Understanding Stem Cell Transplant in Myeloma
The IMF InfoLine team is here to support you and your loved ones with the most up-to-date information about myeloma
Call the IMF InfoLine at 1.800.452.CURE (toll-free in the U.S. & Canada) or 1.818.487.7455 (worldwide), or email InfoLine@myeloma.org with your questions, or if you wish to discuss the contents of this booklet.
Want answers and don’t want to wait?
Get the answers you need anytime from Myelo® , your 24/7 generative AI assistant that is designed to support you living well with myeloma. Ask Myelo your questions at myeloma.org.
Join the Myeloma Knowledge Platform Visit myprofile.myeloma.org and create your online IMF account to receive the most helpful content recommendations tailored to support your personal myeloma experience.
You are not alone
The International Myeloma Foundation (IMF) is here to help you. We are committed to providing information and support for patients with multiple myeloma (which we refer to simply as “myeloma”) and their care partners, friends, and family members.
The IMF supports the myeloma community with a broad range of resources available on our website myeloma.org, and through numerous programs and services such as publications, seminars, webinars, workshops, and the IMF InfoLine.
The IMF InfoLine responds to your myeloma-related questions and concerns in a compassionate and caring manner. To receive the most up-to-date information about myeloma, call 1.818.487.7455, email InfoLine@myeloma.org, or schedule a convenient time to talk with an IMF InfoLine Coordinator at mmsm.link/infoline.
IMF publications
Myeloma is a cancer that is not known to most patients at the time of their diagnosis. If you have been diagnosed with myeloma or if you suspect that you might have myeloma, the IMF can help you become well-informed about this disease so that you can have an active role in your own medical care and make good decisions about your care in partnership with your medical team.
We suggest that you read the IMF’s Patient Handbook, an introductory overview of myeloma diagnosis, risk stratification, effects on the body, as well as treatment options and key supportive care measures approved by the U.S. Food and Drug Administration (FDA). This booklet will also direct you to other resources that may be relevant in your particular case.
The IMF’s Understanding-series publications are intended to offer more detailed information about a broad range of myeloma-specific topics, including drugs and drug regimens, and the symptoms and the side effects of both myeloma and its treatments. All IMF publications are free-of-charge and can be read, downloaded, or requested in printed format at publications.myeloma.org.
Understanding myeloma vocabulary
Words in bold+blue in IMF publications are explained in a companion booklet, Understanding Myeloma Vocabulary. Myeloma is a complicated disease, but the language that describes it doesn’t have to be hard to understand. You can access the electronic edition of this booklet at glossary.myeloma.org.
If you prefer to access any of the IMF’s publications or resources in electronic format, the light blue links will take you there.
What you will learn from this booklet
This booklet is written primarily for people with myeloma who are being treated in the United States and are in discussion with their doctor about the possibility of having an autologous stem cell transplant (ASCT) as part of their overall treatment strategy. You will learn about the typical process of ASCT for a transplant-eligible myeloma patient, and the information provided may be helpful to your decision-making. For links to additional resources, visit myeloma.org/online-resources/transplant .
Rationale for ASCT in myeloma
The medical term for ASCT is “high-dose therapy (HDT) with stem cell rescue.” In myeloma, the use of HDT was introduced in the 1990s. The novel treatment options for myeloma that were approved by the FDA in the 2000s led to improved outcomes in ASCT-eligible patients. More recently, the use of newer therapies throughout the disease course has significantly improved outcomes, including the efficacy of ASCT.
The overall strategy for patients with myeloma is to have as many treatment options available to them as possible, both short-term and long-term, in order to pursue the treatment option most likely to attain a deep and durable response or remission (interchangeable terms to describe the complete or partial disappearance of the signs and symptoms of cancer). You can learn more about how response is assessed by reading the IMF Patient Handbook.
ASCT is one of the treatment options to consider for patients with myeloma. You should discuss and compare the benefits and risks of all options available to you with the doctor treating your myeloma. ASCT can improve the depth of response to treatment and the duration of remission; known as progression-free survival (PFS), the length of time during and after the treatment of myeloma that a patient lives with the disease but the myeloma does not get worse. Although the rates of PFS may be improved with ASCT, the rates of overall survival (OS) are the same with or without transplant. OS is the amount of time from diagnosis or start of treatment until death from any cause. As myeloma treatment options become more effective, the length of OS duration continues to increase.
However, even if you are a good candidate for a specific treatment approach – such as ASCT – there are always many factors to consider and the ultimate decision is always for the patient to make. This is why it is so important to seek an opinion – or a second opinion – from an experienced myeloma specialist.
The importance of consulting with an expert
Myeloma is a highly individualized disease. Do NOT compare your myeloma to that of other patients, as each patient’s myeloma has its own distinct characteristics. Myeloma specialists at large “high-volume” treatment centers or academic institutions care for hundreds of myeloma patients, conduct clinical trials with novel myeloma therapies, and develop the expertise needed to help guide the optimal treatment strategy for your unique case of myeloma.
If an in-person consultation with a myeloma expert cannot be arranged, you or your doctor can schedule a consultation as a video or telephone call. This is a common practice, and the IMF InfoLine can help you identify one or more such specialists. Your goal is to gain a clear understanding of your options so that you can proceed with confidence.
ASCT decision-making Assessment
Eligibility criteria for ASCT varies among institutions. In 2014, the IMF’s International Myeloma Working Group (IMWG) published a consensus statement, which concluded that the arbitrary age of 65 is no longer sufficient to define whether a patient is eligible or ineligible for ASCT. Physiological age is a more important factor than chronological age. General fitness; concurrent illnesses; and function of the kidneys, heart, lungs, and liver are also part of the evaluation to determine appropriate treatment.
In the U.S., there is no upper age limit set in the Medicare National Coverage Determination for ASCT in myeloma, and the Centers for Medicare & Medicaid Services (CMS) have now removed the upper age limit on coverage, leaving the question of eligibility to the patient’s doctor and the Medicare administrative contractor within the patient’s jurisdiction. Visit cms.gov/Medicare/Coverage/DeterminationProcess for more information or speak with your healthcare team.
ASCT is an option for most myeloma patients upon completion of frontline therapy, the initial treatment used in an effort to achieve response in a newly diagnosed patient. But decisions regarding ASCT should be made based on a risk-benefit assessment. You and your doctor must consider all the relevant myeloma-related factors, including the following:
¡ Confirm your diagnosis of myeloma and if your disease is active and if it requires treatment.
¡ Discuss your response to prior treatments, as well as your current range of treatment options and their potential risks and benefits.
¡ Myeloma patients who have no minimal residual disease (MRD) after frontline therapy, have improved OS whether they have undergone ASCT or not.
¡ Your test results, such as beta-2 microglobulin (β2-microglobulin, β2M, or β2M), serum albumin, and any chromosomal abnormalities that might indicate that you have high-risk multiple myeloma (HRMM), disease that is more likely to relapse quickly after treatment. To learn about tests used to monitor and assess myeloma, read the IMF’s publication Understanding Your Test Results.
Patient-related factors to discuss with your doctor include your personal, professional, and financial situations.
Timing
Ask your doctor about the optimal timing for your ASCT. Many transplant doctors favor performing ASCT as part of frontline therapy because this produces a better quality of life (QoL) and higher rates of sustained PFS (sPFS) and MRD-negativity. But there is also evidence that if a patient has a deep response to induction therapy (explained on the next page), stem cells can be collected and frozen for an ASCT performed at the time of disease relapse.
Chemotherapy
Chemotherapy is the use of drugs to kill cancer cells. HDT is more effective at eradicating myeloma cells from the bone marrow than standard-dose chemotherapy. But any treatment that reaches the bone marrow to kill myeloma cells is also capable of damaging normal stem cells.
If your doctor recommends ASCT, then your initial therapy should be with drugs that don’t damage your normal stem cells prior to harvesting. For example, therapy with Revlimid® (lenalidomide) for more than 4 cycles may impair stem cell collection.
Preparing for the experience of ASCT
You should feel comfortable and reassured before you begin your ASCT process. You can do a lot to get ready for your ASCT. The IMF has a library of publications about the therapies used for the treatment of myeloma at every stage of the disease. All are free-of-charge and can be downloaded or requested in printed form at publications.myeloma.org.
Ask your doctor any questions you may have. Some transplant centers may pair you up with a fellow patient who has been through the ASCT process and can share their experience with you. If possible, bring a friend or a family member to your doctor appointments so that they can help take notes, and ask your doctor to provide an “after-visit summary.”
Share what you learn with your loved ones so that they know what to expect – and how they can best help in the weeks and months ahead.
Your transplant center and team
Ask your doctor whether you will receive treatment on an inpatient or outpatient basis. Visit the transplant center and see the rooms where the ASCT process and recuperation would take place. If the transplant center location is far from your home, visit the accommodations where you will stay. Many transplant centers have accommodations nearby or can help you find suitable accommodations.
Ask to meet your myeloma transplant team in advance – the doctors, nurses, social workers, psychologists, and allied healthcare professionals. This will help you know who’s who, as well as what resources are available to you and your care partners. ASCT is a complicated medical procedure and you want your transplant team to have both experience and expertise.
Support resources
Having a support network is very important. ASCT can place overwhelming stresses on patients and their loved ones before, during, and after the procedure. We urge you to take advantage of the support resources offered through your hospital, the IMF InfoLine and support groups, and through other patient-centric organizations. Ask your doctor about the benefits of psychological counseling or psychiatric consultation.
The process of ASCT in myeloma
Induction therapy
Induction therapy is the initial treatment given to a patient in preparation for an ASCT. Depth of response after induction therapy is generally thought to influence the depth of response after ASCT. However, even lesser degrees of response to induction therapy may be sufficient for effective stem cell collection. After each treatment Cycle, ask your doctor about your response to induction therapy and if proceeding to ASCT continues to be the doctor’s recommendation.
Patients have many options for induction therapy prior to ASCT. Previously, triplet (3-drug) regimens had been considered the standard-of-care (SOC) for most patients with myeloma. More recently, the FDA has approved quadruplet (4-drug) regimens that validate the complex biology of myeloma, which can be better controlled with multiple drugs that have different mechanisms of action (MoA), the process through which a drug induces its effect in the body.
FDA-approved induction therapies
The triplet combinations below are listed in alphabetical order.
¡ Kyprolis® (carfilzomib) + Revlimid® (lenalidomide) + dexamethasone [KRd]
¡ Velcade® (bortezomib) + Revlimid + dexamethasone [ VRd]
The quadruplet combinations below are listed in alphabetical order.
¡ Darzalex Faspro® (daratumumab + hyaluronidase-fihj) + KRd [DKRd]
¡ Darzalex Faspro + VRd [DVRd]
¡ Sarclisa® (isatuximab-irfc) + KRd [Isa-KRd]
¡ Sarclisa + VRd [Isa-VRd]
NCCN-listed induction therapies
The National Comprehensive Cancer Network (NCCN) Guidelines for Myeloma include the following induction therapies.
¡ Revlimid + dexamethasone [Rd],
¡ Velcade + cyclophosphamide + dexamethasone [ VCd or CyBorD],
¡ Velcade + Adriamycin® (doxorubicin) + dexamethasone [PAd],
¡ Ninlaro® (ixazomib) + Revlimid + dexamethasone [IRd].
The NCCN Guidelines include the following induction therapies as “useful in certain circumstances.”
¡ Velcade + dexamethasone [ Vd],
¡ Velcade + thalidomide + dexamethasone [ VTd],
¡ Darzalex + VTd [DVTd],
¡ VTd + cisplatin + doxorubicin + cyclophosphamide + etoposide [ VTd-PACE].
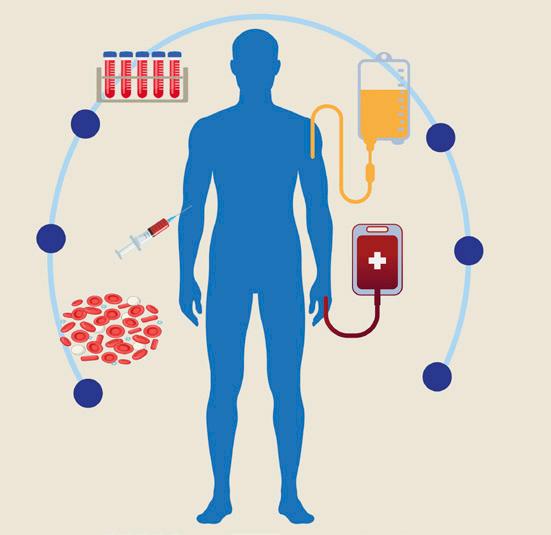
1. The ASCT process
1. Induction therapy is given to prepare the patient for ASCT.
2. Stem cells are mobilized from the bone marrow into the bloodstream.
3. Stem cells are collected from the bloodstream, frozen, and stored in a laboratory.
4. The patient is treated with high-dose chemotherapy to kill remaining cancer cells.
5. Stem cells are thawed and infused back into the patient through a vein.
6. Stem cells travel to the bone marrow and begin producing new blood cells.
Figure
Stem cell collection before HDT
Your stem cells will be harvested through a process called apheresis, which uses a machine to collect stem cells from the bloodstream while the other blood components are immediately returned to you. Apheresis is usually done as an outpatient procedure for 1 to 5 days, lasting from 3 to 4 hours each day. One the following protocols may be used prior to harvesting your stem cells:
1. You will be given injections with a colony-stimulating factor (CSF) to stimulate the development and growth of blood cells, and to mobilize your stem cells from the bone marrow into your bloodstream. Daily injections are followed by daily harvesting of stem cells until a sufficient quantity is collected.
2. You will receive CSF plus chemotherapy. The most commonly used drug to enhance the release of stem cells from the bone marrow into the bloodstream is cyclophosphamide, but there are other drugs that can be used instead. Ask your doctor about potential side effects.
3. You will receive CSF plus a mobilizing agent, a drug to trigger the release of stem cells into the bloodstream. This is particularly helpful for patients who have difficulty generating enough stem cells for harvesting. In 2008, the FDA approved Mozobil® (plerixafor) for stem cell mobilization in combination with a growth factor. In 2023, the FDA approved Aphexda® (motixafortide) to mobilize hematopoietic stem cells for ASCT in combination with filgrastim.
Next, the collected stem cells are taken to a laboratory, where they are frozen in liquid nitrogen and stored at a temperature of –80°C (–112°F). Excellent function of stem cells is retained for at least 10 years.
Note: Scientific evidence indicates that “purging” myeloma cells from the harvested stem cells is not effective in ASCT for myeloma.
High-dose therapy
When you are ready to proceed with ASCT, your doctor will try to first reduce your level of monoclonal protein (myeloma protein, M-protein) by at least 50% by using HDT, which destroys myeloma cells in the bone marrow where they grow. HDT is more effective at eradicating myeloma cells from the bone marrow than standard-dose chemotherapy. However, any treatment that reaches the bone marrow to kill myeloma cells also damages your normal stem cells. The most common type of HDT used in myeloma is melphalan, administered at a dose of 200 milligrams per square meter (mg/m2) of body surface area (size of patient).
Medications are given to prevent or lessen the anticipated side effects of HDT. Common side effects of HDT include nausea, vomiting, diarrhea,
mouth sores, skin rashes, hair loss, fever or chills, and infection. Patients are monitored very closely during and after the administration of HDT, including daily measurement of weight, blood pressure, heart rate, and temperature.
Stem cell rescue
Approximately 36 to 48 hours after HDT, the levels of melphalan in your body are very low and do not harm the reinfused stem cells. Your frozen stem cells are thawed and infused back into your bloodstream over a period of 1 to 4 hours. The chemical used to keep stem cells fresh has a garlic smell – you may even experience the taste of garlic.
Engraftment
Engraftment is the process by which the reinfused stem cells migrate from the bloodstream to your bone marrow, where they begin to produce new blood cells to replace the normal stem cells destroyed by HDT. You may receive SQ injections of growth factors to help stimulate your bone marrow to produce normal blood cells. Your stem cells will begin to grow back within 10 to 14 days after reinfusion, and your blood counts will begin to recover. You may receive transfusions if necessary.
Some transplant centers may require you to remain in the hospital on an inpatient basis after the reinfusion, and some centers have facilities nearby where you may stay while being monitored daily at the hospital on an outpatient basis. The length of stay varies patient-to-patient but is usually around 2 to 3 weeks. If you live near the transplant center, you may be able to sleep at home and come to the hospital for daily monitoring on an outpatient basis.
When you are discharged, your recovery will continue at home for about 2 to 4 months. Often, the most difficult time is waiting for the reinfused stem cells to engraft, for blood counts to return to safe levels, and for side effects to resolve. On some days you may feel better, and on other days you may feel too weak to do much more than sleep.
Frequent visits to the hospital may be required to monitor your progress. It is important to take things one day at a time. As your bone marrow produces new blood cells, symptoms resolve, the risk of serious infections is reduced, and transfusions may no longer be needed.
Depth of response
HDT with stem cell rescue delivers further improvement in the level of response achieved by induction therapy. More than half the time, partial response (PR) will be improved to either very good partial response (VGPR) or complete response (CR). The ultimate goal of HDT with stem cell rescue is to eliminate all residual myeloma cells that have not been killed during induction therapy.
Consolidation therapy
Consolidation therapy is treatment that may be given after ASCT to further deepen response, usually with the same drug regimen used for induction. Several protocols in current clinical practice include additional cycles of induction therapy after ASCT and prior to commencing maintenance therapy.
Maintenance therapy
Maintenance therapy is treatment that may be given after ASCT to prolong response. Currently, Revlimid is the only myeloma treatment approved by the FDA for maintenance after an ASCT. Multiple clinical trials have reported higher rates of PFS and OS in patients who received Revlimid as maintenance therapy post-ASCT (vs. placebo as maintenance therapy), regardless of the depth of response following ASCT.
There is a trend of more frequent use of “doublet” (2-drug) maintenance therapy regimens, especially in patients with higher-risk myeloma who may benefit from a more intense maintenance therapy. Post-ASCT maintenance therapy remains an area of study and data is evolving.
A 2014 meta-analysis of 3,218 patients in 7 clinical trials showed that an increase in second primary malignancies (SPM) could arise from the use of Revlimid in combination with melphalan. There has been no increase in SPMs reported among relapsed or refractory patients treated with Revlimid in the absence of an alkylating agent .
Given the advantages and potential risks of post-ASCT maintenance therapy with Revlimid, discuss with your doctor your individual risk factors and your response to ASCT before making any decision.
The role of tandem ASCT
ASCT can be performed once (a “single” autologous transplant) or twice (“double” or “tandem” autologous transplants). Tandem ASCTs are usually done with an interval of 3 to 6 months between the two transplants. Tandem transplantation for myeloma has become less common due to the emergence of effective novel therapies.
The role of a second ASCT
A second ASCT is an option for patients with relapsed myeloma if they achieved response of at least an 18-month duration following their first ASCT. A second ASCT appears to be beneficial for some patients, and this is one of the reasons that enough stem cells for two ASCTs may be collected in advance of the first transplant.
Possible side effects of ASCT
Side effects are a possibility with every type of medical treatment or procedure. Each patient reacts differently at each step of the ASCT process. No two patients share exactly the same side-effect profile. Following HDT with stem cell rescue, common potential side effects include nausea, mouth sores, hair loss, infection, fatigue, diarrhea, and skin rash.
The appropriate management of side effects is one of the reasons why it is so important to have your ASCT at a transplant center where the doctors, nurses, and allied healthcare professionals have performed the ASCT procedure many times on many myeloma patients. Such a team is more likely to have the expertise to care for each individual patient’s needs.
Until engraftment of the infused stem cells takes place, patients are very susceptible to developing infections, which can cause serious complications or be potentially life-threatening. Even a minor infection like the common cold can lead to complications because the body’s immune system is weakened by the effects of HDT. To protect the patient and prevent infection, the following supportive care measures may be required:
¡ Antibiotics to help prevent infection.
¡ Visitors may be asked to wash their hands, and wear masks and rubber gloves.
¡ Fresh fruits, vegetables, and flowers may be prohibited from the patient’s room as these can carry infectious agents such as bacteria and fungi.
If infection or fever occurs, the patient may be given an intravenous (IV) infusion of antibiotics into the vein.
Life after ASCT
Data from the Health Resources and Services Administration (HRSA) demonstrate that 99.1% of myeloma patients in the U.S. are alive at 100 days following ASCT.
After your ASCT, you will need to rely upon your medical team as well as on the support of a care partner. It is not uncommon for patients to experience a loss of the sense of independence, while at the same time experiencing feelings of isolation, depression, and helplessness. Patients and their care partners may consider seeking assistance from a trained counseling professional. There may also be benefits to participating in patient support groups either in-person or virtually.
On average, it takes 3 to 6 months to recover from an ASCT. By this time, your bone marrow will be producing healthy blood cells and your immune system will once again be able to fight infection. Your hair will grow back,
but some foods that tasted good before your ASCT may no longer taste good. For some patients, it may take 6 months or longer after ASCT to return to normal functioning or to a full-time job.
There will be bad days and good days, and they won’t necessarily come in that order. Patients may feel differently each day during the recovery process. Patients and their care partners must take it one day at a time.
Patients must always inform their myeloma doctor of everything they take in addition to the doctor’s prescribed treatment. Over-the-counter products, natural or synthetic supplements, and alternative or complementary therapies may have unanticipated effects and be harmful to a patient with myeloma.
Vaccination and immunization
Vaccination is the act of introducing a vaccine into a body to produce protection from a specific disease. Immunization is the process by which a body becomes protected against that disease through vaccination.
During HDT that is part of the ASCT process, patients lose the immunity they had acquired from their previous vaccinations. Re-vaccination after ASCT is crucial to rebuilding the immune system. You and your doctor must agree on a set schedule for your re-immunization after ASCT in accordance with your local guidelines (e.g., re-vaccination should take place between 6 and 12 months after ASCT).
ASCT in clinical trials
A clinical trial is a medical research study with people who volunteer to test scientific approaches for preventing, detecting, diagnosing, or treating cancer, or to answer scientific questions. A clinical trial is launched only after laboratory studies have demonstrated the potential of a treatment or procedure to be more effective and/or less harmful than previously existing methods.
The goal of a clinical trial is to improve patient care. If you have myeloma and are considering participation in a clinical trial, it is important to discuss with your doctor all the potential risks and benefits in your particular case.
Many clinical trials have investigated the role of ASCT in myeloma. The following are only three of the key studies that produced important data:
The IFM2009 clinical trial
This trial compared patients receiving ASCT in frontline therapy vs. deferring ASCT until disease relapse. Study patients received induction therapy with Velcade + Revlimid + dexamethasone [ VRd] with or without high-dose
melphalan, plus 12 months of maintenance therapy with Revlimid. PFS was longer in patients who underwent ASCT, but long-term follow-up demonstrated no difference in OS.
Nearly 80% of the study patients in the non-transplant group underwent transplant at first relapse, demonstrating that many patients have the option of deferring their ASCT. The final analysis of this study also confirmed the predictive value of MRD in myeloma; patients who achieved MRDnegativity had similar survival rates whether or not they underwent ASCT.
The DETERMINATION clinical trial
This study was similar to the IFM2009 clinical trial in comparing VRd alone to VRd + ASCT, followed by indefinite Revlimid until disease relapse. Again, PFS was significantly prolonged in the VRd + ASCT group, approximately 21 months longer than in the non-transplant group.
This outcome was even more pronounced in patients with high-risk disease. However, the OS was the same in each study group. Less than 30% of patients in the non-transplant group underwent ASCT at disease relapse. This study continues to note the benefit of transplant in PFS but not with OS.
The MIDAS clinical trial
The Minimal Residual Disease Adaptive Strategy (MIDAS) study used a novel quadruplet (4-drug) combination therapy of Sarclisa® (isatuximab) + Kyprolis® (carfilzomib) + Revlimid + dexamethasone [Isa-KRd] for 6 Cycles, and then assessed MRD status.
Patients who achieved MRD-negativity were randomized either to continuing with the Isa-KRd quadruplet or to having a single ASCT. There was no difference in the short-term outcomes between these two groups, perhaps suggesting that patients who achieve MRD-negativity may not need a transplant.
Patients who did not achieve MRD-negativity were randomized to receive either one transplant or two transplants. Again, there was no significant difference in outcomes between these groups, suggesting that a double ASCT may not provide any more benefit than a single ASCT. This modern clinical trial is particularly important because it used a quadruplet drug combination and MRD guidance in its design.
Finding a study to match your needs
A clinical trial may give you access to treatment that is not yet available outside of a study. If you are interested in participating in a clinical trial, it is essential to discuss with your doctor all the potential risks and benefits in your particular case.
To help with personalized support for exploring clinical trial options across the U.S., the IMF has partnered with SparkCures. Visit myeloma.org/sparkcures or contact the IMF InfoLine for more informationn.
The U.S. government maintains the website clinicaltrials.gov, an online database of thousands of research studies from around the world. You may wish to also explore this resource. However, the U.S. government does not review or approve the safety and science of all the studies listed on this website.
For more information about what’s involved in study participation, read the IMF’s publication Understanding Clinical Trials in Myeloma.
Other types of transplants
ASCT is the type of transplant used most frequently in myeloma. The patient’s own stem cells are collected from the bloodstream, not from the bone marrow. After HDT, these stem cells are returned to the patient to begin producing new blood cells.
Because ASCT uses the patient’s own stem cells, it is extremely rare for the person to develop graft-versus-host disease (GVHD), an immune-related reaction that may affect the skin (rashes), the liver, or the gastrointestinal (GI) tract. If GVHD does occur after an autologous transplant in myeloma, it is usually treatable.
Bone marrow transplant
An autologous transplant with stem cells collected from a patient’s bone marrow, not from a patient’s bloodstream. Bone marrow transplantation is used infrequently in myeloma because ASCT is preferred, but it may be considered if stem cells are not able to be collected from the bloodstream.
Allogeneic (allograft) transplant
Rarely used in myeloma, this type of transplant uses stem cells or bone marrow collected not from the patient, but from a donor who has been determined to be a compatible match with a recipient by means of a human leukocyte antigen (HLA) blood test. Donor cells are infused into the patient after the patient undergoes HDT. Unfortunately, while the donor’s immune system cells recognize the recipient’s myeloma cells as foreign and attack them, the donor’s cells also attack other tissues in the recipient’s body, causing GVHD, an immune-related reaction of the donor’s tissue against the recipient’s tissue. GVHD may cause complications or may even be fatal.
RIC allogeneic transplant
The reduced-intensity conditioning (RIC) allogeneic transplant is sometimes called a “mini-allo.” For myeloma, a mini-allo is a safer technique than a
“full” allogeneic transplant because it uses less intense chemotherapy. RIC transplant is usually performed within 180 days after a standard ASCT.
Syngeneic transplant
An allogeneic transplant where bone marrow or stem cells from one identical twin sibling (donor) are infused into the other identical twin (recipient).
Matched unrelated donor (MUD) transplant
An allogeneic transplant where stem cells are genetically matched to the patient but are not from a donor who is a family member. In myeloma, this type of transplant carries a high risk of GVHD and is rarely used.
Umbilical cord stem cell transplant
An allogeneic transplant where stem cells are harvested from multiple umbilical cords of newborns in order to obtain enough stem cells for an adult transplant. In myeloma, this type of transplant carries a high risk of GVHD and is rarely used.
In closing
This booklet is not meant to replace the advice of your doctors and nurses who are best able to answer questions about your specific healthcare management plan. The IMF intends only to provide you with information that will guide you in discussions with your healthcare team.
To help ensure a good quality of life through effective treatment, you must play an active role in your own medical care. We encourage you to visit myeloma.org for more information and to join the Myeloma Knowledge Platform at myprofile.myeloma.org.
To receive the most up-to-date information about myeloma in a caring and compassionate manner, call the IMF InfoLine at 1.818.487.7455, email InfoLine@myeloma.org, or visit mmsm.link/infoline to schedule a convenient time to talk with an IMF InfoLine Coordinator.
To get answers to your questions without having to wait, ask Myelo® anytime 24/7 at myeloma.org. This generative AI assistant is designed to help you find the right resources.
Use the hyperlinks and web addresses included in this publication for quick access to a variety of resources. Sign up at subscribe.myeloma.org for our quarterly journal Myeloma Today and weekly e-newsletter Myeloma Minute, as well as alerts about IMF news, events, and actions.
Founded in 1990, the International Myeloma Foundation (IMF) is the world’s leading organization dedicated to multiple myeloma. The IMF is steadfast in its mission to improve the quality of life of myeloma patients while working toward prevention and a cure. The IMF serves people affected by myeloma at every stage of the disease.
The IMF combines world-class research, trusted education, global advocacy, and direct support. A cornerstone of this work is the IMF International Myeloma Working Group® (IMWG®), comprised of more than 350 renowned researchers and clinicians who establish the guidelines that shape how myeloma is diagnosed, treated, and managed worldwide.
The IMF ensures that scientific advances translate into better care and outcomes. Through the IMF InfoLine, educational programs, a global network of support groups, the 24/7 generative-AI myeloma assistant Myelo®, and our advocacy for healthcare access, the IMF helps people living with myeloma and their care partners navigate diagnosis and survivorship.
The IMF is driven by its vision of a world where every myeloma patient can live life to the fullest, unburdened by the disease.