BRIEF
Investing in Caregivers:
Low-Cost, High-Impact Strategies to Improve Child Development and Well-Being
Meena Ambati, Ayush Iyer, Merit Onyekwere, Rishi Shah, Yamato Takabe, Sheel Trivedi, Adam Tufts, Cara Kiernan Fallon, Catherine Panter-Brick, Felicity Brown, Joanna Lai
EXECUTIVE SUMMARY
When a child is born, caregivers are born too. As recognized in UNICEF’s Global Parenting Framework, caregivers are the primary, most significant, and consistent agents in a child’s development and wellbeing. Their essential role extends beyond early childhood, continuing through middle childhood and adolescence, fundamentally shaping their present and futures, with effects across generations. Every caregiver needs support to give their child the best start in life. In this way, caregiver mental health is a cornerstone of children’s development and long-term societal prosperity, yet it remains one of the most neglected determinants of population wellbeing in low- and middle-income countries (LMICs). When caregivers experience depression, anxiety, traumatic stress, or chronic stress, the effects extend far beyond the individual, influencing the quality of daily caregiving, household stability, and the environments in which children learn and grow. These early disruptions accumulate across childhood, influencing cognitive development, school readiness, emotional regulation, physical health, and ultimately adult relationships, productivity and economic mobility. Despite this, most health, education, and social protection systems do not address caregiver distress in a systematic way. Mental health screening is rarely embedded into routine antenatal, postnatal, or primary care visits.
The Nurturing Care Framework for Early Childhood Development (developed by UNICEF, WHO, and the World Bank) highlights five inter-related and indivisible components of nurturing care: good health, adequate nutrition, safety and security, responsive caregiving and opportunities for learning.37 Evidence shows that caregiver mental health affects all of these core components, in the early years and beyond:
• Health and nutrition practices such as breastfeeding, feeding routines, health-seeking behavior, and treatment adherence
• Emotionally responsive caregiving that supports language development, stress regulation, and socio-emotional skills
• Maintenance of safe, structured, and predictable home and learning environments.
The economic case for investment supports this sentiment. Globally, depression and anxiety cost over one trillion USD in lost productivity each year, with the
largest burdens falling on LMICs. Many countries lose billions annually to untreated perinatal mental illness, largely due to its impact on ability to provide nurturing care, with long-term consequences for children. Failing to invest in caregiver mental health is therefore not only a social and public health oversight, it is a costly economic error that undermines national development.
Cost-effective, scalable solutions already exist. Low-intensity psychosocial supports delivered by community health workers or peers, such as the WHO-endorsed Thinking Healthy Programme, demonstrate strong effectiveness at very low cost. Family-based interventions like Rwanda’s Bandebereho program show that shared caregiving and gender-equitable household dynamics reduce violence, strengthen relationships, and improve mental health for both parents. Social protection programs, including cash transfers and childcare subsidies, reduce chronic stressors that drive caregiver distress. Embedding these supports into existing health, education, and social systems increases feasibility, reach, and sustainability.
A family-centered, preventive, and system-integrated approach is not only cost-effective but essential for building healthier, more resilient caregivers and societies.
KEY INSIGHTS
Problem Overview:
• Caregivers are the primary, most significant, and consistent agents in a child’s development and wellbeing.
• Caregiver mental health is a major but often overlooked determinant of children’s cognitive, physical, and socio-emotional development.
• Depression, anxiety, traumatic stress, and chronic stress in caregivers directly affect daily caregiving practices, household stability, and children’s learning environments.
• These impacts accumulate across the life course, contributing to lower educational attainment, poorer health outcomes, and reduced economic mobility.
Urgency for Action:
• An estimated 250 million children in LMICs are at
risk of not reaching their developmental potential; caregiver distress is a major contributing factor.
• Early caregiver mental health problems create lifelong disadvantages, widening inequities and reinforcing intergenerational cycles of poverty.
• Poor caregiver mental health is linked to malnutrition, stunting, lower literacy and numeracy, behavioral problems, and diminished school readiness. Strengthening caregiver wellbeing supports national development by improving child outcomes, enhancing adult workforce participation, and reducing long-term public expenditures.
• Evidence shows cost-effective solutions already exist, making timely action feasible and efficient.
BACKGROUND
Addressing caregiver mental health in LMICs remains a persistent challenge as mental health screening is rarely integrated into primary care, and child
development and parenting programs often prioritize child outcomes only, while overlooking caregiver wellbeing as a major driver of these outcomes. Moreover, few countries systematically track caregiver mental health through national data systems, further contributing to a lack of investment in this area. In addition, existing social protection measures often fall short of addressing the underlying determinants of poor caregiver mental health.
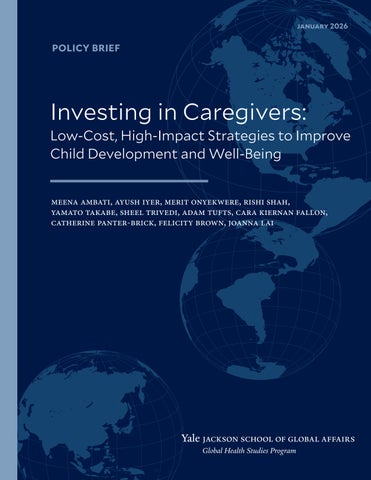
To develop effective strategies for supporting and investing in caregiver mental health, it is essential to understand how caregiver distress affects both caregivers and their children. The UNICEF socioecological model below illustrates how caregiver and child wellbeing are influenced by interconnected systems at individual, family, community, and societal levels (Figure 1). Applying this framework to inform strategy development requires careful consideration of: i) the links between caregiver mental health, caregiving practices, and child wellbeing; ii) broader community and societal factors impacting caregivers; iii) the economic burden of poor caregiver mental health and the cost-effectiveness of relevant interventions.
1
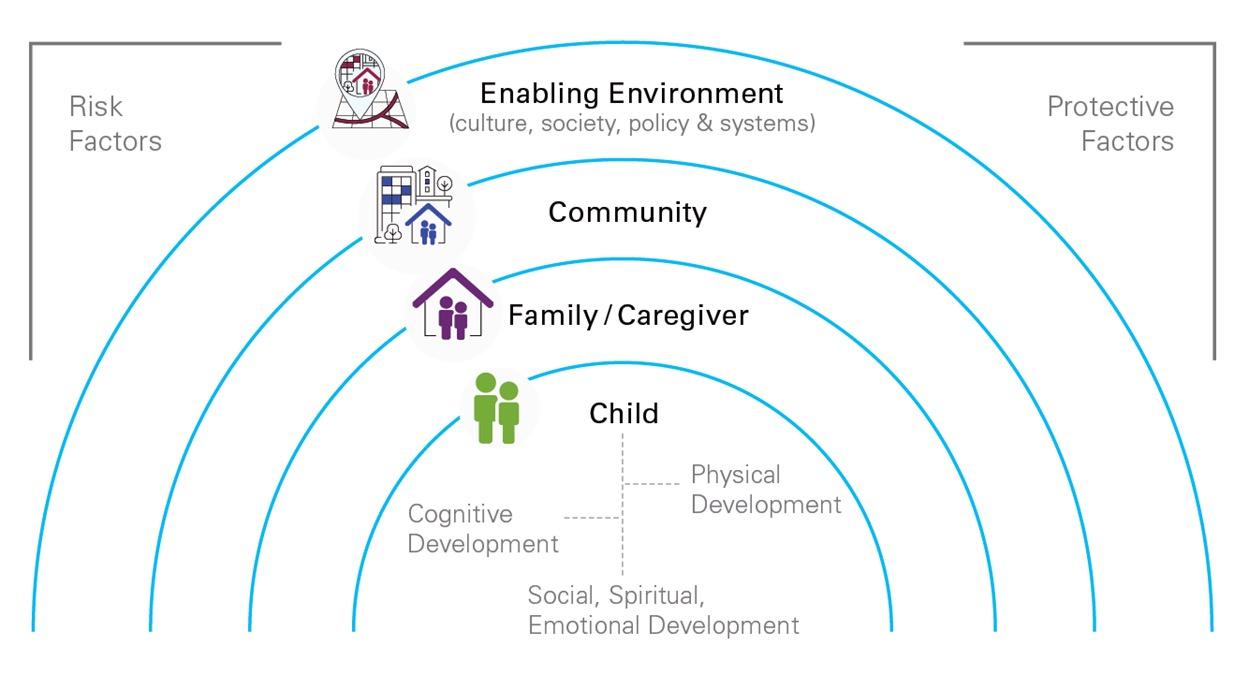
Figure 1: Socioecological model illustrating how child mental health is influenced by multiple nested systems (child, family/ caregiver, community, and the enabling environment), adapted from UNICEF’s MHPSS Operational Framework.1
Figure
IMPACT OF CAREGIVER MENTAL HEALTH ON CAREGIVING AND, ULTIMATELY, CHILD WELLBEING
Figure 2
Parenting Outcomes
Reduced ability to support their child’s health and nutrition
Reduced ability to offer emotionally nurturing care
Reduced ability to provide safe environments and relationships
Impaired cognitive outcomes (educational attainment, literacy, etc.) Child Wellbeing
Impaired social wellbeing and mental health outcomes
Impaired physical and mental health, relationship, employment, and financial outcomes as an adult
Impaired physical health outcomes
Figure 2. Pathways linking caregiver mental health to other parenting outcomes, child wellbeing, and adult outcomes. Illustration by authors.
IMPACTS OF POOR CAREGIVER MENTAL HEALTH ON CAREGIVING PRACTICES:
Caregiver mental health plays a decisive role in shaping how caregiving is carried out on a daily basis. Depression, anxiety, traumatic stress, and chronic stress affect caregivers’ emotional regulation, cognitive bandwidth, energy levels, and capacity for sustained attention, all of which are core psychological resources that nurturing caregiving depends upon. As a result, poor mental health leads to changes in routine behaviors, emotional interactions, and supervisory practices. Because these parenting patterns form the immediate environment in which children eat, learn, regulate emotion, and stay safe, disruptions constitute a primary pathway through which caregiver mental health ultimately affects child wellbeing and development (as conceptualized in Figure 2). The following
subsections examine the key domains in which these changes in parenting practices emerge.
I.
Impact on Caregiver’s Ability to Support Their Child’s
Health and Nutrition
Caregiver mental health affects the consistency and quality of routine caregiving tasks related to health and nutrition. For example, depressive symptoms reduce responsiveness and stamina during breastfeeding, making it harder to maintain structured routines or persist through common feeding challenges. This pattern is reflected in shorter breastfeeding durations; in one study’s cohort, mothers with depressive symptoms stopped exclusive breastfeeding nearly a month earlier on average (2.8 ± 2.1 months vs. 3.7 ± 2.0 months).2 Reduced patience, emotional withdrawal, and difficulty sustaining daily structure all contribute to irregular feeding and less responsive nutritional care.
Poor caregiver mental health
Mental health-related cognitive and emotional strain also influences how caregivers manage treatment plans of children requiring medical care. High parental stress is associated with a greater likelihood of missed doses, inconsistent administration, and lapses in medication routines.3 These challenges reflect the way emotional overload can disrupt day-to-day organizational tasks (timers, schedules, remembering instructions, following through) which are essential for routine health maintenance. When caregivers are overwhelmed or depleted, treatment routines become more fragmented, and adherence becomes significantly harder to sustain.
II. Impact on Caregiver’s Ability to Offer Emotionally Nurturing Care
Caregiver mental health strongly affects the tone, consistency, and quality of emotional engagement within the home. Depressive symptoms can increase irritability, reduce patience, and make consistent warmth more difficult to sustain. In one sample of 242 mother-child dyads, mothers with elevated depressive symptoms demonstrated more negative or conflictual interaction patterns.5 These shifts reflect how emotional exhaustion and internal distress constrain a caregiver’s ability to remain regulated, present, and responsive during everyday interactions. As mental health worsens, caregivers may withdraw more, react more abruptly, or struggle to maintain steady, nurturing communication. A particularly vulnerable group of caregivers is those caring for children with developmental or behavioral conditions, who face substantial stigma. Stigma frequently leads to shame and secrecy which further increase emotional isolation and intensify mental health challenges, leaving caregivers with fewer supports and less emotional bandwidth for positive engagement.4
III. Impact on Caregiver’s Ability to Foster a Safe and Attentive Environment
Caregiver mental health influences the reliability of supervision, the structure of daily routines, and the overall physical and emotional safety of the home environment. Parental mental health difficulties—including depression, emotional dysregulation, and other challenges—are linked to higher rates of supervisory lapses and household instability. In one dataset, neglect was associated with every major category of mental
health diagnosis for both mothers and fathers, with supervisory neglect particularly tied to paternal mental illness (16.7%).6 Emotional problems among caregivers also contributed to general household disorganization and increased the likelihood of educational neglect. These patterns reflect how mental health challenges can interfere with the attentiveness, consistency, and foresight that safe environments require. When caregivers experience substantial emotional strain, it becomes more difficult to maintain routines, track children’s whereabouts, anticipate hazards, and respond promptly to emerging risks. As internal burdens rise, external vigilance falls, reducing the structure and predictability that help keep children safe.
Poor caregiver mental health and high levels of distress increase the risk of harsh and violent discipline, which have clear detrimental impacts on children.39,40
A mediation analysis conducted on the outcomes of a randomised controlled trial of a parenting intervention conducted with over 500 families in South Africa found 4 pathways through which the programme reduced violence against children: improved parenting skills, caregiver mental health, reduced alcohol and drug use, and household economic wellbeing. These findings highlight the importance of addressing caregiver mental health as one of the key factors to reduce family violence.41
CAREGIVER PRACTICES IMPACT CHILD COGNITIVE, PHYSICAL, AND SOCIAL WELLBEING:
Across low- and middle-income countries (LMICs), a consistent body of evidence shows that when caregivers experience depression, anxiety, traumatic stress, or chronic stress, children face substantial and preventable disadvantages in learning, physical growth, and socio-emotional wellbeing. Crucially, these child outcomes do not arise in isolation but are mediated through the everyday caregiving behaviors previously described (feeding practices, emotional responsiveness, supervision, and engagement) that structure children’s daily environments. These effects emerge early, often in infancy, and compound throughout childhood, reinforcing cycles of poor educational attainment and reduced economic opportunity (Figure 2). As such, investing in caregiver wellbeing is both a moral and public health imperative.
I. Impact on Child’s Cognitive & Educational Attainment
Studies demonstrate that caregiver mental distress undermines a child’s early learning development, dampening both school readiness and later academic performance. In Ghana, for example, caregivers experiencing psychological distress have children who score significantly lower in literacy and numeracy.7 Critically, diminished parental engagement explains nearly one-quarter of this literacy gap.7 This mediating effect illustrates how mental health influences everyday interactions that are foundational for language and numeracy development, such as play, conversation, reading, and emotional attunement. Similar evidence from Peru8 and Vietnam9 shows that maternal depression predicts poorer early vocabulary skills, with effects that persist even after controlling for socioeconomic status. Longitudinal analyses from India and Vietnam further reveal that children of caregivers experiencing depression are more likely to score in the lowest quintile on standardized vocabulary tests, suggesting that the cognitive impacts of caregiver mental health extend through the primary school years.9 Indeed, evidence from Syrian refugee families shows that children benefit when caregiving adults, including fathers, are positively involved and coordinated in their roles, with measurable gains in social-emotional learning.10 These findings underscore that supporting caregivers’ psychological wellbeing enhances the quality of stimulation and learning support young children receive at home.
II. Impact on Child’s Physical Health
The effects on physical health and nutrition are equally pronounced. Caregiver depression and high stress levels disrupt critical determinants of infant growth and survival, such as feeding practices, health-seeking behavior, and consistent caregiving routines. A meta-analysis across ten LMICs shows that interventions addressing maternal mental health not only increase exclusive breastfeeding rates by nearly 40% but also modestly improve children’s heightfor-age by six months,11 demonstrating a pathway linking caregiver wellbeing to child growth. Additional systematic reviews reveal that infants of mothers experiencing depression have a 31% higher risk of adverse health outcomes, including a 39% greater risk of malnutrition, a 40% higher risk of stunting, and almost double the odds of common infectious illness-
es.12,13 Recent research further indicates that children of caregivers experiencing depression are 1.4 times more likely to be stunted and 1.5 times more likely to be underweight.25 These findings show that improving caregiver mental health is an essential strategy to reduce undernutrition, strengthen early health, and improve child survival.
III. Impact on Child’s Social and Emotional Wellbeing
Caregiver mental health also profoundly affects children’s emotional and behavioral development. In contexts marked by displacement or chronic stress, these intergenerational effects become particularly acute. Studies among refugee families demonstrate that caregiver post-traumatic stress is associated with harsher or less consistent parenting practices, which in turn heighten children’s emotional and behavioral difficulties.14 Importantly, post-traumatic stress also exerts a direct negative effect on children’s mental health independent of parenting style.14 In Uganda, for example, even small increases in caregiver depression symptoms more than triple adolescents’ odds of experiencing depression,15 highlighting the vulnerability of older children to parental stress exposure. Meta-analyses from LMICs show that young children whose caregivers experience depression, anxiety, or stress have nearly twice the odds of socio-emotional difficulties,16 reinforcing that caregiver wellbeing is a central determinant of children’s emotional resilience. Ultimately, these cognitive, physical, and socio-emotional impacts clarify that caregiver mental health and subsequent conduct are foundational to child development outcomes. Strengthening the wellbeing of the adults who care for children is essential to ensuring that children can learn, grow, and thrive.
RELATIONSHIP BETWEEN CAREGIVER MENTAL HEALTH AND ECONOMIC OUTCOMES
Figure 3
Figure 3. Long-term economic costs associated with inadequate support for children of mothers who experienced depression in the United Kingdom.17
MACROECONOMIC IMPACT OF POOR CAREGIVER MENTAL HEALTH:
The economic implications of caregiver mental health extend far beyond the private realm of families, shaping national productivity, labor market stability, and long-term economic growth. Globally, depression and anxiety cost the world economy over one trillion United States dollars in lost productivity each year, with around 80% of this burden concentrated in lowand middle-income countries (LMICs) where treatment access remains most constrained.18 The economic impact of caregiver poor mental health is particularly salient because it multiplies over time, shaping not only current labor output but also the next generation’s cognitive, physical, and social development. When caregiver mental health deteriorates, the effects extend outward—from reduced workforce participation to diminished educational attainment and weaker
long-term economic performance (Figure 3).18
The magnitude of this burden is staggering when examined at the national level. In South Africa, the lifetime cost of untreated perinatal depression and anxiety for a single annual birth cohort is estimated at 2.8 billion United States dollars, while in Brazil, it reaches nearly 4.9 billion United States dollars.20, 21 These figures capture the fiscal cost of lost productivity, poorer child development, and diminished economic mobility across a generation. Evidence from the United Kingdom shows that approximately 72% of the total cost of perinatal mental illness results from adverse outcomes in children rather than direct losses to caregivers, with similar results found in the United States.22, 23 Given the weaker safety nets in LMICs, this share is almost certainly higher, exacerbating the long-term economic damage of poor caregiver mental health.18
This erosion of human capital is a slow-moving crisis that silently constrains growth. An estimated
250 million children—43% of the child population living in LMICs—are at risk of not reaching their full developmental potential, and poor parental mental health is one of the most consistent predictors of this loss.19 Childhood stunting alone costs the private sector across 95 LMICs at least 135 billion United States dollars in sales annually.25 Such patterns embed inequality into the structure of the economy, lowering aggregate productivity for decades.
Ignoring caregiver mental health is therefore not a matter of social neglect but one of fiscal irresponsibility. Untreated parental mental illness depresses national output, corrodes the future workforce, and widens inequities that limit sustainable development. Protecting caregiver mental health is not a peripheral social goal but a central economic imperative for national stability and growth.
Wide-scale, cost-effective interventions are needed to protect caregiver mental health and reduce the long term burden on society, and available solutions exist. For example, the Thinking Healthy Programme (THP), developed by the World Health Organization (WHO) as part of the Mental Health Gap Action Programme (mhGAP), is a cognitive-behavioral therapy intervention that empowers community health workers to address symptoms of perinatal depression.27,28 A randomized control trial in Pakistan found an economic cost of as little as $2 for every family, for every degree of improvement in self-reported depression scores.29
MICROECONOMIC IMPACT OF POOR CAREGIVER MENTAL HEALTH:
Beyond national economic losses, caregiver mental health also carries direct financial implications for households. These financial burdens can translate to further heightened psychological stress for caregivers and substantial emotional and behavioral challenges for children and family members around them.26 This is even greater in LMICs, due to lower availability of government support and the relatively high cost of healthcare compared to the average income of an individual.
Economic and Policy-Level Interventions to Support Caregiver Mental Health
As illustrated in the socioecological model in Figure 1, community- and society-level influences on caregiver mental health cannot be ignored. Financial stressors have a significant detrimental impact on caregiver
mental health. Several cost-effective financial support policies have demonstrated a significant effect in reducing material hardship and improving both caregivers’ and children' s mental health outcomes on a regional and community level scale. Economic-focused interventions such as cash transfers can have positive effects on mental health outcomes. There is emerging evidence that this can be implemented in LMICs with substantial effects. An evaluation of the Malawi Social Cash Transfer Program—a national unconditional cash transfer program to support labor-constrained households—showed significantly improved mental health outcomes in children for the households that received the cash transfer versus those that did not.30 Providing funds can improve material wellbeing, reduce the need for youth to engage in work to support household income, and increase investment in education—all factors that improve mental health outcomes in children that can improve caregiver stress and life satisfaction. By alleviating financial pressure on households, cash transfers reduce chronic worry, improve daily functioning, and help caregivers instill a sense of control and dignity—key determinants of mental health.
In addition, UNICEF’s Family Friendly Policies Policy Brief outlines policies that must be in place across public and private sectors in order to provide caregivers with three key resources needed for caregivers and children to thrive: time, finances and services.38 Four evidence-based policies are advocated for in order to reduce parenting stress and promote wellbeing among caregivers: adequate paid parental leave, breastfeeding support, access to affordable childcare, child benefits and adequate wages.
These findings emphasize that supporting caregiver mental health is a public health priority and a cost-effective investment. Addressing caregiver mental health is imperative to support wellbeing, resilience, and development across the life course. Investment in strategies such as community-engaging validated behavioral programs, family friendly policies and cash transfers can reduce psychological distress amongst caregivers while improving their own and children’s emotional, cognitive, and educational outcomes. These programs are both scalable and robust in low-resource settings. Committing to such interventions for caregiver mental health is a cost-effective method for building communities that are healthier, happier, and hopeful.
CASE STUDY:
Bandebereho Intervention in Rwanda
The Bandebereho (“role model”) intervention in Rwanda is a highly effective couples’ program designed for expectant fathers and fathers of children under five. Between 2013 and 2015, the program engaged 1,199 couples across four districts and delivered a structured 15-session curriculum adapted from Program P. Sessions used participatory activities and facilitated group dialogue (some for men alone and others for couples) to challenge restrictive gender norms, strengthen communication and joint decision-making, promote men’s engagement in antenatal care, childbirth, and childcare, and build skills in non-violent conflict resolution, positive parenting, and equitable household roles. The curriculum explicitly addressed gender and power, fatherhood, intimate partner violence (IPV), caregiving, child development, and male involvement in maternal and reproductive health.
A randomized controlled trial demonstrated substantial improvements 21 months after baseline. Women reported a 63% reduction in the odds of physical IPV and a 66% reduction in the odds of sexual IPV.32 Both women and men reported lower use of physical punishment of children. The intervention significantly improved maternal health engagement, increasing women’s antenatal care attendance and raising the likelihood of male accompaniment by 50%. Importantly, the program shifted family dynamics: both partners reported increased male participation in childcare and household tasks and substantially reduced men’s dominance in household decision-making.
Six years later, both men and women had markedly lower odds of depressive symptoms and men were 75% less likely to report weekly excessive alcohol use. The long-term follow-up also found sustained reductions in IPV, with women reporting 45% lower odds of physical IPV, 50% lower odds of sexual IPV, and significantly lower odds of economic and emotional IPV. 34 Male accompaniment to antenatal care remained elevated, and men spent approximately 30 more minutes per day on childcare and household tasks. Decision-making also became more equitable, with significantly reduced male control over major household decisions.
Bandebereho offers a compelling demonstration that gender-transformative, family-based interventions can generate sustained reductions in violence, strengthen supportive couple and parenting practices, and improve caregiver mental health even in resource-constrained settings. By reducing the care-
giving and emotional burden placed on women and promoting shared responsibility within households, the program directly advances the policy brief’s call to shift from child-centered to family-centered models, promoting male engagement to improve the mental health of both caregivers. Bandebereho is now being scaled within Rwanda’s health system with support from the Rwanda Biomedical Centre, Rwanda Men’s Resource Centre, and Equimundo.
CASE STUDY:
Preschooler Mental Health in Brazil
In Embu das Artes, a city in Brazil’s São Paulo metropolitan area, the 2021 Brazilian Preschool Mental Health Survey was delivered to 1,292 children attending public preschools. Findings showed that one in four children aged 4-5 experienced internalizing disorders, while approximately one in eight exhibited externalizing disorders using the Child Behavior Checklist (CBCL). 30 Internalizing disorders included emotionally reactive behavior, anxiety/depression, somatic complaints, and withdrawn behavior.31 Externalizing disorders included attention problems and aggressive behavior.31 In addition, nearly one-third of surveyed preschoolers showed delays in socioemotional development according to the Ages and Stages Questionnaires: Social-Emotional (ASQ:SE)—rates 2 to 3 times higher than comparable populations in high-income countries.31
The survey also measured caregiver mental health in two ways: parental stress and parental psychopathology. Stress was measured using the Parental Stress Index, which classified parents into typical stress, high stress, or clinical stress categories. The data revealed a powerful connection between caregiver and child mental health.31 When parents reached clinical levels of distress, their children’s risk was 20 times higher for internalizing disorders and 40 times higher for externalizing disorders.31 Additionally, children whose caregivers experienced anxiety and/or depression showed approximately 3 times the rate of internalizing disorders and more than double the rate of externalizing disorders. This pattern persisted across socioemotional development as well.
These findings demonstrate that significant numbers of young children in urban Brazil are entering their educational journeys already struggling with emotional regulation, behavioral challenges, and developmental
concerns that threaten their future academic success. The parent-child correlation demonstrates a cascade effect: when parents lack adequate mental health support, their children’s developmental trajectories are compromised.
However, the researchers asserted that social networks can improve these outcomes. Children whose families had stronger social capital and social support networks showed lower rates of mental health problems.31 Neighborhood characteristics also impacted children, with those living in areas with higher social order facing decreased risks of internalizing disorders and socioemotional delays.31 These findings highlight how community connections function as protective factors for caregivers and their children.
The Brazilian context offers critical lessons for middle-income countries addressing similar challenges. Early identification proves crucial, as research demonstrates that mental health challenges begin well before school age. Since symptoms in preschoolers often persist into adolescence without intervention, universal preschool attendance in Brazil creates a potential infrastructure for screening and early intervention programs. Furthermore, since parental stress and mental health difficulties represent modifiable risk factors, multi-layered, family-centered interventions that support caregivers and teachers to provide quality care and encourage social support and nurturing communities, may significantly improve outcomes. The strong association between preschooler and caregiver mental health creates both urgency and opportunity for policy interventions to address mental health intergenerationally, rather than focus solely on children.
POLICY RECOMMENDATIONS
1) Act across the full socio-ecology of caregiving.
Evidence from both HICs and LMICs shows that caregiver mental health is a product of layered influences spanning the individual, family, social, and economic environment. Effective policy responses require coordinated action across these levels.
At the individual level, low-intensity psychosocial supports including brief structured interventions delivered by peers or non-specialist workers, such as Thinking Healthy, can reduce distress at a very low cost. These interventions work by strengthening coping skills, stress management, and emotional regulation.33
At the family level, interventions that encourage
shared caregiving and reduce the disproportionate burden on mothers can improve mental health of both mothers and fathers. The Bandebereho couples’ intervention in Rwanda demonstrated that engaging fathers in caregiving through improved communication and reduced conflict and created safer emotional conditions for caregivers. Policies that encourage shared responsibility and gender-equitable caregiving reduce mental health risk at its roots rather than responding after harm has occurred.32
At the social level, community-based group programming, peer networks, faith-based initiatives, and school-linked caregiver support can provide a buffer to caregiving stress and reduce isolation, especially in urban settings where social fragmentation is common.31
At the economic and policy level, cash transfers, access to affordable quality childcare, flexible work policies, breastfeeding support, and paid parental leave can reduce background stressors like income instability and the dual responsibility burden of work and family that place caregivers at an elevated mental health risk.29,38
2) Embed caregiver mental health support into existing systems.
Standalone mental health programs are often costly, more difficult to access, and challenging to scale. In contrast, embedding caregiver mental health supports into systems that families already use can increase feasibility and sustainability and more adequately reflect intersectoral responsibilities and opportunities for supporting caregiver mental health. For example, brief mental health check-ins can be incorporated into antenatal care, postnatal visits, child vaccination days, and growth monitoring appointments. These routine touchpoints allow early identification of distress without requiring caregivers to seek out specialized services. Within education systems, schools can serve as platforms for caregiver engagement and stress management education. Teachers and school counselors often detect early signs of caregiver strain that affect children’s learning and behavior. Within social services, frontline workers can link caregivers to community support or economic programs. Embedding mental health into existing caregiving infrastructure would avoid creating parallel systems that compete for limited resources.
3) Shift from crisis response to prevention.
Low-intensity prevention programs, group-based supports, and stress-management tools can be deliv-
ered at scale to large populations of caregivers. The Brazil case study shows that caregiver distress strongly predicts child mental health outcomes even at early developmental stages, underscoring the importance of intervening upstream. Prevention reduces later reliance on specialized services, improves caregiver function ing, and protects the child’s long-term development.
4) Prioritize proven cost-effective delivery methods.
Cost remains one of the most significant barriers to scaling caregiver mental health interventions; however, emerging evidence demonstrates that cost-effective solutions can and do exist. A technology-assisted, peer-delivered version of Thinking Healthy interven tion delivered in Pakistan showed lower per-patient costs than the standard delivery model. Implementers achieved comparable improvements in a health-related quality of life metric through task-sharing and digital tools to reduce labor and supervision costs while ex panding peer support.33
Community-based and family-centered interven tions such as Bandebereho in Rwanda achieved longterm improvement in violence reduction, caregiving en gagement, and family functioning. Because they don’t rely on specialist mental health professionals, they are cost-effective and potentially scalable models. These delivery models align with health system realities in LMICs where the mental health specialist workforce capacity is limited and workload is already high.

SUMMARY OF POLICY RECOMMENDATIONS
• Invest across the individual, family, social, and economic layers of caregiver support rather than relying on isolated clinical services.
• Embed mental health check-ins and caregiver supports into existing health, education, and social systems to increase feasibility and reach.
• Prioritize prevention through low-intensity, early interventions that identify caregiver distress before it reaches clinical levels.
• Scale cost-effective delivery models such as task-shared, peer-led, and digital interventions that work in low-resource settings.
Figure 4. Photo Credit © UNICEF/UN0241775/Dejongh.42
CONCLUSION
This policy brief argues for a fundamental shift in how caregiver mental health must be understood and addressed. First, it calls for a transition from a predominantly child- or adolescent-centered model toward a family-centered approach that recognizes caregivers as the foundation of early development. Evidence from LMICs demonstrates that when caregivers’ mental health is not supported, children’s emotional, behavioral, and developmental outcomes are directly affected. Supporting caregivers is therefore vital to child wellbeing, not ancillary to it. These family-centred approaches extend beyond the mother-baby dyad, and even beyond the mother-father-baby triad. Caregiving is rooted in relational systems that involve multiple adults, siblings, and extended kin, as highlighted in empirical work on coparenting systems and in global reviews of father engagement in parenting interventions.35,36
Second, the brief advocates for more preventive
HOW TO CITE
support, as most caregivers experience distress long before clinical thresholds are reached. Prevention through low-intensity psychosocial support, community connection, and family-friendly policies offers a more efficient strategy that is economically prudent, given the substantial productivity losses and longterm human capital costs associated with untreated caregiver distress.
Finally, this brief encourages shared responsibility within families. Caregiver mental health must be positioned as a societal and policy priority rather than a private burden on mothers alone. Health systems, workplaces, schools, and communities all determine children’s environments and so when these systems align around caregiver wellbeing, the benefits ripple outward to society at-large and national development.
Investing in caregiver mental health is a moral imperative and a practical, cost-effective strategy for promoting child wellbeing, stronger families, and resilient societies.
Ambati M1, Iyer A1, Onyekwere M1, Shah R1, Takabe Y1, Trivedi S1, Tufts A1, Fallon C1, Panter-Brick C1, Brown F2, Lai J2
1. Jackson School of Global Affairs, Global Health Studies Program
2. UNICEF, Mental Health and Psychosocial Support (MHPSS)
REFERENCES
1. United Nations Children’s Fund. (2021). Global multisectoral operational framework for mental health and psychosocial support of children and families across settings (Field demonstration version). New York, UNICEF.
2. Chee Din, M. A., Mohd Fahmi Teng, N. I., & Abdul Manaf, Z. (2023). Maternal depression and child feeding practices: Determinants to malnutrition among young children in Malaysian rural area. Women’s Health, 19, 174550572211478. https://doi.org/10.1177/17455057221147800
3. Theall, L., Ninan, A., Arbeau, K., Mannone, J., & Stewart, S. L. (2022). Interrupting the Cycle: Association of Parental Stress and Child/Youth Psychotropic Medication Nonadherence. Child Psychiatry & Human Development https://doi. org/10.1007/s10578-022-01448-y
4. Tilahun, D., Hanlon, C., Fekadu, A., Tekola, B., Baheretibeb, Y., & Hoekstra, R. A. (2016). Stigma, explanatory models and unmet needs of caregivers of children with developmental disorders in a low-income African country: a crosssectional facility-based survey. BMC Health Services Research, 16(1). https://doi.org/10.1186/s12913-016-1383-9
5. Lim, J., Wood, B. L., & Miller, B. D. (2008). Maternal depression and parenting in relation to child internalizing symptoms and asthma disease activity. Journal of Family Psychology, 22(2), 264–273. https://doi.org/10.1037/08933200.22.2.264
6. Ben David, V. (2021). Associations between Parental Mental Health and Child Maltreatment: The Importance of Family Characteristics. Social Sciences, 10(6), 190. https://doi.org/10.3390/socsci10060190
7. Ahun, M. N., Appiah, R., Aurino, E., & Wolf, S. (2024). Caregiver mental health and school-aged children’s academic and socioemotional outcomes: Examining associations and mediators in northern Ghana. PLOS Global Public Health, 4(9). https://doi.org/10.1371/journal.pgph.000372
8. Bendini, M., & Dinarte, L. (2020). Does maternal depression undermine childhood cognitive development? evidence from the Young Lives Survey in Peru. International Journal of Environmental Research and Public Health, 17(19), 7248. https://doi.org/10.3390/ijerph17197248
9. Bennett, I. M., Schott, W., Krutikova, S., & Behrman, J. R. (2015). Maternal Mental Health, and child growth and development, in four low-income and middle-income countries. Journal of Epidemiology and Community Health, 70(2), 168–173. https://doi.org/10.1136/jech-2014-205311
10. Hadfield K, Al-Soleiti M, Dajani R, Marechal I, Panter-Brick C. (2024). Father involvement, mental health, and child social emotional learning: Evidence from Syrian refugees in Jordan. Journal of Child and Family Studies 33:10291042. https://doi.org/10.1007/s10826-024-02809-y
11. Tol, W. A., Greene, M. C., Lasater, M. E., Le Roch, K., Bizouerne, C., Purgato, M., Tomlinson, M., & Barbui, C. (2020). Impact of maternal mental health interventions on child-related outcomes in low- and middle-income countries: A systematic review and meta-analysis. Epidemiology and Psychiatric Sciences, 29. https://doi.org/10.1017/ s2045796020000864
12. Dadi, A. F., Miller, E. R., & Mwanri, L. (2020). Postnatal depression and its association with adverse infant health outcomes in low- and middle-income countries: A systematic review and meta-analysis. BMC Pregnancy and Childbirth, 20(1). https://doi.org/10.1186/s12884-020-03092-7
13. Mekuriaw, B. Y., Getnet, B., Seid, E., Teferi, T., Alemwork, A., Aschale, M., & Tsega, A. (2025). Prevalence and associated factors of psychological distress among caregivers of children with malnutrition: A cross-sectional study. BMC Public Health, 25(1). https://doi.org/10.1186/s12889-025-21692-w
14. Bryant, R. A., Edwards, B., Creamer, M., O’Donnell, M., Forbes, D., Felmingham, K. L., Silove, D., Steel, Z., Nickerson, A., McFarlane, A. C., Van Hooff, M., & Hadzi-Pavlovic, D. (2018). The effect of post-traumatic stress disorder on refugees’ parenting and their children’s Mental Health: A Cohort Study. The Lancet Public Health, 3(5). https://doi.org/10.1016/s2468-2667(18)30051-3
15. Meyer, S. R., Steinhaus, M., Bangirana, C., Onyango-Mangen, P., & Stark, L. (2017). The influence of Caregiver depression on adolescent mental health outcomes: Findings from refugee settlements in Uganda. BMC Psychiatry, 17(1). https://doi.org/10.1186/s12888-017-1566-x
16. Honda, T., Tran, T., Popplestone, S., Draper, C. E., Yousafzai, A. K., Romero, L., & Fisher, J. (2023). Parents’ mental health and the social-emotional development of their children aged between 24 and 59 months in low-and middleincome countries: A systematic review and meta-analyses. SSM - Mental Health, 3, 100197. https://doi.org/10.1016/j. ssmmh.2023.100197
17. Jon Franklin. (2022). Breaking the cycle: The economic cost of poor parental mental health. https://www. caringtogether.org/wp-content/uploads/2022/05/Our-Time-Breaking-the-Cycle-the-economic-cost-of-poor-parentalmental-health-May-2022.pdf
18. World Health Organization & World Bank. (2016). Out of the shadows: Making mental health a global development priority. World Health Organization.
19. Black, M. M., Walker, S. P., Fernald, L. C. H., Andersen, C. T., DiGirolamo, A. M., Lu, C., McCoy, D. C., Fink, G., Shawar, Y. R., Shiffman, J., Devercelli, A. E., Wodon, Q. T., Vargas-Barón, E., Grantham-McGregor, S., & Lancet Early Childhood Development Series Steering Committee (2017). Early childhood development coming of age: science through the life course. Lancet, 389(10064), 77–90. https://doi.org/10.1016/S0140-6736(16)31389-7
20. Bauer, A., Garman, E., Besada, D., Field, S., Knapp, M., & Honikman, S. (2022). Costs of common perinatal mental health problems in South Africa. Global mental health, 9, 429–438. https://doi.org/10.1017/gmh.2022.48
21. Bauer, A., Knapp, M., Matijasevich, A., Osório, A., & de Paula, C. S. (2022). The lifetime costs of perinatal depression and anxiety in Brazil. Journal of affective disorders, 319, 361–369. https://doi.org/10.1016/j.jad.2022.09.102
22. Bauer, A., Parsonage, M., Knapp, M., Iemmi, V., & Adelaja, B. (2014). The costs of perinatal mental health problems. Centre for Mental Health and London School of Economics and Political Science https://www.centreformentalhealth. org.uk/publications/costs-perinatal-mental-health-problems
23. Luca, D. L., Margiotta, C., Staatz, C., Garlow, E., Christensen, A., & Zivin, K. (2020). Financial Toll of Untreated Perinatal Mood and Anxiety Disorders Among 2017 Births in the United States. American Journal of Public Health, 110(6), 888–896. https://doi.org/10.2105/AJPH.2020.305619
24. Surkan, P. J., Kennedy, C. E., Hurley, K. M., & Black, M. M. (2011). Maternal depression and early childhood growth in developing countries: systematic review and meta-analysis. Bulletin of the World Health Organization, 89(8), 608–615. https://doi.org/10.2471/BLT.11.088187
25. Akseer, N., Tasic, H., Nnachebe Onah, M., Wigle, J., Rajakumar, R., Sanchez-Hernandez, D., Akuoku, J., Black, R. E., Horta, B. L., Nwuneli, N., Shine, R., Wazny, K., Japra, N., Shekar, M., & Hoddinott, J. (2022). Economic costs of childhood stunting to the private sector in low- and middle-income countries. EClinicalMedicine, 45, 101320. https:// doi.org/10.1016/j.eclinm.2022.101320
26. Chen, J. H., Helton, J. J., Chiang, C. J., Wu, C. F., Jonson-Reid, M., & Drake, B. (2025). Breaking the cycle between caregiver mental health and child behavioral issues: Does food insecurity matter? Social science & medicine, 364, 117488. https://doi.org/10.1016/j.socscimed.2024.117488
27. World Health Organization. (2015). Thinking Healthy: A manual for psychological management of perinatal depression (WHO Reference No. WHO/MSD/MER/15.1). https://www.who.int/publications/i/item/WHO-MSD-MER-15.1
28. World Health Organization. Mental Health Gap Action Programme (mhGAP). https://www.who.int/teams/mentalhealth-and-substance-use/treatment-care/mental-health-gap-action-programme
29. Sikander, S., Ahmad, I., Atif, N., Zaidi, A., Vanobberghen, F., Weiss, H. A., Nisar, A., Tabana, H., Ain, Q. U., Bibi, A., Bilal, S., Bibi, T., Liaqat, R., Sharif, M., Zulfiqar, S., Fuhr, D. C., Price, L. N., Patel, V., & Rahman, A. (2019). Delivering the Thinking Healthy Programme for perinatal depression through volunteer peers: a cluster randomised controlled trial in Pakistan. The Lancet Psychiatry, 6(2), 128–139. https://doi.org/10.1016/s2215-0366(18)30467-x
30. Angeles, G., de Hoop, J., Handa, S., Kilburn, K., Milazzo, A., & Peterman, A. (2019). Government of Malawi’s
unconditional cash transfer improves youth mental health. Social Science & Medicine, 225, 108–119. https://doi. org/10.1016/j.socscimed.2019.01.037
31. Caetano, S. C., Ribeiro, M. V. V., Askari, M. S., Sanchez, Z. M., do Rosário, M. C., Perissinoto, J., Resegue, R., Felix, E., Mariano, M., Fidalgo, T. M., Caetano, M., Mari, J. J., Surkan, P. J., & Martins, S. S. (2021). An epidemiological study of childhood development in an urban setting in Brazil. Revista brasileira de psiquiatria, 43(1), 43–54. doi: 10.1590/1516-4446-2020-0934
32. Doyle, K., Levtov, R. G., Barker, G., Bastianı, G. G., Bingenheimer, J. B., Kazimbaya, S., et al. (2018). Gendertransformative Bandebereho couples’ intervention to promote male engagement in reproductive and maternal health and violence prevention in Rwanda: Findings from a randomized controlled trial. PLoS ONE, 13(4), e0192756. https:// doi.org/10.1371/journal.pone.0192756.
33. Gibbs, N. K., Chen, T., Malik, A., Nazir, H., Nisar, A., Waqas, A., Atif, N., Wang, D., Rahman, A., Sikander, S., & Walker, S. M. (2025). Cost-effectiveness of a technology-assisted peer-delivered perinatal mental health intervention in Pakistan: an economic evaluation using trial evidence. BMJ global health, 10(11), e020833. https://doi.org/10.1136/ bmjgh-2025-020833
34. Doyle, K., Levtov, R. G., Bingenheimer, J. B., Nzabonimpa, A., Sayinzoga, F., & Shattuck, D. (2023). Long-term impacts of the Bandebereho programme on violence against women and children, maternal health-seeking, and couple relations in Rwanda: A six-year follow-up of a randomised controlled trial. eClinicalMedicine, 64, 102282. https://doi. org/10.1016/j.eclinm.2023.102282
35. Panter-Brick, C., Burgess, A., Eggerman, M., McAllister, F., Pruett, K., & Leckman, J. F. (2014). Practitioner review: Engaging fathers--recommendations for a game change in parenting interventions based on a systematic review of the global evidence. Journal of child psychology and psychiatry, and allied disciplines, 55(11), 1187–1212. https://doi. org/10.1111/jcpp.12280
36. Sadruddin, A. F. A., Ponguta, L. A., Zonderman, A. L., Wiley, K. S., Grimshaw, A., & Panter-Brick, C. (2019). How do grandparents influence child health and development? A systematic review. Social science & medicine, 239, 112476. https://doi.org/10.1016/j.socscimed.2019.112476
37. World Health Organization, UNICEF, World Bank Group (n.d.). Nurturing Care For Early Childhood Development, https://nurturing-care.org/what-is-nurturing-care/
38. UNICEF. (2019). Family-Friendly Policies: Redesigning the Workplace of the Future, Policy Brief. https://www.unicef. org/sites/default/files/2019-07/UNICEF-policy-brief-family-friendly-policies-2019.pdf
39. Sim, A., Bowes, L., Gardner, F. (2018). Modeling the effects of war exposure and daily stressors on maternal mental health, parenting, and child psychosocial adjustment: a cross-sectional study with Syrian refugees in Lebanon. Glob Ment Health 4 no.5 e40. doi: 10.1017/gmh.2018.33.
40. Bryant, R.A., Edwards, B., Creamer, M., O’Donnell, M., Forbes, D., Felmingham, K.L., Silove, D., Steel, Z., Nickerson, A., McFarlane, A.C., Van Hooff, M., Hadzi-Pavlovic, D. (2018). The effect of post-traumatic stress disorder on refugees’ parenting and their children’s mental health: a cohort study. Lancet Public Health. 3(5):e249-e258. doi: 10.1016/S2468-2667(18)30051-3.
41. Cluver, L., Shenderovich, Y., Meinck, F., Berezin, M.N., Doubt, J., Ward, C.L., Parra-Cardona, J., Lombard, C., Lachman, J.M., Wittesaele, C., Wessels, I., Gardner, F., Steinert, J.I. (2020). Parenting, mental health and economic pathways to prevention of violence against children in South Africa, Social Science & Medicine, 262 (113194). https:// doi.org/10.1016/j.socscimed.2020.113194.
42. Photo Credit: UNICEF, UN0241775, Dejongh.