BUILDING, STRENGTHENING, INNOVATING

Christine M. Collins, MBA, RPh, FASHP
Senior Vice President, Pharmacy and Perioperative Services, Brown University Health

Building, strengthening, innovating: that is what comes to mind as I look across the accomplishments highlighted in this year’s annual report. We advanced our services not because we must, but because we know that they can be stronger. We leaned into opportunities not because someone asked, but because we understand the impact we can have. We elevated quality, safety, and innovation because of who we are—not what the moment demands.
We have responded to the opportunities before us with this collective mindset. It has shaped a culture of forward movement across our pharmacy enterprise, and it continues to propel us toward continued excellence. Throughout the year, our work strengthened every facet of our health system—from inpatient care to clinical programs, medication use safety and strategy, ambulatory services, informatics, business operations, research, residency and academics, and beyond.
The breadth of what we achieved is remarkable, but what stands out most is the intention behind it: a shared commitment to doing the right things for the right reasons, in the right way. This is what distinguishes Brown University Health Pharmacy Services, and it is why we continue to be recognized as leaders in our field.
We welcomed many new colleagues this year, including team members from Morton Hospital and Saint Anne’s Hospital. Their expertise and enthusiasm have already enriched our department, and it has been inspiring to watch teams in Rhode Island and Massachusetts come together with such collaboration and purpose. The speed of medication-related integration, not to mention the highly successful big-bang implementation of information systems and automation, could never have happened without the foundation of a highly collaborative team. We are truly stronger as a team with our combined pharmacy family.
As we look to the year ahead, there is much to anticipate—major strategic initiatives, expanding programs, continued innovation in technology and analytics, and new opportunities to enhance the patient experience across all care settings. Our foundation is strong, and our direction is clear. I have full confidence that we will continue to build, strengthen and innovate. In doing so, we will advance pharmacy practice and drive meaningful improvements for our patients and the communities we serve.
My sincere thanks to every member of the department. Please take a moment to reflect on your contributions to this past year’s success, and consider the many ways you will help shape the year ahead. Let’s continue to build, strengthen, and innovate—because we understand the impact we can have.

Christine M. Collins, MBA, RPh, FASHP
Mission
To enrich our community’s health by providing exceptional and innovative pharmacy services.
Vision
To transform pharmaceutical care through innovation and adherence to the highest clinical standards.
Values
Compassion Delivering medications to patients with care and empathy.
Excellence Providing our patients with the safest, highest quality of care possible, continually improving our systems, and measuring our performance.
Innovation Committed to pursuing contemporary medication practices and engaging all pharmacy team members to be innovative thinkers.
Integrity Ensuring accountability and respect while adhering to the highest standards of morals and ethics.
Teamwork Working collaboratively across pharmacy services and with multidisciplinary care teams.
Click here to visit brownhealth.org/centers-services/pharmacy











Lifespan, the forerunner of Brown University Health, was Rhode Island's first health system, founded in 1994 by Rhode Island Hospital and The Miriam Hospital. A comprehensive, integrated, academic health system affiliated with The Warren Alpert Medical School of Brown University, Brown Health’s current partners also include Rhode Island Hospital’s pediatric division, Hasbro Children’s; Bradley Hospital, Newport Hospital, Morton Hospital, Saint Anne’s Hospital, Gateway Healthcare and the multispecialty Brown Health Medical Group. Pharmacy Services are well integrated into these partners.
377 Pharmacists
26 Pharmacists with advanced degrees (e.g., MBA, MPH, JD)
107 Pharmacists who are board-certified
12 Pharmacists who are dual board-certified
56 Pharmacists who have completed a PGY1 residency
47 Pharmacists who have completed both PGY1 and PGY2 residencies
279 Technicians
19 Pharmacy residents
9 Residency programs
72% Percentage of residents who stayed with Brown Health after completing residency
Our Hospitals
20,014 Employees 1,473 Licensed beds
Scholarship & Research
119 APPE/IPPE rotations completed
Inpatient Pharmacy Services
Central Pharmacy Services
98 Inpatient units with pharmacy support system wide
8,919,417 Doses dispensed
153,271 Compounded sterile products prepared
Ambulatory Pharmacy Services
72,895 Unique ambulatory patients
88 Clinics with ambulatory pharmacy support
Medication Policy & Safety
~40%
2
Percentage of staff-reported medication-related safety events that were “good catch” prevented errors, signaling a strong culture of reporting
Medication safety topics submitted to Institute for Safe Medication Practices (ISMP) that were published in nationwide Medication Safety Alert
>95% Medication barcode scanning rates (Leapfrogdefined units)
>98% Smart-pump infusion drug library compliance with Epic interoperability
Investigational Drug Services
187 Active protocols
3,449 Active dispenses
Pharmacy Technology Team
>1,000,400
Controlled substance transactions evaluated, resulting in 97% automated closure rate by diversion detection software, limiting need for manual review of transactions
140 Epic system improvements/ maintenance requests completed per month
Overview
The inpatient pharmacy team at Brown University Health plays a vital role in advancing safe, effective, and efficient medication use across the multi-hospital system. During the past year, the team strengthened clinical and operational services through standardized medication-use policies, enhanced EMR-based clinical decision support, and expanded pharmacist-led initiatives that improved safety and outcomes. Operational advances in automation and inventory optimization reinforced resilience and regulatory readiness. Collectively, these efforts reflect our commitment to delivering innovative, patient-centered medication management and positioning Brown University Health as a model for integrated inpatient pharmacy services.
Key Accomplishments (Year in Review)
• Renovated the entire inpatient pharmacy space to meet modern standards for medication storage, handling, compounding, and dispensing.
• Implemented Omnicell carousel automation to provide real-time inventory oversight, improved operational efficiency, and increased medication availability on inpatient units.
• Implemented 7-on/7-off schedule for secondshift clinical pharmacists and improved worklife balance.
• Implemented Adult and Pediatric Emergency Department medication-delivery batching process, improving just-in-time medication availability.
Plans for the Year Ahead
• Expanding dispense-tracking technology to include receipt of medication delivery on patient care units.
• Engagement with anesthesia personnel on several initiatives to improve medication management in perioperative areas.
• Incorporation of new Rhode Island Tech-CheckTech legislation into inpatient operations workflows, providing expanded opportunities for technicians and increasing pharmacists’ capacity to implement clinical interventions.
• Collaborating with high school Career and Technical Education (CTE) Directors across the state to implement a new Allied Health CTE program with a specific track for pharmacy technicians to increase the pharmacy technician workforce.

• Successfully implemented pharmacy-led discharge medication reconciliation program, exceeding the projected 50 percent capture of all discharges and bringing pharmacist review to higher-risk discharges and preventing errors at transition.
• Launched an ASHP/ACPE accreditation-ready, 11-week, PTU-backed technician training program at TMH and placed the first graduates into permanent roles, establishing a scalable pipeline for hiring and certification of Pharmacy Technician and Medication History Technicians.
• Reduced disruptions and optimized central pharmacy workflow by implementing a dedicated phone tree. Call routing now prioritizes emergencies, directs controlled-substance questions to the correct line, and diverts clinical inquiries to secure chat, minimizing interruptions to dispensing/verification and shortening response loops for urgent needs.
• Boosted pharmacist engagement by implementing 10-hour shifts. The schedule redesign improved work-life balance and midday coverage while driving a Clinical Pharmacist engagement score increase from 74.4 to 91.7 percent, reflecting stronger satisfaction and retention potential.
Plans for the Year Ahead
• Pilot and scale a 10-hour workweek for technicians.
• Implement Tech-Check-Tech (TCT) into the operations workflow.
• Expand ED coverage and charge coverage to the weekends.
• Implement a DSCSA-compliant workflow for inpatient and EMS medications.
• Expand our antimicrobial stewardship services.

Pharmacy services at Newport Hospital are provided by a dynamic team of 24 pharmacists and technicians dedicated to ensuring accuracy, efficiency, and clinical excellence. Fiscal year 2025 was distinguished by a focus on expanding patient-care opportunities and improving inventory management.
Key Accomplishments (Year in Review)
• Achieved pharmacist clinical list patient capture rate exceeding 95 percent.
• Implemented pharmacist-to-dose vancomycin protocol.
• Achieved Medication History Technician patient capture rate exceeding 88 percent.
Plans
• Data-driven Omnicell PAR level optimization throughout the facility to enhance in-stock position and technician workflow.
• Support the implementation of an inpatient Adolescent Behavioral Health unit.

• Completed a successful survey by The Joint Commission.
• Performed medication reconciliation for Bradley residential program clients.
Plans
• Implement new workflow to ensure full compliance with Drug Supply Chain Security Act requirements.
The Antimicrobial Stewardship Program is successfully monitoring and reporting on infections, antimicrobial use and resistance data.
The Centers for Disease Control’s (CDC) National Healthcare Safety Network (NHSN) is a surveillance system for healthcare-associated infections (HAI), antimicrobial use and resistance data (AUR). Reporting validated AUR data is a requirement of the Center for Medicare and Medicaid Services (CMS) Medicare Promoting Interoperability Program; failure to comply will result in financial penalty beginning in 2026.
The antimicrobial stewardship and pharmacy IT teams have completed the internal validation of antimicrobial use (AU) data for Rhode Island Hospital, The Miriam Hospital, and Newport Hospital. AU data is now being submitted to NHSN on an ongoing basis after several years of effort by the Antimicrobial Stewardship Program. This data will be used to monitor antimicrobial use and identify opportunities for improvement at our hospitals, and to benchmark against peer hospitals.
Pharmacy Services at Saint Anne’s has entered a new chapter under the leadership of Brown University Health. After a challenging period during Steward Health Care’s financial difficulties, the transition has brought renewed stability, strategic direction, and a commitment to excellence. Despite obstacles, the team has demonstrated remarkable resilience and dedication by successfully completing two major system transitions, along with numerous other system/process changes.
Key Accomplishments (Year in Review)
• Migrated from Meditech to Epic, enhancing clinical workflows, interoperability, and patient care.
• Transitioned from Pyxis to Omnicell, improving safety, inventory control, and operational efficiency.
• Complete conversion of the drug pump library to the Brown Health system formulary and protocol changes.
• Teams adapted quickly, embracing new technologies and workflows with professionalism and dedication.
• Despite the challenges, we maintained high standards of patient care and safety throughout the transition.
Plans
• Create a new clinical program accepting IPPE and APPE students from local universities.
• Improve and broaden the medication history technician program.
• Develop staff expertise in all clinical areas within Epic and expand clinical pharmacy services.
• Add a retail pharmacy space at Saint Anne’s.

Key Accomplishments (Year in Review)
• Expanded collaborative clinical services via new ICU and AMS rounding services, warfarin dosing protocol and onboarding of a clinical specialist/coordinator and two new Medication History Technicians.
• Successfully completed The Joint Commission survey and accreditation under the new health system.
• Aligned with Brown Health’s system-wide P&T Committee, Safety Committee, AMS, Oncology and various other subcommittees.
• Converted from Pyxis to Omnicell automated dispensing cabinets, improving medication safety and inventory control.
• Successfully implemented standardized infusion pump libraries across the system.
• Integrated into Brown Health’s enterprise-wide Epic EMR system, enhancing clinical documentation and interoperability.
• Optimized formularies in alignment with Brown University Health to ensure optimal care.
Plans for the Year Ahead
• Continue optimization of Epic workflows and clinical decision support tools.
• Advance staff development and training to align with Brown Health’s clinical excellence standards.
• Provide learning opportunities to IPPE and APPE students.
• Expand clinical pharmacy services with a retail pharmacy and explore “Meds to Beds” program.
• Implementation of KitCheck.

Overview
This past year, our Clinical Pharmacy Services team has been an indispensable partner in delivering highquality, patient-centered care across the health system. Our team of specialized pharmacists is deeply embedded within multidisciplinary care teams, which champion a philosophy that is outcomes-driven, innovative, and collaborative. We are focused on delivering measurable improvements in both clinical efficacy and operational efficiency, ensuring every patient receives the safest and most effective medication therapy.
Key Accomplishments (Year in Review)
• Implementation of pharmacy-to-dose vancomycin
° Pharmacists have managed the dosing, ordering, and assessment of serum concentration for 85 percent of patients across the system, resulting in a 21 percent reduction in the number of serum concentrations collected per 24 hours of vancomycin exposure without an increase in the incidence of vancomycin-associated acute kidney injury.
• Implementation of a nurse-driven electrolyte repletion protocol
° A pharmacy-led initiative to create an order set and Epic workflow to facilitate protocolized repletion of electrolytes in ICU and step-down patients resulted in a 27 percent reduction in administrations for electrolytes and a 13 percent reduction in the number of orders for electrolytes.
• Creation and implementation of an ICU continuous insulin infusion calculator and protocol
° An EMR-integrated protocol and calculator for insulin infusions in critically ill patients resulted in a 54 percent reduction in incidence of severe hypoglycemia and a 44 percent reduction in incidence of hypoglycemia.
• Implementation of an inhaler-to-nebulizer interchange
° A therapeutic interchange from delivery of inhaled medications via inhaler to a nebulizer resulted in an 87 percent reduction in the average daily missing medication requests for inhaled medications.
• The implementation of a closed formulary where providers are only able to order medications that are on the formulary will maintain fiscal responsibility for cost-effective medications, standardize prescribing practices, enhance expertise in formulary medications, and simplify and streamline purchasing, dispensation, and inventory control processes
• Completed extensive internal validation of antimicrobial use (AU) data for Rhode Island Hospital, The Miriam Hospital, and Newport Hospital, which is now being submitted to the National Healthcare Safety Network (NHSN) on an ongoing basis.
• Cost Savings Initiatives
° Long-Acting Injectable Antipsychotic Replacement Program saved $543,881.
° Heparin Concentration Change is projected to save more than $97,000 annually.
° Levetiracetam IV push transition for adult loading doses is projected to save more than $25,000 annually.
° Argatroban to bivalirudin nurse-driven MAR calculator transition is projected to save more than $20,000 annually.
Plans for the Year Ahead
• Implementation of a standardized multidisciplinary ABCDEF bundle for mechanically-ventilated patients.
• Implementation of a new, standardized, system-wide, nurse-driven protocol for diabetic ketoacidosis.
• Implementation of a new protocol for the treatment of alcohol withdrawal.
• Implementation of a pharmacist-driven protocol for automatic renal dosing adjustments.
• Implementation of a pharmacy-to-dose aminoglycoside protocol and program.
The successful conversion from use of inhalers to nebulizers throughout Brown University Health has resulted in operational efficiency, a reduction in waste and an initial annual drug cost saving of more than $423,000. Patients appreciate the quick relief that nebulized medication delivers.
Whether the patient has asthma, chronic obstructive pulmonary disease (COPD) or another respiratory condition, the vast majority use an inhaler at home, which they bring when they are admitted. “Some inhalers deliver up to 200 puffs and can consist of a combination of medications,” explains Shawn Whitehead, PharmD, BCCCP, Manager, Inpatient Clinical Pharmacy, at Rhode Island Hospital. “Most of those puffs are wasted when the patient moves to a different unit, and the inhaler goes missing, or heads home. We might dispense multiple inhalers for one patient.” Inhalers must be ordered from the main pharmacy, so there is often a wait.
The transition to dispensing nebulized medication required thoughtful planning. “We built the system so that it’s clear to a provider how to convert what the patient is using at home to the combination of nebules—the pre-filled dose—they will receive in the hospital,” says Whitehead. “They can order it easily by selecting the right combination of medications.”
The nebules, in various dosages, are kept in each unit’s Omnicell. “That makes it easy for the nurse to grab the nebule, drop it into a nebulizer cup and hook it up to the wall oxygen so that the handheld device administers that medication to the patient.” The time required to nebulize the medication has gone from 12 minutes to three minutes with a new nebulizer device brought in to facilitate this initiative.
“From a nurse’s standpoint, those minutes are valuable because we have so many things going on,” says Shannon Moran, RN, a nurse at RIH. She adds that the new system is working well, and patients appreciate it.
“ Those with COPD get greater relief with the nebulizer. Someone with a bad cough benefits from having humidity added to their treatment; they cough up more phlegm because the nebulizer helps their airways to open up. Patients often ask us: ‘Can I get this at home?’”
They can, says Whitehead, if they want to purchase a home nebulizer. “Most patients return to using an inhaler, which is easier to use and more portable.”
Back at the hospital, Moran and her colleagues are struck by the huge waste problem that has been solved. “We used to throw all these inhalers away,” she says. “Now that we provide nebulized medication, it’s one and done.”
Key Accomplishments (Year in Review)
• Discharge Medication Reconciliation Program
° This pilot program, established in March 2025, includes dedicated pharmacists at both RIH and TMH—along with trained decentralized pharmacists—who review adult weekday discharges to identify and address medication safety issues and optimize transitions of care and medication access/affordability.
° Rhode Island Hospital pharmacists have reviewed 38.2 percent of applicable discharges with an error capture rate of 21.2 percent. The Miriam Hospital pharmacists have reviewed 45.9 percent of applicable discharges with an error capture rate of 27.4 percent.
» Notable error trends have been identified, and various stakeholders across professions have been engaged to discuss opportunities for improvement.
Plans for the Year Ahead
• Building a risk stratification tool to identify those patients with the greatest need for review of their discharge medication list.
• Collaborating with pharmacy and non-pharmacy services to enhance transitions of care.
• Collecting and presenting data on trends and patterns regarding errors caught to implement systematic improvements for change.

Key Accomplishments (Year in Review)
• Lecture hours
° There were 83 different lectures delivered during the course of 176 hours—JWU: 110 hours; RIC: 48 hours.
° Courses included: Pharmacogenomics and Drug Administration and Informatics at URI College of Pharmacy; a microbiology and antimicrobial course for aspiring medical technologists at Our Lady of Fatima School of Medical Technology; and a Healthcare Finance course at the Massachusetts College of Pharmacy and Health Sciences.
• APPE and IPPE students
° Rhode Island Hospital, 25 APPE students, 8 IPPE students
° The Miriam Hospital, 12 APPE students, 6 IPPE students
° Newport Hospital, 1 APPE student, 5 IPPE students
° Bradley Hospital, 3 IPPE students
° Brown Health Medical Group Primary Care, 9 APPE students
• Longitudinal APPE student projects
° Assessment of an Inhaler to Nebulizer Therapeutic Interchange at a Large Academic Medical Center
° Evaluation of Substance Use and Central Nervous System Adverse Effects in Patients with Human Immunodeficiency Virus Taking Efavirenz
° Comparison of Clinical Outcomes in Subtherapeutic vs. Therapeutic Anticoagulation Goals in Patients Requiring ECMO
° Evaluation of Autoverification Overhaul at a Regional Tertiary Pediatric Emergency Department
° Practices Surrounding P2Y12 Inhibitor Prescribing in Cardiovascular and Neurovascular Populations Regarding the CYP2C19 Genotype and P2Y12 Reactivity Unit Results
° Incentivizing Pharmacist Advancement Through Board Certification: A Prospective Cohort Study of Organizations Across the United States
• Longitudinal APPE future
° Six of the seven Longitudinal APPE students went on to PGY1 programs at Brown Health Medical Group/University of Rhode Island and at other institutions.
° PGY1/2 Health Systems Administration Pharmacy Residency, Brown University Health Rhode Island Hospital
Plans for the Year Ahead
• Leverage RIH institutional rotation to develop discharge counseling program for patients started on high-risk medications in the hospital or patients newly diagnosed with diabetes.
Overview
During the past year, standardizing practices and drug accountability has been a major area of focus; ongoing work with an investigational software provider has led to substantial updates to our SOPs. Revised trial service fees have gone into effect, and we are better aligned with other investigational pharmacies in the northeast region.
Key
We have taken measures to enhance communication and clinical trial patient safety by:
• Adding MAR comment, including physical descriptions for investigational oral drugs (i.e., round, light blue scored tablet). This allows nursing to confirm they are providing patients with the correct medication, which is especially important when the patient brings in their home medication for in-clinic and inpatient dosing.
• Compiling a list of contraindicated medications for each investigational drug built in Epic. If a provider orders a prohibited medication, a best practice alert fires and provides contact information for the research team.
During fiscal year 2025, IDS:
• Set up 70 new protocols and treated 360 patients, resulting in 4,335 dispenses.
• Produced 150 investigational treatment plans.
• Created 181 simple and 61 mixture eRx’s (242 total).
• Received 1,050 shipments and transferred 1,285 products to satellite sites.
Plans for the Year Ahead
• Focus on collaboration with our Epic team to standardize investigational drug builds, most notably for blinded drugs or builds that involve serial dilutions or complex compounding.
• Utilize new, custom IDS-specific IVents for documentation and metric tracking purposes.
• Host nursing in-services when a new trial opens and involves inpatient admission, providing support and knowledge to improve confidence in administering unfamiliar medications.
• Strengthen relationships with other investigational pharmacists in the region, sharing information to facilitate growth.
Key Accomplishments (Year in Review)
• Oncology APC3 Renovations included replacing outdated double compounding aseptic containment isolators with two new biological safety cabinets, completing RIH central cleanroom renovations, building a neutral pharmacy area and a new segregated compounding area with compounding aseptic isolator, and moving the main entrance door to the cleanroom into the pharmacy.
• Opened Foxboro Oncology/Infusion center and received Mass Sterile Compounding license.
• Successfully implemented Epic IV workflow at Massachusetts hospitals and infusion/oncology centers.
• Treated first patient with hemophilia B in Rhode Island with Hemgenix gene therapy.
• Implemented the Drug Supply Chain Security Act for the Brown Health Cancer Institute pharmacy sites.
• Transitioned to Pharmacy Stars management system for compliance software and standardized compounding competencies and tasks throughout BUH.
• Completed successful Cancer Oversight Committee Survey in March 2025.
• Batched Compounded Sterile Products (CSPs)
° Newport Hospital – 7,416
° The Miriam Hospital – 24,364
° Rhode Island Hospital – 47,114
• Brown University Health Cancer Institute CSPs
° RIH Cancer Institute Pharmacy – 29,024
° Lincoln Cancer Institute Pharmacy – 11,532
° Newport Cancer Institute Pharmacy – 4,887
° EG Cancer Institute Pharmacy – 7,701
° Fain Cancer Institute Pharmacy – 21,233
Plans for the Year Ahead
• Renovations to Morton Inpatient Pharmacy Compounding Suite.
• Expand CAR-T cell therapy as needed.

Today, progress in treating cancer means directing the immune system to detect and destroy cancer cells. CAR T-cell therapy represents a giant leap in that progress. In September 2025, the first Brown University Health patient was treated with CAR T-cell therapy.
Launching the program required extensive multidisciplinary planning and preparation. “I would say it was two years in the making,” says Justin Huynh, PharmD, BCOP, Clinical Pharmacy Specialist, Hematology and Oncology. “Pharmacy helped develop the standard operating procedures. How do we safely administer this therapy, what are its unique side effects, and what does obtaining accreditation entail?”
The decision was made to work with Bristol Myers Squibb, which has products for multiple myeloma and nonHodgkins lymphoma. “We held onboarding sessions with company representatives and proceeded to develop detailed protocols and electronic order sets,” explains Hannah Kisla, PharmD, BCOP, Clinical Pharmacy Specialist, Hematology and Oncology. “This helped in managing the unique toxicities associated with CAR T-cell therapy—notably cytokine release syndrome and neurotoxicity syndrome.”
“ We’re the only center in Rhode Island providing CAR T-cell therapy. Now patients don’t have to travel to Boston.”
These inflammatory responses can occur when the patient’s immune system cells have been reprogrammed to attack their cancer cells. “CAR T-cell therapy expresses a chimeric antigen receptor or CAR, so that the patient’s T-cells target cancer cells.”
There is an important step prior to the patient receiving CAR T-cell therapy. “This is the lymphodepletion regimen—chemotherapy—used to wipe out any cancer cells in the body,” says Huynh. “Then the CAR T-cells are infused.” Patients spend approximately two weeks in the hospital so they can be closely monitored.
Selection of the first patient was an important step. “An entire team of people was consulted; the pharmacy team worked on the standard procedure for this,” notes Huynh. “Our first patient, who had lymphoma, didn’t have a single side effect. He felt fine.”
“With lymphoma, we hope the treatment is curative,” Kisla says. “For myeloma, we hope to extend the time of remission post-CAR T-cell therapy. There’s discussion about CAR T-cell therapy becoming outpatient in the future, and we know that this novel treatment will expand to treat solid tumors and non-oncologic diseases.
“We’re the only center in Rhode Island providing CAR T-cell therapy. Now patients don’t have to travel to Boston.”
Pharmacists play a key, ongoing role in this important program, Huynh adds. “The role of pharmacy has grown. Today we’re increasingly involved in patient care plans. With side effects becoming more complex, regulations becoming tougher, and the need to standardize protocols, I believe having a pharmacy member on the team improves outcomes.”
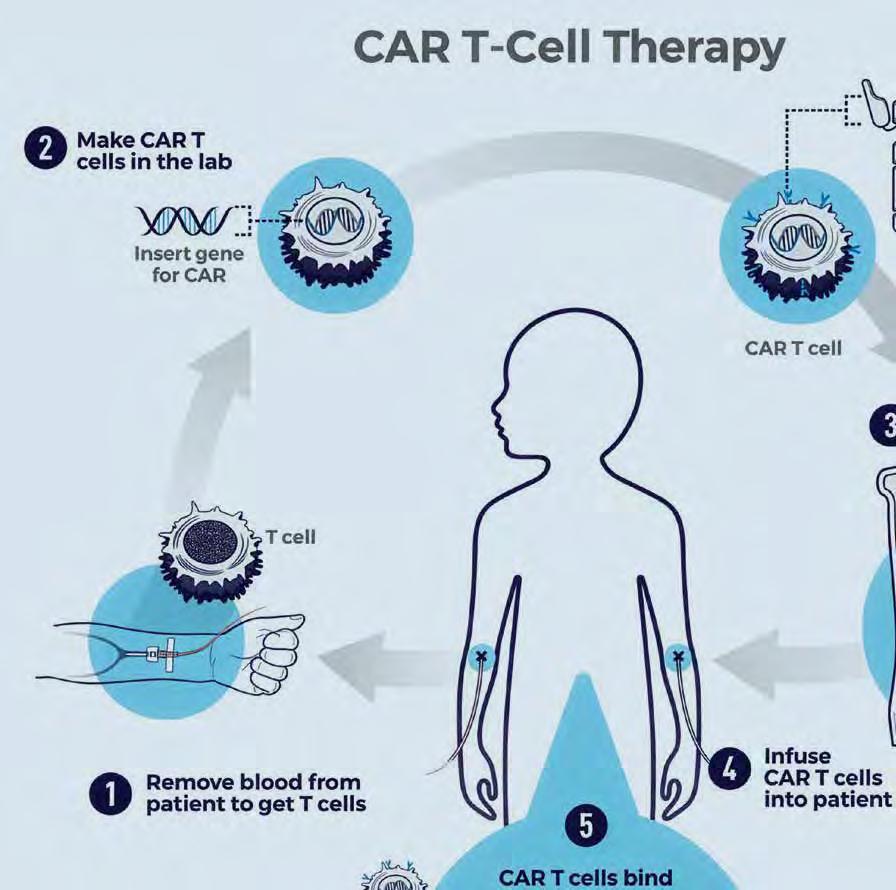

CAR T cell therapy is a type of treatment in which a patient's T cells are genetically engineered in the laboratory so they will bind to specific proteins (antigens) on cancer cells and kill them. (1) A patient's T cells are removed from their blood. Then, (2) the gene for a special receptor called a chimeric antigen receptor (CAR) is inserted into the T cells in the laboratory. The gene encodes the engineered CAR protein that is expressed on the surface of the patient's T cells, creating a CAR T cell. (8) Millions of CAR T cells are grown in the laboratory. (4) They are then given to the patient by intravenous infusion. (5) The CAR T cells bind to antigens on the cancer cells and kill them.
Key Accomplishments (Year in Review)
• Rolled out Omnicell carousels at RIH.
• Converted Morton and Saint Anne’s hospitals from Pyxis to Omnicell.
• Built in-house large-language models (LLMs) and artificial intelligence (AI) automation tools.
• Completely rebuilt the patient assistance/financial aid (PA/FA) tracker as a web application.
• Created analytics reports for the Pharmacy-to-Dose Vancomycin Program.
Plans for the Year Ahead
• Select an enterprise cloud data provider and modernize data usage and sharing at Brown Health.
• Expand task- and work-tracking with Asana software.
• Continue to build dynamic documentation within the new Wiki-style platform.

Overview
The informatics team partners with all sectors of our organization to ensure the clinical content entering our system is appropriate and meaningfully implemented. We support, either directly or collaboratively, by managing preference lists, medication lists, and InBasket pools, facilitate First Databank (FDB) updates, order set updates or new builds, update medication records, create new medication records, maintain the online formulary, troubleshoot (and resolve) issues from frontline staff, implement drug shortage response strategies (alternative alerts, order set updates, medication list modifications), manage billing error work queues, and much more.
This year, the team submitted more than 1,700 service requests and incidents to IS.
Key Accomplishments (Year in Review)
• Supported the submission, testing, and implementation of several large-scale critical clinical initiatives, including pharmacy-to-dose vancomycin, updates to pediatric diabetic ketoacidosis (DKA) protocol, nurse-driven electrolyte repletion protocol, ICU continuous insulin infusion calculator, inhaler-tonebulizer interchange, and many others.
• Contributed to major Omnicell and Epic projects including:
° Conversion to Epic for two new hospitals joining Brown Health.
° Supported implementation of two Omnicell carousels at the Rhode Island Hospital campus and provided post-go-live support.
° Developed Epic build for a new Long-Acting Injectable Antipsychotic Replacement Program.
° Completed optimization of titratable infusion builds that have an impact on a significant number of clinical areas and order set content. Improved age/weight-based dosing defaults for key medications (e.g., daptomycin, acyclovir, rocuronium).
• Implemented Epic changes for updated non-formulary policy, Epic initiatives for IV fluid shortage mitigation strategies, and transitioned IV desensitization preparations to compounding and repackaging.
• Reconfigured pharmacist and hospital facility preference lists.
• Accomplished OR scanning project fixes and optimizations.
• Undertook Formulink implementation to support formulary visibility and compliance.
• Continue to support new Massachusetts sites in their adoption of Epic—updating and optimizing records, protocols, and order sets to create a unified workflow that fits with both states’ regulations.
• Expand and revamp the scope of pharmacist Emergency Department order verification.
• Perform Epic build and implementation of updated protocols (pharmacy to dose aminoglycosides, bolus from bag, updated system-wide diabetes ketoacidosis protocol, updated alcohol withdrawal protocol).
• Establish a Super User program for Epic SlicerDicer with resources identified at each site and empowering pharmacists’ data self-sufficiency with SlicerDicer.
• Created new order panels (eye surgery take-home, oral methotrexate, pediatric pain, others) and updated previously built ones (outpatient diabetes, dialysis, bariatric surgery).
• Implemented and continued optimization of Hello World patient SMS messaging for prescriptions.
• Added electronic date of birth validation to the point-of-sale system to reduce risk of incorrect patient events during transactions.
• Configured safeguard for external electronic prescriptions that were not matching correctly, significantly reducing risk of incorrect selection.
• Optimized compliance packager workflow to proactively identify which medications are in the external device for staff processing prescriptions within Epic.
• Collaborated with IS to ensure that vendor data regarding controlled substance status was appropriate; prevented dozens of incorrect controlled substance record updates in our system and was updated nationwide.
• Built new infrastructure to identify and alert staff to “dispense in original container” products, with a goal to ensure these items have the longest expiration dates possible for patients, and to reduce the financial burden of accidental opening.
• Continue to optimize specialty infusion workflows for long anticipated go-live.
• Make a positive impact on prescribing habits with new order panels, as well as optimizing older ones.
• Collaborate with multidisciplinary group to enhance all aspects of vaccine strategy within the organization, from naming of products to systematically retiring old records.


When Brown University Health acquired two Massachusetts hospitals on October 1, 2024, staff members at Morton Hospital in Taunton and Saint Anne’s Hospital in Fall River celebrated. But right away, they went to work on the conversion of the established electronic medical record (EMR), Meditech, to Epic. Their system for dispensing certain medications needed to be converted to Omnicell, along with the pump system that provides intravenous (IV) fluid.
“We all knew it was going to be a huge undertaking,” says Brian Spadaro, Director of Inpatient Pharmacy Operations at Saint Anne’s. “Christine Collins was the first to reach out, followed by others in BUH pharmacy services. “The meetings started right away—four to six meetings every day.”
During those long days, something important happened. “We gained insight into our Brown colleagues’ process and how they make decisions as a team,” notes Arsenio Martins, PharmD, Director of Inpatient Operations at Morton. “They made sure we became well-ingrained in the culture and mission of Brown so that we were all on the same page and steering toward the same goal.”
That goal was formidable, but the pharmacists, clinicians and other staff at Morton and Saint Anne’s—a er a long struggle as members of Steward Health Care, which filed for bankruptcy in 2024—appreciated seeing all the resources and assistance that BUH provided. “We had classes on using both Epic and Omnicell,” says Spadaro. “There were certain weeks when people signed up for Omnicell training, and we trained the trainers: 30-50 ‘super-users’ who trained their staff.”
Specialized pharmacy staff provided key expertise. “The automation team made sure the interface was built from Epic to Omnicell so that all those medications and orders converted properly,” says Martins. “The informatics folks focused on the clinical side—assuring that all order sets were flowing from Epic.”
A er months of relentless preparation, work and worry, the conversion at both hospitals happened on Saturday, August 23. “The day before, August 22, was a very, very long day, as we started with the offsites for Saint Anne’s,” Spadaro recalls. “One of my managers and I started at 7:30 that morning, and I got home at 11:00 that night. The day of the cutover was even longer. Overall, it went well. Every day got better; we got to where we needed to be.”
“ We went live and saw that all the major things were working,” Martins adds. “Patients were safe, getting their medications, and nurses were able to do their jobs. We could deal with the small stuff later. There was a sigh of relief: we did it. Everybody was really happy.”
Overview
The Center for Medication-Use Policy, Safety, and Outcomes continued to work over the course of the year to advance integration across the pharmacy service line by partnering with operations, clinical services, informatics and business operations and to have an impact on outcomes. Key areas of focus included strengthening medication safety through policy development, regulatory compliance, and systemwide event reporting and analysis.
The center coordinated activities of the Medication Safety Team and the Pharmacy & Therapeutics Committee to align inpatient and outpatient practices across Brown Health. Strategic partnerships with informatics and IS supported safe implementation of policies in LifeChart, while collaborations with Vizient and purchasing coalitions identified opportunities for cost-effective and evidence-based medication use. Through robust communication, data analytics, and continuous quality improvement, the center supported patient-centered, safe, and fiscally responsible medication-use practices.
Key Accomplishments (Year in Review)
• Supported the integration of Saint Anne’s and Morton hospitals into the Brown Health network through the alignment of medication safety practices, policy/governance structures, and the successful implementation of a new electronic health record (EHR), automated dispensing cabinets, and smart infusion pump drug libraries in a unified go-live.
• Partnered with nursing leadership to launch the “Speak Up for Medication Safety” campaign, promoting awareness of safe medication practices and encouraging staff to report potential safety concerns.
• Collaborated with hospital incident command center and clinical leaders to mitigate the national IV fluid shortage by updating clinical guidelines, integrating changes into the EHR, and conducting risk assessments to ensure safe use of alternative products.
• Enhanced detection and reporting of potential adverse drug events using EHR-based screening tools leading to optimized reporting, systemwide tracking for clinical review, and identification of contributing factors.
• Successful support for a wide scope of regulatory surveys, including triennial Joint Commission surveys at Bradley Hospital and Morton Hospital.
Plans for the Year Ahead
• Continued alignment of medication safety practices, formularies, regulatory compliance activity, and policy development at newly integrated Saint Anne’s and Morton hospitals.
• Identify appropriate use cases for artificial intelligence (AI) to optimize performance improvement activities, reduce administrative burden, and expand the impact of the work done by the team in improving safe and effective medication use.
• Increase utilization of formalized quality improvement tools, such as failure mode and effects analysis (FMEA) to help with the implementation and optimization of medication safety-related initiatives (e.g., EnFit syringe and U-500 pens).
• Continued focus on business continuity planning, collaborating with internal pharmacy leadership, system information services and disaster preparedness teams to optimize readiness for system downtimes.
Key Accomplishments (Year in Review)
• Completed analyses to track improvement of hypoglycemia among patients on insulin infusion as a result of implementation of a chart-embedded insulin infusion calculator.
• Provided statistical analysis, data management, and study design support for pharmacy resident projects, leading to one publication.
• Demonstrated increasing rates of pharmacist interventions due to auto-verification overhaul in the pediatric emergency room.
• Provided data management expertise to vancomycin reporting dashboards.
Plans for the Year Ahead
• Optimization of project management structure for research and quality improvement projects.
• Outcome analyses for pharmacy-to-dose vancomycin implementation.
In September 2024, it was reported that the nation’s largest manufacturer of IV fluids had its North Carolina facility destroyed by Hurricane Helene. Baxter International produces 60 percent of the IV fluid used in the U.S. Staff at hospitals and clinics around the country braced themselves.
“Baxter communicated that their plant was impacted, but we didn’t know how bad,” recalls Koren Kanadanian, System Director, Emergency Management, for Brown University Health. Kanadanian and his team went to work, determining what was in stock at each hospital and the IV fluid usage levels—notably in critical settings—and created a chart. “We determined days on hand, and we tried to order from Baxter. They probably had some stock available.”
That is when the extent of the problem revealed itself. “Baxter’s plant was more damaged than we thought, and area roads and bridges were down. Even if they had stock, they couldn’t get it to hospitals or to distributors.” With every hospital in the country calling distributors, the situation became grave: cancer patients, emergency patients and many others might be at risk. Kanadanian established a hospital incident command—a daily 3 p.m. call with all the right people.
“We needed to conserve what we had,” he explains. “We discussed the use of oral rehydration—giving patients Gatorade or Pedialyte—instead of infusing fluid. Most of our physicians agreed that this would work. We weren’t lowering the standard of care; we were giving fluid in a different way.” Pharmacy staff began creating alternative order sets in Epic for providers.
Laryssa Domingo, PharmD, Clinical Pharmacist, Drug Shortage Management, monitors drug sources and the supply-chain to watch for disruptions. “When it happens, we come up with a contingency plan, which may mean turning to a new product,” she explains. “We moved products to where they were most needed, and we reviewed opportunities for conservation, such as administering certain injectables as IV push rather than an IV infusion. Our compounding team studied the data and decided they could compound certain medications to save on IV fluid.”
Baxter’s manufacturing function was back to normal in May, eight months later. “We kept our conservation measures in place until the end of June,” says Kanadanian. A recent shortage of morphine resulted in the same approach—notably, a command call. “If we involve all the right people, we can develop a plan.”
In the face of the IV fluid shortage, many lessons were learned. “That daily communication was so key,” Domingo notes. “That collaboration helped us shift and guide our purchasing patterns—and be innovative throughout the shortage.”
The Brown Ambulatory Care Pharmacy Network is dedicated to improving the health and well-being of our communities by ensuring safe, timely, and equitable access to medications across the continuum of care. Through our integrated network of retail pharmacies, specialty pharmacy services, and expert clinical pharmacist specialists, we provide personalized support, compassionate care, and seamless coordination with providers. We are committed to advancing medication access, optimizing therapy outcomes, and empowering patients to achieve their best possible health.
Key Accomplishments (Year in Review)
• Obtained Massachusetts non-resident pharmacy license for four Rhode Island locations.
• Health plan design updates (deductible, GLP-1 restrictions) led to significant volume impact and patient care complexities.
• Implemented the Hello World patient messaging platform within Willow Ambulatory.
• Established PACE RI partnership for after-hours discharge patients, supporting continuity of care.
• Continued Rhode Island Free Clinic partnership, providing more than 600 prescriptions to approximately 240 patients.
• More than 624,000 total outpatient prescriptions were dispensed, representing higher than 19 percent prescription growth.
• Specialty Drug Prescription Monitoring Program (SDPMP) patient volume grew by 34 percent year-overyear.
• SDPMP patient satisfaction remained excellent, with an overall satisfaction level of 99.12 percent.
• SDPMP added 25 new specialty medications, five of which required REMS program certification.
• Developed a specialty medication mail-away disposal option.
Plans for the Year Ahead
• Opening of the Consolidated Services Center.
• Expansion of the retail footprint with locations at Morton Hospital and Saint Anne’s Hospital.
• Expansion of opt-out Meds to Beds services in both Hasbro and adult emergency departments.
• Implementation of Willow point of sale and a new Medicare Part B processor.
• Development of a prescription delivery process utilizing a major carrier.
Key Accomplishments (Year in Review)
• Successfully obtained both our Organized Ambulatory Care Facility license to open the infusion clinic at 148 West River Street and our Certificate of Need for Home Care.
• The clinic saw its first patients, with the first six individuals receiving infusion therapy in the rheumatology hub and one patient in neurology. These first patients represent not only a significant step forward for our program but also a promise of the impact we will have as we continue to grow.
• Hired our patient care team: a nurse manager, nurses, and a pharmacist.
• Prepared clinic space with the right tools, supplies and resources to support our nurses and provide the optimal care environment for patients.
• The team has developed policies, referral forms, and standard operating procedures.
Plans for the Year Ahead
• We are actively preparing for ACHC accreditation this Fall. ACHC accreditation will allow us to pursue further contracts by establishing our commitment to high-quality care and standards.
• Continue to pursue contracting with payors to expand access to our clinic at West River.
• With a license to now provide care in the home, the specialty infusion team plans to develop workflows as needed.

Specialty infusion has proven to be an effective treatment for a range of acute and chronic conditions, including migraines, cancer, lupus and rheumatoid arthritis. Growth is projected, largely due to an aging population and the increase in chronic conditions. Today more than half of specialty infusion therapies are provided in hospitals.
But that is changing, including at Brown University Health. Amrita Shahani, PharmD, MS, Director, Pharmacy Infusion Services, is helping to establish a specialty infusion center. After obtaining the required license, contracts and a certificate of need for home care, step one was achieved. Patients are receiving infusion therapy in a new clinic designed for their comfort and efficiency.
“At our West River Center in Providence, there are pharmacists, nurses and a medical director who work together collaboratively to provide the best care, as well as patient education,” says Shahani. “The center is focused on providing patients with a positive experience. We have eight comfortable chairs, a coffee station— even a lending library. Patients could be here for a quick 15- or 20-minute visit; others are at the center for four to six hours. This is common for those with certain autoimmune disorders.”
The next step is to provide infusion therapy to patients in the comfort of their homes. “A good example is someone who needs antibiotics three times a day,” Shahani explains. “We can’t ask patients to come in three times a day; they’re perfect candidates for home infusion.
“Now that we have the license to provide this service, we are developing a patient management program. When the patient is heading home, we will reach out and arrange to provide them with all their supplies and schedule a nurse to come to the home for the up-front teaching, followed by administration of the patient’s infusion therapy.” More than 250 intravenous medications are currently in development for additional treatments.
With the establishment of specialty infusion at the West River Center and future launch of a home infusion therapy program, Brown Health patients will have several new options for infusion therapy to fit their specific needs. Meanwhile, the insurance market continues to evolve.
“We’re providing our patients with a full continuum of care,” says Shahani. “It’s been a great challenge, but I’m working with a great team here at Brown Health.”

• To support growing demands, we made strategic investments in program infrastructure by adding a MAP Operations Specialist, MAP supervisor, and fourth Lead Technician role.
• Completed service rollouts at Center of Primary Care specialty clinics (rheumatology, gastroenterology, hepatology) and Brown Health Cancer Institute sites (RIH, TMH, NPH, satellite locations), enhancing access to supportive oncology therapies and strengthened continuity of care.
• As part of a seamless post-merger rollout, extended support to ~1,800 patients and ~30 providers transitioned from Miriam Primary Care to the Center for Primary Care Clinic.
• Partnered with the Division of Addiction Medicine to support a new initiative, the RIH Addiction Care Today walk-in clinic, connecting patients with access to lifesaving medications and transitioning them to longitudinal care at the Brown Health Recovery Center.
• Participated in the pharmacist-supported Remote Weight Management Program pilot, expanding access to GLP-1 therapies for patients referred by the Brown Health Medical Group Primary Care team.
• Secured Pharmacy & Therapeutics Committee approval of the new Brown Health MAP Pharmacist Refill Guideline, replacing the previous Collaborative Practice Agreement and modernizing the refill service model to increase flexibility and align with pharmacist scope.
• Supported 48,000+ unique patients, performed 30,000 coverage investigations and submitted 16,000+ medication prior authorizations with 95 percent approval rate.
• Processed 135,000+ refill requests, averaging same-day turnaround.
• Secured $100M+ in financial assistance through free drug programs, foundations, grants, and copay assistance.
Plans
• Develop and start a MAP Elective Rotation for University of Rhode Island APPE students for 2026-2027 academic year.
• Launch MAP services at Brown Health Medical Group of Massachusetts (Dartmouth), supporting the Inflammatory Disease Hub (rheumatology, gastroenterology, dermatology).
• Expand MAP support within the Brown Health Weight Management Program.
• Participate in a new inpatient discharge medication reconciliation program to improve post-discharge medication safety and access.
• Integrate Real-Time Pharmacy Benefits (RTPB), electronic prior authorization (e-PA), and AI-powered tools to automate and scale services.
Key Accomplishments (Year in Review)
• Implemented new collaborative practice agreements for the management of anxiety, bipolar disorder, depression, alcohol use disorder, stimulant use disorder, osteoporosis, and schizophrenia.
• Continued to expand verification queues in various clinics to allow benefits investigation and therapy evaluation prior to final pharmacy receipt.
• The Ambulatory Care Pharmacy & Therapeutics Subcommittee approved four additions to the formulary.
• Established ambulatory clinical services in Massachusetts, supporting Brown Health Medical Group of Dartmouth’ s dermatology, gastroenterology, and rheumatology clinics.
Plans for the Year Ahead
• Further expansion of pharmacy infrastructure within ambulatory care clinics at Brown Health Medical Group of Massachusetts.
• Coordination with specialty infusion services to further optimize medication access for patients.
• Implementation of CPAs in Massachusetts.

The promise of gene therapy was seen at Brown Health in April 2025, when the first patient received Hemgenix, a one-time treatment designed to relieve individuals with hemophilia B from self-infusing throughout the week and worrying about a potential bleed. The 39-year-old man was the first person in Rhode Island to receive Hemgenix.
It took a year of planning and discussion before the multidisciplinary team at BUH was ready. “We had identified the patient as a potential candidate back in April 2024, but we needed to work through everything, including coverage by his insurance plan,” says Ian Willoughby, PharmD, MS, BCPS, Senior Director, Pharmacy Specialty and Infusion Services. “The treatment is very expensive and requires special handling. Gene therapy is a challenging world to work in, but our goal is to make it work for the patient.”
Those with hemophilia B, who must infuse factor 9—the clotting factor they lack—as often as every three to four days, are motivated to have gene therapy, notes Salley Pels, MD, Medical Director, Rhode Island Hemostasis and Thrombosis Center. “Among our 130 patients with hemophilia, 85 percent have hemophilia A. There is gene therapy available for them as well, but they have more options.”

“ Hemgenix was the catalyst for starting the Brown University Health High-Cost Drug Committee.”
Those with hemophilia B are motivated to receive Hemgenix, but they must comply with intensive follow-up for the first three months and continued monitoring. “We deliver Hemgenix to the patient in the form of an inactive virus, so we have to check for existing antibodies that might destroy the virus,” Dr. Pels explains. “We also watch for inflammation of the liver, notably in those who have had hepatitis.”
All the work required to administer the gene therapy was worth it. “Did we have the right equipment, training/education and the all the right people involved—physicians, pharmacists, billing and coding staff?” says Shannon Baker, PharmD, BCSCP, Pharmacy Director, Oncology and Compounding Service. “For Hemgenix, we had educational sessions with the manufacturer’s representative. The pharmacy team made sure that the medications are received, stored, prepared and handed off to the nurses in a safe manner.”
The era of gene therapy brings hope to patients in the form of very expensive medication. “Hemgenix was the catalyst for starting the Brown University Health High-Cost Drug Committee,” says Willoughby. “We meet monthly to discuss how best to prepare for the various products coming through the pipeline.”
The patient who received Hemgenix is doing well. “We can’t predict how long our patient will continue to express the gene,” adds Dr. Pels, “but we hope this treatment gives him five to ten years without the need for regular factor infusions. He is very happy with the outcome so far.”
Overview
This year continued to present the team with unprecedented challenges relative to the 340B Program. The constant assault by pharmaceutical manufacturers took millions of dollars away from the care of Brown University Health patients. The 340B team worked with legal, government affairs, and statewide partners to advocate for the successful passing of 340B non-discrimination regulations in Rhode Island.
Through contracting efforts, Pharmacy Business Operations was successful in supporting the pharmacy’s strategic plan to contemporize practices and technology through completion of the installation of carousel technology at all Rhode Island hospitals. They also mobilized in a quick and efficient manner to support the onboarding of our two new Massachusetts hospitals to Brown Health systems and vendors.
By leveraging sophisticated analytics, forecasting and financing models, the pharmacy finance team compiled an aggressive operating and capital budget, which met its targets. The pharmacy supply chain, which handles nearly a half-billion dollars in inventory per year, maximized the use of new technology to ensure consistent purchasing patterns, made critical decisions and met aggressive milestones on their Consolidated Services Center (CSC) journey. The pharmacy revenue-cycle integrity team has provided millions of dollars of financial support to seriously ill patients who are on very expensive medications.
Key Accomplishments (Year in Review)
• Maintained wholesale acquisition cost (WAC) expense below four percent, thereby reducing wasteful expense.
• Leveraged contracting parity and pricing validation software to realize more than $1 million in expense cost avoidance.
• Generated more than $4.5 million in savings on pharmaceutical expenses by applying strategic purchasing strategies.
• Negotiated significant savings during renewal of primary pharmaceutical wholesaler agreement.
Plans for the Year Ahead
• Establishment of Brown Health Consolidated Service Center in order to:
° Enhance medication safety by standardizing processes.
° Increase supply chain resilience against drug shortages.
° Improve efficiency and cost-effectiveness.
Key Accomplishments (Year in Review)
• The Drug Shortage Committee played a key role during an IV fluid shortage by utilizing our extensive pharmacy network of vendors, identifying more than 37 conservation strategies and updating our contingency plans and compounding strategies.
• Drugs with minimal or no utilization were identified for Pharmacy & Therapeutics Committee review, streamlining the inpatient formulary and decreasing waste.
• On average, approximately 200 drugs were monitored at any given time. Less than 10 percent required transition to alternative(s) due to complete depletion.
• Developed a 503B preparedness resource that outlined products available across our 503B partners and provided information on a secondary source of procurement if needed.
Plans for the Year Ahead
• Establishment of a monthly financial report to analyze the costs associated with procuring drug shortage items and their respective alternative(s) for stakeholder awareness.
• Continue standardizing our products, practices, and contingency plans across Rhode Island and Massachusetts hospitals.
• Provide a newsletter to retail and ambulatory care spaces summarizing shortage news (e.g., recalls, FDA warnings, etc.).
Key Accomplishments (Year in Review)
• Assisted with more than $5.7 million in cost savings to patients or cost avoidance to Brown Health through manufacturer patient assistance programs.
• Captured appropriate documentation for medications wasted during compounding, adding $1.4M/month in new revenue.
• Copay assistance has saved Brown Health patients nearly $500K in FY25.
• Supported the change of approximately 250 biosimilar products.
• Interdisciplinary work in other areas (prior authorization, revenue integrity, denials management, patient financial services, coding) totaled more than $250K worth of medication cost avoidance for Brown Health.
Plans for the Year Ahead
• Continue to expand copay assistance.
• Increase collaboration and financial interventions within pharmacy.
• Expand role in denials management.
• Engage and offer services to new Massachusetts hospitals.
• Explore implementation of a third-party revenue cycle integrity software program.
Key Accomplishments (Year in Review)
• Registered Morton and Saint Anne’s hospitals in the 340B Program.
• Passage of PBM regulation and contract pharmacy protection law in Rhode Island.
• Developed innovative practices to maximize 340B savings for Rhode Island Hospital.
Plans for the Year Ahead
• Contract pharmacy implementation for Morton and Saint Anne’s hospitals.
• Restore the benefit of our 340B Program, supported by the enforcement of the RI state law.
Overview
• Expansion of PGY2 programs to include one Pediatric PGY2 and one Emergency Medicine PGY2 resident for the 2025-26 residency year.
• All programs successfully recruited an impressive class of residents for the 2025-26 residency year.
• RIH and TMH PGY1 graduates matched successfully into the following programs.
° Amanda Blais (RIH PGY1) - PGY2 Critical Care Pharmacy Residency – Rhode Island Hospital
° Peyton Calvao (RIH PGY1) – PGY2 Pediatrics Pharmacy Residency – Rhode Island Hospital
° Abbigayle Fielder (RIH PGY1) - PGY2 Emergency Medicine Pharmacy Residency – Rhode Island Hospital
° Lauren Fortier (TMH PGY1) - PGY2 Ambulatory Care Pharmacy Residency – Rhode Island Hospital/ University of Rhode Island
° Abigail Horan (RIH PGY1) - PGY2 Oncology Pharmacy Residency – Dana-Farber Cancer Institute
° Ngan Nguyen (RIH PGY1) - PGY2 Oncology Pharmacy Residency – Rhode Island Hospital
° Catherine Smith (RIH PGY1) - PGY2 Infectious Disease Pharmacy Residency – Johns Hopkins Medicine
° Mary Zhuang (RIH PGY1) - PGY2 Critical Care Pharmacy Residency – UH Cleveland Medical Center
Award
Preceptor of the Year
Preceptor Commitment to the Profession Award
Rock Star Resident of the Year
Resident Commitment to the Profession Award
Recipient
Amy Brotherton, PharmD, AAHIVP, BCIDP
Hannah Kisla, PharmD, BCOP
Elizabeth Del Vecchio, PharmD
Alyssa Soares, PharmD
Residency committees include social/wellness, professional development, and community service committees. These committees are run by pharmacy residents throughout the system, with involvement from preceptors to support their efforts.
Key Accomplishments (Year in Review)
• Preceptor and Professional Development Committee:
° Launched a new newsletter, Dose of Development , designed to provide resources to improve precepting practice, tactics to support well-being, and highlight outstanding preceptors and learners.
° Performed a CV and letter of intent review for our LAPPE students from the University of Rhode Island.
° Held North American Pharmaceutical Licensure Examination review sessions for our LAPPE students and others on rotation.
° Coordinated mock residency interviews for our LAPPE students.
° Organized a financial boot camp for incoming PGY1 residents, presented by Joshua Hayden, PharmD, BCPS.
• Community Service Committee:
° Participated in and raised funds for the Walk to End Alzheimer’s in 2024.
° Completed winter clothing and canned food drives.
° Ran a donation drive for a local animal shelter.
• Social/Wellness Committee:
° Resident outing events in Newport and an escape room bonding event early in the residency year.
° Completed holiday events to encourage resident bonding and well-being through Friendsgiving and secret Santa.
Plans for the Year Ahead
• Continue to engage residents, students, and preceptors for ongoing community service efforts.
• Expand the reach of our endeavors to include our new Massachusetts hospitals.
• Utilize the new Dose of Development newsletter to enhance educational efforts across the enterprise.
Overview
Pharmacy practice research in an academic health system encompasses a wide range of objectives and goals aimed at improving the quality of patient care, advancing the pharmacy profession, and contributing to the body of knowledge in healthcare. Key goals include:
• Optim izing Medication Therapy: Improve the safety and effectiveness of medication therapy by conducting research on drug interactions, dosing regimens, and therapeutic outcomes.
• Cli nical Outcomes: Evaluate the impact of pharmacist-led interventions and services on patient clinical outcomes, such as disease management, symptom control, and overall health-related quality of life.
• Hea lth Economics: Analyze the economic implications of pharmaceutical interventions and healthcare services provided by pharmacists. Assess the cost-effectiveness and cost-benefit of various pharmacy practices.
• Pat ient Safety: Study strategies to enhance medication safety, including error reporting systems, medication reconciliation processes, and the use of technology to prevent medication errors.
• Qua lity Improvement: Engage in research projects that assess and enhance the quality of pharmacy services and patient care within the academic health system. Implement continuous quality improvement initiatives based on research findings.
These goals collectively aim to advance the pharmacy profession, improve patient care, and contribute to the overall goals of Brown University Health in research, education, and patient care. Brown Health provides a unique environment for conducting this research due to integration of clinical practice, education, and research activities.
Pharmacy members published 13 peer-reviewed scientific manuscripts between October 1, 2024 and September 30, 2025.
1. Cavallari, L.H., Hicks, J.K., Patel, J.N., Elchynski, A.L., Smith, D.M., Bargal, S.A., Fleck, A., Aquilante, C.L., Killam, S.R., Lemke, L., et. al. (2025). The Pharmacogenomics Global Research Network Implementation Working Group: Global Collaboration to Advance Pharmacogenetic Implementation. Pharmacogenetics and Genomics, 35 (1), 1–11. https://doi.org/10.1097/FPC.0000000000000547
2. Chen, T., Vargas Galvan, L.A., Walsh, K.L., Winegarner, A., Apruzzese, P., Asher, S., & Maslow, A. (2025). A Retrospective Review of the Deep Parasternal Intercostal Plane Block in Patients Undergoing Cardiac Surgery with Median Sternotomy. Journal of Clinical Medicine, 14 (6), 2074. https://doi.org/10.3390/ jcm14062074
3. Duprey, K., Garde, L. (2024). The Ideal Learner “Track” to Prevent Preceptor Burnout. K., Evoy (Ed.), ACCP Ambulatory Care Pharmacist’s Survival Guide (5th Edition, 551-557).
4. Emigh, B., Bose, A., Stephen, A., Arabi, J., & Adams, C. (2025). Perioperative Venous Thromboembolism Prophylaxis in Orthopedic Trauma: A Practical Review. Rhode Island Medical Journal (2013), 108 (2), 63–68.
5. Liauw, J.C., Silveira, S., & Ribizzi-Akthar, I. (2025). Severe hypersensitivity reactions to two immunotherapy agents in a patient with cutaneous squamous cell carcinoma. American Journal of Health-System Pharmacy: AJHP: Official Journal of the American Society of Health-System Pharmacists, 82 (5), e252–e255. https://doi.org/10.1093/ajhp/zxae286
6. Mathew, J., Pagliaro, J.A., Elumalai, S., Wash, L.K., Ly, K., Leibowitz, A.J., & Vimalananda, V. G. (2025). Developing a Multisensor-Based Machine Learning Technology (Aidar Decompensation Index) for Real-Time Automated Detection of Post-COVID-19 Condition: Protocol for an Observational Study. JMIR research protocols, 14 , e54993. https://doi.org/10.2196/54993
7. Mokszycki, R.K., Nagy, J., Arabi, J., & Lawson, C. (2024). Crafting Consistency: A Call to Standardization of Alcohol Withdrawal Treatment in the Emergency Department. Annals of Emergency Medicine, 84 (4), 468–469. https://doi.org/10.1016/j.annemergmed.2024.05.007
8. Nguyen, N.N., Huynh, J.P., Wu, J.J., Kisla, H.M., Read, J.N., La, A.G., Tat, D., & Brown, B.R. (2025). Identifying Health Disparities in Lenalidomide Access. Journal of Oncology Pharmacy Practice: Official Publication of the International Society of Oncology Pharmacy Practitioners, 10781552251348222. Advance online publication. https://doi.org/10.1177/10781552251348222
9. Nolan, K., MacLeod, H., Taman, M., Collins, C., & Zullo, A.R. (2025). Closing the Pharmacy Sector’s Skills Gap: The Solutions Training and Teamwork (STAT) Program’s Approach to Workforce Development and Diversity Enhancement. American Journal of Health-System Pharmacy: AJHP: official journal of the American Society of Health-System Pharmacists, zxaf106. Advance online publication. https://doi.org/10.1093/ajhp/zxaf106
10. Pagliaro, J.A., Wash, L.K., Ly, K., Mathew, J., Leibowitz, A., Cabrera, R., Wormwood, J.B., & Vimalananda, V.G. (2025). Enrollment and Retention Outcomes from the Veterans Health Administration for a Remote Digital Health Study: Multisite Observational Study. JMIR Formative Research, 9, e68676. https://doi.org/10.2196/68676
11. Shearer, E., Nagy, J., Aluisio, A. (2025, April). “Popper”-Induced Methemoglobinemia: A Visual Diagnosis. Rhode Island Medical Journal. Retrieved from: http://www.rimed.org/rimedicaljournal/2025/04/2025-04-11-imagesshearer.pdf
12. Silva, C.R., Nagy, J., Zullo, A.R., & Greene, R.A. (2025). Safety of Peripherally Administered 23.4% Sodium Chloride. Neurocritical Care, 10.1007/s12028-025-02342-w. Advance online publication. https://doi.org/10.1007/ s12028-025-02342-w
13. Walsh, K.L., Silva, C.R., & Lee, P.H. (2024). Occult Methemoglobinemia in a Medically-Complex Seven-YearOld Child and the Opportunity for Pharmacist Intervention in Pediatric Emergency Medicine. The Journal of Pediatric Pharmacology and Therapeutics, 29 (6), 650–653. https://doi.org/10.5863/1551-6776-29.6.650
Pharmacy members completed ten PowerPoint and poster presentations, lectures, and panel discussions between October 1, 2024 and September 30, 2025.
1. Duncan, A., Willis, S. (2024, December 10) CFTR Modulators and Pediatric Intranasal Sedation [presentation]. ASHP Midyear Clinical Meeting. New Orleans, LA.
2. Harrington, B. (2025, March 13). Sustaining the Future: Precepting for Enduring Success and Career Well-being [panel discussion]. University of Rhode Island Seminar by the Sea. Kingston, RI.
3. McCarthy, BC Jr. (2025, April 1). Verbal testimony before the Rhode Island Senate Health and Human Services Committee on Senate Bill 0692. Rhode Island General Assembly. Providence, RI.
4. McCarthy, BC Jr. (2025, Feb 25). Verbal testimony before the Rhode Island House Health and Human Services Committee on House Bill 5353. Rhode Island General Assembly. Providence, RI.
5. Nau, G., Torbey, E., Consaga, M. (2024, December 10). Tick Tick: Early Recognition of Ehrlichiosis as a Source of Sepsis [panel discussion]. Medicine Morbidity and Mortality Conference. Providence, RI.
6. Qureshi, A., McCarthy BC Jr., Dow J. (2025, September 4) Leading the Pharmacy Enterprise through Mergers and Acquisitions [Webinar]. Vizient webinar presentation using Microsoft Teams. Online.
7. Roberts, M., Caetano, N. (2024, November 2). House of Delegates Update [podium]. Rhode Island Society of Health-System Pharmacists Future of Pharmacy Showcase. University of Rhode Island, Kingston, RI.
8. Roberts, M. (2024, December 8) All Hands on Deck: Application and Survey for the Center of Excellence in Medication-Use Safety and Pharmacy Practice Certification [educational session]. ASHP Midyear Clinical Meeting. New Orleans, LA
9. Roberts, M. (2025, May 7) Managing REMS at Your Institution [panel discussion]. Vizient Southern States Pharmacy Leaders Q2 Network Meeting. Online.
10. Vesel, T., Lee, P.H., Lebovitz, A. (2023, October 15-18). The Use of Oral Ketamine in Outpatient Palliative Care Clinics: Development of Institutional Protocol and Case Reviews [presentation]. McGill International Palliative Care Congress. Montreal, QB, Canada.
Key Accomplishments (Year in Review)
• Conducted quarterly performance report-outs using the Strategic Plan Scorecard to track progress and guide strategic actions.
• Held a strategic planning retreat in June as a key component in developing a new three-year Pharmacy Services Strategic Plan.
Plans for the Year Ahead
• Open a pharmacy supply-chain warehouse.
• Open a centralized retail pharmacy to process home delivery and adherence packaging services.
• Establish a specialty infusion pharmacy.

Month
October 2024
Employee of the Month
Site
Michael Iafrate, PharmD, clinical pharmacist, oncology Rhode Island Hospital
November 2024 Eridania Teixeira, PharmD, clinical pharmacist specialist Rhode Island Hospital
December 2024 Daren Rathbun, CPhT, pharmacy technician supervisor BUH Pharmacy
January 2025
February 2025
James Ning, PharmD, supervisor, inpatient pharmacy operations Rhode Island Hospital
Jamie Readey, CPhT, medication access program group lead Rhode Island Hospital
March 2025 Danielle Dubois, CPhT, pharmacy technician supervisorMorton Hospital
March 2025 Christina Correia, PharmD, pharmacy manager Saint Anne’s Hospital
April 2025 Kristi Pereira, CPhT, ambulatory liaison The Miriam Hospital
May 2025
Naomi Shoemo, CPhT, pharmacy technician specialist, ambulatory Newport Hospital
June 2025 Gregory Drummey, PharmD, clinical pharmacist, inpatientThe Miriam Hospital
July 2025
August 2025
Jacob Chevalier, CPhT, lead pharmacy technician, Medication Access Program The Miriam Hospital
Krystal Bevilacqua, PharmD, clinical pharmacist Elyse Gagne, PharmD, clinical pharmacy manager Brown Health Medical Group
September 2025 Nicole Costabile, CPhT, lead pharmacy technician BUH Pharmacy
The pharmacy service line continues to offer a variety of activities—both in-person and virtual—for the staff. Efforts during the past year support the following goals: to enhance the department’s culture, provide teambuilding opportunities, expand the staff’s contribution to innovation, improve work-life balance, and increase options for healthy choices.
The following options were provided during the past year:
• National Pharmacy Week is celebrated for two weeks every October. National Pharmacy Tech Day is celebrated on the third Tuesday of October. Activities included two separate therapy dog visits, Chinese food and dessert party, breakfast prepared by leadership for morning and overnight team members, ice cream social.
• Monthly calendar of events (except for the summer months):
° Fun national day celebrations such as Banana Bread Day, Clean Out Your Computer Day, and Popcorn Day.
° Hospital’s Fun Fridays included participation in events such as wearing the colors of your favorite team or a festive holiday sweater.
° Weekly 15-minute sessions on Teams for exercising, yoga, or learning about the programs available through the Blue Cross Blue Shield Living Well platform.
° Reminders of educational and social events offered by Brown Health, such as discounted tickets to PBruins, Healthcare Worker Appreciation Month at Mystic Aquarium, and financial planning sessions by Fidelity.
• Miscellaneous activities
° August Summer Fling to celebrate a successful carousel implementation.
° Grab and Go nourishment tables at periodic times throughout the year.
° Team participation in events such as the American Heart Association and Walk to End Alzheimer’s.
° Thanksgiving Food Drive and Holiday Adopt-a-Family.

Patrick H. Lee, PharmD, BCPPS, clinical pharmacist specialist, inpatient
Rhode Island Society of Hospital Pharmacists (RISHP)
– Bill Pires New Practitioner Award
Sabrina Silveira DaCosta, PharmD, clinical pharmacist specialist, ambulatory
Adjunct Clinical Assistant Professor, Physician Assistant Program, Johnson & Wales University
Joseph Honig, PharmD, clinical pharmacist specialist, ambulatory
Adjunct Faculty, Physician Assistant Program, Johnson & Wales University
Lauren Lemke, PharmD, BCPS, clinical pharmacist specialist, ambulatory
Board Member at Large, Board of Directors, Rhode Island Society of Health System Pharmacists (RISHP)
Martha Roberts, PharmD, BCCCP, department coordinator, pharmacy services, medication use policy
Alternate Delegate, House of Delegates, Rhode Island Society of Health-System Pharmacists (RISHP)
Committee Member, ICU Liberation Committee, Society of Critical Care Medicine (SCCM)
Council Member, Council on Therapeutics, American Society of Health-System Pharmacists (ASHP)
Past-Chair, Section Advisory Group (SAG) for Emerging Sciences, American Society of HealthSystem Pharmacists (ASHP)
Peer Reviewer for Midyear Clinical Meeting
Educational Content Proposals, American Society of Health-System Pharmacists (ASHP)
Secretary, Board of Directors, Rhode Island Society of Health-System Pharmacists (RISHP)
Keri Aubin, PharmD, BCMTMS, clinical pharmacist, inpatient
Board Certified Medication Therapy Management Specialist (BCMTMS)
Ashley Ayotte, PharmD, BCCCP, clinical pharmacist specialist, inpatient
Board Certified Critical Care Pharmacist (BCCCP)
Alexis Duncan, PharmD, BCPPS, clinical pharmacist specialist, inpatient
Board Certified Pediatric Pharmacy Specialist (BCPPS)
Dawn Feret, RPh, MBA, CDOE, BCSCP, clinical pharmacist specialist, ambulatory
American Society of Health-System Pharmacists (ASHP) Weight Management Certificate
Certified Professional by the American Heart Association – Telehealth (CPAHA)
Rachel Fortin, PharmD, medication quality and safety specialist
American Society of Health-System Pharmacists (ASHP) & Institute for Safe Medication Practices (ISMP) Medication Safety Certificate
Elizabeth Hamilton, PharmD, BCACP, clinical pharmacist specialist, ambulatory
Board Certified Ambulatory Care Pharmacist (BCACP)
Matthew Lariviere, PharmD, BCPS, clinical pharmacist, inpatient
Board Certified Pharmacotherapy Specialist (BCPS)
Courtney Simpanen, PharmD, BCPS, clinical pharmacist specialist, inpatient
Board Certified Pharmacotherapy Specialist (BCPS)
Elise Varkonyi, PharmD, BCACP, clinical pharmacist specialist, ambulatory
Board Certified Ambulatory Care Pharmacist
Audrey Whalen, PharmD, BCACP, clinical pharmacist specialist, ambulatory
Board Certified Ambulatory Care Pharmacist (BCACP)
Lyndsey Wiggin, PharmD, MHA, BCACP, CDOE, manager, specialty pharmacy clinical services
Master of Healthcare Administration, Salve Regina University

Christine M. Collins, MBA, RPh, FASHP Senior Vice President, Pharmacy and Perioperative Services, Brown University Health

Michael Poirier, PharmD, MHL VP, Ambulatory Pharmacy Services

Ian Willoughby, PharmD, MS, BCPS Senior Director, Pharmacy Specialty and Infusion Services

Bethany Carroll, BS, RPh Director, Retail Pharmacy Services

Amrita Shahani, PharmD, MS Director, Home Infusion Services

Michelle Corrado, PharmD, MHA, CPEL, FASHP System Director, Pharmacy Business Operations

Nelson Caetano, PharmD, MBA Director of Periop and Pharmacy Innovation and Technology

Shannon Baker, PharmD, BCSCP Director, Onc & Compound
James Ning, PharmD Director & PIC, The Miriam Hospital

Bryan McCarthy, Jr., PharmD, MS, MJ, FASHP VP, Chief Pharmacy Officer, Inpatient Pharmacy

Donald McKaig, RPh Director, Medication Use Policy, Quality, and Safety

Paul Parchesky, RPh, MS Director & PIC, Newport Hospital

Brian Spadaro, RPh, MBA Director & PIC, Saint Anne’s Hospital

& PIC,

Martins, PharmD Director & PIC, Morton Hospital
Residency Program
PGY1 Pharmacy Residency Program at Rhode Island Hospital
PGY1 Pharmacy Residency Program at The Miriam Hospital
PGY1 Pharmacy Residency Program at Brown Health Medical Group Primary Care
PGY1 Community-Based Pharmacy Residency Program
Resident(s)
Cecilia Ford, PharmD
Madison Hartling, PharmD
Kim Nguyen, PharmD
Alexandria O’Brien, PharmD
Katherine Scroggs, PharmD
Jack Summa, PharmD
Jennifer Van Hook, PharmD
About
Graduate of the University of New England School of Pharmacy
Graduate of the University of Rhode Island
Graduate of the University of Rhode Island
Graduate of the University of Rhode Island
Graduate of the University of Rhode Island
Graduate of the University of Rhode Island
Graduate of the University of Pittsburgh School of Pharmacy
Julia Vigorito, PharmDGraduate of Northeastern University
Tyler Abdallah, PharmD
Kayla Scofield, PharmD
Jamie Read, PharmD
Graduate of the University of Rhode Island
Graduate of the University of Rhode Island
Graduate of the University of Rhode Island
Jamie Coghlan, PharmDGraduate of Binghamton University
Graduate of the University of Rhode Island
Katelyn Choiniere, PharmD
PGY2 Ambulatory Care Pharmacy Residency Program
Morgan Felitte, PharmD
PGY2 Critical Care Pharmacy Residency Program
PGY2 Emergency Medicine Pharmacy Residency Program
PGY2 Oncology Pharmacy Residency Program
PGY2 Pediatrics Pharmacy Residency Program
Lauren Fortier, PharmD
Amanda Blais, PharmD
Abbigayle Fielder, PharmD
Ngan Nguyen, PharmD
Peyton Calvao, PharmD
Completed PGY1 residency at South County Hospital
Graduate of the University of Rhode Island
Completed PGY1 residency at the Brown Health Community-Based Residency Program
Graduate of the University of Rhode Island
Completed PGY1 residency at The Miriam Hospital
Graduate of the University of Rhode Island
Completed PGY1 residency at Rhode Island Hospital
Graduate of the University of Rhode Island
Completed PGY1 residency at Rhode Island Hospital
Graduate of the University of Houston
Completed PGY1 residency at Rhode Island Hospital
Graduate of Western New England University
Completed PGY1 Pharmacy Residency at Rhode Island Hospital

