

Cardio-Renal-Metabolic Syndrome: An updated clinical paradigm By Carolina Solis-Herrera, MD, and Francisca Acosta, PhD
Cardiogenic Syncope in Children: Finding the needle in the haystack By David M. Bush, MD, PhD, on behalf of the University Health Pediatric
Nature’s Stress Test: An interview with Dr. Ildiko Agoston, discussing Cardio-obstetrics and the new Women’s Heart Center at University Health By

Making the Impassable Passable: Advances in coronary artery disease treatment By Angelo Amato Jr., OMS-III; Ravi Patel, OMS-III; and Ramaswamy Sharma, MS, PhD
Endovascular Management of Rutherford Grade 3, Category 6 Chronic Limb-Threatening Ischemia By Esther Shin, OMS-III, and Gabriel Bietz, MD
Aortic Valve Replacement: Seven decades of progress Angelo Amato Jr., OMS-III, and Ramaswamy Sharma, MS, PhD
Artificial Intelligence: Driven decision support for revascularization strategy in Peripheral Artery Disease By Esther Shin, OMS-III, Arya Bietz, and Gabriel Bietz, MD
BCMS President’s Message By John Shepherd, MD, President, Bexar County Medical Society
Beneath the Surface: Recognizing bullying and mental
By Grizelda Anguiano, MD
PUBLISHED BY:
Traveling Blender, LLC. 10036 Saxet Boerne, TX 78006
PUBLISHER: Louis Doucette louis@travelingblender.com
BUSINESS MANAGER: Vicki Schroder vicki@travelingblender.com
GRAPHIC DESIGNER: Jennifer Nelson jennifer@travelingblender.com
ADVERTISING SALES: AUSTIN: Sandy Weatherford sandy@travelingblender.com
SAN ANTONIO: Gerry Lair gerrylair@yahoo.com
For more information on advertising in San Antonio Medicine, Call Traveling Blender at 210.410.0014 in San Antonio and 512.385.4663 in Austin.
San Antonio Medicine is the official publication of Bexar County Medical Society (BCMS). All expressions of opinions and statements of supposed facts are published on the authority of the writer, and cannot be regarded as expressing the views of BCMS. Advertisements do not imply sponsorship of or endorsement by BCMS
EDITORIAL CORRESPONDENCE:
Bexar County Medical Society 4334 N Loop 1604 W, Ste. 200 San Antonio, TX 78249
Email: editor@bcms.org
MAGAZINE ADDRESS CHANGES: Call (210) 301-4391 or Email: membership@bcms.org
SUBSCRIPTION RATES: $30 per year or $4 per individual issue
ADVERTISING CORRESPONDENCE: Louis Doucette, President Traveling Blender, LLC.
A Publication Management Firm 10036 Saxet, Boerne, TX 78006 www.travelingblender.com
For advertising rates and information Call (210) 410-0014
Email: louis@travelingblender.com
SAN ANTONIO MEDICINE is published by SmithPrint, Inc. (Publisher) on behalf of the Bexar County Medical Society (BCMS). Reproduction in any manner in whole or part is prohibited without the express written consent of Bexar County Medical Society. Material contained herein does not necessarily reflect the opinion of BCMS, its members, or its staff. SAN ANTONIO MEDICINE the Publisher and BCMS reserves the right to edit all material for clarity and space and assumes no responsibility for accuracy, errors or omissions. San Antonio Medicine does not knowingly accept false or misleading advertisements or editorial nor does the Publisher or BCMS assume responsibility should such advertising or editorial appear. Articles and photos are welcome and may be submitted to our office to be used subject to the discretion and review of the Publisher and BCMS. All real estate advertising is subject to the Federal Fair Housing Act of 1968, which makes it illegal to advertise “any preference limitation or discrimination based on race, color, religion, sex, handicap, familial status or national origin, or an intention to make such preference limitation or discrimination.
SmithPrint, Inc. is a family-owned and operated San Antonio-based printing and publishing company that has been in business since 1995. We are specialists in turn-key operations and offer our clients a wide variety of capabilities to ensure their projects are printed and delivered on schedule while consistently exceeding their quality expectations. We bring this work ethic and commitment to customers along with our personal service and attention to our clients’ printing and marketing needs to San Antonio Medicine magazine with each issue.
Copyright © 2025 SmithPrint, Inc. PRINTED IN THE USA


Your premium doesn’t just pay for coverage—it pays it forward.
Insurance is designed to cover a claim. But what if it could do more? What if it already was and you just didn’t know it?
At TMA Insurance Trust, we manage coverage and handle claims like any insurer. But what happens beyond that is what sets us apart. When there's a surplus, the funds don't go to shareholders—because we don’t have any. Instead, that profit stays in the Texas medical community, paying it forward by funding resources physicians actually use.
Surplus Funds Pay It Forward
Reinvested in physician resources We Start Working for You With exclusive savings
You're a TMA Member You picked us for your coverage
Premiums Collected We handle coverage & claims
We call it Insurance For Good because that’s exactly what it delivers:
•Free CME courses that can save you hundreds each year
•Confidential, free mental health counseling through Anticipate Joy
•Sponsorships that keep County Medical Societies and physician networks strong
•Dedicated funding for Member Sections to stay active and connected
•Emergency relief funds through the TMA Foundation when physicians face a crisis
These practical, ongoing benefits are available to you, with no hidden costs or inflated premiums. Your TMA membership also includes exclusive insurance savings you won’t find anywhere else.
Since 1955, our focus has stayed the same: supporting Texas physicians. Through purposeful reinvestment, your insurance brings value full circle—back to you and the physician community it was created for.


Get to know your insurance options, member savings, and the programs included with your TMA membership. Visit tmait.org or call 800-880-8181, Monday–Friday, 8:00 AM–5:00 PM CST. SCAN TO CALL


John Shepherd, MD, President
Lyssa Ochoa, MD, Vice President
Jennifer R. Rushton, MD, President-Elect
Lubna Naeem, MD, Treasurer
Lauren Tarbox, MD, Secretary
Ezequiel “Zeke” Silva, III, MD, Immediate Past President
Woodson “Scott” Jones, Member
John Lim, MD, Member
Sumeru “Sam” G. Mehta, MD, Member
M. “Hamed” Reza Mizani, MD, Member
Priti Mody-Bailey, MD, Member
Dan Powell, MD, Member
Saqib Z. Syed, MD, Member
Nancy Vacca, MD, Member
Col Joseph J. Hudak, MD, MMAS, Military Representative
Jayesh Shah, MD, TMA Board of Trustees Representative
John Pham, DO, UIW Medical School Representative
Robert Leverence, MD, UT Health Medical School Representative
Cynthia Cantu, DO, UT Health Medical School Representative
Lori Kels, MD, UIW Medical School Representative
Ronald Rodriguez, MD, UT Health Medical School Representative
Alice Gong, MD, Board of Ethics Representative
Melody Newsom, BCMS CEO/Executive Director
George F. “Rick” Evans, Jr., General Counsel
Melody Newsom, CEO/Executive Director
Brissa Vela, Chief Membership & Development Officer
Yvonne Nino, Controller
Betty Fernandez, BCVI Director of Operations
Phil Hornbeak, Auto Program Director
Al Ortiz, Chief Information Officer
Jacob Hernandez, Advocacy and Public Health Specialist
Jennifer C. Seger MD, Chair
Timothy C. Hlavinka, MD, Member
John Robert Holcomb, MD, Member
Soma S. S. Jyothula, MD, Member
George-Thomas Martin Pugh, MD, Member
Adam Ratner, MD, Member
Rajam Ramamurthy, MD, Member
Patrick Reeves, MD, Member
John Joseph Seidenfeld, MD, Member
Amith Skandhan, MD, Member
Francis Vu Tran, MD, Member
Subhashini Valavalkar, MD, Member
Louis Doucette, Consultant
Brissa Vela, Staff Liaison
Gabriella Bradberry, Staff Liaison
Trisha Doucette, Editor
Ayomide Akinsooto, Student
Elizabeth Allen, Volunteer
Rita Espinoza, DrPH, Volunteer
Ramaswamy Sharma, MS, PhD, Volunteer


11 days after appendectomy, tests for acute abdominal pain revealed a
left inside the patient.
Surgical miscounts are considered never events because they are usually preventable by following established procedures.
ProAssurance offers risk assessments designed to help practices minimize errors by establishing and evaluating safety procedures and communication protocols.
With reliable procedures in place, our insureds are more likely to reduce errors in their medical practice, avoid claims, and make claims more defensible if they do occur.


By John Shepherd, MD, President, Bexar County Medical Society
We’re all pretty good at checking heart rates — but when was the last time we checked in on each other?
As physicians and physician families, we spend our days thinking about matters of the heart — both literally and figuratively. We monitor rhythms. We respond to emergencies. We often push our own needs aside for the sake of someone else’s wellbeing. It’s what we do. But if we’re being honest, we sometimes forget that strong hearts need care, too. Especially the ones right next to us.
There is no shortage of conversation around the emotional toll this work can take. Not every solution to that has to come in the form of large-scale change. Sometimes, it’s the smallest moments that keep the heart of medicine beating strong:
A mentor who asks how you’re really doing.
A partner who covers your shift when life goes sideways.
A coffee you bring to a resident just because you’ve been in their shoes at one time.
These moments matter.
And outside the hospital or clinic, our physician families are often the quiet rhythm that steadies the pace of our lives. Spouses, partners, children and friends — they’re the unsung heroes who can read the kind of day we’ve had just by the look on our face. Their care, humor and unwavering presence keep our emotional circulatory system flowing.
This month’s issue is all about the heart, so I’ve asked three people close to mine to share their thoughts on the ways we care for each other — and ourselves.

My University Medical Associates Pediatric Anesthesia Partners make my life better in immeasurable ways. Whether it’s an extra set of hands when one is needed or a check-in text after a particularly tough case, their support runs deep. We’ve laughed together at the ridiculous things children manage to swallow (and the variety really is endless), and we’ve cried together — through the unthinkable — responding to both the Uvalde school shooting and the Sutherland Springs church tragedy. Dr. Jared Foote is one of those partners I’m especially grateful for.
Then there’s my longtime teammate, Dr. Jeffrey Benzick — a psychiatrist who also happens to be a stalwart goalie in the San Antonio Men’s Lacrosse League. For more than 15 years, he’s been shutting down my shots on the field but we balance the scoreboard later over a cold beer and even better conversation. In a life that constantly pulls us in different directions, friendships like this remind me to stay grounded, present and connected.
And finally, speaking of teammates, there is none more important than my wife, Jenny. She works tirelessly in her own right to support the house of medicine. As the recent president of the Texas Medical Association Alliance, she’s been a fierce advocate for the often-overlooked heroes: the spouses and families of physicians. Jenny reminds me — often — that while the demands of a medical career are great, the need for connection, understanding and support for the Family of Medicine is just as vital.
Each of them brings something uniquely grounding to my life, and I think you’ll feel that in their words. Their perspectives — like their presence — are steady, thoughtful and full of heart.

By Jared Foote, MD
A verse from a poem declares:
Who am I to judge another
When I walk imperfectly?
In the quiet heart is hidden
Sorrow that the eye can’t see.
I would be my brother’s keeper. I would learn the healer’s art.
To the wounded and the weary I would show a gentle heart.
I’m honored to share a few personal reflections on the “quiet hearts” we encounter every day — the unseen burdens carried by our patients, our colleagues and those closest to us. I once heard this simple but profound advice: “When you meet someone, treat them as if they were in serious trouble, and you will be right more than half the time.” I’ve found that to be deeply true.
During my residency, my wife gave birth to our third child. What should have been a joyful season was quickly overshadowed by a serious peripartum complication. She remained hospitalized for nearly a month and required multiple operations. I was suddenly thrust into a profoundly anxious and uncertain world. I remember the helpless fear I felt each time she was wheeled away for surgery. By that point in my training, I had escorted over a thousand patients to the OR but had never experienced how viscerally terrifying that moment can be for patients and families.
That experience, though unpleasant, changed me. It deepened my empathy, grounded me in compassion, and made me a better physician. It also taught me how essential it is to care for each other. The support I received from friends and colleagues during that time meant everything. They showed a “gentle heart” to my “wounded and weary” soul.
I feel incredibly fortunate to work with a group of physicians who genuinely care about one another. Our relationships extend beyond polite hallway conversations. We bounce clinical questions and ideas off each other freely, without fear of being judged or “looking dumb.” We know each other’s families, share in one another’s milestones, and check in when someone is struggling. When life happens, we don’t just step in
to help out of duty, but we do it out of genuine care and sincere desire to support a friend. That kind of camaraderie makes the weight of medicine feel lighter and the daily work more meaningful.

I also want to express my deep gratitude to one mentor in particular: Dr. Deborah Rasch. I first worked with Debbie years ago as a medical student. Since then, she has guided me through every stage of my training and continues to be a steady presence in my life. I’m now honored to call her a colleague and to work alongside her as a pediatric cardiac anesthesiologist. Her influence has shaped the kind of physician I strive to be. Debbie is a gifted educator, with an encyclopedic mind, a deep well of wisdom, and is a paragon of personal integrity. She treats every patient, colleague and trainee with respect and care. Most of all, she taught me — by example — to care for each child as if they were my own. I would not be the physician I am today without her mentorship.
An effective mentor can help you see something in yourself you hadn’t yet recognized. My father used to tell me, “Stop worrying about what others think of you and start worrying about what others think about themselves when they are with you.” I’ve thought about that often in my career. I’ve had the great gift of working with many people who embody that principle and who are dedicated to learning the “healer’s art.” They help others find their place and make them feel valued, capable and seen.
We talk often about burnout, moral injury and the challenges facing physicians today. These are real and pressing concerns. But the antidote isn’t always institutional. Sometimes it’s personal. A small kindness. An encouraging word. A reminder that we’re not alone. These little acts of love ripple outward more than we realize. And usually, when we focus on lifting others, we find that our own troubled hearts are buoyed up in the process.
So, let’s be the kind of colleagues, mentors and friends who keep each other going. Let’s be the quiet strength behind someone else’s hard day. Let’s choose to be kind, patient and generous. Let’s seek out the wounded and weary quiet hearts around us, and practice showing a gentle heart.
By Jeffrey Benzick, MD
In a profession grounded in caring for others, the imperative to care for ourselves often fades into the background. Yet burnout, moral injury and emotional exhaustion have become alarmingly common in medicine — especially in the wake of increasing demands, administrative burdens and the lingering impact of the pandemic. As physicians and healthcare professionals, we are trained to respond to emergencies with composure and precision, but we often neglect to apply the same deliberate thoughtfulness to our own mental and emotional well-being.

Two personal maxims have guided me in recent years: *Respond, don’t react* — and *Boundaries are antidepressants*. They sound deceptively simple, but their application has transformed how I engage with both my patients and myself. In fact, I encourage patients, if they take nothing else away from their visits with me, to hang on to these aphorisms.
To respond over reacting is to choose mindfulness over reflex. In the clinical setting, this principle is second nature: we review labs before making a diagnosis, we pause before operating, we reflect before disclosing bad news. But when it comes to our own stress, our default is often reactivity. A packed inbox, a combative patient or an unexpected administrative demand can ignite a cascade of frustration or anxiety. The pause between stimulus and action — the breath, the moment of reflection — is where our agency lives. Cultivating that pause is an act of self-care. It creates space for wiser choices and shields us from emotional volatility.
Prior to making a decision, we have the power to ask ourselves, “What are my emotions trying to teach me?” “What is my body saying about this?” “What have my prior behaviors been in this situation?” And, often neglected, is “Where is my spirituality (or, inner sense of meaning and purpose) with this?”
The second maxim — *Boundaries are antidepressants* — speaks to an even deeper truth. Many of us entered medicine with a deep sense of duty and an identity intertwined with our work. But when
Jenny Shepherd, Immediate Past President TMAA
Just as the stress of practicing medicine is unique, so too is the stress carried by those who love and live alongside physicians. Medical families inhabit a world that outsiders rarely see: irregular schedules, last minute emergencies and milestones celebrated at odd hours or missed altogether. We joke about “doctor time,” but the reality is deeper — birthdays, anniversaries and even everyday moments are often reshaped by the unpredictability of caring for others.
The challenges extend beyond logistics. Medical families shoulder the emotional weight of medicine’s highs and lows. We absorb stories from the hospital, hold space for our loved one’s exhaustion, and sometimes stand quietly in the background while the world applauds the physician’s work without recognizing the family’s silent sacrifice. That duality — immense pride mixed with quiet fatigue — is something only another medical family truly understands. Because that reality is so unique, the usual support systems don’t always fit. Friends outside medicine might not fully understand why the call from the OR almost always wins or why plans are penciled in rather than inked. That’s where the power of community comes in — specifically, the physician family community.
It’s a place where you don’t have to explain the long nights, the lonely dinners or the long road you’ve had to travel to get to where you are. Everyone in the room already gets it. There’s comfort in that shorthand — a knowing nod, a shared laugh or a well-timed hug that says, “You’re not alone in this.”
The Alliance is more than camaraderie; it’s connection with purpose. Families come together to serve their communities, medicine
that identity becomes porous, we lose track of where our professional responsibilities end and where our personal lives begin. Boundaries are not barriers to compassion; they are the architecture that sustains it. Even more simply put, boundaries keep us out of situations which generate anxiety and tank our mood. Saying no to an extra shift, stepping away from email after hours, or carving out protected time for family and rest are not signs of weakness — they are strategic acts of resilience. The initial discomfort in setting the boundary is well worth it, when we reflect later on what we avoided.
Research continues to affirm what many of us have learned the hard way: sustained empathy requires recovery. Self-care is not indulgent — it is foundational. Whether it’s mindfulness, therapy, physical activity, spiritual practice or just intentional rest, these practices fortify us not only as clinicians, but as human beings.
So let us practice what we preach. Let us pause before we respond. Let us draw boundaries that protect our joy and our energy. And let us remember that in caring for ourselves, we model a healthier path for our colleagues, our trainees and our patients.

and each other. These shared efforts build not just friendships but a sense of meaning: we’re all part of medicine’s bigger picture, even if we don’t wear the white coat. We feel its impact in our homes, in our schedules, in the stories we carry. It’s what allows us to provide the kind of support that doesn’t need explanation. We don’t just understand this life — we live it, together. We lift each other up and hold space for one another, because the strongest hearts aren’t just the ones that endure — they’re the ones that reach out, support, and strengthen the people around them.
John Shepherd, MD, 2025 President of the Bexar County Medical Society and TEXPAC Chair, has been an active advocate for the Family of Medicine at the Texas State Capitol and has held several “Party of Medicine” events, introducing physicians on how to get involved with legislation that affects medical issues. He has been Chief of Surgery at Christus Santa Rosa Children’s Hospital and a past member of the Board of Directors of Tejas Anesthesia. Dr. Shepherd is currently a Pediatric Anesthesiologist with University Medical Associates, and serves on the BCMS Legislative Committee and the Bexar Delegation to TMA.


The Bexar County Medical Society is committed to helping our members find personal balance and improve general well-being.

BCMS Physician Wellness Program
Resources and services provided to help BCMS members maintain a healthy and well-balanced lifestyle through confidential counseling, educational resources, local events, webinars and more.


A BCMS provided resource for physician members who seek counseling from Texas-licensed professionals, discretely and confidentially through BetterHelp. Free 30 days counseling.

Free CME Wellness Coaching Webinars & Events
Nora Vasquez, MD, an Internal Medicine Doctor and Advanced Certified Physician Coach, helps physicians and healthcare professionals overcome burnout so that they can lead with joy and confidence while creating a more harmonious work-life balance that is fulfilling!

Utilize our free Find a Doc service when looking for a new physician. Our members can be found by the specified tabs provided to narrow down your preferred physician.
Physician Support Line (888) 409-0141
Psychiatrists are available to help physicians and medical students navigate the balance of a personal and professional life. Free, confidential and anonymous. No appointment necessary. Call for any issue, not just a crisis.

Physician Coach Support

Free Confidential Physician-to-Physician support line. A group of volunteer physicians using their own personal development skills and life coaching certifications to support other physicians!

Physician Health & Rehabilitation Program
Confidential advocacy group of BCMS physicians that identify and facilitate recovery success for physicians with substance use disorder (Alcohol and/or Drugs) and depression, through support and monitoring.
Please scan QR code for more information and available resources for BCMS Members


By Victoria Kohler-Webb
The Bexar County Medical Society proudly supports physicians and physician families through all stages of their medical journey. One of our biggest achievements is our annual BCMSA Medical Student and Allied Health Student Scholarship program, providing significant cash awards to local Bexar County students to assist them on their path.
This year, we are honored to present four students with the BCMSA scholarships in recognition of their exceptional performance and tireless commitment to their professional program and their future career. The Bexar County Medical Society Alliance wish-
Jessica Autrey
University of the Incarnate Word School of Osteopathic Medicine
2025 BCMSA Medical Student Scholarship, $1,500

“I am incredibly honored to receive this scholarship. I appreciate the support of my school, UIWSOM, in nominating me and to the BCMSA for providing this award. Medical school is an expensive endeavor, and I am very grateful for the financial support and confidence in my abilities. Thank you again for your support of students!”
Julieta Ruiz
St. Mary's University, Major Biology/Minor Chemistry, and planning to attend Physician Assistant graduate program
2025 BCMSA Allied Health Scholarship $1,000

“This scholarship will make a meaningful difference as I continue working toward my goal of becoming a Physician Assistant and serving the communities that have shaped me. It means so much to have my goals and efforts recognized and supported in this way. This award will help ease the financial burden of my education and allow me to stay focused on becoming the kind of provider I aspire to be: compassionate, community-minded and dedicated to improving access to care. Thank you for believing in my potential and for investing in my journey.”
es to thank the Texas Medical Association Foundation for its support and for the Medical Student Scholarship matching grant to make this award even more meaningful. Congratulations and best wishes for a wonderful and rewarding career!

Victoria Kohler-Webb, BBA, MS Marketing Statistics, is the BCMSA Immediate Past President, served as 2024-2025 TMAA Board Secretary and currently serves as Membership Liaison. She and Ben, an ENT/Head & Neck Surgeon, are proud Aggies and parents to Luke, 16, and four rescue dogs
Patryk Tomaszkiewicz
University of the Incarnate Word School of Osteopathic Medicine
2025 BCMSA Medical Student Scholarship, $1,500

“I am honored to be this year’s BCMSA Scholarship recipient. As a 4th year medical student, this scholarship will help with my loans/living expenses and will certainly help in the long term. I will be applying into General Surgery, and am very excited to be starting residency next year! Thank you for considering me for this award. I am truly honored!”
Brittany Edwards
University of the Incarnate Word Doctor of Physical Therapy
2025 BCMSA Rebecca Christopherson Memorial Allied Health Scholarship, $1,000

“I am deeply honored to receive the Rebecca Christopherson Memorial Scholarship from the Bexar County Medical Society Alliance, and I extend my heartfelt gratitude for this recognition. In the everyday moments — the victories and the hardships — I have learned that life’s beauty is inseparable from its fragility. Rebecca Christopherson’s story embodies this truth, and it is a privilege to carry her memory forward. Thank you for supporting me in the journey of Physical Therapy."
TOGETHER, WE CAN IMPROVE COMMUNICATION AND HEALTH LITERACY SKILLS
Join us for a free online learning series designed to empower health professionals with health literacy education, resources and knowledge-sharing tools. The series is presented by Health Confianza, an award-winning health literacy nonprofit funded by Bexar County and housed at The University of Texas Health Science Center at San Antonio.
Who is this for? Health professionals, including physicians, nurses, community health workers, social workers and pharmacists.
Join our expert team the first and third Friday of each month

TOPICS:
• Acknowledging perspectives
• Shame/stigma; Creating a shame-free environment
• Plain language
• Shared decision-making
• Teach Back


WHAT: Free, six-part series
DATE/TIME: Sept. 5th - Nov. 21, 1st and 3rd Fridays of the month, 12:00-1:00 p.m.


REGISTER: bit.ly/Communicatingwith Confianza CE credits are available
By Kit Bjella Powers, MD, FACC, FASE, and Natalie Nyren, PA-C
The evaluation and management of pericarditis, a clinical syndrome referring to inflammation of the pericardial layers of the heart, has undergone revolutionary changes in the last 10 years. The American College of Cardiology has recently published an update of clinical guidelines; this update provides a concise summary of diagnoses and treatment strategies when confronting a patient with pericarditis. New drugs are available for management of acute and recurrent pericarditis, providing new tools to help manage this condition. Over the last few years, we have seen more cases of vaccine-associated pericarditis, as well as viral pericarditis and myopericarditis, especially associated with COVID-19 infections. While causes may be infectious or noninfectious, most cases remain idiopathic. Idiopathic, viral infection or immune-mediated pericarditis is seen in developed countries, while tuberculosis remains the most common cause in developing countries.
The initial step in approaching a patient with symptoms that may be due to pericarditis is to make sure this is an appropriate diagnosis. Pericarditis is a great imitator of other cardiac conditions, including acute myocardial infarction. Approaching a patient with chest pain, EKG abnormalities concerning for ischemia or infarct, and elevated biomarkers can be challenging.
From a clinical standpoint, the quality of chest pain is a key distinguishing feature between acute coronary syndrome and pericarditis. Typically, the pain of pericarditis is sharp, piercing or stabbing, with a pleuritic component that hurts with change of position and with deep breathing or coughing. A classic clinical feature is improvement of this pain while sitting up and leaning forward, thought to help relieve some of the pressure causing the pain.
On the other hand, pain associated with acute coronary syndromes is typically described as pressure or dull aching, mid-chest and not pleuritic; the pain is often described as crushing, constricting or squeezing. Heart attack-type pain may be referred to the jaw, midback, left shoulder, left arm or both arms; there are usually some associated symptoms such as diaphoresis, nausea or shortness of breath. Of course, generalization of the symptoms associated with acute coronary syndromes or myocardial infarction is complicated by the atypical presentation that can be seen in many patients, including the elderly and women, as well as those with angina equivalent symptoms.
A friction rub on physical exam can be a helpful finding associating the clinical symptoms with a pericarditis syndrome; it is less likely to
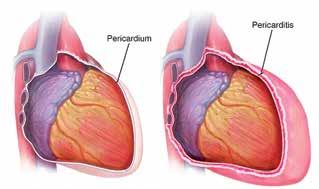
© Mayo Foundation For Medical Education And Research. All Rights Reserved.
be found in acute coronary syndromes. Ewart’s sign, consisting of dullness with bronchial breath sounds below the left scapula, may be found in large pericardial effusions and may be useful on occasion.
The EKG in acute pericarditis often will help the clinician distinguish between cardiac ischemia seen with acute coronary syndromes vs. inflammation of the pericardium seen in pericarditis. These distinguishing features are outlined in Fig. 1 and 2.
Biomarker testing can also be helpful in distinguishing acute coronary syndromes vs. pericarditis. In pericarditis, the elevation of troponin is generally low-level with a flat trajectory time course, while biomarker elevation in acute coronary syndromes is usually more elevated (often dramatically so) with a steep rising trajectory over time.
Bedside echocardiography is a valuable tool to help assess possible pericardial effusion associated with pericarditis, or signs of inflammation of the pericardium; in acute coronary syndromes, identification of regional wall motion abnormalities may help distinguish the presentation.
Once the diagnosis of pericarditis is made, it is appropriate to distinguish acute vs. chronic symptoms. The ACC guidelines define acute pericarditis as symptoms resolving within four weeks, while recurrent pericarditis refers to flares after initial recovery.
As outlined in the recent ACC guidelines, the diagnosis of acute pericarditis should be based on the presence of at least two of the following four criteria: 1) characteristic chest pain, 2) pericardial friction rub, 3) characteristic electrocardiographic changes, and 4) new or worsening pericardial effusion. Laboratory workup, including assessment for inflammation and myocardial damage, is also recommended. Cardiac magnetic resonance (CMR) may be helpful when the diagnosis is uncertain, when echocardiographic imaging is challenging, or when myocardial involvement is suspected.
Treatment of acute pericarditis can be initiated as an outpatient and most of these patients will not need to be hospitalized. However, any of the red flag findings associated with acute pericarditis should be a reason to consider hospitalization: 1) associated acute arrhythmias such as atrial fibrillation, atrial flutter or other arrhythmia, 2) high fever (>38°C), 3) subacute onset, 4) very large effusion or signs of tamponade, 5) signs of myocardial involvement, and 6) no response to initial treatments. Factors that should also prompt a more cautious approach include immunosuppressed patients, patients on oral anticoagulation and pericarditis in the setting of trauma.
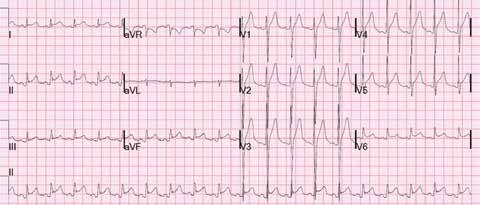
Fig.1 This EKG shows some of the classic findings indicative of pericarditis: Lead II shows PR segment depression, an early change found in the beginnings of pericardial inflammation. There is PR segment in lead aVR. Also noted are upward-coving ST segment changes prominent in the inferior and lateral precordial leads, but occurring in a diffuse pattern of ST segment changes (affecting multiple leads and in non-anatomical lead groups). ST elevation is more prominent in lead II compared to lead III.
https://i0.wp.com/rushem.org/wp-content/uploads/2019/01/Classic-Pericarditis-EKG. jpg?w=1600&ssl=1
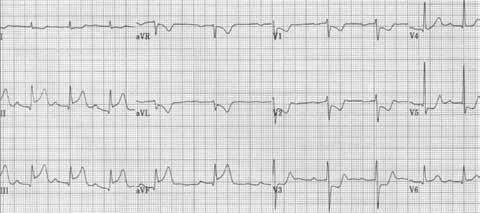
Fig.2 EKG in acute myocardial infarction: This is a classic presentation of acute inferior myocardial infarction, with dramatic ST segment elevation in the inferior leads (anatomical lead groups II, III and aVF). The ST elevation in lead III is of greater magnitude than lead II; this strongly favors acute MI. There are reciprocal changes of ischemia in the anterior precordial and high lateral leads, reflecting an inferolateral or posterior injury pattern. Note the absence of PR segment depression, and absence of PR segment elevation in lead aVR.
https://i0.wp.com/rushem.org/wp-content/uploads/2019/01/STEMI.jpg?w=959&ssl=1
The initial treatment for uncomplicated pericarditis consists of nonsteroidal anti-inflammatory drugs (NSAIDs) for symptoms with a 2- to 4-week taper of these agents as symptoms subside. Many clinicians will also treat concurrently with proton pump inhibitors (PPIs) to reduce the possibility of gastric inflammation or ulcer formation. Additionally, current guidelines call for a 3-month course of colchicine to reduce the possibility of recurrence of pericardial information. During this 3-month period, strenuous activity should be avoided. The use of corticosteroids in the treatment of acute pericarditis has generally fallen out of favor; there is evidence that corticosteroid use may prolong infectious pericarditis and increases the likelihood of recurrent pericarditis. Corticosteroid use may be indicated in a
few special instances: patients unable to take NSAIDs, pregnancy, autoimmune or similar pericarditis such as immune checkpoint inhibitor-associated pericarditis.
Special cases of pericarditis present a need for urgent action: cases of purulent pericarditis associated with bacterial infection, findings of a large pericardial effusion associated with tamponade or impending tamponade, and pericardial inflammation associated with malignancy require careful and expedient intervention.
Recurrent pericarditis may occur in up to 30% of patients after an initial episode of acute pericarditis. Per ACC guidelines: “Treatment should consist of an NSAID, typically with a 2- to 4-week taper after the resolution of symptoms, along with at least six months of colchicine (with weight-adjusted dosing). Corticosteroids (at low doses) should be reserved for those who have failed multiple attempts at therapy with an NSAID plus colchicine. Anti-interleukin 1 therapy (e.g., anakinra and rilonacept) has been shown to be beneficial in patients with refractory, corticosteroid-dependent disease. Other options for consideration in refractory disease include azathioprine, methotrexate, mycophenolate mofetil and intravenous immunoglobulins. Surgical pericardiectomy is considered a last option.”
Pericarditis, especially if chronic or recurrent, can lead to the development of constrictive pericarditis. This syndrome is characterized by thickening and scarring of the pericardium, often associated with calcification. This leads to development of a rigid shell around the heart, typically with adhesions of the parietal pericardium to the visceral pericardium and diminishing the intra-pericardial volume. In this situation, there is no longer enough “room” or space for the heart to operate optimally or with normal efficiency. Because of the reduced intra-pericardial volume, increased filling of one ventricle causes concomitant decrease of filling of the other ventricle (so-called “ventricular interdependence”); this phenomenon is the basis for physical findings such as pulses paradox, when breathing causes respiratory variations in right ventricular filling, which in turn affects left ventricular volume and cardiac output/ stroke volume.
Constrictive pericarditis can be seen after infectious pericarditis, previous heart surgery, history of radiation therapy, autoimmune diseases or in many cases that are idiopathic. Key symptoms include fatigue, exercise intolerance and development of edema. A collection of fluid anywhere in the body that is not well explained (pleural effusion, ascites, leg edema, etc.) should prompt consideration of constrictive pericardial physiology.
Imaging studies are the key to developing a treatment strategy for constrictive pericarditis. Echocardiography, cardiac CT and cardiac MRI help characterize the constricted physiology involved and help with the development of a plan for treatment. Cardiac catheterization is useful to demonstrate hemodynamic findings that are characteristic of constrictive pericarditis.
Once constrictive pericarditis has developed, medical treatment is of limited benefit — helpful for symptoms (diuretics from swelling, anti-inflammatory medications) but the definitive treatment is surgical pericardiectomy. ACC guidelines encourage a multidisciplinary approach to management of complex cases of pericarditis and pericardial constriction, and if needed, a referral to a specialized Pericardial Disease Center with expertise that can improve outcomes compared to a medical facility with less volume of these cases and less expertise.
In summary, the management of pericarditis can be challenging and complex. Fortunately, there are new treatments and evidence-based guidelines available that provide help navigating the problems and pitfalls associated with this condition and help improve patient’s outcomes.
5. Adler, Y., Charron, P., Imazio, M., & Sagristà-Sauleda, J. (2020). Management of pericardial diseases: 2020 ESC guidelines. European Heart Journal, 41(21), 1577-1600. DOI: 10.1093/ eurheartj/ehaa571. European guidelines outlining the diagnostic and therapeutic management of pericardial diseases, including acute, recurrent and constrictive pericarditis.
6. McDonald, S.A., et al. (2019). Purulent pericarditis: Diagnosis, treatment, and outcomes. Journal of Cardiology, 73(4), 303-310. DOI: 10.1016/j.jjcc.2018.06.016. This article covers the management of purulent pericarditis, emphasizing early intervention and antibiotic therapy.
7. Nishimura, R.A., & Tajik, A.J. (2021). Constrictive Pericarditis: Diagnostic and Management Challenges. Journal of the American College of Cardiology, 77(3), 345-355. DOI: 10.1016/j. jacc.2020.10.053. An article discussing the pathophysiology, diagnosis, and surgical management of constrictive pericarditis.
8. Chan, D.Y., & Lee, L.S. (2018). Cardiac Magnetic Resonance Imaging for Pericarditis: Role in Diagnosis and Management. Journal of Clinical Imaging Science, 8, 24. DOI: 10.4103/jcis. jcis_54_18. A study on the utility of cardiac MRI in diagnosing pericardial diseases, especially when echocardiography is inconclusive.
9. Swaans, M.J., et al. (2017). Diagnostic value of the pericardial friction rub in acute pericarditis. The Netherlands Heart Journal, 25(8), 514-520. DOI: 10.1007/s12471-017-1010-9. Exploring the diagnostic value of physical examination findings, particularly the pericardial friction rub, in patients with acute pericarditis.
10. Rush Emergency Medicine: EKG: Pericarditis Vs. STEMI. https://rushem.org/2019/01/20/ekg-pericarditis-vs-stemi/
References:
1. American College of Cardiology (ACC) Guidelines on Pericarditis (2025). Available at: https://www.acc.org/latest-in-cardiology. The American College of Cardiology’s comprehensive guidelines for the management of pericarditis, including diagnostic criteria and treatment strategies.
2. Imazio, M., & Brucato, A. (2011). Management of acute pericarditis: A systematic review. JAMA, 305(15), 1593-1600. DOI: 10.1001/jama.2011.464. This systematic review addresses treatment options, including NSAIDs, colchicine and corticosteroids, for acute pericarditis.
3. Imazio, M., et al. (2020). Colchicine for recurrent pericarditis. The New England Journal of Medicine, 367(3), 249-256. DOI: 10.1056/NEJMoa1200237. A landmark study examining the role of colchicine in preventing recurrence of pericarditis.
4. Li, X., et al. (2023). Pericarditis after COVID-19 Vaccination: A Review of Current Evidence. Journal of the American College of Cardiology, 81(13), 1235-1244. DOI: 10.1016/j. jacc.2023.02.044. A review focused on the emergence of vaccine-associated pericarditis, particularly in the context of COVID-19.

Kit Bjella Powers, MD, FACC, FASE, is a board-certified cardiologist who has been practicing in the greater San Antonio area for the last eight years. He is a cardiologist with University Medicine Associates, a primary care provider group at University Health. He cares for patients at University Health’s Southeast and Dominion clinics. He has focused on non-invasive and general cardiology and has special expertise in echocardiography. Dr. Powers also serves on the Board of the San Antonio Chamber Choir and has an undergraduate degree in Music. He is a member of the Bexar County Medical Society.

Natalie Nyren, PA-C, is a physician assistant who works in an outpatient cardiology clinic at University Health in San Antonio, Texas. She is board-certified in Lifestyle Medicine and is a certified clinical culinary coach who is dedicated to helping her patients achieve optimal health and wellness through evidence-based lifestyle interventions. With over 10 years of experience in the field, she is passionate about empowering individuals to take control of their health by making sustainable lifestyle changes.

By Carolina Solis-Herrera, MD, and Francisca Acosta, PhD
The cardio-renal-metabolic syndrome (CRM syndrome), formerly encompassed by the term "metabolic syndrome," represents a modern, systemic approach to the intersection of metabolic, renal and cardiovascular diseases. Growing clinical evidence and evolving guidelines highlight the necessity to address this interconnected spectrum to improve outcomes and patient quality of life.
Metabolic syndrome traditionally referred to a cluster of conditions — insulin resistance, hypertension, dyslipidemia and central obesity — that predispose individuals to increased risk for type 2 diabetes mellitus (T2D) and atherosclerotic cardiovascular disease (ASCVD). However, the term cardio-renal-metabolic syndrome now denotes a broader concept: a multisystem disorder marked by the intertwined progression of metabolic risk factors (e.g., T2D, obesity), chronic kidney disease (CKD) and cardiovascular disease (CVD) that accelerate each other's onset and complications.
CRM syndrome thus reflects a progressive, multi-organ disease beginning with metabolic risk and culminating in clinical manifesta-
tions such as CKD and heart failure, often with devastating consequences like hospitalization and cardiovascular (CV) mortality.
The prevalence of diabetes and, by extension, CRM syndrome is sharply rising. For example, in Mexico, diabetes prevalence reached 18.3% in adults in 2022, up from 10.7% in 2000. In the United States, 42 million adults have T2D, and of these, nearly 40% will develop CKD. Such convergence of risks creates a population highly vulnerable to adverse outcomes.
Key epidemiological intersections include:
• Up to 40% of those with T2D develop CKD.
• 63% with CKD also harbor CVD.
• Roughly one-third of T2D patients exhibit manifest CVD.
• 20–40% of those with heart failure have T2D, and 30–40% have CKD.
• The coexistence of these conditions magnifies the risks of hospitalization, medical intervention and death.
The relationship between the heart, kidneys and metabolism is synergistic and bidirectional:
• Metabolic factors like hyperglycemia and insulin resistance foster vascular and renal injury.
• Declining renal function exacerbates hypertension and vascular inflammation.
• Heart failure worsens renal perfusion, diminishing metabolic resilience.
Consequently, early occurrence or progression in one organ system accelerates dysfunction in the others. For example, albuminuria (measured by urine albumin-to-creatinine ratio, UACR) may be evident 10–20 years before a detectable decline in glomerular filtration rate (eGFR), signaling early renal insult even with ostensibly normal kidney function.
To counteract the compounded risks, updated guidelines from bodies like the American Diabetes Association (ADA) and KDIGO recommend comprehensive, risk-based screening for patients with diabetes and other at-risk groups:
• UACR testing is the gold standard for detecting early kidney damage yet remains underutilized — only 21% of high-risk patients were assessed for albuminuria pre-CKD diagnosis, compared to 90% tested for eGFR.
• Durable detection of UACR ≥30mg/g for three months or eGFR <60mL/min/1.73m² confirms CKD. Notably, up to 67% of T2D patients with early CKD remain undiagnosed in the absence of UACR monitoring.
• Coexistence of albuminuria amplifies CV mortality fourfold and heart failure hospitalization fivefold in T2D patients — highlighting the predictive and actionable value of routine, thorough screening.
Management of CRM syndrome has moved beyond glucose-centric strategies. Multifactorial intervention is now central, encompassing:
• Strict glycemic control
• Blood pressure and lipid management
• Regular screening for kidney injury (UACR and eGFR)
• Use of medications with proven CV and renal benefits (e.g., SGLT2 inhibitors, GLP-1 receptor agonists, finerenone)
• Intensive lifestyle modifications, including dietary counseling, physical activity and cessation of smoking.
For example, SGLT2 inhibitors, initially developed as antihyperglycemics, now demonstrate robust benefits in reducing heart failure hospitalizations, slowing CKD progression, and lowering CV mortality, independent of glucose effects. These results are likely to relate to pleiotropic effects: improved cardiac and skeletal muscle energetics, reduction of inflammation, and modulation of adiposity and arterial stiffness.
Recent studies underscore the potential impact of newer medications. In 2024, a study on semaglutide found a 40% reduction in CKD outcomes compared to 12% for placebo in patients with T2D, illustrating the potential of incretin-based therapies to modify the natural history of CRM syndrome.
Finerenone, a nonsteroidal mineralocorticoid receptor antagonist, now holds FDA approval for heart failure with preserved ejection fraction (HFpEF), following trials demonstrating significant reductions in CV death and total heart failure events when compared to placebo.
The re-conceptualization of CRM syndrome compels clinicians to adopt early, multidisciplinary and comprehensive risk management strategies. Routine detection of microvascular and macrovascular compromise — by combining metabolic, cardiac and renal evaluations — offers a tangible pathway to limit progression, reduce hospitalizations, and save lives. Failure to comprehensively screen and intervene means missing crucial opportunities to blunt the tide of this multisystem, progressive disorder.
Ongoing research and evolving clinical practice guidelines promise continued refinement of strategies to combat this modern epidemic, ultimately improving patient longevity and quality of life.
References:
1. de Boer, I.H., et al. Diabetes Care. 2022;45(12):3075-3090
2. American Diabetes Association. Diabetes Care. 2024;47(S1):S1-S321
3. Chu, C.D., et al. JAMA Netw Open. 2023;6(7):e2326230
4. Shlipak, M.G., et al. Kidney Int. 2021;99:34
5. Heidenreich, P.A., et al. J Am Coll Cardiol. 2022;79:e263
6. Rossing, P., Epstein, M. Am J Med. 2022;135(5):576-580
7. Perkovic, V., et al. N Engl J Med. 2024;390:208-219
8. Scirica, B.M., et al. JAMA Cardiol. 2018;3(2):155-163

Carolina Solis-Herrera, MD, is Chief of the Endocrinology Division and Associate Professor of Medicine at UT Health San Antonio, where she also directs the Diabetes and Endocrinology Clinics and the Center for Diabetes Excellence. She is an accomplished physician-scientist with over 70 peer-reviewed publications, focusing her research on diabetes, obesity and the cardiovascular effects of novel anti-diabetic therapies, particularly SGLT2 inhibitors. Dr. SolisHerrera is committed to advancing diabetes care, driving innovation, and mentoring the next generation of physicians and researchers.

Francisca Acosta, PhD, is an Assistant Professor/Researcher in Endocrinology and Biochemistry at UT Health San Antonio, with expertise in metabolism, biomedical engineering and translational medicine. She earned her PhD from the UTSAUTHSA Graduate Program in Biomedical Engineering and continues to study the impact of metabolic dysregulation on musculoskeletal health and adiposity. Dr. Acosta is also dedicated to mentoring students and advancing the field through her interdisciplinary research.

By David M. Bush, MD, PhD, on behalf of the University Health Pediatric Cardiology Specialists
As another academic year gets underway for the children of South Texas, the opportunity for routine physical activity through physical education classes, team sports and personal training arises. With this comes the risk of exercise-mediated cardiac events, including a loss of consciousness. While the vast majority of these are “neurocardiogenic,” reflecting a protective, relatively harmless reflex, a very few will be the result of an underlying, potentially life-threatening condition. Recognizing and expeditiously treating these can, quite literally, be life-saving. But how to identify the proverbial “needle in the haystack?” In this article, my team and I would like to share our approach to children and young adults who have experienced a sudden loss of consciousness.
Scope of the Problem
Syncope — the sudden loss of consciousness — is a ubiquitous event in pediatrics. It has been estimated that as many as 25% of all children will experience at least one episode before the age of 18 years (Gilpin, 2024). Historically speaking, the phenomenon has also been recognized for more than two millennia. It was first described by Hippocrates in his Aphorisms: “Those who are subject to frequent and severe fainting attacks without obvious cause die suddenly.” (Mirchandani, 2003). Within his observation is the recognition that those with “obvious causes” of syncope do not experience such outcomes. Indeed, the risk of a sudden cardiac death in pediatrics is extremely low, estimated at approximately 1 in 200,000 annually, a number which is far eclipsed by accidental causes. Thus, the approach to the patient with syncope begins with a thorough inquiry into the circumstances surrounding the event in an effort to root out the “obvious causes.”
Causes of pediatric syncope can be broadly placed into system categories that include the following (in order of decreasing prevalence): neurocardiogenic (95%), psychiatric (2.5%), cardiac (1%), neurologic (1%) and other (0.5%). The broader differential within these categories is demonstrated in Table 1.
The use of broad categories is helpful in that it permits symptom grouping. For example, while both neurocardiogenic and cardiac causes ultimately result from a drop in blood pressure with a resultant drop in cerebral perfusion, it is the manner and rapidity of the drop (along with
the potential circumstances inducing it) that permits categorical differentiation. Thus, an adolescent who experiences an episode of syncope while standing in line in the heat of the day at a local amusement park should suggest the strong possibility of a neurocardiogenic cause, particularly when the event is preceded by symptoms consistent with gradual alterations of vascular tone (such as dizziness, lightheadedness, coning of the vision, etc.). Conversely, a child who passes out when diving into a pool or when engaging in an argument is quite a bit more worrisome, particularly if either event is unaccompanied by antecedent symptoms.
Broadly speaking, cardiovascular causes of syncope can be divided into electrical, structural and hemodynamic subtypes (Table 2). While there is some overlap in this categorization, it does permit for a more focused discussion of causes as well as a useful approach to testing. While the vast majority of the structural forms of cardiovascular disease should have some physical examination stigmata, echocardiography is most likely to yield a diagnosis. This contrasts with the possible electrical diagnoses, which may be revealed by screening electrocardiography or provocative testing, but often require some form of ambulatory rhythm monitoring to permit symptom-rhythm correlation. Finally hemodynamic causes will often require laboratory testing and, in some instances, cardiac catheterization for further assessment.
As was alluded to above, the approach to pediatric syncope must begin with a thorough history. Much like a detective, having the patient
Mitral Stenosis/Insufficiency Bradyarrhythmias Anemia
Hypertrophic Cardiomyopathy High-Grade AV Block Pulmonary Hypertension Form
Dilated Cardiomyopathy Sick Sinus Syndrome - Hereditary Hemorrhagic Telangectasia
Restrictive Cardiomyopathy Blocked Atrial Tachyarrhythmias - Eisenmenger Complex
Subaortic Stenosis Tachyarrhythmias - Idiopathic
Aortic Valve Stenosis Concealed Pathways (SVT/VT)
Supravalvar Aortic Stenosis Manifest Pathways (WPW)
Coronary Stenosis/Anomaly Ion Channelopathies (LQTS, etc.)
Arteriovenous Fistula Arrhythmogenic Cardiomyopathies (ARVC, etc.)
Intracardiac Tumor Idiopathic (VT/VF)
Pericardial Effusion
walk through the event in a stepwise fashion can be quite elucidating. This is particularly true when starting with an open-ended form of questioning before using closed-ended questions to fill in the gaps. Indeed, in a study of 100 pediatric patients between 4-10 years with new onset syncope, a history alone correctly identified the 97 patients ultimately diagnosed with neurocardiogenic syncope from the three with a cardiac cause (Kertesz, 2004). This is not to minimize the role of the physical examination in the process as the presence of a pathological murmur or stigmata of another disease process can further justify additional testing.
Beyond a thorough history and physical examination, resting electrocardiography (ECG) is invaluable in the process of differentiating cardiovascular causes from other forms. It is the “gold standard test” for many forms of ion channelopathy — conditions that arise from genetic changes in ion signaling in cardiac myocytes that destabilizes the action potential. It is also the primary means of diagnosing conditions such as Wolff-Parkinson-White syndrome, which can be associated with supraventricular tachycardia and atrial fibrillation with ultra-rapid ventricular response. Finally, a resting ECG can offer unique insights into those with potential underlying cardiomyopathy, in a manner which is complimentary to imaging modalities.
Use of other imaging modalities, such as echocardiography, standard radiography and advanced cardiac imaging (CT, MRI) should be guided by the above testing. Each of these tests can be individually diagnostic of particular conditions, but are rarely diagnostic alone. Thus, given the ubiquity of pediatric syncope, minimizing the “size of the haystack” before applying the testing will not only increase diagnostic yield, but also help to control healthcare costs.
1
The selection of treatments for pediatric syncope clearly depends upon the cause. For neurocardiogenic forms, lifestyle changes alone may be sufficient to suppress further episodes. Indeed, it is a common historical point that a parent will have experienced similar childhood episodes but “grew out of them.” While this is certainly possible, it is equally likely that habits were adopted that reduced triggering of the vasovagal reflex. In other circumstances, such as cardiovascular
(electrical) causes, interventional treatments (such as ablation), medical treatments (such as beta-blockade) or even surgical ones (such as sympathetic denervation) can dramatically reduce or eliminate further episodes. Regardless of the cause or treatment, foremost in children’s minds is returning to their “normal life.” For many, this includes engaging in competitive athletics. This area provides perhaps the greatest challenge for clinicians, who are asked to provide “clearance” for activities for which even a history of neurocardiogenic syncope may place the child at increased risk of harm. Complicating this decision is a loss of “paternalistic guidelines” with their clear, consensus-driven proscription regarding certain activities in certain conditions. In the current practice era, the emphasis is now on a shared decision-making process in which the physician acts as the subject matter expert, apprising families and athletic staff about the condition in question and reviewing strategies to mitigate any risks. Gone is the “clearance form,” replaced by the “medical contract,” which acknowledges the value of a particular activity to a patient and the agreement of all parties to abide by the risk mitigation strategy.
Pediatric syncope is a common problem, which is fortunately, rarely associated with a life-threatening condition. Promptly finding those “needles in the haystack,” however, can be the difference, quite literally, in saving a life. The most important tools in this process, however, have been with us for centuries — a thorough history and physical examination, along with a knowledge of how the “obvious causes” might present. My partners and I are happy to assist you both in the diagnosis and management of these and any other cardiac patients. We are committed to helping your patients return to their regular lives in a thoughtful and responsible manner.
My partners and I are privileged to have joined the University Health as partners in University Medicine Associates at the beginning of this year. Each of us came from the former Pediatrix Cardiology of San Antonio group and bring the experience of practicing in the South Texas area for nearly three decades. With expertise and national recognition in not only pediatric cardiology but also subspecialty areas such as interventional cardiology, electrophysiology, exercise physiology and adult congenital cardiology, we are uniquely capable of providing state-of-the-art care not only for cardiovascular causes of syncope but also the breadth of other cardiovascular conditions afflicting pediatric and adult congenital patients. With our colleagues from UT Health San Antonio, services in fetal cardiology, as well as surgical correction of congenital defects are available. We remain committed to serving the entire Bexar County community and continue to provide supportive consultative and procedural services.

David M.
Bush,
MD, PhD, Medical Director of
University
Health
Pediatric Cardiology Specialists, is a pediatric cardiologist and electrophysiologist. Dr. Bush is a member of the Bexar County Medical Society.

By Trisha Doucette
Women’s Heart Center: A Trailblazer in South Texas
University Health launched the Women’s Heart Center in May — the first of its kind in South Texas — with a mission to enhance heart health for women throughout all stages of life, with a special focus on pregnancy. Through multidisciplinary collaboration and comprehensive pre-pregnancy counseling, the Women’s Heart Center aims to provide proactive, personalized care.
Leading this initiative is Dr. Ildiko Agoston, who serves as both the founding Director of the Women’s Heart Center and Director of Cardiovascular Imaging at University Health. A dedicated advocate for women’s cardiovascular wellness, Dr. Agoston emphasizes the importance of Cardio-obstetrics, a specialized field that combines expertise from multiple disciplines. “We have a very important segment of care that is different from anywhere in the community and that is Cardio-obstetrics,” Dr. Agoston shared. “This is the joint effort of a multidisciplinary team, and my goal is to make it easy for pregnant women to see multiple doctors on the same day, at the same place, and offer them the diagnostic tools needed to monitor their conditions.” The Women’s Heart Center currently dedicates two days each week exclusively to Cardio-obstetrics.
Cardio-obstetrics is an emerging subspecialty in which cardiologists collaborate closely with obstetricians, gynecologists, maternal-fetal medicine specialists, anesthesiologists, cardiovascular surgeons, pulmonologists and congenital heart disease experts. Recently recognized as a formal subspecialty, there have been discussions around establishing fellowship programs to train clinicians in this intricate area of care. “It’s complex — you’re caring for two patients, the mother and the baby,” Dr. Agoston noted.
Many women may be unaware they have underlying heart conditions such as aortic stenosis, cardiomyopathy, valvular disease, or genetic disorders like Marfan syndrome, Loeys-Dietz syndrome and various connective tissue disorders. These conditions often go undetected in younger women, as symptoms may not yet have appeared. Established care from a PCP or OB-GYN can lead to timely referrals for cardiovascular evaluation and counseling prior to pregnancy.
Some congenital heart conditions — such as mitral valve stenosis, cyanotic congenital heart disease, pulmonary atresia and single-ventricle physiology — require lifelong follow-up by congenital heart specialists. Moreover, women with pulmonary hypertension or heart failure face
heightened risks during pregnancy. The World Health Organization’s classification system for maternal cardiovascular risk highlights these concerns, with Class 4 indicating cases where pregnancy is strongly discouraged due to serious health threats (Table 1).1 “These are desired pregnancies. These women have the best intentions — they just don’t know this is a dangerous journey for them,” Dr. Agoston shared.
The majority of patients referred to the Women’s Heart Center are in need of managing gestational hypertension, gestational diabetes, and mitigating the risk of pre-eclampsia — which can lead to intrauterine growth restriction, low birth weight, and even perinatal mortality.
There are currently well-established guidelines, originally presented by the European Society of Cardiology, and subsequently adapted by the American Heart Association.2,3 However, there are very few cardiac medications that are safe to administer during pregnancy for the management of hypertension. The Cardio-obstetrics team carefully weighs the risks and benefits for both mother and child when crafting individualized management plans.
In challenging cases, the second trimester often presents the best window for intervention. Dr. Agoston said, “For example, we had one patient with Chronic Inflammatory Demyelinating Polyneuropathy who had a thrombosed indwelling catheter during pregnancy despite anticoagulation. The patient was getting regular IVIG therapy and the catheter was needed. We had to extract a large thrombus to prevent pulmonary embolism during the second trimester of her second pregnancy. My colleague, Dr. Ahmed Almomani, performed a successful therapy in the cath lab using the AngioVac system to remove the thrombus.”
As patients near delivery, the priority shifts from medication to timing. “What’s interesting about managing these patients as they are in their third trimester and are closer to delivery, is that instead of giving more medications, we opt to deliver earlier than full term so we can treat their underlying conditions — heart failure, valve disease or blood pressure. For many patients, the solution to their problem is to deliver. This is where it takes all of the subspecialists to determine when the baby is ready to be delivered without compromising the mother’s health,” said Dr. Agoston.
A personalized delivery care plan is coordinated by the multispecialty team, weighing the pros and cons of each delivery method, based on the hemodynamic stability of the mother. “It’s important because one of the leading causes of morbidity/mortality in pregnant women is cardiovascular disease, especially in Texas,” stated Dr. Agoston.
For example, in patients with severe aortic stenosis or mitral stenosis, prolonged second phase during a vaginal delivery could result in pulmonary edema. On the other hand, a C-section may lead to more serious complications in certain cases due to excessive bleeding or infection. To guide decisions, in rare instances aggressive hemodynamic monitoring with arterial lines and right heart catheterization is needed.
WHO Pregnancy
Risk Category
Risk Description
I No detectable increase in maternal mortality and no/mild increase in morbidity risk
II Small increase in maternal mortality and moderate increase in morbidity risk
II–III
Moderate increase in maternal mortality morbidity risk
Postpartum care — often overlooked — is vital for long-term heart health. Women who experienced pre-eclampsia or gestational diabetes during pregnancy have a higher risk of developing hypertension or diabetes later in life, even years down the road. Pregnancy is a stress test — it shows you what can happen if you gain 10 pounds later in life and provides a snapshot of your hemodynamic stability as you age. Dr. Agoston said, “I tell my patients that this is a failed stress test. Post-delivery, the chances are that they will go back to having normal blood pressure and they will lose the weight. But in the long run, this is a warning sign that if they get pregnant again, this will likely happen again, or when they get older, they will be faced with hypertension and diabetes. In fact, pre-eclampsia and gestational diabetes are now recognized risk factors by the American Heart Association.” This emphasizes the importance of monitoring post-delivery with a standard two-week follow-up with an OB-GYN to ensure blood pressure normalizes, but even after the first month or until the hormonal system returns to pre-pregnancy state.
Downloaded from http://ahajournals.org by on July 25, 2025
III Significantly increased maternal mortality or severe morbidity risk. Expert counseling required. In the event of pregnancy, intensive specialist cardiac and obstetric monitoring needed throughout pregnancy, childbirth, and the puerperium.
IV Extremely high maternal mortality or severe morbidity risk. Pregnancy is contraindicated. In the event of pregnancy, termination should be discussed. If pregnancy continues, care should follow class III recommendations.
Maternal Risk Factors
Uncomplicated small/mild pulmonary stenosis, PDA, mitral valve prolapse
Successfully repaired simple lesions (ASD, VSD, PDA, anomalous pulmonary venous drainage)
Atrial or ventricular ectopic beats, isolated
If otherwise well and uncomplicated:
Unoperated ASD, VSD
Repaired TOF
Most arrhythmias
Mild LV impairment
Hypertrophic cardiomyopathy
Native or tissue valvular disease (not considered risk category I or IV)
Marfan syndrome without aortic dilation
Aortic dilation <45 mm in bicuspid aortic valve aortopathy
Repaired coarctation
Mechanical valve
Systemic RV
Fontan circulation
Cyanotic heart disease (unrepaired)
Other complex CHD
Aortic dilation 40–45 mm in Marfan syndrome
Aortic dilation 45–50 mm in bicuspid aortic valve aortopathy
Pulmonary arterial hypertension (of any cause)
Severe systemic ventricular dysfunction (LV ejection fraction <30%, NYHA class III-IV)
Previous peripartum cardiomyopathy with any residual impairment of LV function
Severe mitral stenosis, severe symptomatic aortic stenosis
Aortic dilation >45 mm in Marfan syndrome
Aortic dilation >50 mm in bicuspid aortic valve aortopathy
Native severe coarctation
AS indicates aortic stenosis; ASD, atrial septal defect; CHD, congenital heart disease; LV, left ventricular; NYHA, New York Heart Association; PDA, patent ductus arteriosus; RV, right ventricle; TOF, tetralogy of Fallot; VSD, ventricular septal defect; and WHO, World Health Organization. Modified from Thorne et al2 with permission from the BMJ Publishing Group Ltd. Copyright © 2006, BMJ Publishing Group Ltd and the British Cardiovascular Society. Modified from Balci et al3 with permission from the BMJ Publishing Group Ltd. Copyright © 2014, BMJ Publishing Group Ltd and the British Cardiovascular Society.
References:
A primary fall in systemic vascular resistance (SVR), which reduces preload and afterload, may trigger many of the changes in the hemodynamics and volume homeostasis that accompany early pregnancy. Within 8 weeks after the last menstrual period, SVR has fallen by ≈30%, reaching a nadir at ≈24 weeks’ gestation (Figure 2).23,25,27,43,46–50 After 24 weeks’ gestation, SVR begins to increase again, approaching preconception levels by term.
It is very rare to find national or international studies for pregnant women — this area of medicine is highly regulated as the research involves both the mother and baby. However, a nationwide NIH-funded trial — REBRTH (Randomized Evaluation of Bromocriptine in Myocardial Recovery Therapy) — is exploring whether bromocriptine can help women with peripartum cardiomyopathy recover heart function and improve survival.
tion (measured in the lateral recumbent position), which is followed by a rise toward nonpregnant measurements (Figure 2).27,51
1. Canobbio, M.M., Warnes, C.A, Aboulhosn, J., et al. Management of Pregnancy in Patients with Complex Congenital Heart Disease: A Scientific Statement for Healthcare Professionals from the American Heart Association. Circulation. 2017;135(8):e50–e87. doi:10.1161/CIR.0000000000000458
The fall in SVR is associated with 10 to 15 mm Hg reduction in diastolic pressure at 20 to 24 weeks’ gesta-
Respiratory Changes
Tidal volume increases 40% with a proportional rise in minute ventilation.52–54 This physiological hyperventilation is greater than the increase in oxygen consumption and accounts for the breathlessness that begins in early pregnancy.55–58
February 21, 2017 Circulation. 2017;135:e50-e87. DOI: 10.1161/CIR.0000000000000458
Dr. Agoston feels it is critical to tackle the most common complications of high-risk pregnancies by closely following patients with high blood pressure that can lead to stroke, and gestational diabetes that can lead to real diabetes. “The other complication I see is that before a woman has fully recovered, she might become pregnant again — and what’s going to happen in the next pregnancy. In my opinion, it’s important to look at the life span — what happens beyond the one pregnancy and if there are multiple pregnancies.”
2. Mehta, L.S., Velarde, G.P., Lewey, J., et al. Cardiovascular Disease Risk Factors in Women: The Impact of Race and Ethnicity: A Scientific Statement from the American Heart Association. Circulation. 2023;147(19):e404–e426. doi:10.1161/ CIR.0000000000001139
3. Mehta, L.S., Warnes, C.A., Bradley, E., et al. Cardiovascular Considerations in Caring for Pregnant Patients: A Scientific Statement from the American Heart Association. Circulation. 2020;141(23):e884–e903. doi:10.1161/
CIR.0000000000000772


By Angelo Amato Jr., OMS-III; Ravi Patel, OMS-III; and Ramaswamy Sharma, MS, PhD
Coronary artery disease (CAD) is characterized by the buildup of calcified cholesterol plaques within the coronary arteries, which supply blood to the heart, termed as atherosclerosis, resulting in their blockage. While CAD can be asymptomatic, it can lead to coronary heart disease (CHD), myocardial ischemia and, in severe cases, infarction. CAD remains the leading cause of death globally, with approximately 366,000 Americans dying from CHD every year. Age-adjusted mortality rates for CHD in Bexar County remain elevated compared to national averages; the San Antonio Metropolitan Health District ranks cardiovascular disease consistently among the top causes of mortality in the region, with CAD contributing significantly to this burden.
The etiology of CAD is multifactorial, and risk factors are generally classified as either non-modifiable or modifiable. Non-modifiable factors include age, sex, genetic predisposition and family history, whereas modifiable risk factors include hypertension, tobacco use, obesity, dyslipidemia and/or hypercholesterolemia with elevated levels of low-density lipoprotein (LDL) cholesterol, diabetes and psychosocial influences. Bexar County’s high prevalence of traditional risk factors — hypertension, diabetes, obesity and hyperlipidemia — continues to fuel CAD incidence.
The management of coronary artery disease can be categorized into four primary domains, each targeting a specific aspect of care: pharmacotherapy for symptom control and risk reduction, interventional cardiology that includes procedures for revascularization, lifestyle modifications, and cardiac rehabilitation for holistic recovery.
Pharmacotherapy remains a foundational component in the management of CAD, with recent innovations offering improved clinical outcomes. Newer anti-anginal medications such as ranolazine, through their inhibition of late sodium currents, are effective in alleviating exertional chest pain and improving exercise tolerance, complementing traditional therapies. One of the most significant updates in CAD management came from the 2024 European Society of Cardiology guidelines, which revised recommendations for dual antiplatelet therapy (DAPT) following percutaneous coronary intervention (PCI). DAPT, which combines aspirin with P2Y12 inhibitors such as clopidogrel, prasugrel or ticagrelor, has become a cornerstone of care. Evidence from recent clinical trials show that shorter DAPT can maintain protection against stent thrombosis while reducing bleed-
ing-related complications. The guidelines, therefore, advocate for a shortened DAPT duration of six months in elective PCI cases, followed by monotherapy with either aspirin or clopidogrel, depending on individual ischemic and bleeding risk profiles. Based on DAPT score and clinical judgment, the duration can be further shortened to one to three months in patients with high bleeding risk or extended in those with high ischemic risk. While aspirin after short DAPT has been the default treatment, the recent PANTHER meta-analysis of 23 randomized trials suggests better outcomes from P2Y12 inhibitor monotherapy over aspirin alone for secondary prevention of coronary events, although this has to be validated. Similarly, in patients with atrial fibrillation and chronic stable CAD, the EPIC-CAD trial from South Korea introduced a paradigm shift by evaluating edoxaban monotherapy versus combination therapy with antiplatelet agents. The trial found that edoxaban alone reduced adverse clinical events, primarily by lowering bleeding risk, without compromising efficacy. This finding has implications for patients with complex comorbidities, where balancing thrombotic and hemorrhagic risks is critical. Thus, the shift in guidelines reflects a growing emphasis on personalized medicine and risk stratification.
Secondary prevention aims to halt disease progression, prevent recurrence, and reduce mortality through comprehensive risk factor control and sustained patient engagement. The 2025 Lancet Commission called for redefining CAD as atherosclerotic coronary artery disease (ACAD), emphasizing early detection and prevention over late-stage ischemia management. This reframing could potentially prevent up to 8.7 million deaths globally each year, underscoring the importance of proactive care. Updated clinical guidelines now emphasize tighter targets for blood pressure, glycemic control and LDL cholesterol. New guidelines in 2025 include early initiation of high-intensity statin therapy for acute presentations of CAD (such as acute coronary syndrome, ACS) to stabilize atherosclerotic coronary artery plaques or for long-term management, in conjunction with non-statin lipid-lowering therapies such as ezetimibe or PCSK9 inhibitors such as alirocumab and evolocumab. Recent findings also highlight the benefits of combining coronary calcium scoring with moderate-intensity statin therapy in patients with familial CAD to reduce plaque progression and improve long-term outcomes. Additionally, the SELECT trial introduced semaglutide, a GLP-1 receptor
agonist, as a promising agent for reducing major adverse cardiovascular events in high risk, non-diabetic overweight or obese patients. The trial demonstrated a 20% reduction in cardiovascular events. These insights reflect a broader trend toward precision medicine, wherein individualized risk assessment guides therapeutic decisions. Similarly, SGLT2 inhibitors, such as empagliflozin, initiated soon after acute MI, reduces heart failure risk and preserves kidney function, as shown by the EMPACT-MI trial.
In patients who do require revascularization for definitive treatment of chronic CAD, coronary artery bypass grafting (CABG) is preferred in most patient populations; PCI is preferred in poor surgical candidates and patients presenting with ACS secondary to a ST-elevation myocardial infarction (STEMI) to mitigate complications. The 2025 American College of Cardiology (ACC), American Heart Association (AHA) and American College of Emergency Physicians (ACEP) guidelines suggest that the radial approach is preferred compared to the femoral approach, given the proven lower bleeding risk.
The DanGer Shock trial, a multicenter randomized study, demonstrated that mechanical circulatory support using a microaxial flow pump (Impella CP) significantly reduced 180-day mortality in patients with STEMI that was complicated by cardiogenic shock. This trial filled a longstanding gap in evidence and is expected to reshape treatment protocols for acute MI with shock. Another notable advancement is the FDA approval of Boston Scientific’s AgentTM Drug-Coated Balloon (DCB) for treating coronary in-stent restenosis. The AGENT IDE trial showed that DCBs led to significantly lower target lesion failure at 12 months compared to conventional balloon angioplasty. While DCBs have not yet replaced drug-eluting stents for broader indications, they offer a valuable option for patients with small-vessel disease or restenosis, where stent placement may be suboptimal; trials are ongoing. The Transitional Pass-Through (TPT) payment covering outpatient use, effective from January 2025, and the New Technology Add-On Payment (NTAP), effective from October 2025, covering inpatient use, will reduce the financial barrier for these treatments by helping hospitals adopt the technology quickly without financial loss during its market-entry phase.
Lifestyle modification and cardiac rehabilitation are also integral components of CAD management. Regular aerobic exercise, ideally 150 minutes per week, improves endothelial function, insulin sensitivity and lipid profiles while promoting weight loss and psychological well-being. Evidence-based guidelines recommend a Mediterranean-style diet rich in fruits, vegetables, whole grains, fiber, lean protein and healthy fats, which have been associated with lower cardiovascular mortality. Smoking cessation remains perhaps the single most impactful behavioral intervention. The use of nicotine replacement therapy, pharmacologic aids such as varenicline, and behavioral counseling doubles or triples the odds of quitting successfully. In addition, the importance of stress reduction, adequate sleep and mental health support has gained recognition, with growing evidence linking depression and anxiety to poorer cardiac outcomes.
CAD continues to pose a significant public health challenge in Bexar County, with prevalence driven by entrenched risk factors and socioeconomic disparities. Efforts to mitigate CAD prevalence in Bexar County have included community-based interventions targeting lifestyle modification, improved access to primary care and public health campaigns focused on smoking cessation and dietary education.
However, the persistent rates of CAD suggest that more targeted and innovative approaches are needed, especially in underserved neighborhoods.
References:
1. Calabrò, P. et al. Lipid-Lowering Therapy in Patients With Coronary Artery Disease Undergoing Percutaneous Coronary Interventions in Italy: An Expert Opinion Paper of Interventional Cardiology Working Group of Italian Society of Cardiology. Journal of Cardiovascular Medicine 24, e86-e94 (2023)
2. Cho, M.S. et al. Edoxaban Antithrombotic Therapy for Atrial Fibrillation and Stable Coronary Artery Disease. New England Journal of Medicine 391, 2075-2086 (2024)
3. Giacoppo, D. et al. P2Y12 Inhibitor or Aspirin After Percutaneous Coronary Intervention: Individual Patient Data Meta-Analysis of Randomised Clinical Trials. BMJ 389, e082561 (2025)
4. He, G. et al. SGLT2 Inhibitors for Prevention of Primary and Secondary Cardiovascular Outcomes: A Meta-Analysis of Randomized Controlled Trials. Heart & Lung 59, 109-116 (2023)
5. Kundu, A. & Moliterno, D.J. Drug-Coated Balloons for In-Stent Restenosis—Finally Leaving Nothing Behind for US Patients. JAMA 331, 1011-1012 (2024)
6. Lüsebrink, E., Binzenhöfer, L. & Thiele, H. The DanGer Shock Trial: A New Dawn But Much to Uncover. European Heart Journal 45, 4181-4183 (2024)
7. Marx, N., Husain, M., Lehrke, M., Verma, S. & Sattar, N. GLP-1 Receptor Agonists for the Reduction of Atherosclerotic Cardiovascular Risk in Patients With Type 2 Diabetes. Circulation 146, 18821894 (2022)
8. Nerlekar, N. et al. Effects of Combining Coronary Calcium Score With Treatment on Plaque Progression in Familial Coronary Artery Disease: A Randomized Clinical Trial. JAMA 333, 1403-1412 (2025)
9. Rao, S.V. et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 151, e771-e862 (2025)
10. Sanyal, A.J. et al. Phase 3 Trial of Semaglutide in Metabolic Dysfunction–Associated Steatohepatitis. New England Journal of Medicine 392, 2089-2099 (2025)
11. Zaman, S. et al. The Lancet Commission on Rethinking Coronary Artery Disease: Moving From Ischaemia to Atheroma. The Lancet 405, 1264-1312 (2025)



Angelo Amato Jr., OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2027. His current interests include Emergency Medicine, Cardiology and lifestyle approaches to reduce the instance of cardiovascular diseases.
Ravi Patel, OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2027. He is interested in Emergency Medicine and in the application of artificial intelligence in improving multiple clinical aspects of medicine.
Ramaswamy Sharma, MS, PhD, is a Professor of Pathology at the University of the Incarnate Word School of Osteopathic Medicine. He is interested in delineating the multiple molecular and cellular roles of melatonin in maintaining our quality of life. Dr. Sharma is a member of the BCMS Publications Committee.
By Esther Shin, OMS-III, and Gabriel Bietz, MD
Chronic limb-threatening ischemia (CLTI), formerly referred to as critical limb ischemia, is the most clinically advanced stage of peripheral arterial disease (PAD). Found in 12% of the U.S. adult population, CLTI is a chronic condition that has grown significantly in health and economic burden.1
Among the subcategories of PAD, Rutherford Grade 3, Category 6 describes the most severe cases. Patients in this category have extensive tissue loss and are at high risk for limb loss, systemic complications and mortality. Endovascular revascularization techniques are the foundation of CLTI management, with timely revascularization being critical to limb salvage. This article reviews current endovascular strategies for management of CLTI.
Chronic limb-threatening ischemia is defined by ischemic foot pain at rest, ulcerations or gangrene. 2 Rutherford Category 6 patients specifically demonstrate major tissue loss, tissue loss that extends proximally above transmetatarsal level, and/or the functional foot being unsalvageable.1 Wounds are frequently accompanied by wet or dry gangrene, soft tissue infection, osteomyelitis or sepsis. Patients usually have systemic comorbidities such as diabetes mellitus, chronic kidney disease and coronary artery disease that further contribute to poor perfusion as well as impaired or absent healing capabilities.3 Furthermore, many patients present late in the disease course, further complicating revascularization efforts.
The American College of Cardiology, American Heart Association and Society for Vascular Surgery guidelines recommend a multidisciplinary approach to CLTI that prioritizes pre-amputation evaluation.3,4 Treatment includes medical therapy for reduction of cardiovascular risk, revascularization and local care for wound healing and infection control.2 A comprehensive diagnostic evaluation is therefore critical to examine the extent of ischemia, infection and tis-

sue loss. Initial vascular imaging involves non-invasive methods such as duplex ultrasonography. Computed tomography angiography provides further anatomical detail but is contraindicated with patients with advanced renal disease, to which magnetic resonance angiography serves as an alternative. The gold standard is digital subtraction angiography, which is often used intraoperatively for visualization of arterial patency and fluid dynamics.2,3
The foundational management method for CLTI has been endovascular revascularization due to lower procedural risk and a minimally invasive nature.2,5 The American College of Cardiology and American Heart Association guidelines endorse endovascular treatments for effective limb salvage.
The goal of revascularization is restoration of direct, in-line arterial flow to at least one patent vessel supplying the wound bed. Decision-making is influenced by patient comorbidities, anatomy of occlusion and availability of treatment methods. The standard access vessel for endovascular intervention is the common femoral artery, but alternatively pedal or tibial artery utilization have been used.6
Percutaneous Transluminal Angioplasty (PTA): Among the endovascular techniques, PTA remains the foundational modality, particularly for below-the-knee (BTK) disease. Often the initial approach, this technique is also known for high restenosis rates, most likely due to the complex nature of lesions typically seen in Rutherford 6 patients. Such lesions can be long-segmented or calcified.4 This necessitates close follow-up and even repeated interventions in some cases.
Drug-Coated Balloons (DCB): Drug-coated balloons are coated with antiproliferative agents (commonly paclitaxel) that are released during balloon inflation to inhibit neointimal hyperplasia and thereby restenosis. Recent meta-analyses indicate that DCBs combined with atherectomy have greater 6- and 12- month patency and limb salvage compared to the use of PTA alone in BTK disease.7
Stenting: Bare metal stents (BMS) and drug-eluting stents (DES) immediately scaffold vessels after angioplasty. They are typically reserved for suboptimal angioplasty results such as vessel recoil or residual stenosis. Bare-metal stents, usually self-expanding nitinol stents, reduce the need for repeat interventions and prevent elastic recoil in short to moderate length lesions in femoropopliteal segments. However, they are prone to in-stent restenosis from neointimal hyperplasia.8 In such cases, drug-eluting stents are beneficial.
Atherectomy: Atherectomies are a minimally invasive procedure that debulk plaque buildup in arterial vessels. They are often combined with DCBs, improving lumen gain and facilitating drug delivery. This combination of technique treatments has been proven to offer the highest primary patency rates despite increased risk of embolization.7
Transcatheter Arterialization of Deep Veins: This salvage technique diverts arterial blood into the venous system to perfuse the foot, used for patients without suitable arterial targets for revascularization.9
Bioresorbable Vascular Scaffolds (BVS): Bioresorbable Vascular Scaffolds is an emerging technique that provides temporary scaffolding. Early studies suggest that they improve health outcomes compared to PTA.7
Intravascular Lithotripsy (IVL): Intravascular lithotripsy uses sonic pressure waves to fracture intimal and medial calcium. This method can be used for highly calcified lesions that are resistant to conventional techniques.10
Adjunctive Pharmacologic Therapy: Periprocedural anticoagulation, usually heparin, combined with post-procedure antiplatelet therapy is standard and essential for maintaining patency.
Open surgical bypass: For patients with prior failed endovascular attempts or long-segment disease, open surgical bypass is a suitable treatment method. Autogenous circuits, usually the great saphenous vein, provide superior long-term patency.11
Despite these measures, the prognosis of patients with Rutherford Category 6 CLTI is poor. Recent studies show that CLTI is associated with 25% limb loss and 25% mortality at 1-year.12 Poor outcome predictors include advanced age, comorbidities, smoking history, poor runoff vessels, reduced functionality and persistent pain at rest.13
The LIBERTY 360 study investigated the outcomes of endovascular treatment of symptomatic PAD and reported that the 36-month freedom from major amputation rate was 79.9% in patients with Rutherford 6 disease. At 36 months, the survival rate was 62.0% with improved quality of life from baseline. Patency varies by lesion complexity, comorbidities, calcification extent and adequacy of runoff. 13 The high rates of restenosis and reintervention needs highlight the need for close follow-up observation and monitoring.
Rutherford Grade 3, Category 6 chronic limb-threatening ischemia requires comprehensive management and strategy. Prompt vascular intervention, effective infection control, wound care, tight glucose control and long-term risk management are key components for attempted limb salvage. Early intervention, effective infection control, wound care and long-term risk management are also critical. Tailoring a multidisciplinary approach to individual patients is essential for optimizing successful outcomes due to the complexity and potential for significant burden seen in CLTI patients.
References:
1. Davies, M.G. (2012). Critical Limb Ischemia: Epidemiology. Methodist DeBakey Cardiovascular Journal, 8(4), 10–14. https://doi.org/10.14797/mdcj-8-4-10
2. Farber, A., Menard, M.T., Conte, M.S., Kaufman, J.A., Powell, R.J., Choudhry, N.K., Hamza, T.H., Assmann, S.F., Creager, M.A., Cziraky, M.J., Dake, M.D., Jaff, M.R., Reid, D., Siami, F.S., Sopko, G., White, C.J., van Over, M., Strong, M.B., Villarreal, M.F., & McKean, M. (2022). Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. New England Journal of Medicine, 387(25). https://doi.org/10.1056/nejmoa2207899
3. Gornik, H.L., Aronow, H.D., Goodney, P.P., Arya, S., Brewster, L.P., Byrd, L., Chandra, V., Drachman, D.E., Eaves, J.M., Ehrman, J.K., Evans, J.N., Getchius, T.S.D, Antonio Gutiérrez, J., Hawkins, B.M., Hess, C.N., Ho, K.J., Jones, W.S., Kim, E.S.H, Kinlay, S., & Kirksey, L. (2024). 2024 ACC/AHA/AACVPR/ APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline for the Management of Lower Extremity Peripheral Artery Disease. Journal of the American College of Cardiology, 83(24). https:// doi.org/10.1016/j.jacc.2024.02.013
4. Conte, M.S., Bradbury, A. W., Kolh, P., White, J.V., Dick, F., Fitridge, R., Mills, J.L., Ricco, J.-B., Suresh, K. R., Murad, M.H., Aboyans, V., Aksoy, M., Alexandrescu, V.-A., Armstrong, D., Azuma, N., Belch, J., Bergoeing, M., Bjorck, M., Chakfé, N., & Cheng, S. (2019). Global vascular guidelines on the management of chronic limb-threatening ischemia. Journal of Vascular Surgery, 69(6), 3S125S.e40. https://doi.org/10.1016/j. jvs.2019.02.016
5. Creager, M.A., Matsushita, K., Arya, S., Beckman, J.A., Duval, S., Goodney, P.P., Gutierrez, J.A.T., Kaufman, J. A., Joynt Maddox, K. E., Pollak, A. W., Pradhan, A. D., & Whitsel, L. P. (2021). Reducing Nontraumatic Lower-Extremity Amputations by 20% by 2030: Time to Get to Our Feet: A Policy Statement From the American Heart Association. Circulation, 143(17). https://doi. org/10.1161/cir.0000000000000967
6. Li, J., Varcoe, R., Manzi, M., Kum, S., Iida, O., Schmidt, A., & Shishehbor, M.H. (2024). Below-the-Knee Endovascular Revascularization. КАРДИОЛОГИЯ УЗБЕКИСТАНА, 17(5), 589–607. https://doi.org/10.1016/j.jcin.2023.11.040
7. Tirziu, D., Saleh, A., Huang, H., Akhlaghi, N., Breen, T.J., Parikh, S.., Rosenfield, K., Armstrong, E.J., Geraghty, P. J., Brodmann, M., Adams, G. L., Snyder, D., Zilinyi, R. S., Altin, S. E., Parise, H., & Lansky, A. J. (2025). Safety and Efficacy of Endovascular Treatment Modalities for Below-the-Knee Arterial Disease: A Systematic Review and Network Meta-analysis. Journal of Endovascular Therapy: An Official Journal of the International Society of Endovascular Specialists, 15266028251344809. https://doi.org/10.1177/15266028251344809
8. Schillinger, M., Sabeti, S., Loewe, C., Dick, P., Amighi, J., Mlekusch, W., Schlager, O., Cejna, M., Lammer, J., & Minar, E. (2006). Balloon Angioplasty versus Implantation of Nitinol Stents in the Superficial Femoral Artery. New England Journal of Medicine, 354(18), 1879–1888. https://doi.org/10.1056/nejmoa051303
9. Shishehbor, M.H., Powell, R.J., Montero-Baker, M.F., Dua, A., Martínez-Trabal, J.L., Bunte, M.C., Lee, A. C., Mugglin, A.S., Mills, J.L., Farber, A., & Clair, D.G. (2023). Transcatheter Arterialization of Deep Veins in Chronic Limb-Threatening Ischemia. New England Journal of Medicine, 388(13), 1171–1180. https://doi.org/10.1056/nejmoa2212754
10. Brodmann, M., Werner, M., Brinton, T.J., Illindala, U., Lansky, A., Jaff, M.R., & Holden, A. (2017). Safety and Performance of Lithoplasty for Treatment of Calcified Peripheral Artery Lesions. Journal of the American College of Cardiology, 70(7), 908–910. https://doi.org/10.1016/j.jacc.2017.06.022
11. Golovina, V., Panfilov, V., Seliverstov, E., Erechkanova, D., & Zolotukhin, I. (2024). Availability of the Great Saphenous Veins as Conduits for Arterial Bypass Surgery in Patients with Varicose Veins. Journal of Clinical Medicine, 13(24), 7747. https://doi. org/10.3390/jcm13247747
12. Joshi, G.S., Zhang, S.M., Wang, K., El Khoury, R., Cataneo, J., Jacobs, C.E., White, J.V., & Schwartz, L.B. (2022). Predictors of Amputation-free Survival after Endovascular Intervention for Chronic Limb-Threatening Ischemia in the Modern era. Annals of vascular surgery, 86, 268–276. https://doi.org/10.1016/j. avsg.2022.04.052
13. Mustapha, J.A., Katzen, B.T., Neville, R.F., Lookstein, R.A., Zeller, T., Miller, L.E., Nelson, T.R., & Jaff, M.R. (2019). Propensity Score-Adjusted Comparison of Long-Term Outcomes Among Revascularization Strategies for Critical Limb Ischemia. Circulation. Cardiovascular interventions, 12(9), e008097. https://doi.org/10.1161/CIRCINTERVENTIONS.119.008097


Esther Shin, OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, with an interest in public health.
Gabriel Bietz, MD, is a board-certified vascular surgeon and Chairman of the Board for San Antonio Surgical Center of Excellence. He is a partner at Texas Cardiac and Vascular Institute, serving patients across San Antonio, Seguin and Corpus Christi. He is recognized for his expertise in both open and endovascular procedures, along with his leadership in advancing patientcentered vascular care. In addition to his medical career, Dr. Bietz is a serial entrepreneur with ventures spanning healthcare and private investments, and is a member of the Bexar County Medical Society.
45.2% 28%
of physicians surveyed report feeling the effects of burnout daily1
2 out of 3 physicians who are experiencing depression say it affects their work2 of residents surveyed report experiencing a major depressive episode during training3
• Workload
• Work inefficiency
• Lack of autonomy and meaning in work
• Work-home conflict
Medical students have rates of depression 15-30% higher than the general population4
300 to 400 physicians die by suicide each year4
Talk
• Killing themselves
• Having no reason to live
• Being a burden to others
• Feeling hopeless
• Feeling trapped
• Unbearable pain
Behavior
• Increased use of alcohol or drugs
• Withdrawing from activities
• Isolating from family and friends
• Sleeping too much or too little
The suicide rate among male physicians is 1.41x higher than the general male population4
The suicide rate among female physicians is 2.27x higher than the general female population4
1. “Measuring and addressing physician burnout,” May 15, 2025, https://www.ama-assn.org/practicemanagement/physician-health/measuring-and-addressing-physician-burnout.
2. Leslie Kane, MA, “Medscape National Physician Burnout, Depression & Suicide Report 2019,” Medscape, January 16, 2019.
3. Mata, DA, et al. (2015). Prevalence of Depression and Depressive Symptoms among Resident Physicians. JAMA, 314(22), 2373.
4. “10 Facts About Physician Suicide and Mental Health,” American Foundation for Suicide Prevention.
Mood
• Depression
• Anxiety
• Loss or interest
• Irritability
• Humiliation/shame
• Anger/agitation
Prioritizing mental health enables physicians to provide better patient care and maintain resilience by combining self-care with effective mental health treatment. Learn more at afsp.org/physicians
If you or someone you know needs support now, call or text 988 or chat 988lifeline.org

By Angelo Amato Jr., OMS-III, and Ramaswamy Sharma, MS, PhD
The aortic valve, one of four heart valves, acts as a one-way gate for blood flow to the entire body, opening an astonishing 100,000 times a day. Not surprisingly, lesions of the aortic valve, classified as valvular heart disease (VHD), can have serious repercussions such as severe aortic stenosis, with an opening less than or equal to 1 cm, or aortic regurgitation leading to significant left ventricle dysfunction. The cause of these lesions may vary widely, and may be associated with congenital bicuspid aortic valves, inflammation in patients with atherosclerosis or age-related calcification. VHD is significantly associated with aging, affecting one of every 10 individuals aged 70 and above. In the United States, aortic stenosis affects 1-2% of individuals older than 65, and 12% of individuals aged above 75 years, with a 5-year mortality risk of 94% if symptomatic and left untreated.
Dr. Charles Hufnagel, credit: https://collections. nlm.nih.gov/catalog/nlm:nlmuid-101419151-img
Dr. Charles Hufnagel is credited with the invention of the first artificial “caged ball” heart valve — a simple, plastic ball within a small, 1-inch chamber — and its implantation in the descending thoracic aorta in 1952, revolutionizing the treatment of VHD. The 30-year-old female patient with severe aortic regurgitation who received the valve survived for almost a decade; her death was unrelated to any valve-related disorder. Several modifications of the original valve have been used over the years, such as the use of an ultra-high molecular weight polyethylene disc within a Haynes-25 housing surrounded by a polyethylene terephthalate fabric sewing ring, which has been implanted in more than 100,000 patients. Mechanical valves are also made from pyrolytic carbon or titanium, ensuring a long-lasting valve. However, they can lead to the formation of blood clots. Therefore, bioprosthetic tissue valves, consisting of either bovine or porcine heterograft valves, or homograft valves from deceased human donors can be alternatives.
A Ross procedure involving a pulmonary autograft inclusion technique is also an option, based on the patient’s age and unique anatomy. A recently concluded 22-year study published in January 2025 reported greater than 90% survivability of patients post-Ross procedure over a period of twenty years, with resolution of aortic regurgitation in 84.5% of patients in the same timeframe. This procedure is well-suited for young patients given that it includes living tissue, grows with the patient, and precludes the need for life-long use of anti-coagulation drugs associated with mechanical valves. However, tissue valves last for approximately 15-20 years and may need to be replaced in younger patients. Therefore, the search for better valves with optimal shapes continues. Newer mechanical valves not resulting in blood clots or requiring the need for sutures are currently undergoing clinical trials.
In 2002, Dr. Alain Cribier performed the first minimally invasive transcatheter aortic valve implantation (TAVI; also known as transcatheter aortic valve replacement (TAVR) in the United States). This procedure allows older patients previously not considered for surgical aortic valve replacement (SAVR) to be able to receive a new valve via a less invasive transfemoral or transapical approach. TAVR patients may be discharged from the hospital either after an overnight stay or the same day after the procedure, as compared to four to seven days after SAVR. TAVR has, therefore, changed the accessibility and impact of aortic valve replacements; the complication rate for elective aortic valve replacement of all types decreased by 27% from 2012 to 2019, demon-
“Caged Ball” Heart Valve by Dr. Charles Hufnager, credit: https://americanhistory.si.edu/collections/object/nmah_1196369
strating not only the increasing success of this operation but also its larger applicability to the general population. A metanalysis based on five randomized controlled trials with a total of 3,072 patients found that TAVR in low-risk older patients with an average age of 74.5 years was associated with a lower rate of mortality and morbidity as compared to SAVR, decreased bleeding and post-operative onset of atrial fibrillation, as well as improved quality of life. However, TAVR did have increased incidence of paravalvular leaks and higher rates of pacemaker implantation. Currently, more than a million TAVR procedures are performed globally, and this is set to expand further; this will increase the number of interventions that need to be repeated over time. In March 2025, the Heart Valve Collaboratory suggested the best practices for multimodal imaging for diagnosing transcatheter failures.
In 2005, Dr. Joseph McGinn, Jr. performed the first minimally invasive heart cardiac surgery (MICS) based on a mini-sternotomy, which consists of three small incisions — one at the 4th (or 5th) intercostal space and two at the 6th intercostal space as compared to the traditional median sternotomy or a mini-thoracotomy in which either the 2nd or 3rd right intercostal space is dissected and used as access to the aorta. This procedure results in decreased blood loss and hence less need for blood transfusions, decreased pain

Dr. Alain Cribier, credit: www.leprogres.fr
and discomfort post-surgery, faster recovery and fewer complications such as sternal non-union seen with SAVR.
Last year, on October 31, 2024, Dr. Vinay Badhwar performed the first robotic aortic valve replacement along with coronary artery bypass grafting (CABG) through a single small incision on a 73-year-old patient.
Conclusion

Dr. Vinay Badhwar, credit: https:// www.heart-valve-surgery.com
Patients, after consulting with their cardiologist and cardiac surgeon, may now have the option to select between SAVR, TAVR or MICS as well as between mechanical or bioprosthetic valves or the Ross procedure, based on their pre-existing conditions and clinical risk profile, age, morphology of their aortic valve and anticipated risks from the procedure.
Undoubtedly, we have come a long way — from the first description of the aortic valve, possibly by Galen who worked on monkeys (129 CE-216 CE), to its accurate drawing in 1512 by Leonardo da Vinci, to the first surgery for aortic stenosis by Théodore Tuffier in 1913, to the implantation of the first prosthetic valve by Dwight Harken in 1960 for aortic regurgitation, and now with TAVR as well as minimally invasive cardiac surgery.
References:
1. Badhwar, V., Raikar, G.V., Darehzereshki, A., Mehaffey, J.H., Daggubati, R., & Wei, L.M. (2024). Robotic-Assisted aortic valve replacement and coronary artery bypass grafting. The Annals of Thoracic Surgery. https://doi.org/10.1016/j.athoracsur.2024.12.002
2. Beerkens, F.J., Tang, G.H. L., Kini, A.S., Lerakis, S., Dangas, G.D., Mehran, R., Khera, S., Goldman, M., Fuster, V., Bhatt, D.L., Webb, J.G., & Sharma, S.K. (2025). Transcatheter aortic valve replacement beyond severe aortic stenosis. Journal of the American College of Cardiology, 85(9), 944–964. doi:10.1016/j.jacc.2024.11.051
3. Coffey, S., Roberts-Thomson, R., Brown, A., Carapetis, J., Chen, M., Enriquez-Sarano, M., Zühlke, L., & Prendergast, B.D. (2021). Global epidemiology of valvular heart disease. Nature Reviews Cardiology, 18(12), 853–864. doi:10.1038/s41569-021-00570-z
4. DeMajistre, A. (2024, September 19). Doctor Q&A: The future of transcatheter aortic valve replacement (TAVR)? Adam’s Heart Valve Surgery Blog. https://www.heart-valve-surgery.com/heart-surgeryblog/2024/09/18/tavr-future/
5. Gott, V.L., Alejo, D.E., & Cameron, D.E. (2003). Mechanical heart valves: 50 years of evolution. The Annals of Thoracic Surgery, 76(6), S2230–S2239. doi:10.1016/j.athoracsur.2003.09.002
6. Harvey, J.E., Kapadia, S.R., Cohen, D.J., Gunnarsson, C., Irish, W., Kalra, A., Puri, R., Thompson, C., Chikermane, S.G., & Ryan, M. (2024, August 27). Trends in complications among patients undergoing Aortic Valve Replacement in the United States. Journal of the American Heart Association. https://www.ahajournals.org/ doi/10.1161/JAHA.123.031461
7. Indolfi, C., Esposito, G., & Lüscher, T.F. (2025). TAVI or TAVR: it is time to use a single standardized acronym for percutaneous aortic
valve implantation. OUP Academic. https://doi.org/10.1093/ eurheartj/ehaf048
8. Kapadia, S.R., Leon, M.B., Makkar, R.R., Tuzcu, E.M., Svensson, L.G., Kodali, S., Webb, J.G., Mack, M.J., Douglas, P.S., Thourani, V.H., Babaliaros, V.C., Herrmann, H.C., Szeto, W.Y., Pichard, A.D., Williams, M.R., Fontana, G.P., Miller, D.C., Anderson, W.N., Aikin, J.J., Davidson, M.J., Smith, C.R.; PARTNER trial investigators (2015). 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomized controlled trial. The Lancet, 385(9986), 2485–2491. doi:10.1016/s0140-6736(15)60290-2
9. Khalique, O., Zaid, S., Tang, G., et al. Best Practices for Imaging of Transcatheter Valve Failure: An Update From the Heart Valve Collaboratory. JACC. 2025 Mar, 85 (10) 1042–1055. doi:10.1016/j. jacc.2024.12.017
10. Kheiri, B., Osman, M., Bakhit, A., Radaideh, Q., Barbarawi, M., Zayed, Y., Golwala, H., Zahr, F., Stone, G.W., & Bhatt, D.L. (2019). Meta-Analysis of transcatheter aortic valve replacement in LowRisk Patients. The American Journal of Medicine, 133(2), e38–e41. https://doi.org/10.1016/j.amjmed.2019.06.020
11. Kuijpers, P.M.J.C. (2020). History in medicine: the aortic valve. E-Journal of Cardio. Prac., 18(9). https://doi.org/10.37461/escejcp.18.9
12. Nettersheim, F.S., & Baldus, S. (2025). Precision medicine in the management of valvular heart disease. In Herz (Vol. 1, pp. 1–3); doi: 10.1007/s00059-025-05299-w.
13. Nkomo, V.T., Gardin, J.M., Skelton, T.N., Gottdiener, J.S., Scott, C.G., & Enriquez-Sarano, M. (2006). Burden of valvular heart diseases: a population-based study. The Lancet, 368(9540), 1005–1011. doi:10.1016/s0140-6736(06)69208-8
14. Osnabrugge, R.L., Mylotte, D., Head, S.J., Van Mieghem, N.M., Nkomo, V.T., LeReun, C.M., Bogers, A.J., Piazza, N., & Kappetein, A.P. (2013). Aortic stenosis in the elderly. Journal of the American College of Cardiology, 62(11), 1002–1012. doi: 10.1016/j. jacc.2013.05.015
15. The Society of Thoracic Surgeons. Patients who received Ross procedure demonstrate excellent survival rates after 20 years. (2025, January 26). https://www.sts.org/press-releases/patients-who-received-ross-procedure-demonstrate-excellent-survival-rates-after-20years
16. Valiathan, M. V. S. (2018). Frugal innovation in cardiac surgery. Indian Journal of Thoracic and Cardiovascular Surgery, 34(3), 439–448. doi:10.1007/s12055-018-0652-0
Angelo Amato Jr., OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2027. His current interests include Emergency Medicine, Cardiology and lifestyle approaches to reduce the instance of cardiovascular diseases.
Ramaswamy Sharma, MS, PhD, is a Professor of Pathology at the University of the Incarnate Word School of Osteopathic Medicine. He is interested in delineating the multiple molecular and cellular roles of melatonin in maintaining our quality of life.
Dr. Sharma is a member of the BCMS Publications Committee.


By Esther Shin, OMS-III, Arya Bietz, and Gabriel Bietz, MD
Peripheral artery disease (PAD) is increasing in frequency worldwide, causing significant limb morbidity and mortality. In advanced stages, revascularization is critical to preserving limbs and their functionality. The most appropriate treatments require nuanced decision-making when considering conservative care, endovascular intervention or open surgical management. Although guidelines do exist, major differences in patient complexity and evolving therapeutic options lead to variability in treatment selection and outcomes. Artificial intelligence (AI) has emerged as a potentially powerful tool that can assist clinicians in selecting the optimal revascularization strategy. This article reviews the main roles of AI, current limitations and future potential directions in PAD management.
Artificial intelligence within healthcare involves three categories: natural language processing (NLP), machine learning (ML) and
vision. NLP indicates AI applications towards understanding written/ oral language whereas vision involves applications towards analyzing images or videos. Machine learning is a subcategory within AI that involves algorithms that have the ability to adapt from experience without explicit programming.1
Natural Language Processing techniques can’t extract relevant clinical features from unstructured data sets to improve PAD identification based on medical records. A recent study developed a NLP system to diagnose PAD cases from clinical notes, whose performance was then compared to that of previously developed models that were based on ICD-9 diagnostic codes. The NLP algorithm demonstrated better accuracy with higher positive predictive value and specificity, identifying potential beneficial use in Electronic Health Record system implementation.2
Machine learning models have the capability to analyze structured data points such as age, comorbidities, ABI values and relevant laboratory markers to stratify patients based on expected procedural benefits and risk for each therapeutic option. ML algorithms have also shown promise in improved identification of patients with PAD, evaluation of prognosis and evidence-based treatment methods. 3-6
Convoluted neural networks (CNNs) are a type of machine learning that have demonstrated success in interpreting duplex ultrasound, CT angiography (CTA) and MR angiography (MRA) scans by leveraging its ability to recognize patterns in images.7 These models can detect stenosis, plaque burden and occlusive segments with high sensitivity and specificity.7
Imaging is an essential component of PAD diagnosis and management. AI-assisted image analysis can enhance procedural planning by assessing stenosis, calcification burden and automatic segmentation of vessels. The data from anatomical features with clinical data can help evaluate the feasibility, risk and appropriateness of endovascular versus surgical interventions.3 Some AI systems can even be used to simulate likely outcomes of different interventions — estimating based on structural and lesion morphology, patient individual profile and device selection. This can be particularly useful in more complex cases such as chronic limb-threatening ischemia (CLTI), where choosing between endovascular intervention and surgical bypass is oftentimes debated.
AI can also be used to augment conservative management of PAD. AI models can identify patients for whom conservative treatments, such as diet and lifestyle modifications or pharmacotherapy, are both sufficient and appropriate. Furthermore, sensor data from smartphones or wearables can provide longitudinal activity and physiologic data that can then be analyzed by predictive algorithms to guide conservative treatments or to even detect symptom changes for escalation or de-escalation of current treatment.
Although there are many promising applications of using AI in clinical practice, limitations such as privacy concerns, data dependency or bias are present that should be addressed. Further research is indicated to ensure equitable and effective utilization.
Future directions include a focus on prospective trials that validate AI-assisted decision tools as well as collaboration between clinicians, vascular surgeons, data scientists and regulatory institutions to ensure seamless transitions to routine healthcare.
AI-assisted decision-making has emerged as an increasingly promising tool in the management of PAD, particularly in guiding revascularization strategies with individualized care. Further research is indicated to minimize current limitations and enhance potential positive health outcomes.
References:
1. Nichols, J.A., Herbert Chan, H.W., & Baker, M.A.B. (2019). Machine learning: applications of artificial intelligence to imaging and diagnosis. Biophysical reviews, 11(1), 111–118. https:// doi.org/10.1007/s12551-018-0449-9
2. Afzal, N., Sohn, S., Abram, S., Scott, C. G., Chaudhry, R., Liu, H., Kullo, I.J., & Arruda-Olson, A.M. (2017). Mining peripheral arterial disease cases from narrative clinical notes using natural language processing. Journal of vascular surgery, 65(6), 1753–1761. https://doi.org/10.1016/j.jvs.2016.11.031
3. Lareyre, F., Behrendt, C.-A., Chaudhuri, A., Lee, R., Carrier, M., Adam, C., Lê, C.D., & Raffort, J. (2022). Applications of artificial intelligence for patients with peripheral artery disease. Journal of Vascular Surgery. https://doi.org/10.1016/j.jvs.2022.07.160
4. Liu, Y., Xue, J., & Jiang, J. (2023). Application of machine learning algorithms in electronic medical records to predict amputation-free survival after first revascularization in patients with peripheral artery disease. International journal of cardiology, 383, 175–184. https://doi.org/10.1016/j.ijcard.2023.04.040
5. Berger, J.S., Haskell, L., Ting, W., Lurie, F., Chang, S.C., Mueller, L.A., Elder, K., Rich, K., Crivera, C., Schein, J.R., & Alas, V. (2020). Evaluation of machine learning methodology for the prediction of healthcare resource utilization and healthcare costs in patients with critical limb ischemia-is preventive and personalized approach on the horizon? The EPMA journal, 11(1), 53–64. https://doi.org/10.1007/s13167-019-00196-9
6. Amato, A.C.M., Dos Santos, R.V., Saucedo, D.Z., & Amato, S.J.T.A. (2020). Machine learning in prediction of individual patient readmissions for elective carotid endarterectomy, aortofemoral bypass/aortic aneurysm repair, and femoral-distal arterial bypass. SAGE open medicine, 8, 2050312120909057. https://doi.org/10.1177/2050312120909057
7. Dai, L., Zhou, Q., Zhou, H., Zhang, H., Cheng, P., Ding, M., Xu, X., & Zhang, X. (2021). Deep learning-based classification of lower extremity arterial stenosis in computed tomography angiograp

Esther Shin, OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, with an interest in public health.
Arya Bietz, a junior at Alamo Heights High School, has won numerous journalism contests sponsored by the University Interscholastic League. After high school graduation, she aspires to pursue a degree in construction science with a sub-specialty in healthcare facility development.
Gabriel Bietz, MD, is a board-certified vascular surgeon and Chairman of the Board for San Antonio Surgical Center of Excellence. He is a partner at Texas Cardiac and Vascular Institute, serving patients across San Antonio, Seguin and Corpus Christi. He is recognized for his expertise in both open and endovascular procedures, along with his leadership in advancing patientcentered vascular care. In addition to his medical career, Dr. Bietz is a serial entrepreneur with ventures spanning healthcare and private investments, and is a member of the Bexar County Medical Society.

By Grizelda Anguiano, MD
As the school year begins, the focus often turns to immunizations, forms, sports physicals and managing new schedules. Yet what is often unspoken, and increasingly present in exam rooms and family conversations, is the emotional toll that school re-entry can have on children, particularly those with mental health or neurodevelopmental conditions. For many of these children, school does not feel safe. It can be a minefield of social dynamics, unpredictable transitions and mounting academic expectations.
Neurodivergent learners, including children with ADHD, autism, anxiety or learning differences, are at a significantly higher risk of being bullied. The consequences can be profound, impacting mental health, academic performance and long-term outcomes.
Bullying is not new, but it has evolved. Today’s manifestations often include peer rejection, exclusion from group chats or social media humiliation — forms of harm that are difficult to detect, and even harder to address. According to the CDC’s Youth Risk Behavior Surveillance, nearly 20% of students report being bullied on school property and 15% have experienced cyberbullying.
These statistics are troubling on their own. For neurodivergent children, the risks are amplified. These children may misread social
cues, react impulsively, or express themselves in ways that differ from peer norms. Unfortunately, this can make them easy targets.
The American Academy of Pediatrics (AAP) reports that children with behavioral or emotional disorders are more likely to be both victims and perpetrators of bullying. This bidirectional pattern is critical for providers to understand. When a child presents with sleep difficulty, school refusal or unexplained physical complaints, the cause may be deeper than anxiety or defiance. They may be experiencing relational trauma at school.
Pediatricians are often the first and most trusted resource for families noticing behavioral or emotional shifts. Yet within the constraints of a brief visit, it is easy to miss, or under-address, what is the actual root cause.
Parents may report irritability, stomachaches or withdrawal. Children may disengage entirely. In the urgency to act, medication may be offered before exploring the larger picture.
What’s needed is time and curiosity. The child’s environment, relationships, sleep quality, screen use, executive functioning and social interactions all play a role. Increasingly, I meet children whose academic or attention struggles are rooted in chronic peer rejection or
unprocessed emotional pain. These issues can mimic or even intensify symptoms of ADHD or anxiety.
Children with ADHD or learning differences often live in a double bind. Their strengths, such as creativity, curiosity and unique ways of thinking, are rarely recognized or celebrated in traditional academic settings. Instead, they are often labeled as unmotivated or disruptive. When these strengths are paired with challenges in emotional regulation and executive functioning, it’s easy for both peers and adults to misunderstand their behavior.
Studies show that children with ADHD are two to three times more likely to experience bullying. Many struggle to form lasting friendships or describe their social experiences in detail. When they are mistreated by peers, they may internalize the pain, believing that something is wrong with them. This can lead to a steady decline in self-worth.
As pediatric providers, we can support families by shifting away from yes-or-no questions and instead inviting more open-ended, emotionally reflective conversations:
• “What’s something you’ve enjoyed doing with friends lately?”
• “Who do you usually spend time with during lunch or recess?”
• “Is there anything at school that has felt uncomfortable or upsetting?”
• “What makes you feel included or left out during the day?”
• “What do you look forward to when you go to school? What do you hope doesn’t happen?”
• “When was a time you felt really good or really bad around your classmates?”
Many experts, including Dr. Ross Greene, remind us that behavior is communication. When we explore what lies beneath the behavior, we help children feel safe, understood and supported.
At Anchored Pediatric Mental Health, our goal is to care for children and families beyond symptom management. I am grateful to have the time and structure to explore each child’s story more deeply through comprehensive assessments, including ADHD evaluations, anxiety screenings and executive function mapping.
When families need additional support with communication, regulation or day-to-day functioning, we often recommend Anchored Coaching as a complementary, non-medical resource. There, we integrate family coaching, HeartMath® biofeedback tools and skill-building strategies to strengthen self-awareness and resilience.
Across both practices, we approach each child as a whole person. When a child understands how their brain works and develops tools to manage stress, they feel more empowered to navigate challenges, bullying included.
In the early weeks of the school year, pediatricians are in a unique position to recognize early signs of social stress, relational trauma or emotional overload. These cues may be subtle, but with gentle inquiry and curiosity, they can open the door to meaningful support.
Consider asking:
• “Has your child said anything about other kids being unkind?”
• “Who do they usually spend time with at school?”
• “Have there been any new complaints, fears or changes in behavior since school started?”
• “Are you seeing more emotional outbursts, shutdowns or withdrawal at home?”
When patterns like these emerge, take time to document your observations, validate the family’s concerns, and provide supportive next steps. Encourage parents to connect with school counselors, explore 504 or IEP evaluations, and seek trauma-informed care when distress continues. Even a small moment of attunement in the exam room can change the trajectory of a child’s school experience.
The Bigger Picture: Awareness and Acceptance
We need to keep moving toward early identification and integrated care. In 2021, the American Academy of Pediatrics (AAP), American Academy of Child & Adolescent Psychiatry (AACAP) and Children’s Hospital Association (CHA) jointly declared a national emergency in children’s mental health. That call is still urgent today.
Awareness of what bullying can look like, and acceptance of our role in addressing it, can transform lives. When we validate a child’s experience and help families connect the dots, we foster resilience.
Let’s continue building bridges between medicine, education and coaching. Healing begins with listening. Progress is possible through each visit, each question and each moment of connection.
www.anchoredtx.com www.anchoredtxcoaching.com
References:
1. Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance – United States, 2021. https://www.cdc.gov/ healthyyouth/data/yrbs/index.htm
2. American Academy of Pediatrics. Bullying: It’s Not Just a Phase. https://www.aap.org/en/patient-care/bullying/
3. Twyman KA, et al. Bullying and Children With Disabilities. J Dev Behav Pediatr. 2010;31(4):349-57
4. AAP-AACAP-CHA Declaration of a National Emergency in Children’s Mental Health. https://www.aap.org/en/advocacy/ child-and-adolescent-mental-health/

Grizelda Anguiano, MD, is a board-certified pediatrician specializing in pediatric mental health. She is the founder of Anchored Pediatric Mental Health and Anchored Coaching, where she supports families navigating ADHD, anxiety and executive function challenges. Her work bridges clinical care and family-centered coaching to promote clarity, connection and resilience. Dr. Anguiano is a member of the Bexar County Medical Society.

By Jennifer Page, PhD
High-risk pregnancies bring more than medical concerns — they often come with emotional strain, logistical hurdles and complex care plans. At Methodist Children’s Hospital in San Antonio, our Perinatal Navigation Program is answering this challenge with compassion, clinical coordination and personalized support.
With San Antonio’s maternal health needs rising — particularly in underserved communities — our perinatal navigators serve as trusted guides, ensuring that expectant mothers with pregnancy complications receive timely, tailored care from diagnosis through delivery.
A Local Challenge: Rising Risks in Bexar County
Bexar County is experiencing increasing rates of high-risk pregnancies due to chronic conditions and gaps in early prenatal care. Consider the data:
• Only 67% of women in Bexar County begin prenatal care in the first trimester — far below the national average of 85%.
• 3% of pregnant individuals receive no prenatal care at all.
• Chronic illnesses like diabetes and hypertension are significantly more prevalent locally than statewide.
Hispanic and African American mothers are disproportionately affected by healthcare access barriers, including transportation, delayed Medicaid enrollment and limited health literacy.
These challenges make coordinated care not just helpful — but essential.
“Upon diagnosis of a complication, our navigator is there to guide patients every step of the way,” explains Ashley Klatt, BSN, RN, Perinatal Navigator. “We help families understand their clinical condition and coordinate personalized care across a comprehensive team of specialists.” Our team of navigators are experienced nurses and available across the Methodist system of hospitals, supporting high-level communication between all staff caring for both mom and baby. The
perinatal navigator also serves as a point of contact for the patient to answer questions, assist with barriers to care, connect with resources, and provide support.
• Placenta disorders (PASD spectrum, previa)
• Maternal cardiac concerns
• Congenital anomalies
• Multiple gestations
• Risk of prematurity and NICU admission
• Infants and children with cardiovascular needs
• Patients requiring multidisciplinary care coordination
Maria was overjoyed to learn she was expecting again. With a healthy 4-year-old daughter and no prior complications, she never imagined this pregnancy would be any different. But at just 28 weeks, Maria was diagnosed with both placenta accreta and placenta previa — serious conditions that can lead to severe complications and require a multidisciplinary team to manage the high risk of hemorrhage.
That’s when she was introduced to Ashley, a perinatal nurse navigator, whose role is to guide high-risk expectant mothers through their care journey.
At 30 weeks, Maria’s routine doctor’s visit took an unexpected turn. Due to worsening complications, she needed to be admitted to the hospital immediately. Scared and overwhelmed, the first person she called was Ashley. “Talking to Ashley about my situation was easy,” Maria said. “She was comforting and felt like a friend I had known for a long time. She explained everything — what to expect during delivery and recovery for both me and my baby. It gave me peace.”
Thanks to the coordinated efforts of the perinatal navigation team, Maria’s care was managed seamlessly, even with the early admission.
“On the day of delivery, I was filled with gratitude,” she recalled. “So many experienced providers were there with me. Although my
‘tiny but mighty’ baby girl arrived 10 weeks early, I knew we were in good hands. Ashley wasn’t just my nurse navigator; she was my friend. She visited me, reassured me, and reminded me that everything was going to be all right.”
Ashley’s support didn’t end with delivery. She continued to check in on Maria and her daughter in the NICU until the day they finally went home. Maria’s journey is a powerful reminder that behind every high-risk pregnancy is a team of dedicated professionals, like Ashley, making sure no mother feels alone.
Dr. David Lam, Medical Director of Women’s & Perinatal Services, underscores the power of collaboration: “The navigator is the clinical compass by coordinating care with the multidisciplinary team. The complex team (including OB, MFM, NICU, pediatric and adult subspecialists) is working toward the same goal: safe delivery and maternal well-being. This continuity builds trust with families and ensures seamless transitions between providers.”
Beyond clinical care, many mothers face social stressors that impact their pregnancy journey. Navigation connects families to resources to bridge those gaps — ensuring specialist appointments are scheduled, assisting with barriers to care, connecting with resources, and providing education and guidance based on their needs.
“It is truly an honor to support mothers who carry the emotional weight and stress of a high-risk diagnosis, whether it be for herself, her baby or sometimes both,” Klatt adds. “When mothers are overwhelmed with the amount of information regarding their diagnosis and care, the perinatal navigator walks her step-by-step to help decrease the emotional anxiety. Whether that is taking the patient on a personalized hospital tour, scheduling consultations with hospital specialists, or frequent phone check-ins, these actions help to transform fear into empowerment.”
The Methodist Commitment: “Serving Humanity to Honor God by Providing Exceptional and Cost-Effective Healthcare to All.”
At Methodist Healthcare, we believe high-risk mothers and babies deserve an informed and supported birth experience. Perinatal Navigation is how we deliver on that promise — by lifting barriers, building trust, and walking with moms every step of the way.

Together, we can connect families facing a complex medical diagnosis to a team they feel confident with and experience the compassionate care they deserve — right here in San Antonio.
Methodist Children’s Hospital Perinatal Navigators:


Ashley Klatt, BSN RN 210-877-4696
Ashley Kassner BSN, RNC-NIC 726-437-1453
Perinatal navigators also available across the Methodist Healthcare System:


Metropolitan Methodist Trish Horlacher, MSN, RN 210-917-1300
Methodist Stone Oak: Hannah Uriegas, BSN, RN 726-248-0450
Pediatric congenital heart navigator across the Methodist Healthcare System:

Adri Davenport, MSHA, BSN, RN, CPN 210-575-9088
Methodist Healthcare System is a Silver Member of the BCMS Circle of Friends Program. SAHealth.com

Jennifer Page, PhD, is the Market Director of Communications and Community Engagement at Methodist Children’s Hospital | Methodist Hospital Campus.

As a BCMS member, you can find exclusive discounts on premium products and services that you and your practice use every day.

Sol Schwartz & Associates P.C. (HHH Gold Sponsor)
Sol Schwartz & Associates is the premier accounting firm for San Antonio-area medical practices and specializes in helping physicians and their management teams maximize their financial effectiveness.
Christopher Davis, CPA 210-384-8000, ext. 118 cbd@ssacpa.com www.ssacpa.com
“Dedicated to working with physicians and physician groups.”
CLA - CliftonLarsonAllen LLP (HH Silver Sponsor)
Transform complexity into opportunities. Work with professionals who understand the specific financial, operational, clinical, and strategic needs of physician practices and medical groups. Our team is made up of knowledgeable, accessible, and responsive individuals devoted to the health care industry.
Bryan Garcia
210-298-7924
Bryan.Garcia@CLAconnect.com CLAconnect.com
"We'll get you there."

Aspect Wealth Management (HHH Gold Sponsor)
We believe wealth is more than money, which is why we improve and simplify the lives of our clients, granting them greater satisfaction, confidence and freedom to achieve more in life.
Michael Clark President 210-268-1520
MClark@aspectwealth.com www.aspectwealth.com
“Your wealth. . .All aspects”

Atlas Retirement Strategies LLC (HHH Gold Sponsor)
Atlas Retirement Strategies LLC is a comprehensive financial planning firm dedicated to serving the unique needs of the medical community. We offer customized strategies in business planning, retirement planning, risk management, wealth preservation, estate planning, and wealth transfer – empowering healthcare professionals to achieve long-term financial security, clarity, and peace of mind.
David M. Webb, Ph.D., MSM, CLF, CLTC, LACP
Founder & Principal
210-281-4400
David@atlas-plans.com www.atlas-plans.com

Broadway Bank (HHH Gold Sponsor)
Healthcare banking experts with a private banking team committed to supporting the medical community.
Thomas M. Duran
SVP, Private Banking Team Lead 210-283-6640
TDuran@broadway.bank www.broadwaybank.com
“We’re here for good.”

Texas Partners Banks (HHH Gold Sponsor)
Our private banking team specializes in healthcare banking and will work with you to craft and seamlessly integrate financial solutions for you and your practice, including practice loans, lines of credit and custom local lockbox solutions headquartered in San Antonio.
Maria Breen 210-807-5562
Maria.Breen@texaspartners.bank www.texaspartners.bank

Lone Star National Bank (HHH Gold Sponsor)
Established in 1983, Lone Star National Bank has provided banking services to communities in South Texas for the past 41 years. LSNB is an independent and locally owned bank subsidiary of Lone Star National Bancshares-Texas, Inc with consolidated assets of $3 billion (12/31/23) and 36 full-service banking centers throughout Starr, Hidalgo, Cameron and Bexar counties. Aside from personal and business banking, LSNB offers investments, wealth management & trust along with property and casualty insurance, health insurance and supplemental coverage.
Ivan Corona Molina Assistant VP 210-479-4713
MolinaI@lonestarnationalbank.com www.lonestarnationalbank.com
“We do what the Little Banks can’t, and the Big Banks won’t!”
Amegy Bank of Texas (HH Silver Sponsor)
We believe that any great relationship starts with five core values: Attention, Accountability, Appreciation, Adaptability and Attainability. We work hard and together with our clients to accomplish great things.
Robert Lindley
SVP | Private Banking Team Lead 210-343-4526
Robert.Lindley@amegybank.com
Denise Smith
Vice President | Private Banking 210-343-4502
Denise.C.Smith@amegybank.com
Scott Gonzales
Assistant Vice President | Private Banking 210-343-4494
Scott.Gonzales@amegybank.com www.amegybank.com “Community banking partnership”
Synergy Federal Credit Union (HH Silver Sponsor)
Looking for low loan rates for mortgages and vehicles? We've got them for you. We provide a full suite of digital and traditional financial products, designed to help physicians get the banking services they need.
Synergy FCU Member Services 210-750-8333 info@synergyfcu.org www.synergyfcu.org
“Once a member, always a member. Join today!”


American Health Imaging (HHH Gold Sponsor)
American Health Imaging (AHI) has 5 state-of-the-art imaging centers in San Antonio, TX with industry- boardcertified subspecialized radiologists delivering precise, reliable results. Easy scheduling and prompt report turnaround times, serving both physicians and their patients. Imaging at AHI is priced up to 60% less than hospitals and in-network with 99% of health plans with competitive rates to save patients money. AHI has an additional 37 best-in-class diagnostic imaging facilities in Alabama, Florida, Georgia, Texas and South Carolina. US Radiology Physician Number 210-572-1211
Casey Allen
Regional Sales Director | San Antonio US Radiology Specialists 210-846-0606
Casey.Allen@usradiology.com
Jasmine Mendoza
Jasmine.Mendoza@usradiology.com
Jaime Zamora
Jaime.Zamora@usradiology.com
Sydnie Caradec
Sydnie.Caradec@usradiology.com
Sarah McMindes
Sarah.Mcmindes@usradiology.com
Scott Roberson
Scott.Roberson@usradiology.com
Ryan Denman
Ryan.Denman@usradiology.com www.americanhealthimaging.com (main site) www.americanhealthimaging.com/ physician-resources/ (Physician Resources to refer to American Health Imaging)

Bexar Credentials Verification, Inc. (HHHH 10K Platinum Sponsor)
Bexar Credentials Verification Inc. provides primary source verification of credentials data that meets The Joint Commission (TJC) and the National Committee for Quality Assurance (NCQA) standards for healthcare entities.
Betty Fernandez Director of Operations 210-582-6355
Betty.Fernandez@bexarcv.com www.bexarcv.com
“Proudly serving the medical community since 1998”

Avid Wealth Partners (*** Gold Sponsor)
For over 15 years, Avid Wealth Partners has been the trusted financial partner for local physician specialists and practice owners.
We specialize in physician-focused financial advising, offering proactive tax planning, customized investment strategies, and comprehensive risk management solutions. Our approach addresses every aspect of your financial life, protecting your hardearned assets and building lasting wealth. With a team of credentialed specialists, we simplify complexity so you can focus on what you do best— caring for patients
MDWealth@avidwp.com www.avidforphysicians.com
210-864-3333

Elizabeth Olney with Edward Jones (HHH Gold Sponsor)
We learn your individual needs so we can develop a strategy to help you achieve your financial goals. Join the nearly 7 million investors who know. Contact me to develop an investment strategy that makes sense for you.
Elizabeth Olney Financial Advisor 210-858-5880
Elizabeth.Olney@edwardjones.com www.edwardjones.com/elizabeth-olney
Aspect Wealth Management (HHH Gold Sponsor)
We believe wealth is more than money, which is why we improve and simplify the lives of our clients, granting them greater satisfaction, confidence and freedom to achieve more in life.
Michael Clark President 210-268-1520
MClark@aspectwealth.com www.aspectwealth.com
“Your wealth. . .All aspects”
Hancock Whitney (HH Silver Sponsor)
Since the late 1800s, Hancock Whitney has embodied core values of Honor & Integrity, Strength & Stability, Commitment to Service, Teamwork and Personal Responsibility. Hancock Whitney offices and financial centers in Mississippi, Alabama, Florida, Louisiana and Texas offer comprehensive financial products and services, including traditional and online banking; commercial, treasury management, and small business banking; private banking; trust; healthcare banking; and mortgage services.
John Riquelme
San Antonio Market President 210-273-0989
John.Riquelme@hancockwhitney.com
Serina Perez San Antonio Business Banking 210-507-9636
Serina.Perez@hancockwhitney.com
CARE

UT Health San Antonio
MD Anderson Cancer Center (HHH Gold Sponsor)
UT Health provides our region with the most comprehensive care through expert, compassionate providers treating patients in more than 140 medical specialties at locations throughout San Antonio and the Hill Country.
UT Health San Antonio Physicians
Regina Delgado
Business Development Manager 210-450-3713
DelgadoR4@uthscsa.edu
UT Health San Antonio
MD Anderson Mays Cancer Center
Laura Kouba
Business Development Manager 210-265-7662
NorrisKouba@uthscsa.edu
Appointments: 210-450-1000
UT Health San Antonio 7979 Wurzbach Road San Antonio, TX 78229
SERVICES

Golden Billing & Benefits
(HHH Gold Sponsor)
Golden Billing is owned and operated for over 20 years in Houston, TX. The owner, Marcus Yi, is focused on creating a partnership with clients. We are dedicated to optimizing the small business doctor’s productivity and maximizing practice cash flow by accurate claims coding and timely
processing. Call today for a free consultation. If you don’t want to use us at lease maybe we can help you fine tune your decision.
Marcus Yi 713-263-0054
MYi@goldenbilling.com www.goldenbilling.com

Genuine Health Group (HHH Gold Sponsor)
Genuine Health Group partners with primary care providers to help them successfully adopt value-based payment models and demonstrate better health outcomes. Providers choose us for our proven expertise and consistency both for their patients enrolled in Medicare Advantage plans and for their patients with traditional Medicare who can align with one of ACOs. We have a track record of effectively reducing the cost of care while simultaneously improving care quality.
786-878-5500 info@genuinehealthgroup.com www.genuinehealthgroup.com
Equality Health (HH Silver Sponsor)
Equality Health deploys a wholeperson care model that helps independent practices adopt and deliver value-based care for diverse communities. Our model offers technology, care coordination and hands-on support to optimize practice performance for Medicaid patients in Texas.
Cristian Leos Network Development Manager 210-608-4205
CLeos@equalityhealth.com www.equalityhealth.com “Reimagining the New Frontier of Value-Based Care.”
SpeedEz’s (** Silver Sponsor)
For over three decades, SpeedE’z has been Bexar County’s truly local partner for answering service, contact center and courier solutions. R.N. owned and family-led, we combine compassionate care with professional expertise. Our HIPAA Certification, SOC 2 Type II Compliance and Woman-Owned HUB status reflect our commitment to integrity and security. Ranked Top Ten nationally in the ATSI Award of Excellence, our team delivers results that stand out – rooted right here in San Antonio!
Lauren Garza 210-615-0964. Lauren@speedez.com https://speedez.com/
DialOPS (H Bronze Sponsor)
Dialops is a trusted U.S.-based medical answering service and virtual receptionist solution designed specifically for healthcare practices. We provide 24/7 live call handling, HIPAA-compliant messaging, appointment scheduling, and reliable after-hours and overflow support. Our medically trained agents answer every call with professionalism and care— just like your in-office staff—ensuring your patients always feel heard and supported. From solo providers to busy clinics, Dialops helps reduce missed calls, ease front desk overload, and improve the patient experience—all at a fraction of the cost of hiring in-house.
Rachel Caero
Rachel@dialops.net
Call 877-2-DIALOPS/ 210-699-7198 or visit www.dialops.net to get started today.

TMA Insurance Trust (HHHH 10K Platinum Sponsor)
TMA Insurance Trust is a full-service insurance agency offering a full line of products – some with exclusive member discounts and staffed by professional advisors with years of experience. Call today for a complimentary insurance review. It will be our privilege to serve you.
Wendell England Director of Member Benefits 512-370-1746
Wendell.England@tmait.org 800-880-8181 www.tmait.org “We offer BCMS members a free insurance portfolio review.”

Texas Medical
(HHHH 10K Platinum Sponsor)
With more than 20,000 healthcare professionals in its care, Texas Medical Liability Trust (TMLT) provides malpractice insurance and related products to physicians. Our purpose is to make a positive impact on the quality of healthcare for patients by educating, protecting and defending physicians.
Patty Spann Director of Sales and Business Development 512-425-5932
Patty-Spann@tmlt.org www.tmlt.org
“Recommended partner of the Bexar County Medical Society”
Continued on page 42

The Bank of San Antonio Insurance Group, Inc.
(HHH Gold Sponsor)
We specialize in insurance and banking products for physician groups and individual physicians. Our local insurance professionals are some of the few agents in the state who specialize in medical malpractice and all lines of insurance for the medical community.
Katy Brooks, CIC 210-807-5593
Katy.Brooks@bosainsurance.com www.thebankofsa.com “Serving the medical community.”
MedPro Group
(HH Silver Sponsor)
Rated A++ by A.M. Best, MedPro Group has been offering customized insurance, claims and risk solutions to the healthcare community since 1899. Visit MedPro to learn more.
Kirsten Baze, RPLU, ARM AVP Market Manager, SW Division 512-658-0262
Fax: 844-293-6355
Kirsten.Baze@medpro.com www.medpro.com
LASO Health Telemedicine and Rx App
(HH Silver Sponsor)
LASO Health is the industry’s only solution that makes healthcare services accessible, cost-transparent and convenient. Its mission is to reinvent “healthcare” in the United States by empowering every individual and employer, insured or uninsured to have easy, timely, predictable, cost-effective care. LASO combines an intuitive, mobile superapp with a marketplace of virtual and in-person health services to give customers a one-touch, onestop-shop, comprehensive health solution.
Ruby Garza, MBA 210-212-2622
RGarza@texaskidneycare.com www.lasohealth.com

Parvus Medical Suites (HHHH 10K Platinum Sponsor)
Parvus Medical Suites offers a new way to start your own private clinical practice, either full-time or part-time, at a much lower cost than a traditional clinic. We take care of providing well-qualified employees, so that you can focus solely on delivering high-quality patient care. Our turn-key practice spaces in San Antonio and New Braunfels are available for short- and long-term lease options, and come complete with all amenities. Micropractice medicine is revolutionizing independent clinical care.
John Rodriguez, MD
Chief Medical Officer 210-632-3411
DrJohn@parvussuites.com www.parvussuites.com
Henry Schein Medical (HH Silver Sponsor)
From alcohol pads and bandages to EKGs and ultrasounds, we are the largest worldwide distributor of medical supplies, equipment, vaccines and pharmaceuticals serving officebased practitioners in 20 countries. Recognized as one of the world’s most ethical companies by Ethisphere.
Kelly Emmon Field Sales Consultant 210-279-6544
Kelly.Emmon@henryschein.com www.henryschein.com
“BCMS members receive GPO discounts of 15 to 50 percent.”
Eleos Virtual Healthcare Solutions (HH Silver Sponsor)
Empowering physicians for a Balanced Future. Our virtual health associates alleviate administrative burdens in the evolving healthcare landscape, combatting burnout. Join us in transforming healthcare delivery, prioritizing your wellbeing and patient care.
Darby Rodriguez Regional Client Executive 281-753-3565
D.Rodriguez@eleosvhs.com www.equalityhealth.com
“Reimagining the New Frontier of Value-Based Care”
Methodist Physician Practices (**Silver Sponsor)
Methodist Physician Practices is committed to providing exceptional care for patients in greater San Antonio and South Texas. As part of Methodist Healthcare, we are dedicated to raising the standards of performance excellence while advancing the health and well-being of the communities we serve. Our extensive network of highly-skilled primary care physicians, specialists and surgical care providers ensures patients receive comprehensive, coordinated and compassionate care. As part of the Methodist Healthcare System, our physicians are committed to delivering personalized, high-quality services that meet the diverse needs of our patients. At Methodist Physician Practices, we go beyond healthcare — providing hope, healing and unwavering support for each individual we serve.
Erin Fitzgerald Methodist Healthcare I Methodist Physician Practices M:281-673-7350 methodistphysicianpractices.com
The Health Cell (HH Silver Sponsor)
“Our Focus is People”
Our mission is to support the people who propel the healthcare and bioscience industry in San Antonio. Industry, academia, military, nonprofit, R&D, healthcare delivery, professional services and more!
Kevin Barber President 210-308-7907 (Direct) KBarber@bdo.com
Valerie Rogler Program Coordinator 210-904-5404
Valerie@thehealthcell.org www.thehealthcell.org
“Where San Antonio’s Healthcare Leaders Meet”
San Antonio Medical Group Management Association (SAMGMA)
(HH Silver Sponsor)
SAMGMA is a professional nonprofit association with a mission to provide educational programs and networking opportunities to medical practice managers and support charitable fundraising.
Jeannine Ruffner
President info4@samgma.org www.samgma.org

Favorite Healthcare Staffing (HHHH 10K Platinum Sponsor)
Serving the Texas healthcare community since 1981, Favorite Healthcare Staffing is proud to be the exclusive provider of staffing services for the BCMS. In addition to traditional staffing solutions, Favorite offers a comprehensive range of staffing services to help members improve cost control, increase efficiency and protect their revenue cycle.
San Antonio Office 210-301-4362 www.favoritestaffing.com
“Favorite Healthcare Staffing offers preferred pricing for BCMS members.”


By Stephen Schutz, MD
As I hope most SanAntonio Medicine magazine readers know, I’ve been an automotive writer for more than 30 years, which means countless test drives, reviews, events and pretty much everything else, “car.” This has put me in the mix with other automotive journalists, industry insiders, car enthusiasts, curious novices and everything in between. A few months ago, my Instagram feed featured a post tagging a remarkable moment in car advertising history that stopped me dead in my tracks because it involved me. Kind of.
The post featured a 1990sera glossy magazine ad for BMW featuring a 3-series sedan balancing perfectly, mid-air, on a triangular fulcrum. Just above the hood of the vehicle was a bird’s feather, floating downward toward what one might think was a soft landing. But in truth the feather threatened utter disaster. “OH NO.” was the headline. The ad called out the relentless precision of BMW’s engineering that produced a sports sedan so in balance that it could be thrown off by the weight of a mere feather. It was perfection.

Credit: https://delta.creativecirclecdn.com/cricket/original/20250605-103618-163-BMW_feather.png.jpg

The ad was produced by Mullen Advertising, founded by a remarkable man named Jim Mullen. And in 1993 Mullen stunned the business world by winning the coveted BMW North America (BMW NA) account, and then creating many award-winning ads, some of which are being rediscovered today on Instagram.
Mullen Advertising’s rise from a regional agency founded in the 1970s on a kitchen table to an international powerhouse is a testament to the vision and passion of Jim Mullen. The agency quickly gained a reputation for innovative and successful campaigns for companies like Timberland®, Veryfine Juice™ and Smartfood Popcorn®.
By 1993, Jim, a lifelong car enthusiast and successful race car driver, had nibbled at the edges of the global automotive industry with work for Bentley and Rolls Royce, and was ready to represent a major car brand when the BMW NA account came up for review. Mullen wanted a brand that resonated with enthusiasts but was ready to grow beyond that niche. BMW was that brand, and the agency put together a pitch that has since become legendary in advertising circles: the Mullen team assembled eight historically significant BMW cars and displayed them where the BMW decision makers, who’d flown in from Germany, would walk as they entered the agency. Then they took the extra step of painting a large BMW logo on the courtyard gravel through which the BMW execs would pass on their way inside.
The reason I was and remain so personally interested in all of that is that my sister Erika worked at Mullen in 1993 and witnessed this astounding event. As she described it, Jim and the team’s pitch, which focused on elevating BMW’s identity from being a car company for enthusiasts to becoming an enthusiasts’

brand for everyone, was “magical,” and it was enough to win Mullen the account.
Shortly after the win, I came by the agency for a visit. As I meandered up the same walkway the BMW bigwigs had negotiated six months earlier, Jim Mullen walked out to greet me, dressed in a tweed jacket and a button-down shirt. He shook my hand warmly and said, “Steve, Erika tells me you’re a car guy. I just got a new car, and I want you to drive it when you take her out for lunch.” Handing me the keys to a brand-new, 1994 BMW M5, Jim was trusting me with one of the finest driving machines of the era. After I nervously asked when he needed it back, at like 12:05 p.m., Jim replied, with a furrowed brow, “I have to get to a 5:30 meeting. Is 5:00 p.m. okay?” Umm, yes Jim, that’s fine. I drove it responsibly with occasional bursts of brio and was exhilarated by the experience, returning it well before the generous deadline. It was my first time driving an M car, and it remains one of the best cars I’ve ever driven.
The advertising campaigns produced during this period by Mullen’s BMW creative team earned numerous awards, reinforcing Mullen’s rising global reputation as a creative leader. Unfortunately, the partnership ended a few years later due to political changes at BMW NA, not uncommon in the advertising world, but the work Mullen produced during that time left an indelible mark on BMW’s branding and on the advertising world.
In 1999, Mullen Advertising began a new chapter when it was acquired by the Interpublic Group of Companies (IPG). Jim Mullen retired shortly after the sale of his company, but the agency continued to grow and thrive, merging with Long Haymes Carr in 2001 to form Mullen/LHC. Advertising Age named the firm the third-best agency in the U.S. in 2011, and Fast Company listed it among the top 10 innovative marketing companies that same year. Today, Mullen Advertising is MullenLowe, no longer a small, local company going for its big shot.
And 30-plus years on, I’m a veteran automotive journalist who still loves driving cool cars and writing about them.
Thank you, Jim Mullen, for producing some of the best advertising BMW has ever produced and for giving me my first BMW M-car experience.
And thank you, Instagram, for letting those ads live on.

Credit: https://delta.creativecirclecdn.com/cricket/original/20250605-103623-e0eBMW_ice%20fishing.png.jpg

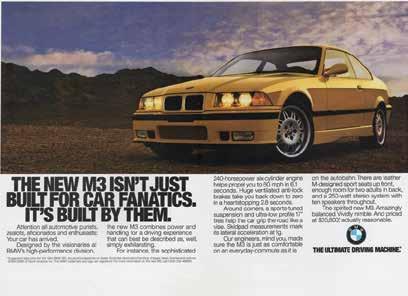
Credit: https://delta.creativecirclecdn.com/cricket/original/20250605-103614-fc7BMW_fanatic.png.jpg

Stephen Schutz, MD, is a board-certified Gastroenterologist who lived in San Antonio in the 1990s when he was stationed here in the U.S. Air Force. He has been writing auto reviews for San Antonio Medicine magazine since 1995.

11911 IH 10 West San Antonio, TX 78230
Coby Allen 210-696-2232
Audi Dominion 21105 West IH 10 San Antonio, TX 78257
Anthony Garcia 210-681-3399
Northside Honda
9100 San Pedro Ave. San Antonio, TX 78216
Daniel Garcia 210-341-1356
Mercedes Benz of Boerne 31445 IH 10 West Boerne, TX 78006
James Godkin 830-981-6000
14610 IH 10 West San Antonio, TX 78249
Tim Rivers 832-428-9507
Northside Chevrolet 9400 San Pedro Ave. San Antonio, TX 78216
Emilio Gonzalez 210-341-3311
Auto Group
North Park Lexus 611 Lockhill Selma San Antonio, TX 78216
Jose Contreras 320-308-8900
Bluebonnet Chrysler
Dodge Ram 547 S. Seguin Ave. New Braunfels, TX 78130
Kersten Thomas 830-606-3463
Cavender Toyota 5730 NW Loop 410 San Antonio, TX 78238
Spencer Herrera 210-581-0474
Mercedes Benz of San Antonio 9600 San Pedro San Antonio, TX 78216
Chris Martinez 210-366-9600
9455 IH 10 West San Antonio, TX 78230
Jordan Trevino 210-764-6945
North Park Lexus at Dominion 25131 IH 10 W Dominion San Antonio, TX 78257
James Cole 210-816-6000
Northside Ford 12300 San Pedro San Antonio, TX 78216
Marty Martinez 210-477-3472
North Park Lincoln 9207 San Pedro San Antonio, TX 78216
Sandy Small 210-341-8841
North Park Subaru 9807 San Pedro San Antonio, TX 78216
Raymond Rangel 210-308-0200
North Park Toyota 10703 SW Loop 410 San Antonio, TX 78211
Justin Boone 210-635-5000
North Park Subaru at Dominion 21415 IH 10 West San Antonio, TX 78257
Phil Larson 877-356-0476
• Fast prior authorizations assistance for easy scheduling
• Prompt turnaround on standard reports within hours, not days
• Easy-to access physician portal for instant access to reports
• Easily accessible subspecialized radiologists for questions
• State-of-the-art imaging equipment for the diagnostic insights you need for next steps in patient care
• 6 convenient locations throughout San Antonio and New Braunfels
• Same-day and next-day appointments
• Extended and weekend hours to fit your patients’ busy schedules
• In-network with 99% of insurance plans and costs up to 60% less than hospital-based imaging
• Faster scanning technology increases patient comfort with an average MRI scan of 15 minutes or less