NEWS: Pharmacies will Close without further Reform Page 5
MEDICINES: Medicine Shortages hit new High Page 6
REPORT: Campaign for Restoration of Pharmacy Fees Page 10
CPD: Pharmacy Robotics Page 37
FEATURE: Migraine, Diet and Sugar Page 42
AWARDS: Irish Pharmacy Awards Red Carpet Page 52
TEAM TRAINING: Vitamin D Page 61
Page 4: Enhancing scope of pharmacy practice being considered by Department of Health
Page 6: 60% of Ireland’s population impacted by medicine shortages, report shows
Page 7: New President and Vice-President for Pharmaceutical Society
Page 9: United Drug partners with Locus Robotics
Page 10: Pharmacy campaigns to have fees restored
Page 17: Back2School essentials for the pharmacy team
Page 44: New screening initiative for diabetes
Page 50: New patient and carer led alliance
PUBLISHER:
IPN Communications Ireland Ltd.
Clifton House, Fitzwilliam Street Lower, Dublin 2 00353 (01) 6690562
MANAGING DIRECTOR
Natalie Maginnis n-maginnis@btconnect.com
EDITOR
Kelly Jo Eastwood: 00353 (87)737 6308 kelly-jo@ipn.ie
ADVERTISING EXECUTIVE Amy Evans: amy@ipn.ie
EDITORIAL/ EVENTS & MARKETING EXECUTIVE
Aoife Hunter: aoife@ipn.ie
CONTRIBUTORS
Ruth Morrow
Joyce Clegg
Dr Kate Gajewska
Allison Dunne
Steven Graham
Dr Edward O’Sullivan
Helen Forristal
Dr Kevin McCarroll
DESIGN DIRECTOR
Ian Stoddart Design
Irish Pharmacy News is circulated to all independent, multiple Pharmacists and academics in Ireland. All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd. has taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
Foreword
As Irish Pharmacy News was going to press, it was revealed that the Minister for Health, Stephen Donnelly, has instructed his officials to meet with the IPU and a meeting was held with representatives of the Department of Health at the end of last month. Following this meeting the IPU’s Pharmacy Contractors Committee met this morning and agreed to enter a process of engagement with the Department of Health.
The IPU has stated that, “The talks are without preconditions on either party, but we are satisfied that we have now entered a process of engagement with the Department of Health with another scheduled meeting already arranged for the end of July.
“This is the most significant development on pay and service talks with the Department in many years and it follows the sustained campaigning by you, our members, in addition to many years of consistent advocacy by IPU staff and the IPU Committees.
“However, we still have a lot of work to do, and the campaign is far from over. There is no commitment that any pay restoration will be forthcoming, so we need you to continue to work with us on our ongoing campaign. This is merely a first step in what may turn out to be a long process, but I assure you our core demand remains the same; a restoration of our dispensing fee to ¤6.50 linked to public sector pay.”
We will bring you more on this news in the August issue.
Medicine shortages continues to hit the headlines and our report on page 6 shows that 60% of Ireland’s population has been impacted by medicine shortages in the last year, with almost half of the population deeply concerned by the deteriorating situation.
In other news, on page 8 of this issue we detail findings from the Pharmaceutical Society of Ireland’s recently published Annual Report. “Given the challenges within healthcare and for pharmacy, the increase in the number of pharmacists is to be welcomed, with a return to pre-pandemic levels of registration activity noticeable for the PSI during 2022,” reflects Registrar and Chief Officer Joanne Kissane.
Our Back to School special focus section discusses some of the most important categories for pharmacies over the summer months, from mental health to sports injuries and diabetes in the classroom to vaccinations.
I hope you enjoy the issue.
Minister considering Expanding Scope of Pharmacy
A number of proposals and ways to potentially enhance the scope of practice of community pharmacists in the short, medium and longer term are currently being considered within the Department of Health, Irish Pharmacy News has learned.
Minister for Health Stephen Donnelly made the comments during a recent Dáil Éireann Debate when he was asked by Deputy Pádraig O’Sullivan if he has plans to expand the scope of practice for pharmacists.
Replying, the Minister stated that, “A proposal for the implementation of a Minor Ailment Scheme will see a scheme put in place where eligible patients will attend their local community pharmacist for assessment and treatment for a number of identified ailments, rather than first initially having to attend their GP to obtain a prescription to access over-thecounter medicines currently on the
PCRS reimbursement list. The HSE have established a Minor Ailments Working Group to consider what is required from a clinical and operational perspective including the development of appropriate protocols. The range of conditions to be included in such a scheme is being finalised.
“The free contraception scheme for women was launched in September 2022, and is currently open to women aged 17-26 who are ordinarily resident in Ireland. Work has commenced on evolving options for an enhanced role for pharmacists in the scheme, with considerations
encompassing issues such as legal basis, training administrative and governance matters.
“Realisation of this ambition will not be without challenges, and paramount to this will be the availability of the appropriate workforce to deliver on the services envisaged. The Emerging Risks to Pharmacy Workforce project, a multi-annual project commenced by the Pharmaceutical Society of Ireland to assess emerging risks to the continued availability of a professional pharmacy workforce within community and hospital pharmacy in Ireland will be relevant.”
Our people - including you | Diversity & Inclusion at PHX Ireland
PHX Ireland recently introduced the ourpeople strategy which forms the basis for Diversity & Inclusion, Charity Partnerships, Health & Wellbeing and Engagement & Feedback across the business. One of the key strengths of each of the ourpeople pillars is the use of champions through the PHX Ireland business units of United Drug, LloydsPharmacy Ireland and TCP Homecare.
In conjunction with PRIDE month, PHX Ireland launched the “ourpeople - including you” initiative which introduced the D&I
Champion, Ray Lynch. Ray has worked for United Drug for several years and is keen to champion the diversity and inclusion already
Campaign in Pharmacy
The Irish Heart Foundation has launched a new campaign asking adults, particularly those aged over-50, to have their blood pressure checked with their local pharmacy or GP.
The charity’s ‘Before Damage is Done’ campaign aims to drive awareness of the link between high blood pressure and heart disease and stroke.
The ‘silent killer’ affects two out of three over-50s – but because it is symptomless, half don’t know they have it.
Previous research shows Ireland has one of the lowest rates of awareness, treatment and control of high blood pressure among 12 high-income countries.
Dr Angie Brown, Consultant Cardiologist and Medical Director with the Irish Heart Foundation, said thousands of people unwittingly go about their daily lives with high blood pressure.
“The only way of finding out is to get it checked with your GP or local pharmacy as you will, most likely, have no symptoms,” she said.
present in the business while encouraging others to learn and celebrate alongside the LGBTQIA+ community.
Throughout the month, the Pride flag has been flown throughout the business, both physically and digitally and prominently displayed at the front of the Magna Park building. Pride support was extended through the hosting of webinars on inclusivity in the workplace and how to be more LGBTQ+ aware in both personal and professional lives. Colleagues were provided with an insight into being their authentic selves during a masterclass delivered by Nigel Owens.
PHX Ireland Group Limited, is Ireland’s leading fully integrated healthcare provider. PHX Ireland Group Limited comprises United Drug, Ireland’s leading pharmaceutical distributor; LloydsPharmacy Ireland, a major community pharmacy chain; and TCP Homecare, innovators in clinical home nursing services and direct to patient delivery solutions. In Ireland, PHX Ireland employs over 1,800 people, operate 5 distribution centres and 85 Pharmacies.
“It is one of the most important risk factors for heart disease and stroke but there are many factors that affect your risk.”
The Irish Heart Foundation’s Mobile Health Unit offers free checks through its heart health checks in communities across Ireland.
Orlaith Gavan, Medical Director, Pfizer Healthcare Ireland, said:
“The Irish Heart Foundation’s ‘Before Damage is Done’ campaign is a really important reminder for people to have their blood pressure checked.
“We are really pleased to support the Irish Heart Foundation’s Mobile Health Unit as it embarks upon its continuous journey across Ireland. With around 10,000 checks undertaken every year, thousands of people in every county have benefitted from the services of the Mobile Health Unit since its launch in 2016.
“Many people may be unaware of their risk factors for cardiovascular disease and we would therefore encourage people to avail of this free and efficient service.”
Pharmaceutical Ecosystem in Europe
Minister for Health Stephen Donnelly recently represented Ireland at a meeting of EU Health Ministers in Luxembourg. This formal meeting of the Employment, Social Policy, Health and Consumer Affairs (EPSCO) Council is held under the Swedish Presidency of the Council of the European Union (January to June 2023). Ministers exchanged views on strengthening the pharmaceutical ecosystem in support of competitiveness and equitable access to medicines.
Minister Donnelly said, “Patients and health systems in the EU need access to new, innovative treatments, as well as older, off-patent products, generics, and biosimilars. We must design a sustainable system that facilitates access throughout the EU, taking into account Member States’ varying market size and ability to pay.”
Minister Donnelly continued, “Ireland supports the use of targeted incentives which play an important role in a needs-driven pharmaceutical approach model. Such incentives must address unmet need, including in relation to AMR. The implications of any incentive on health systems must be carefully assessed, and the effectiveness of any medicine evaluated by comparative trials.
“Ensuring predictability and consistency for innovators and generic manufacturers is fundamental to their continued operation, and the EU system must strive to provide this.
“We need to support the competitiveness of the EU pharma ecosystem, while achieving and maintaining the critical balance between access and innovation.”
Ministers also adopted a Council Recommendation on stepping up EU actions to combat antimicrobial resistance (AMR) in a One Health approach, and agreed a general approach to the Regulation on fees and charges payable to the European Medicines Agency (EMA). They took note of progress reports on the Regulation on a European Health Data Space and the Regulation on the standards of quality and safety for substances of human origin intended for human application.
Pharmacies will Close without Reform
Irish pharmacies are being left in a perilous position due to soaring costs and a 15-year government imposed pay freeze. This was a central finding of a new economic analysis of Ireland’s pharmacy sector conducted by Fitzgerald Power on behalf of the Irish Pharmacy Union (IPU). The IPU has warned that significant reforms are now urgently needed in how the state pays pharmacies for work they provide to the health service.
According to the Review of the Community Pharmacy Sector in Ireland 2023, there are currently 1,910 pharmacies in Ireland. The sector directly employs 14,325 people, but this analysis reveals that trading conditions have become increasingly difficult. The most significant challenges facing pharmacies are reduced community drug scheme revenues and increased costs.
Key findings of the report include:
• Community drugs scheme revenues account for 57% of the turnover for the average pharmacy. This rises to 62% for independent pharmacies.
• However, over the past 15 years core income from community drug schemes decreased by 29%.
• In the same period, the costs associated with dispensing medicines on behalf of the state has increased 23%.
• More than 10% of pharmacies are now loss making which is more heavily concentrated in rural areas.
There are concerns that the impact of lost revenues will become more apparent in the coming months. These losses had been partly offset by COVID-19 vaccinations, which generated nearly ¤26m for the sector in revenue in 2022. However, with demand levels for this service dropping the pressures continue to mount for pharmacists.
At the start of the last decade, wages made up 14% of turnover. However, increased staff costs saw that share of turnover rise to 24% by the end of 2022. Hourly pay rates for pharmacists and technicians have increased by 20% and 14% respectively over the last five years. This means that the cost of dispensing each medicine on behalf of the state has increased by 23% since the 2009 pharmacy pay freeze was imposed.
Fitzgerald Power’s analysis concludes that if personnel costs increase as expected in the coming years, “a large number of pharmacies would go out of business under the current fee structure.”
Commenting on the findings, IPU interim Secretary General Derek Reilly said, “These figures lay
bare that closures of pharmacies, particularly in rural areas, is likely. We have been warned of this for several years and it is now an economic inevitability unless there is meaningful action from government to support the sector.
“Pharmacies are first and foremost healthcare centres that provide vital services to communities nationwide. This includes a wide range of services provided on behalf of the national health service, which are delivered well and make a difference to people’s lives. Pharmacies receive a payment for these services, but it is quite clear that these payments are no longer adequate.
“The Irish Pharmacy Union is now calling for the introduction of a new ¤6.50 flat rate dispensing fee. That would safeguard the future viability of pharmacies. It would allow pharmacy owners to continue to meet increasing wage demands while also investing in expanding services. Alternatively, failure to support the sector will have dire and potentially irreversible consequences.”
Turn to page 10 for further details.
Boots Ireland Raise over ¤125,000
The team at Boots Ireland were celebrating recently, showcasing their pride of Boots pharmacy team members across the country who fundraised, organised raffles, bake sales, quizzes and sold daffodil pins to support this year’s Daffodil Day!
Said the pharmacy group, “Through the generosity of our customers, patients, and team members we ended March with over ¤127,000 fundraised during the month in support of the Irish Cancer Society Night Nursing Service.”
Medicine Shortages Index hits Record High
60% of Ireland’s population has been impacted by medicine shortages in the last year, with almost half of the country’s population deeply concerned by the deteriorating situation, new research has found.
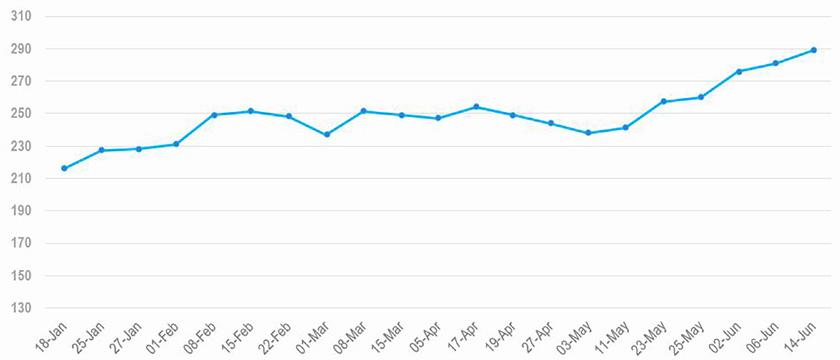
It comes as the number of medicines out-of-stock in Ireland has reached a new record high of 289 as the scale of the shortages of vital medicines continues to worsen for Irish patients.
The latest Medicines Shortages Index shows that in the past four weeks alone, the number of medicines unavailable across the State jumped by almost 50, the largest single monthly increase recorded. Medicine shortages have increased by 50% in just six months and 65% in 12 months.
Among the medicines out-of-stock include low dose packs of Aspirin 75mg, which is dispensed around 4 million times per year in Ireland.
Others out of stock include medicines to treat blood pressure, high cholesterol, common antibiotics, medicines for depression, anxiety and insomnia together with a number of eye drops and topical creams.
Separately, a survey of 1,200 people on their experiences of
Out
of Stock Medicines
Sandra Gannon, CEO, Azure Pharmaceuticals
medicine shortages, conducted by Amárach Research and commissioned by Azure Pharmaceuticals, reveals for the first time the impact medicine shortages are having on the public.
It found that three out of five patients have experienced medicine shortages, with over half being told on more than one occasion by a pharmacist in the last 12 months that the medicine they were seeking was not in stock.
56% of Irish adults said they were aware of the medicine shortages crisis that Ireland has faced over the past year, with 48% of the population reporting a high level of concern about the scarcity of various medicines.
Out of the patients who encountered medicine supply issues at a pharmacy, 44% had difficulties obtaining prescription medicine, 24% faced issues with over-the-counter (OTC) medicine, and 31% encountered shortages for both types of medications.
The cohort most worried by the lack of availability of medicines are females in the age category of 35-44, according to the research findings.
The severity of the medicine shortages crisis and impact on people, pharmacists and doctors should serve as a wake-up call for policymakers involved in the healthcare system, said Sandra Gannon, CEO of Azure Pharmaceuticals,
“These findings, coupled with a new record high in the number of shortages, reflects the worsening nature of this issue since it first emerged at the start of 2020.
Commenting on the survey’s findings, Ms Gannon said, “The high percentage of individuals reporting difficulties in obtaining both prescription and over-thecounter medicines is deeply troubling. It underscores the reach of this issue across communities as many of the medicines out-ofstock are commonly used.
“Almost half of the population is concerned about the deteriorating state of the availability of medicines. This level of concern reflects the tangible impact on individuals’ access to necessary medications and their overall well-being.”
On the policy response, Ms Gannon said, “It appears we are yet to truly understand the nature of this problem and thus are failing to grip it. Diminishing margins for generic medicines, our over reliance on single-sourced medicines, combined with other countries paying higher prices, makes us particularly vulnerable. The medicines market has changed and delays in adapting to this reality are impacting every touchpoint of the health system – patients, pharmacists, doctors and hospitals,”.
She pointed to policy measures taken by several other European nations to address the ongoing medicine shortages crisis across the continent, including improved data reporting, encouraging the entry of new suppliers, price increases and de-risking dependency on particular markets.
¤1.6m funding to University College Cork
University College Cork (UCC) and the Cerebral Palsy Foundation have announced the creation of a new Chair in Early Brain Injury and Cerebral Palsy.
The new ‘Cerebral Palsy Foundation Chair’ is made possible thanks to generous support of ¤1.6 million from the Cerebral Palsy Foundation, a global not-for-profit organisation committed to creating positive change for those with Cerebral Palsy and related disabilities.
“The Cerebral Palsy Foundation looks forward to working with UCC and is so thankful for the funding it has received from donors to drive forward the CP Programme of Excellence in Ireland. We are excited that UCC will lead research and clinical care to change the trajectories of lives of infants with early brain injury and CP,” said Rachel Byrne, Executive Director of the Cerebral Palsy Foundation.
“I would like to sincerely thank the Cerebral Palsy Foundation for this very generous funding. We are committed to working in partnership with the Foundation to make a real difference for people with Cerebral Palsy. Early detection is critical for early intervention and this support will allow INFANT to fast track the translation of research and innovation in early brain injury and Cerebral Palsy to clinical care,” said INFANT and UCC Futures Children Director, Professor Geraldine Boylan.
“This generous support will enable us to build on and translate two decades of interdisciplinary research within our INFANT research Centre with a focus on Cerebral Palsy. This exciting development will undoubtedly enhance the very important areas of prevention, early detection and management of Cerebral Palsy. Philanthropy such as this can ensure that our research can be translated into real-world change, improving maternal and child health,” added Professor Helen Whelton, Head of College of Medicine and Health.
Visual Health Tool
The Minister for Health has launched an innovative new online visual health data monitoring tool, created to provide an overview of the performance and health outcomes of the health service.
Operated by the Department of Health in partnership with the Health Service Executive (HSE), the Prototype Visualisation Platform for the Health System Performance Assessment (HSPA) Framework will help policymakers, healthcare providers, researchers and patients to better assess and improve system accountability, fairness, and efficiency as we progress towards universal healthcare for all.
The new HSPA website has been populated with health data in the areas of life expectancy, disease outcomes, health risk factors such as; smoking and obesity.
The HSPA will enable the public to become better informed about the nation’s health as well as important issues that are central to the provision of health services in Ireland, giving them a clearer picture of how the health service is performing and a better understanding of the impact of health policies on people’s lives.
HSPA data indicates that life expectancy at birth in Ireland is consistently above the EU average, at 84.3 years for women and 80.5 years for men in 2021, with increases of 1.2 years and 1.8 years respectively in the last decade, compared with a decrease of 0.2 years and an increase of 0.1 years respectively for EU-27 member countries in the same period.
Figures for 2022 show the leading causes of death in Ireland include respiratory diseases, circulatory diseases (like stroke and heart attack) and cancer, with overall mortality rates continuing to decline steadily. Ongoing investment, through the National Cancer Strategy, Sharing the Vision, Healthy Ireland initiatives and wider health service reforms and improvements, is intended to support increases in life expectancy, and to reduce mortality rates from chronic disease.
Capacity to increase Pharmacy Places
The Irish Pharmacy Union (IPU) has welcomed the Higher Education Authorities (HEA) findings that there is capacity to increase the number of educational places for pharmacists in Ireland. The IPU has been campaigning for increased educational capacity for several years to address the growing shortage of community pharmacists.
A report from the HEA at the end of last month found that there is potential capacity for almost 200 new pharmacy undergraduate education places in Ireland. This would include the expansion of existing programmes as well as the establishment of new education courses in the Atlantic Technical University and the South-East Technical University.
Tom Murray IPU Honorary Treasurer said, “Ireland has traditionally relied on other countries, primarily Britain, to educate our pharmacists. Last year saw just 155 new pharmacy graduates from Ireland enter
the register less than half of the total new entrants to the professional register. The potential to significantly increase the education of pharmacists in this country would be hugely welcome and provide a much more solid foundation to the community pharmacy sector.”
“Community pharmacy is a vital profession that this is a centre of community-based healthcare. As Ireland’s demographics change and as our model of healthcare evolves pharmacy will play an increasingly important role. We must ensure that we are securing this with greater levels of
education as has been recognised by the HEA.”
“While there is now an action plan to train more pharmacists, this will take time. There is a pressing need to deal with the shortages within the profession today. Many pharmacist vacancies are going unfilled, and this can only have a negative impact on patient experience. With a growing and ageing population, we estimate there is a significant shortfall of pharmacists working in the sector. One short term action we would like is to make it as easy as possible for pharmacists from nonEU countries to relocate and work in Ireland,” concluded Mr Murray.
New Appointments to Pharmacy Council
The Minister for Health, Stephen Donnelly T.D., has appointed nine members to the Council of the Pharmaceutical Society of Ireland (PSI) with seven new appointments and two reappointments.
The new appointees are Joan Peppard, Emily Kelly, Dr Denis O’Driscoll, Dr Laura Jane Sahm, Dr Cyril Sullivan, Martin Higgins, and Martin Sisk, while Geraldine Crowley and Mark Jordan have both been reappointed.
The appointments take effect from June 18th, 2023 for four years. All members of Council are appointed by the Minister to act in the public interest in carrying out the regulatory responsibilities of the PSI.
The PSI Council has also elected Katherine Morrow as PSI President (chair) and Joan Peppard as Vice-President. The President and Vice-President are elected from amongst the Council for a oneyear term and may hold office for up to two years.
Appointed to the Council in 2021, Katherine is Director and National Coordinator of APPEL (Affiliation of Pharmacy Practice Experiential Learning) with responsibility for the experiential learning placements of the integrated pharmacy programmes of the three Schools of Pharmacy in Ireland. A graduate of the School of Pharmacy, Nottingham University, Katherine has over 25 years’ experience, acquired from working across a breadth of sectors including primary care, secondary care, regulation and academia.
She holds an Advanced Diploma in Leadership, Personal and Executive Coaching and has previously qualified as a Supplementary Prescriber in the UK. She has extensive experience in education/CPD, accreditation and competency assurance from previous roles as Operations Director of the Irish Institute of Pharmacy (IIOP) and Head of Education & Professional Competence with the Irish College of General Practitioners (ICGP).
Joan Peppard is the new VicePresident of the PSI. A pharmacist with forty-years’ experience in hospital pharmacy, Joan also holds a degree in Public Management from the Institute of Public Administration (2000) and a Masters in Ethics from Dublin City University (2012). Joan was Chief Pharmacist at the Midlands Regional Hospital from 2006 until 2023. She also held the role of pharmacy lead for the Dublin Midlands Hospital Group (DMHG) in the national COVID-19 vaccination centres. Joan has held the roles of President of the Hospital Pharmacists Association of Ireland and President of the European Association of Hospital Pharmacists.
The PSI – the Pharmacy Regulator is governed by a 21-member Council, with a non-pharmacist majority. Council members are appointed by the Minister for Health in accordance with the
Joan Peppard
Pharmacy Act 2007. The Council meets at least six times each year and is responsible for setting the strategy for the PSI, and overseeing the functions of the PSI, in the public interest.
Katherine Morrow
Pharmacy Regulator publishes Annual Report
The Pharmaceutical Society of Ireland (PSI) - The Pharmacy Regulator has published its annual report for 2022, outlining the significant work undertaken by the regulatory authority to protect the health, safety and wellbeing of patients and the public by regulating pharmacists and pharmacies in Ireland.
The report provides an overview of the work carried out in line with the regulator’s remit and current corporate strategy to ensure pharmacy care and services are regulated to a high standard in Ireland.
Key activities for PSI during 2022 included:
• Continued engagement with the Department of Health on proposals to advance reform of the Pharmacy Act 2007
• 7,067 pharmacists were registered to practise by year end – highest ever number on the Register of Pharmacists
• An 83% increase (compared to 2021) in pharmacists registering from EU (European Union), UK and other non-EU routes
• The launch of the first ever pharmacy workforce survey as part of a multi- stakeholder project to assess the emerging risks to continued availability of pharmacists in Ireland
• Approval of a new Core Competency Framework for pharmacists
• PSI’s ongoing collaboration with Department of Health and others to evolve the legislative framework, and ensure the availability of accredited training for pharmacists, to facilitate the continued, significant involvement of pharmacists in the administration of 635,475 Covid-19 vaccines in 2022
Commenting on the publication of the annual report, PSI Registrar
and Chief Officer Joanne Kissane said, “The report reflects on the current operating environment for pharmacists and pharmacies and the regulatory work undertaken to ensure that the highest standard of care remains at the centre of pharmacy healthcare delivery. It also highlights the range of strategic activities we are seeking to progress to ensure our regulatory framework remains both robust and responsive to meet current and future regulatory and healthcare needs.”
There were 7,067 pharmacists registered with the pharmacy regulator at the end of last year, continuing the year-onyear increase to the Register of Pharmacists in Ireland (with 7,180 pharmacists registered at the end of May 2023). Of the volume of pharmacists registered, there was an 83% increase, in comparison to 2021, with pharmacists registering from the EU (European Union), UK and other non-EU routes. At 1,981, the number of pharmacies in the state remained stable on the previous year.
“Given the challenges within healthcare and for pharmacy, the increase in the number of pharmacists is to be welcomed, with a return to pre-pandemic levels of registration activity noticeable for the PSI during 2022.
“The increase in the number of registered pharmacists corresponds with an increase in queries and applications about registering to work as a pharmacist in Ireland, and our ongoing work to process these requests and to continue to streamline processes,
PSI Registrar and Chief Officer
Joanne Kissane
such as the route to registration for non-EU/EEA pharmacists.
“Overall, the PSI’s focus remains on ensuring that pharmacists available to practice in Ireland can provide quality, safe healthcare and that the profession maintains these high standards.”
During 2022, 53 complaints about pharmacists or pharmacies were received, representing a 33% reduction in formal complaints received from the public, in comparison to the previous year. Of the complaints reviewed last year by the regulator’s Preliminary Proceedings Committee (PPC), the complaint screening committee, 13 were referred for further action, which can include referral to an inquiry or for mediation.
Ensuring a robust, transparent, and streamlined process to facilitate the public and pharmacy profession to raise concerns and bring forward complaints is a critical function of the regulator’s work.
“It is critical that as a regulatory authority we strive to attain and maintain the highest standards possible in all aspects of our work, and particularly regarding responding to issues of concerns, queries and complaints raised by members of the public and pharmacy profession.”
The report also highlights the developments in relation to the reform of the Pharmacy Act 2007 and engagement with Department of Health on this issue. Commenting on the position paper submitted to the Department of Health during 2022, Joanne Kissane said,
“As the regulatory body for pharmacy, we are extremely conscious of the need to reform elements of the Pharmacy Act which has played a critical role in creating an assurance framework for patients and the public to access safe, quality, pharmacy services.
“Our approach centres on ensuring legislation is fit to support effective regulation into the future, and for the overall benefit of patients and the public. To that end, we were pleased to submit a position paper to the Department of Health in
2022, highlighting the need for reform, articulating the challenges in the current legislative framework and the opportunities presented through reform. We look forward to continued engagement with the Department of Health on this matter.”
The report reflects the significance of the regulator’s role in setting and assuring standards for pharmacy education in Ireland and the importance the regulator places upon continuing professional development (CPD) throughout a pharmacist’s career. A specific area of focus in 2022 was the completion of a review in relation to the Core Competency Framework, which underpins the pharmacy curriculum delivered by the Schools of Pharmacy in Ireland and provides structure and guidance for pharmacists’ CPD. There were also advances in relation to the multi-stakeholder project to assess the risks to the future pharmacy workforce, which is taking a medium to long-term view of the factors influencing future workforce availability, the output of which will be a workforce intelligence report.
This project commenced in 2022, with the establishment of a multistakeholder working group and the first ever workforce survey. This survey will be administered annually by the PSI. It will provide an important baseline picture of the current pharmacy workforce and inform future discussions and planning. Participation in the project’s working group is drawn from organisations across the health and the pharmacy sector who, importantly, will be key to ensuring the implementation of the recommendations contained in this project’s concluding report.
Reflecting on the regulator’s ongoing work, Joanne said, “The pharmacy profession and operating environment is continuously evolving, and it is important that all changes are underpinned by a robust regulatory framework, to ensure public and patient trust in pharmacy healthcare and to also ensure pharmacy is part of a fully integrated healthcare system.
“As always, we will continue to work collaboratively and engage positively and constructively with all health stakeholders as part of the broader healthcare system.”
United Drug Partners with Locus Robotics
Ireland’s largest pharmaceutical distribution company has partnered with Locus Robotics, the industry leader in autonomous mobile robots (AMR) for warehouse fulfilment, to deploy 21 LocusBots at their Baldonnel Dublin distribution centre to improve customer order fulfilment productivity. The innovative, robotdriven warehouse automation system will also ensure order pick accuracy and improve workplace quality, ergonomics, and safety. The Dublin site deployment is the first of its kind in Ireland.
With the rapid increases in online volume health care distributors have been challenged to rapidly scale to meet growing wholesale and consumer demand for quick, accurate, and cost-effective order fulfilment. Deploying Locus AMRs within United Drug’s Baldonnel warehouse will proactively position them to meet these demands with a scalable, proven, and costeffective solution.
“This partnership reflects our ongoing commitment to deploy innovative logistics solutions that use advanced technology to address increasingly complex
fulfilment challenges,” says Paul Malone, Head of Operations for UDD & UDC at United Drug Ireland.
“The Locus solution helps us to efficiently optimise productivity across our existing labour force so that we can enhance our customer service levels.”
“We are proud to partner with United Drug to deploy our powerful and efficient multi-bot solution to support their warehouse operations in Baldonnel, Dublin,” said Rick Faulk, CEO of Locus Robotics.
“Our purpose-built robotics solution seamlessly addresses the needs of United Drug’s distribution
Paul Malone, Head of Operations for UDD & UDC at United Drug; Paul Reilly, Managing Director at United Drug, Christy Canavan, Consumer Director at United Drug.
warehouses by eliminating unproductive worker walking time to dramatically improve picking volumes and shorten order cycle times. In addition, Locus helps to ensure key worker health, ergonomic, and safety.”
Powered by LocusOne, the industry’s smartest, fully integrated warehouse orchestration and execution platform, LocusBots are engineered for maximum
warehouse efficiency, delivering optimal productivity utilising the latest navigation and vision system technologies. LocusBots navigate autonomously through the warehouse working closely and safely with associates to improve order picking productivity and throughput efficiency. They can be flexibly and seamlessly deployed as demand changes, supporting a diverse range of picking strategies and workflows.
Disruption to Cancer Diagnoses
The National Cancer Registry Ireland (NCRI) has published a report entitled: COVID-19 impact on cancer incidence in Ireland in 2021: a preliminary analysis. These findings are based on registered and projected cancer cases in 2021, using data available in March 2023. NCRI expects to publish a more definitive update on 2021 case numbers later this year.
Key findings:
• Preliminary data on the impact of the COVID-19 pandemic indicates that the number of cancer cases diagnosed in 2021 was down 1,665 cases or 6% lower than projected.
• This is a smaller shortfall in diagnosis than the 10% observed in 2020.
• Colorectal, female breast, and cervical cancer case numbers, which were notably impacted by the COVID-19 pandemic in 2020, returned to expected case numbers in 2021.
• Liver, pancreatic and kidney cancers appear to have been most significantly impacted by the disruptions that occurred due to COVID-19.
• The combined number of diagnosed cancers during 2020 and 2021 was down 4,320 cases or 8% lower than projected.
Further collaborative work is ongoing to assess the impacts of COVID-19 related disruption on cancer services and outcomes in Ireland.
Professor Deirdre Murray, Director of the National Cancer
Registry said, “The impact of COVID-19 on the health of the Irish population is anticipated to have a long tail as its effects on the diagnosis and management of non-communicable diseases become apparent. While cancer survival rates continue to improve, the incidence of most cancers increases with age. People aged 65 years and older formed the largest cohort of COVID-19 deaths in Ireland, so it is possible that some may have died before being diagnosed and treated for cancer.”
“Cancer never went away during the pandemic but remained
undetected due to a range of reasons including putting off seeking medical advice, disruption to health services and possibly death from Covid. Until we see data that shows the number of cancers diagnosed have returned to expected levels, the Irish Cancer Society will continue to call for urgent and accelerated measures from Government that get people diagnosed in the first instance and secondly, that ensure swift access to cancer treatment,” added Rachel Morrogh, Director of Advocacy & External Affairs at the Irish Cancer Society.
21 LocusBots have been brought to United Drug’s Baldonnel Dublin distribution centre.
Image: Tony Maxwell
Campaign for Restoration of Pharmacy Fees
(This article was first published in the June 2023 issue of IPU Review)
The Minister for Health is obliged under legislation to review services and rates payable to community pharmacists by the end of June. In this article, IPU Acting Secretary General Derek Reilly says enough is enough: pharmacists have endured cuts and increased costs, and despite providing exemplary service to the Irish public, community pharmacy is the only sector that has received no recalibration and restoration of fees since the financial crisis. This needs to change, and the IPU is this month starting a concerted campaign to restore pharmacy fees.
Under the terms of the Public Service Pay and Pensions Act, 2017 the Minister for Health is obliged, before the end of June this year, to review the nature of services provided by community pharmacist contractors and review the operation, effectiveness and impact of the amounts and rates payable to them.
As part of this review the Minister must consider:
• Terms of existing contractual arrangements;
• The terms of any circulars/ documents or understandings with the contractor; and
• The nature of services provided and commitments.
The Minister also has an obligation to have a ‘prudent fiscal policy’ and consider any views expressed or submissions made during the consultation process. The Act requires consultation over a 30-day period but gives no guidance or instruction as to how this ‘consultation’ should take place. In the past we have simply been asked to make a submission without any substantive talks taking place.
In November 2019, after threatening to cut our fees, we had a strong grassroot campaign by IPU members, which succeeded in stopping the proposed cuts with the status quo on fees remaining. The status quo will not do this time, especially as the then Minister for Health, Simon Harris, TD, committed to broader engagement and to adopt a similar approach as was taken with the GP discussions i.e., look at the contract review through a multi-annual lens. This time we will be demanding substantive talks with Department of Health Officials to address the future viability of the community pharmacy network, focusing on the challenges we face to ensure the delivery of a sustainable pharmacy service for the benefit of the citizens of Ireland.
The Pharmacy Contractors Committee and Executive Committee have been working over the course of their current term to position the IPU correctly to ensure successful negotiations.
It should be noted that while the Minister is obliged to ‘consult’ over the month of June, a decision in relation to our fees may not be enacted through legislation until the start of 2024.
Ongoing Engagement
The Department of Health is currently constructively engaging with the IPU on several fronts including talks on enhanced service provision e.g., increasing accessibility of contraception through community pharmacy following a structured consultation with a pharmacist, a medicines shortage protocol, the development of a Minor Ailment Scheme and various aspects of eHealth. We have never been better positioned to engage with the Department than we are now. As June approaches we still have no firm commitment from the Minister for Health to engage with the IPU on substantive talks relating to our core professional dispensing fee. This is in stark contrast to our GP colleagues, who
Derek Reilly, IPU
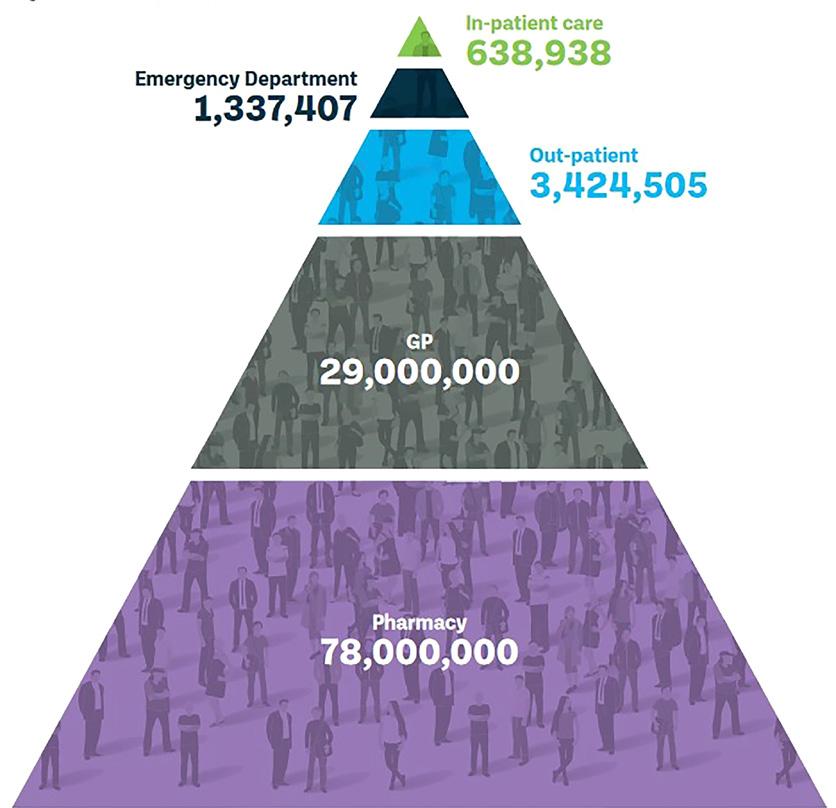
received significant reinvestment in their service provision as a result of the 2019 Agreement, and most notably, the Department have recently announced a strategic review of General Practice. As outlined in the review documents the intention is for “The Department of Health, with the support of the HSE, will undertake this review and will engage with key stakeholders to identify the challenges facing general practice in ensuring the delivery of a sustainable general practice service within the community and to identify the measures necessary to address those challenges in the context of delivering on the principles of Sláintecare”. Given our commitment to community care and prior promises made by Ministers, we expect and demand equity of treatment with other healthcare professionals — after all we are the most accessible healthcare professional, with over 70 million patient care interactions per annum.
Over the last 15 years:
• Revenue reduced: The revenue generated by each pharmacy under the community drug schemes has reduced by 29%;
• Higher costs: The cost of providing a high-quality service, have never been higher with a 29% increase in expenditure on wages. This is on top of significant hikes in energy, utilities, rents and insurance and administration costs;
• Reduced dispensing fee: The rate paid to dispense a medicine under the community drug schemes has reduced by 24% from ¤6.00 to ¤4.58;
• Increased labour costs: The labour costs of dispensing a medicine have increased from ¤3.73 to ¤4.58. This is an increase of 23%, due to higher wage costs and as more resources are required due to the increased administrative burden of the community drug schemes. The average state fee now only covers the cost of dispensing a medicine (¤4.58), merely covering labour costs without contributing to other overheads;
• Price compression: The Consumer Price Index (CPI) has increased by 16%, whereas the CPI for prescribed medicines has declined by 25.5% — we are now experiencing significant price compression;
• No say in reimbursement price: The reimbursement price of medicines is negotiated by the State with drug manufacturers, and as such a pharmacist has not ability to increase or pass any rising business costs on to a patient under the community drug schemes — we are now at an inflection point;
• Pharmacists not being treated on a par with other healthcare workers: The average hourly earnings for healthcare workers have increased by 14%. This includes increases for dentists, nurses, consultants, hospital pharmacists and medical officers in addition to catering staff and hospital porters; and
• Significant engagement with GPs: Since the 2019 GP agreement, the additional annual expenditure provided to GPs has increased by ¤211 million. GP capitation fees have increased by 48.5% (except for
under 6s) since this agreement, recognising their important role in the provision of primary care, however, we have had no such recognition. In fact, the Department has recently agreed a strategic review of general practice to identify the challenges facing general practice in ensuring the delivery of a sustainable service, we are seeking equitable treatment and immediate engagement with pharmacists.
Community Pharmacy is the only sector that has received no recalibration and restoration of our fees since the financial crisis. This needs to change.
What we are seeking on behalf of IPU members is a flat fee of ¤6.50 per medicine dispensed under the community drug schemes, and a very modest increase of 8% on the ¤6.00 average rate that was available in 2009. We are demanding that the Minister for Health engages with community pharmacy ahead of the 30 June deadline.
Mobilise now
It is now time for all of us in the IPU to mobilise and begin a grassroots campaign to highlight the consistent failure by the State to invest in pharmacy services over the last 15 years. Increasing costs are threatening the viability of many pharmacies around the country, particularly in rural areas, with clear evidence of reduced opening hours and a growing inability to maintain key services to patients. Over the month of June, in conjunction with MKC our public affairs advisors, we will be rolling out a campaign, with the support of members, to highlight our key messages and demands to public representatives with the intention of getting the Minister to engage with us.
This campaign will continue well beyond June if no progress is made. We cannot expect pharmacists to do more work for the State, for less money, while continuing to bear higher costs. Also, the administrative and cognitive burden of the community drug schemes needs to be recognised. It will soon be time for us to consider rationalising the services we currently provide for free. The State will not invest in community services and improved patient outcomes if we continue to fill the gap. It need not come to that if the Department engages with us in a positive way over the coming weeks and months. Community pharmacists know that investing in community pharmacy will deliver services with a proven dividend in terms of value for money for both patients and the state.
Figure 1: Where patients attend
United Drug’s CPD webinar on Urology
Catheter use and common challenges
As part of their added value CPD learning programme, United Drug recently hosted an informative webinar on the topic of Urology – specifically focusing on intermittent catheter usage and best practices for Pharmacists to assist their patients in the community. Some key points covered on the night were:
• Catheter use and common challenges faced in pharmacy
• ISC products – examples of different types and sizes of catheters
• Ancillary products for catheter users
• Support available to pharmacists
Hosted by Superintendent Pharmacist at LloydsPharmacy Ireland Denis O’Driscoll, the webinar was designed as a Q&A for Pharmacists to have readily available access to Urology and catheter information they otherwise may not have.
Eve Cullen, a Catheter User and Pharmaceutical Science student, was a panellist on the night. Eve has the unique experience of being both sides of the counter having worked in pharmacy and therefore gave an exclusive insight into giving patient care and using catheter products herself. She gave a particularly good example of how patients might like to receive their treatment products in
a discreet manner after purchase. This information is invaluable to Pharmacists looking to improve their patients experience in store.
Eve was joined by Urology Nurse, Anne Daniels, who provided an incredible medical input to the discussion. All Pharmacists in attendance were given the opportunity to ask Anne any questions they may have encountered through assisting catheter patients in their community. She was also able to inform the Pharmacists where they can get further advice and information on Urology and catheter types, codes, brands etc.
Feedback on the webinar confirmed that by the end of the session, the Pharmacists in attendance felt more confident in discussing catheter usage and urology queries from their patients. All United Drug webinars are held with the patient in mind and aim to equip the Pharmacist to better assist in the community. If this sounds like something you’d be interested in as a fellow Pharmacist, please don’t hesitate to contact United Drug
for information on future webinar topics along with access to previous webinar content.
Don’t forget, this and all webinars by United Drug can be considered in your CPD portfolio. All attendees will be issued with a certificate of attendance.
For more information, please contact UDWMarketing@united-drug.com.
Meaghers Pharmacy Group celebrates Two Awards
The team at Meaghers Pharmacy Group is celebrating again as they enjoy an award-winning few weeks receiving awards from Chambers Ireland and at the Irish Pharmacy Awards 2023.
Meaghers was delighted to win the Retail Excellence of the Year Award at the Chambers Ireland InBusiness Recognition Awards 2023 at Clontarf Castle, Dublin, on Friday May 26th.
Meagher’s Pharmacy Group Managing Director Oonagh O’Hagan
The award recognises Meaghers’ best practice, innovation and excellence in promoting, advertising, communicating or marketing their products and services.
On the following evening, Meaghers was honoured to win the Alliance Online Pharmacy Retailer of the Year Award 2023 as well as the BOI Payment Acceptance (BOIPA) Innovation & Service Development (Chain) Award 2023 at the Irish Pharmacy News Awards at the Clayton Hotel, Burlington Road, Dublin on Saturday May 27th.
The awards come after Meaghers was named as a Great Place to Work and one of Ireland’s Top 30 medium-sized Great Places
2024 Fulbright Programme
The Department of Foreign Affairs, Department of Tourism, Culture, Arts, Gaeltacht, Sport and Media, and US Chargé d’Affaires to Ireland Mike Clausen have announced the Fulbright Irish Awardees for 2023-2024, with three of the awards being made to RCSI. Recipients were presented with Awards at a ceremony in the US Ambassador’s Residence.
The RCSI Fulbright awardees are:
• Dr Natalie McEvoy, a StAR Research Lecturer in Critical Care Nursing at the Department of Anaesthesia and Critical Care and PhD graduate from School of Nursing and Midwifery. As a Fulbright-NUI Scholar, Natalie will travel to the Children’s Hospital of Philadelphia and PENN Nursing to undertake a research study which aims to develop an ICU-specific dashboard that explores the relationship between patient needs and nurse staffing with the goal of optimising patient, nurse, and system outcomes.
to Work for the third consecutive year at the Great Place to Work Ireland Awards in April and Retail Employer of the Year at the Retail Excellence Ireland Awards last November 2022.
Oonagh O’Hagan, Managing Director of Meaghers Pharmacy, says, “It’s such an honour to receive these awards from the Chambers Ireland InBusiness Recognition Awards and the Irish Pharmacy News Awards. My team and I are so proud to receive these prestigious accolades for the work that we do in promoting proactive healthcare and education around many health conditions within our communities and for transitioning this experience into the digital world. Thank you to all of our team members who are dedicated to making a difference to our customers lives and to all our customers who choose Meaghers as their pharmacy of choice.”
• Dr Michael Daly, an Honorary Clinical Lecturer at RCSI SIM Centre for Simulation Education and Research and non-invasive cardiologist whose interests include multimodality cardiovascular imaging, electrocardiography, and the education of multidisciplinary teams and medical students. He is awarded a FulbrightTechImpact Scholarship to Stanford University Medical School in California, to develop a narrative-based medicine educational programme using simulation.
• Dr Lukas O’Brien, a core surgical trainee in plastic and reconstructive surgery at RCSI. As a Fulbright student awardee, he will attend Yale University to pursue a masters in health policy and management.
Welcoming the announcement, Professor Cathal Kelly, Vice Chancellor of RCSI, said, “RCSI’s outstanding success at the 2023-2024 Fulbright Awards is a testament to the innovative health-focused research and education carried out by our academic staff and outstanding calibre of our trainees. One of RCSI’s key strengths is our international collaboration and we are immensely proud of our global connectivity and reach.”
Choice Based Buying Group
Unrivalled scale and range of product offering.
Knowledge Centre
Providing meaningful insights, category management and webinars to optimise your business.
Safe & secure sourcing of unlicensed medicines
Enduring a quick and reliable
Driving Medicines Policy Reform
The EU has initiated a major overhaul of EU pharma legislation ranging from regulation to intellectual property and supply chains. The off-patent medicines industry is fully engaged to ensure that reforms transform healthcare delivery and access for patients. Generic and biosimilar medicines help the majority of patients with major chronic diseases such as cancer, cardiovascular disease, diabetes, autoimmune conditions and others. Value added medicines promise affordable, patient-centred innovation which can address unmet medical needs and the crisis in hospitals with personnel shortages and greater demand for healthcare.
Elisabeth Stampa, President of Medicines for Europe
Medicines for Europe sees the revision of EU pharmaceutical legislation as an opportunity to accelerate patient access to safe, effective, and affordable medicines and to improve Europe’s security of supply.
For this to succeed, Medicines for Europe calls for a particular focus on:
• Optimising use: timely competition and uptake measures that encourage greater access to off-patent medicines.
• Flexibility: A regulatory system that facilitates timely access for patients and embraces digital tools like electronic patient information leaflets.
• Prevention: An emphasis on preventing shortages, through guidance on procurement policies and EU finding policies that safeguard well established, inexpensive but essential medicines, with a dedicated Medicines Security Act.
Speaking at the Medicines for Europe annual conference, association President Elisabeth Stampa said, “Medicines for Europe is strongly engaged in the EU pharma policy reform process to ensure that patients have equitable and timely access to secure supplies of medicines in Europe. This will entail comprehensive support of manufacturing and addressing the trends that persistently drive medicines shortages, through a Medicines Security Act. We believe that a joint effort with the European Parliament, Council and Commission with our industry is essential to tackle the challenges
Making Work safer for Retail
faced by health systems in every country in Europe. By working together, we can develop policies that promote sustainable and efficient manufacturing practices, create a framework for value added, affordable innovation, work to eliminate medicines shortages of essential medicines, and vastly improve access to medicines for better health outcomes for European patients.”
The Deputy Prime Minister and Minister for Health of Malta, Chris Fearne said that he “welcomes the long due reform and the proposed modernisation of the EU Pharmaceutical Regulatory Framework. The current framework is problematic in that it unnecessarily complicates supply chains, is costly to industry, and does not benefit patients. It is essential that we break down current barriers within the internal market to the benefit of all EU patients.”
A new security solution to make public-facing workers, including pharmacy teams, feel safer has been launched by Netwatch, the leading proactive video monitoring company headquartered in Carlow.
While traditional systems, such as a Panic Button, trigger an alarm when an incident occurs or a traditional CCTV system can capture the incident for future analysis, the new Netwatch solution goes further. As was demonstrated to Garda Crime Prevention Officers on a recent visit to the Netwatch headquarters, the Netwatch Staff Safety Solution allows an intervention specialist to observe an incident in real time and intervene when staff are facing intimidation or physical risk, and at the same time alerting the Gardai. The new technology has been launched in the wake of a number of surveys showing that public facing staff in retail premises, pharmacies, hotels, licenced premises and petrol stations are facing intimidation and often physical attacks on a regular basis.
A recent survey from the retail group RGDATA found that 95% of
retailers have been victims of crime over the last 12 months. 25% said that they had been subjected to violent burglaries and robberies in their shops.
The RGDATA survey also found that shop owners and their staff were subject to abusive behaviours by people engaging in criminal activity in their stores, including screaming and shouting, spitting, punching and kicking, sexual harassment and false defamation claims.
Another survey from forecourt and convenience retailer Circle K published in January, found that 83% of retail workers in Ireland have experienced harassment from customers. Physical assault is another serious issue which the research highlights, with 50% of Irish retail workers having witnessed a colleague being physically assaulted by a customer.
The Netwatch Staff Safety Solution can mitigate these issues by
allowing for two-way conversation between staff and a Netwatch specialist in real time if needed. Once activated the Netwatch Staff Safety Solution provides a live visually monitored situation. A highly trained Netwatch specialist will view the scene live. Along with visually verifying what is happening the specialist can also hear the conversation on the premises as it takes place.
The Netwatch team of specialists will follow the agreed course of action, which may involve speaking directly to the people involved, and contacting the Gardai. The priority is keeping the people involved safe.
Colin Hayes, Netwatch Managing Director for Ireland and UK, says, “A safe outcome for all involved is key for Netwatch. Our team has over 20 years’ experience managing high risk situations and knows how to handle them safely. They will visually assess the event
and take the appropriate action, including liaising directly with the Gardai, providing them with live details of the incident.
“Staff can activate the Netwatch Staff Safety Solution as soon as they feel threatened and be confident that someone is instantly available to help manage the situation safely. This is particularly valuable and comforting for situations where just one staff member is on duty such as an evening or late-night opening situation such as a petrol station or chemist.”
Mr Hayes said that the Netwatch Staff Safety Solution is ideal for retail premises, pharmacies, petrol stations, bookmakers, hotel receptionists and lone desk workers as well as charity hostels. “It enhances the protection of people, property and assets without any capital expenditure, just a simple fixed daily fee.”
Back2School - Sports
Bumps and Scrapes – Be
Front of Shop Ready
As summer comes to a close, there is always a lot to be done to get kids ready to go back to school. However, getting kids ready to start the school year involves more than finding the perfect backpack, buying school supplies, and shopping for new clothes. It means safeguarding their health so they’ll be physically ready for the challenges.
For community pharmacists, the event leads to opportunities for effective front of shop category management. Now is the time for retail pharmacies to get ready for the onslaught of pharmacy needs that crop up among their younger patients as they return to school. Children, ‘tweens, and teens cannot be underestimated, and need to be treated with importance. Pharmacists have a key role to play in advising the younger generation on how to take medications and how to stay away from toxic medications.
Back to school is an opportune time to enhance that discussion.
Providing customers with easy to navigate back-to-school sections in community pharmacy, with relevant point of sale and prominent window displays during August and September, will help remind parents and carers that preparation is key when it comes to the management of back-toschool self-treatable conditions.
In addition, many parents worry about whether they should keep their children at home or send them to school when they are ill. Pharmacy teams should be prepared to ask appropriate questions and offer advice to help them to make that decision. For example, does the child seem well enough to carry out the usual
day-to-day activities they would at school, or is their condition serious or contagious enough to be passed on to classmates or teachers? Helping people to make such decisions will add to their self care skills and knowledge for managing coughs and colds.
Highlighting the availability of products, giving advice for back to school ailments and communicating the principles of self care to parents is an important service that community pharmacy offers families as the first port of call.
From head lice and rotavirus, to stomach upsets and cold/ flu symptoms, there are many self-treatable conditions that can hit families hard when September comes. Consider these commonly presented concerns when thinking about your front of shop and category management within the community pharmacy.
Sports and Injuries
Sports-related injuries will also be common and so ensure your pharmacy is stocked with a ready supply of external analgesics and hot and cold treatments. First aid is easy to learn, easy to remember and easy to do. Pharmacists have the opportunity not only to demonstrate how easy first aid is, but also to advocate for the public to learn more themselves
Cuts, scrapes, and bruises are among the most common injuries, and no family member is safe from minor accidents. Fortunately, these injuries usually can be treated at home without a doctor visit. Pharmacists need to be able to advise patients on how to treat these injuries if medical attention is not necessary, as well as to counsel patients as to when they should seek medical attention.
Scrapes (or abrasions) are wounds in which layers of skin are scraped or torn. The most common sites for scrapes are the hands, elbows, and knees. These injuries often are the result of a fall. Although the scrapes may ooze blood, bleeding does not always occur. Objects penetrating the skin cause cuts (or lacerations). Depending on the depth, cuts often will bleed. Bruises are the result of hard contact with a person or an object. The impact causes an injury to the tissue beneath the skin, and blood from the injury settles near the skin. Bruises usually start out looking red, then within a few hours turn blue or purple, and finally appear yellow as they fade.
Treating Cuts and Scrapes
Minor scrapes and cuts are easily treated at home with basic woundcare or first-aid supplies. Because cuts can happen at any time, every home should have tweezers, gauze
pads, bandages, and antibiotic ointment. Here are some steps that pharmacists should tell patients to follow in treating cuts at home:
• Rinse a cut with cool water
• Wash around the cut with soap; avoid getting soap into the wound
• Remove dirt and debris from the wound with tweezers; clean the tweezers with rubbing alcohol before using them
• Apply direct pressure with a clean gauze pad to a bleeding cut
• Treat the cut with antibiotic ointment
• Cover the cut with a bandage (deeper cuts may require a butterfly bandage)
• Do not pick at a scab while a cut is healing
Treating Bruises
Although bruises can be painful, treatment is limited. The best care for bruises involves rest and ice. Ice stops blood flow to the injury site, thus limiting the size of the bruise. Rest allows the site to heal.
Here are some further guidelines for patients for treating bruises at home:
• Apply ice packs or cold compresses as soon as possible
• Reapply ice packs every hour for 10-15 minutes during the first day, if needed
• With bruised legs or feet, elevate the legs as much as possible during the first day
• Take acetaminophen, if needed, for pain; do not take aspirin
• With large bruises, limit activity during the first day
• Use heat packs after 48 hours to promote healing
Here are some signs that bruises need medical attention:
• The bruise swells
• The bruise does not start to fade within a week
• The bruise occurs easily or for no obvious reason
42 Billion Live Bacteria, 8 ‘friendly’ bacterial strains + Vitamin C
Refrigerated in Pharmacies
*Vitamin C contributes to the normal function of the immune system Nutritionist and Author
Back2School - Asthma Care
Back to School Checklist for Children with Asthma
Asthma is the most common chronic condition among children, affecting one in 10 children and adolescents under 18. Children with the condition miss on average five days of school each year, making it one of the leading causes of absenteeism.
There is a dramatic rise in the number of children admitted to hospital for their asthma in September each year known as the “September spike”. Triggers which are commonly found in schools include:
• Chemical fumes
• Perfumes
• Aerosols
• Chalk dust
In addition, changes in weather, an increase in fungal spores, moulds and in an increase in circulating viruses such as RSV all contribute to an increase in asthma symptoms at this time of year.
Advice for parents
This checklist should help you control your child’s asthma during September and into the winter months.
• Have your child’s asthma reviewed by your GP in August/ September
• Ensure your child has an Asthma Action Plan and it is up to date
• Use the inhaler technique videos on asthma.ie to help your child take their inhaler properly
• Make sure your child carries their reliever inhaler (usually blue) at all times
• Check that they take their medication every day with a fridge planner
• Leave a spare reliever inhaler and spacer in the school, with their name clearly labelled
• If your child is participating in PE or other activities, place a reliever inhaler and spacer in their bag
• Never send a sick child to school
• Show them how to wash their hands correctly and explain why this is important
• An older child/teenager often require extra supervision and cannot be relied on to selfmedicate independently - put systems in place as they may avoid taking their medication
• Visit the school and make sure your child’s teacher is aware that they have asthma
• Explain what their triggers are and what to do if your child has an asthma attack
• Check if there is a School Asthma Policy in place
• If your child is starting a new school, speak to teachers about your child’s asthma, even if they are well right now
Asthma Policy for Schools
The Asthma Society of Ireland recommends that all schools have an Asthma Policy in place that is reviewed regularly. As part of their Asthma Policy, it is also recommends that schools create an asthma record sheet for all students with asthma. The Asthma Society is warning teachers to be vigilant for asthma triggers at this dangerous time of year and to talk to parents to ensure you are aware of any students with asthma in your class.
Written by Ruth Morrow, Respiratory Nurse Specialist, Asthma Society of Ireland
Students with Asthma – advice for teachers
When a student with asthma joins your class, there are a number of steps can be taken to ensure they are supported as much as possible which include:
• Familiarise yourself with the school’s Asthma Policy
• Always ensure that students with asthma have access to their reliever inhaler including during school trips, sports and PE. Relievers should never be locked away
• Tell parents when their child has an attack or needs their reliever inhaler in school and encourage older students to tell you or another staff member if they use their reliever
• Speak to parents about concerns over missed days, tiredness in class due to night-time symptoms or lack of concentration due to asthma. Students with severe or poorly controlled asthma may require extra support due to missed school days
• Monitor students with asthma to ensure they don’t feel excluded or experience bullying
• Provide opportunities for all students to learn about asthma in class
• Think about requesting resources from the Asthma Society of Ireland to ensure the school is well informed about asthma and how to manage the condition
Once you know what triggers the child’s asthma, you can take practical steps to reduce their impact.
• Damp dust chalkboard and classrooms regularly to get rid of dust mites and pollen
• Don’t keep furry or feathery pets in the classroom
• Try to avoid fumes in science and art classes
• Rigorously enforce a non-smoking policy on school grounds
• Make sure the school is cleaned regularly
• Heating and ventilation systems should be well maintained.
• Air classrooms to avoid mould and condensation.
• Avoid plants that give off high amounts of pollen
• Use non-latex gloves
• Make sure that play areas and sports fields are free of autumn leaves as they are full of mould and fungal spores
• Avoid mowing sports fields or grassy areas during school hours
• Make sure changing rooms and bathrooms are well ventilated
• Avoid opening windows and allow students with pollen allergies to stay indoors when pollen is high, such as during and after thunderstorms
P.E. and Sports
Exercise improves lung function and is an important part of a healthy lifestyle. Asthma symptoms shouldn’t stop children from taking part in sport and PE, provided that certain precautions are taken.
This article has addressed managing asthma in schools at a time of year when asthma can be increasingly problematic. Strategies for children, parents and teachers were discussed.
Back2School - Headlice
Getting Ahead of Lice
While several health concerns come to the forefront as students head back to their classrooms, head lice seems to top the list at most pharmacies.
Head lice are tan to grayishwhite, 6-legged, wingless insects typically measuring 2 mm to 3 mm in length, or about the size of a sesame seed. Because lice crawl and do not jump, head-to-head contact is the primary route of transmission. Once on the scalp, lice attach eggs to the base of hair shafts a few millimeters from the scalp surface.
Once laid, eggs hatch within 9 to 12 days, and the resulting nymph matures into an adult louse over the subsequent 9 to 12 days, for a full reproductive cycle of approximately 3 weeks’ duration.
Typical signs of head lice are usually itchiness on the scalp, around the ears and the back of the neck. However, some people may experience no symptoms at all.
Because lice eggs are located on hair shafts approximately 4 mm from the scalp, it is often easier to identify eggs by searching at the back of the hairline, where they are most visible. Research suggests that wetting hair before combing improves diagnostic reliability. There are several methods that can be recommended for managing a head lice infestation. Pharmacy teams should help customers choose the most appropriate product for their child because not all treatments will be suitable for everyone.
Understanding a person’s preference, medical and drug history, the product’s active ingredient, how the active ingredient works, how the product should be used and if anything has been tried previously will allow pharmacists and pharmacy staff to recommend and help parents choose the right head lice product.
Mechanical removal involves systematically combing the whole head of wet hair with a detection comb to remove the lice. The comb must be cleaned after each pass through the hair to remove lice and eggs, which is best done by wiping it on clean white paper or cloth.
The process must be repeated every few days for two weeks. Products containing dimeticone or isopropyl myristate kill the lice through physical action. Dimeticone coats the surfaces of head lice and suffocates them, while isopropyl myristate
dehydrates head lice by dissolving their external wax coating.
The advantages of these products are that they are easy to apply, they have few side-effects, are odourless or have only a faint perfume, and the head lice are unlikely to become resistant to them.
Instructions must be followed exactly otherwise the treatment won’t work. Some of these products don’t kill louse eggs either, so it is vital that the treatment is repeated after a week to kill any lice that have hatched since the first application.
Many parents are looking for allnatural remedies, so it would be wise for pharmacies to stock up on both traditional and alternative choices. It’s also important to alert parents to this topic, as they need to be inspecting their children for ticks and lice and so whilst stocking up on head lice products, education shouldn’t be missed.
Make sure head lice products are prominently displayed, along with educational brochures. Remind parents that their children should not share hats and also point out places where lice can be contracted.
Infections
The threat of infections cannot be minimised. Pharmacies should ramp up their supply of antibiotics at this time of year. Children get back together and start spreading infections so the use of antibiotics is expected to increase.
Common infections presenting to the pharmacy in September will be dermatologic infections, such as ringworm and athlete’s foot, as well as of eye, ear, nose, and throat infections.
It’s important to communicate to younger customers the importance of taking their antibiotics as they are prescribed. It’s especially important that children between the ages of 4 and 12 are given the proper instruction with their parents at their side. Empowering the children—and their caregiver— can help increase compliance.
Most ear infections clear up within a couple of days. Paracetamol or ibuprofen (appropriate for the child’s age) can be used to relieve pain and high temperature. Do not give aspirin to children under 16
years old. Antibiotics are usually only needed if symptoms persist or are particularly severe.
Sore throat symptoms are easily recognised. The throat hurts and is irritated, swollen, or scratchy. Pain increases when sufferers swallow. They may also have tenderness in their neck.
Strep throat is an infection caused by a type of bacteria (group A streptococcus). Strep bacteria cause almost a third of all sore throats. Strep throat usually needs treatment with antibiotics. With the proper medical care — and plenty of rest and fluids — most kids get back to school and play within a few days.
Symptoms of strep throat include:
• sore throat
• fever
• red and swollen tonsils
• painful or swollen neck glands
Kids who do have strep throat might get other symptoms within about 3 days, such as:
• red and white patches in the throat
• trouble swallowing
• a headache
• lower stomach pain
• general discomfort, uneasiness, or ill feeling
• loss of appetite
• nausea
• rash
Strep throat is very contagious. Anybody can get it, but most cases are in school-age kids and teens. Infections are common during the school year when big groups of kids and teens are in close quarters.
Children who present with a scaly round patch on the side of their scalp or elsewhere on their skin, and they seems to be losing hair in the same area of the scalp, the problem may be the contagious infection known as ringworm or tinea.
This disorder is caused not by worms but by a fungus. Scalp ringworm often is spread from person to person, sometimes when sharing infected hats, combs, brushes, and hair clips. The first signs of infection on the body are red, scaly patches. They may not look like rings until they’ve grown to half an inch in diameter, and they generally stop growing at about 1 inch. A child may have just one patch or several. These lesions may be mildly itchy and uncomfortable. Scalp ringworm starts the same way the body variety does, but as the rings grow, the child may lose some hair in the infected area. Certain types of scalp ringworm produce less obvious rings and are easily confused with dandruff or cradle cap. Cradle cap, however, occurs only during infancy.
A single ringworm patch on the body can be treated with an overthe-counter cream. A small amount is applied two or three times a day for at least a week, during which time some clearing should begin. If there are any patches on the scalp or more than one on the body, or if the rash is getting worse while being treated, refer to their GP.
Tinea pedis (athlete’s foot), corporis, cruris and manuum can all be successfully managed with over-the-counter products. Topical formulations include creams, sprays or powders. In most instances, treatment with a cream will be appropriate. Tinea capitis requires systemic therapy and if this is suspected patients should be referred to their GP.
Back2School - Vitamins
Vitamin Supplements in Children
To supplement or not to supplement. That is the question. Vitamins and minerals are important for healthy growth and development in children. Children who eat a well-balanced diet usually do not need a vitamin or mineral supplement. However, some children are at risk for deficiencies and may need a supplement.
When to Supplement
Children who follow vegetarian or vegan diets may need to supplement with vitamin B12 since it’s only found in animalbased foods. Children who have coeliac disease are at a higher risk for nutritional deficiencies and may need supplements. Additionally, children who have a poor appetite, drink a lot of sugar-sweetened beverages, take certain medications or have chronic medical conditions that interfere with intake may need a supplement.
Important Considerations
Parents should strive for a wellrounded diet to ensure their child meets the daily recommended vitamin and mineral intakes. A balanced diet includes dairy or dairy alternatives, fruits and vegetables, whole grains and protein foods such as poultry, fish, eggs, nuts and legumes including beans and lentils. While all vitamins and minerals are important for growth and development, some are especially critical for children.
Vitamins, minerals and supplements (VMS) have always been an important category in the pharmacy with various benefits for not only adults but children of all ages from birth right up to the elderly.
It is generally recommended that all children aged 6 months to 5 years are given vitamin
supplements containing vitamins A, C and D every day. Babies who are having more than 500ml (about a pint) of infant formula a day should not be given vitamin supplements. This is because formula is fortified with vitamins A, C and D and other nutrients.
Babies who are being breastfed should be given a daily vitamin D supplement from birth, whether or not mum is taking a supplement containing vitamin D herself.
Vitamin D
Babies need vitamin D for healthy growth and development. It helps them build strong, healthy bones and teeth.
Babies who don’t get enough vitamin D are said to have a deficiency. If the levels are low enough, they are at risk of getting rickets, a disease that affects the way bones grow and develop.
The recent re-emergence of rickets (a severe form of vitamin D deficiency causing deformity of the bones) amongst infants in Ireland indicated the widespread low levels of vitamin D in the Irish population.
FSAI recommendations
The recommendations are as follows:
1. All babies living in Ireland should be given a vitamin D only supplement providing 5µg Vitamin D from birth. This is necessary because babies aged
0-12 months are at high risk of vitamin D deficiency, due to their rapid growth rates during this period.
2. Supplements that provide only vitamin D and are in a suitable form to be given to infants should be used to supplement infants in Ireland. The daily amount of vitamin D provided by such supplements should be 5µg per day.
3. Health professionals and parents need to be made aware that vitamin D deficiency is prevalent in Ireland, particularly among dark-skinned infants and young children.
Vitamin A is important for babies and young children, and some may not be getting enough.
It’s needed for a healthy immune system, can help their vision in dim light, and keeps skin healthy.
Good sources of vitamin A include:
• dairy products
• fortified fat spreads
• carrots, sweet potatoes, swede and mangoes
• dark green vegetables, such as spinach, cabbage and broccoli
Vitamin C
Vitamin C is important for child’s general health and immune system. It can also help their body absorb iron.
Good sources of vitamin C include:
• oranges
• kiwi fruit
• strawberries
• broccoli
• tomatoes
• peppers
Calcium helps build strong bones as a child grows. Good sources include milk, cheese, yogurt, tofu, and calcium-fortified orange juice.
Iron builds muscle and is essential to healthy red blood cells. Iron deficiency is a risk in adolescence, especially for girls once they begin to menstruate. Good sources include beef and other red meats, turkey, pork, spinach, beans, and prunes.
Megavitamins - large doses of vitamins aren’t a good idea for children. The fat-soluble vitamins (vitamins A, D, E, and K) can be toxic if kids get too much of them. The same goes with iron.
For children and teens with highly selective diets, such as vegetarianism or a dairy-free diet, and for children with erratic eating patterns, you can recommend a daily supplement. Over-the-counter vitamin supplements are typically safe and come in chewable forms in case a child has difficulty swallowing.
Remember, however, that higher-than recommended dosages of supplements can cause problems. For example, giving high doses of vitamin C in hopes of preventing colds and the flu can cause a child to have nausea, diarrhoea, and cramps.
Children’s vitamins and supplements may come in fun colours and shapes, but they are not candy. Make sure parents are able to communicate with their child that vitamins are a kind of medicine, not a snack. They should also always follow label instructions about serving size and dosage instructions.
The Importance of Good Gut Health in Children
The bacteria in a child’s gut plays an important role in keeping them healthy, both mentally and physically.
Gut health has become a hot topic in recent years and the discussion is usually about gut microbiome which are the trillions of bacteria that live inside our gut. These bacteria play a key role in keeping children mentally and physically healthy and also reduce the risk of illness and disease.
Symptoms of a poorly functioning gut include uncomfortable digestion, stomach aches, poor nutrient absorption, poor immunity and sleep, mood fluctuations and general fatigue. All can have a detrimental impact on children.
The gut microbiome is established in the early years of life. It’s particularly important to support a child’s gut microbiome to thrive while they’re growing. In fact, it is believed that before the age of four or five children’s microbiome remains flexible. This is a great time to build a strong and healthy gut health in children. Beyond this age the microbiome is harder to change as it becomes well established. Everyone’s microbiome is unique and, interestingly, diet can be responsible for up to 75% of this variation!
Elimination of Waste
The gut removes waste from the body. This is important to help support liver function. So, to
keep a child’s bowel movements regular (and prevent uncomfortable constipation), encourage a diet with plenty of fibre. For instance, include wholegrains, veggies and fruit in their diet. This will keep the bowels regular and also feed the healthy gut bacteria. Water is also important to help keep bowel movements soft and regular.
The Immune System
The gut is home to 70% of the body’s immune system. It is also the main entry point for bugs to get into the body. Therefore, if a child’s gut is not a strong barrier they will be more likely to pick up nasty bugs. This can lead to illness. Research suggests that a poor balance of bacteria in the gut during early childhood can increase risk of gut-related allergies like asthma and eczema. Advise parents that they can help build their child’s immunity by fuelling the good bacteria in their gut. This will, in turn, keep children feeling energetic and healthy.
The Gut-Brain Axis
The Gut-Brain Axis is the physical and chemical connection between the gut and brain. To clarify, it is a network of millions of nerves sending messages both ways. Chemicals called neurotransmitters, such as serotonin and GABA (which
controls feelings of fear and anxiety), are sent to and from the brain. Many of these are produced in the gut. A thriving, healthy gut microbiome contributes to production of chemicals and signalling messages for good mental and physical health in children.
The Role of Probiotics
Probiotics are the “healthy” bacteria that make up the gut microbiome. Probiotics work to maintain health and immunity. They also fight inflammation and disease. Parents can boost the good bacteria in a child’s gut by feeding them probiotic rich foods. Good bacteria can help to form a strong, healthy microbiome. A probiotic supplement is also an option.
Researchers are still learning about all the benefits of probiotics and how they work. Probiotics may help with digestion, preventing infectious diseases and even playing a role in maintaining a healthy weight.
Some studies say probiotics help children with digestive issues such as:
• Constipation
• Inflammatory bowel disease
• Irritable bowel syndrome
• Infectious diarrhea
Though it is unclear if probiotics benefit children, it’s clear they typically won’t cause harm in healthy children. However, pharmacy teams should recommend parents wait until a child is over 1 year of age before giving probiotics.
Children who are seriously ill or who have a compromised immune system should consult their GP before taking probiotics. Some studies suggest that children with a central line or port should also avoid probiotics. In children with these medical devices, there have been reported cases of sepsis.
Fibre
A child’s diet should contain fibre as an essential component. It is required to achieve good gut health in children and different fibres help the gut in their own unique ways.
While we often think of fibre as a singular nutrient there are actually many different types, for example:
• Insoluble fibre: Wholegrain breads and cereals and the skin of fruit and vegetables help to soften bowel content, promoting regular (and comfortable) bowel movements.
• Resistant starch: This is a type of fibre which is not digested as normal by the body. Resistant starch is found in wholegrain cereals, legumes and starchy vegetables like potato. It travels to the large intestine where it feeds good bacteria in the gut. These good bacteria produce what you need for a healthy digestive system and protection against disease.
• Prebiotics: These are another type of fibre which also feed the friendly bacteria in the gut. This provides another nourishing food source to the healthy bacteria in your gut. The great news is prebiotics are found in foods that are very child-friendly and delicious. Think bananas, apples and oats plus foods that are easy to sneak into meals like barley, onion or flaxseed.
• Soluble fibre: These help to slow the emptying process in the stomach, which can help children to feel fuller for longer. Soluble fibre is found in fruits, vegetables, oats, barley and legumes.
Food supplement, not to be used as a substitute for a balanced diet. Always read the label. Clonmel Healthcare Ltd. Date prepared: April 2023. 2023/ADV/ELE/128H
Back2School - Vaccinations
Know your Role in Childhood Vaccinations
The role of pharmacists in immunisation and vaccination varies across the world; in some countries pharmacists are primarily involved in ensuring the safe supply and dispensing of vaccines, as well as advocating for immunisation, while in other countries they are empowered to play a more active role, as they are legally authorised organise vaccinations activities and campaigns.
It is estimated that ten million lives per year could be saved by increasing access to medicines and vaccinations. Community pharmacists are therefore in a strong position to provide a major contribution to public health due to their accessibility, distribution and available medicines expertise.
Vaccines being Offered during the school year:
• Children in Junior Infants will be offered 4 in 1 and MMR vaccines
• Students in first year of secondary school will be offered HPV, Tdap and MenACWY
These vaccines are also available to students who are in special schools or are home schooled in the same age group.
Meningococcal Disease
Meningococcal disease is caused by infection with Neisseria meningitidis and presents as bacterial meningitis (15 per cent of cases), septicaemia (25 per cent of cases), or a combination of the two. It is the leading infective cause of death in early childhood.
There are several strains or ‘groups’ of meningococcal bacteria (A, B, C, W, X and Y). In the past
50 years, most meningococcal disease in the UK and Ireland2has been due to group B (MenB) and group C (MenC), although the MenC vaccine introduced in 1999 has now successfully reduced cases to just a handful each year. Currently MenB accounts for the vast majority of meningococcal disease although we have recently seen an alarming rise in a particularly deadly strain of meningococcal W meningitis and septicaemia.
There are five main groups that commonly cause disease - MenA, MenB, MenC, MenW, MenY.
MenB causes the majority of the disease.
How it is caused:
• Around 10% of the population carries meningococcal bacteria in the back of their throats at any given time. This is usually healthy carriage and helps develop immunity
• Occasionally the bacteria defeat the body’s defences and cause infection
• The bacteria are passed from person to person by coughing, sneezing and intimate kissing
• The bacteria break through the lining at the back of the throat and pass into the bloodstream
• They can travel in the bloodstream to infect the meninges, causing meningitis, or while in the bloodstream they can cause septicaemia
From September 2021, secondary school children in first-year are offered a meningococcal ACWY booster vaccination.
The Meningococcal ACWY vaccine will boost children’s protection against group C meningococcal disease. It will also provide additional protection against meningococcal groups A, W and Y. In addition, this vaccine also reduces the risk of carrying the disease so can help protect other people too.
MenACWY being used in Ireland is Nimenrix. This is a conjugate vaccine containing Group A, C, W and Y polysaccharides conjugated to tetanus toxoid carrier protein. The vaccine protects against N. meningitidis Groups A, C, W and Y invasive disease.
Since 2015 more cases of invasive meningococcal serogroups W and Y disease have been seen in Ireland. Prior to 2015 the annual number of both serogroups was low. Between 1999 and 2014 there was an average of two cases for both serogroups reported per year.
Between 2015 and 2018, a total of 36 serogroup W and 20 serogroup Y cases were reported, giving an average annual notification rate 9 cases per year of serogroup W and for 5 cases per year of serogroup Y.
In view of the emergence of meningococcal serogroups W and Y, the National
Immunisation Advisory Committee (NIAC) recommended that one dose of MenACWY vaccine should be given to all students in 1st year of second level education replacing the MenC vaccine in 2019.
Meningococcal disease can start very suddenly. Symptoms include fever, stiff neck, headache, joint pains and a rash.
Meningococcal disease can occur at any age, but the highest rate
occurs in children under 5 years of age, especially children under 1 year old. The next high-risk group are young people aged 15-19 years.
Importantly for community pharmacists to be aware, they might have school children and/ or their parents presenting to the pharmacy with associated after effects. Some students can have an area of soreness, swelling and redness in their arm where the injection was given. This usually passes after a day or two.
Some students may get a headache, feel sick in their tummy or run a slight temperature. If this happens, paracetamol or ibuprofen will help.
HPV vaccine for girls and boys
The HPV vaccine has been offered to girls in their first year of secondary school since 2010. This is because the most common cancer caused by the HPV virus is cervical cancer which only affects women.
Since September 2019, boys have also been offered the HPV vaccine. This is because HPV can cause cancers and genital warts in boys too.
Conditions caused by HPV infection
In girls, HPV infection can cause cancer of the:
• cervix
• vulva (the area surrounding the opening of the vagina)
• vagina
• anus
• oropharynx (part of the throat at the back of the mouth)
In boys, HPV infection can cause cancer of the:
• anus
• oropharynx (part of the throat at the back of the mouth)
• penis
HPV infection can also cause genital warts in both girls and boys.
TEETHA GRANULES BACK IN STOCK
Back2School - Oral Health
Education is Key in Dental Care
September is just around the corner, which means children heading back into the classroom. Having spent a summer of cooling drinks and snacks, it’s important parents are reminded as to the importance of making sure they have a healthy smile.
Pharmacy teams have an important role to play in helping with the oral care and health of our younger population. Pharmacies are often the first point of contact for healthcare advice for many people. This puts all of the members of your team in a powerful position to offer preventative and emergency advice to patients and parents (including expectant parents) when it comes to oral health care. The earlier the prevention begins, the better!
Smile agus Sláinte, published in 2021, provides the guiding principles to transform Ireland’s current oral healthcare service over the next eight years. The policy states that, “People in Ireland have benefitted greatly from the improvements in oral health over the past thirty years. It is vital that these improvements continue and benefit all our population. This will require a wide range of healthcare professionals, in dental and general health, across community, hospital and public and private sectors, working together for the benefit of all our people.”
Teething
Children have a total of 20 primary (baby/milk) teeth. These begin to appear through the gums at approximately 6 months old, with the last ones coming in at
2.5-3 years old. Every child is different, and many parents will appreciate reassurance that there are several variations of ‘normal’ when it comes to tooth eruption. Children may excessively dribble, experience mild soreness of their gums, and have flushed cheeks. Sugar-free analgesics (such as paracetamol and ibuprofen) can be recommended for short term use, while teething rings cooled in the fridge can soothe irritated gums. It is important to advise parents that diarrhoea, fever, or other systemic symptoms are not caused by teething, and that teething is responsible for only a very mild and transient temperature elevation.
The permanent dentition begins to come in at around age six, and this can begin with either the exfoliation of the front teeth and replacement with new teeth (incisors), or the appearance of new permanent molars behind the baby molars. The last baby tooth tends to fall out at around age 12, however there can again be wide variation in this. By age 12-13, most children will have 28 permanent teeth present.
Brushing
A soft-bristled, age-appropriate toothbrush, wetted with tap water, should be used as soon as the first tooth appears. The teeth and
gum pads should be brushed twice daily, with bedtime brushing being the priority. If brushing proves a challenge, playing music or singing a song as a distraction can help for the two minutes it takes.
From the age of 2 until 7 years old, a pea-sized amount of fluoridated toothpaste (>1000ppm fluoride) should be used on a soft brush, with parental assistance (until children can tie their own shoelaces). The toothpaste can be a ‘children’s’ toothpaste, but ensuring the correct fluoride concentration (>1000ppm) is key.
As children get older, they may be able to brush unsupervised, using a pea sized amount of >1000ppm fluoridated toothpaste, however, every child’s development is different, and some may need assistance for a little longer.
Many children will report a ‘spicy’ taste from mint toothpastes, and some children with oral sensitivities may not be able to tolerate any toothpaste flavours- there are options of flavour-free toothpastes and these have changed toothbrushing time for the better for many parents!
Diet
With regards to caries development, the frequency of food/drink consumption is the most important factor. Sugar
consumption should be minimised, but this is especially important between meals. It can take saliva up to 60 minutes to return to its optimum pH, therefore if snacking occurs more frequently than this, the mouth does not have an opportunity to recover fully before the next acid attack.
Parents and patients can be made aware of ‘good snacks’ such as whole fresh fruit, raw vegetables, unsweetened popcorn, cheese and yoghurt. Raisins and other dried fruits are best avoided, due to their high sugar content and very sticky consistency.
Medications
Where possible, sugar-free versions of medication should be considered. Many over the counter vitamins and oral liquid medications have high sugar concentrations to make them more palatable. Sometimes it is not possible to substitute medications, therefore rinsing with water, or wiping the mouth out following medication administration should be encouraged.
When to refer
Analgesics recommended by dental practitioners for dental pain are paracetamol and ibuprofen. These can be alternated to avoid breakthrough pain prior to the next dose administration. Parents should also be advised to bring their child to the dentist as soon as possible to assess and address the source of the pain.
Children will occasionally develop swelling associated with their dental pain. This can develop and progress very rapidly and be very dangerous, therefore, emergency attendance with a dentist or to a local Emergency Department is required. This is especially important if patients present with systemic symptoms such as a fever, vomiting or nausea, or difficulty opening their mouth/ swallowing/opening their eye, or visible swelling of the face.
Antibiotics are generally not recommended for small localised swelling in the mouth, but are reserved for spreading infection resulting in facial swelling. They will not remove the source of the problem, therefore a dental visit should always be advised.
step by step
Jordan Step by Step
Children have different needs as they grow older. Step by Step is a unique kids range that follows the children's development and offers tailored design with different features to make brushing easy and effective at every age. The handle, head size, bristles and design are all tailor made to help you establish good dental care habits from the first tooth. Choose the one that fits your child.
Back2School - Allergies
What more is there to know about Allergies?
Having “allergies” specifically undiagnosed allergies can be debilitating, frustrating, frightening, and in some cases, life-threatening. With 100 million allergy-related Google searches a year, people are becoming more proactive about their medical health and seeking answers. Sometimes the answers are difficult to find among the noise, with conflicting ideas on how best to treat and more specifically how to live an allergycontrolled life. There can be a tendency with allergy symptoms to reach for over-the-counter medication while not truly knowing what your drivers are.
What is an Allergy?
Allergies occur when your immune system reacts to a foreign substance — such as pollen, bee venom, pet dander, food or metal and believes it is harmful. Your immune system produces substances known as antibodies. When you have allergies, your immune system makes antibodies that identify a particular allergen as harmful, even though it isn’t. The severity of symptoms varies from person to person and can range from minor irritation to anaphylaxis — a potentially life-threatening emergency.
Symptoms of allergies
• sneezing
• a runny or blocked nose
• headaches
• red, itchy, watery eyes
• wheezing and coughing
• a red, itchy rash
• worsening of asthma or eczema symptoms
• Body rash
• Stomach issues
• Low mood
Written by Joyce Clegg – Managing Director, The Allergy Clinic
Importance of having an allergy test
Many people are increasingly misdiagnosing themselves with allergies, leading to an ideology that allergy symptoms are something that you just must live with.
In some studies, 40% of people claimed to have a food allergy, only 5% did, along with one third of parents believing their children suffered from food allergies with only a fraction of which would pass clinical diagnosis. The knockon effect is that people are now eliminating important foods from their own and their children’s diet without a clinical diagnosis. Typical example of this is if an egg allergy is suspected a lot of people also remove milk, wheat, and query other foods. Having an allergy test is the only way to definitively know what our allergy drivers are. It is only then we can commence a treatment plan tailored to the individual and ensure we are not missing out nutritionally. How do we test?
Type 1 hypersensitivity test – Skin prick testing or IGE blood testing.
The most frequent positive responses identified in The Allergy Clinic are grass pollen, tree pollen, dust mite, milk, egg, peanuts, tree nuts, fish, shellfish, and wheat. Bee and wasp venom are the most common insect.
Type IV delayed response – Patch testing over 5 days.
Allergy Patch testing is used for contact dermatitis type symptoms to determine if the body rash is allergic or non-allergic in nature. While we test for everyday substances that come into contact with the body i.e. washing powder, clothes, beauty products, metals, dyes, it is generally hair and nail products or work-related exposure to metals, textiles, dyes that are most common. There has also been a notable increase in anal and vulva irritation due to an allergic response to grooming products.
Metal Allergy testing for orthopaedic implants
Working alongside Mr Paul Nicholson, orthopaedic surgeon, The Allergy Clinic have developed metal allergy testing for orthopaedic prosthesis. We have increased our capabilities to test for titanium, cobalt and nickel among other metal components found in implants. Unfortunately, we see a lot of patient’s postsurgery showing signs of metal allergy resulting in second surgeries to replace the titanium
implant with a cobalt one and vice versa. Symptoms of metal allergy can be a rash or burning sensation around the joint, typically hip or knee, burning sensation with no infection present, depression or failure to recover as expected.
Are allergies for life?
Children diagnosed with milk or egg allergy can outgrow their allergies, however, peanut allergies tend to be for life. We can also develop allergies at any stage in life.
Anaphylaxis
Food/nut allergy, bee or wasp venom allergy, drug allergy and cold urticaria are some of the more serious allergens that can lead to anaphylactic shock.
This can be a life-threatening reaction and requires immediate treatment by adrenaline injection, followed by expert medical attention.
Eczema and allergies
At The Allergy Clinic we see a lot of patients presenting with eczema. Eczema can be triggered or exacerbated by food
RECOMMEND CONTROL HAY FEVER TOTAL
DEFENCE RELIEF
Beconase Hayfever nasal spray 50 micrograms per spray contains beclometasone dipropionate. For the prevention and relief of symptoms of Hayfever and other seasonal allergic conditions. Adults aged 18 and over: 2 sprays into each nostril twice a day. Max 8 applications per day (400 mcg). Seek medical advice if symptoms do not improve after 2 weeks. Do not use continuously for longer than 3 months without consulting a doctor. Do not give to persons under 18 years. Pregnant and breastfeeding mothers should not use without consulting a healthcare professional. Caution: Recent nasal injury or surgery. Side effects: Rare cases of hypersensitivity reactions. Unpleasant taste/smell, dryness/irritation of the nose and throat, raised intraocular pressure, nasal septal perforation. Product not subject to medical prescription. PA 1186/008/001. MAH: Chefaro Ireland DAC, The Sharp Building, Hogan Place, Dublin 2, Ireland. Date of preparation: Feb 2023. SPC https://www.medicines.ie/medicines/beconase-hayfever-31396/spc Becodefence is a medical device. Contraindications: Known hypersensitivity to ingredients or those with a Sesame oil allergy. Date of preparation: 04/2022. IRE BEC 2023 06
Back2School - Allergies
or environmental exposure, e.g. dust mites, moulds, pollens, pets and foods etc. When specific positive allergens are correctly identified a dedicated treatment plan can be implemented to help alleviate some of the symptoms.
Asthma and allergies
It’s estimated that 470,000 people in Ireland have asthma and 60% to 80% of these also have hay fever. We know asthma can really affect a person’s quality of life so correctly identifying where and if allergy plays a role can be very helpful. Some of the most common triggers for asthma sufferers are environmental allergens, house dust mites, pets, pollens, and moulds.
House dust mites
Some studies show a quarter of the Irish population are affected by some form of allergy with house dust mites being a top offender. There is a common misconception when we talk about a dust mite allergy people confuse it with dust and believe there is not much we can do about it. Dust mites belong to the spider family, are microscopic in size and not visible, house dust mites tend to affect us the most when we are sleeping. They live in our mattress and pillows. When our airways are relaxed at night, they travel through our nose down into our lungs. When they reach the lungs the dust mite will then defecate. It is the protein in its faeces that cause the allergic reaction. Symptoms of dust mite allergy are feeling groggy on waking, sneezing, blocked nose etc. Treatment includes putting a regular
Children’s Right to Breathe Clean Air
cleaning regime into your bedroom, using zipped matters protectors on your pillows and your mattress, removing all objects that dust can land on i.e., clothes from around your room, books, curtains, toys etc. Recently introduced to Ireland by ALK, doctors now have the option of sublingual immunotherapy for dust mite allergic patients to help with symptoms.
With no financial benefit, The Allergy Clinic has created a range with Dunnes Stores to make zipped mattress and zipped pillowcases available and affordable in Ireland for dust mite allergic people.
While on every medical form and in most restaurants, we are asked “Do you have any allergies” we never really think of the implications and impact allergies can have on our bodies in a broader scale. Testing is simple, generally noninvasive, and extremely beneficial to understanding what our bodies do and do not perceive as harmful to us.
The Allergy Clinic is the only dedicated allergy testing service in Ireland with clinics in Dublin, Athlone, Cork, Waterford and Galway. Adults can selfrefer; children require a letter of referral from their GP outlining the reason for the test. Adults leave our clinics with their results, a management plan and a referral to a consultant if needed. All results are sent to the patients GP for their medical file.
Our goal is to offer our patients quality medical care, carried out by medical professionals in a safe environment.
A new pilot project launched recently, ahead of World Environment Day (Monday 5th June), at Children’s Health Ireland at Temple Street is highlighting the part we all have to play in improving the quality of the air our children breathe. Children are particularly at risk from air pollution because they breathe faster and are closer to the ground where pollution from vehicles hangs. Air pollution can have short and long term effects on children’s health. Some people, including healthy people, may feel a sore throat, dry eyes, headaches, shortness of breath, or nausea, caused by air pollution. Air pollution can trigger an asthma attack.
The FAIR project is a fun, short animated air quality information video in addition to displaying local air quality on Information screens in CHI at Temple Street. The video explains the importance of clean air for good health. We can all take steps to improve the quality of the air we breathe by tracking our local air quality, avoiding busy roads at peak traffic, exercising when air quality is good and not burning solid fuels in our homes. Remember that every time you walk, cycle or scoot instead of drive you are helping to improve your local air quality (but don’t forget your helmet!).
Dr Sandra Green, Respiratory Specialist Registrar, Irish Doctors for the Environment welcomed the project, “This FAIR Air Quality project sends a clear message that air quality is important for good health for everyone, especially for our children. People who breathe cleaner air live longer, healthier lives. Cleaner air means healthier people and a cooler planet. Knowledge is power, and I hope our patients and their parents will find this information helpful at CHI at Temple Street.”
Following the recent publication of the Clean Air Strategy, it is clear that Ireland needs to take steps to improve our air quality in line with WHO standards. Some examples include making it easier to choose walking or cycling and ensuring that all homes in Ireland do not have to rely on burning solid fuels like coal or wood.
Eilísh Hardiman, Chief Executive, Children’s Health Ireland added, “Looking to the future, we want to improve the air quality in and around our children’s hospitals and at the new children’s hospital. This means raising awareness of the effects of air pollution on health, particularly for children and young people. It also means having a range of reliable, affordable and clean public transport options and encouraging all other sustainable modes of travel whether by bike, e-bike, walking or a blended commute. In keeping with our Green Promise commitment, the new children’s hospital is designed to meet BREEAM international accreditation that recognises best in class green building strategies and practices throughout design, build and lifetime operation.”
FAST RELIEF OF ALLERGIES 24hr
Cetrine Allergy 10mg Film-Coated Tablets available in packs of 7s and 30s. Always read the leaflet.
Composition(s): Each tablet contains 10 mg cetirizine dihydrochloride. One ml of the oral solution contains 1 mg cetirizine dihydrochloride. Description(s): White, oblong lm-coated tablets, scored on one side. Can be divided into equal halves. Clear, colourless liquid with banana avour.
Indication(s): Tablets: Adults and paediatric patients 6 years and above. Oral solution: Adults and children 2 years and above. Relief of nasal and ocular symptoms of seasonal and perennial allergic rhinitis (hay fever); relief of symptoms of chronic idiopathic urticaria.
Dosage: Tablets: Adults, elderly and children aged 12 years and over: 10 mg once daily. Children from 6 years to 12 years: 5 mg (half a tablet) twice daily. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. Children under 6 years: Not recommended. Oral solution: Children aged from 2 to 6 years: 2.5 mg twice daily (2.5 ml oral solution twice daily (half a measuring spoon twice daily)). Children aged from 6 to 12 years: 5 mg twice daily (5 ml oral solution (a full measuring spoon twice daily)). Adults and adolescents over 12 years of age: 10 mg once daily (10 ml oral solution (2 full measuring spoons)). Not recommended in children aged less than 2 years. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. In paediatric patients su ering from renal impairment: Adjust dose on an individual basis taking into account the renal clearance of the patient, his age and his body weight. Contraindications: History of hypersensitivity to the active substance, to any of the excipients, piperazine derivatives or hydroxyzine. Severe renal impairment < 10 ml/min creatinine clearance.
Warnings and Precautions for Use: Cetirizine may increase risk of urinary retention, therefore caution in patients with predisposition factors of urinary retention (e.g. spinal cord lesion, prostatic hyperplasia). Caution in epileptic patients and patients at risk of convulsions. Discontinue use of cetirizine three days before allergy testing. Pruritis and/or urticaria may occur when cetirizine is stopped, even if the symptoms were not present before treatment initiation. In some cases, the symptoms may be intense and may require treatment to be restarted. The symptoms should resolve when the treatment is restarted. Tablets contain lactose. Oral solution contains sorbitol, propylene glycol, sodium (essentially ‘sodium free’), methyl - & propyl-parahydroxybenzoate.
Interactions: Caution is advised when taken concomitantly with alcohol or other CNS depressants. Cetirizine does not potentiate the e ect of alcohol (0.5 g/l blood levels). The extent of absorption of cetirizine is not reduced with food, although the rate of absorption is decreased.
Pregnancy and Lactation: Caution during pregnancy and breast-feeding.
Ability to Drive and Use Machinery: Usually non-sedative, patients should take their response to the product into account. In sensitive patients, concurrent use with alcohol or other CNS depressants may cause additional reductions in alertness and impairment of performance.
Undesirable E ects: Cetirizine at the recommended dosage has minor adverse e ects on the CNS, including somnolence, fatigue, dizziness and headache. In some cases, paradoxical CNS stimulation has been reported. Although cetirizine is a selective antagonist of peripheral H1-receptors and is relatively free of anticholinergic activity, isolated cases of micturition di culty, eye accommodation disorders and dry mouth have been reported. Instances of abnormal hepatic function with elevated hepatic enzymes accompanied by elevated bilirubin have been reported which resolves on discontinuation of the drug. Uncommon: Agitation, diarrhoea, pruritus, rash, asthenia, malaise, paraesthesia. See SPC for all adverse reactions. Marketing Authorisation Holder: Rowex Ltd, Bantry, Co. Cork.
Marketing Authorisation Number: PA0711/075/002-003. Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417 E-mail: rowex@rowa-pharma.ie
Legal Category: Not subject to medical prescription.
Date of Preparation: March 2021
Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
Back2School - Mental Health
Back to School? Don’t Forget about Mental Health
Written by Allison Dunne BPharm MSc MA. IUHPE accredited health promotion practitioner
At this time of year you may see several articles about how you, as a pharmacy team, can help families preparing to go “back to school”. Common topics may include the use of vitamin supplements, prevention of head lice and preparation for in the inevitable cold and flu symptoms. Indeed, these are all important factors for physical health. But what about mental health and wellbeing? This article will consider the mental health impact of the return to school and how pharmacy teams can support families during this exciting, but often challenging, time of year.
When we think about mental health we should consider both the positive and negative aspects. Positive mental health, sometimes called mental wellbeing, includes factors such as happiness, life satisfaction and quality of life. Positive mental health can be protective against some mental health conditions and is important for child development (Department of Children and Youth Affairs, 2014). Young children who have positive relationships with their parents, and teenagers who have supportive peer groups, tend to experience good mental wellbeing (Nolan & Smyth, 2021). The quality of relationships with teachers has also been shown to be important for good mental health, especially among adolescents (Nolan & Smyth, 2021).
Mental health conditions such as depression and anxiety affect a significant number of children. A recent report notes that 16% of 13 year olds in Ireland are at risk from depression (Department of Children, Equality, Disability,
Integration and Youth, 2021) while over 11,700 young people accessed HSE Child and Adolescent Mental Health Services in 2021 (Pollak, 2022). Parents who are concerned that their child has a mental health condition should speak to the pharmacist about whether referral to the GP is appropriate.
Going back to school can trigger feelings of worry and anxiety in some children. In the pharmacy you may meet several parents of children who are concerned about their children experiencing stress during this period. Understanding the causes of common worries can help you to support parents and children during this time. Some of the more common concerns are discussed here.
Exam Stress
Worries about exams and school performance are normal (Duvall & Roddy, 2021). While a small amount of stress around exams is common, if the levels of stress are affecting sleep and daily tasks it is
time to encourage parents to take action. Schools can offer support to students who are worried about exams. If additional help is needed the GP is the first port of call for children who are experiencing high levels of anxiety. In a small number of cases children can be diagnosed with anxiety disorders requiring medical intervention or counselling.
Bullying
The Irish government framework for the health of children and young people is called Better Outcomes, Brighter Futures (Department of Children and Youth Affairs, 2014). The framework identifies bullying as a common concern for school children. The most recent progress report, using data from 2018 noted that 31% of 11-17 year olds have been bullied in school, with 13% stating that they have acted as a bully (Department of Children, Equality, Disability, Integration and Youth, 2022). Worries about bullying may lead to increased stress in the lead up to return to school. Parents can support their children by having regular conversations with their children to talk to them about school worries and encourage reporting of bullying to the school. Each school should have an antibullying policy. Parents can access these (often available online) and should speak to school staff about any concerns.
Sleep
Reduced sleep has been linked to poor concentration and learning during school hours (Hayes & Bainton, 2020). Over the summer holiday it is normal for sleep patterns to be different to during the school term. Bedtimes may be later with the long summer evenings, and a morning lie-in may become a regular occurrence. As the end of the school holiday approaches, bedtimes can be gradually adjusted to match the school routine. Pharmacy staff can remind parents of the importance of good sleep hygiene
in the preparation for the return to school. This will make the first few days of term easier to cope with and start the school year with good sleep habits. Primary school children should sleep for between 9 and 12 hours per night, with teenagers aiming for between 8 to 10 hours (Great Ormond Street Hospital, 2020). Some sleep hygiene tips from Great Ormond Street children’s hospital are;
• Reduce caffeine intake; watch out for caffeine in fizzy drinks as well as tea and coffee.
• Timing of meals; a large meal just before bedtime can disturb sleep. Aim for the main meal to be earlier in the day and give a small snack or warm drink before bedtime.
• Physical activity; sports or a walk in the fresh air during the daytime can help with sleep at night. Avoid vigorous activity just before bedtime.
• Technology; bright lights from mobile phones, televisions or other electronic devices can keep the brain alert. Keep the hours before bedtime devicefree. Try a book or relaxing music at bedtime instead of an electronic device.
• Routine; going to bed and waking at the same time every day (even at weekends) can help with good sleep (Great Ormond Street Hospital, 2020).
Social media
While social media can be a good way for young people to keep in touch with friends, parents may find that children are spending long periods of time online during the holidays. As a return to school date gets closer, the pharmacy team can remind parents to try to gradually reduce screen time to make the transition back to school easier. Late night screen time should be minimised to support good sleep.
Back2School - Skin Care
Practical Tips for Children with Eczema
September is Eczema Awareness month which coincides with back to school for thousands of children around the country. Although it can be a very exciting time for most, it can also be a very daunting time for children with eczema.
The Irish Skin Foundation has the below advice.
Atopic eczema is a very common, non-contagious, chronic (longterm) inflammatory skin condition. For those who have eczema, their skin barrier function (which prevents water loss and protects against allergens and irritants) is impaired or weakened. This makes the skin dry out and becomes more vulnerable to infections by bacteria and viruses. Eczema affects 1 in 5 children which means that in primary school, there will more than likely be a few children in the classroom with the skin condition.
Symptoms of Atopic Eczema include:
The main symptom is an intense itch which can be very uncomfortable, interfere with sleep and impact negatively on the quality of life of the child and their family.
Some children with moderate or severe eczema can experience social embarrassment due to the visibility of their condition.
Typically, eczema goes through phases of being active and under
control. During a ‘flare up’, when eczema is very active, symptoms such as redness, dryness and itch worsen, while at other times, symptoms settle.
Practical tips
With all the excitement and preparation for back to school, we are mindful of the children out there with eczema and what this might mean for them. To help with any worries, we have created some practical tips which may be of benefit.
1. Try to have established a daily bath and emollient regime and continue this routine to aid sleep and prevent flares at this exciting and possibly stress inducing time. If your child is prescribed topical steroids, ensure they are used correctly and step-up treatment if flares occur as advised by your doctor.
2. Aim to buy 100% cotton clothes, especially for garments that are directly in contact with the skin. Some online eczema clothing sites sell cotton shirts and trousers which can sometimes
Healthier Habits: Pause the Treats
New research for the START campaign has revealed that a fifth (20%) of calorie intake for children aged 2-4 is from foods like biscuits, chocolate, soft drinks, and savoury snacks. This calorie intake from these treat foods rises to 25% for children of primary school age. The START campaign from safefood, the HSE and Healthy Ireland is encouraging parents to continue to take steps towards healthier family habits by reducing the amount of treats they give their children and to give healthier snacks when children are hungry. The research also found that treat foods like biscuits, chocolate, soft drinks, and savoury snacks contributed significantly to the total intakes of saturated fat and added sugar among children aged 2-4 and 5-12.
be hard to buy in local shops. When buying socks and tights, be mindful of choosing a high cotton content as opposed to synthetic fabrics.
3. Advise the teacher that your child has eczema. Forewarned is forearmed! This way the teacher can know in advance for instance that it might suit your child to sit in a cooler part of the classroom as opposed to in direct sunlight or beside a radiator. If they are feeling hot or itchy, a gentle reminder to take off a jumper may help. If there is a sand table as there often is in the junior classes, ask the teacher to suggest rinsing hands after the activity.
4. Hand washing with soap and using hand sanitiser at school will probably form part of your child’s daily routine. Washing hands will help remove harmful bacteria and viruses and is important in particular to slow the spread of the coronavirus. To counteract the irritating effect of these products, applying a hand moisturiser immediately after washing will help heal dry skin
and prevent cracking and reduce the risk of itching and scratching. This, in turn, will prevent the skin becoming infected. Allow hand sanitiser to dry before moisturising. Choose a hand cream in a tube that is fragrance free and ideally one that is oil based (an ointment or gel).
5. Try to make the time spent applying emollients fun for children, not a chore. Get them involved to help with application or if distraction or a reward chart appeals, go with what works best for your child.
6. For older children, be aware that activity and sweating can exacerbate itch. If there is an opportunity to shower after exercise, encourage your child to do this.
Over time, most children with eczema will begin to take responsibility for their own skincare. If they know there is support both at home and at school, it will make the transition easier for both child and parents.
Irish Athlete Derval O’Rourke is supporting the START Campaign
Introducing the research, Dr Aileen McGloin, Director of Nutrition with safefood said, “We know that snacks play an important role in children’s diets, particularly so for younger children. However, what this research is showing is that children are getting too many of their snacks from unhealthy foods like biscuits, crisps, chocolate, and sweets. We want to support parents to rethink their children’s snacks, both in terms of what they buy and what they give. Offering healthier snacks particularly during those after-school times during the week would be a good place to start.”
Child and Adolescent Psychotherapist Dr Colman Noctor added, “The latest research from the START campaign underlines how we need to become more proactive about supporting the health of future generations by encouraging good dietary and physical activity habits. The key is to make gradual and progressive small changes. If your children have two treats a day, then aim to reduce that to one treat a day on weekdays and two at the weekend. Once this has been achieved it will provide parents with the confidence to continue introducing healthier diet options. Quick wins are crucial to motivational success and maintaining progress!”
36 Back2School - Diabetes
Type 1 Diabetes in Children
School time for parents, children and teachers can be a fantastic experience, but it has its challenges if a pupil has or has only recently been diagnosed with Type 1 diabetes. Returning to school or joining a new class or school, in the beginning, it can be a bit stressful and busy for all involved.
Preparing for back to school means organising books, uniforms, school lunches and much more. For children living with diabetes, it also means managing or changing insulin regimes and thinking about blood glucose monitoring in school. There can be an added concern for parents, as well as for the teachers if a child with diabetes is starting school for the first time or changing to a new class with a teacher who may not be yet familiar with diabetes or even moving on to post-primary school. The younger the child, the greater the involvement in care of school staff it is, often including Special Needs Assistants.
The HSE ‘Schools’ document’
Knowing that it can be an anxious time for parents and children, as well as for the school staff, Diabetes Ireland has prepared some tips and tools to help all concerned with this challenge. It is important that parents/ carers engage positively with the school, and ensure the teachers understand the condition and how they need to act, bearing in mind that they have other pupils to care for as well. Good written and verbal communication between parents and the school is key. To improve the communication, the ‘Meeting the Care Needs of Primary School Children with Type 1 Diabetes during School Hours’ guideline was released last year. New guidelines recently published by the HSE strongly recommends involving the child’s diabetes team early in the process and provides a number of tools and
Written by Dr Kate Gajewska, Clinical Manager for Advocacy and Research
easy to follow actions to help school staff to understand Type 1 diabetes and the needs of their pupil. The document sets out clear guidelines that will help structure the conversation and preparations between the family, diabetes team, and school staff. It explains diabetes and diabetes management to teachers and school staff, sets out clear lines of responsibility for all partners. It also helps to helps to determine the need for non-teaching support (Special Needs Assistance) and for the first time presents different levels of support needs for children with diabetes based on age and diabetes management skills.
As part of this very comprehensive document, a scheme of a Personal Pupil Plans is included, which can be a very helpful tool to agree on current diabetes management and needs of a child. This includes information such as personal hypoglycaemia symptoms, what to eat during hypoglycaemia, when to check glucose levels and deliver insulin. The school can have such a personalised ‘information pack’ handy for all their students who have diabetes.
Document to improve collaboration
Professor Nuala Murphy, Consultant Paediatric Endocrinologist and National Clinical Lead for Paediatric Diabetes commented: ‘I hope that school leaders and every family of a child with diabetes will familiarise themselves with these recommendations and find the practical tools helpful in managing the care needs of children with diabetes during the school day”. Diabetes Ireland was heavily involved in the development of this document. ‘We are delighted, that after years of preparation and the involvement of many people, the document has been launched. Parents of children with diabetes, teachers, SNAs call us frequently for support and advice. This document will be a tremendous resource for everyone in ensuring the safety of the child and their happiness in school - highlights Dr Kate Gajewska, Diabetes Ireland Research and Advocacy Manager.
Diabetes Ireland has developed a resource for parents and teachers on their website https://www. diabetes.ie/living-with-diabetes/ child-diabetes/school-anddiabetes/ where the Meeting the Care Needs of Primary School Children with Type 1 Diabetes during School Hours document can be downloaded, and with and find lots of useful information on
caring for a child with diabetes in the classroom.
Tips for parents and schools at www.diabetes.ie
There are separate sections for parents and carers, and for the teachers and school staff. The first one includes tips on how to start planning for back to school early, explains how to prepare the school and what to expect, provides information on special needs assistance and requires non-teaching support, gives tips on healthy lunch time snacks, and how to support the child from the mental health and well-being side. In the section for teachers, SNAs and other staff educational materials about type 1 diabetes, hypo- and hyperglycaemia and diabetes management are provided, as well as information on how important it is for their mental health and well-being to be included in the school-life. This section provides tips on what can schools do to support the child and their family, explains how to determine the non-teaching support. All the information is in line with the HSE guidelines.
Professor Murphy also adds: ‘We hope that this guideline will improve communication between parents, school staff and diabetes teams and that it will be a helpful resource in maintaining the safety and diabetes control of the child with diabetes during the school day.”
Continuing Professional Development
CPD
60 Second Summary
Pharmacy automation refers to the processes and technology (hardware/software) that automate the repetitive tasks that prevent pharmacists from being useful in more creativityintensive tasks. Pharmacy automation aids pharmacy management in improving accuracy, reducing labour costs, maintaining stock levels, improving service delivery and customer service.
Pharmacy automation handles the tedious, repetitive, and less creative duties, freeing pharmacists and workers to focus on jobs that demand empathy, discretion, and creativity. Investing in automation at your pharmacy can help reduce the daily labour intensive processes required for your pharmacy to operate.
Reallocating your time and your staff’s time can also allow you to better focus on your patients, a quality that makes your independent community pharmacy stand out from others. Utilising the latest advancements in technology can keep your independent pharmacy competitive. Automation isn’t a one-size-fits-all model.
Pharmacies should be making any services they offer customers available online, ideally it should be from your website but if you do not currently have one, there are plenty of solutions that allow you to offer without it.
Automation does not have to be complicated and when simplified, often means less work to initially set up and ultimately lower cost. Automating is a process and can be adjusted as and when required. Flexibility is always required as existing sop’s and workflows ultimately change at the same time.
Your staff can be the best source for new ideas and suggestions. Invite pharmacy staff members to step back and observe all of your pharmacy’s key processes.
AUTHOR: Steven Graham owner/founder Clover 51
Steven Graham is the owner and founder of Irish pharmacy automation company Clover 51. An automation engineer with nearly 30 years experience of which 18 years have been specifically in pharmacy automation.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
Pharmacy Robotics
4 previous steps, log and record your findings.
Published by IPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
The best way to predict the future is to create it
Imagine a modern pharmacy in which a comprehensive patient service is at the forefront. A pharmacy without queues, losses or mistakes. In it, everyday work devoid of additional, timeconsuming activities becomes a pleasure. Sounds incredible, right?
Pharmacy is filled with highly skilled and knowledgeable individuals and businesses who are trying to improve patient health on a daily basis, yet so many of the tasks are being fulfilled manually. Healthcare is under huge pressures due to many reasons, like an ageing society, labour costs, drug shortages etc there is help available but remember “Nothing can change if you continue to do the same things day in day out” - It is a very logical but truthful statement, while you continue doing the same things, nothing can improve. For most pharmacies that means ever increasing workload, less funding and more stress.
The pharmacist/pharmacy role is forever changing and evolving. There are more expectations being set on pharmacists as the healthcare system changes. Many
new tasks are being asked and it can seem a real challenge to complete them all.
So what is pharmacy automation?
Pharmacy automation refers to the processes and technology (hardware/software) that automate the repetitive tasks that prevent pharmacists from being useful in more creativity-intensive tasks. Pharmacy automation aids pharmacy management in improving accuracy, reducing labour costs, maintaining stock levels, improving service delivery and customer service. When pharmacy automation is mentioned it is common for people to think about large dispensing robots that have a high capital investment requirement but pharmacy automation is software and hardware.
In the 1960’s pharmacy automation hardware started to appear in hospitals and community pharmacies across the globe.. the Kirby Lester pill counter automated the manual task of counting each individual tablet at very high speeds. As technology advanced and manufacturing costs reduced,
we gradually saw an increase in automation machines and manufacturers. As the personal computer industry advanced so did web automation and unlimited access to allow just about any software and process to be linked together.
Pharmacy automation handles the tedious, repetitive, and less creative duties, freeing pharmacists and workers to focus on jobs that demand empathy, discretion, and creativity. It enables them to focus on directly serving clients and developing new opportunities rather than wasting valuable time counting pills.
Here are 6 reasons why you should be considering automation in your pharmacy.
AUTOMATION CAN HELP BY:
Increase workflow efficiency
Investing in automation at your pharmacy can help reduce the daily labour intensive processes required for your pharmacy to operate.
With automation, you can free up your time or your pharmacists’ time, to provide clinical services, such as immunisations or diabetes
38 CPD: Pharmacy Robotics
counselling. It can also give you more time to complete other tasks and allow you to plan your pharmacy growth.
Improved interactions
Reallocating your time and your staff’s time can also allow you to better focus on your patients, a quality that makes your independent community pharmacy stand out from others. You’ll have more time to help patients who have questions, and provide additional services.
Minimise dispensing errors
Humans make errors; robots make next to none. Every once in a while you may give one too many pills. Human dispensing errors are an opportunity for disaster.
Automation can ensure a higher success rate of correctly filled prescriptions, and it also fills prescriptions at a faster rate than by manual process. This saves time and can save you by minimising errors.
Reduced employee stress
Automation can give your pharmacy a more efficient workflow, which can lead to less employee stress (calmer environment). Your pharmacists
and technicians may find that they feel caught up instead of constantly behind. And, if your prescription volume increases, you can utilise the automation process more often, instead of increasing employees’ workloads.
Invest in innovations
Utilising the latest advancements in technology can keep your independent pharmacy competitive. Automation isn’t a one-size-fits-all model. There are all types of automation solutions to fit every size and type of pharmacy—from software automation to various packing, dispensing and delivery robots. If you’re not investing in the types of technologies that can move your business forward, then you may get left behind.
Boosting adherence
If you add a robot or automatic dispensing system to your pharmacy, you have many different packaging options to help improve patients’ medication adherence, such as pouch packaging or blister tray filling robots. These can all be tailored specifically to the patient requirements with all information printed for the patient to easily read and understand.
What processes can pharmacies automate ?
Practically everything can be automated with some development
It is a common thought that to automate a pharmacy, it needs to have a large dispensing volume, this is simply not true. Of course if you have a low volume script dispensing pharmacy and decide to purchase a large dispensing robot, your return of investment will take a considerably longer time but you have to also consider other important factors like patient safety, inventory levels and staffing. A dispensing robot will improve your stock inventory making sure you know exactly what you have in stock at any one time. It can manage your expiry dates and makes sure you get the correct drug dispensed. That being said, automation is all about not having to do the manual intense processes repeatedly. Freeing up the time to add value to the pharmacy business in other areas.
Automation hardware and software types
1) Dispensing robots - used to accurately store and dispense medicines along with speeding up your process. They have a
complete live inventory which can be used for re ordering purposes, to ensure stock is available and reduce over stocking levels. They can vary in height, width and depth depending on manufacturer. Some solutions are modular which allows for increased size in the future.
There are 3 types of dispensing robots:
a) Chaotic - high space efficiency with the only limit to the number of skus, is the number of boxes you can physically store inside the robot i.e. if capacity is 100 then you can have up to 100 sku’s. Manages expiry dates and can handle split packs. Can automate a higher percentage of the pharmacy.
b) Channel system - modular, lower cost, fast dispensing. Limited sku’s to the number of channels available. All skus in each channel have to be the same and also the quantity of tablets has to be the same in each box. Smaller percentage of stock automated due to the number of skus/ channels available. To automate more sku’s, a larger machine is required. Lower intelligence than chaotic roots and less flexibility.
c) Hybrid - Newer type of robot solution and offers the intelligence and storage efficiency of a chaotic robot but with the speed of a channel system. Highly flexible and intuitive solutions. As with the chaotic robots, the number of skus can be up to the robot capacity.
2) Blister filling robots - these automatically fill MDS blister cards for patients. Increase accuracy instantly and reduce filling time by at least 50%. There are various solutions on the market, everything from light to fill entry systems up to fully automated, producing 60 blister cards per hour. Vision systems are available from some manufacturers which increases patient safety. It is important that this type of automation has full traceability of every blister filled, including the drug details.
Some manufacturers are limited to certain blister cards, always check that it is possible to use several different brands or types of blister cards to allow for more options and flexibility, depending on market pricing and also because you may use smaller/bigger blister cards depending on the patient or care facility.
3) Pouch packing robotsanother MDS packing machine but
instead of blisters, medication is filled into clear pouches. Patient/ drug details and administration time of day are all printed onto the pouch with any further details. The pouches are tearable and easy to use. Produce a monthly supply for a patient in under 2.5 mins. Varying sizes of robots to suit pharmacy needs. Usually comes down to the number of different drugs being used to decide machine size. Pouching speed is nearly identical, it is just the number of stored drugs that varies.
4) PMRs are used in all pharmacies. They manage all your patient medication requirements. They are vital to the running of your pharmacy. PMR systems range from simple medication administration software with clunky interfaces and poor loading times to cutting-edge Pharmacy Administration Systems that interact with Dispensing Robots and virtually any healthcare app. PMR systems need to have the ability to easily integrate with new technology and company willingness to do so otherwise you end up creating new inefficiencies as the healthcare landscape
changes. Traditional workflows have significantly changed hugely in the last 10 years.
5) Epos - A good epos is vital to any pharmacy. Automating functions on an epos saves endless hours week in, week out. From understanding what retail and otc is being sold and automatically adding new deliveries to the inventory, can save hours for the average pharmacy per week. It does not matter if you are a small corner pharmacy or large high street pharmacy, a good epos is a must. Epos solutions not only show you busy times during the working hours but with connecting to your accounting software, save administration costs daily. Being able to update pricing, knowing your real profit margins based on each product reorder costing is now fundamental. Epos now has the ability to know who your most valuable customers are.
6) Web automations - In the new age of digital automation, the web is a vital part of what is needed in pharmacy. You may have a pharmacy website where
you list the services that you offer. Traditionally customers would phone or call in to find out more or to book. Pharmacies should be making any services they offer customers available online, ideally it should be from your website but if you do not currently have one, there are plenty of solutions that allow you to offer without it. Booking systems – can be easily created and integrated with minimal work into any website. Create different services, you decide when they are available and you can sync with any existing calendar for example, you have 2 staff members that provide the service, the booking system can be tailored to sync with the calendar so that if booked in shop, it is automatically reserved on the online system. Maximising your services is a must, no more need to have a member of staff available to take the bookings by phone. Implementing web hooks – this is simply a task to be actioned once a process has been started i.e. when you make a booking, an email could be sent with confirmation details and maybe a list or pre defined
rules for the booking. Other web automations could be an online shop, being able to reserve stock for pick up which brings me on to click and collect. A simple solution that automatically does the sales process without a member of staff being tied up with customer 24/7
7) Retail vending - With such a good pharmacy retail market in Ireland, it is a surprise that there has not been a bigger uptake on vending. Gone are the low technology machines from 30-40 years ago. Automatically generate sales via 24/7 vending machines. Very little upkeep required, link with your epos or online shop, use click and collect and even allow vending machines to create reservation stock code. Vending machines can be installed with your pharmacy branding with led lighting showcasing the products on offer while creating an extra service to the local community.
8) Digital - healthmail is a welcomed step forward to allow pharmacies to be able to prepare prescriptions in advance. Digital screens inside pharmacies, shop windows and outside pharmacies
promoting what services you offer and current product offers, is another great low cost way to showcase to your customer base. It is proven technology which often is used as a reminder or “trigger” for a customer that is needing one of your services. Repeat rx order apps are another great example of how using modern technology can make it easier for the customer and allowing pharmacies to advance plans.
9) Workflow software - many new software solutions can be found on the market to help enhance further, different areas in pharmacy. Prescription collection software is one of the examples, allowing patients to be automatically notified when their prescription is ready to be collected. These solutions offer full traceability of who collected and when, often with a signature for verification. The data that is available form prescription collection is vital to the day to day running of the pharmacy, allowing users to understand when patients collect their rx, reducing time on a shelf, full overview of how long prescriptions have been stored and alerts.
10) Invoicing - last but certainly not least. Automating invoicing and back office tasks have been around for many years and have proven cost savings. This could just be verifying stock deliveries match invoicing or automatically checking the price being charged, This is often an area left neglected as it is time consuming. Automating some or all of this
process provides a quick return of any investment made.
There are lots of ways in which you can automate pharmacies and again welcome efficiencies and sometimes a little help of where to start is all that is needed. Automation does not have to be complicated and when simplified, often means less work to initially set up and ultimately lower cost. Automating is a process and can be adjusted as and when required. Flexibility is always required as existing sop’s and workflows ultimately change at the same time.
Filling prescriptions in an efficient, timely manner is vital to both serving your patients and lowering the operating costs of running your pharmacy. But pharmacy efficiency is becoming even more important as industry-wide issues i.e. quality ratings and healthcare reform, continue to put pressure on pharmacy As prescription dispensing volumes increase, you need to gain efficiencies and lower your cost of dispensing in order to maintain patient safety and satisfaction.
1. Measure your workflow
Unless you have set up a way to monitor your process workflow, you will never know if you are making progress or not. A first step is to identify what your basic requirements are and what you need to measure. In pharmacy, we want to measure accuracy but we also should be looking at productivity. Once a basic metric is in place, then you want to hold
staff accountable. Metrics help your staff based on facts and eliminates making decisions based on a whim or personal bias.
2. Stock holding
Having too much or too little stock is a problem. Too much stock ties up working capital and valuable shelf space, while too little can result in owings, customer complaints, and lost patients. Identify your fastestmoving items and consider checking the reorder points regularly. Generally, less safety stock is needed for high-volume items that are being ordered frequently. Slower-moving items can be checked less frequently, but there should be more safety stock on hand. It is a good idea to review stock levels regularly to allow for seasonal trends as well as growth. Controlling the repeat prescriptions will help you with your stock holding. Often the problems arise from new stock not being accounted for when a new order is about to be placed.
3. Motion
Think small. Do you know how many steps your pharmacists and technicians walk each day in your pharmacy? Consider mapping the travel of a technician filling a script. Does he/she have to leave their workstation to complete the order? Does the pharmacist/technician have all of the necessary tools in the workstation to complete the task? Just because you have space doesn’t mean that you need to use it all and spread the work around. To improve operational efficiency try moving the work closer to the worker. By bringing the work closer to the worker you can eliminate
wasteful travel time and improve productivity, while also improving employee satisfaction.
4. Automate
Many outstanding technologies have been designed to aid pharmacists and technicians in the prescription-filling process. Depending on your goals, automation can be used to free up pharmacist time for other patient care activities, to reduce service costs or to maintain service costs without adding extra staff. Remember it does not have to be hardware that you have to automate. It could be software or hardware or both.
5. Listen to what your staff say
Your staff can be the best source for new ideas and suggestions. Invite pharmacy staff members to step back and observe all of your pharmacy’s key processes. Do they see bottlenecks, unnecessary travel, or issues causing delays in the process? Opportunities for improvement? Have them record their observations and report their findings to the team. Have staff brainstorm ideas on how to reduce steps, eliminate bottlenecks and improve the order flow.
Sometimes to move forward, you have to take a step back. I mean literally take a step back and watch what is happening during the working hours of the pharmacy. see at busy times how staff are moving around the shop trying to complete their work. Ask what and why they are doing something. Often this can really help to reduce the steps or time it takes to complete something.
Call for papers: make your contribution to Irish Pharmacy News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to editor
In-depth review articles critique fundamental concepts, issues, and problems that define a field of research or practice and support advanced practitioners as well as aspiring early-year pharmacists.
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients with the aim to improving pharmacy practice.
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions.
Migraine, Diet and Sugar
Introduction: Migraine is the commonest neurological disorder and the most frequent condition for referral to neurological departments. It is a leading cause of disability as ranked by the World Health Organisation and can effect individuals of all ages from childhood to old age. The prevalence of migraine is 10-12% of the population, is three times more common in women, and the peak prevalence is between the ages of 30-50 years. Migraine prevalence declines in post-menopausal women and the natural history is that migraine goes into remission in older age. However there are exceptions and individual can continue to suffer from migraine into old age.
Diagnosis
The International Headache Society has standardised the clinical diagnostic criteria for migraine and these guidelines are universally adopted by physicians worldwide. The majority of migraneurs will diagnostically fulfil one of the list in fig.1.
1. Episodic Migraine Without Aura
2. Episodic Migraine With Aura
3. Chronic Migraine
4. Vestibular Migraine
Fig.1
The cardinal features of a migraine attack are recurrent bouts of severe headaches, which can be unilateral or bilateral, is throbbing and pounding in character and exacerbated by movement. The headaches are accompanied by nausea which can lead to vomiting, photophobia and phonophobia. 20-30% of patient may experience aura symptoms which can either precede or coincide with the headache. The commonest aura symptoms are visual lasting 5-60 minutes and consists of flashing light, zig-zag lines, and an expanding scintillitating scotoma. Other aura symptoms are sensory paraesthesia, motor weakness and dysphasia.
In 10% of migraine patients the condition becomes a progressive disorder and they insidiously develop Chronic Migraine as defined in Fig.2.
Chronic Migraine: 1.3
A. Headache (TTH-like and /or Migraine-like on >15 d/mo for > 3 month and fulfilling criteria B and C.
B. In a patient who has had > 5 attacks of fulfilling criteria B-D
For 1.1 Migraine Without Aura and /or criteria B and C for 1.2 Migraine With Aura
C. On > 8 d/month for > 3 month fulfilling any of the following:
1. Criteria C and D for Migraine Without Aura
2. Criteria B and C for Migraine With Aura
3. Believed by the patient to be migraine at onset and relieved by a triptan or ergot derivative
D. Not better accounted for by another ICHD-3 diagnosis
Fig.2
3% of Episodic Migraine patients convert to Chronic Migraine on an annual basis. Risk factors for progression include: increasing
Written by Dr Edward O’Sullivan, Director, Migraine Clinic, Cork University Hospital
A number of measurement tools are used to evaluate the disability and quality of patients who suffer from migraine. The MIDAS (migraine disability assessment score) and the HIT (headache impact test) were developed in the triptan era and in more recent times the Migraine specific quality of life questionnaire was pioneered to evaluate patients who have Chronic Migraine. Individuals, during attacks are frequently unable to carry out routine daily activities and typically have to lie down in a quiet dark room, resorting to comfort measures such as applying a cold compress or tying a scarf around their head. Time lost from work, lost productivity, cancelled social engagements, and family life are all greatly impacted with consequences for the individual and the wider family.
Pathophysiology of Migraine
Migraine is a recurrent neurological disorder and the trigemino-vascular theory gives a clear understanding of the mechanisms for pain transmission. The ophthalmic division of the trigeminal nerve and the upper cervical nerves are the pain sensitive pathway and these nerves innervate the meninges, dura mater, large intracranial arteries and the dural venous sinuses. During a migraine attack, on activation of the trigemino-vascular system, either spontaneously or by a trigger factor, neuropeptides are released from the peripheral end of these nerves. These neuropeptides include C.G.R.P. (calcitonin gene related peptide), neurokinin and substance P. These peptides cause a neurogenic inflammatory
reaction in the meninges and large intracranial arteries activating first order neurons in the trigeminal nerve and the transmission of a painful afferent signal to the trigeminal nucleus caudalis and upper cervical nuclei (trigeminocervical complex). 2nd order neurons relay messages to the thalamus and 3rd order neurons further relay signals to the higher centres in the cerebral cortex where pain is perceived.
Trigger Factors and Migraine
The identification of migraine trigger factors is a cornerstone in the history taking in patients who suffer from migraine. Notwithstanding their importance, triggers are only identifiable in approximately 40% of patients. The common trigger factors are listed in fig. 3.
Trigger Factors
1. Stress and Anxiety, overtiredness and lack of sleep
1. Caffeine: Caffeine has a similar structure to adenosine and is an antagonist at adenosine A1 and A2 receptors in the brain. Caffeine is rapidly absorbed and easily crosses the blood-brain barrier. It is contained in many drinks most notably coffee, but also cocoa, soft drinks, and energy drinks. Caffeine is also contained in analgesics such as excedrin, solpadeine
and anadin extra. In low dose caffeine has analgesics properties and is often used to enhance the efficacy of simple analgesics, paracetamol and aspirin providing additional and more rapid relief from headache and acute migraine attacks. However, increased intake of caffeine leads to tolerance and habituation and patients are at risk of dependence leading to increased headache frequency and progression to the development of Chronic Migraine. Withdrawal can result in rebound headache and the continued risk of escalating caffeine consumption. The safe daily intake of caffeine should be limited to 200mg (- 3 cups of coffee per day).
2. Food Additives: In a number of studies, 12%-60% of migraineurs have reported dietary foods as a trigger with many identifying more than 1 dietary trigger. The common dietary triggers are foods containing MSG (monosodiumglutamate) e.g curries, pizzas processed meat, aspartate e.g chocolate, and tyramine e.g. cheese. There is no scientific evidence demonstrating causation between dietary triggers and migraine. The link is based on observations facilitated by the use of headache diaries. In addition multifactorial factors involving multiple triggers including diet, overtiredness, lack of sleep, stress and the menstrual cycle are frequently reported by individuals. General advice is to avoid incriminating dietary triggers with the goal of reducing the frequency of migraine.
3. Alcohol and Migraine: Alcohol consumption is frequently reported as a trigger for migraine and other headache types and up to 1/3rd of migraine patients have identified alcohol as a trigger. Red wine is most commonly identified, but white wine and other alcohol beverages can also cause headache. The causative ingredients is controversial but biogenic amines, sulphites, flavonoid phenols, and 5hydroxytyramine mechanisms lead to vasodilating processing and activation of the trigeminovascular system. Alcohol itself is a potent vasodilator and is known to release C.G.R.P. (calcitonin gene related peptide) a neuropeptide which is intrinsically involved in the pathogenesis of migraine. In migraine patients the headache onset is often acute and begins within 3 hours of intake and can occur after a single drink. As a result many migraneurs are fearful of alcohol, reduce their intake and consume with caution.
Delayed onset headache usually begins the following day when the
alcohol level has returned to near zero, hence the term ‘’hangover’’ headache and is probably due to different mechanisms. “Hangover” headache is common, occurs in both migraine and non-migraine individuals and is more likely to occur with alcohol excess.
Sugar and Migraine
The relationship between dieting, food intake, meal times, fasting, missed meals, exercise and migraine is well established. Low blood sugar levels and the sympathetic drivers to maintain normal blood sugars are thought to trigger migraine. The control of appetite is a function of the hypothalmus and disruption of these homeostatic mechanisms in susceptible individuals will trigger migraine. In communities where people fast as in the month of Ramadan, studies have demonstrated an increase in the frequency and severity of migraine attacks. Dehydration and electrolyte imbalance also play a part. Migraine patients commonly report fasting, either intentionally or by a missed meal, as a trigger for their migraines. Recent studies have reaffirmed a genetic predisposition between migraine attacks and low blood sugar.
Altered glucose transport into the brain is associated with hemiplegic migraine and migraine with aura. The hypothalmus is activated early during migraine attacks, the premonitory phase, when symptoms such as tiredness, fatigue, yawning, dizziness and certain food cravings are present. This activation is postulated to be an adaptive behavioural response to hypoglycaemia or an energy compromised brain. There follows a latent period of up to a number of hours before the onset of headache which develops on activation of the trigeminovascular system.
Another hypothesis in migraine is insulin resistance both peripherally and in the brain. This leads to downregulation of insulin receptors in astrocytes and neurons resulting in reduction of glucose uptake and glycogen synthesis particularly at times of high metabolic demand. These leads to a cascade of changes in neuronal metabolism in hippocampus, amygdala and cerebral cortex.
Management of Migraine
It’s never been a better era to be a migraine sufferer. Scientific advancement has lead to the discovery of migraine specific therapeutic medications for both
the treatment of acute attacks and the prevention of future attacks. The triptans, C.G.R.P. monoclonal antibodies, and small molecule gepants are now part of our armamentarium and have transformed our ability to manage migraine. The landscape continues to change with further treatments in late stage clinical development, including the ditans, 5HT1F antagonists for acute attacks and PACAP (pituitary adenylate cyclase activating peptide) inhibitors for prevention.
Conclusions
Migraine is a recurrent headache disorder with most experiencing episodic attacks whilst for others it becomes a progressive disorder leading to chronic migraine. Headache diaries, in clinical practice, have always been a cornerstone in the management of migraine, particularly now that we have new and better medications. The identification of trigger factors, many of which are dietary, is facilitated by keeping accurate up to date diaries. The self-awareness generated and the vigilance applied by this exercise reduces the overall frequency of migraine and the avoidance of certain attacks.
New Screening Initiative
The HSE Diabetic RetinaScreen programme has launched a new screening initiative for women who have diabetes and become pregnant. The risk of diabetic retinopathy may increase during pregnancy and this new initiative will provide more frequent screening to women, protecting their sight during pregnancy. Part of the National Screening Service (NSS), the HSE Diabetic RetinaScreen programme is encouraging women with diabetes to take up their invitation of this free screening during their pregnancy.
Speaking at its launch at the Diabetic Retinopathy Treatment (DRT) Service in the Mater Misericordiae University Hospital in Dublin, Minister for Health Stephen Donnelly said, “This new initiative provides women with Type 1 or Type 2 diabetes with more frequent and potentially sight-saving eye screening during their pregnancy, given that the risk of diabetic retinopathy may increase during their pregnancy. It brings together maternity services and screening services in a way that supports a multi-disciplinary approach and provides local, targeted care for this specific group of women during their pregnancy.
“I was delighted to support the pilot phase of this project through a grant from the Women’s Health
Fund and I commend all those involved in implementing the national roll-out of this important screening. I would particularly like to thank all those involved in the delivery of maternity services across the country, for their support of this new initiative.”
Dr David Keegan, Diabetic RetinaScreen Clinical Director, said, “For women with diabetes, the risk of diabetic retinopathy and sight loss may increase during pregnancy. This new initiative, through the Diabetic RetinaScreen programme, will deliver a specific service for women with diabetes who are pregnant. This will improve equality and quality of access to eye care for women at risk of sight loss.”
Research in Type 2 Diabetes
Helen Kavanagh, Diabetic RetinaScreen Programme Manager added, “The roll out of screening for women during pregnancy shows how population-based screening can protect people who are more at-risk of eye disease. We piloted the scheme last year to great success and this week, as we announce that it’s now available nationwide, we are asking all women who have diabetes and become pregnant to talk to their maternity care provider about their diabetes, and the availability of eye screening.
“This initiative has been welcomed by all the national maternity units and together we will provide a more systematic approach to eye screening for these women.
Dr Maria Byrne, Consultant Endocrinologist, Mater Hospital; Patient Advocate Vicky Doyle, Clinical Director with Diabetic RetinaScreen Professor David Keegan, Minister for Health Stephen Donnelly and guests
We also urge friends and family members of anyone with diabetes to stay informed about the benefits and limitations of eye screening.”
Women who have diabetes at the time they become pregnant will be referred to the Diabetic RetinaScreen programme by their maternity service as part of their initial assessment, or by their diabetes nurse or hospital doctor. The Diabetic RetinaScreen programme will then contact the woman to arrange their invitation to attend a retina screening appointment.
Diabetic retina screening involves digital photos being taken of the eyes. This is painless and safe at all times, including during pregnancy. If retinopathy is detected as a result of screening, the Diabetic RetinaScreen programme will arrange an immediate referral for further investigation or treatment.
Some women may develop gestational diabetes during pregnancy. This usually resolves after their baby is born. Women who develop gestational diabetes do not need to attend diabetic eye screening.
New research carried out as part of the European RHAPSODY project has discovered molecules in diabetic patients that could help personalise treatments
Type 2 diabetes is a progressive multifactorial disease which presently affects over 400m worldwide, with numbers expected to increase to over 700 m by 2045.
RHAPSODY (Risk Assessment and Progression of Diabetes) is a collaborative project involving more than 100 scientists representing 20 academic institutions, including the Department of Metabolism, Digestion and Reproduction’s Professor Guy Rutter, as well as five pharmaceutical companies and two small and medium enterprises.
The study, published in Nature Communications, sheds light on new molecules that could help clinical teams predict and monitor the deterioration of glucose metabolisms.
“In our study, we chose to systematically assay biomarkers for diabetes progression. They belong to three very different molecular classes: small charged molecules (metabolites), lipids and proteins,” explains Professor Rutter.
Thanks to sophisticated molecular tests carried out on blood samples from 3,000 individuals from three cohorts in Europe and one in the U.S., the scientists were able to discover that some 20 molecules—9 lipids, 3 metabolites and 11 proteins—were associated with rapid disease progression.
“In our study, we were also surprised to see that the biomarkers for diabetes progression that we identified are the same as those related to diabetes risk. This suggests that the same biological process is operating in both cases,” said Professor Rutter.
Sometime in the near future, the researcher would like clinical teams to be able to quickly and inexpensively assay these new biomarkers using a single drop of blood in order to better predict the progression of the disease. To do so, they’ll have to wait for a few technological developments.
Diabetes Ireland Reunion Video
Twenty-five years ago, 9 young adults living with Type 1 diabetes plus a medical support team took on a challenge to successfully climb the highest peak in each of the 4 provinces in Ireland in under 36 hours. The young adults came together from different parts of the country with the aim of showing that living with Type 1 diabetes should not be a barrier to achieving your dreams.
At that time, there was a strong misconception of Type 1 diabetes was a barrier to gaining employment, participating in sports and being able to participate in the full school curriculum. Most importantly, there was a need to address the lack of confidence among young people living with Type 1 diabetes themselves.
An RTE documentary team filmed the challenge in 1997, and 25 years on, Diabetes Ireland recently brought some of the participants and the medical team together again to celebrate the achievement by climbing Croagh Patrick and producing a reunion video. The new footage details their lives with diabetes over the last 25 years, the changes they have seen in that time, such as the impact of diabetes technology and the challenges they have ensued. Once again, the aim is to instil confidence in today’s adolescents and young
adults living with Type 1 diabetes and to raise awareness of Type 1 diabetes in the wider population.
Orla McCarrick from Sligo, a lecturer at Atlantic Technological University, and a mother of 2 children said, “Diabetes is now just a part of my life and does not define who I am. Twenty-five years ago it was a much bigger part of my life and a large part of everyday revolved around managing my diabetes.” Orla puts that down to the development of technology such as insulin pumps and continuous glucose monitors, which over the last 8-10 years significantly enhance her daily life and were crucial in successfully controlling her diabetes during 2 pregnancies.
Kieran Flannagan from Galway was in his own words “a young buck” who did not really do the things his mother and diabetes team wanted him to do to manage his diabetes
effectively. Twenty-five years on, Kieran recently had a kidney and pancreas transplant and wants to highlight the importance of managing your condition well today and reap the benefits in later years enjoying a better quality of life. Climbing Croagh Patrick was a huge personal challenge he set for himself 25 years later and is a major focus in the video.
Fergal Cronin from Mallow in Co. Cork highlights the impact technology has on his Type 1 diabetes management, calling it “a game changer” in his working, sporting, and family life encouraging access to diabetes technology for everyone living with Type 1 diabetes in Ireland. Even though he had not seen other participants in many years, he remembers their courage and determination made the event an undoubted lifetime experience with the reunion bringing back
Donation for Diabetes Ireland
strong memories and similar feelings once again. “For me the 4 Peaks was one summer of preparation, 36 hours of gruelling hard slog, leading to a legacy of a lifetime! Only with the benefit of 25 years of hindsight have I had the opportunity to recognise the life skills the 4 Peaks gave me. I’m extremely grateful to the organisers for all they did. An opportunity and experience of a lifetime,” said Fergal.
Professor Chris Thompson, who had the original idea of the 4 Peaks Challenge said “The achievement of completing the challenge in 36 hours was phenomenal and to see many of the same participants achieving great things in life is fantastic to see. To catch up with everyone at Croagh Patrick 25 years later was very special and I hope all people with diabetes will watch the video and enjoy the experience.”
At a recent reception at the Irish Embassy in London to celebrate the 150th anniversary of The Hospital Saturday Fund, Diabetes Ireland was a beneficiary of a grant which will go towards “Teen Activity Day 2023”.
The reception was hosted by Ambassador Martin Fraser. The Hospital Saturday Fund donated a total of £160,000/¤176,000 to thirty-one medical charities and organisations from Ireland and the UK during the event. The occasion was made even more special with the presence of Graham Norton, a celebrity supporter of Bantry Hospice, who presented the donations. Lesley Garrett, the Patron of The Hospital Saturday Fund, also participated in making the presentations to the recipient charities.
For “Teen Activity Day 2023”, Diabetes Ireland has booked 4 Activity Centres for a day of fun and adventure on Friday 7 July 2023. The aim of the day is to bring together young teenagers living with diabetes to have a fun day and to meet other teens with diabetes. “To date, 40 teenagers have registered, and we hope to see more register in the coming days said Kieran O’Leary, CEO, of Diabetes Ireland.
Ambassador Martin Fraser, Graham Norton, Lesley Garret, Patron, The Hospital Saturday Fund, Kieran O’Leary, CEO, Diabetes Ireland, Paul Jackson, Chief Executive, The Hospital Saturday Fund
Paul Jackson, Chief Executive of The Hospital Saturday Fund said:
“We are delighted to continue the tradition of supporting many charities in both Ireland and the UK, many of which are less well known. The Hospital Saturday Fund is honoured to support the efforts of such deserving charities and help in some way with the exceptional, tireless work that they do. We are delighted to have increased our grant-making funds to £2.3/¤2.5 million to over 600 charities in Ireland and the UK over the last 12 months. This evening has been very special, as for the first time, we have been able to give grants to both Irish and British charities at the same reception and mark our commitment to supporting the
communities in these countries for the past 150 years”. “We are also extremely grateful to the Irish Embassy for hosting this reception tonight. Considering our heritage, it is hard to imagine a more appropriate venue”.
“HSF has been a huge supporter of Diabetes Ireland for many years, and we are very appreciative of their ongoing support, and I want to thank Paul and his colleagues for their continuing support” added Kieran.
Acute hepatitis of unknown cause in children
As of 18 May, 43 probable cases of children with hepatitis of unknown cause have been identified in Ireland since 1st October 2021 and a small number of children are under investigation. This is more than would usually be expected over this period of time.
To date no single virus has been identified in all cases. Investigations are currently ongoing to identify the cause of these illnesses. Data are provisional and based on information available at the time of reporting and are subject to change.
All probable cases are in children between the ages of 0 and 16 years of age, 42 of the 43 cases were hospitalised. Two children have received a liver transplant and there has been one death associated with this disease.
The news comes as the world acknowledges World Hepatitis Day this month, being held on July 28th.
In the UK, health authorities have also reported an increase in hepatitis of unknown cause in children. Investigations are underway in the UK to determine the cause of the illness. Information gathered thus far from the UK investigations suggest that the recent cases of hepatitis may be linked to adenovirus infection, however this theory is still under investigation. The Irish cases have no links to the UK cases.
The common viruses that cause hepatitis (hepatitis viruses A, B, C, and E) have not been detected in any of the cases. One area being explored is whether the hepatitis cases are linked to an increase in infections caused by adenovirus, a common cause of childhood and adult illnesses typically causing mild cold- or flu-like illness, or
diarrhoea. Adenovirus infections rarely cause hepatitis. Other possible causes such as another infection (including COVID-19) or something in the environment are also being investigated. In Ireland, as in other countries, investigations are underway to determine if current or prior COVID-19 infection may increase the risk of this disease in some children.
None of the Irish cases who were tested on admission to hospital had evidence of COVID-19 infection at that time. The majority of the cases had not received COVID-19 vaccination. Ireland is liaising closely with ECDC, UK and WHO colleagues in efforts to identify the cause of this illness.
GPs and paediatric consultants are aware of the recent increase in cases of hepatitis amongst children and will be alert to identify any further cases that may develop.
Advice for Parents
Pharmacy staff should advise parents to go to their GP if their
child develops symptoms of hepatitis. Symptoms of hepatitis can include:
• pale, grey-coloured poo (stools)
• dark urine
• yellowing of the eyes and skin (jaundice)
If their child has any of these 3 symptoms, they should contact their GP without delay. The GP will assess the child and refer on for further assessment as indicated. Other symptoms include:
• muscle and joint pain
• a high temperature
• feeling and being sick
• feeling unusually tired all the time
• a general sense of feeling unwell
• loss of appetite
• tummy pain
• itchy skin
All Ireland Pharmacy Conference
The 10th All Ireland Pharmacy Conference (AIPC) will be held at Ballymascanlon House Hotel, Dundalk on 6th and 7th November 2023. The theme for this year’s conference is ‘Creating Momentum & Building Capacity’
This conference is jointly coordinated by the Northern Ireland Centre for Pharmacy Learning and Development and the Irish Institute of Pharmacy. Its focus is to share good practice in pharmaceutical care and practice development across the primary and secondary care sectors.
Pharmacists, technicians and qualified assistants are encouraged to exchange ideas for pharmaceutical service development in the Republic of Ireland and Northern Ireland.
On the evening of Monday 6th November, the conference dinner will take place at 8.00pm and provides an opportunity to network with colleagues. The main conference proceedings will start at 9.30am on Tuesday 7th November and will involve parallel oral sessions and poster presentations. Visit www.allirelandpharmacyconference.com for full details.
Anticoagulants may help treat Sepsis
Scientists have just discovered that the drug dimethylfumarate can block blood clotting during infection. Their work offers hope that it could be used to treat a number of conditions, such as life-threatening disseminated intravascular coagulopathy (DIC), which can occur in serious infections with bacteria that lead to sepsis or in response to viral infections such as COVID-19.
Reporting in leading international journal, Nature Communications, Dr Tristram Ryan and Professor Luke O’Neill from the Trinity Biomedical Sciences Institute (TBSI), with collaborators in Trinity, Royal College of Surgeons in Ireland, Poland, Germany and Australia, describe how dimethylfumarate and a related experimental drug called 4-OI can stop coagulation by decreasing production of a clotting factor called Tissue Factor.
They have shown that the mechanism involves a block in proteins called interferons, which promote tissue factor releases.
Dr Ryan said, “DIC is one of the leading causes of death worldwide so we hope our findings might lead to new therapies that save lives.”
The team demonstrated that life-threatening clotting could be prevented in mice infected with the bacteria E. coli and Staph aureus and also in response to SARS-CoV2, the virus that causes COVID-19. They also showed the process being blocked was dysfunctional in blood samples taken from patients in St James’s hospital with severe COVID-19.
“We hope our work will lead to better therapies to halt the dangerous blood clotting that can occur in people with severe infections, including COVID-19,” said Professor O’Neill.
Dr Ryan added, “Dimethylfumarate is already in use for diseases such as psoriasis and multiple sclerosis and could be repurposed for sepsis and COVID-19, while 4-OI might be used to develop a brand new therapy.”
Management of Prostate Cancer in Ireland
In 2022 3,941 people were diagnosed with prostate cancer, making it the most common cancer in Ireland excluding non-melanoma skin cancer. Worldwide, more than 1 million men are diagnosed with prostate cancer each year and more than 300,000 die of the disease.
Startling statistics show that 1 in 6 men will be diagnosed with prostate cancer during their lifetime, 1 in 8 up to 75 years of age. However, when detected early, prostate cancer has very promising five-year survival rates of 93%.
But like many other forms of cancer, these survival rates are all dependent on when the cancer is detected, and we know that early detection saves lives and improves survival outcomes. The Marie Keating Foundation encourages men to be more open about their health and to speak to their GP about a PSA test when they turn 50, or 45 with a family history of prostate cancer.
Urology Nurse Specialist and Director of Nursing Services at the Marie Keating Foundation, Helen Forristal explains: “Men typically get a bad rap for not speaking about their health, but when resources and supports are put in place, we see that this is not the case. We have yearly Prostate Awareness campaigns urging men to Stand Up For Their Prostate and become more prostate health aware, we provide a host of resources on our website including our Marie Keating Foundation Talks Cancer podcast where we dedicated a whole series to Prostate cancer. We hope that by initiating more conversations we will incite more men to take action. Our message is a simple one, if you are 50, ask your GP to consider checking your PSA levels. If you are 45 with a family history of prostate or breast cancer, have that conversation. It could save your life.”
A PSA or Prostate-Specific Antigen test is a simple blood test that monitors possible changes in your prostate which may need further investigations and follow up. By having regular PSA levels checked as instructed by your GP or Urologist, it can help to detect prostate problems or cancer in its earliest stages, even if you are experiencing no symptoms and please do remember prostate cancer may have no symptoms or signs at all.
More information on the Prostate and Prostate Cancer
What the prostate is
The prostate is a gland found only in those born as males. In younger men, it is about the size
of a walnut, but it can be much larger in older men. The prostate is found below the bladder. It surrounds the first part of the water pipe (urethra), which carries urine from the bladder to the penis. The same tube also carries semen, and the function of the prostate is to thicken the semen for ejaculatory purposes. The prostate gland is divided into 2 lobes, to the left and the right of a central groove.
What the prostate does
The role of the prostate is to make some of the fluid that protects and nourishes sperm cells in semen, making the semen more liquid. The growth and function of the prostate depends on the male sex hormone testosterone, which is produced in the testes. Some treatments for prostate cancer work by lowering the levels of testosterone as prostate cancer is a hormone dependent tumour.
Prostate cancer
Several types of cells are found in the prostate, but almost all prostate cancers develop from the gland cells (the cells that make the prostate fluid that is added to the semen).
Prostate Cancer Facts:
• Prostate cancer is the most common male cancer in Ireland.
• Many men with early prostate cancer have no symptoms at all.
• Because you may not have symptoms, if you are a man over the age of 45 it is really important to talk to your doctor about PSA testing if you have a family history of Prostate or Breast cancer. When you reach 50 irrespective of family history you should talk to your GP about the PSA blood test. It is important to note that the PSA blood test is not a screening tool as it is neither sensitive or specific enough to determine a definite cancer diagnosis and may be elevated because the prostate has simply become enlarged and is producing more PSA. It is also important to note that activities such as cycling and sexual activity can stimulate the prostate to produce more PSA, so important not to embrace such activity the night before an impending test.
• There has been a significant increase in the number of men diagnosed in recent years due to the increasing use of the PSA blood test together with a Digital Rectal Examination (DRE).
• Prostate cancer responds well to treatment and, if detected early, it can be treated successfully. When prostate cancer is detected early, over 93% of men have a really good five-year survival rate.
* If your father or brother has had prostate cancer, you are twice as likely to get prostate cancer at some point in your life.
We encourage men to take an active role in their health, and to speak to their GP if they have any concerns or worries about a change in their bodies. Prostate cancer is very treatable when caught early.
Prostate Cancer’s early warning signs (note that there may not be any) can include:
• frequency passing urine
• getting up a night-time to go to the toilet
• pain on passing urine,
• difficulty passing urine
• blood in your urine
• hesitancy when you go to the toilet
• urgency about getting to the toilet
• your flow has become weak or intermittent
Other factors to consider would be blood in the semen, back pain, unexplained tiredness and weight loss.
Know your risk factors too.
The risk of developing prostate cancer increases with:
• Age - men over 50 years
• Family history - You are two and a half times more likely to get prostate cancer if your father or brother had it.
• Inherited genes - BRCA gene mutation especially BRCA 2 and Lynch Syndrome
• Race - African Americans at greater risk
• Being overweight or obese
Written by Helen Forristal, Director of Nursing Services, Marie Keating Foundation
Having a risk factor doesn’t mean that you will definitely develop prostate cancer.
• If you have any of the discussed symptoms, visit your G.P.
• Tests your G.P. may do include: A blood test called a PSA test. Digital Rectal Examination (DRE) of your prostate
• Based on the results, your G.P. may refer you to one of the HSE 8 Rapid Access Prostate Clinics (RAPC) where you will be reviewed by a Specialist called a Urologist
• Urologist may repeat the above tests and may take a biopsy of your prostate gland – TRUS biopsy/Transperineal biopsy.
• Further tests may also be required and may include one or more of the following: MRI/ Multiparametric MRI (mpMRI)/ CT scan/Pet-CT scan
Osteoporosis
Factors to Consider in Osteoporosis
Written by Dr Kevin McCarroll, Consultant Physician, St James’s Hospital Dublin
Osteoporosis is common and affects an estimated 300,000 people in Ireland though the true prevalence is not known. While the diagnosis is commonly made using DXA (T score ≤ -2.5 at total hip, neck of femur or lumbar spine) patients who have had a fragility fracture of the hip or spine are also considered to have a clinical diagnosis of osteoporosis. Importantly, about 50% of fragility fractures occur in patients who have osteopenia (T score: -1.0 to > - 2.5). This is because while 70% of bone strength relates to bone mineral density (BMD), other factors collectively determining ‘bone quality’ are important. An important area of research is in developing ways of more accurately predicting fracture risk in such patients.
Factors to consider
Patients on steroids, aromatase inhibitors and androgen deprivation therapy are higher risk of fracture independent of BMD as are those with conditions such as diabetes and rheumatoid arthritis. A recent fracture (within 2 years) is also a big predictor of imminent fracture and needs to be considered when assessing fracture risk. Importantly, the majority (70%) of vertebral fractures do not present clinically but increase incident vertebral fracture risk by a factor of 2-5, so any previous x-ray imaging of the spine should be reviewed.
General management
Lifestyle factors (eg smoking, alcohol excess, dietary calcium intake and exercise) should all be addressed. Vitamin D levels should be maintained ≥ 50 nmol/l and attention paid to falls prevention. First line therapy for osteoporosis is usually oral bisphosphonates though zoledronic acid once yearly is an alternative when there are GI contraindications or in patients with more severe osteoporosis. Denosumab is the most potent antiresorptive but may be best reserved for patients with more severe osteoporosis or where there are contraindications to other therapies. In patients at very high risk of fracture (especially in the spine) anabolic therapy (teriparatide) should be considered.
Denosumab
Denosumab must not be stopped unless patients are switched to bisphosphonates due to rebound bone loss at both the spine and hip and increased vertebral fracture risk. However, follow up bisphosphonate treatment (including with zoledronic acid) may not be suffice in some patients to maintain a stable BMD. For this reason the decision to stop denosumab needs to be carefully considered and is generally not appropriate for patients with T
scores ≤ -2.5 or if higher risk of fracture. Lifelong treatment in older patients with a life expectancy of up 10 -15 years should be considered.
Teriparatide
Teriparatide is recombinant parathyroid hormone and is the only anabolic therapy available in Ireland. It reduces vertebral fracture risk by about 70-80% and should always be considered as a possible first line agent in patients with severe osteoporosis of the spine. For patients who sustain new vertebral fractures while on treatment with denosumab (despite therapy compliance and the absence of other causes), the addition of teriparatide should be considered. However, switching from denosumab to teriparatide is not generally recommended as it is associated with a transient decline in BMD at the spine and also hip
Drug holidays, when and for how long?
Drug holidays are only compatible with bisphosphonates due to their long half-life in bone. Oral bisphosphonates are typically used for 5 years and zoledronic acid for 3 years. Drug holidays may then be appropriate if T score > -2.5 (hip and spine), no recent fractures and low risk of future fracture. In older patients at high fracture risk (fallers, hip or recent fractures) or on drugs causing bone loss, therapy with alendronate can be continued for up to 10 years and for 6 years with zoledronic acid. Drug holidays are typically for 18-24 months with oral therapy and 2-3 years with zoledronic acid. Restarting osteoporosis treatment is usually appropriate if there is decline in BMD or rise in bone markers.
Atypical fractures
Atypical femoral fracture (AFF) is a rare and possible adverse effect of bisphosphonates (incidence of 1/1000 after 10 years of oral therapy) but when occurs treatment should be stopped (at least for a period). However, further optimal therapy is unclear. The incidence of AFF with denosumab is lower with the vast majority occurring in patients with prior bisphosphonate use.
Medication Related Osteonecrosis of the Jaw (MRONJ)
This is a rare in the treatment of osteoporosis but more common with potent antiresorptives (denosumab and zoledronic
acid). In the majority of cases, it is precipitated by dental surgery. Importantly, the incidence is highest with denosumab (up to 0.68% per dental procedure). When MRONJ occurs, bisphosphonates may be stopped, though this needs to balanced against risk of fracture. However, stopping denosumab may not be appropriate. For patients on denosumab and at higher risk of MRONJ, elective dental surgery 5-6 months after their last injection followed by re-administration within about 4 weeks has been advised. Decisions regarding osteoporosis treatment in patients with MRONJ should be made by an expert in osteoporosis.
Diabetic Retinopathy in Ireland
Diabetic retinopathy is a common complication of diabetes and occurs when high blood sugar levels damage the cells at the back of the eye, known as the retina. There are no current treatments that prevent the advancement of diabetic retinopathy from its early to late stages, beyond the careful management of diabetes itself. As a result, a significant proportion of people with diabetes still progress to the vision-threatening complications of the disease.
As the number of people with diabetes continues to increase globally, there is an urgent need for new treatment strategies, particularly those that target the early stages of the disease to prevent vision loss.
Diabetic retinopathy is the most common cause of blindness in working age individuals’ in Ireland, at the present time. It is estimated that there are approximately 190,000 people in Ireland with diabetes and 10 per cent of them are at risk of sight threatening retinopathy.
Diabetic RetinaScreen commenced its national population-based diabetic retinopathy screening programme at the end of February 2013 and this is being introduced on a phased basis to ensure quality and safety.
Diabetic RetinaScreen will deliver great benefits to men and women with diabetes in Ireland who are at risk of sight threatening retinopathy, enhancing quality of life and preserving sight for longer. Of the population screened and treated, it is expected that six per cent will be prevented from going blind within a year of treatment and 34 per cent within ten years of treatment.
The test looks for early warning signs of diabetic retinopathy, a complication of diabetes caused by high blood glucose (sugar) levels damaging the back of the eye (retina). If left undiagnosed and untreated diabetic retinopathy may lead to blindness. However, if diabetic eye disease is found early, treatment can reduce or prevent damage to your sight.
Diabetic RetinaScreen Programme Manager, Helen Kavanagh says, “If left undiagnosed and untreated diabetic retinopathy can deprive people of their sight, but it usually takes many years to reach that stage. This free eye screening test offers people with diabetes an opportunity to detect problems early, which can lead to more successful treatment and better outcomes. The longer you have diabetes the higher the risk, that’s why we’re encouraging everyone aged 12 years and older to be registered with Diabetic RetinaScreen today.”
Latest Research
Last year, researchers at Queen’s University in Belfast uncovered a key process that contributes to vision loss and blindness in those with diabetes.
The retina demands a high oxygen and nutrient supply to function properly. This is met by an elaborate network of blood vessels that maintain a constant flow of blood even during daily fluctuations in blood and eye pressure. The ability of the blood vessels to maintain blood flow at a steady level is called blood flow autoregulation. The disruption of this process is one of the earliest effects of diabetes in the retina.
The breakthrough made by researchers at Queen’s University Belfast pinpoints the cause of these early changes to the retina. The study, has discovered that the loss of blood flow autoregulation during diabetes is caused by the disruption of a protein called TRPV2. Furthermore, they show that disruption of blood flow autoregulation even in the absence of diabetes causes damage closely resembling that seen in diabetic retinopathy.
The research team are hopeful that these findings will be used to inform the development of new treatments that preserve vision in people with diabetes.
Professor Tim Curtis, Deputy Director at the Wellcome-Wolfson Institute for Experimental Medicine at Queen’s and corresponding author, explains, “We are excited about the new insights that this study provides, which explain how the retina is damaged during the early stages of diabetes.
“By identifying TRPV2 as a key protein involved in diabetesrelated vision loss, we have a new target and opportunity to develop treatments that halt the advancement of diabetic retinopathy.”
The study was funded by the Biotechnology and Biological Sciences Research Council and the Department for the Economy Postgraduate Studentship scheme. Diabetic retinopathy risk factors:
• Blood sugar levels
The control of blood sugar levels is of immense importance. Lower blood sugar levels can delay the onset and slow the progression of diabetic retinopathy
• Blood pressure
High blood pressure damages blood vessels, raising the chances for eye problems. Effective control of blood pressure reduces the risk of retinopathy progression and visual acuity deterioration
• Duration of diabetes
The risk of diabetic retinopathy developing or progressing increases over time. After 15 years, 80 per cent of Type 1 patients will have diabetic retinopathy. After 19 years, up to 84 per cent of patients with Type 2 diabetes will have diabetic retinopathy
• Blood lipid levels (cholesterol and triglycerides)
Elevated blood lipid levels can lead to greater accumulation of exudates, protein deposits that leak into the retina. This condition is associated with a higher risk of moderate visual loss
• Pregnancy
Women who have diabetes and become pregnant have an increased risk of developing retinopathy. If they already have diabetic retinopathy, it may progress
Symptoms
1. Gradually worsening vision
2. Sudden vision loss
3. Shapes floating in your field of vision (floaters)
4. Blurred or patchy vision
5. Eye pain or redness
Ireland ‘First’ in Cardiovascular Disease
Heart & Stroke Voice Ireland (HSVI), the newly launched patient and carer led alliance, addresses the unmet needs of patient centred care by championing patient engagement and involvement.
“We hope that policy makers will engage and consult with alliances such as Heart and Stroke Voice Ireland when developing any framework of care that accurately addresses the needs of both patients and caregivers, to ensure that the lived experience is at the centre of any policy changes”
The alliance, which operates under the auspices of Croí, heart and stroke charity, is calling for a ‘Patient First’ national cardiovascular disease (CVD) strategy, that is shaped by the lived experience of those living with CVD in Ireland. The alliance, the first of its kind in Ireland, has outlined three initial key areas of focus to support those experiencing CVD, which claims the lives of 9,000 individuals each year in Ireland and significantly impacts countless others.
This is despite an estimated 80% of premature CVD being preventable. The focus areas are:
• Early detection
• Timely diagnosis
• Equitable access to care
HSVI has voiced its willingness to engage with Government officials to collaboratively shape a framework of care that recognises the equal importance of prevention, early detection, timely treatment, and rehabilitation for those directly impacted by CVD. HSVI aims to ensure the patient voice is considered across research, education, and all aspects of CVD healthcare.
HSVI will provide a platform to develop the capacity and capability of the patient voice and to promote greater awareness and understanding of the need for equitable and timely access to quality treatment and care across the patient journey.
David Kelly, Chair of the Alliance said, “We are delighted to be here today to celebrate the
Women in Leadership
Pictured at the launch of Heart Stroke Voice Ireland is (left to right) Heidi Kingston, Neil Johnson, Chief Executive of Croí & Executive Director of Global Heart Hub. David Kelly, Chairperson of HSVI, Magda Daccord, CEO of FH Europe, and Mary Harney, former Minister for Health and Children.
Picture: Julien Behal
establishment of Heart and Stroke Voice Ireland, which marks a milestone in patientcentred care for cardiovascular disease in Ireland. The alliance is committed to ensuring that the first-hand experiences of both patients and carers are central to the development of a comprehensive framework of care that can drive meaningful change in the lives of those caring for and living with cardiovascular disease in Ireland. We believe that by repositioning the patient and carer experience to the centre of a national framework we can make a significant contribution to achieving equity in CVD care.”
Speaking at the launch, former Minister for Health and Children, Mary Harney added, “Today is significant for patients living with cardiovascular disease in Ireland. We hope that policy makers will engage and consult with alliances such as Heart and Stroke Voice Ireland when developing any framework of care that accurately addresses the needs of both patients and caregivers, to ensure that the lived experience is at the centre of any policy changes.
“Patient alliances for numerous diseases are common across Europe and play a vital role in providing a platform for the patient experience which informs policy making. The launch of Heart & Stroke Voice Ireland marks the first such patient alliance in the area of heart disease and stroke in Ireland and this is a very positive and welcome development.”
The Women in Leadership series from The Pharmaceutical Managers’ Institute for 2023 continues with Caroline Keeling, CEO with Keelings Fruit as the guest speaker. MC for this event will be Ingrid Walsh, Head of Foundation, General Medicines UK & Ireland and GM General Medicines Ireland with Sanofi.
The event takes place on Wednesday, September 20th, 2023 from 11.30-2pm in The Address, Old Naas Road, Citywest.
For further details please visit www.thepmi.com
Ireland’s most recent national CVD strategy expired in 2019 and has yet to be replaced, meaning there is currently no overall national approach, despite having the lowest rate of detection of high blood pressure in Western Europe.
A report by the National Institute for Prevention and Cardiovascular Health (NIPC) and the National CVD Prevention Council outlined that waiting times for diagnostic services, such as echo and angiography, can exceed a year in some public hospitals. The lack of a national strategy and waiting times reflect poorly when compared internationally. In the United Kingdom, the NHS Constitution outlines that patients have a ‘legal right to treatment within 18 weeks of referral and as part of this, pledges that patients should not be required to wait six weeks or more for a diagnostic test’.
In Ireland, only private hospitals meet this benchmark for diagnosis. A report published in February 2023 by the National Institute for Prevention and Cardiovascular Health and the National CVD Prevention Council, recommended a screening program for familial hypercholesterolaemia (FH), a genetic condition which causes dangerously high cholesterol levels from birth. FH affects around 1 in 200-250 people in Ireland however the majority of this goes undetected. Childhood FH screening programmes are commonplace throughout Europe. Research published by Croí in 2022 found that 80% of public hospitals do not offer GPs direct access to echocardiograms – an essential diagnostic test for heart patients, significantly increasing wait times for those seeking echocardiograms through the public system.
For more information on Heart and Stroke Voice Ireland, please visit www.heartandstrokevoice.ie
Number 1 Ranking for RCSI
RCSI University of Medicine and Health Sciences has ranked number one in the world for SDG3 ‘Good Health and Well-being’ in the Times Higher Education (THE) University Impact Rankings 2023.
The University Impact Rankings recognise universities around the world for their social and economic impact based on the United Nations’ 17 Sustainable Development Goals (SDGs).
Over 1,200 universities around the world participated in the SDG3 ranking, an increase of 600 since RCSI first achieved the number one position in 2020.
RCSI is Ireland’s only university solely focused on education, training and research in health sciences. As a signatory to the SDG Accord, RCSI is committed to achieving the SDGs through its education, research and university operations.
Critical initiatives over the past year, including the launch of a new School of Population Health, leading a programme to embed sustainability and climate health into Ireland’s medical curriculum and the university’s unique collaboration with the Colleges of Surgeons of East, Central and Southern Africa to address inequalities in surgical access demonstrate the university’s commitment to collaboration to achieve the UNSDGs.
Achieving net zero
Recognising the crucial link between human health and the health of the planet, RCSI has developed a road map to achieving net zero carbon by 2050 which encompasses its campus operations, education and training, research and a focus on leadership in sustainable healthcare.
This commitment is reflected in RCSI also gaining Beacon Status from the UK’s Centre for Sustainable Healthcare and being named the top-performing medical school in Ireland in the Planetary Health Report Card 2023 – a student-led initiative aimed at increasing planetary health awareness and accountability amongst international medical schools.
As a result of this, RCSI’s position in the overall Impact Ranking has also risen to 101-200 in the world.
First in Ulcerative Colitis Management
An international team of scientists led by Professor Marietta Iacucci has developed an artificial intelligence (AI) computer-aided diagnosis system that speeds up, simplifies, improves accuracy and minimises errors in evaluating and predicting outcomes of Ulcerative Colitis (UC).
Professor Marietta Iacucci
Professor Iacucci, an internationally renowned gastroenterologist and leading researcher in the field of AI and ‘endo-omics’ (that fuses endoscopic and histologic information with ‘multi-omics data), recently joined UCC and APC Microbiome Ireland (APC) – a world-leading SFI research centre based in University College Cork (UCC) as Clinical Investigator and Professor of Gastroenterology. In her new roles, Prof Iacucci will also be involved in research with other UCC based SFI centres IPIC/ Tyndall and INSIGHT.
This new AI based diagnostic system can change how clinicians evaluate biopsies with a faster, less expensive and objective assessment tool while being adaptable for a wider field of tissue applications in pathology worldwide. Ulcerative colitis (UC) is a common chronic inflammatory bowel disease (IBD) that induces inflammation and ulcers in the digestive tract. It can lead to a range of complications, ill health and suffering and has no known cure, although several treatments can help alleviate symptoms and reduce or eliminate inflammation. Clinical assessments use histopathology as the most effective means of detecting and identifying inflammation and remission. Traditional UC
assessment involving microscopic inflammation is typically complex, time and training intensive, expensive and subject to high interobserver variability.
Professor Iacucci commented, “This novel AI system can be of great help to pathologists and clinicians in identifying and distinguishing between inflammation and remission - the primary goal in UC treatment. It offers a faster, less expensive and more accurate evaluation methodology, and we believe is set to alter how UC clinical assessments and research trials are conducted.”
In their analysis, the team used a sample of 535 biopsies drawn from 273 patients spread across 11 different international centres - providing the benefit of a large sample size and helping to optimise data fit and suitability for the computer model. Between
Date for your Diary
The Irish Pharmacy Union National Pharmacy Conference takes place this year on Saturday, 21st October in Johnstown House Estate in Enfield, Co. Meath.
This event, plays a vital role in supporting pharmacists with CPD, covering a range of clinical and business topics.
66%-75% of the biopsies were in histologic remission. The AIbased CAD system was used to analyse and detect UC disease presence, predicting endoscopic inflammation at levels of 80% accuracy.
The tool’s key and innovative feature is its ability to stratify and predict disease flare risk – a crucial assessment in UC observationwhere it performed comparably to human pathologist assessments.
Subrata Ghosh, Chair and Head of Medicine, UCC and Deputy Director of APC said: “This AIbased CAD system provides a new tool that enables accurate identification of disease remission and provides accurate prognosis in UC management and treatment. We are excited about this development and believe it can radically change current clinical trial practice and help improve UC monitoring and prediction.”
This is the first face to face conference since 2019 and will also mark the start of the celebrations of the 50th Anniversary of the IPU. The event will provide support to the pharmacy profession through an extensive programme of events, education sessions and ‘The Great Debate’.
Irish Pharmacy AwardsThe Best of Pharmacy Awards
Over 650 pharmacy and industry professionals were in attendance as winners across 14 categories were announced at the annual Irish Pharmacy Awards.
Each year Irish Pharmacy News, Ireland’s only independent monthly publication for community pharmacy, celebrates and acknowledges the achievements of teams and individuals within the pharmacy profession.
The twelfth annual Irish Pharmacy Awards took place on Saturday, May 27th 2023. Hosted by Marty Whelan, the awards ceremony took place in the Clayton Hotel, Burlington Road, Dublin.
The Irish Pharmacy Awards recognise the achievements of individuals and teams working in the community pharmacy sector; their dedication and innovation which positions the profession at the forefront of healthcare, improving the lives of people across the country.
Pictured are some of those who attended.
1. Karen Kane and Kevin Kane, Brandon Ltd 2. Laura Grifton, Kate O’Connell and Amy Cullen from Thea Pharma 3. Pippa Beeley and team from The Pharmacy Store 4. Sarah Smith, Claire Healy, and Ellen Kavanagh from Rye Pharmacy 5. Amy Rossader, Helen Shields, Andrea Murphy, and Paula Morris from Pharmed 6. Natasha Gleeson, Paul Kennedy, and Sarah Leadbetter, Fleming Medical
1. Gary O’Brien, Sam Farag, Simon Racklyeft, and Keith Mullins, TouchStore 2. Reilly Derek and Marin Lara, Irish Pharmacy Union 3. The team from McCartans Pharmacy 4. Maria Barrett, Samantha Lennon, Whites Pharmacy and Orlagh Brennan, Alliance 5. The team from Théa Pharma 6. Sheelagh O’Neill and Dee O’Dwyer, Doctor Greene
1. The team from MedPharm 2. Fergus and Joyce McCauley, IQVIA 3. The pharmacy teams from Bradlong, Carlingford and Drogheda with Cottage Pharmacy 4. AnnaLeigh Hanlon and Angela Hanlon, Foynes Pharmacy 5. Ciara and Pippa Beeley from Daarwood Pharmacy with guest
6. Robin Hanna and Tim O’Brien, McLernons with Conn Loy, iOResource
1. The Pharmacy team from Dunville Pharmacy 2. The pharmacy team from North Long Pharmacy 3. The pharmacy team from Adrian Dunne Pharmacy Group 4. Caroline Finucane and Eimear Kinsella, Ocean Healthcare 5. Ciara Lai and Jenny Gallagher, People’s Pharmacist Finalist, Murphy’s Pharmacy
6. The pharmacy team from Stacks Pharmacy Group
The impact of lidocaine plaster prescribing reduction strategies: A comparison of two national health services in Europe
Written
by Molly Mattsson1, Fiona Boland2, Ciara Kirke3, Michelle Flood1, Emma Wallace4, Mary E. Walsh5, Derek Corrigan6, Tom Fahey7, Richard Croker8, Sebastian C. J. Bacon8, Peter Inglesby8, David Evans8, Ben Goldacre8, Brian MacKenna8, Frank Moriarty1
1School of Pharmacy and Biomolecular Sciences, Royal College of Surgeons in Ireland (RCSI) University of Medicine and Health Sciences, Dublin, Ireland
2Data Science Centre, RCSI University of Medicine and Health Sciences, Dublin, Ireland
3National Medication Safety Programme, HSE National Quality and Patient Safety Directorate, Dublin, Ireland
4Department of General Practice, University College Cork, Cork, Ireland
5School of Public Health, Physiotherapy and Sports Science, University College Dublin, Dublin, Ireland
6FutureNeuro Research Centre (eHealth Group), RCSI University of Medicine and Health Sciences, Dublin, Ireland
7Department of General Practice, RCSI University of Medicine and Health Sciences, Dublin, Ireland
8Bennett Institute for Applied Data Science, Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
What is already known about this subject
• Prescribing reduction measures targeting lidocaine medicated plasters were introduced in both Ireland and England in 2017.
• In Ireland, restrictions on reimbursement were introduced, with the annual expenditure on lidocaine plasters decreasing from ¤27 million in 2016 to just over ¤2 million in 2018.
• In England, guidance was introduced on items which should not routinely be prescribed in primary care. What this study adds
• There were vastly different effects of the introduction of reimbursement restrictions in Ireland and guidelines in England.
• Following the change to reimbursement in Ireland, a 97.3% reduction in the dispensing rate occurred.
• However, this was in the context of a much higher baseline rate of use in Ireland compared to England, which remained higher even after the substantial reduction in dispensing.
Introduction:
Due to limited resources compared with demand, all healthcare systems are required to employ mechanisms to prioritize finite resources in order to maximize health benefits.1 One integral part of healthcare delivery is the provision of medicines, which accounts for a significant proportion of overall health expenditure in most countries. In 2019, spending on retail pharmaceuticals (excluding those used during hospital treatment) accounted for one-sixth of overall healthcare expenditure in Organisation for Economic Co-operation and Development (OECD) countries and represented the third largest component of health spending after inpatient and outpatient care.2
Rational use of medicines may be defined as “patients receiving medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate
period of time, and at the lowest cost to them and their community”.3 In contrast, irrational use of medicines is a problem worldwide, with the World Health Organization (WHO) estimating that more than half of all medicines are prescribed, dispensed or sold inappropriately, and that half of all patients fail to take them correctly.4 Low-value care—the use of health services whose harms or costs exceed their benefits—is also a significant issue that contributes to wasted healthcare resources.5 Various strategies exist to promote rational prescribing, aimed at both patients and prescribers, and ensure safe, effective, and cost-effective medicines use. These strategies can be grouped broadly as targeted or systemoriented approaches, with targeted approaches comprising educational and managerial interventions and system-oriented strategies including regulatory and economic interventions.6
Both the National Health Service (NHS) in England and the Health Service Executive (HSE) in Ireland identified prescribing of lidocaine 5% medicated plasters (Versatis®) as a target for prescribing reduction measures. This medicinal product’s licensed indication is for the treatment of post-herpetic neuralgia (PHN) only. However, it had been prescribed and dispensed in volumes exceeding the likely prevalence of PHN, indicating off-label use. In Ireland, the Medicines Management Programme (MMP) was established in 2013, with the aim to provide sustained national leadership relating to issues such as the quality of the medicines management process, access to medicines and overall expenditure on medicines.7 In March 2017, the MMP published a Prescribing and Cost Guidance document on lidocaine 5% medicated plasters.8 Following publication of these guidelines, the HSE introduced
changes to the reimbursement of lidocaine plasters, introduced in two stages. From 1 September 2017 prescribers were required to apply through an online reimbursement applications system for all new patients, indicating the antiviral that was prescribed for the herpes zoster infection, and the date it was prescribed. From 1 December 2017 this was extended to pre-existing patients in receipt of the medication prior to September 2017. These guidelines additionally outlined suggested alternatives to lidocaine plasters, including capsaicin for PHN and diabetic neuropathic pain and topical non-steroidal antiinflammatory drugs (NSAIDs) for muscular and rheumatic pain. Similarly, in March 2017, NHS England announced a programme to tackle “low value medicines”,9 which subsequently became guidance on items which should not routinely be prescribed in primary care. This included
lidocaine plasters, which were classified as “an item of low clinical effectiveness, where there is a lack of robust evidence of clinical effectiveness or there are significant safety concerns”.10 This guidance advised that prescribers in primary care should not initiate lidocaine plasters for any new patients (unless patients have been treated in line with National Institute for Health and Care Excellence [NICE] CG173 “Neuropathic pain in adults: pharmacological management in non-specialist settings”, but are still experiencing PHN), that prescribers should be supported in deprescribing lidocaine plasters in all patients, and that if there is a clinical need for lidocaine plasters to be prescribed in primary care, this should be undertaken in a cooperation arrangement with a multi-disciplinary team.10
This study aims to describe and compare how the policy and guidance changes have impacted prescribing of lidocaine plasters in the two countries.
Methods
We conducted an interrupted time-series study using segmented regression analysis to assess the change in prescribing rate following the introduction of guidance and policy changes. Interrupted time-series studies of policy interventions can be analysed using segmented regression, allowing for the change in level and trend of an outcome following an intervention to be evaluated.11 The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines are used in reporting this study.12 This study was approved by the RCSI University of Medicine and Health Sciences Human Research Ethics Committee (REC202201015).
Health Service Executive data (Ireland)
The Primary Care Reimbursement Service (PCRS) is the section within the HSE which administers community drug schemes in Ireland, including the GMS scheme. Eligibility for the GMS scheme is means tested and covers approximately 32% of the population, and therefore eligible persons tend to be more socioeconomically deprived than the general population.13, 14 For adults aged ≥70 years, the scheme covers the vast majority of individuals. Pharmacies transmit claims for prescribed medications which were dispensed to individuals eligible for community drug schemes to the PCRS at the end of each month for reimbursement, and the
data therefore provides complete information on prescribed medications that are dispensed to eligible people. As data are not publicly available, a request was submitted to the PCRS in line with their information requests policy, to obtain data aggregated at local health office (LHO) level. The data contains drug information (WHO Anatomical Therapeutic Chemical [ATC] code, strength, defined daily dosage [DDD], and product information), quantity dispensed, month of dispensing and cost.
National Health Service data (England)
The NHS openly publishes GP prescribing data every month, which is available on the OpenPrescribing.net platform, which provides monthly statistics of prescribing aggregated at the level of GP practices for all practices in England.15 The data relate to NHS prescriptions issued by general practices in England (by any practice prescribing staff) and dispensed in any community pharmacy in the UK. Prescribed products are coded based on their British National Formulary (BNF) classification. The monthly prescribing datasets contain one row for each different medication and dose in each prescribing organization in NHS primary care in England, describing the number of items and the total cost. The items variable within the data corresponds to the number of items of each prescribed product that was dispensed in the specified month. This provides comparable rates to the “number of prescription dispensings” indicator as defined in the PCRS data. The data is available at practice level and was aggregated to clinical commissioning group (CCG) level, an NHS administrative region, to allow for equivalent analysis to the PCRS data.
Analysis
Firstly, descriptive statistics were used to summarize dispensings, quantity and costs of lidocaine plasters on a monthly basis in the two countries. We also summarized dispensings of alternatives recommended by the HSE MMP using HSE data.8 These were plotted to allow visual inspection of trends in outcomes in relation to the policy and guideline changes. A segmented regression model was fitted separately on the HSE and NHS data to assess the change in prescribing rates following the intervention affecting lidocaine plasters in each country (i.e., introduction of reimbursement changes/guidelines).
We parameterized each segmented regression model to estimate four elements:
• (i)the rate at the beginning of the study period (i.e., the model intercept),
• (ii)the trend prior to the intervention,
• (iii)immediate change in rate from pre to post intervention, and
• (iv)change in trend over time from pre to post intervention. The analysis included monthly data from 2015 to 2019, allowing for well in excess of the recommended 12 time points before and after an interruption. As Ireland introduced the intervention in stages, with the reimbursement application initially required for only patients newly initiating lidocaine plasters (1 September 2017, intervention 1) before being extended to all patients (1 December 2017, intervention 2), the effects of both interventions
were included. For England, August 2017 was considered the first post-intervention month, as the guidance was first published in July 2017 as part of a consultation. Analyses were conducted using Stata version 17, and statistical significance was assumed at P < .05. For the time-series analysis, the XTITSA command was used, which allows for analysis of panel data at LHO/ CCG level.16
Results
Lidocaine plasters
In Ireland, there were 193 486 individual dispensings for lidocaine plasters in 2015, reducing to 21 886 in 2019. The GMS expenditure similarly decreased during the study period, peaking at ¤27.4 million in 2016 compared to ¤2.7 million in 2019. In England, a slight reduction in dispensings was noted during the study period, with dispensings peaking at 258574 in 2017, and decreasing to 219 177 in 2019. Costs decreased from £19 428 950 in 2017 to £16 211 567 in 2019. Table 1 outlines the yearby-year dispensings, quantity and costs for lidocaine plasters for Ireland and England. Ireland had higher rates of dispensings compared to England throughout the study period. In Ireland, the rate per 1000 eligible GMS population was 8.15 dispensings in January 2015, 15.22 in August 2017, and 1.15 in December 2019. In England, the mean rate per 1000 NHS population was 0.28 dispensings in January 2015, 0.36 in July 2017, and 0.30 in December 2019. See Table 2 and Figure 1 for dispensing rates per 1000 eligible population for Ireland and England.
TABLE 1. Year-by-year dispensings, quantity and costs for lidocaine plasters by country
TABLE 1. Year-by-year dispensings, quantity and costs for lidocaine plasters by country.
Lidocaine 5% medicated plasters
Impact of policy and guidance changes
Interrupted time-series regression results for Ireland and England are outlined in Table 3. For Ireland, the dispensing rate per 1000 GMS eligible population was estimated at 8.59 in January 2015, and appeared to increase monthly prior to September 2017, by 0.23 on average. In the first month post intervention 1, there appeared to be a statistically significant decrease in the level of 5.54 (i.e., change in rate from August 2017 to September 2017), followed by a statistically significant average decrease in the monthly trend, relative to the pre-intervention trend, of 1.93 per month. At the second intervention point (December 2017) there was an immediate significant decrease in rate of dispensings of 4.48 (i.e., November 2017 to December 2017). After intervention 1 there was a decreasing monthly trend of 1.7; however, from December 2017, after intervention 2, there was evidence of a 0.02 monthly increase in trend. Overall, there was a decrease of 15.14 (95% confidence interval [CI] 14.76–15.53) in the rate per 1000 GMS eligible population between August (month prior to first intervention) and December 2017 (month following the second intervention), with the trend from December 2017 (post interventions) 0.2 (95% CI 0.18–0.23) lower than that prior to any interventions. This equates to a 97.3% (95% CI 94.8–99.8) reduction in the dispensing rate post relative to pre intervention.
In England, the dispensings rate per 1000 NHS population was estimated at 0.36 in January 2015 and appeared to increase every month prior to August 2017 by 0.0032. In the first month post intervention (August 2017), there was a statistically significant decrease in the level of 0.0251, equating to a 5.8% (95% CI 3.3–8.4) reduction in the dispensing rate post- relative to pre-intervention. This was followed by a statistically significant decrease in the monthly trend relative to the pre-intervention trend of 0.0057 per month. The estimated trend after the intervention decreased monthly at a rate of 0.0026. Figure 2 provides a visual representation of the time-series analysis.
Lidocaine 5% medicated plasters
Ireland
For the quantity of lidocaine plasters, similar results as for the dispensings were found for both Ireland and England (Tables S1 and S2). In Ireland, an overall decrease of 472.45 (95% CI 459.31–485.58) in the rate per 1000 GMS eligible population was seen between September and December 2017, with the trend from December 6.15 (95% CI 5.31–6.98) lower than that preSeptember. In England, August 2017 saw a level change of 0.62 (95% CI 0.94 to 0.3), followed by a trend change of 0.17 (95% CI 0.19 to 0.15) compared to the pre-intervention trend. Similar changes in the cost of lidocaine plaster dispensing were found (Tables S3 and S4).
Topical alternatives in Ireland
For the topical alternatives recommended as part of the intervention in Ireland, the overall level change in the rate of capsaicin dispensings per 1000 GMS eligible population between September and December 2017 was 0.40 (95% CI 0.37 to 0.44), with the trend from December 0.02 (95% CI 0.022 to 0.018) lower than that pre-September. For topical NSAIDs, the overall level change in the rate per 1000 GMS eligible population between September and December 2017 was 0.61 (95% CI 0.24–0.98), with the trend from December 0.03 (95% CI 0.01–0.06) higher than that pre-September. No significant change in level or trend was observed for topical diclofenac specifically following the intervention. Figures S1–S3 provide a visual representation of the time-series analysis.
Discussion
The findings of this study highlight the vastly different effects of the introduction of reimbursement
restrictions in Ireland and guidelines in England. However, this is in the context of a much higher baseline rate of use in Ireland compared to England. In Ireland, the dispensing rate prior to the intervention was over 15 per 1000 GMS population. The change to reimbursement had a dramatic effect on lidocaine use, with a 97.3% reduction in the dispensing rate of lidocaine medicated plasters post-intervention compared to before. In England, only a small decrease of 5.8% was seen after the guidance changes; however, the dispensing rate prior to the intervention never went above 0.5 per 1000 population. In terms of the recommended alternatives, advice accompanying the reimbursement change in Ireland may have influenced topical capsaicin use in the immediate term; however, this quickly reduced.
The substantial difference in effect may be attributable to the difference in baseline rates, which may indicate that in England, lidocaine prescribing was already at a largely appropriate level prior to the introduction of the guidelines, whereas in Ireland lidocaine may have been overprescribed. Secondly, this could be attributable to the different types of intervention, i.e., a restriction on reimbursement requiring an individual application for a patient to continue to be covered for it (or alternatively paying out-of-pocket which for many patients is likely unaffordable), versus guidance on low-value care without any stringent restrictions, penalties or incentives. A previous systematic review on the effect of formulary restrictions on drug and healthcare resource utilization and economic outcomes, as well as patient outcomes, found that more than 90% of the included
studies showed lower drug utilization after introduction of reimbursement changes. However, when considering all outcomes, around half were negative in direction or unfavourable, compared to around 40% that were positive in direction or favourable, which shows that these types of interventions may have unintended consequences despite lower drug utilization and medication cost savings.17 In this case, the restrictive policy in Ireland may have delayed or prevented patients in pain accessing lidocaine plasters, potentially resulting in initiation or intensification of other alternative treatments, such as gabapentinoids, opioids or NSAIDs. As only aggregate data were analysed for this study, it was not possible to assess the impact of the interventions on individual patients, including switching behaviours and utilization of other types of analgesia. While lidocaine patches are expensive and the evidence for efficacy beyond specific uses is limited, this is based on average treatment effects and so some patients may have experienced a benefit from them.18 Furthermore, they are a low-risk option compared to alternatives. As we have not been able to examine the clinical impact of either policy on patient outcomes, we consequently make no comment on the appropriateness of either English or Irish policy, and believe that further research is warranted. The authors will investigate these issues further in a separate study.19 Low-value care and treatments have been receiving increased attention in recent years, and there has been a rapid growth in studies of interventions that target low-value care. A systematic review of measures
TABLE 2. Year-by-year rates of lidocaine plaster dispensings by country
TABLE 2. Year-by-year rates of lidocaine plaster dispensings by country
A Solution for Every Stage of the Wound Healing Process
A soft silicone foam dressing for moderate to highly exuding wounds, ulcers, second degree burns and traumatic wounds.
Meditull paraffin gauze dressing consists of a leno-weave fabric of 100% absorbent cotton thread, impregnated with white soft paraffin and is used as a primary wound contact layer.
A soft silicone foam dressing for moderate to highly exuding wounds, ulcers, second degree burns and traumatic wounds.
Breathable, transparent dressings suitable for light to moderately exuding wounds.
Available in a thin film, with a dressing pad, and with a wound mapping grid.
used to assess the impact of interventions to reduce low-value care found that most published studies (68%) focused on reductions in utilization rather than on potentially more clinically meaningful measures, such as improvements in appropriateness or patient outcomes.20 In England, research on the trends and variation in prescribing of these low-priority treatments prior to the introduction of the guidelines found that prescribing was extensive but varied widely by treatment, geographic area and individual practice, with the proportion of patients aged ≥65 year at practice level, as well as CCG, strongly associated with low-value prescribing.21
An evaluation of the NHS guidance on items which should not routinely be prescribed in primary care has shown that although there was a reduction in overall use of the targeted medications, that reduction was in line with the existing downward trend, with no change either after the announcement of the consultation on the scheme (July 2017) or publication of the subsequent consultation report (November 2017).22 Previous research on the implementation of new antibiotic prescribing guidelines for urinary tract infection in NHS England primary care suggests that the variation between CCG may be substantial, and that there is strong evidence suggesting that CCGs with minimal prescribing change following the introduction of new guidance did less to implement changes compared to CCGs that saw positive change.23 In Ireland,
recent research has shown that subsequent to the change in reimbursement, the prescribing of lidocaine plasters significantly decreased, with the annual GMS expenditure on lidocaine plasters decreasing from ¤27 million in 2016 to just over ¤2 million in 2018.24
Considering implementation of guidance as an intervention, a systematic review of the evidence to practice gap for complex interventions in primary care found that success is influenced by factors related to the external context (e.g. policies and infrastructure), organization (e.g. culture and resources), individual (e.g. competency) and intervention (e.g. evidence of benefit and ease of use).25
A recent scoping review of strategies for de-implementation of low-value care found that with a few exceptions similar strategies are used for de-implementation and implementation.26
One explanation for the substantial difference in prescribing rates between the two countries may be the difference in study populations and access to healthcare. While the NHS data include all prescriptions dispensed nationally, the HSE data are restricted to individuals eligible for the means-tested GMS scheme, where there is an overrepresentation of older adults, and people of lower socioeconomic status, both of which groups experience higher prevalence of chronic pain. Prevalence of pain in older adults has been widely estimated at between 25% and 75%.27, 28 Similarly,
rather than data on prescriptions which may not be dispensed. The use of real prescribing and dispensing data sourced from pharmacy claims minimizes the potential for obtaining a biased sample, and additionally eliminates the possibility of recall bias. The study does, however, have some limitations. While the English NHS data include prescriptions issued to the whole population, the GMS scheme in Ireland is means tested and therefore represents an older and lower socioeconomic subset of the Irish population. Additionally, the use of aggregate-level data means that we were not able to examine whether increases in recommended alternatives (i.e., capsaicin) was actually among people who switched from lidocaine plasters. It also limits the ability to examine unintended consequences of the interventions, i.e., switching of patients to potentially riskier therapies, such as opioids.
multiple population studies have shown that the prevalence of chronic pain is inversely related to socioeconomic status, and that those who are socioeconomically deprived are also more likely to experience more severe pain and a greater level of pain-related disability.29, 30 It is likely given the scale of use that lidocaine was prescribed off licence in Ireland for GMS patients with other types of pain, including muscular and rheumatic, as well as different types of neuropathic pain, rather than the limited indication of PHN. GMS patients are less likely to have private health insurance and are largely dependent on the public healthcare system, and consequently the long waiting lists for these patients in accessing non-pharmacological therapies, such as physical and psychological therapies as well as specialist pain clinics and surgery clinics, may influence prescribing practices. The large difference in baseline rates may also have impacted on the implementation of the interventions. Although the appropriate rate of prescribing is unknown, it is likely that the scale of off-label or inappropriate use in Ireland was far greater than in England, with a much greater scope for reductions in prescribing. It is possible that had the scale of off-label lidocaine prescribing been similar in England, the introduction of the guidance may have had a more substantial effect.
A strength of this study is the use of robust pharmacy dispensing data, as the data in both countries reflect dispensed prescriptions,
More broadly, this study highlights the importance of open data. The NHS has published publicly available GP prescribing data every month since 2011 for anyone to interrogate. This has supported a rich ecosystem of teams both inside and outside the NHS using differing tools and approaches to monitor data and give feedback to GPs to improve prescribing. Analysis conducted on this NHS open data has also supported original research on a substantial range of prescribing topics,21, 23, 31-34 and data feedback to GPs has been shown to improve prescribing.35-38 We strongly recommend that the HSE advances plans to publish similar data for GP prescribing in Ireland in line with national open data polices.39 This can support a similarly rich ecosystem of feedback to clinicians in Ireland and additionally our paper has demonstrated that by harnessing data from multiple countries we can do innovative research into real-world healthcare policy programmes.
Conclusion
Our study has shown the effects of two different interventions aiming to decrease low-value prescribing and has demonstrated a more substantial reduction in prescribing in a high prescribing setting in Ireland where a patient approval system was introduced, compared to issuing guidance in England in a lower prescribing setting. More research on the effects of these interventions beyond prescribing rates and expenditure, including impact on patient outcomes, is warranted. References available on request
Topic Team Training – Vitamin D
A community pharmacy environment that fosters teamwork ensured high levels of consumer satisfaction. This series of articles is designed for you to use as guide to assist your team in focusing on meeting ongoing CPD targets and to identify any training needs in order to keep the knowledge and skills of you and your team up to date.
The below information, considerations and checklist provides support to enable you to run a team training session and identify opportunities for learning within the topic of Vitamin D. Vitamin D, or ‘calciferol’, is a fat-soluble vitamin essential for musculoskeletal health by promoting the regulation of calcium and phosphorus (Nice, 2021). It circulates in the blood as Vitamin D3 and Vitamin D2. Vitamin D3 is synthesised in the skin through exposure to sunlight. Vitamin D3 and Vitamin D2 can also be obtained from food sources, fortified foods, and supplements (SACN, 2016). Adverse health outcomes associated with lack of vitamin D include autoimmune disorders, diabetes, cardiovascular issues, cancer, cognitive impairment, as well as poor bone health (Engleman, 2011). Media coverage of the widespread benefits of vitamin D, alongside more recent reports of links with COVID-19 and vitamin D deficiency, have led
Consider:
to increased interest in vitamin D testing and use of supplements. How much Vitamin D do we require?
The amount of vitamin D required varies by age, health status, sun exposure, and skin colour, depending on how much is likely to be absorbed through sunlight or diet, or because of health conditions. The recommended level of vitamin D for children over 4 years and adults under 65 years is 10 micrograms per day. While this is usually successfully obtained though sunlight and diet, some groups may require supplementation, either through a specific vitamin D supplement or a general multivitamin. Certain groups of people are advised to take vitamin D supplements, and while the guidance varies by country, the Irish Department of Health recommend the following:
• Breast-fed babies should be given 5 micrograms of vitamin D as a supplement every day from birth to 12 months
Am I, my team, trained in vitamin D supplementation to boost the number of people accessing the pharmacy for advice?
Are the team trained in the benefits and risks associated with vitamin D supplementation?
Does my team know how much vitamin D is required for individuals?
Am I and my team educated the medications which impact on vitamin D levels?
• Formula-fed babies should not have a vitamin D supplement unless they take less than 300ml of infant formula per day
• Children from the age of 1 year to 4 years need a vitamin D supplement every day for a few months each year – from Halloween (31st October) to St Patrick’s Day (17th March), they should be given 5 micrograms of vitamin D every day
• Adults aged 65 and older should take a vitamin D supplement of 15 micrograms every day at all times of year.
There are groups of people who may be absorbing insufficient levels of vitamin D through
Key Points:
Check your pharmacy team are aware and understand the following key points:
What vitamin D is
The recommended levels for babies, children and adults
The signs and symptoms of vitamin D deficiency
The impact on those who may be vitamin D deficient
Those who should be advised not to take vitamin D supplements
Up to date advice for appropriate and healthy diet
poor diet, health conditions, or inadequate sunlight exposure. According to the HSE, studies show that adults and children in Ireland have insufficient levels of vitamin D. A lack of vitamin D in children can lead to bone deformities such as rickets. In adults, not enough vitamin D can cause a condition called osteaomalacia.
Those at risk of insufficient levels and who should take a vitamin D supplement include:
• People who are not often outdoors
• Those living in residential institutions, such as care homes
• People who wear clothes that cover all of their skin when they are outside
• Those who have a dark skin tone.
Those who are obese or who have certain medical conditions may also be at risk from low vitamin D. Certain diets, for instance vegan, may also result in less intake of foods that are fortified with vitamin D. Potential symptoms of vitamin D deficiency include bone pain, muscle weakness, and bone fractures.
Actions:
Include POS with the wider vitamins, minerals and supplements market
Ensure efficient sign posting to further help and advice or reputable sources for vitamins and supplements
Keep products merchandised together, along with related products to help build sales
Ensure that this important category is fully stocked at all times and merchandising plans are amended based on seasonal times of year
Ensure that I know the recommendations for each vitamin and supplement and the OTC medicines which may cause vitamin D deficiency
Train the team to meet all the above considerations
62 Clinical Profiles
CLONMEL HEALTHCARE LAUNCH HUKYNDRA® (ADALIMUMAB) WITH BVB MEDICINE STATUS1
Clonmel Healthcare are delighted to announce the introduction of Hukyndra®, the new Adalimumab biosimilar.
Hukyndra® is approved for the same therapeutic areas and 15 indications as the reference product*2, 3
Rheumatoid arthritis
Chron's Disease
Juvenile idiopathic arthritis
Paediatric Chron's Disease
Axial spondyloarthritis
Ulcerative Colitis
Psoriatic arthritis
Paediatric Ulcerative Colitis
Psoriasis
Uveitis
Paediatric plaque psoriasis
Paediatric Uveitis
Hidradenitis suppurativa (HS)
Hukyndra® is a citrate-free, concentrated formula available in 2 presentations:
Hukyndra® 40mg / 0.4ml solution for injection in pre-filled pen x 2
Hukyndra® 40mg / 0.4ml solution for injection in pre-filled syringe x 2
The Hukyndra pre-filled pen is custom designed for optimal patient convenience, with a soft rubber grip and hidden pen needle. The Hukyndra pre-filled syringe is specifically designed for easy handling with improved grip and thinner needle.
Hukyndra® has also been recommended by the HSE Medicines Management Programme as a best-value biological (BVB) Medicine for Adalimumab.
The launch of Hukyndra® adds a second biosimilar in the field of rheumatology to the Clonmel Healthcare portfolio, alongside Movymia (Teriparatide), which has also been recommended as a Best Value Medicine for Teriparatide on the High-Tech Arrangement.4
Donagh O’Leary, Director of Marketing / Biosimilars Division said “Clonmel Healthcare continues to grow and strengthen its portfolio of Biosimilar medicines, which now spans several therapeutic areas including rheumatology, gastroenterology dermatology and oncology. We remain steadfastly committed to bringing a comprehensive range of
Biosimilar medicines to the market, increasing access for patients, physicians and pharmacists to affordable medicines. We are delighted in doing so to contribute to the ongoing savings to the Irish Healthcare system, as well as supporting patient needs.”
1 Best Value Biological Medicines https:// www.hse.ie/eng/about/who/cspd/ ncps/medicines-management/bestvalue-medicines/best-value-biologicalmedicines/ Accessed June 2023.
*Humira®**Without radiographic evidence of ankylosing spondylitis
2 Hukyndra® SmPC (Jan. 2022).
3 Humira® SmPC (Sep. 2021).
4 Best Value Medicines https://www. hse.ie/eng/about/who/cspd/ncps/ medicines-management/best-valuemedicines/teriparatide/ Accessed February 2023.
ABBREVIATED PRESCRIBING INFORMATION
Hukyndra 40 mg solution for injection in prefilled syringe. One 0.4 ml single dose prefilled syringe contains 40 mg adalimumab. Hukyndra 40 mg solution for injection in prefilled pen. One 0.4 ml single dose pre-filled pen contains 40 mg adalimumab.
Method of administration: Hukyndra is administered by subcutaneous injection. Full instructions for use are provided in the package leaflet. Hukyndra is only available as 40 mg pre-filled syringe and as 40 mg pre-filled pen. Thus, it is not possible to administer Hukyndra to patients that require less than a full 40 mg dose. If an alternate dose is required, other adalimumab products offering such an option should be used.
Contraindications: Hypersensitivity to the active substance or to any of the excipients. Active tuberculosis or other severe infections such as sepsis, and opportunistic infections. Moderate to severe heart failure (NYHA class III/IV).
Warnings and precautions: Infections (Serious infections, Tuberculosis, Other opportunistic infections), Hepatitis B reactivation, Neurological events, Allergic reactions, Immunosuppression, Malignancies and lymphoproliferative disorders, Haematologic reactions, Vaccinations, Congestive heart failure, Autoimmune processes, Concurrent administration of biologic DMARDS or TNF-antagonists, Surgery, Small bowel obstruction, Elderly and Paediatric population
Interactions: Refer to Summary of Product Characteristics.
Fertility, pregnancy and lactation: Women of childbearing potential should consider the use of adequate contraception to prevent pregnancy and continue its use for at least five months after the last Hukyndra treatment. Hukyndra should only be used during pregnancy if clearly needed. Hukyndra can be used during breast-feeding.
Driving and operation of machinery: Hukyndra may have a minor influence on the ability to drive and use machines. Vertigo and visual impairment may occur following administration of Hukyndra.
Undesirable effects: Very common: Respiratory tract infections (including lower and upper respiratory tract infection, pneumonia, sinusitis, pharyngitis, nasopharyngitis and pneumonia herpes viral), Leukopenia (including neutropenia and agranulocytosis), Anaemia, Lipids increased, Headache, Abdominal pain, Nausea and vomiting, Elevated liver enzymes, Rash (including exfoliative rash), Musculoskeletal pain, Injection site reaction (including injection site erythema). Refer to the product SmPC for full prescribing information. A copy of the SmPC is available upon request or go to www.clonmelhealthcare.ie
Pack size: Hukyndra 40 mg solution for injection in pre-filled syringe - 2 pre-filled syringes + 2 alcohol pads, Hukyndra 40 mg solution for injection in pre-filled pen - 2 pre-filled pens + 2 alcohol pads. Marketing authorisation holder: STADA Arzneimittel AG, Stadastrasse 2-18, 61118 Bad Vilbel, Germany. Marketing authorisation numbers: EU/1/21/1589/002, EU/1/21/1589/005. Distributed by Clonmel Healthcare Ltd. Medicinal product subject to medical prescription. Date last revised: December 2021. 2023/ADV/HUK/058H
DATA SHOW NEARLY 19% WEIGHT LOSS IN PEOPLE WITH OVERWEIGHT OR OBESITY IN BOEHRINGER INGELHEIM AND ZEALAND PHARMA PHASE II TRIAL WITH SURVODUTIDE (BI 456906) VS PLACEBO
Boehringer Ingelheim and Zealand Pharma A/S (Nasdaq: ZEAL) today announced additional data demonstrating superior efficacy with survodutide (also known as BI 456906) versus placebo in people with overweight or obesity without type 2 diabetes after 46 weeks of treatment. The findings were presented at the 2023 American Diabetes Association’s 83rd Scientific Sessions in San Diego, CA, U.S.
The primary endpoint was percentage bodyweight change from baseline to week 46. The Phase II study included two analyses: planned (assigned dose at randomisation) and actual (dose at the end of treatment).
People who completed the study on the 4.8 mg dose (actual treatment analysis) achieved nearly 19% weight loss (95% CI; p<0.01) versus just over 2% for those on placebo. As previously announced, the planned treatment analysis demonstrated nearly 15% weight loss for all those randomised to the 4.8 mg dose, versus 2.8% for those receiving placebo. Bodyweight reductions with survodutide had not reached a plateau at week 46, suggesting additional weight loss could be achieved with longer treatment duration.
“Given the prevalence of obesity and its many disease-related complications, there is a dire need for treatments that can help treat the disease of obesity effectively,” said Carel le Roux, MD, Ph.D., Professor at University College in Dublin, Ireland, and Principal
Investigator of the trial. “Current treatments for obesity mainly focus on weight loss by reducing energy intake. By activating both the glucagon and GLP-1 receptors, survodutide may both inhibit appetite and improve energy expenditure, thereby helping to treat the disease of obesity. These encouraging data support the further study of survodutide in larger Phase III trials.”
After 46 weeks of treatment, up to 40% of people who reached the highest two doses of survodutide achieved a weight loss of at least 20%, versus 0% with placebo (actual treatment analysis). Body weight loss of 15% or more was achieved by 67% of people who reached survodutide 4.8 mg versus 4.3% of those on placebo (actual treatment analysis).
Treatment with survodutide did not show unexpected safety or tolerability issues. Serious adverse events were reported by 4.2% of participants on survodutide versus 6.5% of those on placebo. Treatment discontinuation due to adverse events occurred in 24.6% and 3.9% of participants, respectively, mainly due to gastrointestinal adverse events. Most treatment discontinuations due to adverse events occurred during the rapid dose escalation phase and may potentially be mitigated with more gradual dose escalation. The adverse events reported were similar to those expected with the GLP1-R agonist class of drugs.
“With our long heritage in researching and developing new treatments for cardiovascular, renal, and metabolic conditions, we are extremely encouraged by these robust and compelling Phase II data,” said Carinne Brouillon, Head of Human Pharma, Boehringer Ingelheim. “Survodutide may become the first anti-obesity medication to reduce appetite while increasing energy expenditure through the liver. We look forward to furthering our discussions with health authorities to advance this dual receptor agonist into Phase III trials as we aim to fill a treatment gap in this disease area.”
“Obesity is one of the most significant healthcare challenges in medicine today,” said David Kendall, M.D., Chief Medical Officer, Zealand Pharma. “At Zealand Pharma, we have both experience and success in discovering and developing peptide therapeutics that target key metabolic pathways –designed to help people living with overweight and obesity by achieving substantial weight loss while addressing the many complications of this disease.”
ALTUVIIIOTM LATE-BREAKING DATA AT ISTH DEMONSTRATES HIGHLY EFFECTIVE BLEED PROTECTION IN CHILDREN WITH SEVERE HEMOPHILIA A WITH ONCE-WEEKLY DOSING
Pivotal data from the Phase 3 XTEND-Kids study evaluating ALTUVIIIOTM [Antihemophilic Factor (Recombinant), Fc-VWF-XTEN Fusion Protein] once-weekly prophylaxis, a first-in-class, highsustained factor VIII replacement therapy, in previously treated patients younger than 12 years of age with severe hemophilia A were presented today in a late-breaking session at the Annual Meeting of the International Society on Thrombosis and Haemostasis (ISTH) in Montreal, Canada.
The oral presentation detailed results from the XTEND-Kids study and confirmed that ALTUVIIIO met the primary endpoint with no inhibitor development to factor VIII detected, and key secondary endpoints including annualized bleeding rate (ABR) and maintenance of factor VIII activity above pre-specified levels.
In the pediatric population, clearance of administered factor concentrates in the blood is greater than in adults, often meaning injections are needed 2-4 times per week using standard (SHL) or extended half-life (EHL) factor VIII products. These data confirm that a once-weekly 50 IU/ kg dose of ALTUVIIIO provides highly effective bleed protection in both children and adults and can be used across clinical scenarios.
Hemophilia A is a rare, lifelong condition in which the ability of a person’s blood to clot properly is impaired, leading to excessive bleeds and spontaneous bleeds into joints that can result in joint damage and chronic pain, and potentially impact quality of life. The severity of hemophilia is determined by the level of clotting factor activity in a person’s blood, and there is a negative correlation between risk of bleeding and factor activity levels.
ALTUVIIIO is a first-in-class, high-sustained factor VIII replacement therapy approved in February 2023 by the US Food and Drug Administration (FDA) for routine prophylaxis and on-demand treatment to control of bleeding episodes, as well as perioperative management (surgery) for adults and children with hemophilia A. Granted Breakthrough Therapy designation by the FDA in May 2022 — the first factor VIII therapy to receive this designation —ALTUVIIIO also received Fast Track designation in February 2021 and Orphan Drug designation in 2017. The
DELIVERY OF CARE FOR SPINAL CORD INJURIES
The Health Information and Quality Authority (HIQA) has published a health technology assessment (HTA) on domiciliary (at-home) invasive ventilation for adults with severe spinal cord injuries. The report was requested by the Health Service Executive (HSE) in conjunction with the National Rehabilitation Hospital (NRH). It was conducted to inform the national delivery of care for adults with spinal cord injuries who require permanent invasive mechanical ventilation and in whom discharge home is deemed clinically appropriate.
European Commission granted Orphan Drug designation in June 2019, and the European Medicines Agency accepted the Marketing Authorization Application (MAA) for efanesoctocog alfa in May 2023.
Lynn Malec, MD Medical Director of Comprehensive Center for Bleeding Disorders and Associate Investigator at The Versiti Blood Research Institute, and Associate Professor of Medicine and Pediatrics at The Medical College of Wisconsin said, “The results from XTEND-Kids mark an important breakthrough as we strive for optimized bleed protection as the standard of care. Achieving high-sustained factor activity with once weekly dosing means a freedom from the tradeoffs between treatment burden and efficacy we often see in treating severe hemophilia A. The reliable and consistent bleed protection ALTUVIIIO provides offers confidence for children living with hemophilia and their families to manage hemophilia with less worry.”
WALKING THE TALK FOR DEMENTIA
The Walking the Talk for Dementia (WTD), took place in May in Santiago de Compostela, Spain, bringing together approximately 70 participants representing a diverse group of distinguished researchers, healthcare professionals, advocates, and people living with dementia from nearly 30 different nations across the Americas, Europe, Africa, Asia, and Oceania and embarked on a transformative journey, walking 40 km of the world's most renowned pilgrimage route, the Camino de Santiago. A group of nine Atlantic Fellows from the Global Brain Health Institute (GBHI) at Trinity College and the University of San Francisco, were among the group.
The collective journey was enriched by the invaluable participation of eight individuals living with dementia from the United States, England, Ireland, Namibia, Singapore and Spain. Their personal experiences and insights added a profound depth to the event, fostering a deeper understanding and empathy for the challenges and thriving experiences by those living with a dementia diagnosis.
According to global data from the World Health Organization (WHO), approximately 50 million people worldwide are living with dementia, and this number is expected to triple by 2050. Dementia affects individuals, families, and communities, posing significant social and economic challenges.
The Camino de Santiago holds deep historical and spiritual significance, attracting pilgrims from all corners of the globe seeking self-discovery and enlightenment. WTD embraced this tradition, allowing participants to immerse themselves in the essence of the Camino, but this time with a single purpose: to build a better world for people with dementia.
Professor Iracema Leroi, Geriatric Psychiatrist, Trinity College Dublin, the Global Brain Health Institute and Trinity Institute of Neurosciences, who took the Camino journey said, “WTD has been a transformational experience of like-minded individuals from all backgrounds, walking, talking and sharing insights. WTD reflects a genuine and equal partnership that has allowed allowing critical knowledge to emerge. It was an immersive transdisciplinary experience furthering the aim of addressing threats to brain health globally; as such, it aligned perfectly with the mission and vision of GBHI.”
Individuals with high spinal cord injuries have complex healthcare needs due to complications such as the complete paralysis of all four limbs and torso (tetraplegia) and respiratory failure. In order to breathe, a small number of these individuals will have a lifelong dependency on invasive mechanical ventilation via tracheostomy. Currently, an estimated five to ten adults with spinal cord injuries in Ireland receive invasive mechanical ventilation at home. While domiciliary ventilation is currently standard practice in Ireland for these patients, there are many challenges involved in their safe discharge home. As a result, they often remain in hospital for a prolonged period of time. This significantly impacts the quality of life of patients and their families and can place a strain on health service provision.
HIQA reviewed guidelines for domiciliary ventilation from other countries. Guidelines were identified from Australia, Canada, Germany, Italy, New Zealand, Poland, Switzerland, the Netherlands, the UK, and the US. These guidelines gave advice about aspects such as discharging a patient home from the hospital, looking after the patient when they are at home, and the equipment and staff that would be needed. The review highlighted key areas of importance for delivering a domiciliary ventilation service such as ensuring severe spinal cord injury patients had: 24/7 care provided by trained staff, specialised equipment and consumables, an adapted house and vehicle, and access to information and supports.
HIQA estimated the total five-year budget impact for the provision of domiciliary ventilation care to be approximately ¤3.4 million per patient.
Walking the Talk for Dementia team, Global Brain Health Institute at TCD
64 Clinical Profiles
ONETOUCH HEALTH COMPLETES GOVERNMENT BACKED CYBER ESSENTIALS CERTIFICATION
A health and social care specialist is enhancing its commitment to providing secure digital solutions, with a certification to help guard against cyber attacks.
OneTouch Health, a one-stop shop care management solution, has received the Cyber Essential Plus certification, a government-backed industry-supported scheme helping to protect organisations against common online threats.
Data security is integral to the work of OneTouch, with the multifunctional platform enabling care providers to share every aspect of their clients’ needs with all key people involved in their care circle.
While the health and social care sector has been slow to embrace digital solutions, technology is changing its delivery. With the benefits that this technology is bringing, care providers need to be cautious with how their approach to the correct storage of data.
Kieran Darnell, group operations director at OneTouch Health, said: “Maintaining digital security is at the core of what we do and the expertise of our team ensures the ongoing protection of our client data.
“As we see a shift from paper to digital in the sector, we are pleased to be delivering a leading technological solution to care providers that is not just providing efficiencies, but is secured to top industry standards.
“Our latest certifications show our commitment to digital security. We have seen what happens in the industry when security is breached, and so will continue to remain vigilant and well trained to be able to detect cyber threats.”
Digital transformation remains a key focus for the social care industry, with the Department of Health and Social Care (DHSC) recently publishing their latest guidance ‘What Good Looks Like’. The guidance is aimed at those responsible for implementing digital change in local authorities and care provider organizations, with safe practice one of the key areas.
In March 2023, the Government also published its Cyber Security Strategy for Health and Social Care to 2030. With a national implementation plan due to be published by summer 2023, the strategy provides guidance for health and social care providers to achieve cyber resilience across the sector.
As well as the Cyber Essentials certification, OneTouch is accredited with ISO 27001 and ISO 9001 and follows a three part holistic approach to its cyber security and risk management.
BLOOD-BASED CANCER SCREENING LAUNCHES IN IRELAND
Certior Health (“Certior”) is pleased to announce that it has partnered with Datar Cancer Genetics, a leading cancer research company, focussed on evidence-based testing procedures both in the field of therapy management and cancer screening. The initial test being launched is Trucheck™, an innovative cancer screening test that requires a safe, simple and quick blood draw, allowing for early detection of cancer by detecting Circulating Tumour Cells (CTCs). Trucheck™ Intelli can distinguish 70 types of cancers which account for 81% of all cancer cases and 84% of all cancerrelated deaths in Ireland. Certior Health is now offering Trucheck™ testing in Ireland at their clinic in Blanchardstown, Dublin.
A recent survey of 1,034 Irish adults revealed that 88% of participants were aware of blood-based cancer screening and expressed a strong interest in learning more about this innovative approach.1 The survey, commissioned by Certior Health, aimed to assess patient needs, awareness, and understanding of cancer screening, while identifying any concerns around accessing such tests.
The research revealed that 41% of survey participants have had immediate experience with cancer, either themselves or through an immediate family member (parent, child or sibling). Notably, women exhibited a greater understanding and uptake of cancer screening compared to men. However, just 37% of women aged 45-54 are aware of when BreastCheck screening should start. Of all those surveyed, most expressed a strong desire to learn more about their health, whilst 3% said they would prefer not to know if they had cancer. 77% said they would be willing to pay for private screening.
Dr Vineet Datta, Executive Director at Datar Cancer Genetics, said: “We are delighted to partner with Certior. This collaboration will provide advanced cancer genomics to the patient community, and we will work closely with Certior’s medical team to support better-informed clinical decision-making. Trucheck™ is a CE-certified cancer screening solution offered for single and multi-organ cancer screening. We believe the solution will
encourage more men and women to participate in cancer screening for a safer future. “
Dr Nick Flynn, Chief Medical Officer for Certior Health emphasised the importance of cancer screening, stating, “Cancer is the leading cause of death in Ireland, responsible for approximately 30% of all deaths each year.2 By enabling early detection and intervention, Trucheck™ empowers individuals to take charge of their health.
Timely screening not only increases the chances of successful treatment but also offers peace of mind and reassurance to those at risk. It is crucial that we continue to prioritise and expand access to innovative screening options to enhance cancer prevention and ultimately improve health outcomes for the Irish population.”
Maggie Malone, CEO of Certior Health, shared her personal experience with breast cancer in 2017 and highlighted the significance of early detection. She stated, “Each year, an estimated 44,000 people are diagnosed with cancer in Ireland.3 Trucheck™ provides a safe and reliable way for individuals to get screened.
Trucheck™ can detect over 70 types of cancer and is intended to complement routine cancer screenings for early detection. Additionally, this solution can also detect various other cancers, not currently screened for regularly such as ovarian cancer, pancreatic cancer and lung cancer.
TruCheck™ through its innovative and novel process of utilising CTCs to identify cancers in both early and advanced stages, has been validation in more than 40,000 individuals.
Datar stands out due to their advanced technology and unique approach to blood-based cancer screening. We leverage cuttingedge molecular and genetic analysis techniques to detect specific biomarkers associated with different types of cancer.
Our tests are highly sensitive and specific, providing an accuracy rate of 96.8%. We are keen to make our tests accessible and affordable, ensuring that more people can benefit from early cancer detection. To this end, we are currently in talks to be partially reimbursed via private health insurers, as well as several large employers.”
Currently, Trucheck™cancer screening is available at Certior Health’s Centre in Blanchardstown, Dublin. Certior is committed to expanding access to Trucheck™ across Ireland, ensuring that more individuals can
benefit from this groundbreaking screening technology.
Patients can self-refer for screening. The test is suitable for adults over the age of 40 who are asymptomatic and have a risk of cancer. For more information about Trucheck™, please visit certior.com.
EUROPEAN COMMISSION AUTHORISES GSK’S AREXVY (RESPIRATORY SYNCYTIAL VIRUS (RSV) VACCINE, ADJUVANTED), THE FIRST RESPIRATORY SYNCYTIAL VIRUS VACCINE FOR OLDER ADULTS
GSK plc (LSE/NYSE: GSK) announced that the European Commission has authorised Arexvy (respiratory syncytial virus vaccine, adjuvanted) for active immunisation for the prevention of lower respiratory tract disease (LRTD) caused by respiratory syncytial virus (RSV) in adults 60 years of age and older. This is the first time an RSV vaccine for older adults has been granted European Marketing Authorisation. The first launches are planned ahead of the 2023/2024 RSV season which typically starts in the autumn.
Tony Wood, Chief Scientific Officer, GSK, said: “Thousands of older adults across Europe suffer serious respiratory illness due to RSV each year. This authorisation for Arexvy means eligible adults can be vaccinated against RSV disease for the first time, reinforcing GSK’s long history of vaccine innovation. Our strong manufacturing capability and scale, including from our vaccine manufacturing site in Belgium, means we are ready to deliver the vaccine as countries begin to launch.”
RSV is a common, contagious respiratory virus that leads to over 270,000 hospitalisations and approximately 20,000 in-hospital deaths each year in adults aged 60 years and over in Europe1. An estimated 3 million cases of RSV acute respiratory infection (ARI) are reported in this population each year, and the impact on healthcare systems is expected to increase as the population ages1. Those with underlying medical conditions, such as diabetes and chronic heart and lung disease, drive the majority of RSV hospitalisations.2,3
Dr Alberto Papi, Full Professor of Respiratory Medicine and Head at the University of Ferrara, said: “For most, RSV causes cold-like symptoms. For older adults and those with underlying medical conditions however, it can lead to severe disease and is a leading cause of serious respiratory infections. As scientists, we have been trying to find a solution for over 60 years. I am proud to have
been part of the innovation that has resulted in a vaccine now being available to help protect eligible older adults across Europe from severe RSV disease for the first time.”
The authorisation is based on GSK’s landmark positive pivotal AReSVi-006 (Adult Respiratory Syncytial Virus) phase III trial data. In the trial, the vaccine showed statistically significant and clinically meaningful overall efficacy of 82.6% (96.95% CI, 57.9–94.1, 7 of 12,466 vs 40 of 12,494) against RSV-LRTD in adults aged 60 years and older, meeting the primary endpoint. In addition, efficacy was 94.6% (95% CI, 65.9–99.9, 1 of 4,937 vs 18 of 4,861) in older adults with at least one underlying medical condition of interest, such as certain cardiorespiratory and endocrine-metabolic conditions.
The vaccine was generally well tolerated. The most frequently observed solicited adverse events were injection site pain, fatigue, myalgia, headache, and arthralgia. These were generally mild to moderate and transient.
The European Commission’s decision follows the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) positive opinion in April 2023. GSK’s marketing authorisation application was reviewed under the accelerated assessment mechanism because prevention of RSV disease in the older adult population is considered a major public health interest.
Arexvy was the world’s first RSV vaccine to be approved for older adults when, in May 2023, it was approved by the US Food and Drug Administration. Later this month, the Advisory Committee on Immunization Practices (ACIP) will make recommendations on the appropriate use of the vaccine in the US. Regulatory reviews are ongoing in Japan and several other countries.
UNIVERSITY HOSPITAL
GALWAY
TRIALS NEW INNOVATIVE TECHNOLOGY FOR PATIENTS WITH HEART FAILURE
University Hospital Galway (UHG) has completed the final phase of an innovative clinical trial which reduces the hospitalisation rate for patients living with heart failure. The trial which allows patients to be treated for heart failure from home has the potential to be a game changes in the treatment and monitoring of the condition.
Heart failure is a significant public health priority with patients requiring frequent hospitalisations. This new sensor allows cardiology teams to monitor patients remotely,
avoiding hospitalisation. An internal audit in UHG of patients who received the sensor noted a 97% decrease in hospitalisation among this group.
The Cordella Pulmonary Artery Pressure Sensor detects changes in the health of patients with heart failure and securely transmits the information to the care team for review. If a change is detected, the team can then make changes to medications or other clinical interventions to prevent a heart failure flare-up requiring urgent hospitalisation.
“Over the last few years, UHG has conducted and completed three clinical trials with this unique device, in which 37 patients with advanced heart failure from the West and North West of the county have had the Cordella Sensor implanted. The trial was open for patients with heart failure, who met a certain criteria and who were being treated at the Heart Failure Clinic in UHG,” explains Prof Faisal Sharif, Consultant Interventional Cardiologist at UHG and Director of Cardiovascular Research and Innovation Centre, University of Galway, who is the clinical trial’s principal investigator.
“We conducted an internal audit of all the patients in UHG who had the sensor placement, and were pleasantly surprised to see that hospitalisations for heart failure had decreased by 97%. This technology will improve patients’ quality of life and keep them healthy in their own homes, and it has the potential to be a game changer in the treatment and monitoring of heart failure,” he added.
The sensor is placed in the right pulmonary artery of the heart to monitor pulmonary artery pressures within the heart muscle.
Insertion of the sensor is a simple procedure that only requires an overnight stay in hospital.
The sensor is remotely connected to a computer system in the hospital and the heart pressures are transmitted via a cloudbased system where the clinical research nurses can review the pressures and advise accordingly. The Cordella System includes Bluetooth-enabled devices that measure blood pressure, weight, heart rate, and oxygen saturation, all of which are transmitted to the hospital.
“Patients with severe heart failure typically have elevated cardiac pressures before experiencing shortness of breath, so we have three to four days before the patient experiences dyspnea. By monitoring these pressures remotely, we can intervene and adjust their medication to reduce these pressures, prevent shortness of breath and avoid hospitalisation. One of the biggest problems with heart failure is that patients have very frequent hospitalisations.
“We see four to five times as many patients per year with heart failure symptoms and decompensation that require high dependency beds, intravenous medicines, and airway support, resulting in seven to ten days of hospitalisation. So by remotely and actively monitoring these patients, hospitalisation is avoided,” said Prof Sharif.
One of the most important aspects of this therapy is that the patient uses a portable device on their chest that transmits their cardiac pressure to the hospital. With the use of this technology, the patient becomes actively involved in their care.
Prof Faisal Sharif, Consultant Interventional Cardiologist at UHG and Director of the Cardiovascular Research and Innovation Centre at the University of Galway pictured with patient Richard Power from Abbey, Loughrea, County Galway following the successful implantation of the Cordella Pulmonary Artery Pressure Sensor
“This is an example of patient engagement, patient empowerment, and the patient is, in reality, a member of the heart failure treatment team. Patient involvement leads to the monitoring of their weight, blood pressure, and oxygen saturations. And as a result, overall, leads to better quality of life. If you have a baseline of a patient’s heart rate, oxygen saturation, body weight, blood pressure, and pulmonary artery pressure and compare it over time, you can see whether they are progressively worsening, improving, or maintaining volume status. And that’s what keeps them well in the community,” said Prof Sharif.
Patient, Richard Power from Abbey, Loughrea, County Galway said, “Since the implant, I am very pleased with my life. Cordella wakes me at 8 o clock every morning to do my readings. It takes just five minutes and it saves me driving 50 kilometres, three or four times a month, and I am very grateful for Dr Sharif and his staff for what they have done for me.”
Ms Chris Kane, General Manager, Galway University Hospitals said, “The success of this clinical trial can be measured in the improvements in the patients’ quality of life, the dramatic reduction in the need for hospitalisation and the enhanced role that the patients are able to play in their own care. This is an excellent example of providing quality care in a patient’s own home environment to a level as close as possible to a hospital visit.”
The clinical trial is a collaboration between University Hospital Galway, University of Galway, Science Foundation Ireland and Endotronix, USA.
EUROPEAN COMMISSION APPROVES IMBRUVICA® (IBRUTINIB) IN A FIXEDDURATION
The Janssen Pharmaceutical Companies of Johnson & Johnson have announced that the European Commission (EC) granted marketing authorisation for the expanded use of IMBRUVICA® (ibrutinib) in an alloral, fixed-duration (FD) treatment combination with venetoclax (I+V) for adults with previously untreated chronic lymphocytic leukaemia (CLL). The approval is based on the pivotal Phase 3 GLOW study that demonstrated superior progression-free survival (PFS) in patients treated with I+V versus chlorambucil plus obinutuzumab (Clb+O), and the FD cohort of the Phase 2 CAPTIVATE study, which showed deep and durable responses in patients treated with I+V, including those with high-risk features.
66 Clinical Profiles
CLL is generally a slow growing blood cancer that originates from B cells. It has an incidence rate of approximately five cases per 100,000 persons in Europe and about 500 people are diagnosed with it in Ireland each year. The EC approval aims to provide healthcare professionals with the flexibility to use ibrutinib either in a fixed-duration combination with venetoclax or as a continuous monotherapy in first-line CLL. In Ireland, ibrutinib is already approved as a continuous therapy in several indications across three blood cancers (CLL, mantle cell lymphoma and Waldenström’s macroglobulinaemia).
Professor Patrick Thornton, Consultant Haematologist, Clinical Director Hermitage Medical Clinic & Beaumont Hospital laboratory said: “For Irish patients living with CLL, intervention with the most effective front-line treatments is extremely important. In parallel, the development of innovative therapies remains vital to ensure we have the option and ability to best tailor treatment to meet individual patient needs and preferences. The combination of ibrutinib and venetoclax working together has the potential to provide treatmentfree durable remissions and holds significant progress for how we approach the future of front-line CLL therapy in Ireland.”
In CLL, patient outcomes have improved over the last decade. A wave of innovation, including the advent of novel oral therapies that target the underlying disease biology, has shifted the standard of care from chemoimmunotherapy to targeted agents and combination therapies.
Dr Thorsten Giesecke, General Manager, Commercial Business, Janssen Sciences Ireland UC, said: “Janssen is committed to continually advancing and optimising treatment options for patients living with blood cancers, including CLL. This approval is a positive step in improving the quality of lives of Irish patients with CLL and transforming outcomes for a patient cohort where unmet medical need remains.”
The EC approval is supported by data from the pivotal Phase 3 GLOW study (NCT03462719), which demonstrated that I+V was superior to Clb+O with respect to the primary endpoint, PFS assessed by an independent review committee, in elderly or unfit patients with CLL (PFS hazard ratio [HR]: 0.216; 95 percent confidence interval [CI], 0.131 to 0.357; P<0.001).2 The improvement in PFS with I+V was consistent across predefined subgroups, including older patients and those with comorbidities
and high-risk features.2 It is also supported by the FD cohort of the Phase 2 CAPTIVATE study (NCT02910583) which evaluated I+V in patients with previously untreated CLL who were 70 years or younger, including patients with high-risk CLL disease.
The primary analyses from these studies were recently published in NEJM Evidence and Blood, respectively, and were originally featured as oral presentations at the European Hematology Association (EHA) 2021 Congress. Followon analyses from GLOW were presented at the American Society of Hematology (ASH) 2021 Annual Meeting, and additional data from the CAPTIVATE study including clinical outcomes at three years and evidence of immune restoration post-treatment were presented at the EHA 2022 Congress.
Updated data for both studies showed the safety profile of the I+V regimen was consistent with known safety profiles of ibrutinib and venetoclax. In GLOW, the most common adverse events (AEs) were diarrhoea (50.9 percent) and neutropenia (41.5 percent) in the I+V arm and neutropenia (58.1 percent) and infusion-related reactions (29.5 percent) in the Clb+O arm. AEs of Grade 3 or greater occurred in 75.5 percent and 69.5 percent of patients in the I+V and Clb+O arms, respectively.2 Any-grade atrial fibrillation occurred in 15 patients (14.2 percent) receiving I+V and two patients (1.9 percent) receiving Clb+O, however, only two patients (1.9 percent) discontinued ibrutinib due to atrial fibrillation while continuing venetoclax.2 Although overall survival data is not mature, with a median follow-up of 34 months, there were 11 deaths in the I+V arm and 16 deaths in the Clb+O arm (HR: 0.760; 95 percent CI, 0.352 to 1.642). In the CAPTIVATE FD cohort, the most common AEs were diarrhoea (62 percent), nausea (43 percent), neutropenia (42 percent), and arthralgia (33 percent) and were primarily Grade 1 or 2 in severity. The most common Grade 3/4 AEs were neutropenia (33 percent), hypertension (6 percent), and neutrophil count decreased (5 percent). Serious AEs occurred in 36 patients (23 percent) and one fatal AE occured.
HSE COMMENCES
PROGRAMME OF ACTION ON CLIMATE CHANGE
The HSE has launched its Climate Action Strategy 2023-2050. This health service-wide strategy aims to reduce the negative climate impacts of our health service, achieve net-zero emissions for the HSE by 2050, and deliver healthcare that is environmentally and socially sustainable.
Climate change is one of the greatest threats to public health across the globe, and as Ireland’s largest public body, we in the HSE recognise the significant role we can play in tackling the climate crisis. The healthcare sector is a notable contributor to greenhouse gas emissions, accounting for an estimated 5% of total emissions globally and is also responsible for responding to people’s changing health needs affected by climate change.
Care is one of the HSE’s core values, and that includes demonstrating care for our environment and how we use resources as we work. Our climate action strategy sets a high ambition for our health service, and we are committed to the timely implementation of the actions it sets out for our teams and services.
Dean Sullivan, HSE Chief Strategy Officer, said “This programme of work responds to and supports the Government’s Climate Action plans and provides actions and targets to reduce the environmental and social impact of the delivery of healthcare in Ireland. Our health service will be showing leadership and commitment to sustainable actions and principles across areas such as buildings, green space development, transport, greener models for health care, procurement and more.”
Globally, healthcare is a key contributor in fuelling climate harm due to our need for high-energy intensive buildings, transportation footprint of employees and patients, global supply chain emissions including supplies, pharmaceuticals, devices, and food, the uses of single-use goods and more.”
The HSE actions will be focused on 10 areas:
1. Reducing our energy-related greenhouse gas emissions
2. Developing green spaces
3. Decarbonising our fleet of vehicles
4. Promoting low carbon and active travel
5. Aligning our purchasing of goods and services with decarbonisation and sustainability goals
6. Baselining our supply chain emissions
7. Developing greener models of healthcare delivery
8. Reducing and managing waste
9. Conserving and reducing water use
10. Protecting people’s health and wellbeing.
HEALTH SERVICE EXECUTIVE APPROVES
OF UCB’S
REIMBURSEMENT
BIMZELX
(BIMEKIZUMAB) FOR TREATMENT OF PSORIASIS
UCB, a global pharmaceutical company, has announced that bimekizumab has been approved for reimbursement1 by the Health Executive Service (HSE) of the Republic of Ireland for the treatment of adult patients with moderate to severe plaque psoriasis, a common, chronic inflammatory disease that primarily impacts the skin.
Psoriasis affects more than 73,000 people in Ireland, around 2% of the population, with more than 9,000 of these people living with severe psoriasis.
Unfortunately, the unmet need remains in psoriasis with the visible symptoms reported to impact the day-to-day lives of those living with the condition, including employment and social isolation. Bimekizumab is the first available treatment in Ireland to selectively inhibit two key cytokines driving inflammatory processes, known as IL-17A and IL-17F, for moderate to severe plaque psoriasis.
David Lock, Head of Immunology, UCB UK & Ireland said, “Bimekizumab is unique in the way it selectively inhibits both IL-17A and IL-17F and has shown exceptional sustained improvements in psoriasis severity in both head-to-head and placebo controlled clinical trials and we are delighted that bimekizumab will now be a treatment option for eligible Irish patients.”
David McMahon, Chief Executive Officer of the Irish Skin Foundation, added, “People in Ireland living with psoriasis, many struggling to manage their skin condition for decades, deserve access to the newest, innovative treatments for the condition and we welcome the HSE’s acceptance of bimekizumab which offers another option for those eligible Irish patients living with the visible and invisible challenges of an unpredictable condition.”
The HSE acceptance is supported by results from three Phase 3 studies, BE VIVID, BE READY and BE SURE, which evaluated the efficacy and safety of bimekizumab in adults with moderate to severe plaque psoriasis.
All studies met their co-primary endpoints achieving superior levels of skin clearance, and significantly reducing the severity of psoriasis in patients treated with bimekizumab (as assessed by the Psoriasis Area and Severity Index 90 and Investigators Global Assessment
0/1) at week 16, compared to those who received adalimumab (BE SURE), ustekinumab (BE VIVID) and placebo (BE READY).
The most frequently reported adverse events in bimekizumabtreated patients were nasopharyngitis, oral candidiasis, and upper respiratory tract infection.
Professor Brian Kirby, Consultant Dermatologist, St Vincent’s Hospital, Dublin, and Full Clinical Professor at University College Dublin said, “Psoriasis affects every aspect of life for people living with the condition. In head-to-head trials bimekizumab has shown higher rates of skin clearance versus the most commonly prescribed therapies which is a key outcome for patients. I am pleased to see this new, highly effective treatment available for eligible patients living with this chronic condition that affects more than the skin.”
ROCHE AWARDED WHO PREQUALIFICATION FOR THE COBAS® HPV TEST
Roche (SIX: RO, ROG; OTCQX: RHHBY) has announced that the cobas® HPV test for use on the cobas® 6800/8800 Systems has been awarded World Health Organization (WHO) prequalification. WHO prequalification expands the availability of this critical HPV screening tool in countries that rely on the global organisation’s list in making purchasing and implementation decisions.
Screening for Human Papillomavirus (HPV) can help identify women who are at risk of developing cervical cancer, so that the disease can be treated early, before invasive cancer has a chance to develop. In poorer countries, women are often diagnosed with cervical cancer at a more advanced stage, where the opportunity for a cure is low.
“The elimination of cervical cancer is within reach. Roche is committed to working with governments, non-profit organisations and funders to help build sustainable cervical cancer elimination programs so that women, no matter where in the world they live, no longer die from this preventable disease,” said Matt Sause, CEO of Roche Diagnostics. “Today’s action, combined with our recentlylaunched HPV-self sampling solution, further expands access to HPV screening in countries with limited healthcare resources.”
The WHO strategy for global elimination of cervical cancer lists
the following three target goals to reach by 20302:
• 90% of girls should be fully vaccinated with HPV vaccine by 15 years of age;
• 70% of women should be screened using a highperformance test by age 35, and again by age 45;
• 90% of those identified with cervical disease should receive appropriate treatment.
The cobas® HPV test is already part of the Roche Global Access Program, which aims to improve access to cost-effective resources, implement scale-up programs, and contribute to the elimination of diseases in the regions with the greatest need. WHO prequalification helps expand that access and provides healthcare professionals with greater confidence that their clinical decisions will be based on accurate, reliable results.
About the Global Access Program
In 2014, Roche first launched its Global Access Program to support the UNAIDS 2020 targets to address the HIV/AIDS epidemic. Since then, the program was expanded to include solutions for other high-burden diseases such as Tuberculosis, Hepatitis B and C, and cervical cancer. Most recently, in response to the COVID-19 pandemic, the SARS-CoV-2 test was included into the program. The continual expansion of test offerings highlights Roche’s commitment to eliminate cervical cancer and other high burden infectious diseases for patients living in resource-constrained settings with limited access.
Any laboratory that implements a Roche instrument system gains the ability to scale up testing across multiple disease areas, thus improving cost and resource efficiency. An integrated approach supports national programs focused on increasing access to diagnostic testing, to help manage or reduce the impact of preventable disease for patients.
About the cobas HPV test
The cobas® HPV test is indicated for use for routine cervical cancer screening as per professional medical guidelines, including HPV primary screening, co-testing (or adjunctive screen) with cytology, and for triage of women with abnormal cytology, to assess the risk for cervical precancer and cancer. The cobas® HPV test detects the high-risk HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68.
In June 2022, Roche further improved access for women when it launched an HPV self-sampling solution in countries accepting the CE mark. The solution enables a patient to privately and confidently collect her own sample following instruction from a healthcare worker. The clinically-validated vaginal sample is then analysed with the Roche cobas® HPV test on a Roche molecular instrument.
Cervical cancer screening using the cobas® HPV test is clinically validated in large, FDA registrational trials for use on cobas® Systems, and the assay individually identifies the presence of the DNA of HPV genotypes 16 and 18 – the two genotypes responsible for about 70 percent of all cervical cancers – and reporting the 12 other high-risk HPV types as a combined result, all in one test and from one patient sample. More information about the cobas® HPV tests is available at diagnostics. roche.com/cervicalcancer.
The fully automated cobas® 6800/8800 Systems offer the fastest time to results, providing up to 96 results in about three hours and 384 results for the cobas® 6800 System and 1,056 results for the cobas® 8800 System in an eight hour shift. Learn more: diagnostics.roche.com.
RICK OF IRON OVERLOAD
Despite being Ireland’s most common genetic condition, with one in 83 people at risk of developing haemochromatosis and one in five people carrying the gene, it might come as a surprise to learn that haemochromatosis – or ‘iron overload’ - is also one of the lesser-known conditions amongst the Irish population. Haemochromatosis is more common in Ireland than anywhere else in the world, giving it the nickname ‘the Celtic Gene’ as one in five people carry one copy of the gene and one in every 83 Irish people carry two copies of the gene, predisposing them to develop iron overload. Recent research also shows that up to 1 in 10 people in Northern Ireland are at risk of having genetic Haemochromatosis.
Early diagnosis is vital and if left untreated, iron overload can lead to organ damage or even premature death. The Irish Haemochromatosis Association estimates there are at least 20,000 undiagnosed cases of haemochromatosis in Ireland.
To mark World Haemochromatosis Awareness Week, which took place from 1st – 7th June 2023,
the Irish Haemochromatosis Association aims to raise awareness of the condition and is urging people to join the association in calling for a National Strategy for Haemochromatosis. The Association is also asking people to ‘Get Checked for Haemochromatosis’ to highlight the symptoms in order to save lives – symptoms that range from chronic tiredness and joint pain, to abdominal pain and sexual dysfunction.
This year will see several City and County Councils throughout the country supporting the campaign and joining the wider, international initiative to ‘Light Up Red’, lighting up several iconic public buildings during World Haemochromatosis Awareness Week. Buildings being illuminated in the distinct red colour will include the Dublin Convention Centre, Fingal Town Hall, Cork City Hall, Limerick Council Offices, Sligo City Hall, Donegal Public Services Centre and Kerry County Council Buildings, Tralee, Princes Quay and Ashe Memorial Hall Building, Tralee, Killarney Town Hall and Kenmare Courthouse Building, Kenmare, Co. Kerry.
The Irish Haemochromatosis Association has this year teamed up with Tomás O’Leary. Tomás is a well-known former Ireland Rugby international who was part of the Irish team that won the 2009 Grand Slam. As part of Munster Rugby, Tomás won two Heineken Cups in 2006 and 2008. Tomás has family members living with haemochromatosis and is helping to raise awareness of the common condition, in the hope that someday everyone in Ireland will be aware of the symptoms.
Tomás says that it is an honour to be helping raise awareness of the most common genetic condition amongst Irish people.
“As someone who has seen family members diagnosed with haemochromatosis, I want to help highlight just how important early detection really is. If I can help even one person recognise the symptoms and inspire them to go and get checked, I will feel like I have helped make a small difference. I hadn’t heard of haemochromatosis until I learned that my uncles and aunts were living with it. That’s why I’m delighted to be working with the IHA to make sure everyone in Ireland is aware of haemochromatosis and knows exactly what it is and – most importantly – how to recognise the symptoms before it’s too late.”