. The challenges I feared the most have advanced my career the fastest. The working world is no longer based on finding one job and retiring in 40 years. Success is now dependent on the willingness to change. Relocate, move through different companies, try many different job titles, take a pay cut for a healthier environment. The expectation to live outside a comfort zone. To challenge your mind with learning every single day.
I have been part of the HTM community for four and a half years now. I still feel like that 18-year-old girl, graduating during the ruins of a global pandemic. I was told the best years of my life were already over. I never believed what society wanted me to think. There is no limit to potential and growth, at any age of life.
Some of the most respected and influential mentors and leaders of the HTM community have explained to me the
most important key to growth is attitude. The ability to stay positive even on the worst days. Positivity reflects gratitude. In October 2024, had just moved over halfway across the country for a job. After settling into this new endeavor, quickly realized that was not meant to stay. Cautiously, I started looking for a sign that would lead my career to a brighter future. My father had mentioned to me his colleague, Dave Scott, was working on a presentation for MD Expo and was looking for a beginner biomed to share ideas with. explained that I was interested in learning more about this presentation idea, knowing that the deadline for the pitch was quickly approaching. I was completely out of my element. I struggle with social anxiety and had no formal public speaking experience prior to the presentation. I used to do my homework in conference rooms while my dad and Dave Scott taught classes to help prepare individuals for CBET exams. It had been six years since had seen Dave. Six months later, I was in California sharing my ideas with him, in front of an audience. Presenting at the April MD Expo was one of the most terrifying and rewarding experiences of my life. I found a network of like-minded people sharing their experiences and advice. They gave me hope when I needed it most. The encouragement to do other presentations in the future is what led to a major
advancement in my career.
I had a lifelong dream to live in the Rocky Mountains, since growing up in Denver, Colorado.
By the beginning of 2026, I left behind my life in New York and accepted a job at Yampa Valley Medical Center, in Steamboat Springs, Colorado. The promotion moved me from a BMET I to a BMET II. I have officially been on the job for one month. I recently adopted two puppies. am making genuine friends and feel a surge for creativity like never before. I have more energy, smile more, I have learned to be more patient and less critical over small frustrations. My life is not consumed by needing to be more. I am enough, in this moment.
The best gift I could have given myself was to start over. Not from scratch, from experience. I have created a healthy work-life balance. I encourage myself every day to build healthier habits. Wake up earlier, read more, let my mind slow down and enjoy even the simplest moments. My career has advanced my life in every aspect. The best advice I can give anyone is to chase your dreams. Do not worry about the “how” or “when.” Just focus on where you want your life to grow and spend every moment building goals into accomplishments.
A DETAILED LOOK AT PARTSSOURCE PRO SERVICE
The Webinar Wednesday’s Tools of the Trade Live Demo series continues in 2026. The recent live demo of the PartsSource PRO Service was eligible for 1 CE credit from the ACI.
PartsSource Vice President of Product Services Jared Koslosky guided attendees through PartsSource PRO Service. He provided an in-depth look at the digitally powered solution transforming how hospitals manage equipment service and support. The PartsSource PRO Service platform brings an entire service program together in one place, with one workflow and one trusted partner.
Koslosky showed how PRO Service gives healthcare organizations complete transparency into service costs, contract entitlements and provider performance. Attendees witnessed a data-driven approach powered by real benchmarks and continuous vendor monitoring. They saw how PartsSource PRO helps HTM professionals make smarter decisions and ensure every service dollar is spent wisely. He also demonstrated the structured assessment process and how health systems of all sizes are standardizing and simplifying their service programs.
A question-and-answer session provided additional information as Koslosky fielded questions from attendees. Attendee Brian Simson, a certified biomed technician with Ventura Biomedical Services, won a Swiss Force Meister MultiTool for correctly answering a trivia question during the webinar.
He and other attendees provided feedback via a postwebinar survey that included the question, “What was your single biggest takeaway from today’s product demo?”
“Diagnostic AI tools help determine patterns of spend to determine opportunities for savings,” said Paul Neher, a supervisor with Parkview Health.
“I enjoyed the demonstration of the PartsSource dashboard containing the different metrics for tracking,” said Roosevelt Charitable, a medical equipment planner/BMET with Endeavour IO.
“Elevating my understanding of how the HTM environment functions internally and externally,” BMET student Cray Alvarez said.
“That the PRO Service was made with managers and techs in mind and seems to be an ever-evolving tool,” said Sean Sammons, a Biomed Tech II with Fairfield Medical Center.
CLICK. WATCH. EARN.
RTLS SUBJECT OF EXPERT ROUNDTABLE DISCUSSION
The Webinar Wednesday roundtable presentation on Real Time Location Services (RTLS) delivered knowledge to HTM professionals and was eligible for 1 CE credit from the ACI.
TechNation Editor John Wallace was joined by industry leaders for a roundtable discussion on RTLS. Topics of discussion included integration, location tracking in clinical environments, evaluating RTLS accuracy claims, organizational buy-in for RTLS, readiness factors, as well as passive versus active tracking technologies
Panelists who shared their insights were:
• Kerry Brock, vice president of sales-RTLS with HID Global;
• Allen Foucht, RN, BSN, CLSSMBB, senior customer success coaching + education manager with Midmark;
• Dustin K. Telford, AAMIF, CHTM, CBET, CRES, CLES, an associate consultant on device safety consulting; and
• Benjamin Scoggin, MBA, MMCi, senior director of clinical engineering with Duke Health.
The webinar hosted 64 attendees for the live presentation, and a recording of the session is available for on-demand viewing at WebinarWednesday.live.
Sturdy Health Director of HTM Michael Link was the luckiest webinar attendee winning a Swiss Force Meister Multi-Tool for correctly answering a trivia question during the webinar.
Every attendee benefited from the webinar according to a survey that included the question, “What was your single biggest takeaway from today’s roundtable?”
“How beneficial real-time software can be,” said Devin Harback, a BMET student at St. Clair College.
“Having governance for installing tracking equipment on equipment,” said Kelvin Knight, HTM director at Children’s of Alabama.
“There is more to consider than just reliability when choosing an RTLS system,” said Rita Vitela, a clinical engineering technician with Orlando Health Winnie Palmer Hospital.
“Broader understanding of RTLS applications,” said Barrett Bartlett, director of HTM at Lake Charles Memorial Health System.
“The knowledge the speakers had and how it tied into BMETs day to day,” said Dominique Ng, a biomedical engineer with Inova Health System.
SHARED RESPONSIBILITY IN MEDICAL DEVICE CYBERSECURITY EXPLAINED
The Webinar Wednesday session “Patch Me If You Can: Shared Responsibility in Medical Device Cybersecurity” sponsored by Claroty is eligible for 1 CE credit from the ACI. The webinar was based on the fact that cybersecurity risks facing healthcare are growing faster than the defenses. Legacy medical devices, fragmented responsibility across vendors and providers, and slow vulnerability response are leaving critical systems, and patient lives, exposed.
As ransomware, remote access attacks and unpatched assets increase, the need for trusted collaboration between healthcare delivery organizations, medical device manufacturers and threat intelligence partners has become urgent and non-negotiable.
Skip Sorrels, Field CTO at Claroty, dove into the operational and cultural gaps that prevent effective coordination and remediation of risk to patient care. From shared risk models to collaborative patching workflows and faster incident response, he shared what is holding the vulnerability management process back and actionable strategies that are working today.
Attendees obtained a clearer understanding of how to break down silos, align priorities and strengthen the healthcare system before the next crisis forces the issue. An informative question-and-answer session capped off the webinar providing additional insights to attendees.
Noah Clark, a BMET student at Minnesota State College Southeast won a Swiss Force Meister Multi-Tool during the webinar.
Attendees provided feedback after the webinar via a survey. One question was, “How will this webinar help you do your job better?”
“This webinar gave me an interesting perspective of network security, coming from someone who has always been on the biomed/HTM side of things,” said Jimmy Tu, Program Manager, Children’s Health.
“This webinar gave me a stronger understanding of the challenges involved in identifying cybersecurity vulnerabilities. Although do not work directly in cybersecurity, do work with medical equipment, and feel better equipped to identify and address potential issues more efficiently. The platform was an excellent way to ask questions and hear discussions from facilities across this field,” Biomed Specialist Stephanie Puckett, CBET, with Duke University Hospital said.
“It will help me do my job better in the future by reminding me to bring up all security concerns ASAP so that they can be handled before they become an issue,” said
Austin Purney, a BMET student at Minnesota State College Southeast.
Check out upcoming webinars and register today at WebinarWednesday.live.
LIVE DEMO: APRIL 1 at 2 PM ET
Registration on WebinarWednesday.live
Eligible for 1 CE credit from the ACI.
Claroty xDome - Operational Efficiency
Connectivity in modern healthcare networks has dramatically reshaped patient care delivery. Clinical workflows depend on connectivity, requiring proper governance of IoMT devices to ensure operational efficiency. This Tools of the Trade demo will dive into the Operational Efficiency module of Claroty xDome, which helps clinical teams leverage device utilization, location, and operational status to ensure optimal use of device resources and to drive more efficient operational planning and smarter capital expenditures.
Key areas that will be covered in this demo:
• Inventory Reconciliation: Syncing CMMS/CMDB data to create a centralized inventory with device-specific profiles and risk scores
• Utilization and Life Cycle: Using device data to identify patch windows, balance usage, and apply compensating controls to extend the device life cycle
• Resource Optimization: Improving operational uptime by coordinating security patching with scheduled preventative maintenance.
ROUNDTABLE
Equipment Disposition & Recycling
In healthcare, equipment disposition is no longer a back-of-house task relegated to storage rooms and loading docks. It is a decision that must consider clinical operations, cybersecurity, compliance, sustainability and capital recovery. As hospitals and health systems face mounting financial pressures and increasingly complex regulatory requirements, the way they retire, redeploy, resell, recycle or dispose of devices has direct implications for patient safety and the bottom line. In this month’s Roundtable, industry leaders share equipment disposition and recycling insights.
Participants for this discussion are:
• HERO Business Inc. President Kevin Lynskey;
• Image One Medical Group LLC CEO Ric Arcadi; and
• Project C.U.R.E. Director of National Procurement Janet Thomason.
Q: WHAT MISTAKES DO ORGANIZATIONS MOST COMMONLY MAKE WHEN RETIRING MEDICAL EQUIPMENT?
Lynskey: The biggest mistake is treating equipment
retirement like an afterthought instead of a clinical and financial decision. We see hospitals park devices in hallways, closets or “doom rooms” for months waiting for someone to deal with it. That creates compliance risk, lost resale value and inventory blind spots. Another common miss is skipping proper documentation and chain-of-custody tracking. If you can’t prove what happened to a device, that’s a problem. And finally, too many organizations default to scrapping equipment that still has usable life or parts value. That’s literally throwing money away.
Arcadi: They often choose a lower cost service provider during the life of the equipment’s use, which can have a large negative impact on the value of the equipment during trade-in or sale. It also shortens the useful life they could get out of that asset
Thomason: One of the biggest mistakes is equating “no longer right for us” with “no longer valuable.” In U.S. health systems, equipment is often retired because of standardization initiatives, technology upgrades or service contract changes – not because it’s unsafe or unusable. But globally, the need is staggering. The World Health
Organization estimates that nearly half of the world’s population lacks access to essential health services. In many low-resource settings, clinicians are working without reliable imaging, anesthesia or even basic monitoring equipment. So, what may be a prior-generation ultrasound in Phoenix or Chicago can be the first ultrasound in a regional hospital in Ghana or Nepal. Another mistake is looking only at secondary market value. Financial resale price doesn’t capture patient impact. When we talk about disposition, we should be weighing both economic return and healthcare return.
Q: WHAT STEPS MUST BE TAKEN TO PROTECT PATIENTS AND MEET HIPAA REQUIREMENTS WHEN IT COMES TO EQUIPMENT DISPOSITION AND RECYCLING?
Lynskey: It starts with data. Anything with memory, storage or network connectivity needs certified data wiping or physical destruction before it ever leaves the building. That includes monitors, imaging accessories, telemetry, infusion systems, and even certain beds and specialty devices. We always work directly with each facility’s IT and security teams to ensure we are following their HIPAA requirements and internal e-waste policies, not just generic best practices. From there, it’s about documented chain-of-custody, serialized tracking and responsible environmental handling for batteries, fluids and electronic waste. At HERO, we treat disposition like an extension of the HTM program, not a junk pickup. Patient safety, cybersecurity and sustainability all live in the same lane here.
Thomason: Patient privacy is non-negotiable. Any device that stores protected health information must be properly sanitized in compliance with HIPAA. That means secure data wiping and removal or destruction of hard drives where necessary. At the same time, we have to be thoughtful. Data security shouldn’t automatically mean physical destruction of equipment that could safely serve patients. Due diligence is essential, and donation or disposition partners need to have processes in place to ensure safe transition of equipment and transparency about where equipment ultimately goes.
Q: WHAT FACTORS SHOULD HEALTHCARE ORGANIZATIONS CONSIDER FIRST WHEN DECIDING WHETHER TO REDEPLOY, RESELL, RECYCLE OR DISPOSE OF MEDICAL EQUIPMENT?
Lynskey: The first question should always be: Does this asset still have clinical or operational value? Redeployment within the system is often the fastest ROI. Next is condition, serviceability, parts availability and regulatory status. After that, market demand and resale potential come into play. If the device has no redeployment or resale value, then recycling and responsible disposal are the right move. The key is having a structured decision framework instead of making emotional or convenience-based calls.
Arcadi: Choose a trusted equipment partner and stick with them on the front end of an equipment purchase, during the useful life of the asset and when trading it in for a newer piece of equipment at the end of its useful life.
Thomason: would start with alignment. Healthcare organizations exist to improve health outcomes. Equipment donation is an opportunity to extend that purpose beyond your walls. Next, take a realistic look at
Kevin Lynskey HERO Business Inc.
Ric Arcadi Image One Medical Group LLC
Janet Thomason Project C.U.R.E.
One of the biggest mistakes is equating “no longer right for us” with “no longer valuable.”
net financial impact. What are the actual net proceeds after broker fees, logistics, refurbishment, staff time and storage costs? In many cases, resale yields less than expected once all costs are accounted for. Donation can provide taxdeductible value while also advancing community benefit goals and ESG commitments. It also eliminates warehousing costs and frees up space quickly when working with the right nonprofit partner. Don’t forget about operational efficiency. Does your disposition partner provide pickup, documentation and streamlined logistics that quickly free up valuable space and staff resources? And finally, consider supportability. Is the equipment serviceable? Are parts available? Responsible nonprofit partners assess these factors before accepting your donation to ensure equipment strengthens health systems rather than burdens them. A fundamental guideline – would you feel comfortable using this equipment on someone you love.
Q: WHAT OPPORTUNITIES EXIST TO RECOVER VALUE FROM RETIRED OR SURPLUS MEDICAL EQUIPMENT?
Lynskey: There’s more value sitting in hospital back rooms than most people realize. Resale of complete systems, harvesting high-demand parts, redeploying accessories and refurbishing select assets can all drive real dollars back into capital budgets. Clinical assets like beds, stretchers and specialty patient care equipment often represent some of the highest return opportunities when managed correctly. When disposition is done strategically, it becomes a revenue recovery program instead of a cost center.
Arcadi: Properly maintain it during its life and knowing the sweet spot of the asset’s trade-in value a few years ahead of time.
Thomason: There are three kinds of value to think about. First is humanitarian value. The Lancet Commission on Global Surgery reported that five billion people lack access to safe, affordable surgical and anesthesia care. Equipment plays a central role in closing that gap. Reliable operating tables, lights, anesthesia machines – these aren’t luxuries; they’re prerequisites for safe care. Second is environmental value. Extending the life cycle of medical equipment reduces waste and aligns with circular economy principles. Healthcare generates significant surplus globally, and responsible reuse keeps usable technology out of landfills. For us, sustainability is a beautiful by-product of what we do, however our focus is building stronger healthcare systems. Third is financial and reputational value. Donation can generate tax benefits and demonstrates to stakeholders – from employees to patients to boards – that your
Join us April 15 for the Roundtable webinar! webinarwednesday.live
organization is committed to health equity and responsible stewardship. Value recovery is bigger than resale dollars.
Q: WHAT ELSE SHOULD TECHNATION READERS KNOW ABOUT EQUIPMENT DISPOSITION AND RECYCLING?
Lynskey: This is not just about getting rid of stuff. It’s about protecting patients, safeguarding data, supporting sustainability goals and being good stewards of hospital resources. When HTM teams own this process or partner with the right experts, it becomes a powerful extension of the department’s value. At HERO, we believe disposition should be transparent, documented, compliant and financially smart. If it feels messy, unclear or risky, that’s a sign the process needs an upgrade.
Arcadi: Learning the various “use & hold” strategies for buying, using, servicing and capitalizing on the asset at the end of life. You can go shorter term life and maintain it less, or you can invest in proper service and extend the life of the asset for 5 or more years
Thomason: Discarding equipment without evaluating its potential impact should truly be the last step. Well placed donations are done responsibly. Equipment should be tested, matched to validated needs, and placed with facilities that have the capacity to use and maintain it. When done well, equipment donation strengthens health systems and expands access to care. At Project C.U.R.E., our model is built around needs assessments, biomedical testing and careful placement – because our goal isn’t simply to move equipment. It’s to ensure healthcare for people who otherwise might go without it. Disposition isn’t just an operational decision. It’s a strategic one – with implications for global health, sustainability and your organization’s legacy. For more information about Project C.U.R.E. visit projectcure.org/.
Flexible
Inspection Scope Partnership in Every Pixel
The
brings
From capturing detailed lumen images to building complete inspection workflows, Healthmark stands with you every step of the way. The Flexible Inspection Scope pairs precision optics with a full network of support—including a team that customizes implementation and training to ensure your success. Because when it comes to borescopes, it’s more than pixels that matter—it’s partnership.
• A niche job board for the HTM and imaging communities powered by TechNation.
• 4000+ actively looking biomedical and imaging professionals.
TECHNATION TIMES TECHNATION TIMES
Breaking News:
» Completely free and confidential registration and application process.
• The fastest growing HTM talent network in the country.
• 350+ open opportunities throughout the United States.
htmjobs@mdpublishing.com for posting inquiries
htmjobs.com to register today
» A variety of posting options ranging from single-job postings to 12-month unlimited memberships.
“My HR department advertised on various government sites and our web site but we did not get a single applicant in over 120 days. Fairbanks Alaska is hard to recruit for but I took out an ad on HTM Jobs and got two good applicants in less than 30 days. I am hiring them both. Thanks HTM Jobs.”
Featured Employers: Agiliti, Block Imaging, Intelas Health, Renovo Solutions, Trimedx and more!
- D. Anderson, Tanana Chiefs Conference
Top Tech Dangers: ECRIS TOP 10 HEALTH TECHNOLOGY HAZARDS FOR 2026
BY K. RICHARD DOUGLAS
The Hippocratic oath, in more modern times, the Declaration of Geneva, serve as a moral compass, reminding doctors to focus on the whole person, not just the disease, and to balance science with compassion. Most people relate the term “first, do no harm” with the original. This is the patient’s wish that clinicians will treat them as they might treat a family member.
Despite this wish, every year harm does come to patients; not intentional, but because of mistakes, misused technology or misinformation.
Technology may have been developed into applications that can reduce some harms, but technology also introduces new hazards that didn’t exist before.
Every year, ECRI produces a Top 10 Health Technology Hazards report that sheds light on the potential dangers that the healthcare community and patients should be aware of going forward. The organization also offers tips for reducing the risks that these hazards pose.
ECRI’s list for 2026:
1. The Misuse of AI Chatbots in Healthcare
2. Unpreparedness for a “Digital Darkness” Event
3. The Growing Challenge of Combating Substandard and Falsified Medical Products
4. Recall Communication Failures for Home Diabetes Management Technologies
5. Tubing Misconnections Remain a Threat Amid Slow ENFit and NRFit Adoption
6. Underutilizing Medication Safety Technologies in Perioperative Settings
7. Deficient Device Cleaning Instructions Continue to Endanger Patients
8. Cybersecurity Risks from Legacy Medical Devices
9. Technology Designs or Configurations That Prompt Unsafe Clinical Workflows
10. Water Quality Issues During Instrument Sterilization
ECRI states that their annual hazards report “reflects our judgment about which risks should be given attention now to help care providers, device manufacturers, and others prioritize their patient safety efforts.” The organization points out that the information in the report can help avoid or minimize risks through careful management of technologies. Beyond the impact of bad health information, that can affect everyone, this article explores some of the hazards that might involve HTM with the help of ECRI experts.
IT’S NOT WITHOUT ITS FAULTS
While AI may be a significant leap forward in technology, concerns about the misuse of AI chatbots can leave patients with misinformation that could result in life-or-death decisions.
One AI developer even runs commercials boasting about a chatbot’s ability to guide patients with medical decisions, but patients may get a false sense of security from information that is not always reliable. Should warnings be required to inform patients that they should not rely on AI information? If yes, how could this be achieved? Should this warning be directed at the patient? Where would it originate?
“ECRI advocates for both approaches – responsible use and appropriate expectations by the end user (whether a patient or healthcare professional) and developers including as many safeguards as possible. There may be technical differences, as some vendors provide development environments (such as NVIDIA), while others deliver a final product (such as OpenAI or Google). Regardless of the delivery method, warnings should be placed appropriately,” says Christie Bergerson, Ph.D., consultant and AI subject matter expert at ECRI.
She says that some large language models (LLMs) have begun including warnings that they should not be used for medical advice and that users should consult a physician; however, similar to cigarette warnings, these are likely often ignored.
“From ECRI’s perspective, relying primarily on end-user warnings is not an effective way to manage AI-related risk in healthcare, although it is better than having no risk-mitigation strategies in place. The FDA has long recognized that written warnings and disclaimers – referred to as “labeling” – are among the weakest forms of risk mitigation and should not be relied upon when more robust design or system-level controls are feasible,” Bergerson says.
She says that this is especially relevant for AI systems, where fluent, authoritative-sounding outputs can easily override generic disclaimers, particularly in high-pressure clinical settings. Warnings to users may be necessary, but they are insufficient on their own; safety must be designed into AI systems rather than delegated to end-user vigilance. Should physician-centric organizations or the AMA be tasked with originating these warnings?
“Multiple national organizations and associations are actively addressing the issue of artificial intelligence from a range of perspectives and have produced publications offering recommendations. ECRI has repeatedly flagged concerns related to AI over the last few years precisely because we want everyone in the healthcare ecosystem – patients, providers and technology developers – to balance risk and reward in the use of AI,” Bergerson says.
Cyberattacks
are not the only entry point for a digital darkness event
INFORMATION DISRUPTION
Technology remains in the spotlight as ECRI warns of “digital darkness events” and another scenario wrought by technology, and our reliance on it, that may not have existed in the past. The danger involves losing access to electronic systems and patient information. This can occur because of a natural disaster or a cyberattack. How can HTM be prepared for one of these events?
“Cyberattacks are not the only entry point for a digital darkness event. Cyberattacks, natural disasters and other unaccounted for outages all pose equally high risk for a digital darkness event. Many existing safeguards in place solely focus on cyberattacks. While cyber incidents are often the first scenario considered, preparation must also address events such as natural disasters, power outages or other events that cripple critical infrastructure, technology and communication systems,” says Scott Luney, cybersecurity consultant, lead at ECRI.
He says that for healthcare technology management specifically, the cause of the event is less important than proactive preparedness to ensure timely and successful recovery. HTM departments, in coordination with other leadership in IT, cybersecurity, and other stakeholders, should have well-defined disaster recovery and business continuity plans in place, including clear instructions for how to enact business recovery efforts.
Luney says that components of disaster recovery planning should include, but are not limited to:
1. Alternate communication systems between staff, technicians, and leadership. If phone, cellular or Internet service is down, satellite communications (phones or Internet) can be a viable interim solution.
2. Redundant cloud data locations. Many organizations rely on cloud solutions, which are very susceptible to digital
darkness events. As a result, many cloud providers such as AWS, Google, and Microsoft all offer redundant hosting in alternate regions.
3. Alternate care sites. In hospital settings, cost may be a factor, but the ability to operate an additional triage or treatment “hot site” could help maintain some level of patient care capacity.
4. Data integrity. Disaster planning should include regular intervals of data backup and then tests of data restoration ability. If a darkness event destroys a physical data center, having that data backed up/replicated elsewhere is critical to continued operations.
5. Data availability. Along with potential “hot site” clinics, establishing “hot site” technology locations supports access to organizational data in an event, allowing staff to access systems such as cloud-based EMRs from a remote site.
MAINTAINING COMMUNICATIONS FOR DIABETIC HOME CARE
ECRI points out that technological advancements have improved home diabetes management. However, the organization warns that if there is a product recall or update for a device in home use, it may not reach patients and caregivers in a timely manner.
This can present dangers such as an “integrated insulin pump could overdeliver insulin” or “sensors on a CGM could yield incorrectly high glucose readings.”
“Sometimes, important product safety information does not reach patients and caregivers in a timely manner; and sometimes the information they receive is not sufficiently clear, leaving them unsure how to respond. ECRI’s report encourages providers and equipment suppliers to work toward improving the notification process. That said, there are
steps that patients and caregivers can take as well,” says Bradley Bonnette, senior project engineer at ECRI.
Bonnette provides these examples: Register your medical devices with the vendor. If you get the devices/supplies from a third party (typically a DME), reach out to them to understand how recall notifications will be communicated and stay informed. Get involved with communities of other users, who often share recall and safety information.
UNPATCHED AND VULNERABLE
Cyberthreats continue to be a concern for healthcare systems and those tasked with defending against them. ECRI points out that legacy medical devices are a particular concern. These older devices, that aren’t updated with the latest security updates, pose a vulnerability.
In recent years, with the advent of hybrid roles in the HTM department, the role of reviewing legacy equipment and possibly removing it from the network, has been a focus. What information can HTM use to address these vulnerabilities?
“Legacy devices can include aging technology, but also encompass any device, regardless of age, that cannot be successfully patched or updated by the vendor or manufacturer,” Luney says.
He says that guidance around legacy devices has remained largely consistent around making sure the devices are not “attackable” in their degraded state.
Luney says that if a device can be taken off the network and still operate to full capacity, that would be the preferred approach.
“If a device must be on the network, but has open vulnerabilities, it should be segmented so that only the core functionality is enabled, and it cannot communicate with outside networks,” he says.
Luney says that if a device can be upgraded or replaced, whether on a predictive replacement schedule or other opportunity to replace, that is desirable. However, budget constraints and the possible lack of suitable replacement devices on the market may limit this option.
“Physical security of devices is also a risk consideration. If a
legacy device is in an insecure state, it must be physically protected by storing securely in a locked location, and any data must be extracted and deleted from the device prior to storage,” Luney adds.
PURE WATER FOR PATIENT SAFETY
ECRI has identified a risk in the ability to maintain sufficient water quality during instrument disinfection or sterilization. This risk could expose patients to dangerous pathogens. Is there a role that the biomed department plays in maintaining water purity standards?
“Maintaining appropriate water quality in sterilization and reprocessing is an interdepartmental endeavor, and not something that biomedical engineering departments can achieve on their own. Rather, the biomedical engineering department should team up with infection prevention, sterile processing, facilities, surgical suite, and senior leadership members to ensure that they have the needed expertise and resources,” says Mairead Smith, principal project engineer at ECRI.
She says that if biomed departments find that their organizations are not working to adhere to ANSI/AAMI ST108, they can take the lead in establishing a multidisciplinary team and can continue supporting the team’s efforts to adhere to the standard over time.
“Members of the biomed department may have an advantage in that they are more likely to be members of AAMI – the organization that developed the ANSI/AAMI ST108 standard on Water for the Processing of Medical Devices. Through AAMI, they are likely to have access to guidance, resources, and community support to help them navigate water quality issues and adherence to the standard,” Smith says.
As technology aids clinicians and HTM professionals in improving workflows, identifying problems and working more efficiently, it also introduces new concerns that must be addressed. ECRIs annual health technology hazard report brings many of these concerns to light to protect patients and alert caregivers.
Christie Bergerson Consultant and AI Expert
Bradley Bonnette Senior Project Engineer
Scott Luney Cybersecurity Consultant Mairead Smith Principal Project Engineer
THE FUTURE Perspectives from a Seasoned Clinical Engineer
BY CAROL DAVIS-SMITH
Being a clinical engineer isn’t for the faint of heart. Ask the UCONN clinical engineering interns. They will tell you it’s demanding, confusing, intimidating, exciting and inspiring all at the same time. I could not be more proud of them for realizing and articulating this so early in their careers. But then, not everyone gets to be a UCONN clinical engineering intern. These young people are driven and it’s my job to be their initial compass.
In my January column, I shared a glimpse into Clinical Engineering Week. Today, I’ll pull the curtain back a bit further. This past February, we met on the UCONN Storrs campus. Beautiful but frigid.
Our 3½-day agenda included video calls with speakers sharing their career journeys along with education about their current fields of practice – i.e., specialties. I can assure you their silence and/or hesitancy to ask questions was not indicative of their interest. They were inspired and intrigued. They were processing. I know so, because they asked questions afterwards like … “Would it be okay if I reach out to [insert name]?” Ok, so the interns didn’t hear the speaker say they would provide their slides and to reach out if there are questions later. The point is, the interns heard the message and were internalizing it. Mission accomplished!
Accomplished professionals are great, but recent alumni graduates with full-time jobs and full-time paychecks is in another league – especially in these chaotic times. For decades, the program’s alumni have supported the program directly as internship hosts and guest speakers. When I first
arrived on the scene, I invited alumni from across the ages to speak with the interns (in person and/or via video call) to share their experiences and wisdom related to the topic of finding a job. Great advice! However, in the past few years, it became apparent that the world was changing and the nuances of finding a job – especially that elusive first job –were different. So, this year, I invited last year’s graduates. Again, a great experience. The interns asked great questions and the recent graduates answered like seasoned pros. I was pleasantly surprised (OK, maybe not) how poised these individuals were given their aversion to public speaking the year before. Another mission accomplished.
I’m not one to rely on traditional resources such as the campus Career Center. I didn’t as a student nearly 40 years ago. I don’t now. Why? Because department budgets and the talented individual bandwidths are stretched everywhere, so specificity of expertise becomes thin. This is especially true for niche professions like clinical engineering. So instead, invite colleagues who are accomplished in their own rights as human resource professionals. Some provide guidance on resumes and interviewing, while a very specialized colleague explains the components of a “total rewards” package – i.e., the job offer. Then, to complement these presentations, we talk. We have discussions over lunch that the interns refer to as “Carol’s life hacks.” How does PTO really work? How should invest? Like a good clinical engineer, I frequently respond with “It depends.” That leads to deeper conversations during which interns offer their own perspectives based on their parents, social media and occasionally their own experiences. Other interns sit quietly and seem disengaged or maybe working on a class assignment due later that
evening. Nope. Most of them are listening. Processing. I know this because they ask thoughtful questions later. I also want to send a shoutout to our colleagues in the VA HTM program. Some of them host our interns. Some of them would like to host our interns but budget constraints hamper them just like in the private sector. Leaders in the VA HTM community still show up to present their HTM structure and “day in the life” information along with guidance around how to apply to positions. Like so many other aspects of healthcare and HTM, their world is exactly the same as ours but completely different.
Of course, I also include presentations from the American College of Clinical Engineering (ACCE) and the Association for the Advancement of Medical Instrumentation (AAMI).
The presenters focus on why clinical engineers should become members, especially as students. I take time to talk with the interns about how the organizations are complementary and can support their careers in very different ways. While this may seem obvious to us seasoned professionals, it absolutely is not to anyone new to our community.
Last, but certainly not least, are the workshops. I’ve supported, planned, and organized numerous conferences and conference-like events over my career. You would think I’d know what I was doing when planning Clinical Engineering Week. Well, I made plenty of mistakes – some within my control, others completely outside my influence much less my control. The workshops, for the most part, have been a success. The magic of workshops is the peer-to-peer engagement. The disruption to just sitting there while “talking heads” ramble on the screen. The movement from one physical space to another. Even if it’s just across the room. Workshops are sort of the adult education version of “labs” in engineering school. You test theories. You test your understanding of those theories. And maybe best of all, workshops behave like purposeful networking.
Some workshops address a typical problem or assignment a clinical engineer might be asked to complete.
Yes, the underlying theory is presented within their academic courses but plays out sometimes very differently across the health systems where they complete their internships. Remember, hospitals (and health systems) are exactly the same and completely different. In the workshop, interns are grouped so that they must consider diverse perspectives. In the end, they can take home real-world ideas to their host health systems.
One workshop that has become a favorite is the Puzzle Game. It requires inexpensive puzzles, tables and creativity on everyone’s part but especially the facilitator. If the tables vary in size, shape and height that adds to the challenge. The size of the group obviously affects the complexity. The objectives are too many to go into here and, honestly, are somewhat dependent on the players. Yes, I am being protective of the workshop details to allow future interns the full experience. The call to action is – leverage adult learning practices. As formal or informal educators – I’m talking to you, CE managers and directors – we need to learn and develop new knowledge and skills that meet the developmental needs of the next generation of HTM professionals, not to mention the next iterations of medical technology and healthcare delivery.
Graduation and conferences are ahead of us. No doubt those will bring more teaching and learning opportunities. I suspect I will find myself on both sides of those opportunities. Until then, feel free to reach out to me if you have questions or suggestions. And don’t forget to read about the great things Steve Yelton (Cincinnati State ) and Joie Marhefka (Penn State New Kensington) are doing with their students!
Carol Davis-Smith, MS, CCE, FACCE, AAMIF, is the director of the clinical engineering internship program at the University of Connecticut. She is also president of Carol DavisSmith & Associates LLC.
CLICK. WATCH. EARN!
APRIL 1
SPONSORED BY
TOOLS OF THE TRADE
Save the date for this live webinar. Participation is eligible for 1 CE credit from the ACI.
TOOLS OF THE TRADE PartsSource PRO: Smarter Parts Procurement for HTM Teams
ROUNDTABLE ON Toolkits, Cases and Carts
SPONSORED BY AI and tech innovations HTM teams need to succeed
WHow to Use MedWrench for Career Growth
BY JAMES LINTON
hen people think about MedWrench, they usually picture troubleshooting threads or the manual library. Those are powerful, but if you stop there, you’re missing one of the platform’s biggest values: career growth.
MedWrench isn’t just a place to fix devices – it’s a place to build your reputation, expand your network and position yourself for the next step in your professional journey.
I suggest thinking of MedWrench as more than a technical resource. It’s a stage where you can demonstrate your expertise, a classroom where you can keep learning and a networking hub that can connect you to opportunities you didn’t even know existed. Here’s how to use it deliberately to grow your career.
1. Build visibility through consistent contributions Career growth often comes down to visibility. People need to know who you are and what you bring to the table. MedWrench gives you a platform to demonstrate that without self-promotion.
I suggest answering questions regularly, even if your answer is partial. Over time, people notice who consistently contributes. That reputation can lead to mentorships, collaborations and even job offers. Think of every post as a micro-resume: it shows how you think, how you communicate and how you solve problems. Too often people think they need to join formal groups or committees to build their resume/brand, when this grassroots type of approach works as well.
2. Showcase your expertise in a specific niche
Every technician has strengths. Maybe you’re great with imaging, or you’ve mastered anesthesia equipment, or you’re the go-to for infusion pumps. I suggest leaning into that niche on MedWrench. Answer questions in your specialty, share manuals and post tips. When people see your name consistently associated with a certain device family or modality, they start to
think of you as an expert in that area. That reputation can translate into real-world opportunities: being asked to lead training, being recruited for specialized roles or being invited to speak at conferences.
3. Learn from the community to stay current HTM is a fast-moving field. New devices, new regulations, new technologies – there’s always something changing. I suggest using MedWrench as a way to stay current. Read threads about devices you don’t work on yet or maybe have on order. Follow discussions about certifications, cybersecurity and AI in preventive maintenance.
Even if you’re not ready to contribute in those areas, you’re building awareness. That awareness makes you more adaptable and more valuable to employers. It also helps you spot trends early, so you can position yourself for where the field is going, not just where it is today.
4. Use the forums as a portfolio of your thinking Unlike a resume, which lists what you’ve done, the forums show how you think. Employers and managers value technicians who can troubleshoot systematically, communicate clearly and collaborate respectfully. Every time you post, you’re demonstrating those skills.
I suggest treating your forum contributions as part of your professional portfolio. If you’re applying for a new role, you can point to your activity as evidence of your engagement with the field. It shows that you’re not just clocking in and out – you’re part of the professional community. Also, if someone searches your name online and a list of helpful threads pop up then a potential employer may just move you to the top of the pile.
5. Network without the awkwardness Networking can feel forced at conferences or on LinkedIn. On MedWrench, it happens naturally. You connect with people by solving problems together. Over time, you’ll recognize names, build trust and maybe even move conversations offline.
I suggest reaching out when you notice someone consistently posting in your specialty. A quick message of thanks can turn into a professional relationship. And because the connection started with real work, it feels authentic.
6. Find mentors and become one Mentorship is one of the most powerful drivers of career growth. On MedWrench, mentors and mentees find each other organically. If you’re new, you can learn from
experienced Gurus who share our insights openly. If you’re experienced, you can mentor by answering questions, sharing resources and guiding newer techs. suggest embracing both roles. Learn from those ahead of you and teach those coming up behind you. That balance not only accelerates your growth but also strengthens your reputation as someone who contributes to the field.
7. Leverage MedWrench for leadership skills
Career growth isn’t just about technical expertise – it’s also about leadership. The forums give you a chance to practice leadership in small ways:
• Framing your answers clearly.
• Mediating disagreements respectfully.
• Encouraging new voices to participate. suggest treating these interactions as practice for leadership roles. The same skills you use to guide a forum discussion translate directly to guiding a team in the shop. Also for those new to using English, it can be a great tool to learn and express yourself in a technical manner.
8. Spot opportunities you wouldn’t find elsewhere
Sometimes career opportunities come from unexpected places. A vendor might notice your consistent contributions and reach out. A manager might see your expertise in a thread and think of you for a role. A peer might invite you to collaborate on a project. suggest staying open to these possibilities. Don’t use MedWrench just to solve problems – use it to plant seeds. You never know which connection will grow into your next opportunity.
FINAL THOUGHT
MedWrench is more than a troubleshooting forum – it can be a career accelerator. By contributing consistently, showcasing your niche, learning from others, networking authentically, and embracing mentorship, you can use it to grow in ways that go far beyond fixing devices. I suggest treating your time on MedWrench as an investment in your future. The more you give, the more you’ll get back – and the stronger your career will become.
James Linton, MiM, PmP, Cmbb, AAMIF, is a biomedical engineering technology professor/coordinator with St. Clair College.
CYBERSECURITY
AI and Cybersecurity: Understanding Risk and Opportunity
BY ARLEEN THUKRAL, M.S., CCE, CHTM
Artificial intelligence is rapidly transforming the cybersecurity landscape across health systems. For healthcare technology management (HTM) professionals, AI introduces powerful new capabilities – advanced anomaly detection, autonomous device monitoring and riskbased prioritization – that help reduce response times and uncover subtle threats human analysts may never see. These tools allow cybersecurity teams to understand what changed, why it matters, and how to act quickly, reducing noise and sharpening decisionmaking. But while the benefits are substantial, the cybersecurity risks introduced by AI systems demand equal attention. Understanding those risks is now essential for every HTM leader responsible for safeguarding connected clinical environments.
Unlike traditional software, AI systems can learn from data, adapt to new inputs and can behave in ways that are difficult to predict or fully explain. This dynamic behavior introduces novel cybersecurity challenges that HTM professionals must now manage.
One of the most immediate concerns is the dramatically expanded attack surface created by AI integrations. AI tools draw data from multiple interconnected systems, external APIs, cloud-based inference service and model updates. Each component – whether a third-party library, data pipeline or remote model endpoint – represents a potential opening for exploitation.
Another significant category of risk revolves around prompt injection, especially in large language models (LLMs). LLMs can be manipulated through cleverly crafted input that overrides intended instructions. The risk is even greater in agentic AI browsers – tools capable of navigating websites and taking autonomous actions. In these scenarios, hidden malicious instructions embedded in a webpage can cause the AI assistant to navigate to a user’s
HTM professionals can harness the benefits of AI while protecting the safety of clinical systems.
logged-in accounts, extract sensitive information (such as email address or one-time password) and exfiltrate this data to an attacker’s server. These attacks succeed even when standard web security controls are functioning properly.
Another major category of AI-specific vulnerability involves poisoning the data used to train or update models. Toxic or manipulated training data can corrupt model outputs, leading to dangerous or clinically incorrect recommendations in healthcare AI systems. Similarly, federated learning models-which train on decentralized datasets are especially vulnerable because any participating endpoint can introduce hostile updates that skew or degrade the entire global model. In practical terms, this could mean a compromised medical device or untrusted external dataset silently influencing AI risk-scoring models, etc.
To prepare for this new frontier, HTM professionals should prioritize several key actions. First, strong governance frameworks must be established to oversee AI deployment,
data use and model change control. Transparency and auditability are equally important; clinical AI tools must be explainable enough to evaluate their decisions and root out malicious or erroneous behavior. Strengthening patch management and life cycle oversight for AI-enabled medical devices is essential, as well as improving visibility into AI dependencies across networks. Workforce training on AI risk and vendor collaboration is also vital; securing AI requests coordinated efforts across manufacturers, integrators and health system cybersecurity teams. By understanding these risks and developing the skills and structures needed to manage them, HTM professionals can harness the benefits of AI while protecting the safety of clinical systems.
Arleen Thukral, M.S., CCE, CHTM, is a VISN 2 Healthcare Technology Manager with New York/New Jersey VA Health Care Network.
The Massey Method Delegation Done Right: Developing Future Leaders in HTM
BY ERIC MASSEY
In healthcare technology management (HTM), delegation is often treated as a productivity tool. When leaders are overwhelmed, they assign tasks to reduce workload. While this may create short-term efficiency, it rarely builds long-term leadership capacity.
Effective delegation is not about clearing your calendar.
It is about building capability.
If HTM organizations want stronger bench strength, succession depth, and sustainable performance, delegation must become a structured development strategy not a reactive decision.
DELEGATION IS A LEADERSHIP MULTIPLIER
The most common mistake leaders make is asking:
“How do I get this off my plate?”
The better question is:
“Who needs to grow into this responsibility?”
Delegation, when done correctly, accomplishes three things simultaneously:
1. Expands the leader’s strategic capacity
2. Develops the team member’s competence and confidence
3. Strengthens organizational resilience
When done poorly, delegation creates confusion, rework and frustration.
The difference lies in structure.
In HTM, where complexity continues to increase and experienced leaders are in short supply, structured delegation is not optional. It is essential to long-term program strength.
“Ensure our monthly compliance reporting is accurate, on time and clearly communicated to the hospital leadership team.”
Outcome-based delegation requires four elements:
• Defined Result – What does success look like?
• Standard – What level of quality is required?
• Timeline – When must it be completed?
• Checkpoints – When will progress be reviewed?
This approach shifts ownership from execution to accountability.
FRAMEWORK 2: ALIGN RESPONSIBILITY WITH AUTHORITY
Delegation fails when responsibility exceeds authority. If someone is accountable for improving a performance metric, they must have clearly defined decision-making boundaries. Without authority, ownership becomes symbolic rather than functional.
FRAMEWORK 3: STRUCTURED OVERSIGHT WITHOUT MICROMANAGEMENT
Delegation does not eliminate leadership involvement. It changes the nature of involvement. Effective leaders monitor:
• Milestones
• Results
• Obstacles
They do not monitor every step of execution.
A simple oversight structure includes:
• Scheduled progress reviews
• Barrier identification discussions
• Feedback conversations focused on improvement The goal is visibility without interference.
FRAMEWORK 4: DEBRIEF TO ACCELERATE GROWTH
The development value of delegation is realized during reflection.
After completion, leaders should conduct structured debriefs:
• What worked?
• What did not work?
• What decisions were effective?
• What would be adjusted next time?
Without debriefing, delegation becomes repetition. With debriefing, it becomes leadership training.
FRAMEWORK 5: SCALE RESPONSIBILITY GRADUALLY
Leadership development is progressive. Start with contained responsibilities:
• Ownership of a defined metric
• Oversight of a specific workflow
• Coordination of a defined initiative
As capability increases, expand scope. Measured progression builds confidence while protecting operational integrity.
STRATEGIC IMPACT
When delegation is structured and intentional:
• Leaders move from operational bottlenecks to strategic drivers
• Teams become proactive instead of dependent
• Succession risk decreases
• Organizational performance stabilizes
In HTM, where complexity continues to increase and experienced leaders are in short supply, structured delegation is not optional. It is essential to long-term program strength.
FINAL THOUGHT
The objective of leadership is not to be indispensable. It is to build a team that performs consistently with or without direct oversight.
Delegation done right is not about efficiency. It is about multiplication.
Leaders who master this discipline do more than manage work. They develop the next generation of HTM leaders.
Eric Massey is the regional director of operations with Intelas and founder of The Massey Method.
NETWORKING NOTES
Computer Cleaning Tips
BY GARRETT SEELEY
There is an issue in the field that can make some people uncomfortable: dealing with dust. It is one of the least desirable aspects of repairing medical equipment, yet it is unavoidable. The problem is particularly heavy in the summer and winter months when people spend most of their time indoors.
Dust accumulates in any device that uses air cooling, especially if a fan is present. Removing dust is part of preventive maintenance, and it reduces the likelihood of faults. Beyond maintaining a clean environment, dust also poses a significant risk to the equipment by obstructing air-cooled systems. Most computer-based medical devices are air-cooled, and over
time, they can collect dust. So much so that their internal assemblies can often resemble that of a vacuum cleaner. This creates a significant risk of overheating and circuit damage, making it important to perform this task despite the challenges it involves.
DUST SOURCES & HEALTH CONCERNS
Dust is unhygienic and comprises of dead human skin, hair, mites, molds, bacteria, pollen, fabric fibers and airborne debris. Even the cleanest of environments can build up dust whenever people are present. Hospitals combat this with sealed clean rooms, HEPA filtration, independent air handling, and protective clothing like bunny suits and scrubs. These precautions protect the environment from human contaminants. Remember that healthy individuals could transmit infections to more vulnerable patients. These measures support hospital cleaning policies and are essential for any healthcare facility.
CLEANING TECHNIQUE
Because of this dust build up, regular disassembly and cleaning of air paths are required for most fan-cooled equipment. Always refer to the manufacturer’s guidelines for disassembly and cleaning instructions. Perform these tasks with the power off and the unit disconnected from AC or battery power.
For cleaning, use a static/ESD-resistant vacuum with a HEPA filter cartridge. Invest in a quality vacuum designed for electronics as they will be in use for years on delicate equipment. Vacuums with a blower option are best as they can help push out dust.
A good brush is also essential for dust removal. Choose ESD-safe brushes without metal or magnetic assemblies. Brush gently to avoid damaging components, allowing dust to flake off surfaces gradually. A vacuum can assist in removing this flaking dust as it falls out of the assemblies. Compressed air is the best tool for removing dust, but not all compressed air is suitable. High-quality ESD-safe electronic vacuums may have a reverse port for blowing air, which is ideal for flushing dust from a system. Hospital air can also be useful but accessing it can be challenging. If an air compressor is used, make sure to have a humidity trap to prevent condensation ejection. When using canned air, be cautious and use it upright. Propellants can be ejected and there is a risk of freezing, which can damage circuitry. Remove sensitive components like optical drives before using compressed air as dust may damage them.
DUST MUST GO SOMEWHERE
Expect dust to spread everywhere, especially when using compressed air. Therefore, clean the work area afterward. Avoid performing this task in front of hospital staff who might find it repulsive. The best place for dust removal is an enclosed, ventilated area like a painter’s booth, where dust can be instantly removed from the building.
WHAT TO FOCUS ON
The most vulnerable electronic components include large heat sinks, transistors, computer chips, power supplies and video cards – generally, components that supply or use the most power. Video cards and computer processors are particularly difficult to clean because of mounted fans. Avoid spinning the fans with a vacuum or compressed air. This could generate unsafe electrical charges that might damage the circuitry. This is how spinning one fan causes another in a different part of the unit to spin. Don’t do that. Always hold fans stable during cleaning to prevent them from spinning.
FILTERING AND PLACEMENT AS PREVENTION
Some filter materials are washable and reusable, but most HEPA-grade filters are not. Refer to the manufacturer for
guidance on cleaning filters. In general, HEPA filters should be changed regularly to remove unseen particulates. Finally, consider the unit’s placement; if an intake fan is located near the floor, it will suck dust from there into the system. Maintain an air gap between the floor and medical equipment to limit both dust intake and fluid intrusion.
SUMMARY
Dealing with dust is an unavoidable, yet critical, aspect of maintaining and repairing medical equipment. Accumulated dust, particularly prevalent during summer and winter, can obstruct air-cooled systems causing overheating and circuit damage. Hospitals strive to control dust through strict hygiene measures. Effective dust removal requires regular disassembly, cleaning of air paths and the use of tools such as ESD-safe vacuums, brushes and compressed air. The process should be performed carefully to avoid damaging sensitive electronic components. The clean environment should be swept and sanitized afterward. Proper filtering, unit placement and regular maintenance are vital in preventing dust accumulation. Dust removal ensures the efficient and safe operation of medical devices, underscoring its importance in biomed maintenance. Following these techniques will help reduce service incidents and possibly even extend the life cycle of the system.
Garrett Seeley is a Biomedical Equipment Support SpecialistImaging with VISN 17: VA North Texas Health Care System, U.S. Department of Veterans Affairs.
Solving Parts Procurement for Imaging Techs
The Challenge Of Availability And Compatibility
One of the most common concerns that repair technicians see is simply finding the required part. Whether it’s older machines with components no longer manufactured, or newer equipment with higher demand that backorders the part for weeks. Once a part is ordered, technicians need to ensure it’s compatible. A component might look right, but subtle differences in manufacturing runs or software versions can render it useless. Installing an incompatible part not only wastes time but can also risk damaging other components of the imaging system.
Scan QR code to view our complete list of products and services
Navigating Cost And Quality Concerns
The cost of OEM parts can be extremely high, putting a strain on operational budgets. This pressure often leads technicians to explore the third-party market, which introduces another major concern: quality. While a refurbished or third-party part typically is a fraction of the cost, if it fails prematurely, the initial savings are lost. Nothing hurts a technician’s credibility more than getting a DOA part and having the system down an additional day. To remain proactive, technicians must consider the cost-benefit against the potential risks of poor quality if there is no product warranty when sourcing parts.
Solutions For Smarter Sourcing
Overcoming these obstacles requires a strategic approach to parts procurement. The team at Probo Medical offers effective solutions to keep your equipment running smoothly with our high-quality, reliable parts. With locations around the globe,
Probo Medical offers a huge inventory of guaranteed parts for nearly every modality of diagnostic imaging. Our comprehensive quality assurance program includes inspection and testing of: CT, MRI, Ultrasound, Nuclear Medicine, Cath, C-arm, X-ray, BMD, PET and PET/CT, and Flexible & Rigid Endoscopes. Our expert harvesting departments test and certify all parts and accessories at our ISO 13485-managed facilities, as they follow stringent Quality Management System requirements. Plus, we offer same-day shipping, a six-month warranty, and free technical support with every part to ensure you get the most out of your repair. Our goal is to be the single, reliable source you turn to for any part or accessory. Our experienced team is here to help you find the right imaging parts for your specific equipment model. Whether you’re replacing a worn component or upgrading your system, we provide expert guidance and exceptional customer service every step of the way.
Downtime in diagnostic imaging is more than an inconvenience, it’s a critical issue that can delay patient care. For repair technicians, getting equipment such as ultrasound, MRI, and CT scanners back online quickly is the top priority. However, sourcing the right high-quality replacement parts often presents challenges that can slow down the entire repair process.
30 Years in Biomed Service:
What Has Changed – and What Hasn’t
BY NICOLE PALMER, VICE PRESIDENT OF OPERATIONS, MULTIMEDICAL SYSTEMS
Thirty years ago, biomedical equipment technicians were already experts at solving problems – but they were doing it without Google, without tablets, and often without a decent parts database.
Troubleshooting sometimes meant flipping through a binder the size of a phone book and hoping the page you needed wasn’t missing.
This year marks 30 years in business for MultiMedical Systems, and milestones like this have a way of making you look both backward and forward. The tools have changed dramatically. The expectations have changed even more. But some of the most important parts of this profession remain exactly the same.
THEN: FEWER DEVICES, MORE BINDERS
Thirty years ago, equipment fleets were smaller, and most devices were mechanically simpler. Preventive maintenance schedules were often tracked on paper – sometimes on clipboards, sometimes in filing cabinets, and sometimes in systems that depended heavily on someone remembering to update them.
Service records were handwritten. Communication happened by phone or fax. If you needed a manual, you probably walked over to a shelf rather than opening a browser.
Parts sourcing was slower but, in some ways, easier. Devices were less proprietary, and the pace of technological change was more forgiving. A technician could become deeply familiar with a model and work on it for years before it was replaced.
And while response times mattered then, just as they do
now, expectations were different. Facilities understood that some repairs simply took time.
In many ways, the work required patience – and a very organized filing system.
NOW: FASTER, SMARTER & MORE DEMANDING
Fast forward to today, and the landscape looks very different.
Medical devices now incorporate sophisticated electronics, embedded software and network connectivity. Troubleshooting may involve firmware updates, digital diagnostics and coordination with multiple vendors. A modern technician needs not only mechanical aptitude but also comfort with software and systems integration. Documentation expectations have also increased significantly. Facilities must maintain detailed service histories and compliance-ready records. Audits are more frequent, and the margin for error is smaller.
Customers expect visibility, communication and speed. Downtime is measured in lost revenue, disrupted schedules and potential impacts on patient care. Service providers are expected to respond quickly and communicate clearly at every step.
In short, the job has become more complex – and more critical – than ever.
FROM REPAIR VENDORS
TO STRATEGIC PARTNERS
Perhaps the biggest change over the past three decades is how service providers are viewed.
There was a time when many organizations saw thirdparty service primarily as a break-fix resource. If something failed, you called someone to repair it.
Today, the conversation is different. Facilities are looking for partners who can help manage equipment life cycles, plan budgets, maintain compliance and improve operational
efficiency. Preventive maintenance, asset visibility and long-term planning have become central priorities.
The role of the service organization has expanded accordingly. Technical skill is still essential – but organization, communication and operational discipline are just as important.
WHAT HASN’T CHANGED
Despite all the advances in technology and process, several truths about biomed service have proven remarkably durable.
TRUST STILL MATTERS MORE THAN ANYTHING ELSE.
Health care providers need confidence that the people servicing their equipment are capable, responsive and accountable.
PEOPLE ARE STILL THE DIFFERENCE.
Software can track assets. Systems can schedule work orders. But professionalism, judgment and pride in workmanship still come from individuals.
RESPONSIVENESS HAS ALWAYS MATTERED.
Even 30 years ago, a piece of equipment down in a clinical environment was urgent. The tools for responding may be faster today, but the urgency has always been there.
RELATIONSHIPS OUTLAST TRANSACTIONS.
Long-term partnerships are built on consistency, reliability and communication – not just pricing.
These fundamentals have not changed, and they likely never will.
LESSONS FROM THREE DECADES
If there is one lesson that stands out after 30 years, it is this: organizations that endure are the ones that adapt without losing their core identity.
Technology will continue to evolve. Regulations will change.
Expectations will increase. Service organizations must keep learning, keep improving and keep investing in their people and processes.
But the fundamentals – integrity, accountability and commitment to customer success – are timeless.
Those principles were just as important when service records were handwritten as they are today when everything is digital.
LOOKING AHEAD
The next decade will likely bring even more change. Predictive maintenance, data integration and greater connectivity will continue to reshape how service is delivered.
Even as the tools evolve, the mission remains the same: keeping equipment safe, reliable and ready when it matters most.
And while today’s technicians may rely less on binders and more on dashboards, one thing hasn’t changed at all – the satisfaction of solving a problem, restoring a device to service, and knowing that work helped someone, somewhere, receive care.
That part of the job is timeless.
“The
greatest impact of partnering with MMS is their willingness to work first to understand our needs and then work towards finding the right solution to meet them. The needs in our organization are diverse and MMS has the competencies to take on those challenges from scheduled and unscheduled maintenance to specialized project work. It’s wonderful to have a one-stop-shop that we can call when we need it.”
Perry
Nicole Palmer, Vice President of Operations, MultiMedical Systems LLC
RIGHT TO REPAIR
Why is Medical Equipment Legisltaion Difficult to Pass?
BY GAY GORDON-BYRNE
ur Coalition of repair supporters have been able to pass laws in a dozen states making sure their residents can repair the things they own. Most everything made with high-tech parts is covered by at least one law other than for medical equipment. Right to Repair (R2R) has been introduced in all 50 states, multiple territories and federal versions are being filed for Military R2R, Farm R2R, Auto R2R and most everything else.
Politicians love promoting repair of tractors, cars, cellphones and “consumer” electronics but continue to balk at enabling more competition for repair of medical devices. Why? I suggest that while legislators are now confident that a cellphone or refrigerator repair won’t do great bodily harm – they lack confidence for things they don’t understand or never see. All a medical equipment manufacturer needs to do is suggest patients will die and political brains freeze.
Legislative brain freeze is hard to fight. It takes time for supporters to meet with legislators and get their attention for two minutes, never mind enough time to fully explain the medical equipment regulatory environment to a disinterested audience. While we know we have a great issue – there are hundreds of other issues demanding attention from the same people. We aren’t fighting OEMs as much as we are fighting for attention on a crowded calendar.
The uphill battle isn’t technical – it’s about money. OEMs tell legislators that price isn’t supposed to enter into medical repair choices, but price needs to be a consideration. OEMs have fought to make sure to promote the idea that any price is acceptable if it comes from the OEM because it is “the best.” A renewed focus on affordability might allow administrators to “sweat” their assets and make sure they get the most out of their scarce technology budgets. Overpriced repair isn’t better repair – it’s just overpriced.
The discussion of money is an advantage for consideration of Right to Reapir, which is why OEMs are so anxious to avoid the discussion. Repairing things not only keeps products in use and out of the dump but reduces the need for buying replacements. We know from the computer industry that late model (n-1) equipment is almost always suitable for years
beyond the initial warranty period. Pushing early replacements helps keep new revenue flowing even without any technological advantage. Even if there were a technical advantage – the choice of what to purchase still belongs to the owner and not the OEM. One of the main reasons that R2R has become so popular is the long-standing rights of owners to control their property.
I met with a legislator last week who runs a pregnancy clinic. She has to buy new ultrasounds every five years in order to get access to maintenance materials regardless of any decline in image quality. The provider should have agency over how often to replace their equipment – not the OEM refusing to sell repair materials. For example – even if well-meaning – states do not allow car dealerships to write requirements that customers must buy new cars every 5 years. The same prohibitions on unfair and deceptive contracts fit perfectly to ban this OEM overreach.
OEMs can then raise repair prices to make replacement purchases attractive relative to repairs ignoring the fact that the initial purchase was not competitive due to trade-ins and other incentives. Acquisition of medical equipment is a rigged game. So much so that the only body powerful enough to break the stranglehold over pricing is the legislature.
There are other factors as well – such as lack of experience with medical equipment on the part of legislators and staffers. Patients don’t see repair techs at work – so the process is more mysterious for constituents than it is for auto repair. I have met only one legislator out of hundreds whose day job was a hospital administrator. He got a bill moving very easily in Illinois because he could explain the rules around making repairs. Once he left office – no one carried the ball. Perhaps a TV show like “The Pitt” will show a repair tech working to fix a ventilator in real time or for an OEM tech being unavailable at any price.
Lack of experience permeates the lobbyist community as well. Lobbyists are hired for the people they know – not what they know. We try hard to make sure our lobbyists are provided with the best background information possible so they don’t have to make stuff up. Biomeds have been able to provide important expert testimony when we can match their schedules to the random schedules of hearings. Most people have never seen or met a BMET because their jobs are behind the scenes.
Lastly, there is the “whopper” factor when OEMs promote ideas that are preposterous with a straight face. For example, we’ve heard testimony that if Right to Repair were to become law, heart patients would fix their own pacemakers. I’m not kidding. The scary part is that legislators in the hearing were not laughing out loud. Medical equipment repair was stricken from the bill in minutes.
Anyone that has a repair story to tell about medical equipment can do so at any time using our advocacy widget. Go to https://www.repair.org/ stand-up to use our free advocacy tool to reach your legislators directly.
A phone call is even better. Your voice as a constituent and also an expert is powerful. We do not sell our lists and do not want any personal information.
Diagnostic Solutions is a customer service based parts provider that specializes in all imaging modalities and manufacturers.
Created to offer hospitals and ISO’s a cost effective and time saving solution for ordering imaging replacement parts, equipment moves, ultrasound probe repair, and onsite service.
Gay Gordon-Byrne is Executive Director of the Digital Right to Repair Coalition
BIOMED BRAINBUSTER
Showtime!
1. On average, how many sunny days
2. What famous actress was born in Scottsdale?
A. Emma Stone
B. Scarlett Johansson
C. Kerry Washington
D. Julia Roberts
3. How long can a cactus go without water?
A. 30 days
B. 1-2 months
C. 2-4 months
D. 4-6 months
4. Before settling on the name Scottsdale, what was the area almost named?
A. Orangedale
B. Augustine
1 2 3 4 5 6 7
STROLL DOWN OLD TOWN SCOTTSDALE
Scottsdale’s historic Old Town features western-themed stores alongside locally curated art galleries, decadent restaurants, and a rich nightlife.
TEE OFF AT BREATHTAKING GOLF COURSES
It is home to some of the most worldrenowned golf courses, each of which ranges in difficulty and offers unique glimpses of Arizona’s natural landscape.
MCDOWELL SONORAN PRESERVE
Visit this vast natural area that covers over 30,000 acres of protected desert land, making it one of the largest urban preserves in the United States.
HIKE THE SCENIC CAMELBACK MOUNTAIN
Named for its shape, it’s a popular destination for hikers and outdoor enthusiasts looking for an epic desert landscape.
CATCH A BASEBALL GAME
Salt River Fields at Talking Stick is a stateof-the-art baseball facility that functions as the home of the Arizona Diamondbacks and the Colorado Rockies.
HORSEBACK RIDING AT MACDONALD’S RANCH
Beyond horseback riding, you’ll also be able to enjoy more activities like hayrides, stagecoach rides, cowboy games, and guided desert tours.
GO WINE TASTING
Wineries not to miss include LDV Winery, Carlson Creek Vineyard, Merkin Vineyards, and Arizona Stronghold Vineyard.
HTMA-OH SCRAPBOOK
The Healthcare Technology Management Association of Ohio recently held its 2026 HTMA-OH Conference and Expo on Feb. 5-6, 2026, at the Renaissance Hotel and Conference Center in Westerville. The two-day event brought together healthcare technology management (HTM) professionals, industry leaders and solution providers for education, leadership development and networking. The conference also featured a keynote presentation, leadership development workshop, multiple educational sessions, roundtable discussions and an expansive exhibit hall.
1. A strong lineup of industry leaders joins HTMA-OH President Ryan Gonzalez on stage.
2. The Leadership Development Course features Carol Davis-Smith helping leaders turn vision into actionable strategy.
3. A standing-room crowd gathers for the 2026 keynote with Bryant Hawkins, founder of Elevate HTM.
4. Attendees connect and collaborate during a networking break.
5. A full exhibit hall comes alive with buzzing conversation and collaboration.
7. Attendees invest in their expertise while earning continuing education credits.
8. HTMA-OH served up connections and competition at the Smash Park social event.
6. Jayme McKelvey and Megan Cabot connect with attendees while sharing the latest issues of TechNation.
INNOVATIVE RADIOLOGY SCRAPBOOK
Innovative Radiology, founded in 2016, recently celebrated the grand opening of its new location in Gallatin, Tennessee.
The10,000-square-foot facility is a perfect complement to Innovative Radiology’s 45,000-square-foot facility in Conyers, Georgia. Innovative Radiology provides high-quality imaging equipment and parts through a commitment to rigorous testing, sourcing and service. The Gallatin space focuses on mammography and women’s health. The facility tests detectors for patient care to ensure they are fully functional when they leave.
2.
1. Kyle Hall cutting the ribbon at our Gallatin grand opening, marking an exciting milestone for Innovative Radiology as we celebrate continued growth and expansion.
Gallatin Testing Bays.
3. Josh Glas and Kyle Hall presenting John Dimarzo his award for winning Biggest Impact Player of 2025.
4. Courtney, Rika, Kristen, and Kim enjoying conversation at the Gallatin Grand Opening.
5. Josh Glas and Mike Ragan after Mike was presented his award for Top Performer for 2025.
6. The Innovative Radiology Team at the Gallatin Grand Opening.
7. Tommy Paker and Aaron Stanley eating the grazing spread provided by Courtney Lancaster.
8. Kyle Hall and Josh Glas giving their gratitude to the team for their tremendous effort for planning the Grand Opening.
9. Attendees at the Grand Opening enjoying conversation.
10. Bobby Steele, Rob Steele, Josh Glas, and Mike Ragan at the Grand Opening.
844-4RENOVO
Rytex Industries rytexindustries.com
Education/Training
College of Biomedical Equipment Technology cbet.edu • 210-233-1102
Maull Biomedical Training maullbiomedicaltraining.com • 440-724-7511
RSTI
rsti-training.com • 800-229-7784
Webinar Wednesday http://webinarwednesday.live/ •
Endoscopy
Healthmark Industries hmark.com • 800-521-6224
General
General Anesthetic Services generalanestheticservices.com • 800-717-5955
POWER THE FUTURE BE THE CURRENT. AMPLIFY POTENTIAL. BUILD THE FUTURE.
OHMS LAW FOUNDATION IS A REGISTERED 501 (C) (3) NONPROFIT ORGANIZATION DEDICATED TO SUPPORTING THE NEXT GENERATION OF BIOMEDICAL EQUIPMENT TECHNICIANS (BMETS)
OHMSLAWFOUNDATION.ORG
EMAIL: chacetorres@ohmslawfoundation.org
FOUNDATION PARTNER: ohmslawfoundation.org/foundationpartners