Volume 84 | Number 1 | January - February - March - April 2021
Four monthly publication of the Greek Paediatric Society
008
EDITORIAL
Stelios Antoniadis
010
RESEARCH STUDIES
Early cardiac ultrasound targeted treatment of patent ductus arteriosus with paracetamol in infants <30 weeks
Dimitrios C. Konstantinou, George S. Tsaousis, Foteini-Maria Chantzi, Chrissi Zacharioudaki, Panos Papandreou, Maria Klavdianou
022
Incidence of haemodynamically significant Patent Ductus Arteriosus in preterm neonates with extremely low birth weight and comparison of aggressive versus conservative management D. Rallis, F. Balomenou, A. Drougia, T. Benekos, A. Vlahos, V. Giapros
032
REVIEW ARTICLES
Psychosocial care for children and adolescents with hemophilia at the Hemophilia Comprehensive Care Centre for Children and Adolescents, at the “Aghia Sofia” Children’s Hospital Helen Pergantou, Eleni Riga, Vana Kolliopoulou, Georgia Goula, Gerasimos Kolaitis
044
Hypoaldosteronism in children: Diagnosis and management Myrto Bonataki, Elpis-Athina Vlachopapadopoulou, Stefanos Michalacos
056
The microbiome in the first years of life and its health impact
Early cardiac ultrasound targeted treatment of patent ductus arteriosus with paracetamol in infants <30 weeks
Dimitrios C. Konstantinou, George S. Tsaousis, Foteini-Maria Chantzi, Chrissi Zacharioudaki, Panos Papandreou, Maria Klavdianou
Abstract
Background: Prophylactic treatment of patent ductus arteriosus (PDA) with indomethacin had been shown to reduce the incidence of short-term morbidity of preterm infants, but it was abandoned due to its side effects. Paracetamol (PCM) appears to be less toxic than nonsteroidal anti-inflammatory drugs. This study aimed to investigate the efficacy and safety of PCM in early targeted treatment of hemodynamically significant PDA (hsPDA). Methods: Infants less than 30 weeks gestational age (GA) were enrolled. All eligible infants with echocardiographictargeted hsPDA were given, within 24 hours of life, a full course of intravenous PCM (15mg/ kg/dose every 6 hours for 3 days). A second course of PCM was administered if the first course was unsuccessful. If closure was not achieved, infants were managed with ibuprofen. The infants underwent ligation if PDA remained hemodynamically significant. Results: Among the 106 eligible infants included in the study, 49 infants (mean birth weight 1105±241 g, mean GA 28±1 wks) had hsPDAs and received intravenous PCM. Two from the 49 neonates died from causes irrelevant to PCM administration. Forty three (91.5%) had their PDAs closed after two cycles of PCM with no cases of hepatotoxicity. Also, there were no cases of early pulmonary hemorrhage and the incidence of necrotizing enterocolitis was remarkably low (2.1%). Conclusion: Echocardiographically early targeted treatment of hsPDA with intravenous PCM of infants less than 30 weeks is feasible, efficient and safe. Therefore, PCM could be used as a first line treatment for closure of hsPDA in preterm infants.
Department of Cardiology, IASO Children΄s Hospital, Athens
Βιβλιογραφία
1. Singh Y and Gooding N: Paracetamol for the treatment of patent ductus arteriosus in very low birth weight infants. J Neonatal Biol 2016;5:3.
2. Bancalari E: Current approach to the patent ductus arteriosus in extremely low-birth-weight infants. Neonatology 2017;112;300.
3. El-Khufash A, Jain A, Corcoran D, Shah PS, Cooper CW, Brown N, Poole SD, Shelton EL, Milne GL, Reese J and McNamara PJ: Efficacy of paracetamol on patent ductus arteriosus closure may be dose dependent: evidence from human and murine studies. Pediatr Res 2014; Sep 76(3):238-244.
4. Kluckow M, Jeffery M, Gill A, Evans N: A randomized placebo-controlled trial of early treatment of the patent ductus arteriosus. (DETECT). Arch Dis Child Fetal Neonatal Ed 2014;99:F99-F104.
5. Chaudhari N, Fillipov P, Bhutada A, Rastogi S: Controversies in the management of patent ductus arteriosus in preterm infants. J Neonatal Biol 2016;5:238. DOI:10.4172/21670897.1000238.
6. Harkin P, Harma A, Aikio O, Valkama M, Leskinen M, Saarela T and Hallman M: Paracetamol accelerates closure of the ductus arteriosus after premature birth: A randomized trial: J Pediatr 2016; Clinical Trials.gov:NCT01938261.
7. Pacifici GM, Allegaert K: Clinical pharmacology of paracetamol in neonates: A review. Current therapeutic research. Dec 2015;77:24-30.
8. Le J, Gales MA, Gales BJ: Acetaminophen for Patent Ductus Arteriosus. Ann Pharmacother 2015; 49 :241-246, DOI: 10.1177/10600280I4557564.
9. Terrin G, Conte F, Oncel MY, Scipione A, McNamara PJ, Simons S, Sinha R, Erdeve O, Tekgunduz KS, Dogan M, Kessel I, Hammerman C, Nadir E, Jasani B, Alan S, Manguso F, De Curtis M : Paracetamol for the treatment of patent ductus arteriosus in preterm neonates: a
systematic review and meta-analysis. Arch Dis Child Fetal Neonat Ed published on line August 17, 2015.
10. Ohlsson A, Shah PS: Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low-birth-weight infants. Cochrane Database Syst Rev 2015; Mar11:3.CD010061.
11. Hamrick SE, Hansmann G: Patent ductus arteriosus in the preterm infant. Pediatrics 2010; 125:1020-1030.
12. Tacy TA: Abnormalities of the ductus arteriosus and pulmonary arteries, In Wyman W. Lai, Luc L Mertens, Meryl S Cohen, Tal Geva (eds) <Echocardiography in Pediatric and Congenital Heart Disease: From fetus to adult>, Wiley-Blackwell Publishing 2009: 283-296.
13. Allegaert K, Rayyan M, De Rijdt T, Van Beek F, Naulaers G: Hepatic tolerance of repeated intravenous paracetamol administration in neonates. Paediatr Anaesth 2008; May 18(5):388-92.
14. Rayan RM: A new look at bronchopulmonary dysplasia classification. Journal of Perinatology (2006); 26: 207-209.
15. Papile LA, Burstein J, Burstein R, Koffler H,: Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1500 g. J Pediatr 1978 Apr;92(4):529-34.
16. Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, Brotherton T: Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg 1978 Jan;187(1):1-7.
17. International Committee for the classification of retinopathy of prematurity. The International Classification of Retinopathy of Prematurity revisited. Arch Ophthalmol. 2005 Jul;123(7):991-9.
18. Evans N: Diagnosis of the preterm patent ductus arteriosus: clinical sings, biomarkers or ultrasound? Semin Perinatol 2012;36:114-122.
19. Aikio O, Harkin P, Saarela T, Hallman M: Early paracetamol treatment associated with lowered risk of persistent ductus arteriosus in very preterm infants. J Matern Fetal Neonatal Med 2014;27:1252-1256. Doi:10.3109/14767058.2013.854327.
20. Dash SK, Kabra NS, Avasthi BK, Sharma SR, Padhi P, Ahmed J: Enteral paracetamol or intravenous indomethacin for closure of patent ductus arteriosus in preterm neonates: a randomized controlled trial. Indian Pediatr. 2015;52:573-78.
21. Valerio E, Valente MR, Salvadori S, Frigo AC, Baraldi E, Lago P : Intravenous paracetamol for PDA closure in the preterm: a single-center experience. Eur J Pediatr 2016;175:953-966.
22. Allegaert K, Naulaers G. Haemodynamics of intravenous paracetamol in neonates. Eur J Clin Pharmacol 2010;66:855-8.
23. Kluclow M, Evans N: Ductal shunting, high pulmonary blood flow, and pulmonary hemorrhage. J Pediatr 2000;137:68-72.
24. Schmidt B, Davis P, Moddemann D, Ochlson A, Roberts AS, Saigal S, Solimano A, Vincer M, and Wright LL. Long-Term Effects of Indomethacin Prophylaxis in Extremely-Low-BirthWeight Infants. N Engl J Med 2001;344:1966-1972.
25. Benitz WE and COMMITTEE ON FETUS AND NEWBORN. Pediatrics 2016;137:1.
Incidence of haemodynamically significant Patent Ductus Arteriosus in
preterm neonates with extremely low birth weight and comparison of aggressive versus conservative management
D. Rallis, F. Balomenou, A. Drougia, T. Benekos, A. Vlahos, V. Giapros
Abstract
Background
The current evidence remains controversial regarding the conservative in comparison to pharmacological treatment of preterm neonates with haemodynamically significant patent ductus arteriosus (hsPDA). Our aim was to evaluate the outcomes of premature neonates with hsPDA in comparison to those without, and the effectiveness of conservative compared to aggressive approach.
Methods
The medical records of neonates ≤32 weeks’ gestation and birth weight ≤1000g, admitted to the Neonatal Unit of University Hospital of Ioannina during 2010-2017 were reviewed. HsPDA was defined according to clinical or echocardiographic criteria. In primary analysis we evaluated the characteristics and outcomes between neonates with hsPDA compared to those without hsPDA. Moreover, we performed a subgroup analysis of neonates with hsPDA, comparing conservative approach (fluid limitation, diuretics) versus aggressive treatment (paracetamol, ibuprofen).
Results
D. Rallis
F. Balomenou
A. Drougia
V. Giapros
NICU, University Hospital of Ioannina, Ioannina
T. Benekos
A. Vlahos
Department of Pediatrics, University Hospital of Ioannina, Ioannina
In overall 82 neonates identified; 35 with hsPDA and 47 without. Neonates with hsPDA were of lower gestational age, required prolonged mechanical ventilation and received more blood transfusion within the first 28 days. Also, they developed intraventricular hemorrhage and bronchopulmonary dysplasia in higher proportion, and required prolonged hospitalization. Out of the 35 neonates with hsPDA, 10 neonates received aggressive treatment, while 25 neonates had conservative approach. No significant differences were noted regarding the duration of the mechanical ventilation, intraventricular hemorrhage, bronchopulmonary dysplasia or survival.
Conclusions
In preterm neonates with birth weight ≤1000g hsPDA is associated with prolonged duration of mechanical ventilation, intraventricular hemorrhage and bronchopulmonary dysplasia. Conservative approach was related to similar outcome in comparison to aggressive treatment. Keywords: patent ductus arteriosus, bronchopulmonary dysplasia, preterm neonates
ΑΑΠ:
(IBM, Chicago, Illinois,
Correspondence
Helen Pergantou
Thivon 1 and Papadiamandopoulou str.
Goudi - Athens-Greece
Τ. +302132013756
e-mail: hpergantou@gmail. com
Psychosocial care for children and adolescents with hemophilia at the Hemophilia Comprehensive Care Centre for Children and Adolescents, at the “Aghia Sofia” Children’s Hospital
Helen Pergantou, Eleni Riga, VanaKolliopoulou, Georgia Goula, GerasimosKolaitis
Abstract
Psychosocial care is an essential component of the comprehensive care for children and adolescents with haemophilia, and their families. Chronic diseases, including haemophilia, and the associated insecurity created may produce traumatizing experiences not just for the suffering person but also for other members of the family. Moreover, psychological factors relevant to the disease impact upon health outcomes.
The current paper aims to provide insights into the long-term clinical experience of diverse psychosocial interventions employed by the multidisciplinary team atthe European Haemophilia Comprehensive Care Centre (EH-CCC). The fundamental ideas underlying clinical practice include the establishment of a therapeutic alliance among the multidisciplinary health team, the patient and their families and focus on a personalized approach aiming to normality of the child’s and family’s lives. Psychosocial care comprises several interventions developed globally, i.e. early detection of families’ needs (assessment, referrals), psychoeducation (fairy tales, comics, books for parents and teachers), support group for parents, individual counselling/psychotherapy, family therapy and practical help (during hospitalization, educational counselling).
Helen Pergantou
VanaKolliopoulou
Haemophilia Centre/ Haemostasis and Thrombosis Unit, "Aghia Sophia" Children's Hospital, Athens
Eleni Riga
Georgia Goula GerasimosKolaitis
Department of Child
Psychiatry, School of Medicine, National and Kapodistrian University of Athens, "Aghia Sophia" Children's Hospital
Multi-faceted psychosocial care contributes to the child and family adaptation to the disease as well as to creating favourable environments where children can optimally develop.
1. Srivastava A, Santagostino E, Dougall A. et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia. 2020; 26(Suppl 6):1–158. DOI: 10.1111/hae.14046.
2. Oldenburg J. Optimal treatment strategies for hemophilia: achievements and limitations of current prophylactic regimens, Blood. 2015 26; 125(13):2038-44. DOI: 10.1182/ blood-2015-01-528414.
3. Pergantou H, Platokouki H, Matsinos G, Papakonstantinou O, Papadopoulos A, Xafaki P, Petratos D, Aronis S Assessment of the progression of haemophilic arthropathy in children Haemophilia (2010), 16, 124–129
4. Ljung RCR. Prevention and Management of Bleeding Episodes in Children with Hemophilia. Pediatric Drugs. 2018; 455-464. DOI:10.1007/s40272-018-0307-z.
5. Cassis, F. Psychosocial care for people with hemophilia. Treatment of Hemophilia. N. 44,World Federation of Hemophilia.2007.DOI: 10.1111/j.1365-2516.2012.02909.x.
6. Srivastava A, Brewer A, Mauser-Bunschoten, E et al. Guidelines for the management of haemophilia. Haemophilia. 2013;19(1):1-47.DOI:10.1111/j.1365-2516.2012.02909.x.
7. PennP. Chronic Illness: Trauma, Language, and Writing: Breaking the Silence. Family Process. 2001;40(1):33-52.DOI:org/10.1111/j.1545-5300.2001.4010100033.x.
8. Khair K, Chaplin S. The impact on parents of having a child with haemophilia. The Journal of Haemophilia Practice. 2018;3(2):4-14. DOI:org/10.17225/jhp00075.
9. Beeton K, Neal D, Watson T, Lee CA. Parents of children with haemophilia – a transforming experience. Haemophilia. 2007;13(5):570-579. DOI: 10.1111/j.1365-2516.2007.01494.x.
10. Wiedebusch S, Pollmann H, Siegmund B, Muthny FA. Quality of life, psychosocial strains and coping in parents of children with haemophilia. Haemophilia. 2008;14(5):1014-22. DOI: 10.1111/j.1365-2516.2008.01803.x.
11. Garcia-Dasi M, Torres-Ortuño A, Cid-Sabatel R, Barbero J. Practical aspects of psychological support to the patient with haemophilia from diagnosis in infancy through childhood and adolescence. Haemophilia. 2016; 22(5):349-58. DOI: 10.1111/hae.13018.
12. Cassis FRMY. Hemo Action, playing and learning about hemophilia. World Federation of Hemophilia. 2018.Webpage http://www1.wfh.org/publications/files/pdf-1349.pdf.
13. Furmedge J, Lima S, Monagle P, Barnes C, Newall F. “I don’t want to hurt him”. Parents experiences of learning to administer clotting factor to their child. Haemophilia. 2013;19:206211. DOI: 10.1111/hae.12030.
14. Khair K, Meerabeau L, Gibson F. Self-management and skills acquisition in boys with
haemophilia. Health expectations.2015;18(5):1105-13. DOI: 10.1111/hex.12083.
15. Kirk S, Beatty S, Callery P, Milnes L, Pryjmanchuk S. Perceptions of effective self-care support for children and young people with long-term conditions. Journal of Clinical Nursing. 2012; 21 (13-14): 1974-1987. DOI: 10.1111/j.1365-2702.2011.04027.x.
16. Williams K., Chapman M. Social Challenges for Children With Hemophilia: Child and Parent Perspectives. Social Work in Health Care. 2011;50(3):199-214.
17. Liesbet Van Bulck, Koen Luyckx, Eva Goossens, Leen Oris and Philip Moons. Illness identity: Capturing the influence of illness on the person’s sense of self. European Journal of Cardiovascular Nursing. 2019;18(1):4–6. https://doi.org/10.1177/1474515118811960.
18. Tregidgo C, Elander J. The invisible child: Sibling experiences of growing up with a brother with severe haemophilia—An interpretative phenomenological analysis. Haemophilia. 2019; 25:84–91. https://doi.org/10.1111/hae.13659.
19. Myrin Westerson L., Sparud-Lundin C, Wallengren C, Baghaei F. A tortuous route to a capable fatherhood: the experience of being a father to a child with severe haemophilia. Haemophilia.2015;21:799–805.DOI:10.1111/hae.12781.
20. Goldstein G, Kenet G. The impact of chronic disease on the family. Haemophilia. 2002; 8:461-465. DOI: 10.1046/j.1365-2516.2002.00642.x.
21. Bottos AM, Zanon E, Sartori MT, Girolami A. Psychological aspects and coping styles of parents with Haemophilic child undergoing a programme of counselling and psychological support. Haemophilia. 2007;13(3):305-310.DOI: 10.1111/j.1365-2516.2006.01428.x.
22. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient EducCouns.2002;48:177–87.DOI: 10.1016/ s0738-3991(02)00032-0.
23. Dutreil S, Rice J, Merrit D, Kuebler EJ. Parents Empowering Parents (PEP) Program: understanding its impact on the bleeding disorders community. Haemophilia.2011;17:895–900. DOI: 10.1111/j.1365-2516.2011.02512.x.
24. Massimo L. Relationship Between Parents And Sick Children: Difficulties And Possibilities Regarding Understanding.In New Developments in Parent-Child Relations, eds, Nova Science Publishers, Inc, New York. 2006;264-271.
Τ.
F.
Κ.
e-mail: elpis.vl@gmail.com
Correspondence
Elpis-Athina
Vlachopapadopoulou
Thivon 1 and Livadias str. Athens-Greece
Τ. +302132009851
F. +302132009531
Κ. 6932247228
e-mail: elpis.vl@gmail.com
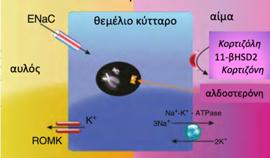
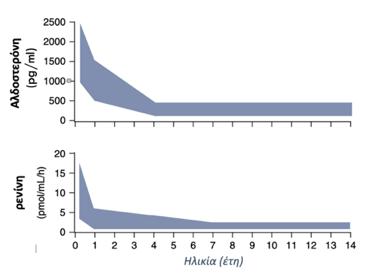
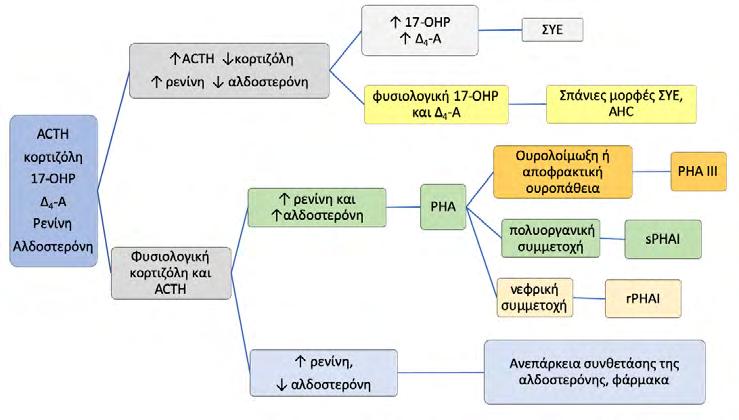
Hypoaldosteronism in children: Diagnosis and management
Hypoaldosteronism is associated with either insufficient aldosterone production or aldosterone resistance. The most common cause of hypoaldosteronism in early infancy is congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Clinical presentation typically includes failure to thrive, vomiting, hyperkalemia, metabolic acidosis and salt losing. In case of a salt wasting crisis, initial management requires collection of a critical sample for the essential hormonal investigations, treatment of electrolyte imbalances and restoration of intravascular fluid volume. The presenting electrolyte abnormalities should raise the clinician’s concern for congenital adrenal hyperplasia, and immediate treatment with steroids can prevent life-threatening complications, while trying to determine the definitive diagnosis. Renal ultrasonography and urine culture are also useful for exclusion of secondary causes of aldosterone resistance. A deeper understanding of the etiology of hypoaldosteronism may prove of great importance in the management of affected infants.
Key words: hypoaldosteronism, salt wasting crisis, hyponatremia, hyperkalemia
από Bhansali A, Gogate Y. Clinical Rounds in Endocrinology [Volume I - Adult Endocrinology]. 2015. 163–185 p
2. Bizzarri C, Pedicelli S, Cappa M, Cianfarani S. Water balance and “salt wasting” in the first year of life: The role of aldosterone-signaling defects. Horm Res Paediatr. 2016;86(3):143–53.
3. McPhee S, Μουτσόπουλος Χ. Παθολογική Φυσιολογία. 737–773 p.
4. Claire R. Hughes , Elim Man and JCA. Brook’s Clinical Pediatric Endocrinology. WileyBlackwell. 2020. 335–407 p.
5. Bhansali A, Gogate Y. Clinical Rounds in Endocrinology [Volume I - Adult Endocrinology]. 2015. 163–185 p.
6. Jain S, Karaviti LP. A 4-year-old Boy with Recurrent Vomiting. Pediatr Rev. 2019;40(8):425–
7.
7. Dina M. Kulik FHM. Poor Feeding and Weight Gain, Tachypnea, and Vomiting in a Neonate. Pediatr Rev. 2011;32(3):123–8.
8. Perl S, Kotz L, Keil M, Patronas NJ, Stratakis CA. Image in endocrinology: Calcified adrenals associated with perinatal adrenal hemorrhage and adrenal insufficiency. J Clin Endocrinol Metab. 2007;92(3):754.
9. Filipa Almeida, Susana Lopes, Margarida Figueiredo, Filipe Oliveira SS, Sequeira and A. Dehydration and Electrolyte Abnormalities in an 11-year-old Boy. Pediatr Rev. 2017;38(9):441–
4.
10. Bizzarri C, Olivini N, Pedicelli S, Marini R, Giannone G, Cambiaso P, et al. Congenital primary adrenal insufficiency and selective aldosterone defects presenting as salt-wasting in infancy: A single center 10-year experience. Ital J Pediatr [Internet]. 2016;42(1):1–8. Available from: http://dx.doi.org/10.1186/s13052-016-0282-3
11. Stapenhorst L. 9Α-Fluorohydrocortisone Therapy in Aldosterone Synthase Deficiency [2]. Pediatr Nephrol. 2005;20(6):839.
12. Lehnhardt A, Kemper MJ. Pathogenesis, diagnosis and management of hyperkalemia. Pediatr Nephrol. 2011;26(3):377–84.
13. Arai K. Aldosterone Deficiency and Resistance Inhibitory agents Defective Stimulation of Aldosterone Secretion Primary Defects in Adrenal Biosynthesis or Secretion of Aldosterone. 2016;2(99):8–9.
14. Auron M, Raissouni N. Adrenal Insufficiency. Pediatr Rev. 2015;36:92–103.
15. Bruno I, Pennesi M, Marchetti F. ACE-inhibitors-induced metabolic acidosis in a child with nephrotic syndrome. Pediatr Nephrol. 2003;18(12):1293–4.
16. Perrin C. White. Abnormalities of aldosterone synthesis and action in children.pdf. Curr Opin Pediatr. 1997;9:424–30.
17. White PC. Aldosterone synthase deficiency and related disorders. Mol Cell Endocrinol. 2004 Mar 31;217(1–2):81–7.
18. Miller WL. Rare defects in adrenal steroidogenesis. Eur J Endocrinol. 2018;179(3):R125–41.
19. Iughetti L, Lucaccioni L, Bruzzi P, Ciancia S, Bigi E, Madeo SF, et al. Isolated
hypoaldosteronism as first sign of X-linked adrenal hypoplasia congenita caused by a novel mutation in NR0B1/DAX-1 gene: A case report. BMC Med Genet. 2019;20(1):1–8.
20. Kanakis G, Kaltsas G. Adrenal Insufficiency Due to X-Linked Adrenoleukodystrophy. Endotext [Internet]. 2000;(3). Available from: http://www.ncbi.nlm.nih.gov/pubmed/25905179
21. Burtman E, Regelmann MO. Endocrine Dysfunction in X-Linked Adrenoleukodystrophy. Endocrinol Metab Clin North Am [Internet]. 2016;45(2):295–309. Available from: http:// dx.doi.org/10.1016/j.ecl.2016.01.003
24. Resende E, Gόmez GN, Nascimento M, Loidi L, Fiaño RS, Rodrίguez PC, et al. Precocious presentation of autoimmune polyglandular syndrome type 2 associated with an AIRE mutation. Hormones. 2015;14(2):312–6.
25. Veldhuis JD, Melby JC. Isolated Aldosterone Deficiency in Man : Acquired and Inborn Errors in the Biosynthesis or Action of Aldosterone *. 2016;2(4):495–517.
26. Üstyol A, Atabek ME, Taylor N, Yeung MCW, Chan AOK. Corticosterone methyl oxidase deficiency type 1 with normokalemia in an infant. JCRPE J Clin Res Pediatr Endocrinol. 2016 Sep 1;8(3):356–9.
27. Riepe FG. Pseudohypoaldosteronism. Horm Resist Hypersensitivity From Genet to Clin Manag. 2013;24:86–95.
28. Sopfe J, Simmons JH. Failure to thrive, hyponatremia, and hyperkalemia in a neonate. Pediatr Ann. 2013 May;42(5):74–9.
29. Zedek S, Medical AH, Med- W. Pulmonary epithelial sodium-channel dysfunction and excess airway liquid in pseudohypoaldosteronism. N Engl J Med. 1999;
30. Brooks AM, Owens M, Sayer JA, Salzmann M, Ellard S, Vaidya B. Pseudohypoaldosteronism type 2 presenting with hypertension and hyperkalaemia due to a novel mutation in the WNK4 gene. Qjm. 2012;105(8):791–4.
31. Furgeson SB, Linas S. Mechanisms of type I and type II pseudohypoaldosteronism. J Am Soc Nephrol. 2010;21(11):1842–5.
32. Luft FC, Wagner CA. Pendred, pendrin, pseudohypoaldosteronism type II, and renal tubular acidosis. Kidney Int [Internet]. 2018;94(3):457–9. Available from: https://doi.org/10.1016/j. kint.2018.05.024
33. Manikam L, Cornes MP, Kalra D, Ford C, Gama R. Transient pseudohypoaldosteronism masquerading as congenital adrenal hyperplasia. Ann Clin Biochem. 2011;48(4):380–2.
34. Al-Mukhaizeem F, Shamsah A, Taher H. Urosepsis simulating congenital adrenal hyperplasia in an infant. Kuwait Med J. 2009;41(3):254–6.
35. Young WF. Etiology, diagnosis, and treatment of hypoaldosteronism (type 4 RTA). UpToDate [Internet]. 2020;1–17. Available from: https://www.uptodate.com/contents/ etiology-diagnosis-and-treatment-of-hypoaldosteronism-type-4-rta
36. Lee BH, Kang HG, Choi Y. Hyporeninemic hypoaldosteronism in a child with chronic kidney disease - Is this condition renoprotective? Pediatr Nephrol. 2009;24(9):1771–2.
37. Nalcacıoglu H, Genc G, Meydan BC, Ozkaya O. Hyperkalaemia in a female patient with systemic lupus erythematosus: answers. Pediatr Nephrol. 2012;27(9):1501–3.
38. Hataya H, Ikeda M, Ide Y, Kobayashi Y, Kuramochi S, Awazu M. Distal tubular dysfunction in lupus nephritis of childhood and adolescence. Pediatr Nephrol. 1999;13(9):846–9.
Τ.
e-mail: gkatsaras@outlook. com.gr
Correspondence
Georgios Katsaras, Vlachernon 16, Kalamaria 55133
Τ. +306939193901
e-mail: gkatsaras@outlook. com.gr
The microbiome in the first years of life and its health impact
Microbiome is a complex interconnected system of microorganisms that live in the human body and is unique to each person, like the fingerprint. It is described as a metabolic "super-organism", consisting of millions microbial genes. The purpose of our review is to investigate the factors affecting the microbiome in childhood, as well as its effect on various systems of the body.
Methods
We conducted literature search in the Pubmed and Scopus databases concerning the microbiome and childhood, its relationship with neuro development, the diseases of the gastrointestinal tract and respiratory system, as well as its role in immunization.
Results
Factors that affect the microbiome in healthy newborns are the mode of delivery, gestational age, feeding, as well as possible hospitalization and exposure to antibiotics. The microbiome directly inhibits the growth of pathogenic microorganisms in the intestine through the production of antibacterial substances. Microbiome strengthens the integrity of the intestine mucosa through the stimulation of epithelial cells and mucus production. In the respiratory system, the growth of Lactobacillus rhamnosus, Bifidobacterium breve or Propionibacterium shermanii and GOS result in fewer respiratory infections. Bifidobacteriaceae and Lactobacillaceae L. Rhamnosus act protectively against allergies, eczema, and asthma. Finally, it has been proven that there is interaction between the gut microbiome and the brain, with possible effect on neurodevelopment.
Conclusions
The impact that microbiome has on our health make it necessary for further research and study with the ultimate goal of understanding how exactly the microbiome affects the previously mentioned systems.
Keywords: microbiome, neonate, infant
Anastasios Vladikas
Evangelos Oikonomou
Georgios Katsaras
Paediatric Department, General Hospital of Pella - Hospital Unit of Edessa, Greece
Georgios Katsaras
2nd Neonatal Department and Neonatal Intensive Care Unit, Aristotle University of Thessaloniki School of Medicine, “Papageorgiou” General Hospital, Greece
Lactobacillus, Prevotella και Sneathia
Staphylococcus, Corynebacterium και Propionibacterium. Escherichia, Shigella και Bacteroides.(10–15)
TLRs: Toll-like receptors
Bifidobacterium.(
1. Fricke WF. The More the Merrier? Reduced Fecal Microbiota Diversity in Preterm Infants Treated with Antibiotics. J Pediatr. 2014;165(1):8–10.
2. Berrington JE, Stewart CJ, Cummings SP, Embleton ND. The neonatal bowel microbiome in health and infection. Curr Opin Infect Dis. 2014;27(3):236–43.
3. Putignani L, Del Chierico F, Petrucca A, Vernocchi P, Dallapiccola B. The human gut microbiota: a dynamic interplay with the host from birth to senescence settled during childhood. Pediatr Res. 2014;76(1):2–10.
4. Palmer C, Bik EM, DiGiulio DB, Relman DA, Brown PO. Development of the Human Infant Intestinal Microbiota. Ruan Y, editor. PLoS Biol. 2007;5(7):e177.
5. Penders J, Thijs C, Vink C, Stelma FF, Snijders B, Kummeling I, et al. Factors Influencing the Composition of the Intestinal Microbiota in Early Infancy. Pediatrics. 2006;118(2):511–21.
6. Adlerberth I, Wold AE. Establishment of the gut microbiota in Western infants. Acta Paediatr. 2009;98(2):229–38.
7. Schwiertz A, Gruhl B, Löbnitz M, Michel P, Radke M, Blaut M. Development of the Intestinal Bacterial Composition in Hospitalized Preterm Infants in Comparison with BreastFed, Full-Term Infants. Pediatr Res. 2003;54(3):393–9.
8. Stinson LF, Boyce MC, Payne MS, Keelan JA. The Not-so-Sterile Womb: Evidence That the Human Fetus Is Exposed to Bacteria Prior to Birth. Front Microbiol. 2019;10.
9. Maynard CL, Elson CO, Hatton RD, Weaver CT. Reciprocal interactions of the intestinal microbiota and immune system. Nature. 2012;489(7415):231–41.
10. Yassour M, Jason E, Hogstrom LJ, Arthur TD, Tripathi S, Siljander H, et al. Strain-Level Analysis of Mother-to-Child Bacterial Transmission during the First Few Months of Life. Cell Host Microbe. 2018;24(1):146--154.e4.
11. Shao Y, Forster SC, Tsaliki E, Vervier K, Strang A, Simpson N, et al. Stunted microbiota and opportunistic pathogen colonization in caesarean-section birth. Nature. 2019;574(7776):117–21.
12. Stewart CJ, Ajami NJ, O’Brien JL, Hutchinson DS, Smith DP, Wong MC, et al. Temporal development of the gut microbiome in early childhood from the TEDDY study. Nature. 2018;562(7728):583–8.
13. Dominguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci. 2010;107(26):11971–5.
14. Lee E, Kim B-J, Kang M-J, Choi KY, Cho H-J, Kim Y, et al. Dynamics of Gut Microbiota According to the Delivery Mode in Healthy Korean Infants. Allergy Asthma Immunol Res. 2016;8(5):471.
15. Azad MB, Konya T, Maughan H, Guttman DS, Field CJ, Chari RS, et al. Gut microbiota of healthy Canadian infants: profiles by mode of delivery and infant diet at 4 months. Can Med Assoc J. 2013;185(5):385–94.
16. Moossavi S, Azad MB. Origins of human milk microbiota: new evidence and arising questions. Gut Microbes. 2020;12(1):1667722.
17. Odamaki T, Bottacini F, Mitsuyama E, Yoshida K, Kato K, Xiao J, et al. Impact of a bathing tradition on shared gut microbes among Japanese families. Sci Rep. 2019;9(1):4380.
18. Korpela K, Costea P, Coelho LP, Kandels-Lewis S, Willemsen G, Boomsma DI, et al. Selective maternal seeding and environment shape the human gut microbiome. Genome Res. 2018;28(4):561–8.
19. Browne HP, Forster SC, Anonye BO, Kumar N, Neville BA, Stares MD, et al. Culturing of ‘unculturable’’ human microbiota reveals novel taxa and extensive sporulation.’ Nature. 2016;533(7604):543–6.
20. McKeen S, Young W, Fraser K, Roy NC, McNabb WC. Glycan Utilisation and Function in the Microbiome of Weaning Infants. Microorganisms. 2019;7(7):190.
21. Liu Y, Qin S, Song Y, Feng Y, Lv N, Xue Y, et al. The Perturbation of Infant Gut Microbiota Caused by Cesarean Delivery Is Partially Restored by Exclusive Breastfeeding. Front Microbiol. 2019;10.
22. Yassour M, Vatanen T, Siljander H, Hämäläinen A-M, Härkönen T, Ryhänen SJ, et al. Natural history of the infant gut microbiome and impact of antibiotic treatment on bacterial strain diversity and stability. Sci Transl Med. 2016;8(343):343ra81--343ra81.
23. Zimmermann P, Curtis N. Effect of intrapartum antibiotics on the intestinal microbiota of infants: a systematic review. Arch Dis Child - Fetal Neonatal Ed. 2020;105(2):201–8.
24. Reyman M, van Houten MA, van Baarle D, Bosch AATM, Man WH, Chu MLJN, et al. Impact of delivery mode-associated gut microbiota dynamics on health in the first year of life. Nat Commun. 2019;10(1):4997.
25. La Rosa PS, Warner BB, Zhou Y, Weinstock GM, Sodergren E, Hall-Moore CM, et al. Patterned progression of bacterial populations in the premature infant gut. Proc Natl Acad Sci. 2014;111(34):12522–7.
26. Grishin A, Papillon S, Bell B, Wang J, Ford HR. The role of the intestinal microbiota in the pathogenesis of necrotizing enterocolitis. Semin Pediatr Surg. 2013;22(2):69–75.
27. Thompson-Branch AM, Havranek T. Influences of Feeding on Necrotizing Enterocolitis. Neoreviews. 2018;19(11):e664--e674.
28. Welsh KM, Bondi DS, Frost B. Probiotics for the Prevention of Necrotizing Enterocolitis in Preterm Neonates. Neoreviews. 2016;17(7):e377--e385.
29. Panigrahi P, Parida S, Nanda NC, Satpathy R, Pradhan L, Chandel DS, et al. A randomized synbiotic trial to prevent sepsis among infants in rural India. Nature. 2017;548(7668):407–12.
30. Biesbroek G, Tsivtsivadze E, Sanders EAM, Montijn R, Veenhoven RH, Keijser BJF, et al. Early Respiratory Microbiota Composition Determines Bacterial Succession Patterns and Respiratory Health in Children. Am J Respir Crit Care Med. 2014;190(11):1283–92.
31. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bønnelykke K, et al. Childhood Asthma after Bacterial Colonization of the Airway in Neonates. N Engl J Med. 2007;357(15):1487–95.
32. Blanken MO, Rovers MM, Molenaar JM, Winkler-Seinstra PL, Meijer A, Kimpen JLL, et al. Respiratory Syncytial Virus and Recurrent Wheeze in Healthy Preterm Infants. N Engl J Med. 2013;368(19):1791–9.
33. Arrieta M-C, Stiemsma LT, Dimitriu PA, Thorson L, Russell S, Yurist-Doutsch S, et al. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci Transl Med. 2015;7(307):307ra152--307ra152.
34. Zimmermann P, Messina N, Mohn WW, Finlay BB, Curtis N. Association between the intestinal microbiota and allergic sensitization, eczema, and asthma: A systematic review. J Allergy Clin Immunol. 2019;143(2):467–85.
35. Borre YE, O’Keeffe GW, Clarke G, Stanton C, Dinan TG, Cryan JF. Microbiota and neurodevelopmental windows: implications for brain disorders. Trends Mol Med. 2014;20(9):509–18.
36. Smolarova S, Kocvarova L, Matasova K, Zibolen M, Calkovska A. Impact of Updated European Consensus Guidelines on the Management of Neonatal Respiratory Distress Syndrome on Clinical Outcome of Preterm Infants. In: Advs Exp Medicine, Biology-Neuroscience and respiration. 2014. p. 61–6.
37. O’Hara AM, Shanahan F. The gut flora as a forgotten organ. EMBO Rep. 2006;7(7):688–93.
38. Sudo N, Chida Y, Aiba Y, Sonoda J, Oyama N, Yu X-N, et al. Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. J Physiol. 2004;558(1):263–75.
39. Barouei J, Moussavi M, Hodgson DM. Effect of Maternal Probiotic Intervention on HPA Axis, Immunity and Gut Microbiota in a Rat Model of Irritable Bowel Syndrome. Heimesaat MM, editor. PLoS One. 2012;7(10):e46051.
40. Takeuchi O, Akira S. Pattern Recognition Receptors and Inflammation. Cell. 2010;140(6):805–20.
like receptor responses in psychosis: further evidence of a pro-inflammatory phenotype. Transl Psychiatry. 2011;1(8):e36--e36.
42. O’Brien SM, Scott L V, Dinan TG. Cytokines: abnormalities in major depression and implications for pharmacological treatment. Hum Psychopharmacol Clin Exp. 2004;19(6):397–403.
43. Manicassamy S, Reizis B, Ravindran R, Nakaya H, Salazar-Gonzalez RM, Wang Y, et al. Activation of Catenin in Dendritic Cells Regulates Immunity Versus Tolerance in the Intestine. Science. 2010;329(5993):849–53.
44. Smith PA. The tantalizing links between gut microbes and the brain. Nature. 2015;526(7573):312–4.
45. Pärtty A, Kalliomäki M, Wacklin P, Salminen S, Isolauri E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: a randomized trial. Pediatr Res. 2015;77(6):823–8.
e-mail: tsergent@med.uoa.gr
Correspondence
Theodoros N. Sergentanis
Mesogeion 24, 11527
Athens T. +302107710824
e-mail: tsergent@med.uoa.gr
A brief review of school dropout rates in Greece
Aikaterini Karavela, Gerasimos Mesiris, Theodoros N. Sergentanis, Artemis Tsitsika
Abstract
Background: School Dropout is a multifactorial educational problem on a global scale. It is inextricably linked to the exclusion of socially vulnerable groups of the population and is a major target of strategies applied in educational policy. The purpose of this review is to examine the situation in Greece, making a rough comparison with other European countries and internationally, to investigate the causes and consequences of the phenomenon, as well as the measures to be taken.
Methods: Information was sought in international, European and Greek bibliographical and statistical databases and the "avalanche procedure" was followed during the review.
Results: Our survey found that in Greece early school dropout rate reached 7.9% in 2015, below the EU average of 11% in the same year. The European Union aspires to reduce the prevalence of the phenomenon by 2020 at less than 10%.
Conclusions: Policies and response measures are organized to eliminate school dropout, both at the school context and at the society in general. Interconnecting the local community with schools, reinforcing training units with qualified staff, educating and informing leavers about reintegration and retraining are essential strategies.
Key words: School dropout, Individuals Not in Education, Employment or Training (NEETs)
Aikaterini Karavela
Gerasimos Mesiris
Theodoros N. Sergentanis
Artemis Tsitsika
Postgraduate Programme
“Strategies of Developmental and Adolescent Health”, Medical School, National and Kapodistrian University of Athens
Aikaterini Karavela
Community Center of Chalandri
Gerasimos Mesiris
Committee for Diagnostic
Educational Evaluation and Support based in Special Primary School of Atalanti of Fthiotida
Early School Leaving),
(ΠΕΕΚ - ELET - Early Leaving from Education and Training), “σχολική διαρροή” (school dropout) ή “μαθητική διαρροή” (students dropout), διακοπτόμενη
(interrupted learning), καθώς και
(ΕΕΑΚ - NEET - Not in Education, Employment or Training) (5).
1. ΟΕCD. (2016). Education at a Glance 2016: ΟΕCD Indicators. Paris: ΟΕCD Publishing.
(Bλ.
2. Mouzelis, N. (1998). Multi-cultural Europe: conceptualizing complexity on the sociocultural and educational levels. Στο A. Μ. Kazamias & M. G. Spillan (eds). Education and the Structuring of the European Space. Athens: Sirios
Απόντων: Οι ΝΕΕΤs (Young People Not in Education, Employment or Training) στην
1999)
7. Out-of-School Children and Youth στο: http://uis.unesco.org/en/topic/out-school-childrenand-youth
8. European Commission/Directorate General for Education and Culture. (2002). Education and Training in Europe: diverse systems, shared goals for 2010. The Work Programme on the future objectives of education and training systems. Brussels: European Commission.
9. Eurostat, Smarter, greener, more inclusive? - Indicators to support the Europe 2020 strategy, Publications Office of the European Union, Luxembourg
10. “Παρακολούθηση
(2015), op.cit.
(2015)
11. Decrease in “early school leavers” in the EU continues, Webpage: https://ec.europa.eu/ eurostat/web/products-eurostat-news/-/EDN-20170908-1
12. Cedefop (2018). How many young people leave education and training too early? Indicator 3010: early leavers from education and training, (2017 update) In: Cedefop. Statistics and indicators: Statistics and graphs. Webpage: http://www.cedefop.europa.eu/en/publications-andresources/statistics-and-indicators/statistics-and-graphs/28-how-many-youngpeople
Διαρροής ΙΕΠ
15. De Witte, K., Cabus, S., Thyssen, G., Groot, W. & Van den Brink, H. M. (2013). A critical review of the literature on school dropout. Educational Research Review 10, 13–28 και Fortin, L., Royer, É., Potvin, P, Marcotte, D. & Yergeau, É. (2004). La prédiction du risque de décrochage scolaire au secondaire: facteurs personnels, familiaux et scolaires. Revue canadienne des sciences du comportement, 36 (3), 219-231
16. Εθνικό
(Επιμ.). (2014).
Παπαζήσης
17. Guigue, Μ. (2013). Les déchirements des institutions éducatives. Jeux d'acteurs face au décrochage scolaire. Paris: L'Harmattan
18. Ενδεικτικά
19. European Cοmmission/EACEA/Eurydice/Cedefop. (2014). Tackling Early Leaving from Education and Training in Europe. Strategies, Policies and Measures. Eurydice and Cedefop Report. Luxembourg: Publications Office of the European Union 20. Unesco. (2015). Rethinking Education. Towards a global common good? Paris: Unesco 21. Έκθεση
3.- Ιπποκράτης, Jacques Jouanna (μτφρ. Δ. Τσιλιβέρδης), εκδ. Ινστιτούτο του βιβλίου Α. Καρδαμίτσα.
4.- Kurt Pollak (μτφρ. Α. Μαυρουδής), Η ιατρική στην αρχαιότητα, εκδ. Παπαδήμα
5.- Kenneth Walker, Histoire de la Médecine, εκδ. marabout Université, 19626.
6.- Iστορία της Ιατρικής Storia della medicina), τ. 1-4, (έκδοση Εταιρείας Εγκυκλοπαιδικών Εκδόσεων - Παπύρου,1968)
7.- Antje Krug (μτφρ. Ε. Μανακίδου, Θ. Σαρτζής), Αρχαία Ιατρική - Επιστημονική και θρησκευτική ιατρική στην αρχαιότητα, εκδ. Παπαδήμα.
8.- Helen King (μτφρ. Α. Γρηγοριάδου), Ελληνική και Ρωμαϊκή Ιατρική, εκδ. Ενάλιος.
9.- UNESCO: Ιστορία της Ανθρωπότητος, εκδ. Τεγόπουλος- Νίκας, Αθήναι
10.- Π. Πεφάνη, Συνοπτική ιστορία της ιατρικής, εκδ. Εξάντας
11.- Μεγάλη Ελληνική Εγκυκλοπαίδεια
Division of Neonatology, Drexel University College of Medicine. Όλα
Department of Health, Education and Welfare, Bureau of Community Environmental Management (1972-1982)
“American Academy of Pediatrics Lifetime Achievement Award” (1995),
Apgar” (1997),
“National Lifetime Achievement Award from the Castle Connolly Ltd” (2007)
(“Legends in Neonatology”).
University of Nancy,
(1996),
(2010).
2.
3.
4.
5.
6.
7.
8.
9. Ενδιαφέρουσες
10. Σύντομα
11. Βραχείες
12.
13.
14.
(Uniform Requirements for Manuscripts Submitted to Biomedical Journals),
International Committee of Medical Journal Editors/Uniform Requirements for Manuscripts Submitted to Biomedical Journals, (www.icmje.org και www.icmje.org/icmje. pdf).
Cumulated Index Medicus [List of Journals Indexed in Index Medicus (www.nlm.nih.goν/bsd/uniform_requirements.html)].
1999;59:272-279.
Proesmans W. Bartter syndrome and its neonatal νariant. Eur J Pediatr 1997;156:669-679.
Flyvbjerg Α. Role of growth hormone, insulin-like growth factors (IGFs) and IGF-binding proteins in the renal complications of diabetes. Kidney Ιnt 1997;52 (60 Suppl):S12-S19.
Χωρίς συγγραφέα:
National Institutes of Health Consensus Deνelopment Conference. Neurofibromatosis conference statement. Arch Neurol1988;45:575-578.
Προσδιορισμός τύπου άρθρου: Schreiner GF, Lange L. Ethanol modulation of macrophage influx in glomerulonephritis [Abstract]. J Am Soc Nephrol 1991;2:562.
Should antileukotriene therapies be used instead of inhaled corticosteroids in asthma? [Editorial]. Am J Respir Crit Care Med 1998;158:1697-1701.
Clark AG, Barratt ΤΜ. Steroid-responsiνe nephrotic syndrome. Ιn: Barratt ΤΜ, Arner ED, Harmon WE, editors. Pediatric Nephrology. 4th ed. Baltimore: Lippincott William Wilkins; 1999. p. 742.
Σύγγραμμα
Gorlin RJ, Cohen ΜΜ, Leνin LS. Syndromes of the head and neck. 3rd ed. New York: Oxford Uniνersity Press; 1990.
Δημοσίευση
Bauer ΑW. The two definitions of bacterial resistance. In: Smith AJ, Rogers CA, eds. Proceedings of the Third International Congress of Chemotherapy; 1962 May 29-31; New York: International Society of Chemotherapy; 1963. p. 484-500.
Διδακτορική
Αθηνών; 1979.
Kaplan SJ. Post hospital home health care: the elderly’s access and utilization [dissertation]. St. Louis (Μο): Washington Univ.;1995.
III. CD-ROM
Andersoη SC, Poulsen ΚΒ. Anderson’s electronic atlas of hematology [CD-ROM]. Philadelphia: Lippincott Williams & Wilkins; 2002.
IV. ΣΤΟ
Abood S. Quality improνement initiatiνe in nursiηg homes: the ΑΝΑ acts in an adνisory role. Am J Nurs [Internet]. 2002 Jun: