
Marzia Chowdhury
Ph.D. Candidate, M.A.
Portfolio of Research, Design, and Teaching Work


chowdhurymarzia00@gmail.com
www.linkedin.com/in/mchowdhury01
Bio
Marzia Chowdhury is a Ph.D. candidate in Architecture at the University of Kansas, specializing in the design of Emergency Departments (EDs) and their capacity to respond to pandemic-related surge events. With over five years of research fellowship experience, she focuses on evidence-based healthcare design, including projects in emergency, behavioral health, and cancer care settings. Her work integrates spatial design, operational performance, and human-centered research to advance resilient and efficient healthcare environments.
She has received multiple recognitions for her contributions, including the AIA Arthur N. Tuttle, Jr. Graduate Fellowship in Health Facility Planning and Design (2022–2023), and the Joseph G. Sprague New Investigator Award (2022).
2024 Fall 2020- Fall 2023
Employment
Ballinger, Philadelphia, United States
Education
Ph.D. Candidate
Department of Architecture, University of Kansas, United States
Project: Design of Emergency Department for Pandemic Scenarios
Supervisor: Kent Spreckelmeyer, University of Kansas
Co-supervisor: Hui Cai, Georgia Tech (2019-current)
MA B.Arch
Department of Architecture, University of Kansas, Kansas, United States (2019-2022)
Architecture
Bangladesh University of Engineering & Technology, Dhaka, Bangladesh (2011-2017)
Fall 2019 -Fall 2023 Spring 2021 Spring 2015
Healthcare Planning Intern
Studio Instructor, ARCH 109: Architectural Foundation II
Teaching Assistant, Arch 108: Architectural Foundation I
ARCH 103: Introduction to Architecture
ARCH 658: Programming and Pre-Design Issues
ARCH 630: Theory of Architecture
Research Assistant
Graduate Assistant
Residential Planning Intern
Selected Fellowships
University of Kansas, United States
University of Kansas, United States
University of Kansas, United States
University of Kansas, United States CubeInside, Dhaka, Bangladesh
2022-2023 AIA Arthur N. Tuttle, Jr. Graduate Fellowship in Health Facility Planning and Design
~$10,000
Issuer: The American Institute of Architects’ Academy of Architecture for Health 2022 Joseph G. Sprague New Investigator Award
Issuer: The Center for Health Design
$10,000
$30,000 Fall 2024
Foundation for Health Environments Research (FHER)
Issuer: AIA-AAH
PI: Hui Cai
Certification
Protection of Human Subjects – Social and Behavioral Research
Collaborative Institutional Training Initiative Program
Health Information Privacy and Security (HIPS) - Health Privacy (HIPAA) for Researchers
Collaborative Institutional Training Initiative Program
GCP: Social and Behavioral Research Best Practices for Clinical Research
Collaborative Institutional Training Initiative Program
Skills
RESEARCH EXPERIENCE
Selected Research Work Sample | 2022
Research Fellow
Selected Recognition Research Background
2022-2023 AIA Arthur N. Tuttle, Jr.
Graduate Fellowship in Health Facility Planning and Design
Issuer: The American Institute of Architects’ Academy of Architecture for Health Project: Emergency Department (ED) Design for Pandemic Conditions: lessons learned from the COVID-19 Pandemic (extension)
2022 Joseph G. Sprague New Investigator Award
Issuer: The Center for Health Design Project: Emergency Department (ED) Design for pandemic conditions: lessons learned from the COVID-19 pandemic
My research lies at the intersection of healthcare architecture, operational resilience, and human well-being. Through my dissertation, I explored how EDs responded to the COVID-19 pandemic, employing a mixed-methods approach that included simulation modeling, thematic analysis, and operational data evaluation. This work uncovered how spatial adaptability and staff-centered design influence both care delivery and provider resilience—insights that continue to shape my long-term research agenda.
Alongside my academic work, I’ve built hands-on experience in applied research and practice-based inquiry. At Ballinger (Philadelphia), I conducted evidence-based literature reviews on decentralized nurse stations, cancer care design, and ambulatory care models, and developed a Post-Occupancy Evaluation proposal for an ambulatory cancer center. I’ve worked on multiple funded projects, contributed to successful grant proposals, and handled project compliance—from budget allocation and progress tracking to manuscript development. My training spans research design, grant writing, data analysis, and project management—skills that equip me to lead interdisciplinary collaborations across academic, healthcare, and design practice settings.
At the core of my research philosophy is a commitment to producing work that is both methodologically rigorous and deeply attuned to real-world complexity. I strive to bridge academia and practice through inquiry that informs policy, empowers healthcare professionals, and supports more adaptable, restorative, and equitable care environments.
Fall 2024
Systematic Literature Review on Design Factors Affecting Staff, Patient, and Operational Efficiency in Cancer Care Settings
Systematic Literature Review on Decentralized Nurse Station
Systematic Literature Review on Design Factors Influencing Ambulatory Cancer Care Centers
Post-occupancy Evaluation Proposal: Ambulatory Cancer Care Center Design Impacts on Staff, Patient, and Operational Efficiency in Cancer Care Settings
Healthcare Planning Research Intern Ballinger, Philadelphia
Fall 2022Fall 2023
Design of Emergency Department (ED): Responding to Pandemic-Related Surge Events (Dissertation)
Grant: Foundation for Health Environments Research (FHER)
PI: Hui Cai, PhD, Professor, Chair, Department of Architecture, University of Kansas
Spring 2021
Pre-Renovation Site Analysis
Department of Architecture, University of Kansas
PI: Joe Colistra, Department Chair and Associate Professor in the Department of Architecture, University of Kansas
Research Fellow
University of Kansas, Lawrence, Kansas
University of Kansas, Lawrence, Kansas
Fall 2021
Fall 2019Spring 2020
Literature Review on Design of Acuity-Adaptable Treatment Rooms, Hoefer Welker Architects, on behalf of The Institute for Health + Wellness Design, KU, School of Architecture and Design
Research Fellow
University of Kansas, Lawrence, Kansas
PI: Hui Cai, PhD, Frank Zilm, D.Arch, FAIA Kent F Spreckelmeyer , PhD, University of Kansas
Miscellaneous Research Activities
PI: Mahbub Rashid, PhD, Professor of Architecture, the Interim Dean, and the Associate Dean for Research and Graduate Studies of the School, University of Kansas
University of Kansas, Lawrence, Kansas
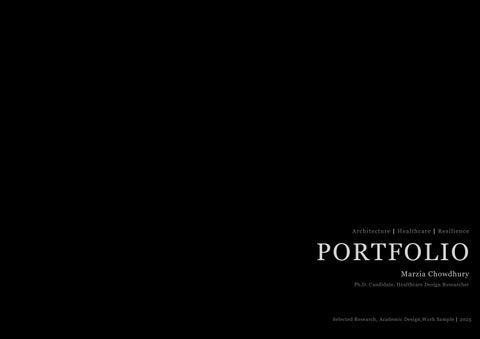
Emergency Department (ED)
Design for Pandemic Conditions: Lessons Learned from the COVID-19 Pandemic
An Evidence-based Design Approach to Maximizing Flexibility for Surge Response and Infection Control, Dissertation Project
Ongoing
Despite the establishment of numerous Alternative Care Sites (ACS) across the United States, many remained underutilized even as hospitals faced overwhelming patient volumes and resource shortages.
Bell SA, Krienke L, Quanstrom K. Alternative Care Sites During the COVID-19 Pandemic: Policy Implications for Pandemic Surge Planning. Disaster Med Public Health Prep. 2021 Jul 23:1-3. doi: 10.1017/dmp.2021.241. Epub ahead of print. PMID: 34296671; PMCID: PMC8446586.
Background
Research Framework
Operational Strategies
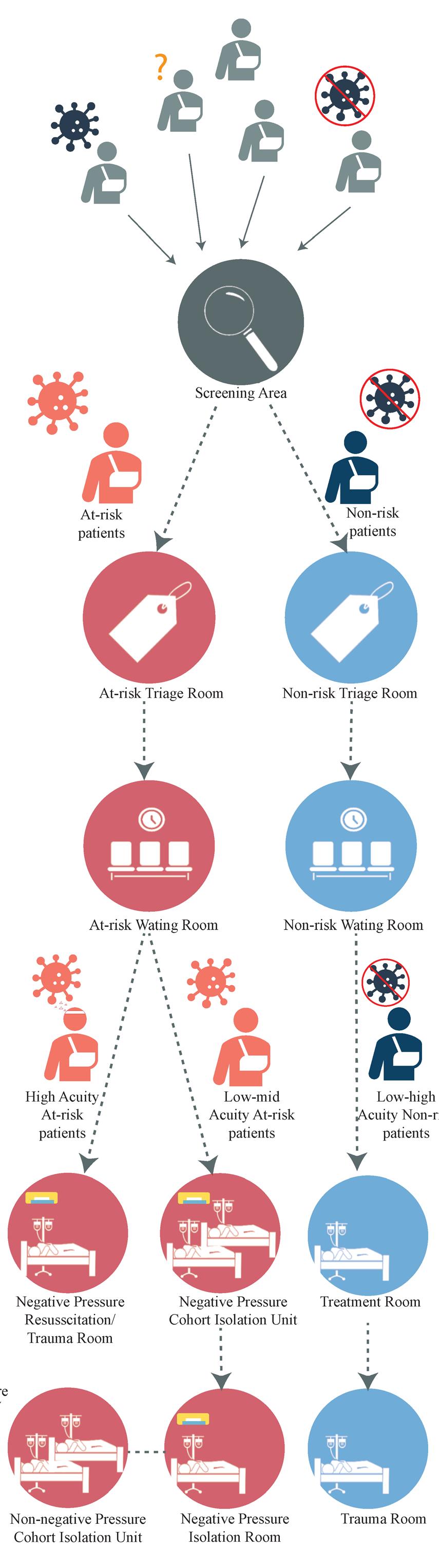
1. Split flow by infection risk and acuity level
2. Staff workflow during pandemic Independent Variables Dependent Variables
Environmental Design Strategies
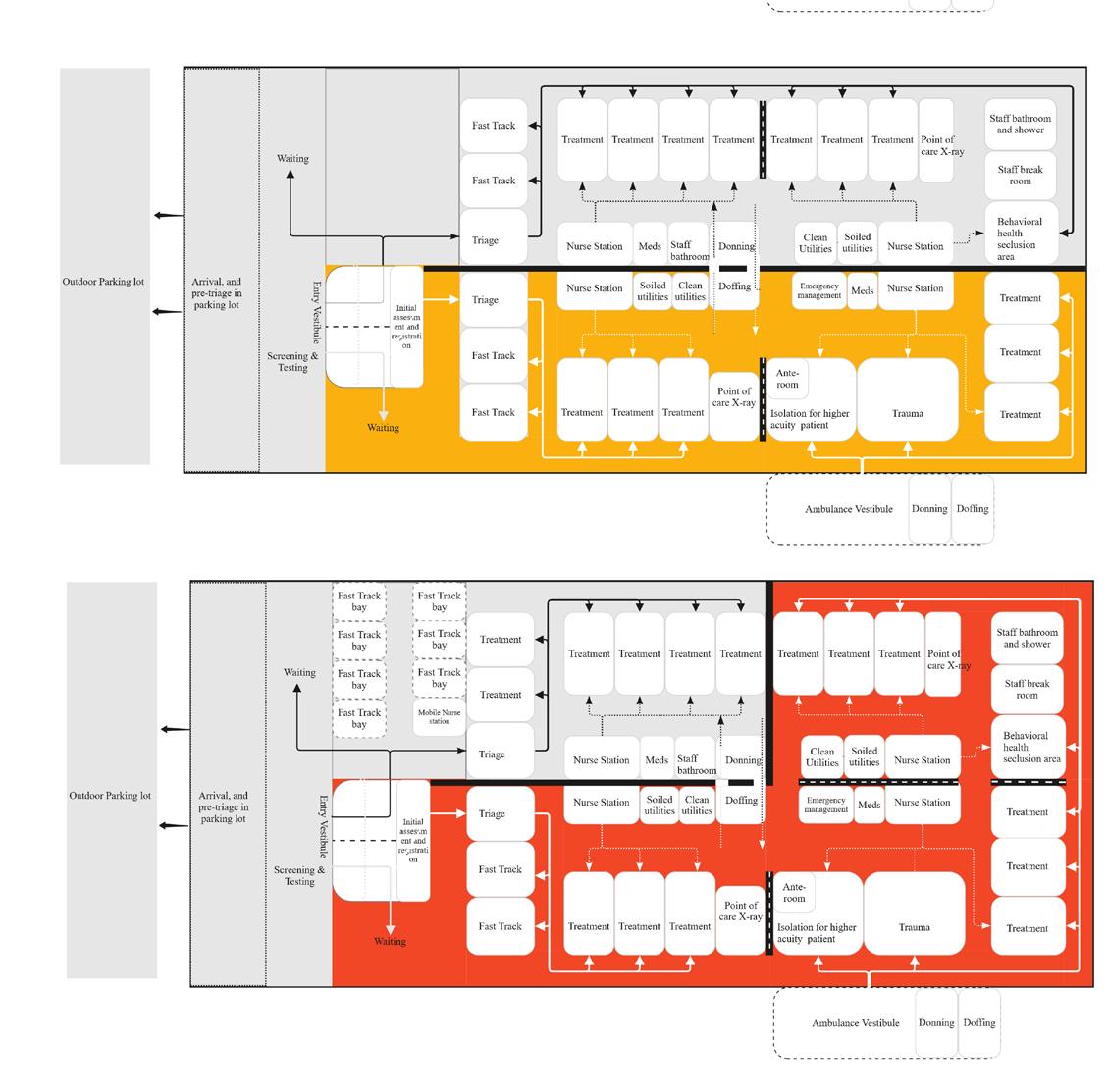
1. Space ability to cohort patients at different stages of the pandemic
2. Space ability to flex up and down in responding different surge volume
Minimizing risk of Exposure
Research Study
Mixed Method Research
Research Tools
Focus group, One-on-one, On-site walk-through interviews
MaxQODA for thematic analysis
IBM SPSS for Descriptive and Inferential Statistical Anaysis of Operational Data
Presentation
Adobe Illustrator, Photoshop, AutoCAD for diagram
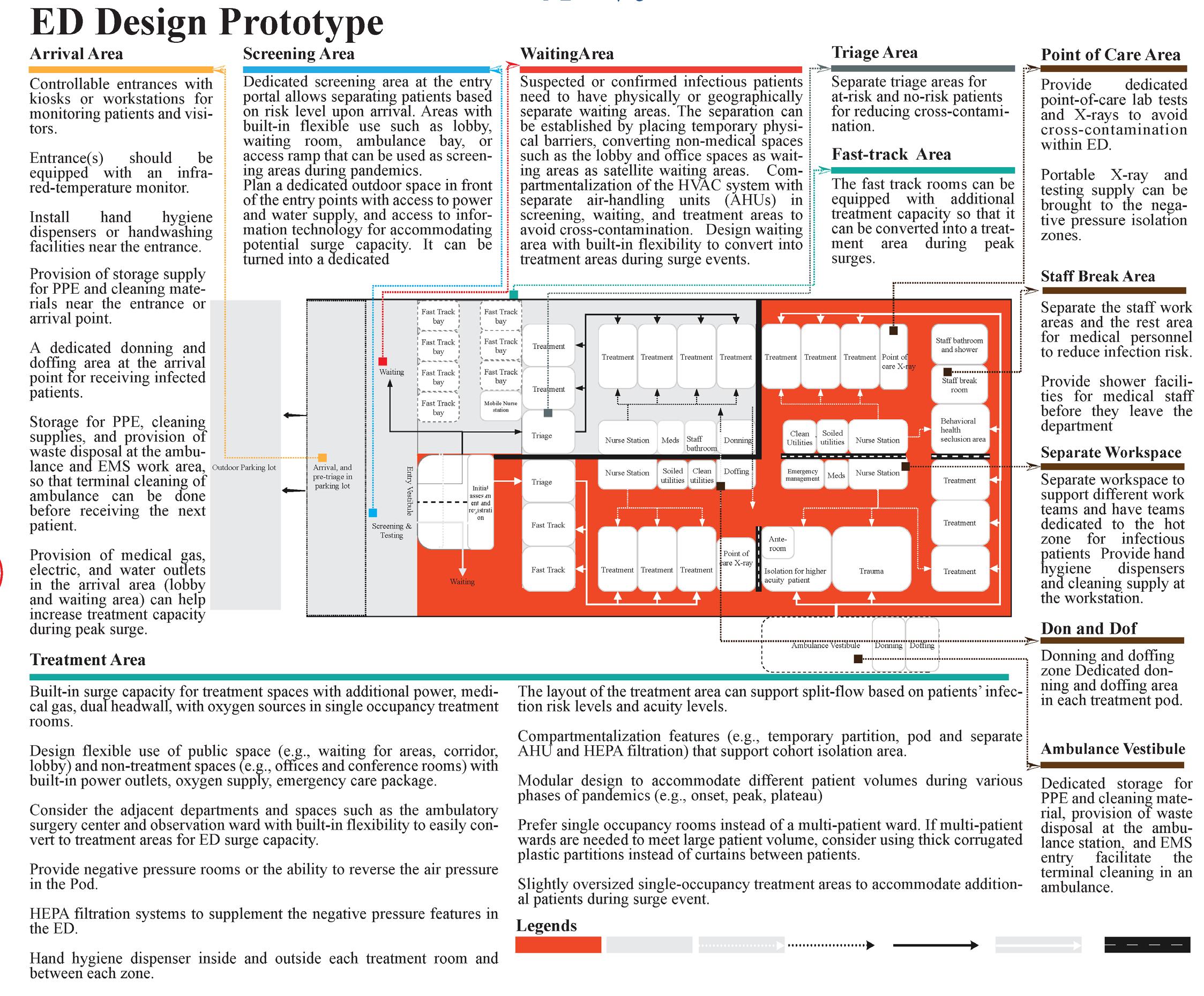
Emergency Departments (EDs) are the front line of healthcare response during pandemics and disasters. Careful planning and design can significantly increase their surge capacity and operational efficiency without requiring excessive contingency space or cost (Zilm et al., 2008). However, one of the major challenges in preparing EDs for surge events lies in identifying a balanced strategy—one that mitigates risks while considering capital costs and institutional priorities.
Research Gap
Limited evidence is available regarding how EDs, particularly different spatial and operational strategies, have been adopted in response to the different phases of the pandemic. More importantly, limited information is available regarding spatial and operational strategies impact ED performance,
such as LOS, bed utilization rate, and waiting time.
Why?
This research investigates how different EDs adapted to the COVID-19 pandemic, with a particular focus on cohort isolation strategies and their operational impacts. By examining real-world case studies, the study aims to fill a critical gap in knowledge regarding the spatial and operational flexibility required during health crises.
Research Questions
1) Does ED design make a difference in responding to the pandemic at different phases?
2) What are the pandemic resilient design features?
3) How did that ED design affect the ED operational metrics, First wait time (door to provider time), and treatment time (provider to disposition time) for different cohort patient groups?
Framework
Since the research objective is to understand the ED responses, the independent variables will be the adopted spatial and operational strategies in treatment area during the pandemic. The dependent variables include ED operational metrics (1) Length of Stay, and patient-centered metrics: (1) waiting time or Door to Provider time and bed utilization rate.
Method
Employing a mixed-methods approach—combining retrospective analysis, predictive simulation, and both qualitative and quantitative data—this research develops evidence-based design recommendations for adaptable and resilient ED environments. Rather than relying on short-term renovations or improvised measures, the study proposes sustainable, longterm design strategies that integrate flexibility directly into ED planning.
Surge Responses
ED Performance Metrics for different patient groups
1. First wait time (Door to Provider time) for different cohort patient groups
2. Treatment time (Provider to departure time) for different cohort patient groups
Mixed Method Research
Systematic Literature Review Interview Statistical analysis on patients’ throughput time
An understanding of the ED space adaptions during different phases of the pandemic.
An understanding of the ED space adaptions, design strategies, staff perception of effective design features for patient care delivery, perceived safety of patient and staff.
Regression analysis to understand the impact of spatial design strategies on first wait and treatment time across different cohort patient groups.
Understand and synthesize of the ED operation and spatial design strategies and the impact on ED performance during different phases of the COVID-19 pandemic.
Case Studies: Pandemic Resilient EDs
Case Study A1
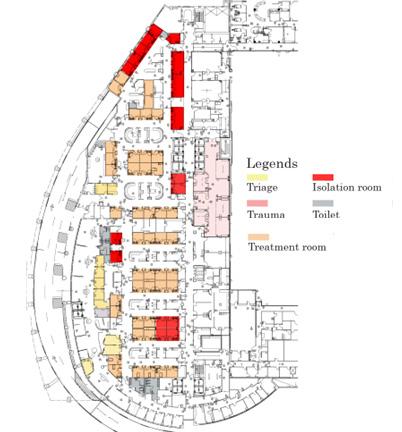
Case Studies: Regular EDs
Case Study B1

Case Study A2

Predictive Analysis
Simulating a hypothetical ED prototype from a real-life data to evaluate different isolation strategies’ effectiveness by comparing length of stay, and utilization rate.
Providing a design recommendation.
Case Study B2


Case Study B3








(March –May 2020)
Period (June-August 2020)
Key Findings and Insights
The thematic analysis—derived from five case studies, focus group interviews, and on-site walkthrough observations—revealed clear spatial and operational patterns that contributed to the adaptability and resilience of EDs during the COVID-19 pandemic.
1. Adjacent Flexible Spaces: EDs that incorporated interconnected or convertible spaces, such as observation units, triage areas, or procedure rooms adjacent to treatment zones, were able to rapidly expand or contract clinical capacity during patient surges. This adjacency allowed spaces to shift between COVID and non-COVID functions with minimal
(Nov. 20- Jan. 2021)
(July-August 21)
(Dec. 21–Jan. 22)
disruption to care flow, demonstrating the value of functional overlap and shared infrastructure in surge response.
2. Volume-Responsive Spatial Design:
Departments with modular layouts and movable partitions effectively managed fluctuating patient volumes. These flexible configurations minimized unused space during low-census periods and prevented overcrowding during surges, resulting in improved throughput and reduced patient wait times.
3. Adaptive Layouts and Circulation Patterns:
Facilities that implemented dual-corridor
systems or segregated circulation routes could adapt quickly to changing isolation protocols. This adaptability ensured safe movement for staff and patients, limited cross-contamination, and supported continuous operational flow even under rapidly evolving infection control measures.
4. Integration of Spatial Flexibility and Staffing Models: The findings emphasized that flexible physical layouts alone were insufficient. Effective response depended on staffing strategies synchronized with spatial adaptability. This alignment between operational planning and physical design proved critical to maintaining efficiency and safety under surge conditions.
Rush University Medical Center staff see patients in the Brennan Pavilion, the hospital’s main lobby, which was transformed into Times
Source: Case Study A2, staff see patients in the Brennan Pavilion, the hospital’s main lobby, which was transformed into a low-acuity treatment area during the coronavirus pandemic. Ashlee Rezin Garcia/Sun-Times
Low acuity surge area in the ambulance bay
Hidden surge cabinet with access to power, medical gas in lobby, waiting area Credit: Md. Jason Wilson
Credit: MD. Jason Wilson, Case Study A1
Photo Source:
Case Study A2
A Nationwide Survey on Emergency Departments Pandemic
Responses
Environmental Design Research Association (EDRA), Part of Dissertation Project
Research Study Survey Study
Research Tools
Qualtrics for data collection
IBM SPSS for non-parametric statistical hypothesis test
Presentation
MS Powerpoint
Background
This research study is a part of the dissertation study, the abstract was published in EDRA 55.
During the COVID-19 pandemic, many Alternative Care Sites (ACS) across the United States were underutilized, even as hospitals faced overwhelming patient surges. This disconnect highlights a critical gap between preparedness planning and actual operational needs. To bridge this gap, a survey was conducted to evaluate pandemic preparedness approaches from a facility design perspective for different periods and identify their relationship to EDs’ characteristics.
Research Method
A qualitative study was conducted, combining a systematic literature review to identify ED design strategies and a nationwide survey (distributed through the Emergency Department Benchmark Alliance from September to October 2022) to assess their implementation across different pan-
demic phases. Descriptive statistics and chi-squared tests were used to examine variations in design strategies among U.S. EDs.
Results
Based on 30 articles from 2004 to 2023, the SLR showed that during major pandemics including the COVID-19 pandemic, some key strategies for EDs’ to address pandemics have been identified: a)the split flow of suspected and non-suspected patients; b) the provision of separate screening, triaging, waiting, and cohort isolation zones for suspected patients; and c) adaptive use of treatment and non-treatment areas within and adjacent to ED spaces and conversion of non-treatment areas to accommodate surge capacity. These strategies were used to build the national survey for Emergency Department Benchmark Alliance (EDBA).
Out of the 130 respondents for the EDBA survey, 57 completed all sections
Importance
There remains a critical need to understand which strategies are most effective during each phase of a pandemic, and how these strategies differ across EDs of varying regions, sizes, and resource levels (Schreyer et al., 2020). Prior studies have
highlighted the importance of adaptive responses to fluctuating patient surges and evolving conditions (Ghazali et al., 2023; Jachetti et al., 2021). However, limited research exists on how the built environment influences or supports these adaptive strategies throughout different stages of a pandemic. This study aims to bridge that gap—providing insights that can guide healthcare facilities, architects, and designers in making evidence-based decisions when planning or modifying spaces for future public health emergencies.
Ghazali, D. A., Choquet, C., Bouzid, D., Peyrony, O., Fontaine, J.-P., Sonja, C., Javaud, N., Plaisance, P., Chauvin, A., & Casalino, E. (2023). The Response of Emergency Departments (EDs) to the COVID-19 Pandemic: The Experience of 5 EDs in a Paris-Based Academic Hospital Trust. Quality Management in Health Care, 32(1), 46-52.
Jachetti, A., Colombo, G., Brignolo-Ottolini, B., Franchi, J., Solbiati, M., Pecorino Meli, M., Bosco, P., & Costantino, G. (2021). Emergency department reorganisation to cope with COVID-19 outbreak in Milan university hospital: a time-sensitive challenge. BMC Emergency Medicine, 21(1), 1-8.
Schreyer, K. E., Daniel, A., King, L. L., Blome, A., DeAngelis, M., Stauffer, K., Desrochers, K., Donahue, W., Politarhos, N., & Raab, C. (2020). Emergency department management of the Covid-19 pandemic. The Journal of emergency medicine, 59(6), 946-951.
Adopted Strategies At Different Periods
Separate staff respite and break area who worked in isolation/ COVID hot zone
Dedicated donning and doffing area
Dedicated donning and doffing area
Separate patient flow for infected and non-infected patients
Separate patient flow for infected and non-infected patients
and were included in the analysis. The most adopted strategies are —a) negative pressure room (95%, n=54/57), b) cohort isolation (84%, n=48/57), and c) separate pre-triage or screening area (84%, n=47/57). Almost half (48%) of the strategies were implemented at the onset, whereas only 17% were before the outbreak.
Separate cohort isolation zone/ COVID hot zone for treatment of infected patients
Separate cohort isolation zone/ COVID hot zone for treatment of infected patients
Negative pressure rooms
Separate waiting area for suspected infectious patients
Separate triage area for suspected infectious patients
The statistical analysis revealed significant differences between the types of EDs and the design strategies they have adopted in response to the pandemic. For example, academic EDs are associated with a higher chance of adopting separate triage X2 (1, N = 57) = 7.75, p = 0.004; separate patient flow X2 (1, N = 57) = 5.53, p = 0.019; and separate dedicated donning and doffing areas X2 (1, N = 57) = 3.989, p = 0.046. Hospital size is also significantly associated with the likelihood of adopting separate screening areas, X2 (1, N = 57) = 4.236, p = 0.04.
Separate pre-triage/screening area
Adopted before the COVID-19 pandemic occurred at your site
Adopted later period (3-6 months after the outbreak) at your site
Adopted at beginning of the COVID-19 pandemic at your site
Top Three Strategies Implemented During the Pandemic
Based on the survey, the first three most common strategies across different periods of the pandemic are negative pressure rooms, cohort isolation strategies, and separate pre-triage or screening areas
The majority of the strategies were implemented at the beginning of the pandemic, but their importance was deemed to lessen as knowledge about the transmission risk was gained over time.
Between ED Characteristics and Pandemic Responses
Separate pre-triage/screening area
Emergency Department in Response to Pandemics, A Systematic Literature Review
Separate
Separate
Presented Environmental Design Research Association (EDRA), : Part of Dissertation Project 2022
Healthcare workers with a known source of exposure, found that 52% of infections from March 2020 to March 2021 were deemed to be workplace-associated.
Reported
Separate
Separate
One size doesn’t fit all
The analysis revealed clear differences in how EDs adapted their spaces in response to the pandemic. Academic hospitals were more likely to create separate triage areas, distinct patient flow paths, and dedicated zones for putting on and removing protective equipment. Larger hospitals also tended to establish independent screening areas to better manage patient surges.
These patterns highlight an essential insight for healthcare design: pandemic response strategies must be tailored to each facility’s size, resources, and operational needs—there’s no single solution that fits every context.
Research Study A Systematic Leterature Review
Research Analysis Tools
MS Excel
Presentation
MS Powerpoint for diagram
Background
The COVID-19 pandemic has presented serious challenges to EDs in managing patients. EDs play an important role in responding to pandemics, as they made the first substantial strides to recuperate patients and protect them from infectious diseases, as shown in experiences of earlier infectious disease surge events (e.g., SARS-CoV, H1N1, and Ebola, etc.). However, there is limited evidence on how facility design can support EDs’ response to pandemics.
Objective
This study aims to provide a systematic literature review (SLR) of EDs’ challenges and responses to pandemics, with a primary focus on adapted spatial and patient flow strategies. The authors followed the “Preferred Reporting Items for Systematic Reviews and Meta-Analysis” (PRISMA) guideline and searched the databases; PubMed, Web
of Science, Science Direct, PubMed central database, covering the literature from March 2000 to March 2021. 2489 studies were identified by the initial database keyword search and additional hand search based on literature search.
Finally, 20 articles met the inclusion criteria.
Findings
Key findings include a) negative pressure rooms b) split flow and cohort isolation that can create various zones for patients with different risk and acuity levels are the most addressed approaches for infection control and accommodating surge capacity. Convertibility and flexibility concept (e.g., reconfiguration of spaces, temporary separation within spaces, reversible air pressure, flexible use of treatment and non-treatment spaces within and adjacent to ED) is key to address unique challenges of evolving nature of pan-
demic outbreaks.
Significance
This study provides a summary of existing design strategies for EDs to respond to pandemics. Multiple design strategies need to be combined to minimize the disease transmission in EDs during pandemics and providing surge capacity for overflow of patients. Detailed design principles were synthesized based on the SLR and translated to a design prototype that can respond to evolving stages of pandemics.
Conclusion
This article can be helpful to front-line staff in clinical settings, hospital administrators, public or government officials, architects, and the like. It also identifies opportunities for further research on EDs design to better respond to pandemics.
Findings From Literature Review



















































Impacts of the Isolation Design Strategy in Emergency Depart-
ment on the Patients’ Opera-
tional Outcome
Predictive Analysis of Spatial Design Strategies for future Pandemic Scenarios: Part of Dissertation Project
Ongoing
Research Study
Quantitative Research
Research Tools
On-site walk-through interviews, Observation, Operational Data, Interviews
Flexsim for model development and running simulation I IBM SPSS for
of
Background
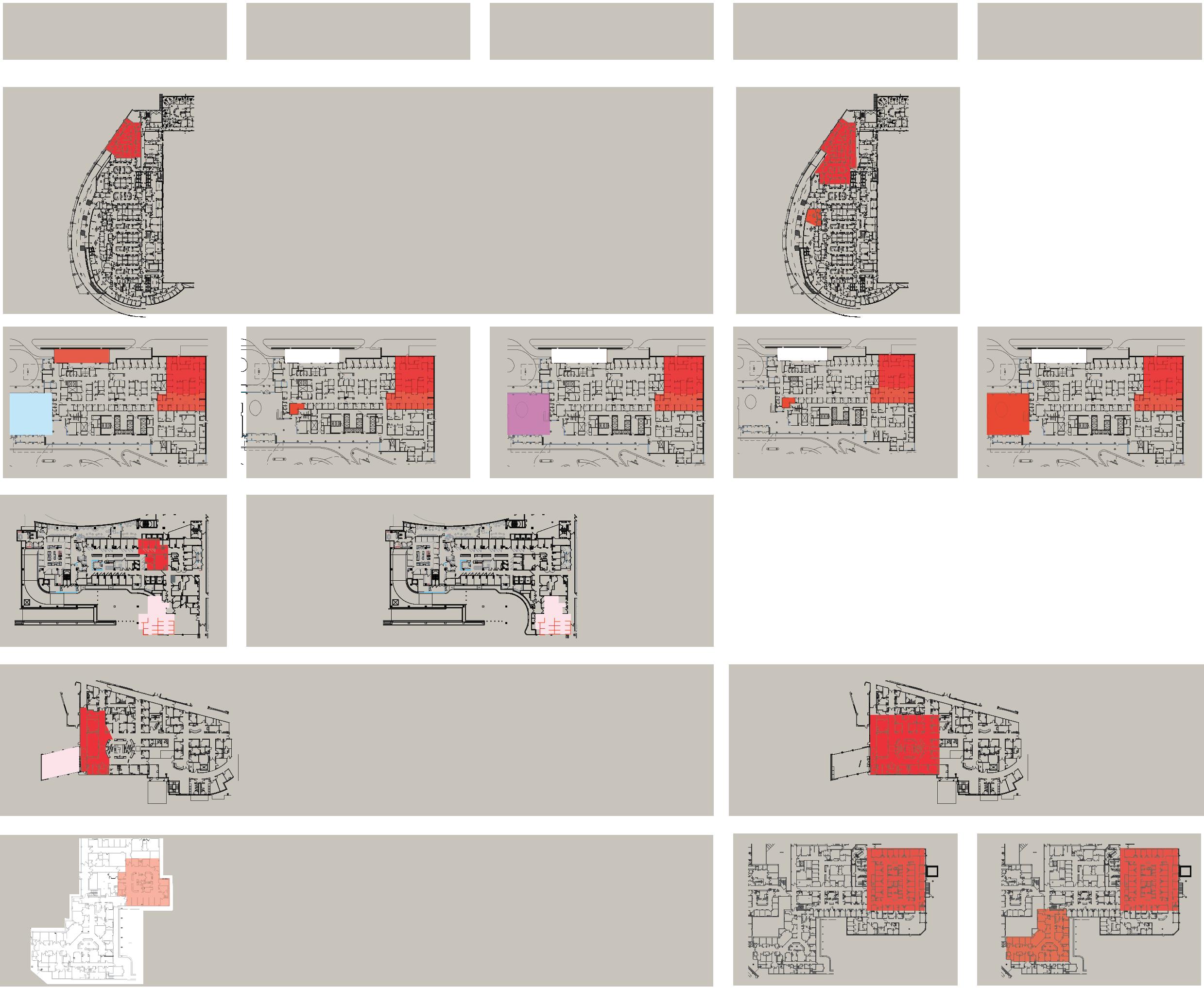
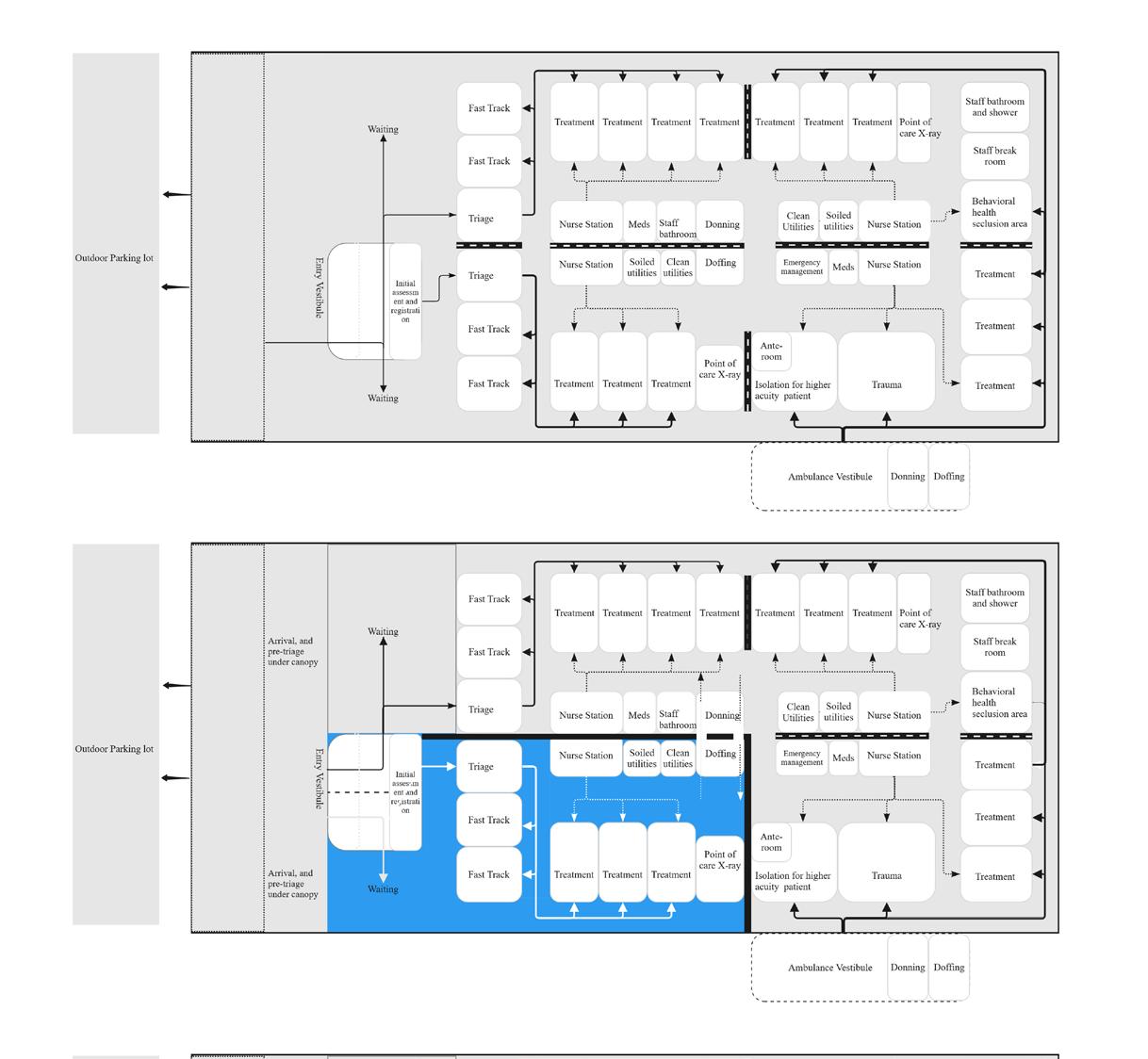
This research, part of my dissertation on predictive analysis in healthcare design, will examine how spatial strategies influence ED performance during pandemics. Early in the COVID-19 crisis, cohort isolation units effectively reduced infection risk but were later discontinued due to low utilization. Insights from this study highlight the need to balance flexibility, adaptability, and operational sustainability when designing for surge conditions—ensuring that healthcare spaces can respond efficiently to both immediate and evolving demands.
Objective
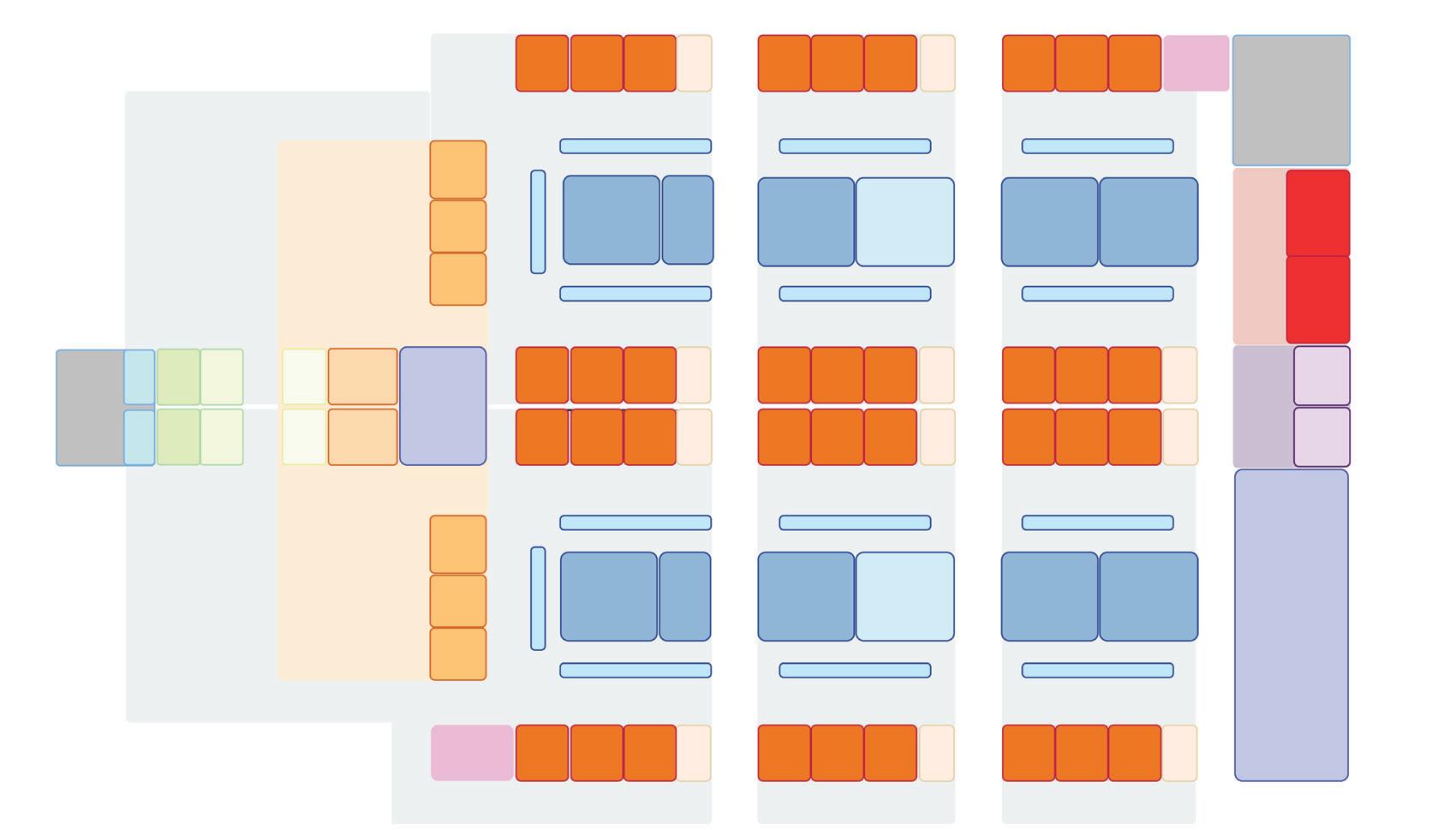
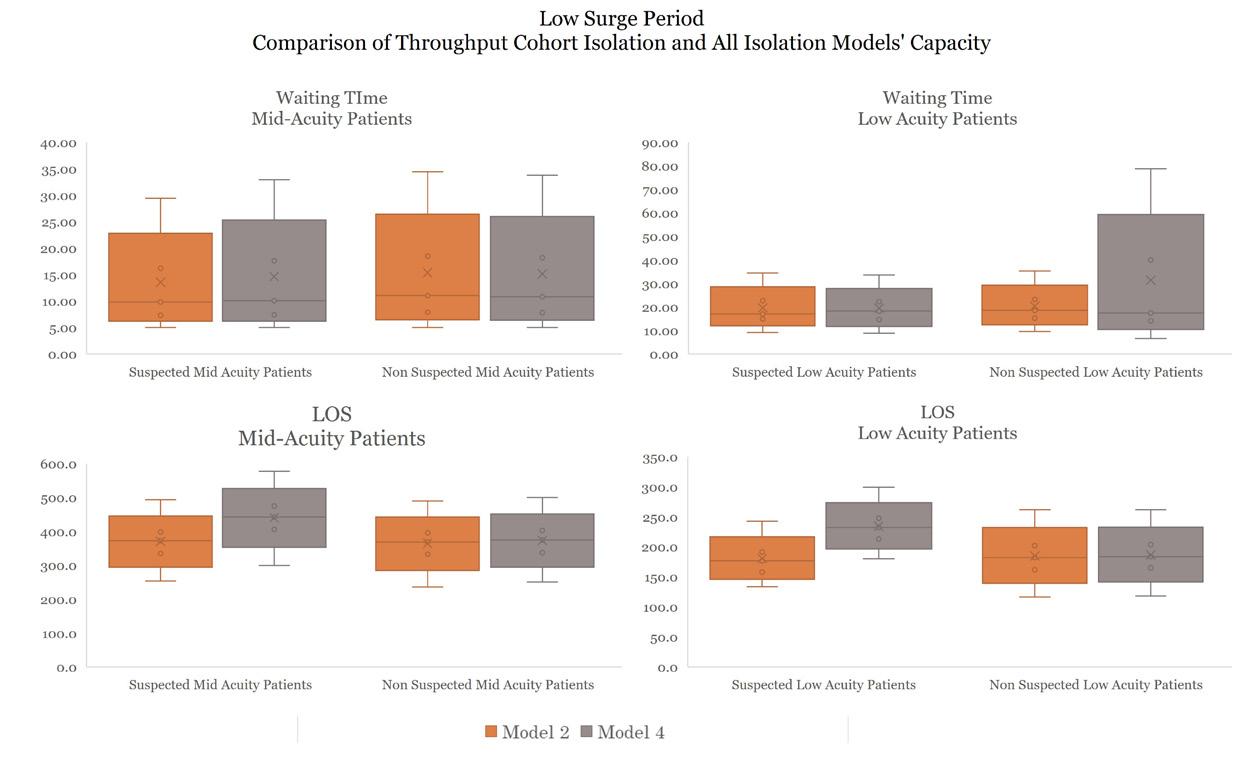
This study aims to determine the optimal performance of various isolation design strategies across for different patient volumes (in an example of low and high surge periods of COVID-19 pandemic period). Eight isolation design models have been developed from the interview findings from five case studies and systematic literature review. It will
compare patient throughput: the door to provider time and length of stay in treatment rooms for suspected and non-suspected patients and cohort and non-cohort isolation unit utilization rates.
Methods
This study is based on predictive analytics using Discrete Event Simulation (DES). It will use the actual ED operational data to build a baseline simulation model and propose a series of “what-if” scenarios to test the effectiveness of various isolation design strategies using hypothetical layouts during two time periods.
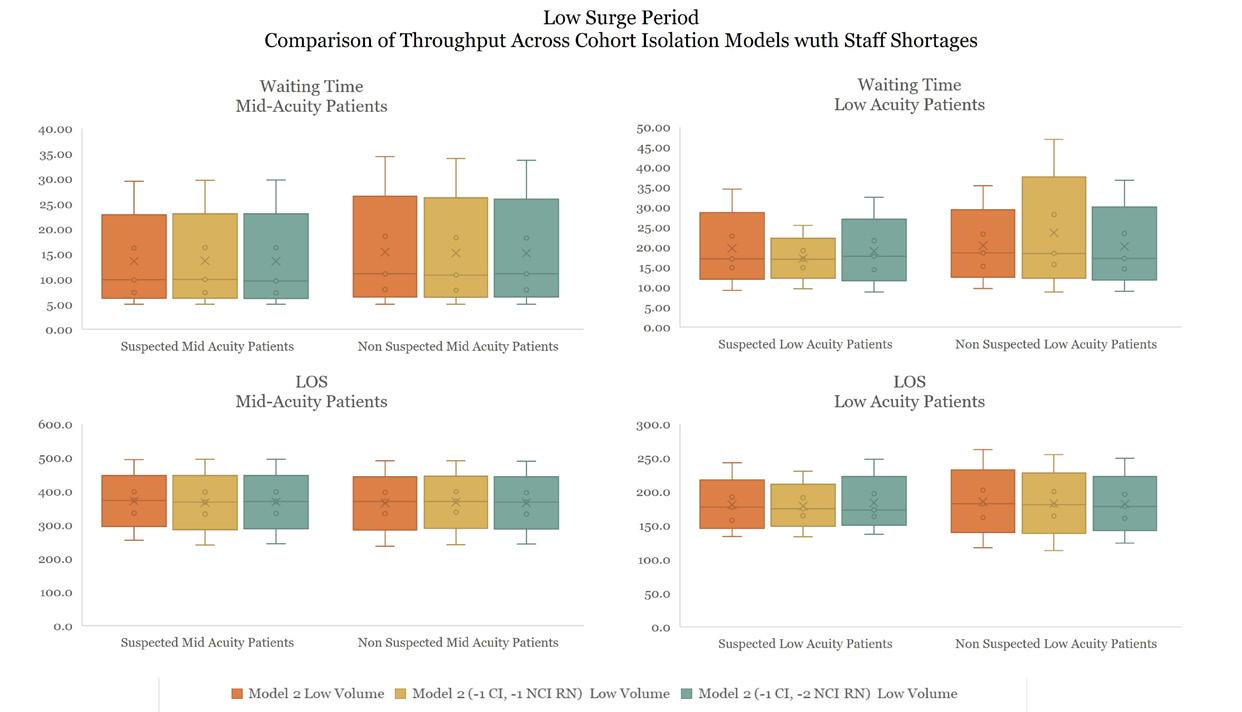
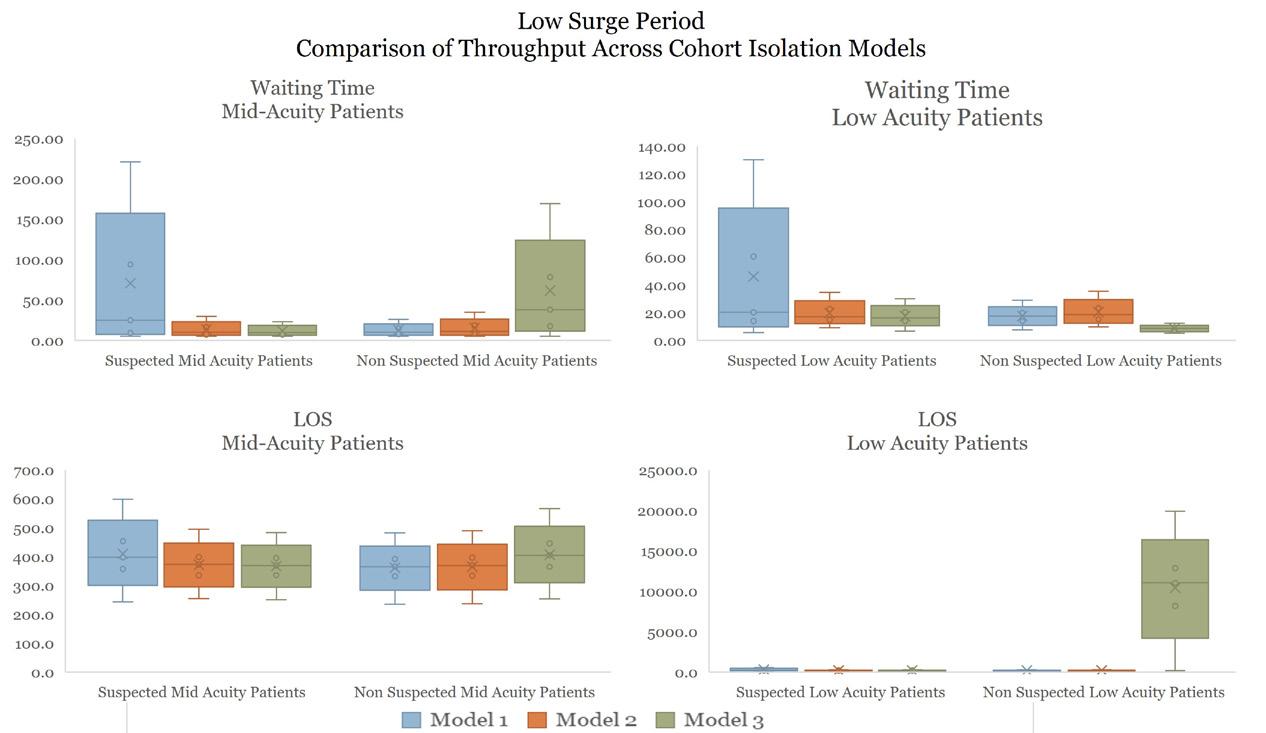
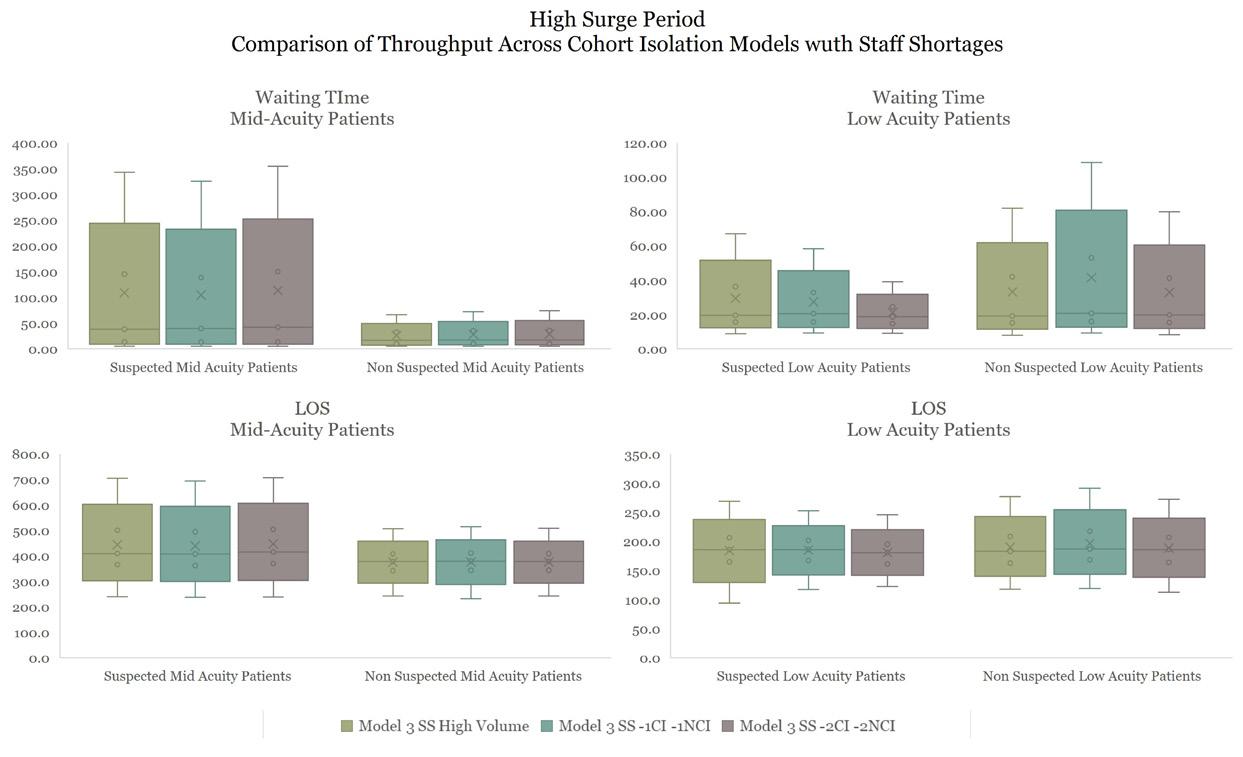
Descriptive and inferential statistics will be conducted to identify the statistical significance differences across design models. First comparison will be across cohort isolation models; second, across best performing cohort and all-isolation room models, and third will best performing model with staff shortages.
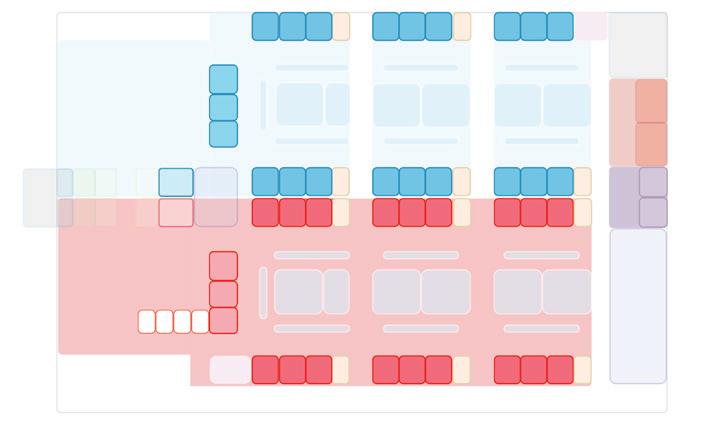
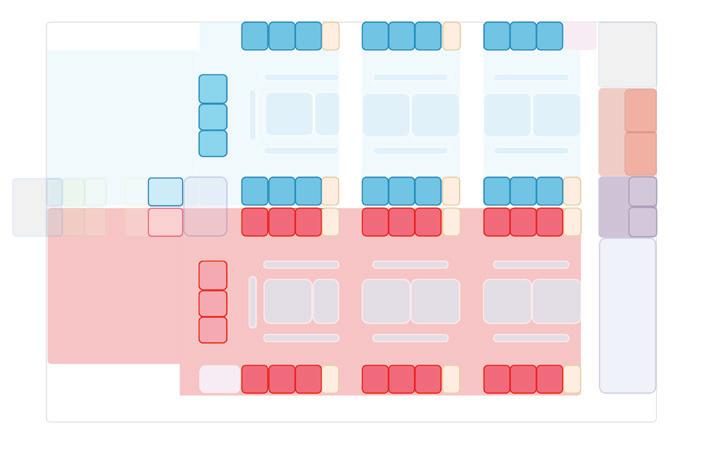
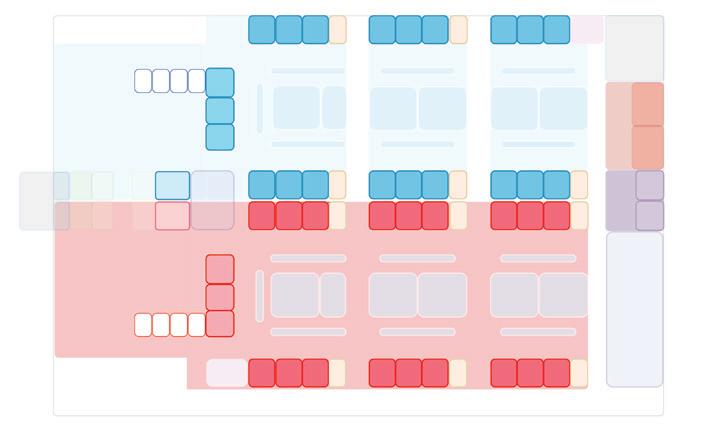
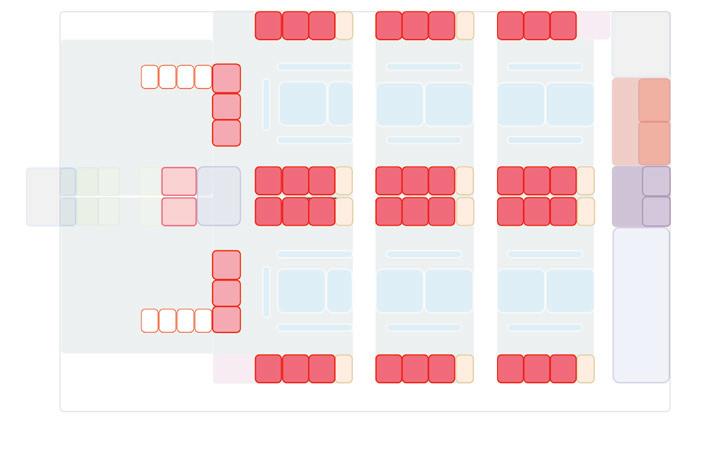
What-if Scenarios
A series of “what-if” scenarios were developed to explore how different cohort isolation strategies and staffing conditions— with nurse-to-patient ratios ranging from 1:3 to 1:4—affect ED performance during varying levels of pandemic surge. Each scenario illustrates a progressive design response aimed at maintaining operational sustainability under low and high-demand conditions.
Significance
This study aim to illustrate how simulation modeling can inform evidence-based decisions in ED design during pandemic surges. By testing multiple cohort isolation strategies, it will highlight how spatial layouts influence patient length of stay, room utilization with operational efficiency. Although the model was limited to a single academic tertiary care ED, the approach provides a transferable framework for evaluating design strategies in similar healthcare settings.
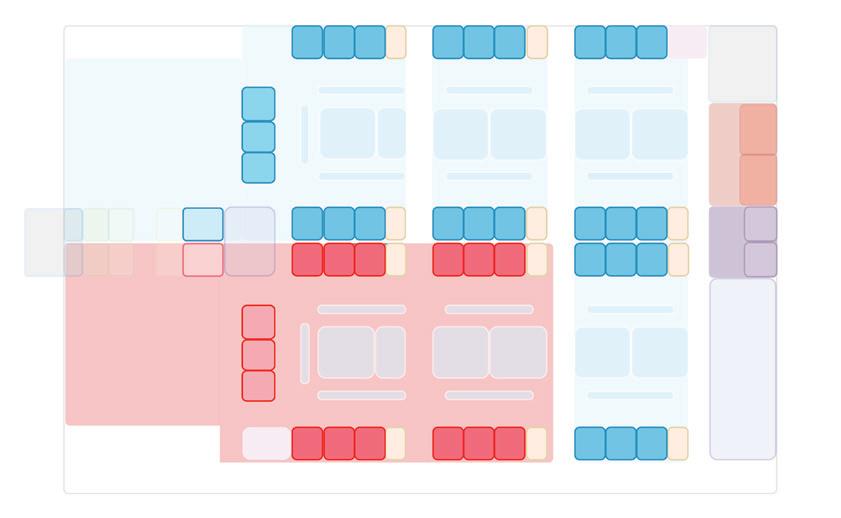
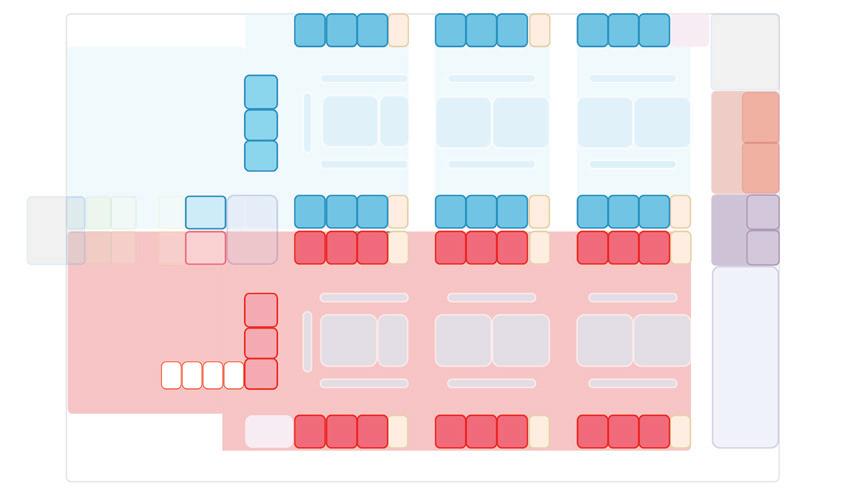
Model 1: 10 treatment spaces in negative pressure cohort isolation unit
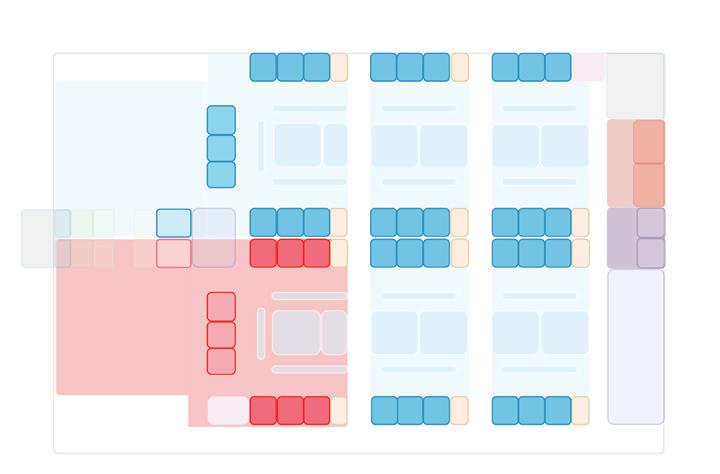
Model 2: 16 treatment spaces in negative pressure cohort isolation unit
Design Models
Model 3: 22 treatment spaces in negative
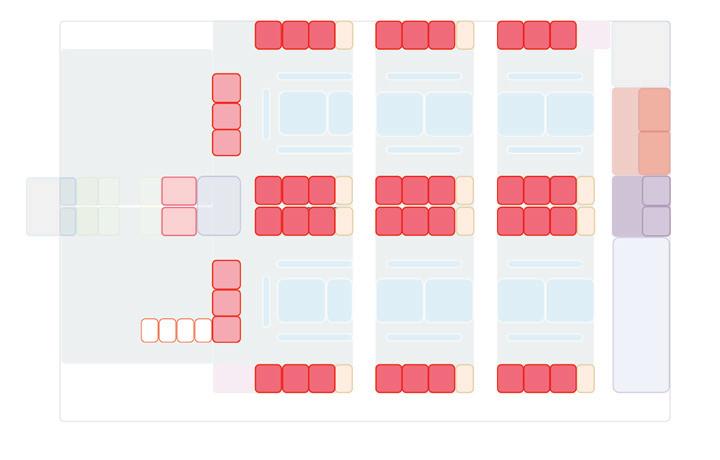
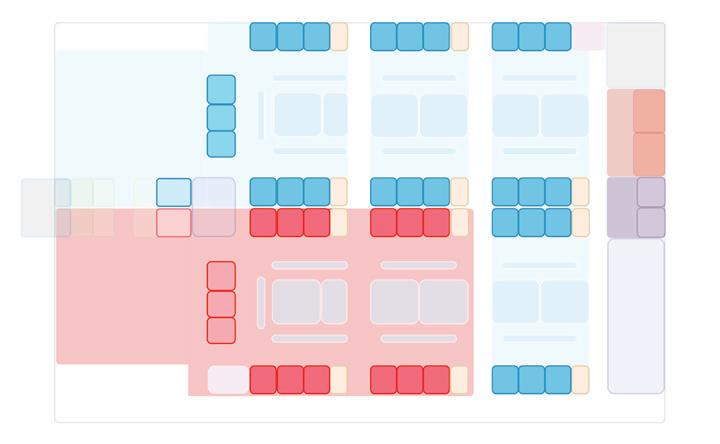
Comparison of Operational Performance Across Different Design Models in Two Volume Scenarios
Low Surge Period
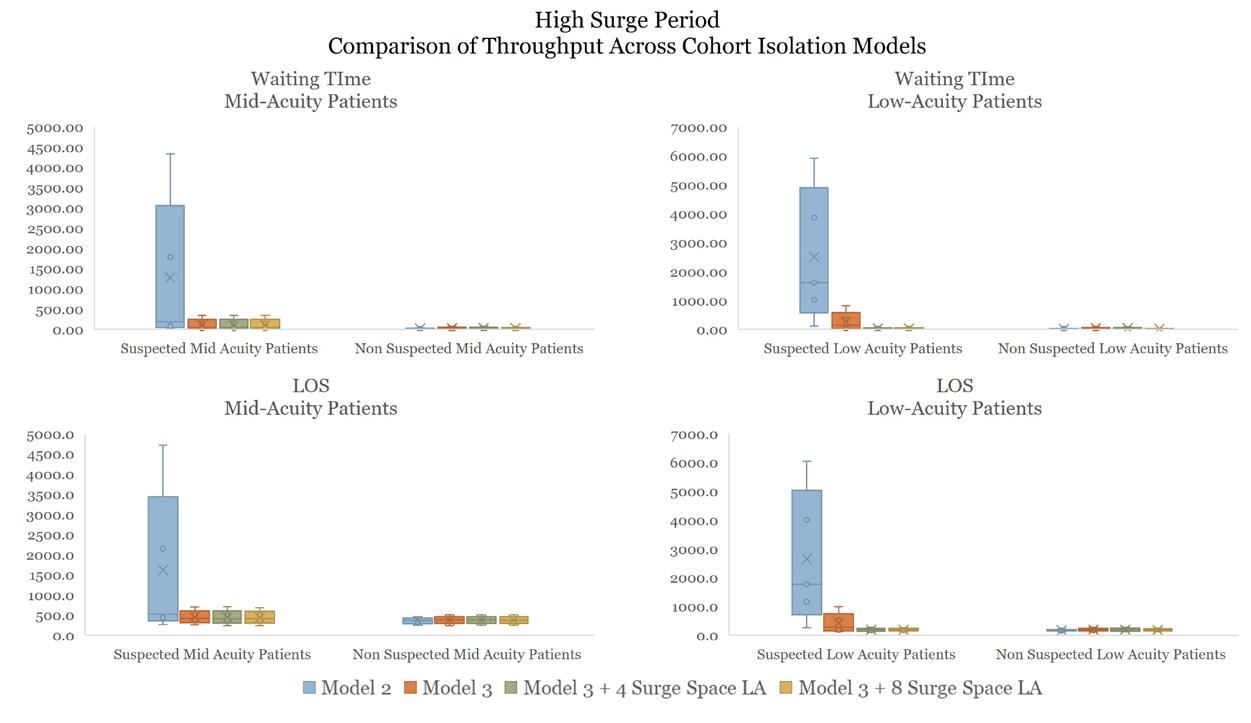
Performance in
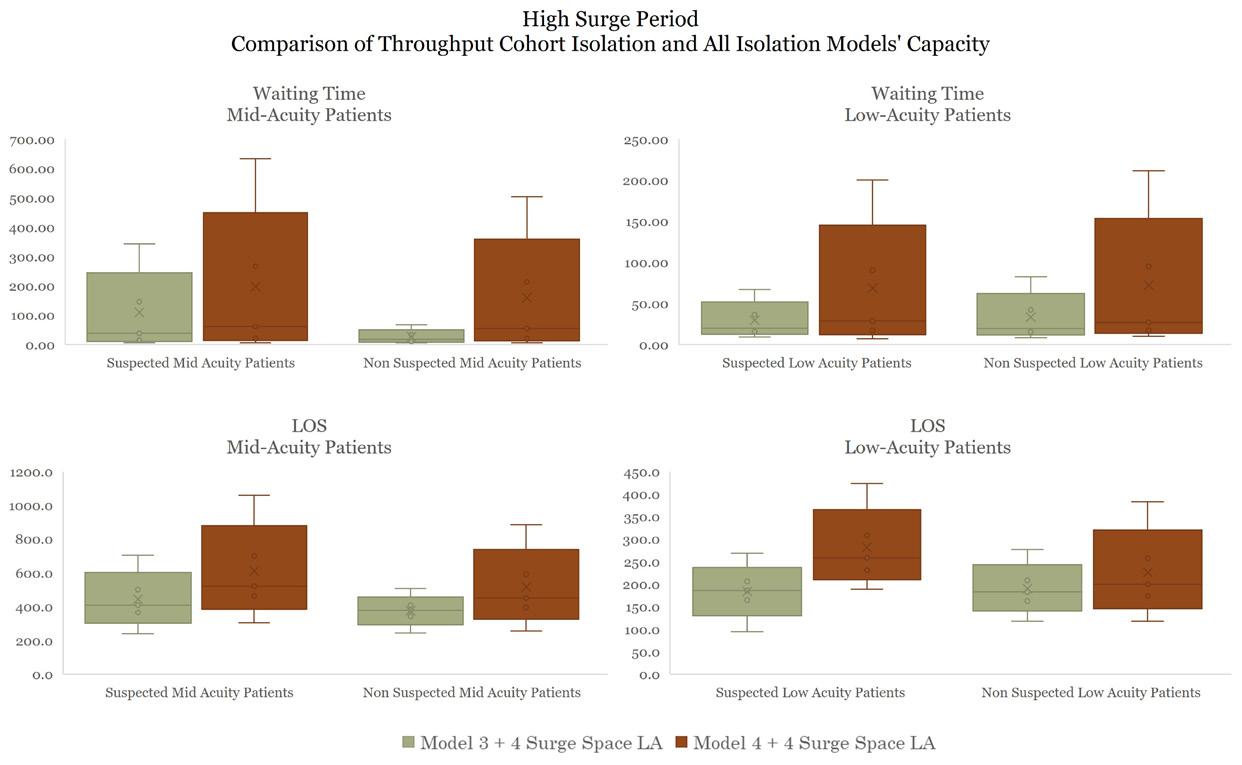
Optimal
Model
Optimal Performance in Model 5