Matter of Spirit, Winter 2026, I Health Care is a Human Right
From the Editor
In January 2026, 2.5 million people living in North Carolina received an unexpected letter: their medical debt, some dating back more than 12 years, had been erased.
In an agreement between the state government and hospitals, all 99 hospitals in North Carolina agreed to stop collection on certain debts going back as far as 2014. They also agreed that, going forward, care will automatically be discounted for patients who qualify. For a family of four, that means an annual income of less than $96,000.
This is a fantastic step forward for people living in North Carolina. But the rest of the country isn’t that lucky. According to an NPR article, assistance with health care bills is patchy: Arizona and New Jersey use their federal budget to forgive medical debt. Oregon and Illinois screen patients to see if they qualify for financial assistance.1 Other states, like New York and Colorado, ban medical debt from credit reports. But what about everyone else who isn’t lucky enough to live in one of those states?
Even among people with insurance—which currently is the vast majority of Americans—over half of U.S. adults say that it’s difficult to afford health care.2 According to the Federal Reserve, in 2024 28 percent of adults skipped some sort of medical care because of the cost.3 In 2025, the government shut down for weeks, in large part because of disagreements over whether to extend the tax credits for the Affordable Care Act (these tax credits were not extended, and the effect it will have on premiums is unclear, with some estimating that they might go up, on average, by 114 percent).
What these facts and figures and political machinations fail to reflect, however, is that health care access is not merely a political issue, an economic problem, or even a matter of personal responsibility. It is a moral measure of our society. How we treat our sick—who receives care, who must wait, who is turned away, who goes into debt to receive life-saving care—reveals what we truly believe about human dignity and the value of human life. In the United States, access to health care is increasingly shaped not by need, but by income, employment, disability, immigration status, and geography. These distinctions may be normalized in policy debates, but they are profoundly at odds with the Catholic conviction that every human life bears equal worth.
1 Alex Olgin, “How North Carolina Erased Medical Debt for 2.5 Million People,” NPR, January 21, 2026, https://www.npr.org/2026/01/21/ nx-s1-5678541/north-carolina-undue-medical-debt-erased
2 Cynthia Cox et al., “Health Care Costs and Affordability,” KFF, October 8, 2025, https://www.kff.org/health-costs/health-policy101-health-care-costs-and-affordability/
3 “Report on the Economic Well-Being of U.S. Households in 2024 - May 2025 - Income and Expenses,” The Federal Reserve, accessed February 6, 2026, https://www.federalreserve.gov/ publications/2025-economic-well-being-of-us-households-in-2024income-and-expenses.htm.
“It is a moral measure of our society.”
This issue of A Matter of Spirit examines some of the issues at stake when it comes to health care and explores the role our faith might play in building a better world, one where everyone receives the health care they need to flourish. In “Made in the Image of God,” author Madison Chastain looks at how U.S. policy dehumanizes people with disabilities. “The image of God is not a human body with certain limbs and capabilities,” she writes. “The image of God is a deeper reality, a reflection of the Holy Spirit, the creative potentiality of the Divine. The disabled bear the full image and likeness of God, no matter how they may look or how their bodies may function.”
In “The Work Ahead,” Wendy Maimone looks at how cuts to mental health care—an area often forgotten in the discourse around health care access—also affect families. And in “Stretched to the Breaking Point,” Mia Isabel Lazo reflects on how current health care inequities especially affect young adults. “My story is just one example of what happens when a system is stretched to its breaking point,” she writes. Finally, in “Healing As Holy Work,” Erica Torres looks at how women religious offer an enduring model for integrating health care with our faith.
The good news is that a better way is possible: Just look at what North Carolina has just done! Not to mention the work that so many religious congregations have been doing for centuries. Now the fight continues to ensure that everyone, no matter where they live or how much money they make, receives the same care.
—Emily Sanna, Editor
IPJC Community Assembly participants engage in Conversations in the Spirit and discern the critical issues in our community.
MADE IN THE IMAGE OF GOD
U.S. POLICIES DEHUMANIZE DISABLED PEOPLE AND FAIL TO ACKNOWLEDGE THAT WE ARE ALL PART OF THE BODY OF CHRIST
BY MADISON CHASTAIN
In the Gospel of Mark, Jesus passes the blind man, Bartimaeus, and asks him, “What do you want me to do for you?” Bartimaeus replies, “Let me receive my sight” (Mark 10:46–52).
We encounter a similar scene in the Gospel of John: “As [Jesus] passed by, he saw a man blind from birth. And his disciples asked him, ‘Rabbi, who sinned, this man or his parents, that he was born blind?’ ” (John 9:1–3). Jesus answered, in effect, neither. His blindness was not due to anyone’s sin.
For centuries, people believed that disabilities were retributive curses from God, so they cast out the disabled from society. We see across all four gospels how Jesus cared distinctly for the disabled; he performs more healing miracles than any other kind. And yet, in the context of the rest of his ministry, it’s clear Jesus is not as concerned with physical health and medical healing as he is with removing the labels that make people outcasts and bringing them back into community.
Jesus also makes clear that healing is not a project of unidirectional charity, but of listening, exchange, and consent. Jesus does not assume that Bartimaeus wants literal healing: Jesus asks.
It can be easy to assume that all disabled people must want physical healing. But for many disabled people, their diagnosis is so totalizing, so integrated into who they are, that to become un-disabled would be to completely alter who they are as a person. For many disabled people, what they need is a nondisabling society, one that includes and welcomes them and considers them for what they like and want, not for how they make the rest of society feel. Disabled people need tools, not transformation.
It’s surprising, then, how many U.S. Christians conceive of disability in totally contradicting ways. The Bible is ambiguous on many things, but regarding disability, we’ve received crystal clear directives. Where does our culture’s insistence on villainizing and eliminating disability come from?
Perhaps it is because we don’t want to believe that unpredictable things can happen to good people. When we’re confronted with a life circumstance that defies reason—that occurs regardless of our
“Jesus is not as concerned with physical health and medical healing as he is with removing the labels that make people outcasts and bringing them back into community.”
efforts, prayers, or preoccupations—we invent a reason to reassure and insulate ourselves from the reality that, it’s true, disability could even happen to us. Instead, we say someone must’ve done something wrong.
“America is obsessed with earning human rights through labor. But are they human rights if some people can’t have them?”
In much the same way, U.S. Christians worship the prosperity gospel, the idea that if we just work hard enough, pull ourselves up by our bootstraps, and pray, God will reward our labors.
Combined, these misbeliefs lead us to perceive the disabled—as well as the poor, the unhoused, and the addicted—as people who have somehow earned their suffering and can thereby earn their way out of it. We choose to believe that oppressive social circumstances are individual moral failings, because it is less scary to think that an individual has contracted their own oppression through conscious decision-making than it is to admit that our society’s leaders have designed a system that oppresses in order to make the rich richer.
These beliefs about disability extend far beyond how we behave around the disabled in public, whether we scorn the person moving slowly on the sidewalk or stare at the person with limb differences. These beliefs also motivate policy.
One of the clearest examples is the recent passage of H.R.1, otherwise known as the “Big Beautiful Bill.” Included in H.R.1 are substantial changes to the qualifications for Medicaid.
Medicaid was originally established to enable the poor, of any age and bodily condition, to afford health care. So long as a person could prove their low income, they generally qualified for Medicaid. This was especially important for people who are older and people with disabilities who could not work.
In fact, U.S. disability policy incentivizes the disabled not to work: To qualify for federal disability social security benefits, a disabled person may earn no more than $1,620 a month. That’s a yearly salary of less than $20,000. For context, the United States considers the poverty line to be at $15,000.
Even worse, the government implicitly discourages disabled people from marrying under the same guidelines. If a married couple’s yearly income is above $30,000, the disabled spouse loses their disability benefits. The poverty line for a married couple is $32,000. There can be no other reason for systematically discouraging disabled people from marriage than the fear of how marriage and romance challenge our social narratives around disability: the way we view disability as intrinsically childlike, genetically inferior, even dangerous.
In the United States, the average monthly rent has now risen to $1,700 for a studio apartment. A person with a disability receiving social security benefits from the government cannot afford to live on their own. Add to this the costs of food and health care, which are significantly higher for a disabled person purchasing medications, therapies, and mobility aids, and it becomes clear that the amount from the government is dehumanizingly insufficient.
Medicaid, along with so many other tools that the current administration seeks to roll back, seeks to step into this gap and help provide necessary services. However, instead of fixing government overspending, it is easier to blame those who rely upon government
services and reignite the same old narrative: that the poor and disabled are taking advantage of government charity and should, instead, work their way out.
Starting in 2027, when H.R.1’s changes go into effect, Medicaid will have both age limitations as well as robust work requirements. People who are 19 and older and who do not meet one of the “qualifying exceptions” will have to prove that they have “contributed meaningfully to society” through a minimum of 20 hours of work, volunteering, or education each week. That’s the equivalent of a half-time job.
Although many lawmakers insist that people with severe disabilities fall under those certain exceptions, the fact remains: America is obsessed with earning human rights through labor. But are they human rights if some people can’t have them?
In the Catholic tradition, all people have intrinsic human dignity rooted in the image and likeness of God. The image of God is not a human body with certain limbs and capabilities. The image of God is a deeper reality, a reflection of the Holy Spirit, the creative potentiality of the Divine. The disabled bear the full image and likeness of God, no matter how they may look or how their bodies may function.
Catholics also believe that civil government is a natural extension of human community, that the role of a “higher social institution” like a governmental body is to intervene in a subsidiary fashion that encourages individual human development in alignment with the common good (see, for example, paragraphs 1883–1885, 1894, and 1897–1902 of the Code of Canon Law). The question our lawmakers seem to be asking is: What is a fairly subsidiary government intervention? According to canon law, the answer is: “[One that] offers help with a task that is beyond [one’s] abilities . . . what an individual cannot accomplish from their own initiative and efforts.”
In the United States, the disabled cannot be housed, work, marry, or receive education or health care because of our government. We should be removing barriers, not creating them.
In other parts of the world, universal health care and disability services are considered fundamental, nonpartisan systems. We must press on our “America First” lawmakers to see that, in this area, America is lagging far, far behind.
More importantly, we must uproot the harmful narratives that are at work in American minds and which motivate dehumanizing policies in the first place. We must speak openly in community and online about the dignity of disabled people. We must amplify disabled voices and make intentional efforts to include and accommodate disabled community members.
In short, we must follow the example of Jesus.
Madison Chastain writes about the body, faith, and culture. You can find more of her writing at madisonchastain.com, and on Instagram at @maddsienicole
Jesus’ Healing Miracles:
It’s About More Than Bodies
BY EMILY SANNA
The stories of Jesus healing people are some of the most famous in the gospels. But far too often, interpreters miss the point of these stories. They aren’t just about healing physical ailments, somehow “fixing” people who are broken and magically restoring them to wholeness. Instead, as Madison Chastain writes in an article for U.S. Catholic, when it comes to healing, “Jesus is primarily concerned with social outcasts who are separated from their communities because of their identities. By giving attention to a disabled person—and removing the obstacle to social belonging—Jesus returns each marginalized person back to their community.”1
The below examples show how, over and over again, Jesus uses healing in a way that is deeply tied to inclusion and community.
SIGHT RESTORED
Two of Jesus’ most famous examples of healing involve blindness. In Mark 10, Bartimaeus, a “blind beggar,” calls out to Jesus as he and his disciples pass by. While many people in the crowd tell him to be quiet, Jesus asks him what he wants. He doesn’t assume this man wants to be able to see; he waits and listens to the man’s wishes. Why should we, then, always assume that healing is what disabled people are seeking?
In John 9, Jesus heals a man blind from birth. He explicitly rejects the cultural belief that disability is a punishment for sin. Instead, he says, he was born blind “so the works of God might be made visible through him” (9:3). “We tend to assume this means the literal healing God provided,” Chastain writes. “But again, that’s an interpretation we place upon the text.” What if the works of God were the man’s own actions, something he could only contribute because of his lack of sight, not in spite of it?
PARALYSIS AND MOBILITY
In Mark 2, a paralyzed man is lowered through the roof of a crowded home so he can reach Jesus. The crowd is astonished, but Jesus focuses on the man himself: first forgiving his sins, then restoring his ability to walk. The story reminds us that healing isn’t just about physical restoration—it’s about full participation in community and society.
At the pool of Bethesda (John 5), a man who had been unable to walk for 38 years waits for healing. Jesus asks, “Do you want to be made well?” Again, he respects the man’s agency and invites participation rather than imposing a cure.
1 Madison Chastain, “Disabled Catholics deserve more than parish accessibility,” U.S. Catholic, November 25, 2024, https://uscatholic. org/articles/202411/is-the-catholic-church-ableist/
SKIN DISEASE AND SOCIAL OUTCASTS
In Mark 1, a leper approaches Jesus and is healed. Jesus reaches out, touching the man, defying social norms. Healing here is an act of inclusion, signaling that people who have been isolated and stigmatized are still worthy of dignity and physical connection.
HEARING, SPEECH, AND CHRONIC ILLNESS
In Mark 7, Jesus heals a man who is deaf and has a speech impediment. He places his fingers in the man’s ears, touches his tongue, and says, “Be opened.” The man’s senses are restored, but what’s more important is how Jesus shows attentive, physical, and relational care. Healing is not a spectacle for others; it is about honoring the person’s experience and capacity to engage with the world.
RAISING THE DEAD AND HEALING THE MENTALLY ILL
In other stories, Jesus raises the dead, as with Jairus’ daughter (Luke 8), and frees those suffering from mental illness or possession (Mark 5). These acts demonstrate that healing can restore not just bodies but life, relationships, and possibility itself. When society writes people off—whether through disability, illness, or stigma—Jesus’ example insists that every person’s dignity and potential must be honored.
MORE THAN PHYSICAL HEALTH
Across these stories, a pattern emerges: Physical healing must be relational and respectful. Jesus does not assume that everyone wants physical healing. Instead, he asks, listens, and works with the person. This reflects a profound ethic that challenges cultural and religious assumptions about disability, illness, and social value. Healing is about dignity, consent, and community; it does not merely involve a medical cure.
For modern readers, Jesus’ example offers a powerful lens for thinking about disability, social exclusion, and justice. True care does not demand conformity or “fixing” people to meet society’s expectations. It involves removing barriers, providing tools, and respecting agency, whether through health care, social support, or inclusive policies. Just as Jesus welcomed the marginalized, we are called to honor the full humanity of disabled people and ensure that society supports their rights, dignity, and participation.
THE WORK AHEAD
RECENT CUTS TO MENTAL HEALTH CARE PUT BOTH INDIVIDUALS AND FAMILIES IN DANGER
BY WENDY MAIMONE
CONTENT WARNING: This article contains discussion of mental health struggles, lack of access to care, and the real consequences these gaps have on individuals and communities.
My clinical experience has been in the realm of mental health, specifically acute mental health. I have worked as an intake clinician screening patients for a partial hospitalization program, as a social work case manager for people receiving inpatient mental health treatment, and as an emergency room social worker providing mental health assessments and substance use assessments. The bulk of the patients I work with have been so impacted by their mental health symptoms that they are no longer able to remain in the community, either functionally or safely. I’ve heard from many patients during our interactions that they are experiencing one of the worst days of their life.
I am always surprised at the number of people who are shocked to learn that a social worker can be Catholic. For me, the core beliefs of both the social work profession and the Catholic faith are very similar: humans’ autonomy and innate dignity, the importance of working together for the common good, services of the underserved, and the endless pursuit of peace.
My Catholic faith serves as the foundation of my social work practice, and it is how I work to support my community. It also serves as my solace when I worry about where we are heading as a community and as a country. As our government scales back programs and resources on which our most vulnerable populations rely, I find myself in a near constant state of fear for my community.
About eight years ago, while working as an intake clinician for a partial hospitalization program, I encountered a woman on Medicaid seeking treatment for her symptoms. Partial hospitalization programs are often a great alternative to inpatient treatment or serve as a transitional treatment after people are discharged from inpatient treatment. The program length depends on a person’s symptoms, but often people can expect to attend for up to 10 days. They come into the hospital for 6 hours a day where they learn coping skills to manage
their symptoms and meet with a psychiatrist for medication management. They then return home at the end of the day.
I distinctly remember this woman, even years later. She had been trying desperately for months to find outpatient treatment, both in the form of therapy and medication. The waiting lists for people with Medicaid were very long, as there wasn’t an abundance of providers. While she was on such a list, her symptoms began to increase. She began struggling to get out of bed to go to work. When she was able to go to work, she struggled to concentrate. She began to neglect her personal hygiene and was experiencing some suicidal ideation. The week prior to our meeting, the thoughts of suicide became a daily occurrence. The increase in suicidal ideation alarmed her, and she began looking for alternatives to outpatient treatment in order to begin treatment right away: hence our interaction.
After completing her assessment and determining that she met the criteria for the program, the next step was getting insurance authorization. However, after reviewing of the information and symptoms, her insurance determined that she did not meet the criteria; her symptoms were not “severe” enough. The insurance company felt that because she was still able to maintain employment and her suicide risk stratification was still considered low, partial hospitalization was not warranted at this time.
I can still remember the sounds of her sobs on the phone and her expressions of hopelessness when I had to tell her that we weren’t able to admit her into our program. At that time, there weren’t many programs in the area that took her insurance. Her only plan of action was to continue to wait for her outpatient appointment, still a month out, and to go to the emergency room should her symptoms and thoughts of suicide increase. Essentially, our health-care system told her that she didn’t qualify for help because things weren’t bad enough. And this was eight years ago, a time when there was considerably more access to mental health care resources for patients with Medicaid and Medicare.
This story sticks with me when I see the cuts in support of people’s basic needs, health care, and mental health treatment. More and more people on Medicaid and Medicare will
experience the same difficulties. The needless suffering that they will have to endure until their symptoms get “bad enough” is enough to take my breath away. Suicidal ideation alone can have severe consequences to a person’s emotional, cognitive, and behavioral health. Left untreated or not properly treated, a person can experience an increase in negative self-perception, social isolation, substance use, and cognitive impairment. They also run the risk of negative effects on their physical health, such as cardiovascular problems, a weakened immune system, and gastrointestinal issues. All because they need help and help isn’t readily available with their insurance. They can do nothing but sit with these thoughts, waiting for help to come in any form. And they suffer until it gets “bad enough.”
This is when being a Catholic gets hard for me as a social worker. We are taught to love others as God loves us, even if that means loving others who are actively harming your community— including those politicians who support and push for these cuts. For me, it’s easy to take a position of entitlement and look down on them as being wrong or even evil, because they don’t see the negative consequences of their actions. They don’t see people showing up in their places of work with lacerations to their wrists or detailed plans of how they are going to end their life. They don’t have to make a safety plan with families and ensure there are no weapons, firearms, or large doses of medication loved ones could potentially use to harm themselves. I can begin to feel utterly helpless, as though I’m fighting an uphill battle, and nothing’s going to change, because no one really cares anymore.
“All I can do is continue to show up and advocate from a position of humility for my patients and my community and pray that those in positions of power make decisions rooted in love and compassion…”
It’s at this moment that I have to let go and trust God. I’m not serving anyone or changing any minds by pointing out what others are doing wrong or looking down on them. All I can do is continue to show up and advocate from a position of humility for my patients and my community, pray that those in positions of power make decisions rooted in love and compassion, and try to find ways to reflect God’s love to others during the darker periods of their life. I hope in doing so that my patients are reminded that they are human beings of worth and value. And I pray that this will be enough as we move forward into the months ahead and the ramifications of these cuts.
Wendy Maimone is a clinical social worker living in East King County, Washington, where she balances her work with the beautiful chaos of raising two kids. She’s a lover of grandma hobbies, chihuahuas, her hedgehog, and finding small pockets of cozy joy in everyday life.
THE COST OF HEALTH CARE
About half of all adults say that it is difficult to afford medical care. Even among those with insurance, about 40% worry about affording their monthly insurance premiums, and 62% worry about affording their deductible before insurance kicks in.1
According to the Federal Reserve, in 2024 28% of adults skipped medical treatment because of the cost.
40% of adults have debt due to medical bills.2
The biggest health care companies and their annual revenue:
• UnitedHealth Group Inc.: $435.16 billion
• CVS Health Corp.: $394.08 billion
• The Cigna Group (CI): $268.22 billion
• Elevance Health (ELV): $194.82 billion
• Centene Corp. (CNC): $155.6 billion3
In 2023, the United States spent about $13,432 per person on health, almost double the average amount in comparable countries, according to the Peterson-KFF Health System Tracker.
In 2021, the United States spent almost 18% of its GDP on health care.
The United States is the only high-income country in the world that does not guarantee health coverage. According to the CDC, in 2025 about 8% of the population was uninsured—about 27.5 million people. This number was the highest (about 25%) for people earning less than 2x the federal poverty level.
ourteen years ago, on my last day of kindergarten before Thanksgiving break, I stepped out of my father’s car and straight into a sinkhole. My small body was scraped and bruised, and when my dad pulled me out, he did the only thing he could in that moment: He patched me together with Scotch tape and scraps of paper from his glove compartment. He asked me to be brave and go to the school nurse.
As I watched him drive away, I burst into tears, not only from pain but from wanting to be held. It took years for me to understand why he reacted that way. He was working two jobs, and we relied on food stamps; we had no health insurance. His fear was not only for my injuries but for the medical bill he knew our family could not afford if he missed even a single shift.
This past summer, 14 years later, I found myself in almost the same situation. After passing out one afternoon, I woke up with a fever of 105 degrees. For the first time since childhood, I was uninsured again, this time because my father had lost his job to cancer. I was living more than 300 miles from my parents, completely on my own, and the only medical provider in reach was a single for-profit hospital.
For days, I tried to convince myself I was not sick enough to go to the doctor. I did not have money for an Uber, much less a hospital bill. Eventually, my symptoms became too severe to ignore, and I took a bus across town, dragging myself into the waiting room.
Inside, every seat was filled. Mothers held their children in their laps, because there were not enough chairs. Staff had propped the main door open with a phonebook, because the line of patients stretched all the way to the entrance. In the emergency room, I overheard people talking about how many of them had traveled from counties with no hospitals at all. Many people had Medi-Cal, a California state-provided health insurance for lowincome people, yet they had still been waiting for hours.
I sat in a plastic chair, dehydrated and shaking, crying from fear and loneliness until a staff member called someone to be with me. Hours passed. My IV bag ran dry more than once before anyone noticed. When a doctor finally located my chart in a pile of others, he told me I had severe sepsis and that if I had waited any longer, I would have died.
My first feeling was not relief that I would live but dread. I thought about the cost. I thought about my family. I worried about losing my job. I wondered how I was supposed to build a future when a single medical emergency could bury us
TO THE BREAKING POINT
AWAY FROM IMPOSSIBLE FINANCIAL CHOICES
“The truth is that most young people are one illness, one missed paycheck, or one family crisis away from facing the same impossible choices.”
financially. In that moment, the fear of the bill pressed on me almost as heavily as the diagnosis.
This experience forced me to see clearly how deeply healthcare policy shapes ordinary life. When coverage is cut and clinics close, people are pushed into impossible decisions. No one should have to fight for their life and simultaneously wonder how much that fight will cost. People go to work sick because they cannot afford to lose their hourly wages. They put off taking themselves or their children to the doctor, because even the cost of transportation feels out of reach. They hope their symptoms will disappear. They wait until they collapse at school or work. Parents go without their own medication so their kids can be treated. These are not abstract policy debates. They are daily realities that determine whether people get to grow up, stay healthy, or stay alive.
Young adults especially live at the crossroads of instability and responsibility. Many of us are students, working jobs with no benefits, or supporting family members whose health depends on programs constantly under threat. When insurance becomes unaffordable or disappears entirely, we are the ones most vulnerable to falling through the cracks. And because we have the longest futures ahead of us, we are the generation that will feel the consequences of today’s decisions long after the lawmakers responsible for them have moved on.
My story is just one example of what happens when a system is stretched to its breaking point. The truth is that most young people are one illness, one missed paycheck, or one family crisis away from facing the same impossible choices. When health-care systems weaken, the results are not just higher co-pays
or longer lines. There are people rationing medication. There are people delaying care until it is too late. There are people dying alone in overcrowded hospitals, wanting nothing more than to be held.
Speaking up is not about politics. It is about survival, stability, and dignity. It is about fighting for a future in which getting sick does not mean risking everything we have.
Mia Isabel Lazo is a student researcher and social justice advocate with NETWORK. Her work bridges the topics of environmental and human health, focusing on antibiotic resistance in urban watersheds, and ensuring that all people have access to services that enable them to live a free and just life. A first-generation American and college student navigating policy and injustices, she writes and advocates about the urgent need for accessible, community-centered health policies. She hopes to pursue a career that bridges science, public health, and social justice.
THE MORAL STAKES OF PROTECTING PUBLIC HEALTH PROGRAMS
HEALING AS HOLY WORK
BY ERICA TORRES
Women religious communities’ health care ministry began long before modern-day hospital systems or health insurance companies that we see and experience today. Their mission is grounded in concrete experiences, a deep understanding of what happens when people are unable to receive adequate care, and an unrelenting commitment to upholding the dignity of all people.
One of the pioneers in health care access was Margaret Anna Cusack, later known as Mother Francis Clare, who was born in Dublin, Ireland in 1829. She didn’t set out to found a healthcare system; her mission was to confront the suffering she saw around her that she believed to be both avoidable and unjust. And yet, her ministry—and her conviction that charity alone can never address the root causes of illness and poverty—has had lasting impacts on Catholic health care and the entire health care system today.
After converting to Catholicism in her late 20s, Cusack became a Poor Clare Sister and was sent to Kenmare, Ireland, to help found a convent there. It was here in Kenmare that she started working for a more equitable society through public ministry. She experienced first-hand the effects of famine, poverty, and the oppression of women and children and dedicated her ministry to feeding the hungry while also fighting for housing rights, education, and for the rights of women.
“If Mother Francis Clare were alive today, she would remind lawmakers that systems that deny care to the poor violate both justice and peace. The well-being of the sick is not expendable; it cannot be simplified to some budgetary line item that can be struck for the sake of saving money.
Eventually, she founded her own community: The St. Joseph’s Sisters of Peace.
Mother Clare was also a prolific writer; many of her books addressing the realities of injustice and calling the church to accountability and action are still available today. It’s evident from both her writing and her work that she understood public health in a strikingly holistic way: as inclusive of not only medical care but also safe housing, adequate wages, education, and equal access.
Across the Atlantic Ocean, at roughly the same time, another woman religious was also building a health-care ministry. Esther Pariseau, later known as Mother Joseph of the Sacred Heart, was born in 1823 in Quebec, six years before Mother Francis Clare. Like Mother Francis Clare, she also entered religious life in her 20s, joining the Sisters of Charity of Providence.
Ten years later, she was sent to what is now Vancouver, Washington to serve in the mission diocese there. Over the
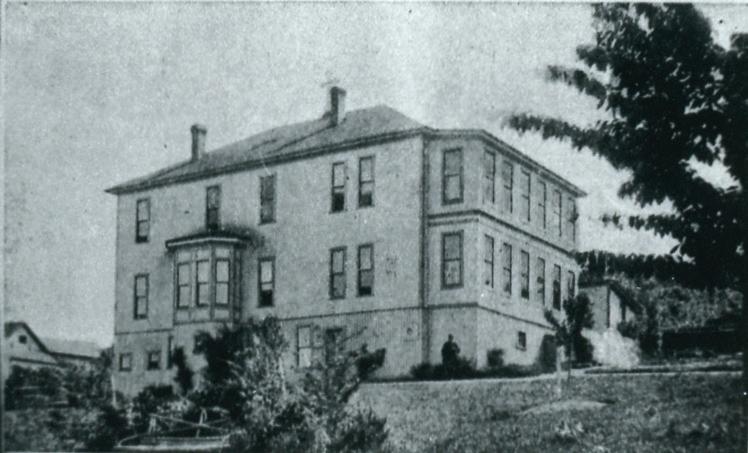
Article photos: Archive of the Congregation of the Sisters of St. Joseph of Peace with permission.
Page 10 left: The first permanent hospital in the Pacific Northwest, 1858, St. Joseph Hospital Vancouver, Washington
Page 10: Original St. Joseph Hospital, Fairhaven (Bellingham), undated.
Below: Second St. Joseph Hospital at Forest Street, undated.
Page 11: Margaret Anna Cusack, “Mother Francis Clare” Circa 1884.
ensuing decades, she played an instrumental role in the area, planning and building some of the area’s first schools and hospitals. Under her leadership, the order founded the Northwest’s first school of nursing in 1892. She helped found and build 17 hospitals, all of which—at least in 2022—continued to operate in some form. Her community also introduced the “Providence ticket,” an early form of health insurance that guaranteed hospital coverage for a fee of $10 per year.
Mother Francis Clare and Mother Joseph of the Sacred Heart are just two examples of how, for generations, Catholic sisters have served as the backbone of American health care. Long before the development of federal safety net programs and before hospitals evolved into complex medical systems, women religious recognized healing the sick as a moral and theological act.
THE SISTERS OF ST. JOSEPH OF PEACE
One way the legacy of these women endures today is through the PeaceHealth system, a not-for-profit health-care system with medical centers, critical access hospitals, and medical clinics located in Washington, Oregon, and Alaska.
In 1890, two Sisters of St. Joseph of Peace—Mother Francis Clare’s community—left their convent in New Jersey to go to the far northwest corner of Washington. Their goal was to build a hospital to care for the loggers, mill workers, fishermen, and
their families that lived in the area. This one hospital grew over time to include medical facilities in Alaska, British Columbia, and Oregon.
Now, more than 120 years later, their ministry continues. In the 1970s, the sisters formed a separate organization to oversee their medical services and in 1994, this became PeaceHealth. The mission, however, is the same as that of Mother Francis Clare and the two sisters who originally brought this mission to the Pacific Northwest: to provide medical care to all who need it and with the understanding that medical care and social justice are integrally connected.
THE PROPHETIC WITNESS OF WOMEN RELIGIOUS
Understanding this history helps us see the moral dimensions of modern policy debates, like the proposed cuts to Medicaid, Medicare, and other public health programs. More than 200 years ago, women religious knew that poverty worsened illness and that the lack of health care devastated families. They understood that health is not a luxury, but rather a human right grounded in the inherent dignity of every person. Somehow, we have lost this understanding today.
If Mother Francis Clare were alive today, she would remind lawmakers that systems that deny care to the poor violate both justice and peace. The well-being of the sick is not expendable; it cannot be simplified to some budgetary line item that can be struck for the sake of saving money. Health care access is a moral and spiritual issue, not merely a political one.
Catholic health care did not begin as a corporate enterprise; it began as a spiritual movement. It was animated by a belief that every person carries the divine image, and that caring for the sick is to touch that sacred presence. Mother Francis Clare shaped a community whose identity rests on the inseparability of healing and justice. Their charism continues in organizations like PeaceHealth, where commitments to charitable care, community health initiatives, and service to rural and underserved regions are not strategic choices but moral imperatives.
Their ministry reminds us that healing is holy work—work that requires just structures, compassionate systems, and the courage to protect the vulnerable. As public health debates intensify, Catholics are called not to neutrality but to advocacy grounded in our values.
To defend strong and accessible health-care systems is to walk in the footsteps of the sisters who built them—women who believed with their whole hearts that peace comes through justice, and that justice demands that every person receive the care they need to flourish.
Erica Torres, PsyD, System Vice President of Mission Integration, PeaceHealth.
Health Care Access in the United States
2021–2022
For two years during the COVID-19 pandemic, the American Rescue Plan Act (ARPA) afforded financial support for individuals buying their own health care insurance through the Affordable Care Act’s health care marketplace.
Enrollment ceremony for H.R. 1319, the American Rescue Plan Act, Congress signed the bill to send to President Biden’s desk and deliver big, bold, urgent COVID relief to Americans, U.S. Capitol in Washington D.C., Wednesday, Mar. 10, 2021. Wikimedia Commons.
2022
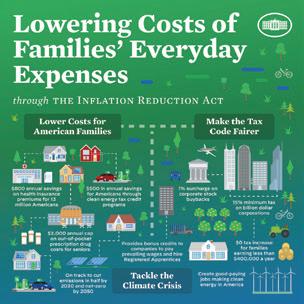
The Inflation Reduction Act (IRA) extended these enhanced health care subsidies through the end of 2025.
Together, the ARPA and IRA doubled the number of people enrolled in ACA marketplace insurance, from 11.4 to 24 million. This expansion increased insurance coverage for people who don’t qualify for Medicaid and are not eligible for employer-sponsored coverage. The non-renewal of these subsidies is expected to double insurance prices and increase the number of uninsured to 10 million people by 2034.
The IRA also authorized the federal government to phase in negotiated Medicare prices for commonly used expensive drugs that have no generic competitor. Starting in 2025, the prices for the negotiated drugs are expected to decrease prices by approximately 40 to 80 percent.
OVER THE PAST FIVE YEARS, THE U.S. GOVERNMENT HAS PASSED SEVERAL BILLS THAT IMPACT ACCESS TO HEALTH CARE
2025
The One Big Beautiful Bill Act enacted $4.5 trillion in tax cuts, predominantly to benefit higher-income households and offset by deep Medicaid cuts.
The bill cuts the total U.S. health care budget by $1.1 trillion, with 75 percent of these cuts coming from Medicaid, 24 percent from policy changes in ACA marketplace insurance, and 1 percent in Medicare cuts.
The majority of the Medicaid cuts result from: changes in work requirements, increasing barriers to enrolling in or renewing Medicaid, and cuts that apply only to states that adopted ACA expansion.
The Medicare cost cuts result from restricting coverage for immigrants legally in the United States.
Despite a $50 billion increase in the Rural Health Transformation fund, rural hospitals will be hit hardest, with over 300 rural hospitals at risk of closing.
Immigrant Health Care Access in Washington
Data from the Washington Immigrant Solidarity Network Deportation Defense Hotline shows that many immigrants in Washington continue to face significant barriers to health care. In 2024, 38 percent of callers reported having no health insurance, and among more than 2,600 callers who completed demographic surveys since 2022, many reported chronic illnesses or disabilities.1
Washington Immigrant Solidarity Network Deportation Defence
Hotline 2022–2024, 1,612 of 2,600 of immigrant callers are uninsured and many reported chronic illness or disabilities.1
These challenges highlight the continued need for policies that increase access to health care for immigrants, such as the Apple Health Expansion (AHE), Washington State’s effort to provide state-funded health-care coverage to income-eligible residents regardless of immigration status.
AHE is designed to provide basic medical coverage, preventive care, and treatment for chronic conditions for people who are otherwise excluded from federal programs. Ongoing funding is necessary to maintain existing coverage and meet the high levels of need reflected in these hotline data.
Medical Neglect in ICE Detention: The Case of “Kuya G”
In March 2025, Filipino Green-Card holder Greggy “Kuya G” Sorio was detained by U.S. Immigrations and Customs Enforcement (ICE) and held at the Northwest Detention Center in Tacoma, where he experienced prolonged medical neglect, including a bone infection that led to the amputation of his toe and a diagnosis of ulcerative colitis requiring continuous treatment.
His case escalated in December, when ICE attempted to deport him despite 18 pages of medical documentation showing he was unfit to travel. Only minutes before takeoff, an airline medical review halted the removal, which was the result of tireless organizing and activism on the ground. His experience reflects wider patterns of inhumane treatment in ICE facilities. 2025 marked the deadliest year in two decades for people in ICE custody, with 32 deaths reported nationwide in addition to widespread instances of preventable fatalities linked to untreated illness, poor oversight, and inadequate medical care in overcrowded facilities. Advocates and medical reviewers have repeatedly identified substandard treatment, including preventable deaths from seizures, heart failure, respiratory illness, and suicide.1
2025 marked the deadliest year in two decades for people in ICE custody, with 32 deaths reported nationwide in addition to widespread instances of preventable fatalities linked to untreated illness, poor oversight, and inadequate medical care in overcrowded facilities.
Kuya G’s case exemplifies how serious health conditions can worsen in detention, underscoring documented systemic failures in medical oversight throughout ICE’s expanding national detention network.
If you’d like to support or learn more about the Tanggol Migrante Movement (Defend Migrants Alliance) or to be involved, go to https://www.tanggolmigrante.org
1 2025 was ICE’s deadliest year in two decades. Here are the 32 people who died in custody | ICE (US Immigration and Customs Enforcement) | The Guardian
Reflection
When Jesus heals someone, He not only eradicates the physical ailment from the body, but also restores dignity, reintroducing him or her into society, giving a new life. Of course, only He can do this, but the attitude, the approach toward the person is a model for us. A holistic view of care helps counter the “throwaway culture” which excludes those who, for various reasons, do not meet certain standards. This is a culture of today, of discarding. That which does not work is thrown out: use and discard on all levels. In a society that is in danger of seeing the sick as a burden, a cost, we need to restore to the centre what is priceless and cannot be bought or sold, that is, the dignity of the person. Illnesses may mark the body, confuse thoughts, take away strength, but they can never nullify the value of human life, which must always be protected, from conception to its natural end. I hope that research and the various health professions will always have this outlook. . . .
Even in the field of healthcare a common temptation is to make the economic or political interests of one group prevail at the expense of the majority of the population. . . . The fundamental right to healthcare, “pertains to the value of justice, whereby there are no distinctions between peoples and ethnic groups, taking into account their objective living conditions, and stages of development, in pursuing the common good, which is at the same time the good of all and of each individual.” . . . It is necessary to work to ensure that everyone has access to care, that the healthcare system is supported and promoted, and that it continues to be free of charge. Cutting healthcare resources is an outrage against humanity.
—Pope Francis (Address to Members of the Federsanità Confederation, June 2022)
Questions for Reflection:
n Pope Francis highlights the “holistic view of care” and the importance of restoring dignity. How can you, in your own community or parish, reflect this model of care for those who are marginalized or uninsured?
n Pope Francis speaks about ensuring the health system “continues to be free of charge.” How does this vision shape how we think about public versus private responsibility for care in our society?
n How does the idea of a “throwaway culture” challenge your understanding of the gospel’s call to love and protect all life, from birth to natural death?
n How do systemic inequities in the U.S.—like geographic, racial, or economic disparities—show that health care is still treated as a privilege rather than a right?
n What role does prayer, advocacy, or community action play in upholding the value of human life when systemic barriers exist?
n What concrete steps can individuals or faith communities take to address gaps in access, whether through advocacy, education, or direct service?
LOOKING BACK
. IPJC Community Assembly
More than 200 Catholic leaders representing more than 50 communities gathered for a powerful event focused on relationship building, leadership development, prayer, and collective action. The community engaged in more than 800 one-to-one relational meetings, 30 conversations in the Spirit, (pictured right), nominated over 150 women to IPJC’s new Women’s Leadership Team, and made a commitment to mobilize 1,000 people for immigration justice during the month of March. When we come together, we are powerful!
LOOKING FORWARD
. . . Town Hall - Thriving Together: Care, Community, and Creation Saturday, March 7, 10–11:30 a.m. Seattle University Student Center
Led by IPJC’s Youth Action Team and Seattle University students, the community will share a vision for a flourishing in King County with King County Council representatives. Learn more and register here: https:// ipjc.or g/ thriving-together-townhall-registration/
NW Ignatian Advocacy Summit
March 5–7
Seattle University & Bellarmine College Preparatory
IPJC is excited to cohost and organize the fourth annual NW Ignatian Advocacy Summit! Join more than 65 youth from throughout the PNW region for two evenings of storytelling and relationship building and a community town hall on Saturday morning. Learn more and register here: https://www.jesuitswestcore.org/ nw-summit-adults-info
by Paul Dehmer unless noted.
Women’s Leadership Team
Over the next few months, IPJC will be forming a new leadership team responsible for conducting a robust listening campaign in the community. The campaign will inform the formation of a new strategic plan as well as identify the center’s priority issue areas into the future. If you are interested or would like to nominate a woman for the team, please reach out to IPJC’s lead organizer, Mattie Gottbrath (mgottbrath@ipjc.org)
The Way of the Cross:
Immigration Stations of the Cross
Monday, March 30, 6 p.m.
Location TBD
Intercommunity Peace & Justice Center
Earth Summit Laudato Si' Movement
Washington State Chapter Saturday, April 25 I 9 a.m.–4 p.m. Seattle University
IPJC Spring Benefit: “Spark Hope” Thursday, May 14 | 6:30–8:30 p.m.
St. Catherine of Siena School, Seattle
As has become our practice, We will host our annual stations of the cross connected to the current immigration injustices our community is experiencing. This year we will be partnering with several other Catholic communities and the Youth Action Team to bring our ritual into the public and participate in the “Season of Faithful Witness,” a national effort to mobilize Catholic communities to stand of dignity and justice in the public sphere. Please consider joining us!
Donations
IN MEMORY OF Mary Fran Barkshire
If you would like to honor a loved one, you may note with a
Intercommunity Peace & Justice Center
1216 NE 65th St Seattle, WA 98115-6724
SPONSORING COMMUNITIES
Adrian Dominican Sisters
Congregation of the Sisters of St. Joseph of Peace
Jesuits West
Sisters of the Holy Names of Jesus and Mary, U.S.-Ontario Province
Sisters of Providence, Mother Joseph Province
Sisters of St. Francis of Philadelphia
Tacoma Dominicans
AFFILIATE COMMUNITIES
Benedictine Sisters of Cottonwood, Idaho
Benedictine Sisters of Lacey
Benedictine Sisters of Mt. Angel
Dominican Sisters of Mission San Jose Dominican Sisters of Racine
Dominican Sisters of San Rafael Sinsinawa Dominicans
Sisters of Charity of the Blessed Virgin Mary Sisters of St. Francis of Redwood City Sisters of St. Joseph of Carondelet Sisters of St. Mary of Oregon Society of the Holy Child Jesus Sisters of the Holy Family
Sisters of the Presentation, San Francisco Society of Helpers
Society of the Sacred Heart Ursuline Sisters of the Roman Union
EDITORIAL BOARD
Don Clemmer
Cassidy Klein
Will Rutt
Editor: Emily Sanna
Copy Editor: Cassidy Klein
Design: Sheila Edwards
A Matter of Spirit is a quarterly publication of the Intercommunity Peace & Justice Center, a 501(c)3 nonprofit organization, Federal Tax ID# 94-3083964. All donations are tax-deductible within the guidelines of U.S. law. To make a matching corporate gift, a gift of stocks, bonds, or other securities please call (206) 223-1138. Printed on FSC® certified paper made from 30% post-consumer waste.
O God, you are life, source of all that is. By your word you brought forth sun and moon, stars and planets, plants and every green thing, animals and all that has breath. By your wisdom you evolved our fragile home through the millennia. By your mercy you sustain your creation, today and everyday.
In one particular time and place, you made yourself known to us in Jesus, whose ministry took him to the margins. In a spirit of mercy and holy rebellion, Jesus reached across boundaries and healed by his touch, restoring life and life abundant to those who had been cut off from community.
Your healing is known across all faiths and among all cultures. So inspired by the great love you have shown us, make us agents of that same holy rebellion–the divine obedience that manifests your love and mercy for all whom you have created.
Bless the work of our elected officials and the ministry to which you have called them. Remind them of the communities they have promised to serve, and inspire them to strive for justice, especially for those most vulnerable, that all may have access to quality health care, and so all may be strengthened in body and spirit to serve your planet and your people.
Send us forth with your blessing, to be a blessing to all we meet, to receive blessing from those we least expect, to bear one another’s burdens, and to love, fiercely and unapologetically; in the strong name of the Holy One to whom we pray. Amen.
Source: Adapted from the Social Justice Resource Center (https://socialjusticeresourcecenter.org/ prayers/health-care-prayers/)