International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056

Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056
Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
1 FINAL YEAR PG STUDENT, St. Xavier’s Catholic College of Engineering 2 ASSOCIATE PROFESSOR St. Xavier’s Catholic College of Engineering ***
Fetal MRI volumetry is a valuable method yet it is restricted by a reliance upon movement free sweeps, monotonous manual division, and spatial error because of thick slice checks. A picture handling pipeline that locations these impediments was created and tested. The chief successionsgainedinfetalMRIclinicalpracticearedifferent symmetrical single- shot quick twist reverberation checks. Cutting edge picture handling methods were utilized for between cut movement adjustment also, super-goal recreation of high-goal volumetric pictures from these outputs. The recreated volume pictures were processed with force non-consistency amendment furthermore, the fetal mind removed by utilizing directed robotized segmentation. Reconstruction, division and volumetry of the fetal cerebrums for a partner of 25 clinically procured fetal MRI filters was finished. Execution measurements for volume reproduction, division and not entirely set in stone by contrasting with manual drawings in five arbitrarily picked cases. At long last, examination of the fetal mind and parenchymal volumes was performed in view of the gestational age of the babies. The picture handling pipeline created in this study empowers volume delivering and precise fetal cerebrum volumetry by tending to the impediments of current volumetry methods, which remember reliance for movement free filters, manual division,anderroneousthick-cutinsertion.
Abstract
Key Words : Fetal MRI · Brain volumetry ·Image reconstruction · Segmentation
Theprogressfrom woman tomotherhoodhasbeengiven significance from days of yore. The parenthood is a wonderful stage in ladies' life. During pregnancy, care to themotherandhatchlingarefundamental.Inthisperioda few pregnancy related issues are happen to the mother. Mother might experience a few medical issues, such as morning disorder, clogging, gestational diabetes, queasinessandretching,visionissuesandsoon.Similarly significant is the wellbeing of the baby and its turn of events. In this way the baby is to be checked persistently
till its introduction to the world. The existence of a baby insidethemother'sbellyisseparatedintothreeperiods.
In-vivo fetal imaging procedures, for example, ultrasonography and attractive reverberation imaging (MRI) areof central significanceinassessingand deciding the improvement of the hatchling. Biometric regulating values for gestational age (GA) have been laid out in-vitro by assessment of fixed minds, and furthermore through estimating huge partners of sameage babies utilizing ultrasonography.FetalMRIisasomewhatmoreuptodate methodology, used in the assessment of high-risk pregnancies where there is worry for peculiarities in light of distinguished chances, like high level maternal age, family ancestry, maternal openings, and irregularities identified by routine pre-birth ultrasound. X-ray has been helpful in assessing anomalies of fetal designs which are hard to completely survey by pre-birth sonography alone, like those including the fetal mind, chest, and aviation route. X-ray doesn't include ionizing radiation, affects either the pregnant patient or the hatchling, and enjoys numerous upper hands over sonography, including that it is less restricted by diminished amniotic liquid, maternal corpulence, or troublesome fetal position. Fetal cerebral biometry principally includes length estimates which are evaluated by obstetric imagers on two-layered sees. The most generally acquired proportions of fetal mind size incorporate cerebral and skull biparietal width (BPD), occipito front facing measurement (OFD), and head periphery (HC). Cross over cerebellar width, vermian profundity and level, corpus callosal length, and the size and distance between circles are likewise every now and again estimated . Regularizing biometric values have been gottenthroughevaluationsofextremelyhugeassociatesof fetal sonographic pictures. Reference biometric values for thefetalcerebrumhavebeenasoflateacquiredinlightof huge arrangements of MRI pictures of 589 hatchlings [6]. Thehighlevelimagingadvancementspast2Dsonography, for example 3D ultrasound and MRI, lead to more illustrative biometric measures in view of the volume and state of fetal organs and designs. Fetal mind volumetry is viewedascriticalintheassessmentoffetalturnofevents. Atypicalpregnancyperiodasarulerangesbetween38to
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056
Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
42 gestational weeks (GW). The pregnancy is partitioned into three-month time frames called trimesters. First Trimester(0to13GW):Theinitial three-monthtrimester is by and large determined as beginning the initial day of the last time frame and goes through the thirteenth seven day stretch of the pregnancy. During this trimester, the embryoinsertsintothebellyofthelady.SecondTrimester (14to27GW):Thisperiod beginsinthefourteenthseven day stretch of the pregnancy and goes through the 27th week. During the second trimester, the hatchling starts to quickly develop. By about the twentieth seven day stretch of the incubation time frame, most ladies will start to feel development of the embryo. Third Trimester (28 to conveyance): This period begins in the 28th seven day stretch of the development time frame and goes through the introduction of the youngster. During this period, the hatchling expansions in size and stretches the uterus and mid-region of the lady. In the initial segment of the third trimester,the embryowill beatitsgenerallydynamicand development will be hard to miss. As the kid occupies the accessible space, development will turn out to be less yet more grounded and the lady will turn out to be more awkward. The fetal mind is a unique construction, radiologists genuinely must get to know the ordinary appearance of the fetal cerebrum at various GW to be better ready to recognize and portray fetal cerebrum irregularities . During the most recent twenty years, fetal mental health has turned into a significant subject in neuroscience because of current painless and computational procedures. The consequences of such methods permit quantitative depiction of the fetal mind structure, which incorporates improvement of individual nerve cells and whole organizations inside unambiguous cerebrum regions . A few surveys on fetal mental health showed up during the past. In-vivo fetal imaging is a significant method in envisioning and assessing the advancement of fetal designs, particularly for fetal cerebrum.Whileittendstobeexceptionallypulverizingto figure out that the embryo has an irregularity, pre-birth determination can permit time to settle on informed choices. Research investigations of fetal MRI of ordinary cerebrums at various GW permit laying out of standardizing measures that can be utilized in early distinguishing proof of formative mind irregularities. Research examinations keep on distinguishing a rising number of explicit quality imperfections for mind distortions.Theeffectiveconveyanceofhereditarymaterial to the creating fetal mind addresses an advancement in concentrating on mental health and treating of various deadly cerebrum problems. Fetal MRI, particularly with utilizing new arrangements, can possibly characterize underlying,physiological,andmetabolicpartsofcerebrum
contortionsthatcanupholdresearchonqualitytreatment andleadtothetreatmentoravoidanceofthesesicknesses.
Many articles have tended to fetal cerebrum volumetry utilizingbothMRIand3Dultrasound[7-16],howeverlittle advancementhas beenmadeinthecalculationtechniques utilized.Moststrategiesdependonthe(changed)Cavalieri technique for fair-minded volume assessment. Based on theCavalieriguideline,an unprejudicedassessment ofthe mean absolute volume of an arbitrary shaped item can be acquired from the areas on systematic uniform-arbitrary cuts (areas). A few strategies exist for assessment of the areas of cuts, yet the most effective strategy is viewed as point-counting. Early MRI-put together volumetry techniques [10,11] depended with respect to cuts as thick as 10mm which incite too extraordinary an estimation mistake for tiny fetal mind sizes (for example 50th percentile typical cerebral BPD is 80mmfor a 35weekGAfetus).Comparablevolumetrystrategiesinlight of ultrasonography [7,13] likewise depend on manual following and estimation of the area of 8-10 sequential coronal cuts. In these examinations, the fetal cerebrum volumeisassessedviaconsequentlyaddingverticalround andhollow in themiddle of between thecuts whichlooks like a direct insertion between thick-cut areas. In another examination in light of ultrasound [16], a circular shape was expected for fetal head and the assessed volumes werecontrastedwithdistributedposthumousinformation on fetal brain weight matched for GA also, the particular gravity of the brain. An assessment factor was consequently got for mind volumetry. In different examinations [8,12], mind volumetry was performed by choosing the best unique single-shot quick twist reverberation(SSFSE)X-rayexaminesgotduringasolitary filtering meeting. Volume Calculation was acted in these examinations through devoted programming, however oncemore,thecomputation wasinviewofMRIsweepsof 4-5mm cut thickness and utilization of manual tracing. Volumetry was performed for ten babies in [12] and for fifty embryos of 17-37 weeks GA in [8]. The length of the time expected to perform manual drawings has been distinguished as a significant constraint [8].Three basic impediments exist in fetal cerebrum MRI volumetry strategies; first, fetal and maternal motion may fundamentally debase the MRI examines and their reasonablenessforvolumetryestimation. Albeit topnotch cuts are regularly gotten by SSFSE because of short cut obtaining time, serious inter slice movement actuated contrasts often show up in out of- plane perspectives. Accordingly, the gained SSFSE outputs can seldom be
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056
Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
resampled and meant satisfactory volumetric pictures. Second, thick cuts (ordinarily 3-5mm) are gained in fetal MRI to keep a high sign to-commotion proportion. This constraint brings about significant estimation mistakes in resamplingandvolumetry,explicitlywhilelookingat little measured fetal designs. Third, physically following and dividing fetal cerebrum structures is dreary and tedious, altogether lessening interest in the standard utilization of fetal cerebrum volumetry. To address the impediments of fetal mind MRI volumetry methods, we have fostered a picture handling pipeline in light of between cut movement revision, super goal volume remaking, force non-consistency remedy and directed division. Our technique depends on an as of late evolved strategy for super-goalvolumeremakingfromcutacquisitions[17,18]. The created strategy gives high-goal volumetric pictures which address reasonable anatomic limits that are not clear in unique SSFSE filters. Accordingly, the remade volumetricpicturespermittedustocreatedirectedpicture division procedures to work on the exactness and simplicityofacquiringexactfetalcerebrumvolumetry.
Fetal cerebrum MRI includes various single-shot quick twist reverberation (SSFSE) picture acquisitions in the symmetrical perspectives on the hatchling which typically give high-goal and great cuts within the sight of discontinuous fetal and maternal movement. In any case, because of thick-cut acquisitions and between cut movement, these pictures don't mirror the anatomic subtleties and cognizant tissue limits in the three layered seeshencecan'tbeactuallyutilizedfortissuedivisionand exact mind volume attempt. A portrayal of our picture handlingpipelineinlightofmovementrevision,super-goal volume recreation, and managed mind tissue division whichpermitsexactfetalcerebrumvolumetry
Fig-1 SystemArchitectureTherehavebeenacoupleofongoingexaminationstending to high resolution volumetric picture recreation from numerous multislice MRI filters [22-24]. These methods depend on between cut movement adjustment and dispersed information insertion (SDI) for volumetric pictureremaking.Therearespecializedcontrastsbetween these strategies in light of movement remedy draws near and the SDI strategies utilized [22-24]. By the by, these methods don't give an fitting numerical plan to legitimize that the recreated volume is a base mistake portrayal of the fundamental life systems given the gained thick-cut checks. In our recent work on super-goal volume recreation from cut acquisitions [17,18], we fostered a numerical structure for mistake minimization in light of a cut
Acquisition model. This approach thinks about an actual modelfortheSSFSEchecksaspilesofthickcutssituatedin the three-layered space. The cut securing model is a forward model, which depicts how the procured cuts are gotten from the imaged object during the MRI cut procurementtechnique.
Figure 1 portrays a straightforward chart of the cut procurement model. This model integrates movement of the imaged object in three-layered space and the MRI cut securing process which includes cut choice, signal obtaining, quantization also, examining. The result is a computerizedportrayalofathickcutoftheimagedobject. Inthesuper-goalvolumeremakingplan,adiscreteformof thismodelisviewedasinwhichtheinformationisanideal high-goal volumetric portrayal of the imaged object. The info and result pictures are addressed by vectors of the picture voxels in the lexicographical request. All the picture administrators between the info furthermore, the result can be demonstrated as grid tasks, consequently a straight model portrayal is accomplished. The super-goal volume remaking is accordingly characterized as the converse issue of tracking down the ideal high-goal portrayal of the imaged object given an adequate number ofobtainedcut examines. Thedefinitionandarrangement ofthisstraightbackwardsissueiscompletelytalkedabout in[17]and[18].
On super-goal volume recreation from cut acquisitionsA numerical system for mistake minimization in light of a cut procurement model. This approach considersanactual model fortheSSFSEchecksaspiles of
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056
Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
thick cuts situated in the three-layered space. The cut securingmodelisaforwardmodel,whichdepictshowthe gained cuts are gotten from the imaged object during the MRI cut obtaining technique. portrays a straightforward graphof thecutobtaining model. Thismodel consolidates movementoftheimagedobjectinthree-layeredspaceand the MRI cut obtaining process which includes cut determination, signal procurement, quantization and examining. The result is a computerized portrayal of a thick cut of the imaged object. In the super-goal volume reproduction plan, a discrete variant of this model is viewedasinwhichtheinfoisanidealhigh-goalvolumetric portrayaloftheimagedobject.Theinformationandresult pictures are addressed by vectors of the picture voxels in the lexicographical request. All the picture administrators betweentheinfoandtheresultcanbedisplayedaslattice tasks, in this manner a direct model portrayal is accomplished. The super-goal volume recreation is consequently characterized as the converse issue of finding the ideal high-goal portrayal of the imaged object givenanadequatenumberofgainedcutfilters.
Cut movement assessment in fetal MRI is very troublesome. This procedure is like the strategies utilized execution contrasts in view of the expense capabilities utilized and the improvement methods. In cut to-volume enrollment, the movement boundaries of each cut are figured by enlisting that cut to a reference volume. For each cut, a 6 level of-opportunity three-layered inflexible change is figured by limiting the mean square power contrasts (MSD) between that cut and the reference volume. By the by, a high-goal reference volume isn't accessible for this reason. Accordingly, a guess of the remade volumetric picture is utilized as the reference for enlistment.Thisguessisatfirstregisteredasthenormalof the resampled SSFSE checks and is worked on through cyclesofcutmovementassessmentandsuper-goalvolume remaking. After cut to-volume enrollment, the cut picture voxelswon'tbeonanordinarymatrixandareconsidered as dispersed data of interest in the three-layered space. Dispersed information introduction (SDI) is expected to get a first assessment of the remade volume picture from this information. The SDI approach used here depends on nearby force infusion through Gaussian bits. The dissipated information focuses got from movement amendedcutsareplannedtotheirclosestneighbormatrix focuses in the reproduced picture space, and their force values are infused into the local focuses through Gaussian portion loads. This underlying appraisal of the recreated
volume is refined through greatest probability super-goal volume remaking created to this whole iterative reproduction calculation as ML-SVR here, for most extremeprobabilitysuper-goalvolumereproduction.
The correction of intensity non-uniformity is crucial prior to automated image segmentation. The intensity nonuniformity artifacts can be severe in fetal images due to weak signal, fetal positioning, cardiac coil placement, and magnetic field bias. We use the fully automatic entropy minimizationapproachofManginfor estimatinga smooth multiplicativefieldforintensitynon-uniformitycorrection . The idea is to find the parameters of a regular grid of points with cubic Spline interpolation as a smooth model ofthecorrectionfield(Fc).
Fopt c = argfc min Fc [KH H (FcX) + KR R (Fc) + KM M (FcX)]
where X is the reconstructed volumetric image, H (FcX) is the entropy of the corrected image, R (Fc) is a regularization function which measures the field smoothness, and M (FcX) is a quadratic measure of the distance between the reconstructed volume and the correctedvolume.TheweightingconstantsaresetasKH= 1,KR=0.01,andKM=0.5,andthegridpointspacingwas setbetween32and64mm inour experimentsdepending onthesizeoftheimageandtheintensitydistortions.
Segmentation of fetal MRI images is very challenging due to low resolution, low signal contrast, the differences in developingbraintissuetypes,andmotionandintensityno uniformityartifacts.Therefore,mostofthestudiesonfetal brainvolumetryrelyonmanualtracingsforsegmentation of original thick-slice SSFSE scans. The super-resolution reconstruction of high-resolution volumetric images discussedearlierallowsustouseautomatedsegmentation algorithmsmoreeffectively.Sinceourgoalisbrainvolume try, we focus on the segmentation of brain tissue and cerebrospinalfluid(CSF).Bonestructuressuchasskullare hypointenseandtheCSFishyperintenseonT2-weighted fetal MRI images, so if the motion artifacts and intensity non-uniformityareeffectivelycorrectedbythealgorithms discussed in the previous sections, automated segmentation is feasible. Nevertheless, due to the complexity and high variability of the developing brain tissue and the differences in contrast due to clinical imaging parameters and the positioning of the fetal brain,
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056
Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
itisdifficulttoestablishasetofparametersforautomated segmentationoffetalbrainsforallgestationalages.
Fetal MRI information were gotten from clinical MRI of patients with analyzed or associated cases with fetal inconsistencies later indicative ultrasonography. Clinical fetalMRIwasperformedutilizinga1.5-TTwinSpeedSigna framework (GE medical care) what's more, a 8-channel staged cluster cardiovascular loop, without maternal sedation or breath-hold, with the mother in left decubitus position to limit caval pressure. The convention involved various acquisitions in the fetal sagittal, pivotal furthermore, coronal sees utilizing half-Fourier obtaining single-shot quick twist reverberation (SSFSE)magnetic reverberationimagingwithTRdifferingsomewhereinthe rangeof1,000and4,500ms;TEshiftingbetween80 also, 100 ms; variable field of view in light of the maternal and fetalbodysize(somewhereintherangeof24and40cm); variablegridsizesomewhereintherangeof160and512; and cut thickness of 3 or 4mm. Clinical fetal MRI at our foundationincludesSSFSEexamineswithdifferentTRand TEvalueswhichbringaboutvariouspicturecontrasts.For thetestsinthisreviewwejustusesets ofSSFSEexamines withasimilardifference.
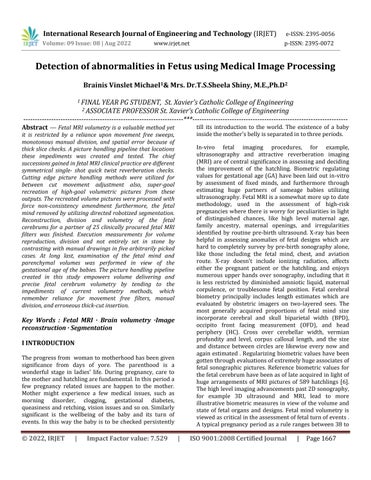
algorithm, morphological filtering, and level set segmentation, and finally brain volume segmentation by adding parenchymal and ventricular volumes processed with morphological filtering (closing operation) and connected components algorithm. The brain volume is segmented with this procedure because in practice the brainvolumeiscomputedasthevolumeenclosedbybrain parenchymaincludingtheventricles.
The reconstructed volumetric fetal MRI images were processed by intensity non-uniformity correction and segmentationalgorithmsdiscussedinthisarticle.Figure3 shows different stages of segmentation to achieve brain volumetry.Thesestagesinvolveintracranialsegmentation, tissue classification using multiple intensity-based thresholding, brain parenchyma segmentation based on the tissue classifications using connected components
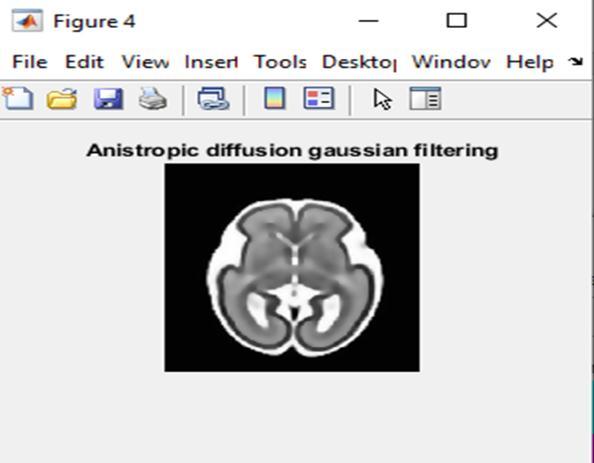
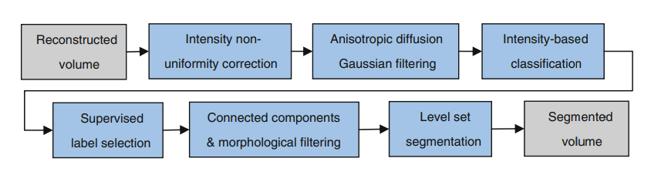
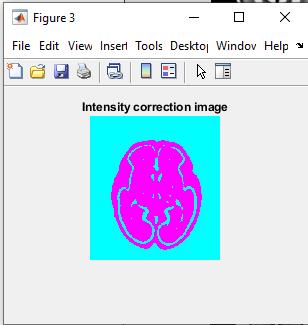
FIG-4 The performance of data enhancement
The catch scope of our cut to-volume enrollment calculation relies upon a few boundaries including the nature of the assessed volumetric picture utilized as enlistment focus, as well as the picture highlights which thus relies upon the GA of the embryo and the picture contrast. Practically speaking we don't anticipate that the calculation should catch and address between cut movement of 8 mm or more. Assuming movement antiques stay in the recreated picture or the force nonconsistencycan'tbereestablished,thedivision.calculation might come up short and volumetry may not be precise. Nonetheless, it is normal that with better and quicker imagingmethodsfetalpicturesofasuperiorqualitycanbe gained which will prompt expansions in the achievement pace of our calculation. At last, the created strategies in this study can be applied to other fetal organs. Here we report a starter reproduction, division, and delivering test fora33.28-weekembryowhichdidn'tmoveatthehourof securing.
Notwithstanding cerebrum and organ volumetry, the picture handling methods created here can be utilized for
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056 Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
the assessment and appraisal of the shape and design of fetal body and organs. The most basic issue for the recreation of the craniofacial structures and other fetal organs is the non-unbending nature of the movement in those areas. Assuming the movement is immaterial or on the other hand in the event that it very well may be assessed precisely, recreation, division, and perception willbedoable.
1. Reddy UM, Filly RA, Copel JA (2008) Prenatal imaging: ultrasonography and magnetic resonance imaging. Obstet Gynecol112(1):145–157
2. Coakley FV, Glenn OA, Qayyum A, Barkovich AJ, Goldstein R, Filly RA (2004) Fetal MRI: a developing techniqueforthedevelopingpatient.AJRAmJRoentgenol 182(1):243–252
3.GuibaudL (2009)Contributionof fetal cerebral MRIfor diagnosisofstructuralanomalies.PrenatDiagn29(4):420–433
4.Garel C(2008)Imagingthefetus:when doesMRIreally help.PediatrRadiol3(38Suppl):S467–S470
5. Garel C (2005) Fetal cerebral biometry: normal parenchymal findings and ventricular size. Eur Radiol 15(4):809–813
6.TileaB,AlbertiC,AdamsbaumC,ArmoogumP,OuryJF, Cabrol D, Sebag G, Kalifa G, Garel C (2009) Cerebral biometry in fetal magnetic resonance imaging: new referencedata.UltrasoundObstetGynecol33(2):173–181
7.ChangCH,YuCH,ChangFM,KoHC,ChenHY(2003)The assessment of normal fetal brain volume by 3-D ultrasound.UltrasoundMedBiol29(9):1267–1272
8. Kazan-Tannus JF, Dialani V, Kataoka ML, Chiang G, Feldman HA, Brown JS, Levine D (2007) MR volumetry of brainandCSFinfetusesreferredforventriculomegaly.AJR AmJRoentgenol189(1):145–151
9. Roberts N, Garden AS, Cruz-Orive LM, Whitehouse GH, Edwards RH (1994) Estimation of fetal volume by magnetic resonance imaging and stereology. Br J Radiol 67(803):1067–1077
10. Baker PN, Johnson IR, Gowland PA, Hykin J, Adams V, MansfieldP, WorthingtonBS(1995)Measurementof fetal liver, brain and placental volumes with echo-planar
magnetic resonance imaging. Br J Obstet Gynaecol 102(1):35–39
11.GongQY,RobertsN,GardenAS,WhitehouseGH(1998) Fetal and fetal brain volume estimation in the third trimester of human pregnancy using gradient echo MR imaging.MagnResonImaging16(3):235–240
12. Schierlitz L, Dumanli H, Robinson JN, Burrows PE, Schreyer AG, Kikinis R, Jolesz FA, Tempany CM (2001) Three-dimensional magnetic resonance imaging of fetal brains.Lancet357:1177–1178
13. Endres LK, Cohen L (2001) Reliability and validity of threedimensional fetal brain volumes. J Ultrasound Med 20:1265–1269
14. Kinoshita Y, Okudera T, Tsuru E, Yokota A (2001) Volumetric analysis of the germinal matrix and lateral ventricles performed using MR images of postmortem fetuses.AJNRAmJNeuroradiol22(2):382–388
15. Roelfsema NM, Hop WC, Boito SM, Wladimiroff JW (2004) Three-dimensional sonographic measurement of normal fetal brain volume during the second half of pregnancy.AmJObstetGynecol190(1):275–280
16.BoitoS,StruijkPC,UrsemNT,FedeleL,WladimiroffJW (2003) Fetal brain/liver volume ratio and umbilical volume flow parameters relative to normal and abnormal human development. Ultrasound Obstet Gynecol 21(3):256–261
17. Gholipour A, Warfield SK (2009) Super-resolution reconstruction of fetal brain MRI. In: Studholme C, RousseauF(eds)MICCAIWorkshoponImageAnalysisfor theDeveloping Brain (IADB’2009).London,UK,pp45–52, 24 Sept 2009 [Online]. Available: http://www.crl.med.harvard.edu/ publications/SR-FetalBrain-MRI-IADB-MICCAI2009.pdf
18. Gholipour A Estroff JA, Warfield SK (2010) Robust superresolution volume reconstruction from slice acquisitions: application to fetal brain MRI. IEEE Trans MedImaging.doi:10.1109/TMI.2010.2051680(inpress)
19. Rousseau F, Glenn OA, Iordanova B, RodriguezCarranza C, Vigneron DB, Barkovich JA, Studholme C (2006) Registration based approach for reconstruction of high-resolutioninuterofetalmrbrainimages.AcadRadiol 13(9):1072–1081
International Research Journal of Engineering and Technology (IRJET) e-ISSN:2395-0056 Volume: 09 Issue: 08 | Aug 2022 www.irjet.net p-ISSN:2395-0072
20. Jiang S, Xue H, Glover A, Rutherford M, Rueckert D, Hajnal J (2007) MRI of moving subjects using multislice snapshot images with volume reconstruction (SVR): applicationtofetal,neonatal,andadultbrainstudies.IEEE TransMedImaging26(7):967–980
21. Prayer D, Brugger PC, Prayer L (2004) Fetal MRI: techniquesandprotocols.PediatrRadiol34:685–693
22. Lee S, Wolberg G, Shin S (1997) Scattered data interpolation with multilevel b-splines. IEEE Trans Vis ComputGraph3(3):228–244
23. Kim K, Habas PA, Rousseau F, Glenn OA, Barkovich AJ, Studholme C (2010) Intersection based motion correction of multislice MRI for 3D in utero fetal brain image formation.IEEETransMedImag29(1):146–158
24.LevineD,BarnesPD,RobertsonRR,WongG,Mehta TS (2003) Fast MR imaging of fetal central nervous system abnormalities.Radiology229:51–61
25. Mangin J (2000) Entropy minimization for automatic correction of intensity nonuniformity. In: Proceedings of the of the IEEE workshop on mathematical methods in biomedicalimageanalysis.p162