This publication is available digitally at https://isass.org/category/news/ vertebral-columns/
From the ¹Department of Orthopaedic Surgery at Rush University Medical Center in Chicago, Illinois, and ²Drexel University College of Medicine in Philadelphia, Pennsylvania.
Ergonomic Considerations in Spine Surgery
Protecting the Surgeon While Advancing Care
Spine surgery is physically demanding, placing surgeons at an increased risk for work-related musculoskeletal disorders (MSDs). Surgeons performing spine surgery are subject to repetitive motions, extended periods of stiff posture, and non-neutral positioning. Over time, these occupational stressors contribute to poor ergonomics, which can lead to overuse injuries, pain, need for medical or surgical treatment, loss of operative income, surgeon dissatisfaction, and potentially increase in medical errors. Ergonomics for spine surgeons remain poorly defined, leaving inconsistency in daily motions and an unavoidable pain that is accepted as part of operating. As surgical techniques evolve and the operative volume increases, recognizing the ergonomic risks and embedding practical protocols is essential for maintaining surgeon health, operational efficiency, and career longevity.1
Why Spine Surgeons Are at Risk
Spine surgery specifically requires forceful repetitive motions that are often done in mechanically disadvantageous positions. Common risk factors are prolonged gripping of instruments, repetitive hand motions,
cervical hyperflexion, forward trunk lean, and shoulder abduction. These positions place the operator’s joints in a non-neutral position. Thus, it can result in increased joint strain and injury. 2,3
Ergonomics is the scientific study of optimizing the interaction between individuals, their tools, and the working environment to reduce physical strain and improve efficiency. Despite the physically demanding nature of operative practice, formal ergonomic training remains uncommon in surgical education. Surveys indicate that more than 60% to 80% of surgeons report work-related musculoskeletal symptoms during their careers, highlighting the need for greater ergonomic awareness in surgical practice.1,2 In other industries, ergonomics have suggested adjustments for environments to decrease the body strain, yet surgeons rarely receive formal guidance on injury prevention. Like individuals in various workforces, occupational safety requires formal instruction.
Clinical literature and experience highlight that musculoskeletal pain is widely present among spine surgeons. Systematic reviews report that approximately 70% of orthopedic surgeons
Aimen A. Khan, BS1
Sehajvir Singh, BS2
Aryan Patel, BS1
Noah A. Pogonitz, BS1
Puranjay Gupta, BS1
Daniel K. Park, MD¹
Kern Singh, MD¹
experience work-related musculoskeletal pain, most commonly involving the neck (up to 59%), lower back (up to 49%), and shoulders (35%–40%).2 These overuse injuries are not just common in older surgeons but have been shown to begin early in training as well. Survey-based studies, including surgical trainees, report that approximately 70% of residents experience work-related musculoskeletal symptoms during training, suggesting that ergonomic strain begins early in operative exposure. 3 Furthermore, early in training, a surgeon may adopt certain positions and habits that feel comfortable but contribute to later symptoms consistent
with overuse and misuse of muscles (Figure 1).1-3 These injuries can be prevented early on with guidance on best practices for operating ergonomics. 3-6
To induce change, one must understand risk behavior that can contribute to these injuries. Several variable, identifiable factors have been shown to influence overuse injuries in spine surgeons.
Visualization: Loupes, Microscopes, and Monitors
Visualization modality plays a central role in musculoskeletal load and surgeon posture. Surgical loupes are a widely used tool
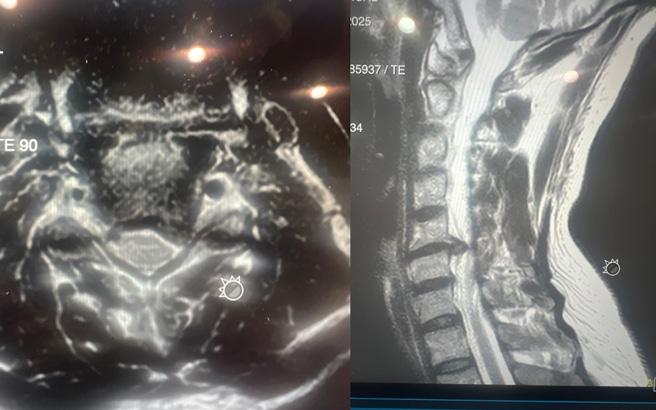
Figure 1. 40-year-old orthopedic spine surgeon with cervical radiculopathy involving the left upper extremity, resulting in sleep disturbance and eventual cervical disc replacement. The surgeon required time away from operative practice for recovery.
for magnification yet require frequent neck flexion. A prolonged downward gaze during loupe use may increase cervical loading and lead to further neck strain.7-9 Biomechanical analysis demonstrates that cervical flexion significantly increases mechanical load on the cervical spine. When the head is held in a neutral position, the cervical spine supports approximately 10–12 lb of load, whereas 30° of flexion increases this load to ~40 lb and 60° of flexion increases it to ~60 lb, illustrating how prolonged downward gaze during loupe use can substantially increase cervical strain during operative procedures. 5 Being mindful of neck extension and flexion while wearing loupes is a small adaptation that surgeons should use to minimize the strain on the cervical spine. 5,6 To aid in decreasing strain, a newer prismatic loupe has been designed aimed at promoting a neutral and aligned head position.
Another adaptation that minimizes neck strain but provides excellent visualization is the use of an operating microscope over surgical loupes. An operating microscope provides magnification and illumination in the operating room. However, poor usage of the microscope can aid in unfavorable ergonomics resulting in different overuse injuries.
Changing the eyepiece, height, and angle of the microscope can help minimize strain to the body. In lumbar surgery, specifically at L5-S1, where lordosis is pronounced, the microscope’s positioning can increase cervical and thoracolumbar strain if not adjusted to the surgeon’s height and preferences. A potential ergonomic intervention is adjusting
the head up or head down position, so the angle of the microscope is as perpendicular to the floor, so the surgeon’s body is in a relative upright position.
A last visualization aid that has ergonomic implications is the use of an exoscope or endoscope in spine surgery. These modalities allow surgeons to operate forward-facing positions with heads-up posture. With the monitor positioned exactly at eye level, the need for extensive cervical flexion is eliminated. Bigger screens and projections of the surgical field can also minimize eye strain on the surgeon. It should be noted, however, that improper monitoring placement can induce other strains to the body. If the body has to be turned or rotated to see the monitor, there can be undue strain on the torso and upper extremity. 8
Because each visualization technique results in different surgical postures for the surgeon, survey-based observation studies have showcased that some operations are associated with a different pain profile than others. For example, surgeons who primary operate with open techniques report higher neck pain than surgeons who primarily operate endoscopically.1,2
Operating Room and Ergonomic Optimization
Upper extremity symptoms are also frequently reported among spine surgeons. Survey-based studies have found that approximately 38% of surgeons report shoulder pain and 29% report hand or wrist symptoms, often attributed to repetitive instrument manipulation, sustained gripping, and
prolonged shoulder abduction during operative procedures. 2,12,13 Having an organized operating room setup allows the surgeon to smoothly maneuver throughout the surgery and plays a key role in mitigating ergonomic risks. Simple adjustments can meaningfully reduce progressive strain.
The operating table height should be adjusted to allow for relaxed shoulders and elbows near the torso. Positioning the table at or slightly above the umbilicus level helps reduce upper-extremity strain.7,11 Hand positioning should be maintained close to the body, minimizing sustained shoulder abduction and excessive wrist strain. A uniform and comfortable grip avoids unnecessary contraction and may help reduce fatigue in prolonged procedures. 8,12 Instrument design and positioning that reduces large shoulder and wrist movement can also play a key role in hand and upper extremity strain. Traditional pistol-grip instruments, in contrast to newer wishbone-style handles, allow for greater freedom of hand positioning and significantly less need for shoulder elevation and wrist tension when twisting in some endoscopic surgeries (Figure 2).12,13
Strategies for Improvement and Future Directions
The previous scenarios provide a glimpse in the varied scenarios that can make a substantial impact on surgeon health. Improving ergonomics in
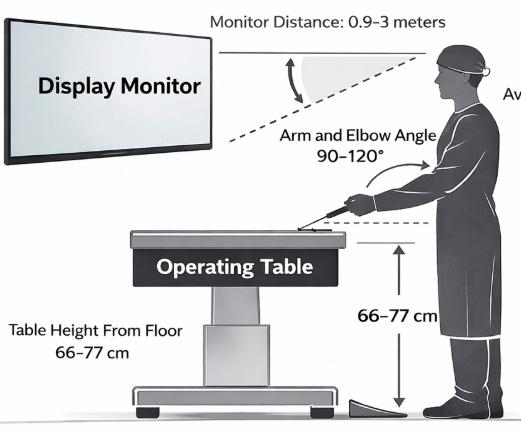
Figure 3. Ergonomic operating room setup for spine surgery. Schematic illustration demonstrating best practices: forward-facing monitor, relaxed shoulder position, optimal table height, and foot pedal placement. Image generated using artificial intelligence.
Figure 2. (A) Traditional pistol-grip instrument design. (B) Wishbone-style handle configuration designed to permit multiple hand positions and improved alignment.
spine surgery does not require abandoning established surgical techniques. However, by incorporating ergonomic principles early in surgical training, along with attention to operating room setup, allows surgeons to carry out best practices from the onset rather than attempting to modify technique after the onset of pain or injury (Figure 3).1 Ergonomic adjustments can be tailored to each surgical approach, including tubular, open, and endoscopic techniques. For example, in minimally invasive microscopic procedures, a key ergonomic change can be made through camera positioning, which can improve posture and reduce cervical flexion strain. As surgical techniques evolve and surgeons adopt new systems, maintaining consistent ergonomic principles may help the surgeon remain aligned in posture while
References
1. Kolz JM, Wagner SC, Vaccaro AR, Sebastian AS. Ergonomics in spine surgery. Clin Spine Surg. 2022;35(8):333-340.
2. Vasireddi N, Vasireddi N, Shah AK, et al. High prevalence of work-related musculoskeletal disorders and limited evidence-based ergonomics in orthopaedic surgery: a systematic review. Clin Orthop Relat Res . 2024;482(4):659-671.
3. Riccio A, Entezami P, Bishop A, Carl A. Debility among spinal surgeons. World Neurosurg. 2020;141:e254-e260.
4. Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153(2):e174947.
5. Hansraj KK. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int . 2014;25:277-279.
confidently adapting to new workflows. 6,13 Education and awareness of overuse injuries is paramount to prevent injury.
Conclusion
Surgeons face long-term stress through poor ergonomic positioning while operating. Healthy ergonomic guides for seated work environments apply similarly to standing surgeons. Clinical experiences, survey-based analyses, and biomechanical studies showcase that proper operating room setup allows surgeons to naturally adhere to best ergonomic practices and reduce meaningful musculoskeletal risk.1 Implementing ergonomic practices into surgical training and operating room design can decrease longterm risk of injury and maintain surgical efficiency for high-quality patient care.6 l
6. Cerier E, Hu A, Goldring A, Rho M, Kulkarni SA. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res . 2022;280:567574. doi:10.1016/j.jss.2022.06.014
7. Park JY, Kim KH, Kuh SU, Chin DK, Kim KS, Cho YE. Spine surgeon’s kinematics during discectomy according to operating table height and the methods to visualize the surgical field. Eur Spine J. 2012;21(12):2704-2712.
8. Park JY, Kim KH, Kuh SU, et al. Spine surgeon’s kinematics during discectomy, part II: operating table height and visualization methods including microscope. Eur Spine J. 2014;23:1067–1076.
9. Fisher SM, Teven CM, Song DH. Ergonomics in the operating room: the cervicospinal health of today’s surgeons. Plast Reconstr Surg. 2018;142(5):1380-1387.
10. Fan X, Yang L, Young N, Kaner I, Kjellman M, Forsman M. Ergonomics and
performance of using prismatic loupes in simulated surgical tasks among surgeons - a randomized controlled, cross-over trial. Front Public Health. 2024;11:1257365.
11. Janki S, Mulder EEAP, IJzermans JNM, Tran TCK. Ergonomics in the operating room. Surg Endosc . 2017;31(6):2457-2466.
12. Alaqeel M, Tanzer M. Improving ergonomics in the operating room for orthopaedic surgeons in order to reduce work-related musculoskeletal injuries. Ann Med Surg (Lond). 2020;56:133-138.
13. Schupper AJ, Hrabarchuk EI, McCarthy L, Hadjipanayis CG. Improving surgeon well-being: ergonomics in neurosurgery. World Neurosurg. 2023;175:e1220-e1225.
From the Department of Orthopaedic Surgery at Rush University Medical Center in Chicago, Illinois.
Osteolysis:
A Long-Term Risk of Cervical Arthroplasty
Cervical disc arthroplasty has emerged as an increasingly adopted alternative to anterior cervical discectomy and fusion. However, unlike fusion, which represents a biological endpoint, arthroplasty introduces a permanent mechanical interface that must remain biologically compatible with host bone for decades. As indications have expanded and younger patients receive these implants, attention has increasingly turned toward the long-term biological interaction between cervical disc prostheses and host bone. One complication that has emerged in longer follow-up studies, yet remains incompletely understood, is periprosthetic osteolysis.
Importantly, several distinct biological processes are often grouped under the term “osteolysis.” Early postoperative bone loss, often seen within the first 3–6 months, represents adaptive remodeling secondary to altered load transfer, endplate vascular disruption, or minor implant micromotion. This phenomenon is typically nonprogressive and clinically silent.1,2 True osteolysis, however, appears to represent a particle-mediated inflammatory process that may emerge years after implantation and demonstrate
progressive bone resorption at the bone–implant interface.
Mechanism of Wear-Induced Osteolysis
The biologic mechanism underlying wear-related osteolysis parallels the particle-mediated responses more extensively described in hip and knee arthroplasty over the past 2 decades. Macrophage activation leads to the release of pro-inflammatory cytokines, including tumor necrosis factor- α (TNF- α), interleukin-1 β (IL-1 β), and interleukin-6 (IL-6). These mediators promote osteoclast differentiation through activation of the RANK/RANKL signaling pathway, which represents the central molecular driver of particle-mediated osteolysis in orthopedic arthroplasty. 3–6 Activated osteoclasts subsequently resorb periprosthetic trabecular bone, resulting in progressive radiographic lucency and weakening of the bone–implant interface. Histopathologic analysis of revision cases has demonstrated foreign-body granulomatous reactions, which are characterized by macrophages and multinucleated giant cells surrounding particulate debris. Polymer fragments, metal particles, and ceramic debris have been identified within macrophages at the bone–implant interface, further supporting a particle-mediated inflammatory mechanism like that observed in large-joint arthroplasty.7
Mattin Moazzam, BS
Aditya Mazmudar, MD, MBA
Arash Sayari, MD
Mechanical factors may further amplify this biologic process. Implant micromotion, incomplete osseointegration, or mismatch between prosthetic endplates and vertebral body anatomy can generate repetitive instability at the bone–implant interface. This instability may increase wear particle generation while simultaneously impairing bone healing, creating a self-perpetuating cycle of debris formation and inflammatory osteolysis. 2
Device-Specific Patterns and Incidence
The incidence of osteolysis following cervical disc arthroplasty appears to vary across implant designs and has been reported to be as high as 64%, likely reflecting differences in bearing surface materials, implant architecture, and load transfer characteristics rather than a single uniform mechanism. 2 Cervical arthroplasty devices can broadly be categorized according to their articulating surfaces, including metal-on-metal, metal-on-polymer, and viscoelastic or polymer-core constructs, each of which introduces distinct wear characteristics that may influence the long-term biologic response of the vertebral body. Greater variability exists when examining individual implants. For example, the M6-C artificial disc manufactured by Orthofix, which utilized an ultra-high-molecular-weight polyethylene core, was associated with a 34% revision rate at an average of 67 months (about 5 and a half years) owing to wear-related osteolysis in one series.7 Reports exist describing polyetheretherketone
(PEEK)-on-ceramic design wear and osteolysis, histologically linked to an inflammatory process. 8 Such analyses have suggested PEEK, titanium, and zirconia debris are linked to inflammatory reactions that may contribute to osteolysis. Metal-on-metal devices have shown radiographic bone loss as high as 52.8%, although most cases are nonprogressive. 9
In contrast, metal-on-polyethylene bearing devices have demonstrated lower rates of osteolysis but higher rates of heterotopic ossification (74%), a separate biologic response that may limit motion over time.10
These findings underscore that osteolysis is not uniform across designs and may reflect differences in bearing materials, fixation strategy, and load transfer. Further, many radiographic changes have gone undiagnosed as patients remain asymptomatic, and there has been inconsistent reporting differentiating osteolysis from other processes such as stress shielding. 9
Clinical Presentation and Diagnostic Challenges
Cervical osteolysis often is asymptomatic early on, thus delaying diagnosis.7,11 Radiographically, osteolysis may present as progressive radiolucent zones surrounding the implant endplates, focal vertebral body cavitation, or erosion extending into the posterior vertebral body. CT often provides superior characterization of bone loss.
Symptomatically, patients may present progressive neck pain or neurologic change related to implant subsidence or device migration. Such delays in diagnosis often lead
References
CERVICAL SPINE
to substantial bone loss limiting the ability of revising to another arthroplasty construct and require a fusion with or without a corpectomy.7
Regulatory and Surveillance Considerations
The discrepancy between controlled bench testing and long-term in vivo performance highlights inherent limitations in premarket device evaluation. Two-year FDA Investigational Device Exemption (IDE) trials, while essential for regulatory approval, are not designed to capture complications that manifest at 5–7 years or beyond. Independent registry analyses have at times reported higher complication rates than industry-sponsored IDE trials. For example, severe heterotopic ossification was reported at 21.6% in IDE studies versus 27.9% in independent investigations.12
1. Wahbeh JM, Park SH, Campbell P, Ebramzadeh E, Sangiorgio SN. The lexicon for periprosthetic bone loss versus osteolysis after cervical disc arthroplasty: a systematic review. Eur Spine J. 2022;31(4):830-842.
2. Joaquim AF, Lee NJ, Lehman RA, Tumialán LM, Riew KD. Osteolysis after cervical disc arthroplasty. Eur Spine J. 2020;29(11):2723-2733.
3. Green TR, Fisher J, Stone M, Wroblewski BM, Ingham E. Polyethylene particles of a “critical size” are necessary for the induction of cytokines by macrophages in vitro. Biomaterials . 1998;19(24):2297-2302.
4. Kaufman AM, Alabre CI, Rubash HE, Shanbhag AS. Human macrophage response to UHMWPE, TiAlV, CoCr, and alumina particles: analysis of multiple cytokines using protein arrays. J Biomed Mater Res A . 2008;84(2):464-474.
Such differences may reflect variations in follow-up duration, imaging protocols, or reporting methodology. These observations emphasize the importance of post-market surveillance and long-term follow-up by both companies and surgeons.
Conclusion
As cervical arthroplasty continues to expand into younger patient populations with decades of expected implant lifespan, understanding the long-term biological response to implant wear will become increasingly important. While osteolysis remains uncommon, its potential to compromise fixation and necessitate complex revision surgery underscores the need for continued surveillance, device design refinement, and thoughtful patient selection. l
5. Hallab NJ, McAllister K, Brady M, Jarman-Smith M. Macrophage reactivity to different polymers demonstrates particle size- and material-specific reactivity: PEEK-OPTIMA(®) particles versus UHMWPE particles in the submicron, micron, and 10 micron size ranges. J Biomed Mater Res B Appl Biomater. 2012;100(2):480-492.
6. Jämsen E, Pajarinen J, Kouri VP, et al. Tumor necrosis factor primes and metal particles activate the NLRP3 inflammasome in human primary macrophages. Acta Biomater. 2020;108:347-357.
7. Scott-Young M, Rathbone E, Grierson L. Midterm osteolysis-induced aseptic failure of the M6-CTM cervical total disc replacement secondary to polyethylene wear debris. Eur Spine J. 2022;31(5):1273-1282.
8. Scott-Young M, Blumenthal S, Lanman T, et al. Beyond the two-year trial: real-world failure mechanisms of the simplify cervical disc. Eur Spine J. 2026;35(2):499-509.
9. Wu TK, Liu H, Wang BY, et al. Incidence of bone loss after Prestige-LP cervical disc arthroplasty: a single-center retrospective study of 396 cases. Spine J. 2020;20(8):1219-1228.
10. Zhao Y, Zhou F, Sun Y, Pan S. Single-level cervical arthroplasty with ProDisc-C artificial disc: 10-year follow-up results in one centre. Eur Spine J. 2020;29(11):2670-2674.
11. Spece H, Khachatryan A, Phillips FM, et al. Clinical management of bone loss in cervical total disc arthroplasty: literature review and treatment recommendations. Eur Spine J. 2024;33(8):2969-2981.
12. Dowdell JE, Kim JS, Mikhail C, et al. The rate of heterotopic ossification following cervical disc arthroplasty: a systematic review and comparison of data. Spine . 2020;45(18):E1197-E1202.
Cryotherapy for Pain Control and Functional Recovery After Lumbar Spine Surgery
Postoperative pain heavily influences early recovery following spine surgery. Advances in minimally invasive techniques and perioperative analgesic strategies have dramatically improved patients’ ability to achieve early mobilization, improve patient satisfaction, and facilitate participation in rehabilitation. These issues are increasingly relevant as spine procedures shift toward outpatient or short- stay surgical pathways where rapid recovery and early ambulation are central goals.
Within modern perioperative care, multimodal analgesia strategies combine pharmacologic therapy, regional anesthesia techniques, and nonpharmacologic interventions. 1 Cryotherapy, the therapeutic application of cold to injured or surgically treated tissue, has long been used in sports medicine and orthopedic rehabilitation to reduce pain, swelling, and inflammation. Although it has been studied most extensively in large joint surgery, the mechanisms by which cryotherapy acts are also relevant to spinal surgery. 2 Because cryotherapy produces analgesic effects without systemic pharmacologic exposure, it has significant utility in enhanced recovery pathways focused on reducing opioid use.
Physiologic Mechanisms of Cryotherapy
The biologic rationale for cryotherapy in postoperative recovery centers on its ability to influence nociceptive signaling, inflammation, and tissue edema. Cooling peripheral tissues slows nerve conduction velocity within sensory fibers, reducing transmission of nociceptive signals to the central nervous system. Experimental physiologic studies demonstrate that reductions in tissue temperature produce measurable decreases in nerve conduction velocity and increase in both pain threshold and pain tolerance. 3 Cryotherapy also modulates the inflammatory response associated with surgical trauma. Tissue injury initiates the release of inflammatory mediators, including prostaglandins, cytokines, and bradykinin, which increase vascular permeability and contribute to edema and hyperalgesia. Localized cooling produces vasoconstriction and reduces metabolic activity in inflammatory cells, which may attenuate this response.4
A third mechanism relates to postoperative tissue swelling. Capillary permeability and interstitial fluid accumulation contribute to edema within injured soft tissues. By limiting this process, cryotherapy may reduce postoperative swelling and tissue pressure
Brandon Hirsch, MD
within muscular compartments. 5 In lumbar surgery patients, where paraspinal muscle trauma contributes to postoperative discomfort, this effect may meaningfully influence recovery (Figure 1).
Evidence From Orthopaedic Surgery
Large joint arthroplasty literature provides important insight into how cryotherapy may influence postoperative recovery. A Cochrane systematic review evaluating cryotherapy after total knee arthroplasty analyzed randomized and quasi-randomized trials comparing cold therapy with standard postoperative care. 2 Across studies, cryotherapy was associated with modest reductions in early postoperative pain and small improvements in knee range of motion during the first postoperative week. Several trials also demonstrated reductions in postoperative blood loss. Although the overall magnitude of benefit was modest, and study of heterogeneity was significant, the findings support the concept that localized cooling can influence early inflammatory recovery after major orthopedic procedures. Evidence from arthroscopic surgery provides additional support for the analgesic effects of cryotherapy. A recent systematic review and meta-analysis by Ekhtiari et al evaluated 21 randomized controlled trials involving 2,148 patients undergoing shoulder, knee, and hip arthroscopic procedures and examined several noninvasive strategies for postoperative pain control. 6 Across the included studies, cryotherapy was identified as one of several adjunctive modalities associated with improved postoperative pain control and reduced opioid consumption compared with standard care alone. Cryotherapy demonstrated consistent reductions in early postoperative pain scores and analgesic requirements, supporting its utility as a component of multimodal recovery protocols following arthroscopic procedures. Device design has also been investigated. Continuous cryotherapy systems attempt to
Figure 1. A lumbar cryotherapy device.
maintain stable cooling using circulating water devices. In a randomized evaluation of such systems after knee arthroplasty, Thienpont reported that advanced cryotherapy devices did not clearly outperform traditional ice therapy in terms of pain scores or early functional outcomes.7 These findings highlight that simple cooling protocols may provide similar physiologic benefit to more technologically complex systems.
Results From Spine-Specific Studies
Spine -specific literature suggests that cryotherapy produces measurable physiologic effects following lumbar surgery and may contribute to improved postoperative comfort. One important observation is that cryotherapy clearly alters local tissue physiology even when clinical pain differences are modest. In a study evaluating cryotherapy after lumbar decompression, Murata et al demonstrated a significant reduction in wound temperature at the operative site following application of cryotherapy. 8 Although postoperative pain scores were not significantly different between groups, the study confirmed that localized cooling effectively modifies the biologic environment of the surgical wound.
Clinical benefits may be more apparent in procedures involving greater tissue trauma. Multilevel posterior lumbar fusion procedures often involve substantial paraspinal muscle dissection and postoperative inflammation. In a randomized trial evaluating cryotherapy after posterior lumbar fusion, Quinlan et al reported reduced opioid consumption during the early postoperative peri-
“Patients treated with cryo‐compression therapy experienced lower postoperative pain scores and reduced analgesic requirements compared with those receiving conventional postoperative management.”
od among patients treated with localized cold therapy compared with controls receiving standard care. 9 Although pain score differences were modest, the reduction in opioid requirements suggests that cryotherapy may augment multimodal analgesia strategies in more invasive lumbar procedures. Control of postoperative swelling may represent an additional mechanism of benefit.
Nabıyev et al evaluated cryo - compression therapy combining localized cooling with intermittent mechanical compression after instrumented lumbar surgery. 10 Patients treated with cryo - compression therapy experienced lower postoperative pain scores and reduced analgesic requirements compared with those receiving conventional postoperative management. The authors proposed that the combination of cooling and compression may reduce both tissue temperature and paraspinal muscular edema following surgery.
Timing of cryotherapy effects may also be relevant. In a randomized prospective
References
PAIN MANAGEMENT
study, Akta ş et al found that pain scores during the first postoperative day were similar between groups but were significantly lower in patients receiving cryotherapy at 48 hours after surgery. 11 These findings suggest that cryotherapy may exert its greatest clinical effect during the inflammatory phase of postoperative recovery when tissue swelling and inflammatory mediator activity peak.
Discussion
Taken together, the available evidence suggests that cryotherapy may serve as a useful adjunct within multimodal postoperative recovery pathways for lumbar surgery. Although spine -specific studies remain small, they consistently demonstrate measurable physiologic effects and suggest potential reductions in opioid requirements and postoperative pain.
1. Fujii T, Kumar R, Lipson P, et al. Enhanced recovery after surgery protocol in patients with adult spinal deformity: a systematic review and meta-analysis. Global Spine J. 2025;15:3426–3438.
2. Aggarwal A, Adie S, Harris IA, et al. Cryotherapy following total knee replacement. Cochrane Database Syst Rev. 2025;10:CD007911.
3. Algafly AA, George KP. The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. Br J Sports Med. 2007;41:365–359.
4. Bleakley CM, Costello JT. Do thermal agents affect range of movement and mechanical properties in soft tissues? A systematic review. Br J Sports Med. 2013;47:242–8.
Procedures involving greater muscular dissection and soft-tissue trauma appear most likely to demonstrate clinically meaningful benefits. This observation aligns with the mechanisms of cryotherapy, which primarily influence inflammatory responses and tissue edema rather than structural sources of pain. Cryotherapy has the potential to speed up postoperative recovery after spine surgery by reducing inflammation, nociception, and narcotic requirements following lumbar spine surgery. Although current spine-specific evidence remains limited, available studies suggest that localized cooling may reduce postoperative pain, limit opioid consumption, and improve patient comfort during early recovery. Given its efficacy combined with its inherently minimal risk and cost, cryotherapy remains a vital component of multimodal postoperative care following modern spine surgery. l
5. Merrick MA. Secondary injury after musculoskeletal trauma: a review and update. J Athl Train. 2002;37:209–217.
6. Ekhtiari S, Nucci N, Uddin F, et al. Opioid-sparing strategies in arthroscopic surgery: a systematic review and meta-analysis of randomized controlled trials. JBJS Rev. 2023;11(7).
7. Thienpont E. Does advanced cryotherapy reduce pain and narcotic consumption after knee arthroplasty? Clin Orthop Relat Res. 2014;472:3417–3423.
8. Murata K, Yoshimoto M, Takebayashi T, et al. Effect of cryotherapy after spine surgery: wound temperature changes and clinical outcomes after microendoscopic lumbar decompression. Asian Spine J. 2014;8:753–758.
9. Quinlan P, Davis J, Fields K, et al. Effects of localized cold therapy on postoperative pain in patients following posterior lumbar spinal fusion. Spine (Phila Pa 1976). 2017;42:1649–1655.
10. Nabıyev VN, Ayhan S, Adhikari P, et al. Cryo-compression therapy after elective spinal surgery for pain management: a controlled comparison. Neurospine . 2018;15:348–352.
11. Aktaş YY, Durgun H, Durhan R. Cold therapy and the effect on pain and physiological parameters in patients recovering from spine surgery: a randomized prospective study. Complement Med Res . 2021;28:31–39.
From the Department of Orthopaedic Surgery, University of California, Davis, in Sacramento, California.
Nutritional Assessment in Adult Spinal Deformity:
Screening, Imaging Correlates, and Perioperative Optimization
Adult spinal deformity (ASD) surgery is among the most physiologically demanding procedures in spine surgery, with higher complication rates and less favorable outcomes compared to many other spine surgeries. As the ASD population increasingly consists of elderly and frail patients with multiple medical comorbidities, attention has shifted toward modifiable risk factors that may mitigate perioperative morbidity. Among these, nutritional status has emerged as a critical determinant
of perioperative and postoperative outcomes. Contemporary literature consistently demonstrates that malnutrition, particularly hypoalbuminemia and a low prognostic nutritional index (PNI), is independently associated with increased mortality, complications, transfusion requirements, and prolonged hospitalization after ASD surgery. Despite this growing body of evidence, standardized perioperative nutritional optimization protocols remain underdeveloped.
Hania Shahzad, MD
Audrey Zhao, BS
Hai V. Le, MD
Yashar Javidan, MD
Safdar N. Khan, MD
Wyatt Vander Voort, MD
Preoperative Nutritional Screening:
Serum Albumin, Prognostic
Nutritional Index (PNI), CONUT Score, Vitamin D, and Other Biomarkers
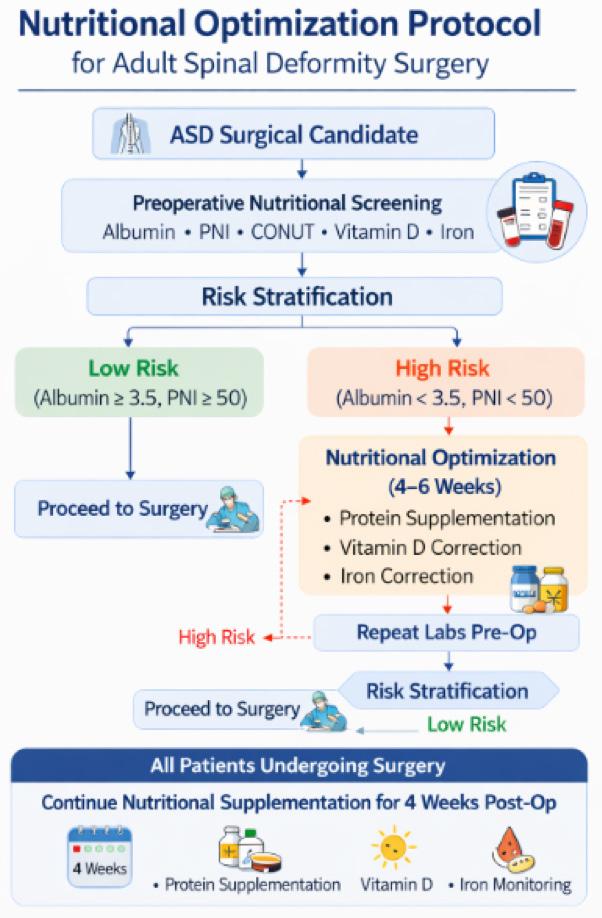
Patients undergoing ASD surgery should be screened preoperatively for malnutrition using objective laboratory markers and validated nutritional indices, as poor nutritional status is strongly associated with increased complications. Serum albumin remains the most widely used screening tool,1 with hypoalbuminemia, defined as <3.5 g/dL, consistently linked to longer hospital stays, higher transfusion rates, greater medical complications, and increased 90-day readmissions. 2,3 Beyond albumin alone, composite indices such as the Prognostic Nutritional Index (PNI), which is calculated from serum albumin and total lymphocyte count (PNI <50 indicating malnutrition), have demonstrated strong predictive value for postoperative complications, including cardiovascular events, blood loss, delayed recovery, and postoperative delirium.4,5 The Controlling Nutritional Status (CONUT) score, which incorporates albumin, lymphocyte count, and cholesterol levels, can further stratify malnutrition severity and has been associated with risks such as pneumonia, sepsis, pulmonary embolism, and major bleeding.6 However, its predictive value for delirium is less consistent than PNI. In clinical practice, patients with albumin <3.5 g/dL, PNI <50, or high CONUT scores (≥5-8) should be flagged for nutritional optimization prior to surgery to reduce perioperative morbidity, with recognition that larger studies are still needed to refine risk thersholds in ASD populations.
Beyond macronutrient markers, micronutrient deficiencies also play a meaningful role in ASD optimization. Hypovitaminosis D, defined as serum vitamin D less than 30 ng/mL, is common in elderly spinal deformity patients and has implications for bone metabolism, fusion success, and pseudarthrosis risk.7 All patients undergoing ASD surgery should have preoperative 25-hydroxyvitamin D levels checked. If deficient, correction with 50,000 IU vitamin D weekly for 8 weeks prior to surgery can optimize bone healing and fusion outcomes.
Preoperative nutritional assessment should extend beyond standard laboratory indices to include a thoughtful evaluation of caloric adequacy, anemia, and micronutrient status. Many elderly ASD patients exhibit subclinical malnutrition despite a normal or elevated BMI, and inadequate caloric intake has been associated with higher infection rates, delayed wound healing, and prolonged postoperative recovery. 2,8 Screening for anemia, including iron deficiency anemia, is equally important, as it has been linked to increased transfusion requirements, greater infection and thromboembolic risk, longer hospital stays, and impaired bone mineralization that may adversely affect fusion biology. 9 When identified, iron deficiency should be addressed through supplementation or erythropoietin analogs as appropriate. Assessment of vitamin B12 status may also be warranted, especially in older adults with polypharmacy or potential malabsorption, though ASD-specific outcome data remain limited.10
Imaging Findings Associated With Malnutrition
In patients undergoing adult spinal deformity surgery, imaging markers of malnutrition often manifest as radiographic evidence of sarcopenia, particularly reduced psoas muscle index (PMI) on cross-sectional imaging and increased fatty infiltration of the paraspinal musculature (eg, multifidus).11 Undernourished patients demonstrate significantly lower skeletal muscle mass and higher rates of intramuscular fat degeneration, reflecting compromised muscle quality and diminished postural support capacity.11 These imaging findings are clinically important, as paraspinal sarcopenia and fatty degeneration are linked to proximal junctional kyphosis/failure,12,13 and poorer long-term sagittal alignment (eg, increased SVA).11 However, few studies have correlated quantitative CT-based muscle metrics with biochemical markers such as albumin or PNI, highlighting a key gap and an opportunity for integrated radiographic-nutritional risk stratification research.
Protein and BCAA Supplementation in the Perioperative Period
In ASD patients, direct high-level evidence on perioperative branched-chain amino acids (BCAA) or protein supplementation is limited, but extrapolated spine literature suggests that protein optimization may improve surgical outcomes. Clinically, protein sufficiency should be assessed and addressed, as perioperative protein supplementation in spinal arthrodesis cohorts has been associated with improved fusion rates, enhanced
“Preoperative nutritional assessment should extend beyond standard laboratory indices to include a thoughtful evaluation of caloric adequacy, anemia, and micronutrient status. Many elderly ASD patients exhibit subclinical malnutrition despite a normal or elevated BMI.”
wound healing, reduced pain and disability scores, and preservation of paraspinal muscle mass14 —factors that may theoretically mitigate proximal junctional complications. For example, a randomized trial in lumbar fusion patients demonstrated that 36 g/d of whey protein initiated 48 hours preoperatively and continued for 1 month reduced paraspinal muscle atrophy and improved postoperative pain and disability scores.15 In contrast, a separate randomized trial evaluating BCAA plus vitamin D supplementation following lumbar surgery showed preservation and improvement of early postoperative muscle strength, though without clear improvements in patient-reported outcomes or complication rates.16 Collectively, the literature supports perioperative protein optimization in ASD patients, particularly those at risk for malnutrition; however, an independent association between supplementation and improvements in wound healing, pseudarthrosis, and infection mitigation, particularly in ASD patients, remains unexplored.
Supplementation Protocols: Timing and Objective Optimization
Based on the available literature, perioperative supplementation in ASD patients should begin preoperatively, particularly in those identified as malnourished (eg, PNI <50, albumin <3.5 g/dL, elevated CONUT).
Nutritional intervention can be initiated approximately 4–6 weeks before surgery,17,18 as ASD patients demonstrate a natural decline in nutritional status while awaiting surgery. Objective confirmation of optimization should include repeat laboratory testing prior to admission, specifically serum albumin, total lymphocyte count, prealbumin, and recalculated PNI/CONUT scores to assess stabilization or improvement. Oe et al demonstrated that preoperative nutritional guidance with oral supplementation (approximately 6 weeks) reduced postoperative medical complications and attenuated deterioration in PNI and prealbumin levels.18 Regarding postoperative continuation, protein supplementation trials in spine fusion suggest maintaining supplementation for at least 4 weeks postoperatively, as this timeframe aligns with early wound healing and initial fusion biology. Additionally, vitamin D and iron deficiencies should be corrected preoperatively and monitored longitudinally, given their associations with pseudarthrosis and postoperative anemia. Collectively, the evidence supports a structured protocol of screening, 4–6 weeks of preoperative supplementation with laboratory reassessment, and continuation for approximately 1 month postoperatively, although high-level ASD-specific duration data remain limited (Figure 1).
Conclusion
In conclusion, malnutrition is a powerful, modifiable risk factor in adult spinal deformity surgery. Hypoalbuminemia and low PNI independently predict increased mortality,
Figure 1. Recommended nutrition optimization protocol for patients undergoing adult spinal deformity surgery. Image created using artificial intelligence.
complications, transfusion requirements, and prolonged hospitalization. Prospective evidence demonstrates that structured nutritional intervention can significantly reduce postoperative morbidity in malnourished patients. Despite this, standardized perioperative supplementation protocols including optimal protein dosing, timing, duration, and objective optimization thresholds are not yet fully defined. Future research should focus on randomized trials evaluating protein and BCAA supplementation, integration of radiographic sarcopenia metrics, and development of comprehensive nutritional optimization pathways. As deformity surgery continues to expand in elderly populations, nutritional optimization should become a cornerstone of multidisciplinary preoperative planning. l
References
1. Maitra S, Mikhail C, Cho SK, Daubs MD. Preoperative maximization to reduce complications in spinal surgery. Global Spine J. 2020;10(1 Suppl.):45S-52S.
2. Phan K, Kim JS, Xu J, et al. Nutritional insufficiency as a predictor for adverse outcomes in adult spinal deformity surgery. Global Spine J. 2018;8(2):164-171.
3. Gehrchen ML, Bari TJ, Dahl B, Andersen TB, Gehrchen M. Is preoperative S-albumin associated to postoperative complications and readmission in patients with adult spinal deformity: a prospective analysis of 128 patients using the Spine AdVerse Event Severity (SAVES) system. Spine Deform. 2022;10(4):893-900.
4. Oe S, Yamato Y, Hasegawa T, et al. Association between a prognostic nutritional index less than 50 and the risk of medical complications after adult spinal deformity surgery. J Neurosurg Spine . 2020;33(2):219-224.
5. Oe S, Togawa D, Yamato Y, et al. Preoperative age and prognostic nutritional index are useful factors for evaluating postoperative delirium among patients with adult spinal deformity. Spine . 2019;44(7):472.
6. Miura K, Koda M, Funayama T, et al. Surgical Apgar score and controlling nutritional status score are significant predictors of major complications after cervical spine surgery. Sci Rep. 2022;12:6605.
7. Katiyar P, Reyes J, Coury J, Lombardi J, Sardar Z. Preoperative optimization for adult spinal deformity surgery: a systematic review. Spine . 2024;49(5):304.
8. Angus M, Jackson K, Smurthwaite G, et al. The implementation of enhanced recovery after surgery (ERAS) in complex spinal surgery. J Spine Surg. 2019;5(1):116-123.
9. Jung A, Kong R, Tracey O, et al. 113. Impact of iron deficiency anemia on postoperative outcomes of thoracolumbar spinal fusion (≥2-level) on patients with adult spinal deformity with minimum two-year follow-up surveillance. Spine J. 2022;22(9 Suppl.):S60-S61.
10. Snetselaar LG, de Jesus JM, DeSilva DM, Stoody EE. Dietary guidelines for Americans, 2020–2025: Understanding the scientific process, guidelines, and key recommendations. Nutr Today. 2021;56(6):287.
11. Ouchida J, Nakashima H, Ito S, et al. Preoperative undernutrition in older people with adult spinal deformities is associated with worse postoperative sagittal vertical axis. J Orthop Sci. 2026;31(2):277-283.
12. Park JS, Cho KJ, Kim JS, Park SJ, Baek H. Sarcopenia in paraspinal muscle as a risk factor of proximal junctional kyphosis and proximal junctional failure after adult spinal deformity surgery. J Neurosurg Spine . 2023;40(3):324-330.
13. Zhang T-T, Ding J-Z, Kong C, Zhu W-G, Wang S-K, Lu S-B. Paraspinal muscle degeneration and lower bone mineral density as predictors of proximal junctional kyphosis in elderly patients with degenerative spinal diseases: a propensity score matched case–control analysis. BMC Musculoskelet Disord. 2022;23(1):1010.
14. Khalooeifard R, Oraee-Yazdani S, Keikhaee M, Shariatpanahi ZV. Protein supplement and enhanced recovery after posterior spine fusion surgery: a randomized, double-blind, placebo-controlled trial. Clin Spine Surg. 2022;35(3):E356.
15. Khalooeifard R, Shariatpanahi ZV, Ahani A, et al. Effect of protein supplement on paraspinal muscles in spine fusion surgery: a randomized, double-blind, placebo-controlled trial. Int J Spine Surg. 2021;15(1):47-54.
16. Minetama M, Kawakami M, Teraguchi M, et al. Branched-chain amino acids plus vitamin D supplementation promote increased muscle strength following lumbar surgery for lumbar spinal stenosis: a randomized trial. Spine J. 2023;23(7):962-972.
17. Reyes J, Katiyar P, Greisberg G, et al. Preoperative nutritional optimization for adult spinal deformity: review. Spine Deform. 2024;12(2):257-262.
18. Oe S, Watanabe J, Akai T, et al. The effect of preoperative nutritional intervention for adult spinal deformity patients. Spine . 2022;47(5):387.
From the Department of Orthopaedic Surgery at Rush University Medical Center in Chicago, Illinois.
Neurologic Complications in Adult Spinal Deformity Surgery
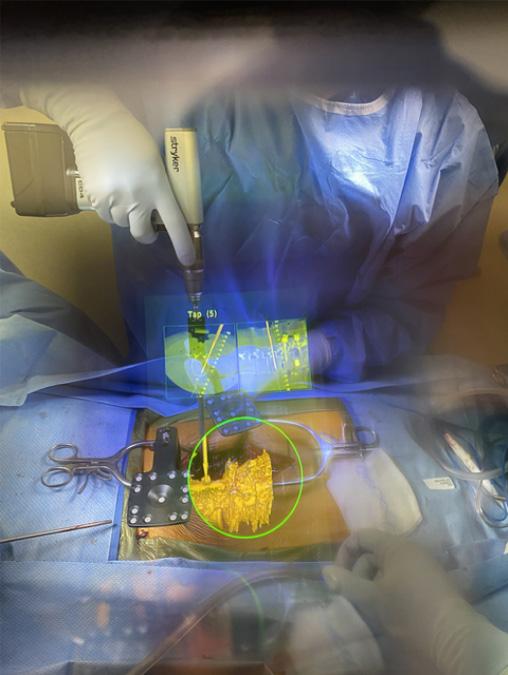
In the surgical management of adult spinal deformity (ASD), the primary limiting factor in complex reconstructions is the preservation of neurologic integrity. Early research into the incidence of neurologic complications in these procedures was subject to wide variability owing to the retrospective nature of most clinical series. However, the maturation of prospective, multicenter data have established a clear benchmark for patient counseling and surgical expectations. Radiographic metrics and anatomical classifications help in risk stratification, and machine-learning algorithms have been developed to quantify a patient’s risk of intraoperative neuromonitoring (IONM) data loss with a high degree of accuracy.
The
Scoli-RISK-1
Study: Longitudinal Incidence and Motor Recovery
The Scoli-RISK-1 study was a landmark prospective study on the neurologic consequences of complex ASD surgery.1 By using the validated American Spinal Injury Association (ASIA) Lower Extremity Motor Score (LEMS), the study aimed to eliminate the reporting bias inherent in earlier literature,
which often used a binary “intact vs. deficit” reporting method. The LEMS evaluates 5 muscle groups bilaterally on a 0–5 scale (totaling 50 points), providing an objective assessment of motor function.
A total of 272 patients were enrolled across 15 international centers. At the time of hospital discharge, 23% of patients exhibited a decline in LEMS compared to their preoperative baseline. This reflects the significant mechanical and physiological stresses placed on the spinal cord and nerve roots during complex reconstructions, including direct iatrogenic trauma, ischemic events related to corrective forces, and the systemic effects of massive blood loss.
Despite the high incidence of early deficit, the longitudinal data are more encouraging and demonstrate a robust potential for recovery. The incidence of LEMS deterioration relative to baseline follows a downward trajectory during the first 6 months postoperatively. By 6 months, the rate of deterioration stabilizes at approximately 10%, which remains consistent at the 2-year and 5-year follow-up intervals. 2,3 These findings indicate that many early deficits are transient neuropraxias or reversible ischemic injuries.
Although the mean rate of deterioration stayed stable after 6 months, an interval analysis of the 2- to 5-year window showed that 11% experienced a decline in motor function
Jonathan A. Gabor, MD
Joshua M. Samaniego BS, MS
Nathan J. Lee, MD
during this period. Late neurologic deterioration is often driven by mechanical failures of the spinal construct—most commonly, rod fracture and pseudarthrosis—rather than the initial surgical correction. Conversely, 8% of patients made a late recovery, continuing to regain strength by year 5, likely due to long-term neural plasticity or dedicated physical therapy.
Risk Factors for Cord-Level Deficits
The risk of sustaining a cord-level neurologic deficit in ASD surgery is multifactorial. Risk factors can be broadly categorized into patient factors, curve/cord factors, and surgical factors. Critical windows of intraoperative vulnerability occur during spinal cord decompression, osteotomy closure, and rod cantilever maneuvers.4
The Deformity Angular Ratio
Two curves of similar magnitude can have vastly different neurologic risk profiles depending on their focal angularity. The Deformity Angular Ratio (DAR) was developed to quantify this angularity. 5 It is calculated by dividing the maximum Cobb angle of a deformity by the number of vertebrae spanned by that curve. A higher DAR indicates a sharper, more focal angularity more likely to cause cord impingement or tension. It is evaluated in both the coronal (cDAR) and sagittal (sDAR) planes, and a composite total (tDAR) is calculated as their sum. A cDAR >10, sDAR >15 and total DAR >25 have been identified as specific thresholds correlated with an increased risk of IONM cord data loss and a greater chance of neurologic
“Quantifying neurological risk preoperatively enables more informed surgical decision-making and more transparent, patientspecific discussions about risk.”
deficits postoperatively. These patients are often characterized by severe deformities that necessitate aggressive corrective maneuvers. Importantly, patients with a tDAR >25 are at high risk regardless of whether a 3-column osteotomy is performed. 6 Routine maneuvers—such as rod reduction, translation, or the minor lengthening associated with a Ponte osteotomy—can push a stretched or compressed cord beyond its physiological limit.
Spinal Cord Shape Classification
The anatomical relationship between the spinal cord and the apical vertebrae is equally critical. The Spinal Cord Shape Classification (SCSC), an MRI-based system introduced by Sielatycki et al, categorizes the morphology of the cord and the presence of a cerebrospinal fluid (CSF) buffer at the apex of the deformity.7
A type 1 spinal cord is circular and symmetric, surrounded by a visible CSF buffer. It is protective against signal loss during correction (OR 0.17). A type 2 cord is circular or oval but lacks a visible CSF buffer between the neural tissue and the
vertebral body. This type does not show a statistically significant association with increased risk compared with type 1.
A type 3 spinal cord (T3SC) is visibly deformed, often flattened or crescent-shaped, and is pressed against the concavity of the vertebral column with no CSF buffer present. Those with T3SC have odds of intraoperative signal loss that are 28.3 times higher than those with type 1 cords. The mechanism of injury in T3SC is believed to be 2-fold: the lack of a fluid buffer makes the cord highly susceptible to direct mechanical compression during corrective maneuvers, and the flattened morphology often indicates a cord that is already under significant tension, leaving little physiological reserve for the stress of surgical correction.
In a cohort of 79 patients with T3SC, the largest reported cohort, 39% had IONM data loss. 8 A major finding was that there was a statistically significantly higher EBL (as well as TXA use and cell saver salvage) in the IONM-loss group, but no difference
in DAR (coronal, sagittal, and total), use of 3-column osteotomy, or cross-sectional area of cord deformation between those with and without IONM loss.
Machine Learning in Risk Quantification
A machine-learning approach was used to develop a preoperative scoring system to predict cord-level IONM data loss. 9 The scoring model was derived from a database of 1,106 patients and more than 200 variables. Eight nonmodifiable preoperative factors that were most critical for prediction were identified (Table 1). Point values were assigned by rounding the regression coefficients.
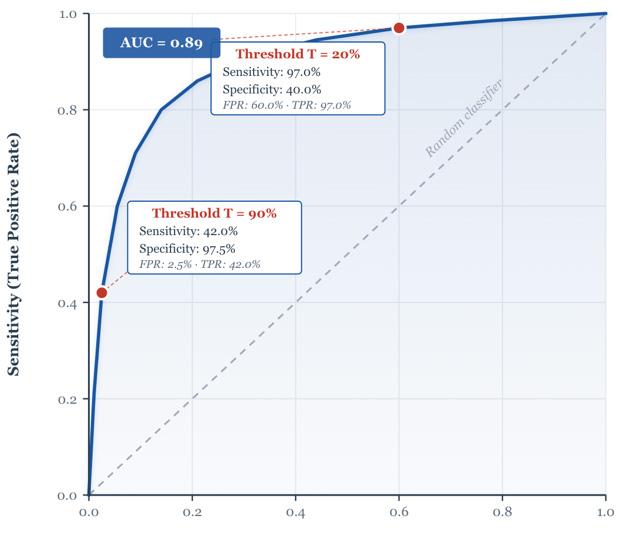
Patients were stratified into low (score ≤2), moderate (score 3-6), and high (score ≥7) risk categories. These were associated with a 0.9%, 19.8%, and 85.7% incidence of IONM data loss, respectively (Table 2). The scoring system achieved an overall accuracy of 93.1% with an area under the receiver operating characteristic curve of 0.898, indicating excellent discriminative ability in distinguishing cases with and without signal loss. Its high specificity (94%) suggests a strong ability to identify patients unlikely to develop signal loss; its moderate sensitivity (75%) indicates that some at-risk patients may still be missed.
Prognostic Impact of Intraoperative Data Recovery
Lee et al also published a comprehensive analysis evaluating the prognostic effects of intraoperative improvements in cord signal
Table 1. Preoperative risk factors included in the scoring system to predict cord-level IONM loss, developed by Lee et al.
data.10 In their series of 1,106 patients, any improvement in IONM data was significantly associated with a lower risk for new motor deficits on postoperative day 1 (POD1). Of those who suffered IONM data loss, 85% saw improvement after intraoperative intervention, such as increasing mean arterial pressure, releasing correction, or performing further decompression. Crucially, the timing of recovery (before or after 60 minutes) did not significantly impact the rate of POD1 deficits, suggesting that the occurrence of signal return is more prognostic than the speed of return. By hospital discharge, the rate of new motor deficits was 3.6% for patients who achieved full IONM recovery and 11.8% for those with partial recovery.
Root-Level Neurologic Deficits and Stretch Neuropraxia
While cord-level injuries carry the highest morbidity, root-level complications can still
profoundly impact postoperative function. Root-level alerts are characterized by IONM signal change in 1 or 2 muscle groups, often following rod/screw placement or decompression. Nearly half of patients who experience an intraoperative root alert will exhibit a POD1 motor deficit.11 Intraoperative intervention (primarily additional decompression) often leads to partial or full IONM recovery, which is protective against severe motor weakness on POD1.
A distinct mechanism of root-level injury in ASD surgery is stretch neuropraxia, particularly during the correction of sharp lumbosacral fractional curves. As these curves are realigned, the chronically shortened neural elements on the concavity are suddenly subjected to significant lengthening forces. Ha et al identified a novel radiographic parameter to predict this complication—the change in distance between the lower lumbar neural foramen (L4 and L5) and the ipsilateral fem-
Table 2. Risk of neurologic injury according to the preoperative scoring method developed by Lee et al.
References
oral head (ΔL4-FH and ΔL5-FH).12 On logistic regression, a ΔL4-FH greater than 20 mm was associated with about 15-fold higher odds of postoperative stretch neuropraxia, and a ΔL5-FH greater than 15 mm was associated with about 21-fold higher odds.
Conclusion
Significant efforts have been made to quantify neurologic risk in ASD surgery. The maturation of prospective data from Scoli-RISK-1 established the baseline incidence
1. Lenke LG, Fehlings MG, Shaffrey CI, et al. Neurologic outcomes of complex adult spinal deformity surgery: results of the prospective, multicenter scoli-RISK-1 study. Spine (Phila Pa 1976). 2016;41(3):204-212.
2. Lenke LG, Zuckerman SL, Cerpa M, et al. The Scoli-RISK 1 results of lower extremity motor function 5 years after complex adult spinal deformity surgery. Eur Spine J. 2021;30(11):3243-3254.
3. Lenke LG, Shaffrey CI, Carreon LY, et al; AO Spine International and SRS Scoli-RISK-1 Study Group. Lower extremity motor function following complex adult spinal deformity surgery: two-year follow-up in the Scoli-RISK-1 prospective, multicenter, international study. J Bone Joint Surg Am. 2018;100(8):656-665.
4. Iyer RR, Vitale MG, Fano AN, et al. Establishing consensus: determinants of high-risk and preventative strategies for neurological events in complex spinal deformity surgery. Spine Deform. 2022;10(4):733-744.
5. Wang XB, Lenke LG, Thuet E, Blanke K, Koester LA, Roth M. Deformity angular ratio describes the severity of spinal deformity and predicts the risk of neurologic deficit in posterior vertebral column resection surgery. Spine (Phila Pa 1976). 2016;41(18):1447-1455.
of complications, while radiographic and anatomical metrics such as the DAR and SCSC laid the groundwork for identifying at-risk patients. A machine-learning-derived scoring system was developed to categorize patients into low-, moderate-, and high-risk categories with a high degree of accuracy. Additionally, the evidence consistently shows that the intraoperative recovery of IONM signals is the most potent determinant of early postoperative function at both the cord and root levels. l
6. Illingworth KD, Siddiqui AA, Skaggs DL, Andras LM. Deformity angular ratio is associated with neuromonitoring changes without a vertebral column resection: spinal deformity is more influential than type of surgery. Spine Deform. 2023;11(4):951-956.
7. Sielatycki JA, Cerpa M, Baum G, et al. A novel MRI-based classification of spinal cord shape and CSF presence at the curve apex to assess risk of intraoperative neuromonitoring data loss with thoracic spinal deformity correction. Spine Deform. 2020;8(4):655-661.
8. Hung CW, Hassan FM, Lee NJ, et al. Higher intraoperative blood loss is associated with increased risk of intraoperative neuromonitoring data loss for the type 3 spinal cord shape during spinal deformity surgery. Spine Deform. 2025;13(5):1573-1583.
9. Lee NJ, Lenke LG, Arvind V, et al. A novel preoperative scoring system to accurately predict cord-level intraoperative neuromonitoring data loss during spinal deformity surgery: a machine-learning approach. J Bone Joint Surg Am. Published online November 20, 2024. doi:10.2106/JBJS.24.00386
10. Lee NJ, Lenke LG, Yeary M, et al. Does an improvement in cord-level intraoperative neuromonitoring data lead to a reduced risk for postoperative neurologic deficit in spine deformity surgery? Spine Deform. 2025;13(1):261-272.
11. Lee NJ, Hassan F, Dionne A, et al. Can the recovery of root-level intraoperative neuromonitoring data result in a lower risk for postoperative lower extremity weakness in spine deformity surgery? Spine J. 2024;24(9):S17.
12. Ha AS, Cerpa M, Mathew J, et al. Femoral head to lower lumbar neural foramen distance as a novel radiographic parameter to predict postoperative stretch neuropraxia. J Neurosurg Spine . 2022;36(1):23-31.
From 1Wayne State University School of Medicine in Detroit, Michigan; 2 Department of Orthopedic Surgery at the Henry Ford Health System in Detroit, Michigan; and 3Department of Orthopedic Surgery at Rush University Medical Center in Chicago, Illinois.
Wearable Technology in Spine Surgery
Current Evidence on Patient Outcomes and Postoperative Recovery
Traditional postoperative clinical assessments after spine surgery are reliant on clinic visits and patient-reported outcome measures, which capture discrete time points and may not fully reflect patient recovery trajectories. These approaches are limited by recall bias and the inability to detect subtle changes between visits. As healthcare shifts toward value-based care and expanded telehealth capabilities, wearable technology has emerged as a tool for continuous recovery monitoring. Smartphones and body-worn sensors collect real-time information on activity, mobility, and physiologic parameters without patient input, supporting objective recovery assessment and earlier detection of deviations that may signal complications.1-3 The present review focuses on practical, evidence-based applications of wearable technology that can be realistically integrated into contemporary spine surgery practices.
Definition and Scope of Wearable Technology
For this review, wearables were defined as consumer-grade and medical-grade
devices worn on the body that collect data related to physical activity or physiologic parameters either continuously or intermittently.1 This definition includes smartphones with built-in accelerometers, fitness trackers, and specialized medical sensors designed specifically for patient monitoring by measuring gait and mobility and recording vitals.4
Types of Wearable Technologies Used in Spine Surgery
Wearable devices can be categorized into three primary domains: activity and mobility monitoring, physiologic monitoring, and remote postoperative medical monitoring platforms. Activity and mobility monitoring represent the most well-studied applications of wearable technology in spine surgery. Smartphone accelerometers and consumer fitness trackers quantify step counts, walking distance, cadence, and activity duration, while more advanced sensors capture detailed gait parameters such as stride length, walking speed, and posture.5-9 Despite their widespread availability, these technologies remain underutilized in routine clinical prac-
Alqasim Elnaggar, BA1
Ahmad Almaat, BSc1
Ali Mehaidli, MD2
Kevin Taliaferro, MD2
Daniel Park, MD3
PATIENT OUTCOMES
tice, representing an opportunity to enhance postoperative monitoring and personalize rehabilitation strategies.
Physiologic monitoring devices measure variables including heart rate, sleep quality, and in some cases, respiratory function.10
Advanced fitness trackers and smart rings may additionally detect physiologic stress responses and sleep disturbances that can serve as markers of pain or complications.
Device Type Description Data Captured
Smartphone accelerometers
Consumer fitness trackers
Built-in sensors within smartphones that quantify activity through passive or app-based monitoring
Wrist-worn devices that continuously monitor activity and physiologic parameters over prolonged periods
Remote medical monitoring platforms integrate sensor data with PROMs, medication use, and wound photographs to support longitudinal recovery surveillance.4 By facilitating continuous communication between patients and providers, these systems enable early identification of recovery deviations supporting timely clinical intervention. Table 1 summarizes the wearable technologies currently applicable to spine surgery practice.
Preoperative phenotyping to quantify baseline mobility; postoperative recovery tracking and remote assessment of functional improvement
Daily activity monitoring for objective evaluation of patient adherence to rehabilitation; early detection of deviations in activity or recovery
Objective assessment of mobility and functional recovery after spine surgery; standardized gait analysis for surgical outcome comparison; guide rehabilitation interventions based on patient-specific gait deficits
Multi-modal data (activity, symptoms, patient-reported outcome measures, vitals) Comprehensive postoperative surveillance; early detection of complications; continuous remote monitoring of recovery and adherence to rehabilitation protocols
smartphones
Fitbit, Apple Watch, Garmin, Samsung Galaxy Watch
Ametris, GaitUp, MetaMotion, APDM Opal
Greenberg et al (2024); Tiao et al (2025); Bienstock et al (2022)
ViSi Mobile, HealthArc RPM, Teladoc Health RPM
Miller et al (2026); Ma et al (2025); Triantafyllou et al (2022); Khan et al (2022); Natarajan et al (2022)
Restrepo et al (2022); Sripadrao et al (2025); Maharaj et al (2022)
Table 1. Digital and Wearable Technologies for Objective Measurement of Physical Activity and Gait in Spine Surgery Patients
iPhone, Android
Ahmad et al (2022); Basil et al (2021); Zhang et al (2025)
Evidence Linking Wearable Technology to Patient Outcomes
Postoperative Recovery and Functional Improvement
Bienstock et al used accelerometer data to identify three distinct phases of recovery following lumbar laminectomy: an acute healing phase from 0-40 days characterized by rapid increases in step counts, a recovery phase from 40-130 days with slower gains, and a stabilization phase beyond 130 days during which activity plateaued near preoperative levels.11 This temporal characterization of function extends beyond the episodic insights provided by traditional assessments and PROMs.
Comparative studies utilizing gait analysis reveal differences between surgical approaches. Miller et al demonstrated that patients undergoing minimally invasive transforaminal lumbar interbody fusion achieved faster mobilization compared to traditional open posterolateral fusion. 8 Similarly, Ma et al revealed that uniportal endoscopic lumbar surgery was associated with superior early mobility compared to open surgery in patients monitored with wearable sensors.7
The standardization of physical activity monitoring has emerged as a priority in spine surgery literature. Evidence suggests that a 10-14 day postoperative monitoring window provides reliable step-count data while capturing meaningful improvements in physical function.12,13 By defining an optimal monitoring duration, these findings may support the creation of more efficient clinical protocols and enhance the clinical application of this technology.
Pain Trajectories and Opioid Use
While wearable devices primarily capture activity data, the literature suggests potential utility in pain assessment. Tiao et al demonstrated that fitness tracker data can validate patient reports, showing that the Oswestry Disability Index and SF-12 scores are not significantly affected by recall bias when compared with objective activity metrics captured with wearable devices.14
A systematic review by Sripadrao et al further reported that integrated monitoring platforms collecting both activity and pain scores enabled a more comprehensive recovery assessment, although direct wearable measurement of pain remained limited to physiologic correlates such as heart rate variability and sleep disturbances.4
Complications, Readmissions, and Delayed Recovery
Wearable technology enables early identification of recovery deviations, potentially
allowing intervention before complications that result in an emergency department visit or readmission. Sripadrao et al identified reduced emergency room visits and earlier complication detection as benefits of wearable monitoring for patients who underwent lumbar fusion. 4 Continuous data capture allows clinicians to distinguish normal recovery variation from a clinically significant decline, which is particularly valuable given that routine postoperative imaging often fails to change clinical management.1
Patient Engagement and Adherence
Patient engagement with wearable technology is high, with studies reporting compliance and satisfaction.10 Voglis et al found that smartphone-based activity data correlated with physical performance outcomes and provided real-world functional assessment beyond what clinic-based testing can capture.15 The term “recovery kinetics,” introduced by Maharaj et al, describes the use
of continuous postoperative monitoring to characterize individual recovery patterns, potentially enhancing patient education and expectation management.16
Clinical Applications for the Practicing Spine Surgeon
Remote postoperative recovery monitoring represents the most immediate clinical application of wearable technology in spine surgery. Continuous step count and activity data provide objective metrics of functional improvement between office visits, complementing patient-reported outcomes, and offering quantitative benchmarks for recovery trajectories. 3 Establishing normative recovery curves for specific procedures allows surgeons to identify patients whose progress diverges from expected patterns, enabling earlier intervention when delays or complications arise.6,16
Wearable data also offer potential for risk stratification and outcome prediction. Incorporating preoperative mobile health data can improve the accuracy of recovery predictions by 30%-34% compared with traditional evaluations alone, while preoperative smartphone accelerometry may detect patterns of functional decline that inform surgical decision-making and individualized patient counseling. 5,10
Successful implementation requires careful integration into clinical workflows. Considerations include data management, patient onboarding and education, and staff training. Standardized protocols and clinician education are critical to ensure consistent use and interpretation, with
ongoing research highlighting the need for structured approaches to fully leverage wearable technology in orthopedic and spine surgery practice.17
Limitations of Current Evidence
Despite promising findings, important limitations remain in the current evidence base. Variability across wearable devices, monitoring durations, outcome definitions, and analytic approaches complicate comparisons across studies and limit standardization. 4 Although postoperative activity changes are observed, clinically meaningful thresholds and procedure-specific benchmarks remain poorly defined, limiting translation into routine clinical decision-making.18,19
Additional limitations include short follow-up periods and small sample sizes, with most studies monitoring recovery for only 3-6 months and enrolling fewer than 50 patients, thereby restricting assessment of long-term recovery patterns and generalizability.1 Challenges also persist in distinguishing clinically significant deviations from normal recovery variation and integrating multimodal wearable data into actionable recommendations. While wearable sensors can capture detailed kinematic and functional metrics during daily activities, further work is required to determine how these measurements should guide postoperative management. 20
Future Directions
Integration of wearable technology into enhanced recovery after surgery pathways represents a logical next step, enabling objective monitoring of early mobilization and
identification of patients requiring additional support or targeted rehabilitation.18,21
Predictive analytics and artificial intelligence applications are rapidly evolving, with emerging evidence suggesting that machine learning approaches applied to wearable data may improve risk stratification, detect delayed recovery, and refine personalized care pathways.4,10 However, these approaches remain largely exploratory and require validation in prospective cohorts.
Establishing standardized, recovery benchmarks specific to each surgical technique remains a priority. Efforts to normalize activity data using age- and sex-adjusted metrics provide a framework for interpreting recovery relative to expected functional gains and may enhance clinical utilit.12,13 Future research should prioritize randomized trials, longer follow-up, and cost-benefit analyses to determine whether wearable technologies improve outcomes beyond monitoring alone and support their transition into routine practice.18
Conclusion
Wearable technology provides objective insight into postoperative recovery and complements traditional patient-reported outcome measures. Evidence supports their clinical utility for monitoring functional improvement, identifying recovery deviations, and predicting outcomes. Continuous data capture enables a more granular understanding of recovery and may create opportunities for earlier clinical intervention when complications arise. However, broader adoption requires standardization
PATIENT OUTCOMES
of devices, metrics, and data interpretation, along with validation through randomized trials. As digital health tools continue to evolve, wearable technology is positioned to become a valuable component of spine surgery care. l
References
1. Natarajan P, Fonseka RD, Maharaj MM, Koinis L, Mobbs RJ. Continuous data capture of gait and mobility metrics using wearable devices for postoperative monitoring in common elective orthopaedic procedures of the hip, knee, and spine: a scoping review. J Orthop Surg Res. 2023;18(1):812.
2. Natarajan P, Fonseka RD, Sy LW, Maharaj MM, Mobbs RJ. Analysing gait patterns in degenerative lumbar spine disease using inertial wearable sensors: an observational study. World Neurosurg. 2022;163:e501-e515.
3. Basil GW, Sprau AC, Eliahu K, Borowsky PA, Wang MY, Yoon JW. Using smartphone-based accelerometer data to objectively assess outcomes in spine surgery. Neurosurgery. 2021;88(4):763-772.
4. Sripadrao S, Carr C, Quraishi M, et al. A systematic review of the role of wearable devices and artificial intelligence applications in assessing functional outcomes after lumbar fusion. Spine J. Advance online publication October 15, 2025.
5. Ahmad HS, Singh S, Jiao K, et al. Data-driven phenotyping of preoperative functional decline patterns in patients undergoing lumbar decompression and lumbar fusion using smartphone accelerometry. Neurosurg Focus . 2022;52(4):E4.
6. Zhang JK, Yakdan S, Zhang J, et al. Establishing objective markers of physical activity to identify early improvement after lumbar spine surgery. J Neurosurg Spine . 2025;43(5):584-592.
7. Ma A, Mobbs RJ, Maharaj MM. Patient recovery following uniportal endoscopic vs open lumbar spine surgery: objective analysis of postoperative mobility and gait patterns using wearable sensors. Int J Spine Surg. 2025;19(1):39-48.
8. Miller AK, Goldstein Z, Sayeed A, Zakko P, Park DK. Comparison of post-operative mobilization after minimally invasive transforaminal lumbar interbody fusion and traditional open posterolateral fusion using objective gait analysis data. Global Spine J. Advance online publication January 20, 2026.
9. Restrepo A, Saha AK, Khanna AK, Huang E, Clark CJ. Use of a multi-sensor monitoring device in an early post-operative mobilization program. Am Surg. 2022;88(8):1861-1867.
10. Greenberg JK, Frumkin M, Xu Z, et al. Preoperative mobile health data improve predictions of recovery from lumbar spine surgery. Neurosurgery. 2024;95(3):617-626.
11. Bienstock DM, Shankar D, Kim J, et al. Accelerometry data delineate phases of recovery and supplement patient-reported outcome measures following lumbar laminectomy. World Neurosurg. 2022;160:e608-e615.
12. Maldaner N, Tang M, Fatemi P, et al. Standardizing physical activity monitoring in patients with degenerative lumbar disorders. Neurosurgery. 2024;94(4):788-796.
13. Gonzalez-Suarez AD, Maldaner N, Tang M, et al. Determining critical monitoring periods for accurate wearable step counts in patients with degenerative spine disorders. Sci Rep. 2024;14(1):19988.
14. Tiao J, Rosenberg AM, Bienstock DM, et al. The Oswestry Disability Index and 12-Item Short Form Health Survey Physical Component scores are not affected by recall bias in posterior lumbar spine surgery patients: a prospective study using data from fitness trackers. J Am Acad Orthop Surg Glob Res Rev. 2025;9(4):e24.00185.
15. Voglis S, Ziga M, Zeitlberger AM, et al. Smartphone-based real-life activity data for physical performance outcome in comparison to conventional subjective and objective outcome measures after degenerative lumbar spine surgery. Brain Spine . 2022;2:100881.
16. Maharaj M, Natarajan P, Fonseka RD, et al. The concept of recovery kinetics: an observational study of continuous post-operative monitoring in spine surgery. J Spine Surg. 2022;8(2):196-203.
17. Iwasyk AW, Gaur SS, Federico A, et al. Wearable Technology in Orthopaedic Surgery: Applications and Future Directions. JBJS Rev. 2025;13(7).
18. Leibold A, Mansoor Ali D, Harrop J, Sharan A, Vaccaro AR, Sivaganesan A. Smartphone-based activity tracking for spine patients: current technology and future opportunities. World Neurosurg X . 2024;21:100238.
19. Khan S, Mageswaran P, Brock G, Eisner M, Ferguson SA, Marras WS. Quantitative dynamic wearable motion-based metric compared to patient-reported outcomes as indicators of functional recovery after lumbar fusion surgery. Clin Biomech (Bristol). 2022;97:105706.
20. Triantafyllou A, Papagiannis G, Stasi S, et al. Application of wearable sensors technology for lumbar spine kinematic measurements during daily activities following microdiscectomy due to severe Sciatica. Biology (Basel). 2022;11(3).
21. Aubry C, Nüesch C, Fiebig O, et al. Accelerometry-based physical activity, disability and quality of life before and after lumbar decompression surgery from a physiotherapeutic perspective: an observational cohort study. N Am Spine Soc J. 2021;8:100087.
22. Maldaner N, Gonzalez-Suarez AD, Tang M, et al. Standardizing continuous physical activity monitoring in patients with cervical spondylosis. Spine (Phila Pa 1976). 2024;49(16):1145-1153.
From the 1Department of Orthopaedics at the Hospital for Special Surgery in New York City, New York; 2 Department of Orthopedics at the University of Tsukuba Hospital in Tsukuba, Japan; and 3Weill Cornell Medical College in New York City, New York.
Augmented Reality and Virtual Reality Navigation in Spine Surgery:
Clinical Accuracy, Workflow Integration, and Barriers to Adoption
The adoption of augmented reality (AR) and virtual reality navigation in spine surgery mirrors a shift to precision, technology-integrated care. As spine surgery becomes more complex, technologies that improve visualization and spatial orientation are increasingly important, where high spatial accuracy in narrow corridors near critical neural and vascular structures is crucial.1
Conventional intraoperative guidance provides essential anatomy but comes with trade-offs. Fluoroscopy is accessible and real-time, but it exposes patients and staff to radiation, can prolong surgery, and has limited precision in implant positioning and depth estimation. 2,3 Conventional computed tomography (CT)–based navigation improves anatomical localization, but it cannot update in real time to reflect anatomical changes as the procedure progresses, system accuracy may decline over the course of the case, and it remains vulnerable to CT artifacts from metallic implants.4,5 These limitations are compounded by a steep learning curve and high costs. 6,7 Additional drawbacks include a longer setup time, increased radiation exposure from thin-cut imaging, the need for a separate incision for a pelvic reference
pin, and susceptibility to navigation errors caused by patient movement or reference array displacement. 2,8,9 Line-of-sight tracking systems are further vulnerable to obstruction by instruments or personnel.10 The system also requires surgeons to divert their gaze from the operative field to an external monitor, fragmenting attention and increasing cognitive load.11,12
AR and VR navigation systems support intraoperative judgment by integrating virtual data into the surgeon’s view, allowing for simultaneous visualization of the operative field and digital guidance without disrupting attention.11 In procedures needing high spatial accuracy, such as pedicle screw placement and deformity correction, this integration simplifies intraoperative decision-making by showing anatomical landmarks and surgical plans together.13 These technologies aim to support safe spine surgery by reducing unnecessary
Atahan Durbas, MD1
Vishaal Nayagam, BS1
Tomoyuki Asada, MD, PhD1,2
Sheeraz A. Qureshi, MBA, MD1,3
intraoperative navigation, which influences perioperative outcomes. 2,13
cognitive load without replacing surgical expertise (Figure 1).
Accuracy and Technical Performance of AR Navigation
AR navigation systems in spine surgery register pre- or intraoperative imaging to the patient’s anatomy and project virtual overlays into the surgeon’s view via head-mounted displays or projection systems. They use optical, electromagnetic, or robotic tracking to locate instruments in real time. Intraoperative 3-dimensional fluoroscopy allows real-time navigation updates that reduce registration drift. VR platforms are used preoperatively for planning and simulation, offering immersive rehearsal before surgery. Most clinical studies focus on AR-guided
For example, evidence shows that AR-guided systems improve surgical precision in pedicle screw placement (PSP), a key benchmark given its technical difficulty, clear error consequences, and validated assessment methods. Compared with freehand, fluoroscopy, CT, and robotic methods, AR often yields better accuracy, though results depend on the system and the surgeon’s experience. 2,14 AR navigation shows higher placement accuracy and fewer cortical breaches than freehand methods. Liu et al reported 98.0% accuracy for AR-assisted PSP using a head mounted display across 205 cases.10 Loggia et al, in the largest study comparing approaches, found AR-guided navigation had higher PSP accuracy than the freehand technique, suggesting that AR offers more consistent precision across surgeons and spinal levels.15 Elmi-Terander et al showed that clinically accurate screws were significantly more common in the AR group (93.9% vs 89.6%), and screws without cortical breach occurred twice as often (63.4% vs 30.6%).16 In thoracic PSP specifically, AR demonstrated superiority over freehand technique in overall accuracy (85% vs 64%), with significant reductions in breaches exceeding 4 mm (2% vs 25%).17 In the context of deformity surgery, AR navigation has also been shown to significantly increase pedicle screw density while minimizing hook usage compared to freehand without prolonging operative time.18
AR navigation outperforms freehand, but the advantage depends on the surgeon’s
Figure 1. Surgeons using the Augmedics xVision Spine System, combining preoperative CT with intraoperative 2D C-arm fluoroscopy to show 3D spinal navigation in the surgeon’s view. Source: Augmedics. Xvision spine system. Retrieved March 6, 2026, from https://augmedics.com/
experience. For novices, AR significantly reduces screw perforation and improves inclination angles and convergence compared to the freehand technique.14 Expert surgeons showed no significant difference between AR and freehand, indicating that AR’s precision benefits may be more apparent in early surgical stages of training.14 This finding suggests AR may act as an equalizer for young surgeons by closing the performance gap between novice and experienced surgeons. An important clinical implication, however, is the meaningful difference in the accuracy of pedicle screw placement. Although accuracy has been increased, the rate of surgical take back or clinically meaningful malpositioned screw rate has not shown significant differences. While fluoroscopy demands mental 3-dimensional reconstruction from 2-dimensional images, AR systems lessen the burden by overlaying implant plans directly within the operative field.19 Peh et al showed in a cadaveric study that AR-guided lumbar PSP had 94.2% accuracy compared to 88.2% for fluoroscopy-guided placement, without extra navigation time or intraoperative delays in radiation. 20 A systematic review by Taylor et al confirmed these findings with a larger evidence base, reporting an average PSP accuracy of 93.33% for AR navigation across 2,157 screws from C1 to the iliac spine, versus 86.79% for fluoroscopy across 3,773 screws. 21 AR navigation reduces intraoperative blood loss (470 mL vs 802 mL) compared to freehand and fluoroscopic methods. However, operative time was slightly longer with AR
(281.6 vs 255.5 minutes). 21 Despite this, AR systems can significantly reduce radiation exposure versus traditional fluoroscopy without affecting screw insertion time. 22 By maintaining fluoroscopic images within the surgeon’s field of view, AR guidance enables more stable screw insertion and reduces the need for repeated fluoroscopic checks (Figure 2).
Figure 2. Intraoperative view via Augmedics xVision display showing CT-based spinal anatomy and pedicle screw plan overlaid on the surgical field with augmented reality (AR) navigation. Source: Augmedics. Xvision spine system. Retrieved March 6, 2026, from https://augmedics.com/
Workflow Integration and Adoption Barriers
Despite promising accuracy of data for AR navigation, its real-world use remains limited. The gap between technical performance and clinical adoption stems from workflow, ergonomic, financial, and institutional challenges. Understanding these barriers clarifies AR navigation status and the conditions needed for broader use.
Setup Time
AR navigation increases preparation time before incision due to setup steps such as CT imaging, registration, reference array placement, and tracking, unlike freehand or fluoroscopy-guided methods that need less infrastructure. 2 Each step causes delays and demands technical skill. Kong et al noted that integrating AR with surgical guides and navigation is complex, costly, and requires maintaining calibration to ensure system accuracy and reliability. 23
Of note, the setup time compared to traditional CT-based navigation and robotics is likely similar.
Operative Workflow Ergonomic Challenges
Beyond setup, AR navigation must fit into the surgical workflow, which is rarely seamless. Integration needs initial training and a period of reduced efficiency as teams adapt to new protocols.13 This challenge goes beyond the surgeon; mastering AR systems requires extensive training in hardware, software, workflow adaptation, and intraoperative technique. The hardware presents ergo -
nomic and perceptual challenges, including depth perception. Microsoft HoloLens 2 shows holograms in the surgeon’s view but is monocular, lacking stereoscopic cues for depth judgment. This hinders the assessment of the instrument trajectory relative to patient anatomy. Hardware limitations include limited fields of view, low resolution, and latency, impairing usability and accuracy in complex spinal procedures.13
Cost and Infrastructure
Many AR systems rely on intraoperative CT or cone-beam CT, which can increase infrastructure requirements and limit access to facilities without advanced imaging. The financial barrier to AR navigation is significant, with systems like Augmedics xVision costing $200,000 to $300,000, which doesn’t include training, maintenance, and onboarding expenditures.13 Many community hospitals and small surgical centers find upfront investments prohibitive without proven cost-effectiveness data.13
Technical Reliability and Visual Fatigue
Poorly constructed or overly complex visualizations distract and diminish the intended precision of AR navigation. The clinical utility of AR navigation depends on system reliability, as minor calibration errors can cause deviations in surgical guidance, affecting patient outcomes and safety. 24 Continuous intraoperative calibration and validation are needed to maintain accuracy, increasing procedural steps and cognitive load. User experience varies; Wolf
et al noted that AR visualization designs impact trajectory deviation, visual attention, and overall experience, highlighting that interface quality directly influences surgical outcomes performance. 25
Institutional and Regulatory Challenges
Adoption of AR navigation is complicated by diverse institutional receptivity and strict regulations. Acceptance of new surgical technology varies across healthcare systems, and organizational inertia can delay implementation even where funds are available. 24 AR systems add data governance duties owing to real-time transmission and storage of patient imaging data, raising privacy, security, and compliance concerns. Securing regulatory approval is time-consuming, with standards differing across regions, creating uncertainty for institutions and developers’ entry.13
Lack of Long-Term Outcomes Data
The most significant barrier to broader adoption is the scarce long-term clinical and economic evidence. The literature mainly comprises observational studies, proof-ofconcept investigations, and small pilot series with short follow-ups, which are inadequate for drawing conclusions about long-term skill retention, patient outcomes, or cost savings.13,24 Fewer than a third of studies in systematic reviews were randomized controlled trials, and fewer than a third enrolled more than 50 participants.13 Confounding factors, such as users’ familiarity with AR hardware unrelated to surgical skill, were rarely con-
trolled, suggesting that performance gains may be due to device habituation rather than real clinical improvement.13 Until larger randomized controlled trials are conducted and outcome guidelines standardized, the evidence remains insufficient for broad institutional investment or evidence-based adoption policy. 24
Conclusion
AR navigation shows notable accuracy benefits over freehand and fluoroscopic methods in pedicle screw placement, with studies confirming higher screw accuracy, fewer cortical breaches, and lower intraoperative blood loss. 21 Compared to CT-based and robotic navigation, AR has similar overall accuracy, but robotic systems achieve the optimal screw placement trajectory slightly better. 26 These findings show that AR navigation complements surgical expertise, reducing cognitive load and supporting precision without replacing the judgment needed for safe spine surgery. However, despite this evidence, workflow integration remains the main barrier to wider adoption. Setup demands, hardware limitations, high costs, and team adaptation hinder real-world use, especially outside high-volume academic centers.13 Looking ahead, the key advancements are in integrating AR navigation with robotic systems and artificial intelligence, which may improve registration accuracy and workflow efficiency. As these technologies develop and evidence grows, AR navigation is likely to become a standard part of modern spine surgery. l
NEW TECHNOLOGY
References
1. Mensah EO, Chalif JI, Baker JG, Chalif E, Biundo J, Groff MW. Challenges in contemporary spine surgery: a comprehensive review of surgical, technological, and patient-specific issues. J Clin Med. 2024;13(18):5460.
2. Sharma AK, de Oliveira RG, Suvithayasiri S, et al. The utilization of navigation and emerging technologies with endoscopic spine surgery: a narrative review. Neurospine . 2025;22(1):105–117.
3. Qin H, Huang S, Xu L, et al. Radiation exposure and operation time in percutaneous endoscopic lumbar discectomy using fluoroscopy-based navigation system. World Neurosurg. 2019;127:e39–e48.
4. Otomo N, Funao H, Yamanouchi K, Isogai N, Ishii K. Computed tomography-based navigation system in current spine surgery: a narrative review. Medicina (Kaunas, Lithuania). 2022;58(2):241.
5. Peltonen JI, Kaasalainen T, Kortesniemi M. Metal artifacts in intraoperative O-arm CBCT scans. BMC Med Imaging. 2021;21(1):2.
6. Hadgaonkar S, Gupta A, Aiyer S, Bhilare P, Sancheti P. Learning curve across 2000 thoracolumbar pedicle screw placements using O-arm navigation: technical difficulties and their solutions. Eur Spine J. 2023;32(11):3753–3763.
7. Virk S, Qureshi S. Navigation in minimally invasive spine surgery. J Spine Surg (Hong Kong) 2019;5(suppl 1):S25–S30.
8. Tabaraee E, Gibson AG, Karahalios DG, Potts EA, Mobasser JP, Burch S. Intraoperative cone beam-computed tomography with navigation (O-ARM) versus conventional fluoroscopy (C-ARM): a cadaveric study comparing accuracy, efficiency, and safety for spinal instrumentation. Spine . 2013;38(22):1953–1958.
9. Overley SC, Cho SK, Mehta AI, Arnold PM. Navigation and robotics in spinal surgery: where are we now? Neurosurgery. 2017;80(3S):S86–S99.
10. Liu A, Jin Y, Cottrill E, et al. Clinical accuracy and initial experience with augmented reality-assisted pedicle screw placement: the first 205 screws. J Neurosurg Spine . 2021;36(3):351–357.
11. Burström G, Persson O, Edström E, Elmi-Terander A. Augmented reality navigation in spine surgery: a systematic review. Acta Neurochirurgica. 2021;163(3):843–852.
12. Schütz L, Brendle C, Esteban J, Krieg SM, Eck U, Navab N. Usability of graphical visualizations on a tool-mounted interface for spine surgery. J Imaging. 2021;7(8):159.
13. Nadeem-Tariq A, Kazemeini S, Kaur P, et al. Augmented reality in spine surgery: a narrative review of clinical accuracy, workflow efficiency, and barriers to adoption. Cureus. 2025;17(6):e86803.
15. Loggia G, Alakmeh A, Avrumova F, et al. Accuracy of augmented reality navigation versus freehand pedicle screw placement. Spine . Published online December 11, 2025. https://doi. org/10.1097/BRS.0000000000005594
16. Elmi-Terander A, Burström G, Nachabé R, et al. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: a matched-control study comparing accuracy. Sci Reports . 2020;10(1):707.
17. Elmi-Terander A, Skulason H, Söderman M, et al. Surgical navigation technology based on augmented reality and integrated 3D intraoperative imaging: a spine cadaveric feasibility and accuracy study. Spine . 2016;41(21):E1303–E1311.
18. Edström E, Burström G, Persson O, et al. Does augmented reality navigation increase pedicle screw density compared to free-hand technique in deformity surgery? Single surgeon case series of 44 patients. Spine . 2020;45(17):E1085–E1090.
19. Jud L, Fotouhi J, Andronic O, et al. Applicability of augmented reality in orthopedic surgery - a systematic review. BMC Musculoskelet Disord. 2020;21(1):103.
20. Peh S, Chatterjea A, Pfarr J, et al. Accuracy of augmented reality surgical navigation for minimally invasive pedicle screw insertion in the thoracic and lumbar spine with a new tracking device. Spine J. 2020;20(4):629–637.
21. Taylor C, Lam C, Manoj N, Divekar O. The clinical impact of augmented reality surgical navigation on pedicle screw placement and its effect on perioperative outcomes: a systematic review. Spine Surg Relat Res. 2024;9(3):269–282.
22. Hiranaka Y, Takeoka Y, Yurube T, et al. The utility and feasibility of smart glasses in spine surgery: minimizing radiation exposure during percutaneous pedicle screw insertion. Neurospine . 2024;21(2):432–439.
23. Kong H, Wang S, Zhang C, Chen Z, Wu Z, Wang J. A novel pedicle screw placement surgery based on integration of surgical guides and augmented reality. J Neurol Surg A Cent Eur Neurosurg. 2025;86(4):383–389. https://doi.org/10.1055/a-2200-3585
24. Xiao SX, Wu WT, Yu TC, Chen IH, Yeh KT. Augmenting reality in spinal surgery: a narrative review of augmented reality applications in pedicle screw instrumentation. Medicina (Kaunas, Lithuania). 2024;60(9):1485.
25. Wolf J, Luchmann D, Lohmeyer Q, Farshad M, Fürnstahl P, Meboldt M. How different augmented reality visualizations for drilling affect trajectory deviation, visual attention, and user experience. Int J Comput Assist Radiol Surg. 2023;18(8):1363–1371. https:// doi.org/10.1007/s11548-022-02819-5
26. Altorfer FCS, Kelly MJ, Avrumova F, et al. Pedicle screw placement with augmented reality versus robotic-assisted surgery. Spine . 2025;50(15);1058–1064.
From the 1Department of Orthopaedics at the Hospital for Special Surgery in New York City, New York; 2 Department of Orthopedics at the University of Tsukuba Hospital in Tsukuba, Japan; and 3Weill Cornell Medical College in New York City, New York.
Artificial Intelligence Risk Prediction in Spine Surgery:
From ROC Curves to Clinical Decisions
Spine surgery encompasses a broad spectrum of procedures that carry substantial risks, with complications that may result in significant morbidity, such as infection, hardware failure, or neurological impairments.1 Accurate preoperative risk prediction remains a critical component. Historically, risk assessment in surgery has largely relied on individual judgement and heuristics, which can be highly variable and lead to diagnostic bias and preventable clinical error. 2,3 Additionally, risk assessment classification tools have faced challenges concerning limited predictive accuracy due to their reliance on a small subset of clinical variables. 4 Consequently, they are unable to capture the often complex and nonlinear interactions between risk factors in clinical practice.
Recent advances in integrating artificial intelligence (AI) and machine learning (ML) for spine surgery have demonstrated increasing promise in efficient management, processing, and analysis of patient data for effective surgical risk prediction by means of algorithms capable of learning complex patterns from large, multidimensional datasets. 5–7 Published studies demonstrate AI models’ ability to predict postoperative outcomes, such as readmission rates and patient-reported outcome measures, by
integrating more spine-specific complication data and a larger diversity of risk factors, such as surgical invasiveness, degree of sarcopenia, and genetic biomarkers. 5,8
However, a critical gap exists between published model performance and direct clinical utility at the point of care. Clinicians may encounter graphical representations of ML models such as receiver operating characteristic (ROC) curves and metrics such as area under the curve (AUC) values without a clear understanding of how these metrics can be translated into actionable clinical decisions. This review examines how modern developments in AI have refined risk prediction in spine surgery and how they influence clinical decision-making.
How AI Has Affected Risk Prediction in Spine Surgery
The emergence of AI in spine surgery research has fundamentally expanded the range of methods available to analyze clinical data. AI and modern ML methods enable
Adrian T.H. Lui, MBBS1
Christopher J. Yoo, BA1
Tomoyuki Asada, MD PhD1,2
Sravisht Iyer, MD1,3
integration of highly dimensional clinical, imaging, and perioperative data and the discovery of complex nonlinear patterns that conventional statistics had historically struggled to capture. 9,10 Furthermore, because healthcare datasets reflect real-world clinical practice, they are often affected by data inconsistencies and missingness, which are common obstacles in spine research.11 However, certain ML models can natively accommodate missing data, thereby mitigating its adverse impact on model performance and analytical validity.12
Despite the evolving complexity of AI modeling modalities, prediction models in spine research still rely on familiar statistical approaches such as logistic or linear regression. These are supervised learning models usually employed to train on retrospective clinical datasets to predict either binary or linear outcomes, and they remain valuable because of their ease of interpretability, ability to identify the independent contribution of individual preoperative variables to predicted outcomes, and relatively modest data requirements.13 Other models include tree-based models (random forests, gradient boosting) and neural networks, which are particularly adept at predicting nonlinear relationships.14 Regardless of the modeling approach, most prediction models follow the same structure: preoperative or perioperative patient characteristics are used to estimate the probability of a defined postoperative outcome.
Predictive performance depends on the quality and relevance of input variables. Demographic characteristics such as age,
sex, and body mass index, together with comorbidity indices such as the Charlson Comorbidity Index and American Society of Anesthesiologists classification, as well as clinical risk factors such as smoking and diabetes, represent the most consistently incorporated variables.15 Beyond these traditional variables, radiographic parameters have also emerged as important predictors, including spinopelvic alignment measures and morphological assessments of paraspinal muscle health, foraminal stenosis, and spondylolisthesis.16,17 More recently, biochemical and serological markers have begun to enter the predictive landscape, with preoperative laboratory values such as insulin-like growth factor-1 demonstrating early correlations with postoperative recovery.18 Collectively, these variables reflect the multidimensional clinical portrait of the surgical patient, and their systematic integration into ML frameworks enables a far more nuanced risk stratification than any single variable or traditional scoring system could provide in isolation.
The outputs that ML models can be trained to predict are equally diverse and can be used to infer preoperative state and to predict clinically meaningful postoperative events. Preoperatively, ML models have demonstrated utility in predicting bone mineral density and identifying osteoporosis from computed tomography imaging without the need for dedicated dual-energy X-ray absorptiometry imaging, as well as detection of spondylolisthesis through analysis of flexion-extension radiographs.19,20 However, the most clinically impactful and widely
studied application remains the prediction of postoperative outcomes, including failure to achieve a minimum clinically important difference on patient-reported outcome measures such as the Oswestry Disability Index, as well as discrete surgical complications, including pseudarthrosis, proximal junctional kyphosis, surgical site infection, and reoperations.14,21 This breadth highlights a defining advantage of ML over traditional statistical methods: its capacity to integrate interacting clinical, radiographic, biochemical, and surgical variables to predict outcomes of direct relevance to both patients and surgeons. As these tools inform clinical decision-making, clinicians must
Figure 1. Receiver operating characteristic (ROC) curve illustrating the trade-off between sensitivity and specificity at 2 risk probability thresholds (T = 20%, T = 90%). The diagonal dashed line represents a random classifier (area under the curve [AUC] = 0.50). FPR = false positive rate; TPR = true positive rate.
understand how models are evaluated. In particular, the ROC curve and its summary statistic, AUC, represent the most reported metrics of model discrimination in spine surgery research.
What Are ROC Curves and AUC?
The ROC curve is a graphical representation of a model’s ability to distinguish between high-risk patients (positive class) and low-risk patients (negative class). 22 It displays different risk probability thresholds as points along a curve and allows for determination of sensitivity and specificity of each threshold value (Figure 1). A model with no discriminatory ability (equivalent to random guessing) produces an ROC curve that follows the diagonal line from (0,0) to (1,1), while an ideal model that perfectly separates patients who will and will not experience the outcome produces a curve that reaches the upper-left corner, achieving 100% sensitivity and 100% specificity. 23
To translate these predicted probabilities into binary classifications, such as high-risk or low risk, a decision threshold must be identified. Different thresholds yield opposing trade-offs between sensitivity (true positive rate) and specificity (true negative rate). 24 A lower threshold (eg, ≥20%) increases sensitivity and allows the model to capture more patients who may experience the outcome, but in turn, decreases specificity, resulting in more false positives. Conversely, a higher threshold (eg, ≥80%) increases specificity but may miss true cases.
The AUC provides a single summary measure of discriminatory performance,
illustrating the overall ability to distinguish between positive and negative risk classes. 25 It represents the probability that the model assigns a higher predicted risk to a randomly selected patient who experiences the outcome compared to a randomly selected patient who does not. AUC values range from 0.5 (no discrimination, equivalent to random chance) to 1.0 (perfect discrimination). By convention, AUC values of 0.70–0.80 are considered acceptable, 0.80–0.90 as excellent, and >0.90 as outstanding, though these thresholds are often arbitrary and context dependent. 26 The AUC can also be used for simple comparison of relative performance between different prediction models. 27 While the AUC characterizes a model’s ability to discriminate between high-risk and low-risk patients, it does not indicate the accuracy of risk estimation. 28 The clinical decision of whether to proceed with surgery, modify the surgical plan, or counsel against intervention may require considerations besides discrimination alone.
Translating ROC Curves Into Clinical Decisions: A Practical Example
To illustrate how ROC curve analysis can inform clinical decision-making, consider a hypothetical ML model trained to predict pseudarthrosis following lumbar spinal fusion. The model incorporates preoperative variables including age, body mass index, smoking, bone mineral density, diabetes, and surgical invasiveness, and it achieves an AUC of 0.83 – indicating a strong discriminatory ability to distinguish patients who will from those who will not develop pseudarthrosis.
ROC curve analysis identifies an optimal probability threshold of 35%, at which the model achieves a sensitivity of 79% and specificity of 74%.
In practical terms, a patient whose preoperative profile generates a predicted pseudarthrosis probability above 35% is classified as high-risk. For this binary, highstakes complication, this classification alone is clinically actionable and is sufficient to prompt targeted preoperative optimization such as smoking cessation and bone quality optimization, as well as intraoperative considerations such as augmented fixation strategies or adjunctive use of bone morphogenetic protein. It may also inform a more detailed informed consent discussion around the possibility of reoperation. For a complication of this consequence, knowing that the patient crosses the high-risk threshold is enough to change management.
This example illustrates the clinical utility of a well-constructed ROC model for discrete, high-stakes outcomes: when the consequence of a complication is severe and the clinical response to a high-risk classification is predefined, AUC and threshold-based classification can translate meaningfully into surgical decision-making. As discussed below, however, not all outcomes lend themselves to this threshold-based approach equally well, and AUC alone does not capture the full picture of a model’s clinical utility.
What Challenges and Limitations Does AI Face in Spine Research?
Despite their promise, AI-based prediction models in spine surgery face several import-
ant limitations that clinicians must recognize when appraising the literature. A critical and consistently overlooked limitation is the distinction between discrimination and calibration. While AUC summarizes how well a model rank-orders patients by risk, it says nothing about whether the predicted probabilities themselves are accurate. This distinction has direct clinical consequences. For severe, discrete complications such as major cardiopulmonary events or perioperative mortality, a high AUC model with a well-chosen risk threshold may be genuinely actionable: identifying a patient as having considerable risk is itself informative enough to prompt surgical delay, medical optimization, or reconsideration of the procedure. However, for more nuanced outcomes, such as failure to achieve a clinically meaningful improvement in neurological function or disability, the exact predicted probability becomes far more important. A surgeon may proceed in a patient with a 30% predicted risk of functional nonimprovement if the alternative is progressive deformity or intractable pain, yet the surgeon may reconsider at 60% predicted risk. In this context, a poorly calibrated model that systematically overestimates or underestimates risk does not only underperform statistically, but also actively distorts the risk-benefit conversation at the point of care. Calibration, assessed through calibration plots, is the metric that captures this accuracy, yet it remains rarely reported in the spine surgery literature. 29
Closely related is the issue of external validation, the testing of a model on independent patient populations from different institutions.
Strong internal performance, even with high AUC, is insufficient to establish that a model generalizes beyond the dataset from which it was derived.30 Spine surgery populations vary considerably across institutions in case mix, surgical technique, and postoperative care pathways, all of which can substantially alter the relationship between predictive variables and outcomes. Without prospective external validation across diverse patient populations, even well-constructed models risk encoding institutional idiosyncrasies rather than generalizable clinical signal.
Additional limitations relate to the underlying data and modeling process itself. Spine surgery ML models are frequently trained on retrospective, single-institution datasets subject to inconsistent variable definitions, coding errors, and incomplete follow-up, all of which introduce systematic bias that no amount of computational sophistication can fully correct. Compounding this is the risk of overfitting, whereby a model learns the specific patterns of its training data so precisely that it fails to perform on new patients—a risk that increases with model complexity and is not captured by internal validation metrics alone.
Future Directions
For AI prediction models to become clinically useful in spine surgery, changes in how they are developed and reported will be necessary. Future studies should routinely report calibration alongside AUC. Recognizing that clinical utility also depends on the accuracy of predicted probabilities, not merely the ability to rank patients by relative risk, is
also important. External validation across diverse, multi-institution cohorts should be considered a prerequisite for clinical adoption rather than an optional subsequent study. Standardized reporting frameworks such as TRIPOD and its AI-specific extension, TRIPOD+AI, provide a practical foundation for this shift, and their wider adoption by spine surgery journals as both author guidance and reviewer expectation would meaningfully raise the evidentiary standard. 31 Ultimately, the goal is not to build models with impressive performance metrics but to develop tools whose outputs are accurate and generalizable enough to genuinely inform the risk conversations that surgeons and patients have together before any operation.
Conclusion
AI and machine learning models have demonstrated a meaningful capacity to inform preoperative risk assessment and support clinical decision-making in spine surgery, offering a pathway from complex multidimensional data to actionable, patient-specific risk stratification. Realizing this potential, however, requires clinicians to engage critically with how these models are evaluated and understand that an ROC curve illustrates discriminatory performance, and that translating a predicted probability into a clinical decision demand more than a statistically derived threshold. Clinicians, researchers, and journal reviewers should hold AI tools to a higher standard before clinical adoption, particularly as these technologies move closer to the point of care. l
References
1. Swann MC, Hoes KS, Aoun SG, McDonagh DL. Postoperative complications of spine surgery. Best Pract Res Clin Anaesthesiol. 2016;30(1):103-120.
2. Loftus TJ, Tighe PJ, Filiberto AC, et al. Artificial intelligence and surgical decision-making. JAMA Surg. 2020;155(2):148.
3. Healey MA. Complications in surgical patients. Arch Surg 2002;137(5):611-618.
4. Pajak A, Samuel JT, Subramanian T, et al. Do publicly available risk calculators apply to adult spinal deformity surgery? J Clin Med. 2025;14(24):8618.
5. Ton A, Wishart D, Ball JR, et al. The evolution of risk assessment in spine surgery: a narrative review. World Neurosurg. 2024;188:1-14.
6. Benzakour A, Altsitzioglou P, Lemée JM, Ahmad A, Mavrogenis AF, Benzakour T. Artificial intelligence in spine surgery. Int Orthop. 2023;47(2):457-465.
7. Scheer JK, Ames CP. Artificial intelligence in spine surgery. Neurosurg Clin N Am. 2024;35(2):253-262.
8. Merali ZG, Witiw CD, Badhiwala JH, Wilson JR, Fehlings MG. Using a machine learning approach to predict outcome after surgery for degenerative cervical myelopathy. PLoS ONE . 2019;14(4):e0215133.
9. Galbusera F, Casaroli G, Bassani T. Artificial intelligence and machine learning in spine research. JOR Spine . 2019;2(1):e1044.
10. Browd SR, Park C, Donoho DA. Potential applications of artificial intelligence and machine learning in spine surgery across the continuum of care. Int J Spine Surg. 2023;17(S1):S26-S33.
11. Meyer B, Shiban E, Albers LE, Krieg SM. Completeness and accuracy of data in spine registries: an independent audit-based study. Eur Spine J. 2020;29(6):1453-1461.
12. Huang CC, Peng KP, Hsieh HC, et al. Does the presence of missing data affect the performance of the SORG machine-learning algorithm for patients with spinal metastasis? Development of an internet application algorithm. Clin Orthop Relat Res . 2024;482(1):143-157.
13. Lubelski D, Hersh A, Azad TD, et al. Prediction models in degenerative spine surgery: a systematic review. Global Spine J. 2021;11(1 suppl):79S-88S.
14. Adida S, Legarreta AD, Hudson JS, et al. Machine learning in spine surgery: a narrative review. Neurosurgery. 2024;94(1):53-64.
15. Kim JS, Merrill RK, Arvind V, et al. Examining the ability of artificial neural networks machine learning models to accurately predict complications following posterior lumbar spine fusion. Spine . 2018;43(12):853-860.
16. Schönnagel L, Caffard T, Vu-Han TL, et al. Predicting postoperative outcomes in lumbar spinal fusion: development of a machine learning model. Spine J. 2024;24(2):239-249.
17. Rasouli JJ, Shao J, Neifert S, et al. Artificial intelligence and robotics in spine surgery. Global Spine J. 2021;11(4):556-564.
18. Bay A, Kim HJ, Durbas A, et al. Association of insulin-like growth factor 1 serum levels with early recovery and in-hospital complications after spinal fusion: presented at the 2025 AANS/ CNS Joint Section on Disorders of the Spine and Peripheral Nerves. J Neurosurg Spine . 2025;43(5):593-600.
19. Zhang B, Yu K, Ning Z, et al. Deep learning of lumbar spine X-ray for osteopenia and osteoporosis screening: a multicenter retrospective cohort study. Bone . 2020;140:115561.
20. Trinh GM, Shao HC, Hsieh KLC, et al. Detection of lumbar spondylolisthesis from x-ray images using deep learning network. J Clin Med. 2022;11(18):5450.
21. Lubelski D, Alentado V, Nowacki AS, et al. Preoperative nomograms predict patient-specific cervical spine surgery clinical and quality of life outcomes. Neurosurgery. 2018;83(1):104-113.
22. Fawcett T. An introduction to ROC analysis. Pattern Recognition Letters . 2006;27(8):861-874.
23. Çorbacıoğlu ŞK, Aksel G. Receiver operating characteristic curve analysis in diagnostic accuracy studies: A guide to interpreting the area under the curve value. Turk J Emerg Med. 2023;23(4):195-198.
24. Perkins NJ, Schisterman EF. The inconsistency of “optimal” cutpoints obtained using two criteria based on the receiver operating characteristic curve. Am J Epidemiol. 2006;163(7):670-675.
25. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1):29-36.
26. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. 2010;5(9):1315-1316.
27. Hajian-Tilaki K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Caspian J Intern Med. 2013;4(2):627-635.
28. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115(7):928-935.
29. Canturk TC, Czikk D, Wai EK, et al. A scoping review of complication prediction models in spinal surgery: an analysis of model development, validation and impact. N Am Spine Soc J. 2022;11:100142.
30. Kundu S, Mazumdar M, Ferket B. Impact of correlation of predictors on discrimination of risk models in development and external populations. BMC Med Res Methodol. 2017;17(1):63.
31. Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024;385:e078378. doi:10.1136/bmj-2023-078378
From the Department of Orthopaedic Surgery at the University of California, Irvine, School of Medicine in Costa Mesa, California.
Peptides in Spine Surgery:
Current Evidence
The use of peptides has become more common in spine surgery.1
The simplest definition of a peptide is a short chain of amino acids. Amino acids have many essential functions in the human body. Amino acids are essential building blocks of protein. Proteins are enzymes, hormones, and neurotransmitters that control and regulate the body’s functions. Peptides act to signal molecules to repair tissue, produce collagen, reduce
inflammation, and enhance bone formation ( Figure 1). Many peptides are commonly used in spine surgery today. The most well-known peptides are BPC-157, P-15, and CJC-1295. This article discusses the use of these peptides in spine surgery today and reviews the literature regarding their use. One of these peptides may assist with chronic pain, another promotes spinal fusion, and the last increases generalized strength and recovery of muscles.
Figure 1. Anteroposterior view (left) and lateral view (right) of 67-year-old woman who had a C5-6, C6-7 anterior cervical discectomy and fusion with P-15 in an allograft strut.
Yu-Po Lee, MD
EMERGING THERAPIES
BPC-157
BPC-157 (Body Protection Compound-157) is a gastric peptide that is being evaluated for its role in healing musculoskeletal injuries such as fractures, tendon injuries, ligament tears, and muscle injuries. Although it does not have US Food and Drug Administration approval and is currently not allowed in professional sports, there is a growing interest in BPC-157.1 Vasireddi et al performed a literature review on BPC-157 and identified a total of 544 relevant articles published between 1993 and 2024, including 36 studies (35 preclinical studies, 1 clinical study).1 In preclinical models, BPC-157 was noted to improve functional, structural, and biomechanical outcomes in muscle, tendon, ligament, and bony injuries. 1 In preclinical animal models, BPC-157 was not associated with acute (<6 weeks) gross or histologic toxicity across several organs, including the liver, spleen, lung, kidney, brain, thymus, prostate, and ovaries.1 Of note, all of these studies focused on musculoskeletal applications rather than spinal applications.
So far, only one clinical study has been performed. In that study, Lee and Padgett performed a retrospective review on patients who had a BPC-157 injection for knee pain. 2 Patients were asked to rate their pain prior to the injection, the length of time the peptides helped ease the pain, and the degree to which the injection helped them. No specific tools were used to measure their improvement in function, quality of life, stiffness, or activities of daily living. Furthermore, radiographs and advanced
“Peptides act to signal molecules to repair tissue, produce collagen, reduce inflammation, and enhance bone formation. In spine surgery, of the three most well-known peptides, one may assist with chronic pain, another promotes spinal fusion, and the last increases generalized strength and muscle recovery.”
imaging were not reported. Of the 16 patients, 12 had received only BPC-157 as an intra-articular injection. In this group, 11 of the 12 patients (91.6%) had significant improvement in knee pain, whereas one patient (8.3 %) had no improvement. The other 4 patients received a combination of BPC-157 and Thymosin Beta-4 (TB4), which is a regenerative peptide that promotes tissue repair and wound healing. Of the patients who received both peptides, 3 showed significant improvement, but 1 had no relief from their knee pain. Overall, 14 of 16 patients (87.5%) had relief of their knee pain when BPC-157 or a combination of BPC-157 and TB4 was used. However, no follow-up imaging or histological studies were conducted to evaluate the effectiveness of BPC-157 in healing tissues. 2
There is interest in using BPC-157 in patients with chronic back pain to promote
EMERGING THERAPIES
muscle healing of the back extensor muscle or aid in facet-mediated pain. However, when discussing BPC-157 with patients in any orthopedic application, it is important to bear in mind that there are limited clinical data.
P-15
P-15 (i-FACTOR, Cerapedics, Westminster, CO, USA) is a small synthetic peptide that is identical in sequence to the cell-binding domain of type I collagen. 3 There is a growing demand for synthetic bone graft materials in spine surgery. P-15 stimulates new bone formation by enhancing osteogenic cell attachment, proliferation, and differentiation. A literature review was performed by Spanninga et al, who identified 9 clinical articles on P-15. 3 In one study, Arnold et al published their 6-year results on the efficacy of i-FACTOR when used for single-level anterior cervical discectomy and fusion (ACDF).4 Radiographic fusion was achieved in 99% (103/104) of i-FACTOR cases and in 98.2% (109/111) of local autograft subjects.
In another study, Lauweryns et al evaluated the efficacy of P-15 in comparison to local autograft when used for fusion in a posterior lumbar interbody fusion. 5 The authors found that intra-cage bridging bone occurred earlier with local autograft and P-15 than with local autograft alone (97.73% vs. 59.09% at 6 months). Andresen et al reported their 5-year results from a randomized controlled trial of 58 patients comparing P-15 to local autograft mixed with allograft. 6 At 5-year computed tomography follow-up, 60% in the P-15 group vs
30% in the allograft group were classified as fused ( p = 0.037). There were no differences in complication, reoperation, or infection rates between the 2 groups. Overall, the fusion rates with P-15 seemed to be at least noninferior to local bone and work well as a bone graft extender/enhancer. It will be interesting to see the success rate in multilevel cases or in high-risk patient populations.
CJC-1295 and Growth Hormone Pathways
CJC-1295 is a synthetic growth hormone-releasing hormone (GHRH) analog that stimulates the pituitary gland to increase growth hormone (GH) and IGF-I levels. It is administered via subcutaneous injection. In a study by Teichman et al, the authors performed a randomized, placebo-controlled trial evaluating the effect of subcutaneous CJC-1295 injections.7 The authors found that subcutaneous administration of CJC1295 resulted in sustained, dose-dependent increases in GH and IGF-I levels in healthy adults and was safe and relatively well tolerated.
There is the theory that elevating GH and IGF-I can increase muscle mass, physical strength and performance, and sleep and cognition. 8 Short-term treatment studies have shown that GHRH can enhance GH secretion and elevate IGF-I levels. Some studies have shown that GHRH may promote sleep and that these agents are well tolerated.8 Longer-term studies assessing the effects on body composition and physical and psychological function are underway.
EMERGING THERAPIES
Specific spine applications are yet to be investigated but may play a role in chronic pain and surgical recovery.
Current Limitations and Future Directions
Involvement in peptide-based therapies in bone formation, tissue repair, and inflammatory pathways has led to an increased interest in spine surgery. However, future implementation is limited in supporting their clinical application of musculoskel -
etal conditions, and especially in spinal pathology. Early research indicates that drugs like BPC-157, P-15, and CJC-1295 may influence biological processes related to musculoskeletal recovery, but most available data are derived from preclinical models or limited clinical trials. To further understand their safety, efficacy, and potential role in spinal therapeutics, larger prospective clinical trials are required. Studies are currently being performed to answer these questions. l
References
1. Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging use of BPC157 in orthopaedic sports medicine: a systematic review. HSS J. 2025:15563316251355551.
2. Lee E, Padgett B. Intra-articular injection of BPC 157 for multiple types of knee pain. Altern Ther Health Med. 2021;27(4):8-13.
3. Spanninga BJ, Hoelen TA, Johnson S, et al. Clinical efficacy and safety of P-15 peptide enhanced bone graft substitute in surgical bone regenerative procedures in adult maxillofacial, spine, and trauma patients: a systematic literature review. Bone Joint Res . 2025;14(2):77-92.
4. Arnold PM, Vaccaro AR, Sasso RC, et al. Six-year follow-up of a randomized controlled trial of i-FACTOR peptide-enhanced bone graft versus local autograft in single-level anterior cervical discectomy and fusion. Neurosurgery. 2023;92(4):725-733.
5. Lauweryns P, Raskin Y. Prospective analysis of a new bone graft in lumbar interbody fusion: results of a 2- year prospective clinical and radiological study. Int J Spine Surg. 2015;9:2.
6. Andresen AK, Carreon LY, Overgaard S, Jacobsen MK, Andersen MØ. Safety and reoperation rates in non-instrumented lumbar fusion surgery: secondary report from a randomized controlled trial of ABM/P-15 vs allograft with minimum 5 years follow-up. Global Spine J. 2024;14(1):33-40.
7. Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805.
8. Merriam GR, Buchner DM, Prinz PN, Schwartz RS, Vitiello MV. Potential applications of GH secretagogs in the evaluation and treatment of the age-related decline in growth hormone secretion. Endocrine . 1997;7(1):49-52.